Submitted:
18 December 2025
Posted:
19 December 2025
You are already at the latest version
Abstract
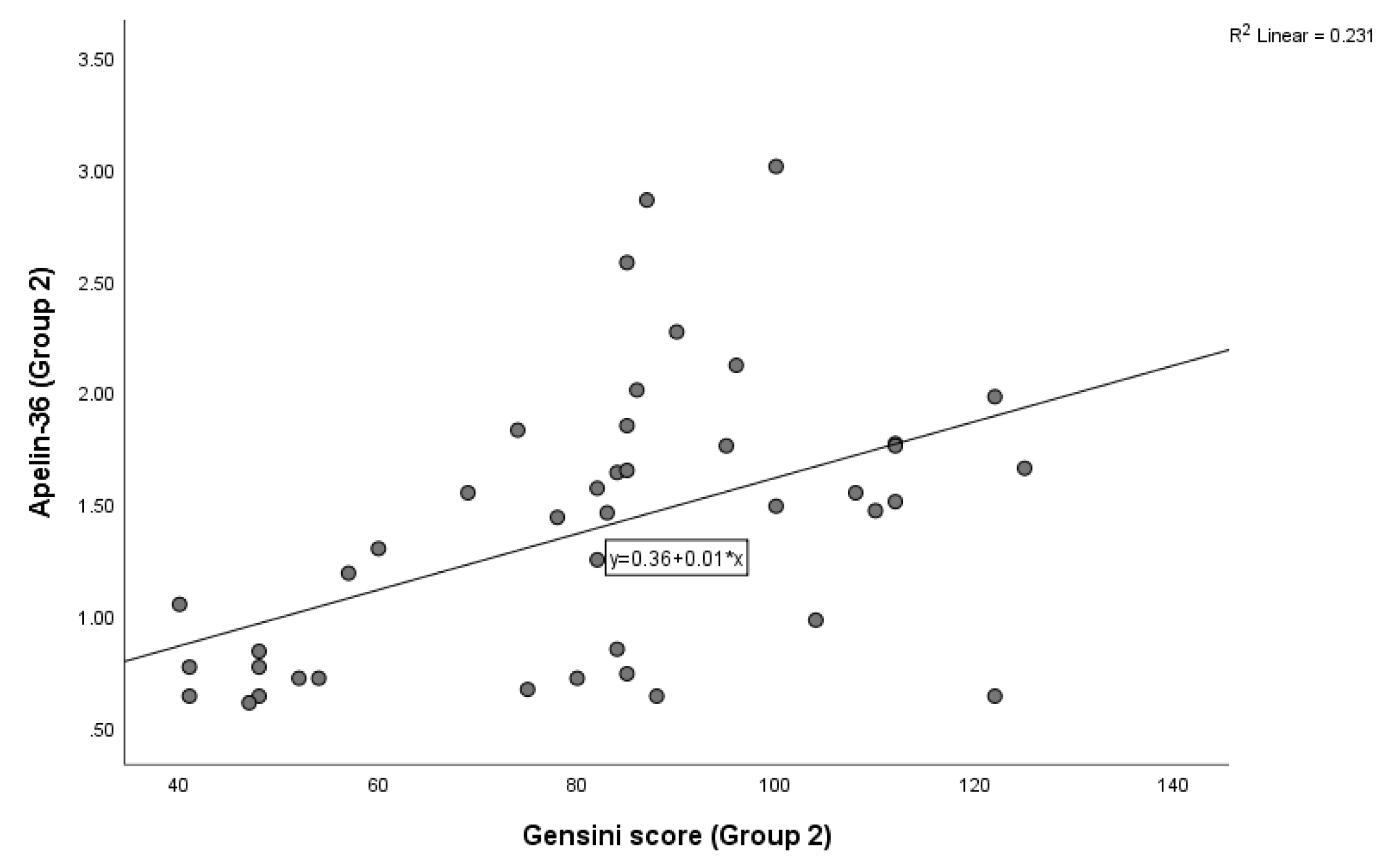
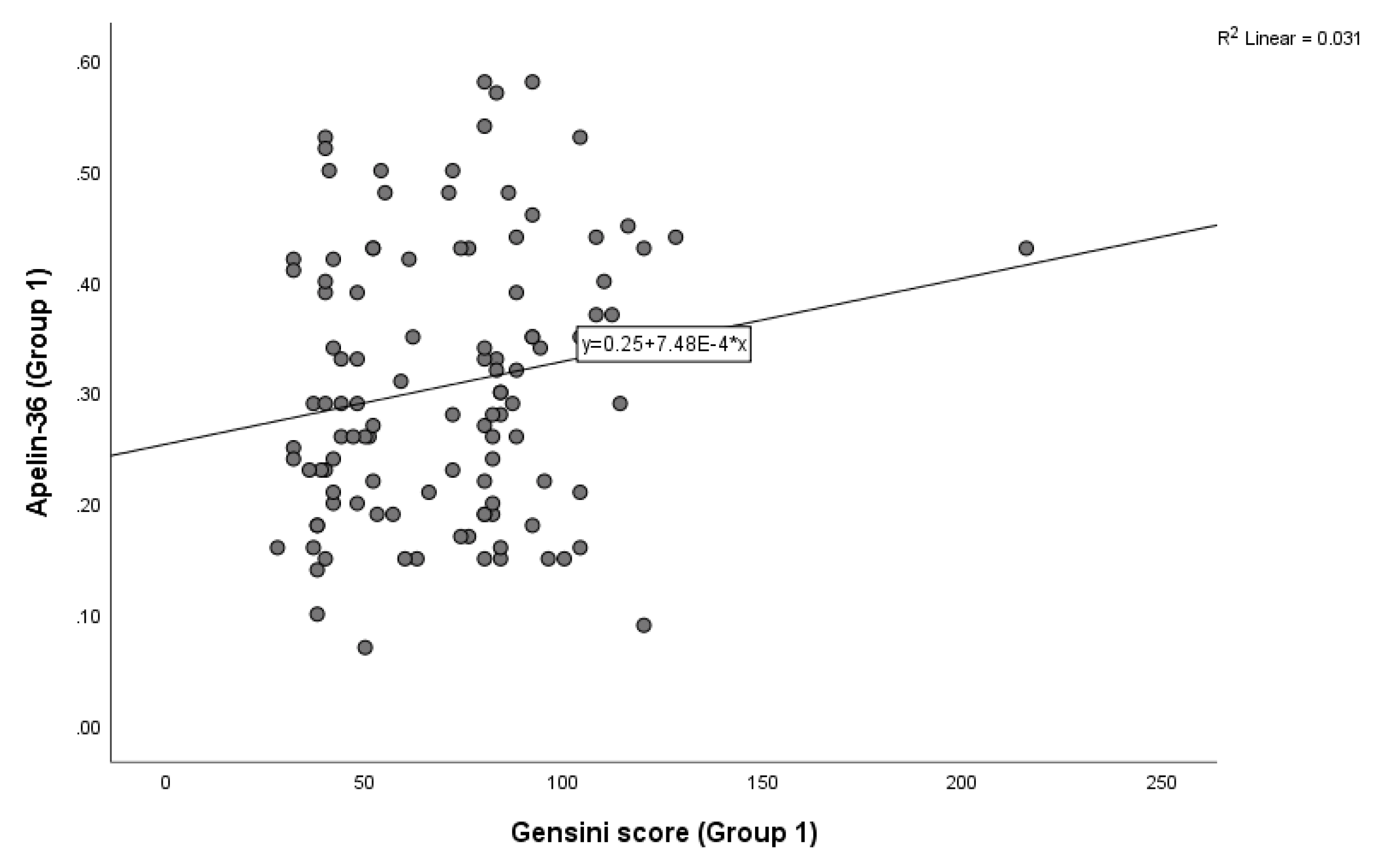
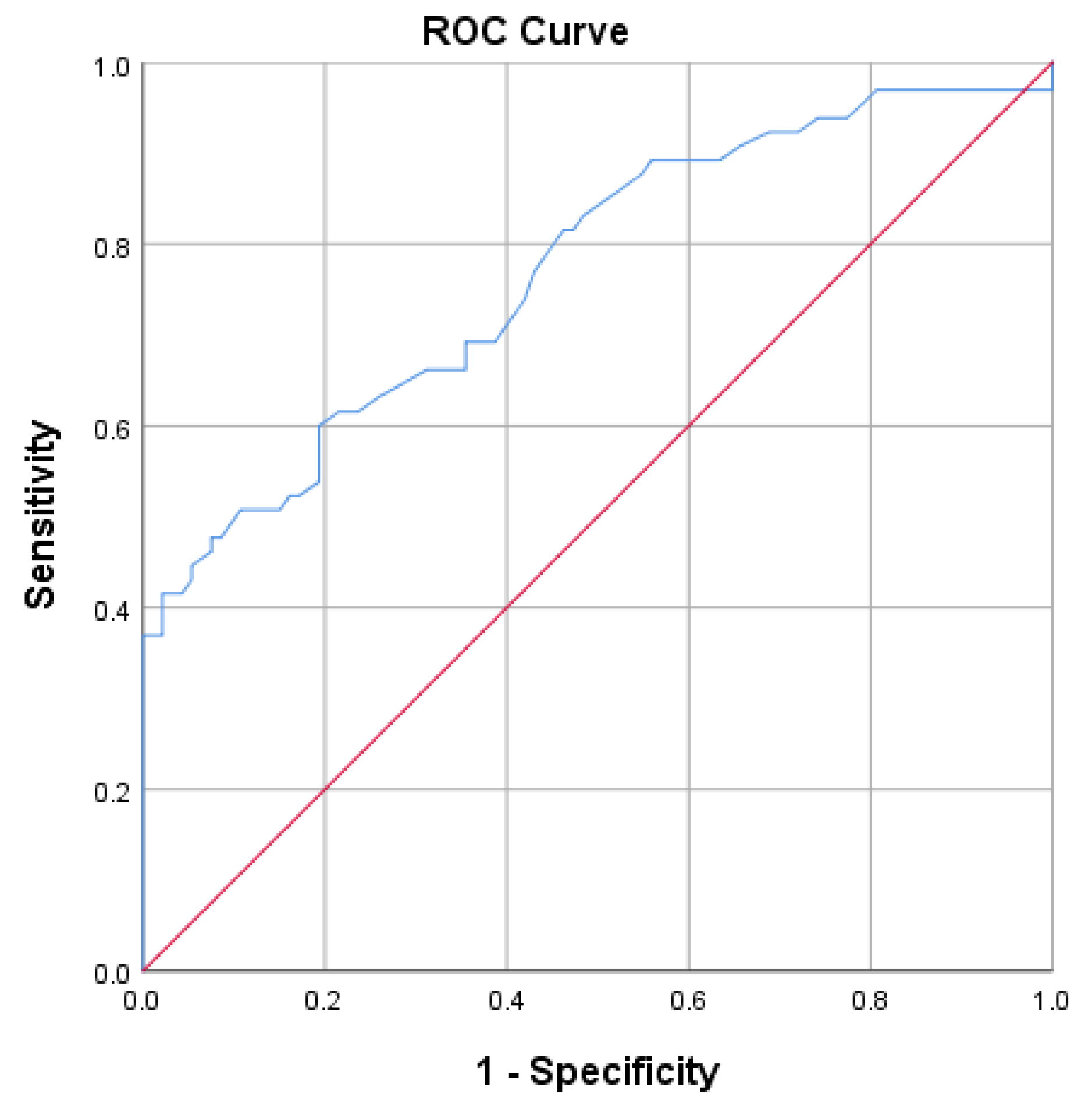
Background: Apelin-36 may be used to identify patients with ST-segment elevation myocardial infarction (STEMI) who are at risk for the no-reflow phenomenon. Patients presenting with STEMI were evaluated and stratified according to their apelin-36 levels. Methods: In this study, 161 patients presenting with STEMI within 12 hours of symptom onset and undergoing primary percutaneous coronary intervention (pPCI) were enrolled. Biochemical parameters, including apelin-36, troponin T, creatine kinase (CK), the MB fraction of creatine kinase (CK-MB), total cholesterol, triglycerides, and other routine laboratory parameters, were measured. Blood samples for apelin-36 measurement were collected prior to PCI, centrifuged to obtain serum, and preserved at -80⁰C until being assayed. Two-dimensional echocardiography was performed in all patients. Thereafter, patients were divided into two groups according to their level of Apelin-36. Results: Among the 161 consecutive STEMI patients, 115 (71.42%) had Apelin-36 levels ≤0.58ng/mL (group 1), whereas 46 (28.57%) had Apelin-36 levels >0.58ng/mL (group 2). In total, 51 (31.67%) STEMI patients experienced no-reflow phenomenon after PCI: 29 (18.01%) patients with apelin-36 ≤ 0.58ng/mL and 22 (13.66%) with a value > 0.58ng/mL (p < 0.001). In terms of Gensini score, the mean value in group 1 was (70.29 (±28.76), while in group 2, it was 81.95 (±23.82) (p=0.004). Overall, a positive correlation between apelin-36 and Gensini score was observed in both groups using Kendall’s correlation analysis (group 1: Figure 2, p=0.05; group 2: Figure 2, p<0.0001). Binary logistic regression analysis identified apelin-36 and diabetes mellitus as significant predictors at the 5% level, with p-values of 0.045 and 0.036, respectively. Patients with apelin-36 levels ≤ 0.58ng/mL had troponin T levels of 290.0 (8.5-9510.0), while those with a value > 0.58ng/mL had troponin T levels of 132.15 (9.4-5190.0) (p < 0.012). The receiver operating characteristics (ROC) curve of apelin-36 was used to plot the true positive rate against the false positive rate at different cut-off points, with AUC=0.67 (95% CI, 0.57-0.76), and the cut-off value for apelin-36 was 0.58ng/mL, with p=0.001. Conclusions: Significant associations were observed between apelin-36 and no-reflow phenomenon in patients with STEMI. An apelin-36 cut-off value of 0.58ng/mL, measured at admission, could be used to identify patients who were at increased risk of no-reflow phenomenon/reperfusion injury.
Keywords:
1. Introduction
2. Methods
2.1. Study Design
2.2. Statistical Analysis
3. Results

| Parameter | OR | 95% CI | P-value |
|---|---|---|---|
| BMI (kg/m2) | 0.89 | 0.69-1.16 | 0.41 |
| Diabetes mellitus (n/%) | 0.07 | 0.007-0.85 | 0.036 |
| Smoking (n/%) | 4.96 | 0.76-32.10 | 0.09 |
| Apelin-36 (ng/mL) | 0.038 | 0.002-0.92 | 0.045 |
| Creatine kinase-MB (U/L) | 1.003 | 0.99-1.01 | 0.57 |
| Creatine kinase (U/L) | 0.99 | 0.99-1.00 | 0.15 |
| Troponin T (pg/mL) | 1.00 | 1.00-1.001 | 0.16 |
4. Discussion
5. Conclusions
Disclosure statement
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hu, G.; Wang, Z.; Zhang, R.; Sun, W.; Chen, X. The role of apelin/apelin receptor in energy metabolism and water homeostasis: a comprehensive narrative review. Front Physiol. 2021, 12, 632886. [Google Scholar] [CrossRef]
- Tatemoto, K.; Hosoya, M.; Habata, Y.; Fujii, R.; Kakegawa, T.; Zou, M.X.; Kawamata, Y.; Fukusumi, S.; Hinuma, S.; Kitada, C.; et al. Isolation and characterization of a novel endogenous peptide ligand for the human APJ receptor. Biochem Biophys Res Commun. 1998, 251, 471–476. [Google Scholar] [CrossRef]
- Wang, W.; Shen, M.; Fischer, C.; Basu, R; Hazra, S.; Couvineau, P.; Paul, M.; Wang, F.; Toth, S.; Mix, D.S.; et al. Apelin protects against abdominal aortic aneurysm and the therapeutic role of neutral endopeptidase resistant apelin analogs. Proc Natl Acad Sci. 2019, 116, 13006–13015. [Google Scholar] [CrossRef] [PubMed]
- McKinnie, S.M.; Fischer, C.; Tran, K.M.; Wang, W.; Mosquera, F.; Oudit, G.Y.; Vederas, J.C. The metalloprotease neprilysin degrades and inactivates apelin peptides. Chembiochem. 2016, 17, 1495–1498. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; McKinnie, S.M.; Farhan, M.; Paul, M.; McDonald, T.; McLean, B.; Llorens-Cortes, C.; Hazra, S.; Murray, A.G.; Vederas, J.C.; et al. Angiotensin-converting enzyme 2 metabolizes and partially inactivates pyr-apelin-13 and apelin-17: physiological effects in the cardiovascular system. Hypertension. 2016, 68, 365–377. [Google Scholar] [CrossRef]
- Kawamata, Y.; Habata, Y.; Fukusumi, S.; Hosoya, M.; Fujii, R.; Hinuma, S.; Nishizawa, N.; Kitada, C.; Onda, H.; Nishimura, O.; et al. Molecular properties of apelin: tissue distribution and receptor binding. Biochim Biophys Acta 2001, 1538, 162–171. [Google Scholar] [CrossRef] [PubMed]
- Read, C.; Nyimanu, D.; Williams, T.L.; Huggins, D.J.; Sulentic, P.; Macrae, R.G.; Yang, P; Glen, R.C.; Maguire, J.J.; Davenport, A.P. International union of basic and clinical pharmacology. CVII. Structure and pharmacology of the apelin receptor with a recommendation that elabela/toddler is a second endogenous peptide ligand. Pharmacol Rev. 2019, 71, 467–502. [Google Scholar] [CrossRef]
- Kleinz, M.J.; Davenport, A.P. Immunocytochemical localization of the endogenous vasoactive peptide apelin to human vascular and endocardial endothelial cells. Regul Pept. 2004, 118, 119–125. [Google Scholar] [CrossRef]
- Medhurst, A.D.; Jennings, C.A.; Robbins, M.J.; Davis, R.P.; Ellis, C.; Winborn, K.Y.; Lawrie, K.W.; Hervieu, G.; Riley, G.; Bolaky, J.E.; et al. Pharmacological and immunohistochemical characterization of the APJ receptor and its endogenous ligand apelin. J Neurochem. 2003, 84, 1162–1172. [Google Scholar] [CrossRef]
- Perjes, A.; Skoumal, R.; Tenhunen, O.; Konyi, A.; Simon, M.; Horvath, I.G.; Kerkelä, R.; Ruskoaho, H.; Szokodi, I. Apelin increases cardiac contractility via protein kinase Cε-and extracellular signal-regulated kinase-dependent mechanisms. PloS one 2014, 9, e93473. [Google Scholar] [CrossRef]
- Tang, L.; Qiu, H.; Xu, B.; Su, Y.; Nyarige, V.; Li, P.; Chen, H.; Killham, B.; Liao, J.; Adam, H.; et al. Microparticle mediated delivery of apelin improves heart function in post myocardial infarction mice. Circ Res. 2024, 135, 777–798. [Google Scholar] [PubMed]
- Krasniqi, X.; Berisha, B.; Gashi, M.; Koçinaj, D.; Jashari, F.; Vincelj, J. Influence of apelin-12 on troponin levels and the rate of MACE in STEMI patients. BMC cardiovasc Disord. 2017, 17, 195. [Google Scholar] [CrossRef] [PubMed]
- Pi, Y.; Zhang, D.; Kemnitz, K.R.; Wang, H.; Walker, J.W. Protein kinase C and A sites on troponin I regulate myofilament Ca2+ sensitivity and ATPase activity in the mouse myocardium. J Physiol. 2003, 552, 845–857. [Google Scholar] [CrossRef]
- Popov, S.V.; Maslov, L.N.; Mukhomedzyanov, A.V.; Kurbatov, B.K.; Gorbunov, A.S.; Kilin, M.; Azev, V.N.; Khlestkina, M.S.; Sufianova, G.Z. Apelin is a prototype of novel drugs for the treatment of acute myocardial infarction and adverse myocardial remodeling. Pharmaceutics 2023, 14 15, 1029. [Google Scholar] [CrossRef]
- Davidson, S.M.; Adameová, A.; Barile, L.; Cabrera-Fuentes, H.A.; Lazou, A.; Pagliaro, P.; Stensløkken, K.O.; Garcia-Dorado, D. EU-CARDIOPROTECTION COST Action (CA16225). Mitochondrial and mitochondrial-independent pathways of myocardial cell death during ischaemia and reperfusion injury. J Cell Mol Med 2020, 24, 3795–3806. [Google Scholar] [CrossRef]
- Kim, J.S.; Jin, Y.; Lemasters, J.J. Reactive oxygen species, but not Ca2+ overloading, trigger pH-and mitochondrial permeability transition-dependent death of adult rat myocytes after ischemia-reperfusion. Am J Physiol Heart Circ Physiol. 2006, 16 290, H2024–H2034. [Google Scholar] [CrossRef] [PubMed]
- Yellon, D.M.; Hausenloy, D.J. Myocardial reperfusion injury. N Engl J Med. 2007, 17 357, 1121–1135. [Google Scholar] [CrossRef]
- Bugger, H.; Pfeil, K. Mitochondrial ROS in myocardial ischemia reperfusion and remodeling. Biochim Biophys Acta Mol Basis Dis. 2020, 18 1866, 165768. [Google Scholar] [CrossRef]
- Timmers, L.; Pasterkamp, G.; de Hoog, V.C.; Arslan, F.; Appelman, Y.; de Kleijn, D.P. The innate immune response in reperfused myocardium. Cardiovasc Res. 2012, 94, 276–283. [Google Scholar] [CrossRef]
- García-Niño, W.R.; Zazueta, C.; Buelna-Chontal, M.; Silva-Palacios, A. Mitochondrial quality control in cardiac-conditioning strategies against ischemia-reperfusion injury. Life 2021, 11, 1123. [Google Scholar]
- Zeng, X.J.; Zhang, L.K.; Wang, H.X.; Lu, L.Q.; Ma, L.Q.; Tang, C.S. Apelin protects heart against ischemia/reperfusion injury in rat. Peptides 2009, 30, 1144–1152. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; McKinnie, S.M.; Patel, V.B.; Haddad, G.; Wang, Z.; Zhabyeyev, P.; Das, S.K.; Basu, R.; McLean, B.; Kandalam, V.; Penninger, J.M. Loss of Apelin exacerbates myocardial infarction adverse remodeling and ischemia-reperfusion injury: therapeutic potential of synthetic Apelin analogues. J Am Heart Assoc. 2013, 2, e000249. [Google Scholar] [PubMed]
- Simpkin, J.C.; Yellon, D.M.; Davidson, S.M.; Lim, S.Y; Wynne, A.M.; Smith, C.C. Apelin-13 and apelin-36 exhibit direct cardioprotective activity against ischemia reperfusion injury. Basic Res Cardiol. 2007, 23 102, 518–528. [Google Scholar]
- Fernandez Rico, C.; Konate, K.; Josse, E.; Nargeot, J.; Barrère-Lemaire, S.; Boisguérin, P. Therapeutic peptides to treat myocardial ischemia-reperfusion injury. Front Cardiovasc Med. 2022, 9, 792885. [Google Scholar] [CrossRef]
- Bäck, M.; Yurdagul, A.; Tabas, I.; Öörni, K.; Kovanen, P.T. Inflammation and its resolution in atherosclerosis: mediators and therapeutic opportunities. Nat Rev Cardiol. 2019, 16, 389–406. [Google Scholar] [PubMed]
- Chapman, F.A.; Maguire, J.J.; Newby, D.E.; Davenport, A.P.; Dhaun, N. Targeting the apelin system for the treatment of cardiovascular diseases. Cardiovasc Res. 2023, 119, 2683–2696. [Google Scholar]
- 27; Byrne, R.A.; Rossello, X.; Coughlan, J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.A.; Dweck, M.R.; Galbraith, M.; Gilard, M. 2023 ESC guidelines for the management of acute coronary syndromes: developed by the task force on the management of acute coronary syndromes of the European Society of Cardiology (ESC). Eur Heart J Acute Cardiovasc Care 2024, 13, 55–161. [Google Scholar]
- Sousa-Uva, M.; Neumann, F.J.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; Jüni, P. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur J Cardiothorac Surg. 2019, 55, 4–90. [Google Scholar]
- O’Connell, E.J.; Martinez, C.A.; Liang, Y.G.; Cistulli, P.A.; Cook, K.M. Out of breath, out of time: interactions between HIF and circadian rhythms. Am J Physiol Cell Physiol. 2020, 319, C533–C540. [Google Scholar]
- Abe, H.; Semba, H.; Takeda, N. The roles of hypoxia signaling in the pathogenesis of cardiovascular diseases. J Atheroscler Thromb. 2017, 24, 884–894. [Google Scholar]
- Yu, P.; Ma, S.; Dai, X.; Cao, F. Elabela alleviates myocardial ischemia reperfusion-induced apoptosis, fibrosis and mitochondrial dysfunction through PI3K/AKT signaling. Am J Transl Res. 2020, 12, 4467. [Google Scholar]
- Deng, J. Advanced research on the regulated necrosis mechanism in myocardial ischemia-reperfusion injury. Int J Cardiol. 2021, 32 334, 97–101. [Google Scholar]
- Welt, F.G.; Batchelor, W.; Spears, J.R.; Penna, C.; Pagliaro, P.; Ibanez, B.; Drakos, S.G.; Dangas, G.; Kapur, N.K. Reperfusion injury in patients with acute myocardial infarction: JACC scientific statement. J Am Coll Cardiol. 2024, 33 83, 2196–2213. [Google Scholar]
- Sagris, M.; Apostolos, A.; Theofilis, P.; Ktenopoulos, N.; Katsaros, O.; Tsalamandris, S.; Tsioufis, K; Toutouzas, K.; Tousoulis, D. Myocardial Ischemia–Reperfusion injury: Unraveling pathophysiology, clinical manifestations, and emerging prevention strategies. Biomedicines 2024, 12, 802. [Google Scholar] [CrossRef]
- Welt, F.G.; Batchelor, W.; Spears, J.R.; Penna, C.; Pagliaro, P.; Ibanez, B.; Drakos, S.G.; Dangas, G; Kapur, N.K. Reperfusion injury in patients with acute myocardial infarction: JACC scientific statement. J Am Coll Cardiol. 2024, 83, 2196–2213. [Google Scholar] [CrossRef]
- Pisarenko, O.I.; Shulzhenko, V.S.; Studneva, I.M.; Serebryakova, L.I.; Pelogeykina, Y.A.; Veselova, O.M. Signaling pathways of a structural analogue of apelin-12 involved in myocardial protection against ischemia/reperfusion injury. Peptides. 2015, 73, 67–76. [Google Scholar] [CrossRef] [PubMed]
- 37; An, S.; Wang, X.; Zhang, X.; Meng, H.; Li, W.; Chen, D.; Ge, J. Apelin protects against ischemia-reperfusion injury in diabetic myocardium via inhibiting apoptosis and oxidative stress through PI3K and p38-MAPK signaling pathways. Aging (Albany NY). 2020, 12, 25120. [Google Scholar]
- 38; Wang, X.; Zhang, L.; Feng, M.; Xu, Z.; Cheng, Z.; Qian, L. ELA-11 protects the heart against oxidative stress injury induced apoptosis through ERK/MAPK and PI3K/AKT signaling pathways. Front Pharmacol. 2022, 13, 873614. [Google Scholar]
- 39; Rakhshan, K.; Sharifi, M.; Ramezani, F.; Azizi, Y.; Aboutaleb, N. ERK/HIF-1α/VEGF pathway: a molecular target of ELABELA (ELA) peptide for attenuating cardiac ischemia–reperfusion injury in rats by promoting angiogenesis. Mol Biol Rep. 2022, 49, 10509–10519. [Google Scholar]
- Wang, W.; McKinnie, S.M.; Patel, V.B.; Haddad, G.; Wang, Z.; Zhabyeyev, P.; Das, S.K.; Basu, R.; McLean, B.; Kandalam, V.; Penninger, J.M. Loss of Apelin exacerbates myocardial infarction adverse remodeling and ischemia-reperfusion injury: therapeutic potential of synthetic Apelin analogues. J Am Heart Assoc. 2013, 2, e000249. [Google Scholar]
- Rossin, D.; Vanni, R.; Lo Iacono, M.; Cristallini, C.; Giachino, C.; Rastaldo, R. APJ as promising therapeutic target of peptide analogues in myocardial infarction-and hypertension-induced heart failure. Pharmaceutics 2023, 41 15, 1408. [Google Scholar] [CrossRef]
- Chandrasekaran, B.; Dar, O.; McDonagh, T. The role of apelin in cardiovascular function and heart failure. Eur J Heart Fail. 2008, 42 10, 725–732. [Google Scholar] [CrossRef]
- Khatami, S.; Faghihi, M.; Zarrin, A.; Sarveazad, A.; Yousefifard, M.; Ghorbani, A. Cardioprotective Effects of Apelin in Myocardial Ischemia/Reperfusion Injury: A Systematic Review and Meta-Analysis. J Cardiovasc Pharmacol. 2022, 43, 10–97. [Google Scholar] [CrossRef]
- Wyderka, R.; Osuch, Ł.; Ołpińska, B.; Łoboz-Rudnicka, M.; Diakowska, D.; Leśków, A.; Jaroch, J. The Impact of the Apelinergic System on the Cardiovascular System. Int J Mol Sci. 2025, 26, 10087. [Google Scholar] [CrossRef] [PubMed]
- Szokodi, I.; Tavi, P.; Földes, G.; Voutilainen-Myllylä, S.; Ilves, M.; Tokola, H.; Pikkarainen, S.; Piuhola, J.; Rysä, J.; Tóth, M.; Ruskoaho, H. Apelin, the novel endogenous ligand of the orphan receptor APJ, regulates cardiac contractility. Circ Res. 2002, 91, 434–440. [Google Scholar] [CrossRef]
- Namazi, G.; Salami, R.; Pourfarzam, M.; Asa, P.; Mafi, A.; Raygan, F. Association of the serum apelin, but not ghrelin, with the presence and severity of coronary artery disease. Indian Heart J. 2021, 73, 214–217. [Google Scholar] [CrossRef] [PubMed]
- 47; Lu, Y.; Zhu, X.; Liang, G.X.; Cui, R.R.; Liu, Y.; Wu, S.S.; Liang, Q.H.; Liu, G.Y.; Jiang, Y.; Liao, X.B.; Xie, H. Apelin–APJ induces ICAM-1, VCAM-1 and MCP-1 expression via NF-κB/JNK signal pathway in human umbilical vein endothelial cells. Amino Acids 2012, 43, 2125–2136. [Google Scholar]
- 48; Liu, L.Q.; Zhang, P.; Qi, Y.Z.; Li, H.; Jiang, Y.H.; Yang, C.H. Quercetin attenuates atherosclerosis via modulating apelin signaling pathway based on plasma metabolomics. Chin J Integr Med. 2023, 29, 1121–1132. [Google Scholar]
- Hendrianus; Adiarto, S.; Prakoso, R.; Firdaus, I.; Indriani, S.; Rudiktyo, E.; Widyantoro, B.; Taofan; Ambari, A.M.; Sukmawan, R. A novel peptide elabela is associated with hypertension-related subclinical atherosclerosis. High Blood Press Cardiovasc Prev. 2023, 30, 37–44. [Google Scholar] [CrossRef] [PubMed]
- 50; Li, Z.; Bai, Y.; Hu, J. Reduced apelin levels in stable angina. Intern Med. 2008, 47, 1951–1955. [Google Scholar]
- Güzelburç, Ö.; Demirtunç, R.; Altay, S.; Kemaloğlu Öz, T.; Tayyareci, G. Plasma apelin level in acute myocardial infarction and its relation with prognosis: a prospective study. JRSM Cardiovasc Dis. 2021, 10, 2048004020963970. [Google Scholar] [PubMed]
| Characteristics | Apelin-36 ≤ 0.58ng/mL (n=115) |
Apelin-36 > 0.58ng/mL (n=46) |
P-value |
|---|---|---|---|
| Age (year) | 62.61 (±10.95) | 59.37 (±11.30) | 0.22 |
| Gender (male) (n/%) | 96 (59.62) | 36 (22.36) | 0.80 |
| BMI (kg/m2) | 27.28 (±5.32) | 26.24 (±5.64) | 0.96 |
| Medical history | |||
| Hypertension (n/%) | 66 (40.99) | 24 (14.90) | 0.61 |
| Diabetes mellitus (n/%) | 35 (21.73) | 10 (6.21) | 0.006 |
| Smoking (n/%) | 69 (42.85) | 27 (16.77) | 0.54 |
| Laboratory values | |||
| Hemoglobin (mg/dL) | 138.55 (±23.68) | 141.0 (±15.49) | 0.99 |
| Cholesterol (mmol/L) | 5.17 (1.16) | 5.02 (1.49) | 0.33 |
| Triglyceride (mmol/L) | 1.75 (±1.12) | 1.52 (±0.75) | 0.43 |
| Glucose (mmol/L) | 10.27 (±5.77) | 8.48 (±4.21) | 0.02 |
| Creatinine (umol/L) | 105.73 (31.27) | 92.95 (26.97) | 0.014 |
| Creatine kinase-MB (U/L) | 124.0 (15.0-466.0) | 90 (16.0-520.0) | 0.17 |
| Creatine kinase (U/L) | 431.0 (210-7224.0) | 752.50 (350.0-5057.0) | 0.61 |
| Troponin T (pg/mL) | 290.0 (8.5-9510.0) | 132.15 (9.4-5190.0) | 0.012 |
| Ejection fraction (%) | 49.43 (±6.55) | 50.30 (±7.14) | 0.44 |
| Gensini score (Mean ±s.d) | 70.29 (±28.76) |
81.95 (±23.82) |
0.004 |
| Final TIMI grade flow ≤ 2 (n/%) | 29 (18.01) | 22 (13.66) | 0.001 |
| Parameter | AUC (95% CI) | P-value |
|---|---|---|
| Apelin-36 | 0.77 (0.69-0.84) | <0.001 |
| Creatine kinase | 0.57 (0.34-0.80) | 0.49 |
| Creatine kinase-MB | 0.59 (0.37-0.80) | 0.40 |
| Troponin T | 0.57 (0.36-0.78) | 0.49 |
| Na+ | 0.41 (0.20-0.62) | 0.41 |
| K+ | 0.55 (0.33-0.77) | 0.61 |
| Ca++ | 0.51 (0.31-0.72) | 0.88 |
| Cholesterol | 0.70 (0.51-0.58) | 0.07 |
| Triglyceride | 0.42 (0.20-0.64) | 0.47 |
| Hemoglobin | 0.59 (0.37-0.81) | 0.37 |
| Glucose | 0.67 (0.48-0.86) | 0.10 |
| BUN | 0.60 (0.40-0.80) | 0.33 |
| Creatinine | 0.59 (0.36-0.81) | 0.40 |
| Uric acid | 0.65 (0.45-0.85) | 0.15 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



