Introduction
Menopause is a universal biological milestone, defined as the permanent cessation of menstruation for 12 consecutive months in the absence of other pathological or physiological causes [
1]. It signifies the transition from the reproductive to the non-reproductive stage of life. It is typically preceded by a perimenopausal phase characterised by irregular menstrual cycles and the onset of vasomotor, somatic, and psychological symptoms. Following the final menstrual period, women enter the post-menopausal stage. In Sri Lanka, the average age at natural menopause is reported to be between 49 and 51 years, which means that many women will spend almost one-third of their lifespan in the post-menopausal period [
2,
3]. With female life expectancy now approaching 78 years, an estimated one-quarter of Sri Lankan women over the age of 50 are post-menopausal, underscoring the growing demographic and public health significance of this life stage [
4]. Further, Sri Lanka is ageing rapidly; the proportion of older adults is growing and projections show a large rise in the share of elderly people over the coming decades making mid-life and post-reproductive health an expanding national priority.
Menopause can occur spontaneously through the natural depletion of ovarian follicles, or it may be induced [
5,
6]. Induced menopause arises either surgically, through bilateral oophorectomy or hysterectomy involving the ovaries, or medically, as a result of gonadotoxic therapies such as chemotherapy or pelvic radiotherapy [
7]. Induced menopause frequently occurs at younger ages than natural menopause. It is associated with a more abrupt decline in oestrogen, often resulting in more severe symptoms and an elevated risk of long-term sequelae such as osteoporosis, cardiovascular disease, and cognitive decline [
8].
Despite this, cultural attitudes in Sri Lanka, just like for any other low- and middle-income countries or ethnic minority population, continue to frame menopause largely as a natural and inevitable stage of ageing [
3]. Many women, therefore, manage symptoms independently and may not seek medical support due to limited awareness, socio-cultural stigma, or restricted access to care [
9,
10]. This tendency contributes to under-reporting of symptoms and low healthcare utilisation, leaving the broader epidemiological and clinical profile of menopause insufficiently characterised.
Moreover, much of the current Sri Lankan data are cross-sectional, geographically limited, qualitative or focused on single outcomes (symptoms, knowledge, or attitudes). A comprehensive clinical-epidemiological profile spanning perimenopause, menopause and post-menopause across diverse settings is lacking. Hence, this study aims to address this gap by describing the demographic and clinical characteristics of Sri Lankan women across the perimenopausal, menopausal, and post-menopausal stages, and by examining the distribution of natural, surgical, and medical menopause, to inform healthcare strategies tailored to this growing population.
Methods
Study Design and ๒
We conducted an epidemiological analysis of data from the Sri Lankan chapter of the MARIE-WP2a work-stream that enrolled women experiencing perimenopause, menopause and post-menopause.
Case Definitions
Perimenopausal status was defined as irregular menstrual cycles accompanied by typical menopausal symptoms. Post-menopausal status was defined as the absence of menstruation for at least 12 consecutive months. Natural menopause was defined as the spontaneous cessation of menstruation due to ageing. Surgical menopause was recorded when ovarian function ceased due to bilateral oophorectomy. Medical menopause was attributed to the use of chemotherapy or radiotherapy, resulting in ovarian failure. Where menopause type was missing but hysterectomy was reported, the case was recoded as surgical menopause.
Data Collection and Variables
Structured questionnaires and interviews collected demographic data such as age, city of residence, ethnicity, and reproductive and clinical histories, and menopause-related details (status, type, age at menopause). Free-text responses on long-term conditions, medication use, and reasons for non-use of hormone replacement therapy (HRT), use of traditional medicines were systematically coded.
Ethics
All participants provided written informed consent, and the study protocol was approved by Ethical Review Committee, Faculty of Allied Health Sciences, University of Ruhuna, Sri Lanka (Ref. No: 2025.02.532). The study was conducted in accordance with the Declaration of Helsinki.
Data Cleaning and Quality Control
Implausible values were excluded a priori: age outside 35–100 years and age at menopause outside 20–65 years were treated as missing. No imputation was performed; complete-case analysis was adopted.
Statistical Analysis
Descriptive analyses summarised continuous variables using mean, standard deviation (SD), median, and range, and categorical variables as counts and proportions with Wilson 95% confidence intervals (CIs) (Supplementary S2). Menopausal status and type distributions were reported for the overall cohort and stratified where relevant. Age at menopause was described overall and by type of menopause. Inequalities analysis examined menopause type across cities and ethnic groups. To avoid instability, strata with fewer than five women were excluded from range estimates. We report absolute ranges of prevalence across groups.
Basic demographic information, such as age and parity, was collected via a structured questionnaire or interview. Clinical details, including the type of menopause (natural/medical/surgical) and any relevant medical diagnoses, were confirmed based on the participant responses within the demographic questionnaire. Descriptive statistics were used to summarise the data. We computed measures of central tendency (mean, median) and dispersion (SD, range) for age. The proportions of women in each category of menopausal status and menopause type were calculated. The results are presented in tables for clarity.
We conducted a multilevel analysis using individual-level data from the Sri Lankan arm of the MARIE dataset (n ≈670). Outcomes of interest included hysterectomy, traditional remedy use, and HRT use, each treated as binary variables. Fixed effects comprised age (z-scored), ethnicity (Sinhalese reference category), menopausal stage (Perimenopause reference), and presence of any long-term condition. To account for contextual heterogeneity, we fitted logistic generalised linear mixed models (GLMMs) with a random intercept for city of residence, using a Bayesian variational approximation to estimate posterior means and standard deviations. Odds ratios (OR) with 95% credible intervals (CrI) were calculated. The intraclass correlation coefficient (ICC) on the logistic scale was derived from the random effect variance to quantify clustering by city.
An exploratory burden score was developed to capture cumulative disadvantage across three domains:
Clinical burden (0–3 points): presence of long-term conditions, premature ovarian insufficiency, or surgical menopause.
Treatment burden (0–3 points): ≥2 concurrent medications, reported barrier or contraindication to HRT use, or use of GnRH analogues.
Socio-cultural burden (0–2 points): reliance on traditional remedies or residence outside Colombo.
The composite score ranged from 0 to 8. Burden score distributions were summarised overall and by menopausal stage. Analyses were performed in Python (pandas) (Supplementary Table).
Results
A total of 720 women were included in this study (Supplementary S1). The sample was classified into one of four menopausal stages (
Table 1): 137 (19·0%) were pre-menopausal, 69 (9·6%) perimenopausal, 49 (6·8%) reported being in “menopause”, and 465 (64·6%) were post-menopausal. Age was reported by 673 women (93·5%), with a mean of 54·1 (SD±13.0) years and median 56 years ([IQR] 49–62).
The sample was predominantly Sinhalese (n=626, 92%), with smaller numbers of Tamil (n=43, 6.3%) and other ethnic groups. Most participants were Buddhist (n=635, 88.2%), followed by Hindu (n=39, 5.4%) and Catholic (n=35, 4.9%). The majority were married (n=530, 73.6%), living mainly in nuclear families (n=583, 81%), with an average of 2.5 (SD ± 1.3) children among those with offspring (n=569).
Educational attainment showed 42.5% (n=306) with A-level or higher, 23.6% (n=170) with secondary education, 16.4% (n=118) with undergraduate, 4.7% (n=34) with postgraduate, and 12.8% (n=92) with no formal education. Employment patterns indicated 30.7% (n=221) employed full-time, 17.1% (n=123) homemakers, 10.7% (n=77) retired, and 29.7% (n=214) unemployed. Most participants resided in semi-urban (n=332, 51.7%) or urban (n=193, 30%) areas, while 18.2% (n=117) were from rural settings.
A total of 28.6% (n=206) reported at least one comorbidity, most commonly hypertension (n=83, 40.3%), diabetes (n=72, 34.9%), and dyslipidaemia (n=58, 28.1%). Among those on medication (n=527, 73.2%), the most frequently used were metformin (n=87, 16.5%), losartan (n=86, 16.3%), and atorvastatin (n=75, 14.2%), with a small proportion (n=7, 1.3%) using Ayurveda remedies.
Geographically, the largest clusters were from Colombo (n=73), Galle (n=68), Gampaha (n=67), and Kandy (n=52), with additional participants from Jaffna, Matara, Kalutara, Ampara, Puttalam, and several rural towns, ensuring coverage across the Western, Southern, Central, Northern, and Eastern provinces.
Menopause
Information on menopause type was available for 671 women (93·2%). The majority reported natural menopause (n=602; 83·5%), while 53 (7·4%) reported surgical menopause and 16 (2·2%) medical menopause. Among those reporting an age at menopause (n=528; 73·3%), the mean age was 49·7 years (SD ±4.1), with a median of 50 years (IQR 48–52).
A trend analysis (
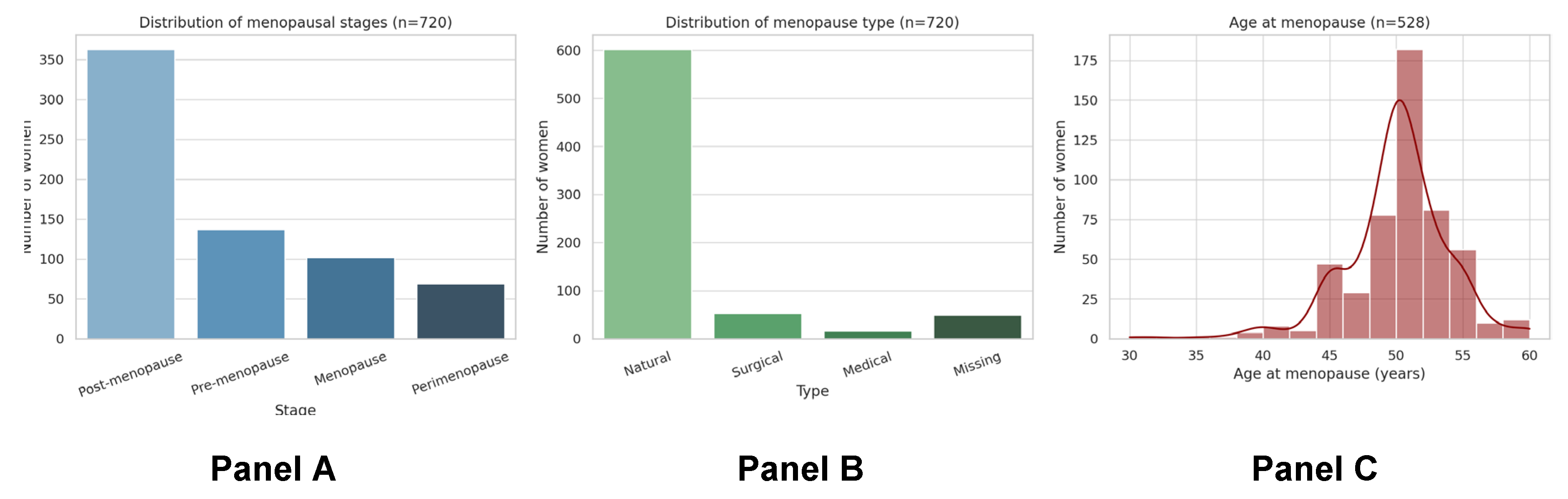
Figure 1) indicated that the distribution of menopausal stages (
Figure 1, Panel A) showed that nearly two-thirds of women were post-menopausal, while smaller but important groups were classified as pre-menopausal, perimenopausal, or in menopause. Natural menopause was the predominant pathway (
Figure 1, Panel B), though approximately one in ten women reported surgical or medical menopause, highlighting a clinically distinct subgroup requiring targeted support. The age at menopause clustered tightly around 50 years (
Figure 1, Panel C), with most women transitioning between the ages 47 and 52, consistent with regional estimates. Taken together, these trends demonstrate that although menopause is largely a natural process, induced menopause and variability in timing contribute substantially to women’s health trajectories in Sri Lanka.
Panel A shows the distribution of menopausal stages across the study population, with most women being post-menopausal, and smaller proportions classified as pre-menopausal, perimenopausal, or in menopause. Panel B illustrates the distribution of menopause type. Natural menopause predominated, while a notable minority of women experienced surgical menopause and a smaller proportion medical menopause; a small fraction did not report type. Panel C presents the distribution of self-reported age at menopause (restricted to 20–65 years; n=528), demonstrating a mean of 49·9 years, with clustering around 50 years, consistent with regional patterns.
Together, the panels highlight that while natural menopause is the dominant pathway, induced menopause represents a significant subgroup, and that considerable variation exists in the timing of menopause across the population.
Table 2.
Menopause type among all participants (n=720).
Table 2.
Menopause type among all participants (n=720).
| Menopause type |
n |
% (95% CI) |
| Natural |
602 |
83·5 (80·7–86·0) |
| Surgical |
53 |
7·4 (5·7–9·6) |
| Medical |
16 |
2·2 (1·4–3·7) |
| Missing/not reported |
49 |
6·8 (—) |
Inequalities in Menopausal Status and Type
Marked geographical and ethnic disparities were evident. By city, the proportion of post-menopausal women ranged from 33·3% to 100·0%, while the prevalence of pre-menopause varied between 0·0% and 66·7%. Smaller but notable variation was observed for perimenopause (0·0–33·3%) and “menopause” (0·0–33·3%). By ethnicity, the prevalence of post-menopause ranged from 60·0% to 93·1%, pre-menopause from 6·9% to 33·3%, perimenopause from 0·0% to 13·8%, and menopause from 0·0% to 20·7%. When stratified by menopause type, the distribution also varied. Across 21 cities with ≥5 respondents, natural menopause ranged from 57·9% to 100·0%, surgical menopause 3·9% to 40·0%, and medical menopause 1·4% to 15·8%. By ethnicity, natural menopause ranged from 60·0% to 93·1%, surgical menopause 6·9% to 40·0%, while medical menopause was observed in one group (1·6%).
Table 3.
Inequalities in menopausal status and type (groups with ≥5 respondents).
Table 3.
Inequalities in menopausal status and type (groups with ≥5 respondents).
| Panel |
Category |
Range min (%) |
Range max (%) |
Number of groups |
| Status by city |
Pre-menopause |
0·0 |
66·7 |
21 |
| Status by city |
Perimenopause |
0·0 |
33·3 |
21 |
| Status by city |
Menopause |
0·0 |
33·3 |
21 |
| Status by city |
Post-menopause |
33·3 |
100·0 |
21 |
| Status by ethnicity |
Pre-menopause |
6·9 |
33·3 |
3 |
| Status by ethnicity |
Perimenopause |
0·0 |
13·8 |
3 |
| Status by ethnicity |
Menopause |
0·0 |
20·7 |
3 |
| Status by ethnicity |
Post-menopause |
60·0 |
93·1 |
3 |
| Type by city |
Natural |
57·9 |
100·0 |
21 |
| Type by city |
Surgical |
3·9 |
40·0 |
14 |
| Type by city |
Medical |
1·4 |
15·8 |
3 |
| Type by ethnicity |
Natural |
60·0 |
93·1 |
3 |
| Type by ethnicity |
Surgical |
6·9 |
40·0 |
3 |
| Type by ethnicity |
Medical |
1·6 |
1·6 |
1 |
The prevalence of hysterectomy was 9.4%. In contrast, the use of traditional remedies was 6.9%, and HRT was 3.4%. The traditional remedies included herbal plants, herbal oils, yoga, regular massage therapies, deep breathing exercises, rituals in religion and Ayurveda medicine. In the hysterectomy model, menopausal stage was a strong predictor: women in menopause (OR 3.83, 95% CrI 2.17–6.77) and post-menopause (OR 3.00, 2.16–4.16) had higher odds than perimenopausal women. The ICC was 0.13, indicating a modest clustering of city. In the traditional remedy model, Tamil women had greater odds of use compared to Sinhalese (OR 4.02, 1.68–9.61), while post-menopausal women were less likely to use remedies than perimenopausal women (OR 0.49, 0.31–0.78). The ICC was 0.42, reflecting substantial between-city variation. In the HRT model, women with long-term conditions had over twice the odds of HRT use (OR 2.25, 1.17–4.32), while those in menopause (OR 0.20, 0.07–0.59) or post-menopause (OR 0.14, 0.07–0.28) had lower odds relative to perimenopause. The ICC was 0.37, suggesting marked clustering by setting.
Exploratory Burden Score
The composite burden score (range 0–8) quantified cumulative disadvantage across clinical, treatment, and sociocultural domains. The overall mean burden score was 1·1 (SD 0·7), with a median of 1 (range 0–4). Burden scores were broadly similar across stages: 1·05 in pre-menopausal, 1·10 in perimenopausal, 1·12 in menopause, and 1·11 in post-menopausal women.
Table 1.
Characteristics of the study population.
Table 1.
Characteristics of the study population.
| Characteristic |
n |
Summary |
| *Age (years) |
673 |
Mean: 54·1±13.0; median: 56 (IQR 49–62) |
| Menopausal status |
720 |
100% |
| Pre-menopausal |
137 |
19·0% |
| Perimenopausal |
69 |
9·6% |
| Menopause |
49 |
6·8% |
| Post-menopausal |
465 |
64·6% |
| *Age at menopause (years)† |
546 |
Mean: 49·7±4.1; median 50 (48–52) |
| *Age at menarche (years)† |
712 |
Mean: 13.2±1.6; median: 13 (12-14) |
| Race |
680 |
94.4% |
| Sinhala |
626 |
92% |
| Tamil |
43 |
6.3% |
| Muslim |
6 |
0.8% |
| Burger |
1 |
0.1% |
| Other |
4 |
0.5% |
| Missing values |
40 |
5.6% |
| Religion |
720 |
100% |
| Buddhism |
635 |
88.2% |
| Hindu |
39 |
5.4% |
| Catholic |
35 |
4.9% |
| Islam |
6 |
0.8% |
| Christian |
4 |
0.5% |
| Other |
1 |
0.1% |
| Marital Status |
720 |
100% |
| Married |
530 |
73.6% |
| Single |
103 |
14.3% |
| Widowed |
73 |
10.1% |
| Divorced |
10 |
1.4% |
| Live-in |
3 |
0.4% |
| Other |
1 |
0.1% |
| Family Status |
720 |
100% |
| Nuclear |
583 |
81% |
| Single parenting |
25 |
34.7% |
| Other (Extended or living with other family) |
112 |
15.5% |
| *Number of Children |
569 |
Mean: 2.5±1.3 |
| Education level |
720 |
100% |
| A-level, higher grade or equivalent |
306 |
42.5% |
| O-level, higher grade or equivalent |
170 |
23.6% |
| Undergraduate (e.g., BA or BSc) or equivalent |
118 |
16.4% |
| Postgraduate (e.g., MA or PhD) or equivalent |
34 |
4.7% |
| No formal educational qualifications |
92 |
12.8% |
| Employment status |
720 |
100% |
| Employed full-time |
221 |
30.7% |
| Employed part-time |
34 |
4.7% |
| Employed casually |
35 |
4.9% |
| Retired |
77 |
10.7% |
| Home maker |
123 |
17.1% |
| Cared for a family member |
16 |
2.2% |
| Unemployed |
214 |
29.7% |
| Setting |
642 |
89.2% |
| Urban |
193 |
30% |
| Semi-urban |
332 |
51.7% |
| Remote |
117 |
18.2% |
| Missing values |
78 |
10.8% |
| *Comorbidities |
206 |
28.6% |
| Hypertension |
83 |
40.3% |
| Diabetes |
72 |
34.9% |
| Dyslipidaemia |
58 |
28.1% |
| Endometriosis |
33 |
16% |
| Arthritis |
24 |
11.6% |
| Back pain |
8 |
11.6 |
| Hypothyroidism |
8 |
3.9% |
| Cancer |
2 |
1% |
| Vision problems |
2 |
1% |
| Hyperthyroidism |
1 |
0.5% |
Table 4.
Exploratory burden score (0–8) by menopausal stages.
Table 4.
Exploratory burden score (0–8) by menopausal stages.
| Group |
n |
Mean |
SD |
Median |
Min |
Max |
| Overall |
720 |
1·10 |
0·68 |
1 |
0 |
4 |
| Pre-menopausal |
137 |
1·05 |
0·66 |
1 |
0 |
3 |
| Perimenopausal |
69 |
1·10 |
0·61 |
1 |
0 |
3 |
| Menopause |
49 |
1·12 |
0·64 |
1 |
0 |
3 |
| Post-menopausal |
465 |
1·11 |
0·70 |
1 |
0 |
4 |
Discussion
This study provides the most comprehensive epidemiological characterisation to date of menopausal transitions among Sri Lankan women. The majority of women were post-menopausal (64·6%), with natural menopause being the dominant pathway (83.5%). Induced menopause was reported by approximately one in ten women, either surgically (7.4%) or as a result of health conditions such as chemotherapy or radiotherapy (2.2%). Among those reporting an age at menopause (n=560), the mean was 49.7 years (SD 4.19), with a median of 50 years and clustering between 48–52 years (range 28–63). Premature menopause (<40 years) was uncommon, affecting only 2.0% of women (n=11), and early menopause (<45 years) occurred in 6.4% (n=36). These findings demonstrate that menopause in Sri Lanka largely follows global and regional patterns, with the majority of women experiencing natural menopause around the age of 50. However, the presence of a clinically significant subgroup experiencing induced menopause highlights the need for targeted support and follow-up, particularly given the abrupt symptom burden and long-term health risks associated with surgically or medically induced ovarian insufficiency.
Marked geographical and ethnic disparities were observed in both menopausal stage and type, suggesting that access to services, surgical practices, and sociocultural influences play a role in shaping women’s menopausal experiences. These disparities indicate that menopause is not solely a biological event but a transition influenced by health system structures, socioeconomic status, and cultural factors. Taken together, these findings emphasise the necessity of contextualised health system responses that address both the biological and structural determinants of women’s health in midlife.
Population Science
From a population health perspective, these data confirm that most Sri Lankan women will spend approximately one-third of their lives in the post-menopausal state. This has profound implications for chronic disease prevention, healthy ageing, and long-term health planning. The observed heterogeneity across urban, semi-urban, and rural areas, as well as between ethnic groups, underscores the role of geography and social determinants in shaping health outcomes.
To address these inequalities, menopause must be integrated into routine surveillance systems and existing well-woman programmes. Midlife health reviews at ages 35 and 45 offer an important opportunity to identify risks early and provide counselling on symptom management, lifestyle interventions, and preventive care. Additionally, public health initiatives should normalise menopause as a life stage requiring proactive support, thus reducing stigma and improving health-seeking behaviours. Targeted outreach to underserved populations will be essential to closing gaps in access to care and ensuring that menopause-related services are equitably distributed.
Regional Differences and Environmental Factors
Sri Lanka’s tropical climate and environmental variability shape women’s menopausal experiences in multiple ways. In hot and humid lowland and coastal regions, high ambient temperatures intensify vasomotor symptoms such as hot flushes and night sweats, often disrupting sleep and daily activities. Conversely, cooler conditions in the central highlands may moderate such symptoms but bring challenges of joint stiffness and bone health in older women, particularly where access to vitamin D is reduced due to frequent cloud cover and limited sun exposure. Monsoonal patterns also influence food security and nutritional status, key determinants of symptom severity. Seasonal flooding or prolonged droughts in the dry zones (north and east) can exacerbate dietary deficiencies in calcium, iron, and protein, aggravating osteoporosis risk and fatigue among post-menopausal women. Environmental stressors such as water scarcity or displacement during extreme weather events may further restrict access to healthcare, compounding inequalities [
11,
12].
Cultural practices linked to the environment such as reliance on herbal remedies in rural areas where biomedical facilities are sparse, can affect women’s management choices. Women in agricultural communities face high physical workloads under harsh climatic conditions, which may worsen musculoskeletal pain, urinary incontinence, and fatigue during menopause. Together, these climate environment interactions highlight the importance of locally adapted health interventions that address both physiological and environmental determinants of menopausal health in Sri Lanka.
The InterLACE pooled analysis by Mishra et al. (2017) demonstrated that early menarche (≤11 years) and nulliparity substantially increase the risk of premature and early menopause, with the joint exposure conferring more than a fivefold risk of menopause before 40 [
13]. Compared with this, findings from MARIE Sri Lanka indicate a strikingly different landscape: almost 39% of Sri Lankan women reported menarche at ≤11 years and nearly 45% experienced premature menopause, far exceeding the proportions observed in Western and East Asian cohorts [
2]. Early menopause was rare, suggesting that once menopause occurred, it tended to cluster before 40 rather than between 40–44 years. These patterns highlight a unique reproductive trajectory in Sri Lanka, where earlier biological ageing may be amplified by nutritional transitions, psychosocial stressors, and evolving fertility behaviours. The implications are profound: without structured surveillance or specialised menopause care pathways, Sri Lankan women may face disproportionately high risks of cardiovascular disease, osteoporosis, and mental health decline linked to premature ovarian ageing. For the Sri Lankan diaspora, particularly those living in high-income countries, the biological predisposition to early menarche and premature menopause may persist despite access to more advanced health systems, underscoring the need for culturally sensitive clinical screening and preventive strategies across both local and global Sri Lankan communities.
Comorbidity–Menopause Interaction
Within this group, the prevalence of comorbidities was notably higher across almost every domain. Cardiovascular diseases and endocrine/metabolic disorders (notably diabetes) also clustered more strongly among women with premature menopause, suggesting an accelerated trajectory of non-communicable disease (NCD) risk. Musculoskeletal conditions, including back pain, fractures, and arthritis, were the most frequently reported, reflecting the combined effects of early oestrogen loss and lifelong physical labour. Sensory impairments, particularly vision problems, were also reported, aligning with Sri Lanka’s ageing-related cataract burden and potentially exacerbated by premature hormonal decline. The data suggest that premature menopause and comorbidities act synergistically, compounding health risks and compressing the window of healthy midlife for women.
Contextualisation
These findings underscore how premature reproductive ageing amplifies Sri Lanka’s existing NCD burden. Unlike in high-income InterLACE countries, where comorbidity patterns emerge later, Sri Lankan women are facing cardiovascular, musculoskeletal, and metabolic risks in their 30s and 40s, decades earlier than expected. This has profound implications for workforce participation, caregiving roles, and health system planning, as many women enter post-menopause during peak economic productivity years. For the Sri Lankan diaspora, while healthcare access may be broader, the biological predisposition to early menopause and high comorbidity risk remains. Without targeted awareness, these women may continue to be under-diagnosed or mismanaged in host countries where guidelines assume later menopausal onset.
The comorbidity and drug profiles highlight a health system blind spot: Sri Lankan women are navigating premature menopause with limited therapeutic support, placing them at disproportionate risk of long-term disability and mortality. Integrated, gender-sensitive NCD strategies and expanded menopause-specific services are urgently required.
Clinical Implications
Clinically, these findings highlight a critical need to embed menopause care within primary care pathways. Routine consultations should include screening for osteoporosis, cardiovascular risk, and other non-communicable diseases common at midlife, alongside assessment of symptom burden. Women experiencing induced menopause should receive tailored counselling and follow-up that includes information on hormonal and non-hormonal management options, delivered in a manner sensitive to individual risk factors such as cancer history or surgical indications.
Training healthcare providers to recognise and manage menopausal symptoms is vital to improving care quality. Given the low uptake of HRT observed in this study, professional education should also focus on dispelling misconceptions and ensuring that evidence-based treatments are accessible and appropriately prescribed. Strengthening referral systems between tertiary surgical or oncology services and community-based care will ensure continuity and reduce the risk of women being lost to follow-up after induced menopause.
Comorbidity Impact Profile & Contextualisation
The MARIE Sri Lanka cohort reveals a diverse spectrum of comorbidities, with musculoskeletal conditions (back/neck problems, fractures, arthritis) and sensory issues (notably eye/vision problems) reported most frequently. Cardiovascular risks, including hypertension and heart disease, are also prominent, consistent with Sri Lanka’s rising NCD burden. Endocrine and metabolic conditions such as diabetes feature heavily, reflecting the well-documented epidemiological shift in South Asia towards metabolic syndrome at younger ages. Mental health conditions appear less frequently reported, but this may reflect under-recognition and stigma rather than true absence.
The impact of these comorbidities is magnified in the context of very early menopause observed in this cohort (with almost 60% reporting menopause <40). Premature loss of oestrogen exacerbates cardiovascular, metabolic, skeletal, and cognitive risks, creating a compounding effect where comorbidities and reproductive ageing accelerate each other. The clustering of chronic disease in midlife women thus signals an urgent need for integrated, gender-sensitive NCD strategies.
For the Sri Lankan diaspora, while healthcare access may improve in high-income countries, the underlying biological predisposition to early menopause and high comorbidity burden persists. Without culturally adapted screening and prevention, these women may continue to face disproportionate health risks, even in well-resourced settings. This highlights the importance of both local systems strengthening in Sri Lanka and diaspora-specific awareness in host countries.
From a public health and clinical perspective, these findings highlight the need to strengthen menopausal health services in Sri Lanka, as indicated in
Table 5.
Conclusions
This study provides a comprehensive, data-driven characterisation of menopausal transitions in Sri Lanka. Natural menopause was the dominant pathway, occurring around a mean age of 49.7 years, with premature menopause uncommon (2.0%) and early menopause relatively rare (6.4%). However, approximately one in ten women experienced induced menopause, underscoring the need for targeted clinical pathways and support.
Significant geographic and ethnic disparities highlight persistent health inequalities and the influence of social determinants on menopausal experiences. Strengthening Sri Lanka’s response to midlife women’s health will require integrating menopause education and screening into existing well-woman programmes, improving equity in access to care, and embedding prevention and symptom management into primary care systems. Recognising menopause as both a biological transition and a public health priority is essential to promoting healthy ageing, enhancing quality of life, and reducing long-term morbidity for women across the country.
Supplementary Materials
The following supporting information can be downloaded at website of this paper posted on Preprints.org.
Author Contributions
GD developed the ELEMI program and conceptualised this paper. TM and VP collected data. TM and VP wrote the first draft and furthered by all other authors. All authors critically appraised, reviewed and commented on all versions of the manuscript. All authors read and approved the final manuscript.
Institutional Review Board Statement
Ethical Review Committee, Faculty of Allied Health Sciences, University of Ruhuna, Sri Lanka (Ref. No: 2025.02.532).
Informed Consent Statement
Obtained.
Data Availability Statement
The principal investigator and the study sponsor may consider sharing anonymous data upon reasonable a request.
Acknowledgements
MARIE Consortium: Om Kurmi, Ganesh Dangal, Aini Hanan binti Azmi, Alyani binti Mohamad Mohsin, Arinze Anthony Onwuegbuna, Artini binti Abidin, Ayyuba Rabiu, Chijioke Chimbo, Chinedu Onwuka Ndukwe, Choon-Moy Ho, Chinyere Ukamaka Onubogu, Diana Chin-Lau Suk, Divinefavour Echezona Malachy, Emmanuel Chukwubuikem Egwuatu, Eunice Yien-Mei Sim, Farhawa binti Zamri, Fatin Imtithal binti Adnan, Geok-Sim Lim, Halima Bashir Muhammad, Ifeoma Bessie Enweani-Nwokelo, Ikechukwu Innocent Mbachu, Jinn-Yinn Phang, John Yen-Sing Lee, Joseph Ifeanyichukwu Ikechebelu, Juhaida binti Jaafar, Karen Christelle, Kathryn Elliot, Kim-Yen Lee, Kingsley Chidiebere Nwaogu, Lee-Leong Wong, Lydia Ijeoma Eleje, Min-Huang Ngu, Noorhazliza binti Abdul Patah, Nor Fareshah binti Mohd Nasir, Kathleen Riach, Norhazura binti Hamdan, Nnanyelugo Chima Ezeora, Nnaedozie Paul Obiegbu, Nurfauzani binti Ibrahim, Nurul Amalina Jaafar, Odigonma Zinobia Ikpeze, Obinna Kenneth Nnabuchi, Pooja Lama, Puong-Rui Lau, Rakshya Parajuli, Rakesh Swarnakar, Raphael Ugochukwu Chikezie, Rosdina Abd Kahar, Safilah Binti Dahian, Sapana Amatya, Sing-Yew Ting, Siti Nurul Aiman, Sunday Onyemaechi Oriji, Susan Chen-Ling Lo, Sylvester Onuegbunam Nweze, Nimesha Wijayamuni, Prasanna Herath, Thamudi Sundarapperuma, Vaitheswariy Rao, Xin-Sheng Wong, Xiu-Sing Wong, Yee-Theng Lau, Heitor Cavalini, Jean Pierre Gafaranga, Emmanuel Habimana, Chigozie Geoffrey Okafor, Assumpta Chiemeka Osunkwo, Gabriel Chidera Edeh, Esther Ogechi John, Kenechukwu Ezekwesili Obi, Oludolamu Oluyemesi Adedayo, Odili Aloysius Okoye, Chukwuemeka Chukwubuikem Okoro, Ugoy Sonia Ogbonna, Chinelo Onuegbuna Okoye, Babatunde Rufus Kumuyi, Onyebuchi Lynda Ngozi, Nnenna Josephine Egbonnaji, Oluwasegun Ajala Akanni, Perpetua Kelechi Enyinna, Yusuf Alfa, Theresa Nneoma Otis, Catherine Larko Narh Menka, Kwasi Eba Polley, Isaac Lartey Narh, Bernard B. Borteih, Andy Fairclough, Kingsley Emeka Ekwuazi, Michael Nnaa Otis, Jeremy Van Vlymen, Chidiebere Agbo, Francis Chibuike Anigwe, Kingsley Chukwuebuka Agu, Chiamaka Perpetua Chidozie, Chidimma Judith Anyaeche, Clementine Kanazayire, Jean Damascene Hanyurwimfura, Nwankwo Helen Chinwe, Stella Matutina Isingizwe, Jean Marie Vianney Kabutare, Dorcas Uwimpuhwe, Melanie Maombi, Ange Kantarama, Uchechukwu Kevin Nwanna, Benedict Erhite Amalimeh, Theodomir Sebazungu, Elius Tuyisenge, Yvonne Delphine Nsaba Uwera, Emmanuel Habimana, Nasiru Sani and Amarachi Pearl Nkemdirim, Rukshini Puvanendram, Manisha Mathur, Rajeswari Kathirvel, Farah Safdar, Raksha Aiyappan, Jean Pierre Gafaranga, Bertin Ngororano, Victor Archibon, Ibe Michael Usman, Baraka Godfrey Mwahi, Filbert Francis Ilaza, Zepherine Pembe, Clement Mwabenga, Mpoki Kaminyoghe, Brenda Mdoligo, Thomas Alone Saida, Nicodemus E. Mwampashi, Olisaemeka Nnaedozie Okonkwo, Bethel Chinonso Okemeziem, Bethel Nnaemeka Uwakwe, Goodnews Ozioma Igboabuchi, Ifeoma Francisca Ndubuisi
Consent for Publication
ll authors consented to publish this manuscript.
Conflicts of Interest
All authors report no conflict of interest. The views expressed are those of the authors and not necessarily those of the NHS, the National Institute for Health Research, the Department of Health and Social Care or the Academic institutions.
References
- Delanerolle, G.; Phiri, P.; Elneil, S.; Talaulikar, V.; Eleje, G.U.; Kareem, R.; Shetty, A.; Saraswath, L.; Kurmi, O.; Benetti-Pinto, C.L. Menopause: a global health and wellbeing issue that needs urgent attention. The Lancet Global Health 2025, 13, e196–e198. [Google Scholar] [CrossRef] [PubMed]
- Rathnayake, N.; Lenora, J.; Alwis, G.; Lekamwasam, S. Prevalence and severity of menopausal symptoms and the quality of life in middle—aged women: A study from Sri Lanka. Nursing research and practice 2019, 2019, 2081507. [Google Scholar] [CrossRef] [PubMed]
- Ilankoon, I.; Samarasinghe, K.; Elgán, C. Menopause is a natural stage of aging: a qualitative study. BMC women’s health 2021, 21, 47. [Google Scholar] [CrossRef] [PubMed]
- Rao, D.B. Status and Advancement of women; APH Publishing: 2000.
- Hamoda, H.; Sharma, A. Premature ovarian insufficiency, early menopause, and induced menopause. Best practice & research Clinical endocrinology & metabolism 2024, 38, 101823. [Google Scholar]
- Nelson, L.M.; Covington, S.N.; Rebar, R.W. An update: spontaneous premature ovarian failure is not an early menopause. Fertility and sterility 2005, 83, 1327–1332. [Google Scholar] [CrossRef] [PubMed]
- Pillay, O.C.; Manyonda, I. The surgical menopause. Best practice & research clinical obstetrics & gynaecology 2022, 81, 111–118. [Google Scholar]
- Sochocka, M.; Karska, J.; Pszczołowska, M.; Ochnik, M.; Fułek, M.; Fułek, K.; Kurpas, D.; Chojdak-Łukasiewicz, J.; Rosner-Tenerowicz, A.; Leszek, J. Cognitive decline in early and premature menopause. International journal of molecular sciences 2023, 24, 6566. [Google Scholar] [CrossRef]
- Samuel, R.L. From Menarche to Menopause: A Systematic Review of Black and Asian Minority Ethnic (BAME) Women’s Reproductive Health Challenges in the UK. University of Wales Trinity Saint David (United Kingdom), 2024.
- Angaye, U.S.; Sibiri, E.A. Between stigma and support: how socio-cultural norms shape health decisions among perimenopausal women in bayelsa central, Nigeria. African journal for the psychological studies of social issues 2025, 28. [Google Scholar]
- Stevens, B.; Watt, K.; Brimbecombe, J.; Clough, A.; Judd, J.; Lindsay, D. The role of seasonality on the diet and household food security of pregnant women living in rural Bangladesh: a cross-sectional study. Public health nutrition 2017, 20, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Hunter, M.; Gupta, P.; Chedraui, P.; Blümel, J.; Tserotas, K.; Aguirre, W.; Palacios, S.; Sturdee, D. The international menopause study of climate, altitude, temperature (IMS-CAT) and vasomotor symptoms. Climacteric 2012, 16, 8–16. [Google Scholar] [CrossRef]
- Mishra, G.D.; Pandeya, N.; Dobson, A.J.; Chung, H.-F.; Anderson, D.; Kuh, D.; Sandin, S.; Giles, G.G.; Bruinsma, F.; Hayashi, K. Early menarche, nulliparity and the risk for premature and early natural menopause. Human Reproduction 2017, 32, 679–686. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Distribution of menopausal stage, type, and age at menopause among Sri Lankan women (n=720).
Figure 1.
Distribution of menopausal stage, type, and age at menopause among Sri Lankan women (n=720).
Table 5.
Public health and clinical recommendations for improving menopausal health services in Sri Lanka.
Table 5.
Public health and clinical recommendations for improving menopausal health services in Sri Lanka.
| Domain |
Recommendation |
Public health perspective |
Clinical perspective |
| Awareness and education |
Normalise menopause as a health issue, not just a life stage |
Community-based programmes to educate women, families, and communities; leverage well-woman clinics at ages 35 and 45 for counselling |
Routine primary care consultations to validate symptoms, provide anticipatory guidance, and promote healthy ageing |
| Support for induced menopause |
Dedicated follow-up for women with surgical or medical menopause |
Integrate counselling into surgical pathways; ensure continuity between tertiary care and community follow-up |
Offer counselling on HRT, non-hormonal options, and lifestyle advice to reduce immediate symptoms and long-term risks |
| Screening and preventive care |
Proactive assessment at midlife |
Implement population-level screening campaigns for osteoporosis, cardiovascular risk, and cancers; reduce stigma to improve clinic attendance |
Embed midlife screening in primary care, gynaecology, and oncology; link findings to tailored preventive interventions |
| Research and policy |
Strengthen evidence base and allocate resources |
Conduct epidemiological studies across rural and urban areas; assess socioeconomic inequalities |
Train healthcare providers in menopausal medicine; ensure consistent supply of MHT and alternatives; embed menopause care in national health strategies |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).