
Submitted:
04 July 2025
Posted:
04 July 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
BACKGROUND: Long COVID can persist for years, but little is known about its prevalence in relation to the number of infections. This study examines the prevalence of Long COVID in association with the number of infections and vaccination status. METHODS: We analyzed anonymized data on Long COVID cases and thrombotic events from March 2020, provided by the Data Analysis Control Department for the population assigned to the CST (192,651 at March 2025). Additionally, we evaluated responses from a specific Long COVID symptom survey distributed to the entire CST population (n=1871 respondents). Symptomatic patients suspected of having Long COVID underwent blood tests to exclude alternative diagnoses. RESULTS: The overall detected prevalence of Long COVID was 2.4‰, with higher frequency among women aged 30–59 years. The survey, combined with blood test, improved detection rates by 26.3%. Long COVID prevalence was 3-10 times higher in individuals with three or more infections than in those with only one recorded infection (based on survey/CST data, respectively). The absolute number of thrombotic events doubled from 2020 to 2024 (p<0.0000001), occurring in both vaccinated and unvaccinated individuals, as well as in those with prior COVID-19 infection. CONCLUSION: Our findings demonstrate a link between SARS-CoV-2 reinfection and Long COVID prevalence. Furthermore, we observed a significant post-pandemic increase in thrombotic events across all populations, regardless of vaccination status or documented prior COVID-19 infection. Results suggest that COVID diagnosis should continue in suspected cases and that healthcare workers attending respiratory patients should continue wearing protective masks.
Keywords:
long covid
; thrombosis
; vaccine
; covid-19
; prevalence
1. Introduction
The appearance of a wide variety of persistent symptoms after a COVID-19 infection was described early during the pandemic and included neuropsychiatric, cardiovascular, gastrointestinal, hepatobiliary, and renal sequelae, as well as multisystem inflammatory syndrome in children [1,2], and has been extensively reviewed [3].
Cognitive impairment, including brain fog, may manifest as difficulties with concentration, memory, receptive language, and/or executive function, even after a mild infection [4,5,6]. Dyspnea, pain symptoms, headache, arthralgia, and myalgia, as well as loss of taste and smell, may also persist for months [7].
Long COVID symptoms [8] and cardiovascular sequelae could also be present even after mild or asymptomatic SARS-CoV-2 infection in young people: up to 15% of myocarditis and 30.9% of myocardial injury were found after performing MRI in competitive college athletes [9]. The involvement of the cardiovascular system by SARS-CoV-2 infection includes cardiac arrest, heart failure, myocardial inflammation, stroke, endothelial dysfunction, microangiopathy, and hematological conditions such as coagulopathy, deep vein thrombosis, microclots, and endothelial irregularities [10]. Several biological mechanisms are implicated in hyperinflammation and thrombosis, key factors in COVID-19 severity and long COVID [11]. On the other hand, the newly developed mRNA COVID-19 vaccines [12,13,14,15] also showed increased cardiovascular risk [16,17,18,19], but the benefits of vaccination in preventing severe COVID-19 outcomes have been considered to outweigh the potential complications [19].
Several studies have reviewed the prevalence of long COVID, but most conclude that symptoms may persist for over a year [20,21]. However, there is a gap in knowledge regarding the long-term persistence of symptoms, as well as their relationship with multiple infections and vaccination, which needs to be addressed. Recent studies suggest an increase of long COVID prevalence depending on the number of infections [22].
The present study assesses the prevalence of long COVID in an integrated public health care consortium -which comprises eight primary health care centers, one long-term care center and a referral hospital- analyzing the number of infections, vaccination status, and persistent or transient symptoms affecting functional status.
2. Materials and Methods
The cross-sectional study of long COVID-19 prevalence in the Consorci Sanitari de Terrassa (CST) (Ref 02-24-156-028) was approved by the Ethics Committee of the CST on January 29, 2024, while the observational clinical trial registered on April 29, 2020 (NCT04367883) (https://clinicaltrials.gov/study/ NCT05504057, accessed on June 30, 2025) was expanded to include long COVID syndrome and thrombotic events on February 24, 2025. The planning, conduct, and reporting of the study adhered to the principles of the Declaration of Helsinki.
All assisted patients signed an informed consent indicating whether they accept or decline receiving SMS messages from the CST on their contact phone.
2.1. Socioeconomic Environment
The details of the socioeconomic characteristics of the CST have been published previously [23,24]. In summary, the CST is public health organization in the North Metropolitan Barcelona Health Region that provides healthcare to 192,651 residents (population as of March, 2025).
The centers are located in rural (Castellbisbal), residential (Matadepera), or metropolitan areas (Terrassa and Rubí), and the population lives within less than 30 minutes by car from the Hospital of Terrassa. Despite variable socioeconomic factors among centers (pre-pandemic incomes below EUR 18,000 ranging from 58% to 67%, and incomplete primary education affecting 16.9–26.6% of the population), the different centers showed a pre-pandemic life expectancy above 81 years, comparable COVID-19 vaccination rates above 90% in patients over 60 years old with two or more chronic prescriptions, and pandemic infection rates between 22% and 27% [23]. The population over 60 years old ranges from 15.1% to 24% among centers, being above 20% in most of them [24].
2.2. Quantification of Long COVID Syndrome Prevalence
The Data Analysis Control Department collected anonymized data on COVID-19 cases, hospitalizations, long COVID syndrome, and thrombotic events from March 2020 to March 2025, along with data on gender, age, number of chronic treatments, and COVID-19 vaccination status prior to the first infection in the CST population. Data on cases and hospitalizations have been analyzed previously [23,24,25]. Here, we will focus on long COVID syndrome and thrombosis incidence.
2.3. Survey: Persistent Symptoms
A link to an online survey was sent to the CST population via SMS in April 19, 2024. The questionnaire is available in Appendix A. Medical records of patients who gave their consent to be contacted were reviewed. If no preexisting morbidity explaining the symptoms was identified, an analysis was performed to exclude incident pathology (Appendix B). If the analysis did not lead to new diagnoses, a long COVID diagnosis was added to the medical record.
Anonymized survey data were analyzed by one of the researchers, independently and blinded to the part of the team that contacted patients.
2.4. Statistical Analysis
Numbers of COVID-19-infected patients were analyzed, excluding duplicate codification of the same episode by different healthcare workers by excluding infections whose infection date differed in less than 45 days of another infection.
Patients were stratified by age (≤60 or >60 years), number of SARS-CoV-2 infections, and vaccination status. The prevalence of long COVID across subgroups -defined by age, number of infections, and vaccination status- was compared using OpenEpi chi-square tests [25]. Additionally, paired Student’s t-tests were employed to analyze changes in self-reported health perception before and after SARS-CoV-2 infection.
3. Results
3.1. Prevalence of Long Covid and Number of Infections
The overall detected prevalence of long covid is 2.4 ‰ (3.3‰ in women vs. 1,6 ‰ in men). The survey has allowed for an increase in detection of 26.3‰, identifying 99 new cases compared to the previous 376, resulting in 475 among the population of 192651 residents assigned to the CST at March 2025 (Table 1).
Most of the long COVID cases corresponded to infections that occurred in 2020 (Figure 1). The number of registered cases decreased progressively until the survey was launched in 2024 and new cases were reclassified. The decline in long COVID diagnoses paralleled the decrease in the number of COVID-19 cases following the end of protocols that required test confirmation for any symptomatic patient and their close contacts in March 2022 (Figure 2).
Based on CST registry data, patients with multiple infections were recorded as fol-lows: 49914 (one infection), 5190 (two), 480 (three), 61 (four), 14 (five), 3 (six), 2 (seven), and 1 (eight multiple infections).
Long COVID prevalence increased significantly with the number of infections, showing an odds ratio (OR) of >10 across all groups suffering 3 or more infections compared to a single infection. It was also higher among those who received the first vaccine dose after their first COVID-19 infection (Table 2). LC prevalence related to number of doses of vaccine received is presented in Appendix C.
3.2. Survey: Reported Persistent and Transient Symptoms
A 19.7% (368) of 1871 survey respondents (about a 1% of the CST population) reported being diagnosed with Long COVID, while 15 % were unsure about this diagnosis (Table 2).
Reported symptoms are summarized in Table 3. Among those diagnosed with Long COVID, 38% reported being currently asymptomatic. All respondent groups rated their overall health perception above 8 points out of 10 prior to COVID-19 infection. Those who felt recovered rated their current health at 6.97 ± 1.8 vs. 8.18 ± 1.41 pre-infection (p<0.001), while those with persistent symptoms rated theirs at 5.41 ± 2.08 vs. 8.2 ± 1.71 pre-infection (p<0.001).
A total of 881 respondents (47%) needed COVID-19-related sick leave. Most were on leave for <1 month (79.5%), 10.3% for 1-3 months, 2.7% for up to 6 months, 2.6% for up to one year, and 4.9% for more than one year.
The percentage of Long COVID relative to the number of SARS-CoV-2 infections and vaccines received among survey respondents is detailed in Table 4. The overall odds ratio for Long COVID syndrome between unvaccinated and vaccinated respondents increased with infection count (from 1.13 after one infection to 1.34 after ≥3 infections). Long COVID prevalence increased with infection number in both unvaccinated (from 10 % to 33%) and vaccinated (from 8 % to 24.9%, p<0.0001) respondents when comparing 1 infection with ≥3 infections. Among respondents, Long COVID rates decreased in those receiving one vaccine (13–37.9%) versus ≥3 vaccines (6.9–21.4%) (p=0.01-0.23).
3.3. Thrombotic Events
Anonymized data from CST patients with thrombosis from March 2020 show a linear increase in this phenomenon (Figure 3), particularly in patients aged over 60 years. Increased incidence is evident among those with prior COVID-19 infection and unvaccinated individuals without detected infection.
4. Discussion
4.1. Increased Prevalence with Multiple Infections
To our knowledge, this is the first study to demonstrate a significant association between the number of SARS-CoV-2 infections and increased long COVID prevalence. Both anonymized population-wide data and survey-based analyses consistently revealed higher prevalence rates in individuals with three or more recorded infections compared to those with only one infection.
Data extracted from electronic medical records by the Management, Control, and Information Analysis Unit—coded by primary care physicians—revealed a tenfold increase in long COVID prevalence among individuals with three or more infections. Prevalence exceeded 2% in those vaccinated prior to their first infection and was even higher in other groups (e.g., unvaccinated: OR 1.30).
This trend was corroborated by survey respondents, where individuals reporting three or more infections exhibited triple the rate of persistent symptoms (affecting >20% across all groups) compared to those with only one infection, regardless of vaccination status. While potential respondent bias may influence survey results [8,22,27], the consistency with the Unit’s recorded cases strengthens the evidence for a dose-dependent relationship between reinfection and long COVID risk.
4.2. Increase in Thrombotic Events
To our knowledge, this is also the first study to demonstrate a linear increase in thrombotic events over the past five years, with rates doubling since 2020 among patients aged ≥60 years. This rise was most pronounced in individuals with documented COVID-19 infections but remained significant even in those without recorded infections or vaccinations, potentially reflecting undiagnosed mild or asymptomatic cases following the discontinuation of universal testing protocols.
While our findings should be interpreted cautiously due to a 15% increase in the assigned population (resulting from a healthcare restructuring, including the addition of a new primary care center in Terrassa in October 2022), this demographic shift cannot account for the initial rise in thrombotic events observed as early as 2021, nor the magnitude of the increase (approximately 100% by 2025 compared to 2020).
Although global hospital admissions for acute coronary syndrome (ACS) declined during the early pandemic phase—attributed to patient reluctance to seek care and undiagnosed cases—studies anticipated both short- and long-term complications of myocardial infarction [28].
Multiple biological mechanisms associated with COVID-19 infection may explain the increased thrombotic risk: severe cases exhibit elevated soluble ICAM-1 (intercellular adhesion molecule 1) and VCAM-1 (vascular cell adhesion molecule 1), driving endothelial dysfunction and multiorgan damage [11], while recurrent infections are linked to disrupted homocysteine metabolism, perpetuating cycles of inflammation and hypercoagulability [29].
4.3. Persistent and Transient Symptoms-Functional Affectation
The temporal alignment between the date of first COVID-19 infection and long COVID diagnosis aligns with studies documenting its persistence beyond one year [8,20, 21, 22, 30, among others], with the present results suggesting symptoms may last for over four years. Our finding of higher long COVID frequency in females corroborates previous reports [20,21,28,30,31].
While many patients experienced persistent symptoms, some reported gradual recovery; however, overall self-rated health remained significantly impaired compared to pre-infection levels. This pattern mirrors studies describing partial improvement over time despite lasting health impacts [30,31].
Our finding that nearly half of respondents required sick leave aligns with prior studies identifying work incapacity as a common functional consequence of long COVID (20). However, fewer than 5% needed extended sick leave (>1 year), consistent with evidence of gradual functional improvement over time.
4.4. Long COVID and Future
From the pandemic's early stages, multiple drugs have been explored for repurposing (33), including antihistamines and antiparkinsonian agents. Primary care reports describe empirical antihistamine use to prevent post-COVID syndrome [34], while amantadine -an antiparkinsonian drug with historical use as an influenza antiviral- has demonstrated efficacy in alleviating fatigue [35] and depressive symptoms [36]. Notably, metformin, a commonly prescribed medication, exhibits broad-spectrum antiviral activity against RNA viruses, reducing hospitalization/mortality rates [37] and lowering long COVID incidence by approximately 40% [38].
Randomized controlled trials have evaluated diverse interventions for post-COVID syndrome: biologic drugs designed to clear extracellular RNA from latent reservoirs show promise in reducing fatigue by improving chronic inflammation [39]; antiviral agents yield mixed results, with ensitrelvir demonstrating efficacy [40] but nirmatrelvir-ritonavir showing no benefit [41]; and micronutrient supplementation likewise failed to improve outcomes [32].
Additional therapeutic approaches include rehabilitation, whether supervised telerehabilitation [42], asynchronous [43], or face-to-face [44], all of which have demonstrated clinical benefits, as well as cognitive exercises [45]. In contrast, cognitive interventions remain limited in scope, though future strategies may incorporate combined neurostimulation and cognitive training [46].
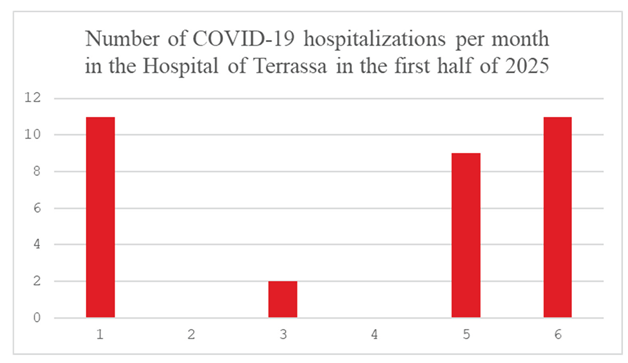
Further investigation is ongoing since COVID-19 hospitalizations continue (Appendix D), with variant XFG in 58% of random samples of symptomatic patients [47], with incidence in June 2025 being similar to that of January 2025.
4.5. Limitations of the Study
As previously reported [25], the limitations of the study include: (1) the inability to precisely quantify first-wave cases due to diagnostic test shortages in primary care until June 2020; (2) the 78% sensitivity ceiling of publicly available antigen tests (introduced November 2020) [48]; and (3) the discontinuation of systematic COVID-19 testing protocols for symptomatic patients after 24 March 2022 [49], which precipitated a sharp decline in detected cases despite sustained weekly hospital admissions through January 2025 [23,24,25]. Consequently, both COVID-19 infection rates and syndrome incidence could be underestimated, with undocumented infections potentially contributing to undiagnosed cases.
Another factor of confusion for the calculation of long COVID prevalence is that either long COVID (‘COVID persistent’) and COVID sequelae share the same ICD-10-CM code (U09.9) in the medical software for history records. Furthermore, although the medical record software allows clinicians to close open diagnoses once symptoms are resolved, a long COVID diagnosis will likely remain open until actively closed during a follow-up consultation with the patient's primary care physician. This follow-up is unlikely to occur if the patient feels better. Furthermore, clinicians might omit this step to save time during the visit. Consequently, the current absolute prevalence could overestimate the symptomatic population. Other groups [50,51] have also reported those codification difficulties.
An additional limitation involves decentralized vaccination in 2021 for individuals under 60 years, which may have led to incomplete records in CST vaccination registries—despite >90% vaccination coverage in those over 60 at primary care centers during early 2021. In the other hand, the contact phone number of older patients uses to coincide with the phone number of younger relatives leading to a potential underestimation of respondents in older ages.
Data comparability with other teams from surrounding institutions confirm the decline of symptomatology after several months [30], although regional results may be influenced by Spain’s unique variant evolution early in the pandemic, particularly the dominance of the B3a strain, which was uncommon elsewhere in Europe [51]. Further research should investigate whether this distinct variant’s virulence contributes to divergent long COVID manifestations.
5. Conclusions
Our findings demonstrate a relationship between SARS-CoV-2 reinfection and long COVID prevalence. Additionally, we observed a significant post-pandemic rise in thrombotic events across all populations, regardless of vaccination status or documented prior COVID-19 infection. Results suggest that COVID diagnosis should continue in suspected cases to reassess future long COVID cases and cardiovascular risk, and that healthcare workers attending respiratory patients should continue wearing protective masks.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, all authors.; methodology, C.G.-A., M.Ll, A.P.-S., R.R.-P.,.; validation, all authors.; formal analysis, C.G.-A., M.Ll., A.P-S.; investigation, C. G.-A., M. G.-N., V. M.-C., C. P.-D., M. Ll.; resources, A. A.-G., R.R,-P.; data curation, A.P.-S..; writing—original draft preparation, review and editing, A. P.-S..; supervision, R.R.-P., A.A.-G.; project administration, R.R.-P., A.A.-G.; All authors have read and agreed to the published version of the manuscript.”.
Funding
The PT-082023-EP research was funded by the GENERALITAT DE CATALUNYA, grant number PT-082023-EP subproject COVID-P.
Institutional Review Board Statement
The original descriptive study of patients with COVID-19 was approved by the Ethics Committee of CST on 8 April 2020, (ref 02-20-161-021), and the observational clinical trial was posted on 29 April 2020 (NCT 04367883). The study has been prolonged successively and complemented with several repurposing drugs on 13 June 2022 ((https://clinicaltrials.gov/study/NCT05504057, accessed on 11 March 2025). The study has been prolonged, including post-COVID syndrome, on 24 February 2025. The planning, conduct, and reporting of the study were in line with the Declaration of Helsinki.
Informed Consent Statement
Patient consent was waived due the use of anonymized data.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Acknowledgments
The authors wish to acknowledge the support preparing anonymized data of Marta González Salvador, from the Management, Control and Information Analysis Unit, Hospital de Terrassa, Consorci Sanitari de Terrassa (CST).
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results”.
Abbreviations
The following abbreviations are used in this manuscript:
| LC | Long Covid |
| No V | Non vaccinated |
| Preinf | Previously to the COVID-19 infection |
| Postinf | Posterior to the COVID-19 infection |
| PreThr | Previously to the thrombosis |
| PostThr | Posterior to the thrombosis |
| CoV | COVID-19 infection |
| CST | Consorci Sanitari de Terrassa |
Appendix A
English translation of the survey questionnaire, that was sent in either catalan and Spanish:
Since 2020, many people have suffered from COVID-19. The aim of this survey is to assess the current situation from the patients' point of view. We would appreciate it if you could answer this survey, which will take no more than 3 minutes to complete and may help improve your healthcare.
Gender
Woman
Man
I identify differently
2. Age
18 to 35
36 to 50
51 to 65
66 to 75
76 or older
3. Have you received any COVID-19 vaccines?
No
Yes. 1 dose
Yes. 2 doses
Yes. 3 doses
Yes. More than 3 doses
4. Have you ever been diagnosed with COVID-19?
No
Yes. Once
Yes. Twice
Yes. Three or more times
IF YOUR ANSWER IS NO, GO TO QUESTIONS 7 AND 8 AND YOU WILL HAVE COMPLETED THE SURVEY.
- 5.
- How was the diagnosis made?
- ∙
- I had a rapid test
- ∙
- I had a PCR test
- ∙
- I had a blood test
- ∙
- No test was done. Diagnosis based only on symptoms
- ∙
- I did the test myself
- 6.
- >6. Have you been diagnosed with "Long COVID" or had symptoms attributed to COVID that lasted more than 2 or 3 months?
- ∙
- Yes. I still have symptoms
- ∙
- Yes, but I am now recovered
- ∙
- No
- ∙
- I don’t know
- 7.
- Overall rating of your current health status (on a scale from 0 to 10, where 0 is the worst possible health status and 10 is excellent health)
- ∙
- 0 1 2 3 4 5 6 7 8 9 10
- 8.
- Overall rating of the worsening of your health compared to before COVID (on a scale from 0 to 10, where 0 is no change and 10 is maximum worsening)
- ∙
- 0 1 2 3 4 5 6 7 8 9 10
- 9.
- Do you have functional limitations in your daily life (personal hygiene, household tasks, work activity, relationships with friends and/or close family)?
- ∙
- Yes
- ∙
- No
- 10.
- If you answered yes, please indicate which of the following apply:
- ∙
- Personal hygiene
- ∙
- Household tasks
- ∙
- Work activity
- ∙
- Relationships with friends and/or close family
- 11.
- Are your symptoms mainly physical or psychological?
- ∙
- Physical symptoms
Alteration in smell or sense of taste
Persistent Fatigue
Joint pain
Headache
Shortness of breath
- Psychological symptoms
Memory loss
Difficulty concentrating
Anxiety
Depression
Sleep compalins
- Both physical and psychological symptoms
- Have you had to take sick leave for more than a month due to persistent COVID-related symptoms?
- Yes
- No
- If you answered yes to the previous question, how long were you on sick leave?
- Between 1 and 3 months
- 3 to 6 months
- 6 to 12 months
- More than a year
- Do you consent to being contacted by your health center (CAP) in case there is any treatment or intervention that could benefit you?
- Yes
- No
Appendix B
General blood test for Long COVID suspected patients:
Complete blood count with white blood cell differential
Glucose
C-reactive protein
Bilirubin
Alanine aminotransferase
Aspartate aminotransferase
Gamma-glutamyl transferase
Alkaline phosphatase
Urea
Sodium
Potassium
Creatine phosphokinase
Lactate dehydrogenase
Albumin
Thyroid-stimulating hormone
Ferritin
Vitamin B12
Folate
Calcium
Phosphorus
D-dimer
Specific profile depending on symptoms:
Myalgia, asthenia, fatigue, articular pain:
Protein electrophoresis
Uric acid
Rheumatoid factor
Antinuclear antibodies
Complement C3
Complement C4
Antiphospholipid antibodies
Cortisol
Dyspnea, thoracic pain:
Pro B-type natriuretic peptide
Amylase
Digestive symptoms:
Amylase
Lipase
Fecal calprotectin
Fecal occult blood
Anti-transglutaminase antibodies
Appendix C
Appendix C.1

Table A1.
Number of Long COVID cases (LC) depending on the number of COVID-19 recorded infections (n infection) and the number of COVID-19 vaccines administered (nV), before (nV preinf) or after (nV postinf) the first COVID-19 infection. Statistical p values are calculated between 1 and >3 doses received and between non vaccinated and those full vaccinated receiving >=3 doses. Significant differences are marked with *.
Table A1.
Number of Long COVID cases (LC) depending on the number of COVID-19 recorded infections (n infection) and the number of COVID-19 vaccines administered (nV), before (nV preinf) or after (nV postinf) the first COVID-19 infection. Statistical p values are calculated between 1 and >3 doses received and between non vaccinated and those full vaccinated receiving >=3 doses. Significant differences are marked with *.
| nV | p | No V | p | ||||||||||
| n infection | n V preinf | 1 | 2 | 3 | >=3 | 1 vs >=3 doses | vs >=3 doses | ||||||
| ? | COV | 5811 | 21171 | 12447 | 21556 | 75685 | |||||||
| LC | 7 | 13 | 10 | 15 | 21 | ||||||||
| 1 | COV | 1342 | 7272 | 3778 | 5992 | 21608 | |||||||
| LC | 2 (0.1%) | 22 (0.3%) | 11 (0.3%) | 13 (0.2%) | 92 (0.42%) | ||||||||
| 2 | COV | 601 | 934 | 578 | 835 | 1833 | |||||||
| LC | 14 (2.3%) | 12 (1.3%) | 5 (0.9%) | 12 (1.4%) | 18 (0.97%) | ||||||||
| >=3 | COV | 70 | 106 | 87 | 94 | 136 | |||||||
| LC | 2 (2.8%) | 2 (1.9%) | 2 (2.2%) | 2 (2.1%) | 10 (6.8%) | ||||||||
| OR vs 1 dose | 2,03 | 1,95 | 1,45 | 0.61 | 1,96 | 0.02* | |||||||
| OR vs 1 dose | 0,56 | 0,38 | 0,62 | 0.22 | 0,69 | 0.30 | |||||||
| OR vs 1 dose | 0,67 | 0,81 | 0,75 | 0.77 | 3,29 | 0.047* | |||||||
| n infection | nV postinf | 1 | 2 | 3 | >=3 | ||||||||
| 1 | COV | 3854 | 2523 | 1314 | 2193 | ||||||||
| LC | 55 (1.4%) | 42 (1.16%) | 25 (1.9%) | 49(2.2%) | |||||||||
| 2 | COV | 113 | 72 | 47 | 103 | ||||||||
| LC | 4 (3.4%) | 4 (5.3%) | 5(4.6%) | ||||||||||
| >=3 | COV | 7 | 7 | 5 | 23 | ||||||||
| LC | 4 (36.4%) | 1(16.7%) | 1 (4.2%) | ||||||||||
| OR vs 1 dose | 1,1638 | 1,327 | 1,5533 | 0.02* | |||||||||
| OR vs 1 dose | 1,5395 | 0 | 1,3542 | 0.64 | |||||||||
| OR vs 1 dose | 0 | 0,4583 | 0,1146 | 0.01* | |||||||||
Appendix D
References
- Nalbandian A, Sehgal K, Gupta A, Madhavan MV, McGroder C, Stevens JS, Cook JR, Nordvig AS, Shalev D, Sehrawat TS, Ahluwalia N, Bikdeli B, Dietz D, Der-Nigoghossian C, Liyanage-Don N, Rosner GF, Bernstein EJ, Mohan S, Beckley AA, Seres DS, Choueiri TK, Uriel N, Ausiello JC, Accili D, Freedberg DE, Baldwin M, Schwartz A, Brodie D, Garcia CK, Elkind MSV, Connors JM, Bilezikian JP, Landry DW, Wan EY. Post-acute COVID-19 syndrome. Nat Med. 2021 Apr;27(4):601-615.
- Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol. 2023 Mar;21(3):133-146. Epub 2023 Jan 13. Erratum in: Nat Rev Microbiol. 2023 Jun;21(6):408. [CrossRef]
- O'Mahoney LL, Routen A, Gillies C, Jenkins SA, Almaqhawi A, Ayoubkhani D, Banerjee A, Brightling C, Calvert M, Cassambai S, Ekezie W, Funnell MP, Welford A, Peace A, Evans RA, Jeffers S, Kingsnorth AP, Pareek M, Seidu S, Wilkinson TJ, Willis A, Shafran R, Stephenson T, Sterne J, Ward H, Ward T, Khunti K. The risk of Long Covid symptoms: a systematic review and meta-analysis of controlled studies. Nat Commun. 2025 May 7;16(1):4249. [CrossRef]
- Ceban, F.; et al. Fatigue and cognitive impairment in post-COVID-19 syndrome: a systematic review and meta-analysis. Brain Behav. Immun. 101, 93–135 (2022).
- Ariza, M.; Cano, N.; Segura, B.; Adan, A.; Bargalló, N.; Caldú, X.; Campabadal, A.; Jurado, M.A.; Mataró, M.; Pueyo, R.; et al. Neuropsychological impairment in post-COVID condition individuals with and without cognitive complaents. Front. Aging Neurosci. 2022, 14, 1029842. [Google Scholar] [CrossRef] [PubMed]
- Doskas T, Vavougios GD, Kormas C, Kokkotis C, Tsiptsios D, Spiliopoulos KC, Tsiakiri A, Christidi F, Aravidou T, Dekavallas L, Kazis D, Dardiotis E, Vadikolias K. Neurocognitive Impairment After COVID-19: Mechanisms, Phenotypes, and Links to Alzheimer's Disease. Brain Sci. 2025 May 25;15(6):564.
- Zayet S, Zahra H, Royer PY, Tipirdamaz C, Mercier J, Gendrin V, Lepiller Q, Marty-Quinternet S, Osman M, Belfeki N, Toko L, Garnier P, Pierron A, Plantin J, Messin L, Villemain M, Bouiller K, Klopfenstein T. Post-COVID-19 Syndrome: Nine Months after SARS-CoV-2 Infection in a Cohort of 354 Patients: Data from the First Wave of COVID-19 in Nord Franche-Comté Hospital, France. Microorganisms. 2021 Aug 12;9(8):1719. [CrossRef] [PubMed]
- Massey D, Saydah S, Adamson B, Lincoln A, Aukerman DF, Berke EM, Sikka R, Krumholz HM. Prevalence of covid-19 and long covid in collegiate student athletes from spring 2020 to fall 2021: a retrospective survey. BMC Infect Dis. 2023 Dec 13;23(1):876.
- Rajpal S, Tong MS, Borchers J, Zareba KM, Obarski TP, Simonetti OP, Daniels CJ. Cardiovascular Magnetic Resonance Findings in Competitive Athletes Recovering From COVID-19 Infection. JAMA Cardiol. 2021 Jan 1;6(1):116-118. Erratum in: JAMA Cardiol. 2021 Jan 1;6(1):123.
- Koutsiaris AG, Karakousis K. Long COVID Mechanisms, Microvascular Effects, and Evaluation Based on Incidence. Life (Basel). 2025 May 30;15(6):887.
- Eltayeb A, Adilović M, Golzardi M, Hromić-Jahjefendić A, Rubio-Casillas A, Uversky VN, Redwan EM. Intrinsic factors behind long COVID: exploring the role of nucleocapsid protein in thrombosis. PeerJ. 2025 May 20;13:e19429.
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D. ; Zerbini,C. ; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Ramasamy, M.N.; Minassian, A.M.; Ewer, K.J.; Flaxman, A.L.; Folegatti, P.M.; Owens, D.R.; Voysey, M.; Aley, P.K.; Angus, B.; Babbage, G.; et al. Safety and immunogenicity of ChAdOx1 nCoV-19 vaccine administered in a prime-boost regimen in young and old adults (COV002): A single-blind, randomised, controlled, phase 2/3 trial. Lancet 2021, 396, 1979–1993. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, K.E.; Le Gars, M.; Sadoff, J.; de Groot, A.M.; Heerwegh, D.; Truyers, C.; Atyeo, C.; Loos, C.; Chandrashekar, A.; McMahan, K. Immunogenicity of the Ad26. COV2.S Vaccine for COVID-19. JAMA 2021, 325, 1535–1544. [Google Scholar]
- Faksova, K.; Walsh, D.; Jiang, Y.; Griffin, J.; Phillips, A.; Gentile, A.; Kwong, J.C.; Macartney, K.; Naus, M.; Grange, Z.; et al. COVID-19 vaccines and adverse events of special interest: A multinational Global Vaccine Data Network (GVDN) cohort study of 99 million vaccinated individuals. Vaccine 2024, 42, 2200–2211. [Google Scholar] [CrossRef] [PubMed]
- Yardibi F, Demirci S. Global trends and hot spots in cerebral venous sinus thrombosis research over the past 50 years: a bibliometric analysis. Neurol Res. 2025 Jan;47(1):23-34.
- Nitz JN, Ruprecht KK, Henjum LJ, Matta AY, Shiferaw BT, Weber ZL, Jones JM, May R, Baio CJ, Fiala KJ, Abd-Elsayed AA. Cardiovascular Sequelae of the COVID-19 Vaccines. Cureus. 2025;17(4):e82041.
- Satyam SM, El-Tanani M, Bairy LK, Rehman A, Srivastava A, Kenneth JM, Prem SM. Unraveling Cardiovascular Risks and Benefits of COVID-19 Vaccines: A Systematic Review. Cardiovasc Toxicol. 2025 Feb;25(2):306-323.
- Taher MK, Salzman T, Banal A, Morissette K, Domingo FR, Cheung AM, Cooper CL, Boland L, Zuckermann AM, Mullah MA, Laprise C, Colonna R, Hashi A, Rahman P, Collins E, Corrin T, Waddell LA, Pagaduan JE, Ahmad R, Jaramillo Garcia AP. Global prevalence of post-COVID-19 condition: a systematic review and meta-analysis of prospective evidence. Health Promot Chronic Dis Prev Can. 2025 Mar;45(3):112-138. Erratum in: Health Promot Chronic Dis Prev Can. 2025 Jun;45(6):307-308. [CrossRef]
- Sk Abd Razak R, Ismail A, Abdul Aziz AF, Suddin LS, Azzeri A, Sha'ari NI, Post-COVID syndrome prevalence: a systematic review and meta-analysis. BMC Public Health. 2024 Jul 4;24(1):1785. [CrossRef]
- Obeidat M, Abu Zahra A, Alsattari F. Prevalence and characteristics of long COVID-19 in Jordan: A cross sectional survey. PLoS One. 2024 Jan 26;19(1):e0295969. PMCID: PMC10817197. [CrossRef] [PubMed]
- Puigdellívol-Sánchez, A.; Juanes-González, M.; Calderón-Valdiviezo, A.; Valls-Foix, R.; González-Salvador, M.; Lozano-Paz, C.; Vidal-Alaball, J. COVID-19 in Relation to Chronic Antihistamine Prescription. Microorganisms 2024, 12, 2589. [Google Scholar] [CrossRef] [PubMed]
- Puigdellívol-Sánchez A, Juanes-González M, Calderón-Valdiviezo AI, Losa-Puig H, González-Salvador M, León-Pérez M, Pueyo-Antón L, Franco-Romero M, Lozano-Paz C, Cortés-Borra A, Valls-Foix R. COVID-19 Pandemic Waves and 2024-2025 Winter Season in Relation to Angiotensin-Converting Enzyme Inhibitors, Angiotensin Receptor Blockers and Amantadine. Healthcare (Basel). 2025 May 27;13(11):1270.
- Puigdellívol-Sánchez A, Juanes-González M, Calderón-Valdiviezo A, Valls-Foix R, González-Salvador M, Lozano-Paz C, Vidal-Alaball J. COVID-19 in Relation to Polypharmacy and Immunization (2020-2024). Viruses. 2024 Sep 27;16(10):1533.
- Dean, A.G.; Sullivan, K.M.; Soe, M.M. OpenEpi: Open Source Epidemiologic Statistics for Public Health, Versión. Available online: https://www.openepi.com/Menu/OE_Menu.htm (accessed on 30 March 2025).
- Chen YC, Chiu CH, Chen CJ. Neurological and psychiatric aspects of long COVID among vaccinated healthcare workers: An assessment of prevalence and reporting biases. J Microbiol Immunol Infect. 2025 Jun 23:S1684-1182(25)00125-2.
- Cameli M, Pastore MC, Mandoli GE, D'Ascenzi F, Focardi M, Biagioni G, Cameli P, Patti G, Franchi F, Mondillo S, Valente S. COVID-19 and Acute Coronary Syndromes: Current Data and Future Implications. Front Cardiovasc Med. 2021 Jan 28;7:593496.
- Nair AS, Tauro L, Joshi HB, Makhal A, Sobczak T, Goret J, Dewitte A, Kaveri S, Chakrapani H, Matsuda MM, Joshi MB. Influence of homocysteine on regulating immunothrombosis: mechanisms and therapeutic potential in management of infections. Inflamm Res. 2025;74(1):86.
- Carrera Morodoa M, Pérez Orcerob A, Ruiz Moreno J, Altemir Vidal A, Larrañaga Cabrerab A, Fernández San Martín MI, Prevalencia de la COVID persistente: seguimiento al año de una cohorte poblacional ambulatoria, Rev Clin Med Fam. 2023; 16( 2 ): 94-97. [CrossRef]
- Pisaturo M, Russo A, Grimaldi P, Monari C, Imbriani S, Gjeloshi K, Ricozzi C, Astorri R, Curatolo C, Palladino R, Caruso F, Ambrisi F, Onorato L, Coppola N. Prevalence, Evolution and Prognostic Factors of PASC in a Cohort of Patients Discharged from a COVID Unit. Biomedicines. 2025 Jun 9;13(6):1414. PMCID: PMC12191248. [CrossRef] [PubMed]
- Tomasa-Irriguible TM, Monfà R, Miranda-Jiménez C, Morros R, Robert N, Bordejé-Laguna L, Vidal S, Torán-Monserrat P, Barriocanal AM. Preventive Intake of a Multiple Micronutrient Supplement during Mild, Acute SARS-CoV-2 Infection to Reduce the Post-Acute COVID-19 Condition: A Double-Blind, Placebo-Controlled, Randomized Clinical Trial. Nutrients. 2024 May 26;16(11):1631.
- Gordon, D.E.; Jang, G.M.; Bouhaddou, M.; Xu, J.; Obernier, K.; White, K.M.; O’Meara, M.J.; Rezelj, V.V.; Guo, J.Z.; Swaney, D.L. A SARS-CoV-2 Protein Interaction Map Reveals Targets for Drug-Repurposing. Nature 2020, 583, 459–468. [Google Scholar] [CrossRef] [PubMed]
- Morán Blanco, J.I.; Alvarenga Bonilla, J.A.; Fremont-Smith, P.; Villar Gómez de Las Heras, K. Antihistamines as an early treatment for COVID-19. Heliyon 2023, 9, e15772. [Google Scholar] [CrossRef] [PubMed]
- Harandi, A.A.; Pakdaman, H.; Medghalchi, A.; Kimia, N.; Kazemian, A.; Siavoshi, F.; Barough, S.S.; Esfandani, A.
- M. H.; Sobhanian, S.A. A randomized open-label clinical trial on the effect of Amantadine on post COVID 19 fatigue. Sci. Rep. 2024, 14, 1343.
- Rejdak, K.; Fiedor, P.; Bonek, R.; Łukasiak, J.; Chełstowski, W.; Kiciak, S.; Dąbrowski, P.; Gala-Błądzińska, A.; Dec, M.; Papuć,E.; et al. Amantadine in unvaccinated patients with early, mild to moderate COVID-19: A randomized, placebo-controlled, double-blind trial. Eur. J. Neurol. 2024.
- Bramante CT, Beckman KB, Mehta T, Karger AB, Odde DJ, Tignanelli CJ, Buse JB, Johnson DM, Watson RHB, Daniel JJ, Liebovitz DM, Nicklas JM, Cohen K, Puskarich MA, Belani HK, Siegel LK, Klatt NR, Anderson B, Hartman KM, Rao V, Hagen AA, Patel B, Fenno SL, Avula N, Reddy NV, Erickson SM, Fricton RD, Lee S, Griffiths G, Pullen MF, Thompson JL, Sherwood NE, Murray TA, Rose MR, Boulware DR, Huling JD; COVID-OUT Study Team. Favorable Antiviral Effect of Metformin on SARS-CoV-2 Viral Load in a Randomized, Placebo-Controlled Clinical Trial of COVID-19. Clin Infect Dis. 2024 Aug 16;79(2):354-363.
- Bramante CT, Buse JB, Liebovitz DM, Nicklas JM, Puskarich MA, Cohen K, Belani HK, Anderson BJ, Huling JD, Tignanelli CJ, Thompson JL, Pullen M, Wirtz EL, Siegel LK, Proper JL, Odde DJ, Klatt NR, Sherwood NE, Lindberg SM, Karger AB, Beckman KB, Erickson SM, Fenno SL, Hartman KM, Rose MR, Mehta T, Patel B, Griffiths G, Bhat NS, Murray TA, Boulware DR; COVID-OUT Study Team. Outpatient treatment of COVID-19 and incidence of post-COVID-19 condition over 10 months (COVID-OUT): a multicentre, randomised, quadruple-blind, parallel-group, phase 3 trial. Lancet Infect Dis. 2023 Oct;23(10):1119-1129.. Erratum in: Lancet Infect Dis. 2023 Oct;23(10):e400. [CrossRef]
- Assessment of the Impact of RNase in Patients With Severe Fatigue Related to Post-Acute Sequelae of SARS-CoV-2 Infection: A Randomized Phase 2 Trial of RSLV-132. Clin Infect Dis. 2024 Sep 26;79(3):635-642.
- Yotsuyanagi H, Ohmagari N, Doi Y, Yamato M, Fukushi A, Imamura T, Sakaguchi H, Sonoyama T, Sanaki T, Ichihashi G, Tsuge Y, Uehara T, Mukae H. Prevention of post COVID-19 condition by early treatment with ensitrelvir in the phase 3 SCORPIO-SR trial. Antiviral Res. 2024 Sep;229:105958.
- Geng LN, Bonilla H, Hedlin H, Jacobson KB, Tian L, Jagannathan P, Yang PC, Subramanian AK, Liang JW, Shen S, Deng Y, Shaw BJ, Botzheim B, Desai M, Pathak D, Jazayeri Y, Thai D, O'Donnell A, Mohaptra S, Leang Z, Reynolds GZM, Brooks EF, Bhatt AS, Shafer RW, Miglis MG, Quach T, Tiwari A, Banerjee A, Lopez RN, De Jesus M, Charnas LR, Utz PJ, Singh U. Nirmatrelvir-Ritonavir and Symptoms in Adults With Postacute Sequelae of SARS-CoV-2 Infection: The STOP-PASC Randomized Clinical Trial. JAMA Intern Med. 2024 Sep 1;184(9):1024-1034.. Erratum in: JAMA Intern Med. 2024 Sep 1;184(9):1137.
- Yasacı Z, Mustafaoglu R, Ozgur O, Kuveloglu B, Esen Y, Ozmen O, Yalcinkaya EY. Virtual recovery: efficacy of telerehabilitation on dyspnea, pain, and functional capacity in post-COVID-19 syndrome. Ir J Med Sci. 2025.
- Carpallo-Porcar B, Calvo S, Pérez-Palomares S, Blázquez-Pérez L, Brandín-de la Cruz N, Jiménez-Sánchez C. Perceptions and Experiences of a Multimodal Rehabilitation Program for People With Post-Acute COVID-19: A Qualitative Study. Health Expect. e: 2025 Jun;28(3), 2025.
- Daynes E, Evans RA, Greening NJ, Bishop NC, Yates T, Lozano-Rojas D, Ntotsis K, Richardson M, Baldwin MM, Hamrouni M, Hume E, McAuley H, Mills G, Megaritis D, Roberts M, Bolton CE, Chalmers JD, Chalder T, Docherty AB, Elneima O, Harrison EM, Harris VC, Ho LP, Horsley A, Houchen-Wolloff L, Leavy OC, Marks M, Poinasamy K, Quint JK, Raman B, Saunders RM, Shikotra A, Singapuri A, Sereno M, Terry S, Wain LV, Man WD, Echevarria C, Vogiatzis I, Brightling C, Singh SJ; PHOSP-COVID Study Collaborative Group. Post-Hospitalisation COVID-19 Rehabilitation (PHOSP-R): a randomised controlled trial of exercise-based rehabilitation. Eur Respir J. 2: 2025 ;65(5), 22 May 2025.
- Seers K, Nichols VP, Bruce J, Ennis S, Heine P, Patel S, Sandhu HK, Underwood M, McGregor G; our REGAIN collaborators.; REGAIN collaborators.. Qualitative evaluation of the Rehabilitation Exercise and psycholoGical support After COVID-19 InfectioN (REGAIN) randomised controlled trial (RCT): 'you are not alone'. BMJ Open. e: 2025 Jan 29;15(1), 2025.
- Weix NM, Shake HM, Duran Saavedra AF, Clingan HE, Hernandez VC, Johnson GM, Hansen AD, Collins DM, Pryor LE, Kitchens R, Armstead A, Hilton C. Cognitive Interventions and Rehabilitation to Address Long-COVID Symptoms: A Systematic Review. OTJR (Thorofare N J). 2025 May 19:15394492251328310.
- Generalitat de Catalunya. Sistema d’Informació per a la Vigilància d’Infeccions a Catalunya. Available online: https://sivic.salut. gencat.cat/ (accessed on 3 July 2025).
- Dinnes, J.; Deeks, J.J.; Berhane, S.; Taylor, M.; Adriano, A.; Davenport, C.; Dittrich, S.; Emperador, D.; Takwoingi, Y. ; Cunningham,J. ; et al. Cochrane COVID-19 Diagnostic Test Accuracy Group 2. Rapid point-of-care antigen and molecular-based tests for diagnosis of SARS-CoV-2 infection. Cochrane Database Syst. Rev. 2021, 3, CD013705. [Google Scholar]
- World Health Organization. Available online: https://iris.who.int/bitstream/handle/10665/360580/WHO-2019-nCoVSurveillanceGuidance-2022.2-eng.pdf (accessed on 18 September 2024).
- Ford ND, Baca S, Dalton AF, Koumans EH, Raykin J, Patel PR, Saydah S. Use and Characteristics of Clinical Coding for Post-COVID Conditions in a Retrospective US Cohort. J Public Health Manag Pract. 2025 Mar 5. Epub ahead of print. [CrossRef] [PubMed]
- Hendrix N, Parikh RV, Taskier M, Walter G, Rochlin I, Saydah S, Koumans EH, Rincón-Guevara O, Rehkopf DH, Phillips RL. Heterogeneity of diagnosis and documentation of post-COVID conditions in primary care: A machine learning analysis. PLoS One. 2025 May 16;20(5):e0324017. PMCID: PMC12083802. [CrossRef]
- Gómez-Carballa, A.; Bello, X.; Pardo-Seco, J.; Pérez del Molino, M.L.; Martiñón-Torres, F.; Salas, A. Phylogeography of SARS-CoV-2 pandemic in Spain: A story of multiple introductions, micro-geographic stratification, founder effects, and super-spreaders. Zool. Res. 2020, 41, 1–16. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Long COVID cases detected every six months (1–6 indicate the first half of the year, and 7–12 the second half). The year of the first COVID-19 infection is also shown, indicating whether vaccination occurred prior to infection (V preinf), after infection (V postinf), or not at all (No V). The dashed line marks the end of the protocol recommending testing for any symptomatic patient. The increase observed in 2024 coincides with active case finding in the CST via survey. In some Long COVID records, the exact date of infection is uncertain, likely due to previous unreported self-diagnosis by the patient.
Figure 1.
Long COVID cases detected every six months (1–6 indicate the first half of the year, and 7–12 the second half). The year of the first COVID-19 infection is also shown, indicating whether vaccination occurred prior to infection (V preinf), after infection (V postinf), or not at all (No V). The dashed line marks the end of the protocol recommending testing for any symptomatic patient. The increase observed in 2024 coincides with active case finding in the CST via survey. In some Long COVID records, the exact date of infection is uncertain, likely due to previous unreported self-diagnosis by the patient.
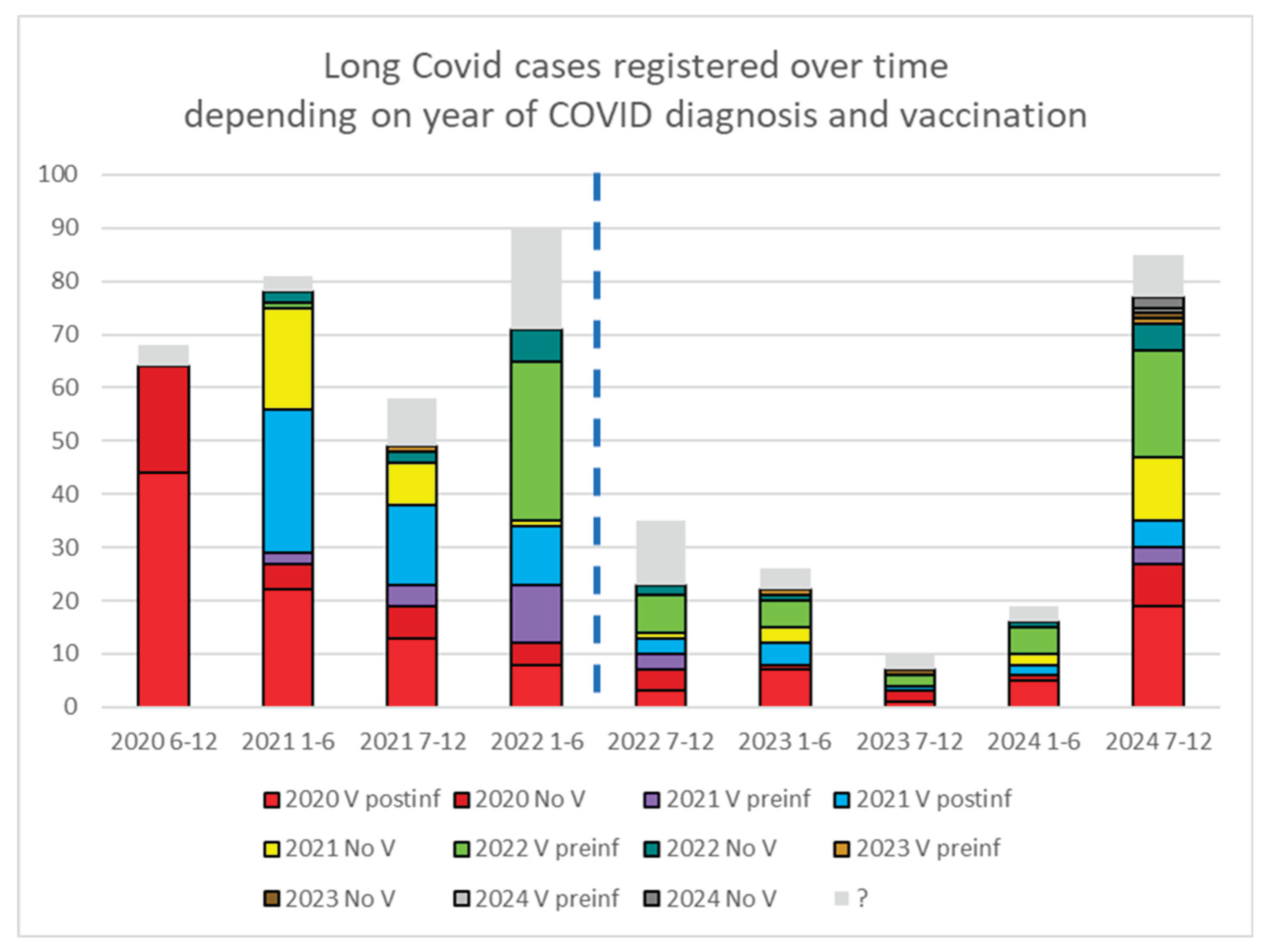
Figure 2.
Period of the first SARS-CoV-2 infection. The number of detected cases decreased dramatically in March 2022, after the end of protocols that required case detection beyond symptomatic patients.
Figure 2.
Period of the first SARS-CoV-2 infection. The number of detected cases decreased dramatically in March 2022, after the end of protocols that required case detection beyond symptomatic patients.
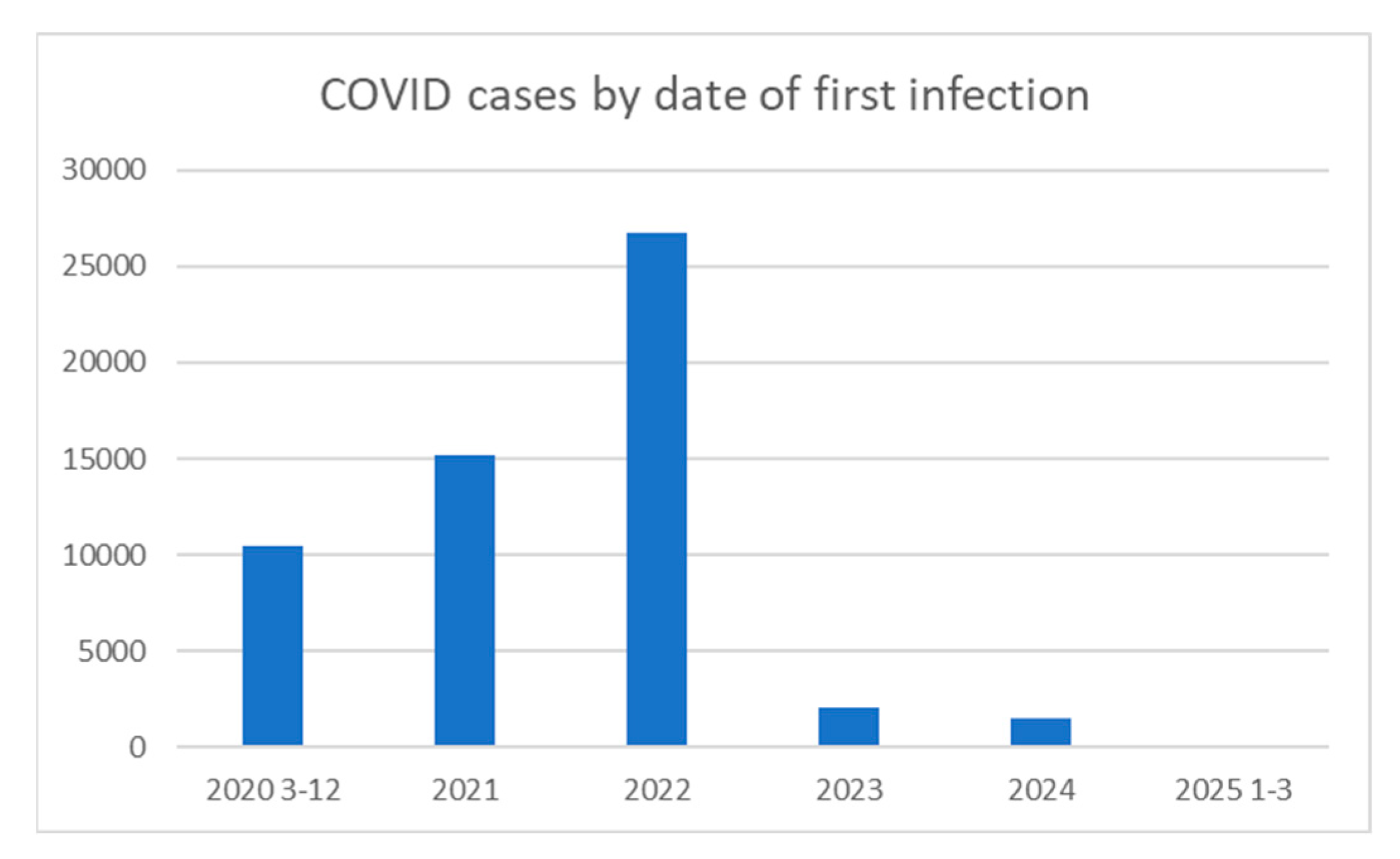
Figure 3.
Cumulative thrombotic events from March 2020 to March 2025, stratified by age (≥60 vs. <60 years), vaccination status (Vaccinated [V] vs. Non-Vaccinated [NoV]) and SARS-CoV-2 infection (CoV or NoCoV, together with the temporal relation to thrombotic events -before (preThr) or after (postThr) the event-. Annual thrombosis estimates (2020, 2025) were extrapolated from monthly averages of recorded events, adjusting for months with missing data.
Figure 3.
Cumulative thrombotic events from March 2020 to March 2025, stratified by age (≥60 vs. <60 years), vaccination status (Vaccinated [V] vs. Non-Vaccinated [NoV]) and SARS-CoV-2 infection (CoV or NoCoV, together with the temporal relation to thrombotic events -before (preThr) or after (postThr) the event-. Annual thrombosis estimates (2020, 2025) were extrapolated from monthly averages of recorded events, adjusting for months with missing data.
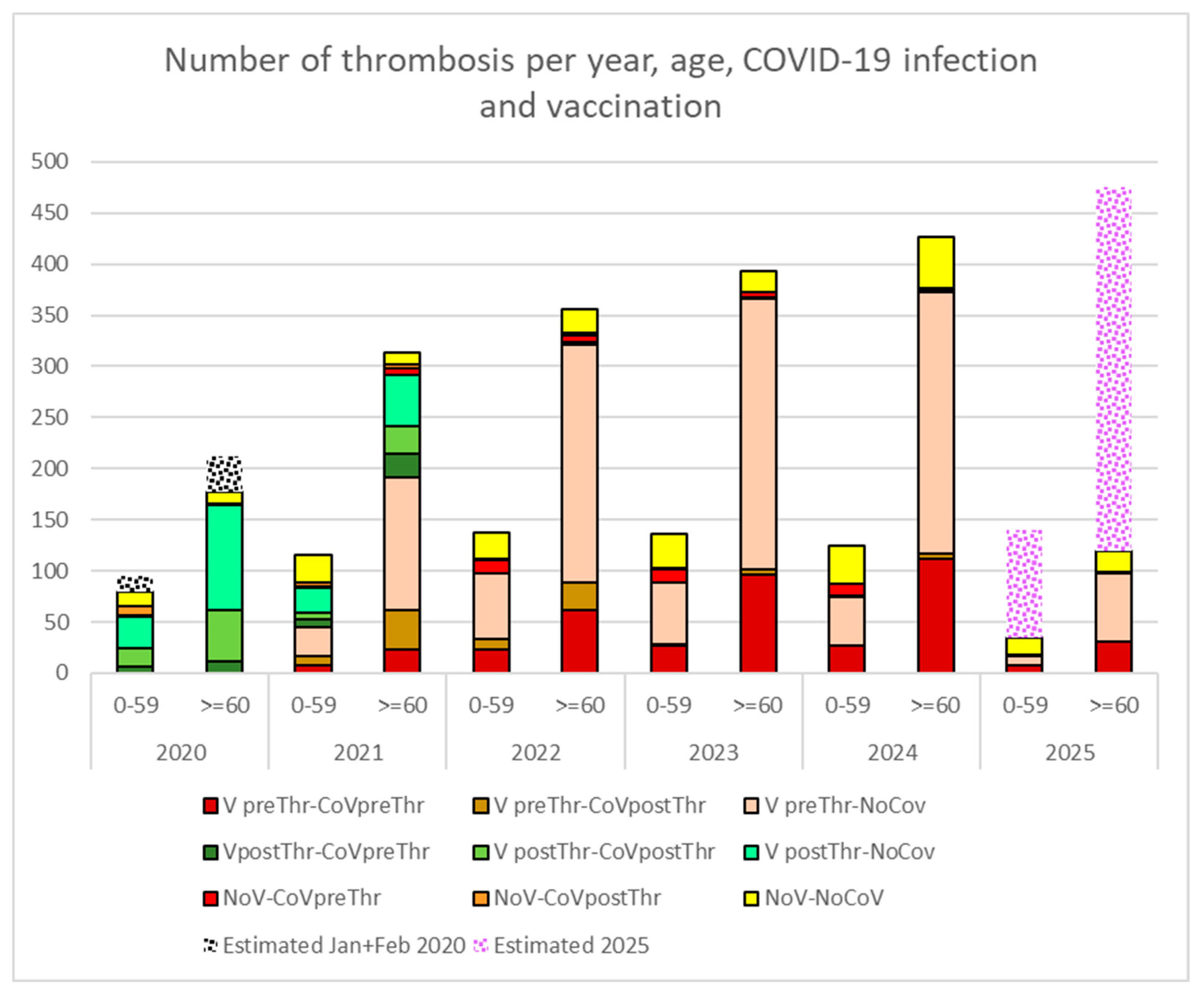
Table 1.
Prevalence of long covid by age and gender among the CST population.
| Longcovid | Total | |||||
| Post survey | Pre survey | Long covid | No long COVID | Population | ||
| Women/age | 80 | 242 | 322 (3.3‰) | 96676 | 96998 | |
| 0-29 | 2 | 19 | 21 (0.7‰) | 30907 | 30928 | |
| 30-59 | 63 | 171 | 234 (5.6‰) | 41530 | 41764 | |
| ≥60 | 15 | 52 | 67 (2.7‰) | 24239 | 24306 | |
| Men/age | 19 | 134 | 153 (1.6‰) | 95500 | 95653 | |
| 0-29 | 1 | 16 | 17 (0.5‰) | 32850 | 32867 | |
| 30-59 | 11 | 90 | 101(2.3‰) | 43054 | 43155 | |
| ≥60 | 7 | 28 | 35 (1.7‰) | 19596 | 19631 | |
| Total general | 99 | 376 | 475 (2.4‰) | 192176 | 192651 | |
Table 2.
Long COVID registered cases (LC) depending on the number of registered infections (n infections), including those without a confirmed infection date (?) and having received at least one vaccine prior (V preinf) or after (V postinf) the first COVID-19 infection.
Table 2.
Long COVID registered cases (LC) depending on the number of registered infections (n infections), including those without a confirmed infection date (?) and having received at least one vaccine prior (V preinf) or after (V postinf) the first COVID-19 infection.
| n infection | V | CoV | LC | (%) | OR vs 1inf | p | vs V preinf | p |
|---|---|---|---|---|---|---|---|---|
| ? | V | 60985 | 45 | 0.07% | ||||
| ? | No V | 75664 | 21 | 0.03% | ||||
| 1 | V preinf | 18386 | 46 | 0.25% | ||||
| 1 | V postinf | 9889 | 168 | 1.67% | ||||
| 1 | No V | 21608 | 94 | 0.43% | ||||
| 2 | V preinf | 2948 | 43 | 1.44% | 5.8 | <0.0001 | ||
| 2 | V postinf | 335 | 14 | 4.01% | 2.4 | 0.001 | ||
| 2 | No V | 1833 | 18 | 0.97% | 2.2 | 0.001 | ||
| >=3 | V preinf | 355 | 10 | 2.74% | 11.0 | <0.0001 | ||
| >=3 | V postinf | 37 | 8 | 17.78% | 10.6 | <0.0001 | 6.49 | <0.0001 |
| >=3 | No V | 136 | 8 | 5.56% | 12.8 | <0.0001 | 2.03 | 0.06 |
Table 3.
Percentage of each symptom among patients with Long COVID diagnoses and percentage of patients recovered spontaneously. Absolute numbers of respondents uncertain about their diagnosis and respondents without Long COVID are also included.
Table 3.
Percentage of each symptom among patients with Long COVID diagnoses and percentage of patients recovered spontaneously. Absolute numbers of respondents uncertain about their diagnosis and respondents without Long COVID are also included.
| Responders with Long covid diagnosis: |
Yes 368 |
Yes, and I'm still symptomatic | Yes, but I already feel good |
Unsure 281 | No 1222 | |
|---|---|---|---|---|---|---|
| Physical complains | ||||||
| Anosmia or dysgeusia | 23.4% | 86 | 20 | 18.9% | 40 | 39 |
| Shortness of breath | 27.2% | 100 | 28 | 21.9% | 74 | 66 |
| Headache | 22.3% | 82 | 23 | 21.9% | 75 | 79 |
| Joint pain | 32.9% | 121 | 58 | 32.4% | 135 | 160 |
| Persistent Fatigue | 41.6% | 153 | 68 | 30.8% | 159 | 209 |
| Psychological complains | ||||||
| Memory complains | 30.7% | 113 | 35 | 23.6% | 91 | 104 |
| Lack of concentration | 31.0% | 114 | 37 | 24.5% | 86 | 131 |
| Depression | 16.6% | 61 | 20 | 24.7% | 52 | 69 |
| Anxiety | 31.3% | 115 | 48 | 29.4% | 101 | 147 |
| Sleep complains | 26.6% | 98 | 34 | 25.8% | 98 | 151 |
| Functional impairment | ||||||
| Home task | 20.4% | 75 | 19 | 20.2% | 55 | 52 |
| With friends or relatives | 17.4% | 64 | 14 | 17.9% | 42 | 62 |
| Impaired personal hygiene | 4.1% | 15 | 5 | 25.0% | 11 | 16 |
| Work interference | 25.8% | 95 | 35 | 26.9% | 69 | 79 |
| COVID-19 related sick leave | 37.5% | 138 | 75 | 35.2% | 127 | 541 |
Table 4.
Percentages of responders reporting longcovid syndrome are related to the number of COVID 19 infections and the number of vaccines (V) received. Odds radio (OR) between Non vaccinated patients (NoV) and Vaccinated (V) are presented per each number of infection.
Table 4.
Percentages of responders reporting longcovid syndrome are related to the number of COVID 19 infections and the number of vaccines (V) received. Odds radio (OR) between Non vaccinated patients (NoV) and Vaccinated (V) are presented per each number of infection.
| No V | V | OR | V | |||||||||
| NoV vs V | 1 | 2 | 3 | >=3 | ||||||||
| 1 COVID-19 infection | 50 | 1008 | 75 | 394 | 364 | 175 | ||||||
| No | 38 | 717 | 49 | 266 | 269 | 133 | ||||||
| Unsure | 6 | 143 | 6 | 58 | 59 | 20 | ||||||
| Long CoV still symptomatic | 5 | 10.0% | 89 | 8.8% | 10 | 13.3% | 47 | 11.9% | 20 | 5.5% | 12 | 6.9% |
| Transient Long Cov | 1 | 59 | OR 1.13 | 10 | 23 | 16 | 10 | |||||
|
2 COVID 19 infections |
21 | 574 | 57 | 231 | 217 | 69 | ||||||
| No | 12 | 343 | 28 | 132 | 141 | 42 | ||||||
| Unsure | 2 | 95 | 9 | 42 | 32 | 12 | ||||||
| Long CoV still symptomatic | 4 | 19.0% | 84 | 14.6% | 15 | 26.3% | 36 | 15.6% | 26 | 12.0% | 7 | 10.1% |
| Transient Long Cov | 3 | 52 | OR 1.30 | 5 | 21 | 18 | 8 | |||||
|
3 COVID 19 infections |
6 | 173 | 29 | 75 | 55 | 14 | ||||||
| No | 2 | 78 | 11 | 37 | 23 | 7 | ||||||
| Unsure | 30 | 6 | 13 | 9 | 2 | |||||||
| Long CoV still symptomatic | 2 | 33.3% | 43 | 24.9% | 11 | 37.9% | 15 | 20.0% | 14 | 25.5% | 3 | 21.4% |
| Transient Long Cov | 2 | 22 | OR 1.34 | 1 | 10 | 9 | 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



