
Submitted:
27 March 2025
Posted:
31 March 2025
You are already at the latest version
Abstract
Background: Sterile body fluids (SBF) are fluids that, under typical human body conditions, do not contain any microorganisms, which are important in transporting nutrients as well as waste products, regulating body temperature, and assessing the respiration process. The SBF infections are a serious and urgent condition that requires immediate treatment because untreated infections at SBF sites can lead to severe, potentially life-threatening infection throughout the body.
Objective: This study is designed and aimed to assess the bacterial profile of sterile body fluid (SBF) infection and their antibiotic susceptibility patterns from patients attending at Minilik II Comprehensive Specialized Hospital and Yekatit 12 Hospital Medical College, Addis Ababa.
Method: A hospital-based cross-sectional study was conducted from February 2024 to June 2024 at Minilik II Comprehensive Specialized Hospital and Yekatit 12 Hospital Medical College in Addis Ababa. A total of 186 study participants were recruited using convenient sampling techniques. Any consenting patients submitting SBF specimens (CSF, pleural, synovial and ascetic fluid) for testing at clinical laboratory were included and analyzed using conventional culture methods and biochemical tests. The antimicrobial susceptibility test (AST) was determined using the disk diffusion method and interpreted as per Clinical Laboratory Standard Institute (CLSI) guidelines. Data was entered into IBM SPSS version 27.0 and analyzed. Bivariate logistic regression analysis was used.
Result: A total of 186 SBF, including CSF, pleural, synovial, and ascetic fluid. Pleural and CSF fluids, respectively, were the most dominant samples in the study. This study revealed a 9.1% (17/186) prevalence of bacterial SBF infection. From the overall 17 isolated bacteria, 70.6 % (12/17) were gram-negative bacteria. From the isolated bacteria, K. pneumoniae and E.coli were the frequently isolated bacteria. The highest bacteria isolates were found in < 10-year-old participants and CSF samples. In the present study, from the isolated bacteria, 70.6 % (12/17) showed MDR pattern for the antibiotic drugs tested.
Conclusion: The prevalence of bacterial isolates in this study from SBF was remarkable, and Klebsiella pneumonae was found as the most dominant etiologic agent for SBF infection. Higher resistance of bacteria for 3rd-generation cephalosporin was recorded. Culture and AST practice with continuous surveillance should be an integral part of the laboratory investigation for better outcome and management of patients’ national concerns.
Keywords:
Sterile body fluids
; bacterial profile
; MDR
; Addis Ababa
; Ethiopia
Introduction
Sterile body fluids (SBF) are fluids that, under typical human body conditions, do not contain any microorganisms. The purpose of these fluids is to reduce inter-organ friction by bathing the organs and membranes. According to human physiology, these bodily fluids play a crucial role in the transportation of waste materials and nutrients, the regulation of body temperature, and the evaluation of the respiratory process. Our bodies include a variety of bodily fluids, including blood, pericardial, synovial, pleural, peritoneal, and cerebrospinal fluid (CSF). These fluids are usually free of microorganism’s including bacteria. Critical phenomena can occur when germs infiltrate sterile bodily areas and cause severe invasive illnesses. Fluids may build up in any bodily cavity as a result of infection and are linked to invasive disorders like sepsis, bacterial meningitis, bacterial peritonitis, bacteremia, and other complications. Infections of the SBF, when occurs typically have greater clinical urgency and these infections could be life threatening [1,2,3].
Low inoculum of pathogenic bacteria and early administration of empirical antibiotics there were fewer chances of retrieving positive cultures The morbidity and ability to cause life threatening infections has categorized the cases as a medical emergency that demands early diagnosis and suitable treatment thereby, it will assist the clinician to start more targeted treatment earlier and shortens the patients' hospital stays [4,5].
The SBF infections can have a variety of conditions, such as burn injuries, trauma, and surgery could expose the typically sterile areas to infectious angent. Infection of each sterile site or SBF is separately defined and may describe the anatomical site, organ involved, etiology, clinical parameters/presentation and pathophysiology such as bacteremia, sepsis, bacterial meningitis and bacterial peritonitis [6].
Globally, infections brought on by resistant pathogens continue to be a major source of serious infections, with rising rates of morbidity and mortality. SBF infections caused by antimicrobial-resistant (AMR) bacteria can even be more dangerous and lead to longer hospital stays, higher medical costs, and increased mortality [3].
AMR and bacterial infections are major public health issues in poor countries. Understanding the local antimicrobial sensitivity pattern and the causing bacteria is crucial for empirical treatment.. Moreover, for better management of patients and framing the antibiotic policy, the knowledge of likely prevalent strains along with their AMR pattern is essential [4].
The pathologic and noticeable accumulation of fluid in the peritoneal cavity is referred to as "ascites" or peritoneal effusions. Ascites is the most common complication of cirrhosis and 60% of patients with cirrhosis develop ascites within 10 years during the course of their disease. The pathophysiology of spontaneous bacterial peritonitis (SBP) is thought to be the movement of bacteria across the intestinal-mucosal barrier from the intestinal lumen to mesenteric lymph nodes or other extra-intestinal locations. Likely, the CSF, which is created by ultra-filtration or secretion, travels through the ventricles and the spinal cord, providing brain cells with nourishment and acting as a cushion. A severe headache, fever, muscle rigidity, seizures, elevated intracranial pressure and stroke are all signs of meningitis, an inflammation of the meninges that line the central nervous system (CNS). Bacterial meningitis is a medical emergency that require urgent rational antibiotics therapy. An estimated 200,000 deaths occur worldwide each year, with mortality that rates ranging from 16% to 32% in underdeveloped nations, particularly Sub-Saharan Africa. Similarly, synovial fluid is a viscous substance that lubricates the joints and many bacteria which are responsible for the occurrence of arthritis due to presence of bacterial cell wall fragments and the bacterial DNA as indicated from experiments. Numerous microbes could be implicated for causing of arthritis, including S. aureus, S. epidermidis, S. pyogenes and N. gonorrhoeae. Pleural effusions are caused by an excessive buildup of fluid in the pleural space. The fluid appearance possibly can be clear, straw-colored, odorless and non-viscous fluids [2,4,7].
In Ethiopia context, scarcity of data about the bacterial profile and AMR of bacteria causing infection of various body fluids is obstacle for the health service. Data on AST of the organisms isolated from SBF over a period of time can be used to create a local SBF infections antibiogram. Knowledge on common causative organisms in various sterile body sites and their antimicrobial susceptibility pattern can help in starting appropriate empirical antibiotics [8,9].
Methodology
- Study Area
The study was conducted at Minilik II Comprehensive Specialized Hospital and Yekatit 12 Hospital Medical College, which are located in the capital city of Ethiopia, Addis Ababa. The hospitals provide service for wide scale of population from the city and for those who are from all corner regions with diverse socio-demographic background resident society.
Minilik II Comprehensive Specialized Hospital has various professionals that included more than 85 sub specialized and medical physicians, 203 nurses, 123 other health professionals, and 250 administrative staff, making nearly 700 staffs.
Yekatit 12 Hospital Medical College was build and starts to serve for the last 100 years which makes the hospital one of the few oldest institutes in Ethiopia. It is supposed to serve more than 5 million patients who are from the city and away from the catchment area. It has six major departments. In the hospital estimated 200 to 250 patients are being served per day through six units of the OPD.
- Study Designs and Period
A hospital based cross-sectional study was conducted from February to June, 2024.
- Population
- Source Population
All patients who were attended Minilik II Comprehensive Specialized Hospital and Yekatit 12 Medical College Hospital.
- Study Populations
All patients who were attended Minilik II Comprehensive Specialized Hospital and Yekatit 12 Medical College Hospital for diagnosis of SBF infection and ordered SBF analysis for microbiology laboratory study during the study period.
- Inclusion and Exclusion Criteria
- Inclusion Criteria
All suspected patients for bacterial SBF infection that were cooperative to provide the clinical specimen and other required information.
- Exclusion Criteria
Patients who were on antibiotic treatment in the last two weeks prior to the data collection period and those patients who had follow up at the same time at Minilik II Comprehensive Specialized Hospital and Yekatit 12 Hospital Medical College during the study period.
- Sample Size Determination and Sampling Techniques
The sample size was calculated based on single population proportion formula as described below.
The value of p is taken as 14.1% (0.14) referring from a study conducted at Tikur Anbessa Specialized hospital [2].
n= Z2 P (1− P)
d²
Where, n = sample size,
Z = Z-score, confidence interval (95% confidence interval, 1.96) P = 0.141 (Prevalence from previous study)
P = expected prevalence or proportion (P = 0.5)
d = precision (d = 0.05) and
(1.96)² X 0.141(1-0.14) =185.011~186
0.05²
Therefore, a total of 186 study participants were recruited using convenient sampling technique with equal proportion of participants from Minilik II Comprehensive Specialized Hospital and Yekatit 12 Hospital Medical College.
- Study Variables
- Dependent Variable
- Prevalence of bacterial pathogens.
- Antibiotic susceptibility patterns.
- Independent Variable
Socio-demographic characteristics such as, age, gender, residence, educational background, occupational status, marital status, monthly income, and clinical related data such as, specimen type, previous SBF infection history, ward unit, other known medical disease, and appearance of specimen.
- Data Collection and Laboratory Methods
- Data Collection
Clinical and socio-demographic data were collected by assigned nurses at the study site hospital using a pretested structured questionnaire. The pretest was done at Kebena Health Centre, Arada Kifle Ketema, Addis Abeba.
All specimens, such as pleural fluid, peritoneal fluid, CSF, synovial, and pericardial fluids were collected and transported to the microbiology laboratory and processed within two (02), hours of collection. Simple and précised checklist was designed to collect participant’s information like participants code number, age, sex, date, medical record number, inpatient, and outpatient.
- Specimens Collection and Transport
Following a signed agreement, a doctor used a needle and syringe to collect samples aseptically. After being collected, the samples were sent to a lab for gram staining, culture, and WBC count. Every collected fluid's physical characteristics including whether it is clear, bloody or traumatized, turbid, or straw-like was recorded.
- Culture and Bacteria Identification
- Microbiological Investigation
Microbiology analysis was performed at Yekatit 12 Hospital Medical College laboratory, microbiology department for the isolation and determination of bacteria. The collected specimens were prepared in accordance with established procedures for gram staining, culture and biochemical testing followed to inoculating on blood agar, chocolate agar and MacConkey agar plates. Inoculated medium were aerobically incubated for 24 to 72 hours at 35 to 37°C. In order to create a microareophilic state for picky bacteria, the chocolate agar plates were specially incubated in a candle jar with a CO2 concentration of 5–10%.
Plates were investigated for the growth of bacterial colonies and those which had culture growths were taken for gram stain and biochemical tests based on the standards of the laboratory procedures. Identification of isolates was applied based on standard bacteriological techniques, such as colony morphology, gram staining and biochemical test.
Biochemical characteristics of gram-positive bacteria were determined by carrying out catalase test, coagulase test, optochin sensitivity test, bacitracin sensitivity test, mannitol test, and hemolytic activity on blood agar. While indole production test, citrate utilization test, kliger’s iron test, urease test, oxidase test, lysine decarboxylase (LDC) test, methyl red/voges proskauer (MR/VP) test, motility test, and hydrogen sulfide gas production test were carried out for the identification of gram-negative bacteria.
- Drug Susceptibility Testing
Susceptibility of bacterial isolate to antimicrobial agents of different classes were assessed by the Kirby-Bauer disk diffusion method in compliance with a commercially prepared antibiotic discs of known concentration on Mueller–Hinton agar(MHA) standard media per Clinical Laboratory Standard Institute (CLSI) guidelines [10].
The MHA were applied with inoculums prepared with 0.5 McFarland turbidity standard following antimicrobial discs were applied on to the plate. Antimicrobial discs such as: Amikacin (30 ug Oxoid),Ceftazidime (30ug Oxoid), Ceftriaxone (30ug BD), Gentamycin (10ug Oxoid), TMP-SXT (1.25+23.75ug BD), Clindamycin(2μg BD), cefoxitin (10 ug BD), Erythromycin (15ug Oxoid), Ciprofloxacillin (5ug BD), Vancomycin (30ug BD), and amoxa-clavulanic acid (10ug Oxoid) were used.
- Quality Control
The QC was performed to check the quality of the medium. Each new lot of stock reagents which were used for preparation of media was passed through quality control panel before used by testing with known standard strains. To observe the potency of performance of reagents, methods and techniques, QC was applied on staining reagents with known organisms.
Standard Operating Procedures (SOPs) were strictly applied, and verified if the media met an expiration date and quality control parameters per CLSI. Data collectors were trained before the data collection procedure and 5% of total prepared questionnaires were pre-tested before the data collection.
The Quality control of culture medias was assured by concurrent testing with the American Type Culture Collection (ATCC) strains including E. coli (ATCC 25922), P. aeruginosa (ATCC 27852), and S. aureus (ATCC 25923). Also visual inspections of cracks in media or plastic petri-dishes, unequal fill, hemolysis, evidence of freezing, bubbles, and contamination were performed.
- Data Management and Analysis
The data entry was performed by EPI INFO version 3.1 statistics software and the entered data was double-checked before the analysis. The descriptive statistics (means, percentages or frequency) and the bi-variant logistic regression analysis were performed. The final results are presented in different forms of descriptive charts, graphs and tables.
- Dissemination of Results
Laboratory results were reported for respective physician/nurses using a cell phone and written report for better patient management. The findings of the study were re-reported to the hospital`s research director office. The study abstract submitted to Addis Ababa health bureau in order to use the findings as a baseline for further related studies and build general conceptual understanding about the issue also, to assist the responsible bodies to practice and thereby maximize the benefits of the patients and health services. The final report is submitted and presented to Wollo University, Department of Medical Laboratory Science.
- Ethical Clearance
The study was approved by the Department of Medical Laboratory Science, Wollo University. The proposal document was re-evaluated and represented to the Addis Ababa Health Bureau research directorate office and acknowledged the topic to accomplish the study at Minilik II Comprehensive Specialized Hospital and Yekatit 12 Hospital Medical College. The final permission letter was received from the hospital research and social service office with letter of assistance to the researcher after presentation and explanation of the purpose and procedures of the study. All information of patients remained as confidential as national protocol suggests. The necessary information about the purpose and procedures of the study was explained to the study participants and attendants and for professionals who has participated in the data collecting. Each laboratory result of study participants was reported to the requesting physicians on time.
- Operational Definition
Sterile body fluids: biological fluids found in human body which do not contain any microorganisms at normal state such as, cerebrospinal fluid, pleural fluid, pericardial fluid, peritoneal or ascitic fluid, synovial fluid [9].
Sterile body fluids infection: microbial invasion and physiochemical change in the SBF site [11].
Gross appearance: naked eye observable physical status of sample if it`s clear, turbid, bloody, yellowish, or purulent.
Types of specimens: referencing the site of the sterile fluid sample collected to classify as cerebrospinal fluid, pleural fluid, pericardial fluid, peritoneal or ascitic fluid, synovial fluid etc.
Multidrug resistance (MDR): resistant at least one agent in three or more antimicrobial categories [12].
Results
- Socio-Demographic Characteristics
In this study, 186 SBF samples were collected from patients attending at Minilik II Comprehensive Specialized Hospital and Yekatit 12 Medical College Hospital from February - June, 2024. From total participants, 110 (59.1%) were female and 54 (29.0%) were over 50 years old. Correspondingly, government employees took 48 (25.7%) while, based on participant`s monthly income, 69 (36.9%) had in a range 10001-20000 ETB. Similarly, 120 (64.5%) were above college level in their education status (Table 1).
- Clinical and Sample-Related Characteristics
Sterile samples were collected aseptically from four (04) different sites secreting SBFs. In this study; CSF, pleural, synovial and peritoneal fluids were collected from participants. From these collected samples, Pleural fluid 55 (29.6%), Cerebrospinal fluids 52 (28.0%), Ascitic/peritoneal fluid 43 (23.1%) and synovial fluid 36 (19.4%) were encountered in the study. Among these samples types collected and investigated for bacterial growth on culture, CSF found with the highest burden among the collected SBF sample followed by pleural fluid, 6/17 (35.3%) and 5/17 (29.4%) respectively (Figure 2).
- Prevalence of Bacterial Isolates
According to the present study, the overall prevalence of SBF bacterial infection among participants is 17 /186 (9.1%) (CI=95%, 3.8-14.5).
Regarding to the gram stain characteristics of the isolated bacteria, 12/17 (70.6%) were gram-negative bacteria.
From the culture growth isolated bacteria, K. pneumoniae was found as the most predominant one 29.4% (5/17) and followed by E. coli attaining 23.5% (4/17) for SBF infection (Figure 3).
In this study, the incidence of bacterial SBF infection was higher in females when compared to males. From the isolated bacteria, 11/17 (64.7%) were from female study participants.
Similarly, the highest prevalence was recorded from under ten (<10) years study participants with burden of 6/17 (35.5%). (Figure 4).
- Antimicrobial Susceptibility Patterns
A drug sensitivity test was performed for all (17) bacterial isolates. These isolates had shown various resistance and susceptibility patterns against different antibiotics that were tested on MHA. The AST pattern of gram-negative bacteria was observed that antibiotics drugs of Meropenem and Amikacin had showed the most effectiveness against gram-negative isolates both with 83.3% effective action on the isolates consequently also, Amoxa-clavlanic acid at 75% effect over the isolated bacteria. However, highest resistance rate was observed on third-generation cephalosporin, Ceftazidime and Ceftraxone with 58.3% weak effect on gram-negative isolates also; Trimethoprim-Sulfamethoxazole had expelled 41.7% resistance to isolated gram negatives. Most effective antibiotics against K. pneumoniae isolates (n=5) on AST were Amikacin, Meropenem and Amoxa-clavlanic acid which showed 80% effectiveness. In contrast, the highest resistance was observed for Ceftraxone and Ceftazidime each with 60% résistance rate. All the E. coli isolates (n=4) were susceptible to Amikacin, Meropium and Amoxa-clavulanic acid 75% for each isolates. But they were 50% resistant to Gentamycin, Trimethoprim-Sulfamethoxazole and third-generation cephalosporins such as Ceftazidime and Ceftriaxone.
The overall resistance rate of Gram positive bacteria had showed that, Trimptoprin-sulfamethoxazole 60% (3/5), ceftriaxone 60% (3/5) and ciprofloxacilin 40% (2/5). However, the gram positive isolates showed no resistance for Cefoxtin and Vancomycin that isolates were 100% sensitive and Erythromycin showed 80% effective action on isolates (Table 2).
- Multi-Drug Resistance
According to the present study, 12 (70.5%) bacteria isolated were MDR. From these, 66.7% (8/12) MDR isolates were gram-negative isolates and 80% (4/5) of isolates of Gram-positive isolates. From the frequently isolated bacteria, 75% (3/4) of E. coli and 2/5 (40%) of K. Pneumoniae isolates were found as MDR (Table 3).
Discussion
Biological fluids collected from sterile bodily areas are anticipated to be free from both pathogenic and commensal bacteria. Any pathological agents or environmental skin pollutants could be the source of infection in these SBFs. Although SBFs, such as pleural fluid, ascitic fluid, and CSF, are typically sterile, they may become contaminated by various microorganisms and develop potentially fatal diseases. Microbial invasion of normally sterile parts of the body can cause systemic illness. Meningitis, pericarditis, pleural infection either complicated parapneumonic effusion or empyema and septic arthritis cover major forms of SBFs infections [13,14].
In the present study, the overall prevalence of bacterial SBF infection was 9.1% (17/186). This prevalence finding in some extent is close with most previous studies, while offset with few studies.
Accordingly, the prevalence of bacterial SBF infection in this study found similar to the study conducted in Turkey in 2021, which was 9.7%, and Nepal in 2019, 10.7% [14,15]. In advance, studies from Addis Ababa, Ethiopia, at EPHI and TASH, reported a prevalence of bacterial SBF infection as 11.5% and 14.1%, respectively [2,4]. These results tell that the prevalence of bacteria causing SBF infection in studies done in Addis Ababa in some extent is similar. Although, for the least contradictions observed, study population socio-economic background, study methods and sample sizes are noted as contributing factors.
In contrast, the prevalence of this study is found higher than study from Debremarkos, North-western Ethiopia, (7.5%), and lower to the study from Mekele, Ethiopia, (20.2%) [16,17]. For the variations of the prevalence’s among studies can be attributed to differences in sample processing/laboratory technique, environmental status of the study area and the practice of infection control. Accordingly, the appropriate management of patient, early detection and identification of organism with the results of AST is crucial. Positive cultures are usually low because of less number of pathogens and prior administration of empirical antibiotics in patients [14,18,19,20].
In the present study, the most frequently isolated bacteria are gram-negative bacteria (70.6%) that`s identical with the study conducted at HFSH, Harar, Ethiopia. Similarly, study from India, gram negative isolates were 71% likely, from EPHI, Addis Ababa, Ethiopia, 74.6% of total isolates were gram negative [4,21,22].
In contrast, clashing with this study, studies conducted in Mekelle, Ethiopia and India, gram positive bacteria were the dominant isolates as 52.3% and 85.2% of total isolates respectively [16,23]. This obverse finding on the bacterial characteristics in these studies, can possibly be due to differences on sample sizes, study areas, hospital-acquired infections, and different epidemiological factors also standard infection control precautions applied on the sites [24].
In general, from isolated bacteria in this study, K. pneumoniae (5/17, 29.4%), E.coli (4/17, 23.5%), and S. aureus (2/17, 11.8%) were the most frequently isolates causing SBF infection. This data record is similar with earlier studies done in Ethiopia (HFSH and TASH), Turkey, India, and Kenya. This uniform data pattern observed could be explained by their distinctive structure of gram-negative bacteria, are their increasingly resistant presentation to most available antibiotics or opportunistic nature of organisms [9,14,22,25].
In the present study, antibiotics, Meropenem (83.3%) and Amikacin (83.3%) found with the most effective action against gram-negative isolates. Whereas, cefraxone and cefepime found as the least effective antibiotics against gram -negatives in which 58.3% of each antibiotics were resisted by isolates. This result is complementary with the studies carried out from HFSH, Harar, tertiary care hospital, India, Accra, Gana, and with Debremarkos, North west Ethiopia [9,17,22,26].
In contrast to the Gram positives bacteria isolates of this study, 100% of the isolates were noted as sensitive to Cefoxin and vancomycin, and 80% of the isolates were found sensitive to Erytromycin. Contrarily, 60% of gram positives executed resistance to ceftriaxone and Sulfamethoxazole-trimethoprim. In advance, S. pneumoniae and Entrococcus were found resistant for most classes of antibiotics such as Sulfamethoxazole-trimethoprim, ciprofloxacilin and ceftriaxone. This record of data is homogenous with study from Turkey that showed both isolates, S. pneumoniae and Entrococcus were the most frequent isolate with the most problematic resistance patterns [14].
From this study, the increased rate of phenomenon of beta-lactam including third generation cephalosporins drug resistance may be linked to various factors, including but not limited to the frequent use of antibiotics, their easy availability, and the practice of self-medication, the scarcity of diagnostic facilities, the inappropriate use of antibiotics and the tradition of manipulation of prescriptions without susceptibility data. Also a survey in Sub-Saharan Africa and Asia reveal that affordable first line agents such as ampicillin and gentamicin are unlikely to be clinically efficacious in a substantial proportion of infections. This results in increasing reliance on the third generation cephalosporins for empirical treatment of serious infections. However, the spread of extended-spectrum beta-lactamase producing strains into the community, probably accelerated by this increased consumption, is eroding the usefulness of these drugs. Alternative agents for treating multi-resistant coliform infections, such as the carbapenems, are unaffordable for treatment of community-acquired infections in low-income countries. In addition, these organisms have a range of mechanisms to prevent the action of many antimicrobials used in clinical medicine such as efflux pumps, alteration of the drug binding site and membrane permeability, degradation enzymes [27,28].
Multi drug resistance (MDR) pattern at 70.6% of isolates was recorded in this study. This result in fewer extents is similar with the studies from HFSH, TASH in Addis Ababa, and Debremarkos, north-west Ethiopia with 76.4, 75% and 78.6% respectively. However, this finding had higher MDR rate with the study from Mekele, Northern Ethiopia, which is 40.1% also, higher than study in Nepal that had 30% MDR rate. There are many possible explanations for this difference and increased prevalence among the studies conducted socio-demography and clinical determinants status including: Self-medication, poor adherence to complete antibiotic regimens and low quality, often counterfeit drugs are all common. The disease burden from bacterial pathogens is greatest different bacterial strains, geographic variation, patients’ awareness towards the use of the antimicrobials, the difference in infection control practice, the difference in antibiotic prescribing policies, easy availability of some drugs without a prescription, and indiscriminate/prolonged use of common antibiotics lead to rapid and extensive spread of antimicrobial resistance Also, the environmental persistence of resistance genes or drug residues. Antibiotic resistance spreads through a variety of environmental reservoirs, such as soil, water, hospitals, industries, farm waste, and other contaminated ecological niches [1,2,17,22,29].
- Strength and limitations of the Study
- Limitation of the Study
The etiology of bacteria for infections of SBF being at minimal dose, detection rate is reduced as of the growing inquiry on culture media also, the avoidance of anaerobic bacteria enrichment, which were excluded from this investigation due to the seldom availability of national laboratory setup, the overall culture positivity rate of SBF samples was relatively low. Since the diagnosis of anaerobic bacteria is expensive and requires special facilities and expertise to perform this study doesn`t include anaerobic bacteria. The risk of false-negative results in agar-based culture media is high because only a small number of microorganisms may be present in the specimens.
- Strength of the Study
The present study, unlike most previous studies, it is conducted at the two of the largest highest hospitals, Minilik II Comprehensive Specialized Hospital and Yekatit 12 Hospital Medical College which brought a better diverse participant population that built the study finding represents a wide and diverse population so that it assure to develop a better generalization for further hypothetical study.
- Conclusions and Recommendation
Conclusions
A variety of gram-positive, as well as gram-negative organisms, were isolated from collected SBF samples analyzed in the study, which yielded 17 of 186 (9.1%). Dominantly, K.pneumoniae and E.coli were the leading causative agents for SBF infection. Amikacin and meropenem were found to be the most effective drugs, both executing 83.3% effective action against gram-negative isolates. However, the gram negatives were 58.3% resistance to third-generation cephalosporin. Also the gram-positive isolates showed 60% resistant to trimethoprim-sulfamethoxazole and ceftriaxone. While, cefoxitin and erytromycin, were observed with effective action against gram- positive isolates 100% and 80%, respectively. The majority, (70.5%) of the isolates have shown multidrug resistance (MDR) pattern, especially to commonly in use and easily available drugs.
- Recommendations
The following recommendations are made based on the findings of the present study.
For Yekatit 12 hospital medical college and Minilik II comprehensive hospital Hospital:
The hospital should acknowledge that Culture and susceptibility testing has to be an integral part of routine laboratory tests for the best management of infections in patients, and the choice of drugs should be based on results of sensitivity testing.
For Addis Ababa health bureau:
This data should be used as a baseline for development of better formulation of practical antibiotic policy and a regular surveillance of hospital-associated infections and monitoring of antibiotic susceptibility pattern based on the current study are suggested. In addition, advancement and technical support for laboratories found under AAHB on the bacteria growing and identification technique like molecular and automated machines is preferable for a better detection capability.
For health care workers:
The antibiotic sensitivity profile suggests that ciprofloxacin and amikacin are a choice of drugs for sterile body infections. However, Beta-lactam antibiotics such as third-generation cephalosporins, ampicillin, and penicillin should be used carefully unless tested.
The careful prescribing practice or rational use of antibiotics based on sensitivity testing result is needed to halt the trend of increasing antibiotic resistance. Besides, great care should be given to inpatients, as they are more vulnerable to bacterial infections in sterile body areas.
For future researchers:
Since this study was not conducted alongside the nation with well enough data. The present study was conducted on a limited number of samples; this may not reflect the entire scenarios of the study. This highlights the need for further studies to be conducted on larger sample sizes. Further, antimicrobial resistance is also gradually increasing, which needs much attention. Thus, continuous monitoring of susceptibility profile of the clinically important pathogens is of great importance to guide effective antimicrobial therapy.
References
- Shrestha LB, Bhattarai NR, Khanal B. Bacteriological profile and antimicrobial susceptibility pattern among isolates obtained From body fluids. Journal of Nepal Health Research Council. 2019;17(2):173-7. [CrossRef]
- Teklehymanot F, Legese M, Desta K. Bacterial profile and their antimicrobial resistance patterns from body fluids at Tikur Anbesa Specialized Hospital, Addis Ababa, Ethiopia. Biol Med (Aligarh). 2017;9(05):408.
- Shume T, Tesfa T, Mekonnen S, Asmerom H, Tebeje F, Weldegebreal F. Aerobic Bacterial Profile and Their Antibiotic Susceptibility Patterns of Sterile Body Fluids Among Patients at Hiwot Fana Specialized University Hospital, Harar, Eastern Ethiopia. Infection and Drug Resistance. 2022:581-93. [CrossRef]
- Ebrahim S. Bacterial profile and antimicrobial susceptibility pattern of isolates recovered from sterile body fluids referred to the national reference laboratory. Ethiopian Journal of public health and nutrition. 2020;4(1).
- Kar M, Chaudhary R, Sahu C, Dubey A, Patel SS. Bacterial Isolates and Drug Susceptibility Pattern of Sterile Body Fluids at a Tertiary Care Hospital in Northern India. [CrossRef]
- Altun O. Rapid microbiological diagnosis of infections in sterile body fluids including blood: Karolinska Institutet (Sweden); 2020.
- Assefa Y, Moges F, Endris M, Zereay B, Amare B, Bekele D, et al. Bacteriological profile and drug susceptibility patterns in dacryocystitis patients attending Gondar University Teaching Hospital, Northwest Ethiopia. BMC ophthalmology. 2015;15:1-8. [CrossRef]
- Sodani S, Hawaldar R. Bacteriological profile and antibiotic sensitivity pattern in various body fluids–A retrospective study. Indian J Microbiol Res. 2020;7(1):1-58. [CrossRef]
- Madigubba H, Deepashree R, Gopichand P, Sastry AS. Bacteriological profile and antimicrobial susceptibility pattern in sterile body fluid specimens from a tertiary care hospital, South India. Journal of Current Research in Scientific Medicine. 2020;6(2):96.
- CLSI. Performance standards for antimicrobial susceptibility testing 32th ed. Supplement M100S. Wayne, PA: Clinical and Laboratory Standards Institute; 2022.
- Singh P, Pandey A, Bisht ASJIJoMS. Sterile body fluids infections: Profile of bacteria and their antimicrobial resistance pattern in a tertiary care hospital from Uttar Pradesh. 2023;75(3):161. [CrossRef]
- Magiorakos A-P, Srinivasan A, Carey RB, Carmeli Y, Falagas M, Giske C, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. 2012;18(3):268-81. [CrossRef]
- Kar M, Chaudhary R, Sahu C, Dubey A, Patel SSJJoAiM. Bacterial Isolates and Drug Susceptibility Pattern of Sterile Body Fluids at a Tertiary Care Hospital in Northern India. 2022;22(8):6-15. [CrossRef]
- Duran AÇ, Atik TK, Özen N, Sig AK, Irmak OJJoHS, Medicine. Distribution of clinical isolates obtained from sterile body fluids: a four-year retrospective data. 2021;4(6):907-11. [CrossRef]
- SHRESTHA LB, BHATTARAI, N. R. & KHANAL, B. Bacteriological Profile and Antimicrobial Susceptibility Pattern among Isolates Obtained From Body Fluids. Journal of Nepal Health Research Council. 2019;17:173-7. [CrossRef]
- Tsegay E, Hailesilassie A, Hailekiros H, Niguse S, Saravanan M, Abdulkader M. Bacterial isolates and drug susceptibility pattern of sterile body fluids from tertiary hospital, Northern Ethiopia: a four-year retrospective study. Journal of pathogens. 2019;2019. [CrossRef]
- Admas D, Demeke G, Adugna A, Esmael AJFiM. Bacterial etiologies, antimicrobial susceptibility pattern and associated factors among patients suspected sterile body site infections at Debre Markos Comprehensive Specialized Hospital, Northwest Ethiopia. 2024;11:1260841. [CrossRef]
- Shrestha LB, Bhattarai NR, Khanal B. Bacteriological profile and antimicrobial susceptibility pattern among isolates obtained from body fluids. 2019. [CrossRef]
- Fleischmann-Struzek C, Goldfarb DM, Schlattmann P, Schlapbach LJ, Reinhart K, Kissoon NJTLRM. The global burden of paediatric and neonatal sepsis: a systematic review. 2018;6(3):223-30. [CrossRef]
- Fatema K, Barai LJBMJ. Infection prevention and control in health care settings during COVID-19 pandemic. 2020:81-92.
- Sandhya E, Savio R, Dutta A, Das B, Sharma T, Hazarika MJIJSR. A study of bacteriological profile of sterile body fluids in a tertiary care hospital. 2019;8(S11):41-5.
- Shume T. BACTERIAL PROFILE IN STERILE BODY FLUIDS, ASSOCIATED FACTORS, AND ANTIBIOTIC SUSCEPTIBILITY PATTERNS AMONG PATIENTS AT HIWOT FANA SPECIALIZED UNIVERSITY HOSPITAL, HARAR, EASTERN ETHIOPIA: Haramaya university; 2021.
- Mehta Y, Gupta A, Todi S, Myatra S, Samaddar D, Patil V, et al. Guidelines for prevention of hospital acquired infections. 2014;18(3):149. [CrossRef]
- Vishalakshi B, Hanumanthappa P, Krishna SJIJoCM, Sciences A. A study on aerobic bacteriological profile of sterile body fluids. 2016;5(5):120-6.
- Bwisa L. Antimicrobial susceptibility patterns of bacteria isolated from sterile sites: cerebral spinal fluid, blood, peritoneal fluid, pleural fluid and synovial fluid at Kenyatta National Hospital 2014.
- Mohammed J, Hounmanou YMG, Thomsen LEJBRN. Antimicrobial resistance among clinically relevant bacterial isolates in Accra: a retrospective study. 2018;11:1-6. [CrossRef]
- Chokshi A, Sifri Z, Cennimo D, Horng HJJogid. Global contributors to antibiotic resistance. 2019;11(1):36-42. [CrossRef]
- TIWARI S, NANDA M, PATTANAIK S, PRASAD A, KAR A, NAYAK SK, et al. Bacteriological Profile and Antibiotic Susceptibility Pattern in Sterile Body Fluids from a Tertiary Care Hospital in Bhubaneswar, Odisha, India: A Cross-sectional Study. 2023;17(11). [CrossRef]
- Lubell Y, Turner P, Ashley EA, White NJJTM, Health I. Susceptibility of bacterial isolates from community-acquired infections in sub-Saharan Africa and Asia to macrolide antibiotics. 2011;16(10):1192-205. [CrossRef]
Figure 2.
The SBF sample type proportion causing SBF infection at Yekatit 12 Hospital and Minilik II Hospital, February-June 2024.
Figure 2.
The SBF sample type proportion causing SBF infection at Yekatit 12 Hospital and Minilik II Hospital, February-June 2024.
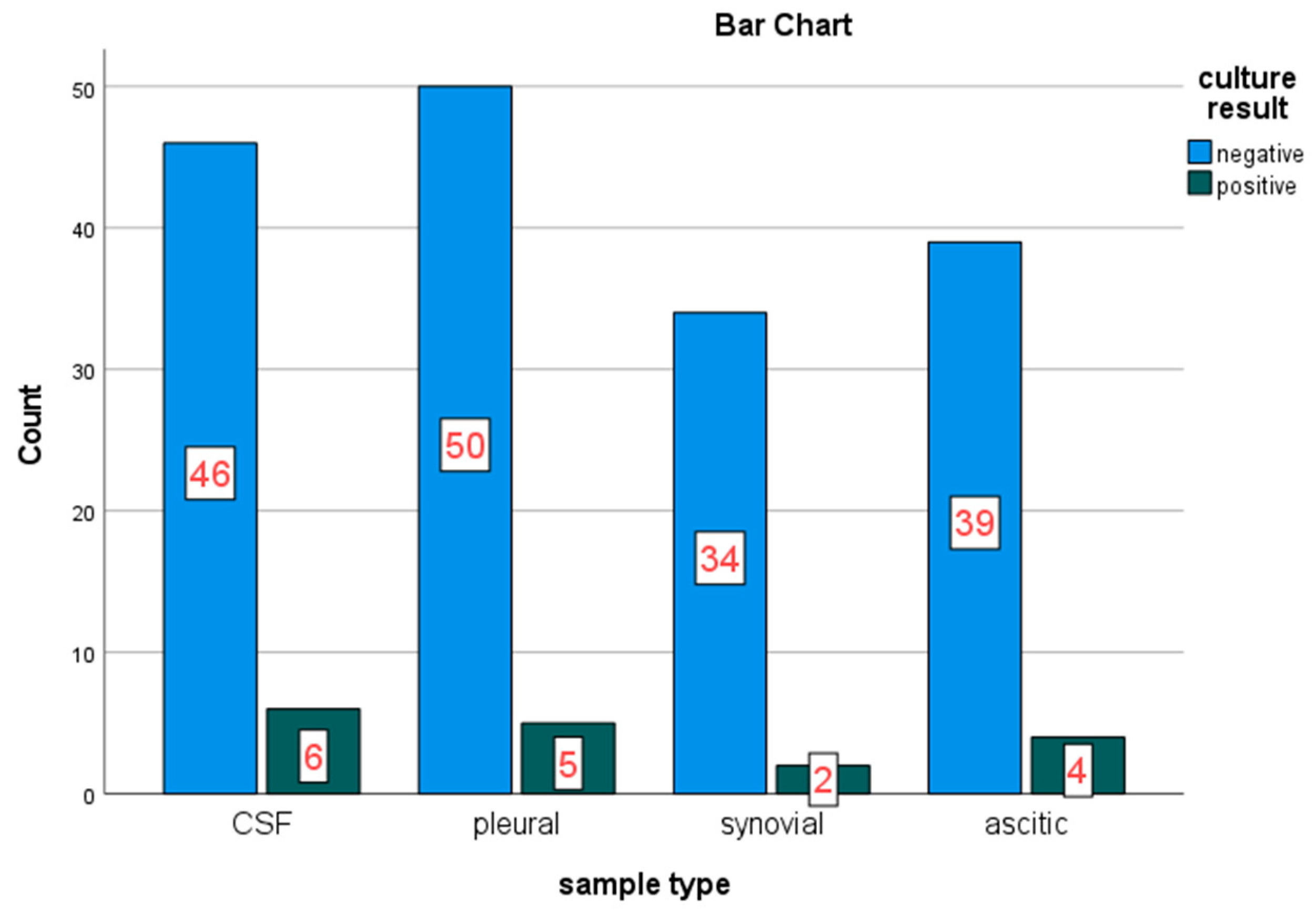
Figure 3.
Bacterial isolates on patients with SBF infections at Yekatit 12 Hospital and Minilik II Hospital, February-June 2024.
Figure 3.
Bacterial isolates on patients with SBF infections at Yekatit 12 Hospital and Minilik II Hospital, February-June 2024.
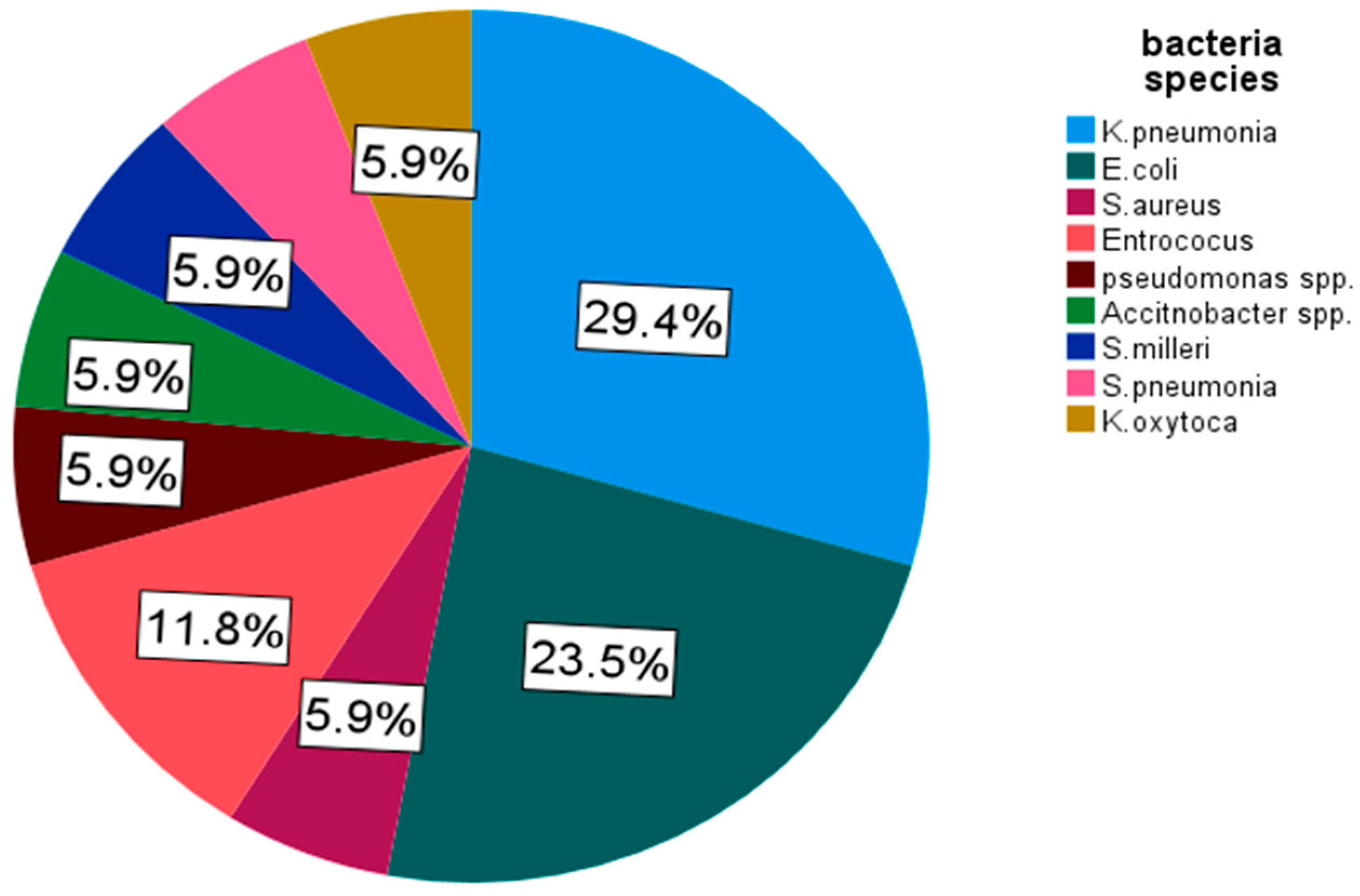
Figure 4.
Prevalence of SBF bacterial infection amidst to patient`s age category at Yekatit 12 Hospital and Minilik II Hospital, February-June 2024.
Figure 4.
Prevalence of SBF bacterial infection amidst to patient`s age category at Yekatit 12 Hospital and Minilik II Hospital, February-June 2024.
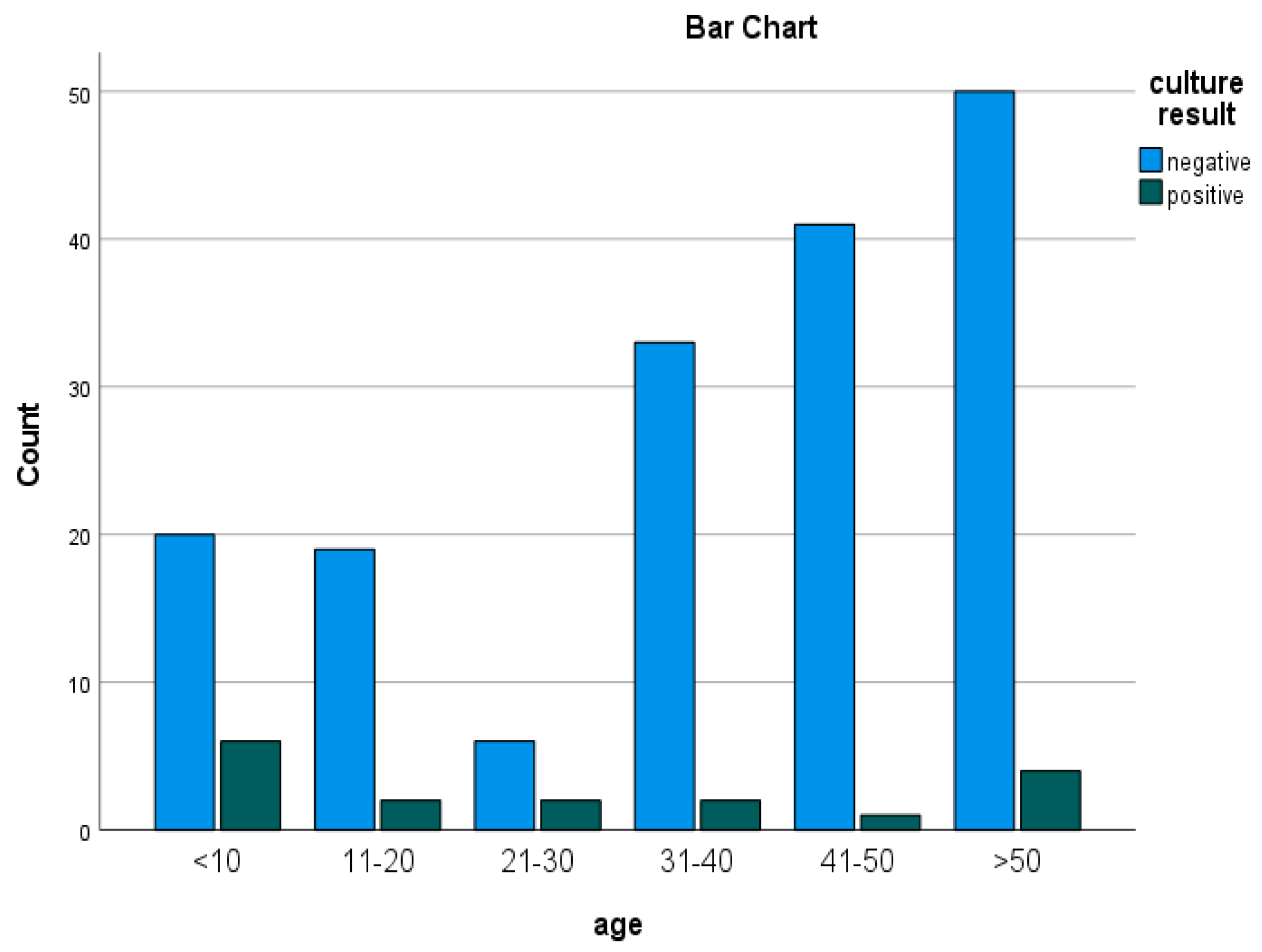

Table 1.
Socio-demographic character of participants in SBF infection suspects at Yekatit 12 Hospital and Minilik II Hospital, February-June 2024.
Table 1.
Socio-demographic character of participants in SBF infection suspects at Yekatit 12 Hospital and Minilik II Hospital, February-June 2024.
| Category | Frequency | % | |
|---|---|---|---|
| Age | <10 | 26 | 14.0 |
| 11-20 | 21 | 11.3 | |
| 21-30 | 8 | 4.3 | |
| 31-40 | 35 | 18.8 | |
| 41-50 | 42 | 22.6 | |
| >50 | 54 | 29.0 | |
| Sex | Male | 76 | 40.9 |
| Female | 110 | 59.1 | |
| EducationalStatus | Pre-school | 10 | 5.4 |
| Unable to read or write | 1 | 0.5 | |
| Primary | 33 | 17.7 | |
| Secondary/High school | 22 | 11.8 | |
| College and above | 120 | 64.5 | |
| Occupation | Government employee | 48 | 25.8 |
| Labor worker | 26 | 14 | |
| Student | 46 | 24.7 | |
| Farmer | 14 | 7.5 | |
| Housewife/househusband | 9 | 4.8 | |
| Merchant | 17 | 9.1 | |
| Other | 26 | 14.0 | |
| Monthly-income | No income | 50 | 26.9 |
| 100-5000 | 16 | 8.6 | |
| 5001-10000 | 26 | 14 | |
| 10001-20000 | 69 | 37.1 | |
| ≥20000 | 25 | 13.4 |
Table 2.
Antibiotic resistance pattern of gram positive and gram negative bacteria isolates from suspected patients who had body fluids infections at Yektit 12 Hospital and Minilik II Hospital, Addis Ababa, 2024.
Table 2.
Antibiotic resistance pattern of gram positive and gram negative bacteria isolates from suspected patients who had body fluids infections at Yektit 12 Hospital and Minilik II Hospital, Addis Ababa, 2024.
| GRAM POSTIVE ISOLATES | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| AMC | CLN | FOX | VA | SXT | CRO | CPR | ERY | |||
|
S.aureus (N=1) |
S | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||
| R | 1 | |||||||||
| Enterococcus (N=2) | S | 1 | 1 | 2 | 2 | 1 | 1 | 1 | 2 | |
| R | 1 | 1 | 1 | 1 | 1 | |||||
|
S.milleri (N=1) |
S | 1 | 1 | 1 | 1 | 1 | 1 | |||
| R | 1 | 1 | ||||||||
| S. pneumoniae (N=1) | S | 1 | 1 | 1 | 1 | |||||
| R | 1 | 1 | 1 | 1 | ||||||
| N (%) | S | 3(60) | 3(60) | 5(100) | 5(100) | 2 (40) | 2(40) | 3(60) | 4 (80) | |
| N (%) | R | 2(40) | 2(40) | 0(0) | 0(0) | 3 (60) | 3(60) | 2 (40) | 1(20) | |
| GRAM NEGATIVE ISOLATES | ||||||||||
| CPR | MER | CRO | AMC | SXT | GEN | CTZ | AMK | |||
|
K.Pneumonia (N=5) |
S | 3 | 4 | 2 | 4 | 3 | 3 | 2 | 4 | |
| R | 2 | 1 | 3 | 1 | 2 | 2 | 3 | 1 | ||
| E.coli (N=4) | S | 3 | 3 | 2 | 3 | 2 | 2 | 2 | 3 | |
| R | 1 | 1 | 2 | 1 | 2 | 2 | 2 | 1 | ||
|
Pseudomonas (N=1) |
S | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | |
| R | ||||||||||
|
Acitnobacter (N=1) |
S | 1 | 1 | 1 | 1 | 1 | ||||
| R | 1 | 1 | 1 | |||||||
|
K.oxytoca (N=1) |
S | 1 | 1 | 1 | 1 | |||||
| R | 1 | 1 | 1 | 1 | ||||||
| N (%) | S | 8(66.7) | 10(83.3) | 5(41.7) | 9(75) | 7(58.3) | 8(66.7) | 5(41.7) | 10(83.3) | |
| N (%) | R | 4(33.3) | 2 (16.7) | 7(58.3) | 3(25) | 5(41.7) | 4(33.3) | 7(58.3) | 2 (16.7) | |
Note; SXT: Trimethoprim-sulfamethoxazole; CRO: Ceftriaxone; AMC: Amoxicillin-Clavulanic acid; GN: Gentamicin; VA: Vancomycin; CPR: Ciprofloxacin; FOX: cefoxitin; ERY: Erythromycin; CLN: Clindamycin; CTZ:Ceftazidime: AMK, Amikacin : S: sensitive; R: resistant.
Table 3.
Multidrug resistance pattern of bacterial isolates.
| Bacterial isolates | Antibiotic-resistant | ||||||
|---|---|---|---|---|---|---|---|
| Gram-negative | R0 | R1 | R2 | R3 | R4 | ≥R5 | MDR |
| K. pneumoniae (n=5) | - | 2 | - | 2 | - | 1 | 3 |
| E. coli (n=4) | - | 1 | - | 1 | 2 | - | 3 |
| Pseudomonas (n=1) | - | 1 | - | - | - | - | 0 |
| Acitnobacter (n=1) | - | - | - | 1 | - | - | 1 |
| K.oxytoca (n=1) | - | - | - | - | 1 | - | 1 |
| Total (n=12, %) | 0(0%) | 4(33.3) | 0((0) | 4(25) | 3(25) | 1(8.3) | 8 (66.7%) |
| Gram-positive bacteria | |||||||
| S. aureus (n=1) | - | - | - | - | 1 | - | 1 |
| Enterococcus spp. (n=2) | - | 1 | - | 1 | - | - | 1 |
| S. milleri (n=1) | - | - | - | 1 | - | - | 1 |
| S. pneumoniae (n=1) | - | - | - | - | - | 1 | 1 |
| Total n=5, (%) | 0 | 1(20) | 0(0) | 2(40) | 1(20) | 1(20) | 4(80%) |
Note: - R0: Sensitive for all, R1: resistance to one drug, R2: resistance to two drugs, R3: resistance to three drugs, R4: resistance to four drugs, ≥R5: resistance to five and above.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



