Submitted:
01 April 2025
Posted:
02 April 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background/Objectives: Recent studies brought evidence that the Long-Covid / post-COVID-19 Syndrome (PCS) and the related Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) have an autoimmune pathomechanism[1]. It could be triggered by various infectious pathogens, like SARS-CoV-2, which may be one of the most common triggering factors of the disease. The identification of increased levels of autoantibodies alleged with the typical symptom-constellation of post-exertional malaise, sleeping disorders, cognitive malfunction, postural orthostatic tachycardia syndrome (POTS), etc. and several subjective health problems can lead to the correct diagnosis. ME/CFS patients have a high suffering level. Making a correct diagnosis is challenging, as well as the therapy of the complex and individual constellation of physical and psychical symptoms. Methods: Our aim was to identify the ME/CFS patients correctly, including an initial rule-in screening by investigating other possible causes (pulmonal/cardial/endocrine, etc.). In 7 cases we applied plasmapheresis (PE) with repetitive autoantibody-measurements. Additionally, according to references from literature, for monitoring the clinical outcomes psychometric follow-up assessments had been conducted: with the ISI (insomnia), FSS (fatigue), HADS (depression and anxiety) and EQ-5D-5L (quality of life) questionnaires. Patients who met the inclusion criteria received 4 PE sessions on day 1, 5, 30 and 60 and a low-dose intravenous immunoglobulin (IVIG) therapy after each treatment. The psychometric evaluation had been conducted before the first PE, 2 weeks after the second and two weeks after the last PE-therapy. All 4 antibodies were measured two times per patient over the course of the study at standardized sampling time points: baseline before starting PE and 2 weeks after the last PE. Results: It could be found a negative correlation between the ꞵ-Adrenergic and M3-muscarinic receptor antibodies concentration and the quality of life measurements assessed with the EQ-5D-5L questionnaire. Conclusions: In this pilot study a correlation could be shown between the autoantibody-concentration and the physical and psychical wellbeing of the treated ME/CFS patients. These first results should be seen as a hypothesis-building assessment, further investigation is needed to validate these promising pilot-study results of therapeutic PE and IVIG in ME/CFS cases.
Keywords:
ME/CFS
; Long-COVID
; post-COVID-19
; plasmapheresis
; psychometrics
; G protein-coupled receptors
; quality of life
; ꞵ-Adrenergic receptor antibody
; M3-muscarinic receptor antibody
1. Introduction
The COVID-19 pandemic, caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has led to a global health crisis with profound immediate and long-term consequences. While the acute phase of COVID-19 has been well-documented, increasing attention is being directed toward the persistent, debilitating symptoms experienced by a subset of patients well beyond the initial infection period. These prolonged symptoms fall under the umbrella term Post-COVID-19 Syndrome (PCS), also referred to as Long COVID [1]. PCS encompasses a wide range of symptoms, including fatigue, exertion intolerance, cognitive impairment, orthostatic intolerance, and autonomic dysfunction, which can persist for months or even years after the acute infection has resolved [1].
Epidemiological studies suggest that approximately 5-10% of individuals who recover from the acute phase of COVID-19 develop PCS. The clinical presentation of PCS is highly variable, with symptoms overlapping significantly with those of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS)[1,2]. This overlap includes characterized symptoms such as profound fatigue, post-exertional malaise (PEM), myalgias and arthralgias, sleep disturbances, neurocognitive impairment, and autonomic dysregulation [1,2]. The pathophysiological mechanisms underlying PCS are complex and multifactorial, involving immune dysregulation, autoimmunity, endothelial dysfunction, viral persistence, and reactivation of latent viruses such as Epstein-Barr virus (EBV) [2].
Recent research has highlighted the role of immune activation and dysregulation in PCS, with several studies reporting the presence of autoantibodies, including those targeting G protein-coupled receptors (GPCRs) like the ß2-adrenergic receptor [1]. These autoantibodies have been associated with symptom severity and functional impairment in both PCS and ME/CFS [3]. Additionally, endothelial dysfunction, characterized by inflammation, microclots, and hypoperfusion has been identified as a significant contributor to the persistent symptoms observed in PCS [4].
Fatigue is a main symptom of PCS, it is in the literature well documented, that there are significant disturbances affecting numerous functions such as sleep, cognitive dysfunction, anxiety, depression, impairment of executive functions, psychomotor coordination. Patients with long COVID may suffer from brain hypometabolism, aligned with hypoperfusion of the cerebral cortex and changes in the brain structure and functional connectivity [5].
ME/CFS is not just significantly overlapping with PCS, recent studies implicate that the chronification of PCS could possibly fulfill the criteria of ME/CFS (one of the main diagnostics criteria of ME/CFS is an at least 6 months persistence of the symptoms) [6,7]. Therefore, further research is needed to find proof that there is not only a significant clinical and pathophysiological overlap, but shared therapeutic possibilities of ME/CFS and PCS could also exist. Despite growing knowledge about the mechanisms of PCS, unfortunately, there is limited evidence based data on effective curative therapies available today. In this observational study, we aimed to present how the wellbeing develops of our patients during and after the extracorporeal PE + IVIG treatments.
There are assumed to be three key steps underlying the initiation and persistence of ME/CFS [12]:
- Triggering Immune Response—An infection-induced immune response acts as the initial trigger, with B cells, plasma cells, and autoantibodies playing a role in the underlying pathology.
- Vascular and Autoantibody-Mediated Dysfunction—Autoantibodies, particularly those targeting GPCRs, may affect the vascular system, leading to endothelial dysfunction, impaired neurovascular control, and autonomic small nerve fiber involvement. These autoantibodies—whether pathogenic IgGs or functional autoantibodies that persist beyond the usual resolution—disrupt homeostasis. This disturbance manifests as endothelial dysfunction in both large and small arteries, impaired venous return, preload failure, and arteriovenous shunting, ultimately contributing to blood flow dysregulation and exertion-induced tissue hypoxia.
- Secondary Compensatory Mechanisms—In response, the body adopts compensatory adaptations, including increased sympathetic tone and metabolic shifts aimed at maintaining energy supply. These adaptations further shape the clinical presentation and symptomatology of ME/CFS.
There are numerous potential therapeutic strategies targeting these pathways [3]:
-
Interfere with the pathological immune response:
- with B-cell depletion therapy (anti-CD20 antibody)
- use of cytotoxic drugs (cyclophosphamide)
- modulate the plasma cell survival factors (Anti BAFF antibody)
- Plasma cell inhibition (Anti-CD38 antibody, proteasome inhibition)
- or through Immunoglobulin manipulation (neonatal fragment crystallizable receptor (FcRn) targeting, immunoadsorption, IVIG)
- Address the vascular dysregulation: endothelial dysfunction, arteriovenous shunting, impaired autoregulation (plasmapheresis had been proven to improve endothelial dysfunction in critically ill patients with Disseminated intravascular coagulation (DIC) [12])
- Support the patient’s compensatory adaptation by pacing therapy [13], acetylcholinesterase inhibition or cognitive techniques.
Our study group decided to address all three major potential therapeutic strategies of the ME/CFS patients, firstly by applying plasmapheresis for improving the endothelial dysfunction and platelet function, secondly in term of administering IVIG to regulate the derailed, inadequate immune response, and thirdly by performing pacing therapy to support the compensatory adaptation mechanisms.
Even if there is no reliable research data at the current date that PE could improve the clinical outcome by extracting the microclots [14] that have been identified in PCS and ME/CFS patients, it has been proven that PE can reduce IgG levels [15] and can improve endothelial dysfunction and platelet function [12]. Given the better availability and lower cost of PE than immunoadsorption, positive results with PE-technique could provide a treatment option even for lower-income countries in demanding need for ME/CFS therapy.
2. Materials and Methods
2.1. Study Protocol
Adult patients (≥18 years) with elevated autoantibodies (ꞵ1, ꞵ2, M3, M4), measured between January 2023 and September 2024, were enrolled in this pilot study at a Swiss tertiary care hospital. The patients had typical chronic fatigue symptoms like exertion intolerance, post-exertional malaise, orthostatic dysregulation, concentrating difficulty, brain fog, headache, insomnia, high resting pulse, some even elevated body temperature or pain. We worked together with the Outpatient Clinic of Internal Medicine (Long COVID consultation) and the Clinic of Nephrology and Transplant Medicine (extracorporeal therapies, i.e., PE).
The patients went through a comprehensive work-up before being referred to plasmapheresis. Other possible causes that can mimic ME/CFS-symptoms have been ruled out: cardiac testing by echocardiography, in some cases also bicycle ergometry or cardiac MRI. Testing for early-onset neurodegenerative diseases by functional testing with the Montreal Cognitive Assessment (MoCA) and/or neuroimaging cerebral computed tomography (CT) or cerebral magnetic resonance imaging (cMRI) scans to rule out demyelinating diseases. Functional pulmonary testing by body plethysmography and carbon monoxide (CO) diffusing capacity testing have been performed, in a few cases also chest imaging to assess possible pulmonary embolism, and sleep apnea screening for rule-out this possibility as well. Every patient completed a 6-minute walk test (6MWT) and a Schellong test as a baseline assessment. Some patients had been examined for possible gastrointestinal, rheumatological, and for other neurologic causes of their symptoms.
Prior to the referral for PE, the patients were individually treated with various conservative therapeutic measures (professionally instructed pacing therapy, physiotherapy, psychotherapy, tricyclic antidepressive, Serotonin–norepinephrine reuptake inhibitors (SNRIs), selective serotonin reuptake inhibitors (SSRIs), H1-antihistaminergic agents, ritaline, antiepileptics, naloxone, and in some cases even inpatient rehabilitation).
Inclusion criteria were clinically diagnosed CFS/ME with elevated GPCRs. Other pilot studies have shown an effect of repeated immunoadsorption on CFS/ME patients [2], therefore we decided to perform PE with intravenous immunoglobulin (IVIG)- infusions as in the Kiprov-case [16] as an off-label therapy. This method could also remove the autoantibodies and may remove the microclots as well. Newest research implicates that in ME/CFS cases a dysregulation of the coagulation system is present, the endothelial dysfunction, and the downregulation of complement machinery can be assessed on a molecular level [17].
However, there are some raising concerns about the pathophysiological role of microclots in developing ME/CFS, implying that microclots do not play a significant role in the pathomechanism [14].
For PE, we used the machine Spectra Terumo Optia Apheresis System. For the exchange we gave albumin 5%, one time of the plasma volume. A total of 4 treatments (on day 1 and 5, and in 1 to 4 months interval) were performed. We measured the autoantibodies before and two weeks after the fourth (in two cases after the third) plasma exchange. At the Outpatient Clinic of Internal Medicine the patients received standardized tests for the assessment of physical function and symptoms in a standardized manner (interdisciplinary workflow, Table 1).
At the end of every PE session the patients received additionally 2 Grams of OctagamⓇ intravenous independently of their body weight. Human immunoglobulins are meant to have an immunomodulatory and immunosuppressive effect, even in low dosage [18].
All of the patients were regularly monitored at the Long COVID Consultation during and after the series of 4 plasma exchange therapies. All of the collected data was documented in the patient management system (PMS) of our hospital.
The ISI (Insomnia Severity Index), FSS (Fatigue Severity Scale), HADS (Hospital Anxiety and Depression Scale) and EQ-5D-5L (European Quality of Life 5 Dimensions 5 Level Version) questionnaires had been applied to assess the symptoms of the patients with standardized methods. The EQ-5D-5L questionnaire has been developed by the EuroQol Group and it is a well studied tool for assessing the Quality of Life. The EQ-5D-5L descriptive system comprises five dimensions (mobility, self-care, usual activities, pain / discomfort and anxiety / depression). Each dimension has five response levels: no problems, slight problems, moderate problems, severe problems, unable to/extreme problems. The index-value is calculated by deducting the appropriate weights from 1, the value for full health [19].
2.2. Study Procedure and Data Collection
All four autoantibodies were measured two times per patient over the course of the study at the measurement time points: baseline before starting PE, and 2 weeks after the last PE. Clinical outcomes–consisting of the 6MWT, Schellong test, as well as psychometric assessments with the ISI (insomnia), FSS (fatigue), HADS (depression and anxiety) and EQ-5D-5L (quality of life) questionnaires–were measured three times at T1, T2, and T3. See Appendix A Table A1 for psychometric properties of the validated questionnaires used in this study.
2.3. Statistical Analyses
Concerning a potential main trial, the study design requires a total of 56 patients for an expected 80% statistical power based on an a-priori power analysis calculated with the SIMR package v.1.0.7 using Monte Carlo simulations [27]. The power analysis is based on a multilevel model (MLM) with two measurement time points for each patient and each of the two investigated variables, namely antibody concentration and clinical outcome measures. We expected a medium to large effect size R2 of 0.16 as comparable studies investigating the effect of plasma exchange treatments in ME/CFS patients with elevated β2-adrenergic receptor autoantibodies [28], and adrenergic dysfunction in ME/CFD patients [29] reported medium to large effect sizes. Cocks and Torgerson (2013) recommend having at least 9% of the sample size of the main planned trial when conducting a pilot study, resulting in 5 patients for the present pilot study [30].
Statistical analyses were performed using R Project for Statistical Computing v4.4.2 [31]. After inspecting incomplete data by using the VIM package v6.2.2 [32], we imputed missing values with the MICE package v3.17.0 based on the multivariate imputation by chained equations algorithm for the missing at random (MAR) scenario [33]. After imputation, we evaluated the imputed data using convergence diagnostic tools such as trace and density plots. Estimates of model parameters and weights obtained in the imputed datasets were further pooled over all imputations according to Rubin’s rule [34]. All statistical models were two-sided and based on a significance level of 5% (alpha = 0.05) [35].
To investigate the association between repeat-measured antibodies and clinical outcomes–both measured twice per patient–we created a MLM using the LME4 package v1.1-36 [36]. MLM is superior to the repeated-measures correlation (rmcorr) analysis when dealing with small sample sizes and data models with both random intercepts and slopes [36]. We considered Bonferroni correction for multiple testing [37]. Standardized beta coefficients of all MLM comparisons were visualized through a heatmap plot and use of the GPLOTS package v3.2.0 [38].
We further compared clinical outcomes across three measurement time points with one-way (time) repeated-measures analysis of variance (rmANOVA). Creating linear mixed-effects models (LMM) using the LME4 package v1.1-36, we controlled random subject effects [36]. We used Mauchly’s test of sphericity to test clinical outcome data for normality [35] and visualized data through box plots generated with the GGPLOT2 package v3.5.1 [39]. Concerning the EQ-5D-5L questionnaire we used the eq5d package v0.15.2 to calculate the index score based on a reference German population as there was no Swiss population available [40,41].
3. Results
This pilot study with a statistical power of 10% included seven patients with five being male and two being female. Their mean age was 45 ± 10.13 years with a range between 30 and 57 years.
Due to time constraints, two patients prematurely terminated the study after T1 and T2, lacking two-thirds and one-third of clinical outcome data, respectively. One of these two patients lacked antibody data at the end of therapy. The missing values of these patients were further imputed and included in the analyses. Across all MLM comparisons between antibodies and clinical outcomes, there were two statistically significant associations: Higher concentrations of β2-adrenergic receptor antibodies (R2 =.32, t(504) = -2.46, p = .014*) and M3-muscarinic acetylcholine receptor antibody (R2 = .46, t(110) =-3.17, p = .002**) were both relevant predictors of a lower and therefore worse EQ-5D-5L index score.
However, these results did not remain statistically significant after Bonferroni adjustment for multiple testing. Table 2 shows detailed results of all MLM comparisons between antibodies and clinical outcomes measured at T1 and T3, while Figure 1 illustrates all MLM comparisons using a heatmap plot.
There were no statistically significant improvements in clinical outcomes across T1, T2, and T3. However, we found trends towards improvement of health-related quality of life measured with the index score of the EQ-5D-5L questionnaire. See Table 3 for detailed results of the rmANOVA of clinical outcomes over the course of the study. Figure 2 shows unimputed clinical outcomes over the course of the study, measured at T1, T2, and T3 using box plots.
4. Discussion
4.1. Patient Selection
In this pilot study we focused on the central entity ME/CFS, regardless of the presumed triggering factor. It has been proven that ME/CFS is a constellation of symptoms, a well-defined clinical state that could be evoked by several different catalysts. In this chapter we discuss the choice of therapy in this pilot study, namely the combination of PE followed by low-dose IVIG-administration after each session.
- Reasons for IVIG-administration
IVIG is a highly purified concentrate of immunoglobulins, primarily IgG, derived from the pooled plasma of 1,000 to 100,000 healthy donors. Its composition reflects the diverse immunological exposures and antibody repertoires of the donor population. This gives IVIG its broad functionality and utility in both immunodeficiency and autoimmune conditions.[42] ME/CFS patients could benefit from the so-called anti-idiotype antibodies, which neutralize pathogenic autoantibodies and restore immune balance. Furthermore, there are immunomodulatory effects, IVIG impacts immune regulation by modulating both the innate and adaptive arms of the immune system. It can bind to Fc receptors, interact with complement proteins, and neutralize pro-inflammatory mediators, making it effective in autoimmune and inflammatory diseases.[43]
There are various immunomodulatory effects of intravenous immunoglobulins, that can be summarized as follows:
Inhibition of Monocyte and Macrophage Activation: IVIG reduces the activation of monocytes and macrophages. It induces anti-inflammatory cytokines from innate immune cells. Decreases macrophage responsiveness to interferon, dampening inflammatory responses.[18]
Cytotoxicity to Neutrophils and Eosinophils: IVIG exerts cytotoxic effects on neutrophils and eosinophils. This shifts the immune environment from pro-inflammatory to anti-inflammatory.
Expansion of Regulatory T Cells: IVIG enhances immunosuppressive effects by expanding the population of regulatory T cells, promoting immune tolerance.
Suppression of B-Lymphocytes: IVIG suppresses the proliferation of B lymphocytes, reducing antibody production. It also suppresses autoreactive B lymphocytes and neutralizes their cytokines, mitigating autoimmunity.
Modulation of Endothelial Cells: IVIG influences endothelial cell proliferation and adhesion molecule expression in vascular lumens. This leads to an anti-inflammatory effect, particularly beneficial in vascular disorders.[44]
This combination of mechanisms allows IVIG to effectively modulate cellular immunity and combat a range of autoimmune and inflammatory conditions, furthermore it can address the endothelial dysfunction, which is consumed to play a major role in the pathogenesis of Long-COVID and ME/CFS.
- Plasma exchange for removing micro-clots
The discussion of the major problems was on the one hand the autoantibodies, on the other hand the micro-clots that was found at the Stellenbosch University in South Africa [45]. A summary from 2023 could not prove that the micro-clots are responsible for the symptoms [14]. There again we know that plasma-exchange can improve microcirculation. In this correlation, we decided to perform plasma-exchange, with the hypothesis to put out the micro-clots and the autoantibodies at once.
Other studies observed significant correlations between the levels of most antibodies and key symptoms such as fatigue and muscle pain in patients with an infection-triggered onset. Cognitive impairment severity was associated with AT1-R(angiotensin-1 receptor)-antibody and ETA-R-AAB (Endothelin-1 type A receptor antibody), while gastrointestinal symptom severity correlated with anti-adrenergic α1/2 receptor antibody (alpha1/2-AdR-AAB). In contrast, patients with non-infection-triggered ME/CFS exhibited fewer and distinct correlations [9].
4.2. Data Collection and Patient Compliance
Working with ME/CFS patients can be challenging. The core symptom, the post-exertional malaise (the so-called “crushes”) could interfere with the adequate data collection, even if the study group works with a well-established study protocol. Some of the patients suffered from recurring post-exertional malaise after the conduction of 6MWT. Therefore our study group decided to cease the 6MWT for the wellbeing of our patients. Consequently, the 6MWT dataset was not eligible for statistical analysis. ME/CFS itself, due to its main clinical manifestation characterized by exertion intolerance and the post-exertional malaise poses a huge challenge for adequate data collecting. Sometimes during the crushes, ME/CFS patients have to cancel consultations or a blood test because of the major malaise. This can negatively impact the exact sample collection. One patient had to be excluded because of lacking baseline and follow-up clinical outcome data. 2 patients could be analyzed after data imputation.
4.3. Subjective Experience of Patients
Most patients reported a subjective benefit after the first PE + IVIG therapy, however it could be observed that many of them were crushed after the second round. This deterioration of the clinical status led to premature termination of the therapy in 3 cases. During the 4 treatments most patients experienced a gradual improvement in their symptoms. 5 of a total of 7 patients reported a subjective benefit after the PE therapy.
4.4. Vascular Access
Vascular access is often a subject of discussion related to extracorporeal therapies. Among the seven enclosed patients, five have had peripheral venous access, inserted directly before the PE. Two of them needed a central venous catheter for the PE, one of them was reported to have been infected and therefore must have been prematurely extracted. All therapies have been performed in an outpatient-setting.
5. Conclusions
Our study has identified a significant association between elevated levels of ꞵ2-adrenergic receptor antibodies and M3-receptor antibodies in patients with post-COVID syndrome. The data indicate that higher concentrations of these autoantibodies are associated with a deterioration in quality of life, highlighting their potential role in the pathophysiology of this condition.
Five of seven patients reported an explicit benefit after the treatments. Even though these subjective patient-experiences are not suitable for statistical analysis, they gave us a confirming hint that our statistical evaluations are correlating with the beneficial clinical outcome of our patients.
To mitigate the effects of these autoantibodies, we implemented plasma exchange as a therapeutic intervention, successfully reducing their levels in patients. Following each plasma exchange procedure, we administered 2g of human immunoglobulin (Octagam) to support the immune system and replenish necessary antibodies. This approach not only aims to alleviate symptoms associated with autoantibody-mediated dysfunction but also to provide a protective effect against potential infections.
However, our findings suggest that additional therapeutic strategies may be warranted for these patients. Specifically, B cell depletion therapy could further reduce the production of these harmful autoantibodies and enhance overall treatment efficacy. By integrating plasma exchange, human immunoglobulin administration, and B cell-targeted therapies, we may be able to significantly improve the quality of life for individuals suffering from ME/CFS. Future studies are needed to validate these therapeutic strategies and optimize management approaches for this complex and challenging condition.
Author Contributions
Conceptualization: Boglárka Oesch-Régeni, Georg Hafer, Norbert Arn; Methodology: Georg Hafer, Dagmar Schmid , Norbert Arn; software: Nicolas Germann; validation: Georg Hafer, Dagmar Schmid, Norbert Arn, formal analysis: Boglárka Oesch-Régeni, Nicolas Germann; investigation: Boglárka Oesch-Régeni, Norbert Arn, resources,: Boglárka Oesch-Régeni, Nicolas Germann, Norbert Arn; data curation: Nicolas Germann, Boglárka Oesch-Régeni; writing-original draft preparation: Boglárka Oesch-Régeni, Nicolas Germann; writing—review and editing: Georg Hafer, Dagmar Schmid , Norbert Arn; visualization: Nicolas Germann; supervision: Georg Hafer, Dagmar Schmid , Norbert Arn; project administration: Norbert Arn.
Funding
This research received no external funding.
Informed Consent Statement
Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
Research data is available at: https://dx.doi.org/10.6084/m9.figshare.28692593.
Acknowledgments
We acknowledge technical support of the Clinic of Nephrology and Transplant Medicine, HOCH Health Ostschweiz Cantonal Hospital St. Gallen, Switzerland, to provide us the infrastructure of the Dialysis Unit where all plasmapheresis treatments have been conducted.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following supporting information can be downloaded at: https://dx.doi.org/10.6084/m9.figshare.28692593.
The following abbreviations are used in this manuscript:
| 6MWT | 6-minute walk test |
| ACTH | adrenocorticotropic hormone |
| AT1-R | angiotensin-1 receptor |
| CO | carbon monoxide |
| CRH | corticotropin releasing hormone |
| CT | computed tomography |
| DIC | Disseminated intravascular coagulation |
| EBV | Epstein-Barr virus |
| EQ-5D-5L | European Quality of Life 5 Dimensions 5 Level Version |
| ETA-R-AAB | Endothelin-1 type A receptor antibody |
| FcRn | neonatal fragment crystallizable receptor |
| FSS | Fatigue Severity Scale |
| GPCRs | G protein-coupled receptors |
| HADS | Hospital Anxiety and Depression Scale |
| IGF-1 | Insulin-like growth factor 1 |
| IGF-2 | Insulin-like growth factor 2 |
| ISI | Insomnia Severity Index |
| IVIG | intravenous immunoglobulin |
| LMM | linear mixed-effects models |
| ME/CFS | Myalgic Encephalomyelitis/Chronic Fatigue Syndrome |
| MLM | multilevel model |
| MoCA | Montreal Cognitive Assessment |
| PCS | Long-Covid / post-COVID-19 Syndrome |
| PE | plasmapheresis/ plasma exchange |
| PEM | post-exertional malaise |
| POTS | postural orthostatic tachycardia syndrome |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| SNRIs | Serotonin–norepinephrine reuptake inhibitors |
| SSRIs | selective serotonin reuptake inhibitors |
| alpha1/2-AdR-AAB | anti-adrenergic α1/2 receptor antibody |
Appendix A

Table A1.
Interdisciplinary workflow, patient management, and consultations during the study.
| 1. | Outpatient Clinic of Department of Internal Medicine Consultation of Long COVID |
Relevant laboratory results:β1-adrenergic receptor antibody, β2-adrenergic receptor antibody, M3-muscarinic acetylcholine-receptor-antibody, M4-muscarinic acetylcholine-receptor-antibody, Standardized tests Schellong test, 6MWT with Borg-Score, echocardiography, pulmonal functional tests, psychiatric evaluation, EQ-5D-5L Health VAS, EQ-5D-5L, HADS Anxiety, HADS Depression, ISI, FSS, IES-R If the detected autoantibodies showed a relevant elevation, the patients had been assigned to the apheresis consultation. |
| 2. | Consultation Apheresis at the Clinic of Nephrology and Transplant Medicine | The patients were informed about all side effects and complications of the plasma exchange and albumin application. |
| 3. | 1st plasma exchange | Clinical visit Nephrology |
| 4. | 2nd plasma exchange after 5 days | Clinical visit Nephrology |
| 5. | Back to Consultation of Long COVID within 2 weeks | Clinical visit and standardized tests Internal Medicine |
| 6. | 3rd plasma exchange after 1 month | Clinical visit Nephrology |
| 7. | Back to Consultation of Long COVID within 8 weeks | Clinical visit and standardized tests Internal Medicine |
| 8. | 4th plasma exchange after 1 month | Clinical visit Nephrology |
| 9. | Back to Consultation of Long COVID within 2 weeks | Clinical visit, laboratory and standardized tests, follow up |
Table A2.
Psychometric properties of the validated questionnaires completed at three measurement time points (T1, T2, T3).
Table A2.
Psychometric properties of the validated questionnaires completed at three measurement time points (T1, T2, T3).
| Outcome | Questionnaire / reference | Score building / range / cut-off / (sub)scale |
| Insomnia | ISI (Insomnia Severity Index) [20,21] | Sum score / 0 to 28 / ≥ 15 / global |
| Fatigue | FSS (Fatigue Severity Scale) / [22,23] | Sum score / 9 to 63 / ≥ 36 / global |
| Depression and anxiety | HADS (Hospital Anxiety and Depression Scale) / [24,25] | Sum score / 0 to 21 / ≥ 8 / depression Sum score / 0 to 21 / ≥ 8 / anxiety |
| Health-related quality of life | EQ-5D-5L (European Quality of Life 5 Dimensions 5 Level Version) / [26] | Visual analogue scale score / 0 to 100 / no cut-off / current health Index score / -0.59 to 1 / no cut-off / Quality of life consisting of five dimensions; mobility, self-care, usual activities, pain/discomfort, anxiety/depression |
References
- E. Stein u. a., „Observational Study of Repeat Immunoadsorption (RIA) in Post-COVID ME/CFS Patients with Elevated ß2-Adrenergic Receptor Autoantibodies—An Interim Report“, J. Clin. Med., Bd. 12, Nr. 19, 2023. [CrossRef]
- C. Scheibenbogen u. a., „Fighting Post-COVID and ME/CFS—development of curative therapies“, Front. Med., Bd. 10, S. 1194754, Juni 2023. [CrossRef]
- Ø. Fluge, K. J. Tronstad, und O. Mella, „Pathomechanisms and possible interventions in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS)“, J. Clin. Invest., Bd. 131, Nr. 14, S. e150377. [CrossRef]
- M. K. Sandvik u. a., „Endothelial dysfunction in ME/CFS patients“, PloS One, Bd. 18, Nr. 2, S. e0280942, 2023. [CrossRef]
- J. B. Zawilska und K. Kuczyńska, „Psychiatric and neurological complications of long COVID“, J. Psychiatr. Res., Bd. 156, S. 349–360, Dez. 2022. [CrossRef]
- T. L. Wong und D. J. Weitzer, „Long COVID and Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS)—A Systemic Review and Comparison of Clinical Presentation and Symptomatology“, Medicina (Mex.), Bd. 57, Nr. 5, S. 418, Apr. 2021. [CrossRef]
- S. Morita u. a., „Phase-dependent trends in the prevalence of myalgic encephalomyelitis / chronic fatigue syndrome (ME/CFS) related to long COVID: A criteria-based retrospective study in Japan“, PLOS ONE, Bd. 19, Nr. 12, S. e0315385, Dez. 2024. [CrossRef]
- L. Komaroff und W. I. Lipkin, „ME/CFS and Long COVID share similar symptoms and biological abnormalities: road map to the literature“, Front. Med., Bd. 10, S. 1187163, Juni 2023. [CrossRef]
- H. Freitag u. a., „Autoantibodies to Vasoregulative G-Protein-Coupled Receptors Correlate with Symptom Severity, Autonomic Dysfunction and Disability in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome“, J. Clin. Med., Bd. 10, Nr. 16, S. 3675, Aug. 2021. [CrossRef]
- Szewczykowski u. a., „Long COVID: Association of Functional Autoantibodies against G-Protein-Coupled Receptors with an Impaired Retinal Microcirculation“, Int. J. Mol. Sci., Bd. 23, Nr. 13, S. 7209, Juni 2022. [CrossRef]
- Kruger u. a., „Proteomics of fibrin amyloid microclots in long COVID/post-acute sequelae of COVID-19 (PASC) shows many entrapped pro-inflammatory molecules that may also contribute to a failed fibrinolytic system“, Cardiovasc. Diabetol., Bd. 21, Nr. 1, S. 190, Sep. 2022. [CrossRef]
- J. Weng, M. Chen, D. Fang, D. Liu, R. Guo, und S. Yang, „Therapeutic Plasma Exchange Protects Patients with Sepsis-Associated Disseminated Intravascular Coagulation by Improving Endothelial Function“, Clin. Appl. Thromb. Off. J. Int. Acad. Clin. Appl. Thromb., Bd. 27, S. 10760296211053313, 2021. [CrossRef]
- N. E. M. Sanal-Hayes u. a., „A scoping review of ‚Pacing‘ for management of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS): lessons learned for the long COVID pandemic“, J. Transl. Med., Bd. 21, Nr. 1, S. 720, Okt. 2023. [CrossRef]
- T. Fox u. a., „Plasmapheresis to remove amyloid fibrin(ogen) particles for treating the post-COVID-19 condition“, Cochrane Database Syst. Rev., Bd. 7, Nr. 7, S. CD015775, Juli 2023. [CrossRef]
- E. Cervantes, E. M. Bloch, und C. J. Sperati, „Therapeutic Plasma Exchange: Core Curriculum 2023“, Am. J. Kidney Dis., Bd. 81, Nr. 4, S. 475–492, Apr. 2023. [CrossRef]
- D. Kiprov u. a., „Case Report: Therapeutic and immunomodulatory effects of plasmapheresis in long-haul COVID“, F1000Research, Bd. 10, S. 1189, 2021. [CrossRef]
- M. Nunes, M. Vlok, A. Proal, D. B. Kell, und E. Pretorius, „Data-independent LC-MS/MS analysis of ME/CFS plasma reveals a dysregulated coagulation system, endothelial dysfunction, downregulation of complement machinery“, Cardiovasc. Diabetol., Bd. 23, Nr. 1, S. 254, Juli 2024. [CrossRef]
- V. B. Arumugham und A. Rayi, „Intravenous Immunoglobulin (IVIG)“, in StatPearls, Treasure Island (FL): StatPearls Publishing, 2025. Zugegriffen: 22. Januar 2025. [Online]. Verfügbar unter: http://www.ncbi.nlm.nih.gov/books/NBK554446/.
- „EQ-5D-5LUserguide-23-07.pdf“. Zugegriffen: 16. Februar 2025. [Online]. Verfügbar unter: https://euroqol.org/wp-content/uploads/2023/11/EQ-5D-5LUserguide-23-07.pdf.
- C. M. Morin u. a., „Effect of Psychological and Medication Therapies for Insomnia on Daytime Functions: A Randomized Clinical Trial“, JAMA Netw. Open, Bd. 6, Nr. 12, S. e2349638, Dez. 2023. [CrossRef]
- Dieck, C. M. Morin, und J. Backhaus, „A German version of the Insomnia Severity Index: Validation and identification of a cut-off to detect insomnia“, Somnologie, Bd. 22, Nr. 1, Art. Nr. 1, März 2018. [CrossRef]
- L. B. Krupp, „The Fatigue Severity Scale: Application to Patients With Multiple Sclerosis and Systemic Lupus Erythematosus“, Arch. Neurol., Bd. 46, Nr. 10, Art. Nr. 10, Okt. 1989. [CrossRef]
- P. O. Valko, C. L. Bassetti, K. E. Bloch, U. Held, und C. R. Baumann, „Validation of the Fatigue Severity Scale in a Swiss Cohort“, Sleep, Bd. 31, Nr. 11, Art. Nr. 11, Nov. 2008. [CrossRef]
- S. Zigmond und R. P. Snaith, „The Hospital Anxiety and Depression Scale“, Acta Psychiatr. Scand., Bd. 67, Nr. 6, Art. Nr. 6, Juni 1983. [CrossRef]
- Petermann, „Hospital Anxiety and Depression Scale, Deutsche Version (HADS-D)“, Z. Für Psychiatr. Psychol. Psychother., Bd. 59, Nr. 3, Art. Nr. 3, Juli 2011. [CrossRef]
- M. Herdman u. a., „Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L)“, Qual. Life Res., Bd. 20, Nr. 10, Art. Nr. 10, Dez. 2011. [CrossRef]
- P. Green und C. J. MacLeod, „SIMR : an R package for power analysis of generalized linear mixed models by simulation“, Methods Ecol. Evol., Bd. 7, Nr. 4, Art. Nr. 4, Apr. 2016. [CrossRef]
- Stein u. a., „Efficacy of repeated immunoadsorption in patients with post-COVID myalgic encephalomyelitis/chronic fatigue syndrome and elevated β2-adrenergic receptor autoantibodies: a prospective cohort study“, Lancet Reg. Health - Eur., Bd. 49, S. 101161, Feb. 2025. [CrossRef]
- J. Hendrix u. a., „Adrenergic dysfunction in patients with myalgic encephalomyelitis/chronic fatigue syndrome and fibromyalgia: A systematic review and meta-analysis“, Eur. J. Clin. Invest., Bd. 55, Nr. 1, Art. Nr. 1, Jan. 2025. [CrossRef]
- K. Cocks und D. J. Torgerson, „Sample size calculations for pilot randomized trials: a confidence interval approach“, J. Clin. Epidemiol., Bd. 66, Nr. 2, S. 197–201, Feb. 2013. [CrossRef]
- Team R. Core. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. Online: http://www. R-project. org. 2013;201. .
- M. Templ, A. Kowarik, A. Alfons, G. De Cillia, und W. Rannetbauer, „VIM: Visualization and Imputation of Missing Values“. S. 6.2.2, 11. Oktober 2012. [CrossRef]
- S. V. Buuren und K. Groothuis-Oudshoorn, „mice : Multivariate Imputation by Chained Equations in R“, J. Stat. Softw., Bd. 45, Nr. 3, Art. Nr. 3, 2011. [CrossRef]
- D. B. Rubin und N. Schenker, „Multiple imputation in health-are databases: An overview and some applications“, Stat. Med., Bd. 10, Nr. 4, Art. Nr. 4, Apr. 1991. [CrossRef]
- Field, Discovering statistics using IBM SPSS statistics, 6th edition. Los Angeles London New Delhi Singapore Washington DC Melbourne: Sage, 2024.
- D. W. Bates, S. Saria, L. Ohno-Machado, A. Shah, und G. Escobar, „Big data in health care: using analytics to identify and manage high-risk and high-cost patients“, Health Aff. Proj. Hope, Bd. 33, Nr. 7, S. 1123–1131, Juli 2014. [CrossRef]
- R. A. Armstrong, „When to use the B onferroni correction“, Ophthalmic Physiol. Opt., Bd. 34, Nr. 5, Art. Nr. 5, Sep. 2014. [CrossRef]
- R. Warnes u. a., „gplots: Various R Programming Tools for Plotting Data“. S. 3.2.0, 30. Mai 2005. [CrossRef]
- Wickham, „ggplot2“, WIREs Comput. Stat., Bd. 3, Nr. 2, Art. Nr. 2, März 2011. [CrossRef]
- F. Morton und J. S. Nijjar, „eq5d: Methods for Analysing ‚EQ-5D‘ Data and Calculating ‚EQ-5D‘ Index Scores“. S. 0.15.6, 22. Mai 2019. [CrossRef]
- K. Ludwig, J.-M. Graf von der Schulenburg, und W. Greiner, „German Value Set for the EQ-5D-5L“, PharmacoEconomics, Bd. 36, Nr. 6, S. 663–674, Juni 2018. [CrossRef]
- F. Barahona Afonso und C. M. P. João, „The Production Processes and Biological Effects of Intravenous Immunoglobulin“, Biomolecules, Bd. 6, Nr. 1, S. 15, März 2016. [CrossRef]
- R. J. Ludwig u. a., „Mechanisms of Autoantibody-Induced Pathology“, Front. Immunol., Bd. 8, S. 603, 2017. [CrossRef]
- C. Xu u. a., „Modulation of endothelial cell function by normal polyspecific human intravenous immunoglobulins: a possible mechanism of action in vascular diseases“, Am. J. Pathol., Bd. 153, Nr. 4, S. 1257–1266, Okt. 1998. [CrossRef]
- E. Pretorius u. a., „Persistent clotting protein pathology in Long COVID/Post-Acute Sequelae of COVID-19 (PASC) is accompanied by increased levels of antiplasmin“, Cardiovasc. Diabetol., Bd. 20, Nr. 1, S. 172, Aug. 2021. [CrossRef]
Figure 1.
Standardized beta coefficients showing the association between repeated-measured antibodies and clinical outcomes (T1 and T3) using a heatmap plot. Legend 1. Heatmap consisting of predictor variables (x-axis), endpoints (y-axis), standardized beta coefficients (red for coefficients close to −1, blue for coefficients close to +1), and p-values (inside the heatmap plot). The terms “ACh” and “RAb” as predictor labels stand for “Acetylcholine” and “Receptor Antibody”, respectively. Next to the endpoints, green and red triangles show that higher scores indicate better or worse outcomes, respectively.
Figure 1.
Standardized beta coefficients showing the association between repeated-measured antibodies and clinical outcomes (T1 and T3) using a heatmap plot. Legend 1. Heatmap consisting of predictor variables (x-axis), endpoints (y-axis), standardized beta coefficients (red for coefficients close to −1, blue for coefficients close to +1), and p-values (inside the heatmap plot). The terms “ACh” and “RAb” as predictor labels stand for “Acetylcholine” and “Receptor Antibody”, respectively. Next to the endpoints, green and red triangles show that higher scores indicate better or worse outcomes, respectively.
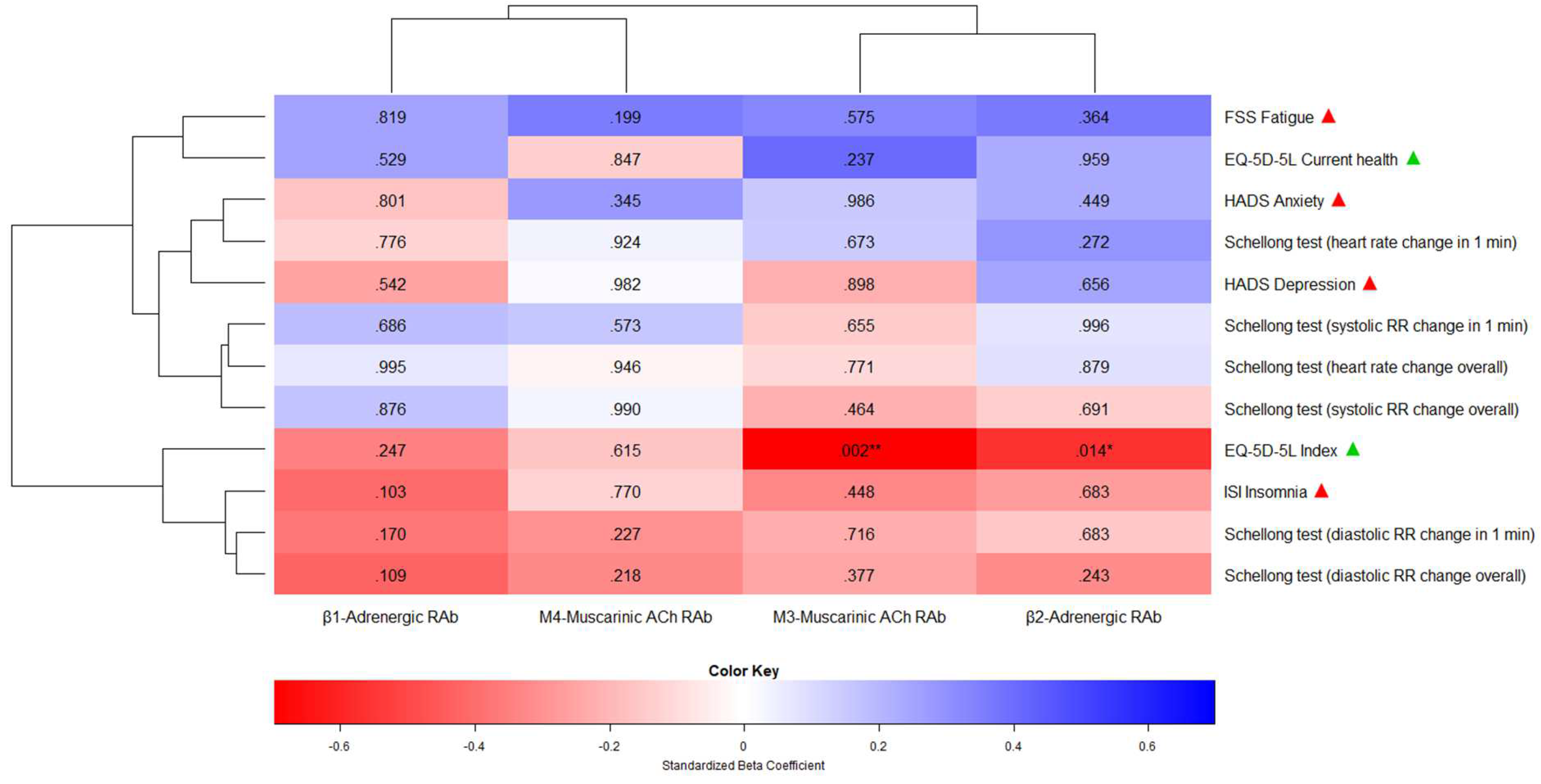
Figure 2.
Change of repeated-measured clinical outcomes (T1, T2, and T3) using box plots. Legend 2. In each box plot, solid and dashed lines indicate median and mean values, respectively. Next to the main title of the boxplot, green and red triangles show that higher scores indicate better or worse outcomes of the clinical outcomes, respectively.
Figure 2.
Change of repeated-measured clinical outcomes (T1, T2, and T3) using box plots. Legend 2. In each box plot, solid and dashed lines indicate median and mean values, respectively. Next to the main title of the boxplot, green and red triangles show that higher scores indicate better or worse outcomes of the clinical outcomes, respectively.
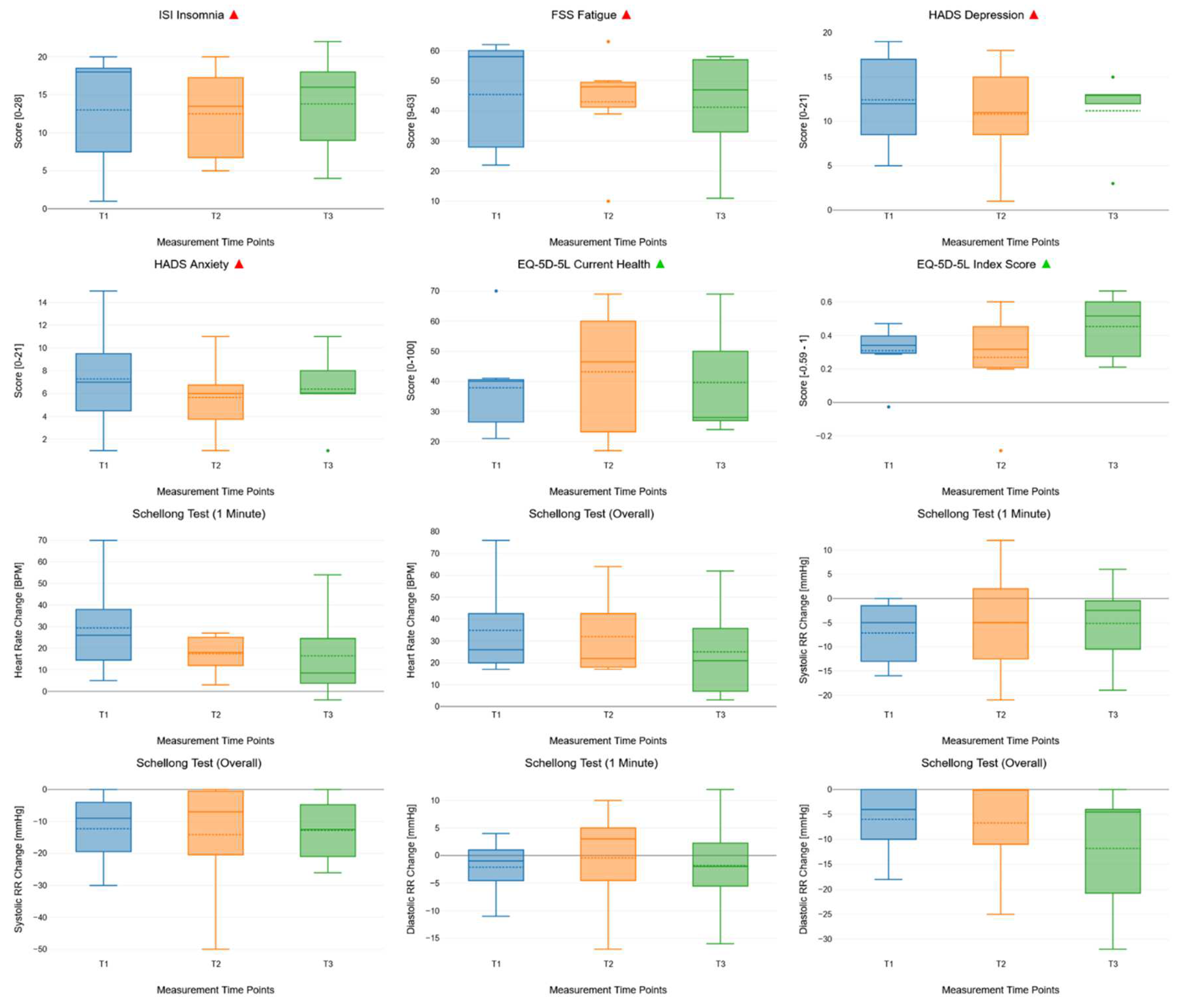
Table 1.
Comparison of similarities of ME/CFS and PCS symptoms and characteristics findings [8].
Table 1.
Comparison of similarities of ME/CFS and PCS symptoms and characteristics findings [8].
| Main symptom by category | ME/CFS | PCS |
|---|---|---|
| Cognitive impairment | attention, reaction time, which worsens after physical/cognitive exertion | memory, attention, executive functions |
| cerebral hypometabolism | up to 10 months* | |
| reduced cerebral blood flow | reduced cerebral blood flow (up to 10 months post-infection) | |
| Hypothalamic-pituitary growth hormon abnormalities | reduced peripheral CRH, ACTH, cortisol and IGF1 and IGF2 levels* | reduced peripheral CRH, ACTH, cortisol and IGF1 and IGF2 levels* |
| Autonomic dysfunction | a variety of autonomic testing showed impairments, autonomic dysfunction correlates with symptom severity* | similar findings to ME/CFS-group |
| Pain | lowered treshold | central sensitisation possible |
| small fiber neuropathy | ||
| Sleep disturbances | insomnia, non-restorative sleep*, irregular sleep patterns | chronic insomnia, hypersomnia, irregular sleep patterns |
| Autoantibodies | anti-adrenergic α1 receptor antibody (gastrointestinal symptoms)[9] anti-adrenergic α2- receptor antibody (gastrointestinal symptoms)[9] Mas-receptor antibody against angiotensin-II T1 receptor Endothelin-1 type A receptor antibody (cognitive impairment)[9] |
anti-adrenergic α1 receptor antibody [10] anti-adrenergic β2 receptor antibody [10] Mas-R antibody against angiotensin-II T1 receptor [10] |
| Clotting abnormalities | microclots, hyperactivated platelets | fibrin amyloid microclots, with entrapped pro-inflamatory molecules ↓ plasma Kallikrein, ↑ platelet factor 4,, ↑ von Willebrand factor, marginally increased level of α-2 antiplasmin [11] |
CRH= corticotropin releasing hormon, ACTH= adrenocorticotropic hormone, IGF-1= Insulin-like growth factor 1, IGF-2= Insulin-like growth factor 2. * existing confirming as well as negative studies
Table 2.
Pooled results of the associations between antibodies and imputed clinical outcomes using a multilevel model (MLM) with point estimate values representing non-standardized MLM coefficients. Up to two decimal places were added to the figures when rounding issues occurred.
Table 2.
Pooled results of the associations between antibodies and imputed clinical outcomes using a multilevel model (MLM) with point estimate values representing non-standardized MLM coefficients. Up to two decimal places were added to the figures when rounding issues occurred.
| Independ. variable / predictor | Depend. variable / endpoint | Point estimate | Lower 95% CI | Upper 95% CI | Std. error | T-stat. | Degrees of freedom | P-val. | R2 |
|---|---|---|---|---|---|---|---|---|---|
| β1-Adrenergic Receptor Antibody | ISI Insomnia | -0.30 | -0.67 | 0.06 | 0.19 | -1.63 | 2910.66 | .103 | 0.17 |
| FSS Fatigue | 0.16 | -1.31 | 1.63 | 0.70 | 0.23 | 17.10 | .819 | 0.04 | |
| HADS Anxiety | -0.03 | -0.30 | 0.23 | 0.14 | -0.25 | 86.63 | .801 | 0.02 | |
| HADS Depression | -0.11 | -0.47 | 0.25 | 0.18 | -0.61 | 64.73 | .542 | 0.06 | |
| EQ-5D-5L Index | -0.01 | -0.02 | 0.01 | 0.01 | -1.16 | 156.69 | .247 | 0.12 | |
| EQ-5D-5L Current health | 0.39 | -0.84 | 1.62 | 0.61 | 0.63 | 52.83 | .529 | 0.06 | |
| Schellong test | |||||||||
| Heart rate change (1 min) |
-0.20 | -1.57 | 1.17 | 0.70 | -0.28 | 424.78 | .776 | 0.01 | |
| Heart rate change (overall) | 0.004 | -1.32 | 1.33 | 0.67 | 0.01 | 1300.64 | .995 | 0.003 | |
| Systolic RR change (1 min) |
0.11 | -0.41 | 0.62 | 0.26 | 0.41 | 106.71 | .686 | 0.03 | |
| Systolic RR change (overall) | 0.06 | -0.71 | 0.83 | 0.39 | 0.16 | 68.47 | .876 | 0.02 | |
| Diastolic RR change (1 min) | -0.07 | -0.45 | 0.31 | 0.16 | -0.42 | 7.30 | .683 | 0.06 | |
| Diastolic RR change (overall) | 0.44 | -0.66 | 1.54 | 0.44 | 0.99 | 5.75 | .364 | 0.09 | |
| β2-Adrenergic Receptor Antibody | ISI Insomnia | -0.07 | -0.45 | 0.31 | 0.16 | -0.42 | 7.30 | .683 | 0.06 |
| FSS Fatigue | 0.44 | -0.66 | 1.54 | 0.44 | 0.99 | 5.75 | .364 | 0.09 | |
| HADS Anxiety | 0.06 | -0.10 | 0.23 | 0.08 | 0.76 | 72.77 | .449 | 0.05 | |
| HADS Depression | 0.06 | -0.21 | 0.33 | 0.12 | 0.46 | 12.24 | .656 | 0.04 | |
| EQ-5D-5L Index | -0.01 | -0.02 | -0.002 | 0.003 | -2.46 | 504.26 | .014* | 0.32 | |
| EQ-5D-5L Current health | 0.02 | -0.99 | 1.04 | 0.48 | 0.05 | 15.92 | .959 | 0.04 | |
| Schellong test | |||||||||
| Heart rate change (1 min) |
0.49 | -0.39 | 1.38 | 0.45 | 1.10 | 147.33 | .272 | 0.08 | |
| Heart rate change (overall) | 0.07 | -0.87 | 1.01 | 0.48 | 0.15 | 685.47 | .879 | 0.01 | |
| Systolic RR change (1 min) |
0.00 | -0.34 | 0.34 | 0.17 | 0.01 | 763.25 | .996 | 0.004 | |
| Systolic RR change (overall) | -0.09 | -0.54 | 0.36 | 0.23 | -0.40 | 342.55 | .691 | 0.02 | |
| Diastolic RR change (1 min) | -0.05 | -0.28 | 0.19 | 0.11 | -0.41 | 26.13 | .683 | 0.02 | |
| Diastolic RR change (overall) | -0.28 | -0.75 | 0.19 | 0.24 | -1.17 | 312.92 | .243 | 0.11 | |
| M3-Muscarinic Acetyl-choline Receptor Antibody | ISI Insomnia | -0.18 | -0.72 | 0.35 | 0.23 | -0.80 | 7.23 | .448 | 0.09 |
| FSS Fatigue | 0.43 | -1.34 | 2.21 | 0.74 | 0.59 | 6.40 | .575 | 0.06 | |
| HADS Anxiety | 0.00 | -0.27 | 0.27 | 0.13 | 0.02 | 48.48 | .986 | 0.01 | |
| HADS Depression | -0.02 | -0.40 | 0.35 | 0.18 | -0.13 | 17.53 | .898 | 0.03 | |
| EQ-5D-5L Index | -0.02 | -0.02 | -0.01 | 0.01 | -3.17 | 110.29 | .002** | 0.46 | |
| EQ-5D-5L Current health | 0.72 | -0.50 | 1.94 | 0.60 | 1.21 | 30.06 | .237 | 0.15 | |
| Schellong test | |||||||||
| Heart rate change (1 min) | 0.29 | -1.07 | 1.66 | 0.70 | 0.42 | 322.16 | .673 | 0.02 | |
| Heart rate change (overall) | -0.20 | -1.57 | 1.17 | 0.70 | -0.29 | 822.55 | .771 | 0.01 | |
| Systolic RR change (1 min) | -0.11 | -0.60 | 0.38 | 0.25 | -0.45 | 635.23 | .655 | 0.02 | |
| Systolic RR change (overall) | -0.25 | -0.91 | 0.41 | 0.33 | -0.73 | 249.11 | .464 | 0.04 | |
| Diastolic RR change (1 min) | -0.08 | -0.55 | 0.39 | 0.21 | -0.37 | 10.23 | .716 | 0.04 | |
| Diastolic RR change (overall) | -0.31 | -0.99 | 0.38 | 0.35 | -0.88 | 503.73 | .377 | 0.06 | |
| M4-Muscarinic Acetyl-choline Receptor Antibody | ISI Insomnia | -0.08 | -0.61 | 0.45 | 0.27 | -0.29 | 216.60 | .770 | 0.01 |
| FSS Fatigue | 0.90 | -0.48 | 2.28 | 0.69 | 1.30 | 68.50 | .199 | 0.10 | |
| HADS Anxiety | 0.15 | -0.17 | 0.47 | 0.16 | 0.95 | 411.64 | .345 | 0.08 | |
| HADS Depression | 0.01 | -0.40 | 0.41 | 0.21 | 0.02 | 155263.9 | .982 | 0.0003 | |
| EQ-5D-5L Index | -0.004 | -0.02 | 0.01 | 0.01 | -0.50 | 585.01 | .615 | 0.03 | |
| EQ-5D-5L Current health | -0.15 | -1.63 | 1.34 | 0.75 | -0.19 | 180.80 | .847 | 0.01 | |
| Schellong test | |||||||||
| Heart rate change (1 min) |
0.09 | -1.70 | 1.87 | 0.91 | 0.10 | 96242.33 | .924 | 0.001 | |
| Heart rate change (overall) | -0.06 | -1.80 | 1.68 | 0.89 | -0.07 | 23644.78 | .946 | 0.001 | |
| Systolic RR change (1 min) |
0.17 | -0.43 | 0.78 | 0.31 | 0.56 | 905826.11 | .573 | 0.03 | |
| Systolic RR change (overall) | 0.01 | -0.88 | 0.90 | 0.45 | 0.01 | 40299.40 | .990 | 0.001 | |
| Diastolic RR change (1 min) | -0.30 | -0.78 | 0.19 | 0.25 | -1.21 | 609.36 | .227 | 0.10 | |
| Diastolic RR change (overall) | -0.51 | -1.33 | 0.30 | 0.42 | -1.23 | 9418.34 | .218 | 0.11 |
Table 3.
Pooled results of one-way (time) repeated-measures analysis of variance (rmANOVA) of imputed clinical outcomes across three measurement time points (T1, T2, T3).
Table 3.
Pooled results of one-way (time) repeated-measures analysis of variance (rmANOVA) of imputed clinical outcomes across three measurement time points (T1, T2, T3).
| Outcome | Effect | Degrees of freedom (nom.) | Degrees of freedom (denom.) | Mauchly’s test of sphericity | F | p | R2 |
|---|---|---|---|---|---|---|---|
| ISI | Time | 2 | 13.44 | Equal variances | 0.2 | 0.818 | 0.03 |
| Insomnia | |||||||
| FSS | Time | 2 | 24.43 | Equal variances | 0.41 | 0.667 | 0.04 |
| Fatigue | |||||||
| HADS | Time | 2 | 49.56 | Equal variances | 0.48 | 0.621 | 0.03 |
| Depression | |||||||
| HADS | Time | 2 | 293.17 | Equal variances | 0.65 | 0.521 | 0.04 |
| Anxiety | |||||||
| EQ-5D-5L | Time | 2 | 26.89 | Equal variances | 0.38 | 0.686 | 0.05 |
| Current health | |||||||
| Schellong test | |||||||
| Heart rate change | Time | 2 | 216.16 | Equal variances | 1.84 | 0.162 | 0.12 |
| (1 min) | |||||||
| Systolic RR change | Time | 2 | 198.57 | Equal variances | 0.16 | 0.853 | 0.02 |
| (1 min) | |||||||
| Systolic RR change (overall) | Time | 2 | 612.6 | Equal variances | 0.06 | 0.945 | 0.01 |
| Diastolic RR change | Time | 2 | 64.26 | Equal variances | 0.36 | 0.698 | 0.01 |
| (1 min) | |||||||
| Diastolic RR change (overall) | Time | 2 | 1232.92 | Equal variances | 1.59 | 0.204 | 0.1 |
Abbreviations: RR = Riva-Rocci / Blood pressure.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



