Submitted:
02 July 2025
Posted:
03 July 2025
You are already at the latest version
Abstract
Between 2015 and 2022, we evaluated a novel BR 16S PCR rDNA PCR/Sanger sequencing assay to improve diagnosis of invasive infections in culture-negative specimens. Using dual-priming oligonucleotide (DPO), this assay analyzed ribo-somal DNA from sterile fluids or tissues. A total of 772 specimens from 661 patients were studied: 425 specimens (61%) had negative culture and BR 16S PCR tests; 245 specimens (35%) had negative cultures but positive BR 16S PCR tests; and 29 specimens (4%) had negative cultures with indeterminate BR 16S PCR results. Excluding indeterminate results, the assay showed sensitivity, specificity, PPV, NPV, and accuracy of 93.9%, 99.77%, 99.64%, 95.97%, and 97.38%, re-spectively. Gram stain purulence predicted the BR 16S PCR result better (69.4%) than organisms (24.6%) but the latter had a higher PPV (78.5%). Increased peripheral WBC (86.1%) or CRP (71.8%) predicted positive BR 16S PCR results. Our DPO BR 16S PCR assay improved pathogen detection with minimal contamination.
Keywords:
broad-range BR 16S PCR rDNA PCR
; bacterial pathogen
; molecular diagnosis
; culture-negative
; invasive infection
1. Introduction
Clinical management of serious invasive diseases requires accurate organism identification often to the species-level [1,2,3,4,5,6]. Accurate organism detection and identification not only allows for appropriately directed antimicrobial therapy but also allows for a more narrow-based antimicrobial regimen to be used and improves duration of parenteral and stepdown oral therapy [7,8,9]. However, standard culture techniques may not yield a pathogen because the causative organism(s) are fastidious or uncultivatable, or prolonged antibiotic courses of therapy are given prior to clinical specimen collection (i.e., suspected endocarditis and operatively harvesting heart valve tissue during valve replacement) [10,11,12,13]. Chronic infections involving biofilms such as prosthetic joint infections (PJIs) may also not yield a pathogen by culture due to the sessile nature of these infections [14,15].
Increasingly, molecular methods are being used to try and detect pathogens in clinical specimens where patients have documented or confirmed invasive infections, and cultures have been negative [16,17]. Broad range BR 16S PCR/sequencing has been used to directly detect bacterial molecular signatures from clinical specimens without requiring microbial culture growth [10,11,12,13,14,15,18,19,20,21]. Routine BR 16S PCR rRNA gene PCR/sequencing was implemented in our laboratory more than two decades ago as a routine part of our diagnostic algorithms for identification of bacterial isolates [3,4,6]. We then developed and published our evaluation of a novel broad-range BR 16S PCR/sequencing assay for detection of fastidious or uncultivatable bacterial organisms from excised heart valve tissue for diagnosis of culture-negative infectious endocarditis [11]. This study outlines our subsequent experience deploying this novel broad range BR 16S PCR/Sequencing assay on a wide variety of other sterile fluids and tissues. Although broad-range PCR/sequencing in many jurisdictions is widely ordered without medical assessment of whether the clinical situation or available clinical specimens are of adequate quality to be tested, our center developed and used a scoring system for the clinical and laboratory criteria for approving this specialized test. BR 16S PCR BR-PCR/sequencing was evaluated for diagnosis of infectious diseases herein for central nervous system, bone and joint infection, and endovascular infection. We evaluated whether the molecular assay results against clinically relevant diagnostic test results and clinical diagnosis including the outcomes on management.
2. Materials and Methods
2.1. Study Design
We performed a retrospective cross-sectional study evaluating the effects of BR-PCR/sequencing on the diagnosis and management of infectious diseases in the Calgary Health Zone between the time our assay was implemented for routine use in 2015 until 2022. A total of 761 individual clinical specimens were sent from 662 patients for in-house molecular testing during this 7-year period. If more than one clinical specimen was sent from the same patient, results were scored once if all results agreed but scored individually if different results were obtained for each sample. Performance of all BR-PCR/sequencing results were evaluated against clinical specimen Gram stains, all culture results for the patient, and changes in clinical management brought about by BR 16S PCR BR PCR/sequencing test results.
2.2. Patient Population
Patients were enrolled at the request of the patient’s attending Infectious Diseases physician after consultation with a Medical Microbiologist. Patients had a high pre-test likelihood of having an invasive infection. Electronic medical records were reviewed for demographics, BR 16S PCR assay acceptance criteria and characteristics of clinical specimens.
2.3. Laboratory Setting and Clinical Specimens
Microbiology testing was performed by the Division of Microbiology, Alberta Precision Laboratories (APL), Diagnostic and Scientific Centre (DSC), and Calgary Zone. APL is a large regional centralized laboratory that performs diagnostic testing for the entire Calgary Zone, including all ambulatory, hospitalized and long-term care patients. Clinical specimens were collected by experienced physicians, surgeons or interventional radiology under sterile conditions during each procedure or operation. Fluids and tissues were immediately placed into a sterile container and promptly transported to the centralized laboratory within 2 h after collection. Clinical specimens were immediately processed and set-up for culture as outlined below. Residual material from each specimen was stored at -80 to -86oC until DNA extraction.
Acceptance of clinical specimens for broad-range BR 16S PCR/sequencing analysis was based on a direct request by the patients consulting Infectious Diseases specialist to the on-call Medical Microbiologist to determine if the clinical diagnosis was invasive, and defining the microbial etiology impacts clinical management. Clinical specimens were then only sent for molecular analysis after review by the Medical
Microbiologists if the sterile fluid/tissue culture was confirmed negative, there was sufficient remaining clinical specimen with sterility to provide a high quality BR 16S PCR assay result and specific microscopic examination criteria and patient biomarker indicated active infection. Specifically, clinical specimens were preferred where the original Gram stain showed purulence and/or organisms, and the patient had an elevated peripheral white blood cell count that was predominantly neutrophils and an elevated C-reactive protein.
2.4. Microbiology Methods
- Culture
Blood and fluid cultures were performed using standard methods. Briefly, two separate sets of blood cultures [BacT/Alert FA (Aerobic) and FN (Anaerobic)] were collected from adults, immediately incubated in Virtuo instruments (bioMérieux, Laval, Quebec), and continuously monitored for up to 4-days for growth. Positive blood cultures were immediately removed, and an aliquot spun into pellet before plating onto routine media including Columbia blood agar (BA), chocolate agar (CHOC), MacConkey (MAC) agar and Brucella blood agar (BBA) for isolation of aerobic and anaerobic bacteria. BA, CHOC and MAC plates were incubated aerobically at 35oC for up to 7 days, while the BBA plate underwent anaerobic incubation in an Anoxamat cabinet (Mart Microbiology Inc., Drachten, Netherlands) for the same period. Sterile fluids were also handled and planted using similar methods. Tissues were aseptically disrupted in a tissue grinder in 0.5 mL brain heart infusion (BHI) broth. The BHI tube was centrifuged at 3000 x g centrifugal force for 15 min, and the supernatant was discarded. Aliquots (100 µL) of the prepared tissue sediment was immediately inoculated into a BacT/Alert FA and FN bottle, placed into the Virtuo cabinets for incubation and continuously monitored for up to 7 days. A 20-30 µL drop of the sediment was also planted onto BA, CHOC, MAC and BBA agars for aerobic and anaerobic culture. Plates were incubated as described earlier for positive blood cultures. Isolates were identified using a combination of matrix assisted laser-desorption ionization time of flight mass spectrometry (MALDI-TOF MS), rapid phenotypic tests (Gram stain, catalase, coagulase, oxidase, indole) and BR 16S PCR/sequencing whenever the initial MALDI-TOF MS result was discordant with phenotypic methods, gave a low discrimination result (i.e., ≤99.9%) or gave no result.
- Molecular Methods
Sterile fluids (i.e., a minimum of 100 µL) were placed into a sterile 1.5 mL microcentrifuge tube and centrifuged at 18,200 X g for 5 min.: supernatant was removed, and the pellet was extracted thereafter using the procedure outlined below. Tissues were minced manually with sterile scalpels before being placed into a sterile 1.5 mL microcentrifuge tube. DNA was extracted using the QIAmp UCP Pathogen DNA Mini Kit protocol for tissues (QIAGEN, Hilden, Germany). Briefly, the tissue was re-suspended in 100 µL of digestion Buffer ATL and 40 µL of 20 mg/mL Proteinase K solution. The samples were then briefly vortexed and incubated at 56oC in a 10,400 rpm Eppendorf thermomixer for a minimum of 1 h. DNA in the proteolytic digest was further purified according to the manufacturer’s instructions. DNA was eluted in 150 µL of Buffer AVE. DNA eluate was stored in -20oC until use. Broad range BR 16S PCR rRNA PCR was performed using dual priming oligonucleotide (DPO) primers that were purchased from Exiqon (Worburn, MA) and used as previously described [11,22] with Mastermix BR 16S PCR/18S Basic Kit (Molzym, Bremen, Gernany). PCR was set up in a 25 µL reaction volume with 5 µL of template DNA. Standard Fast PCR was performed in an ABI Veriti thermocycler (Thermo Fisher – Life Technologies, Carlsbad, CA) under the thermocycling protocol previously published [11]. A BLAST search against the SmartGene Integrated Database Network System (IDNS) (Lausanne, Switzerland) bacterial database indicated the most closely related species (http://www.Smartgene.com) and the overall identify score compared to a well characterized reference sequence for all isolates was 99.9% with 0-2 mismatches. Pathogenomix Ripseq (https://www.ripseq.com) was used to interpret mixed sequencing results.
2.5. Data Analysis
Data was analyzed according to standard descriptive statistics. The performance of the BR 16S PCR assay was compared to culture results and the patient’s clinical infectious diseases diagnosis to calculate sensitivity, specificity, positive predictive value, negative predictive value and accuracy. Odds ratio and relative risk were also determined for each laboratory and patient parameter used to predict the BR 16S PCR result. A true positive result was defined as one in which at least one clinical specimen culture or PCR sequencing assay was positive in a patient with a clinical diagnosis. A false-positive result was one in which a microorganism was isolated in at least one clinical specimen, but the PCR was negative, and the patient didn’t have a confirmed clinical diagnosis. A true negative culture or PCR was defined as those that occurred for clinical specimens from patients with no signs of infection. A false-negative culture occurred when the PCR or culture was negative in a patient with invasive infection. Indeterminate BR 16S PCR results were approached in two ways in the calculation of diagnostic assay performance; 1) they were excluded, and 2) they were positive results since they are treated like true positive results for clinical management requiring further patient testing and treatment.
3. Results
3.1. Patient Characteristics
A total of 661 individual patients were enrolled. Most were adults (≥14 yrs, 80%) and the rest were children and adolescents ≤14 years of age (Table 1). The overall age was 41.8 ± 7.7 yrs (mean ± SD). For adults, more males (56.4%) were enrolled than females (43.6%) but there was no difference in the ages of these groups. The same was found for pediatrics with males (60%) being enrolled more often than females (40%) but there was no difference in the ages of these groups. Most patients were either initially assessed in the Emergency Department or were hospitalized. Few patients were ambulatory, and none were enrolled from long-term care. Most patients (98.6 %) had been placed on antimicrobial therapy. Overall, the average duration of therapy was 9 d ± 6.4 d. Patients with CVR infections had the highest average duration of antibiotic therapy prior to surgery of 15.4 d. Patients with suspected septic arthritis or osteomyelitis had an average of 1.6 d of antibiotic therapy prior to clinical specimen collection. Most patients with meningitis without EVD insertion had CSF collected in the ED prior to antibiotics being initiated.
3.2. Distribution of Clinical Specimens
Figure 1 shows the overall distribution of clinical specimens. Most clinical specimens were collected for suspected septic monoarticular arthritis (n=245; 35.8%) in the hip (n=62; 25.3%), knee (n=150; 61.2%), shoulder (n=8; 3.3%), ankle (n=16; 4.6%), elbow (n=4;1.6%) or wrist (n=5; 2.0%). A total of 64 cases of prosthetic joint infections were tested including total hip (n=16; 25%), knee (n=39; 61%) or shoulder (n=5; 7.8%) arthroplasty or infected hardware following ORIF for a long bone fracture (n=4; 6.3%). A smaller number of cases were due to suspected spinal infection 49(15.9%) with discitis with or without vertebral osteomyelitis and/or paraspinal abscesses. Cardiovascular infections were the next most common reason for culture-negative invasive infection. A total of 146(92.4%) of these cases were due to infective endocarditis either of native or prosthetic valves (n=132; 90.4%), vascular graft infections 8(5.1%) or infected intracardiac device/lead infections 3(1.9%) and pericarditis 3(1.9%). Meningitis and meningitis/ventriculitis (n=101; 40.1%) due to an implanted external-ventricular drain (CSF-EVD) accounted for (n=21; 20.8%) of these cases. Another 12(17.5%) cases had brain abscesses, cerebritis or brain lesion. Pleuropulmonary infections (n= 44; 6.4%) included empyema, pleural or pulmonary lesions. Only five clinical samples were tested that were blood cultures (n=2, 0.3%) from culture-negative infective endocarditis patients or bone marrow (n=3, 0.4%). Peritonitis (n=11, 0.6%) with culture-negative peritoneal fluid cultures were tested by patients with end-stage renal disease on peritoneal dialysis and those with ascites and spontaneous bacterial infection. Other abscesses and skin and soft tissue infections (SSTIs) were tested from a variety of body sites including liver, breast, limbs, scalp, central venous catheter site, sternum and one case of necrotizing fasciitis.
3.3. Performance of BR 16S PCR Compared to Culture
Table 2outlines the performance of the BR 16S PCR assay compared to the culture of the primary clinical specimen (Table 2A) and other clinically relevant specimens from the same patient (Table 2B). The original specimen was culture negative in 703/761 specimens (92.5%). BR 16S PCR was positive in 35% of culture negative specimens but save for one case, all were true positive results that correlated with the clinical case. Overall, the BR 16S PCR assay had a sensitivity, specificity, positive predictive value, negative predictive value and accuracy for a disease prevalence of 40.69% of 93.9%, 99.77%, 99.64%, 95.97% and 97.38% when all indeterminate molecular assays were excluded (n=30). When indeterminate BR 16S PCR results were considered positive the disease prevalence increased to 43.12% and the assay had a sensitivity, specificity, positive predictive value, negative predictive value and accuracy of 94.48%, 99.77%, 99.68%, 95.97% and 97.49%. In 57 instances, BR 16S PCR was performed despite culture ultimately becoming positive because the original culture results represented a likely contaminant or not a definite pathogen (designated “possible pathogen” in Table 2). BR 16S PCR was positive in only 29% (6/21) of specimens growing a likely contaminant, like the positivity rate in culture negative specimens. In all cases, the organism detected by PCR was distinct from culture. When a possible pathogen was cultured, BR 16S PCR positivity increased to 69% (9/13) and in 5/9 (56%) PCR detected the same organism thus providing additional evidence of its clinical significance. PCR was positive in 22/23 (96%) cases when a definite pathogen was cultured, detecting the same organism in all cases.
In 82.3% of cases where BR 16S PCR was done (Table 2B), other clinically relevant specimens were also culture negative (e.g., other specimens from same/similar body site, blood cultures). Other cultures detected a definite pathogen in 46 cases. BR 16S PCR was positive in 76% of these (36.5%) and detected the same pathogen in all but one (34/35, 97%). When other cultures detected a possible pathogen, BR 16S PCR was positive in only 44% (15/35). Overall, the BR 16S PCR assay had a sensitivity, specificity, positive predictive value, negative predictive value and accuracy for a disease prevalence of 24.24% of 75%, 100%, 100.0%, 92.59% and 93.94% when all indeterminate molecular assays results were excluded (n=217). When indeterminate BR 16S PCR results were considered positive the disease prevalence increased to 47.33% and the assay had a sensitivity, specificity, positive predictive value, negative predictive value and accuracy of 91.1%, 100%, 100%, 92.59% and 95.79%. BR 16S PCR detected the same organism in 8 of these (8/15, 53%), again supporting the organism’s clinical significance. Likely contaminants were cultured from other specimens in 51 cases, but BR 16S PCR was positive in only 13(25%). Organisms detected by PCR in most cases (12/13. 92%) was distinct from that detected by culture. However, in one instance, an organism deemed to be a likely contaminant (single colony of S. epidermidis on one culture plate from a valve tissue culture) was also detected by BR 16S PCR
3.4. Performance of Acceptance Criteria for Prediction of Molecular Assay Result
Table 3, Table 4, Table 5 and Table 6 show the ability of specific Gram stain and patient biomarkers to predict the results of the BR 16S PCR-sequencing assay. Overall, the presence of purulence on Gram stain had a higher sensitivity than the presence of organisms for prediction of a positive BR 16S PCR result (Table 3). However, the overall sensitivity of finding organisms on Gram stain gave the best overall sensitivity for BR 16S PCR assay performance for pathogen detection. An elevated WBC and CRP were the best predictive patient biomarkers. None of the patient biomarkers have a sensitivity >50% for BR 16S PCR positivity. Overall, the Odds ratio (OR) was highest for Gram stain organism positivity (OR=7.7) and lowest for a high patient PMN count (OR=1.97) while other parameters had an OR>2.0<3.0. Relative risk (RR) for all parameters was also highest for Gram stain organism positivity (RR=2.50) while other parameters had RR between 1.5 to 2.0 (Table 3).
Table 5 outlines the specific analysis for only cardiovascular (CVR) cases including culture negative infective endocarditis, pericarditis vascular graft/ICD infections. Both purulence of Gram stain (47.7%) and seeing organisms (22.73%) had low sensitivity for prediction of the BR 16S PCR result while absence of organisms or purulence in the Gram stain was highly specific of the BR 16S PCR being negative. Increased WBC and PMNs were highly predictive (>95%) of a positive BR 16S PCR result. A high PMN and CRP were also good (~80%) at predicting a positive BR 16S PCR result. Overall, the OR was highest for Gram stain organism positivity (OR=10) and a high patient WBC (OR=7.07) while other parameters had an OR>3.0<5.0. RR for all parameters was also highest for the patient having an elevated WBC (RR=3.51) while other parameters had RR between 1.62 to 2.22 (Table 5). Absence of WBC elevation was predictive of negative BR 16S PCR result (NPV 86.2%).
Table 6 outlines the specific analysis for central nervous system (CNS) specimens including cerebrospinal fluids (CSFs) (both direct and EVD specimens) and brain tissues from cases of culture-negative meningitis and/or ventriculitis, cerebritis/brain abscesses. Purulence of Gram stain (96%) was a much better indicator than seeing organisms (56%) for prediction of the BR 16S PCR result while the absence of organisms in the Gram stain was highly specific of a negative BR 16S PCR result. Increased WBC and PMNs were highly predictive (>90%) of the BR 16S PCR result. High PMNs and CRP (>70%) were moderately predictive of a positive BR 16S PCR result. Overall, the OR was highest for Gram stain purulence and organism positivity (OR=26.67 and 47.09 respectively). Elevation of the patient’s WBC and CRP had OR >8<10, with the lowest OR for a high patient PMN count (OR=5.07). RR for all parameters was also highest for purulence on Gram stain (RR=16.40) while other parameters had RR between 3.58 to 7.44 (Table 6). For CSF specimens, the absence of PMNs in the Gram stain was highly predictive of negative BR 16S PCR (NPV 97.6%).
4. Discussion
Our large multiyear regional evaluation of a novel fast broad-range BR 16S PCR rDNA PCR/sequencing assay using DPO primers is the first report of the clinical performance of this unique assay approach in testing hundreds of different culture negative specimens from patients with a wide variety of well characterized invasive infections. Overall, the diagnostic performance of our BR 16S PCR assay has one of the highest sensitivity, specificity, PPV, NPV and accuracy to date. Use of DPO primers also provides a low rate of overall contamination [22]. Use of fast PCR protocols also allows BR 16S PCR assay results to be reported the same day if results are urgently required. Our study confirms and expands on the higher sensitivity of our fast DPO BR 16S PCR assay compared to culture, particularly for endovascular infection [11]. Molecular detection of the pathogen(s) causing invasive infection changed and improved the clinical management of approximately one-third of study patients, particularly those suspected of having septic arthritis, PJIs, infective endocarditis of native/prosthetic valves.
Previous evaluations of users developed broad-range BR 16S PCR assays used standard primers directed to either the V1-3 or V3-4 gene regions with variable assay configurations and results for various clinical specimen types [12,13,14,17,18,19,20,21,22,23]. Overall, the highest concordance rates between culture and a BR 16S PCR occurred in the above studies for heart valve tissues and joint fluids/tissues with a range of reported sensitivities between ~58-85%. Use of a BR 16S PCR test led to a change in clinical management in ~5-10% of patients. However, some studies have shown lower sensitivity for BR 16S PCR followed by Sanger sequencing than synovial fluid culture for diagnosing PJI infections [28]. One large study used BR 16S PCR to analyze 469 PJI specimens and 430 other types of sterile fluids/tissues that had been cultured [24]. Culture was positive for 170 (36.2%) of PJI specimens but only 41.2% of them were positive for a pathogen by BR 16S PCR. Another 13/299 (4.3%) culture-negative PJI specimens were positive by BR 16S PCR. Culture was positive for 52/430 (12.1%) of other types of sterile fluids and tissues, but only 61.5% were positive by BR 16S PCR. Another 31/378(8.2%) of culture-negative samples were positive by BR 16S PCR alone. Another retrospective evaluation used BR 16S PCR to analyze 566 specimens from 460 patients; 17% had a positive molecular assay result and in 5% of these this led to a change in clinical management [25]. Overall, BR 16S PCR/sequencing detected a pathogen in 10% of culture-negative specimens. BR 16S PCR had the highest positivity in cardiovascular specimens (37%) in clinically infected patients while musculoskeletal specimens were more likely to be culture positive (p<0.001) [25]. Several prospective studies have also used standard BR 16S PCR testing to improve pathogen detection in specific types of invasive infections.
Commercially available BR 16S PCR assays have also shown performance variability with a range of reported sensitivities reported (i.e., ~60-95%), albeit the Septifast (Roche) and UDM (Molyzym) assays have different configurations and have only been evaluated in very small numbers of patients [19,29,30]. A large prospective cohort study evaluated a commercial BR 16S PCR/sequencing assay compared to culture for pathogen detection in 1370 clinical specimens (75 heart valves, 151 joint tissue specimens, 230 synovial fluids, 840 whole blood specimens and 66 culture-negative cerebrospinal fluid specimens) [30]. The added value of PCR was shown in 173 of 555 positive specimens (0.126: 0.109-0.144 95%CI), and heart valve tissues and joint tissues had the highest yields. Blood cultures however had a high false-negative rate compared to culture and missed up to 7.1% of positive bloodstream infections [30].
Sterile clinical specimens of sufficient amount and quality should only be accepted for BR 16S PCR or targeted BR 16S PCR metagenomic analysis to expect a quality assured molecular result. The best recovery comes from sterile fluid and tissue specimens that have had minimal prior handling and been stored refrigerated or frozen prior to testing although few clinical studies have focused on optimizing specimen collection and storage processes [31,32,33]. Our laboratory restricts requests for BR 16S PCR testing to Infectious Diseases physicians in consultation with a clinical microbiologist who must approve the order based on the pre-test likelihood of improved BR 16S PCR pathogen detection using Gram stain and patient inflammatory marker assessment. Our study shows that selection of specimens with purulence and/or organisms on Gram stain in patients with clinical signs of infection including elevated inflammatory biomarkers improves the predictive sensitivity of our BR 16S PCR assay across the various types of clinical specimens. Other investigators have also recently shown that a positive Gram stain had a 12X greater odds ratio for yielding a positive molecular result [25].
More recently, next-generation sequencing (NGS) has been added as a diagnostic tool for PJI diagnosis, particularly for pathogen detection in culture negative cases [34]. Because NGS is labour intensive and costly for clinical laboratories [35], targeted metagenomic sequencing based assays (tMGS) for pathogen detection and identification in sterile fluids and tissues have recently been developed that use either Sanger sequencing and/or NGS after BR 16S PCR rRNA gene amplification depending on the individual tests’ cycle threshold (Ct) [35]. Several clinical studies have recently been reported using this method for diagnosis of PJI, and infectious endocarditis (IE), and show similar or improve diagnostic performance compared to culture alone [17,36,37,38,39,40,41,42,43,44]. A retrospective study was done analyzing synovial fluids at a single center that included 154 patients who had synovial fluid aspirated from their hip, knee, shoulder or elbow arthroplasties; 118 patients had noninfectious arthroplasty failure and 36 had PJI [41]. Clinical sensitivity and specificity for diagnosis of PJI were 69% and 100% respectively for the tMGS assay and 72% and 100%, respectively, for culture (P=0.74). The combination of both tests had the highest sensitivity compared to culture alone (P=0.04). Results of the tMGS assay led to changes in therapy in 4/36 (11%) of PJI patients. Another study by the same investigator group used tMGS compared to a commercial shotgun metagenomics assay, the Karius tests, to detect a pathogen in blood and plasma from 34 patients with suspected infectious endocarditis. The Karius test was positive for 24/34(75%), including 3/6(50%) with blood culture negative IE [40], which was not significantly different than the tMGS assay (P=0.41). Use of culture, the Karius test and tMGS found a potential pathogen in 97% of ID cases including 5/6 with negative cultures.
Our study has several important limitations. This study reports the accrued experience of a single centralized laboratory with decades of experience in developing molecular assays. The results reported herein may not reflect the accuracy of the utilization of this technology in jurisdictions without expertise in broad range BR 16S PCR/sequencing testing. Cases were only enrolled at the request of the Infectious Diseases service after consultation with the Microbiologists, but chart reviews were otherwise not done. This approach may have introduced selection bias but ensured that appropriate clinical specimens were selected on patients with culture-negative patients where the molecular assay was predicted to have the highest value-added clinical benefit.
5. Conclusions
Our novel BR 16S PCR assay improved detection for identifying underlying bacterial pathogens in a wide range of culture negative clinical specimens while having a low rate of contamination. Future evaluation should be done of our BR 16S PCR assay against a targeted metagenomics method.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figure S1: Microorganisms detected by BR 16S PCR assay according to type of clinical specimen.
Author Contributions
Conceptualization, Data curation, Methodology, Project administration, Writing – original draft, Writing – review and editing. B Chow: Methodology, Data curation, Writing – original draft, Writing – review and editing. T. Griener: Data analysis, Methodology, Writing – review and editing.
Funding
This study was unsupported.
Institutional Review Board Statement
This study was reviewed and approved by the Conjoint Health Research Ethics Board, University of Calgary and Alberta Health Services (Ethics ID No: REB15-069).
Data Availability Statement
The data that support the findings of this study are available from Alberta Health Services (AHS), Alberta Precision Laboratories (APL) (formerly CLS) but restrictions apply to the availability to these data, which were used under the ethics agreement for the current study and so are not publicly available. Data are, however, available from the author upon reasonable request and with permission of AHS/APL.
Acknowledgments
We thank the Alberta Precision Laboratory – Calgary Zone Microbiology staff for their help with sample processing and isolate analysis.
Conflicts of Interest
None of the authors have a conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| BR 16S PCR | Broad range BR 16S PCR rDNA polymerase chain reaction and Sanger sequencing |
| BR 16S PCR rRNA gene | BR 16S PCR ribosomal ribonucleic acid gene |
| DNA | Deoxyribonucleic acid |
| APL | Alberta precision laboratories |
| DSC | Diagnostic and Scientific centre |
| BA | Blood agar |
| BBA | Brucella blood agar |
| CHOC | Chocolate agar |
| MAC | MacConkey agar |
| MALDI-TOF MS | Matrix assisted laser desorption-time of flight mass spectrometry |
| MSK | Musculoskeletal |
| PJI | Prosthetic joint infection |
| CVR | Cardiovascular |
| CNS | Central nervous system |
| CSF | Cerebrospinal fluid |
| SSTI | Skin and soft tissue infection |
| CRP | C-reactive protein |
| WBC | White blood cell count |
| PMN | Polymorphonuclear |
| PPV | Positive predictive value |
| NPV | Negative prediction value |
| OR | Odds ratio |
| RR | Relative risk |
| tMGS | Targeted metagenomics |
| Ct | Cycle threshold |
References
- Branda, J. A.; Rychert, J.; Burnham, C. A.; Bythrow, M.; Garner, O. B.; Ginocchio, C. C.; Jennemann, R.; Lewinski, M. A.; Manji, R.; Mochon, A. B.; et al. Multicenter validation of the VITEK MS v2.0 MALDI-TOF mass spectrometry system for the identification of fastidious gram-negative bacteria. Diagn Microbiol Infect Dis 2014, 78, 129–131. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Chung, H. S.; Moon, H. W.; Lee, S. H.; Lee, K. Comparative evaluation of two matrix-assisted laser desorption ionization time-of-flight mass spectrometry (MALDI-TOF MS) systems, Vitek MS and Microflex LT, for the identification of Gram-positive cocci routinely isolated in clinical microbiology laboratories. J Microbiol Methods 2015, 113, 13–15. [Google Scholar] [CrossRef] [PubMed]
- Church, D. L.; Griener, T.; Gregson, D. Multi-year comparison of VITEK(R) MS and BR 16S PCR rRNA gene sequencing performance for the identification of rarely encountered anaerobes causing invasive human infections in a large Canadian region: can our laboratory abandon BR 16S PCR rRNA gene sequencing? Anaerobe 2022, 78, 102640. [Google Scholar] [CrossRef]
- Church, D. L.; Griener, T.; Gregson, D. Multi-year comparison of VITEK MS performance for identification of rarely encountered pathogenic Gram-negative organisms (GNOs) in a large integrated Canadian healthcare region. Microbiol Spectr 2024, 12, e0227624. [Google Scholar] [CrossRef]
- Sharma, K.; Angrup, A.; Ghosh, A.; Singh, S.; Sood, A.; Arora, A.; Sharma, M.; Sethi, S.; Rudramurthy, S. M.; Kaur, H.; et al. Evaluation of VITEK MS Version 3.0 MALDI-TOF for the identification of anaerobes, mycobacteria, Nocardia, and moulds. Diagn Microbiol Infect Dis 2024, 110, 116477. [Google Scholar] [CrossRef]
- Church, D.; Griener, T.; Gregson, D. Multi-year comparison of VITEK MS performance for identification of rarely encountered pathogenic gram-positive organisms (GPOs) in a large integrated Canadian healthcare region. Microbiol Spectr 2025, 13, e0254524. [Google Scholar] [CrossRef]
- Stokes, W.; Campbell, L.; Pitout, J.; Conly, J.; Church, D.; Gregson, D. Comparison of Accelerate PhenoTest BC Kit and MALDI-TOF MS/VITEK 2 System for the rapid identification and antimicrobial susceptibility testing of gram-negative bacilli causing bloodstream infections. J Assoc Med Microbiol Infect Dis Can 2020, 5, 145–157. [Google Scholar] [CrossRef]
- Perez, K. K.; Olsen, R. J.; Musick, W. L.; Cernoch, P. L.; Davis, J. R.; Peterson, L. E.; Musser, J. M. Integrating rapid diagnostics and antimicrobial stewardship improves outcomes in patients with antibiotic-resistant Gram-negative bacteremia. J Infect 2014, 69, 216–225. [CrossRef]
- Dalai, A. S.; Monti, E. B.; Mallesho, R.; Obeda, M.; Evans, G. A.; Perez-Patrigeon, S.; Wilson, E.; Martinez-Cajas, J. L.; Sheth, P. M.; Tomalty, L.; et al. Increasing evidence-based care practices for patients with Staphylococcus aureus bacteraemia through required infectious diseases consultation in a tertiary care hospital: a quality improvement initiative. BMJ Open Qual 2025, 14. [Google Scholar] [CrossRef]
- Fournier, P. E.; Thuny, F.; Richet, H.; Lepidi, H.; Casalta, J. P.; Arzouni, J. P.; Maurin, M.; Celard, M.; Mainardi, J. L.; Caus, T.; et al. Comprehensive diagnostic strategy for blood culture-negative endocarditis: a prospective study of 819 new cases. Clin Infect Dis 2010, 51, 131–140. [Google Scholar] [CrossRef]
- Miller, R. J.; Chow, B.; Pillai, D.; Church, D. Development and evaluation of a novel fast broad-range BR 16S PCR ribosomal DNA PCR and sequencing assay for diagnosis of bacterial infective endocarditis: multi-year experience in a large Canadian healthcare zone and a literature review. BMC Infect Dis 2016, 16, 146. [Google Scholar] [CrossRef] [PubMed]
- Muller Premru, M.; Lejko Zupanc, T.; Klokocovnik, T.; Ruzic Sabljic, E.; Cerar, T. Broad-Range BR 16S PCR rDNA PCR on Heart Valves in Infective Endocarditis. J Heart Valve Dis 2016, 25, 221–226. [Google Scholar] [PubMed]
- Kim, M. S.; Chang, J.; Kim, M. N.; Choi, S. H.; Jung, S. H.; Lee, J. W.; Sung, H. Utility of a Direct BR 16S PCR rDNA PCR and Sequencing for Etiological Diagnosis of Infective Endocarditis. Ann Lab Med 2017, 37, 505–510. [Google Scholar] [CrossRef]
- Marin, M.; Garcia-Lechuz, J. M.; Alonso, P.; Villanueva, M.; Alcala, L.; Gimeno, M.; Cercenado, E.; Sanchez-Somolinos, M.; Radice, C.; Bouza, E. Role of universal BR 16S PCR rRNA gene PCR and sequencing in diagnosis of prosthetic joint infection. J Clin Microbiol 2012, 50, 583–589. [Google Scholar] [CrossRef]
- Qu, X.; Zhai, Z.; Wu, C.; Jin, F.; Li, H.; Wang, L.; Liu, G.; Liu, X.; Wang, W.; Li, H.; et al. Preoperative aspiration culture for preoperative diagnosis of infection in total hip or knee arthroplasty. J Clin Microbiol 2013, 51, 3830–3834. [Google Scholar] [CrossRef]
- Godfrey, R.; Curtis, S.; Schilling, W. H.; James, P. R. Blood culture negative endocarditis in the modern era of BR 16S PCR rRNA sequencing. Clin Med (Lond) 2020, 20, 412–416. [Google Scholar] [CrossRef]
- Tan, J.; Liu, Y.; Ehnert, S.; Nussler, A. K.; Yu, Y.; Xu, J.; Chen, T. The Effectiveness of Metagenomic Next-Generation Sequencing in the Diagnosis of Prosthetic Joint Infection: A Systematic Review and Meta-Analysis. Front Cell Infect Microbiol 2022, 12, 875822. [Google Scholar] [CrossRef]
- Peeters, B.; Herijgers, P.; Beuselinck, K.; Verhaegen, J.; Peetermans, W. E.; Herregods, M. C.; Desmet, S.; Lagrou, K. Added diagnostic value and impact on antimicrobial therapy of BR 16S PCR rRNA PCR and amplicon sequencing on resected heart valves in infective endocarditis: a prospective cohort study. Clin Microbiol Infect 2017, 23, 888–e881. [Google Scholar] [CrossRef]
- Borde, J. P.; Hacker, G. A.; Guschl, S.; Serr, A.; Danner, T.; Hubner, J.; Burrack-Lange, S.; Ludke, G.; Helwig, P.; Hauschild, O.; et al. Diagnosis of prosthetic joint infections using UMD-Universal Kit and the automated multiplex-PCR Unyvero i60 ITI((R)) cartridge system: a pilot study. Infection 2015, 43, 551–560. [Google Scholar] [CrossRef]
- Carter, K.; Doern, C.; Jo, C. H.; Copley, L. A. The Clinical Usefulness of Polymerase Chain Reaction as a Supplemental Diagnostic Tool in the Evaluation and the Treatment of Children With Septic Arthritis. J Pediatr Orthop 2016, 36, 167–172. [CrossRef]
- Akram, A.; Maley, M.; Gosbell, I.; Nguyen, T.; Chavada, R. Utility of BR 16S PCR rRNA PCR performed on clinical specimens in patient management. Int J Infect Dis 2017, 57, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Kommedal, O.; Simmon, K.; Karaca, D.; Langeland, N.; Wiker, H. G. Dual priming oligonucleotides for broad-range amplification of the bacterial BR 16S PCR rRNA gene directly from human clinical specimens. J Clin Microbiol 2012, 50, 1289–1294. [Google Scholar] [CrossRef] [PubMed]
- Sebastian, S.; Malhotra, R.; Sreenivas, V.; Kapil, A.; Chaudhry, R.; Dhawan, B. Utility of BR 16S PCR rRNA PCR in the Synovial Fluid for the Diagnosis of Prosthetic Joint Infection. Ann Lab Med 2018, 38, 610–612. [Google Scholar] [CrossRef]
- Reuwer, A. Q.; van den Bijllaardt, W.; Murk, J. L.; Buiting, A. G. M.; Verweij, J. J. Added diagnostic value of broad-range BR 16S PCR on periprosthetic tissue and clinical specimens from other normally sterile body sites. J Appl Microbiol 2019, 126, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Fida, M.; Khalil, S.; Abu Saleh, O.; Challener, D. W.; Sohail, M. R.; Yang, J. N.; Pritt, B. S.; Schuetz, A. N.; Patel, R. Diagnostic Value of BR 16S PCR Ribosomal RNA Gene Polymerase Chain Reaction/Sanger Sequencing in Clinical Practice. Clin Infect Dis 2021, 73, 961–968. [Google Scholar] [CrossRef]
- Rodriguez-Garcia, R.; Rodriguez-Esteban, M. A.; Fernandez-Suarez, J.; Morilla, A.; Garcia-Carus, E.; Telenti, M.; Morales, C.; Albaiceta, G. M.; Fernandez, J. Evaluation of BR 16S PCR rDNA Heart Tissue PCR as a Complement to Blood Cultures for the Routine Etiological Diagnosis of Infective Endocarditis. Diagnostics (Basel) 2021, 11. [Google Scholar] [CrossRef]
- Anton-Vazquez, V.; Dworakowski, R.; Cannata, A.; Amin-Youssef, G.; Gunning, M.; Papachristidis, A.; MacCarthy, P.; Baghai, M.; Deshpande, R.; Khan, H.; et al. BR 16S PCR rDNA PCR for the aetiological diagnosis of culture-negative infective endocarditis. Infection 2022, 50, 243–249. [Google Scholar] [CrossRef]
- Lane, M. A.; Ganeshraj, N.; Gu, A.; Warren, D. K.; Burnham, C. D. Lack of Additional Diagnostic Yield of BR 16S PCR rRNA Gene PCR for Prosthetic Joint Infections. J Appl Lab Med 2019, 4, 224–228. [Google Scholar] [CrossRef]
- Stavnsbjerg, C.; Frimodt-Moller, N.; Moser, C.; Bjarnsholt, T. Comparison of two commercial broad-range PCR and sequencing assays for identification of bacteria in culture-negative clinical samples. BMC Infect Dis 2017, 17, 233. [Google Scholar] [CrossRef]
- Tkadlec, J.; Peckova, M.; Sramkova, L.; Rohn, V.; Jahoda, D.; Raszka, D.; Berousek, J.; Mosna, F.; Vymazal, T.; Kvapil, M.; et al. The use of broad-range bacterial PCR in the diagnosis of infectious diseases: a prospective cohort study. Clin Microbiol Infect 2019, 25, 747–752. [Google Scholar] [CrossRef]
- Velasquez-Mejia, E. P.; de la Cuesta-Zuluaga, J.; Escobar, J. S. Impact of DNA extraction, sample dilution, and reagent contamination on BR 16S PCR rRNA gene sequencing of human feces. Appl Microbiol Biotechnol 2018, 102, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Dyrhovden, R.; Rippin, M.; Ovrebo, K. K.; Nygaard, R. M.; Ulvestad, E.; Kommedal, O. Managing Contamination and Diverse Bacterial Loads in BR 16S PCR rRNA Deep Sequencing of Clinical Samples: Implications of the Law of Small Numbers. mBio 2021, 12, e0059821. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, D.; Rajan, D.; Bellis, K. L.; Betteridge, E.; Brennan, J.; de Sousa, C.; Carriage Study, T.; Parkhill, J.; Peacock, S. J.; de Goffau, M. C.; et al. Optimization of high-throughput BR 16S PCR rRNA gene amplicon sequencing: an assessment of PCR pooling, mastermix use and contamination. Microb Genom 2023, 9. [Google Scholar] [CrossRef]
- Parvizi, J.; Tan, T.L.; Goaswami, K.; Higuera, C.; Della Valle, C.; Chen, A.F.; Shohat, N. The 2018 defintion of periprstheitic hip and knee infection: an evidence-based and validated criteria. J Arthro, 1016. [Google Scholar]
- Boers, S. A.; Jansen, R.; Hays, J. P. Understanding and overcoming the pitfalls and biases of next-generation sequencing (NGS) methods for use in the routine clinical microbiological diagnostic laboratory. Eur J Clin Microbiol Infect Dis 2019, 38, 1059–1070. [CrossRef]
- Wang, C. X.; Huang, Z.; Fang, X.; Li, W.; Yang, B.; Zhang, W. Comparison of broad-range polymerase chain reaction and metagenomic next-generation sequencing for the diagnosis of prosthetic joint infection. Int J Infect Dis 2020, 95, 8–12. [Google Scholar] [CrossRef]
- Fida, M.; Wolf, M. J.; Hamdi, A.; Vijayvargiya, P.; Esquer Garrigos, Z.; Khalil, S.; Greenwood-Quaintance, K. E.; Thoendel, M. J.; Patel, R. Detection of Pathogenic Bacteria From Septic Patients Using BR 16S PCR Ribosomal RNA Gene-Targeted Metagenomic Sequencing. Clin Infect Dis 2021, 73, 1165–1172. [Google Scholar] [CrossRef]
- Mishra, D.; Satpathy, G.; Chawla, R.; Paliwal, D.; Panda, S. K. Targeted metagenomics using next generation sequencing in laboratory diagnosis of culture negative endophthalmitis. Heliyon 2021, 7, e06780. [CrossRef]
- Flurin, L.; Wolf, M. J.; Mutchler, M. M.; Daniels, M. L.; Wengenack, N. L.; Patel, R. Targeted Metagenomic Sequencing-based Approach Applied to 2146 Tissue and Body Fluid Samples in Routine Clinical Practice. Clin Infect Dis 2022, 75, 1800–1808. [Google Scholar] [CrossRef]
- Flurin, L.; Fisher, C. R.; Wolf, M. J.; Pritt, B. S.; DeSimone, D. C.; Patel, R. Comparison of Blood-Based Shotgun and Targeted Metagenomic Sequencing for Microbiological Diagnosis of Infective Endocarditis. Open Forum Infect Dis 2023, 10, ofad546. [Google Scholar] [CrossRef]
- Flurin, L.; Wolf, M. J.; Greenwood-Quaintance, K. E.; Sanchez-Sotelo, J.; Patel, R. Targeted next generation sequencing for elbow periprosthetic joint infection diagnosis. Diagn Microbiol Infect Dis 2021, 101, 115448. [Google Scholar] [CrossRef]
- Hong, H. L.; Flurin, L.; Thoendel, M. J.; Wolf, M. J.; Abdel, M. P.; Greenwood-Quaintance, K. E.; Patel, R. Targeted Versus Shotgun Metagenomic Sequencing-based Detection of Microorganisms in Sonicate Fluid for Periprosthetic Joint Infection Diagnosis. Clin Infect Dis 2023, 76, e1456–e1462. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Wang, S.; Dong, G.; Niu, Y. Diagnostic Performance of Metagenomic Next rectangleGeneration Sequencing in the Diagnosis of Prosthetic Joint Infection Using Tissue Specimens. Infect Drug Resist 2023, 16, 1193–1201. [Google Scholar] [CrossRef] [PubMed]
- Mahnic, A.; Rak, M.; Trebse, R.; Rupnik, M.; Cor, A. Identification of prosthetic joint infections with BR 16S PCR amplicon metagenomic sequencing - comparison with standard cultivation approach. Diagn Microbiol Infect Dis 2024, 109, 116188. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Distribution of Clinical Specimens According to Primary Site of Infectiona. aDefinitions: 1) Skin and soft tissue infections (SSTIs), 2) musculoskeletal (MSK), 3) cardiovascular (CVR), 4) cerebrospinal fluid-external ventricular drain (CSF-EVD), 5) Cerebrospinal fluid (CSF).
Figure 1.
Distribution of Clinical Specimens According to Primary Site of Infectiona. aDefinitions: 1) Skin and soft tissue infections (SSTIs), 2) musculoskeletal (MSK), 3) cardiovascular (CVR), 4) cerebrospinal fluid-external ventricular drain (CSF-EVD), 5) Cerebrospinal fluid (CSF).
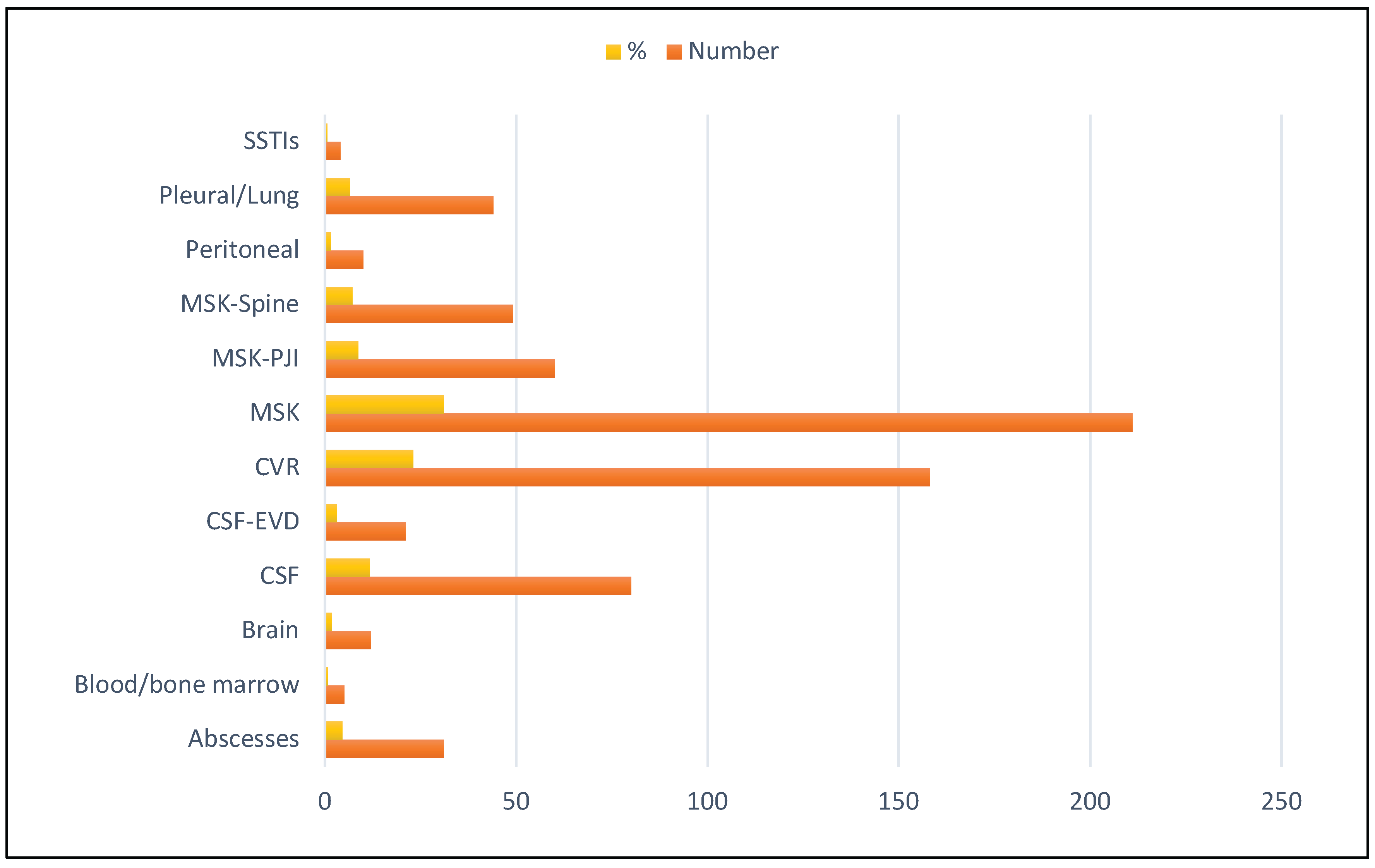

Table 1.
Characteristics of Patient Population.
| Parameter | Characteristic | N (%) ± SD |
|---|---|---|
| Number of subjects | 662 | |
| Age, years (mean ± SD) | 41.8 ± 7.7 | |
| Adults (≥14 yrs) | 532 (80.4); 56.95 ± 10.8 |
|
| Male; Age, years (mean ± 2SD) | 300 (56.4); 56.5 ± 6.6 | |
| Female; Age, years (mean ± 2SD) | 232 (43.6); 57.6 ± 4.5 | |
| Pediatrics (≤14 yrs) | 130 (19.6); 6.3 ± 9.6 | |
| Male; Age, years (mean ± 2SD) | 78 (60.0); 6.7 ± 7.4 |
|
| Female; Age, years (mean ± 2SD) | 52 (40.0); 6.6 ± 9.9 | |
| Location | Hospitalized or ED | 589 (89) |
| Ambulatory | 33 (11) | |
| Prior antibiotic therapy | 652(98.6) | |
| Therapy prior to specimen collection | 9 d ± 6.4 d |
Table 2.
A Comparison of culture and BR 16S PCR assay results for primary clinical specimens.
| Original Culture Result | BR 16S PCR Negative | BR 16S PCR Indeterminate | BR 16S PCR Positive | BR 16S PCR Positive – Same Organism as Culture | BR 16S PCR Positive – Different Organism as Culture |
|---|---|---|---|---|---|
| Pathogen | 1 (4%) | 0 (0%) | 22 (96%) | 22 (100%) | 0 (0%) |
| Possible Pathogen | 3 (23%) | 1 (8%) | 9 (69%) | 5 (56%) | 4 (44%)a |
| Likely Contaminant | 14 (67%) | 1 | 6 (29%) | 0 (0%) | 6 (100%)b |
| Negative | 429 (61%) | 29 (4%) | 245 (35%) | NA | NA |
aIn these 4 cases, BR 16S PCR detected organisms that were possible pathogens based on the clinical context. Organisms were distinct from those detected by culture. bIn all 6 cases, BR 16S PCR detected organisms that were clear pathogens in the clinical context.
Table 2.
B Comparison of culture and BR 16S PCR assay for other clinically relevant specimens.
| Other Relevant Culture Result | BR 16S PCR Negative | BR 16S PCR Indeterminate | BR 16S PCR Positive | BR 16S PCR Positive – Same Organism as Culture | BR 16S PCR Positive – Different Organism as Culture |
|---|---|---|---|---|---|
| Pathogen | 11 (24%) | 0 (%) | 35 (76%) | 34 (97%) | 1 (3%)a |
| Possible Pathogen | 19 (56%) | 1 (3%) | 15 (44%) | 8 (53%) | 7 (47%)b |
| Likely Contaminant | 38 (75%) | 0 (0%) | 13 (25%) | 1 (8%) | 12 (92%)c |
| Negative | 375 (63%) | 216 (37%) | 29 (5%) | NA | NA |
aIn this one case BR 16S PCR detected an organism that was a likely contaminant/non-pathogen. b In these 7 cases, BR 16S PCR detected 4 clear pathogens and 3 possible pathogens based on clinical context. c In these 12 cases, BR 16S PCR detected 10 clear pathogens, one possible pathogen and one likely contaminant, based on the clinical context.
Table 3.
Prediction of BR 16S PCR assay to detect pathogen(s) in clinical specimens according to Gram stain and patient inflammatory markers.
Table 3.
Prediction of BR 16S PCR assay to detect pathogen(s) in clinical specimens according to Gram stain and patient inflammatory markers.
| Bone and Joint Specimens (N=309) |
Gram PMN (N=309, 23.0%) |
Gram Organism (N=309, 23.0%) |
WBC >9.0 X 109/L (N=274, 23.7%) |
Neutrophils HIGH (N=166, 28.9%) |
CRP>50 mg/L (N=249, 25.3%) |
|---|---|---|---|---|---|
|
TRUE POSITIVE (Parameter Predicts positive/BR 16S PCR positive) |
55 | 5 | 42 | 12 | 38 |
|
FALSE POSITIVE (Parameter Predicts positive/BR 16S PCR negative) |
128 | 13 | 131 | 45 | 103 |
|
FALSE NEGATIVE (Parameter Predicts Negative/BR 16S PCR positive) |
16 | 66 | 23 | 36 | 25 |
|
TRUE NEGATIVE (Parameter Predicts negative/BR 16S PCR negative) |
110 | 225 | 78 | 73 | 83 |
| BR 16S PCR Assay Performance | |||||
| Sensitivity (correct prediction of positive) | 77.5% (95% CI 66.0% - 86.5%) |
7.0% (95% CI:2.3% - 15.7%) |
64.6% (95% CI:51.8% - 76.1%) |
25.0% (95% CI:13.6\% - 39.6%) |
60.3% (95% CI:47.2% - 72.4%) |
| Specificity (correct prediction of negative) | 46.2% (95% CI:39.8% - 52.8%) |
94.5% (95% CI:90.8% - 97.1%) |
37.3% (95% CI:30.8% - 44.4%) |
61.9% (95% CI:52.5 - 70.65%) |
45.0% (95% CI:37.4% - 52.1%) |
| Positive Predictive Value | 30.1% (95% CI:26.6% - 33.8%) |
27.8% (95% CI:12.4% - 51.0%) |
24.3% (95% CI:20.7% - 28.3%) |
21.1% (95% CI:13.4% -31.4%) |
27.0% (95% CI:22.5% -31.9%) |
| Negative Predictive Value | 87.3% (95% CI:81.4% - 91.5%) |
77.3% (95% CI:76.1% - 78.5%) |
77.2% (95% CI:70.0% - 83.1%) |
67.0% (95% CI:62.0% _ 71.6%) |
76.9% (95% CI:70.2% - 82.4%) |
| Accuracy | 53.4% (95% CI:47.7% - 59.1%) |
74.4% (95% CI 69.1% - 79.2%) |
43.0% (95% CI:37.8% - 49.9%) |
51.2% (95% CI: 43.3% - 59.0%) |
48.6% (95% CI:42.2% - 55.0%) |
| Odds Ratio | 2.95 | 1.31 | 1.09 | 0.54 | 1.22 |
| Relative Risk | 2.37 | 1.22 | 1.07 | 0.64 | 1.16 |
Table 4.
Prediction of BR 16S PCR Assay to detect pathogen(s) in musculoskeletal (MSK) specimens according to Gram stain and patient inflammatory markers.
Table 4.
Prediction of BR 16S PCR Assay to detect pathogen(s) in musculoskeletal (MSK) specimens according to Gram stain and patient inflammatory markers.
| Bone and Joint Specimens (N=309) |
Gram PMN (N=309, 23.0%) |
Gram Organism (N=309, 23.0%) |
WBC >9.0 X 109/L (N=274, 23.7%) |
Neutrophils HIGH (N=166, 28.9%) |
CRP>50 mg/L (N=249, 25.3%) |
|---|---|---|---|---|---|
|
TRUE POSITIVE (Parameter Predicts positive/BR 16S PCR positive) |
55 | 5 | 42 | 12 | 38 |
|
FALSE POSITIVE (Parameter Predicts positive/BR 16S PCR negative) |
128 | 13 | 131 | 45 | 103 |
|
FALSE NEGATIVE (Parameter Predicts Negative/BR 16S PCR positive) |
16 | 66 | 23 | 36 | 25 |
|
TRUE NEGATIVE (Parameter Predicts negative/BR 16S PCR negative) |
110 | 225 | 78 | 73 | 83 |
| BR 16S PCR Assay Performance | |||||
| Sensitivity (correct prediction of positive) | 77.5% (95% CI 66.0% - 86.5%) |
7.0% (95% CI:2.3% - 15.7%) |
64.6% (95% CI:51.8% - 76.1%) |
25.0% (95% CI:13.6\% - 39.6%) |
60.3% (95% CI:47.2% - 72.4%) |
| Specificity (correct prediction of negative) | 46.2% (95% CI:39.8% - 52.8%) |
94.5% (95% CI:90.8% - 97.1%) |
37.3% (95% CI:30.8% - 44.4%) |
61.9% (95% CI:52.5 - 70.65%) |
45.0% (95% CI:37.4% - 52.1%) |
| Positive Predictive Value | 30.1% (95% CI:26.6% - 33.8%) |
27.8% (95% CI:12.4% - 51.0%) |
24.3% (95% CI:20.7% - 28.3%) |
21.1% (95% CI:13.4% -31.4%) |
27.0% (95% CI:22.5% -31.9%) |
| Negative Predictive Value | 87.3% (95% CI:81.4% - 91.5%) |
77.3% (95% CI:76.1% - 78.5%) |
77.2% (95% CI:70.0% - 83.1%) |
67.0% (95% CI:62.0% _ 71.6%) |
76.9% (95% CI:70.2% - 82.4%) |
| Accuracy | 53.4% (95% CI:47.7% - 59.1%) |
74.4% (95% CI 69.1% - 79.2%) |
43.0% (95% CI:37.8% - 49.9%) |
51.2% (95% CI: 43.3% - 59.0%) |
48.6% (95% CI:42.2% - 55.0%) |
| Odds Ratio | 2.95 | 1.31 | 1.09 | 0.54 | 1.22 |
| Relative Risk | 2.37 | 1.22 | 1.07 | 0.64 | 1.16 |
Table 5.
Prediction of BR 16S PCR Assay to detect pathogen(s) in cardiovascular (CVR) specimens according to Gram stain and patient inflammatory markers.
Table 5.
Prediction of BR 16S PCR Assay to detect pathogen(s) in cardiovascular (CVR) specimens according to Gram stain and patient inflammatory markers.
|
CVR Specimens (N=158) |
Gram PMN (N=158, 55.7%) |
Gram Organism (N=158, 55.7%) |
WBC >9.0 X 109/L (N=148, 56.1%) |
Neutrophils HIGH (N=59, 54.2%) |
CRP >50 mg/L (N=47, 68.1%) |
|
TRUE POSITIVE (Parameter Predicts positive/BR 16S PCR positive) |
42 | 20 | 82 | 26 | 26 |
|
FALSE POSITIVE (Parameter Predicts positive/BR 16S PCR negative) |
15 | 2 | 58 | 13 | 8 |
|
FALSE NEGATIVE (Parameter Predicts Negative/BR 16S PCR positive) |
46 | 68 | 1 | 6 | 6 |
|
TRUE NEGATIVE (Parameter Predicts negative/BR 16S PCR negative) |
55 | 68 | 5 | 14 | 7 |
| BR 16S PCR Assay Performance | |||||
|
Sensitivity (correct prediction of positive) |
47.7% (95% CI:37.0% - 58.7%) |
22.7% (95% CI:14.5% - 32.9%) |
98.8% (95% CI:93.5% - 99.9%) |
81.3% (95% CI:63.6% - 92.8%) |
81.3% (95% CI:63.6% - 92.8%) |
|
Specificity (correct prediction of negative) |
78.6% (95% CI:67.1% - 87.5%) |
97.1% (95% CI:90.1% - 99.7%) |
7.9% (95% CI:2.6% - 17.6%) |
51.9% (95% CI:32.9% - 71.3%) |
46.7% (95% CI:21.3% - 73.4%) |
| Positive Predictive Value | 73.7% (95% CI:63.0% - 82.2%) |
90.9% (95% CI:70.8% - 97.6%) |
58.6% (95% CI:56.7% - 60.4%) |
66.7% (95% CI:56.6% - 75.4%) |
76.5% (95% CI:66.3% - 84.3%) |
| Negative Predictive Value | 54.5% (95% CI:48.6% - 60.2%) |
50.0% (95% CI:47.0% - 53.0%) |
83.3% (95% CI:37.5% - 97.7%) |
70.0% (95% CI:60.0% - 84.0%)% |
53.9% (95% CI:32,1% - 74.2%) |
| Accuracy | 61.4% (95% CI:53.3% - 69.0%) |
55.7% (95% CI:47.6% - 63.6%) |
59.6% (95% CI:51.2% - 67.6%) |
67.8% (95% CI:54.4% - 79.4%) |
70.2% (95% CI:55.1% - 82.7%) |
Table 6.
Prediction of BR 16S PCR assay to detect pathogen(s) in cerebrospinal fluid (CSF) specimens according to Gram stain and patient inflammatory markers.
Table 6.
Prediction of BR 16S PCR assay to detect pathogen(s) in cerebrospinal fluid (CSF) specimens according to Gram stain and patient inflammatory markers.
| CSF Specimens (n=101) | Gram PMN (N=101, 24.8%) |
Gram Organism (N=101, 24.8%) |
WBC >9.0 X 109/L (N=95, 24.2%) |
Neutrophils HIGH (N=69, 21.7%) |
CRP >50 mg/L (N=66, 22.7%) |
|---|---|---|---|---|---|
|
TRUE POSITIVE (Parameter Predicts positive/BR 16S PCR positive) |
24 | 14 | 22 | 11 | 11 |
|
FALSE POSITIVE (Parameter Predicts positive/BR 16S PCR negative) |
36 | 2 | 49 | 19 | 13 |
|
FALSE NEGATIVE (Parameter Predicts Negative/BR 16S PCR positive) |
1 | 11 | 1 | 4 | 4 |
|
TRUE NEGATIVE (Parameter Predicts negative/BR 16S PCR negative) |
40 | 74 | 23 | 35 | 38 |
| BR 16S PCR Assay Performance | |||||
| Sensitivity (correct prediction of positive) | 96% (95% CI: 79.7% - 99.9%) |
56% (95% CI:34.9% - 75.6%) |
95.7% (95% CI: 78.1% - 99.9%) |
73.3% (95% CI:44.9% - 92.2%) |
73.3% (95% CI:44.9% - 92.2%) |
| Specificity (correct prediction of negative) | 52.6% (95% CI:40.8% - 64.2%) |
97.4% (95% CI: 90.8% - 99.7%) |
31.9% (95% CI: 21.4% - 44.0%) |
64.8% (95% CI:50.6% - 77.3%) |
74.5% (95% CI: 60.4% - 85.7%) |
| Positive Predictive Value | 40.0% (95% CI: 34.2% - 46.1%) |
87.5% (95% CI:63.1% - 96.6%) |
31.0% (95% CI:27.3% - 35.0%) |
36.7% (95% CI: 26.5% - 48.2%) |
45.8% (95% CI:32.6% - 59.7%) |
| Negative Predictive Value | 97.6% (95% CI:85.3% - 99.6%) |
87.1% (95% CI: 81.2% - 91.3%) |
95.8% (95% CI:76.7% - 99.4%) |
89.7% (95% CI:78.7% - 95.4%) |
90.5% (95% CI: 80.2% - 95.7%) |
| Accuracy | 63.4% (95% CI:53.2% - 72.7%) |
87.1% (95% CI:79.0% - 93.0%) |
47.4% (95% CI:37.0% - 57.9%) |
66.7% (95% CI: 54.3% - 77.6%) |
74.2% (95% CI:62.0% - 84.2%) |
| Odds Ratio | 26.67 | 47.09 | 10.33 | 5.07 | 8.04 |
| Relative Risk | 16.40 | 6.76 | 7.44 | 3.58 | 4.81 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



