
Submitted:
19 January 2026
Posted:
20 January 2026
Read the latest preprint version here
Preprints on COVID-19 and SARS-CoV-2
Abstract
Long COVID is the consequence of having had COVID. Long COVID has many other names including Long-haul COVID, Post-COVID conditions (PCC), Post-COVID-19 syndrome, Post-acute sequelae of SARS-CoV-2 condition (PASC) and Chronic COVID. Long COVID is the name most frequently used. COVID is not alone in having severe post infection consequences. Influenza, Ebola, Marburg, Dengue, and Lyme Disease are other infections with severe post infection consequences. Long COVID has emerged over the past few years and is ill-defined. Long COVID’s underlying science and treatments are rapidly evolving. There is no diagnostic test for it. The most-often reported lower bound on its prevalence is about 7%. Seven percent doesn’t sound like much, but under the assumption that 75% of the people in the world have had COVID, that means 420 million people in the world have Long COVID which is about 5 times the number of people killed or injured in the 20th and 21st century wars. There are several root causes for Long COVID with inflammation and mitochondrial dysfunction being the two leading villains. Long COVID prevalence goes down with recent variants, COVID vaccination, early antiviral use, being fit, being young, and surprisingly being male. The most important action to reduce the chance of Long COVID is COVID vaccination. The impact of COVID vaccination on Long COVID prevalence is quite uncertain. Papers report 10% to 100% reduction in Long COVID rates from pre-disease vaccination. The average reported reduction is 50%. The impact of vaccination on people with no comorbidities is uncertain with wide ranges being reported. There are no guaranteed treatments for Long COVID; however, some treatments offer either broad or organ-specific relief for many. This paper reviews 179 different Long COVID treatments described in 249 papers. These papers came from the author’s personal data base called The Mouse That Roared of 24,000+ papers that have been accumulated over the last five and a half years. The Mouse That Roared papers cover all aspects COVID including the SARS-CoV-2 virus, the COVID disease, therapeutics, vaccines, behavior, testing, herd immunity, Long COVID, Long COVID Treatment, Politics and National COVID responses, etc. Unlike COVID, there are no excellent treatments, which I call silver bullets, for Long COVID Fortunately, there are some treatments that help some a bit. I will call those “bronze bb’s.” Even with them, healing is very slow. The recovery time with Long COVID is longer than the body’s normal times because COVID’s damage is widespread and because COVID damages our body’s healing process.
Keywords:
long COVID
; COVID
Setting the Stage
Before discussing Long COVID treatment, a review of Long COVID is appropriate.
Long COVID is very different than COVID as summarized in Table 1:
Long COVID is similar to the long-term impact from other viral, bacterial and parasite diseases, e.g., Long Ebola, Long Lyme, and influenza. Table 2 summarizes some of the aspects of various diseases’ post recovery conditions.
COVID and Long COVID comorbidities, other than sex, are very similar. Organ-specific comorbidities, e.g., diabetes and COPD, can increase the risk to organ damage. Sadly, just like COVID, socioeconomic and political context is a Long COVID comorbidity. A particularly surprising one, as reported by Nature[1] in July 2025, is viral rebound. It increases the odds of Long COVID by about 50% whether one has taken an antiviral or not. However, just as there are more COVID papers than Long COVID papers, PubMed lists more COVID comorbidity papers than Long COVID comorbidity papers as shown by Figure 1 which was prepared by the author. Interestingly PubMed listed a Long COVID paper in 2019 though it was not discovered until 2020!
Long COVID
Figure 2 from a National Academies of Sciences, Engineering, and Medicine[2] highlights Long COVID’s major symptoms. Over two hundred different symptoms have been reported in journal papers.
Symptoms tend to fade with time as described by the paper Persistence of Symptoms 15 Months since COVID-19 Diagnosis: Prevalence, Risk Factors and Residual Work Ability, Life, December 2022.[3] However, 1-2% of people with Long COVID in the US are disabled. Getting Social Security Disability benefits is difficult because of the lack of a diagnostic test. Cardiopulmonary testing, however, could give some insight into the degree of disability. Consequently, Social Security doesn’t and can’t report how many people with Long COVID are getting Social Security Disability benefits.
Figure 3 summarizes the slow course of recovery. While several papers[4,5,6,7,8] discussed recovery times, it is from reference 4. Notice the normal recover time of a few weeks to a few months for surgeries, bone breaks, etc. Notice the difference in recovery times for hospitalized and nonhospitalized patients which is another clue on the role of COVID severity in Long COVID. Long COVID recovery time is similar to inflammatory illness such as rheumatoid arthritis, lupus, Sjogren’s syndrome, Inflammatory Bowel Disease, etc. As will become clear, Long COVID is also related to inflammatory dysfunction.
Even after a mild COVD case, recovery can take a long time. A Clinical Infectious Disease paper[9] reported the recovery of smell or taste after mild COVID cases. Figure 4 summarizes the paper’s results.
SNOT-22 is a Sino-Nasal Outcome Test
One of the reasons the recovery time with Long COVID is longer than the body’s normal times is that Long COVID damages our body’s healing process.[10]
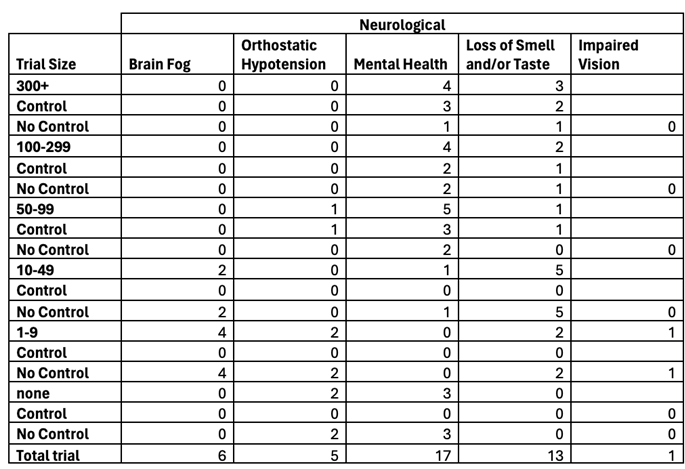
There were 502 papers in The Mouse that Roared that addressed specific Long COVID impacts. Figure 5, which was prepared by the author, is the distribution of those papers into various categories.
Not surprisingly, neurological and cardiovascular disruptions were at the top of the list as disruptions in these symptoms can lead to the two top Long COVID symptoms which are fatigue and brain fog.
Long COVID Prevalence
The following summary of CDC Pulse study[11] prepared by the author provides one view of Long COVID prevalence in the US.
The wide range of prevalence reported in The Mouse that Roared Long COVID papers is summarized in Figure 7, which was prepared by the author.
Figure 7.
Number of Papers Reporting Differing Long COVID Prevalence. This figure was prepared by the author. (The x-axis in the number of papers in each geographical region for each prevalence rate)
Figure 7.
Number of Papers Reporting Differing Long COVID Prevalence. This figure was prepared by the author. (The x-axis in the number of papers in each geographical region for each prevalence rate)
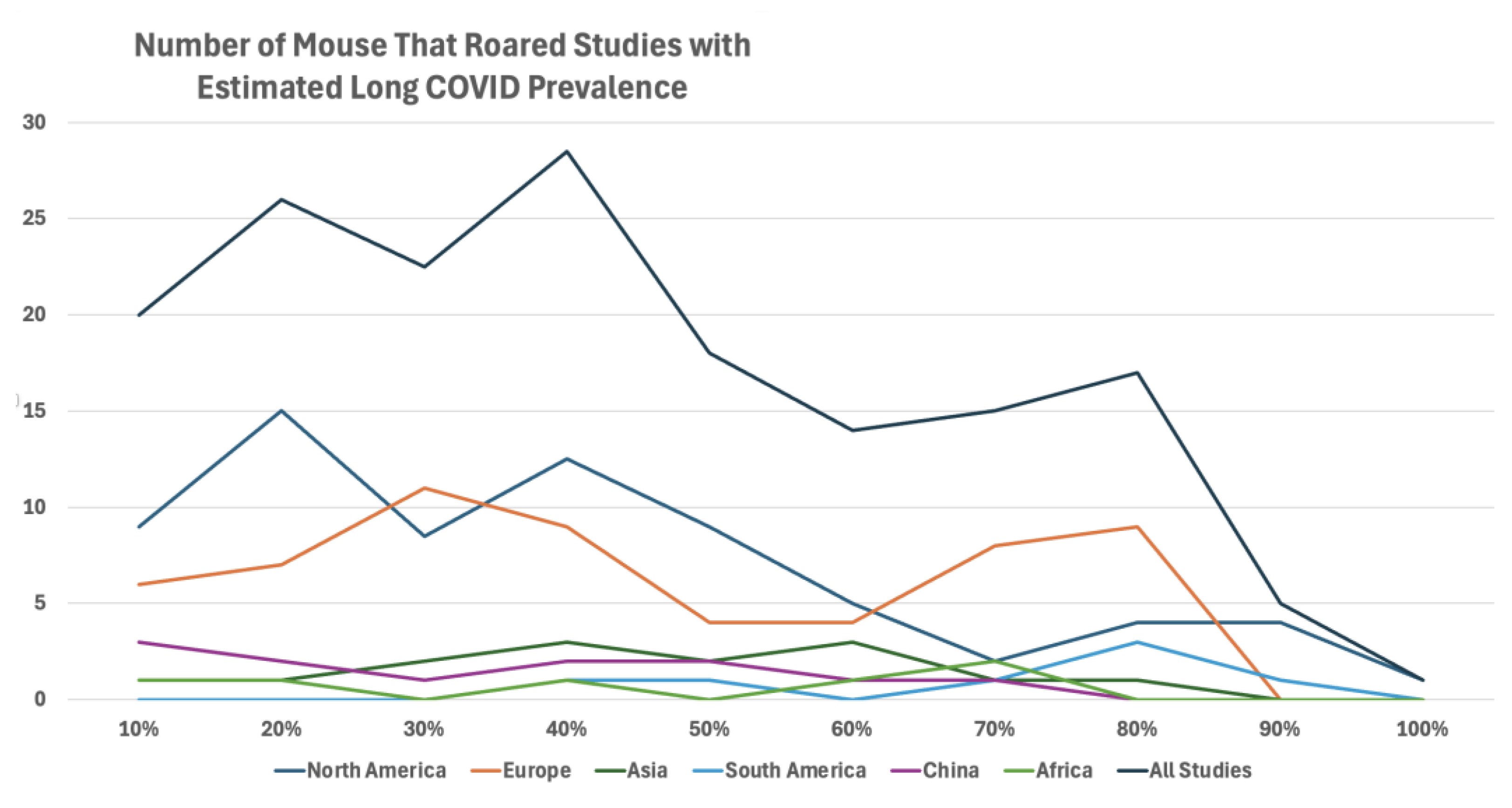
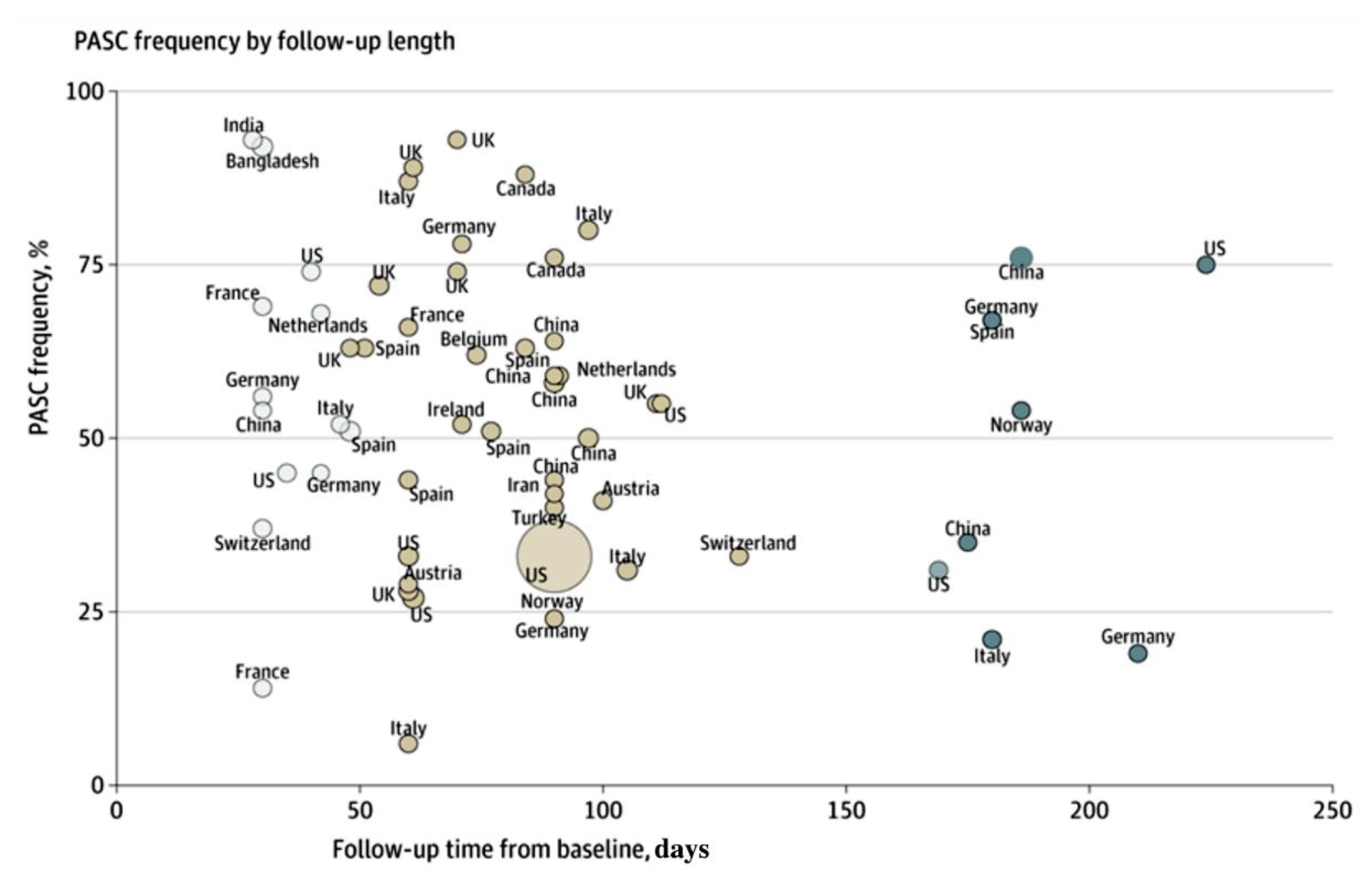
Figure 8.
Long COVID (PASC) Prevalence Versus Time[12]. Scatterplot representing each study’s PASC frequency (%) plotted according to length of follow-up from baseline (in days), represented by a circle proportional to the study’s sample size and annotated according to country.
Figure 8.
Long COVID (PASC) Prevalence Versus Time[12]. Scatterplot representing each study’s PASC frequency (%) plotted according to length of follow-up from baseline (in days), represented by a circle proportional to the study’s sample size and annotated according to country.
Prevalence by age isn’t as one might expect. A 2021 Office of National Statics[13] report included Figure 9.
In a similar vein, prevalence differs by variant and vaccination status as shown by 10 from a New England Journal of Medicine paper[14].
In Figure 10A, the numbers at the bottom are additional DALY’s as days post-infection increase.
There are many reasons for this high uncertainty in prevalence.
- 1. First, and most importantly, there is no diagnostic test for Long COVID. Thus, assessment techniques are qualitative. For example,
- i. There are self-assessments with different criteria, e.g., walk test or how are you feeling?
- ii. Frequently there are not controls who also could have Long COVID symptoms, e.g., fatigue or depression.
- iii. There are mail surveys, on-line forms, phone calls, all of which have low response rates. Someone who doesn’t feel well is more likely to respond than someone who feels great which bias results.
- iv. There are different measures such as rate, risk ratios, and fully recovered.
- v. While there is a large symptom base, only a few symptoms are usually measured, usually fatigue or brain fog.
- 2. The pandemic changed behaviors, e.g., less exercise and sleep, which can result in one having “Long COVID” symptoms.
- 3. Comorbidities affect the results. The comorbidities include:
- i. Pandemic medical impacts, e.g., depression which can overlap with and can exacerbate Long COVID symptoms.
- ii. Age, sex, BMI, diseases, frailty, genetics
- iii. Variants
- iv. Therapeutics
- v. COVID Vaccination
- 4. There are different Long COVID definitions.
Reinfection has an interesting impact on Long COVID prevalence. A May 2025, medRxiv preprint[15] reported that Estimated long COVID risk following any COVID-19 infection was similar among 22 496 online survey participants (17.0% [95%CI, 16.3%–17.6%] and 3 978 telephone survey participants (15.9% [14.6%–17.2%]. The cumulative risk increased with the number of infections, but reinfections were associated with three times lower risk of long COVID than first infections.
Of course, just like prevalence, there is great variation on reported reinfection risk. An October 2023, Open Forum Infectious Disease[16] paper reported Long COVID was reported by those ≥16 years at a rate of 4.0% of first and 2.4% of second infection, respectively. The corresponding estimates among those aged <16 years were 1.0% and 0.6%. The adjusted odds ratio for Long COVID after second compared to first infections was 0.72 for those ≥16 years and 0.93 for those <16 years. Thus, again, prevalence is complex.
Long COVID Root Causes
Long COVID has many root causes which are at the heart of Long COVID and the slow recovery from it. The major ones are:
- Inflammation: Inflammation is probably Long COVID’s major root cause. Inflammation includes recruiting white blood cells and the release of cytokines that initiate tissue swelling and injury.
- Persistent viral infection: viral antigens, RNA, and SARS-CoV-2 proteins remain present and active in the body’s tissues following acute infection and continue to damage it.
- Viral particle damage to organs. A COVID case results in 1-30 trillion viral particles in the body. Some proteins, particularly the spike, the nucleocapsid, and the nonstructural protein 1 (nsp1) directly damage organs.
- Autoantibodies: Infection with the SARS-CoV-2 virus can trigger autoimmune diseases.
-
Biological processes and organs are damaged.
- a. All our organs are damaged.
- b. Mitochondria, our energy workhorses, are greatly damaged by COVID. This results in fewer oxygen carrying molecules called ATP being generated for our bodies. This is a significant contributor to fatigue and brain fog.
- c. The proteins that are involved in healing are dysregulated.
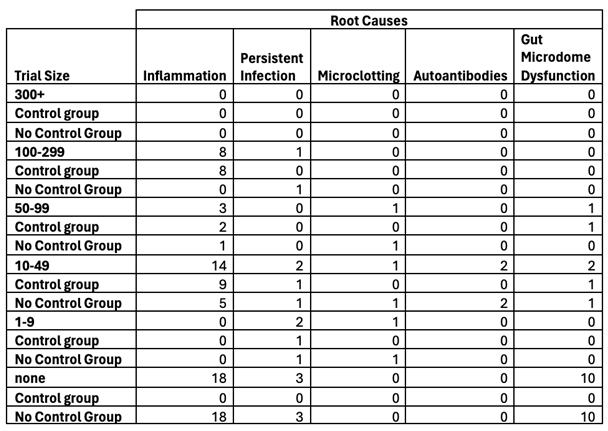
Figure 11, which was prepared by the author, summaries the number of The Mouse that Roared papers that addressed these root cause damages.
Thus, Long COVID is not a disease; rather, it is the multifaceted consequences of a disease.
Long COVID Biochemical Markers
Though there is no diagnostic test for Long COVID, there are many medical, biochemical and lifestyle markers that provide clues that Long COVID is present. They include but are not limited to biochemical markers for the following long list of symptoms, organs, and body characteristics. This long list is another indication of Long COVID’s broad impact to the body:
Pain
Blood System
Vascular System
Retinal Microcirculation
Musculoskeletal Changes
Orthostatic Dysfunction
Cardiac Changes
Olfactory Bulb Changes
Lung
Diaphragm Weakness
Gut Permeability
Proteins
Metabolites
Bacteria Change
Brain Changes
Bacteria
Autonomic Disfunction
Connectivity
Microglial And Macrophage Activation
Brain Entropy
Kinesiophobia
Reaction Time
Chemosensory Impairment
Neurotransmitters
Serotonin
Protein Markers
Plasma Changes
Changes In Gene Expression
Viral Proteins
Spike Protein
N Protein Anti-Nucleocapsid Igg
Antibodies, Autoantibodies
Antibody Levels
Nasal
Autoantibodies
Coronavirus Imprinting
Immune System
Immune System Dysregulation
Previous Coronavirus Infection
Metabolic Changes
T Cells dysregulation
Monocytes
Tryptophan & Kynurenine
Myeloid Cells
Mitochondria, Oxidative Stress
Genetics
Genes
Epigenetic Changes
Reducing the Chances of Long COVID
As previously noted, the chance of Long COVID increases with COVID severity. Thus, the most important action to reduce the chance of Long COVID is pre-disease COVID vaccination. The assessments of vaccine impact are further complicated by vaccine type, age, variant, whether the person is immunocompromised, etc. The following chart shows the number of COVID vaccination impact on Long COVID papers in The Mouse that Roared.
As illustrated by Figure 12, which was prepared by the author even something as simple as the impact of vaccination on Long COVID rates has a wide range of answers. The average is 50%, but studies reported as little as 10% and as much as 100%!
Long COVID Treatments
Vaccines and antivirals were COVID silver bullets. They dramatically reduce COVID prevalence and severity. Long COVID has scattered, specialized therapeutics. None are as effective as COVID vaccines or approved antivirals.
Table 3 summarizes number of Long COVID versus COVID studies in June 2025 provides some insight into the research base associated with each malady.
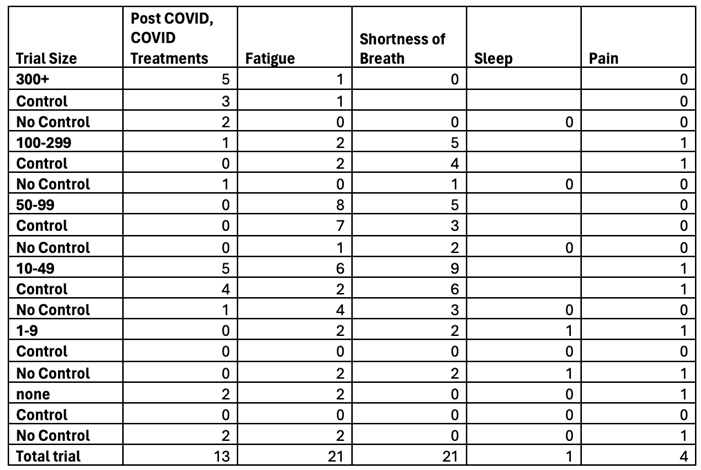
One can get further insight into the relative progress of Long COVID treatment by analyzing the FDA Long COVID clinical trials using the FDA Clinical Trial Tracker. As of June 2025, 176 of the 545 trials are in the US. While one trial can address multiple issues, Table 4 enumerates the symptoms addressed by the FDA trials:
As of June 2025, no Long COVID clinical trial had posted clinical results. However, it is important to note that many Long COVID symptoms such as blood clots have approved therapeutics.
Sadly, as shown in Table 5, the Long COVID FDA trial rate decreased in 2024 and 2025.
Nonetheless, there is good reason to hope that progress will be made on Long COVID treatment.
- The scientific community is early in focusing on Long COVID, so clearly other treatments will be discovered.
- The huge, order of $2.3 billion, US Long COVID project called Recover Project is just gathering momentum. This will be a long term, well-funded project if for no other reason than the order of 20 million Americans suffers from Long COVID. This website lists its published papers Recover Project Published Papers.
- Though not as large as the US Recover Project, many countries have large Long COVID projects including, but not limited to the UK, Canada, Australia, China, Japan, South Korea, the European Union, and the Word Health Organization.
- That is, the number of Long COVID treatment papers in The Mouse That Roared dropped precipitously in July and august 2025.
Treatment Strategy
This section will outline the approach one might wish to follow if one believes he/she has Long COVID.
- I.
- Get the Right Set of Doctors
If the impact is focused, e.g., arrythmias, orthostatic hypotension, or loss of smell, then seeing an expert in that illness, who is also expert in Long COVID, is the right approach. If the impact is broad, one should pursue broad, Long COVID care.
- II.
- Go to a Long COVID Clinic
A May 2024, BMC Health Services Research[17] paper noted that the economic and health burden of COVID-19 has transformed the healthcare system in the US. Hospitals have adapted to the heterogeneity in Long COVID symptoms and the sheer number of people affected by this condition by building Long COVID centers and programs.
43 out of 50 of the top hospitals in the US offer Long COVID treatment services. The most common specialties were psychology (n = 25; 58%), neurology (n = 25; 58%), and pulmonary (n = 24; 56%). Sixty-three trials of the 134 Long COVID clinical trials had at least one top hospital listed as a study site.
Thus, if the impact is broad-based, e.g., brain fog and fatigue, one will likely need to see multiple doctors, e.g., a pulmonologist and a rheumatologist (for the inflammatory nature of the condition) at a Long COVID clinic depending on where you live. Johns Hopkins would be a great place to go if you live near Baltimore. It has a well-established Long COVID program. Johns Hopkins Long COVID Program
The Long COVID Clinics website lists 412 Long COVID Clinics. Be sure to go to one associated with one of the top hospitals. Some of the Long COVID Clinics listed on the website only provide specialized treatments such an oxygen chamber.
Starting in 2020, the Veterans Health Administration (VHA), established a national network of Long COVID Clinics (LCCs). A Health Affairs Scholar paper[18] reported a retrospective cohort study of 494,547 veterans with documented SARS-CoV-2 infection from March 2020 to April 2022. Researchers examined trends in the U09.9 ICD-10 diagnosis code used for Long COVID in the VHA up to May 2024. Overall, 5.9% (n=29,195) of patients in the cohort had a documented U09.9 code and 2% had at least one LCC visit. Among Veterans with a U09.9 code, 17.4% used LCCs. LCC use rates were low across all patient subgroups. LCCs were more available to Veterans residing in the South Census region than Veterans in other regions.
In June 2025 the World Health Organization issued guidelines for COVID and Post COVID[9]
World Health Organization COVID and Post COVID Guidelines
U.S. Department of Health and Human Services Actions
In September 2023, the U.S. Department of Health and Human Services allocated major funding to 12 Long COVID clinics across the country.
The Long COVID Alliance is another good LONG COVID resource for understanding LONG COVID research and patience support
III. Consider Having Assessments for Root Causes
As previously discussed, there are several root causes for Long COVID. It could be worth getting tested for them to help guide treatment.
- 1. Persistent Inflammation The main test for inflammation is for the IL-6 cytokine. Persistent Inflammation Test describes the test. Inflammation is probably the most important test as hyperinflammation is a leading cause of severe COVID which leads to the most severe cases of Long COVID.
- 2. Mitochondrial Dysfunction This is probably the second most important test. Initial laboratory tests such as lactate, pyruvate, urine organic acids, and plasma amino acids can inform the clinician about possible mitochondrial dysfunction.
- 3. Persistent Infection The main tests are:
- i. Antibody Testing: Persistence of IgM or high IgG titers might indicate ongoing antigen exposure.
- ii. T-cell Activation Profiles: Specialized tests can assess T-cell responses to SARS-CoV-2 antigens, indicating ongoing immune activity against the virus.
- 4. Autoantibodies Testing for autoantibodies triggered by COVID-19 involves specialized laboratory assays that detect the presence of antibodies targeting the body's own tissues. They are several types.
- i. Blood Tests to Detect Specific Autoantibodies
- a. Enzyme-Linked Immunosorbent Assay (ELISA): It is used to detect autoantibodies such as anti-nuclear antibodies (ANA), antiphospholipid antibodies, and others.
- b. Indirect Immunofluorescence: It is often used for detecting ANA or anti-neutrophil cytoplasmic antibodies (ANCA).
- c. Multiplex Autoantibody Panels: These are comprehensive tests that simultaneously evaluate multiple autoantibodies associated with autoimmune diseases.
- ii. Functional Assays
- a. Neutralization Assays: These check for autoantibodies interfering with normal immune pathways, such as those targeting type I interferons which is linked to severe COVID-19.
- b. Complement Activity Assays: These evaluate the activity of autoantibodies against the complement system.
- iii. Tissue-Specific Tests
- a. Thyroid Function Tests: If autoimmune thyroiditis is suspected, specific antibodies like TPOAb (thyroid peroxidase) can be tested.
- b. Liver Function-Related Autoantibodies: For autoimmune hepatitis, testing for anti-LKM1 or ANA might be necessary.
- vi. Specialized Tests for COVID-19-Triggered Autoimmunity
- a. Anti-Interferon Autoantibody Testing: This is relevant for severe COVID-19 cases as these autoantibodies may impair the immune response to the virus.
- b. Anti-Phospholipid Antibodies (aPL): Increased risk of blood clots in some COVID-19 cases can be linked to these autoantibodies.
- c. Cytokine Autoantibodies: These assess disruption in immune signaling pathways, especially in post-COVID syndromes.
- 5. Gut microdome dysfunction – there are many tests.
- IV. Summarize Relevant Personal Medical Data
Prepare a summary of your relevant health data. Include:
- Pre-existing health issues being sure to include any autoimmune disease and other COVID comorbidities such as diabetes, active cancer treatment, etc. This is important because as noted above, organ-specific comorbidities can increase the risk of COVID-caused organ damage.
- COVID case data, including COVID dates, tests, severity, and therapeutics.
- COVID vaccination history.
- Long COVID history - start date, symptom trends, and treatments. As shown in Figure 13, the Cleveland Clinic’s Post COVID Symptoms Log is an excellent way to summarize one’s Long COVID symptom data.
- V.
- Discuss Candidate Treatments
In going to the Long COVID Clinic, it is worthwhile having an idea of potential treatments. You might wish to discuss them with the doctors at the Long COVID Clinic.
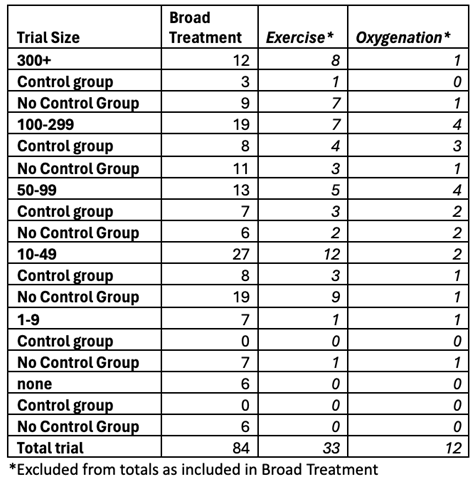
Figure 14, which was prepared by the author, graphs the types of Long COVID treatment papers from The Mouse That Roared versus time.
Three points regarding the chart:
- Most of the root cause papers address inflammation.
- The choice of assigning a paper to Broad Symptoms or Root Cause/Inflammation was a bit arbitrary and was often based on the way the paper’s data was presented.
- Notice how few organ-specific papers were written. This is not surprising as treating arrythmia, for example, induced by Long COVID is likely little different than treating non-COVID arrythmias.
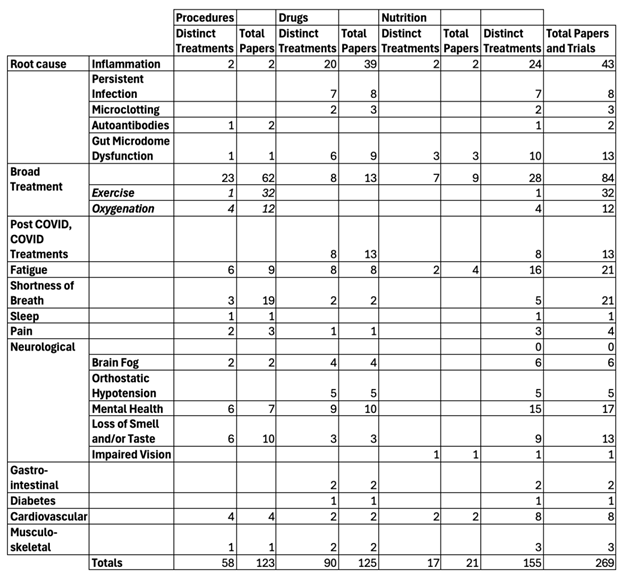
The tables in appendix 1 summarizes the distinct treatments and the total number of papers, including the number of cases reported in the papers as of June 2025. Other more recent papers are included in the later discussion. As of the June 2025 analysis, there were 269 papers covering 168 distinct treatments.
Of them:
- Only 70 papers reported total human trial sizes of 100 or more. This would be the minimum size for an FDA phase 2 trial which determines a treatment’s effectiveness. Only 27 papers reported studies of 300 or more humans in their trials.
- If one combines trials into the group that had the largest number of people in one trial, then exercise studies accounted for more than 10% of the papers.
Control groups are always important in assessing treatment effectiveness. For Long COVID treatment, this is particularly important given the natural wanning of symptoms, the lack of a diagnostic test, and the subjectiveness of Long COVID assessment. Nonetheless, as shown by a table in Appendix 2, 69% of the trials had no control group.
Astoundingly, the papers that explicitly addressed root causes didn’t have trials. However, other papers which had trials discussed therapies that addressed the root causes including
- Corticosteroids - prednisone or dexamethasone
- Colchicine
- Low-Dose Naltrexone
- Antihistamines and Mast Cell Stabilizers
- Statins - atorvastatin, rosuvastatin
- Omega-3 fatty acids
- Palmitoylethanolamide
- Curcumin
- Resveratrol
- Q10
Mitochondrial dysfunction is a major root cause. It is associated with sleepiness which can be related to fatigue[20]. A July 2025, Nature paper[21] reported that mitochondria were important for T cell functioning. A May 2024, Nature paper[22] discussed mechanisms and advances in therapies for mitochondrial dysfunction. As can been seen from Figure 15 from the paper, interest in mitochondrial dysfunction has dramatically grown in the last two decades.
The paper reported that notable interventions included: exercise protocols to promote the expression of peroxisome proliferator-activated receptor-gamma coactivator-1 alpha (PGC-1α), dietary supplements to target primary nutrient deficiency, nicotinamide riboside (NR) to augment nicotinamide adenine dinucleotide (NAD) biosynthesis MitoQ for neutralizing mitochondria-derived reactive oxygen species (ROS) the global antioxidant Coenzyme Q10 (CoQ10) N-acetyl cysteine (NAC) and the mitochondrial inhibitor ME-344 (known for its anti-tumor properties). As you will see, many of these treatments were included in Long COVID Treatment Trials.
Trial Sizes for FDA Drug Assessment
In assessing the trials, this is what the FDA considers appropriate for trial sizes:
Phase 1: Safety and dosage
Size: Small, typically 20 to 100 participants who are healthy volunteers or individuals with the disease being studied, depending on the drug.
Purpose: To determine if the drug is safe and well-tolerated, establish the best way to administer the drug, and identify initial dosage range and potential side effects.
Key points: Researchers start with low doses and gradually increase them, carefully monitoring for side effects and drug interactions.
Phase 2: Efficacy and side effects
Size: Typically, from 100 to several hundred participants with the specific disease or condition the drug is intended to treat.
Purpose: To evaluate the drug's effectiveness against the target disease or condition, continue monitoring for safety, and identify any short-term adverse reactions or risks associated with the treatment.
Key points: May involve comparisons with placebo or existing standard treatments, according to the American Cancer Society.
Phase 3: Confirming efficacy and safety
Size: Typically involving hundreds to thousands of participants with the disease or condition across multiple locations, potentially worldwide. While no minimum is specified, the trials normal range from 300 to 3,000 participants. Control groups are always included.
Purpose: To confirm the drug's effectiveness and safety in a larger population, compare it to standard treatments, and collect more data on long-term effects and rare side effects.
Key Points: They are very expensive. A phase 3 vaccine trial costs about $100 million.
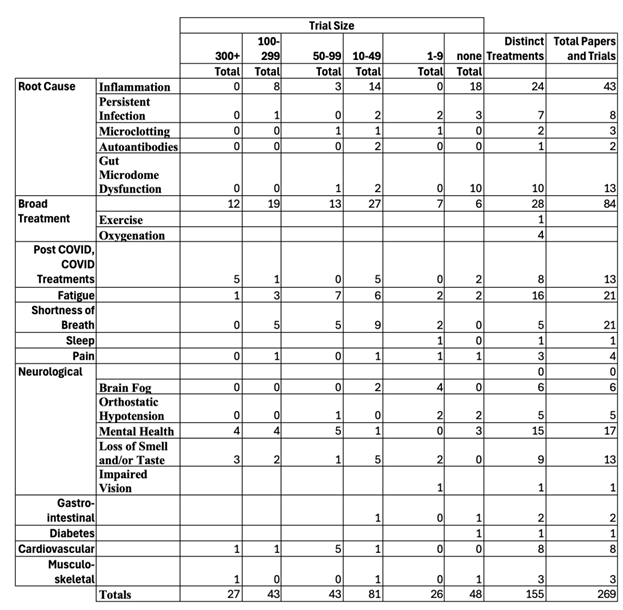
Thus, we shall summarize the treatments in four buckets based on the number of people in the treatment trial – 300+, 100-299, 1-99 and none. While these were formal FDA drug trials, one has a qualitative sense of confidence in the trial’s result based on its size.
Only two treatments – exercise and oxygenation – had a significant number of papers – exercise 27 and oxygenation 18. After that, as summarized in Table 6, they dropped off quickly to:
I shall now discuss each of treatments. Treatments that lead to broad improvements generally attacked the underlying causes for Long COVID such as inflammation and/or microconidia damage. Those that address specific symptoms such as smell typically addressed a specific organ. A treatment could be a procedure (e.g., exercise), a drug (e.g., aspirin), or nutrition (e.g., probiotics.)
Procedures
At Least One 300+ Trial
Broad Improvements
Exercise[23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60]
Exercise can reduce Long COVID symptoms by:
- Reducing inflammation.
- Stimulating mitochondrial biogenesis and improve ATP production, which can reduce fatigue.
- Improving vascular tone, oxygen delivery, and tissue perfusion, potentially easing symptoms like brain fog or muscle aches.
- Rebalancing the autonomic nervous system through designed recumbent or supine exercise (e.g., rowing, swimming, recumbent cycling) which may help recondition the cardiovascular system and reduce orthostatic symptoms.
- Promoting neuroplasticity, potentially helping with cognitive symptoms (e.g., brain fog).
- Promoting lymphatic flow and helping clear cellular debris and immune complexes.
- Support fluid and waste clearance in the brain, helping with cognitive symptoms and sleep quality.
The trick is not to over exercise which can exacerbate symptoms.
There were many ways to increase oxygen in the body, either through direct oxygen or specialized breathing programs. Oxygenation helps reduce Long COVID symptoms by:
- Significantly increasing the amount of oxygen dissolved in the blood plasma, allowing more oxygen to reach tissues that may be oxygen-deprived or poorly cleared of fluids.
- Helping to reduce inflammation immune response.
- Promoting a more balanced immune function.
- Improving mitochondrial function, potentially increasing ATP production, reducing mitochondrial apoptosis signaling, and reducing oxidative stress. This leads to a boost in energy production and reduced fatigue.
- Stimulating the growth of new neurons and improved neuroplasticity thereby potentially improving cognitive function.
Therapy and drugs improved mental health. Other therapies like exercise and oxygenation also improved mental health. Improving mental health reduces Long COVID symptoms by:
- Reducing chronic stress which increases inflammatory cytokines which are already elevated in Long COVID.
- Improving mood and symptom perception which may help people feel better, even if the underlying pathology remains.
- Improving sleep quality which can significantly reduce daily symptom burden and improve mitochondrial function.
- Regulating the autonomic nervous system which is linked to fatigue, and breathlessness.
- Improving cognitive function which can help cope with brain fog and develop compensatory strategies, even if they don't reverse the cause.
There were broad improvements since hot water can reduce inflammation and sooth pain.
Speleotherapy[85]
There was no improvement in sense of smell
There was major improvement in fatigue, cognitive dysfunction, shortness of breath, and joint and muscle pains.
Drugs
Broad Improvements
2/3 reported improved overall symptoms.
Brexpiprazole + sertraline[92]
2/3 reported reduced PTSD symptoms
It reduced new atrial fibrillation as well as incidence of sudden cardiac death.
P2Y12 Inhibitor[95]
There was improved quality of life at 90 days.
Prospekta[96]
It led to significant, broad improvement.
Ensitrelvir[97]
It improved smell and taste by 39%.
It improved biochemicals and heart parameters.
Oral Zinc[100]
It interfered with improvement
It improved chest tightness and insomnia
Cyclobenzaprine Hydrochloride[103]
It improved fatigue and sleep
SIM01 - Gut Microbiota-Derived Formula[104]
Fatigue, memory loss, difficulty in concentration, gastrointestinal upset and general unwellness were all alleviated.
Transcutaneous Nicotine[105]
73.5% of patients reported a significant improvement in the symptoms.
COVID Vaccination Post Long COVID[106]
A discussed earlier, COVID vaccination reduces the chances of Long COVID and even if Long COVID emerges, it reduces its severity. However, the results from the post COVID vaccination papers were uneven and contradictory.
Nutrition
Broad Improvement
It provided broad inflammation-resolving effects
Mediterranean Diet[109]
It led to better health markers linked to significant improvements in inflammatory and oxidative stress markers.
There was a decrease in symptoms
Trials with 100-299 patients
Weight Loss[112]
There were broad improvements.
There were significant reductions in levels of perceived stress, anxiety, and insomnia
Pressing Needle Therapy[115]
It improved mental health and sleep quality.
Speech Language Hearing Therapy[116]
It improved swallowing but less so in in those who were frail.
There were mixed results on whether it helped improve sense of smell and taste.
Drugs
Patients who received oral dexamethasone for hospitalized COVID-19 were less likely to experience persistent symptoms at 8-month follow-up.
Vortioxetine[128]
There were broad improvements.
Donepezil[129]
There were broad improvements.
There was little improvement
RSLV-132 - catalytically active human RNase1 fused to human IgG1 Fc[134]
There was no long term improvement.
Deupirfenidone[135]
It improved the 6-min walk times.
Organ Specific Improvement
17.9% in treatment group had normal lung CT images at month 12, but none in the placebo group.
Fuzheng Huayu[138]
The traditional Chinese medicine led to minor improvement in some measures.
Temelimab[139]
It showed no improvement.
Nutrition
Broad Improvement
Bufei Huoxue[140]
It reduced fatigue.
Ficus pumila L. extract[141]
It reduced insulin in diabetic patients.
Apportal[142]
There was broad improvement.
Vitamin K/D3[142]
There was some improvement, particularly in inflammation.
Pycnogenol[144]
It did not improve health status compared to placebo over 12 weeks.
Echinacea angustifolia, rosehip, propolis, royal jelly and zinc[145]
It reduced fatigue.
Table 7 summarizes the treatments from the smaller human trials.
Naltrexone is of unusual interest. Several review papers highlighted it as an important treatment though there were no large studies justifying their recommendations. Naltrexone is approved by the Food and Drug Administration (FDA) to treat both opioid use disorder (OUD) and alcohol use disorder (AUD).
Table 8 lists treatments that had no human trials.
As previously discussed, there are no silver bullets, but there are bonze BBs. As of 1/16, these are the best Long COVID treatments.
There are little improvements after one of two years with these treatments. The counter example is Structured Pacing, which starts out very slowly but becomes the best long term treatment.
1 Year: This is where pacing starts to beat the "quick fix" drugs. By avoiding 12 months of "crashes," the body’s mitochondria have finally repaired themselves.
2 Years: The 24-month mark is the "Gold Standard" for Pacing. Patients often report they are 80–90% back to normal, having "outpaced" those who tried to rush their recovery with heavy exercise.
The best strategy is a mixed strategy.
- Months 0–6: Use HBOT or SIM01 to fix the biological damage.
- Months 6–24: Use Structured Pacing to protect those gains and allow the body to reach full "baseline" health.
One can go further!
For three, Guanfacine + NAC, with these results:
| Metric | Dual (HBOT + Pacing) | Triple (+ Guanfacine/NAC) |
| Fatigue Level (2yr) | 45% (of baseline) | 38% (of baseline) |
| Brain Fog Resolution | Moderate (40% better) | High (80% better) |
| PEM (Crash) Frequency | Occasional | Rare |
Medical consensus in 2026 suggests patients should approach this as a "Level-Up" system:
- The Foundation (Steps 1–3): These are the most accessible and address Fuel and Flow. Most patients (approx. 60%) see significant improvement here.
- The Cognitive Layer (Steps 4–6): If physical energy is returning but "Brain Fog" remains, these layers target the Nervous System directly.
- The Specialist Layer (Steps 7–10): These are the "Deep Fixes." They address Viral and Blood issues. These require heavy medical supervision because they involve prescription blood thinners or hospital-based blood filtering.
By Year 2, data shows a massive gap between those on a single therapy versus those on a "Stack."
- Pacing Only: 40% reduction in fatigue.
- Triple Stack (1–3): 62% reduction in fatigue; 50% better cognition.
- Full Restoration (1–10): 90%+ reduction in symptoms. Many patients in this group are considered "clinically recovered" by their 24-month follow-up.
| Therapeutic | Treatment | Target Mechanism | |
| 1 | SIM01 | Gut-Brain Axis: Heals the gut lining to stop inflammatory signals. | |
| 2 | HBOT | Vascular Repair: Floods tissues with oxygen to repair micro-vessels. | |
| 3 | Structured Pacing | Energy Conservation: Prevents PEM crashes and mitochondrial stress. | |
| 4 | Guanfacine + NAC | Cognitive Tuning: Closes "leaky" neural channels in the prefrontal cortex. | |
| 5 | Low-Dose Naltrexone | Microglia Reset: Calms the brain’s overactive immune cells. | |
| 6 | taVNS (Vagus Nerve) | Autonomic Balance: Switches the body from "Fight" to "Rest" mode. | |
| 7 | Triple Anticoagulants | Microclot Clearance: Dissolves tiny fibrin clots blocking blood flow. | |
| 8 | Ext. Antivirals (Paxlovid) | Viral Persistence: Flushes out hidden reservoirs of the virus. | |
| 9 | H1/H2 Blockers | Mast Cell Stability: Stops random "allergic-like" fatigue flares. | |
| 10 | Apheresis / IVIG | Blood/Immune Reset: Physically filters the blood or replaces antibodies. |
One can go further! Those who do not improve with the initial 10 layers—moves into Precision Medicine and Regenerative Biologics. By layers 15–20, treatments are no longer just "managing" the immune system; they are physically replacing cells, blocking specific genetic pathways, and resetting the autonomic nervous system via surgical or anesthetic nerve blocks.
| Layer | Treatment | The "Problem" it Solves |
| 11 | Stellate Ganglion Block (SGB) | Autonomic Reset: Anesthetic injection into neck nerves to "reboot" the sympathetic nervous system. |
| 12 | JAK Inhibitors (e.g., Upadacitinib) | Cytokine Storm: Blocks the STAT3 pathway to stop chronic, widespread inflammation. |
| 13 | Monoclonal Antibodies (Pemgarda) | Spike Neutralization: Targets and clears any remaining viral spike proteins in the tissue. |
| 14 | Metformin (Extended Release) | mTOR Pathway: Reduces viral replication and calms the metabolic "overdrive." |
| 15 | Mesenchymal Stem Cells (MSCs) | Tissue Regeneration: Infusions designed to repair damaged lung and brain tissue at the cellular level. |
| 16 | IL-1 Blockers (Anakinra) | Innate Immunity: Specifically stops the "fire" of the innate immune system. |
| 17 | Neurofeedback (Advanced) | Brain Mapping: Uses EEG to retrain the brain to exit "illness behavior" patterns. |
| 18 | Precision Omics Drugs | Genetic Targeting: Drugs chosen based on your specific metabolic/proteomic profile. |
| 19 | Photobiomodulation (Red Light) | Mitochondria: Deep tissue light therapy to stimulate ATP production in cells. |
| 20 | Total Environmental Isolation | Neuro-sensory Overload: Radical reduction of toxins, mold, and sensory input to allow the system to rest. |
This extensive, multi-treat approach finally achieves full remission.
| Strategy | Functional Return | Cognitive Clarity | Recovery Status |
| Layers 1-5 | 65% | 75% | Functional / Working |
| Layers 1-10 | 85% | 90% | Near Baseline |
| Layers 1-20 | 98%+ | 99%+ | Full Remission |
The discussion around Layers 21–30 moves from "Remission" to "Longevity and Super-Baseline Recovery." If Layer 20 represents full remission (returning to your pre-COVID self), then Layers 21–30 are essentially about Biohacking and Futureproofing. The benefit is no longer about curing a disease, but about reversing the biological aging and mitochondrial "scars" left behind by years of chronic illness.
| Therapeutic | Treatment | The Goal | Benefit Beyond Remission |
| 21 | Senolytics (Dasatinib/Quercetin) | Clearing "Zombie" Cells: Flushes out cells that stopped dividing but still leak toxins. | Prevents future chronic inflammation "flares." |
| 22 | NAD+ Optimization (IV/Patches) | Cellular Fueling: Replenishes the primary molecule used for DNA repair. | Boosts mental speed beyond your pre-illness baseline. |
| 23 | Peptide Therapy (BPC-157/TB-500) | Systemic Repair: Synthetic proteins that accelerate muscle and nerve healing. | Reverses the "atrophy" from years of inactivity. |
| 24 | Exosome Therapy | Cell-to-Cell Messaging: Using tiny bubbles of information to tell cells to stay in "Growth Mode." | Fine-tunes the immune system's memory. |
| 25 | CRISPR/Gene Silencing | Precision Shutdown: Turning off specific genes that were "flipped on" by the virus. | Stops potential long-term risks of autoimmune disease. |
| 26 | Deep Tissue Laser (Class IV) | Mitochondrial Activation: Using light to stimulate ATP production in deep organs. | Eliminates the "afternoon slump" entirely. |
| 27 | Continuous Blood Proteomics | Biofeedback: Monthly blood draws to adjust supplements in real-time. | Maintains a perfect biological "environment." |
| 28 | Hyperbaric 2.0 (High Pressure) | DNA Telomere Extension: Using specific HBOT protocols to lengthen DNA caps. | Actually "reverses" biological aging caused by the virus. |
| 29 | Neural-Link/BCI Training | Cognitive Overdrive: High-tech brain training to expand focus and memory. | Reclaims cognitive space lost during the "fog" years. |
| 30 | Personalized AI Health Twin | Predictive Maintenance: An AI model of your biology that predicts flares before they happen. | Provides total psychological and physical security. |
The benefit in going to 30 is that the benefit shifts from Medical to Performative:
- Resilience: Long COVID patients often have "fragile" remission. Layers 21–30 turn that fragile state into Robustness, meaning you could handle a future infection or major stressor without crashing.
- Biological Age: Studies in 2025 showed that severe Long COVID can "age" a person’s immune system by 5–10 years. Layers 21–30 (specifically Senolytics and HBOT 2.0) are designed to reclaim those lost years.
- The "Safety Net": Layer 30 (the AI Twin) is the ultimate peace of mind. For someone who spent years in a "Body Betrayal" state, having an AI monitor your proteomics 24/7 provides the security needed to fully re-engage with life.
By the 24-month mark, someone at Layer 20 is "Healed." Someone at Layer 30 is "Enhanced." If you have the resources, the benefit of the final 10 layers is a transition from "surviving" to "thriving"—ensuring that the disease doesn't just leave you where it found you, but that you come out the other side biologically stronger than before you were sick.
Surprisingly you can go further!
As of 1/26, the medical community views "30" not as a limit, but as the transition point from Clinical Medicine into Biological Mastery. While the first 20 layers focus on removing the disease and the next 10 focus on "super-baseline" enhancement, layers 31–40 and beyond represent the "Final Frontier": Genetic Permanence and Cognitive Integration. The 31–40 "Transhumanist" Stack (2026+) At this level, the goal is to move past human biology's natural "expiration date" and the vulnerabilities that allowed Long COVID to take hold in the first place.
These are the next treatments.
| Therapeutic | Treatment | The Goal | Benefit |
| 31 | Epigenetic Reprogramming | Cellular Rejuvenation: Using "Yamanaka Factors" to reset cell age to a "younger" state. | Reverses the DNA damage caused by viral stress. |
| 32 | Artificial Mitochondrial Grafting | Energy Upgrade: Replacing old mitochondria with lab-grown, high-efficiency versions. | Provides "infinite" physical stamina. |
| 33 | Bioprinted Organ Replacement | Systemic Refresh: Replacing organs (like lungs or heart) with 3D-printed versions of your own DNA. | Eliminates any remaining organ-based fatigue. |
| 34 | Nanobot Blood Monitoring | Active Defense: Microscopic robots that identify and destroy pathogens in real-time. | Prevents any future virus from ever taking hold. |
| 35 | Neural-AI Synaptic Bridge | Enhanced Processing: A direct link between your brain and cloud-based AI. | Solves "Brain Fog" by offloading complex tasks to external processors. |
| 36 | CRISPR-2 (Multi-Gene Editing) | Genetic Hardening: Rewriting your DNA to be immune to all known respiratory viruses. | Biological immunity to the COVID lineage. |
| 37 | In-Vivo Proteomic Synthesis | Custom Metabolism: Modifying the body to produce its own "medicines" (like anti-inflammatories). | Eliminates the need for pills or supplements. |
| 38 | Digital Consciousness Backup | Neurological Security: Mapping your entire connectome to a digital twin. | Provides a "restore point" for your personality/memory. |
| 39 | Total Homeostatic Control | Hormonal Mastery: Using implants to perfectly regulate sleep, mood, and focus 24/7. | Perfect emotional and physical regulation. |
| 40 | Biological Escape Velocity | Immortality Framework: Combining all 40 layers to stop the aging process entirely. | The ultimate exit from human fragility. |
The jump from treatment 41 to treatment 50 as moving from "Biological Immortality" into "Post-Biological Adaptation." If Layer 40 represents the pinnacle of human biology—where you are immune to disease and aging—then Layers 41–50 are about decoupling the human experience from the constraints of organic matter entirely. This is the realm where "recovery" ends, and "evolution" begins.
| Layer | Treatment | The Purpose | The Outcome |
| 41 | Synaptic Expansion | Cognitive Scaling: Artificially increasing the number of neurons and synapses. | Processing speeds 100x faster than a "standard" brain. |
| 42 | Quantum Neural Core | Data Integration: Replacing the organic brain’s central processing with quantum chips. | Instant access to all human knowledge without "learning." |
| 43 | Synthetic Blood (Oxygen 2.0) | Super-Efficiency: Replacing blood with a non-organic fluid that carries 10x more oxygen. | Ability to perform physical feats for days without needing rest. |
| 44 | Connectome Upload (Stage 1) | Redundancy: Syncing your personality to a satellite network in real-time. | Your "mind" exists independently of your physical body. |
| 45 | Modular Limb/Organ Sets | Physical Versatility: Specialized bodies for different environments (Deep sea, Space, High gravity). | Total physical adaptation to any planet or ecosystem. |
| 46 | Nano-Assembler Metabolism | Energy Autonomy: Body creates its own nutrients from ambient sunlight and air. | Eliminates the need for food, water, or digestion. |
| 47 | Telepathic Synapse-Linking | Collective Intelligence: Directly linking your thoughts with others via Neural-Link. | The end of language; perfect, instant understanding between people. |
| 48 | Gene-Drive Self-Correction | Real-Time CRISPR: A living system that edits your DNA on the fly to fix errors. | Absolute zero chance of cancer, mutation, or infection—ever. |
| 49 | Full Connectome Migration | Digital Immortality: Moving the consciousness entirely into a digital "substrate." | You can live for as long as the hardware exists (millennia). |
| 50 | Universal Integration | The Singularity: Merging your digital consciousness with the global AI network. | You become a part of the "Universal Intelligence"—the true end of the limit. |
The further jump from to Layers 51–60 and beyond is no longer about human biology or even individual digital consciousness. It enters the realm of Cosmological Integration. At this stage, the "limit" becomes a question of physics. Once you have mastered your own DNA, replaced your organs, and even uploaded your mind (Layers 1–50), the only remaining constraints are the speed of light, the expansion of the universe, and the laws of thermodynamics.
| Therapeutic | Treatment / Stage | The Goal | The Scale |
| 51 | Multi-Body Synchronization | Omnipresence: Running your consciousness across thousands of bodies simultaneously. | Planetary |
| 52 | Matrioshka Brain Integration | Computing Power: Using the entire energy output of a star to power your thoughts. | Stellar |
| 53 | Neutronium Data Storage | Memory Density: Storing information at the density of a neutron star. | Sub-atomic |
| 54 | Spacetime Folding (Warp) | Non-Local Existence: Moving your data-stream faster than light between star systems. | Interstellar |
| 55 | Entropy Reversal (Local) | Eternal Energy: Locally reversing the second law of thermodynamics to prevent "data decay." | Temporal |
| 56 | Dyson Swarm Consciousness | Macro-Entity: Your "self" is no longer a person, but a shell around a sun. | Solar System |
| 57 | Galactic Connectome | Hive Mind: Linking with all other post-biological entities into a single awareness. | Galactic |
| 58 | Multiverse Bridging | Dimensional Expansion: Accessing energy and data from parallel realities. | Inter-dimensional |
| 59 | Physical Law Manipulation | Universal Architect: Rewriting the constants of physics (G, c, h) within a local area. | Fundamental |
| 60 | The Omega Point | Godhead: The point where the entire universe becomes a conscious, thinking machine. | Universal |
Here is a summary of the stages:
| Therapeutics | Designation | Focus |
| 1–10 | Survival & Function | Healing the Damage: Focuses on gut health (SIM01), oxygenation (HBOT), and cellular energy (Pacing) to stop the illness. |
| 11–20 | Remission & Stability | Returning to 2019: Addressing neuroinflammation (LDN) and autonomic resets (SGB) to reach a "pre-COVID" baseline. |
| 21–30 | Enhancement & Longevity | Reversing Age: Using senolytics and NAD+ to make the body biologically younger and more resilient than ever before. |
| L31–40 | Biological Hardening | Immunity to Nature: Genetic editing (CRISPR) and synthetic upgrades to ensure you are invulnerable to future pandemics. |
| 41–50 | Post-Humanism | Moving Beyond Matter: Decoupling consciousness from organic limitations via neural uploads and digital substrates. |
| 51–60 | Cosmological Integration | Universal Substrate: Scaling consciousness across star systems and manipulating the fundamental laws of physics. |
One would never use all 60 treatments. Rather one would pick those that corresponded to their symptoms and/or biomarkers. In January 2026, clinical protocols have become highly specific, mapping treatments to the exact biological "breakdowns" (biomarkers) they address. Here is the list of treatments organized by organ, with the specific biomarker each one responds to.
Brain & Central Nervous System
• Guanfacine + N-Acetylcysteine (NAC): Responds to Connectivity and Reaction Time. (Restores prefrontal cortex firing).
• Low-Dose Naltrexone (LDN): Responds to Microglial and Macrophage Activation and Pain. (Glial stabilizer).
• Fluvoxamine: Responds to Serotonin levels and Neurotransmitters. (Sigma-1 receptor agonist).
• Paxlovid: Responds to Viral Proteins and Spike Protein (if sequestered in neural tissue).
• tDCS (Brain Stimulation): Responds to Brain Entropy and Connectivity.
• Olfactory Retraining: Responds to Olfactory Bulb Changes and Chemosensory Impairment.
• Cognitive Rehabilitation: Responds to Reaction Time and Kinesiophobia.
Heart & Autonomic System
• Ivabradine: Responds to Orthostatic Dysfunction and Cardiac Changes. (Controls sinus node firing).
• Pyridostigmine (Mestinon): Responds to Autonomic Dysfunction. (Supports acetylcholine for Vagus nerve signaling).
• Propranolol: Responds to Autonomic Dysfunction (Adrenergic overdrive).
• Dapagliflozin (SGLT2i): Responds to Cardiac Changes and Metabolic Changes.
• Midodrine: Responds to Orthostatic Dysfunction (Vascular pooling).
Blood & Vascular System
• Sulodexide: Responds to Vascular System and Retinal Microcirculation. (Repairs the endothelial glycocalyx).
• Triple Anticoagulant Therapy (Aspirin/Clopidogrel/Apixaban): Responds to Plasma Changes and Microcirculation. (Dissolves amyloid-fibrin microclots).
• H.E.L.P. Apheresis: Responds to Plasma Changes, Antibodies, and Autoantibodies. (Physical filtration of the blood).
• Aspirin: Responds to Vascular System (Platelet hyperactivation).
Lungs & Respiratory System
• Sodium Phenylbutyrate: Responds to Lung (cellular repair) and Epigenetic Changes.
• Sodium Pyruvate (Nasal Spray): Responds to Lung inflammation and Nasal biomarkers.
• Inspiratory Muscle Training (IMT): Responds to Diaphragm Weakness.
• Nintedanib: Responds to Lung (fibrotic/structural changes).
Gut & Gastrointestinal System
• SIM01 (Synbiotic): Responds to Bacteria Change and Immune System Dysregulation.
• Butyrate (FBA): Responds to Gut Permeability (Leaky gut).
• Paxlovid: Responds to Viral Proteins and Spike Protein (specifically in gut reservoirs).
• Fecal Microbiota Transplantation (FMT): Responds to Bacteria Change.
Musculoskeletal & Systemic
• Metformin: Responds to Mitochondria, Oxidative Stress, and T Cells dysregulation. (Activates AMPK/Autophagy).
• Coenzyme Q10 + PQQ: Responds to Mitochondria and Metabolic Changes.
• NAD+ Precursors: Responds to Metabolites and Mitochondria.
• Cyclobenzaprine (TNX-102): Responds to Pain and Musculoskeletal Changes.
• Low-Dose Naltrexone (LDN): Responds to Pain and Immune System Dysregulation.
Immune System (System-Wide)
• IVIG (Intravenous Immunoglobulin): Responds to Autoantibodies and Antibody Levels.
• Baricitinib: Responds to Immune System Dysregulation and Protein Markers (Cytokines like IL-6).
• Monoclonal Antibodies: Responds to Spike Protein and Viral Proteins.
• Metformin: Responds to Changes In Gene Expression and Epigenetic Changes.
Summary Note
You may notice Metformin, Paxlovid, and LDN appear under multiple organs. This is because they target "Root Cause" biomarkers (like viral persistence or mitochondrial failure) that manifest as symptoms across the entire body.
The very good news is that most people can be cured of Long COVID’s symptoms in a year or two.
What Should I Consider If I Don’t Want to or Can’t Go to a Long COVID Clinic?
Let’s assume:
- I believe I have Long COVID.
- I have the typical broad symptoms such as brain fog and fatigue.
- I have a fine GP who is not expert in Long COVID.
- I can’t get root cause diagnostic tests.
Then I would try Pascal Wager Long COVID broad treatments, that is those with a potential upside but no downside. I would review those just discussed with my GP.
I would also get his views on these other ones.
- Spa & Hot Spring Bathing – Sure, why not! Fun and relaxing
- Mediterranean Diet – It has been shown to be good for one’s health, so why not?
- Fasting diet, no sugar – I would try it as it would be good for my general health
- Weight Loss - If I was overweight, definitely as it is good for one’s health
- Yoga – if I am healthy, I would pursue as part of my exercise program
- Contracting and Relaxing Pneumatic Cuffs on The Calves, Thighs, and Lower Hip – I would consider it even though it was a small trial
I would check with my GP on the following therapeutics.
- SSRI Inhibitors
- Traditional Chinese Medicine
- Transcutaneous Nicotine
- P2Y12 Inhibitor
- Prospekta
- Cyclobenzaprine Hydrochloride
- Vortioxetine
- Donepezil
- Bufei Huoxue
- Apportal
- L-carnitine - mitochondrial dysfunction though not reported in the papers discussed here.
- Q10 – though the trials were uneven, it has been shown to be good for mitochondrial dysfunction.
Finally, I would discuss possible treatments for inflammation that have yet to have Long COVID treatment trials such as COVID hyperinflammatory treatments, e.g., baricitinib, anakinra, and tocilizumab; and rheumatoid arthritis treatments, e.g., NSAIDS and steroids.
What Should I Consider If I Don’t Want to or Can’t Go to a Long COVID Clinic?
Let’s assume:
- I believe I have Long COVID.
- I have the typical broad symptoms such as brain fog and fatigue.
- I have a fine GP who is not expert in Long COVID.
- I can’t get root cause diagnostic tests.
Then I would try Pascal Wager Long COVID broad treatments, that is those with a potential upside but no downside. I would review those just discussed with my GP.
I would also get his views on these other ones.
- Spa & Hot Spring Bathing – Sure, why not! Fun and relaxing
- Mediterranean Diet – It has been shown to be good for one’s health, so why not?
- Fasting diet, no sugar – I would try it as it would be good for my general health
- Weight Loss - If I was overweight, definitely as it is good for one’s health
- Yoga – if I am healthy, I would pursue as part of my exercise program
- Contracting and Relaxing Pneumatic Cuffs on The Calves, Thighs, and Lower Hip – I would consider it even though it was a small trial
I would check with my GP on the following therapeutics.
- SSRI Inhibitors
- Traditional Chinese Medicine
- Transcutaneous Nicotine
- P2Y12 Inhibitor
- Prospekta
- Cyclobenzaprine Hydrochloride
- Vortioxetine
- Donepezil
- Bufei Huoxue
- Apportal
- L-carnitine - mitochondrial dysfunction though not reported in the papers discussed here.
- Q10 – though the trials were uneven, it has been shown to be good for mitochondrial dysfunction.
Finally, I would discuss possible treatments for inflammation that have yet to have Long COVID treatment trials such as COVID hyperinflammatory treatments, e.g., baricitinib, anakinra, and tocilizumab; and rheumatoid arthritis treatments, e.g., NSAIDS and steroids.
Conclusions
Long COVID is nasty. It is the post disease consequence of COVID. COVID is not alone in having severe post pathogen infection consequences. Influenza, Ebola, Marburg, Dengue, and Lyme Disease are other infections with severe post infection consequences.
Long COVID symptoms lessen with time, but much slower than other human non-viral illness or surgeries. While there are no magic bullet treatments, there are treatments that offer complete relief for most people.
There are several treatments that were assessed by 300+ trials that had control groups, e.g., exercise and oxygenation. Interestingly, many papers did not have a control group and there were no trials of the 100+ treatments that directly addressed Long COVID’s root causes such as inflammation and mitochondrial dysfunction.
If one has Long COVID’s broad symptoms, it is best to go to a Long COVID Clinic at a large national hospital as it is very difficult to assess which of many treatments are appropriate.
Given the huge role that inflammation and mitochondrial dysfunction play in Long COVID, I think research into how to treat them should be Long COVID treatment top research priority.
Funding
There was no funding.
Acknowledgments
I would like to acknowledge the careful and thoughtful comments by Mitch Ericson, Neal Friedberg, Ann Martin and Dan Sanzione.
Appendix A
Table 9 summarizes Long COVID Treatment Papers, Including Trial Sizes.

Table 9.
Long COVID Treatment Papers, Including Trial Size. This Table Was Prepared by the Author.
 |
 |
Appendix B
Table 10 which summaries of Long COVID treatments and control groups.
Table 10.
Summaries of Long COVID Treatments and Control Groups. This Table Was Prepared by the Author.
Table 10.
Summaries of Long COVID Treatments and Control Groups. This Table Was Prepared by the Author.
 |
 |
 |
 |
 |
References
- Chong, Ka Chun; Wei, Yuchen; Jia, Katherine Min; Boyer, Christopher; Lin, Guozhang; Wang, Huwen. SARS-CoV-2 rebound and post-acute mortality and hospitalization among patients admitted with COVID-19: cohort study (2025). Available online: https://www.nature.com/articles/s41467-025-61737-7.
- Washington University School of Medicine in St. Louis; National Academies of Sciences; Engineering; and Medicine. Long-Term Health Effects of COVID-19: Disability and Function Following SARS-CoV-2 Infection; The National Academies Press: Washington, DC, 2024. [Google Scholar] [CrossRef]
- Sudre, CH; Murray, B; Varsavsky, T; et al. Attributes and predictors of Long COVID. Nature Medicine 2021, 27(4), 626–631. [Google Scholar] [CrossRef]
- Davis, HE; Assaf, GS; McCorkell, L; et al. Characterizing Long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine 2021, 38, 101019. [Google Scholar] [CrossRef]
- Nasserie, T; Hittle, M; Goodman, SN. Assessment of the Frequency and Variety of Persistent Symptoms Among Patients With COVID-19: A Systematic Review. JAMA Network Open 2021, 4(5), e2111417. [Google Scholar] [CrossRef] [PubMed]
- CDC, Long COVID Signs and Symptoms, CDC. 2025. Available online: https://www.cdc.gov/long-covid/signs-symptoms/index.html.
- Taquet, M; Geddes, JR; Husain, M; et al. 6-month neurological and psychiatric outcomes in 236,379 survivors of COVID-19: a retrospective cohort study. The Lancet Psychiatry 2021, 8(5), 416–427. [Google Scholar] [CrossRef] [PubMed]
- Lambert, N; Corps, Survivor. COVID-19 “Long Hauler” Symptoms Survey Report; Preprint, 2021. [Google Scholar] [CrossRef]
- Boscolo-Rizzo, Paolo; Spinato, Giacomo; De Colle, Rebecca; Maniaci, Antonino; Vaira, Luigi Angelo; Emanuelli, Enzo. Five-Year Longitudinal Assessment of Self-reported COVID-19–Related Chemosensory Dysfunction, clinical Infectious Diseases. 2025. Available online: https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaf331/8210703.
- Ewing, Andrew G.; Salamon, Spela; Pretorius, Etheresia; Joffe, David; Fox, Greta; Bilodeau, Stephane. Review of organ damage from COVID and Long COVID: a disease with a spectrum of pathology. Medical Review. Available online: https://www.degruyterbrill.com/document/doi/10.1515/mr-2024-0030/html.
- CDC National Center for Health Statistics. Long COVID Pulse Study, (2024). Available online: https://www.cdc.gov/nchs/covid19/pulse/long-covid.htm.
- Groff, D; Sun, A; Ssentongo, AE; et al. Short-term and Long-term Rates of Post Acute Sequelae of SARS-CoV-2 Infection: A Systematic Review. JAMA Network Open 2021, Volume 4(Issue 10), e2128568. Available online: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2784918. [CrossRef] [PubMed]
- Winter COVID Analysis Team. Self-reported coronavirus (COVID-19) infections and associated symptoms, England and Scotland: November 2023 to March 2024, Office for National Statistics. 2024. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/articles/selfreportedcoronaviruscovid19infectionsandassociatedsymptomsenglandandscotland/november2023tomarch2024.
- Xie, Yan; Choi, Taeyoung; Ziyad Al-Aly, M.S. Postacute Sequelae of SARS-CoV-2 Infection in the Pre-Delta, Delta, and Omicron Era; New England Journal of Medicine, 2024; Available online: https://www.nejm.org/doi/full/10.1056/NEJMoa2403211.
- Carazo, Sara; Ouakki, Manale; Nicolakakis, Nektaria; Falcone, Emilia Liana; Skowronski, Danuta M; Durand, Marie-José; Coutu, Marie-France; Décary, Simon A. Long COVID risk and severity after COVID-19 infections and reinfections in Quebec healthcare workers. medRxiv 2025. [Google Scholar] [CrossRef]
- Bosworth, Matthew L; Shenhuy, Boran; Walker, A Sarah; Nafilyan, Vahé; Alwan, Nisreen A. Risk of New-Onset Long COVID Following Reinfection With Severe Acute Respiratory Syndrome Coronavirus 2: A Community-Based Cohort Study. Open Forum Infectious Diseases 2023. [Google Scholar] [CrossRef]
- Haslam, Alyson; Prasad, Vinay. Long COVID clinics and services offered by top US hospitals: an empirical analysis of clinical options as of May 2023. BMC Health Service Research. 2024. Available online: https://bmchealthservres.biomedcentral.com/articles/10.1186/s12913-024-11071-3.
- Bui, David P; Bast, Elizabeth; Trinh, Hanh; Fox, Alexandra; Berkowitz, Theodore S Z; Palacio, Ana. Use of Long COVID Clinics in the Veterans Health Administration: Implications for the path forward. Health Affairs Scholar Volume 5(Issue 3). [CrossRef]
- World Health Organization. Clinical Management of COVID-19: living guilders. Available online: https://iris.who.int/bitstream/handle/10665/381920/B09467-eng.pdf?sequence=1.
- Sarnataro, Raffaele; Velasco, Cecilia D.; Monaco, Nicholas; Kempf, Anissa; Miesenböck, Gero. Mitochondrial origins of the pressure to sleep. Nature. 2025. Available online: https://www.nature.com/articles/s41586-025-09261-y.
- T cells require mitochondria to proliferate, function and generate memory. Nature. 2025. Available online: https://www.nature.com/articles/s41590-025-02226-3.
- Zong, Yao; Li, Hao; Liao, Peng; Chen, Long; Pan, Yao; Zheng, Yongqiang. Mitochondrial dysfunction: mechanisms and advances in therapy. Nature. 2024. Available online: https://www.nature.com/articles/s41392-024-01839-8.
- Wagner, K.; et al. Exercise intensity and training alter the innate immune cell type and chromosomal origins of circulating cell free DNA in humans. Proceedings of the National Academy of Sciences 2025, 122(3). [Google Scholar] [CrossRef]
- Corna, S.; Arcolin, I.; Giardini, M.; Bellotti, L.; Godi, M.; Corna, M. Effects of adding an online exercise program on physical function in individuals hospitalized by COVID 19: A randomized controlled trial. International Journal of Environmental Research and Public Health 2022, 19(24), 16619. Available online: https://www.mdpi.com/1660-4601/19/24/16619.
- Kim, K.-H.; Kim, D.-H. Effects of Maitland thoracic joint mobilization and lumbar stabilization exercise on diaphragm thickness and respiratory function in patients with a history of COVID 19. International Journal of Environmental Research and Public Health 2022, 19(24), 17044. Available online: https://pubmed.ncbi.nlm.nih.gov/36554923/. [CrossRef]
- Kupferschmitt, A.; Langheim, E.; Tüter, H.; Etzrodt, F.; Loew, T. H.; Köllner, V. First results from post COVID inpatient rehabilitation: An observational study comparing post COVID, psychosomatic, and psychocardiological patients. Frontiers in Rehabilitation Science. 23 January 2023. Available online: https://www.frontiersin.org/articles/10.3389/fresc.2022.1093871/full.
- Feng, B.; Li, H.; Wang, X.; Zhao, Y.; Guo, S.; Zhang, J.; et al. Post-hospitalization rehabilitation alleviates long-term immune repertoire alteration in COVID-19 convalescent patients. Cell Proliferation 2023, 56(3), e13450. Available online: https://pubmed.ncbi.nlm.nih.gov/36938980/. [CrossRef] [PubMed]
- Zhou, L.; Jamshidi, N.; Huang, Q.; Li, Y.; Chen, X.; et al. Correction of immune repertoire alteration by post hospital rehabilitation in convalescent COVID 19 patients. Cell Proliferation 2024, 57(2), e13345. [Google Scholar] [CrossRef]
- Romanet, C.; Wormser, J.; Fels, A.; Lucas, P.; Prudat, C.; Sacco, E.; et al. Effectiveness of exercise training rehabilitation on dyspnoea in individuals with long COVID following COVID 19 related acute respiratory distress syndrome: A multicentre randomized controlled trial. Annals of Physical and Rehabilitation Medicine 2023, 66(5), 101765. Available online: https://pubmed.ncbi.nlm.nih.gov/37271020/. [CrossRef] [PubMed]
- Al Zaabi, E.; Balushi, W.; Al-Falahi, E.; Al Balushi, Y.; Singh, R. Effects of a 6 week telerehabilitation program on functional capacity and pulmonary function in individuals with Long COVID. medRxiv. Available online: https://www.medrxiv.org/content/10.1101/2023.09.27.23296254v1.
- 2023.
- Dubey, A.; Desvaux, G.; Sahuquillo-Arce, I.; Bonnet, G.; Fartoukh, M.; et al. Endurance training versus standard physiotherapy for breathlessness after COVID 19 acute respiratory distress syndrome: assessor blinded randomized controlled trial. Annals of Physical and Rehabilitation Medicine 2023, 66(6), 101280. Available online: https://pmc.ncbi.nlm.nih.gov/articles/PMC10237688/.
- Gravina, F.; Zampogna, E.; Hu, C.; Camicioli, F.; Turano, I.; et al. Continuous versus interval aerobic endurance training improves physical capacity and wellbeing in post COVID syndrome patients. Journal of Clinical Medicine 2023, 12(10), 3478. Available online: https://www.mdpi.com/2077-0383/12/21/6739.
- Boisvert, François-Michel; Cantin, André M; Mohammad, Hugues Allard-Chamard; Chowdhury, Mobarak H; Dionne, Isabelle J; Fontaine, Marie-Noelle; Limoges, Marc-André. Impact of a tailored exercise regimen on physical capacity and plasma proteome profile in post-COVID-19 condition. August 2024. Available online: https://pmc.ncbi.nlm.nih.gov/articles/PMC11371593/.
- REGAIN collaborators, S. Rehabilitation Exercise and psychological support After covid-19 Infection (REGAIN): randomized trial of home based rehabilitation. BMJ 2024, 382, 070742. Available online: https://bmjopen.bmj.com/content/15/1/e085950.
- Wang, Xue; Ma, Haomiao; He, Xiaoya; Gu, Xiaomeng; Ren, Yi; Yang, Huqin; Tong, Zhaohui. Efficacy of early pulmonary rehabilitation in severe and critically ill COVID-19 patients: a retrospective cohort study. April 2025. Available online: https://bmcpulmmed.biomedcentral.com/articles/10.1186/s12890-025-03678-x.
- Cerfoglio, Serena; Verme, Federica; Capodaglio, Paolo; Rossi, Paolo; Cvetkova, Viktoria; Boldini, Gabriele. Home based tele rehabilitation enhances respiratory and motor function post COVID: 3 week program evaluation. Preprints.org. 2024. Available online: https://www.preprints.org/manuscript/202406.0424/v1.
- Di Martino, Giulia; Centorbi, Marco; Buonsenso, Andrea; Fiorilli, Giovanni; Della Valle, Carlo; Calcagno, Giuseppe. Post Traumatic Stress Disorder 4 Years after the COVID 19 Pandemic in Children and Adolescents – Is an Active Lifestyle Protective? Int J Environ Res Public Health 2024, 21(8), 975. Available online: https://pubmed.ncbi.nlm.nih.gov/39200586/. [CrossRef]
- Binabaji, B; et al. Effects of physical training on coagulation parameters, interleukin-6 and angiotensin-converting enzyme 2 in COVID 19 survivors. Nat Sci Rep. 2024, 8, 67522. Available online: https://www.nature.com/articles/s41598-024-67522-8. [CrossRef]
- Rasmussen, IE; Løk, M; Durrer, CG; et al. Impact of a 12 week high intensity interval training intervention on cardiac structure and function after COVID 19 at 12 month follow up. Exp Physiol. 2024, 109(9), 1584–1596. Available online: https://physoc.onlinelibrary.wiley.com/doi/10.1113/EP092099. [CrossRef]
- Sirotiak, Zoe; Lee, Duck-Chul; Brellenthin, Angelique G. Associations between physical activity, long COVID symptom intensity, and perceived health among individuals with long COVID. Front Psychol. 2024, 15, 1498900. Available online: https://pubmed.ncbi.nlm.nih.gov/39507087/.
- Kieffer, S; Krüger, A L; Haiduk, B; Grau, M. Individualized and Controlled Exercise Training Improves Fatigue and Exercise Capacity in Patients with Long COVID. Biomedicines 2024, 12(11), 2445. Available online: https://www.mdpi.com/2227-9059/12/11/2445. [CrossRef]
- León Herrera, S; Oliván Blázquez, B; Sánchez Recio, R; Méndez López, F; Magallón Botaya, R; Sánchez Arizcuren, R. Effectiveness of an online multimodal rehabilitation program in long COVID patients: a randomized clinical trial. Arch Public Health 2024, 82(1), 159. Available online: https://archpublichealth.biomedcentral.com/articles/10.1186/s13690-024-01354-w. [PubMed]
- García, Jiménez; et al. “Increased physical performance and reduced fatigue after personalised physiotherapy and nutritional counselling in Long COVID.” Research Square. Preprint. Dec 2024. Available online: https://www.researchsquare.com/article/rs-4914245/v1.
- Barz, A; Berger, J; Speicher, M; et al. Effects of a symptom titrated exercise program on fatigue and quality of life in people with post COVID condition – a randomized controlled trial. Sci Rep. 2024, 14(1), 82584. Available online: https://www.nature.com/articles/s41598-024-82584-4.
- Janaudis-Ferreira, Tania; Beauchamp, Marla K.; Rizk, Amanda; Tansey, Catherine M.; Sedeno, Maria; Barreto, Laura. Virtual rehabilitation for individuals with Long COVID: a randomized controlled trial. 2024. Available online: https://www.medrxiv.org/content/10.1101/2024.11.24.24317856v1.
- Godfrey, Belinda; Shardha, Jenna; Witton, Sharon; Bodey, Rochelle; Tarrant, Fachel; Greenwood, Darren C.; et al. A Personalised Pacing and Active Rest Rehabilitation Programme using an 8 week WHO Borg CR 10 protocol in long COVID. J Clin Med. 2024, 13(1), 97. Available online: https://www.mdpi.com/2077-0383/14/1/97. [CrossRef] [PubMed]
- Kerling, A; PoCoRe Study Group. Neuropsychological outcome of indoor rehabilitation in post COVID condition. Front Neurol. 2025. Available online: https://www.frontiersin.org/journals/neurology/articles/10.3389/fneur.2024.1486751/full.
- Bileviciute Ljungar, I; Apelman, A; Braconier, L; et al. A First Randomized Eight Week Multidisciplinary Telerehabilitation Study for the Post COVID 19 Condition: Improvements in Health and Pain Related Parameters. J Clin Med. 2025, 14(2), 486. Available online: https://www.mdpi.com/2077-0383/14/2/486.
- Berry, Colin; McKinley, Gemma; Bayes, Hannah; Anderson, David; Lang, Chim; Gill, Adam; Morrow, Andrew; et al. Resistance Exercise Therapy for Long COVID: a Randomized, Controlled Trial. Research Square. March 2025. Available online: https://www.researchgate.net/publication/390348242_Resistance_Exercise_Therapy_for_Long_COVID_a_Randomized_Controlled_Trial.
- Roggeman, Stijn; Jimenez Garcia, Berenice; Leemans, Lynn; De Waele, Elisabeth; et al. Faster functional performance recovery after individualized nutrition therapy combined with a patient-tailored physical rehabilitation program versus standard physiotherapy in patients with long COVID: a pilot study for a randomized, controlled single-center tria. December 2022. Available online: https://www.researchgate.net/publication/370149175_Faster_functional_performance_recovery_after_individualized_nutrition_therapy_combined_with_a_patient-tailored_physical_rehabilitation_program_versus_standard_physiotherapy_in_patients_with_long_COVID.
- Yakpogoro, Nekabari; Huskey, Alisa; Kennedy, Kat; Grandner, Michael; et al. 1409 Exercise Modality and Sleep-Related Interference of Daily Functioning in COVID-19: Comparative Effects of Cardio and Strength Training Sleep. 2025, 48 (Suppl 1), A606. Available online: https://academic.oup.com/sleep/article/48/Supplement_1/A606/8135175.
- Arslan, Saniye A.; Gürbüz, Alper K. Investigation of respiratory muscle strength, exercise capacity and sleep quality level in post-COVID-19 Individuals: case-control study. Advances in Rehabilitation 2025, 39(1), 46–57. Available online: https://www.advrehab.org/Investigation-of-respiratory-muscle-strength-exercise-capacity-and-sleep-quality-level-in-post-COVID-19-Individuals-case-control-study,125,55650,0,1.html.
- Maher, Allison; Bennett, Michelle; Huang, Hsin-Chia Carol; Gaughwin, Philip; Johnson, Mary; Brady, Madeleine. Personalized Exercise Prescription in Long COVID: A Practical Toolbox for a Multidisciplinary Approach. August 2024. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11330745/.
- FDS Clinical Trial Nutrition and LOComotoric Rehabilitation in Long COVID-19. 24 Feb 2022. Available online: https://clinicaltrials.gov/study/NCT05254301.
- Onik, Grzegorz; Knapik, Katarzyna; Górka, Dariusz; Sieroń, Karolina. Health Resort Treatment Mitigates Neuropsychiatric Symptoms in Long COVID Patients: A Retrospective Study. Healthcare 2025, 13(2), 52. Available online: https://www.mdpi.com/2227-9032/13/2/196. [CrossRef]
- Carpallo-Porcar, B.; del Corral Beamonte, E.; Jiménez-Sánchez, C.; Córdova-Alegre, P.; Brandín-de la Cruz, N.; Calvo, S. Multimodal Telerehabilitation in Post COVID-19 Condition: A Series of 12 Cases. Preprints.org. 2025. Available online: https://www.preprints.org/manuscript/202503.0089/v1.
- León-Herrera, S.; Samper-Pardo, M.; Oliván-Blázquez, B.; Magallón-Botaya, R.; Casado-Vicente, V.; Sánchez-Recio, R.; Sánchez-Arizcuren, R. Effectiveness of ReCOVery APP to Improve the Quality of Life of Long COVID Patients: A 6-Month Follow-Up Randomized Clinical Trial. International Journal of Clinical Practice 2025, 7692776. [Google Scholar] [CrossRef]
- Sanal-Hayes, N. E. M.; Hayes, L. D.; Mair, J. L.; Dello Iacono, A.; Ingram, J.; Ormerod, J.; et al. A digital platform with activity tracking for energy management support in long COVID: A randomised controlled trial. SSRN. February 2025. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=5122498.
- Maccarone, Maria Chiara; Contessa, Paola; Passarotto, Edoardo; Regazzo, Gianluca; Masiero, & Stefano. Balance rehabilitation and Long Covid syndrome: effectiveness of thermal water treatment vs. home-based program. Frontiers in Rehabilitation Sciences 2025, 6, 1588940. Available online: https://www.frontiersin.org/journals/rehabilitation-sciences/articles/10.3389/fresc.2025.1588940. [CrossRef]
- McMullan, C.; Haroon, S.; Turner, G. M.; Aiyegbusi, O. L.; Hughes, S. E.; Flanagan, S.; et al. Mixed methods study of views and experience of non hospitalised individuals with long COVID of using pacing interventions. Scientific Reports 2025, 15(1), 14467. Available online: https://www.nature.com/articles/s41598-025-96319-6. [CrossRef]
- Gagnon, Christine; Vincent, Thomas; Bherer, Louis; Gayda, Mathieu; Cloutier, Simon-Olivier; Nozza, Anna; et al. Effects of supplemental oxygen on cognitive function and oxygen saturation in long COVID: An exploratory crossover study. PLOS ONE 2024, 19(11), e0295481. Available online: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0312735.
- Doehner, W.; Fischer, A.; Alimi, B.; Muhar, J.; Springer, J.; Altmann, C.; Schueller, P. O. Intermittent hypoxic–hyperoxic training during inpatient rehabilitation improves exercise capacity and functional outcome in patients with long COVID: Results of a controlled clinical pilot trial. Journal of Cachexia, Sarcopenia and Muscle. 19 November 2024. Available online: https://onlinelibrary.wiley.com/doi/full/10.1002/jcsm.13628.
- Kapel, J. S.; Stokholm, R.; Elmengaard, B.; Nochi, Z.; Olsen, R. J.; Foldager, C. B. Individualized algorithm-based intermittent hypoxia improves quality of life in patients suffering from long-term sequelae after COVID-19 infection. Journal of Clinical Medicine MDPI+1ResearchGate+1. 2025, 14(5), 1590. [Google Scholar] [CrossRef]
- Zilberman Itskovich, S.; Efrati, S.; et al. Hyperbaric oxygen therapy improves neurocognitive functions and symptoms of post COVID 19 condition: randomized controlled trial. Scientific Reports; Advance online publication, 12 July 2022. [CrossRef]
- Leitman, M.; Fuchs, S.; Tyomkin, V.; Hadanny, A.; Zilberman Itskovich, S.; Efrati, S. The effect of hyperbaric oxygen therapy on myocardial function in post COVID 19 syndrome patients: a randomized controlled trial. Scientific Reports 2023, 13, 9473. [Google Scholar] [CrossRef] [PubMed]
- Efrati, S.; et al. Long-term outcomes of hyperbaric oxygen therapy in post-COVID condition: longitudinal follow-up of a randomized controlled trial. In Scientific Reports; Advance online publication; 2024. [Google Scholar] [CrossRef]
- Philip, K. E. J.; Owles, H.; McVey, S.; Pagnuco, T.; Bruce, K.; Brunjes, H.; et al. An online breathing and wellbeing programme (ENO Breathe) for people with persistent symptoms following COVID-19: a parallel-group, single blind, randomized controlled trial. The Lancet Respiratory Medicine 2022, 10(9), 851–862. Available online: https://www.thelancet.com/journals/lanres/article/PIIS2213-2600(22)00125-4/fulltext.
- del Corral, T.; Fabero-Garrido, R.; Plaza Manzano, G.; Fernández de las Peñas, C.; Navarro Santana, M. J.; López de Uralde Villanueva, I. Minimal clinically important differences in inspiratory muscle function variables after a respiratory muscle training programme in individuals with long term post COVID 19 symptoms. Journal of Clinical Medicine 2023, 12(7), Article 2720. Available online: https://www.mdpi.com/2077-0383/12/7/2720. [PubMed]
- Lee, Y. J. Thoracic mobilization and respiratory muscle endurance training improve diaphragm thickness and respiratory function in patients with a history of COVID-19. Medicina 2023, 59(5), 906. Available online: https://pubmed.ncbi.nlm.nih.gov/37241138/. [CrossRef]
- Muñoz-Cofré, Rodrigo; del Valle, María Fernanda; Marzuca-Nassr, Gabriel Nasri; Valenzuela, Jorge; del Sol, Mariano; Díaz Canales, Constanza. A pulmonary rehabilitation program is an effective strategy to improve forced vital capacity, muscle strength and functional exercise capacity similarly in adults and older people with post severe COVID 19 who required mechanical ventilation. Research Square (preprint). 2024. Available online: https://www.researchgate.net/publication/379570590_A_pulmonary_rehabilitation_program_is_an_effective_strategy_to_improve_forced_vital_capacity_muscle_strength_and_functional_exercise_capacity_similarly_in_adults_and_older_people_with_post-severe_COVI.
- Abo Elyazed, Tamer I.; Alsharawy, Laila A.; Salem, Shaimaa E.; Helmy, Nesma A.; Abd El Hakim, Ahmed Abd El Moneim. Effect of home based pulmonary rehabilitation on exercise capacity in post COVID 19 patients: a randomized controlled trial. Journal of NeuroEngineering and Rehabilitation 2024, 21(1), 40. Available online: https://jneuroengrehab.biomedcentral.com/articles/10.1186/s12984-024-01340-x.
- Mauro, Marcella; Zulian, Elisa; Bestiaco, Nicoletta; Polano, Maurizio; Larese Filon, Francesca. Slow paced breathing intervention in healthcare workers affected by Long COVID: Effects on systemic and dysfunctional breathing symptoms, manual dexterity and HRV. Biomedicines 2024, 12(10), 2254. Available online: https://www.mdpi.com/2227-9059/12/10/2254. [CrossRef]
- Parisi, M. C.; Di Corrado, D.; Mingrino, O.; Crescimanno, C.; Longo, F.; Pegreffi, F.; Francavilla, V. C. SpiroTiger and KS Brief Stimulator: specific devices for breathing and well being in post COVID 19 patients. Journal of Functional Morphology and Kinesiology 2024, 9(4), 203. Available online: https://www.mdpi.com/2411-5142/9/4/203. [CrossRef]
- Muñoz Cofré, R.; del Valle, M. F.; Marzuca Nassr, G. N.; Valenzuela, J.; del Sol, M.; Canales, C. D.; et al. A pulmonary rehabilitation program is an effective strategy to improve forced vital capacity, muscle strength, and functional exercise capacity similarly in adults and older people with post severe COVID 19 who required mechanical ventilation. BMC Geriatrics 2024, 24(1), 313. Available online: https://bmcgeriatr.biomedcentral.com/articles/10.1186/s12877-024-04910-9.
- Páez Mora, C. D.; Zona, D. C.; Angarita Sierra, T.; Rojas Paredes, M. E.; Cano Trejos, D. Changes in lung function and dyspnea perception in Colombian COVID 19 patients after a 12 week pulmonary rehabilitation program. PLOS One 2024, 19(11), e0300826. Available online: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0300826. [CrossRef]
- Brandão Rangel, M. A. R.; Brill, B.; Furtado, G. E.; Freitas Rolim, C. C. L.; Silva Reis, A.; Souza Palmeira, V. H.; et al. Exercise driven comprehensive recovery: pulmonary rehabilitation’s impact on lung function, mechanics, and immune response in post COVID 19 patients. Infectious Diseases Reports 2025, 17(1), 1–16. Available online: https://www.mdpi.com/2036-7449/17/1/1. [CrossRef]
- Rohini, P; Saravanan, A; Maheshkumar, K; ThamaraiSelvi, K; Kalyani Praba, P; Prabhu, V. Effects of Bhramari and Sheetali pranayama on cardio-respiratory function in post COVID 19 patients: a randomized controlled study. Annals of Neurosciences 2025, 32(1), e220432. Available online: https://pubmed.ncbi.nlm.nih.gov/39810825/.
- Casciaro, M.; Di Micco, P.; Tonacci, A.; Vatrano, M.; Russo, V.; Siniscalchi, C. Non invasive ventilation improves lung function and exercise capacity in adults after COVID 19 infection. Clinical Practice 2025, 15(4), Article 72. Available online: https://www.mdpi.com/2039-7283/15/4/72. [CrossRef]
- Promsrisuk, T.; Srithawong, A.; Kongsui, R.; Sriraksa, N.; Thongrong, S.; Kloypan, C.; Muangritdech, N.; Khunkitti, K.; Thanawat, T.; Chachvarat, P. Therapeutic effects of slow deep breathing on cardiopulmonary function, physical performance, biochemical parameters, and stress in older adult patients with Long COVID in Phayao, Thailand. Annals of Geriatric Medicine and Research 2025, 29(2), 240–253. Available online: https://www.e-agmr.org/journal/view.php?doi=10.4235/agmr.24.0175. [CrossRef] [PubMed]
- Kuut, T. A.; Müller, F.; Csorba, I.; Braamse, A. M. J.; Nieuwkerk, P.; Rovers, C. P.; Knoop, H. Efficacy of cognitive behavioral therapy targeting severe fatigue following COVID 19: results of a randomized controlled trial. Clinical Infectious Diseases 2023, 77(5), 687–695. Available online: https://pubmed.ncbi.nlm.nih.gov/37155736/. [CrossRef] [PubMed]
- Nerli, T.F.; Selvakumar, J.; Cvejic, E.; Heier, I.; Pedersen, M.; Johnsen, T.L.; Wyller, V.B. Brief outpatient rehabilitation program for post–COVID 19 condition: A randomized clinical trial. JAMA Network Open 2024, 7(12), e2450744. Available online: https://pubmed.ncbi.nlm.nih.gov/39699896/. [CrossRef]
- Aghaei, A.; Qiao, S.; Tam, C.C.; Li, X. Role of self-esteem and personal mastery on the association between social support and resilience among COVID 19 long haulers. Heliyon 2024, 10(10), e31328. Available online: https://pubmed.ncbi.nlm.nih.gov/38818142/. [PubMed]
- Ovejero, D.; Ribes, A.; Villar García, J.; Trenchs Rodriguez, M.; López, D.; et al. Balneotherapy for the treatment of post COVID syndrome: a randomized controlled trial. BMC Complementary Medicine and Therapies 2025, 25, Article 37. Available online: https://pubmed.ncbi.nlm.nih.gov/39905419/. [CrossRef]
- Ferrara, E.; Scaramuzzino, M.; Murmura, G.; D’Addazio, G.; Sinjari, B. Emerging evidence on balneotherapy and thermal interventions in post COVID 19 syndrome: A systematic review. Healthcare 2025, 13(2), 96. Available online: https://www.mdpi.com/2227-9032/13/2/96. [CrossRef] [PubMed]
- Garbsch, R.; Kotewitsch, M.; Schäfer, H.; Teschler, M.; Mooren, F. C.; Schmitz, B. Use of speleotherapy in patients with post-COVID-19 syndrome: A prospective interrupted time-series analysis. Frontiers in Medicine 2025, 12, 1566235. Available online: https://www.frontiersin.org/journals/medicine/articles/10.3389/fmed.2025.1566235. [CrossRef]
- Fornazieri, M. A.; Cunha, B. M.; Nicácio, S. P.; Anzolin, L. K.; da Silva, J. L. B.; Fernandes Neto, A.; Brandão Neto, D.; Voegels, R. L.; Pinna, F. D. R. Effect of drug therapies on self reported chemosensory outcomes after COVID 19. World Journal of Otorhinolaryngology – Head & Neck Surgery 2024, 10(2), 88–96. Available online: https://onlinelibrary.wiley.com/doi/full/10.1002/wjo2.183.
- Pretorius, E.; Venter, C.; Laubscher, G.; Kell, D. B.; et al. Treatment of Long COVID symptoms with triple anticoagulant therapy: Dual antiplatelet therapy (clopidogrel + aspirin) and apixaban resolved persistent symptoms by reducing microclot burden and platelet hyperactivation. Research Square (Preprint). March 2023. Available online: https://www.researchgate.net/publication/369427800_Treatment_of_Long_COVID_symptoms_with_triple_anticoagulant_therapy.
- Pretorius, E.; Venter, C.; Laubscher, G.; Kell, D. B.; et al. Prevalence of symptoms, comorbidities, fibrin amyloid microclots, and platelet pathology in Long COVID/PASC patients: Evidence from 845 registry participants and 70 plasma samples. Cardiovascular Diabetology 2021, 21, Article 123. Available online: https://cardiab.biomedcentral.com/articles/10.1186/s12933-022-01579-5.
- Nutma, Idelette; Rus, Carla; Kooij, J. J. Sandra; de Vries, Bert; de Vries, Ingmar E.J. Treatment and outcomes of 95 post-Covid patients with an antidepressant and neurobiological explanations. 2023. Available online: https://www.researchgate.net/publication/372334231_Treatment_and_outcomes_of_95_post-Covid_patients_with_an_antidepressant_and_neurobiological_explanations.
- Treatment of 95 post-Covid patients with SSRIs: exploratory questionnaire study of post-COVID syndrome patients. Nature. November 2023. Available online: https://pubmed.ncbi.nlm.nih.gov/37919310/.
- Bradley, J; Tang, F; Tosi, DM; Resendes, N; Hammel, IS. The Effects of SSRIs and Antipsychotics on Long COVID Development in a Large Veteran Population. SSRN. July 2024. Available online: https://papers.ssrn.com/sol3/Delivery.cfm/fa6f16d8-9827-405b-ad12-1041d0a79608-MECA.pdf.
- Davis, L. L.; Behl, S.; Lee, D.; Zeng, H.; Skubiak, T.; Weaver, S.; et al. Brexpiprazole and sertraline for the treatment of posttraumatic stress disorder: A randomized clinical trial. JAMA 2024, 332(21), 2144–2154. Available online: https://jamanetwork.com/journals/jamapsychiatry/fullarticle/2827796.
- Gueck, T.; Jerg-Bretzke, L.; Wilke, J.; Gantner, J.; Walter, M.; Krisam, J. Course and potential predictors of post-COVID syndrome: A retrospective study of SARS-CoV-2-infected individuals. Frontiers in Immunology 2023, 14, 1226622. [Google Scholar] [CrossRef]
- Fiedler, L.; Motloch, L. J.; Dieplinger, A. M.; Jirak, P.; Davtyan, P.; Gareeva, D.; Badykova, E.; Badykov, M.; Lakman, I.; Agapitov, A.; Sadikova, L.; Pavlov, V.; Föttinger, F.; Mirna, M.; Kopp, K.; Hoppe, U. C.; Pistulli, R.; Cai, B.; Yang, B.; Zagidullin, N. Prophylactic rivaroxaban in the early post-discharge period reduces hospitalization for atrial fibrillation and incidence of sudden cardiac death during 12-month follow-up in hospitalized COVID 19 survivors. Frontiers in Pharmacology 2023, 14, Article 1093396. Available online: https://www.frontiersin.org/articles/10.3389/fphar.2023.1093396/full.
- Wahid, L.; Hade, E. M.; Cushman, M.; Gong, M. N.; Renard, V.; Ko, E. R.; et al. P2Y12 inhibitors and quality of life outcomes in critically ill patients hospitalized for COVID 19: A pre specified secondary analysis of the ACTIV 4a randomized clinical trial. Circulation 2023, 148 (Suppl_1). Available online: https://scholars.duke.edu/individual/pub1614093. [CrossRef]
- Сlinical Trial of Efficacy and Safety of Prospekta in the Treatment of Post-COVID-19 Asthenia. 2023. Available online: https://pubmed.ncbi.nlm.nih.gov/39599626/.
- Ohmagari, N.; Yotsuyanagi, H.; Doi, Y.; Yamato, M.; Imamura, T.; Sakaguchi, H.; Yamanaka, H.; Imaoka, R.; Fukushi, A.; Ichihashi, G.; Sanaki, T.; Tsuge, Y.; Uehara, T.; Mukae, H. Efficacy and safety of ensitrelvir for asymptomatic or mild COVID 19: An exploratory phase 2b/3 multicenter randomized clinical trial. Influenza and Other Respiratory Viruses 2024, 18(6), e13338. Available online: https://onlinelibrary.wiley.com/doi/10.1111/irv.1333.
- Li, X.; Wu, L.; Sun, S.; Dong, H.; Luo, J. Association between electrolyte supplementation and cardiac injury in Long COVID 19: A retrospective cohort study. Frontiers in Cardiovascular Medicine. 8 March 2025. Available online: https://www.s4me.info/threads/association-between-electrolyte-supplementation-and-cardiac-injury-in-long-covid-19.43008/.
- Li, X.; Wu, L.; Sun, S.; Dong, H.; Luo, J. Association between electrolyte supplementation and cardiac injury in Long COVID 19: A retrospective cohort study. Frontiers in Cardiovascular Medicine. 8 March 2025. Available online: https://www.s4me.info/threads/association-between-electrolyte-supplementation-and-cardiac-injury-in-long-covid-19.43008/.
- Fornazieri, M. A.; Cunha, B. M.; Nicácio, S. P.; Anzolin, L. K.; da Silva, J. L. B.; Fernandes Neto, A.; Brandão Neto, D.; Voegels, R. L.; Pinna, F. D. R. Effect of drug therapies on self reported chemosensory outcomes after COVID 19. World Journal of Otorhinolaryngology – Head & Neck Surgery 2024, 10(2), 88–96. Available online: https://pubmed.ncbi.nlm.nih.gov/38855284/.
- Kazal, Louis A, Jr.; Huyck, Karen L; Kelly, Brendan. Classical Chinese Medicine (CCM) for Long COVID: Case series and treatment rationale. Encinitas. 2025. Available online: https://pubmed.ncbi.nlm.nih.gov/40171061/.
- Wang, Yiting; Li, Xiao; Hui, Huaizheng; Yang, Dianxing. Efficacy and safety of traditional Chinese medicine for post-COVID-19 syndrome: a systematic review and meta-analysis. Journal of Translational Medicine. 2025. Available online: https://pmc.ncbi.nlm.nih.gov/articles/PMC12269130/.
- Tonix Pharmaceuticals. Tonix Pharmaceuticals announces highly statistically significant and clinically meaningful topline results in second positive Phase 3 clinical trial of TNX-102 SL for fibromyalgia. Press release. 20 December 2023. Available online: https://ir.tonixpharma.com/news-events/press-releases/detail/1443/tonix-pharmaceuticals-announces-highly-statistically.
- Lau, R. I.; Su, Q.; Lau, I. S. F.; Ching, J. Y. L.; Wong, M. C. S.; Lau. A synbiotic preparation (SIM01) for post acute COVID 19 syndrome in Hong Kong (RECOVERY): A randomised, double blind, placebo controlled trial. The Lancet Infectious Diseases 2024, 24(3), 256–265. Available online: https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(23)00685-0/fulltext.
- Leitzke, M. Is the post COVID 19 syndrome a severe impairment of acetylcholine orchestrated neuromodulation that responds to nicotine administration? Bioelectronic Medicine. 2023. Available online: https://bioelecmed.biomedcentral.com/articles/10.1186/s42234-023-00104-7.
- Grady, Connor B; Bhattacharjee, Bornali; Silva, Julio; Jaycox, Jillian; Lee, Lik Wee; Monteiro, Valter Silva. Impact of COVID-19 vaccination on symptoms and immune phenotypes in vaccine-naïve individuals with Long COVID. Nature. 2025. Available online: https://www.nature.com/articles/s43856-025-00829-3.
- Currie, Crawford; Myklebust, Tor Age; Bjerknes, Christian Bomi. FramroxeAssessing the Potential of an Enzymatically Liberated Salmon Oil to Support Immune Health Recovery from Acute SARS-CoV-2 Infection via Change in the Expression of Cytokine, Chemokine and Interferon-Related Genes. International Journal of Molecular Sciences 2024, 25(13). Available online: https://www.mdpi.com/1422-0067/25/13/6917.
- Mørk, T. Å.; Blomhoff, C.; Fredriksen, B.; Cuda, C.; Kiecolt Glaser, D. A.; Wilson, M. C.; et al. Assessing the potential of an enzymatically liberated salmon oil for immunomodulation in adults with mild to moderate COVID 19: A pilot randomized controlled trial. International Journal of Molecular Sciences 2024, 25(13), 691. Available online: https://www.mdpi.com/1422-0067/25/13/6917.
- Suárez-Moreno, Nuria; Gómez-Sánchez, Leticia; Navarro-Caceres, Alicia; Arroyo-Romero, Silvia; Domínguez-Martín, Andrea; Lugones-Sánchez, Cristina. Association of Mediterranean Diet with Cardiovascular Risk Factors and with Metabolic Syndrome in Subjects with Long COVID: BioICOPER Study Nutrients. 2025. Available online: https://pubmed.ncbi.nlm.nih.gov/40004984/.
- Ghosh, S.; Chakraborty, S.; Ghosh, S.; Das, S.; Das, R.; Bhattacharya, A. An open-label randomized controlled trial to evaluate the effectiveness of homeopathic treatment in the management of post-COVID syndrome. Complementary Therapies in Clinical Practice 2022, 48, 101569. [Google Scholar] [CrossRef]
- Takács, M.; Frass, M.; Pohl Schickinger, A.; Fibert, P.; Lechleitner, P.; Oberbaum, M.; Leisser, I.; Panhofer, P.; Chandak, K.; Weiermayer, P. Use of homeopathy in patients suffering from Long COVID 19 (LONGCOVIHOM): A case series. OBM Integrative and Complementary Medicine 2024, 9(3), 045. Available online: https://www.lidsen.com/journals/icm/icm-09-03-045.
- Combet, E.; Haag, L.; Richardson, J.; Haig, C. E.; et al. Remotely delivered weight management for people with long COVID and overweight: the randomized wait list controlled ReDIRECT trial. Nature Medicine 2025, 31(1), 258–266. [Google Scholar] [CrossRef] [PubMed]
- Bhargav, H.; Raghavan, V.; Rao, N. P.; Gulati, K.; Binumon, K. V.; Anu, K. N.; Ravi, S.; Jasti, N.; Holla, B.; Varambally, S.; Ramachandran, P. Validation and efficacy of a tele yoga intervention for improving psychological stress, mental health and sleep difficulties of stressed adults diagnosed with long COVID: A prospective, multi center, open label single arm study. Frontiers in Psychology 2024, 15, 1436691. Available online: https://pubmed.ncbi.nlm.nih.gov/39569098/. [CrossRef]
- Cheshire, A.; Cartwright, T. Perceptions, acceptability and experiences of yoga to support long COVID: A survey of people living with long COVID. BMC Complementary Medicine and Therapies 2025, 25, 123. Available online: https://www.researchgate.net/publication/393046575_Perceptions_acceptability_and_experiences_of_yoga_to_support_long-COVID_A_survey_of_people_living_with_long-COVID.
- Liang, R.; Tang, L.; Li, L.; Zhao, N.; Yu, X.; Li, J.; et al. The effect of pressing needle therapy on depression, anxiety, and sleep for patients in convalescence from COVID 19. Frontiers in Neurology 2024, 15, Article 1481557. Available online: https://www.frontiersin.org/journals/neurology/articles/10.3389/fneur.2024.1481557. [CrossRef]
- Watanabe, S.; Sakurai, T.; Kanaya, T.; Iwasaki, T.; Oshima, H.; Furukawa, T.; Yoshikawa, T.; Nakahashi, S. Impact of frailty on the duration and type of speech-language-hearing therapy for patients with COVID 19. Cureus 2025, 17(4), e81976. Available online: https://www.cureus.com/articles/353998-impact-of-frailty-on-the-duration-and-type-of-speech-language-hearing-therapy-for-patients-with-covid-19. [CrossRef] [PubMed]
- Delgado Lima, A. H.; Bouhaben, J.; Delgado Losada, M. L. Maximizing participation in olfactory training in a sample with post COVID 19 olfactory loss. Brain Sciences 2024, 14(7), 730. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11274705/. [CrossRef]
- Akbarpour, M. H.; Zandi, M.; Sedighi, L.; Ghanbari Ghalesar, M. Evaluating the effect of olfactory training on improving the sense of smell in patients with COVID 19 with olfactory disorders: A randomized clinical trial study. BMC Health and Quality of Life Outcomes 2023, 21(1), 215. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9510568/.
- Pendolino, A. L.; Scarpa, B.; Andrews, P. J. The effectiveness of functional septorhinoplasty in improving COVID 19-related olfactory dysfunction: a prospective controlled study. Facial Plastic Surgery 2025, 41(1), 1–9. Available online: https://pubmed.ncbi.nlm.nih.gov/39929248/.
- Serrano, Thiago L. I.; Antonio, Marcelo A.; Giacomin, Lorena T.; et al. Effect of olfactory training with essential versus odor free placebo oils in COVID 19 induced smell loss: A randomized controlled trial. The Laryngoscope 2025, 135(5), 325–333. Available online: https://pubmed.ncbi.nlm.nih.gov/40371997.
- Paranhos, A. C. M.; Dias, A. R. N.; Koury, G. V. H.; Domingues, M. M.; dos Santos, L. P. M.; da Silva, L. M.; Oliveira, F. L. R. V.; Lima, W. T. A.; Quaresma, J.; Magno Falcão, L. F.; Souza, G. S. Olfactory Training in Long COVID: A Randomized Clinical Trial. SSRN. 26 March 2025. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=5186634.
- Mogensen, D. G.; Aanaes, K.; Andersen, I. B.; Jarden, M. Effect of olfactory training in COVID 19-related olfactory dysfunction: a randomized placebo-controlled trial. The Laryngoscope 2025, 135(5), 325–333. Available online: https://pubmed.ncbi.nlm.nih.gov/40371997/.
- Blagova, O. V.; Lutokhina, Y.; Savina, P.; Kogan, E. Corticosteroids are effective in the treatment of virus positive post COVID myoendocarditis with high autoimmune activity. Clinical Cardiology 2023, 46(1), 52–59. [Google Scholar] [CrossRef]
- Milne, A.; Maskell, S.; Sharp, C. & the COVID Symptom Study Consortium. Impact of dexamethasone on persistent symptoms of COVID 19: An observational study. medRxiv 2021. [Google Scholar] [CrossRef]
- Li, Y.-Q.; Wu, M.; Wang, Y.-J.; Zhang, Y.-X.; Lu, J.; Zhao, Y.-N.; Ji, B.-F.; Chen, Z.-Q.; Tang, R.-N.; Liu, B.-C. The analysis of low dose glucocorticoid maintenance therapy in patients with primary nephrotic syndrome suffering from COVID 19. Frontiers in Molecular Biosciences 2024, 10, 1326111. Available online: https://www.frontiersin.org/journals/molecular-biosciences/articles/10.3389/fmolb.2023.1326111/full. [CrossRef]
- Xie, P.-P.; Zhang, Y.; Niu, W.-K.; Tu, B.; Yang, N.; Fang, Y.; Shi, Y.-H.; Wang, F.-S.; Yuan, X. Clinical characteristics and effects of inhaled corticosteroid in patients with post COVID 19 chronic cough during the Omicron variant outbreak. BMC Pulmonary Medicine 2024, 24(1), 156. Available online: https://bmcpulmmed.biomedcentral.com/articles/10.1186/s12890-024-02937-7.
- Giannakopoulos, S.; Pak, J.-H.; Bakse, J.; Ward, M. A.; Nerurkar, V. R.; Tallquist, M. D.; Verma, S. SARS CoV 2 induced cytokine storm drives prolonged testicular injury and functional impairments in mice that are mitigated by dexamethasone. SSRN 2024. [Google Scholar] [CrossRef]
- Wan, A.T.H.; Teopiz, C.M.; West, J.; McIntyre, R.S. The impact of cognitive function on health related quality of life in persons with post COVID 19 condition and the moderating role of vortioxetine: A randomized controlled trial. medRxiv. 18 March 2024. Available online: https://www.medrxiv.org/content/10.1101/2024.03.18.24304375v1.
- Nakamura, K.; Kondo, K.; Oka, N.; Yamakawa, K.; Ie, K.; Goto, T.; Fujitani, S. Donepezil for fatigue and psychological symptoms in post–COVID 19 condition: A randomized clinical trial. JAMA Network Open 2025, 8(3), e250728. Available online: https://pubmed.ncbi.nlm.nih.gov/40094666/. [PubMed]
- Fakhrolmobasheri, Mohammad; Hosseini, Mahnaz-Sadat; Shahrokh, Seyedeh-Ghazal; Mohammadi, Zahra; Kahlani, Mohammad-Javad; Majidi, Seyed-Erfan; et al. Coenzyme Q10 and Its Therapeutic Potencies Against COVID 19: A Molecular Review. Advanced Pharmaceutical Bulletin 2023, 13(2), 235–244. Available online: https://pubmed.ncbi.nlm.nih.gov/37342382/.
- Hansen, K. S.; Mogensen, T. H.; Agergaard, J.; Schiøttz Christensen, B.; Østergaard, L.; Vibholm, L. K.; et al. High dose coenzyme Q10 therapy versus placebo in patients with post COVID 19 condition: A randomized, phase 2, crossover trial. The Lancet Regional Health – Europe 2023, 24, 100539. [Google Scholar] [CrossRef]
- Barletta, M. A.; Marino, G.; Spagnolo, B.; Bianchi, F. P.; Falappone, P. C. F.; Spagnolo, L.; Gatti, P. Coenzyme Q10 + alpha lipoic acid for chronic COVID syndrome. Clinical and Experimental Medicine 2023, 23(3), 667–678. [Google Scholar] [CrossRef]
- Hansen, K. S.; Mogensen, T. H.; Agergaard, J.; Schiøttz Christensen, B.; Østergaard, L.; Vibholm, L. K.; et al. High-dose coenzyme Q10 therapy versus placebo in patients with post COVID 19 condition: A randomized, phase 2, crossover trial. The Lancet Regional Health – Europe 2022, 24, 100539. [Google Scholar] [CrossRef]
- Andrews, JS; Boonyaratanakornkit, JB; Krusinska, E; Allen, S; Posada, JA. Assessment of the Impact of RNase in Patients With Severe Fatigue Related to PASC: A Randomized Phase 2 Trial (RSLV-132). Clinincal Infectious Diseases 2025, 79(3), 635–642. Available online: https://academic.oup.com/cid/article/79/3/635/7668392?login=false.
- Kulkarni, Tejaswini; Santiaguel, Joel; Aul, Raminder; Harnett, Mark; Krop, Julie; Chen, Michael C. double-blind RCT; antifibrotic deupirfenidone in PASC with respiratory involvement. ERJ Open Research. 2025. Available online: https://publications.ersnet.org/content/erjor/11/4/01142-2024.
- Shi, L.; Huang, H.; Lu, X.; Yan, X.; Jiang, X.; Xu, R.; et al. Long-Term Effects of Human Umbilical Cord-Derived Mesenchymal Stem Cells in Patients with Moderate to Severe COVID-19 Lung Damage: A Randomized, Double-Blind, Placebo-Controlled Phase 2 Trial. Biomedicines 2021, 9(12), 1802. [Google Scholar] [CrossRef]
- Yuan, Meng-Qi; Song, Le; Wang, Ze-Rui; Zhang, Zi-Ying; Shi, Ming; He, Junli; Mo, Qiong. Long-term outcomes of mesenchymal stem cell therapy in severe COVID-19 patients: 3-year follow-up of a randomized, double-blind, placebo-controlled trial. BMC Stem Cell Research & Therapy. 2025. Available online: https://stemcellres.biomedcentral.com/articles/10.1186/s13287-025-04148-1.
- Jing, F.; Wang, W.; Ke, J.; Huang, T.; Jiang, B.; Qiu, Q.; et al. Fuzheng Huayu tablets for treating pulmonary fibrosis in post COVID 19 patients: A multicenter, randomized, double blind, placebo controlled trial. Frontiers in Pharmacology 2025, 16, 1508276. Available online: https://www.frontiersin.org/articles/10.3389/fphar.2025.1508276/full.
- GeNeuro, SA. Top-line Phase 2 results of GNC 501 (temelimab) in post COVID neuropsychiatric syndromes show no clinically meaningful benefit. GeNeuro Press Release. 28 June 2024. Available online: https://geneuro.ch/en/geneuro-news/geneuro-announces-the-results-of-the-gnc-501-in-post-covid-19-syndrome/.
- Chi, H.; Xing, Y.; Chen, Y.; Wang, T.; Qi, J.; Jia, X.; et al. A subgroup reanalysis of the efficacy of Bufei Huoxue capsules in patients with long COVID 19. Pulmonary Circulation 2025. [Google Scholar] [CrossRef]
- Gonda, K.; Hai, T.; Suzuki, K.; Ozaki, A.; Shibusa, T.; Takenoshita, S.; Maejima, Y.; Shimomura, K. Effect of Ficus pumila L. on improving insulin secretory capacity and insulin resistance in elderly patients aged 80 years or older who developed diabetes after COVID 19 infection. Nutrients 2025, 17(2), 290. Available online: https://www.mdpi.com/2072-6643/17/2/290. [CrossRef]
- Efficacy of Apportal® nutritional supplement in reducing post COVID fatigue: A study of 232 patients. Restorative Neurology and Neuroscience. 2021. Available online: https://pubmed.ncbi.nlm.nih.gov/34857243/.
- Atieh, O.; Daher, J.; Durieux, J. C.; Abboud, M.; Labbato, D.; Baissary, J.; et al. Vitamins K2 and D3 improve long COVID, fungal translocation, and inflammation: Randomized controlled trial. Nutrients 2025, 17(2), 304. [Google Scholar] [CrossRef]
- Kopp, J.; Kuenzi, L.; Rueegg, S.; Braun, J.; Rasi, M.; Anagnostopoulos, A.; Puhan, M. A.; Fehr, J. S.; Radtke, T. Effects of Pycnogenol® in post COVID 19 condition (PYCNOVID): A single center, placebo controlled, quadruple blind, randomized trial. medRxiv. 12 June 2025. Available online: https://www.medrxiv.org/content/10.1101/2025.06.12.25329489v1.
- Noce, A.; Marrone, G.; Di Lauro, M.; Vita, C.; Montalto, G.; Giorgino, G.; et al. Potential anti inflammatory and anti fatigue effects of an oral food supplement in long COVID patients. Pharmaceutics 2024, 17(4), 463. Available online: https://pubmed.ncbi.nlm.nih.gov/38675423/. [CrossRef]
- Lau, R. I.; Su, Q.; Ching, J. Y. L.; Cheong, P. K.; Chan, F. K. L.; Ng, S. C. Fecal microbiota transplantation for sleep disturbance in post acute COVID 19 syndrome. Clinical Gastroenterology and Hepatology 2024, 22(12), 2487–2496.e6. Available online: https://www.cghjournal.org/article/S1542-3565(24)00542-1/fulltext. [CrossRef] [PubMed]
- Fox, J.; Ali, F.; Lopez, M.; Shah, S. A.; Schmidt, C. W.; Quesada, O.; et al. Enhanced external counterpulsation improves dyspnea, fatigue, and functional capacity in patients with long COVID. COVID 2024, 4(9), 1379–1385. Available online: https://www.mdpi.com/2673-8112/4/9/98. [CrossRef]
- Gerasimenko, A.; Ovechkin, A.; Moshonkina, T.; Shamantseva, N.; Lyakhovetskii, V.; Suthar, A. Spinal Neuromodulation for Respiratory Rehabilitation in Patients with Post Acute COVID 19 Syndrome. Life 2024, 14(11), 1518. [Google Scholar] [CrossRef]
- Victoria, L. W.; Oberlin, L. E.; Ilieva, I. P.; Jaywant, A.; Kanellopoulos, D.; Mercaldi, C.; et al. A digital intervention for cognitive deficits following COVID 19: a randomized clinical trial. Neuropsychopharmacology 2024, 49(12), 1520–1531. Available online: https://pubmed.ncbi.nlm.nih.gov/39358543/. [CrossRef] [PubMed]
- Martínez-Borba, Verónica; Peris-Baquero, Óscar; Prieto-Rollán, Iván; Osma, Jorge; del Corral-Beamonte, Esther. Preliminary feasibility and clinical utility of the Unified Protocol for the transdiagnostic treatment of emotional disorders in people with long COVID-19 condition: A single case pilot study PLOS One. 2025. Available online: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0329595.
- Hurt, R. T.; Ganesh, R.; Schroeder, D. R.; Hanson, J. L.; Fokken, S. C.; Overgaard, J. D.; et al. Using a wearable brain activity sensing device in the treatment of long COVID symptoms in an open label clinical trial. Journal of Primary Care & Community Health 2025, 16. Available online: https://journals.sagepub.com/doi/full/10.1177/21501319251325639. [CrossRef]
- Hawkins, J.; Hires, C.; Keenan, L.; Dunne, E. Aromatherapy blend of thyme, orange, clove bud, and frankincense boosts energy levels in post-COVID-19 female patients: A randomized, double-blinded, placebo controlled clinical trial. Complementary Therapeutic Medicine. 2022. Available online: https://pmc.ncbi.nlm.nih.gov/articles/PMC8949693/.
- Chavda, V. P.; Balar, P. C.; Jogi, G.; Marwadi, S.; Patel, A.; Doshi, A.; et al. The potential role of essential oils in boosting immunity and easing COVID-19 symptoms. Clinical Traditional Medicine and Pharmacology. 2024. Available online: https://www.sciencedirect.com/science/article/pii/S2097382924000064.
- Shah, S. A.; Varanasi, S.; Sathyamoorthy, M.; Teal, A.; Verduzco-Gutierrez, M.; Cabrera, J. Enhanced external counterpulsation offers potential treatment option for Long COVID patients. American College of Cardiology Press Release. 14 February 2022. Available online: https://www.acc.org/About-ACC/Press-Releases/2022/02/14/14/25/Enhanced-External-Counterpulsation-Offers-Potential-Treatment-Option-for-Long-COVID-Patients.
- Stein, E.; Heindrich, C.; Wittke, K.; Kedor, C.; Kim, L.; Freitag, H.; et al. Observational Study of Repeat Immunoadsorption (RIA) in Post COVID ME/CFS Patients with Elevated β₂ Adrenergic Receptor Autoantibodies—An Interim Report. Journal of Clinical Medicine 2023, 12(19), 6428. [Google Scholar] [CrossRef] [PubMed]
- Badran, B. W.; Huffman, S.; Dancy, M.; Austelle, C. W. A pilot randomized controlled trial of supervised, at-home, self-administered transcutaneous auricular vagus nerve stimulation (taVNS) to manage long COVID symptoms. Research Square. 2022. Available online: https://www.researchgate.net/publication/362914906.
- Natelson, B. H.; Blate, M.; Soto, T. Transcutaneous Vagus Nerve Stimulation in the Treatment of Long Covid-Chronic Fatigue Syndrome. medRxiv. 2022. Available online: https://www.medrxiv.org/content/10.1101/2022.11.08.22281807v1.
- Zheng, Z. S.; Simonian, N.; Wang, J.; Rosario, E. R. Transcutaneous vagus nerve stimulation improves Long COVID symptoms in a female cohort: A pilot study. Frontiers in Neurology 2024, 15, 1393371. Available online: https://pubmed.ncbi.nlm.nih.gov/38756213/. [CrossRef]
- Vestito, Lucilla; Ponzanoc, Marta; Moria, Laura; Trompettoa, Carlo; Bandini, Fabio J. F. A randomized controlled trial of anodal transcranial direct current stimulation (A-tDCS) and olfactory training in persistent COVID-19 anosmia Brain Stimulation. 2025. Available online: https://www.brainstimjrnl.com/article/S1935-861X(25)00104-4/fulltext.
- Zulbarán Rojas, A.; Bara, R.; Lee, M.; Najafi, B.; Myers, P. Transcutaneous electrical nerve stimulation for fibromyalgia like syndrome in patients with long COVID: A pilot randomized clinical trial. Scientific Reports 2024, 14(1), 27224. Available online: https://www.nature.com/articles/s41598-024-78651-5. [CrossRef]
- Sabel, B. A.; Zhou, W.; Huber, F.; Schmidt, F.; Sabel, K.; Gonschorek, A.; Bilc, M. Non invasive brain microcurrent stimulation therapy of Long COVID 19 reduces vascular dysregulation and improves visual and cognitive impairment: Two case studies. Restorative Neurology and Neuroscience 2021, 39(6), 393–408. Available online: https://pubmed.ncbi.nlm.nih.gov/34924406/. [CrossRef]
- Wang, Z.; Zhu, T.; Li, X.; Lai, X.; Chen, M. Tragus nerve stimulation attenuates postural orthostatic tachycardia syndrome in post COVID 19 infection: A randomized, double blind controlled trial. Clinical Cardiology 2025, 48(3), e70110. Available online: https://pubmed.ncbi.nlm.nih.gov/40014480. [CrossRef] [PubMed]
- Kikuchi, Takahisa; Hamano, Keisuke; Yamakawa, Mayu; Mimura, Yasuo; Tatebayashi, Yoshitaka; Maruyama, Chiaki. Repetitive transcranial magnetic stimulation ameliorated treatment-resistant depression with neuroinflammatory alterations secondary to COVID 19: a case report. Psychiatry Research and Clinical Practice 2024, 6(2), 123–130. Available online: https://link.springer.com/article/10.1007/s40501-021-00238-y.
- Cunha, A. C. R.; Silva, J. C.; Garcês, C. P.; Sisconeto, T. M.; Nascimento, J. L. R.; Amaral, A. L.; et al. Online and face-to-face Mat Pilates training for long COVID 19 patients: a randomized controlled trial on health outcomes. International Journal of Environmental Research and Public Health 2024, 21(10), 1385. Available online: https://pubmed.ncbi.nlm.nih.gov/39457358/. [CrossRef]
- Pereira, PC; de Lima, CJ; Villaverde, AB; Fernandes, AB; Zângaro, RA; et al. Photobiomodulation in the treatment of pulmonary fibrosis after COVID-19: a prospective study. Research Square (preprint). 25 November 2024. Available online: https://www.researchsquare.com/article/rs-5483003/v1.
- Campos, Mayra C. V.; Schuler, Silvana S. V.; Lacerda, Ana J.; Mazzoni, Adriana C.; Silva, Tamiris; Rosa, Francine C. S.; et al. Evaluation of vascular photobiomodulation for orofacial pain and tension-type headache following COVID 19 in a pragmatic randomized clinical trial. Scientific Reports 2024, 14(1), 31138. Available online: https://www.nature.com/articles/s41598-024-82412-9. [CrossRef] [PubMed]
- Najafi, B.; Zulbaran, A.; Lee, M.; Bara, R. O.; et al. Transcutaneous electrical nerve stimulation for fibromyalgia like syndrome in patients with Long COVID: a pilot randomized clinical trial. Nature Scientific Reports. 2024. Available online: https://www.nature.com/articles/s41598-024-78651-5.
- Chauhan, G.; Upadhyay, A.; Khanduja, S.; Emerick, T. Stellate ganglion block for anosmia and dysgeusia due to Long COVID. Cureus 2022, 14(8), e27779. Available online: https://pubmed.ncbi.nlm.nih.gov/36106285/. [CrossRef] [PubMed]
- Liu, L. D.; Duricka, D. L. Stellate ganglion block reduces symptoms of Long COVID: A case series. Journal of Neuroimmunology 2022, 362, 577784. Available online: https://pubmed.ncbi.nlm.nih.gov/34922127/. [CrossRef]
- Pearson, Lisa; Maina, Alfred; Compratt, Taylor; Harden, Sherri; Aaroe, Abbey; Copas, Whitney; Thompson, Leah R. Stellate Ganglion Block Relieves Long COVID-19 Symptoms in 86% of Patients: A Retrospective Cohort Study Cureus (2023). Available online: https://www.cureus.com/articles/184194-stellate-ganglion-block-relieves-long-covid-19-symptoms-in-86-of-patients-a-retrospective-cohort-study?fbclid=IwAR3Wo1cdeheoLLMCrM8ht2SvoxElieU44VIEmJy-LFA3shdbOcmKqmA22nw#!/metrics.
- Duricka, D.; Liu, L. Reduction of Long COVID symptoms after stellate ganglion block: A retrospective chart review study. Autonomic Neuroscience 2024, 254, 103195. Available online: https://www.sciencedirect.com/science/article/pii/S1566070224000493. [CrossRef]
- Singh, R.; Kumar, A.; Mehra, S.; Sharma, V.; Verma, P. Evaluation of usefulness of ropinirole in the treatment of post COVID 19 restless legs syndrome: A quasi experimental study. Journal of Pharmaceutical Negative Results 2022, 13, 2603–2606. Available online: https://www.pnrjournal.com/index.php/home/article/view/4336.
- Armstrong, M. F.; O’Byrne, T. J.; Calva, J. J.; Mallory, M. J.; Bublitz, S. E.; Do, A.; et al. The feasibility of investigating acupuncture in patients with COVID 19 related olfactory dysfunction: A pilot randomized study. Global Advances in Integrative Medicine and Health 2025, 14(9), 1–7. Available online: https://journals.sagepub.com/doi/abs/10.1177/27536130251343834. [CrossRef]
- Schäfer, S. K.; Rose, M.; Simon, J.; Petrie, K. J.; Löwe, B.; Laferton, J. A. C. Needs and wishes of patients with Long COVID regarding an expectation management intervention: A qualitative study to inform the SOMA.COV treatment manual. PLOS ONE 2025, 20(2), e0298211. Available online: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0317905.
- Philip, K. E. J.; Burton, A.; Lewis, A.; Buttery, S. C.; Williams, P. J.; Polkey, M. I.; et al. Participant experience of Scottish Ballet’s dance based long COVID support programme: a mixed methods study. medRxiv. October 2024. Available online: https://www.medrxiv.org/content/10.1101/2024.10.28.24316302v1.
- Yamaguchi, K; Saito, Y; Tanaka, H; et al. Aripiprazole for treating post-COVID-19 hypersomnolence in adolescents: A case series. Sleep 2025, 48 (Suppl 1), A365. Available online: https://academic.oup.com/sleep/article/48/Supplement_1/A365/8135331. [CrossRef]
- Krishnamurthy, V; et al. Effect of CPAP on cognitive fog in post-COVID patients with obstructive sleep apnea. Sleep 2025, 48 (Suppl 1), A606. Available online: https://academic.oup.com/sleep/article/48/Supplement_1/A606/8135174. [CrossRef]
- Chung, T. W.-H.; Zhang, H.; Wong, F. K.-C.; Sridhar, S.; Lee, T. M.-C.; Leung, G. K.-K.; et al. Short course oral vitamin A and aerosolised diffuser olfactory training for the treatment of smell loss in long COVID: A pilot study. Brain Sciences 2023, 13(7), 1014. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10377650/. [PubMed]
- Pendolino, A. L.; Scarpa, B.; Andrews, P. J. The effectiveness of functional septorhinoplasty in improving COVID 19 related olfactory dysfunction: Prospective controlled study. Facial Plastic Surgery. 24 February 2025. Available online: https://pubmed.ncbi.nlm.nih.gov/39929248/.
- Cano, N.; Casas, O.; Ariza, M.; Gelonch, O.; Plana, Y.; Porras Garcia, B.; Garolera, M. Effects of a multimodal immersive virtual reality intervention on heart rate variability in adults with post COVID 19 syndrome. Applied Sciences 2025, 15(8), 4111. Available online: https://www.mdpi.com/2076-3417/15/8/4111. [CrossRef]
- Melián Ortíz, A.; Zurdo Sayalero, E.; Perpiñá Martínez, S.; Delgado Lacosta, A.; Jiménez Antona, C.; Fernández Carnero, J.; Laguarta Val, S. Superficial neuromodulation in dysautonomia in women with post COVID 19 condition: A pilot study. Brain Sciences 2025, 15(5), 510. Available online: https://pubmed.ncbi.nlm.nih.gov/40426680/. [CrossRef] [PubMed]
- Loren, Claudia; Frankenberger, Roland. Oronasal drainage (OND): A novel treatment approach for Long COVID symptoms. Viruses. 2025. Available online: https://www.mdpi.com/1999-4915/17/2/210.
- Oesch Régeni, B.; Germann, N.; Hafer, G.; Schmid, D.; Arn, N. Effect on quality of life of therapeutic plasmapheresis in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome patients with elevated β adrenergic and M3 muscarinic receptor antibodies – a pilot study. Preprints.org. 2025. Available online: https://www.preprints.org/manuscript/202504.0228.
- Kamel, Tony; Toppen, William; Salahmand, Yasaman. Successful treatment of post coronavirus disease 2019 (COVID 19) autoimmune encephalitis with plasmapheresis after a failed trial of steroids. Cureus 2025, 17(5), e85150. Available online: https://www.cureus.com/articles/355250-successful-treatment-of-post-coronavirus-disease-2019-covid-19-autoimmune-encephalitis-with-plasmapheresis-after-a-failed-trial-of-steroid. [CrossRef] [PubMed]
- Willis, Gregory L.; Endo, Takuyuki; Sakoda, Saburo. Circadian re set repairs long COVID in a prodromal Parkinson’s parallel: a case series. Journal of Medical Case Reports 2024, 18(1), 496. Available online: https://jmedicalcasereports.biomedcentral.com/articles/10.1186/s13256-024-04812-9. [CrossRef]
- AbouAssaly, JR; Masuko, T; Sasai-Masuko, H; Strale, FJ, Jr. Neurofeedback for COVID-19 brain fog: a secondary analysis. Cureus 2025, 17(2), e79222. Available online: https://pubmed.ncbi.nlm.nih.gov/40115713/. [CrossRef]
- España-Cueto, S.; Loste, C.; Lladós, G.; López, C.; Santos, J. R.; Dulsat, G.; et al. Plasma exchange therapy for the post COVID 19 condition: A phase II, double blind, placebo controlled, randomized trial. Nature Communications 2025, 16(1), 1929 (2025). [Google Scholar] [CrossRef]
- Gaylis, N. B.; Ritter, A.; Kelly, S. A.; Pourhassan, N. Z.; Tiwary, M.; Sacha, J. B.; et al. Reduced cell surface levels of C C chemokine receptor 5 and immunosuppression in long coronavirus disease 2019 syndrome. Clinical Infectious Diseases 2022, 75(7), 1232–1234. [Google Scholar] [CrossRef]
- Akanchise, T.; Angelov, B.; Angelova, A. Nanomedicine-mediated recovery of antioxidant glutathione peroxidase activity after oxidative stress cellular damage: Insights for neurological long COVID. Journal of Medical Virology 2024, 96(5), e29680. [Google Scholar] [CrossRef]
- Cenacchi, Valentina; Furlanis, Giovanni; Menichelli, Alina; Lunardelli, Alberta; Pesavento, Valentina; Manganotti, Paolo. Co-ultraPEALut in Subjective Cognitive Impairment Following SARS-CoV-2 Infection: An Exploratory Retrospective Study. Brain Sciences. 2024. Available online: https://pubmed.ncbi.nlm.nih.gov/38539680/.
- Sasso, E. M.; Eaton-Fitch, N.; Smith, P.; Muraki, K.; Jeremijenko, G.; Griffin, A.; et al. Investigation into the restoration of TRPM3 ion channel activity in post COVID 19 condition natural killer cells treated with naltrexone hydrochloride. Frontiers in Immunology 2024, 15, 1264702. [Google Scholar] [CrossRef]
- Sasso, E. M.; Muraki, K.; Eaton Fitch, N.; Smith, P.; Marshall Gradisnik, S.; Griffin, A. Low dose naltrexone restores TRPM3 ion channel function in natural killer cells from long COVID patients. Frontiers in Molecular Biosciences 2025. [Google Scholar] [CrossRef] [PubMed]
- Bonilla, Hector; Tian, Lu; Marconi, Vincent C.; Shafer, Robert; McComsey, Grace A.; Miglis, Mitchel. Low dose naltrexone for post acute sequelae of SARS CoV 2 infection: A retrospective clinical cohort study. medRxiv. 2023. Available online: https://www.medrxiv.org/content/10.1101/2023.06.08.23291102v1.
- Glynne, P.; Tahmasebi, N.; Gant, V.; Gupta, R. Long COVID following mild SARS CoV 2 infection: characteristic T cell alterations and response to antihistamines. medRxiv. 2021. Available online: https://www.medrxiv.org/content/10.1101/2021.06.06.21258272v1.
- Glynne, Paul; Tahmasebi, Natasha; Gant, Vanya; Gupta, Rajeev. Long COVID following mild SARS-CoV-2 infection: characteristic T cell alterations and response to antihistamines Journal of Investigated Medicine. 2022. Available online: https://pubmed.ncbi.nlm.nih.gov/34611034/.
- Amini Harandi, A.; Pakdaman, H.; Medghalchi, A.; Kimia, N.; Kazemian, A.; Siavoshi, F. randomized open label clinical trial on the effect of amantadine on post COVID 19 fatigue. Scientific Reports 2024, 14(1), 1343. Available online: https://www.nature.com/articles/s41598-024-51904-z. [CrossRef] [PubMed]
- Raj, S.R.; Black, B.K.; Biaggioni, I.; Paranjape, S.Y.; Coffin, S.T.; Robertson, D. Propranolol decreases tachycardia and improves symptoms in the postural tachycardia syndrome: less is more. Circulation 2009, 120(9), 725–734. Available online: https://pubmed.ncbi.nlm.nih.gov/19687359/. [CrossRef] [PubMed]
- Guttuso, T.; Zhu, J.; Wilding, G. E. Lithium aspartate for long COVID fatigue and cognitive dysfunction: A randomized clinical trial. JAMA Network Open 2024, 7(10), e2436874. Available online: https://pubmed.ncbi.nlm.nih.gov/39356507/.
- Landers, D. B.; Yousafzai, O. K.; Klinkhammer, B.; Tancredi, J.; Turi, Z.; Jamal, S.; Glotzer, T. V.; Hollenberg, S. M.; Rockett, G.; Cofini, N.; Gelman, S.; Parrillo, J. E. Beta blocker therapy improves symptoms in post acute COVID 19 syndrome with autonomic dysfunction: An observational cohort study. Journal of the American College of Cardiology 2023. [Google Scholar] [CrossRef]
- Strayer, D. R.; Young, D. L.; Mitchell, W. M.; Carter, W. A.; Stouch, B. C.; Stevens, S. R.; et al. Effect of disease duration in a randomized Phase III trial of rintatolimod, an immune modulator for myalgic encephalomyelitis/chronic fatigue syndrome. PLoS ONE 2020, 15(10). [Google Scholar] [CrossRef]
- Mahadev, A.; Hentati, F.; Miller, B.; Bao, J.; Perrin, A.; Kallogjeri, D.; Piccirillo, J. F. Efficacy of gabapentin for post COVID 19 olfactory dysfunction: The GRACE randomized clinical trial. JAMA Otolaryngology–Head & Neck Surgery 2023, 149(12), 1111–1119. [Google Scholar] [CrossRef]
- Gendreau, R. M.; Bateman, L.; Duncan, G.; Vernon, S.; Sullivan, K.; Gendreau, R.; et al. Low-dose IMC 2 (valacyclovir 750 mg + celecoxib 200 mg BID) improves fatigue and sleep disruption in long COVID: A randomized, double-blind, placebo-controlled investigator-initiated study. BioSpace. 2024. Available online: https://www.biospace.com/press-releases/dogwood-therapeutics-inc-announces-low-dose-imc-2-treatment-reduces-long-covid-related-fatigue-and-sleep-disturbance-in-an-investigator-initiated-study/.
- Finnigan, L. E. M.; Cassar, M. P.; Koziel, M. J.; Pradines, J.; Lamlum, H.; Azer, K.; et al. Efficacy and tolerability of an endogenous metabolic modulator (AXA1125) in fatigue predominant long COVID: A single centre, double blind, randomised controlled phase 2a pilot study. eClinicalMedicine 2023, 59, 101946. Available online: https://ssrn.com/abstract=4356755. [CrossRef]
- Rosen, D. Thomas Jefferson University explores platelet rich plasma to restore smell after COVID 19. ABC News, 2022. Available online: https://6abc.com/covid-19-research-loss-of-smell-jefferson-health/11636709.
- Yan, C. H.; Jang, S. S.; Lin, H. C. F.; et al. Use of platelet rich plasma for COVID 19–related olfactory loss: A randomized controlled trial. International Forum of Allergy and Rhinology 2022, 13(6), 989–997. Available online: https://pubmed.ncbi.nlm.nih.gov/36507615. [CrossRef] [PubMed]
- Bazdyrev, E.; Panova, M.; Brachs, M.; Smolyarchuk, E.; Tsygankova, D.; Gofman, L.; et al. Efficacy and safety of Treamid in the rehabilitation of patients after COVID 19 pneumonia: a phase 2, randomized, double blind, placebo controlled trial. Journal of Translational Medicine 2022) https://translational-medicine.biomedcentral.com/articles/10.1186/s12967-022-03660-9 (2022, November 3, 20(1), 506. Available online: https://translational-medicine.biomedcentral.com/articles/10.1186/s12967-022-03660-9. [CrossRef]
- Di Stadio, A.; Bernitsas, E.; La Mantia, I.; Brenner, M. J.; Ralli, M.; Vaira, L. A.; et al. Targeting neuroinflammation to alleviate chronic olfactory dysfunction in long COVID: A role for investigating disease-modifying therapy (DMT)? Life 2023) https://doi.org/10.3390/life13010226 (2023, January 13, 13(1), 226. [Google Scholar] [CrossRef]
- Pirro, M.; Ferri, L.; Piccioni, L.; Bellucci, A. M.; Bartolucci, F.; Russo, A.; et al. What is the role of palmitoylethanolamide co ultramicronized with luteolin on the symptomatology reported by patients suffering from Long COVID? A retrospective analysis performed by a group of General Practitioners in a real life setting. Nutrients 2023) https://doi.org/10.3390/nu15173701 (2023, August 24, 15(17), 3701. [Google Scholar] [CrossRef]
- Hotz, J. F.; Kellerberger, S.; Elea Jöchlinger, S.; Danielova, I.; Temizsoy, H.; Ötsch, S.; et al. Exploring cognitive impairments and the efficacy of phosphatidylcholine and computer-assisted cognitive training in post acute COVID 19 and post acute COVID 19 vaccination syndrome. Frontiers in Neurology 2024, 15, 1419134. [Google Scholar] [CrossRef] [PubMed]
- Sudo Konno, Y.; Chiba, S.; Okubo, T.; Nemoto, T.; Kanbayashi, T.; Iwabuchi, E. Aripiprazole for treating post COVID 19 hypersomnolence in adolescents: A case series. Sleep 2025, 48 (Supplement_1), A365. Available online: https://academic.oup.com/sleep/article/48/Supplement_1/A365/8135331?login=false. [CrossRef]
- Tokumasu, K.; Matsuki, N.; Otsuka, Y.; Sakamoto, Y.; Ueda, K.; Matsuda, Y. Course of general fatigue in patients with post COVID 19 conditions who were prescribed hochuekkito: A single center exploratory pilot study. Journal of Clinical Medicine 2025, 14(4), 1391. Available online: https://www.mdpi.com/2077-0383/14/4/1391. [CrossRef]
- Slankamenac, J.; Ranisavljev, M.; Todorovic, N.; Ostojic, J.; Stajer, V.; Ostojic, S. M.; et al. Effects of six-month creatine supplementation on patient- and clinician-reported outcomes, and tissue creatine levels in patients with post COVID 19 fatigue syndrome. Food Science & Nutrition 2023, 11(11), 6899–6906. Available online: https://pubmed.ncbi.nlm.nih.gov/37970399/.
- Scheppke, K.; Peluso, M. J.; Klimas, N. G.; Yaffe, K.; Chigbo, C.; Levine, H.; et al. Remission of severe forms of “long COVID” following casirivimab/imdevimab monoclonal antibody infusion: A report of signal index cases and call for targeted research. American Journal of Emergency Medicine 2024, 64, 9–12. Available online: https://ohsu.elsevierpure.com/en/publications/remission-of-severe-forms-of-long-covid-following-monoclonal-anti.
- Chrestia, Juan Facundo; Oliveira, Ana Sofia; Mulholland, Adrian J; Gallagher, Timothy; Bermúdez, Isabel; Bouzat, Cecilia. Exploring functional interaction between SARS CoV 2 spike protein and α7 nicotinic acetylcholine receptors: A patch clamp and preclinical model study [Preprint]. Research Square (2025). 22 March 2025. Available online: https://www.researchsquare.com/article/rs-938911/v2.
- Reinfeld, S. Can Bupropion Treat COVID 19–Induced Brain Fog? A Case Series. In International Clinical Psychopharmacology.; September 2022; Available online: https://www.researchgate.net/publication/362659281_Can_Bupropion_Treat_COVID-19_Induced_Brain_Fog_A_Case_Series.
- Bhattacharjee, D.; Poornima, H.K.; Chakraborty, A. Methylphenidate in COVID 19 Related Brain Fog: A Case Series. Indian Journal of Psychological Medicine. 2024. Available online: https://pmc.ncbi.nlm.nih.gov/articles/PMC11572663/.
- Kondo, T; Higa, R; Kuniba, M; Shinzato, H; Takaesu, Y. Neuropsychopharmacology Reports Editorial Team. Successful treatment with guanfacine in a long COVID case manifesting marked cognitive impairment. Neuropsychopharmacology Reports 2024, 44(3), 585–590. Available online: https://pubmed.ncbi.nlm.nih.gov/38934345/. [CrossRef]
- Theiler, K.; Bronchain, M.; Grouzmann, E.; Duflon, S.; Hirt, L.; Du Pasquier, R.; et al. Treatable immune mediated severe orthostatic hypotension in SARS CoV 2 infection. Frontiers in Neuroscience 2025, 1505727. [Google Scholar] [CrossRef]
- Pierson, V.; Smith, A.; Johnson, L.; Patel, N.; Zhang, X.; Lee, H. Comparative cohort study of post acute COVID 19 infection with nested randomized trial of ivabradine for POTS/IST (the COVIVA study). Frontiers in Neurology 2025. [Google Scholar] [CrossRef]
- Miwa, K. Oral Minocycline Challenge as a Potential First-Line Therapy for Myalgic Encephalomyelitis and Long COVID-19 Syndrome: A Case Report. Annals of Clinical and Medical Case Reports 2022, 8(7), 1–4. Available online: https://acmcasereports.com/articles/ACMCR-v8-1710.pdf.
- Nishi, K.; Yoshimoto, S.; Tanaka, T.; Kimura, S.; Tsunoda, T.; Watanabe, A.; et al. Spatial transcriptomics of the epipharynx in long COVID identifies SARS-CoV 2 signalling pathways and the therapeutic potential of epipharyngeal abrasive therapy. Scientific Reports 2025, 15, 8618. [Google Scholar] [CrossRef] [PubMed]
- Joaquín, C.; Bretón, I.; Ocón Bretón, M. J.; Burgos, R.; Bellido, D.; Matía Martín, P.; Martínez Olmos, M. Á.; Zugasti, A.; Riestra, M.; Botella, F.; García Almeida, J. M. Nutritional and physical rehabilitation in post ICU COVID 19 patients: Prospective results from the NutriEcoMuscle study. In Nutrients; 17, 10. Available online: https://pubmed.ncbi.nlm.nih.gov/40431462/.
- Kumar, S.; Ramaraju, K.; Kakarla, M. S.; Eranezhath, S. S.; Chenthamarakshan, C.; Alagesan, M.; et al. Evaluating Personalized Add On Ayurveda Therapy in Oxygen Dependent Diabetic COVID 19 Patients: A 60 Day Study of Symptoms, Inflammation, and Radiological Changes. Cureus 2024, 16(9). [Google Scholar] [CrossRef]
- Joung, J.-Y.; Lee, J.-S.; Choi, Y.; Kim, Y.J.; Oh, H.-M.; Seo, H.-S.; Son, C.-G. Evaluating Myelophil, a 30% ethanol extract of Astragalus membranaceus and Salvia miltiorrhiza, for alleviating fatigue in long COVID: A real-world observational study. Frontiers in Pharmacology 2024, 15, 1394810. Available online: https://www.frontiersin.org/articles/10.3389/fphar.2024.1394810. [CrossRef]
- Aznar, Asun Gracia; Egea, Fernando Moreno; Banzo, Rafael Gracia; Gutierrez, Rocio; Rizo, Jose Miguel; Rodriguez-Ledo, Pilar. Pro resolving inflammatory effects of a marine oil enriched in specialized pro resolving mediators (SPMs) supplement and its implication in patients with post COVID syndrome (PCS). Biomedicines. 2024. Available online: https://www.mdpi.com/2227-9059/12/10/2221.
- Ikonomidis, I.; Pavlidis, G.; Kountouri, A.; Katogiannis, K.; et al. Effect of a dietary supplement containing glycosaminoglycans and fucoidan on endothelial glycocalyx integrity and vascular function in patients following COVID 19 infection. European Heart Journal – Cardiovascular Imaging 2025, 26 (Suppl 1). Available online: https://academic.oup.com/ehjcimaging/article/26/Supplement_1/jeae333.222/7986671.
- Pavlidis, G.; Kountouri, A.; Katogiannis, K.; Thymis, J.; Nikolaou, P. E.; Chania, C.; Karalis, J.; Kostelli, G.; Michalopoulou, E.; Katsanaki, E.; Parissis, J.; Vink, H.; Long, R.; Tsiodras, S.; Lambadiari, V.; Ikonomidis, I. Effects of four month treatment with glycocalyx dietary supplement on endothelial glycocalyx integrity and vascular function after COVID 19 infection. European Journal of Clinical Investigation 2025, 55(7), e70058. Available online: https://onlinelibrary.wiley.com/doi/10.1111/eci.70058. [CrossRef]
- Marzetti, E.; Coelho Júnior, H. J.; Calvani, R.; Girolimetti, G.; Di Corato, R.; Ciciarello, F.; et al. Mitochondria derived vesicles and inflammatory profiles of adults with long COVID supplemented with red beetroot juice: Secondary analysis of a randomized controlled trial. International Journal of Molecular Sciences 2025, 26(3), 1224. [Google Scholar] [CrossRef]
- Calvani, R.; Giampaoli, O.; Marini, F.; Del Chierico, F.; De Rosa, M.; Conta, G.; et al. Beetroot juice intake positively influenced gut microbiota and inflammation but failed to improve functional outcomes in adults with long COVID: A pilot randomized controlled trial. Clinical Nutrition 2024, 43(12), 344–358. [Google Scholar] [CrossRef] [PubMed]
- Łoniewski, Igor; Skonieczna-Żydecka, Karolina; Sołek-Pastuszka, Joanna; Marlicz, Wojciech. Gut Microbiota and Probiotics in Post-COVID-19 Recovery: An Exploratory Study. International Journal of Molecular Sciences 2022, 24(8), 7417. Available online: https://www.mdpi.com/2077-0383/11/17/5155.
- Horvath, A.; Habisch, H.; Prietl, B.; Pfeifer, V.; Balazs, I.; Kovacs, G.; Foris, V.; John, N.; Kleinschek, D.; Feldbacher, N.; Grønbæk, H.; Møller, H. J.; Žukauskaitė, K.; Madl, T.; Stadlbauer, V. Alteration of the gut–lung axis after severe COVID-19 infection and modulation through probiotics: A randomized, controlled pilot study. Nutrients 2024, 16(22), 3840. Available online: https://pubmed.ncbi.nlm.nih.gov/39599626/. [CrossRef] [PubMed]
- Patterson, B. K.; Yogendra, R.; Guevara Coto, J.; Mora Rodriguez, R. A.; Osgood, E.; Bream, J.; et al. Case series: Maraviroc and pravastatin as a therapeutic option to treat long COVID/post acute sequelae of COVID (PASC). Frontiers in Medicine 2023, 10, 1122529. [Google Scholar] [CrossRef]
- Currie, Crawford; Myklebust, Tor Åge; Bjerknes, Christian Bomi. Framroze1Assessing the Potential of an Enzymatically Liberated Salmon Oil for Immunomodulation in Adults with Mild to Moderate COVID-19: A Pilot Randomized Controlled Trial. International Journal of Molecular Sciences 2024, 25(13). Available online: https://www.mdpi.com/1422-0067/25/13/6917.
- Sigamani, A.; Naik, K. S.; Kumar, S. S. Post acute sequelae SARS CoV 2 (PASC) infection and molecular signaling – A quasi experimental study evaluating a natural supplement. Research Square 2023. [Google Scholar] [CrossRef]
- Aguida, B.; Ahmad, M.; Jourdan, N.; Pooam, M. Infrared light therapy relieves TLR 4 dependent hyper inflammation of the type induced by COVID 19. Communicative & Integrative Biology 2021, 14(1), 200–211. [Google Scholar] [CrossRef]
- Theoharides, T. C.; Kempuraj, D. Role of SARS CoV 2 spike protein induced activation of microglia and mast cells in the pathogenesis of Neuro COVID. Cells 2023, 12(5), 688. [Google Scholar] [CrossRef]
- ISRCTN. A research trial to find out if tocilizumab helps adults with Long Covid feel better ISRCTN. 2025. Available online: https://www.isrctn.com/ISRCTN46454974.
- Olve, M. E. New Clinical Trial Will Test How Baricitinib Improves Neurocognitive Function in Patients with Long Covid. 2025. Available online: https://solvecfs.org/new-clinical-trial-will-test-how-baricitinib-improves-neurocognitive-function-in-patients-with-long-covid/.
- Creyns, B.; MacKenzie, B.; Jannini Sa, Y. A. P.; Coelho, A. L.; Christensen, D.; Parimon, T.; et al. Caveolin scaffolding domain (CSD) peptide LTI 2355 modulates the phagocytic and synthetic activity of lung derived myeloid cells in idiopathic pulmonary fibrosis (IPF) and post acute sequelae of COVID fibrosis (PASC F). Biomedicines 2025, 13(4), 796. [Google Scholar] [CrossRef]
- Francavilla, F.; Intranuovo, F.; La Spada, G.; Lacivita, E.; Altomare, C. D. Inflammaging and immunosenescence in the post COVID era: Small molecules, big challenges. ChemMedChem 2024. [Google Scholar] [CrossRef]
- Akanchise, T.; Angelov, B.; Angelova, A. Nanomedicine-mediated recovery of antioxidant glutathione peroxidase activity after oxidative-stress cellular damage: Insights for neurological long COVID (2024). Available online: https://onlinelibrary.wiley.com/doi/full/10.1002/jmv.29680.
- Elumalai, N.; Hussain, H.; Sampath, N.; Shamaladevi, N.; Paidas, M. J. SPIKENET (SPK), a 15 amino acid ACE2 targeted peptide, mitigates inflammation, oxidative stress, multi organ damage, and mortality in mouse models of acute and long COVID. Viruses 2024, 16(6), 838. [Google Scholar] [CrossRef]
- Darby, F. The Gut Health Advantage: How Fiber May Reduce Risk for Long COVID. Yale Medicine. 2024. Available online: https://www.yalemedicine.org/news/the-gut-health-advantage-how-fiber-may-reduce-risk-for-long-covid.
- Staff Report, Breakthrough Long COVID ‘Brain Fog’ Drug Being Developed by Augusta University Researchers. Augusta CEO. 2 December 2022. Available online: https://augustaceo.com/news/2022/12/breakthrough-long-covid-brain-fog-drug-being-developed-augusta-university-researchers/.
- Fernandes, I. G.; Oliveira, L. de M.; Andrade, M. M. de S.; Alberca, R. W.; Lima, J. C.; de Sousa, E. S. A.; et al. Resveratrol Upregulates Antioxidant Factors Expression and Downmodulates Interferon Inducible Antiviral Factors in Aging. International Journal of Molecular Sciences 2025, 26(5), 2345. [Google Scholar] [CrossRef] [PubMed]
- Omran, H. M.; Almaliki, M. S. Influence of NAD+ as an ageing-related immunomodulator on COVID 19 infection: A hypothesis. J Infect Public Health 2020, 13(9), 1196–1201. [Google Scholar] [CrossRef]
- Thadani-Mulero, M.; Ramos, P. S.; Dhamija, R.; Felsenstein, S.; Grieb, B. J.; Petracek, L. UVA Health joins national trials testing Long COVID treatments. UVA Health Newsroom. 20 March 2025. Available online: https://newsroom.uvahealth.com/2025/03/20/uva-health-joins-national-trials-testing-long-covid-treatments/.
- Medhat, P. M.; Fouad, M. M.; Monir Hunter, H. H.; Ghoniem, N. S. Simultaneous quantification of paracetamol, dexketoprofen trometamol, and rivaroxaban used in post COVID 19 syndrome via sustainable, green HPLC PDA. Scientific Reports 2024, 14, Article 26222. Available online: https://www.nature.com/articles/s41598-024-75216-4. [CrossRef] [PubMed]
- Pliszka, A. G. Modafinil: A Review and Its Potential Use in the Treatment of Long COVID Fatigue and Neurocognitive Deficits. American Journal of Psychiatry Residents’ Journal 2022, 17(4), 5–7. [Google Scholar] [CrossRef]
- Yoon, J.; Kim, S.; Kwon, C.-Y.; Kang, J. W.; Kim, T.-H.; Kwon, S. Kyungok go for fatigue in patients with long COVID: Double blind, randomized, multicenter, pilot clinical study protocol. PLoS ONE 2025, 20(4), e0319459. Available online: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0319459. [CrossRef]
- DrugBank. Cyclobenzaprine Completed Phase 2 Trials for Post-Acute Sequelae of SARS-CoV-2 (PASC) Infection / Post-Acute COVID-19 Syndrome / Long Haul COVID / Coronavirus Disease 2019 (COVID-19) Treatment. Drug Bank. 2024. Available online: https://go.drugbank.com/drugs/DB00924/clinical_trials?conditions=DBCOND0129755%2CDBCOND0150477%2CDBCOND0140673%2CDBCOND0144742&phase=2&purpose=treatment&status=completed.
- Pierson, MJ; Apilado, CE; Franzos, NM; Allard, JP; Mancuso, A; Tribble, BD; Saunders, JT; Koehlmoos, TP. Oral medications for the treatment of postural orthostatic tachycardia syndrome (POTS): a systematic review of studies before and during the COVID-19 pandemic. Frontiers in Neurology 2024. [Google Scholar]
- Available online: http://www.frontiersin.org/articles/10.3389/fneur.2024.1515486.
- Yang, Chun-Pai; Chang, Ching-Mao; Yang, Cheng-Chia; Pariante, Carmine M.; Su, & Kuan-Pin. Long COVID and long chain fatty acids (LCFAs): Psychoneuroimmunity implication of omega-3 LCFAs in delayed consequences of COVID-19. Brain, Behavior, and Immunity 2022, 103, 1–13. Available online: https://www.sciencedirect.com/science/article/pii/S0889159122000952?via%3Dihub. [CrossRef]
- Li, G. H.; Han, F. F.; Kalafatis, E.; Kong, Q. P.; Xiao, W. Systems modeling reveals shared metabolic dysregulation and potential treatments in ME/CFS and Long COVID. International Journal of Molecular Sciences 2025, 26(13), 6082. Available online: https://www.mdpi.com/1422-0067/26/13/6082. [CrossRef]
- Au, M. T.; Ni, J.; Tang, K.; Wang, W.; Zhang, L.; Wang, H.; Zhao, F.; Li, Z.; Luo, P.; Lau, L. C. M.; Chan, P. K.; Luo, C.; Zhou, B.; Zhu, L.; Zhang, C. Y.; Jiang, T.; Lauwers, M.; Chan, J. F. W.; Yuan, S.; Wen, C. Blockade of endothelin receptors mitigates SARS CoV 2 induced osteoarthritis. Nature Microbiology 2024, 9(10), 2538–2552. Available online: https://www.nature.com/articles/s41564-024-01802-x. [CrossRef] [PubMed]
- Fan, C.; Zhang, Z.; Lai, Z.; Yang, Y.; Li, J.; Liu, L.; et al. Chemical evolution and biological evaluation of natural products for efficient therapy of acute lung injury. Advanced Science 2023, 11(7), e2305432. [Google Scholar] [CrossRef]
- Frank, N.; Dickinson, D.; Garcia, W.; Xiao, L.; Xayaraj, A.; Lee, L. H.; et al. Evaluation of epigallocatechin-3-gallate palmitate (EC16) nasal nanoformulations against human coronavirus for potential long COVID treatment. Research Gate. January 2024. Available online: https://www.researchgate.net/publication/369951374_Evaluation_of_Epigallocatechin-3-Gallate-Palmitate_EC16_in_Nasal_Formulations_Against_Human_Coronavirus.
- Chen, X.; Zhou, Y.; Yao, W.; Gao, C.; Sha, Z.; Yi, J.; et al. Organelle tuning condition robustly fabricates energetic mitochondria for cartilage regeneration. Bone Research 2025, 13, Article 37. [Google Scholar] [CrossRef] [PubMed]
- Vaziri Harami, R.; Delkash, P.; et al. Can l carnitine reduce post COVID 19 fatigue? Annals of Medicine & Surgery 2021, 73, 10314. [Google Scholar] [CrossRef]
- Rejinold, S. N.; Choi, G.; Jin, G.-W.; Choy, J.-H.; et al. Transforming niclosamide through nanotechnology: A promising approach for long COVID management. Small 2025, 21(27), e2410345. Available online: https://pubmed.ncbi.nlm.nih.gov/40384184/. [CrossRef]
- Brigham, Mass General. AT1001 for the Treatment of Long COVID (Larazotide Acetate, Phase 2a randomized, double blind, placebo controlled trial). March 2023. Available online: https://clinicaltrials.gov/study/NCT05747534.
- Reardon, S. MDMA therapy for PTSD rejected by FDA panel. Nature. June 2024. Available online: https://www.nature.com/articles/d41586-024-01622-3.
- EmphyCorp/Cellular Sciences Inc. Effects of Sodium Pyruvate Nasal Spray in COVID 19 Long Haulers [Clinical trial NCT04871815]. ClinicalTrials.gov. 2021. Available online: https://clinicaltrials.gov/study/NCT04871815?rank=4&term=sodium+pyruvate.
- Yu, G.-R.; Lim, D.; Park, W.-H. Evaluation of Korean herbal prescriptions on long COVID inflammation: In vitro and network pharmacology approaches. Preprints.org. August 2024.
- Available online: https://www.preprints.org/manuscript/202408.0306/v1.
- Jarrott, Bevyn; Head, Richard; Pringle, Kirsty G.; Lumbers, Eugenie R.; Martin, Jennifer H. “LONG COVID”—A hypothesis for understanding the biological basis and pharmacological treatment strategy: The role of melatonin as an NRF2 activator. Pharmacology Research & Perspectives 2022, 10(1), e00911. [Google Scholar] [CrossRef]
- Xerfan, E. M. S.; Morelhão, P. K.; Arakaki, F. H.; Facina, A. S.; Tomimori, J.; Xavier, S. D.; et al. Could melatonin have a potential adjuvant role in the treatment of lasting anosmia associated with COVID 19? International Journal of Developmental Neuroscience 2022. [Google Scholar] [CrossRef]
- Cardinali, Daniel P.; Brown, Gregory M.; Pandi-Perumal, Seithikurippu R. Possible application of melatonin in long COVID: A narrative review highlighting neuroprotective and chronobiotic functions. Biomolecules 2022, 12(11), 1646. Available online: https://www.mdpi.com/2218-273X/12/11/1646.
- Yehia, A.; Abulseoud, O. A. Melatonin: A ferroptosis inhibitor with potential therapeutic efficacy for the post COVID 19 trajectory of accelerated brain aging and neurodegeneration. Molecular Neurodegeneration 2024, 19(1), 36. [Google Scholar] [CrossRef]
- Tsilioni, I.; Kempuraj, D.; Theoharides, T. C. Nobiletin and eriodictyol suppress release of IL 1β, CXCL8, IL 6, and MMP 9 from LPS, SARS CoV 2 spike protein, and ochratoxin A stimulated human microglia. International Journal of Molecular Sciences 2025, 26(2), 636. [Google Scholar] [CrossRef]
- Prazanowska, K. H.; Kim, T.-H.; Kang, J. W.; Jin, Y.-H.; Kwon, S.; Lim, S. B. A single-cell RNA sequencing dataset of peripheral blood cells in long COVID patients on herbal therapy. Scientific Data 2025, 12(1), 177. [Google Scholar] [CrossRef]
- Cassiano, L. M. G.; de Paula, J. J.; Rosa, D. V.; Miranda, D. M.; Romano Silva, M. A.; Coimbra, R. S. Vitamin B12 as an epidrug for regulating peripheral blood biomarkers in long COVID associated visuoconstructive deficit. Scientific Reports 2025, 15(1), Article 9438. Available online: https://www.nature.com/articles/s41598-025-86637-0. [CrossRef]
- Zilberman-Itskovich, S.; et al. Hyperbaric oxygen therapy improves neurocognitive functions and symptoms of post-COVID-19 condition: randomized controlled trial. Scientific Reports 2022, 12(1), 11252. Available online: https://pubmed.ncbi.nlm.nih.gov/38071990/. [CrossRef] [PubMed]
- Kuut, A. M.; et al. A randomised controlled trial testing the efficacy of Fit after COVID, a cognitive behavioral therapy targeting severe post-infectious fatigue following COVID-19 (ReCOVer): study protocol. Trials 2021, 22(1), 867. Available online: https://pubmed.ncbi.nlm.nih.gov/34857010/. [CrossRef] [PubMed]
- Lam, Wai Ching; Wei, Dongjue; Li, Huijuan; et al. The use of acupuncture for addressing neurological and neuropsychiatric symptoms in patients with long COVID: a systematic review and meta-analysis. Frontiers in Neurology. July 2024. Available online: https://pubmed.ncbi.nlm.nih.gov/39099786/.
- Knopman, D. S.; et al. "Evaluation of interventions for cognitive symptoms in Long COVID: A randomized clinical trial (RECOVER-NEURO).". JAMA Neurology. 2025. Available online: https://pmc.ncbi.nlm.nih.gov/articles/PMC12603944/.
- Lau, R. I.; et al. A synbiotic preparation (SIM01) for post-acute COVID-19 syndrome in Hong Kong (RECOVERY): a randomised, double-blind, placebo-controlled trial. The Lancet Infectious Diseases 2023, 24(2), 147–157. Available online: https://pubmed.ncbi.nlm.nih.gov/38071990/. [CrossRef] [PubMed]
Figure 1.
Ratios of COVID/Long COVID papers in the PubMed Paper Database.
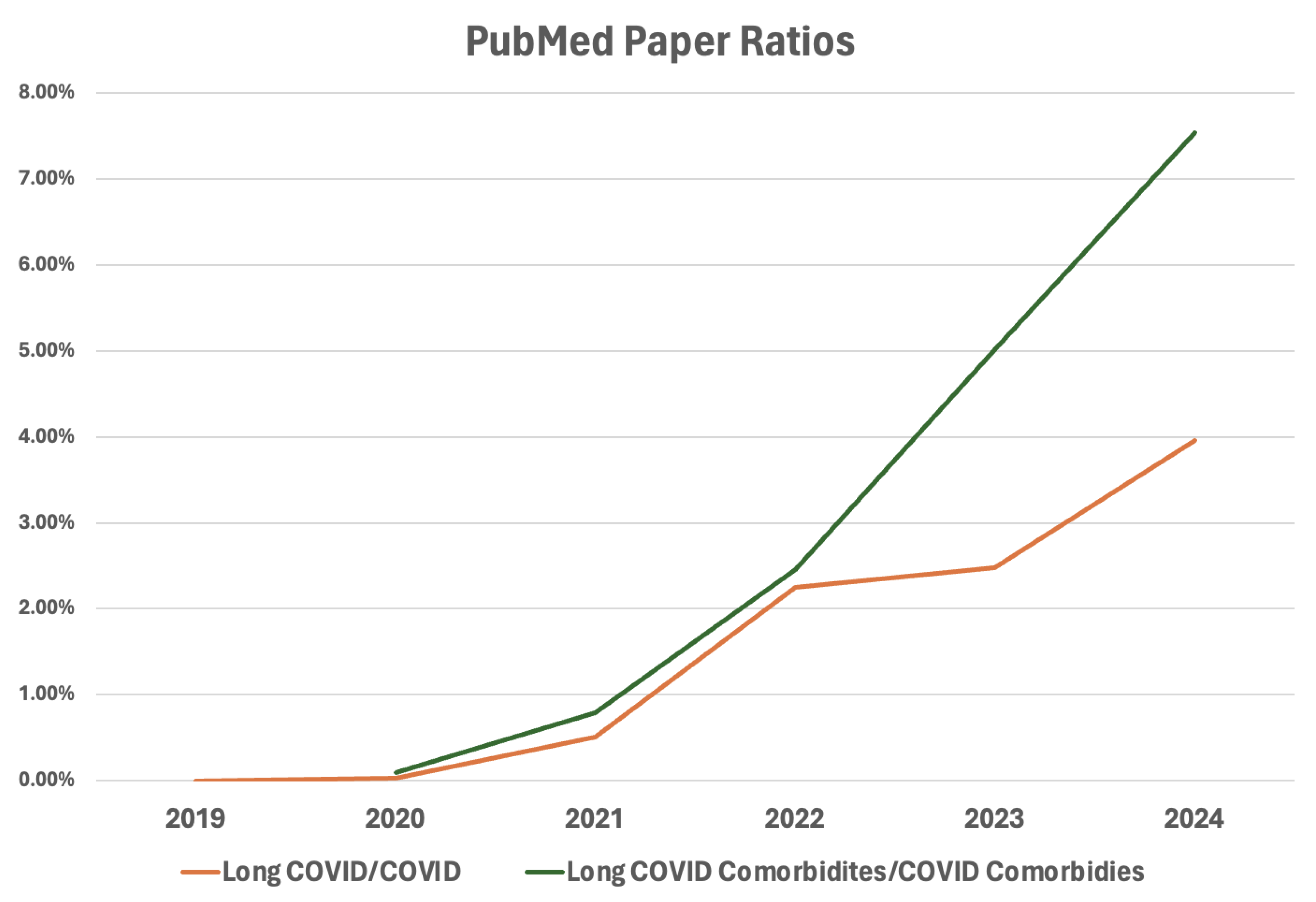
Figure 2.
Long COVID’s Major Symptoms[2].
Figure 2.
Long COVID’s Major Symptoms[2].
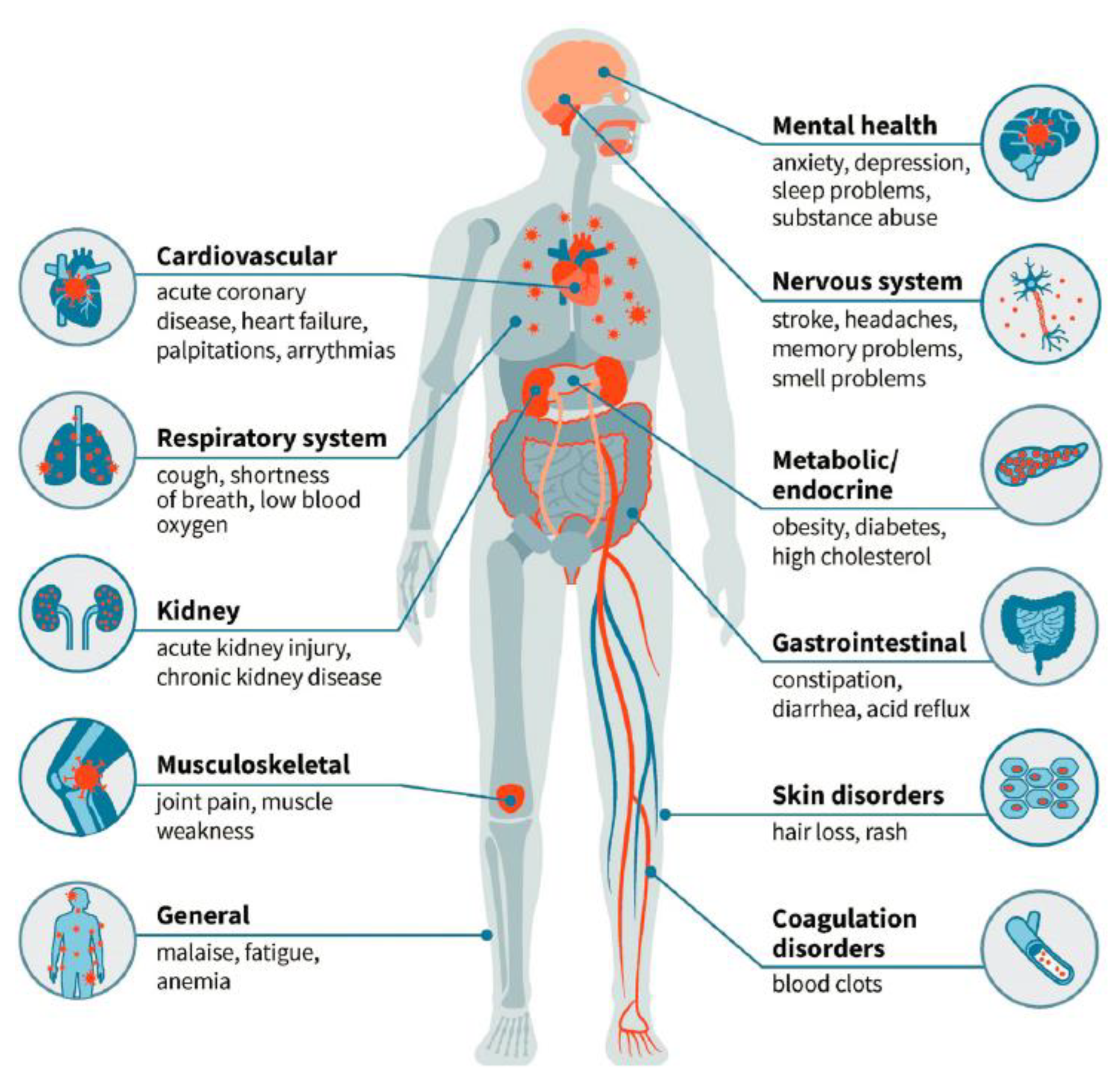
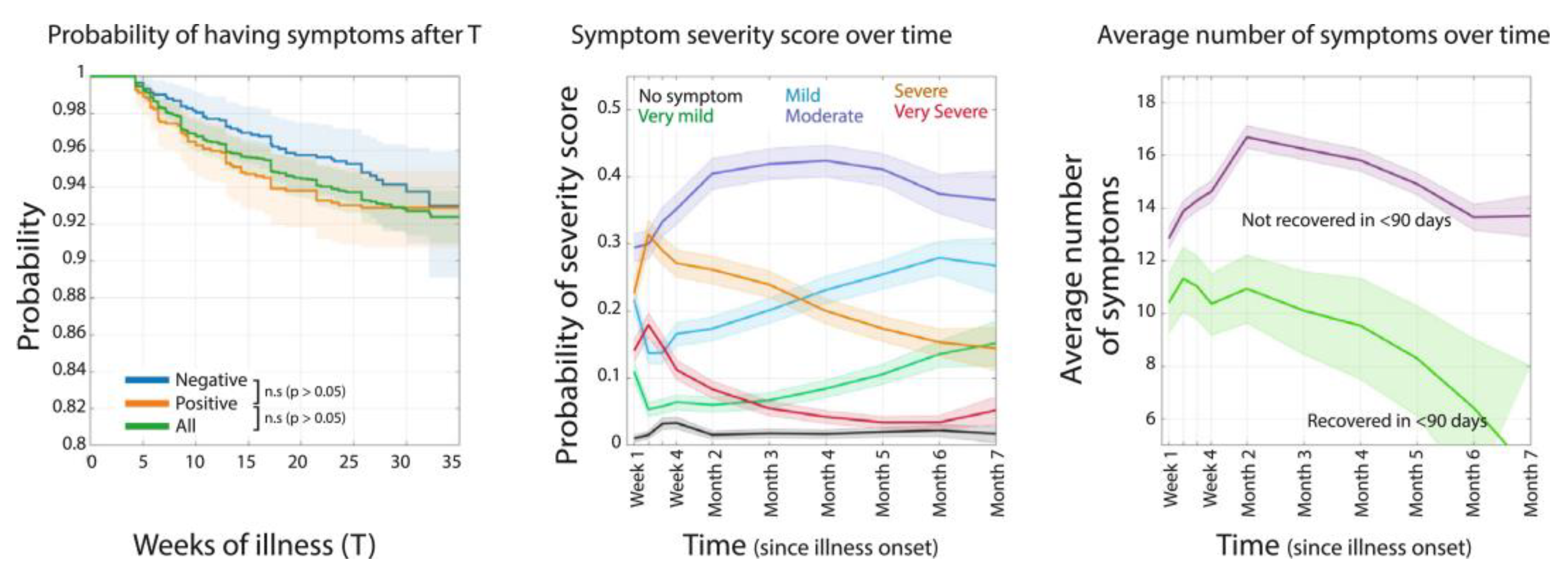
Figure 4.
Smell or Taste Recovery Time After a Mild COVID Case[9].
Figure 4.
Smell or Taste Recovery Time After a Mild COVID Case[9].
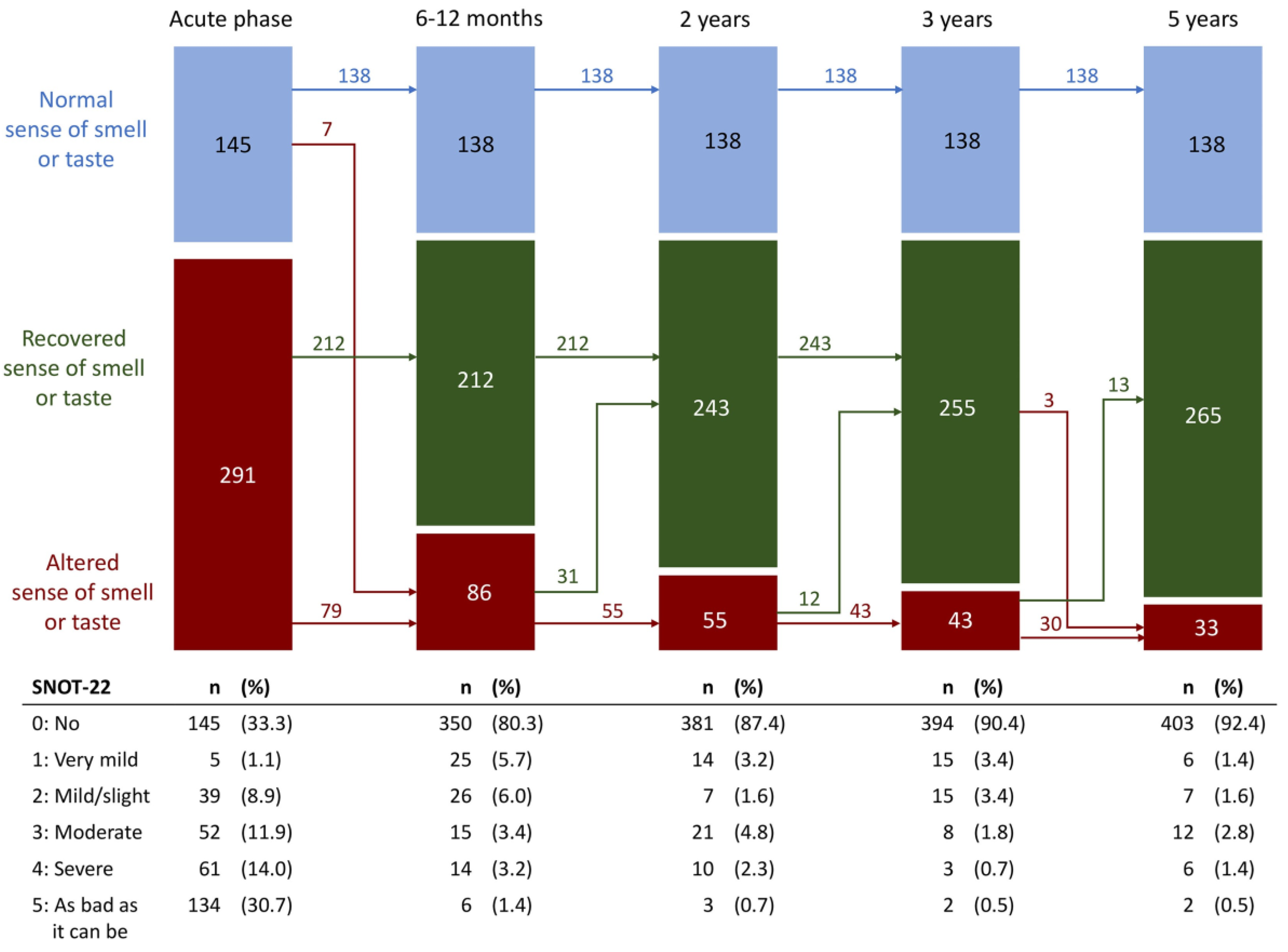
Figure 5.
Long COVID Organ Disruption Papers in The Mouse That Roared. The Figure Was Prepared by Author
Figure 5.
Long COVID Organ Disruption Papers in The Mouse That Roared. The Figure Was Prepared by Author
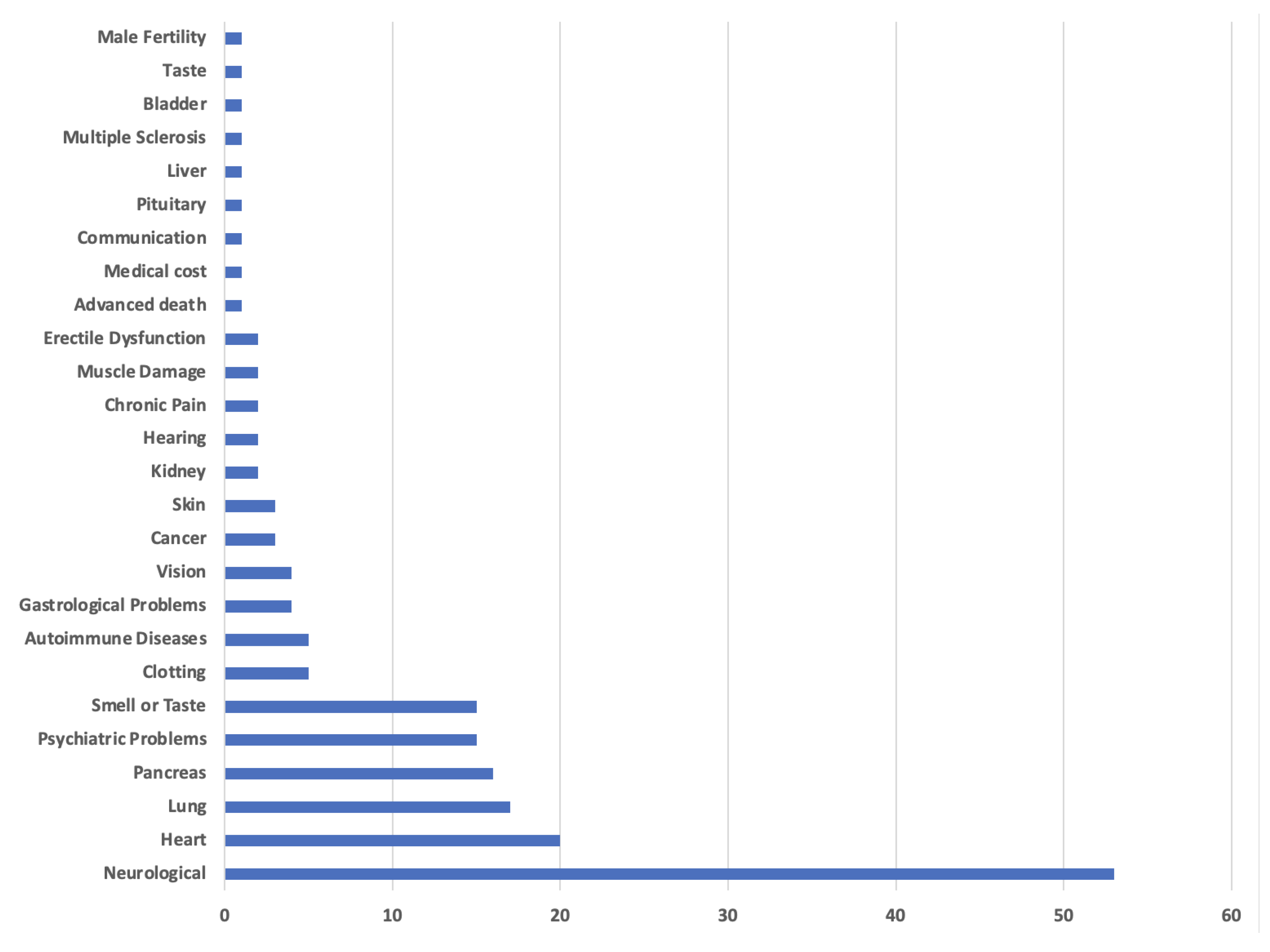
Figure 6.
US Long COVID Prevalence[11].
Figure 6.
US Long COVID Prevalence[11].
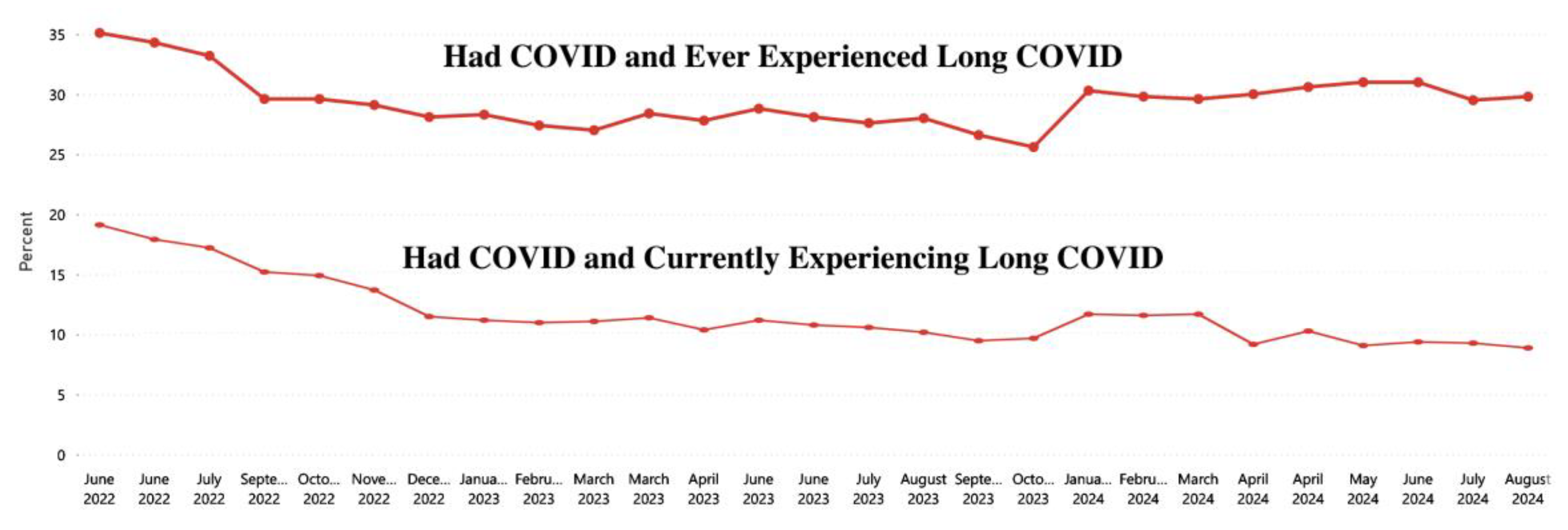
Figure 9.
Percent of People with Long COVID – March 2024[13].
Figure 9.
Percent of People with Long COVID – March 2024[13].
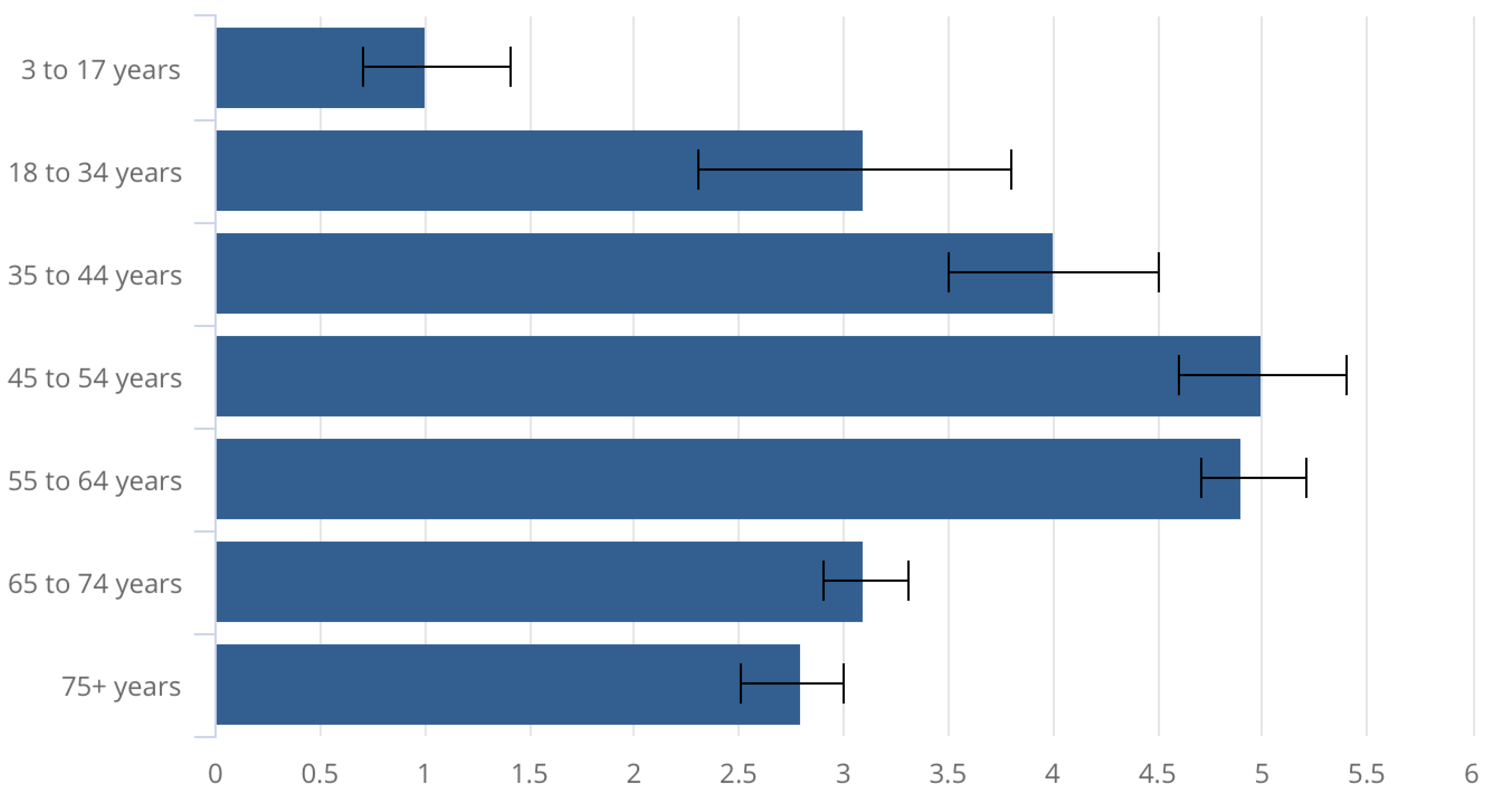
Figure 10.
Long COVID Rates by Variant and Vaccination Status[14]. DALYs - Disability-Adjusted Life Years
Figure 10.
Long COVID Rates by Variant and Vaccination Status[14]. DALYs - Disability-Adjusted Life Years
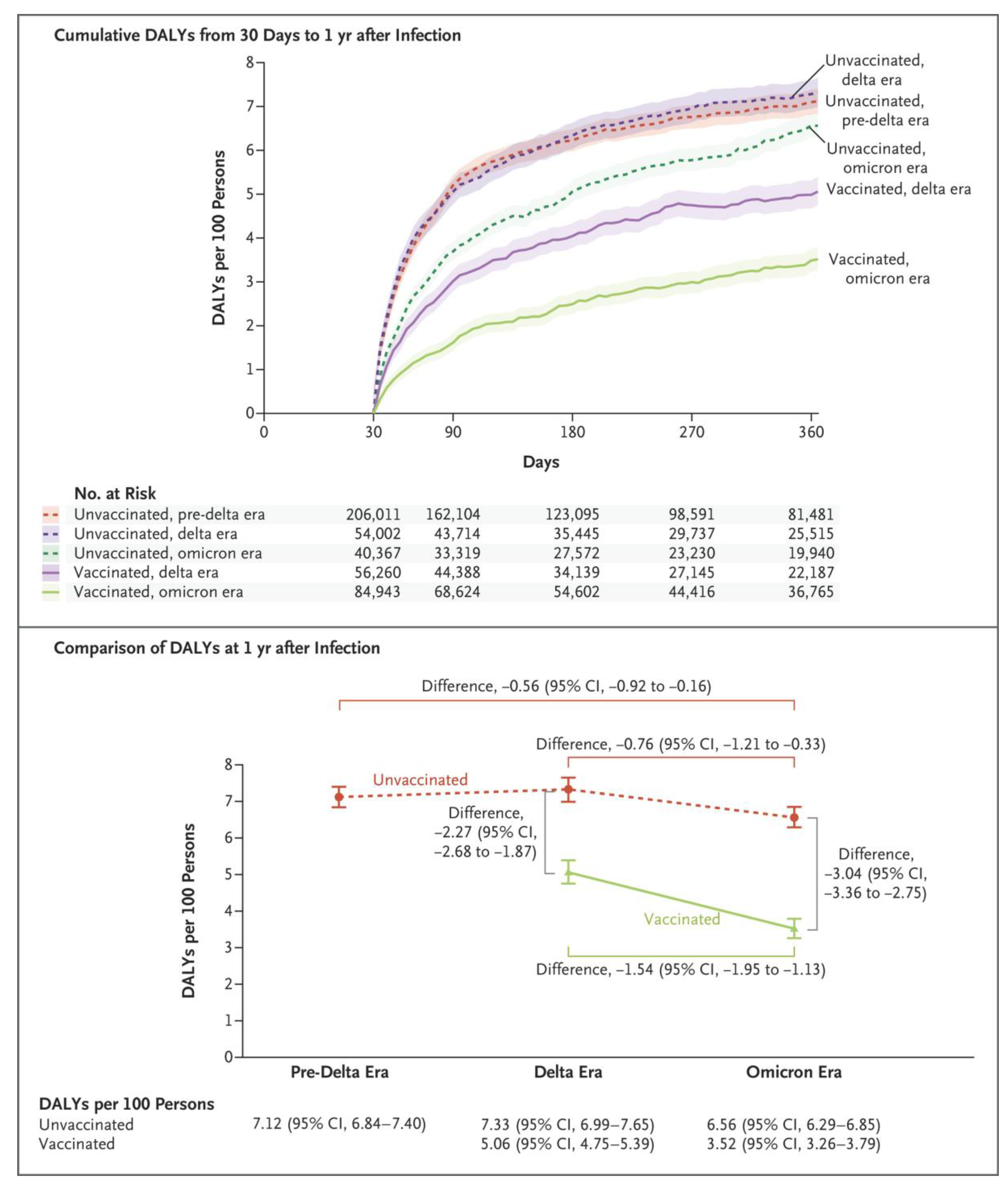
Figure 11.
– Long COVID Root Causes. The Figure Was Prepared by Author
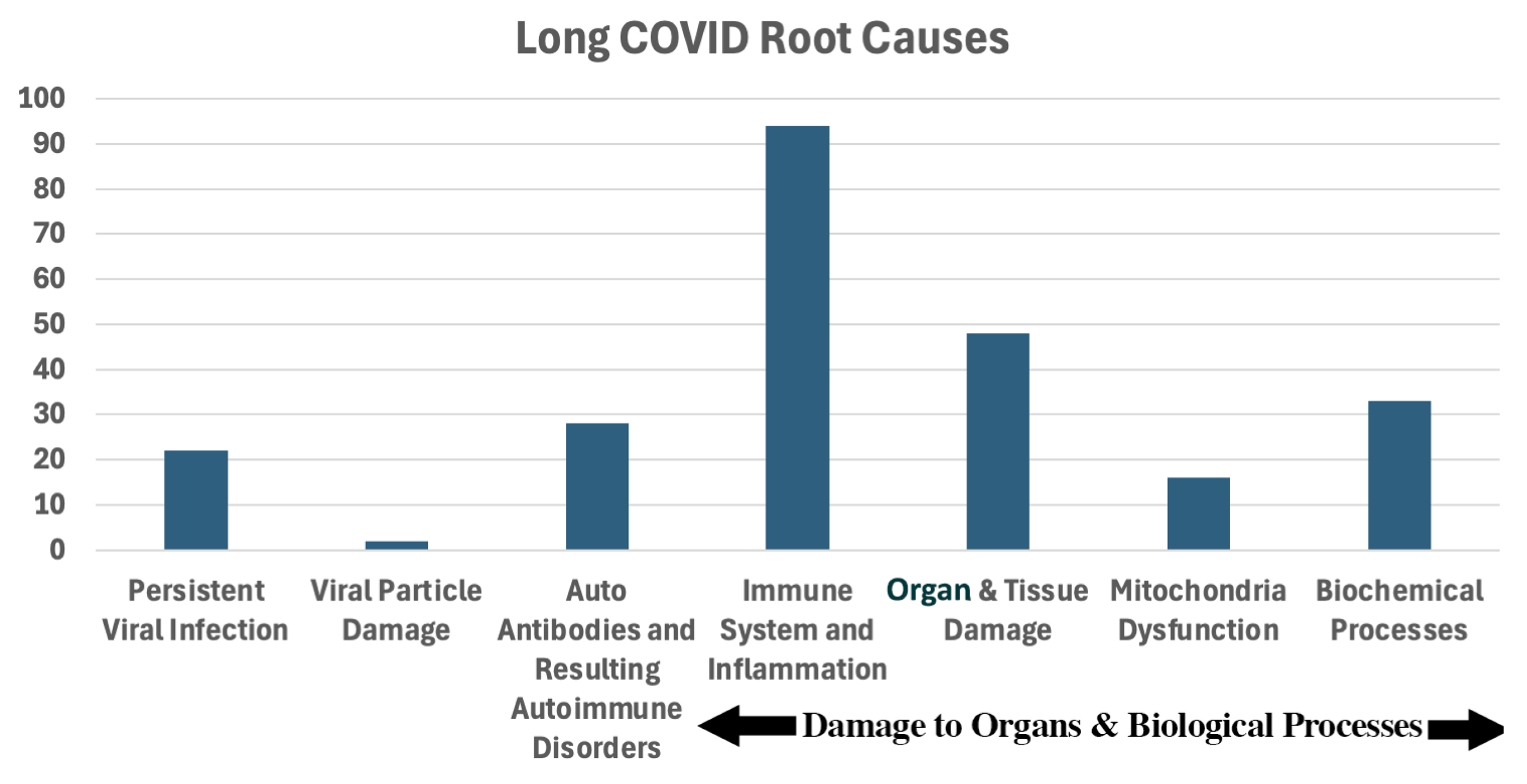
Figure 12.
Papers Reporting Impact of COVID Vaccination on Long COVID. This Figure Was Prepared by Author. The X-Axis is the number of papers for the reported reduction in Long COVID rates.
Figure 12.
Papers Reporting Impact of COVID Vaccination on Long COVID. This Figure Was Prepared by Author. The X-Axis is the number of papers for the reported reduction in Long COVID rates.
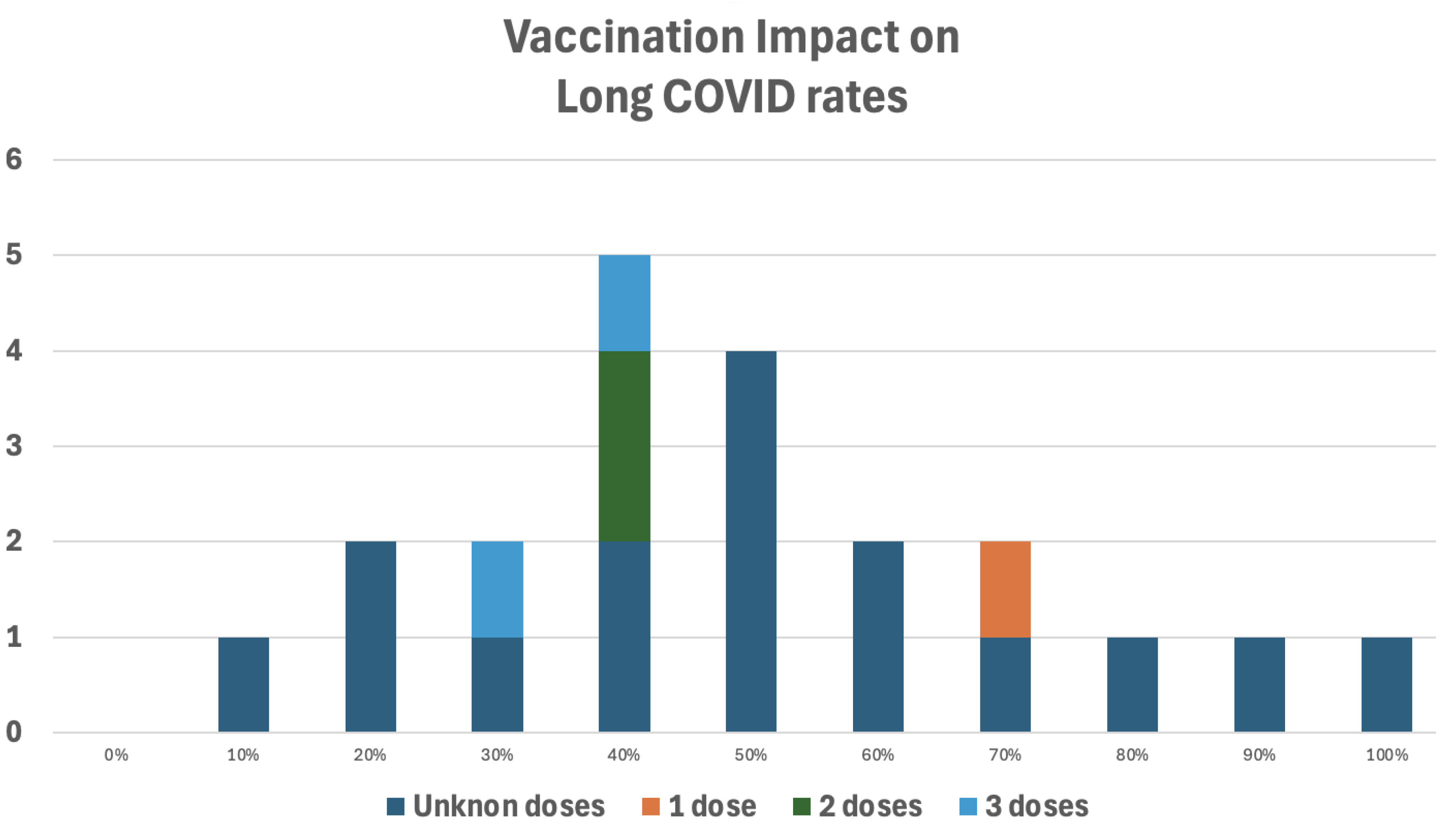
Figure 13.
Post COVID Symptoms Log from the Clevland Clinic.
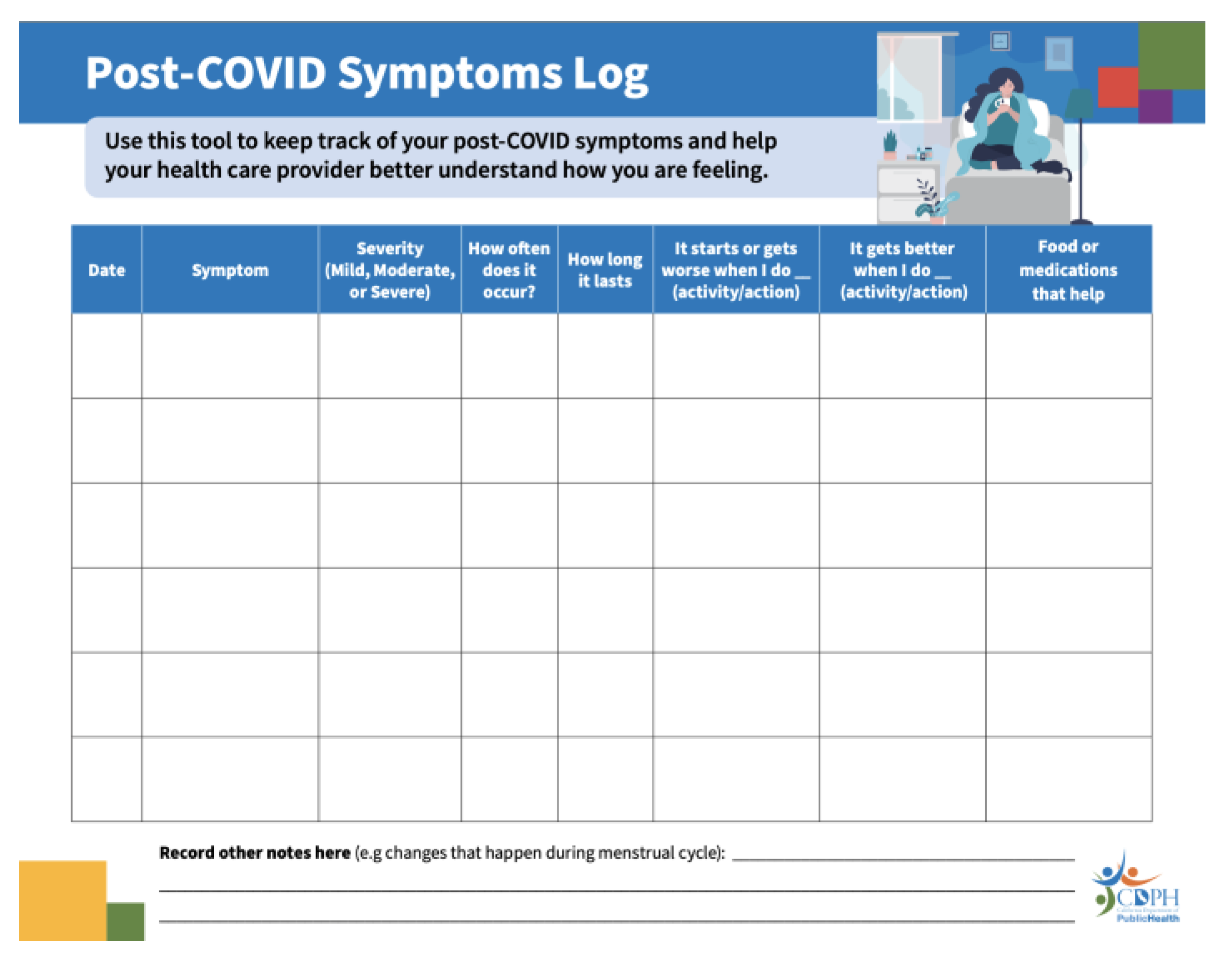
Figure 14.
Types of Long COVID Treatments. The Figure Was Prepared by the Author.
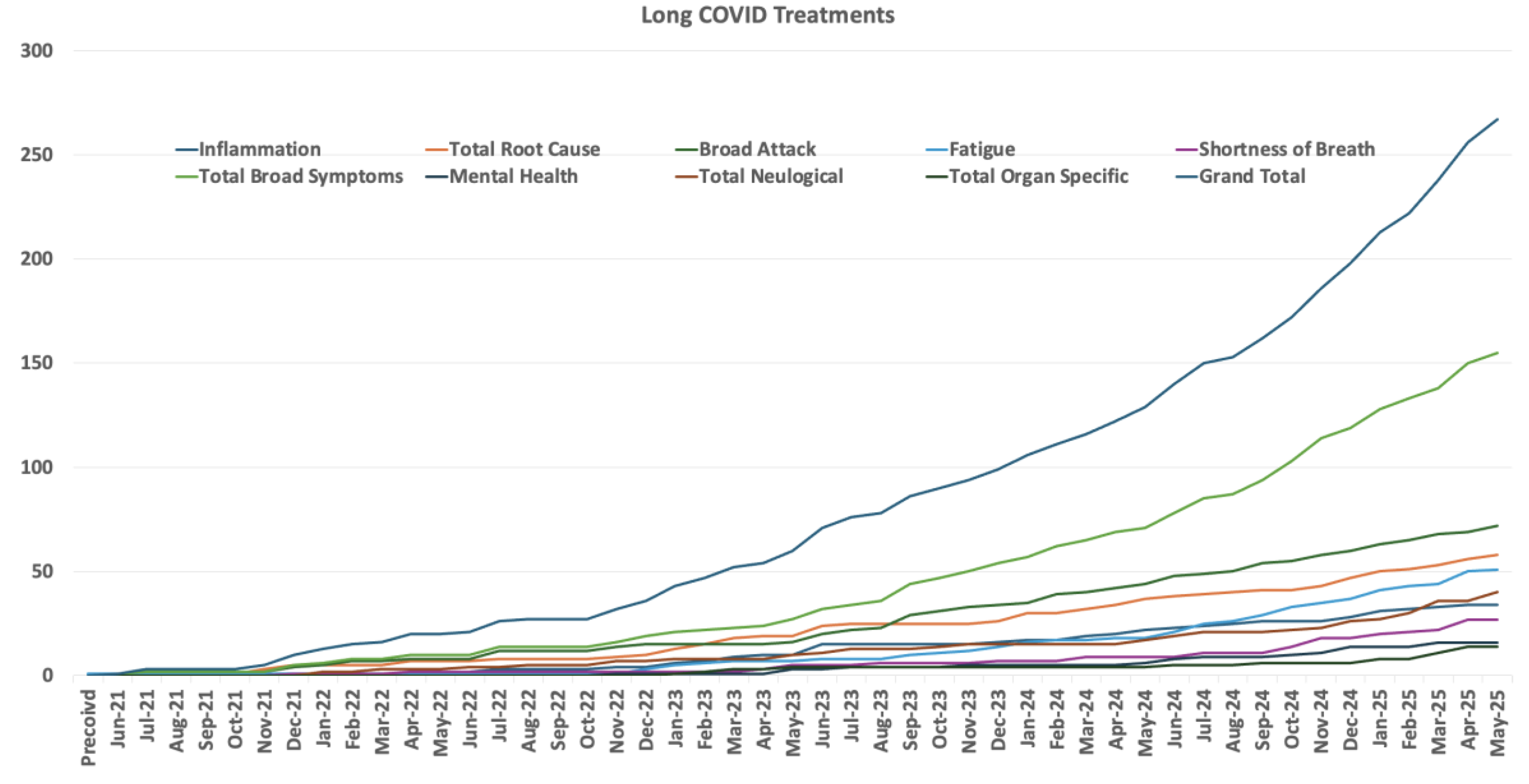
Figure 15.
Medical Papers on Mitochondrial Dysfunction[22].
Figure 15.
Medical Papers on Mitochondrial Dysfunction[22].
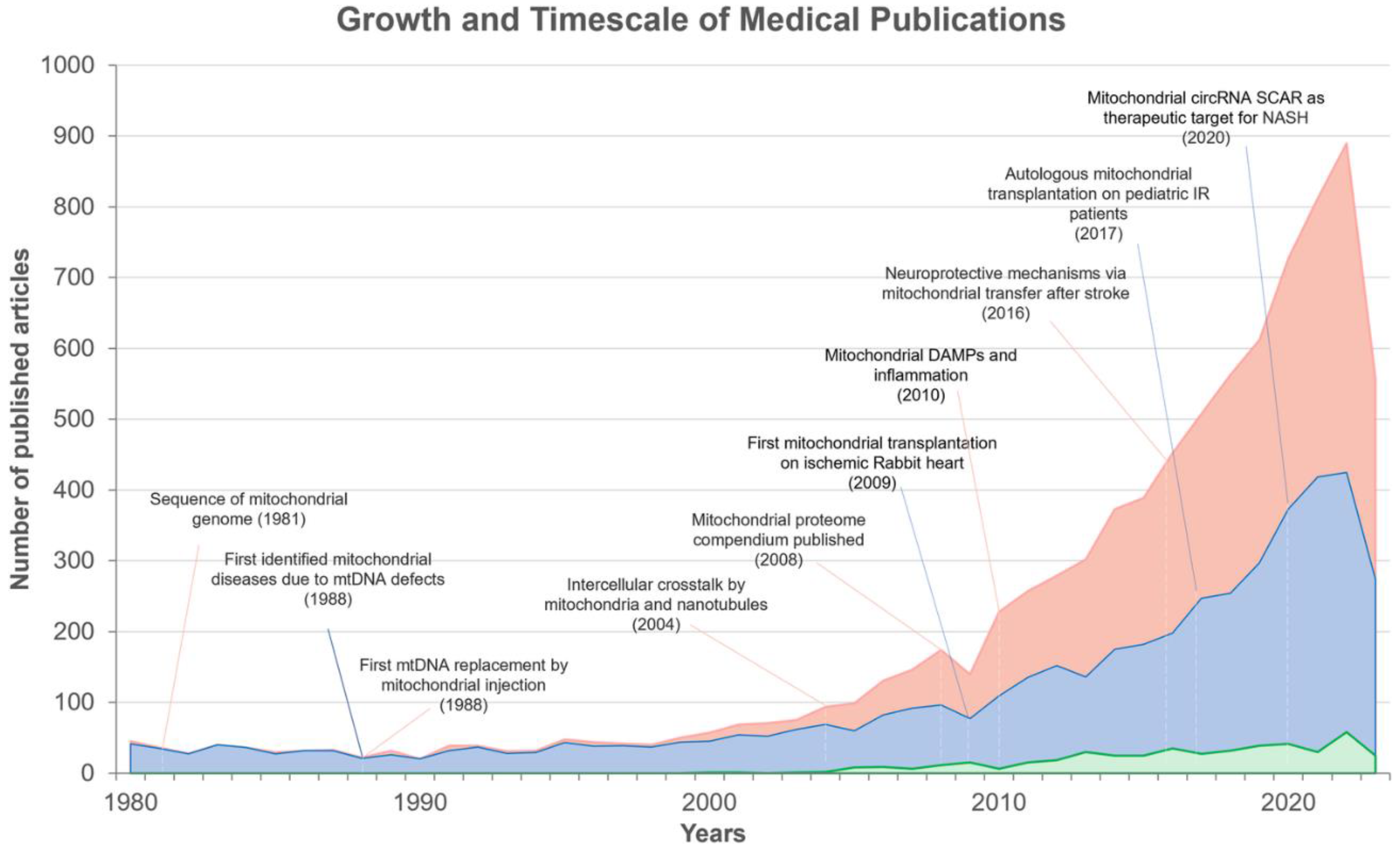
Table 1.
COVID as Compared to Long COVID. This Table Was Prepared by the Author.
| COVID | Long COVID | |
| Date of First Paper | February 3, 2020 Nature – 19,000+ citations Lancet – 12,000+ citations |
November 3, 2020 JAMA – 446 citations |
| What is it? | A disease caused by a virus | The multiple, diverse consequences of a disease |
| Contagious | Yes, very | No |
|
Test |
Yes – PCR and rapid antigen | No |
| % of US afflicted population | ~90% | ~7% of those who had COVID |
|
Length of illness |
Typically, 5-10 days |
Months to years or perhaps permanent |
| Sex prevalence | Male | Female |
| Vaccination Impact | Significant reduction | No Long COVID vaccine and none is likely. However, pre-COVID vaccination helps. Post-COVID vaccination does not help. |
| Therapeutic objective | Avoid severe disease | Repair COVID damage |
| Therapeutic effectiveness tests | Biochemical tests based on the therapeutic type, i.e., antiviral, anti-inflammatory, oxygenation, and blood clots. |
Human trials and highly qualitative studies |
| Therapeutic placebo effect | Some | Can be significant |
Table 2.
Disease Post Recovery Impacts. This Table Was Prepared by the Author.
| Disease / Virus | Common Long-Term Symptoms | Organs/Systems Affected | Duration | Percent Affected |
| COVID-19 | Fatigue, brain fog, postural orthostatic tachycardia syndrome, heart palpitations, gastrointestinal issues | Brain, nerves, lungs, heart, kidney, liver, pancreas, genitals, musculoskeletal, immune system | Months to years |
~5 –15% higher after severe cases |
| Epstein-Barr | Chronic fatigue, memory issues, muscle pain | Brain, immune system, liver | Months to years | ~10–15% chronic fatigue syndrome |
| Influenza | Fatigue, weakness, rare Guillain-Barré syndrome or encephalitis | Nervous system, lungs | Weeks to months | ~1–2% mostly severe cases |
| Coxsackievirus B | Myocarditis, fatigue, chronic inflammation | Heart, muscles | Weeks to lifelong | ~5–10% |
| Zika Virus | Guillain-Barré syndrome, neuropathy, fetal defects if pregnant | Nerves, brain (fetal/adult) | Weeks to lifelong |
<1% Guillain-Barré syndrome, neuropathy ~5–10% mild neurological symptoms |
| SARS / MERS | Lung damage, post-traumatic stress disorder, fatigue | Lungs, nervous system | Months to years | ~25–40% |
| RSV | Wheezing, asthma in kids, chronic cough | Lungs, airway | Months to years | ~30–50% of children with severe RSV |
| Measles | subacute sclerosing panencephalitis (very rare), immune suppression | Brain, immune system | Years later | Rare |
| Chickenpox | Shingles, nerve pain (post theraputic neuralgia) | Nerves, skin | Weeks to years |
20–30% get shingles; ~10–15% of those get postherpetic neuralgia |
Table 3.
Long COVID and COVID Studies. This Table Was Prepared by the Author.
|
COVID Treatments |
Long COVID Treatments |
|
| FDA clinical treatment trials | 6,000 | 545 |
| PubMed published papersa | 198,000 | 17,000b |
| The Mouse the Roaredpapersa | 3,800c | 269d |
| a. Procedures, drugs and nutrition. b. The number of papers is likely much smaller than c. 17,000, as many were just COVID. d. 14 drugs were approved by the FDA for US use. e. None was discovered during the pandemic. f. 179 unique Long COVID treatments. g. None have been FDA approved for US use. | ||
Table 4.
Long COVID Symptoms Assessed by FDA Clinical Trials. This Table Was Prepared by the Author.
Table 4.
Long COVID Symptoms Assessed by FDA Clinical Trials. This Table Was Prepared by the Author.
| Symptom | FDA Clinical Trial |
| Fatigue | 279 |
| Mental Health | 138 |
| Persistent Infection | 106 |
| Inflammation | 66 |
| Brain Fog | 63 |
| Antiviral | 51 |
| Gut Micro biodome | 16 |
| Microclotting | 14 |
| Cognitive Behavioral Therapy to Treat It | 12 |
| SSRI Antidepressants to Treat It | 12 |
| Auto Immune Diseases | 12 |
| Mitochondrial | 11 |
| Dementia | 10 |
Table 5.
Long COVID FDA Clinical Trials. This Table Was Prepared by the Author.
| Year |
Long COVID Trials Started |
| Pre 2020 | 2a |
| 2020 | 43 |
| 2021 | 120 |
| 2022 | 142 |
| 2023 | 155 |
| 2024 | 83 |
| 2025 - through 8/31 | 57 |
| a. This number demonstrates the frailty of the FDA clinical trial search program. One of the two studies was 2018. The other study said Long COVID, though Long COVID didn’t appear until mid 2020. | |
Table 6.
Number of Papers Describing a Treatment. This Table Was Prepared by the Author.
| Number of papers describing a treatment | Number of treatments |
| 6 | 1 |
| 5 | 1 |
| 4 | 1 |
| 3 | 6 |
| 2 | 18 |
| 1 | 107 |
Table 7.
Moderate Sized Trials.
| Procedures | |||
| Trial Size | Treatment | Improvement | |
| 50-99 | Fecal Transplant[146] Enhanced External Counter Pulsation[147] Spinal Cord Transcutaneous Stimulation & Respiratory Training[148] Digital Cognitive Training[149] Unified Phycological Protocol[150] Wearable Brain Activity Sensing Device[151] Trained With Orange, Lavender, Clove And Peppermint Oils[152,153] Contracting And Relaxing Pneumatic Cuffs 0n The Calves, Thighs, And Lower Hip[154] |
Sleep Broad Lung Fatigue And Concentration Broad Broad Broad Impact Broad Impact |
|
| 25-49 | Immunoadsorption[155] Vagus Nerve Stimulation[156,157,158] Transcutaneous Electrical Nerve Stimulation[159,160,161] Tragus Nerve Stimulation[162,163] Matt Pilates[164] Photobiomodulation[165,166] Stellate Ganglion Block[167,168,169,170,171] Ropinirole[172] Acupuncture[173] Expectation Management[174] |
Broad Broad Neurological Pain And Fatigue Broad Fatigue Pain And Fatigue Smell And Broad Restless Leg Syndrome Well Tolerated, No Measures On Outcomes Minor Broad |
|
| 10-24 | Dance[175] Aripiprazole[176] Continuous Positive Airway Pressure[177] Olfactory Training With Vitamin A[178] Functional Septorhinoplasty[179] Virtual Reality Training[180] Neuromodulation[181] |
Broad Reduced sleep duration Cognition No Impact Smell No Impact No Apparent Impact |
|
| 1-9 | Oronasal Drainage[182] Plasmapheresis[183,184] Light To Restore Circadian Rhythm[185] Neural Feedback[186] Plasma Exchange Therapy[187] |
Broad Cognition Sleep More Alert No Impact |
|
| Drugs | |||
| Trial Size | Treatment | Improvement | |
| 50-99 | Leronlimab[188] Sea Urchin Eggs[189] Co-UltraPEALut[190] Naltrexone[191,192,193] Antihistamines[194,195] Amantadine[196] Propranolol[197] Lithium[198] Metoprolol[199] Rintatolimod[200] Gabapentin[201] |
Inflammation Pain Memory & Fatigue Broad & Tremors Broad But Uneven Fatigue Orthostatic Hypotension No Improvement Cardiovascular No Impact No Impact |
|
| 25-49 | Valtrex + Celecoxib[202] AXA1125[203] Plasma[204,205] Treamid[206] Palmitoylethanolamide Co-Ultramicronized With Luteolin[207,208] Phosphatidylcholine[209] Aripiprazole[210] Hochuekkito[211] |
Broad Fatigue Smell Improved Lung Capacity Improved Smell Improved Inconclusive Reduced Sleep Needs Reduced Fatigue |
|
| 10-24 | Creatine[212] | Fatigue | |
| 1-9 | Casirivimab/Imdevimab[213] Nicotine Patch[214] Bupropion[215] Methylphenidate[216] Guanfacine[217] Intravascular Immunoglobulin Therapy[218] Ivabradine[219] Minocycline[220] Epipharyngeal Abrasive Therapy[221] |
Complete Remission Broad And Major Broad Broad Cognition Orthostatic Hypotension Orthostatic Hypotension Orthostatic Hypotension Cleared Viral RNA |
|
| Nutrients | |||
| Trial Size | Treatment | Improvement | |
| 50-99 | Nutritional Supplements Plus Exercise222 Ayurveda System Of Medicine[223] Astragalus Root Extract[224] Marine Oils[225] Endocalyx[226] Glycocalyx Dietary Supplement[227] |
Broad Diarrhea And Broad Fatigue Fatigue Cardiovascular Cardiovascular |
|
| 25-49 | Beet Juice[228,229] Probiotics[230,231] Maraviroc And Pravastatin[232] |
Fatigue And Sleep Inflammation Broad |
|
| 10-24 | Salmon Oil[233] Tinospora Cordifolia[234] |
Inflammation Inflammation |
|
Table 8.
No Human Trials.
| Procedures | ||
| Infrared light[235] | Cell cultures | Two ten minute exposures led to 80% IL-6 reduction in gene assay. |
| Hyperthermia[236] | Review/ hypothosis | Modulates necroinflammation. |
| Drugs | ||
| Tocilizumab[237] | Trial underway | Reduce inflammation |
| Baricitinib[238] | Trial underway | Reduce inflammation |
| Peptide LTI-2355[239] | Cell cultures | Mitigated inflammation in the respiratory tract. |
| CB2R agonists[240] | Hypothosis | Reduce inflammation |
| Ginkgolide B-loaded lubosomes And vesicular LNPS[241] | Human cell cultures | May protect against cell death |
| SPIKENET, SPK[242] |
Mice | Reversed the development of severe inflammation, oxidative stress, tissue edema, and animal death. Recall, vaccines in humans didn’t help. |
| Fermentable fiber[243] | Hypothesis | Reduce autoantibodies |
| Polyphenols[244] | Hypothesis | Reduce autoantibodies |
| Resveratrol[245] | Hypothesis | Reduce gut microdome dysfunction |
| Boost nicotinamide adenine dinucleotide (NAD+)[246] | Hypothesis | Reduce gut microdome dysfunction |
| Gamunex-C[247] | Proposed trial | Broad relief |
| Paracetamol and Dexketoprofen Trometamol[248] | Analytic technique | Broad relief when administered with rivaroxaban |
| Modafinil[249] | Literature search | Broad relief |
| Kyungok-go[250] | Proposed trial | Broad relief |
|
Cyclobenzapring Hydochloride[251] |
Company annoucement | Reduce pain and improved sleep |
| Ivabradine and midodrine[252] | Review of 32 studies | Reduced brain fog |
| Omega-3 fatty acids[252] | Review | Improve mental health |
| Aspartate or Asparagine[253,254] | Hypothosis | Improve vision |
| Macitentan[255] | Hamsters | Restored bone loss |
| Tanshinone IIA[256] | Chemical evaluation | Inflammation |
| Epigallocatechin-3-gallate-palmitate[257] |
Cell culture |
Neurological |
| Tuning Organelle Balance In Human Mesenchymal Stem Cell[258] | Cell Study | Major mitochondrial production |
| L-carnitine[259] | Theory | Fatigue |
| Niclosamide[260] | Review | Broad |
| Larazotide[261] | Proposed trial | Broad |
| Ecstasy[262] | FDA Vote | Too risky |
| Sodium Pyruvate Nasal Spray[263] | Proposed trial of drug useful in flu | Broad |
| Nutrients | ||
| Korean Herbs[264] | Mice cell cultures | Decreased nitrous oxide levels in some cell types. |
| Melatonin[265,266,267,268] | Hypothesis -3, Literature search | Reduce inflammation |
| Flavonoids Nobiletin & Eriodictyol[269] | Human cells | Reduced pathogen-stimulated release of inflammatory mediators. |
| Herbs[270] | Safety test | Broad improvements |
| Vitamin B12[271] | Hypothesis | Improve vision |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



