
Submitted:
05 May 2025
Posted:
06 May 2025
You are already at the latest version
Abstract
Objective: To evaluate the economic impact associated with the use of specific brain biomarkers glial fibrillary acid protein (GFAP) and ubiquitin C-terminal hydrolase L1 (UCH-L1) in adult patients with suspected mild traumatic brain injury (TBI) in a standard Spanish hospital setting. Methods: We used a budget impact analysis (BIA) to compare the cost of standard of care using head computed tomography (CT) to evaluate intracranial injury with a scenario incorporating specific biomarkers GFAP and UCH-L1 in an estimated population of 3,500 adult patients attending the hospital emergency department with a score of 13 to 15 on the Glasgow Coma Scale (GCS). The probabilities associated with clinical procedures were obtained from a multidisciplinary group of experts from Spanish hospitals and supplemented with data from the literature. Costs were estimated using hospital tariffs from the Spanish autonomous communities and other official sources. Results: The incorporation of specific biomarkers GFAP and UCH-L1 in the management of mild TBI could generate estimated annual savings of €696,634 in a standard Spanish hospital, mainly due to reduced CT use. The average saving per patient would be €199.04, and the care time would be reduced by 111 minutes. Sensitivity analysis, with variations of ±20% in the parameters, confirms these savings. Conclusions: This study suggests that the use of specific biomarkers GFAP and UCH-L1 in the management of mild TBI patients in Spain could reduce the average cost per patient, generating significant savings for hospitals. Future studies that incorporate data from clinical records will help validate these results.
Keywords:
Mild traumatic brain injury
; intracranial injury
; biomarkers
; budget impact analysis
; computed tomography
; emergency department
1. Introduction
Traumatic brain injury (TBI) is the leading cause of death and disability worldwide among all traumatic injuries and is costly for both the healthcare system and society [1,2,3]. Some studies estimate that, globally, there are between 50 and 60 million new cases of TBI every year, of which more than 90% are mild [3,4].
Computed tomography (CT) scan is currently the standard diagnostic tool in the assessment of intracranial injury in patients with TBI and the identification of individuals who need immediate surgery [5,6]. There is a general consensus on performing head CT in patients with moderate or severe TBI, but there is no agreement on the use of this procedure in patients with mild TBI (score on the Glasgow Coma Scale –GCS– between 13-15), given the low prevalence of intracranial abnormalities detected by CT and the low associated mortality in this population [7]. The need to identify patients with mild TBI at high risk of acute intracranial injury (AII), coupled with the lack of objective diagnostic tools to determine the neurocognitive status of patients, has led to an exponential increase in head CT requests in hospital emergency departments (ED) [7]. This situation results in not only increased radiation exposure in patients and saturated EDs but also has a significant economic impact on health systems [7,8,9].
There have been recent advances in the study of biomarkers in blood that improve the clinical characterization of patients with possible brain damage. Among these, the rapid serum/plasma test for specific biomarkers glial fibrillary acid protein (GFAP) and ubiquitin C-terminal hydrolase L1 (UCH-L1) for mild TBI represents a paradigm shift in the evaluation of the lesion [7]. The inclusion of this test in the clinical evaluation of adult patients with GCS 13-15 in the first 12 hours after the TBI guides the need for scans, reserving the use of CT for necessary cases [7,10].
The Spanish Society of Emergency Medicine (SEMES) recently collaborated with another 5 scientific societies in the publication of a set of guidelines, based on an updated, mutually agreed algorithm to standardize the management of patients with mild TBI and incorporate the use of specific biomarkers GFAP and UCH-L1 in routine clinical practice [7]. This approach offers a more detailed risk stratification, aimed at defining best patient management and optimizing the use of resources. Nevertheless, economic evidence on the incorporation of specific biomarkers GFAP and UCH-L1 in the Spanish setting is limited.
The objective of this study was to evaluate the economic impact associated with the use of specific biomarkers GFAP and UCH-L1 in adult patients with GSC 13-15 admitted to an ED, in a standard Spanish hospital setting. The secondary objective was to analyze the impact on management times for the different processes involved.
2. Materials and Methods
A budget impact analysis (BIA) model was developed to evaluate the economic impact associated with the use of specific biomarkers GFAP and UCH-L1 in patients with suspected mild TBI admitted to the ED. The direct costs, updated to 2023, and time dedicated to the management of these patients were quantified. The model was developed following specific methodological guidelines and recommendations for studies of this type [11,12,13].
2.1. Study Population, Perspective, and Timelines
The study included patients aged 18 years or older with suspected mild TBI, defined by a GCS score of 13-15, who attended the ED. The BIA model was developed from the perspective of a Spanish hospital. The timeline of the study was 1 year, and the population with suspected mild TBI seen in a standard Spanish hospital was estimated to be approximately 3,500 patients per year.
2.2. Structure of the Model and Comparators
The BIA model is based on a decision tree developed in Microsoft Excel. It was constructed from the SEMES recommendations on the use of the specific biomarkers GFAP and UCH-L1, published in December 2023, aimed at standardizing the management of patients with mild TBI in Spain [7]. The decision tree compared 2 scenarios: standard of care, which consists of performing a head CT to evaluate possible AII (Figure 1); and the updated scenario, which incorporates the use of specific biomarkers GFAP and UCH-L1 in patients with suspected mild TBI who attend the ED within 12 hours of injury (Figure 2) [10,14]. The proposed model compares the average cost per patient for each of the 2 scenarios.
2.3. Identification, Quantification, and Evaluation of Clinical Inputs
The probabilities associated with the clinical procedures included in the model (Table 1) were based on estimates provided by a group of experts from various specialties (emergency medicine, radiology, clinical laboratory, and clinical biochemistry), based on their practical experience with specific biomarkers GFAP and UCH-L1 in Spanish hospitals. In cases where no information was available, a literature review was used to complete the data.
2.4. Cost Estimation
To estimate the costs of the procedures included (Table 2), we examined data from the official tariffs of the most representative autonomous communities and official sources, such as the Minimum Basic Data Set (MBDS) [16] which collects clinical and service usage information, and the Spanish Network of Hospital Costs (RECH) [17]. All costs are expressed in euros updated to the year 2023. The economic modeling of the cost of the specific biomarkers GFAP and UCH-L1 was calculated based on the experience of their use in 1 hospital over a period of 2 years. During this time, 2 annual calibrations were performed due to a change in lot number; 1 control level was run daily, and between 15 and 20 measurements were performed per day. Under these specific conditions of use and efficiency, the reagent efficiency is 94%.
2.5. Management Time Estimation
To estimate the time required to manage these patients in both scenarios, we used the times reported by the experts for the different stages of the care process, based on their own experience in clinical practice in Spain (Table 3).
2.6. Sensitivity Analysis
A univariate sensitivity analysis was performed to address the uncertainty associated with both the structure and the parameters of the model and to evaluate the robustness of the results. In this analysis, the values of the parameters were modified within a range of ±20%, in order to identify the variables that have the greatest impact on the savings generated by the use of specific biomarkers GFAP and UCH-L1, compared to the standard management of patients with mild TBI attending the ED.
3. Results
3.1. Budgetary Impact
The use of specific biomarkers GFAP and UCH-L1 results in a reduction in the number of CT scans performed in patients with suspected mild TBI attending the ED (in routine clinical practice, 93% of these patients would undergo a CT scan, whereas, with the use of specific biomarkers GFAP and UCH-L1, only 66.5% would undergo the procedure). Taking the estimated costs into account, Table 4 shows the average cost for each procedure included in the decision tree.

Table 2.
Mean cost for each procedure included in the model, routine clinical practice vs. specific biomarkers GFAP and UCH-L1.
Table 2.
Mean cost for each procedure included in the model, routine clinical practice vs. specific biomarkers GFAP and UCH-L1.
| Procedure | Routine clinical practice | Specific biomarkers | Difference |
|---|---|---|---|
| Emergency visits | €215.00 | €215.00 | - € |
| Specific biomarkers GFAP and UCH-L1 | - € | €28.10 | €28.10 |
| CT | €171.12 | €122.35 | - €48.77 |
| Follow-up CT | €48.46 | €20.29 | - €28.18 |
| Observation in ED | €376.34 | €268.82 | - €107.52 |
| Admission to Neurosurgery | €28.90 | €10.54 | - €18.36 |
| Outpatient monitoring | €34.75 | €12.55 | - €22.20 |
| Operating room | €16.90 | €16.29 | - €0.61 |
| ICU | €2.66 | €1.28 | - €1.38 |
| Readmission to ED | €4.63 | €4.52 | - €0.12 |
| Abbreviations: CT, computed tomography; ED, emergency department; GFAP, glial fibrillary acid protein; ICU, intensive care unit; UCH-L1, ubiquitin C-terminal hydrolase L1. NB: The table reflects the average cost, which in turn represents the expected cost. It is calculated by multiplying the cost of each event by its respective probability of occurrence. This approach offers a balanced overview of the real economic impact of each event, since some events that might be highly expensive have a low probability of occurrence. | |||
The estimated annual cost for managing patients with mild TBI in a standard hospital setting in Spain has been estimated at €3,145,712 for the current scenario in which CT is the standard tool for diagnosis. This cost falls to €2,449,078 when specific biomarkers GFAP and UCH-L1 are incorporated. This translates to an annual saving of €695,706 for the estimated 3,500 patients seen in EDs for mild TBI. The average cost per patient is €899 for the standard of care with CT, compared to €700 for specific biomarkers GFAP and UCH-L1, yielding a saving of €199.04 per patient.
3.2. Impact on Management Times
Taking into account the calculated times and the probabilities included in the decision tree, the estimated management time per TBI patient in Spain is 577 minutes (approximately 9.5 hours) in a routine clinical practice setting. When specific biomarkers GFAP and UCH-L1 are incorporated into the process, the time is reduced to 466 minutes (approximately 7.5 hours). This translates to an average savings of 111 minutes per patient, or 1 hour and 51 minutes.
3.3. Sensitivity Analysis
The parameters that most influence the savings generated by the addition of specific biomarkers GFAP and UCH-L1 are shown at the top of Figure 3. The variables with the greatest impact were the percentage of patients with positive results for specific biomarkers GFAP and UCH-L1 and the percentage of patients in whom these were measured. These variables proved to be the most sensitive for determining the savings generated by the use of specific biomarkers GFAP and UCH-L1, since small variations in these parameters led to significant changes in the cost difference between the 2 strategies (with and without biomarkers). Despite these variations, the results of the sensitivity analysis show that the use of specific biomarkers GFAP and UCH-L1 consistently generates economic savings compared to management based on the use of CT.
4. Discussion
The results suggest that testing for specific biomarkers GFAP and UCH-L1 during the evaluation of adult patients with GCS 13-15 in the first 12 hours after TBI could generate a significant reduction in costs, with annual savings per patient of €199.04. This saving may be explained by the reduction in the number of CTs performed, along with other factors, such as a reduced need for observation in the ED.
Other studies have also recently evaluated the use of biomarkers, although their results vary depending on the context and the methodologies used. In the United States, Ruan et al. (2009) [15] evaluated the economic impact of determining S-100B before CT in the management of adult patients with mild TBI. However, the authors do not report a reduction in hospital costs because the low specificity of this test in detecting abnormal intracranial lesions fails to generate significant savings ($281 versus $160). However, sensitivity analyses showed that the incorporation of this biomarker could result in savings if the percentage of patients undergoing CT is greater than 78%. Most recently, Zimmer et al. (2023) [18] evaluated the combined use of specific biomarkers GFAP and UCH-L1 versus CT in a French setting. Specifically, patients evaluated with specific biomarkers GFAP and UCH-L1 received fewer CTs (770.88 versus 1,096.30 per 1000 patients). These findings support the evidence that the use of biomarkers can optimize the management of mild TBI, although differences in care pathways and clinical practice between different healthcare systems can significantly influence the results obtained. The organizational structure, clinical protocols, and guidelines vary considerably depending on the healthcare context of each country, underlining the importance of adapting economic analyses to the specific national framework.
This study, based on the consensus published by SEMES and experts from 5 other scientific societies on the management of mild TBI [7], is the first to evaluate the economic impact of specific biomarkers GFAP and UCH-L1 in the Spanish setting. This is a significant and fundamental advance in optimizing decision-making by implementing efficient tool adoption in a setting marked by limited resources and increasing pressure on the healthcare system.
It is important to note that the adjustment made for the cost of the test, following the recommendations of the national experts, reflects an optimal scenario that might not necessarily be the case in laboratories with less specialized protocols. Factors such as frequency of use, number of controls required, and staff experience directly affect the real achievable test efficiency in the laboratory setting. These results should therefore be interpreted as the upper limit of efficiency in a highly optimized setting.
Nevertheless, sensitivity analysis shows that, despite variations in the most sensitive parameters, the savings generated by the use of this test remain consistent. These observations support the robustness of the model since the use of specific biomarkers GFAP and UCH-L1 remains a more economical strategy than standard management with CT.
This study has some limitations. The data were not obtained from a retrospective analysis based on clinical practice data. The incorporation of real clinical records in future studies would help validate the data used in this study, thus providing more accurate results, while also testing the hypotheses and robustness in real clinical practice. Economic savings could be greater if indirect costs, such as travel, waiting times, and losses in labor productivity, that were not included in this analysis, were taken into account. This clearly highlights the need for future studies that quantify these dimensions.
Another factor to bear in mind, as pointed out by some researchers (Ladang A., et.al; 2024) [19], is that a cut-off point adjusted to different age groups could influence the results of specific biomarkers GFAP and UCH-L1. However, additional studies are required to confirm this hypothesis. For now, the results of this study confirm that the incorporation of specific biomarkers GFAP and UCH-L1 testing could decrease the use of CT, resulting in a significant reduction in ED costs and management times in Spain.
5. Conclusions
This study suggests that the use of specific biomarkers GFAP and UCH-L1 in the management of patients with suspected mild TBI, according to the consensus of SEMES and experts from 5 other scientific societies, could not only generate significant direct economic savings but also optimize care times in a high-pressure care setting. Although this analysis has focused on the hospital setting, further studies should be performed to estimate the potential savings for the Spanish national health system, given the high prevalence of TBI.
Author Contributions
FMT conceived the idea for this study. FMT, GAC, EGP, DM-G, JOP, BMR, and FTR performed the study analysis and contributed equally to the interpretation of the results, preparation of the manuscript and revisions, and approval of the final manuscript. LSM provided support in the design and development of the economic model. All authors have read and agreed to the published version of the manuscript.
Funding
Abbott has facilitated the participation of an independent external consulting team to coordinate and energize all phases of the study. There has been no other funding for the development of this research.
Informed Consent Statement
Not applicable.
Data Availability Statement
The original contributions presented in this study are included in the article material. Further inquiries can be directed to the corresponding author(s).
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| GFAP | Glial fibrillary acid protein |
| UCH-L1 | Ubiquitin C-terminal hydrolase L1 |
| TBI | Mild traumatic brain injury |
| LD | Linear dichroism |
| BIA | Budget impact analysis |
| CT | Computed tomography |
| GCS | Glasgow Coma Scale |
| AII | Acute intracranial injury |
| ED | Emergency departments |
| SEMES | Spanish Society of Emergency Medicine |
| ICU | Intensive care unit |
| RCP | Routine clinical practice |
| MBDS | Minimum Basic Data Set |
| RECH | Spanish Network of Hospital Costs |
References
- Dewan MC, Rattani A, Gupta S, Baticulon RE, Hung YC, Punchak M; et al. Estimating the global incidence of traumatic brain injury. J Neurosurg. 2018;130(4):1080–97.
- Blennow K, Brody DL, Kochanek PM, Levin H, McKee A, Ribbers GM; et al. Traumatic brain injuries. Nat Rev Dis Primers. 2016;2(1):1–19.
- Maas A, Menon D, Adelson P, Andelic N, Bell M, Belli A; et al. Traumatic brain injury: Integrated approaches to improve prevention, clinical care, and research. Lancet Neurol. 2017;16(12):987–1048.
- Freire-Aragón MD, Rodríguez-Rodríguez A, José Egea-Guerrero J. Update in mild traumatic brain injury. Med Clin (Barc). 2017;149(3):122–7.
- Faisal M, Vedin T, Edelhamre M, Forberg JL. Diagnostic performance of biomarker S100B and guideline adherence in routine care of mild head trauma. Scand J Trauma Resusc Emerg Med. 2023 Dec 1;31(1).
- Su YS, Schuster JM, Smith DH, Stein SC. Cost-Effectiveness of Biomarker Screening for Traumatic Brain Injury. J Neurotrauma. 2019;36(13):2083–91.
- Temboury Ruiz F, Moya Torrecilla F, Ángel Arráez Sánchez M, Arribas Gómez I, Bártulos AV, José F; et al. Traumatismo craneoencefálico leve y biomarcadores de lesión cerebral aguda. Rev Esp Urg Emerg. 2024;3:31–6.
- Sierzenski PR, Linton OW, Amis ES, Courtney DM, Larson PA, Mahesh M; et al. Applications of justification and optimization in medical imaging: Examples of clinical guidance for computed tomography use in emergency medicine. Ann Emerg Med. 2014;11(1):36–44.
- Sharp AL, Nagaraj G, Rippberger EJ, Shen E, Swap CJ, Silver MA; et al. Computed Tomography Use for Adults With Head Injury: Describing Likely Avoidable Emergency Department Imaging Based on the Canadian CT Head Rule. Acad Emerg Med. 2017;24(1):22–30.
- Bazarian JJ, Welch RD, Caudle K, Jeffrey CA, Chen JY, Chandran R; et al. Accuracy of a rapid glial fibrillary acidic protein/ubiquitin carboxyl-terminal hydrolase L1 test for the prediction of intracranial injuries on head computed tomography after mild traumatic brain injury. Acad Emerg Med. 2021;28(11):1308–17.
- Sullivan SD, Mauskopf JA, Augustovski F, Jaime Caro J, Lee KM, Minchin M; et al. Budget impact analysis - Principles of good practice: Report of the ISPOR 2012 budget impact analysis good practice II task force. Value Health. 2014;17(1):5–14.
- Husereau D, Drummond M, Augustovski F, de Bekker-Grob E, Briggs AH, Carswell C; et al. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) 2022 Explanation and Elaboration: A Report of the ISPOR CHEERS II Good Practices Task Force. Value Health. 2022;25(1):10–31.
- López Bastida J, Oliva J, Antoñanzas F, García-Altés A, Gisbert R, Mar J; et al. Propuesta de guía para la evaluación económica aplicada a las tecnologías sanitarias. Gac Sanit. 2010 Mar;24(2):154–70.
- Bazarian JJ, Biberthaler P, Welch RD, Lewis LM, Barzo P, Bogner-Flatz V; et al. Serum GFAP and UCH-L1 for prediction of absence of intracranial injuries on head CT (ALERT-TBI): A multicentre observational study. Lancet Neurol. 2018;17(9):782–9.
- Ruan S, Noyes K, Bazarian JJ. The Economic Impact of S-100B as a Pre-Head CT Screening Test on Emergency Department Management of Adult Patients with Mild Traumatic Brain Injury. J Neurotrauma. 2009;26(10):1655–1654.
- Ministerio de Sanidad. Registro de Actividad de Atención Especializada. RAE-CMBD. Available from: https://www.sanidad.gob.es/estadEstudios/estadisticas/cmbdhome.htm.
- Grupo RECH. Red Española de Costes Hospitalarios (RECH). Available from: https://www.rechosp.org/faces/es/jsf/index.jsp.
- Zimmer L, McDade C, Beyhaghi H, Purser M, Textoris J, Krause A; et al. Cost-Effectiveness of Blood-Based Brain Biomarkers for Screening Adults with Mild Traumatic Brain Injury in the French Health Care Setting. J Neurotrauma. 2023;40(7–8):706–19.
- Ladang A, Vavoulis G, Trifonidi I, Calluy E, Karagianni K, Mitropoulos A; et al. Increased specificity of the “GFAP/UCH-L1” mTBI rule-out test by age dependent cut-offs. Clin Chem Lab Med. 2024;0.
Figure 1.
Scenario without the use of specific biomarkers GFAP and UCH-L1.
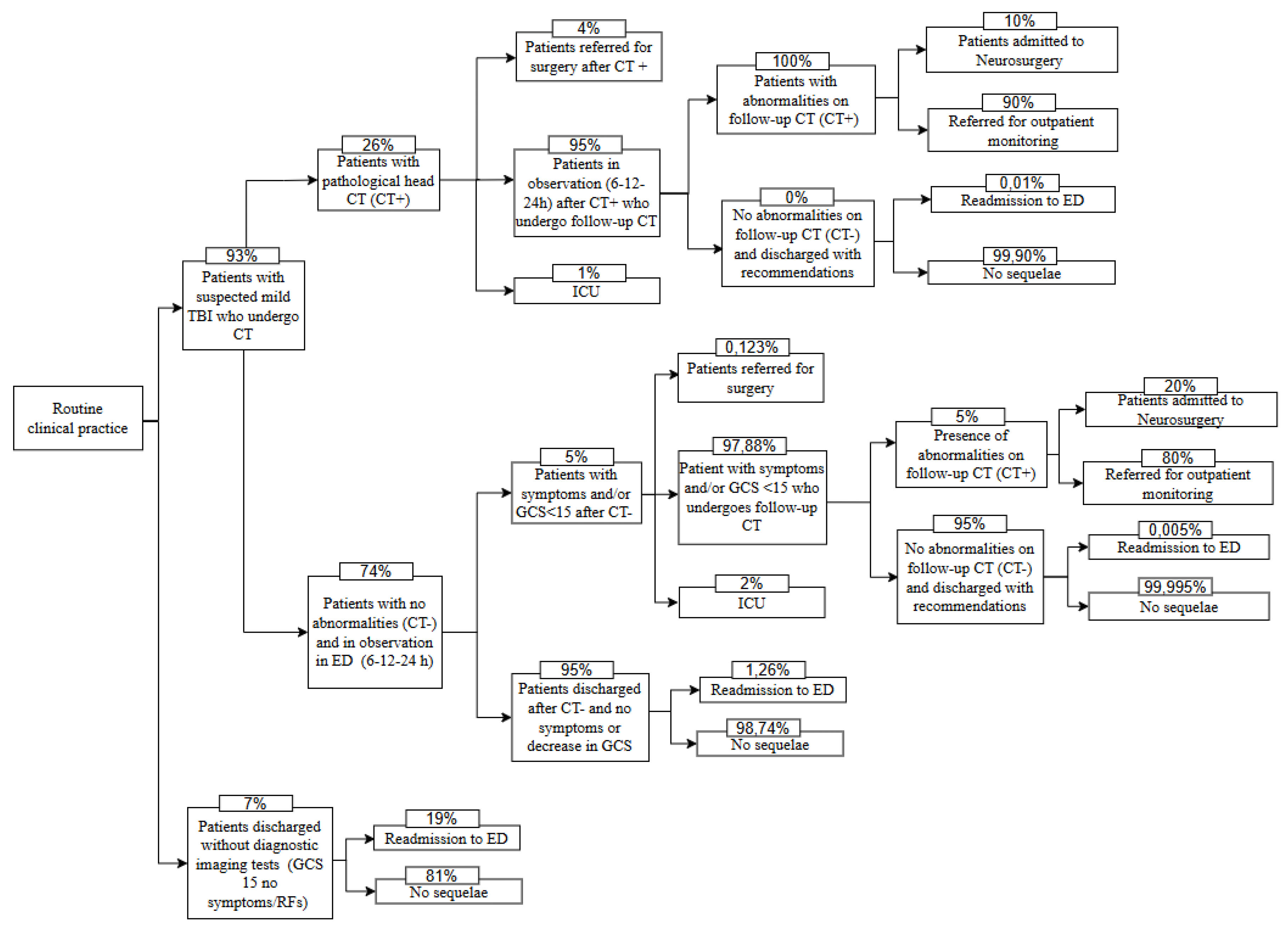
Figure 2.
Scenario using specific biomarkers GFAP and UCH-L1.
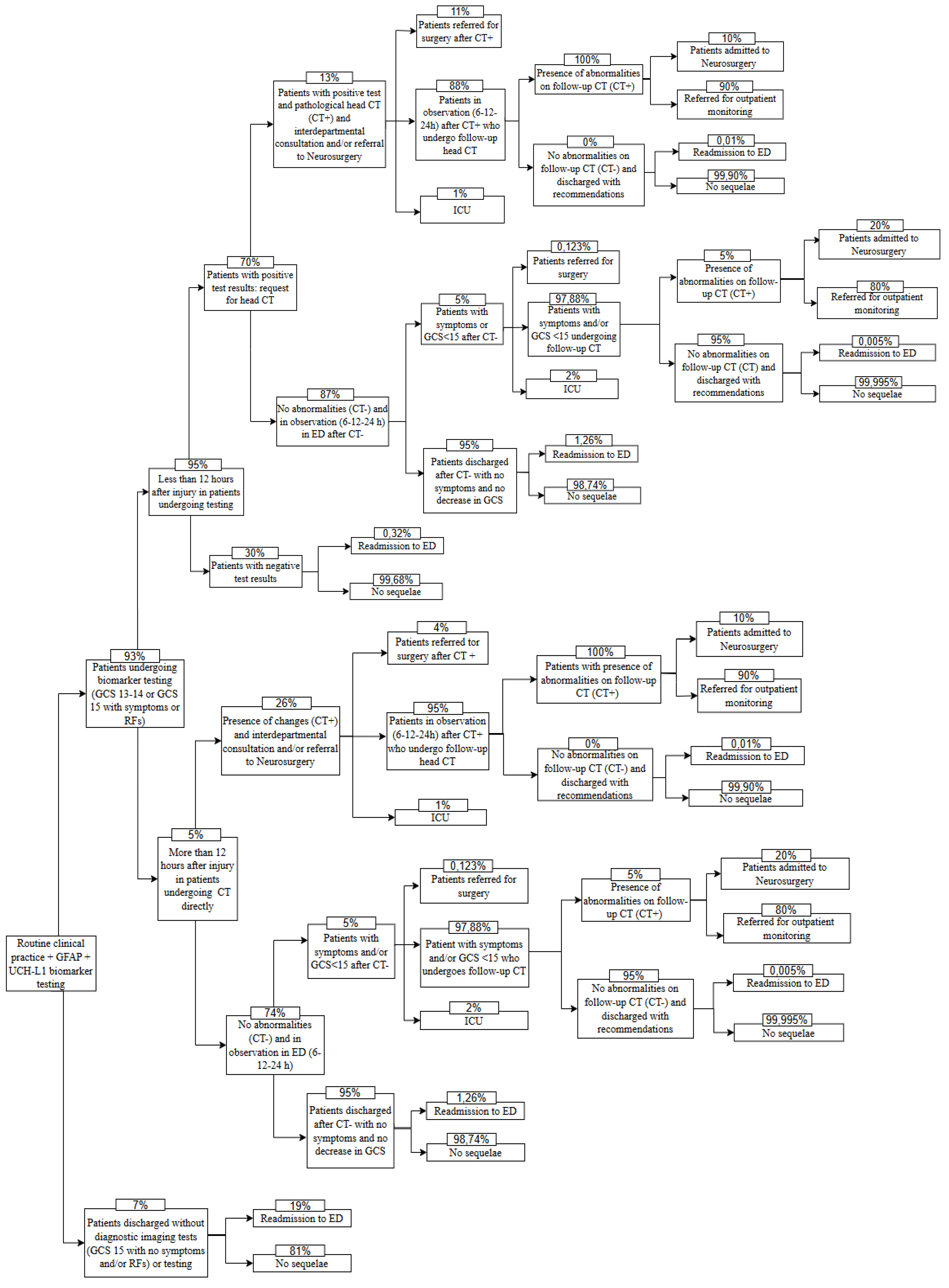
Figure 3.
Univariate sensitivity analysis. Impact of variables on cost difference.
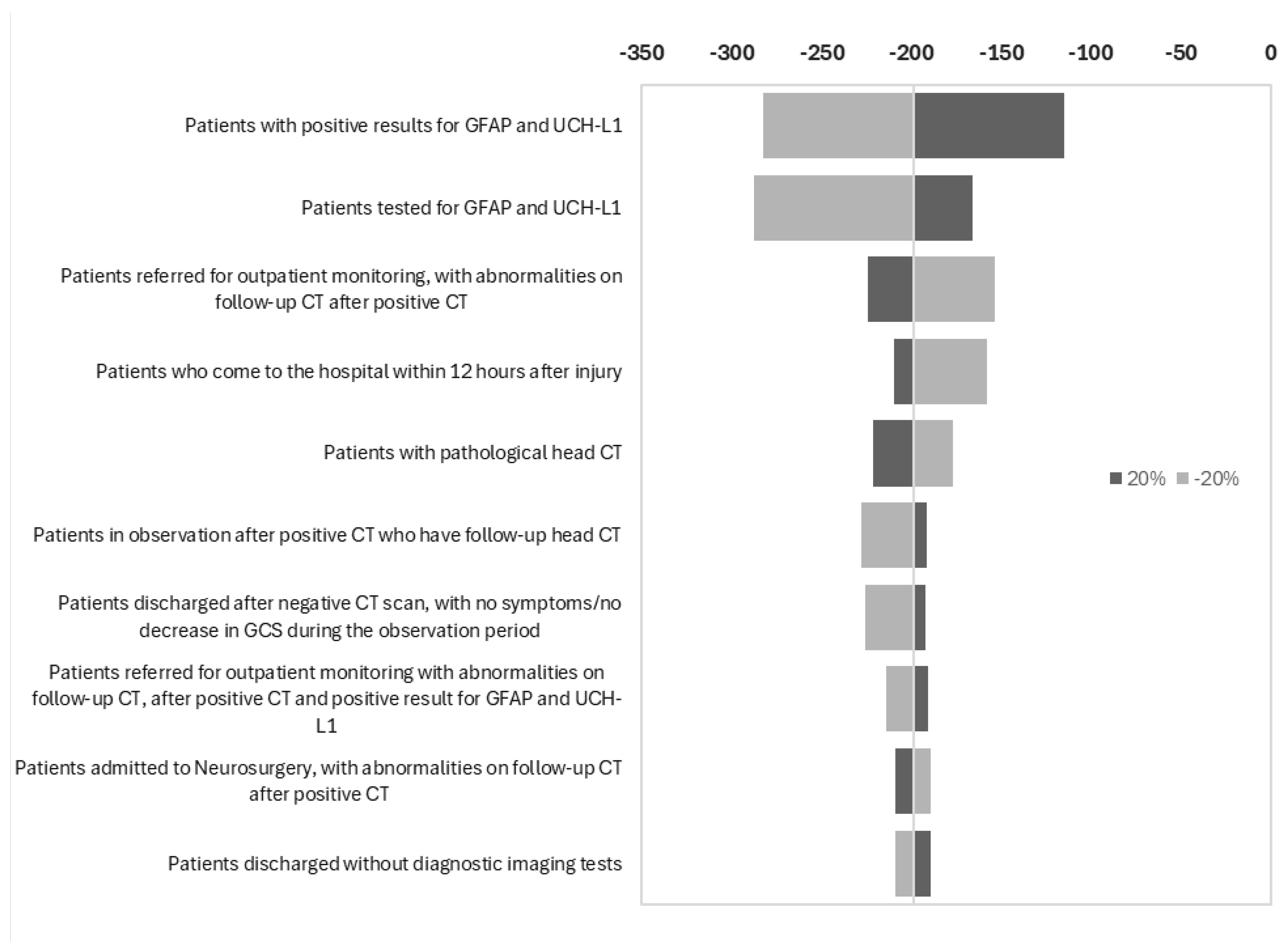
Table 1.
Clinical inputs used in budget impact analysis for patients with mild TBI.
| Description | Value (%) | Source |
|---|---|---|
| Patients discharged without diagnostic imaging tests* | 7.00 | RCP experience |
| Patients readmitted to the ED after discharge without any type of test | 19.00 | RCP experience |
| Patients with pathological head CT | 26.00 | RCP experience |
| Patients discharged after negative CT scan, no symptoms/no decrease in GCS during the observation period | 95.00 | RCP experience |
| Patients referred for surgery after negative CT but with symptoms/decrease in GCS | 0.123 | Ruan et al. (2009) [15] |
| Patients admitted to the ICU after negative CT, with symptoms/decrease in GCS | 2.00 | RCP experience |
| Symptomatic patients/GCS <15 who undergo follow-up CT after negative CT | 97.88 | -** |
| Patients with no abnormalities on follow-up CT and discharged after negative CT | 95.00 | RCP experience |
| Patients readmitted to the ED after negative CT | 1.26 | Ruan et al. (2009) [15] |
| Patients admitted to neurosurgery, with abnormalities on follow-up CT, after negative CT | 20.00 | RCP experience |
| Patients referred for outpatient monitoring, with abnormalities on follow-up CT, after negative CT | 80.00 | RCP experience |
| Patients readmitted to the ED, after negative follow-up CT and negative CT | 0.005 | Ruan et al. (2009) [15] |
| Patients referred for surgery after positive CT | 4.00 | RCP experience |
| Patients admitted to ICU after positive CT | 1.00 | RCP experience |
| Patients in observation after positive CT who have follow-up head CT | 95.00 | -** |
| Patients with abnormalities on follow-up CT, after positive CT | 100.00 | RCP experience |
| Patients admitted to Neurosurgery, with abnormalities on follow-up CT, after positive CT | 10.00 | RCP experience |
| Patients referred for outpatient monitoring, with abnormalities on follow-up CT, after positive CT | 90.00 | RCP experience |
| Patients readmitted to the ED, after positive CT and negative follow-up CT | 0.01 | Ruan et al. (2009) [15] |
| Patients tested for specific biomarkers GFAP and UCH-L1 | 93.00 | RCP experience |
| Patients who come to the hospital within 12 hours after sustaining injury | 95.00 | RCP experience |
| Patients with positive results for specific biomarkers GFAP and UCH-L1 | 70.00 | RCP experience |
| Patients with negative results for specific biomarkers GFAP and UCH-L1 readmitted to the ED | 0.32 | RCP experience |
| Patients with positive results for specific biomarkers GFAP and UCH-L1 and pathological head CT | 13.00 | RCP experience |
| Patients referred for surgery after positive CT and positive result for specific biomarkers GFAP and UCH-L1 | 11.00 | RCP experience |
| Patients admitted to the ICU after positive CT and positive result for specific biomarkers GFAP and UCH-L1 | 1.00 | RCP experience |
| Patients in observation after positive CT and positive result for specific biomarkers GFAP and UCH-L1 who undergo follow-up CT | 88.00 | -** |
| Patients with abnormalities on follow-up CT, after positive CT and positive result for specific biomarkers GFAP and UCH-L1 | 100.00 | RCP experience |
| Patients admitted to Neurosurgery with abnormalities on follow-up CT, after positive CT and positive result for specific biomarkers GFAP and UCH-L1 | 10.00 | RCP experience |
| Patients referred for outpatient monitoring with abnormalities on follow-up CT, after positive CT and positive result for specific biomarkers GFAP and UCH-L1 | 90.00 | RCP experience |
| Patients readmitted to the ED, after positive result for specific biomarkers GFAP and UCH-L1, positive CT and negative follow-up CT*** | 0.01 | Ruan et al. (2009) [15] |
| Patients with positive results for specific biomarkers GFAP and UCH-L1, with symptoms/decrease in GCS after observation period and negative CT | 5.00 | RCP experience |
| Patients readmitted to ED due to TBI, after negative CT and positive result for specific biomarkers GFAP and UCH-L1*** | 1.26 | Ruan et al. (2009) [15] |
| Patients referred for surgery after negative CT and positive result for specific biomarkers GFAP and UCH-L1, with symptoms/decrease in GCS after observation period*** | 0.123 | Ruan et al. (2009) [15] |
| Patients with mild TBI admitted to ICU after negative CT and positive result for specific biomarkers GFAP and UCH-L1, but with symptoms/decrease in GCS after the observation period | 2.00 | RCP experience |
| Patients with symptoms/GCS <15 undergoing follow-up CT after negative CT and positive result for specific biomarkers GFAP and UCH-L1 | 97.88 | -** |
| Patients with abnormalities on follow-up CT, after negative CT and positive result for specific biomarkers GFAP and UCH-L1 | 5.00 | RCP experience |
| Patients admitted to Neurosurgery with abnormalities on follow-up CT, after negative CT and positive result for specific biomarkers GFAP and UCH-L1 | 20.00 | RCP experience |
| Patients referred for outpatient monitoring with abnormalities on follow-up CT, after negative CT and positive result for specific biomarkers GFAP and UCH-L1 | 80.00 | RCP experience |
| Patients readmitted to the ED, after negative follow-up CT, and negative CT, with positive result for specific biomarkers GFAP and UCH-L1*** | 0.005 | Ruan et al. (2009) [15] |
| Abbreviations: CT, computed tomography; ED, emergency department; GCS, Glasgow Coma Scale; GFAP, glial fibrillary acid protein; ICU, intensive care unit; RCP, routine clinical practice; TBI, traumatic brain injury; UCH-L1, ubiquitin C-terminal hydrolase L1. *GCS 15 with no symptoms and/or risk factors. **The value of the third branch has been calculated as the difference between 100 and the sum of the 2 previous known values. ***For these variables, the data are based on the model published by Ruan et al. (2009), which uses S100B. In this analysis, this information has been extrapolated for application to GFAP and UCH-L1. It is acknowledged that these biomarkers have differences in specificity and kinetics, which could influence the results. | ||
Table 2.
Costs of procedures included in the BIA.
| Costs | Value (€) |
|---|---|
| Visit for outpatient monitoring | 167 |
| Hospital stay: admission to Neurosurgery | 1,240 |
| Admission to ICU | 857 |
| Neurosurgical intervention (operating room) | 1,740 |
| Repeat visit to ED | 215 |
| Observation in ED | 410 |
| Specific biomarkers GFAP and UCH-L1 | 32 |
| CT | 184 |
| Standard visit to ED | 215 |
| Abbreviations: CT, computed tomography; ED, emergency department; GFAP, glial fibrillary acid protein; ICU, intensive care unit; UCH-L1, ubiquitin C-terminal hydrolase L1. Source: Data from the autonomous community tariffs and Minimum Basic Data Set (MBDS). | |
Table 3.
Estimated time for each event included in the model.
| Description of the event | Minutes |
|---|---|
| Standard ED visit time (patients who do not require CT) | 98 |
| Time for request, preparation, transport, examination and interpretation of the CT | 156 |
| Mean time of observation in the emergency department for patients requiring observation | 319 |
| Mean response time of the laboratory performing the test | 43 |
| Abbreviations: CT, computed tomography; ED, emergency department | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



