
Submitted:
09 October 2025
Posted:
10 October 2025
You are already at the latest version
Abstract
Introduction
Breast cancer is the most common cancer in women, with 80% being oestrogen receptor positive, requiring endocrine treatment to reduce recurrence. Treatment compliance is vital; however, 10-50% of patients take an incorrect dosage or discontinue therapy. This has shown a 20% mortality increase. Additionally, endocrine therapy has been said to negatively impact patient’s bone health. This study’s aim is to explore patient’s beliefs about endocrine treatment, how perception of medication risk and benefit affects adherence; as well as investigate the treatments effect on bone health.
Methods: 100 patients diagnosed with oestrogen receptor positive breast cancer in 2020 were sent the Beliefs about Medicine Questionnaire-Adjuvant Endocrine Therapy (BMQ-AET). A further 101 semi-structured telephone interviews were conducted. Initial and recent DEXA scans were compared to assess bone density changes.
Results
The response rate for the questionnaire was 55%(N=55). 49 patients returned the postal paper survey, and 6 patients responded via QR code. 101 patients participated in semi-structured telephone interviews. 13 patients were non-adherent (8.3%). Non-adherent patients showed decreased BMQ-AET Necessity scores and higher scores for BMQ-AET Concerns subscales. Joint pain and poor quality of life were the most common reason for non-adherence, 58%(N=97), which confirmed the need for more help managing side effects.
BMQ-AET NECESSITY SCORE
N MEAN P-VALUE
NON-ADHERENT 13 17.54 < 0.001
ADHERENT 143 10.86
BMQ-AET CONCERNS SCORE
N MEAN P-VALUE
NON-ADHERENT 13 13 0.002
ADHERENT 143 16.54
Of participants suitable for DEXA comparison, the majority (54.2%) showed an increase in bone density.
Conclusion
This study demonstrated good compliance to endocrine treatment. Non-adherent patients showed significantly low BMQ-AET necessity and high BMQ-AET concerns subscale scores. This highlights that patient’s non-adherent to AET have a lowered perception of necessity and greater concern regarding the medication, confirming a further need to address patient’s beliefs about endocrine treatment. DEXA comparison showed increased BMD, which challenges the previously held beliefs.
Keywords:
Breast Cancer
; Adherence
; Endocrine therapy
; Compliance
; Questionnaire
1. Introduction
1.1. Background
Breast cancer (BC) is the most common cancer in women in United Kingdom as well as in the world, accumulating to 15% of all newly diagnosed cancer cases between 2017-2019 [1,2]. Primary management usually involves surgery, including breast conservation surgery, mastectomy or axillary lymph node surgery, often followed by radiotherapy to reduce reoccurrence risk [3]. For patients with oestrogen receptor-positive (ER-Positive) tumours, accounting for approximately 80% of cases, adjuvant endocrine therapies (AET) such as Tamoxifen or Aromatase Inhibitors (AIs) are recommended [4].
1.2. Relationship Between The Endocrine System and Breast Cancer
Oestrogen plays a central role in breast tissue, including promoting the proliferation of epithelium, both of a normal and neoplastic state. In BC, oestrogen receptor signalling increases cell proliferation whilst suppressing apoptosis, favouring the survival of malignant cells [5] High systemic oestrogen levels are associated with an increased BC risk [6]. Oestrogen has been suggested to have a direct effect, with oestrogen being shown to induce genomic changes that contribute directly to carcinogenesis [7]. These insights into oestrogen-driven tumorigenesis underpin the development of endocrine therapies targeting oestrogen receptor pathways.
1.3. Current Endocrine Treatment
Tamoxifen works as a selective oestrogen receptor modulator with both anti-oestrogenic and oestrogenic effects, primarily working on breast tissue [8]. Conversely, AIs inhibit the aromatase enzyme, therefore blocking the conversion of androgens to oestrogens [9]. The therapeutic regimen prescribed is dependent on menopausal status. For postmenopausal women with ER-positive BC, AIs are the first line treatment, shown to be substantially more effective than Tamoxifen reducing mortality within 15 years by 30% [10]. AIs are ineffective in premenopausal women, as ovarian oestrogen production predominates [11]. In premenopausal women, Tamoxifen can be prescribed alone, or combined with GnRH agonists, with the premise to exchange to AI once menopause initiates. This combination induces reversible ovarian suppression, creating a postmenopausal hormonal environment [12]. The reversible nature of the GnRH agonists results in preservation of the ovaries, as opposed to a full oophorectomy, the historic resolution to this.
1.4. Efficacy of AET
Research has found the use of AET’s following primary BC treatment to be effective at reducing tumour reoccurrence and decreasing the mortality rate. A meta-analysis by the Early Breast Cancer Trialist’s Collaborative Group found 5 years of Tamoxifen that reduced death rates by 31% [13]. Another study indicated that Tamoxifen halved the recurrence risk during the first 4 years of treatment, and reduced it by a third during years 5-9, yielding an overall reduction of 39% [14]. The ATAC Trial compared the effectiveness of Tamoxifen and Anastrozole in 9366 postmenopausal women with BC over a 5-year period. Results showed higher efficacy in Anastrozole than Tamoxifen, with fewer side effects experienced [15]. Studies have also investigated the long-term effects of continuing AET past the 5-year mark. Davies et al. demonstrated that continuing Tamoxifen for 10 years caused a reduction in tumour recurrence and mortality; with approximately 50% decrease in BC mortality during the second decade post diagnosis [16].
1.5. Compliance and Adherence of AET
Despite the efficacy of AET, adherence following BC treatment remains poor. Adherence refers to an active choice by a patient to engage with the treatment, whereas compliance describes passively following of medical instructions [17]. Throughout literature, adherence is typically assessed in 3 ways: initiation of treatment, taking medication as prescribed and persistence across the treatment duration [18].
AET is commonly prescribed for 5-10 years, therefore adherence often declines over time. Reports indicate a compliance rate of approximately 80% within the first year dropping to 55% by the fifth year [19]. On the contrary, a large cohort study of 8700 participants by Hershman et al. [20] showed that those adherent within the first year of AET were likely to complete the full treatment course, although full duration compliance only amounted to 51%. This nonadherence of the medication can potentially lead to a poorer quality of life [21] and to a 49% increase in the risk of mortality [20]. These findings highlight the need to better understand and address the barriers to persistence with AET.
1.6. Reasons for Non-Adherence
AET adherence is multifactorial, extending beyond side effects. Age influences adherence with extremes of ages (<45 years old and >80) showing trends of non-adherence, potentially due to fertility concerns, comorbidities or body image [22,23].
Gender may also play a role as research has shown that men taking AET had a higher adherence compared to women [24].
Another potential factor negatively influencing AET adherence is polypharmacy, especially in the older generations [25].
A major factor contributing to whether a patient is compliant to their medication is their health care provider. Factors such as patient-centred communication, inclusion in decision making and clear guidance can improve adherence, whilst poor relationships contribute to discontinuation [26,27].
Side effects of AET are common, with 94% of patients being affected, and include hot flushes, arthralgia and menopausal symptoms, which can reduce quality of life and adherence [28,29,30].
The severity of the side effects experienced can cause a detrimental view of the medication, resulting in a decrease in the persistence and adherence of the AET. Whilst there is evidence suggesting a negative correlation between AET adherence and side effects, there is limited, or inconsistent findings regarding what specific side effects are responsible [31].
Education on potential side effects and ways to manage them have been shown to be pivotal in compliance [32,33].
Other psychosocial factors, such as prior experiences, rumours or beliefs about medications, also influence adherence. While positive initial perceptions may motivate initial therapy, the effects of symptoms or poor quality of life may cause adherence to decline over time [34,35,36,37,38]. Education levels have shown a trend with higher academic attainment generally being associated with improved medication adherence, potentially due to increased understanding of treatment importance [39].
Overall, AET adherence is multifactorial, involving patient characteristics, healthcare support, and psychosocial attitudes.
1.7. AET’s Effect on Bone Health
AET has been found to affect bone mass density (BMD), with effects varying by drug type and menopausal status. In postmenopausal women, Tamoxifen acts as a partial oestrogen agonist within the bone [40]. A RCT reported a 32% reduced fracture rate with 5 years of Tamoxifen compared to placebo [41]. Conversely, in premenopausal women, Tamoxifen competes with endogenous oestrogen, leading to bone loss [40]. AIs are associated with increased bone loss and fracture risk, with a study finding an 83% lower fracture risk in untreated women compared to those receiving AIs [42]. A further, meta-analyses showed AIs confer a 47% increase in fracture risk than Tamoxifen [43]. In premenopausal women, AIs combined with ovarian suppression cause the most severe oestrogen depletion and BMD loss [40].
As a result, it can be inferred that the use of AET, can lead to a higher osteoporosis rate and a significant reduction in the bone health compared to untreated patients. Clinical guidance recommends bone health monitoring using Dual-Energy X-ray Absorptiometry (DEXA). Baseline scans before commencement of AET, followed by regular monitoring, can identify patients at risk of osteoporosis [43,44]. Bone-related strategies including Bisphosphonates vitamin D and calcium can mitigate AET-related bone loss [45].
1.8. Aims of Study
There is a lack of consistency in publication reporting on the levels of adherence of AET for patients with BC after primary BC treatment, due to varying factors. Therefore, the aim of this study is to gain an understanding into the rates of adherence to AET, garner a better insight into the reasons behind this, and assess the effects the medication has on BMD.
2. Methodology
2.1. Questionnaire
2.1.1. Participants
The participants were patients diagnosed with BC, who had received treatment with curative intent within the high volume breast centre in a district general hospital in the United Kingdom in 2020 and had commenced AET, allowing for adequate duration of treatment. Inclusion criteria consisted of the year of diagnosis and surgery as well as the prescription of AET. Patients were excluded if they had more advanced cancer, were deemed too unwell, or those who were seriously unwell due to other conditions.
2.1.2. Questionnaire Creation
An extensive literature search was conducted using PubMed and Google Scholar with terms such as “medication compliance,” “endocrine therapy adherence,” and “breast cancer medication compliance.” Three validated questionnaires were identified as relevant: the ASK-12 Survey [46], General Medication Adherence Scale (GMAS) [47], and the Beliefs about Medicines Questionnaire (BMQ). The BMQ had previously been adapted for adjuvant endocrine therapy (BMQ-AET) [48] to assess adherence in women with breast cancer. After evaluating each survey’s strengths and limitations, the BMQ-AET was selected as most suitable for the study’s aims.
To address gaps in existing questionnaires, particularly regarding degree of adherence, age at diagnosis, education level, side effect profile, and suggestions for improvement, custom questions were added. These included Likert-scale items (1=Strongly Agree, 5=Strongly Disagree), yes/no items, and optional open-ended responses to allow participants to elaborate.
2.1.3. Data Collection
One hundred surveys were distributed in November 2024, accompanied by a cover letter explaining the study purpose and an estimated completion time of 10 minutes. To maximise participation, participants could complete the survey either on paper, returned via prepaid envelope, or digitally via a QR code or web link provided on the cover letter. This mixed-mode approach aimed to enhance response rates within the study timeframe.
2.2. Semi-Structured Telephone Interviews
2.2.1. Participants
A further pool of participants was selected from the database of patients that been diagnosed with ER-positive BC in 2020 who were treated with curative and prescribed AET.
2.2.2. Study Design
The semi-structured telephone interviews mainly used questions from the survey, however the interviewer allowed more open-ended responses from participants. The use of semi-structured telephone interviews was to maximise response, whilst also gauging the participants feelings behind their response.
2.2.3. Data Collection
The semi-structured telephone interviews occurred at the end of October and throughout November 2024. The interviewer explained the reasoning and purpose of the interviews before any questions were asked and consent was gained. The semi-structured aspect of the interviews allowed for more flexible questioning to gain further insight into the participants belief or burden, behind the treatment.
2.3. DEXA Scan Comparison
2.3.1. Participants
Of those participants who completed the questionnaires or semi-structured interviews, DEXA scan results were compared. Patients who had not attended any DEXA scan or only attended the initial DEXA scan were discarded from the comparison, however the BMD on the baseline DEXA was recorded.
2.3.2. Data Collection
In December 2024, the participant’s most recent DEXA scans were compared against their initial DEXA scans in order to assess any change in BMD after taking AET.
2.4. Data Analysis
Questionnaire and semi-structured interview responses were manually entered into Microsoft Excel. Participants were grouped by adherence to AET (adherent vs. non-adherent) based on their response to Question 1 (see Appendix). Due to unequal group sizes (143=adherent, 13=non-adherent), results were presented as percentages rather than raw counts, with trends visualized using bar and pie charts.
Responses from the BMQ-AET were converted into ordinal numerical values (1 = Strongly Agree, 5 = Strongly Disagree) and separated into Necessity and Concerns subscales, via the DATAtab Statistics Calculator software [49]. Non-parametric analysis was performed using the Mann-Whitney U test to compare adherent and non-adherent groups, with mean ranks, medians, and standard deviations reported. P-values were calculated for each subscale (Concerns= 0.002; Necessity: p=0.001) and visualized with box-and-whisker plots.
For DEXA scan comparisons, baseline BMD and subsequent changes were recorded. Bar and pie charts were used to display BMD changes and the proportion of patients in each category
2.5. Ethical Considerations
Participants of both the questionnaire and the semi-structured telephone interview were informed of the optional nature of taking part, and it was highlighted to them that they could retract their data and withdraw at any point. Confidentiality was of upmost importance within the study, therefore the anonymity of the data collected was emphasized to the participants. The study was approved by the Institutional Governance department and the Patient Experience department and registered as a quality improvement project.
3. Results
3.1. Response Rates
100 patients were contacted via post using the BMQ-AET questionnaire (Necessity and Concerns subscales) alongside custom-made questions. The response rate for the postal questionnaires was 55 (55%); of which 49 responded by returning the paper questionnaire by post and 6 responded using the QR Code. (Figure 1). A further 101 patients were contacted for a semi-structured interview via the telephone. Therefore, a total population of 156 patients were included within this study.
3.2. Demographics
The age of diagnosis of breast cancer within the population was shown to be older, with 28.88% (n=45) within the 70+ age group. The subsequent most prevalent age group was between 61-70, as a further 28.21% (n=44) belonged within this category. 23.07% [35] of the patients were between the ages of 51-60 as opposed to the 41-50 age group which consisted of 15.38% (n=24) of the respondents. Alternatively lower quantities of the population occurred in younger age groups, as only 5.13% (n=8) within 31-40 years of age at diagnosis. (Figure 2).
Participants were asked a question about the highest level of education they have achieved. The most abundant education level was O-Levels/GCSE’s, with 46 (29.49%) of patients completing them as their highest educational level. Patients who answered ‘No Formal Qualifications’ made up 19.23% (n=30) of the cohort, and those who chose not to specify their education levels made up a further 21.15%% (n=33). Graduates included 26 participants (16.67%). The next group consisted of patients who had completed A-Levels as their highest level of education, consisting of 10 individuals (6.41%). The remaining individuals, 11 (7.05%), answered the “Other” section which included certifications such as diplomas and apprenticeships.
The breakdown of the Education level relating to adherence within this trial is seen in Figure 3 but will be examined in greater detail later in this section.
3.3. Adherent Group
Of the total 156 participants, 143 (91.67%) were found to be adherent to AET after BC. (Figure 4).
Within the Adherent Group, the age of diagnosis of participants can be seen. The most populous age within the adherent group was 61-70 with 43 (30.07%) patients. Similarly, 41 (28.67%) of participants were aged 70 and above. Patients who were diagnosed with BC between the ages of 51-60 made up 21.68% [31] of the population. 23 (16.08%) of those adherents with AET were diagnosed between the ages of 41-50. Finally, the age group with the least number of participants within the adherent group was 31-40, having 5 participants (3.5%). This is shown in Figure 5.
Next to be tested was Education status within the Adherent Group. O-Levels/GCSE had the highest percentage, 30.1%, within the adherent group (n=43). The second most popular group within the adherent group included those with no formal qualifications, amounting to 29 patients (20.3%). Similarly to the previous, 28 individuals (19.6%) chose the “Prefer Not to Say” option. 15.4% of the adherent group were Graduates, with 22 patients. A further 9 patients (6.29%) completed A-Levels as the highest form of formal qualifications and 7 more (4.9%) achieved Postgraduate status. The “Diploma” and “Apprenticeships” educational groups consisted of 2 individuals, both accounting for 1.4% of the adherent group each. The final 1 individual stated CSE’s was their highest form of qualification, representing 0.699% of the adherent group. (Figure 6).
3.4. Non-Adherent Group
Non-adherence to AET within the 156 participants, was shown with 13 (8.33%) of the participants of the study. This was highlighted previously, in Figure 4.
The age of BC diagnosis within the non-adherent group differs to the adherent group, as the ages of 51-60 accounted for the most populous group, making 30.77% (n=4) within those non-compliant with AET. 3 individuals were aged 70 or over at diagnosis made up 23.08% of the non-adherent group. These numbers are identical for the age range of 31-40 years. Of the 13 patients in this group, 15.38% (n=2) fell within the 61-70 age category, and the final 1 individual (7.69%) was between the ages of 41-50 at diagnosis. (Figure 7).
Education status within the non-adherent group was also measured. The main proportion of responses of the group was “Prefer Not to Say”, which consisted of 5 participants (38.5%). Of the individuals who specified their education status, 30.8% (n=4) held graduate level qualifications. 3 patients stated that they held O-Levels/GCSE’s as their highest form of formal qualification, accumulating to 23.1% of the non-adherent group. Finally, 1 individual (7.69%) held postgraduate level of education. (Figure 8).
Patients who stated that they were non-compliant with their AET were asked about the duration of treatment (in months) before stopping. 38.46% of those asked [5] stated they were on AET for less than 3 months. 3 patients (23.08%) had a duration of treatment lasting 36-48 months. A further 2 patients (15.38%) reported that it took 24-36 months of being on AET before discontinuation. The duration of 12-24 months is what it took for 2 patients (15.38%) to discontinue AET. 1 individual (7.69%) was on AET for 3-6 months, and 1 individual (7.69%) took 6-12 months before stoppage. 0 patients reported stopping after 6-12 months (Figure 9).
The reasoning behind the termination of AET adherence was asked. Of the 13 within the non-adherent group, 30.77% (4 individuals) stated that it was due to side effects consisting of both Joint Pain and Poor Quality of Life. Furthermore, an additional 3 (23.08%) said their AET discontinuation was due to Poor Quality of Life alone. 2 patients (15.38%) admitted that isolated joint pain was the reasoning behind stoppage of AET. 1 patient (7.69%) stopped medication due to wanting to start a family. Menopausal symptoms were the reasoning behind another [1] patient’s cessation of AET, accounting for 7.69%. A combination of brain fog and insomnia led to an additional individual (7.69%) to stop AET. The final participant within the 13 of the non-adherent group stated that joint pain alongside hot flushes led to non-adherence of the treatment. Overall, 7 out of the 13 participants (53.85%) within the non-adherent group had to stop the medication due to join pain.
The 156 participants of the study were asked what improvements could have been made to support them whilst taking the medication. This question’s qualitative nature allowed for patients to expand their answers. 70 of the participants (44.87%) answered that the question was not applicable. Of the responses, 26 (16.67%) included that better guidance on how to deal with side effects would have helped. Similarly, 25 (16.03%) responses included emotional support as a reason that would have been of benefit to them whilst taking the medication. 23 (14.74%) answers included the need for more information on the medication was a way to support individuals on AET. Help with managing multiple medications was present in 7 (4.49%) of the answers for participants asked this question. 12 (7.69%) answers contained “Other” in which participants shared experiences regarding communication and attitudes of their healthcare professionals.
3.5. BMQ-AET Score Comparison
The necessity subscale of the BMQ-AET was utilised to assess the patient’s beliefs about how necessary AET is. The comparison of the non-adherent group (n=13) against the adherent group (n=143) was conducted. Table 1 shows the results.
Following this, a Mann-Whitney U-Test was performed. The test revealed a statistically significant difference between the BMQ-AET specific necessity score for the adherent group and the BMQ-AET necessity score for the non-adherent group (U=122, z=-5.2) The asymptomatic p value was <0.001 with the exact p value equally <0.001. The median values were increased in the non-adherent group as opposed to the adherent group, indicating a medium effect size (r=0.42). Therefore, at a 5% significance level, the null hypothesis is rejected.
The results from the BMQ-AET Necessity Score Comparison can be shown in Figure 10.
Alternatively, the concerns subscale of the BMQ-AET was used to assess the patient’s concerns over AET. Another comparison against the non-adherent group (n=13) and the adherent group (n=143) was made. Table 2 shows the results.
The results and distribution of results of the comparison between the BMQ-AET Concerns score between the non-adherent and adherent groups can be seen in Figure 11.
A sum of ranks and a mean rank was calculated for both the non-adherent and the adherent group of participants using the BMQ-AET specific concerns score. From the non-adherent group (n=13) the sum of ranks equalled 543.5, therefore a mean rank of 41.81 was deduced. The adherent group (n=143) had a sum of ranks amounting to 11702.5, resulting in the mean rank of 81.84.
A final Mann-Whitney U-Test was carried out to analyse whether there is a difference between the BMQ-AET Concerns Score of both groups. The results from the Mann-Whitney U-Test are shown in Table 3.
These results suggest that there is a small affect size between both groups. The median values were increased in the adherent group as opposed to the non-adherent group. The difference is statistically significant at a 5% significance level. Thus, the null hypothesis is rejected.
3.6. DEXA Scan Comparison
In 156 participants DEXA scans were compared. For the initial baseline DEXA, 6 participants (3.85%) were invalid and withdrawn. This left a pool of 150 (96.15%) suitable patients to compare. Of these, 54 (34.62%) individual’s baseline DEXA showed evidence of osteopenia. A further 43 (27.56%) participants were deemed not applicable for a baseline DEXA scan. Patients who had normal BMD within the baseline DEXA scan amounted to 38 (24.36%). 13 participants (8.33%) were deemed osteoporotic and the final 2 participants (3.85%) had a high BMD within their baseline DEXA scan. This is shown in Figure 12.
The baseline DEXA scans were then compared to the participant’s most recent scan. 82 participants (53.25%) were deemed invalid for BMD comparison on follow up DEXA scan, leaving a population of 72 (46.75%) to compare from. Of these 72, an increase in BMD was seen in 39 patients (25.32%). There was no change observed in BMD on the follow up DEXA scan for 19 individuals (12.34%). Finally, 14 participants (9.09%) were shown to have a decrease in BMD on comparison with their follow up DEXA scan. (Figure 13).
4. Discussion
4.1. Main Findings
This study found high adherence to AET, with 91.67% of patients taking it as prescribed, contrasting with previous literature that report lower adherence of AET in BC [50,51]. Contributing factors to this may include demographics, social desirability bias, and the cohort’s educational level, with 52.6% (n=82) obtaining O-Levels or higher. Access to a Cancer Nurse Specialist Helpline and routine holistic needs assessments 12 months post-diagnosis likely supported adherence by providing information and guidance on treatment. Notably, high adherence persisted in patients during their fourth and fifth year of AET, exceeding expectations from previous studies that report declining adherence over longer periods [14].
Participants were typically older at BC diagnosis, consistent with age as a primary risk factor [52]. However, non-adherent patients were generally younger, most commonly 51–60 years, compared to 61–70 in the adherent group. This aligns with studies showing younger patients are less likely to adhere to AET [53,54], though contrasts with Unni et al. [55], who found adherence was influenced more by individual beliefs than age, despite using a similar measurement tool.
Education levels varied within the cohort, typical of a general population [56], demonstrating no correlation between educational levels and rates of breast cancer, as previously suggested [57].In the adherent group, most participants had O-levels/GCSEs, while graduates were more common in the non-adherent group, contrasting prior studies that link higher education with improved AET adherence [54,58]. However, the non-adherent group was significantly smaller, limiting the reliability of this comparison.
In the non-compliant group, most participants had been on AET for less than 3 months, with no clear trend in duration before stopping. Side effects were the primary reason for discontinuation, consistent with prior research showing that around 70% of AET patients experience side effects [59]. Joint pain was most common (53.85%), followed by menopausal symptoms, hot flushes, brain fog and insomnia, all of which negatively impacted quality of life and adherence [60,61]. One participant discontinued due to fertility concerns, highlighting the need for guidance for premenopausal patients. Studies indicate short-term treatment cessation to conceive do not increase recurrence risk [62,63].
Most participants (44.9%) reported no additional support was needed whilst taking AET. Guidance on managing side effects (16.7%), emotional support, and clear medication information were identified as key facilitators of adherence [64,65,66]. Support from healthcare professionals also enhanced adherence, particularly for older adults managing multiple medications, a finding supported by existing research [67,68]
BMQ-AET analysis showed non-adherent participants had lower perceived necessity of AET (mean=17.54 vs 10.86) and higher concerns about side effects (mean=13 vs 16.54), consistent with literature linking beliefs and adherence [69,70,71,72,73,74,75,76]. While adherent group demonstrated more variability in responses, the overall trend indicates that addressing patient concerns early in treatment, through education may support adherence.
Interestingly, majority of participants with follow-up DEXA scans showed an increase in BMD despite being on AET, with only 19.4% showing a decrease, which is generally associated with bone loss [77,78,79,80]. At baseline, 34.6% had osteopenia and 8.3% osteoporosis, yet subsequent monitoring revealed improvements in most cases. The positive trend is likely due to the combined use of AET with anti-bone resorptive therapies, including calcium, vitamin D and bisphosphonates, as well as lifestyle advice such as exercise. These findings challenge conventional expectation of BMD decline in AET patients, highlighting the potential for proactive management to not only prevent but improve bone health, reducing long-term fracture risk. This underscores the value of regular monitoring and early intervention in BC care.
4.2. Strengths
A major strength of this study was its methodological rigor, using a mixed-methods approach combining semi-structured telephone interviews with questionnaires. This approach allowed a comprehensive representation of adherence to AET, capturing both quantitative and qualitative insights [81,82,83,84]. Participants could respond via QR code or prepaid envelope, maximizing response rates, which reached 55%, higher than the average 44.1% for similar surveys [85,86].
The study utilized the validated BMQ-AET questionnaire, a reliable tool for assessing medication beliefs and adherence, enhancing the validity and reliability of findings [87]. Open-ended questions in the interviews and survey provided additional qualitative insight beyond closed-ended responses, offering a fuller understanding of adherence behaviours [88,89].
Inclusion criteria limited participants to those treated within the last five years, reducing recall bias while allowing adequate time on AET to assess adherence [90]. Although cross-sectional, the study’s medium-term follow-up of four years enabled a more accurate evaluation of adherence patterns and the impact of AET on bone health [91].
Finally, the participant cohort was diverse in age, education, ethnicity, gender, and socioeconomic background, supporting the generalizability of the findings [92]
4.3. Limitations
Despite the strengths, several limitations should be acknowledged. Although the study achieved a promising response rate (156 participants), a larger sample would improve generalizability and statistical power, enabling finer detection of differences between subgroups [93]. Non-response bias may also have influenced results, as certain groups, such as those with lower income, lower education, or children, may be less likely to respond [94].
The study population was limited to single centre in the United Kingdom, which may not represent the broader population on AET after breast cancer treatment. Geographic and demographic differences, such as education and socioeconomic status, could limit generalizability and introduce selection bias [95,96].
Use of self-reported data via questionnaires and semi-structured interviews introduces potential biases. Social desirability bias may have led participants to overestimate adherence, particularly during interviews [97], and the Hawthorne effect could have altered responses [16]. Acquiescent responding may also have influenced answers, though its exact impact could not be assessed [98]. Interviewer confirmation bias was mitigated through standardized questions [99].
Postal questionnaires risked misinterpretation of questions, especially custom items, despite using validated measures for most content [100]. Likert-scale questions may introduce extremity bias, though the 5-point odd-numbered scale was used to reduce this risk [101].
Confounding factors remain a concern. Participants’ multiple medications and conditions may have influenced their experiences with AET and recall bias or subjective perception of side effect severity may have affected reporting [102].
4.4. Recommendations for Future Research
This study highlights trends in adherence and non-adherence to AET post-primary BC treatment, revealing avenues for further exploration. Future research should include multiple centres with larger cohort of patients to enhance the generalizability of findings. Larger sample sizes would allow deeper analysis of non-adherence reasons within subgroups [103].
Longitudinal studies could clarify how adherence evolves over time and the factors influencing persistence, as demonstrated by Thomson et al. [104]. Additionally, incorporating face-to-face interviews, particularly for older patients, may provide richer qualitative insights, promoting a more supportive environment [105]. A mixed approach combining in-person and telephone interviews could optimize response rates while balancing feasibility.
5. Conclusion
The aim of this study was to investigate adherence and non-compliance rates for patients with BC who are undergoing AET, as well as the effects that the medication has on BMD. The findings demonstrated evidence investigating the levels of adherence, as well as the differing factors and mindsets as to why an individual would be non-adherent with their treatment. Overall, significantly high adherence rates were seen within the cohort of the study. However, it highlighted the significance and extent to which side effects result in the discontinuation of treatment. Demographics were discussed in an attempt to identify any trends within the adherent and non-adherent population. Patients who were non-compliant to their AET did show significantly low BMQ-AET necessity and high BMQ-AET concerns subscale scores. This highlights that patient’s non-adherent to AET have a lowered perception of necessity and greater concern regarding the medication. Furthermore, this confirms the importance of healthcare professionals addressing the patients’ beliefs about AET, in the hope of potentially improving adherence rates.
Comparison between AET adherent patient’s baseline and follow up DEXA scan, revealed interesting rates of increased BMD, which challenges previously held beliefs, potentially warranting the need for future research.
In conclusion, this study provides a valuable insight into the trends and behaviours of patients requiring AET, impacting medication adherence, alongside the effect on bone health.
6. Appendix: The AET Adherence Questionnaire
This paper was presented as a poster at Association of Breast Surgery Conference in Birmingham, United Kingdom in May 2025 and abstract published in European Journal of Surgical Oncology
Source of Funding
Nil
BMQ-AET NECESSITY SCORE
| N | MEAN | P-VALUE | |
| NON-ADHERENT | 13 | 17.54 | <0.001 |
| ADHERENT | 143 | 10.86 |
BMQ-AET CONCERNS SCORE
| N | MEAN | P-VALUE | |
| NON-ADHERENT | 13 | 13 | 0.002 |
| ADHERENT | 143 | 16.54 |
Abbreviations
List of abbreviations used as follows:
BC, Breast Cancer; AET, Adjuvant Endocrine Therapy; ER-positive, Oestrogen Receptor Positive; AI, Aromatase Inhibitor; GnRH, Gonadotropin Hormone-releasing Hormone; RCT, Randomised Controlled Trial; BMD, Bone Mass Density; DEXA, Dual-Energy X-ray Absorptiometry; ULHT, United Lincolnshire Hospitals NHS Trust; BMQ-AET, Beliefs about Medicine Questionnaire-adjuvant endocrine therapy
References
- Cancer Research UK. Breast Cancer Statistics. [Internet]. 2024 [cited 2024 September 27]. Available from: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/breast-cancer#heading-Zero.
- World Health Organisation. Breast Cancer. [Internet]. 2024 [cited 2024 September 27]. Available from: https://www.who.int/news-room/fact-sheets/detail/breast-cancer.
- Joint Formulary Committee (JFC). Breast Cancer. 2024 London: BMJ Group and Pharmaceutical Press. Available from: https://bnf.nice.org.uk/treatmentsummaries/breast-cancer/ [cited 2024 October 15].
- Rosso, R., D’Alonzo, M., Bounous, V.E., Actis, S., Cipullo, I., Salerno, E, Biglia, N. Adherence to Adjuvant Endocrine Therapy in Breast Cancer Patients. Current Oncology 2023 Jan 21; 30(2): 1461-1472. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC9955792/.
- Al-Shami K, Awadi S, Khamees A, Alsheikh AM, Al-Sharif S, Ala’ Bereshy R, Al-Eitan SF, Banikhaled SH, Al-Qudimat AR, Al-Zoubi RM, Al Zoubi MS. Estrogens and the risk of breast cancer: A narrative review of literature. Heliyon. 2023 Sep 17;9(9): e20224. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10559995/.
- Russo J, Russo IH. The role of estrogen in the initiation of breast cancer. J Steroid Biochem Mol Biol. 2006 Dec;102(1-5):89-96. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC1832080/.
- Lee JJ, Jung YL, Cheong TC, Espejo Valle-Inclan J, Chu C, Gulhan DC, Ljungström V, Jin H, Viswanadham VV, Watson EV, Cortés-Ciriano I, Elledge SJ, Chiarle R, Pellman D, Park PJ. ERα-associated translocations underlie oncogene amplifications in breast cancer. Nature. 2023 Jun;618(7967):1024-1032. Available from: https://pubmed.ncbi.nlm.nih.gov/37198482/.
- Patel P, Jacobs TF. Tamoxifen. StatPearls [Internet]. 2025 Jan. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532905/.
- Peters A, Tadi P. Aromatase Inhibitors. [Updated 2023 Jul 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557856/.
- University of Oxford [Internet]. Aromatase inhibitors better than tamoxifen at reducing risk of breast cancer recurrence in premenopausal and postmenopausal women. 2022 [cited 6 November 2024]. University of Oxford Medical Sciences Division. Available from: https://www.ndph.ox.ac.uk/news/aromatase-inhibitors-are-better-than-tamoxifen-at-reducing-the-risk-of-breast-cancer-recurrence-in-premenopausal-as-well-as-postmenopausal-women.
- Simpson ER. Sources of estrogen and their importance. J Steroid Biochem Mol Biol. 2003 Sep;86(3-5):225-30. Available from: https://pubmed.ncbi.nlm.nih.gov/14623515/.
- McCann, K.E., Goldfarb, S.B., Traina, T.A., Regan, M.M., Vidula, N., Kaklamani, V. Selection of appropriate biomarkers to monitor effectiveness of ovarian function suppression in pre-menopausal patients with ER+ breast cancer. npj Breast Cancer 2024 [cited 6 November 2024] 10, 8 (2024). [CrossRef]
- Early Breast Cancer Trialist’s Collaborative Group. Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. The Lancet. 2005 May 14; 365(9472), 1687–1717. Available from https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(05)66544-0/abstract.
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG); Davies C, Godwin J, Gray R, Clarke M, Cutter D, Darby S, McGale P, Pan HC, Taylor C, Wang YC, Dowsett M, Ingle J, Peto R. Relevance of breast cancer hormone receptors and other factors to the efficacy of adjuvant tamoxifen: patient-level meta-analysis of randomised trials. Lancet. 2011 Aug 27;378(9793):771-84. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC3163848/.
- ATAC Trialist’s Group. Results of the ATAC (Arimidex, Tamoxifen, Alone or in Combination) trial after completion of 5 years’ adjuvant treatment for breast cancer. The Lancet 2005 Jan; 365(9453), 60-62. Available from: https://www.sciencedirect.com/science/article/pii/S0140673604176666.
- Davis, S.A., Feldman, S.R. Using Hawthorne Effects to Improve Adherence in Clinical Practice: Lessons From Clinical Trials. JAMA Dermatology 2013;149(4),490–491. Available from: https://jamanetwork.com/journals/jamadermatology/fullarticle/1679347.
- Mir, T.H. (2023) Adherence Versus Compliance. HCA Healthcare Journal of Medicine 2023 April 28; 4(2), 219-220. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10324868/.
- Wassermann, J., Rosenberg, S.M. (2017) Treatment Decisions and Adherence to Adjuvant Endocrine Therapy in Breast Cancer. Current Breast Cancer Reports 2017 June;9, 100– 110. Available from: https://link.springer.com/article/10.1007/s12609-017-02485.
- Chamalidou, C., Nasic, S., Linderholm, B. Compliance to adjuvant endocrine therapy and survival in breast cancer patients. Cancer Treatment and Research Communications 2023; 35, 100704. Available from: https://www.sciencedirect.com/science/article/pii/S2468294223000254.
- Hershman, D.L., Shao, T., Kushi, L.H., Buono, D., Tsai, W.Y., Fehrenbacher, L., Kwan, M., Gomez, S.L., Neugut, A.I. Early discontinuation and non-adherence to adjuvant hormonal therapy are associated with increased mortality in women with breast cancer. Breast Cancer Res. Treat 2010 Oct 2; 126, 529–537. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC3462663/.
- McCowan, C., Wang, S., Thompson, A.M., Makubate, B., Petrie, D.J. The value of high adherence to tamoxifen in women with breast cancer: a community-based cohort study. Br J Cancer 2013 Aug 15; 109(5), 1172-80. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC3778308/.
- Yussof, I., Mohd Tahir, N.A., Hatah, E., Mohamed Shah, N. (2022) Factors influencing five-year adherence to adjuvant endocrine therapy in breast cancer patients: A systematic review. The Breast 2022 Jan 24; 62: 22-35. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC8818734/.
- Gremke, N., Griewing, S., Chaudhari, S., Upadhyaya, S., Nikolov, I., Kostev, K., Kalder, M. (2022) Persistence with tamoxifen and aromatase inhibitors in Germany: a retrospective cohort study with 284,383 patients. Journal of Cancer Research and Clinical Oncology 2022 Sep 23; 149(8), 4555-4562. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10349696/.
- Ali, A., Xiem, Z., Stanko, L., De Leo, E., Hong, YR., Bian, J., Daily, K.C. Endocrine adherence in male versus female breast cancer: a seer-medicare review. Breast Cancer Res Treat 2022 Feb 10; 192, 491–499. Available from: https://link.springer.com/article/10.1007/s10549-022-06536-0.
- Marcum ZA, Gellad WF. Medication adherence to multidrug regimens. Clin Geriatr Med. 2012 May;28(2):287-300. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC3335752/.
- Panahi, S., Rathi, N., Hurley, J., Sundrud, J., Lucero, M., Kamimura, A. Patient Adherence to Health Care Provider Recommendations and Medication among Free Clinic Patients. J Patient Exp 2022 Feb 9;9, 23743735221077523. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC8832560/.
- Lambert LK, Balneaves LG, Howard AF, Chia SK, Gotay CC. Understanding adjuvant endocrine therapy persistence in breast Cancer survivors. BMC Cancer. 2018 Jul 11;18(1):732. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC6042363/.
- Toivonen, K.I., Williamson, T.M., Carlson, L.E., Walker, L.M., Campbell, T.S. Potentially Modifiable Factors Associated with Adherence to Adjuvant Endocrine Therapy among Breast Cancer Survivors: A Systematic Review. Cancers (Basel) 2020 Dec 31; 13(1), 107. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC7794693/.
- Cancer Research UK [Internet]. 2024. Side effects of hormone therapy in women. [cited 8 November 2024]. Available from: https://www.cancerresearchuk.org/about-cancer/treatment/hormonetherapy/side-effects-women.
- Wagner LI, Zhao F, Goss PE, et al. Patient-reported predictors of early treatment discontinuation: treatment-related symptoms and health-related quality of life among postmenopausal women with primary breast cancer randomized to anastrozole or exemestane on NCIC Clinical Trials Group (CCTG) MA.27 (E1Z03). Breast Cancer Res Treat. 2019 Jun 1;169(3):537-548. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC6092930/.
- Fleming, L., Agnew, S., Peddie, N., Crawford, M., Dixon, D., MacPherson, I. The impact of medication side effects on adherence and persistence to hormone therapy in breast cancer survivors: A quantitative systematic review. Breast 2022 May 14; 64,63-84. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC9130570/.
- Peddie, N., Agnew, S., Crawford, M., Dixon, D., MacPherson, I., Fleming, L. The impact of medication side effects on adherence and persistence to hormone therapy in breast cancer survivors: A qualitative systematic review and thematic synthesis. Breast 2021; 58, 147-159. Available from: https://pubmed.ncbi.nlm.nih.gov/34049260/.
- Briot, K., Tubiana-Hulin, M., Bastit, L., Kloos, I., Roux, C. Effect of a switch of aromatase inhibitors on musculoskeletal symptoms in postmenopausal women with hormone-receptor-positive breast cancer: the ATOLL (articular tolerance of letrozole) study. Breast Cancer Res Treat 2010 Feb; 120(1), 127-34. Available from: https://pubmed.ncbi.nlm.nih.gov/20035381/.
- Al-Tarawneh, F., Ali, T., Al-Tarawneh, A., Altwalbeh, D., Gogazeh, E., Bdair, O., Algaralleh, A. Study of Adherence Level and the Relationship Between Treatment Adherence, and Superstitious Thinking Related to Health Issues Among Chronic Disease Patients in Southern Jordan: Cross-Sectional Study. Patient Prefer Adherence 2023 Mar 9; 17, 605-614. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10010127/.
- Berkowitz, M.J., Thompson, C.K., Zibecchi, L.T., Lee, M.K., Streja, E., Berkowitz, J.S., Wenziger, C.M., Baker, J.L., DiNome, M.L., Attai, D.J. (2021) How patients experience endocrine therapy for breast cancer: an online survey of side effects, adherence, and medical team support. Journal of Cancer Survivorship, 15(1),29-39. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC7430212/.
- Ramchand, S.K., Cheung, Y-M., Yeo, B., Grossmann, M. The effects of adjuvant endocrine therapy on bone health in women with breast cancer. Journal of Endocrinology 2019; 241(3), 111-124. Available from: https://joe.bioscientifica.com/view/journals/joe/241/3/JOE-19-0077.xml.
- Fisher B., Costantino, J.P., Wickerham, D.L., Cecchini, R.S., Cronin, W.M., Robidoux, A., Bevers, T.B., Kavanah, M.T., Atkins, J.N., Margolese, R.G., Runowicz, C.D., James, J.M., Ford, L.G., Wolmark, N. Tamoxifen for the Prevention of Breast Cancer: Current Status of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. JNCI: Journal of the National Cancer Institute 2005; 97(22), 1652–1662. Available from: https://academic.oup.com/jnci/article/97/22/1652/2521468?login=true.
- Ahlstedt Karlsson, S., Wallengren, C., Olofsson Bagge, R., Henoch, I. “It is not just any pill”- Women’s experiences of endocrine therapy after breast cancer surgery. European Journal of Cancer Care 2019; 28(3), e13009. Available from: https://pubmed.ncbi.nlm.nih.gov/30748038/.
- Verbrugghe, M., Verhaeghe, S., Decoene, E., De Baere, S., Vandendorpe, B., Van Hecke, A. Factors influencing the process of medication (non-)adherence and (non-)persistence in breast cancer patients with adjuvant antihormonal therapy: a qualitative study. Eur J Cancer Care (Engl) 2017 Mar; 26(2). Available at: https://pubmed.ncbi.nlm.nih.gov/26059246/.
- Tseng, O.L., Spinelli, J.J., Gotay, C.C., Ho, W.Y., McBride, M.L., Dawes, M.G. Aromatase inhibitors are associated with a higher fracture risk than tamoxifen: a systematic review and meta-analysis. Ther Adv Musculoskelet Dis 2018; 10(4),71-90. Available at: https://journals.sagepub.com/doi/10.1177/1759720X18759291. [CrossRef]
- Amir, E., Seruga, B., Niraula, S., Carlsson, L., Ocaña, A. (2011) Toxicity of adjuvant endocrine therapy in postmenopausal breast cancer patients: a systematic review and meta-analysis. J Natl Cancer Inst 2011; 103(17),1299-309. Available from: https://academic.oup.com/jnci/article/103/17/1299/2516517?login=true.
- Al-Farhat, Y. Detecting bone density in early breast cancer survivors: The arm-DXA method. Annals of Oncology 2018; 29(8), VIII84. Available from: https://www.annalsofoncology.org/article/S0923-7534(19)48688-2/fulltext.
- Ahmed, S., Banerjee, S., Horsnell, J. (2023) The management of bone health in breast cancer patients on aromatase inhibitors. European Journal of Surgical Oncology 2023; 49(5), 238. Available from: https://www.ejso.com/article/S0748-7983(23)00258-5/fulltext.
- Xu, J., Cao, B., Li, C., Li, G. The recent progress of endocrine therapy induced osteoporosis in estrogen-positive breast cancer therapy. Frontiers in Oncology 2023; 13, 1218206.Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10361726/.
- Gallagher J.C., Tella S.H. Controversies in osteoporosis management: antiresorptive therapy for preventing bone loss: when to use one or two antiresorptive agents? Clin Obstet Gynecol 2013; 56(4), 749-56. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC4140184/.
- Matza, L.S., Park, J., Coyne, K.S., Skinner, E.P., Malley, K.G., Wolever ,R.Q. “Derivation and validation of the ASK-12 adherence barrier survey. Ann Pharmacother 2009; 43(10), 1621-1630. Available from: https://pubmed.ncbi.nlm.nih.gov/19776298/.
- Naqvi, A.A, Hassali, M.A., Jahangir, A., Nadir, M.N, Kachela, B. Translation and validation of the English version of the general medication adherence scale (GMAS) in patients with chronic illnesses. J Drug Assess 2019; 8(1), 36-42. Available from: https://pubmed.ncbi.nlm.nih.gov/33719815/.
- Brett, J., Hulbert-Williams, N.J., Fenlon, D., Boulton, M., Walter, F.M., Donnelly, P., Lavery, B., Morgan, A., Morris, C., Horne, R., Watson, E. Psychometric properties of the Beliefs about Medicine Questionnaire-adjuvant endocrine therapy (BMQ-AET) for women taking AETs following early-stage breast cancer. Health Psychol Open 2017; 4(2), 2055102917740469. [online]. Available from: https://pubmed.ncbi.nlm.nih.gov/29379627/.
- DATAtab: Online Statistics Calculator. DATAtab e.U. Graz, Austria. Available from: https://datatab.net.
- Lee, H.S., Lee, J.Y., Ah, Y.M., Kim, H.S., Im, S.A., Noh, D.Y., Lee, B.K. Low adherence to upfront and extended adjuvant letrozole therapy among early breast cancer patients in a clinical practice setting. Oncology 2014; 86(5-6),340-349. Available from: https://karger.com/ocl/article/86/56/340/238958/Low-Adherence-to-Upfront-and-Extended-Adjuvant.
- Beryl, L.L., Rendle, K.A.S., Halley, M.C., Gillespie, K.A., May, S.G., Glover, J., Yu, P., Chattopadhyay, R., Frosch, D.L. Mapping the Decision-Making Process for Adjuvant Endocrine Therapy for Breast Cancer: The Role of Decisional Resolve. Medical Decision Making 2017; 37(1),79-90. Available from: https://journals.sagepub.com/doi/10.1177/0272989X16640488.
- Breast Cancer Research UK [internet]. Breast cancer risk. 2025 [cited 2025 January 2]. Available from: https://www.cancerresearchuk.org/health-professional/cancerstatistics/statistics-by-cancer-type/breast-cancer/risk-factors.
- Woolpert, K.M., Schmidt, J.A., Ahern, T.P., Hjorth, C.F., Farkas, D.K., Ejlertsen, B., Collin, L.J., Lash, T.L., Cronin-Fenton, D.P. Clinical factors associated with patterns of endocrine therapy adherence in premenopausal breast cancer patients. Breast Cancer Research 2024; 26(1), 59. Available from: https://breast-cancer-research.biomedcentral.com/articles/10.1186/s13058-024-01819-4.
- Brito, C., Portela, M.C., de Vasconcellos, M.T. Adherence to hormone therapy among women with breast cancer. BMC Cancer 2014; 14,397. Available from: https://bmccancer.biomedcentral.com/articles/10.1186/1471-2407-14-397.
- Unni, E., Shiyanbola, O.O., Farris, K.B. Change in Medication Adherence and Beliefs in Medicines Over Time in Older Adults. Global Journal of Health Science 2015 Aug 31; 8(5),39-47. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC4877212/.
- Office for National Statistics. How qualification levels across England and Wales differ by country of birth [internet].2023 [cited 2025 January 2]. Available from: https://www.ons.gov.uk/peoplepopulationandcommunity/educationandchildcare/articles/howqualificationlevelsacrossenglandandwalesdifferbycountryofbirth/2023-05-15.
- Karlsen, R. V., Høeg, B.L., Dalton, S.O., Saltbæk, L., Dehlendorff, C., Johansen, C., Svendsen, M.N., Bidstrup, P.E. Are education and cohabitation associated with health-related quality of life and self-management during breast cancer follow-up? A longitudinal study. Acta Oncologica 2023; 62(4),407–413. Available from: https://medicaljournalssweden.se/actaoncologica/article/view/34998.
- Brito, C., Portela, M.C., Vasconcellos, M.T. Factors associated to persistence with hormonal therapy in women with breast cancer. Revista de Saude Publica 2014; 48(2),284-95. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC4206152/.
- Spencer, J.C., Reeve, B.B., Troester, M.A., Wheeler, S.B. Factors Associated with Endocrine Therapy Non-Adherence in Breast Cancer Survivors. Psychooncology 2020; 29(4), 647-654. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC7190446/.
- Bertaut, A., Badovinac Crnjevic, T., Martin, A-L, Gaudin, C., Chen, L. 346P Quality of life (QoL) and toxicity in patients (pts) with hormone receptor-positive, HER2-negative early breast cancer (HR+, HER2– eBC) treated with adjuvant (adj) endocrine therapy (ET) in the CANcer TOxicities (CANTO) study. Annals of Oncology 2023; 34, S320 - S321. Available from: https://www.annalsofoncology.org/article/S0923-7534(23)01912-9/fulltext.
- Jing, F., Zhu, Z., Qiu, J., Tang, L., Xu, L., Xing, W., Hu, Y. Contemporaneous symptom networks and correlates during endocrine therapy among breast cancer patients: A network analysis. Frontiers in Oncology 2023; 13, 1081786. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10103712/.
- Sella, T., Poorvu, P.D., Ruddy, K.J., Gelber, S.I., Tamimi, R.M., Peppercorn, J.M., Schapira, L., Borges, V.F., Come, S.E., Partridge, A.H., Rosenberg, S.M. Impact of fertility concerns on endocrine therapy decisions in young breast cancer survivors. Cancer 2021; 127(16), 2888-2894. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC8351455/.
- Winstead, E. (2023) Pausing Long-Term Breast Cancer Therapy to Become Pregnant Appears to Be Safe. Cancer Currents Blog. [internet]. 2023 [cited 2025 January 2] Available from: https://www.cancer.gov/news-events/cancer-currents-blog/2023/pausing-breastcancer-treatment-to-conceive.
- Partridge, A.H., Nima, S.M., Ruggeri, M., Peccatori, F.A., Azim, Colleoni M., Saura, C., Shimizu, C., Sætersdal, A.B., Kroep, J.R., Mailliez, A., Warner, E., Borges., Amant, F., Gombos, A., Kataoka, A., Rousset-Jablonski, C., Borstnar, S., Takei, J., Lee, J.E, Walshe, J.M., Ruíz-Borrego ,M., Moore, H.C.F., Saunders, C., Bjelic-Radisic, V., Susnjar, S., Cardoso, F., Smith, K.L., Ferreiro, T., Ribi, K., Ruddy, K., Kammler, R., El-Abed, S., Viale, G., Piccart ,M., Korde, L.A., Goldhirsch, A., Gelber, R.D., Pagani, O. Interrupting Endocrine Therapy to Attempt Pregnancy after Breast Cancer. The New England Journal of Medicine 2023; 388(18),1645-1656. Available from: https://www.nejm.org/doi/full/10.1056/NEJMoa2212856.
- Jimmy, B., Jose, J. Patient medication adherence: measures in daily practice. Oman Medical Journal 2011; 26(3),155-9. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC3191684/.
- Haskins, C.B., McDowell, B.D., Carnahan, R.M., Fiedorowicz, J.G., Wallace, R.B., Smith, B.J., Chrischilles, E.A. Breast cancer endocrine therapy adherence in health professional shortage areas: Unique effects on patients with mental illness. Journal of Psychosomatic Research 2021; 140, 110294. Available from: https://www.sciencedirect.com/science/article/pii/S0022399920308564.
- Sharma, A., Jasrotia, S., Kumar, A. Effects of Chemotherapy on the Immune System: Implications for Cancer Treatment and Patient Outcomes. Naunyn-Schmiedeberg’s Arch Pharmacology 2024; 397, 2551–2566. Available from: https://link.springer.com/article/10.1007/s00210-023-02781-2.
- Hung, W., Chow, S. Optimizing Medication Use in Older Adults. Clinical Therapeutics 2020; 42(4), 556-558. Available from: https://www.clinicaltherapeutics.com/article/S0149-2918(20)30126-0/fulltext.
- Salter, C., McDaid, L., Bhattacharya, D., Holland, R., Marshall, T., Howe, A. Abandoned acid? Understanding adherence to bisphosphonate medications for the prevention of osteoporosis among older women: a qualitative longitudinal study. PLoS One 2014; 9(1), e83552.Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC3879247/.
- Sipos, M., Farcas, A., Prodan, N., Mogosan, C. Relationship between beliefs about medicines and adherence in elderly patients with cardiovascular and respiratory diseases: A cross-sectional study in Romania. Patient Education and Counselling 2021; 104(4), 911-918. Available from: https://www.sciencedirect.com/science/article/abs/pii/S0738399120304766.
- Al-Qerem, W., Jarab, A.S., Badinjki, M., Hyassat, D., Qarqaz, R. Exploring variables associated with medication non-adherence in patients with type 2 diabetes mellitus. PLoS One 2021; 16(8), e0256666. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC8382191/.
- Ozumba, L.N., Dienye, P., Ndukwu, G. Role of Illness Perception and Medication Beliefs in Medication Adherence among Hypertensive Patients. The Anatolian Journal of Family Medicine 2023; 6(1),31-36. Available from: https://jag.journalagent.com/ajfamed/pdfs/ANATOLJFM_6_1_31_36.pdf.
- Al Bawab, A.Q., Al-Qerem, W., Abusara, O., Alkhatib, N., Mansour, M., Horne, R. What Are the Factors Associated with Nonadherence to Medications in Patients with Chronic Diseases? Healthcare (Basel) 2021; 9(9), 1237. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC8469667/.
- Rathbone, A.P., Jamie, K., Todd, A., Husband, A. (A qualitative study exploring the lived experience of medication use in different disease states: Linking experiences of disease symptoms to medication adherence. Journal of Clinical Pharmacy and Therapeutics 2021; 46(2), 352-362. Available from: https://onlinelibrary.wiley.com/doi/10.1111/jcpt.13288.
- Świątoniowska-Lonc, N., Polański, J., Mazur, G., Jankowska-Polańska, B. Impact of Beliefs about Medicines on the Level of Intentional Non-Adherence to the Recommendations of Elderly Patients with Hypertension. International Journal of Environmental Research and Public Health 2021; 18(6), 2825. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC7998243/.
- Marasine, N.R., Sankhi, S. Factors Associated with Antidepressant Medication Non-adherence. Turkish Journal of Pharmaceutical Science 2021; 18(2), 242-249. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC8100773/.
- Cinar, F.I., Mumcu, Ş., Kiliç, B., Polat, Ü., Bal Özkaptan, B. Assessment of Medication Adherence and Related Factors in Hypertensive Patients: The Role of Beliefs About Medicines. Clinical Nursing Research 2021; 30(7),985-993. Available from: https://journals.sagepub.com/doi/10.1177/1054773820981381.
- Kim, S.H., Cho, Y.U., Kim, S.J., Han, M.S. Changes in Bone Mineral Density in Women With Breast Cancer: A Prospective Cohort Study. Cancer Nursing 2019; 42(2), 164-172. Available from: https://journals.lww.com/cancernursingonline/fulltext/2019/03000/changes_in_bone_mineral_density_in_women_with.9.aspx.
- Malik, L. (The dilemmas of breast cancer treatment and increased fracture risk. Annals of Oncology, 2014;25(8), 1664. Available from: https://www.annalsofoncology.org/article/S0923-7534(19)34831-8/fulltext.
- Rachner, T.D., Coleman, R., Hadji, P., Hofbauer, L.C. Bone health during endocrine therapy for cancer. Lancets Diabetes & Endocrinology 2018; 6(11), 901-910. Available from: https://www.sciencedirect.com/science/article/abs/pii/S2213858718300470.
- Bouvard, B., Soulié, P., Hoppé, E., Georgin-Mege, M., Royer, M., Mesgouez-Nebout, N., Lassalle, C., Cellier, P., Jadaud, E., Abadie-Lacourtoisie, S., Tuchais, C., VinchonPetit, S., Audran, M., Chappard, D., Legrand, E. Fracture incidence after 3 years of aromatase inhibitor therapy. Annals of Oncology 2014; 25(4),843-847. Available from: https://www.sciencedirect.com/science/article/pii/S092375341936497X.
- Smajic, E., Avdic, D., Pasic, A., Prcic, A., Stancic, M. Mixed Methodology of Scientific Research in Healthcare. Acta Informatica Medica 2022; 30(1), 57-60. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC9226784/.
- Greenlaw, C., Brown-Welty, S. A Comparison of Web-Based and Paper-Based Survey Methods. Evaluation Review 2009; 33(5),464-80. Available from: https://www.researchgate.net/publication/26674054_A_Comparison_of_Web-Based_and_Paper-Based_Survey_Methods_Testing_Assumptions_of_Survey_Mode_and_Response_Cost.
- Lee, A.Y., Lyons, A.T., Makris, V., Kamaraju, S., Stolley, M.R., Neuner, J.M., Flynn, K.E. Adherence to adjuvant endocrine therapy for breast cancer: a qualitative exploration of attribution of symptoms among post-menopausal women. Support Care Cancer 2024; 32(4):265. Available from https://link.springer.com/article/10.1007/s00520-024-08463-w.
- Chalela, P., Munoz, E., Inupakutika, D., Kaghyan, S., Akopian, D., Kaklamani, V., Lathrop, K., Ramirez A. Improving adherence to endocrine hormonal therapy among breast cancer patients: Study protocol for a randomized controlled trial. Contempory Clinical Trials Communications 2018; 12,109-115. Available from: https://www.sciencedirect.com/science/article/pii/S2451865418300784.
- Wu M-J., Zhao K., Fils-Aime F. Response rates of online surveys in published research: A meta-analysis. Computers in Human Behavior Reports 2022 May 5;7, 100206. Available from: https://www.sciencedirect.com/science/article/pii/S2451958822000409.
- Gumpili, S.P., Das, A.V. Sample size and its evolution in research. IHOPE Journal of Ophthalmology 2022; 1(1), 9-13. Available from: https://ihopejournalofophthalmology.com/sample-size-and-its-evolution-in-research/.
- Jimenez, K., Vargas, C., Garcia, K., Guzman, H., Angulo, M., Billimek, J. Evaluating the Validity and Reliability of the Beliefs About Medicines Questionnaire in Low-Income, Spanish-Speaking Patients With Diabetes in the United States. Diabetes Education 2017; 43(1), 114-124. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC5899517/.
- Harland, N., Holey, E. Including open-ended questions in quantitative questionnaires—theory and practice. International Journal of Therapy and Rehabilitation 2013; 18(9). Available from: https://www.magonlinelibrary.com/doi/full/10.12968/ijtr.2011.18.9.482.
- Singer, E., Couper, M.P. Some Methodological Uses of Responses to Open Questions and Other Verbatim Comments in Quantitative Surveys. Methods, Data, Analyses 2017; 11(2),20. Available from: https://d-nb.info/1192141725/34.
- Riegel B. I Forgot: Memory and Medication Adherence in Heart Failure. Circulation. Heart Failure 2016; 9(12). Available from: https://www.ahajournals.org/doi/10.1161/CIRCHEARTFAILURE.116.003642.
- Glick, I., Zamora, D., Davis, J.M., Suryadevara, U., Goldenson, A., Kamis, D. Are Patients With Schizophrenia Better Off With Lifetime Antipsychotic Medication?: Replication of a Naturalistic, Long-Term, Follow-Up Study of Antipsychotic Treatment. Journal of Clinical Psychopharmacology 2020; 40(2),145-148. Available from: https://journals.lww.com/psychopharmacology/abstract/2020/03000/are_patients_with_schizophrenia_better_off_with.7.aspx.
- Wright, F., Malone, S.K., Wong, A., D’Eramo Melkus, G., Dickson, V.V. Addressing Challenges in Recruiting Diverse Populations for Research: Practical Experience From a P20 Center. Nursing Research 2022; 71(3), 218-226. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC9038626/.
- Andrade, C. Sample Size and its Importance in Research. Indian Journal of Psychological Medicine 2020; 42(1), 102-103. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC6970301/.
- Guyot, M., Pelgrims, I., Aerts, R., Keune, H., Remmen, R., De Clercq, E.M., Thomas, I., Vanwambeke, S.O. Non-response bias in the analysis of the association between mental health and the urban environment: a cross-sectional study in Brussels, Belgium. Archives of Public Health 2023; 81(1), 129.Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10327324/ [Accessed 30 December 2024].
- Curtis, S. and Rees Jones, I. Is There a Place for Geography in the Analysis of Health Inequality? Sociology of Health & Illness 1998; 20, 645672. Available from: https://onlinelibrary.wiley.com/doi/epdf/10.1111/1467-9566.00123.
- Cabral, A.C., Moura-Ramos, M., Castel-Branco, M., Caramona, M., Fernandez-Llimos, F., Figueiredo, I.V. Influence of the mode of administration on the results of medication adherence questionnaires. Journal of Evaluation in Clinical Practice 2017; 23(6), 1252-1257. Available from: https://onlinelibrary.wiley.com/doi/epdf/10.1111/jep.12773.
- Lechner, C.M., Partsch, M.V., Danner, D., Rammstedt, B. (2019) Individual, situational, and cultural correlates of acquiescent responding: Towards a unified conceptual framework. British Journal of Mathematical and Statistical Psychology 2019; 72(3),426-446. Available from: https://bpspsychub.onlinelibrary.wiley.com/doi/10.1111/bmsp.12164.
- Adams-Quackenbush, N.M., Horselenberg, R., Hubert, J., Vrij, A., van Koppen, P. Interview expectancies: awareness of potential biases influences behaviour in interviewees. Psychiatry, Psychology Law and Law 2019; 26(1), 150-166. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC6762119/.
- Jindal, T., Sinha, R.K., Mukherjee, S., Mandal, S.N., Karmakar, D. Misinterpretation of the international prostate symptom score questionnaire by Indian patients. Indian Journal of Urology 2014; 30(3), 252-5. Available from: https://journals.lww.com/indianjurol/fulltext/2014/30030/misinterpretation_of_th e_international_prostate.4.aspx.
- Kusmaryono, I., Wijayanti, D., Maharani, H.R. Number of Response Options, Reliability, Validity, and Potential Bias in the Use of the Likert Scale Education and Social Science Research: A Literature Review. International Journal of Educational Methodology 2022; 8(4), 625-637. Available from: https://pdf.ijem.com/IJEM_8_4_625.pdf.
- Zulman, D.M, Slightam, C.A., Brandt, K., Lewis, E.T., Asch, S.M., Shaw, J.G. “They are interrelated, one feeds off the other”: A taxonomy of perceived disease interactions derived from patients with multiple chronic conditions. Patient Education and Counselling 2020; 103(5), 1027-1032. Available from: https://www.sciencedirect.com/science/article/pii/S0738399119305270.
- Sun, X., Briel, M., Busse, J.W., You, J.J., Akl, E.A., Mejza, F., Bala, M.M., Bassler, D., Mertz, D., Diaz-Granados, N., Vandvik, P.O., Malaga, G., Srinathan, S.K., Dahm, P., Johnston, B.C., Alonso-Coello, P., Hassouneh, B., Truong, J., Dattani, N.D., Walter, S.D., Heels-Ansdell, D., Bhatnagar, N., Altman, D.G., Guyatt, G.H. The influence of study characteristics on reporting of subgroup analyses in randomised controlled trials: systematic review. BMJ 2011; 342, d1569. Available from: https://www.bmj.com/content/342/bmj.d1569.
- Thomson, P., Rushworth, G.F., Andreis, F., Angus, N.J., Mohan, A.R., Leslie, S.J. Longitudinal study of the relationship between patients’ medication adherence and quality of life outcomes and illness perceptions and beliefs about cardiac rehabilitation. BMC Cardiovasc Disorders 2020; 20(1),71. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC7011382/.
- Luong, G., Charles, S.T., Rook, K.S., Reynolds, C.A., Gatz, M. Age differences and longitudinal change in the effects of data collection mode on self-reports of psychosocial functioning. Psychol Aging 2015; 30(1), 106-119. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC4362730/.
Figure 1.
Response Rates of Distributed Postal Questionnaire.
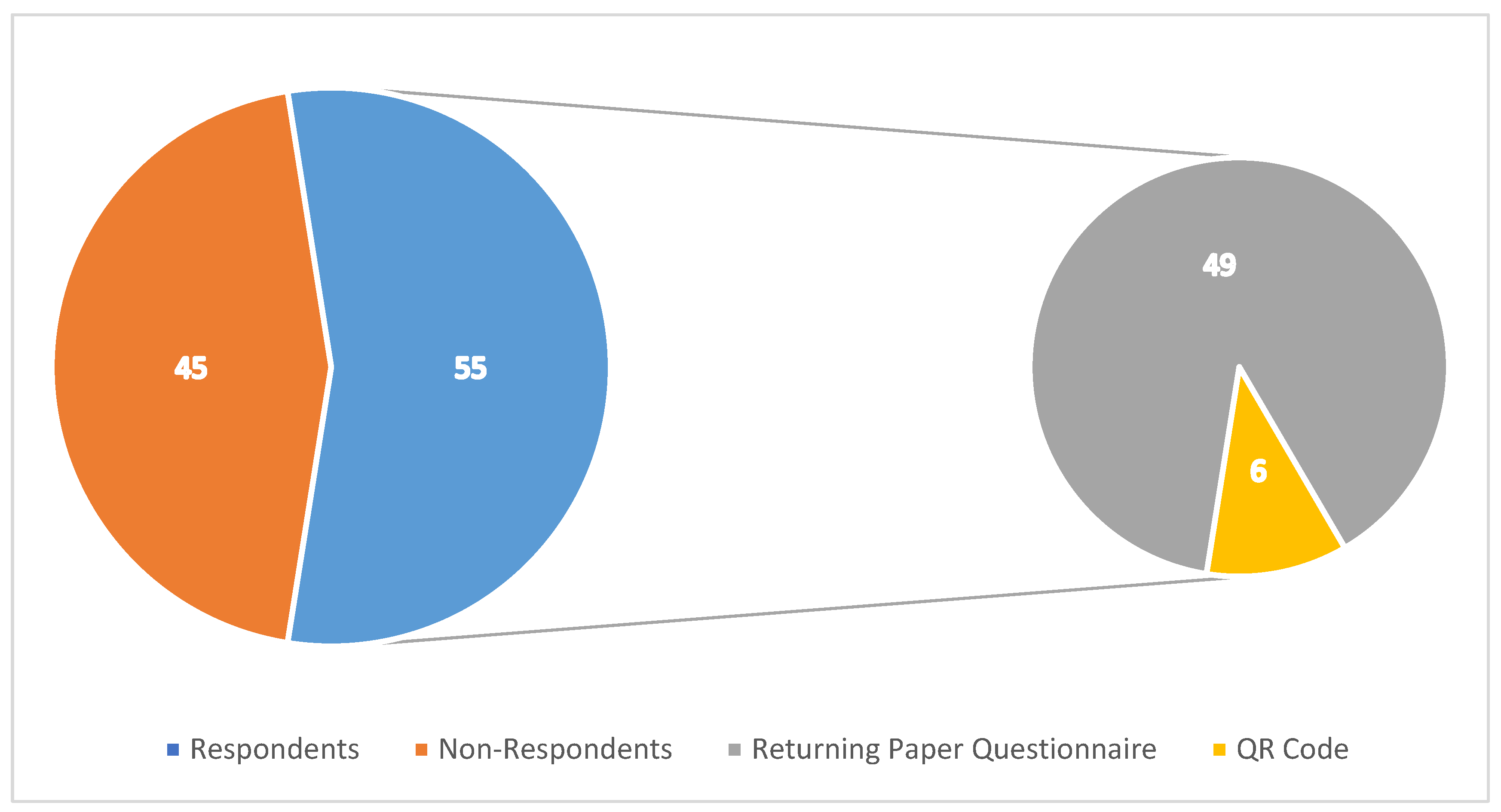
Figure 2.
Age of Diagnosis of Patients.
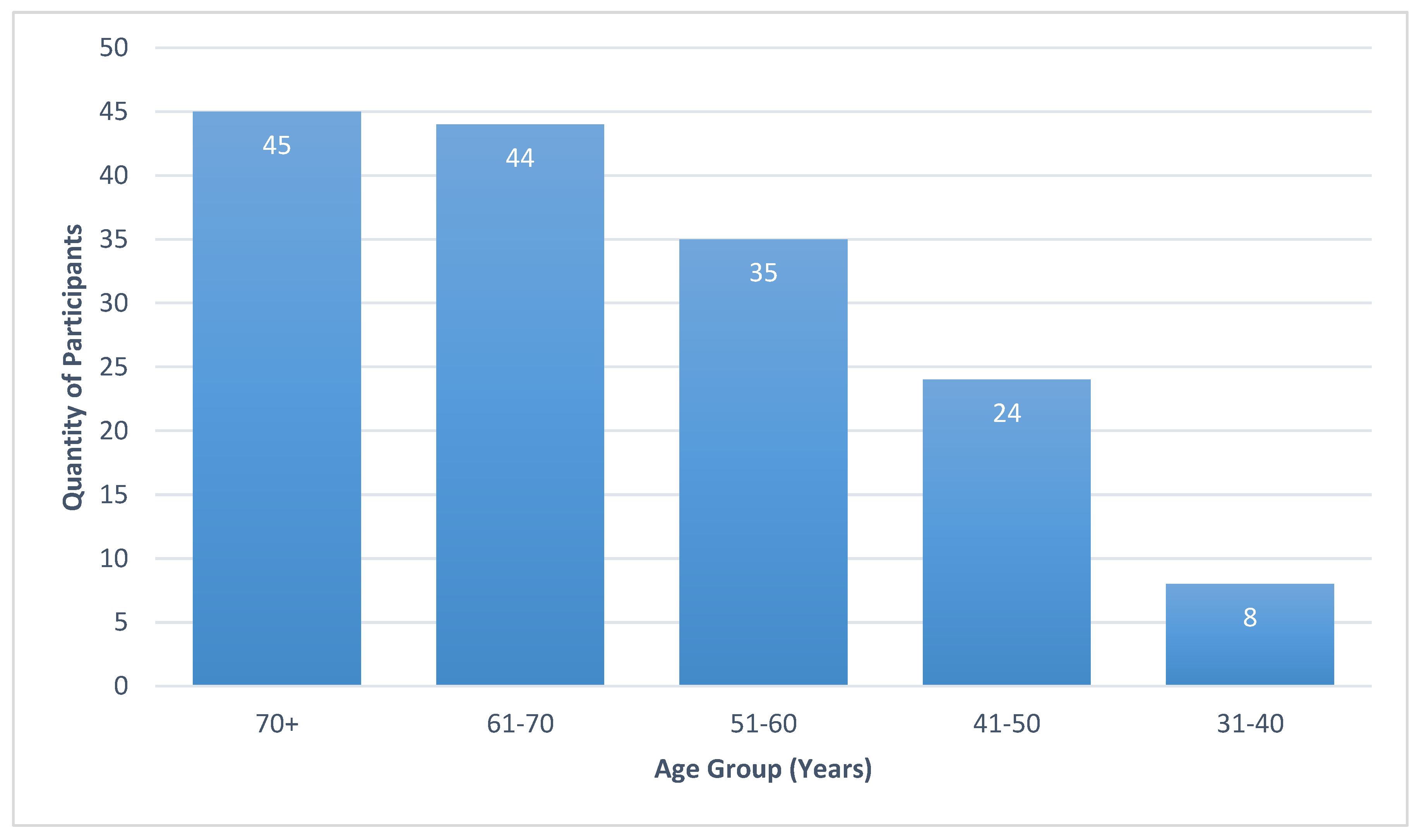
Figure 3.
The Highest Level of Education Achieved by Participants of the Study.
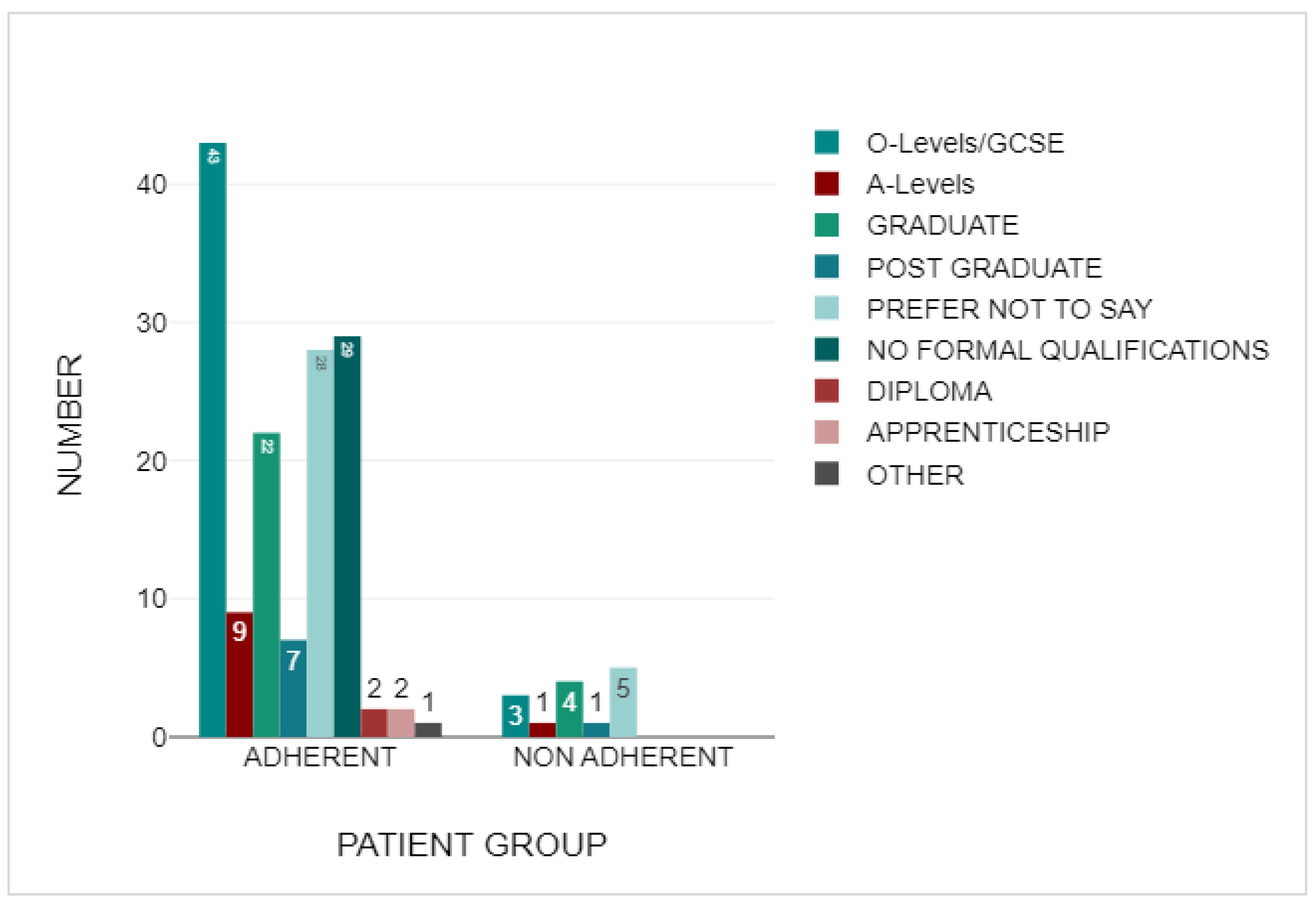
Figure 4.
Proportion of Patients within this trial who were Adherent and Non-Adherent to their AET.
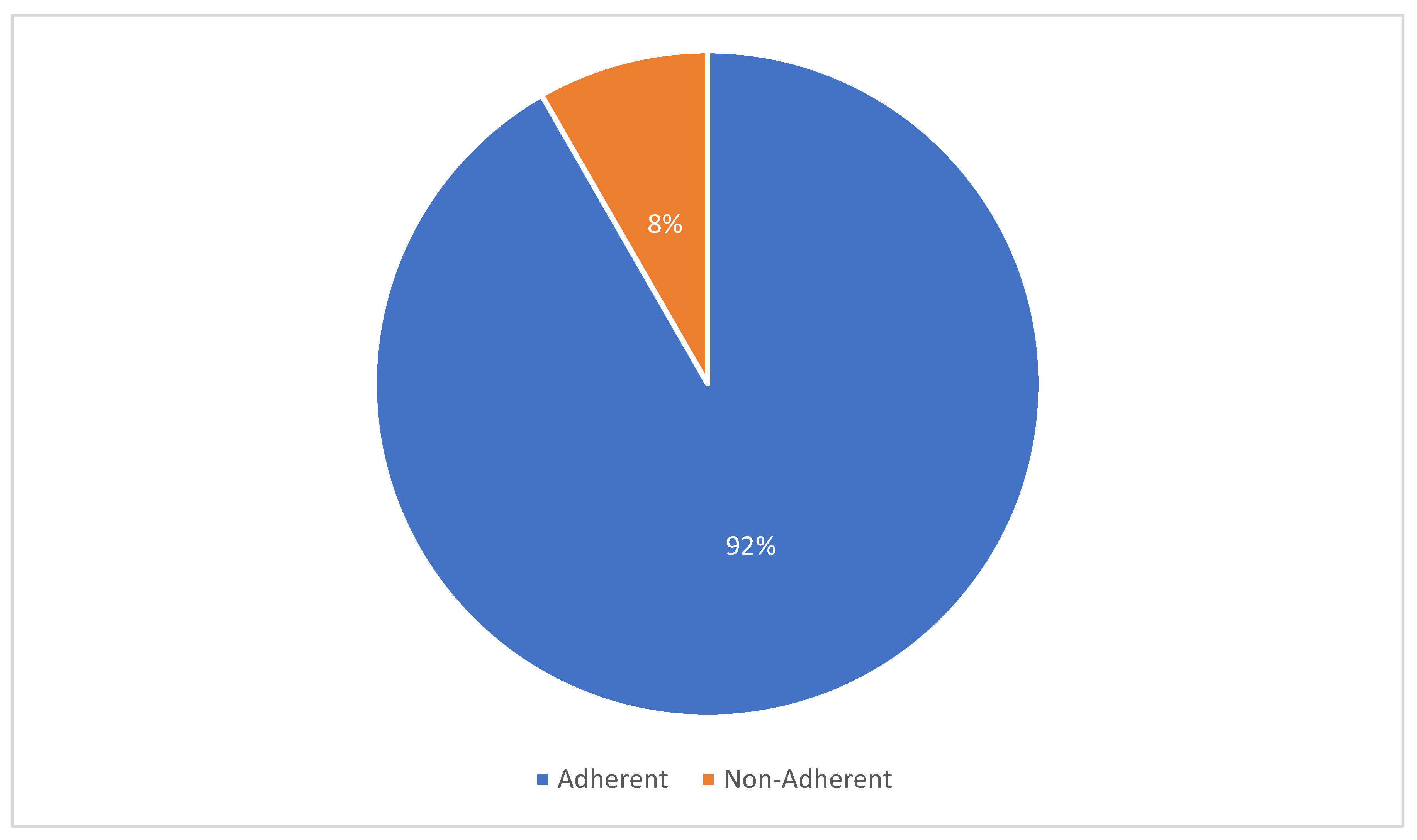
Figure 5.
The age of diagnosis for BC of individuals within the Adherent group.
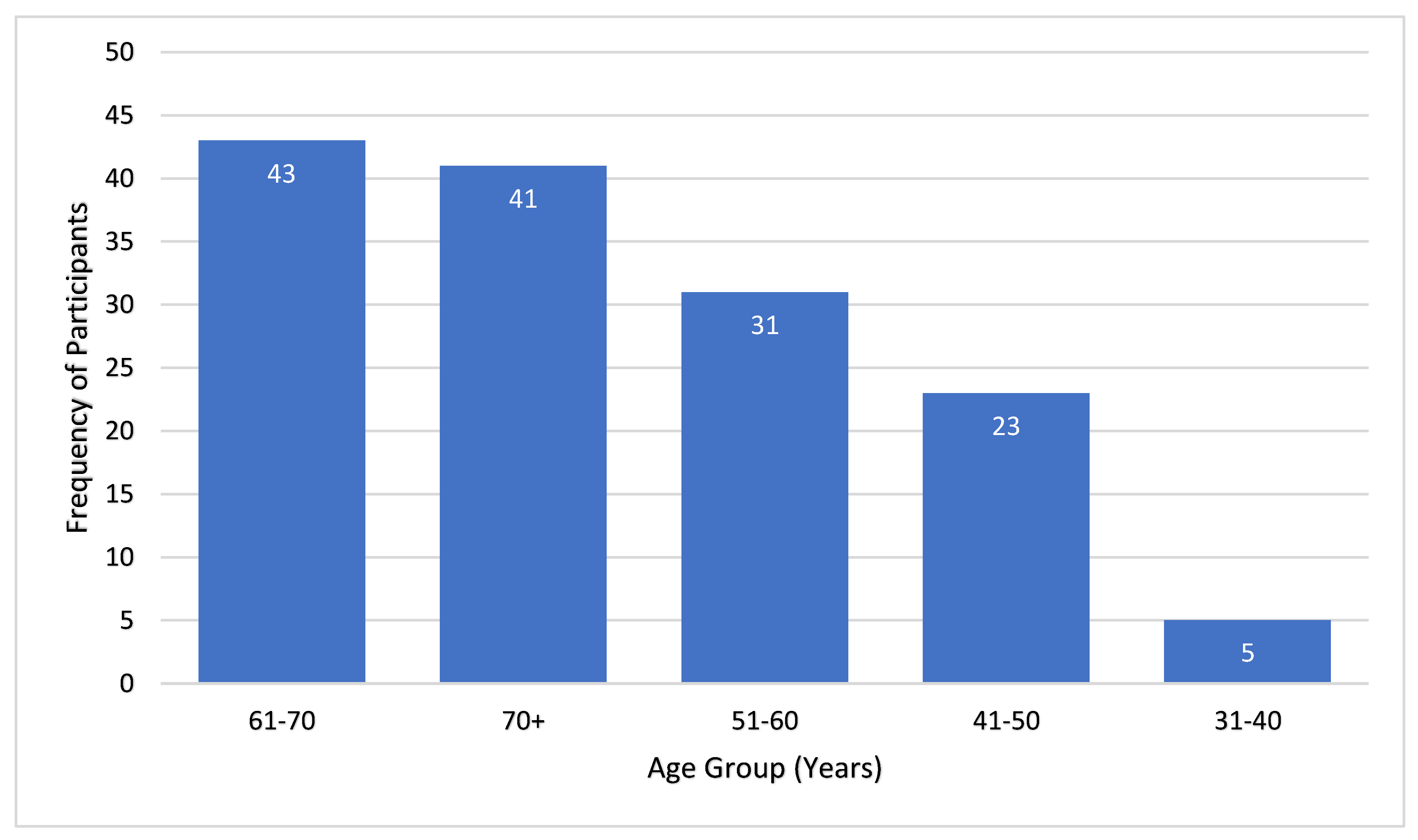
Figure 6.
The Highest Level of Education Achieved within the Adherent Group.
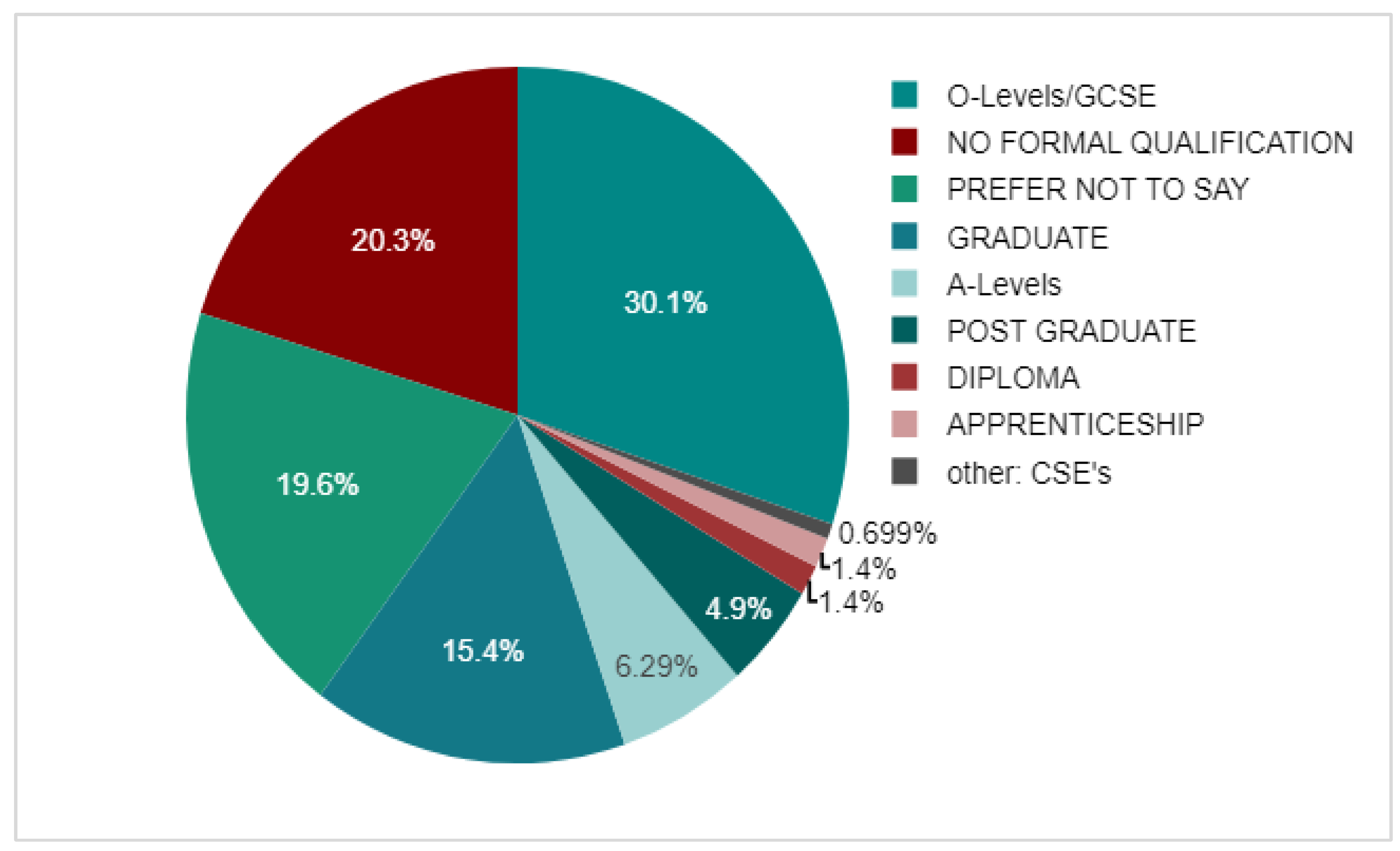
Figure 7.
The age of diagnosis for BC of individuals within the non-adherent group.
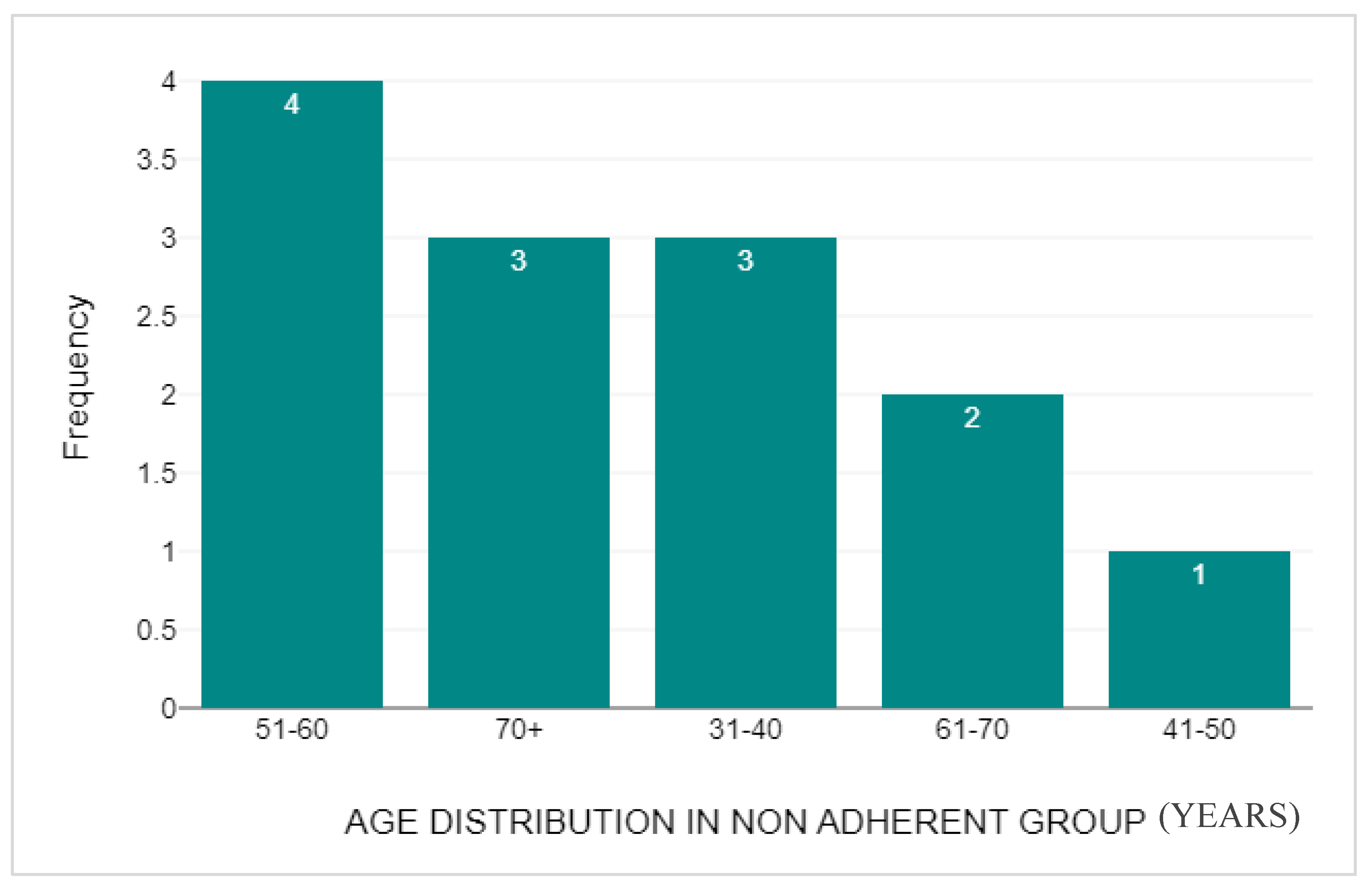
Figure 8.
The Highest Level of Education Achieved within the Non-adherent Group.
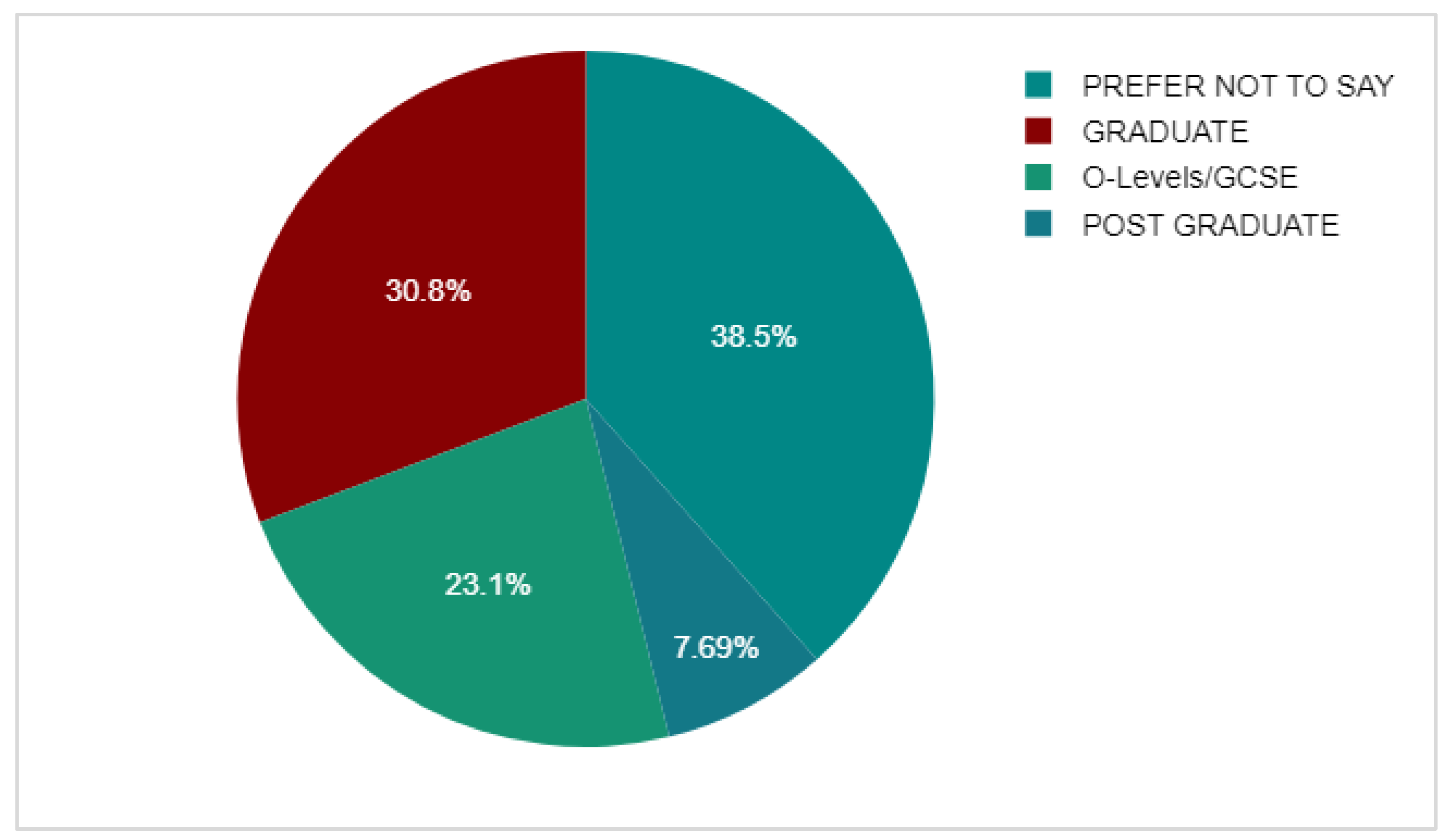
Figure 9.
The Duration in Months of AET Treatment before stoppage within Non-adherent Group.
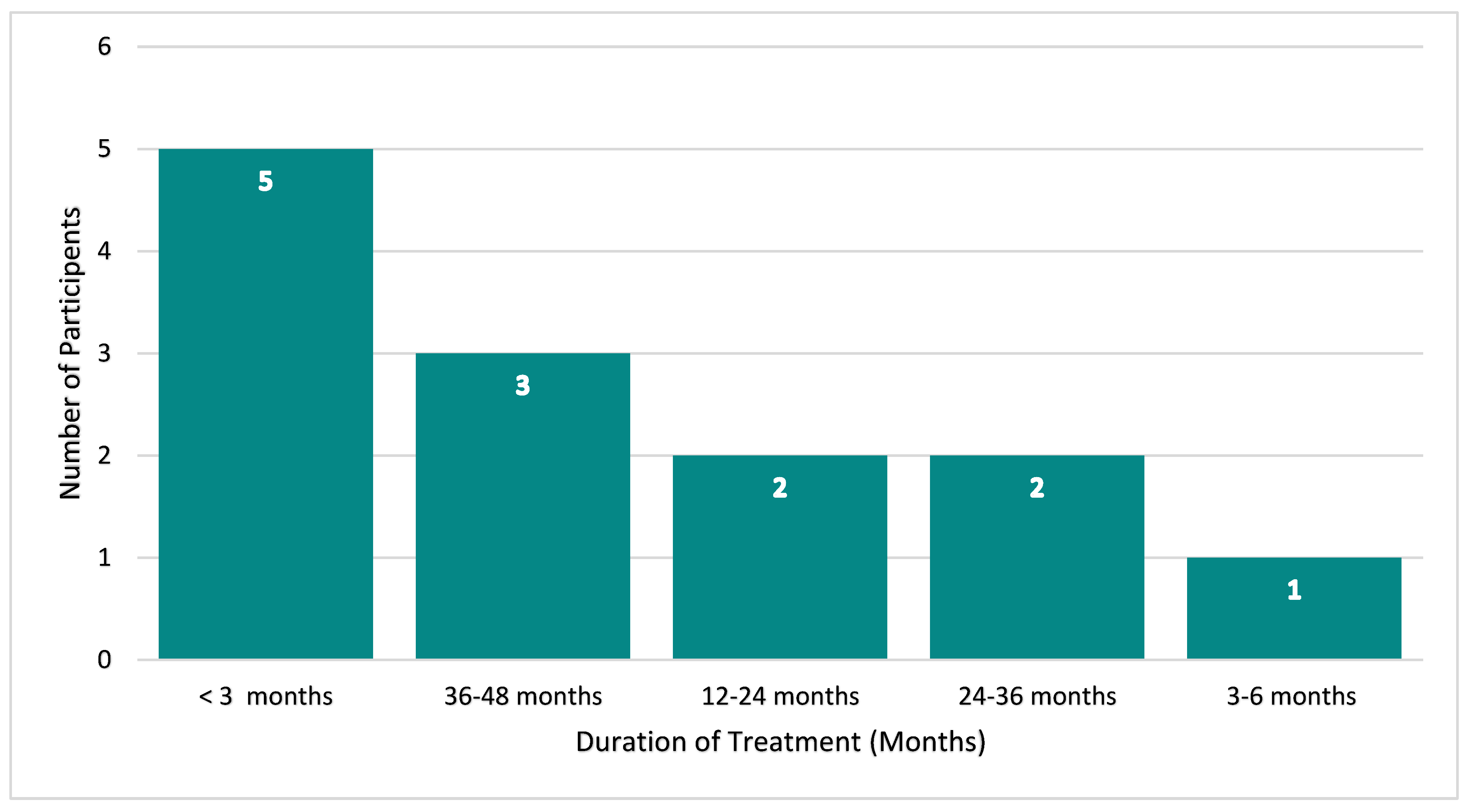
Figure 10.
The Comparison between BMQ-AET Necessity Score between the Non—Adherent and Adherent Group.
Figure 10.
The Comparison between BMQ-AET Necessity Score between the Non—Adherent and Adherent Group.
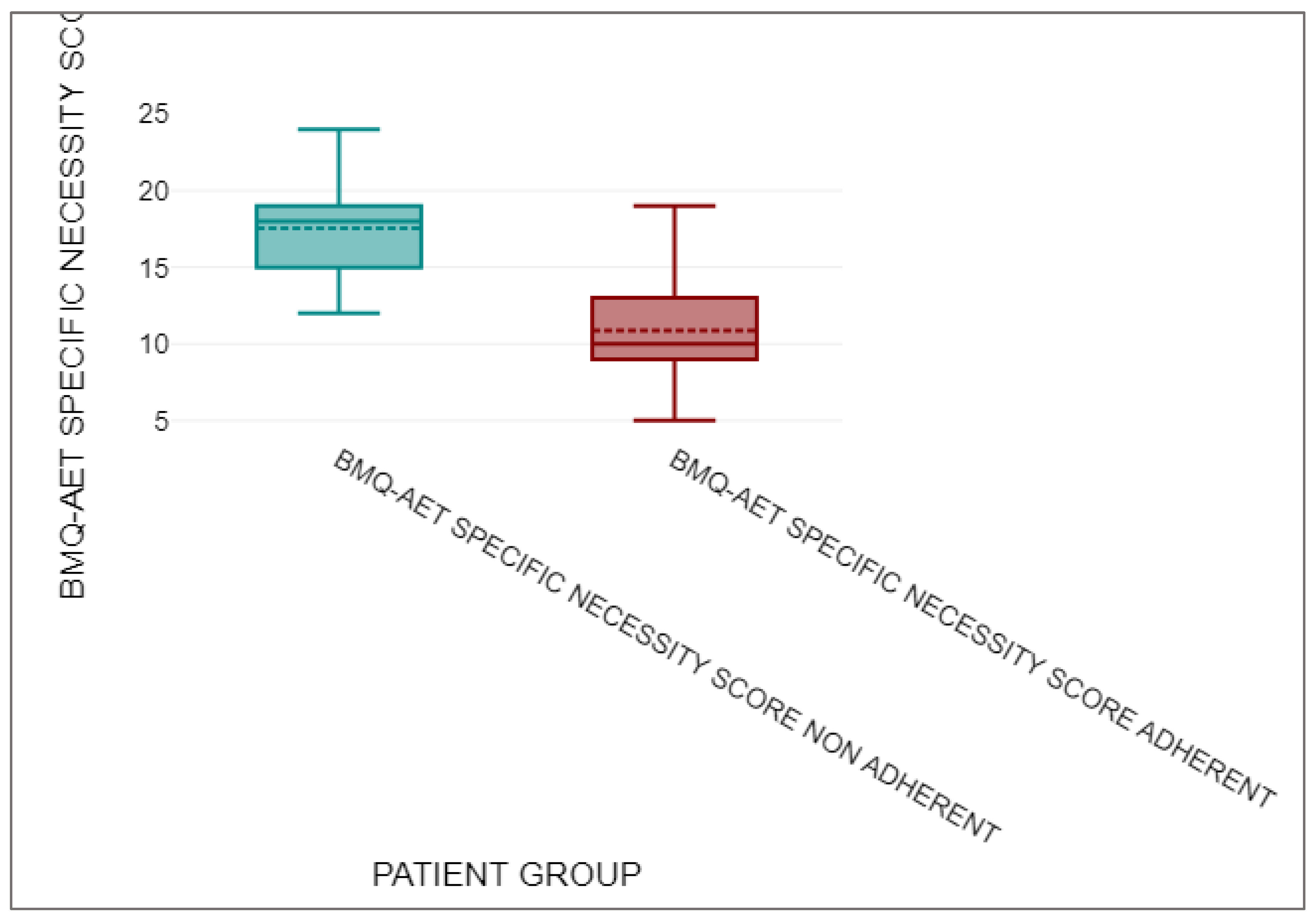
Figure 11.
The Comparison between BMQ-AET Concerns Score between the Non—Adherent and Adherent Group.
Figure 11.
The Comparison between BMQ-AET Concerns Score between the Non—Adherent and Adherent Group.
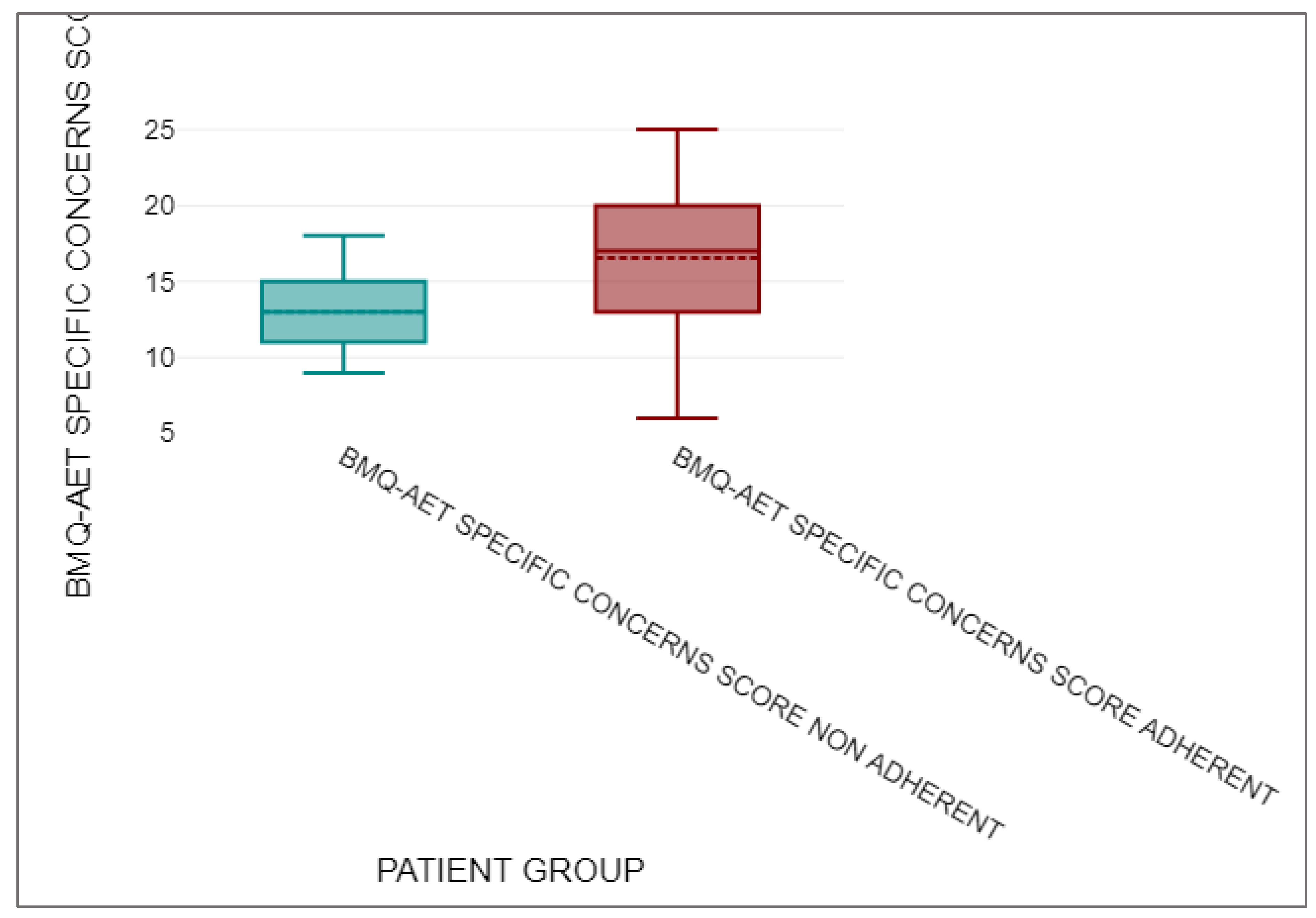
Figure 12.
The Number of Participants with various BMD on the baseline DEXA scan.
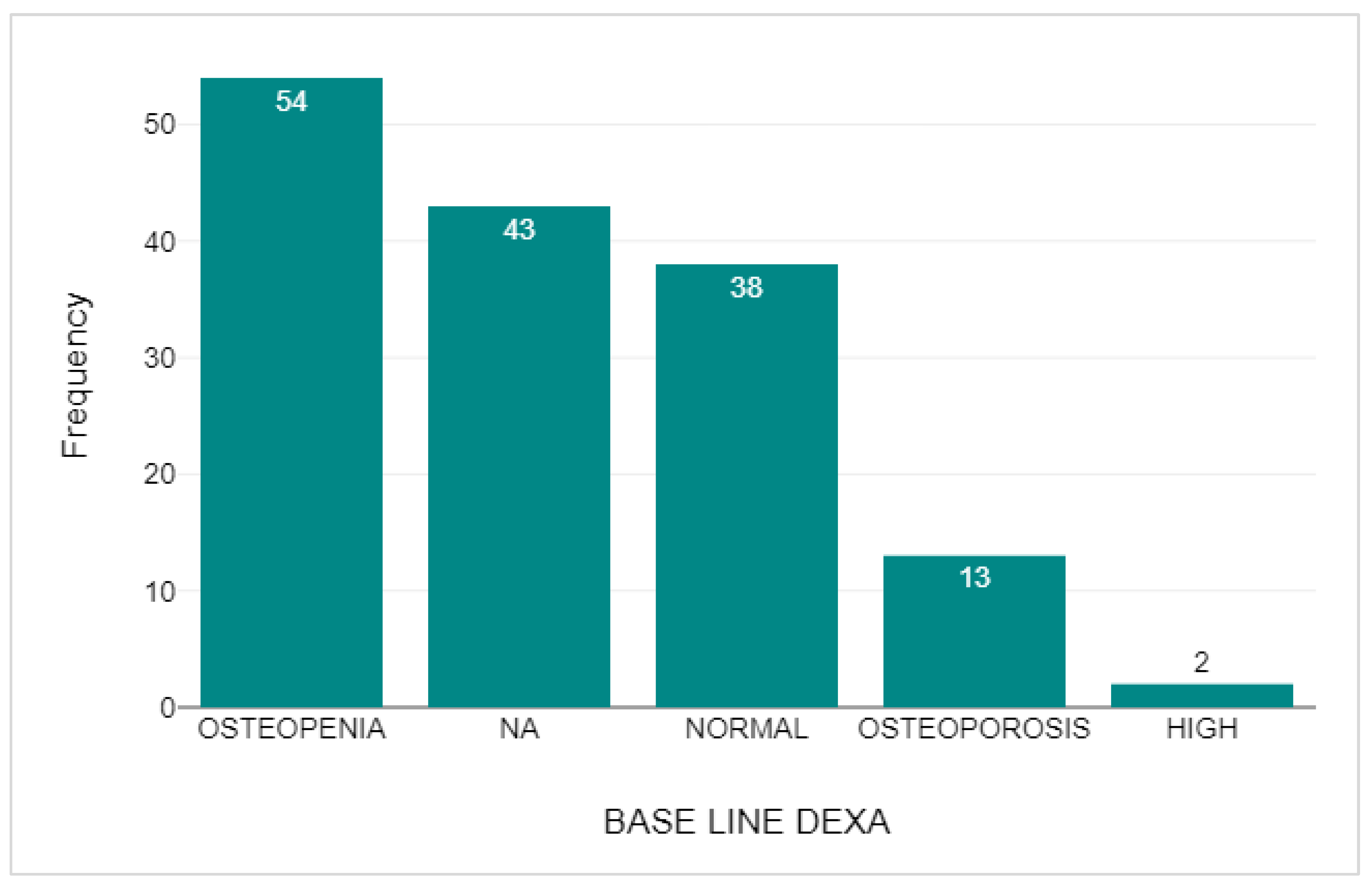
Figure 13.
The Comparison of BMD on follow up DEXA against baseline DEXA scan.
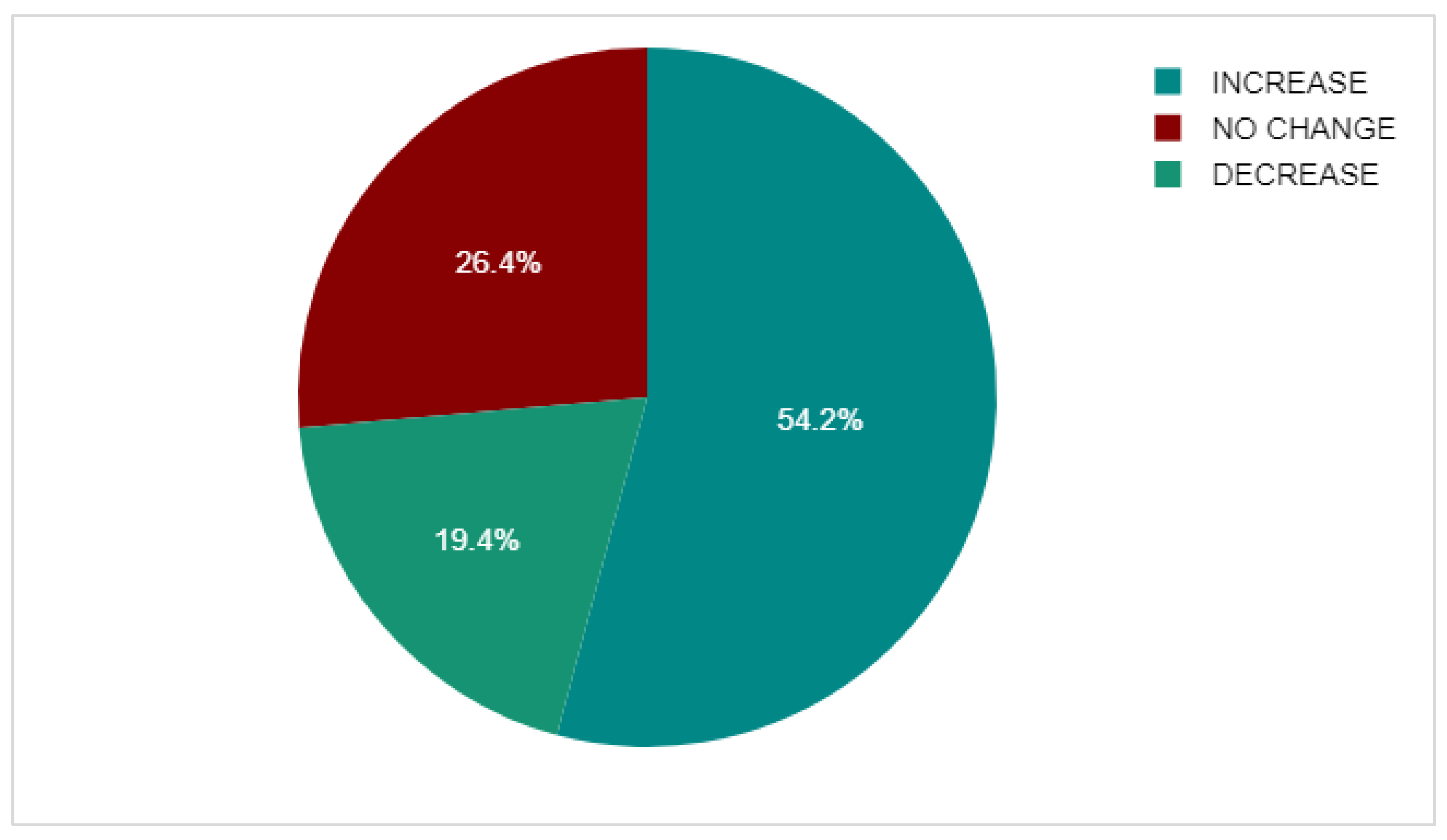

Table 1.
The results found from the comparison of BMQ-AET Necessity score between the adherent and non-adherent groups within the study.
Table 1.
The results found from the comparison of BMQ-AET Necessity score between the adherent and non-adherent groups within the study.
| n | Mean | Median | Standard deviation | ||
| BMQ-AET SPECIFIC NECESSITY SCORE NON-ADHERENT | 13 | 17.54 | 18 | 3.15 | |
| BMQ-AET SPECIFIC NECESSITY SCORE ADHERENT | 143 | 10.86 | 10 | 3.13 |
Table 2.
The Results found from the Comparison of BMQ-AET Concerns Score between the adherent and non-adherent groups within the study.
Table 2.
The Results found from the Comparison of BMQ-AET Concerns Score between the adherent and non-adherent groups within the study.
| n | Mean | Median | Standard deviation | ||
| BMQ-AET SPECIFIC CONCERNS SCORE NON-ADHERENT | 13 | 13 | 13 | 2.68 | |
| BMQ-AET SPECIFIC CONCERNS SCORE ADHERENT | 143 | 16.54 | 17 | 4.24 |
Table 3.
The Results found from the Mann-Whitney U-Test comparing BMQ-AET Specific Concerns Score for the Adherent Group against the BMQ-AET Specific Concerns Score for the Non-Adherent Group.
Table 3.
The Results found from the Mann-Whitney U-Test comparing BMQ-AET Specific Concerns Score for the Adherent Group against the BMQ-AET Specific Concerns Score for the Non-Adherent Group.
| U | z | asymptotic p | exact p | r | |
| 452.5 | -3.07 | 0.002 | 0.002 | 0.25 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



