
Submitted:
20 August 2025
Posted:
21 August 2025
You are already at the latest version
Abstract
Background: Trousseau’s syndrome, characterized by recurrent thromboembolic events and non-bacterial thrombotic endocarditis, represents a severe paraneoplastic condition associated with poor prognosis in cancer patients. Methods: We describe a case of a 63-year-old male presenting with ischemic stroke and mitral valve marantic endocarditis, ultimately diagnosed with pulmonary adeno-carcinoma. The case description is followed by a brief review of the current literature on the condition. Discussion and Conclusion: This case highlights the complexity of diagnosing and managing Trousseau’s syndrome. Early recognition, appropriate anti-coagulation strategies, and the need for multidisciplinary management are crucial to improve the outcomes and the quality of life of cancer patients.
Keywords:
Trousseau’s syndrome
; venous thromboembolism
; marantic endocarditis
; cancer
1. Introduction
Thromboembolic events represent the second leading cause of death among patients with malignant neoplasms [1] and may even constitute the first clinical manifestation of an underlying cancer [2]. The combination of recurrent venous and/or arterial thromboses in association with non-bacterial (marantic) endocarditis is known as Trousseau’s syndrome. This condition was first described in 1865 by Armand Trousseau [3], who self-diagnosed it two years later, shortly before his death due to gastric cancer [4]. Trousseau’s syndrome is associated with poor prognosis and reduced quality of life in cancer patients [5]. However, specific histological subtypes and targeted oncologic therapies may influence clinical outcomes [5] making early recognition and diagnosis essential. Here, we report the case of a 63-year-old man diagnosed with Trousseau’s syndrome, followed by a brief review of the current literature on this condition.
2. Ethical Statement and Patient Consent
All procedures at our institution are performed following the ethical standards set by institutional and national research committees and the 1975 Helsinki Declaration and its amendments. Our institution does not require ethical approval for reporting individual cases or case series. The patient’s consent was obtained for publication of this report and images.
3. Case Report
In March 2022, a 63-year-old Caucasian male patient presented to our Emergency Department (ED) with dysphagia and dysarthria, which had begun approximately seven hours earlier. Upon arrival, he was alert, aphasic, with a right-sided facial nerve deficit, and intact Mingazzini signs. The National Institutes of health Stroke Scale (NIHSS) score was 6, while the modified Rankin Scale score was 3. Cardiac auscultation revealed a regular rhythm with a 3/6 systolic murmur. The remainder of the physical examination was unremarkable.
At admission, the patient’s body weight was 75 kg, with a body mass index (BMI) of 26 kg/m². Laboratory tests showed a white blood cell (WBC) count of 9,670/μL (reference range: 4,000–10,000/μL), hemoglobin of 11 g/dL (13–17 g/dL), platelet count of 170,000/μL (150,000–400,000/μL), markedly elevated D-dimer at 21,268 EEU (0–500 EEU), serum creatinine of 0.76 mg/dL (0.6–1.2 mg/dL), and a negative C-reactive protein (CRP) test (<5 mg/L). Autoimmune markers including antinuclear antibodies (ANA), extractable nuclear antigens (ENA), anticardiolipin antibodies, and β2-microglobulin were negative.
Past medical history included hypertension, hyperuricemia, and follicular lymphoma, initially treated with the CHOP + bendamustine regimen and later with Rituximab. One month earlier, enlarged lymph nodes with poorly defined margins raised suspicion for disease recurrence, but treatment was deferred due to the absence of GELF criteria [6]. Two weeks before the presentation, the patient developed left femoropopliteal deep vein thrombosis and started edoxaban 60 mg daily. His other chronic medications included ramipril and allopurinol. The patient was also a heavy smoker (35 pack-years).
A cranial CT scan and CT angiography revealed ischemic lesions in the left post-central insular gyrus and the left occipital gyrus, along with a complete occlusion of the left middle cerebral artery (Figure 1). No indication for endovascular treatment was found. Follow-up cranial CT scans excluded hemorrhagic infarctions. Anticoagulation with edoxaban was continued. No arrhythmias were detected on Holter ECG.
Transthoracic echocardiography (TTE) showed normal left ventricular systolic function with severe mitral regurgitation but no evidence of endocavitary masses. A transesophageal echocardiogram (TOE) ruled out a patent foramen ovale and identified endocarditis of the mitral valve, with distal thickening of both mitral leaflets (maximum 3 mm) resulting in multiple, predominantly eccentric, regurgitant jets, causing severe mitral regurgitation (Figure 2), with no indications for urgent/emergency cardiac surgery. Considering findings suggestive of endocarditis and coexisting aspiration pneumonia, empirical antibiotic therapy was initiated with ceftriaxone, vancomycin, and clarithromycin. However, the patient remained afebrile, with negative blood cultures, WBC counts 6390 /μL and stable CRP levels between 10-12 mg/L (likely related to the pneumonia). Serial procalcitonin (PCT) levels were always negative.
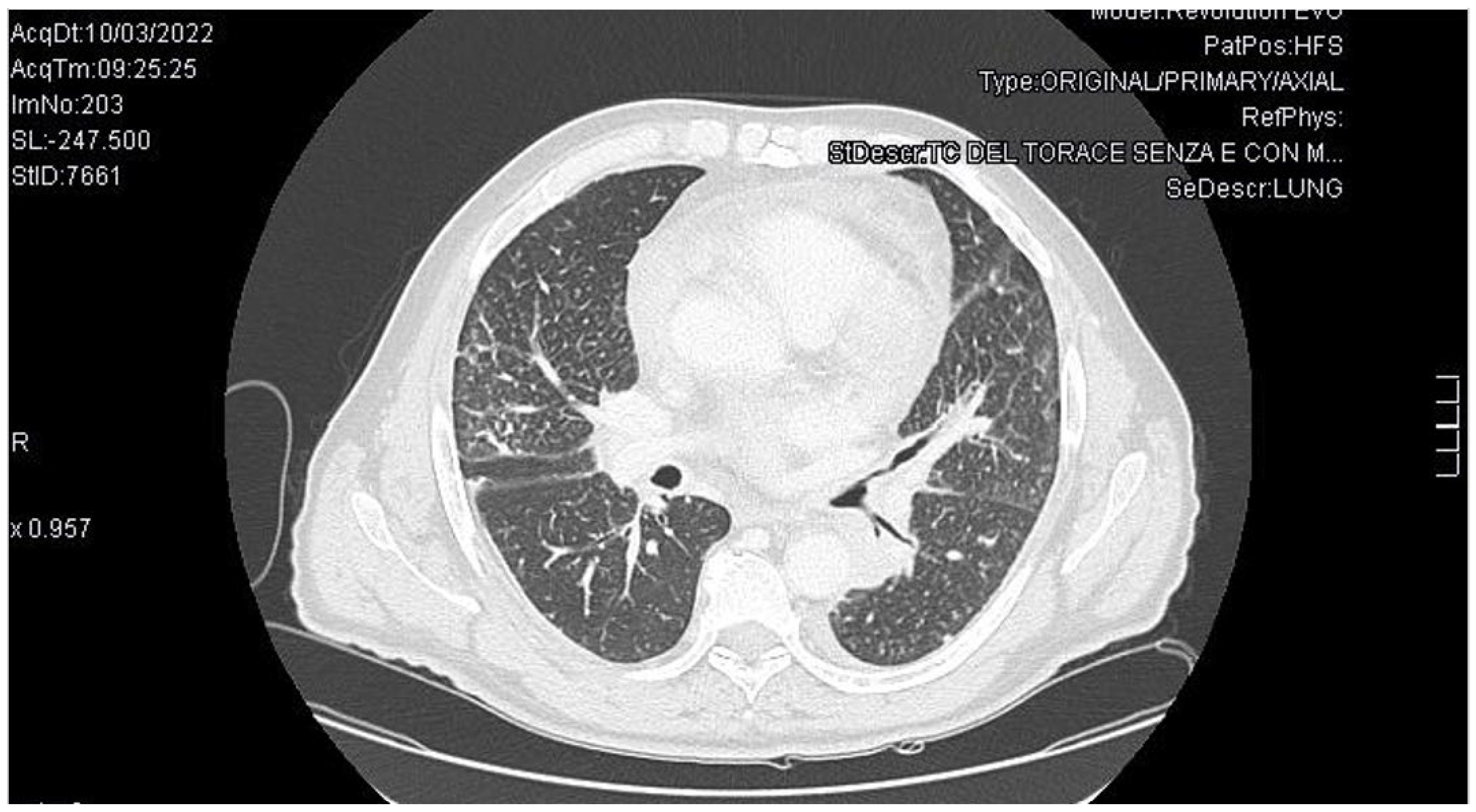
Therefore, given the negative blood cultures and absence of fever or other minor criteria, the patient did not meet the Duke’s criteria for infective endocarditis [7]. Suspecting lymphoma recurrence, a CT scan of the neck, chest, and abdomen was performed. The examination revealed ischemic-infarct areas in the spleen and a tissue mass with contrast enhancement in the left hilar para-aortic region causing narrowing of the bronchial structures (Figure 3). Consequently, bronchoscopy was performed with biopsy of the left upper lobe bronchus.
Soon after, the patient developed thrombosis of the proximal left axillary artery, right axillary vein at a PICC (Peripherally Inserted Central Catheters) line site. Edoxaban was replaced by LMWH at an anticoagulant dosage. The pulmonary biopsy report revealed the presence of pulmonary adenocarcinoma. The patient passed away two months later due to progression of malignancy.
4. Discussion
According to the ESC Cardioncology guidelines [1] malignancies increase the risk of venous thromboembolism (VTE) by fivefold and the risk of arterial thromboembolism by twofold. In the treatment and secondary prevention of venous thromboembolism in cancer patients, the guidelines recommend LMWH. LMWH is generally preferred to unfractioned heparin (UFH) because LMWH does not require blood test monitoring and hospitalization. LMWH was also more effective than warfarin in reducing the risk of VTE without increasing the risk of bleeding in patients with high thrombotic risk [8,9]. Direct acting oral anticoagulants (DOACs) such as edoxaban , rivaroxaban or apixaban [10,11,12] are potential alternatives (Table 1).
In head-to-head trials with LMWH, all three DOACs were non-inferior in treating venous thromboembolism; however, only apixaban, in the CARAVAGGIO trial, did not increase the bleeding risk. Consequently, the 2023 update of the ASCO guidelines [13] included apixaban amog the preferred DOACs. In the API-CAT trial [14] reduced-dose apixaban (2.5 mg twice daily) was found to be non-inferior to the full-dose regimen (5 mg twice daily) in preventing venous thromboembolism in cancer patients who had already completed 6 months of anticoagulant therapy for VTE/PE (pulmonary embolism). Moreover, the reduced dose was associated with a lower rate of clinically relevant bleeding compared to the full-dose regimen.
Nevertheless, DOACs are contraindicated in patients with one of the following bleeding factors: unoperated gastrointestinal (GI) or genitourinary (GU) malignancies, history of recent bleeding or within 7 days of major surgery, significant thrombocytopaenia (platelet count < 50 000/μL), severe renal dysfunction (creatinine clearance (CrCl <15 mL/min), or GI comorbidities. The minimal duration of anticoagulation is 6 months [1,15]. However, patients with cancer are also at high risk of bleeding during anticoagulant treatment. For this reason, a periodic assessment of the risk/benefit ratio should be performed. The most famous and well validated score to calculate VTE in cancer patients is the Khorana score [16] while existing risk scores for bleeding perform poorly after cancer associated thromboses (CAT) [17].
It is mandatory to highlight that the patient described in the report came to our attention before the publication of the 2022 ESC cardio-oncology guidelines and the 2023 update of the ASCO guidelines. He developed episodes of both venous and arterial thrombotic non-infective (marantic) endocarditis with multiple embolic events involving the brain and spleen. Recurrent thrombosis with no other explanation, associated with marantic endocarditis, in cancer patient, is known as Trousseau’s syndrome [4]. Although neither the ASCO guidelines nor the ESC cardio-oncology guidelines specifically mention it, Trousseau’s syndrome is associated with reduced quality of life and worsened prognosis [5]. The overall incidence in hospitalized cancer patients was 8.0 cases per 1000 person-years (p-y), with the highest incidence in the first year after cancer diagnosis (15.0 cases per 1000 p-y), decreasing to 6.3 cases per 1000 p-y in the second year, and 4.2 cases per 1000 p-y thereafter [18]. A study by Sørensen and coworkers found that one-year survival rate for the cancer group with VTE was 12%, compared with 36% in the control group without VTE [19].
This paraneoplastic syndrome involves hypercoagulability related to patient, cancer and treatment (Table 2). Patient-related factors include age, inactivity, and cardiovascular comorbidities. Cancer-related factors include tissue factor (TF), plasminogen activator inhibitor (PAI-1), mucins, cytokines, and hypoxia [4]. TF directly induces the conversion of factor VII to factor VIIa, resulting in the constitutive activation of the coagulation cascade. It has been reported that, in addition to coagulation, TF is also associated with cancer metastasis and angiogenesis [20]. Moreover, the sialic acid moieties of mucin from adenocarcinomas cause a nonenzymatic activation of factor X. All in all, hypoxia (decreased oxygenation) could increase the expression of genes that facilitate coagulation, including TF and PAI-1 [4]. PAI-1 inhibits the activation of plasminogen, a key step in the dissolution of blood clots. On the other hand, about treatment related factors, chemotherapeutic agents such as platinum compounds, hormonal agents, tamoxifen, growth factors (granulocyte colony-stimulating factor and erythropoiesis-stimulating agents) and antiangiogenic agents increase the risk of thrombosis [20]. Chemotherapy itself, independently of the underlying pathophysiology of the neoplastic process, induces a hypercoagulable state by also acting on TF and PAI-1. Indeed, Wrzeszcz et al. demonstrated that adjuvant therapy in patients with invasive breast cancer significantly increased plasma concentrations of TF and PAI-1 [21]. However, when anticoagulant therapy is added, the hemostatic balance may shift toward bleeding risk. In fact, several studies have shown that the concomitant administration of DOACs and chemotherapeutic agents increases the risk of bleeding, primarily due to pharmacokinetic interactions involving CYP3A4 and P-glycoprotein (P-gp) inhibitors or inducers. The tyrosine kinase inhibitors (TKIs) represent the most clinically significant class of agents in terms of drug–drug interactions (DDIs) with DOACs, as they are potent inhibitors of P-gp [22].
Nowadays CVCs (Central Venous Catheter) are gaining a pivotal role for the long-term administration of anticancer drugs and blood sampling, but they are associated to an increased thrombotic risk [23], as illustrated by the case presented.
Several types of cancer are associated with the Trousseau’s syndrome. Of these, lung cancer is most frequently associated with malignancy-related ischaemic stroke [24]. Although the diagnosis is generally associated with a worse prognosis in such patients, early recognition—particularly with regard to histological subtypes—may improve clinical outcomes. In a recent study, Yoshimine et al. [5] observed that patients with more favourable prognoses exhibited non-adenocarcinoma histotypes, a high frequency of EGFR mutations, and were more likely to receive immune checkpoint inhibitor (ICI) therapy. Based on these observations, the authors propose that when Trousseau’s syndrome develops in patients with lung cancer, continuous heparin therapy should be initiated, and genetic testing along with PD-L1 immunostaining should be promptly performed to guide appropriate treatment. However, this study has several limitations, including its monocentric design and limited sample size. Therefore, further research is warranted to validate these findings.
Additionally, since our patient did not meet the Duke’s criteria and had an active tumor, the endocarditis seen on TOE is categorized as marantic endocarditis [7], t ypically linked to paraneoplastic hypercoagulability from solid tumors, especially lung, gastrointestinal, and pancreatic cancers. This form of endocarditis is often underestimated on TTE but should be suspected in the presence of Trousseau’s syndrome [25]. The mitral valve is the most frequently affected. Its involvement is associated with a high rate of clinical complications and mortality [26]. The ESC guidelines recommend LMWH as the first-line treatment [7] in marantic endocarditis. Valid alternatives may include vitamin K antagonists (VKA) or UFH. There are no data to support the use of direct oral anticoagulants in non-bacterial thrombotic endocarditis (NBTE) [27]. The role of surgery is controversial, but it may be considered in select cases with significant persistent valvular dysfunction [28]. ntibiotics are not indicated.

| Therapy | Indications | Advantages | Limitations/Contraindications |
|---|---|---|---|
| Low Molecular Weight Heparin (LMWH) | First-line for treatment and prevention of VTE in cancer patients. | Proven efficacy, reduced VTE vs warfarin, easy dosing | Injection route, bleeding risk, impaired renal function. |
| Direct Oral Anticoagulants (DOACs)#break# (edoxaban, rivaroxaban, apixaban) |
Alternative to LMWH in selected patients. | Oral administration, non-inferior efficacy. Apixaban don not increased bleeding risk. | Avoid in unresected GI/GU cancers, CrCl <15, platelets <50k, recent surgery, bleeding risk |
| Vitamin K Antagonists (VKAs) | Alternative if DOACs/LMWH not suitable | Oral, long experience | Drug–food interactions, INR monitoring required, less preferred |
| Unfractionated Heparin (UFH) | Hospitalized patients, rapid reversal needed | Short half-life, reversible | Requires monitoring (aPTT), IV route |
| Anticoagulation Duration | ≥6 months recommended (individualized) | Reduces recurrence | Reassess bleeding periodically, especially in advanced cancer |
| Category | Risk Factors |
|---|---|
| Patient-related | Older age, immobility, comorbidities (e.g., hypertension), history of thrombosis |
| Tumor-related | Histological type (especially adenocarcinoma), tumor burden, metastasis |
| Biological mediators | Tissue factor (TF), mucins, PAI-1, cytokines, hypoxia |
| Treatment-related | Chemotherapy (e.g., platinum compounds), hormonal therapy, antiangiogenics |
| Drug interactions | DOAC metabolism affected by CYP3A4/P-gp inhibitors (e.g., tyrosine kinase inhibitors) |
| Procedural | Central venous catheters (CVCs), recent surgery |
5. Conclusions
Our case highlights the severity of Trousseau’s syndrome and marantic endocarditis, conditions that should be suspected in cancer patients. Early diagnosis and appropriate anticoagulation therapy can significantly reduce mortality and morbidity. However, the risk of bleeding must be weighed, especially in advanced cancer patients, necessitating a multidisciplinary approach and a stretched follow-up involving an expert in thrombosis and hemostasis.
Author Contributions
L.C.: conceptualization, writing up. A.S. graphical abstract. M.M., A.B., A.G., A.P.P.: supervision. M.P, M.B. and R.M.: supervision; final revision. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of Mayo Clinic (IRB#22-004000 2024-04-20) for studies involving humans.
Informed Consent Statement
Not applicable as this study involves a retrospective review of previously collected clinical data and all the reviewed data were de-identified to protect patient privacy.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Acknowledgments
Italian Ministry of Health, RC2025.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ANA: | antinuclear antibodies |
| ASCO: | American Society of Clinical Oncology |
| CAT: | Cancer associated thromboses |
| CRP: | C-reactive protein |
| CVC: | Central Venous Catheter |
| DDIs: | drug–drug interactions |
| DOAC: | Direct oral anticoagulant |
| ED: | Emergency department |
| ENA: | extractable nuclear antigens |
| ESC: | European Society of Cardiology |
| EEU: | Enzyme-Linked Immunosorbent Assay Equivalent Units |
| GI: | gastrointestinal |
| GU: | genitourinary |
| ICI: | immune checkpoint inhibitor |
| LMWH: | low-molecular-weight heparin |
| NBTE: | non-bacterial thrombotic endocarditis |
| NIHSS: | National Institutes of health Stroke Scale |
| PAI-1: | plasminogen activator inhibitor |
| PE: | Pulmonary embolism |
| PICC: | peripherally inserted central catheter |
| P-gp: | P-glycoprotein |
| TF: | tissue factor |
| TKIs: | Tyrosine kinase inhibitors |
| TOE: | transesophageal echocardiogram |
| TTE: | Transthoracic echocardiography |
| UFH: | unfractioned heparin |
| VKA: | vitamin K antagonists |
| VTE: | venous thromboembolism |
| WBC: | white blood cell |
References
- Lyon, A.R.; López-Fernández, T.; Couch, L.S.; Asteggiano, R.; Aznar, M.C.; Bergler-Klein, J.; et al. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur. Heart J. 2022, 43, 4229–4361. [Google Scholar] [CrossRef]
- Mulder, F.I.; Horváth-Puhó, E.; van Es, N.; et al. Risk scores for occult cancer in patients with unprovoked venous thromboembolism: Results from an individual patient data meta-analysis. J. Thromb. Haemost. 2020, 18, 2622–2628. [Google Scholar] [CrossRef]
- Trousseau, A. Lectures on Clinical Medicine; The New Sydenham Society: London, UK, 1868; Volume 5, pp. 281–331. [Google Scholar]
- Varki, A. Trousseau’s syndrome: Multiple definitions and multiple mechanisms. Blood 2007, 110, 1723–1729. [Google Scholar] [CrossRef] [PubMed]
- Yoshimine, K.; Ooka, Y.; Ochi, N.; et al. Trousseau’s Syndrome in Lung Cancer Patients: A Retrospective Study in a Japanese Community Hospital. Cureus 2024, 16, e68400. [Google Scholar] [CrossRef] [PubMed]
- Brice, P.; Bastion, Y.; Lepage, E.; et al. Comparison in Low-Tumor-Burden Follicular Lymphomas Between an Initial No-Treatment Policy, Prednimustine, or Interferon Alfa: A Randomized Study From the Groupe D’Etude Des Lymphomes Folliculaires. J. Clin. Oncol. 1997, 15, 1110–1117. [Google Scholar] [CrossRef] [PubMed]
- Delgado, V.; Ajmone Marsan, N.; de Waha, S.; et al. 2023 ESC Guidelines for the management of endocarditis. Eur. Heart J. 2023, 44, 3948–4042. [Google Scholar] [CrossRef]
- Lee, A.Y.Y.; Levine, M.N.; Baker, R.I.; et al. Low-Molecular-Weight Heparin versus a Coumarin for the Prevention of Recurrent Venous Thromboembolism in Patients with Cancer. N. Engl. J. Med. 2003, 349, 146–153. [Google Scholar] [CrossRef]
- Woodruff, S.; Lee, A.Y.Y.; Kakkar, A.K.; et al. Low-molecular-weight-heparin versus a coumarin for the prevention of recurrent venous thromboembolism in high- and low-risk patients with active cancer: A post hoc analysis of the CLOT Study. J. Thromb. Thrombolysis 2019, 47, 495–504. [Google Scholar] [CrossRef]
- Raskob, G.E.; van Es, N.; Verhamme, P.; et al. Edoxaban for the Treatment of Cancer-Associated Venous Thromboembolism. N. Engl. J. Med. 2018, 378, 615–624. [Google Scholar] [CrossRef]
- Young, A.M.; Marshall, A.; Thirlwall, J.; et al. Comparison of an Oral Factor Xa Inhibitor With Low Molecular Weight Heparin in Patients With Cancer With Venous Thromboembolism: Results of a Randomized Trial (SELECT-D). J. Clin. Oncol. 2018, 36, 2017–2023. [Google Scholar] [CrossRef]
- Agnelli, G.; Becattini, C.; Meyer, G.; et al. Apixaban for the Treatment of Venous Thromboembolism Associated with Cancer. N. Engl. J. Med. 2020, 382, 1599–1607. [Google Scholar] [CrossRef]
- Key, N.S.; Khorana, A.A.; Kuderer, N.M.; et al. Venous Thromboembolism Prophylaxis and Treatment in Patients With Cancer: ASCO Guideline Update. J. Clin. Oncol. 2023, 41, 2373–2390. [Google Scholar] [CrossRef]
- Mahé, I.; Meyer, G.; Puglisi, R.; et al. Extended Reduced-Dose Apixaban for Cancer-Associated Venous Thromboembolism. N. Engl. J. Med. 2025, 392, 1363–1373. [Google Scholar] [CrossRef]
- Key, N.S.; Khorana, A.A.; Kuderer, N.M.; et al. Venous Thromboembolism Prophylaxis and Treatment in Patients With Cancer: ASCO Clinical Practice Guideline Update. J. Clin. Oncol. 2019, 38, 496–520. [Google Scholar] [CrossRef] [PubMed]
- Khorana, A.A.; Kuderer, N.M.; Culakova, E.; Lyman, G.H.; Francis, C.W. Development and validation of a predictive model for chemotherapy-associated thrombosis. Blood 2008, 111, 4902–4907. [Google Scholar] [CrossRef] [PubMed]
- De Winter, M.A.; van Es, N.; van den Berg, M.E.L.; et al. Estimating Bleeding Risk in Patients with Cancer-Associated Thrombosis: Evaluation of Existing Risk Scores and Development of a New Risk Score. Thromb. Haemost. 2022, 122, 818–829. [Google Scholar] [CrossRef] [PubMed]
- Wan, H.; Lin, L.; Li, C.; et al. Clinical characteristics and risk factors for mortality in Trousseau syndrome: A multicenter retrospective cohort study. Thromb. J. 2025, 23, 35. [Google Scholar] [CrossRef]
- Sorensen, H.T.; Mellemkjaer, L.; Olsen, J.H.; Baron, J.A. Prognosis of cancers associated with venous thromboembolism. N. Engl. J. Med. 2000, 343, 1846–1850. [Google Scholar] [CrossRef]
- Ikushima, S.; Ono, R.; Fukuda, K.; Sakayori, M.; Awano, N.; Kondo, K. Trousseau’s syndrome: Cancer-associated thrombosis. Jpn. J. Clin. Oncol. 2016, 46, 204–208. [Google Scholar] [CrossRef]
- Wrzeszcz, K.; Rhone, P.; Kwiatkowska, K.; Ruszkowska-Ciastek, B. Hypercoagulability State Combined with Post-Treatment Hypofibrinolysis in Invasive Breast Cancer: A Seven-Year Follow-Up Evaluating Disease-Free and Overall Survival. Life 2023, 13, 1203. [Google Scholar] [CrossRef]
- Ferri, N.; Colombo, E.; Tenconi, M.; Baldessin, L.; Corsini, A. Drug-Drug Interactions of Direct Oral Anticoagulants (DOACs): From Pharmacological to Clinical Practice. Pharmaceutics 2022, 14, 1120. [Google Scholar] [CrossRef]
- Fioretti, A.M.; Tartaglia, D.; Silvestri, M.; et al. Prevention of Peripherally Inserted Central Catheter (PICC)-Associated Vein Thrombosis in Cancer: A Narrative Review. Biomedicines 2025, 13, 786. [Google Scholar] [CrossRef]
- Toda, Y.; Kano, Y. Three-territory sign in Trousseau’s syndrome. BMJ Case Rep. 2022, 15, e250640. [Google Scholar] [CrossRef]
- Lee, Z.X.; Cheng, J.O.S.; Sharip, M.T.; Hlaing, H.H.; Allison, M. Trousseau’s syndrome with non-bacterial thrombotic endocarditis (NBTE) in a patient with advanced pancreatic cancer. Clin. Med. 2023, 23, 36–37. [Google Scholar] [CrossRef]
- Celeng, C.; Takx, R.A.P. Cancer-associated marantic endocarditis: a rare but relevant complication. Eur. Heart J. Cardiovasc. Imaging 2023, 24, 1627–1628. [Google Scholar] [CrossRef] [PubMed]
- Pengo, V.; Denas, G.; Zoppellaro, G.; et al. Rivaroxaban vs Warfarin in High-Risk Patients with Antiphospholipid Syndrome. Blood 2018, 132, 1365–1371. [Google Scholar] [CrossRef] [PubMed]
- Zmaili, M.; Alzubi, J.; Lo Presti Vega, S.; Ababneh, E.; Xu, B. Non-bacterial thrombotic endocarditis: A state-of-the-art contemporary review. Prog. Cardiovasc. Dis. 2022, 74, 99–110. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Cranial TC scan: ischemic area in the left post-central insular gyrus and the left occipital gyrus.
Figure 1.
Cranial TC scan: ischemic area in the left post-central insular gyrus and the left occipital gyrus.
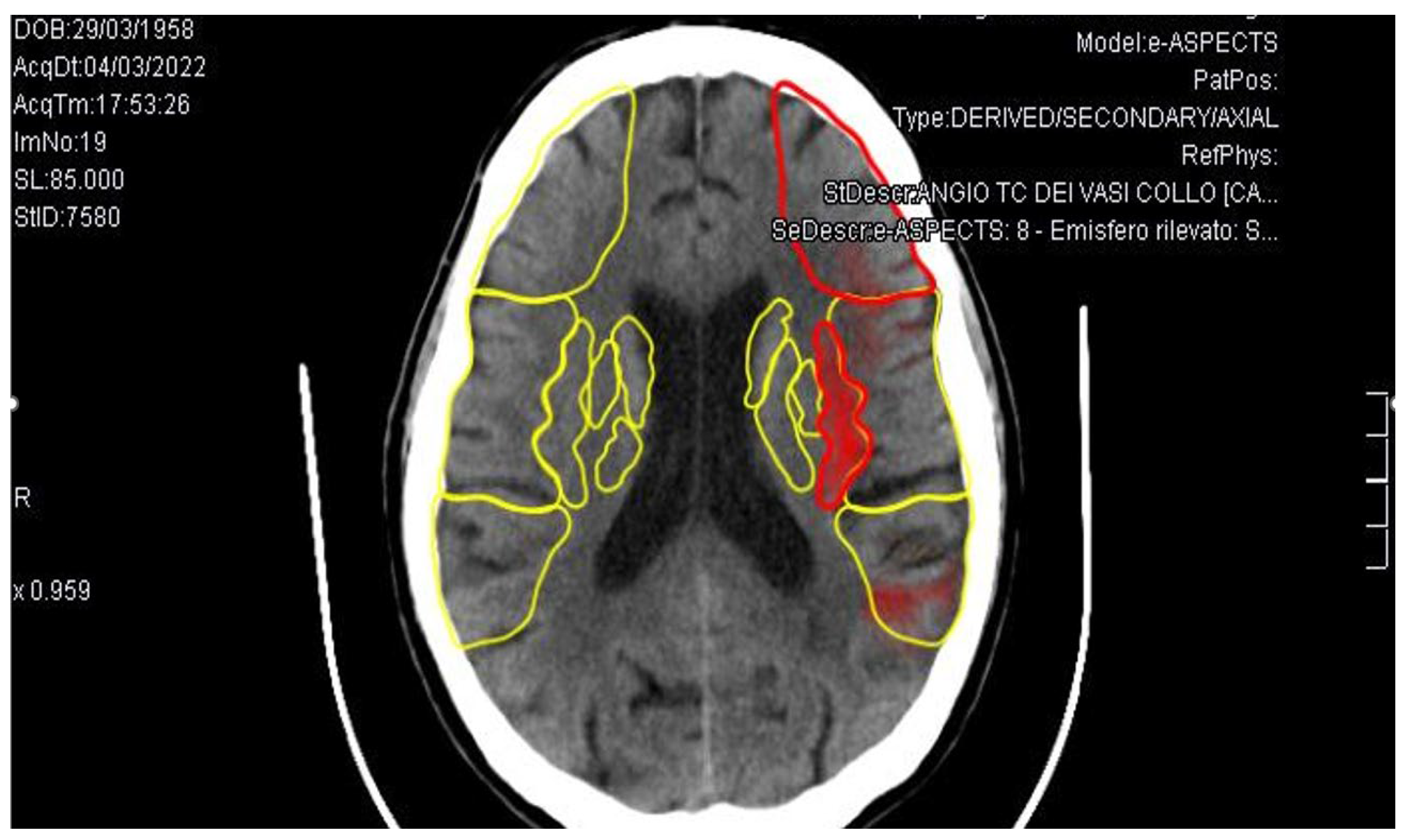
Figure 2.
A, B and C): TOE: Distal thickening of both mitral leaflets (white arrows), with a maximum thickness of three millimeters, impairing proper systolic coaptation and resulting in multiple, predominantly eccentric, regurgitant jets, overall consistent with severe mitral regurgitation. Findings suggestive of mitral valve endocarditis.
Figure 2.
A, B and C): TOE: Distal thickening of both mitral leaflets (white arrows), with a maximum thickness of three millimeters, impairing proper systolic coaptation and resulting in multiple, predominantly eccentric, regurgitant jets, overall consistent with severe mitral regurgitation. Findings suggestive of mitral valve endocarditis.
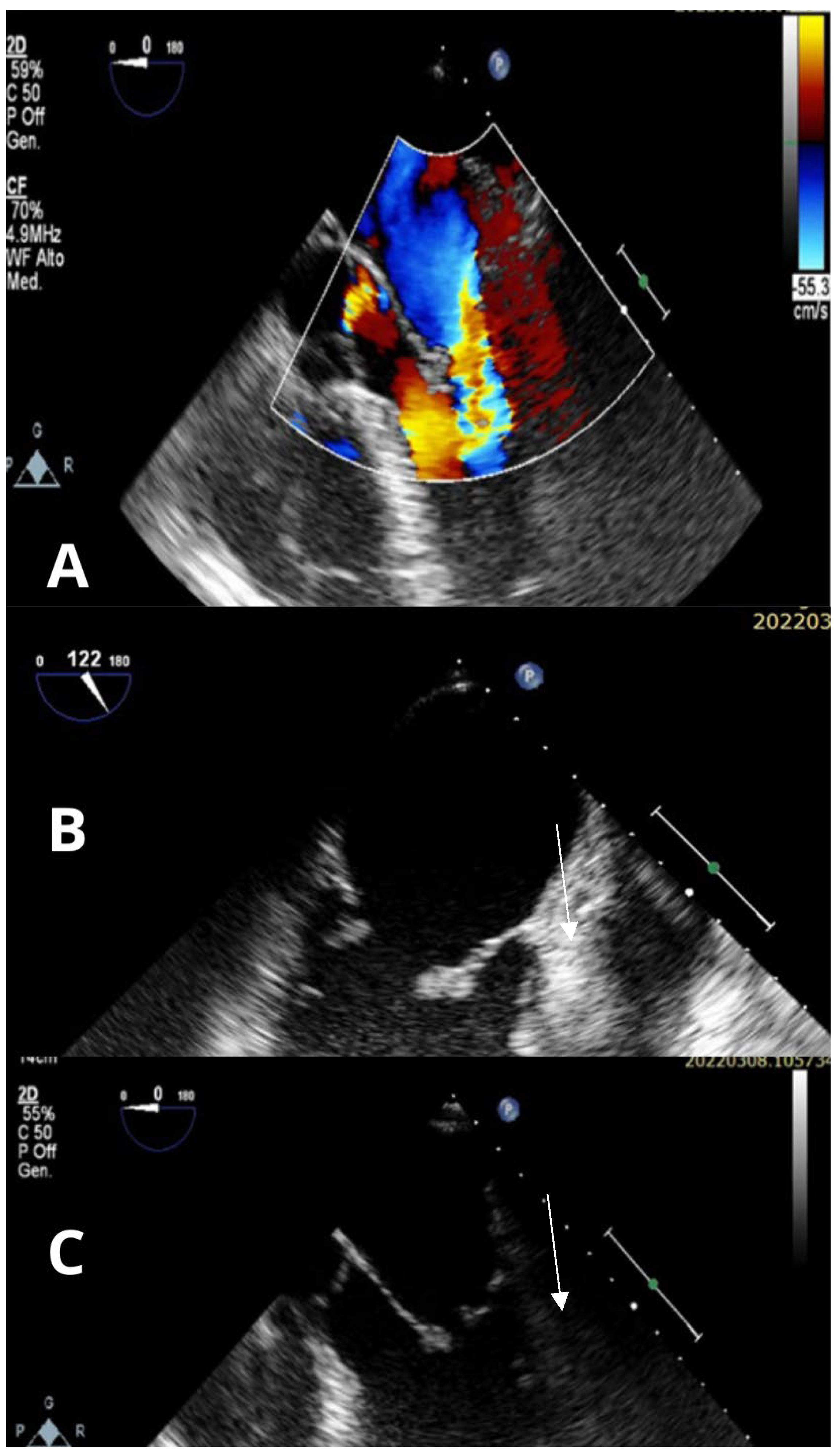
Figure 3.
Chest CT scan: a tissue mass in the left hilar para-aortic region causing narrowing of the bronchial structures.
Figure 3.
Chest CT scan: a tissue mass in the left hilar para-aortic region causing narrowing of the bronchial structures.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



