
Submitted:
11 July 2025
Posted:
14 July 2025
You are already at the latest version
Abstract
Microorganisms are abundantly dispersed in nature and can also be found in hospital environments, causing high rates of infections. This study aims to identify bacteria isolated from a veterinary hospital as well as carry out antimicrobial susceptibility testing, biofilm production tests, and genetic analysis of the ica operon of the isolates. Three collections were carried out on 11 surfaces and objects from general areas and the hospital’s operating room, totaling 33 samples, with 66 different bacterial species isolated, 77% (51/66) of them gram-positive and 23% (29/66) gram-negative. MDR, MRSA, MRS and ESBL resistance profiles were found, as well as biofilm production rates of 57% (38/66) of the isolates. Analysis of operon genes for Staphylococcus sp. demonstrated divergence in some samples when compared to the phenotypic test performed. In summary, there is a high presence of microorganisms with resistance and virulence factors spread throughout the various facilities of the veterinary hospital.
Keywords:
pathogenic microorganisms
; biofilms
; veterinary environments
; resistance
1. Introduction
Hospital environments are considered important reservoirs of microorganisms, playing a significant role in the selection and dissemination of multidrug-resistant pathogens, leading to cases of secondary cross-infections [1,2]. In hospital environments and veterinary practices, the intense and constant movement of people and animals associated with animal health immunosuppression and risk factors such as increased hospital stays, high incidence of invasive procedures, and excessive and inadequate use of antimicrobial therapies contribute to the incidence of Healthcare-Associated Infections (HAIs) [3,4]. The rapid spread of microorganisms and the high capacity to produce virulence factors lead to an increase in antimicrobial resistance rates and the formation of biofilms, making the treatment of infections even more difficult [5]. Biofilms are structured and complex bacterial communities, wrapped in a self-producing polymeric matrix, which is composed of proteins, lipids, carbohydrates, extracellular nucleic acids (eRNA and eDNA), and extracellular polymeric substance (EPS) [6,7,8]. The intense bacterial proliferation and interaction provides genetic exchange between different bacterial strains, ensuring survival and conferring resistance to antimicrobials, disinfectants, and against mechanisms of the host’s immune response [9].
The process of bacterial biofilms formation involves four main stages, which include initial reversible adhesion, irreversible adhesion, and formation of microcolonies, maturation and dispersion of persister cells [10,11]. This process is genetically regulated by specific genes for the coding of adhesion proteins [12]. For the species of Staphylococcus sp., ica operon (icaADCB and gene ica R) responsible for the production of Polysaccharide intercellular adhesin (PIA), the homologous biofilm-associated protein (Bhp), and the accumulation-associated protein (Aap) are the most important [13,14]. In addition to these, the communication system between cells, quorum sensing, plays an important role in the production of autoinducers and accessory gene regulators such as the agr locus (agr I, II and III) [12,13].
The obstacles in this issue, besides causing severe infections with permanent consequences and even the death of the animal, lead to the possibility of social and psychological repercussions for the guardians, with high hospital costs, traumas, and loss of credibility of the team and the institution [15]. Concomitant to this, there is the ability of transmission of these multiresistant bacterial infections from animals to their owners, professionals, employees and, in teaching hospitals, to academics and residents in the area, which can cause outbreaks and acquire zoonotic potential, raising concerns at the level of One Health [3,16,17]. Furthermore, studies in veterinary environments and epidemiological data regarding bacterial contamination are still scarce and underreported, with the topic being little discussed [18].
The aim of this study was to isolate and identify bacteria from surfaces and objects in general areas and in the operating room of a veterinary hospital, as well as to evaluate the antimicrobial resistance profile, the biofilm formation capacity, and the presence of ica operon genes in isolated bacteria.
2. Materials and Methods
Study Design
Samples were collected from 11 surfaces and/or objects at a veterinary teaching hospital in the Southwest Region of Goiás, totaling 33 samples. The objects and surfaces were selected based on literature research on the main potential locations for harboring microorganisms in the hospital environment. After analyzing several studies, the locations were selected and adapted in some cases.
Collection and Transportation of Samples
Sample collection was divided into two distinct environments: non-critical areas and critical area (surgical suite), with one and two collection moments respectively, totaling three collection moments (33 samples). The first collection covered non-critical areas: reception desk, offices, isolation area, hospitalization area, infectious diseases area, and pre-operative areas of the hospital. The other two collections were carried out exclusively in the two operating room areas of the hospital surgical suite. The collections were carried out with the use of sterile swabs soaked in 0.9% saline, which were passed over the objects and surfaces and then placed in identified test tubes containing Brain Heart Infusion (BHI) (OXOID®) broth, placed on shelves in a thermal box and transported to the Bacteriology and Mycology Laboratory, remaining incubated for 24 hours in a BOD incubator at a temperature of 35±2 ºC, under aerobic conditions.
Sample Processing and Identification
Samples positive for bacterial growth (turbidity of the BHI broth) were plated on Blood Agar—BA (HIMEDIA®) and incubated for a period of 24 hours in a BOD incubator at a temperature of 35±2 ºC (95°F+35,5°F) in an aerobic atmosphere. After the incubation time, the samples were analyzed for the diversity of colonies grown as well as their hemolysis pattern. Plates with distinct colonies were transferred to new BA plates for these colonies to be purified. Then, an isolated colony from each sample was subjected to the Gram staining technique (NewProv Kit®) and thus seeded on specific agar and incubated for 24 hours. Subsequently, phenotypic identification tests through conventional biochemical tests were performed: fermentation of Salted Mannitol agar (HIMEDIA®), catalase, coagulase, DNAse, polymyxin B, and novobiocin test for gram-positive cocci bacteria (catalase positive); catalase, optochin, bacitracin, bile-esculin test and NaCl tolerance test for gram-positive cocci bacteria (catalase negative); catalase test and Gram technique for gram-positive bacilli; and for gram-negative, lactose fermentation in MacConkey agar (HIMEDIA®), oxidase, and rugai tests (Newprov®) [19].
Antimicrobial Susceptibility Testing
Antimicrobial susceptibility testing (AST) was performed using the disk diffusion method (Kirby-Bauer). A bacterial suspension was prepared with 0.9% sterile saline in turbidity of 1.5 x 108 CFU/ml (0.5 on the McFarland scale), and then seeded in a Petri dish (140x15mm) with Mueller Hinton agar (HIMEDIA®); the antimicrobials corresponding to each isolated strain were deposited and incubated in a BOD incubator at 35º ± 2º C for 18 to 24 hours. The interpretation of the inhibition halos and the selection of antimicrobials was carried out according to parameters recommended by BrCAST [20] and the strains were classified as Multidrug-resistant (MDR), extensively drug-resistant (XDR), pandrug-resistant (PDR) [21].
Biofilm Production
To perform this test, an isolated colony of each strain identified was transferred to the BHI broth and incubated in a BOD incubator, 35±2 ºC, for a period of 24 hours. Subsequently, the test was assembled in sterile 96-well polystyrene microtiter plates and deposited in all wells of the plate, 198 μL of Tryptic Soy Broth—TSB (OXOID®), supplemented with 1% glucose (MERCK®) and 2 μL of BHI + Strain, totaling 200 μL per well. The positive control used was the ATCC 0027 strain Pseudomonas aeruginosa and the negative control was TSB broth + 1% glucose. All samples and controls were tested in triplicate. The plate was covered and taken to the BOD incubator, 35±2 ºC, for 48 hours and the reading continued in four different steps: plate washing 3 times with 300 uL of 0.9% sterile saline, heat fixation in an incubator at 60°C (1 hour), staining with 150 uL of crystal violet at 2% (15 minutes), and resolubilization with 150 uL of 95% alcohol (30 minutes), and finally, measurement of the results in a microtiter plate reader (Thermo Plate®) at 550 nm. The averages of the triplicates were calculated and compared with the average of the negative control, performed using the cutoff point (Cut off—ODc) according to the formula: ODc = (Average OD-) + (3 x sd). The strains were classified as non-biofilm producers, and weak, moderate and strong biofilm producers [22].
DNA Extraction from Isolates
DNA extraction was performed on all gram-positive strains isolated by the boiling method, following the technique of Olsvick and Strockbine [23] with minor modifications. The isolates were resuspended in BHI broth and incubated in a BOD incubator overnight, and then transferred to 1.5 mL microtubes, centrifuged at 8000 rpm for 4 minutes, and the supernatant was discarded. They were then resuspended in 200μl of TE (Tris-Acetate-EDTA) buffer solution, vortexed and centrifuged again, with supernatant being discarded and the process repeated three times. At the end of the last wash, the pellet was resuspended, placed in a water bath at 95ºC for 10 minutes, centrifuged for 20 seconds at 8000 rpm, and the supernatant was then transferred to a 500uL microtube and stored at -20ºC until use.
Detection of Operon Genes ica (icaA and icaD)
The strains were subjected to the PCR technique as described by Proietti et al. [24], with the primers F: ACTGTTTCGGGGACAAGCAT and R: ATTGAGGCTGTAGGGCGTTG (134 bp) for the gene ica A and F: CGTTAATGCCTTCTTTCTTATTGCG and R: ATTAGCGCACATTCGGTGTT (166 bp) for the gene ica D. The reaction was performed with 25 μL and with reagents from the PCR kit from Promega Corporation (GoTaq® G2 Master Mix) containing 5 μL of Buffer with MgCl2 (5X), 200 μM of deoxyribonucleotide triphosphates (dNTP), 10 μM of each primer, 1 U of Taq polymerase and 30 ng/μl of DNA (Nanodrop®) from each sample. The amplification cycle used was (94°C/3 min, 35 × (94°C/15 s, 60°C/20 s, 72°C/20 s), final extension at 4°C) performed in a thermocycler (Bioer®) and the visualization of the reaction products was done in 1.5% agarose gel electrophoresis in 0.5X TBE buffer (0.05 mM Tris, 1.25 mM EDTA, and 0.05 M boric acid stained with ethidium bromide), using 10 uL of each sample and 1 uL of 1 Kb molecular size marker (Kasvi®), this only in the first well. The gel was visualized under ultraviolet light after the products were stained with Gelred (Invitrogen®). The positive control of the reaction was a strain of S. pseudintermedius carrier of the operon genes ica.
Statistics
The results regarding identification, antimicrobial susceptibility testing, and phenotypic biofilm production were expressed as a percentage of positivity frequency (%), while the results of genetic analysis were entered into the software BioEstat® version 5.0, to calculate the Kappa coefficient agreement [25].
3. Results
Of the 33 samples collected, 66 isolates were obtained, 22 isolates from the general areas, 21 isolates from the first collection from the surgical suite, and 23 isolates from the second collection from the surgical suite. Of these, 77% (51/66) were gram-positive and 23% (15/66) were gram-negative. The frequency of positivity for the isolated gram-positive species were respectively: Bacillus sp. 27% (18/66), Staphylococcus epidermidis 17% (11/66), coagulase-negative Staphylococcus 15% (10/66), Staphylococcus pseudintermedius 12% (8/66), Staphylococcus aureus 3% (2/66), and Enterococcus sp. 3% (2/66). For gram-negative bacteria, they were: Enterobacter sp. 9% (6/66), Escherichia coli 8% (5/66), Klebsiella pneumoniae 4% (3/66), and Acinetobacter sp. 1.5% (1/66). Table 1 shows the collected locations, the identified species, and their respective resistance profiles and biofilm production capacity through the phenotypic test.
Regarding the antimicrobial susceptibility test (AST), it was possible to observe MDR, ESBL, MRSA/MRSP resistance patterns and methicillin-resistant Staphylococcus sp. (MRS). In this study, 44% (29/66) bacteria were MDR, with 90% (26/29) being gram-positive and 10% (3/29) gram-negative, and no bacteria were classified as XDR and PDR. For ESBL profile, 36% (5/14) samples presented this profile. The only species that did not show resistance to any antimicrobial was the isolate of Acinetobacter sp., which was tested for the antimicrobials: ticarcillin/clavulanic acid (85 µc), imipenem (10 µc), meropenem (10 µc), ciprofloxacin (0.5 µc), amikacin (30 µc), gentamicin (10 µc) and levofloxacin (0.5 µc). Figure 1 and Figure 2 show the resistance profiles found for the species of the genus Staphylococcus and isolated Enterobacteriaceae.
For the Enterococcus sp., the two isolated samples presented NDR profiles. As for the species of Bacillus sp., two samples were MDR and sixteen were NDR.
Biofilm production by the phenotypic test resulted in a total of 57% (38/66) of the isolates capable of forming biofilm. Approximately 79% (30/38) of these forming bacteria were gram-positive ones, with 12 isolates from Bacillus sp., 5 isolates of S. epidermidis, 5 isolates of coagulase-negative S., 5 isolates of S. pseudintermedius, 2 isolates of S. aureus, and 1 isolate of Enterococcus sp. For gram-negatives, 21% (8/38) were biofilm formers, with 3 isolates of Enterobacter sp., 3 isolates of E. coli, 1 isolate of K. pneumoniae, and 1 isolate of Acinetobacter sp. Regarding the classification according to degree of formation, 42% (28/66) of the samples were not biofilm formers, 92% (35/38) were weak formers, and 8% (3/38) were moderate producers, with no strong producer samples (0/38).
Genetic analysis of the operon ica (ica A and ica D) was carried out for the species of Staphylococcus sp., with the results being compared with those obtained by phenotypic analysis, which are expressed in Table 2 below:
Phenotypically, 55% (17/31) bacteria were able to produce biofilm, while 45% (14/31) were not. Genotypically, 23% (7/31) were positive only for the gene ica D, 19% (6/31) were positive for the gene ica A and D, and 58% (18/31) did not present any of the genes researched. When comparing the results, a discrepancy between them could be observed, with the Kappa index being -0.0164, with weak agreement between the two parameters analyzed.
4. Discussion
Hospital surfaces, equipment and objects are important sources of microorganisms and have been currently and constantly studied [26,27,28,29,30,31]. In this study, 66 bacteria from different surfaces and objects were isolated from the veterinary hospital, 77% (51/66) being gram-positive bacteria and 23% (15/66) being gram-negative bacteria. Souza et al. [31] obtained 105 isolates from different surfaces and objects of a hospital for humans in Paraná, of which 84% (88/105) were gram-positive bacteria and 16% (17/105) gram-negative bacteria, data that corroborate this study.
These comparative results, despite not being from veterinary hospitals due to the scarcity of studies in this area, promote the observation of a pattern regarding the species most frequently isolated in general and veterinary hospitals and thus, at the level of One Health. In addition, the pathogens accounting for human HAIs are the same as those responsible for veterinary HAIs [32], which justifies the comparison between these different facilities and the high antimicrobial resistance present today, since the medications used are also the same.
Bacillus sp. (27%) (18/66) was the most frequently isolated bacteria. Similar results were found for Palace et al. [28], who obtained 52% (11/21) of Bacillus sp. in their hospital isolates; Renner and Carvalho [29], who found 15% (6/40) of Bacillus sp. on surfaces of an Intensive Care Unit (ICU); and Rosa et al. [33], who identified 9.66% (38/392) of this species in aerosols from an ICU. These findings indicate that this species, despite not being considered a pathogen for HAIs, may be present on any hospital surface, and that the high rate of biofilm production identified in the present study becomes a problem, mainly due to the knowledge that biofilms are capable of harboring other microorganisms, being a potential reservoir for them [34].
S. epidermidis 17% (11/66) was isolated on various surfaces and objects analyzed in this study, while coagulase-negative S., 15%, (10/66) was identified only in the hospital’s surgical suite. Conversely, S. pseudintermedius 12% (8/66) was isolated from various surfaces and objects in the hospital, being mostly present in general areas, as well as S. aureus 3% (2/66). These species are frequently found on hospital equipment such as stethoscopes and bed side rails [35], on doorknobs, computer keyboards, countertops, tables, beds, monitors, IV dispensers, and ICU bed ventilators [29,36,37,38], and are increasingly present in cultures from animals admitted to veterinary hospitals [39]. They are considered opportunistic pathogens, accounting for infectious processes in animals, such as pyoderma, external otitis, uropathies, pneumonia, and bacteremia, in addition to causing around 74% of surgical site infections in veterinary hospitals, of which only 26% respond to preoperative medications, extremely worrying rates for animal health and public health [40].
Enterococcus sp. 3% (2/66) was isolated from two rooms of the surgical suite. In the study by Grosh et al. [41], this species has been isolated from cage doors, stethoscopes, and veterinary hospital thermometers. It was also found on hospital surfaces and floors [29,42]. Its natural presence in the gastrointestinal flora of cats and dogs suggests its spread to the hospital environment through the feces of these animals. Despite the low incidence reported, these species should be monitored, a fact that is already happening in some veterinary environments, mainly because they cause diseases that are difficult to treat [43].
For gram-negative species, Enterobacter sp. 9% (6/66) was isolated from the general areas of the hospital, while E. coli 8% (5/66) and K. pneumoniae 4% (3/66) were found in both areas. They are included in the family Enterobacteriaceae and participate in the human and animal intestinal microbiota, having been reported as having high antimicrobial resistance profiles, causing urinary and bloodstream infections in hospitalized patients [44]. Several studies report the prevalence of these species on floors, waste bins, and bed rails for human hospitals [45,46,47] and on surfaces and objects in veterinary hospitals with ESBL and MDR profiles [27,30]. Acinetobacter sp., 1.5% (1/66), was isolated in the hospital’s surgical suite, showing sensitivity to all antimicrobials. Souza et al. [48], evaluating the surfaces of stretchers in a hospital, found 4 strains of this species, 2 of which were 100% sensitive to the antimicrobials tested, which corroborates this study.
Data relating to sensitivity profiles are similar to the rates found in other studies, and the threat to global health is clear [27]. These facts are related to overdose used as prophylaxis of infections, promotion of animal growth, and promotion of reliability in export. Accordingly, there is a lack of regulation and inspection of sales, excessive and inappropriate use and improper dumping in industrial effluents, which are important sources of dissemination and selection of multiresistant microorganisms in the environment [49,50].
Biofilm production demonstrates that at least one microorganism of each isolated species was capable of producing it. These findings are also a great concern, since biofilms provide a favorable environment for the exchange of genetic material and thus make recommended treatments even more difficult, increasing animal death rates. Most studies that aim to evaluate biofilm production are related to clinical samples from patients, with few studies on hospital objects and surfaces. However, Silva et al. [51], in their study, identified 93% (13/13) of microorganisms in 13 stethoscopes of employees of a general hospital, of which 85% (11/13) showed moderate biofilm formation, demonstrating that strains from abiotic surfaces can be as harmful as those from clinical samples.
Thus, it is concluded that biofilms are important mechanisms of virulence and resistance, being regulated by several different pathways, this being the hypothesis when the divergence in our comparative data of phenotypic formation and presence of genes ica A and D [12] were found. Studies indicate that the frequency of biofilm formation and consequent presence of operon genes ica vary according to the sample studied and also according to environmental criteria, such as the low expression of this operon in anaerobic and in vitro growth, a fact that was induced in this study [12,52]. Furthermore, the expression of regulatory inducer genes and proteins can suppress the expression of ica, and the biofilm can form through other mechanisms such as the operon agrABCD, RNAII and RNAIII, and the Bhp or Aap proteins, these being independent pathways of the Polysaccharide Intercellular Adhesive (PIA) [13,53].
5. Conclusions
The present study identified a series of microorganisms that may be pathogenic, distributed throughout the various facilities of the veterinary hospital, and there is a great lack of studies of surfaces and objects related to veterinary environments in the literature. There was a predominance of gram-positive bacteria, which is explained by the fact that they are largely present in the microbiota of human and animal skin, with high rates of antimicrobial resistance and the ability to form biofilms. The results emphasize the concern regarding the dissemination of these microorganisms in hospital environments and regarding a possible zoonotic potential, stressing the need for correct prevention measures, hospital infection control programs in veterinary environments, and performance of new studies, to identify possible reservoirs, avoiding outbreaks and contributing to epidemiological data.
Author Contributions
Conceptualization: VB, DPGP and HHAR; methodology: VB, DPGP, SRRF, CPP and EGPF; formal analysis: VB, SRRF and HHAR; investigation: VB; CPP and EGPF; data curation: VB, SRRF, WGS and HHAR; writing—original draft preparation: VB, DPGP, SRRF and HHAR; writing—review and editing: VB, WGS and HHAR; supervision: WGS and HHAR; project administration: HHAR. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| MDR | Multidrug-resistant |
| MRSA | Methicillin-resistant Staphylococcus aureus |
| MRSP | Methicillin-resistant Staphylococcus pseudintermedius |
| MRS | Methicillin-resistant Staphylococcus sp., |
| ESBL | Extended spectrum β-lactamase |
| NDR | Does not present multidrug resistance |
| XDR | Extensively drug-resistant |
| PDR | Pandrug-resistant |
| HAIs | Healthcare-Associated Infections |
| EPS | Extracellular polymeric substance |
| PIA | Polysaccharide intercellular adhesin |
| ICA | ica operon |
| BHP | Homologous biofilm-associated protein |
| AAP | Accumulation-associated protein |
| BHI | Brain Heart Infusion |
| AST | Antimicrobial susceptibility testing |
| BrCAST | Brazilian Committee on Antimicrobial Susceptibility Testing |
| TSB | Tryptic Soy Broth |
| dNTP | deoxyribonucleotide triphosphates |
References
- Brasil (1998). Ministério da Saúde. Portaria nº 2.616 de 12 de maio de 1998. Dispõe sobre as diretrizes e normas para a prevenção e o controle das infecções hospitalares. Brasília, DF.
- Hayashi CMT, Silva PS, Silva RM, Ribeiro T (2017). Prevenção e controle de infecções relacionadas a assistência à saúde: fatores intrínsecos ao paciente. HU revista., 43(3):277-283.
- Stull JW, Weese JS (2015). Hospital-Associated Infections in Small Animal Practice. The Veterinary Clinics of North America Small Animal Practice, 45(2):217–233. [CrossRef]
- Verdial CSS (2020). Prevenção de Infecções Nasocomiais: Controle bacteriológico de superfícies hospitalares de unidade de isolamento e contenção biológica do hospital escolar da FMV-ULisboa. Dissertação de mestrado integrado em medicina veterinária—Universidade de Lisboa.
- Rowlinson MC, Lebourgeois P, Ward K, Song Y, Finegold SM, Bruckner DA (2006). Isolation of a strictly anaerobic strain of Staphylococcus epidermidis. J. Clin. Microbiol.,44:857–860. [CrossRef]
- Arnaouteli S, Bamford NC, Stanley-Wall NR, Kovács ÁT (2021). Bacillus subtilis biofilm formation and social interactions. Nat. Rev. Microbiol., 2021, 19(9):600–614. [CrossRef]
- Ciofu O, Tolker-Nielsen T (2019). Tolerance and resistance of Pseudomonas aeruginosa biofilms to antimicrobial agents-how P. aeruginosa can escape antibiotics. Frontiers in Microbiology., 10:913. [CrossRef]
- Chiba A, Seki M, Susuki Y, Kinjo Y, Mizunoe Y, Sugimoto S (2022). Staphylococcus aureus utilizes environmental RNA as a building material in specific polysaccharide-dependent biofilms. NPJ Biofilms Microbiomes., 8(1):17. [CrossRef]
- Yin W, Wang Y, Liu L, He J (2019). Biofilms: the microbial “protective clothing” in extreme environments. International Journal of Molecular Sciences., 20(14): 3423. [CrossRef]
- Abebe GM (2020). The role of bacterial biofilm in antibiotic resistance and food contamination. Int. J. Microbiol.. doi: 2020:1705814. [CrossRef]
- Zhao A, Sun J, Liu Y (2023). Understanding bacterial biofilms: From definition to treatment strategies. Front. Cell Infect Microbiol., 13:1137947. [CrossRef]
- François P, Schrenzel J, Götz F (2023). Biology and Regulation of Staphylococcal Biofilm. Int J Mol Sci., 9;24(6):5218. [CrossRef]
- Cataneli Pereira V, Pinheiro-Hubinger L, de Oliveira A, Moraes Riboli DF, Benini Martins K, Calixto Romero L, Ribeiro SCML (2020). Detection of the agr System and Resistance to Antimicrobials in Biofilm-Producing S. epidermidis. Molecules. 3;25(23):5715. [CrossRef]
- Ruhal R, Kataria R (2021). Biofilm patterns in gram-positive and gram-negative bactéria. Microbiological Research, 251:126829. [CrossRef]
- Stull JW, Bjorvik E, Bub J, Dvorak G, Petersen C, Troyer HL (2018). AAHA Infection Control, Prevention, and Biosecurity Guidelines. Journal of the Americam Animal Hospital Association., 54(6):297–326. [CrossRef]
- Gaschen F (2008). Nosocomial Infection: Prevention and Approach. Dublin (IE): World Small Animal Veterinary Association World Congress.
- Portner JA, Johnson JA (2010). Guidelines for reducing pathogens in veterinary hospitals: disinfectant selection, cleaning protocols, and hand hygiene. Compend Contin Educ Vet., 32(5):E1-11.
- Mann A (2018). Hospital-acquired infections in the veterinary establishment. Vet Nurs J., 33(9):257– 261. [CrossRef]
- Anvisa (2013). Agência Nacional de Vigilância Sanitária. Microbiologia Clínica para o controle de infecção Relacionada à Assistência a Saúde. Módulo 6: Detecção e identificação de bactérias de importância médica. Brasília.
- Brazilian Committee on Antimicrobial Susceptibily Testing, BRCast. (2023). Orientações do EUCast/BRCast para a detecção de mecanismos de resistência e resistências específicas de importância clínica e/ou epidemiológica. Versão 2.0. 2023.
- Magiorakos AP et al. (2012). Bactérias multirresistentes, extensivamente resistentes e pan droga resistentes a medicamentos: uma proposta internacional especializada para definições padrão provisórias para resistência adquirida. Clinical Microbiology and Infection., 18(3):268–281.
- Stepanovic S, Vukovic D, Hola V, Bonaventura GD, Djukic S, Cirkovic I, Ruzicka F (2007). Quantification of biofilm in microtiter plates: overview of testing conditions and practical recommendations for assessment of biofilm production by Staphylococci. APMIS. 115(8):891-899. [CrossRef]
- Olsvick O, Strockbine NA (1993). PCR detection of heat-stable, heat-labile, and Shiga-like toxin genes in Escherichia coli. In: Diagnostic Molecular Microbiology: Principles and Applications. American Society for Microbiology, 271–276.
- Proietti PC, Stefaneti V, Hyatt DR, Marenzoni ML, Capomaccio S, Coletti M, Bietta A, Franciosini MP, Passamonti F (2015). Phenotypic and genotypic characterization of canine pyoderma isolates of Staphylococcus pseudintermedius for biofilm formation. Journal of Veterinary Medical Science, 77(8): 945-951. [CrossRef]
- Pereira MG (1999) Epidemiologia: Teoria e Prática. Guanabara Koogan, Rio de Janeiro.
- Mahl S, Rossi EM (2017). Suspectibilidade antimicrobiana de bactérias isoladas de colchões hospitalares. RBAC., 49(4): 371-375. [CrossRef]
- Oliveira FA, Stella AE (2019). Enterobactérias multirresistentes presentes em ambiente hospitalar veterinário. Pesquisa Veterinária Brasileira.
- Palácio PB, Aquino PEA, Silva ALA, Sousa KRF, Leandro LMG, Guedes TTAM, Macedo RO (2018). Perfil de resistência em bactérias isoladas de superfícies de um hospital público de Juazeiro do Norte-CE. Revista Saúde (Sta. Maria).,44(2). [CrossRef]
- Renner JDP, Carvalho ED (2013). Microrganismos isolados de superfícies da UTI adulta em um hospital do Vale do Rio Pardo—RS. Revista de Epidemiologia e Controle de Infecção., 3(1): 40-44.
- Sfaciotte RAP, Passurolo L, Melo FD, Bordignon G, Israel ND, Salbego FZ, Wosiacki SR, Ferraz SM (2021). Detection of the main multiresistant microorganisms in the environment of a teaching veterinary hospital in Brazil. Brazilian Journal of Veterinary Research., 41:e06706, 2021. [CrossRef]
- Souza SGP, Santos IC, Bondezan MAD, Corsatto LFM, Caetano ICS, Zaniolo MM, Matta R, Merlini LS, Barbosa LN, Gonçalves DD (2020) Bacteria with a Potential for Multidrug Resistance in Hospital Material. Microbial Drug Resistance. [CrossRef]
- Anvisa (2017). Agência Nacional de Vigilância Sanitária. Critérios diagnósticos de infecção relacionada a assistência à saúde. 2.ed. Brasília: Anvisa, 2017. Disponível em: http://portal.anvisa.gov. br/documents/33852/3507912/Caderno+2+-, 2017.
- Rosa NOM, Costa CP, Castro MFL, Gaggini MCR, Favaleça MF, Andreani DIK (2021). Análise Microbiológica de Bioaerossóis em uma Unidade de Tratamento Intensivo de Pacientes Afetados por COVID-19. International Journal of Development Research., 11(11): 51938-51941.
- Flemming HC, Wingender J, Szewzyk U, Steinberg P, Rice AS, Kjelleberg S (2016). Biofilms: an emergent form of bacterial life. Nature Reviews Microbiology.,14(9):563–575.
- Damasceno Q (2010). Características epidemiológicas dos microrganismos resistentes presentes em reservatórios de uma Unidade de Terapia Intensiva. Dissertação. Belo Horizonte: Escola de Enfermagem/UFMG.
- Bender JB, Schiffman E, Hiber L, Gerads L, Olsen K (2012). Recovery of Staphylococci from computer keyboards in a veterinary medical centre and the effect of routine cleaning. Vet Rec.,170(16): 414–414. [CrossRef]
- Cordeiro LAO, Oliveira MM, Fernandes JD, Marinho CS, Barros A, Castro LMC (2015).Equipment contamination in an intensive care unit. Acta Paul Enferm.,8(2):160-165. [CrossRef]
- Corrêa ER, Machado AP, Bortolini J, Miraveti JC, Corrêa LVA, Valim MD (2021). Bactérias resistentes isoladas de superfícies inanimadas em um hospital público. Cogitare enferm., 26:e74774. [CrossRef]
- Shoen HRC, Rose S, Ramsey AS, Morais H, Bermudez LE (2019). Analysis of staphylococcus infections in a veterinary teaching hospital from 2012 to 2015. Comparative Immunology, Microbiology and Infectious Diseases, 66:101332. [CrossRef]
- Turk R, Singh A, Weese JS (2015). Prospective surgical site infection surveillance in dogs. Vet Surg.,44(1):2–8. [CrossRef]
- Ghosh A, Kukanich K, Brown CE, Zurek L (2012). Resident Cats in Small Animal Veterinary Hospitals Carry Multi-Drug Resistant Enterococci and are Likely Involved in Cross Contamination of the Hospital Environment. Frontiers Microbiology., 3:62. [CrossRef]
- Deshpande A, Cadnum J, Fertelli D, Sitzlar B, Thota P, Mana TS, Jencson A, Alhmidi H, Koganti S, Donskey CJ (2017). Are Hospital floors na underappreciated reservoir for transmission of health care-associated pathogens? American Journal of Infection Control. 1;45 (3): 336-338. [CrossRef]
- Ye-In Oh, Baek J, Kim SH, Kang BJ, Youn H (2018). Antimicrobial Susceptibility and Distribution of Multidrug-Resistant Organisms Isolated From Environmental Surfaces and Hands of Healthcare Workers in a Small Animal Hospital. Japanese Journal of Veterinary Research., 66(3): 193-202.
- Paula VG, Quintanilha LV, Silva Coutinho FA, Rocha HF, Santos FL (2016). Enterobactérias produtoras de carbapenemase: prevenção da disseminação de superbactérias em UTI’s. Ciências da Saúde., 14(2): 175-185. [CrossRef]
- Lago A, Fuentefria SR, Fuentefria DB (2010). Enterobactérias produtoras de ESBL em Passo fundo, Estado do Rio Grande do Sul, Brasil. Soc Bras Med Trop., 43(4):430-34. [CrossRef]
- Mahl S, Rossi EM (2017). Suspectibilidade antimicrobiana de bactérias isoladas de colchões hospitalares. RBAC., 49(4): 371-375. [CrossRef]
- Nogueira PSF, Moura ERF, Costa MMF, Monteiro WMS, Brondi L (2009). Perfil da Infecção Hospitalar em um Hospital Universitário. Rev. Enferm. UERJ., 17(1):96-101.
- Oliveira FA, Stella AE (2019). Enterobactérias multirresistentes presentes em ambiente hospitalar veterinário. Pesquisa Veterinária Brasileira.
- Souza WKS, Santana MMR, Libório RC, Santos HAS, Oliveira KR, Guimarães MD, Shiosaki RK, Naue CR (2021) Avaliação da população bacteriana na superfície de macas de um hospital universitário de Pernambuco. Research Society and Development.,10(14):e20101421509. [CrossRef]
- Samreen I.A. et al. (2021). Environmental antimicrobial resistance and its drivers: a potential threat to public health. Journal of Global Antimicrobial Resistance., 27:101-111. [CrossRef]
- Tang kl. et al. (2017). Restricting the use of antibiotics in food-producing animals and its associations with antibiotic resistance in food-producing animals and human beings: a systematic review and meta-analysis. Lancet Planet Health., 1(8):e316-e327. [CrossRef]
- Silva IA, Melo CC, Barbosa TSL, Martins LR, Oliveira SR (2023). Estetoscópios de uso hospitalar como fonte de infecção por bactérias resistentes produtoras de biofilme. RBAC. [CrossRef]
- Qin Z, Yang X, Yang L, Jiang J, Ou Y, Molin S, Qu D. (2007). Formation and properties of in vitro biofilms of ica-negative Staphylococcus epidermidis clinical isolates. J. Med. Microbiol. 56:83–93. [CrossRef]
- Otto M. (2009). Staphylococcus epidermidis—The “accidental” pathogen. Nat. Rev. Microbiol., 7:555–567. [CrossRef]
Figure 1.
Resistance profiles for isolated species of the genus Staphylococcus.
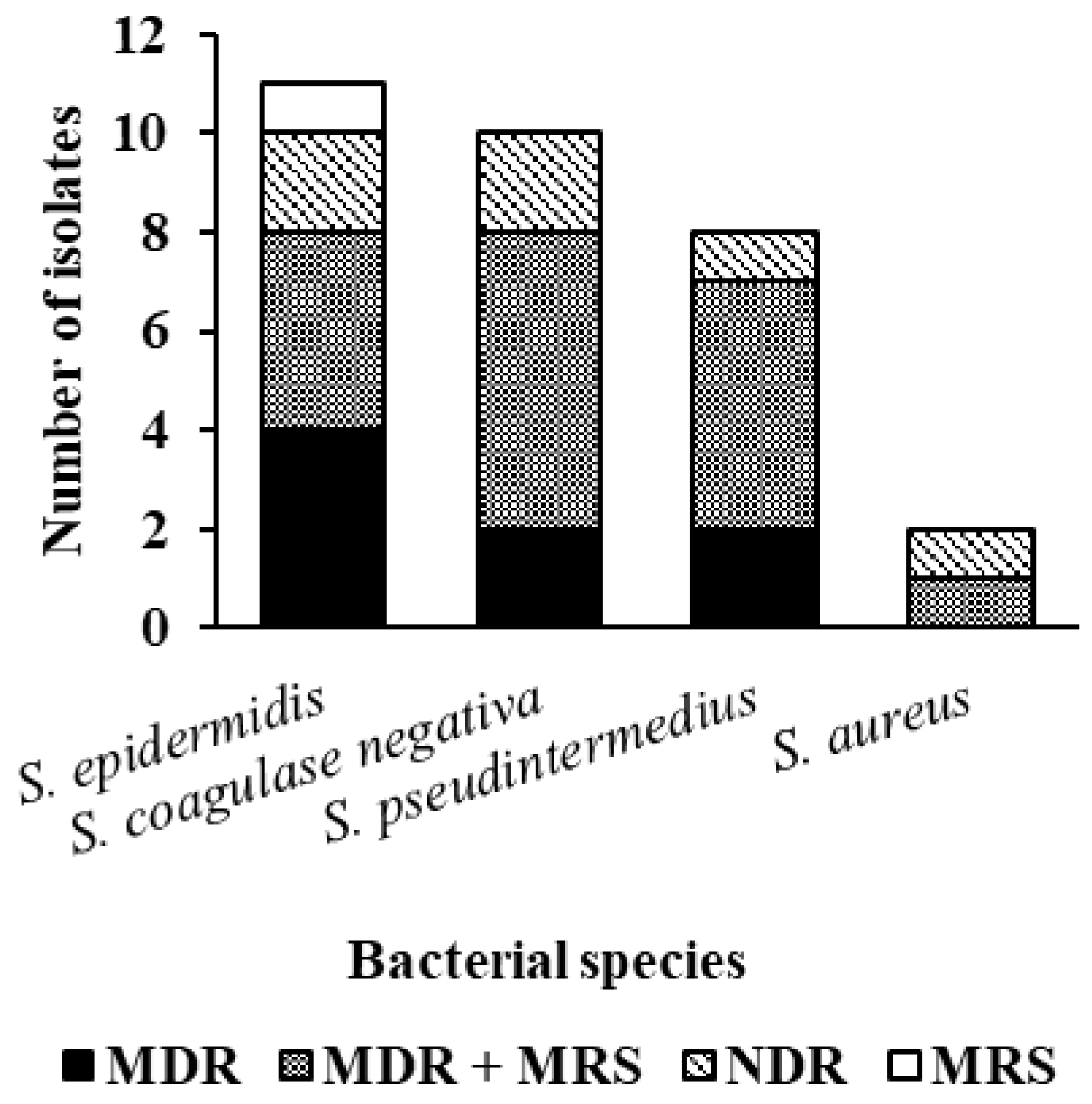
Figure 2.
Resistance profiles for isolated species of the genus Enterobacteriaceae.
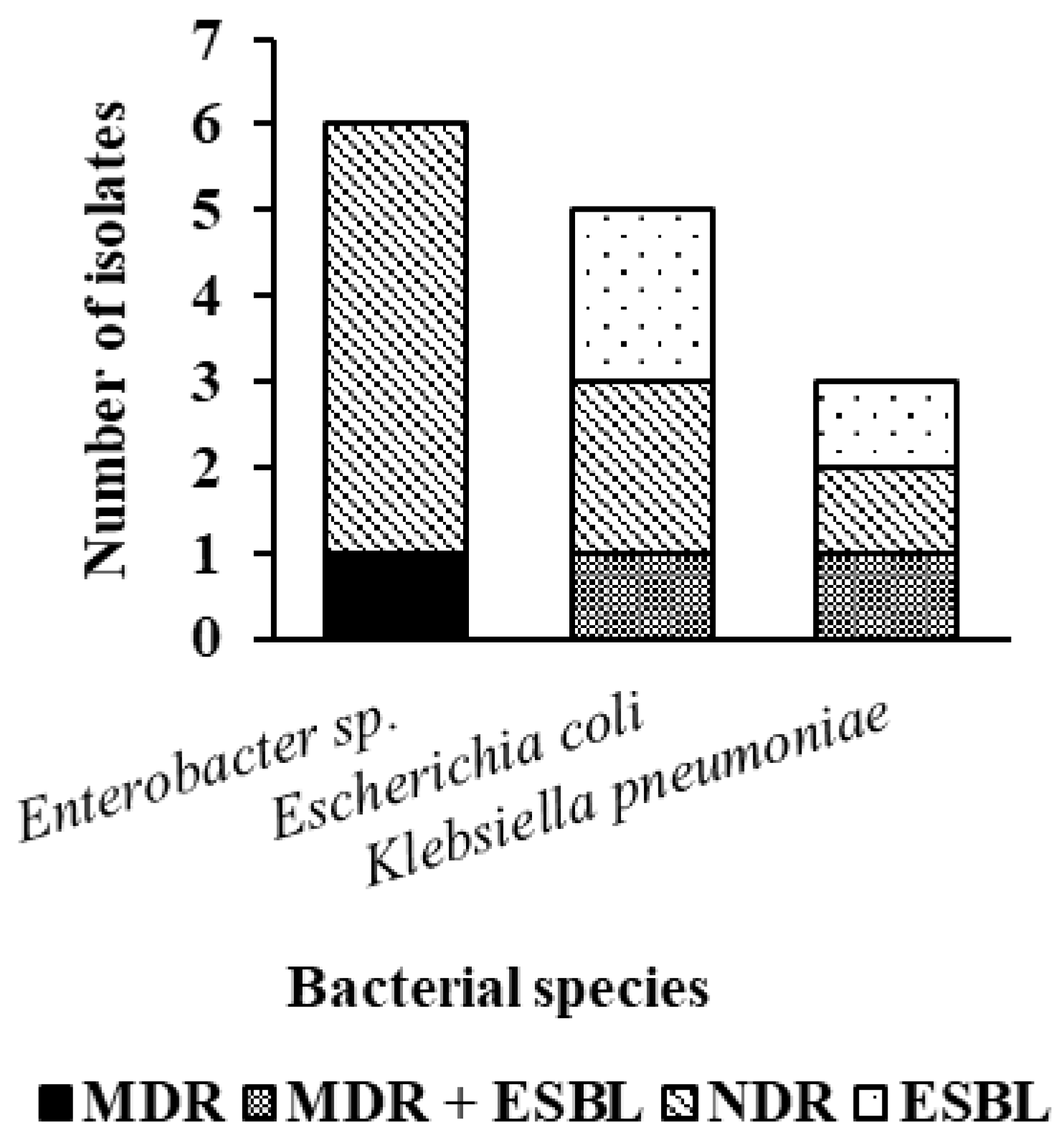

Table 1.
Collection sites, identified species, resistance profile, and biofilm production in general areas and operating room of the veterinary hospital.
Table 1.
Collection sites, identified species, resistance profile, and biofilm production in general areas and operating room of the veterinary hospital.
| General areas | Operating Room | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Collection 01 | Collection 02 | Collection 03 | ||||||||
| Locations of Collection |
Species bacterial |
Resistance Profile | Biofilm production | Locations of Collection |
Species bacterial |
Resistance Profile | Biofilm production | Species bacterial |
Resistance Profile | Biofilm production |
| Reception desk computer keyboard |
K. pneumoniae S. pseudintermedius |
ESBL MDR |
No Weak |
Heart rate monitor cable pigtails |
S. epidermidis (S2) Bacillus sp. (S2) |
MDR MDR |
Weak Moderate |
Bacillus sp. (S1) Bacillus sp.(S2) Enterobacter sp. (S2) |
NDR NDR NDR |
No Moderate No |
| Screening room stethoscope | S. pseudintermedius | MDR | No | Heart monitor |
S. epidermidis (S1) S. epidermidis (S2) |
MDR/MRS MDR |
No Weak |
Bacillus sp.(S1) S. coagulase-negative (S2) Enterobacter sp. (S2) |
NDR MDR/MRS NDR |
No Weak No |
| Reception desk table |
S. pseudintermedius S. epidermidis E. coli |
MDR/MRSP MRS ESBL |
No No Weak |
Anesthesia machine (vaporizer) |
S. coagulase-negative (S2) S. coagulase-negative (S2)S. epidermidis (S2) |
MDR MDR/MRS NDR |
No Moderate No |
S. coagulase-negative (S1)Bacillus sp. (S1) S. epidermidis (S2) |
NDR NDR MDR |
Weak Weak No |
| Office 02 reception desk |
E. coli Bacillus sp. |
ESBL NDR |
Weak Weak |
Operating table |
S. pseudintermedius Acinetobacter sp. (S2) |
NDR NDR |
No Weak |
Bacillus sp. (S1) Bacillus sp.(S2) |
NDR NDR |
No No |
| Office 02 table for animal screening |
Enterobacter sp. S. epidermidis |
NDR MDR/MRS |
No Weak |
Thermal mat | No bacterial growth | - | - |
Enterococcus sp.(S1) Bacillus sp. (S2) |
NDR NDR |
Weak No |
| Marble counter in the admission room | Enterobacter sp. S. pseudintermedius |
MDR/ESBL MDR/MRSP |
Weak Weak |
Table of surgical instruments |
S. epidermidis (S1) S. pseudintermedius (S2) |
MDR MDR/MRSP |
No Weak |
S. pseudintermedius (S2) Bacillus sp.(S2) |
MDR/MRSP MDR |
Weak Weak |
| Animal care table in the admission room |
E. coli S. aureus |
NDR MDR/MRSP |
No Weak |
Marble countertop |
S. epidermidis (S1) K. pneumoniae (S1) coagulase-negative S. (S2) K. pneumoniae (S2) |
MDR/MRS NDR MDR/MRS MDR/ESBL |
Weak Weak No No |
Bacillus sp.(S1) S. epidermidis (S1) Bacillus sp.(S2) |
NDR MDR/MRS NDR |
Weak Weak Weak |
| Microwave in the admission room |
S. aureus Enterobacter sp |
NDR MDR |
Weak Weak |
Surgical light | coagulase-negative S. (S2) | NDR | Weak |
Bacillus sp. (S1) S. epidermidis (S1) S. coagulase-negative (S2) |
NDR NDR MDR/MRS |
Weak No No |
| Animal pen in the admission room |
S. pseudintermedius Enterobacter sp. |
MDR/MRSP NDR |
Weak Weak |
PPE cabinet surface | coagulase-negative S. (S2) S. coagulase-negative (S2) |
MDR MDR/MRS |
No No |
No bacterial growth | ||
| Infectious Diseases Animals pen |
Bacillus sp. Bacillus sp. |
NDR NDR |
Weak No |
*Sink tap and basin | No growth bacterial |
- | - | No bacterial growth | - | - |
| Equipment named preoperative room trachea |
Bacillus sp. Bacillus sp. |
NDR NDR |
Weak Weak |
*Microwave |
E. coli E. coli Enterococcus sp. |
NDR NDR NDR |
No Weak No |
coagulase-negative S. Bacillus sp. |
MDR/MRS NDR |
Weak Weak |
MDR—Multidrug-resistant; NDR—Does not present multidrug resistance; MRSA—methicillin-resistant Staphylococcus aureus; MRSP—methicillin-resistant Staphylococcus pseudintermedius; MRS—methicillin-resistant Staphylococcus sp., ESBL—extended spectrum β-lactamase. S1—room 1 of the surgical suite, S2—room 2 of the surgical suite. * common areas for both rooms of the operating room. PPE: Personal Protective Equipment. For the general areas, the place with the highest number of isolates was the reception desk with three isolates: S. pseudintermedius, S. epidermidis, and E. coli, while the place with the least isolates was the stethoscope in the triage office, with only one isolate, which was S. pseudintermedius. For the surgical suite, the place with the most isolates was the marble bench, which with the two collections added totaled seven isolates: two isolates of S. epidermidis, two isolates of K. pneumoniae, an isolate of coagulase-negative S. and two isolates of Bacillus sp., while the place that had the least isolates was the sink, which with the two collections added and this being a common place for the two surgical rooms of the suite, had no isolates.
Table 2.
Comparison between the results of the phenotypic test with crystal violet and the genotypic test of the genes ica A and ica D for biofilm formation.
Table 2.
Comparison between the results of the phenotypic test with crystal violet and the genotypic test of the genes ica A and ica D for biofilm formation.
| Collection 1 | Collection 2 | Collection 3 | ||||||
|---|---|---|---|---|---|---|---|---|
| Bacterial species | Biofilm phenotypic |
Biofilm genotypic |
Bacterial species | Biofilm phenotypic |
Biofilm genotypic |
Bacterial species | Biofilm phenotypic |
Biofilm genotypic |
|
S. pseudintermedius S. pseudintermedius S. pseudintermedius S. epidermidis S. epidermidis S. pseudintermedius S. aureus S. aureus S. pseudintermedius |
Weak No No No Weak Weak Weak Weak Weak |
No No No No No No No No No |
S. epidermidis S. epidermidis S. epidermidis Coagulase-negative S. Coagulase-negative S. S. epidermidis S. pseudintermedius S. epidermidis S. pseudintermedius S. epidermidis Coagulase-negative S. Coagulase-negative S. Coagulase-negative S. Coagulase-negative S. |
Weak No Weak No Moderate No No No Weak Weak No Weak No No |
Ica A and D No Ica D Ica D Ica D Ica D Ica D Ica A and D Ica A and D Ica D No Ica D No No |
Coagulase-negative S. Coagulase-negative S. S. epidermidis S. pseudintermedius S. epidermidis S. epidermidis Coagulase-negative S. Coagulase-negative S. |
Weak Weak No Weak Weak No No Weak |
No No No No No Ica A and D Ica A and D Ica A and D |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



