
Submitted:
19 January 2026
Posted:
20 January 2026
You are already at the latest version
Abstract
Although Gibbons et al. (2025) found that fear and sleep deprivation combined to predict unique variance in 5 out of 6 everyday and heroic courage measures, those measures either measured willingness to engage in courageous behaviors or fear when engaging in these behaviors, as suggested by the revised 20-item Woodard Pury Courage Scale (R-WPCS-20). However, most courage definitions involve risky behaviors considered courageous that elicit fear, which means that fear, when willing to engage in risky/courageous behaviors, indicates courage. Conversely, fear when unwilling to engage in risky/courageous behaviors indicates cowardice. The current study used the data from 256 participants in the Gibbons et al. study using the R-WPCS-20 to combine the ratings for willingness to engage in 20 risky behaviors and fear to engage in each of those behaviors into 20 courage ratings. Specifically, 3 was subtracted from each of the willingness ratings, ranging from 1 (low) to 5 (high), and multiplied by the fear rating, ranging from 1 (no fear) to 5 (high fear), resulting in 20 combined courage measures ranging from -10 (high cowardness) to 10 (high courage). The 20 combined ratings loaded well onto a single factor of courage with high factor loadings (the lowest factor loading was .764) and a Cronbach’s alpha of .99, demonstrating excellent interitem reliability. The results showed that fear/anxiety interacted with 2 measures of sleep (hours and poor sleep quality) to predict the single measure of courage that combined willingness to engage in courageous behaviors and fear when engaging in them, which clearly emphasized the contribution of fear in defining and predicting courage.
Keywords:
courage
; anxiety
; fear
; sleep quality
; quantity
1. Introduction
Everyone wants their actions to be considered courageous, but such displays are uncommon because they threaten survival as risks, and they are scary. In fact, the courage literature has defined courage as risky behavior (Norton & Weiss, 2009; Rachman, 2004) that elicits fear (Rate, 2010; Rorty, 1986), and behaviors may not be considered courageous unless they elicit fear (Gal & Ruckers, 2018). With this thought in mind, we consider Gibbons et al. (2025), who recently found that fear and sleep deprivation combined to account for unique variance in 5 of 6 courage measures on the revised Woodard Pury Courage Scale-20 (R-WPCS-20) that measured willingness to engage in courageous acts and fear to engage in these actions. In following the guidelines of the scale they revised, these researchers did not combine willingness to engage in courageous acts with fear to engage in these acts, even though both of these two factors are critical components of courage. Therefore, the current study reanalyzed the data used in the Gibbons et al. study to create a courage measure that combined willingness to engage and fear when engaging, and we tested whether fear and sleep deprivation would combine to predict unique variance in this courage measure.
1.1. Risky Behaviors and Courage
As previously stated, courage is defined by risk (Lei et al., 2017; Wei et al., 2024) and Howard and Alipour (2014) found that courage was positively related to risk-taking behaviors. According to several researchers, risky decision-making is a critical component of courage (Bowers et al., 2022; Hawkins & Morse, 2014; Norton & Weiss, 2009), which is enhanced by large rewards and high stakes (Wiseman & Levin, 1996). Gal and Rucker (2018) argued that high stakes often necessitate risky decisions irrespective of context, which may include investments, gambling, or even theft. The literature clearly substantiates the contention that risky decision-making is a pivotal component of courage, and it makes an additional point that large rewards increase risk, which means that they also enhance courage.
1.2. Fear/Anxiety and Courage
Fear is an important, hardwired instinct that enables all animals to avoid or escape danger and survive (Rate, 2010; Rorty, 1986). The relation between fear and courage, however, is very complex. On the one hand, fear reduces courage (Rorty, 1986; Schueller & Parks, 2014), and fear treatment interventions that reduce fear can improve demonstrations of courage (Eix, 2021). On the other hand, Gal and Rucker (2021) suggested that fear, along with purpose, agency, and availability, should be viewed as a precondition of courage, and other researchers defined courage as the willingness to act in the presence of fear (Norton & Weiss, 2009; Rachman, 2004; Rorty, 1986). Bowers et al. (2022) suggested that courage buffers individuals from feeling overly scared in very tense situations, which enhances performance. As examples of courageous individuals who perform well in stressful situations, Cox et al. (1983) observed 7 decorated bomb-disposal operators outperform 7 undecorated bomb-disposal operators and 7 civilian control participants on a stressful test, and McMillan and Rachman (1984) found similar results in paratroopers. Chockalingam and Norton (2018) suggested that true courage helps individuals act in ways that help them overcome their fears, and Chowkase et al. (2024) stated that fear is the driving factor in courage, making courage the act of overcoming fear.
The courage literature strongly suggests that fear is 1) a pivotal part of courage that reduces courage, which highlights a negative relation between fear and courage, but it also demonstrates that fear must be overcome to demonstrate courage, which indicates a positive relation between fear and courage. Although these two different findings seem contradictory, the resolution to this “problem” is simple, and it shines a light on a flaw in the WPCS-23 and the R-WPCS-20. Specifically, courage must be defined by both the risk/willingness to engage in a behavior and the fear experienced when engaging in that behavior, not one factor or the other. Consequently, high willingness to engage in a risky behavior that elicits high fear when engaging in it defines intense courage and low willingness to engage in a risky behavior that elicits high fear when engaging in it defines intense cowardice. Although the WPCS-23 and the R-WPCS-20 measure both willingness to engage in risky/courageous behaviors and the fear elicited when engaging in them, they do so separately, rather than combining these constructs into a single courage measure.
2. The Current Study
The current study was created to combine the willingness to engage in a risky/courageous behavior and the fear elicited when engaging in that behavior for each of the 20 items on the R-WPCS-20 and determine the best solution pertaining to the number of factors for those 20 items. The rating for the willingness to engage in a particular risky/courageous behavior and the fear to engage in that behavior was combined into a single measure (subtract 3 from the willingness score and multiply that difference by the fear to engage score) that ranged from -10 (High Cowardice) to +10 (High Courage) for all 20 items. In determining the best factor solution for the 20 combined items, we expected either a three-factor or a one-factor solution to best fit the data. The three-factor solution was expected to match the one demonstrated by Gibbons and colleagues with heroic courage, everyday courage, and overall (heroic and everyday) courage. The one-factor solution was expected to represent overall courage.
After determining the best factor solution for the 20 combined items from the R-WPCS-20 scale, we wanted to determine if sleep would combine with anxiety/fear to predict unique variance in the resulting courage measure(s), which was done successfully by Gibbons and colleagues. In addition to fear, sleep measures (sleep hours and poor sleep quality) combined with fear and predicted unique variance in 5 of the 6 courage measures in the study by Gibbons and colleagues. Sleep and the sleep by anxiety/fear interactions were expected to predict courage because research has shown that sleep deprivation can cloud judgment and critical thinking skills to increase risk (Csipo et al., 2021; Örsa et al., 2012; Wei et al., 2024), which is a critical component of courage. We expected fear/anxiety and sleep to combine and predict unique variance in the courage measure(s).
3. Method
3.1. Participants, Materials, Procedure, and Measures
The participants, materials, and procedure in the current study were the same as the ones used by Gibbons et al. (2025). The measures in the current study differed from the measures in the previous study. The new measure for each of the 20 items of the revised WPCS-20 was calculated by subtracting 3 from the original willingness scale for each item, which originally ranged from 1 (Low Willingness) to 5 (High Willingness). The difference ranged from -2 (Not Willing to Engage) to +2 (Very Willing to Engage), and it was multiplied by the fear/anxiety measure, which was the same one used by Gibbons and colleagues, and it ranged from 1 (Little Fear) to 5 (Very High Fear). The resulting product of the aforementioned measures created a combined courage measure for each item that ranged from -10 (High Cowardice) to +10 (High Courage).
4. Results
The 20 resulting, combined courage items from the R-WPCS-20 best loaded on a single factor, with the smallest factor loading being .764, with a Cronbach’s alpha of .99. Consequently, the 20 combined items were averaged to create a single measure of courage. The anxiety/fear, hours slept, poor sleep quality, and the anxiety/fear by hours slept interaction and the anxiety/fear x poor sleep quality interaction were placed in a stepwise multiple regression equation as predictors of the courage measure. The results of the stepwise regression Model 1 showed that the Fear/Anxiety x Hours of Sleep interaction, B = -0.111 (SE = 0.038), t(196) = -2.931, p = .004, negatively predicted courage and accounted for 4.2% of the variance in courage. The results of the stepwise regression Model 2 showed that the Fear/Anxiety x Hours of Sleep interaction, B = -0.199 (SE = 0.058), t(195) = -3.430, p < .001, negatively predicted courage, whereas the Fear/Anxiety x Poor Sleep Quality interaction, B = 0.333 (SE = 0.167), t(197) = 1.996, p = .047, positively predicted courage and accounted for 1.9% of the variance in courage, which meant that the two interactions together accounted for 6.1% of the variance in courage. The results showed that fear/anxiety interacted with two measures of sleep (hours and poor sleep quality) to predict a single measure of courage that combined willingness to engage in courageous behaviors and fear when engaging in them.
5. Discussion
The results of the current study demonstrated that combining the willingness to engage in risky/courageous behaviors and the fear when engaging in these behaviors across 20 items of the R-WPCS-20 produced a single measure of courage that ranged from fear and unwillingness to engage in risky/courageous behaviors (i.e., cowardice) to fear and willingness to engage in risky/courageous behaviors (courage). These results supported the concept that willingness to engage in risky/courageous acts and the fear when engaging in them should be combined to define and measure courage. In addition, the results showed that the Fear/Anxiety by Hours of Sleep interaction and the Fear/Anxiety by Poor Sleep Quality interaction negatively and positively predicted unique variance in the combined courage, respectively. These results supported the hypotheses and extended the work by Gibbons et al. (2025), which showed that fear/anxiety would combine with sleep measures to predict unique variance in courage.
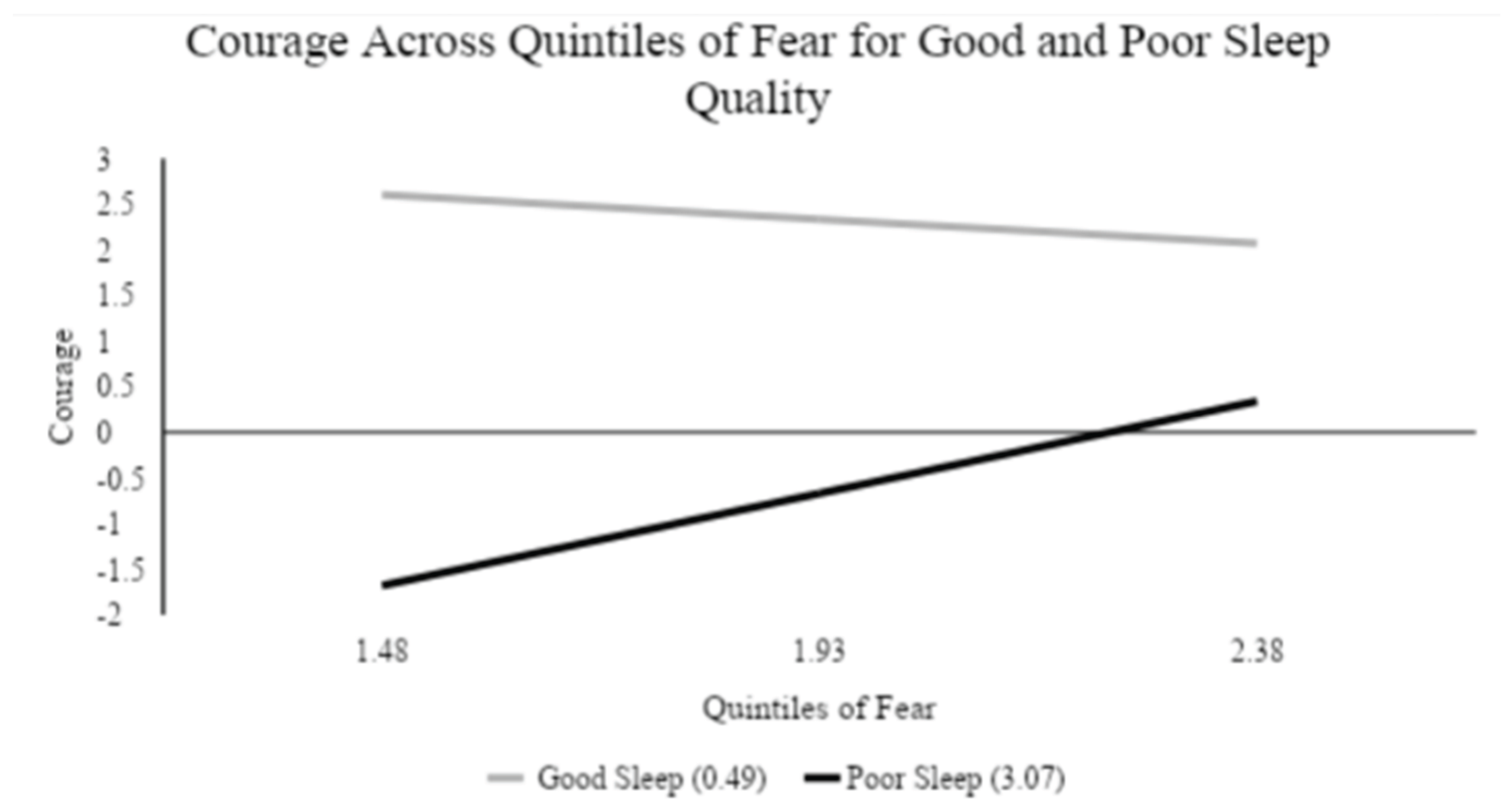
As for the specifics of the two interactions predicting the combined courage measure, Figure 1 and Figure 2 tell two very different stories. Figure 1 describes the two-way interaction in which sleep hours and fear/anxiety worked together to predict the combined courage measure. These results showed that courage decreased with fear for participants reporting low and high sleep hours, but it decreased less with fear for participants reporting low sleep hours than participants reporting high sleep hours. These findings suggest that poor sleep in the form of low sleep hours buffered the courage-decreasing effects of fear/anxiety. Figure 2 describes the two-way interaction in which sleep quality and fear/anxiety worked together to predict the combined courage measure. These results showed that courage decreased with fear for participants reporting good sleep quality, but it increased with fear/anxiety for participants reporting poor sleep quality. Therefore, fear/anxiety decreases courage in good sleep conditions, but increases courage in poor sleep conditions. Rather than merely buffering the reduction of courage produced by fear, poor sleep quality changes fear/anxiety into a courage enhancer.
Altogether, the results lead to several important conclusions. First, the results showed that courage can be sufficiently measured through a single measure using the two defining components of courage: risk (willingness to engage) and fear. This study was the first one to combine the two measures obtained on the revised Woodard Pury Courage Scale, the factor loadings were very high, and the Cronbach’s alpha level was nearly perfect. Second, sleep and fear/anxiety combined to predict unique variance in this combined measure, just as they combined to account for 5 out of 6 courage measures described by Gibbons et al. (2025). Third, the way sleep is measured produces very different results and interpretations about the way poor sleep combines with fear/anxiety to predict a combined courage measure that was created from willingness to engage in behaviors and fear from engaging in those behaviors.
The results of the current study are based on 245 mostly female (n = 162), young adult (18 to 28 years old) undergraduate students. Many psychology studies use sample characteristics that match the sample in the current study; a national average reported that psychology samples include 78% female undergraduate students and 71% female graduate psychology students (National Science Foundation, National Center for Science and Engineering Statistics, 2018). Nevertheless, future studies should replicate the findings in the current study with participants who report different characteristics. One striking fact that could have been important in affecting the results in the current study is that women report higher levels of sleep deprivation than men (Yaqoot et al., 2016). In addition, younger adults tend to be more vulnerable to the negative impact of sleep deprivation than older adults (Zitting et al., 2018), which could have influenced the results. In addition, most college students report feeling tired during the day between 3 and 5 days of the week (American College Health Association, 2025), which may be very different from adults with jobs who must push past their tiredness to perform sufficiently to stay employed. Alternatively, students may have more reason to be tired than adults with jobs. Regardless, participant characteristics could have influenced participant outcomes in the current study, so the results must be replicated with participants reporting different characteristics.
When future research does collect new data using the R-WPCS-20, courage can conveniently be calculated as six measures of courage, as it was in the Gibbons et al. (2025) study, or as a single courage measure, like it was in the current study, or it can be calculated in both ways. Future studies should also use the method for calculating courage in the current research with the WPCS-23 to examine whether it produces 23 individual measures that combine willingness to engage in behaviors and fear/anxiety when engaging in them and load onto a single measure of courage. Future research could also replicate the Gibbons et al. study and use all the overlapping and different items from the WPCS-23 and the R-WPCS-20, and then separate the items into the two different scales and compare how well sleep, fear/anxiety, and their interactions predict combined measures of courage from each scale. In addition, future research could use these scales to determine optimal levels of fear/anxiety, courage, and poor sleep to produce the highest levels of courage.
The R-WPCS-20 uses questions that most people can resonate with, such as, “I would meet my supervisor at work about a problem I believed was important.” However, the revised scale was patterned after the WPCS-23, which uses some questions that are not directly relevant to students and other university-aged participants. For example, participants should experience great difficulty imagining the scenario in which “I would have hidden Jewish friends during the time of the Holocaust” or “I would undergo physical pain and torture rather than tell political secrets.” Many people were not alive to not hide their Jewish friends during the Holocaust, and many people today may not believe in the Holocaust or realize that many of those individuals who hid their Jewish friends at that time were captured and killed. In other words, people today do not understand the high risk of such an action and they could not truly imagine such a situation, because they have no frame of reference from their own lives. Similarly, most people do not know political secrets that might lead to their torture. Consequently, participants are likely to overestimate their courage when answering such questions. Therefore, future research should adapt the scenarios on the WPCS-23 and the R-WPCS-20 to ensure that all the questions are relevant and current, so that students and non-students can provide honest and informed answers to questions based on scenarios that fit into a modern lens of experiences.
The issues with the WPCS-23 and the R-WPCS-20 also suggest that future research should employ behavioral risk scenarios in the lab to measure courage because they protect participants from getting physically hurt, but measure whether participants actually engage in scary/risky behaviors. For example, the distance between participants and creatures that inspire fear in many people (e.g., spiders) could be measured, as in the BAT spider procedure (e.g., Bevers et al., 2013; Norton & Weiss, 2009; Szymanski & O’Donahue, 1995). Participant engagement could be measured via distance to the feared creature and fear could be measured via heart rate, blood pressure, and respiration rate. A combined courage measure could then be calculated from engagement via distance and fear via the physiological metrics. Alternatively, participants’ willingness to take real risks could be measured in games in which participants win or lose money, which is done in the the Iowa Gambling Task (e.g., Brewers et al., 2013). These gambling tasks could include games against the house/computer (e.g., roulette, slot spins, black jack, poker) or socially interactive games (i.e., poker) and they could vary participants’ minimum risk levels.
Increases in minimum bet levels are expected to induce and increase fear, which could be measured via heart rate, blood pressure, and respiration rate, whereas participants’ willingness to continue playing and increased bet levels would gauge engagement. As with the willingness to engage and fear measures in the R-WPCS-20, a combined courage measure could be calculated that would involve fear and engagement and it would range from cowardice to courageousness. In both the approaching-a-feared-creature task and gambling task, the results should follow the same pattern as in the current study. Specifically, the combined courage measure should be negatively and positively predicted by the Fear/Anxiety by Sleep Hours interaction and the Fear/Anxiety by Poor Sleep Quality interaction, respectively.
Future research could use “act-out” scenarios as another way to measure courage because they require participants to immediately make behavioral decisions in a risky situation producing fear. These scenarios could require participants to demonstrate a willingness to engage in risky behaviors while experiencing fear (Norton & Weiss, 2009; Rachman, 2004; Rate, 2010; Rorty, 1986). The participants could then be rated on the degree they were willing to engage in the behavior by observers/confederates and they could rate the fear they experienced while engaging in that behavior. Participant willingness to engage and fear measures could be combined to create a single scale that would range from cowardice to courageousness. The “act-out” scenarios could be conducted in the laboratory and involve staged confrontations or behavioral approach tasks in which participants must step toward a fear-inducing stimulus. These observable interactions could be performed in front of one or two experimental confederates or larger groups composed of experimenters and/or participants.
As these social interactions would be much more immersive and natural than completing questionnaires, these methods would enhance the ecological validity of the combined courage measure concept and potentially yield a naturalistic index of courage. The main limitation of these act-out methods, however, is that they could elicit social anxiety, which is a different type of fear elicited by a different type of risk and danger that must be overcome to demonstrate courage (Bowers et al., 2022; Cox et al., 1983; McMilan & Rachman, 1984). As social anxiety would likely suppress approach behavior, it would need to be statistically controlled in any analyses predicting a combined measure of courage to avoid contaminating these analyses with social performance anxiety. Nevertheless, we would still expect the combined courage measure to be negatively and positively predicted by the Fear/Anxiety by Sleep Hours interaction and Fear/Anxiety by Poor Sleep Quality interaction, respectively.
Virtual Reality (VR) would offer a controlled alternative to the “act-out” scenarios that would not be influenced by social anxiety, because they do not need anyone to directly see the way they are behaving. Instead, this technology can create scenarios that are so immersive that they would effectively generate fear in anyone and make them feel like they were in real physical danger, even though they are essentially in a game (A. M. Gibbons, personal communication, December 11, 2025). For example, participants could be placed in a dark forest where someone or something is following them and the VR computer could measure participants’ willingness to engage behaviors via distances to fear-provoking stimuli in the depictions and participants’ heart rates, blood pressures, respiration, and oxygen flow could be assessed to evaluate fear.
As VR would depict risky, fear-provoking situations in which participants can engage or flee and demonstrate fear or not, the stage would be set to assess participant responses (action and fear) and create a combined measure of courage in conditions that meet the qualities to display courage as defined in the literature (Norton & Weiss, 2009; Rachman, 2004; Rate, 2010). An important control in these studies would be degree of immersion as people would vary on such measures even though these scenarios should produce generalizable effects across participants. After controlling for self-reported degree of immersion, we expect that the Fear/Anxiety by Sleep Hours interaction and Fear/Anxiety by Poor Sleep Quality interaction would negatively and positively predict the combined courage measure, respectively.
In summary, the willingness to engage and the fear when engaging in risky actions were successfully combined into a single measure of courage, and that measure was significantly predicted by two interactions that combined fear/anxiety with two different forms of sleep: sleep hours and poor sleep quality. These two interactions showed that fear/anxiety combined very differently with sleep hours than sleep quality to predict the combined measure of courage. Specifically, low sleep hours buffered the courage-decreasing effects of fear/anxiety slightly more than high sleep hours, whereas fear produced courage-enhancing and courage-increasing effects for poor sleep quality and good sleep quality, respectively. Future research should replicate and extend the current study by using the same materials employed in the current study, as well as different materials and procedures, to determine if the results generalize to different populations and methods. Everyone engages in risk, experiences situations that would or do elicit fear in many individuals, and spends some of their days recovering from poor sleep. However, courage occurs where the rubber meets the road because everyone is given a chance to act courageously, but only the few, the proud, the willing push past their fear and demonstrate courage. Although sleep deprivation seems to make courage a little more possible in scary circumstances, fear combines with risk (as measured via engagement) to define courage, and it combines with poor sleep to predict courage, which convincingly conveys the primary point of this paper that courage is not courage without fear.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
References
- American College Health Association (2025). American College Health Association-National College Health Assessment III: Undergraduate Student Reference Group Executive Summary Spring 2025. https://www.acha.org/wp-content/uploads/NCHAIIIb_ SPRING_2025_UNDERGRADUATE_REFERENCE_GROUP_INSTITUTIONAL_EXECUTIVE_SUM MARY.pdf.
- Bowers, C. A., Beidel, D. C., & Marks, M. R. (2022). Obstacles to mental health treatment: Similarities and differences among first responder groups. Journal of Community Safety and Well-Being, 7(2), 42-46.
- Chockalingam, M., & Norton, P. J. (2018). Facing fear-provoking stimuli: The role of courage and influence of task-importance. The Journal of Positive Psychology, 14(5), 603-613.
- Chowkase, A. A., Parra-Martínez, F. A., Ghahremani, M., Bernstein, Z., Finora, G., & Sternberg, R. J. (2024). Dual-process model of courage. Frontiers in Psychology, 15, 1376195, .
- Cox, D., Hallam, R., O’Connor, K., & Rachman, S. (1983). An experimental analysis of fearlessness and courage. British Journal of Psychology, 74(1), 107–117.
- Csipo, T., Lipecz A., Owens, C., Mukli, P., Perry, J. W., Tarantini, S., Balasubramanian, P., Nyúl-Tóth, Á., Yabluchanska. V., Sorond, F. A., Mikhail Kellawan, J., Purebl, G., Sonntag, W. E., Csiszar, A., Ungvari, Z., & Yabluchanskiy, A. (2021). Sleep deprivation impairs cognitive performance, alters task-associated cerebral blood flow and decreases cortical neurovascular coupling-related hemodynamic responses. Scientific Reports, 11(1), 20994.
- Eix, A. K. (2021). Calling on courage: The use of a courage intervention to increase engagement in exposure for specific fears (Order No. 28548495). [Doctoral Dissertation, Northwestern University]. Proquest Dissertations & Theses Global. https://cnu.idm.oclc.org/login?url=https://www.proquest.com/dissertations-theses/calling-on-courageuse- intervention-increase/docview/2572572795/se-2?accountid=10100.
- Gal, D., & Rucker, D. D. (2018). The loss of loss aversion: Will it loom larger than its gain? Journal of Consumer Psychology, 28(3), 497–516.
- Gal, D., & Rucker, D. D. (2021). Act boldly: Important life decisions, courage, and the motivated pursuit of risk. Journal of Personality and Social Psychology, 120(6), 1607.
- Hawkins, S. F., & Morse, J. (2014). The praxis of courage as a foundation for care. Journal of Nursing Scholarship, 46(4), 263-270.
- Howard, M. C., & Alipour, K. K. (2014). Does the courage measure really measure courage? A theoretical and empirical evaluation. The Journal of Positive Psychology, 9(5), 449-459,.
- Lei, Y., Wang, L., Chen, P., Li, Y., Han, W., Ge, M., & Yang, Z. (2017). Neural correlates of increased risk-taking propensity in sleep-deprived people along with a changing risk level. Brain Imaging and Behavior, 11(6), 1910-1921.
- Lejuez, C. W., Read, J. P., Kahler, C. W., Richards, J. B., Ramsey, S, E., Stuart, G. L., Strong, D. R., & Brown, R. A. (2002). Evaluation of a behavioral measure of risk taking: The Balloon Analogue Risk Task (BART). Journal of Experimental Psychology: Applied, 8(2), 75-84.
- McMillan, T. M., & Rachman, S. J. (1988). Fearlessness and courage in paratroopers undergoing training. Personality and Individual Differences, 9(2), 373–378.
- National Science Foundation, National Center for Science and Engineering Statistics. (2018). Doctorate recipients from U.S. universities: 2017 (Special Report NSF 19-301). https://ncses.nsf.gov/pubs/nsf19301.
- Norton, P. J. & Weiss, B. J. (2009). The role of courage on behavioral approach in a fear-eliciting situation: A proof-of-concept pilot study. Journal of Anxiety Disorders, 23(2), 212-217.
- Rachman, S. J. Fear and courage. Behavior Therapy 1984, 15(1), 109–120. [Google Scholar] [CrossRef]
- Rachman, S. J. Fear and courage: A psychological perspective. Social Research: An International Quarterly 2004, 71(1), 149–176. [Google Scholar] [CrossRef]
- Rate, C. R. (2010). Defining the features of courage: A search for meaning. In C. L. S. Pury & S. J. Lopez (Eds.), The psychology of courage: Modern research on an ancient virtue (pp. 47-66). American Psychological Association.
- Rorty, A. O. The two faces of courage. Philosophy 1986, 61(236), 151–171. [Google Scholar] [CrossRef]
- Schueller, S.; Parks, A. C. The Wiley Blackwell Handbook of Positive Psychology Interventions. In John Wiley & Sons; 2014. [Google Scholar] [CrossRef]
- Szymanski, J., & O’Donahue, W. (1995). Fear of spiders questionnaire. Journal of Behavior Therapy and Experimental Psychiatry, 26(1), 31-34.
- Wei, X.; Ma, J.; Liu, S.; Li, S.; Shi, S.; Guo, X.; Liu, Z. The effects of sleep deprivation on risky decision making. Psychonomic Bulletin & Review 2024. [Google Scholar] [CrossRef]
- Wiseman, D. B.; Levin, I. P. Comparing risky decision making under conditions of real and hypothetical consequences. Organizational Behavior and Human Decision Processes 1996, 66(3), 241–250. [Google Scholar] [CrossRef]
- Woodard, C. R.; Pury, C. L. S. The construct of courage: Categorization and measurement. Consulting Psychology Journal: Practice and Research 2007, 59(2), 135–147. [Google Scholar] [CrossRef]
- Yaqoot, F., Doi, S. A. R., Najman, J. M., & Mamun, A. A. (2016). Exploring gender differences in sleep quality of young adults: Findings from a large population study. Clinical Medicine & Research, 14(3-4), 138-144.
- Zitting, K. M., Münch, M. Y., Cin, S. W., Wang, W., Wong, A., Ronda, J. M., Aeschback, D., Czeisler, C. A., & Duffy, J. F. (2018). Young adults are more vulnerable to chronic sleep deficiency and recurrent circadian disruption than older adults. Scientific Reports, 8(1), 11052.
Figure 1.
The combined courage measure across low and high sleep hours as well as low, medium, and high fear/anxiety levels.
Figure 1.
The combined courage measure across low and high sleep hours as well as low, medium, and high fear/anxiety levels.
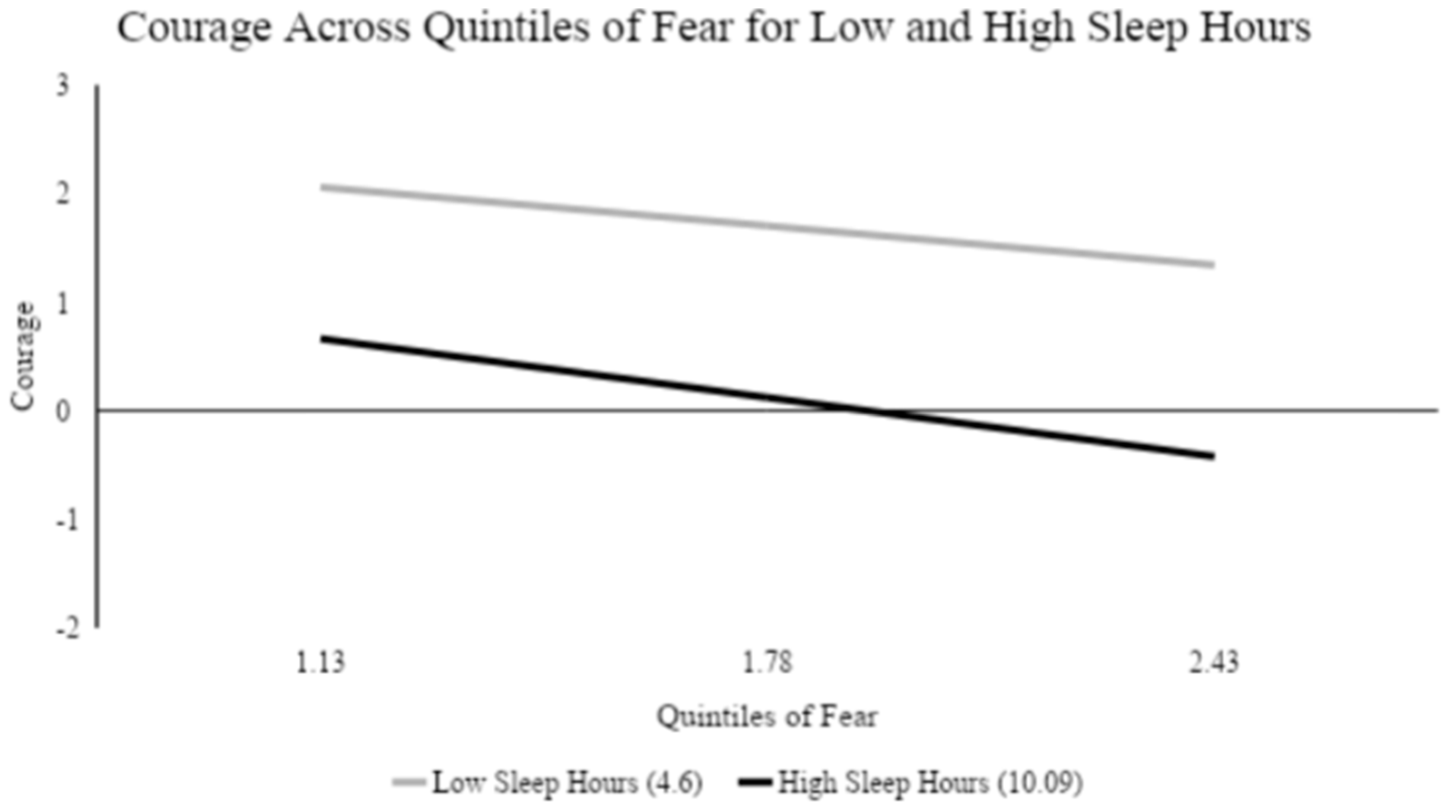
Figure 2.
The combined courage measure across low and high sleep quality as well as low, medium, and high fear/anxiety levels.
Figure 2.
The combined courage measure across low and high sleep quality as well as low, medium, and high fear/anxiety levels.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



