
Submitted:
16 June 2025
Posted:
17 June 2025
You are already at the latest version
Abstract
Objective Deep vein thrombosis (DVT) occurring in cancer patients accounts for about 9.2% of deaths. Here we retrospectively analyzed patients who had been newly diagnosed with solid cancers over a 7-year period in the Japanese population.
Patients or Materials We analyzed a series of 1,399 patients with solid cancers and suspected DVT treated at Ehime University Hospital. As controls, cancer patients with suspected DVT upon physical and hematological examinations and those in whom DVT had been not confirmed by detailed examination (echography and/or contrast-enhanced CT) were used. Several prognostic factors for DVT and non-DVT patients were extracted from the electronic medical record.
Results From among the 1,399 patients, leaving 224 patients with DVT and 560 without DVT as controls. The median overall survival (OS) period was 5.87 years for patients with DVT and 6.81 years for patients without DVT (p=0.0014). Anemia and thrombocytopenia were found to be strong risk factors related to an increased incidence of DVT. Female cancer patients with DVT had a significantly worse outcome than those without DVT (p=0.028). Analysis of OS in patients with DVT associated with gynecological cancers following treatment with three different direct oral anticoagulants (DOACs; edoxaban, rivaroxaban, and apixaban) indicated that those treated with apixaban had a significantly worse outcome than those treated with the others (p=0.019).
Conclusion Our findings suggest that patients with solid cancers, especially gynecological cancers, have a poorer prognosis if they also have anemia and a low platelet count. Furthermore, the choice of DOAC for treatment of DVT may impact the prognosis.
Keywords:
cancer patient
; deep vein thrombosis (DVT)
; prognostic factor
; direct oral anticoagulant (DOAC)
1. Introduction
Venous thromboembolism (VTE) for cancer patients, which mainly includes deep vein thrombosis (DVT), pulmonary embolism (PE), and mesenteric venous thrombosis (MVT) [1], occurs over 20% of the population with cancer [2] and leads to increased morbidity, such as the need for anticoagulation treatment, delays in delivering chemotherapy, a risk of fatal bleeding and infarction, and ultimately a decreased quality of life (QOL) [3,4]. The Khorana score (KRS), a model for prediction of venous thromboembolism (VTE), also has been proposed for evaluating the risk of DVT in cancer patients recently [5]. The KRS assesses the risk of developing VTE based on information such as the cancer site (especially cancers located in abdominal organs), blood parameters (white blood cell, red blood cell, and platelet counts), and body mass index (BMI). However, this scoring system has been based predominantly on Western data, raising uncertainties about its ability to predict VTE risk among individuals of Asian descent.
The purpose of the present study was to investigate in detail the risk factors associated with VET, focused on DVT development, in Japanese patients newly diagnosed with cancers, especially gynecologic or gastrointestinal cancers. Disparities in the incidence and clinical manifestation of DVT among patients with gynecologic and gastrointestinal cancers, both classified as high-risk groups according to the KRS score, were then clarified, allowing DVT treatment-associated outcome to be evaluated.
2. Materials and Methods
2.1. Studied Patients and Exclusion Criteria
A total of 1,399 patients newly diagnosed as having solid cancers, and with diagnosed or suspected DVT, were reviewed based on their electronic medical records in the Cancer Registries at Ehime University Hospital, covering the period from January 2013 to December 2020. These included (#1) all diagnosed cases of cancer based on their pathological diagnosis, (#2) patients receiving any first-line treatments, (#3) excluded patients with more than one type of cancer awaiting first-line treatment and considered unsuitable for the present prognostic analysis. In addition, (#4) cases in which patients had been prescribed medication for a diagnosis of VTE prior to the diagnosis of cancer were excluded. These cases were classified according to the Multiple Primary and Histology Coding Rules for the National Program of Cancer Registries in Japan in the present study. (This is nationally registered information about cancer patients and the treatments they receive.) [6]
2.2. Analysis of Cancer Patients and Their Survival in Relation to Prognostic Factors
For analysis of prognostic factors, the survival time of the study patients was investigated from the date of enrollment for any treatment in 2013 to the date of the last follow-up (at the end of 2023) or date of death. However, this included some patients who had requested hospital transfers for further treatment after first-line treatment (hospital-change cases). Clinical data for cancer patients gathered from the electronic medical records included cancer type, sex, age, ECOG performance status (PS), primary site, body mass index (BMI), blood and biochemical test data, details of treatment and outcomes, and outcomes associated with direct oral anticoagulant (DOAC) administration. The disease stage in each patient was based on the AJCC Cancer Staging System 8th edition. For cases complicated by DVT, the presence of thrombus was confirmed by ultrasonography of the lower extremity veins (compression ultrasonography) or contrast-enhanced CT scan. Cancer patients with suspected DVT upon physical and hematological examination on admission but without confirmed DVT complications after several examinations such as ultrasonography and contrast-enhanced CT scan were defined as controls (patients without DVT). These patients instead of all cancer patients were used as controls. The reasons for using this group (patients without DVT) as controls were, if all cancer patients were used as controls, it would include patients in whom DVT had not been confirmed (those who had not been examined for DVT), and it would include many patients with localized stage I or II cancer without any complications such as DVT [7].
Overall survival (OS) curves were calculated for each prognostic group according to the Kaplan-Meier method and analyzed using the log-rank univariate test. Fisher’s exact test and chi-squared test were performed to detect significant differences among the groups at P <0.05. Prognostic factors were subjected to univariate and multivariate analyses using Cox’s proportional hazard model. All statistical analyses were performed using the SAS software package version 9.4 (SAS Institute Inc., Cary, NC, USA).
2.3. Ethical Considerations
This study was approved by the Ethics Committee for Clinical Studies at Ehime University Graduate School of Medicine (study IRB; Ehime 2109016), and carried out in accordance with the ethical standards of the 1995 Declaration of Helsinki (as revised in Brazil 2013). Informed consent was by the opt-out principle; we disclosed information about the study on the associated website (https://www.m.ehime-u.ac.jp/school/clinical.oncology/?page_id=1487) and provided patients an opportunity to decline to participate in the study.
3. Results
3.1. Patient Demographics
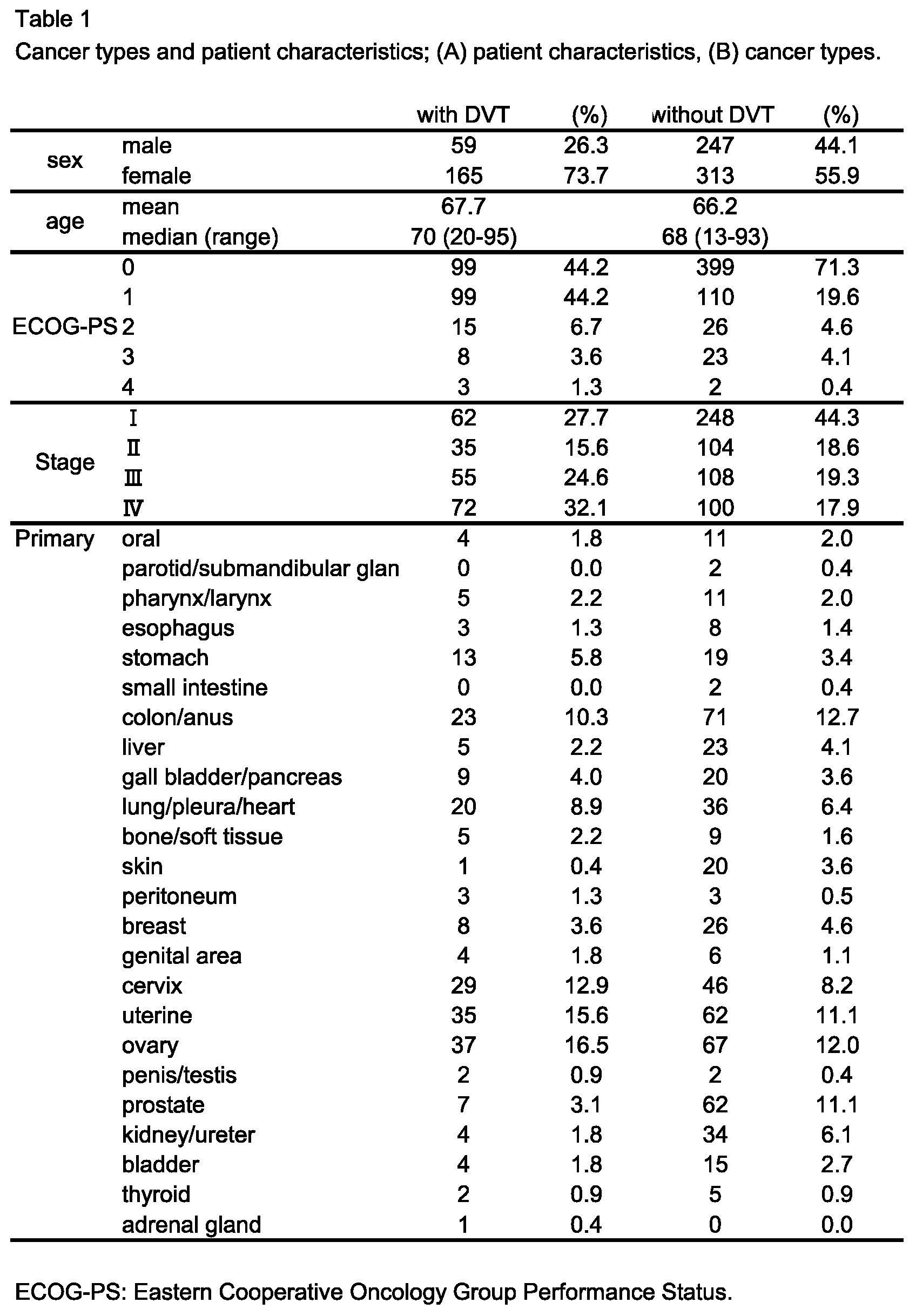
We first tried to predict the risk factors for DVT among a non-Caucasian population with solid cancers, especially Japanese patients, focusing on three types of solid cancers: gastrointestinal cancers, gynecological cancers, and other cancers. KRS had indicated higher risks of DVT among patients who had primary cancers located in abdominal organs. However, the results had been based on data from Caucasians, who differ in various aspects from Asians. We confirmed that the study population comprised 784 patients, comprising 224 patients and 560 patients as controls. From the electronic medical records, we selected cancer patients with suspected DVT, and in whom DVT had been ruled out after thorough examinations as controls. Figure 1 shows a flow diagram of the procedures used for patients with or without DVT, and Table 1 A and B show the patient characteristics and the cancer types.
3.2. Analysis of Outcome in Patients with or Without DVT and Risk Factors for DVT
We performed baseline Kaplan-Meier survival analysis to estimate the OS of the patients with or without DVT. Figure 2 shows the Kaplan-Meier overall survival (OS) curves of the four groups of cancer patients: cancer patients overall (A) (n=784), female cancer patients (B) (n=478), patients with gynecological cancer (C) (n=276), and patients with gastrointestinal cancer (D) (n=185). Table 2 shows the multivariate analysis of risk factors related to an increased incidence of DVT. The OS curves showed that patients who had DVT at the time of cancer diagnosis had a poorer outcome, and that this tendency was particularly marked for female patients with cancer and patients with gynecological cancer. Multivariate analysis revealed that advanced stage, a low creatinine level, anemia (Hb <11 g/dL) and thrombocytopenia (Plt <15 x 104/μL) were risk factors for development of DVT (Table 2). Table 3 focuses on risk factors for DVT in female patients and patients with gynecological cancer. This analysis indicated that female patients, especially those with gynecological cancer, those who were elderly, and those who had a poor performance status (PS), anemia, and thrombocytopenia, had a higher risk of DVT. Interestingly, BMI was not a risk factor in this current Japanese cohort.

Table 2.
Multivariate analysis of risk factors for DVT in patients with cancer (n=784).
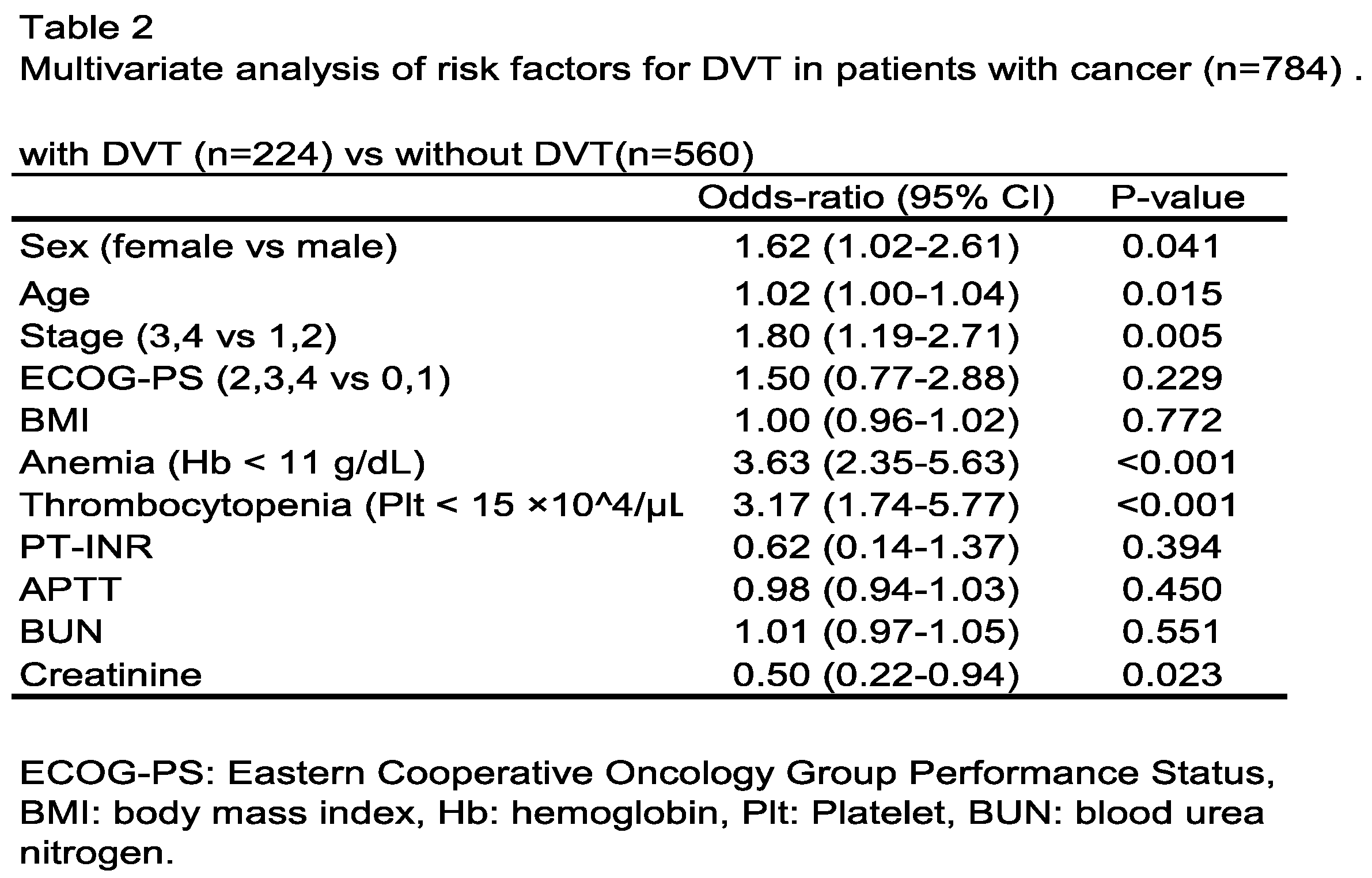
Table 3.
Multivariate analysis of prognostic factors among female patients with or without DVT; (A) female patients, (B) patients with gynecological cancer.
Table 3.
Multivariate analysis of prognostic factors among female patients with or without DVT; (A) female patients, (B) patients with gynecological cancer.
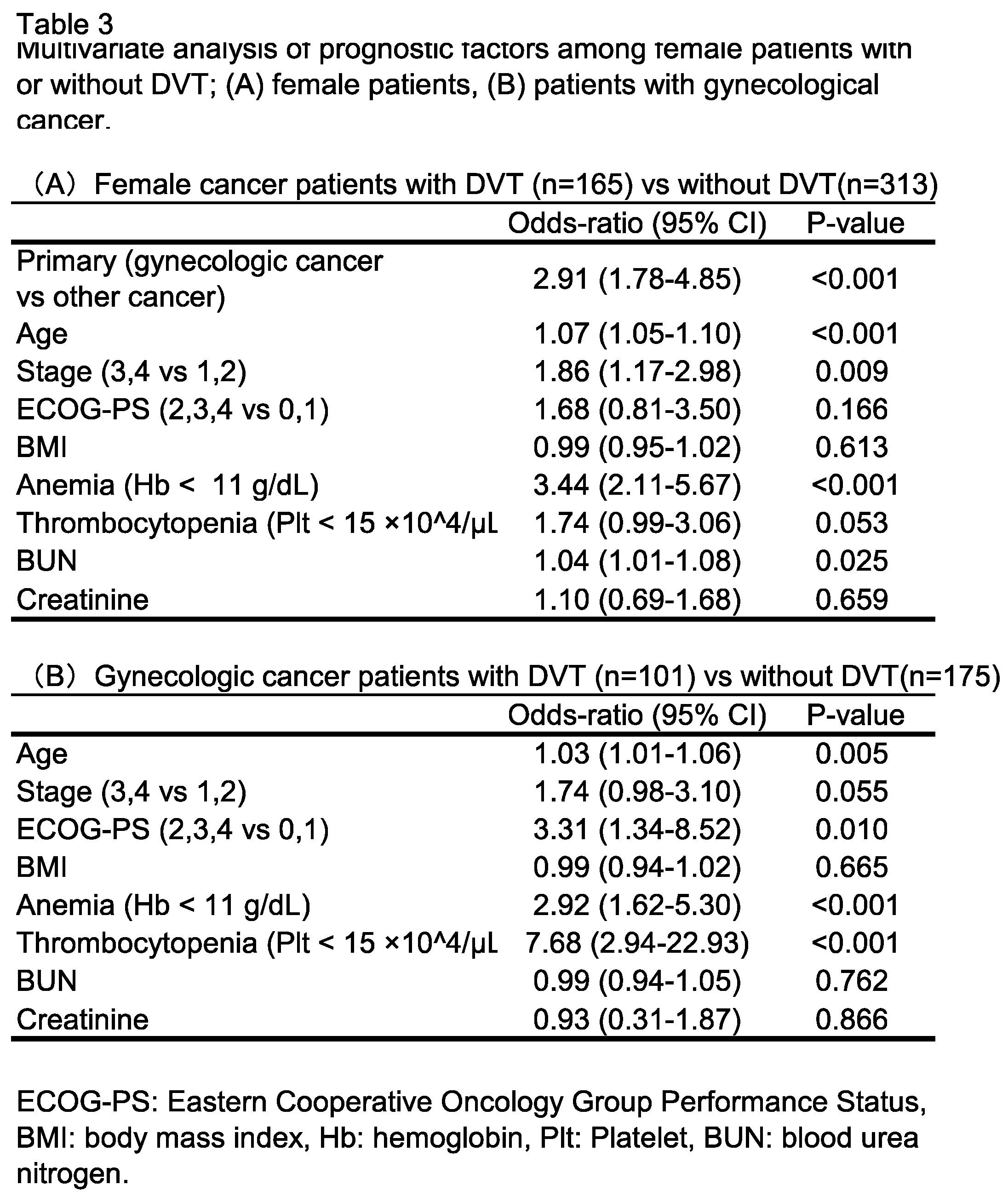
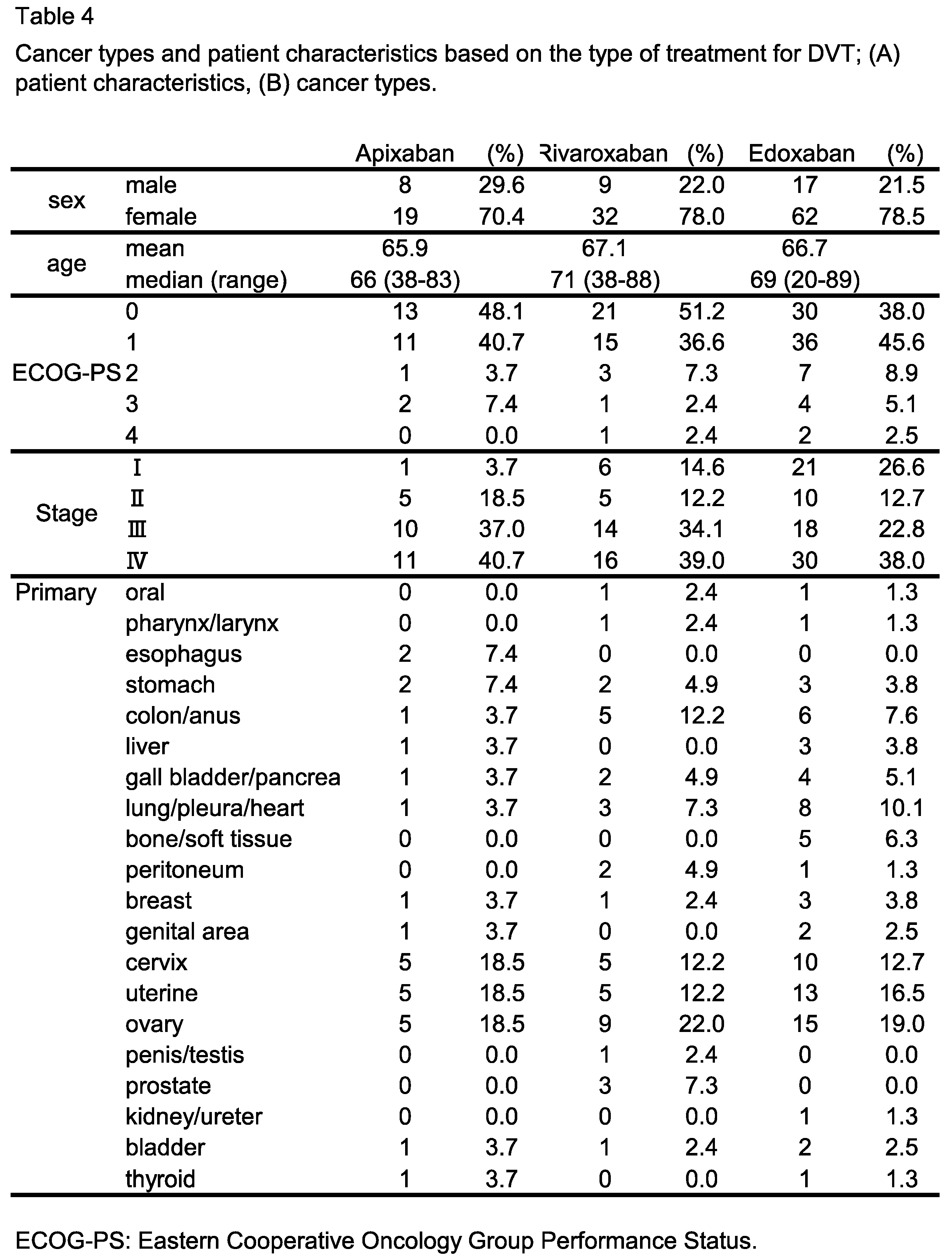
Table 4.
Cancer types and patient characteristics based on the type of treatment for DVT; patient characteristics and cancer types.
Table 4.
Cancer types and patient characteristics based on the type of treatment for DVT; patient characteristics and cancer types.
3.3. Impact of DVT Treatment with Oral Anticoagulants on Patient Outcome
Recently in Japan, three direct oral anticoagulants (DOACs), rivaroxaban, edoxaban, and apixaban, had been introduced into clinical practice in 2012 and had been approved for DVT in 2015. Analysis of DOAC-associated patient mortality, indicated in Figure 3, revealed that the mortality of cancer patients treated with apixaban was slightly higher than that of patients treated with the other agents. This tendency was more pronounced for patients with gynecological cancer (Figure 4).
4. Discussion
Despite being a single-center study, our current analysis included 784 cancer patients and revealed that the incidence of DVT was significantly higher in patients with gynecological cancers, as well as those with hematological abnormalities, such as a hemoglobin level of <11 g/dL or a platelet count of <15 x 104/μL. These findings suggest that the primary tumor site and anemia are significant risk factors for DVT, being consistent with the KRS findings. Conversely, body mass index (BMI), another risk factor identified on the basis of the KRS, was found not to be a significant risk factor in the present Japanese cohort.
It is well established that intra-abdominal cancers and patient obesity contribute to deep venous stasis, thereby increasing the risk of DVT. Additionally, anemia exacerbates hypoxia and circulatory failure in peripheral tissues, leading to endothelial damage and an increased tendency for coagulation due to endothelium-derived coagulation factors [8,9]. Furthermore, in cancer patients, platelet activation, rather than quantitative abnormalities, has been implicated in increased coagulability [10], with consequent platelet consumption and reduction reflecting a higher risk of DVT [11]. Our present findings suggest that risk factors similar to those on which the KRS is based, in conjunction with a reduced platelet count, were significant contributors to DVT in this cohort. Moreover, DVT was significantly more prevalent among patients who received radiotherapy during post-treatment follow-up (data not shown), potentially due to vascular endothelial damage [12]. The absence of obesity as a risk factor for DVT in our cohort may be attributed to the lower prevalence of obesity in the general Japanese population, in comparison to Western populations.
Our comparison between patients with and without DVT showed that the former had poorer outcomes across all cancer types. This finding suggests that, beyond the direct impact of DVT on life expectancy, complications arising from DVT and its treatment may adversely affect the management of the underlying malignancy. However, differences in patient demographics, such as sex ratio, age, and disease stage, between the DVT and control groups may have introduced variability into the prognostic analysis. To address this, we conducted an additional analysis focusing on female patients with gynecological cancers, as per the KRS guidelines. This analysis revealed a more pronounced negative impact of DVT on life expectancy among women with cancer, particularly gynecological cancers (Figure 2C). This aligns with previous studies [13,14,15], which have reported that thrombotic complications worsen patient outcome. These results are noteworthy, as they indicate that the presence of DVT not only significantly influences the prognosis of patients with gynecological cancers but may also affect the course of treatment for the tumor itself. One plausible example of this is a reduction in the intensity of anti-tumor therapy due to DVT complications. For instance, bevacizumab, an anti-vascular endothelial growth factor (VEGF) antibody commonly used for patients with gynecological tumors, has a well-documented profile of adverse effects, including an increased risk of thrombosis and bleeding due to vascular endothelial damage. This may limit its use in patients with DVT. Additionally, DVT-related complications may contribute to anemia and thrombocytopenia, potentially compromising the maintenance of therapeutic intensity. These issues are particularly relevant for colorectal cancer, for which bevacizumab is frequently administered. Unfortunately, the present study did not undertake a detailed assessment of DVT complications in relation to the types of anticancer treatment.
Recent randomized phase III trials comparing DOACs with low-molecular-weight heparin, which is traditionally considered safe, effective, and associated with a lower recurrence rate for treating VTE in cancer patients, have demonstrated that DOACs are not inferior in terms of treatment efficacy and recurrence rate [16]. In addition, trials comparing individual DOACs with vitamin K antagonists (VKAs) for the treatment of VTE have shown that DOACs are not inferior in terms of efficacy and recurrence rate [17,18,19,20]. Consequently, VTE treatment has shifted from VKAs to DOACs in view of their efficacy, standardized dosing, reduced requirement for monitoring, less frequent follow-up, and fewer interactions with food or drugs [21].
In the present study, we also examined the impact of each DOAC on patient outcome. Interestingly, while the type of DOAC employed affected outcome across all cancer types (Figure 3A), apixaban in particular was associated with a poorer outcome, especially in patients with gynecological cancer (Figure 4B). Although DOACs are generally associated with fewer drug-drug interactions, the potential for antitumor medications affecting CYP3A4 enzymes or P-glycoprotein to alter the blood concentrations of DOACs, and thus their anticoagulant effects, warrants consideration. Recently, DOACs have been evaluated for their use in cancer patients. For examples, apixaban has been deemed the most effective and safest treatment for DVT in cancer patients in a systematic review [22]. In contrast, a study using a small number of patients has indicated that edoxaban might be a viable treatment option for gynecological cancer, because as multiple cycles of taxane-based chemotherapy were shown not to significantly alter edoxaban trough blood concentrations or the area under the curve (AUC) [23]. In addition, to a retrospective study about the clinical safety of edoxaban [24], increased risk of bleeding in the use of rivaroxaban or apixaban for patients with gynecological cancer has been reported [25,26]. At present, interactions between DOACs and antitumor treatments, such as alterations of the blood concentration levels, remain inadequately studied. As a twice-daily apixaban dosing regimen may negatively impact treatment compliance for both VTE and cancer, selection of an appropriate DOAC for each type of cancer warrants further investigation.
One of the limitations of this study was that it was a single-center, retrospective analysis. Therefore, future prospective, multi-center studies, along with basic research into pharmacological interactions, will be necessary to further explore the issues raised by the present findings.
Ethics approval and consent to participate
This study was approved by the Ethics Committee for Clinical Studies at Ehime University Graduate School of Medicine (study IRB; Ehime 2109016), and carried out in accordance with the ethical standards of the 1995 Declaration of Helsinki (as revised in Brazil 2013). Informed consent was by the opt-out principle; we disclosed information about the study on the associated website (https://www.m.ehime-u.ac.jp/school/clinical.oncology/?page_id=1487) and provided patients an opportunity to decline to participate in the study.
Consent for publication
Not applicable.
Availability of data and materials
Competing interests
The authors have no competing interests to declare.
Funding
Not applicable.
Author contributions
YM and YY designed the study, collected the clinical data, and drafted the manuscript. TF, JY and KT participated in the design of the study and oversaw the clinical data. SY and SH carried out the statistical analysis. YY conceived the study, participated in its design and coordination, and helped to draft the manuscript. All authors read the draft, revised it critically, and approved the final manuscript.
Acknowledgments
We appreciate the cooperation of the staff members of the Department of Hematology, Clinical Immunology, and Infectious Diseases, Ehime University Hospital.
References
- Heit, J.A. Epidemiology of Venous Thromboembolism. Nat. Rev. Cardiol. 2015, 12, 464–474. [Google Scholar] [CrossRef] [PubMed]
- Lyman, G.H. Venous Thromboembolism in the Patient with Cancer: Focus on Burden of Disease and Benefits of Thromboprophylaxis. Cancer 2011, 117, 1334–1349. [Google Scholar] [CrossRef]
- Prandoni, P.; Falanga, A.; Piccioli, A. Cancer and Venous Thromboembolism. Lancet Oncol. 2005, 6, 401–410. [Google Scholar] [CrossRef]
- Elting, L.S.; Escalante, C.P.; Cooksley, C.; Avritscher, E.B.C.; Kurtin, D.; Hamblin, L.; Khosla, S.G.; Rivera, E. Outcomes and Cost of Deep Venous Thrombosis among Patients with Cancer. Arch. Intern. Med. 2004, 164, 1653–1661. [Google Scholar] [CrossRef]
- Khorana, A.A.; Kuderer, N.M.; Culakova, E.; Lyman, G.H.; Francis, C.W. Development and Validation of a Predictive Model for Chemotherapy-Associated Thrombosis. Blood 2008, 111, 4902–4907. [Google Scholar] [CrossRef]
- Higashi, T.; Nakamura, F.; Shibata, A.; Emori, Y.; Nishimoto, H. The National Database of Hospital-Based Cancer Registries: A Nationwide Infrastructure to Support Evidence-Based Cancer Care and Cancer Control Policy in Japan. Jpn. J. Clin. Oncol. 2014, 44, 2–8. [Google Scholar] [CrossRef]
- Pung, L.; Moorin, R.; Trevithick, R.; Taylor, K.; Chai, K.; Garcia Gewerc, C.; Ha, N.; Smith, S. Determining Cancer Stage at Diagnosis in Population-Based Cancer Registries: A Rapid Scoping Review. Front. Health Serv. 2023, 3, 1039266. [Google Scholar] [CrossRef]
- Arisato, T.; Hashiguchi, T.; Sarker, K.P.; Arimura, K.; Asano, M.; Matsuo, K.; Osame, M.; Maruyama, I. Highly Accumulated Platelet Vascular Endothelial Growth Factor in Coagulant Thrombotic Region. J. Thromb. Haemost. 2003, 1, 2589–2593. [Google Scholar] [CrossRef]
- Tezono, K.; Sarker, K.P.; Kikuchi, H.; Nasu, M.; Kitajima, I.; Maruyama, I. Bioactivity of the Vascular Endothelial Growth Factor Trapped in Fibrin Clots: Production of IL-6 and IL-8 in Monocytes by Fibrin Clots. Haemostasis 2001, 31, 71–79. [Google Scholar] [CrossRef]
- Riedl, J.; Kaider, A.; Marosi, C.; Prager, G.W.; Eichelberger, B.; Assinger, A.; Pabinger, I.; Panzer, S.; Ay, C. Decreased Platelet Reactivity in Patients with Cancer Is Associated with High Risk of Venous Thromboembolism and Poor Prognosis. Thromb. Haemost. 2017, 117, 90–98. [Google Scholar] [CrossRef]
- Kenmotsu, H.; Notsu, A.; Mori, K.; Omori, S.; Tsushima, T.; Satake, Y.; Miki, Y.; Abe, M.; Ogiku, M.; Nakamura, T.; et al. Cumulative Incidence of Venous Thromboembolism in Patients with Advanced Cancer in Prospective Observational Study. Cancer Med. 2021, 10, 895–904. [Google Scholar] [CrossRef] [PubMed]
- Temraz, S.; Moukalled, N.; Gerotziafas, G.T.; Elalamy, I.; Jara-Palomares, L.; Charafeddine, M.; Taher, A. Association between Radiotherapy and Risk of Cancer Associated Venous Thromboembolism: A Sub-Analysis of the COMPASS-CAT Study. Cancers 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, K.; Moeini, A.; Machida, H.; Fullerton, M.E.; Shabalova, A.; Brunette, L.L.; Roman, L.D. Significance of Venous Thromboembolism in Women with Cervical Cancer. Gynecol. Oncol. 2016, 142, 405–412. [Google Scholar] [CrossRef]
- Yamaguchi, K.; Tsuruga, T.; Taguchi, A.; Tanikawa, M.; Sone, K.; Mori-Uchino, M.; Iriyama, T.; Matsumoto, Y.; Hiraike, O.; Hirota, Y.; et al. Comorbid Thrombosis as an Adverse Prognostic Factor in Patients with Ovarian Clear Cell Carcinoma Regardless of Staging. Int. J. Clin. Oncol. 2024. [Google Scholar] [CrossRef]
- Suzuki, T.; Tsurimoto, S.; Tada, T.; Yamamura, R.; Katoh, H.; Noji, Y.; Yamaguchi, M.; Fujino, S. Venous Thromboembolism in Japanese Patients with Gynecologic Cancer. Clin. Appl. Thromb. Hemost. 2023, 29, 10760296221124120. [Google Scholar] [CrossRef]
- Young, A.M.; Marshall, A.; Thirlwall, J.; Chapman, O.; Lokare, A.; Hill, C.; Hale, D.; Dunn, J.A.; Lyman, G.H.; Hutchinson, C.; et al. Comparison of an Oral Factor Xa Inhibitor With Low Molecular Weight Heparin in Patients With Cancer With Venous Thromboembolism: Results of a Randomized Trial (SELECT-D). J. Clin. Oncol. 2018, 36, 2017–2023. [Google Scholar] [CrossRef]
- van Es, N.; Coppens, M.; Schulman, S.; Middeldorp, S.; Büller, H.R. Direct Oral Anticoagulants Compared with Vitamin K Antagonists for Acute Venous Thromboembolism: Evidence from Phase 3 Trials. Blood 2014, 124, 1968–1975. [Google Scholar] [CrossRef]
- Agnelli, G.; Buller, H.R.; Cohen, A.; Curto, M.; Gallus, A.S.; Johnson, M.; Masiukiewicz, U.; Pak, R.; Thompson, J.; Raskob, G.E.; et al. Oral Apixaban for the Treatment of Acute Venous Thromboembolism. N. Engl. J. Med. 2013, 369, 799–808. [Google Scholar] [CrossRef]
- EINSTEIN Investigators; Bauersachs, R.; Berkowitz, S.D.; Brenner, B.; Buller, H.R.; Decousus, H.; Gallus, A.S.; Lensing, A.W.; Misselwitz, F.; Prins, M.H.; et al. Oral Rivaroxaban for Symptomatic Venous Thromboembolism. N. Engl. J. Med. 2010, 363, 2499–2510. [Google Scholar]
- Hokusai-VTE Investigators; Büller, H.R.; Décousus, H.; Grosso, M.A.; Mercuri, M.; Middeldorp, S.; Prins, M.H.; Raskob, G.E.; Schellong, S.M.; Schwocho, L.; et al. Edoxaban versus Warfarin for the Treatment of Symptomatic Venous Thromboembolism. N. Engl. J. Med. 2013, 369, 1406–1415. [Google Scholar]
- Nasiri, A.; AlQahtani, A.; Rayes, N.H.; AlQahtani, R.; Alkharras, R.; Alghethber, H. Direct Oral Anticoagulant: Review Article. J Family Med Prim Care 2022, 11, 4180–4183. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Lv, M.; Chen, J.; Jiang, S.; Chen, M.; Fang, Z.; Zeng, Z.; Qian, J.; Xu, W.; Guan, C.; et al. Direct Oral Anticoagulants for Venous Thromboembolism in Cancer Patients: A Systematic Review and Network Meta-Analysis. Support. Care Cancer 2022, 30, 10407–10420. [Google Scholar] [CrossRef] [PubMed]
- Oride, T.; Sawada, K.; Shimizu, A.; Kinose, Y.; Takiuchi, T.; Kodama, M.; Hashimoto, K.; Kobayashi, E.; Nakatani, E.; Kimura, T. Clinical Trial Assessing the Safety of Edoxaban with Concomitant Chemotherapy in Patients with Gynecological Cancer-Associated Thrombosis (EGCAT Study). Thromb. J. 2023, 21, 57. [Google Scholar] [CrossRef] [PubMed]
- Odajima, S.; Seki, T.; Kato, S.; Tomita, K.; Shoburu, Y.; Suzuki, E.; Takenaka, M.; Saito, M.; Takano, H.; Yamada, K.; et al. Efficacy of Edoxaban for the Treatment of Gynecological Cancer-Associated Venous Thromboembolism: Analysis of Japanese Real-World Data. J. Gynecol. Oncol. 2022, 33, e62. [Google Scholar] [CrossRef]
- Lee, J.H.; Lee, J.H.; Jo, K.W.; Huh, J.W.; Oh, Y.M.; Lee, J.S. Comparison of Rivaroxaban and Dalteparin for the Long-Term Treatment of Venous Thromboembolism in Patients with Gynecologic Cancers. J. Gynecol. Oncol. 2020, 31, e10. [Google Scholar] [CrossRef]
- Carrier, M.; Abou-Nassar, K.; Mallick, R.; Tagalakis, V.; Shivakumar, S.; Schattner, A.; Kuruvilla, P.; Hill, D.; Spadafora, S.; Marquis, K.; et al. Apixaban to Prevent Venous Thromboembolism in Patients with Cancer. N. Engl. J. Med. 2019, 380, 711–719. [Google Scholar] [CrossRef]
Figure 1.
Flow diagram of procedures for patients with or without DVT.
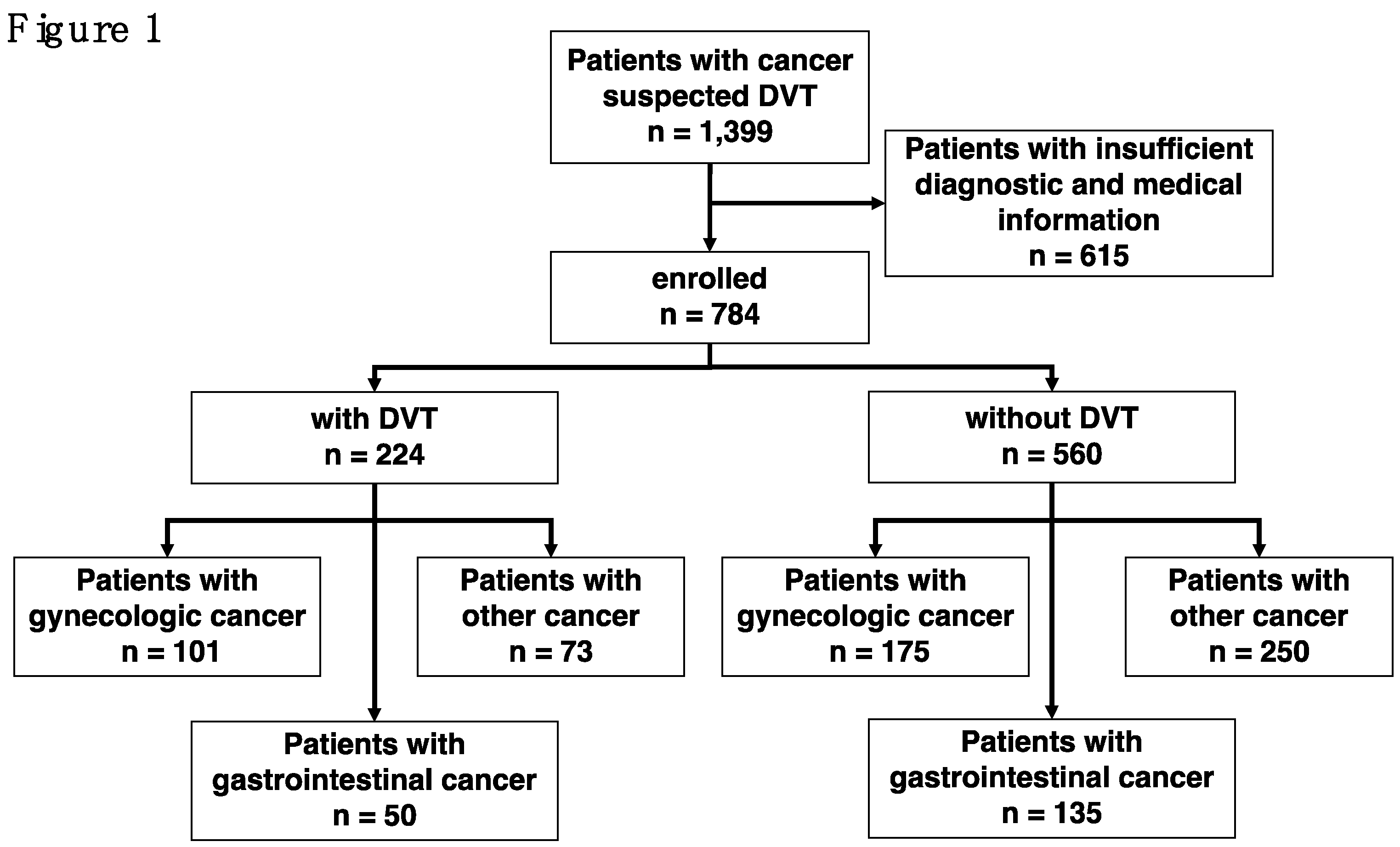
Figure 2.
Overall survival of patients with or without DVT; (A) all patients, (B) female patients, (C) patients with gynecological cancer, (D) patients with gastrointestinal cancer.
Figure 2.
Overall survival of patients with or without DVT; (A) all patients, (B) female patients, (C) patients with gynecological cancer, (D) patients with gastrointestinal cancer.
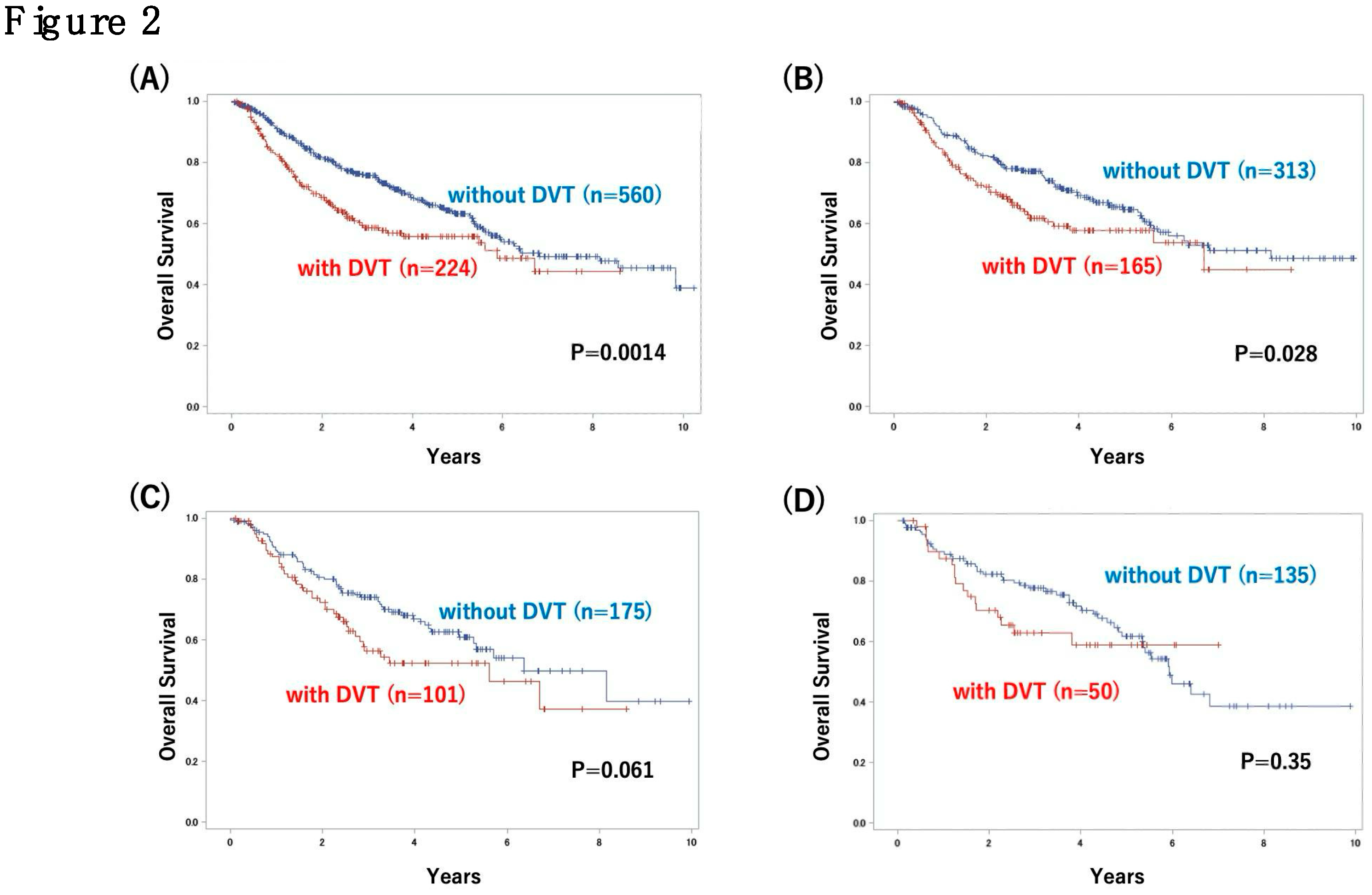
Figure 3.
Overall survival based on the type of treatment for DVT; (A) all patients, (B) female patients.
Figure 3.
Overall survival based on the type of treatment for DVT; (A) all patients, (B) female patients.
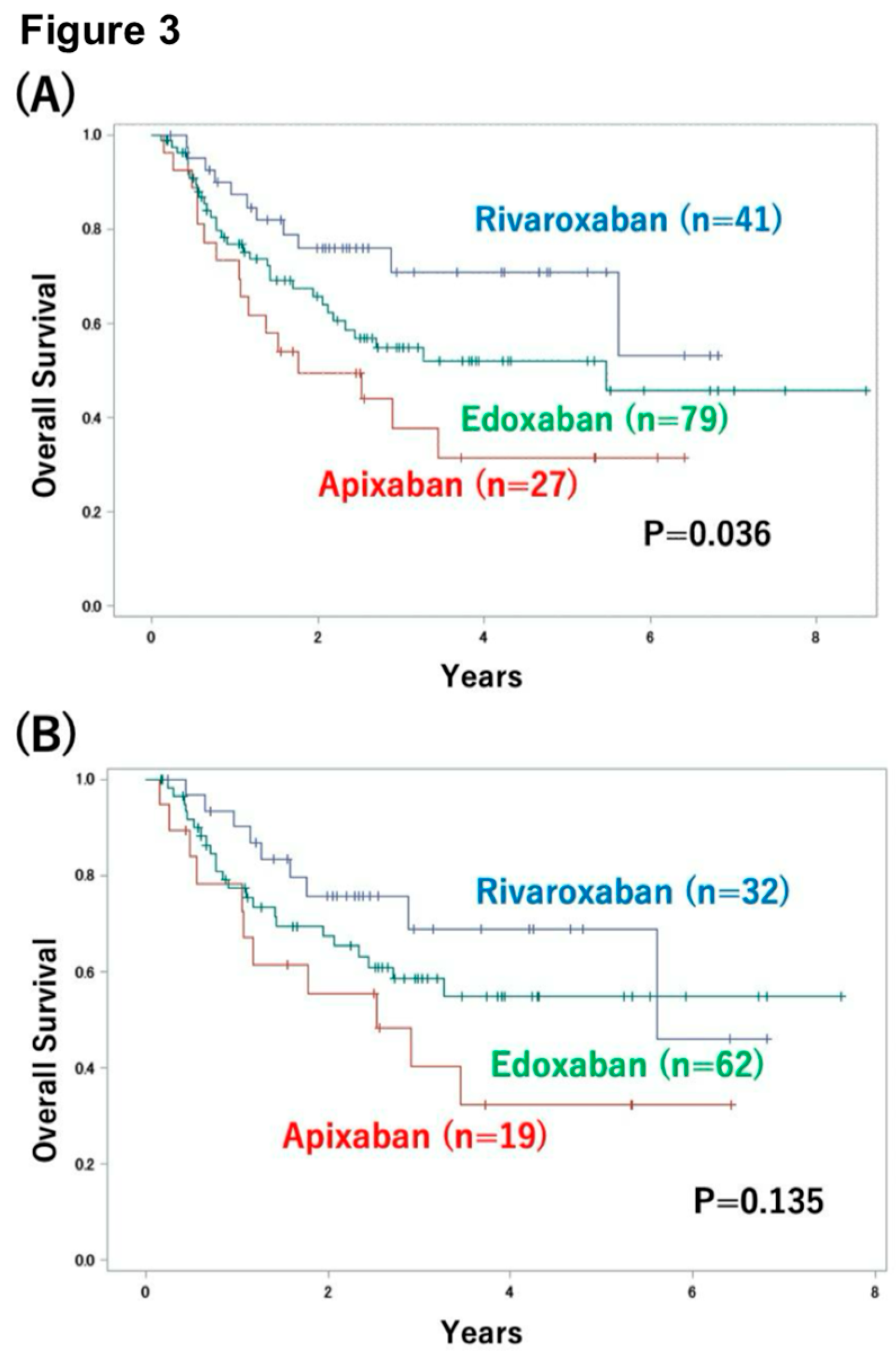
Figure 4.
Overall survival based on the type of treatment for DVT (apixaban versus others); (A) female patients, (B) patients with gynecological cancer.
Figure 4.
Overall survival based on the type of treatment for DVT (apixaban versus others); (A) female patients, (B) patients with gynecological cancer.
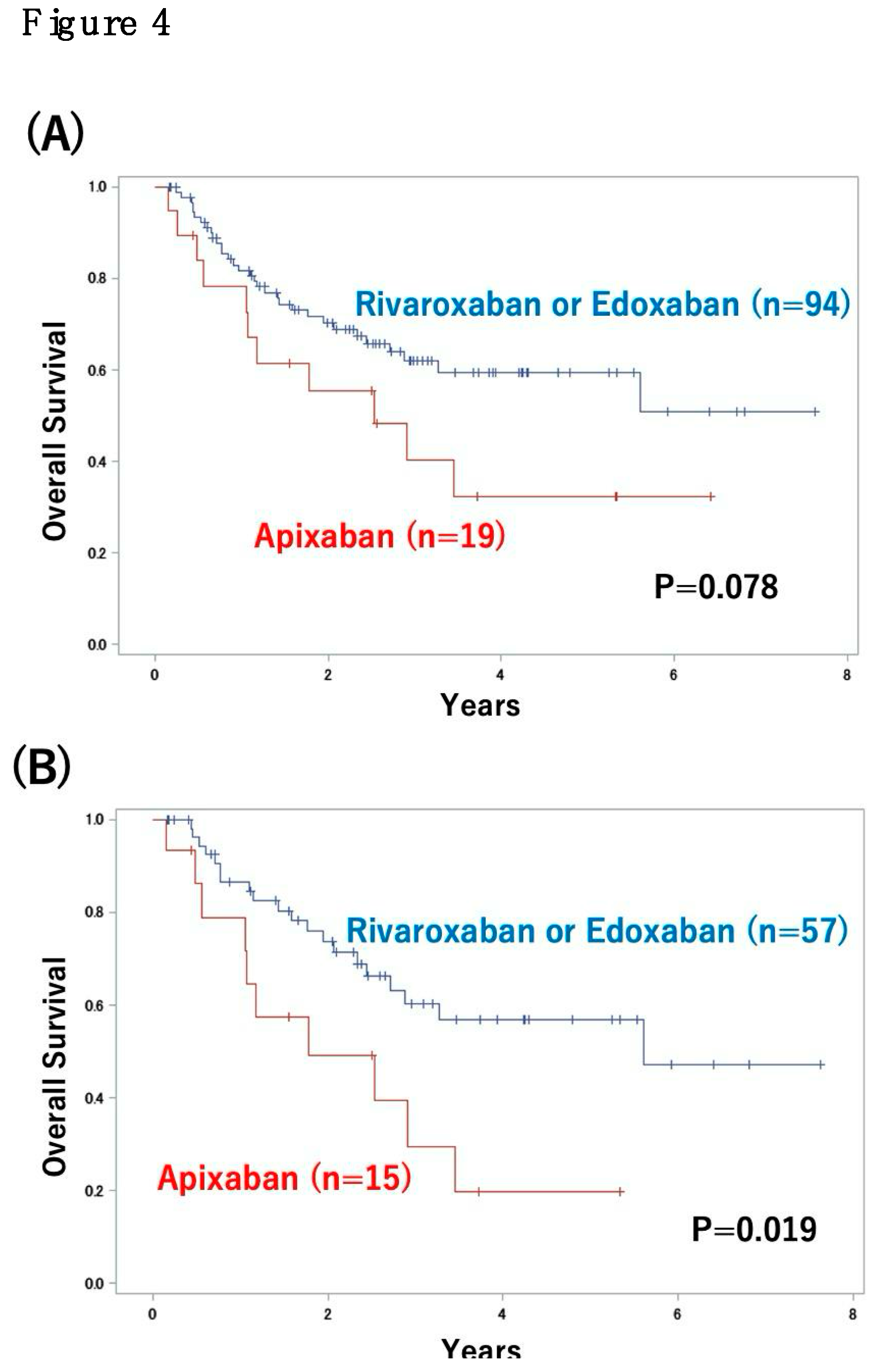
Table 1.
Cancer types and patient characteristics; patient characteristics and cancer types.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



