
Submitted:
24 April 2025
Posted:
24 April 2025
You are already at the latest version
Abstract
Background and Objective:The aim of this study was to investigate the immediate effects of deep core muscle training in the plank position using the Icaros® system, integrated with virtual reality (VR), on selected posturographic parameters. Methods: To meet the stated objective, we utilized the Icaros® therapeutic system (Icaros GmbH, Martinsried, Germany) for VR-based exercise. Posturographic parameters were measured using the FootScan® force platform (Materialise Motion, Paal, Belgium). A representative sample of 30 healthy participants,13 females and 17 males (age: 22.5 ± 2.1 years; weight: 65 ± 2.9 kg; height: 1.68 ± 0.4 m; BMI: 23.04 ± 1.75) was included in the study. All participants had no prior experience with VR. The selected posturographic parameters were Ellipse Area (mm²) and Traveled Distance (mm), assessed four times at five-minute intervals following a 15-minute VR-based training session on the Icaros® system. Results: The results revealed that participants experienced a sense of instability after completing the 15-minute VR session, as objectively demonstrated by changes in the measured parameters. Both Ellipse Area and Traveled Distance showed a worsening trend during the first three measurements—immediately post-exercise, at 5 minutes, and at 10 minutes post-exercise. A downward trend was observed in the fourth measurement, taken 15 minutes after exercise. Statistically significant differences were found in both parameters: Ellipse Area (p = 0.000) and Traveled Distance (p = 0.000). Post-hoc analysis further confirmed significant differences between the time points. Conclusion: Based on the findings, it is recommended that trainers and physiotherapists supervising athletes or patients using the Icaros® VR system allow for a minimum rest period of 15 minutes in a seated or lying position following exercise. This recovery period appears essential to mitigate the sensation of instability and to reduce the risk of complications or injury due to potential falls.
Keywords:
virtual reality
; Icaros®
; deep muscle system
; posturography
1. Introduction
Postural stability is essential for maintaining balance and proper body biomechanics. It is influenced by several factors, including the function of the deep core muscle system, sensory integration, and motor control. In recent years, there has been a growing interest in innovative approaches in sports training, rehabilitation, and physiotherapy, with virtual reality emerging as one such method. This technology offers new opportunities for enhancing muscle activity and delivering therapeutic interventions through immersive therapy, which can effectively stimulate the deep core musculature. The deep core muscle system plays a crucial role in spinal stabilization and maintaining correct posture [1]. Dysfunction in this system may result in impaired balance, musculoskeletal pain, and an increased risk of falls [1,2,3]. Traditional methods of strengthening deep muscles include stabilization exercises, training on unstable surfaces, and proprioceptive training [4,5,6]. Novel technological solutions, such as VR, allow for a more interactive and potentially more effective approach to core training.
The interactive and immersive nature of virtual reality can enhance patient motivation and improve adherence to training or rehabilitation protocols [7]. VR technology enables users to experience presence within a computer-generated three-dimensional virtual environment so realistically that they may perceive it as being physically part of it [8,9]. Simulated environments created through VR can provide varying degrees of perceived realism and presence. The more realistic the virtual environment appears to the user, the more intense the immersive experience becomes. This experience depends on the number of physiological senses stimulated, the level of interaction with the virtual environment, and the degree of isolation from external stimuli, such as light or ambient noise [10].
In physiotherapy, VR has also proven to be an effective tool for managing acute pain [11]. In the treatment of chronic patients, it can be utilized for cognitive rehabilitation by applying principles of cognitive-behavioral therapy [12]. Furthermore, the positive effects of VR-based kinesiotherapy have been demonstrated in the re-education of balance skills and gait patterns in individuals diagnosed with multiple sclerosis, Parkinson’s disease, stroke, and spinal cord injuries [13,14,15,16].
Several studies have confirmed that exposure to virtual reality (VR) may induce VR sickness, characterized by symptoms such as nausea, disorientation, a sense of instability, and impaired balance [17]. According to current evidence, no studies have specifically investigated the effects of plank-position exercises in VR on the function of the deep core muscle system using the Icaros® device.
The aim of this study is to analyze the impact of deep core muscle activation during virtual reality exercise on selected posturographic parameters in healthy individuals immediately after training. This research explores the potential and applicability of VR in clinical practice, with findings that may contribute to a better understanding of the influence of VR on postural control. An additional motivation for conducting this study was the recurrent reports of instability and dizziness observed in previous clients following their first VR training session on the Icaros® system.
2. Materials and Methods
The present research is designed as an experimental study aimed at evaluating the immediate effect of exercise using the Icaros® system in a virtual reality environment on postural stability, thereby examining the influence of VR on postural control mechanisms.
2.1. Participants
The study sample consisted of 30 healthy participants, including 17 males and 13 females, with the following characteristics: age: 22.5 ± 2.1 years; weight: 65 ± 2.9 kg; height: 1.68 ± 0.04 m; and BMI: 23.04 ± 1.75. All participants were free of any medical conditions or coordination disorders that could have influenced the study outcomes. The selected participants were recreational athletes with no prior experience in VR-based exercise. Each participant received comprehensive information regarding the research objectives and measurement procedures. Prior to participation, all subjects voluntarily signed a written informed consent form. They were informed of their right to withdraw from the study at any time and assured that the data would be processed and published with full anonymity. The study was approved by the institutional ethics committee under approval number 02/2024. The research protocol was conducted in accordance with the principles of the Declaration of Helsinki and other applicable data protection regulations.
2.2. Measuring Protocol
To examine the effects of deep core muscle training using virtual reality, the intervention was conducted with the Icaros® virtual reality training and therapeutic system (Icaros GmbH, Martinsried, Germany). Posturographic parameters were assessed using the FootScan® pressure platform (Materialise Motion, Paal, Belgium). Both systems are non-invasive and pose no health risks to the participants. The research procedure consisted of two main components. The therapeutic phase involved participants activating their deep core muscle system to control the Icaros® device in a VR environment. Immediately following this, the diagnostic phase was conducted, in which posturographic parameters were measured and evaluated using the pressure platform. This allowed for assessment of the immediate impact of the VR-based intervention on postural control.
2.2.1. Icaros®
Icaros® is a modern and unique therapeutic device that combines core strengthening with virtual reality training (Figure 1). It is specifically designed to facilitate assisted, comprehensive training of the abdominal and back core zones, offering a wide range of training modalities that ensure both safety and high training efficacy. The system enables activation and simultaneous training of the core musculature along with other muscle groups using the so-called plank position, which is widely recognized as one of the most effective and essential positions for engaging the abdominal and spinal cord regions. The device allows therapists or trainers to create individualized programs tailored to each athlete or client, enabling the repeated application of targeted exercises based on specific issues or desired training goals. VR has a broad spectrum of applications in enhancing deep core stability (DCS) function in both athletes and the general population, as well as in pain management for the lumbar spine [8,9]. Moreover, it has shown potential in improving cognitive function in systemic neurological conditions such as multiple sclerosis [18], Parkinson’s disease [14], and others.
By adjusting the range of motion and reactivity levels of the device to different virtual scenarios, various levels of exercise difficulty can be implemented, thereby simulating an unstable environment that challenges multiple sensory modalities. The Icaros® system is characterized by a high safety standard, making it suitable even for relatively demanding training sessions for individuals without prior experience with this type of exercise. This unique combination allows for the execution of advanced exercises by users regardless of their previous training background.
2.2.2. Footscan®
The Footscan® pressure platform has been widely used in numerous studies for the objective assessment of foot function, gait analysis, and postural control. It provides quantitative data on plantar pressure distribution [19,20], posturographic parameters, and the projection of the centre of gravity onto the base of support [21,22], as well as gait cycle diagnostics [23].
In this study, we focused on the parameters Ellipse Area and Traveled Distance. The Ellipse Area (mm²) is defined as the area encompassing 95% of the Centre of Pressure (CoP) trajectory during foot-ground contact. This parameter is commonly used to evaluate postural stability and balance during standing or gait. A larger ellipse area typically indicates postural instability or impaired movement control, whereas a smaller area reflects better stability. Traveled Distance (mm) represents the total length of the CoP trajectory recorded during static or dynamic standing and gait assessments. Higher values may indicate inefficient postural control or compensatory movements to maintain balance. It is important to note that there are no universal normative values for these parameters, as they vary based on factors such as age, sex, physical fitness, and health status (Figure 1).
2.3. The Measurement Procedure
Data collection was conducted in the indoor facilities of the Faculty of Health Sciences, within the kinesiology laboratory of the Department of Physiotherapy, where both the therapeutic VR system Icaros® and the diagnostic Footscan® system are located. The controlled indoor environment provided uniform testing conditions for all participants. Due to the time-consuming nature of the measurements, data collection was carried out progressively throughout November 2024. The measurement procedure was as follows: upon arrival at the laboratory, each participant changed into comfortable sportswear. Participants received instructions on how to operate the Icaros® system, followed by individual calibration of the equipment, including a practical trial to determine the range of motion in all directions. The optimal position was established, with support under the forearms and lower legs, while the core remained unsupported. Virtual reality goggles were individually adjusted for clarity and comfort. After mastering the control of the Icaros® system, participants took a short break to rest and prepare for the 15-minute training session. During this break, participants were introduced to the scenario and virtual environment they would be navigating. The same standardized VR scenario was used for all participants. It involved a simulated flight experience in a mountainous setting (Dolomites), where the participant, controlling an avatar in a wingsuit, was required to fly through checkpoints, each associated with a score, thus serving as a motivational element to perform well. The VR flight session on the Icaros® system lasted 15 uninterrupted minutes. For added safety, the system was connected to an external monitor, allowing researchers to observe the participant’s VR experience and monitor the session in real time (Figure 2). Immediately after completing the 15-minute exercise, the goggles were removed, and the participant stepped directly onto the Footscan® pressure plate. The posturographic measurement began immediately and lasted for 30 seconds. During this time, the participant stood motionless in the centre of the platform, arms relaxed alongside the body, feet shoulder-width apart, and eyes open (Figure 3). This posturographic assessment was repeated three more times at 5-minute intervals. Thus, each participant underwent four measurements in total: immediately after the VR training, and then after 5, 10, and 15 minutes. Between each measurement, participants were not allowed to move freely and were required to remain seated on a chair. The same protocol was followed for all participants, and all data collection sessions proceeded without complications. Subjectively, most participants reported feelings of instability immediately after the VR session using the Icaros® system. The entire data collection process concluded with the fourth posturographic measurement, after which participants changed clothes and exited the laboratory.
2.4. Statistical Analysis
All numerical data were processed using the Statistica 13.3 software (Hamburg, Germany). The normality of data distribution was assessed using the Shapiro-Wilk test (Table 1). Based on the results of this normality testing, we selected appropriate statistical methods to evaluate the significance of differences between the measurements. For data with a normal distribution, repeated measures ANOVA was used. In cases where normality was violated, the non-parametric Friedman test was applied as an alternative. To perform a more detailed analysis and determine statistically significant differences between individual measurements, post-hoc tests were conducted. For normally distributed data, Tukey’s post-hoc test was used, while the Bonferroni correction was applied for data that did not meet the assumption of normality.
3. Results
By evaluating these parameters, we can demonstrate the impact of deep core muscle training on the Icaros® therapeutic device in virtual reality on motor stability and coordination of the body after therapy. These parameters were analyzed across the entire sample of participants and subsequently evaluated separately for males and females.
Table 2 presents the results of the statistical evaluation of the selected posturographic parameter Ellipse Area for all participants. The results indicate a deterioration of this parameter during the first, second, and third measurements. In the final measurement, taken 15 minutes after the completion of the therapy on the Icaros® VR system, a decrease in Ellipse Area values was observed. The results are supported by a statistically significant value (p ≤ 0.05), indicating a significant difference between the measurements. A graphical representation of the results is shown in Figure 4.
Table 3 presents the results of the post-hoc analysis for the Ellipse Area parameter. This analysis compares the individual measurements and evaluates statistically significant differences. Significant differences were observed when comparing the 1st, 2nd, and 3rd measurements with the 4th measurement. No statistically significant differences were found between the remaining measurements.
Table 4 provides the basic statistical evaluation of the Ellipse Area parameter in comparison between genders. The results indicate that the average values of this parameter are higher in males, suggesting that the male population may require a longer period to stabilize the observed parameters and reduce the sensation of instability.
Table 5 presents the results of the statistical evaluation of the selected posturographic parameter Traveled Distance for all participants. The values of this parameter showed a slight deterioration in the first three measurements, as demonstrated by the median values. Improvement and stabilization occurred in the fourth and final measurement, during which the participants also reported feeling subjectively more stable. The results are supported by a statistically significant value (p ≤ 0.05), indicating a significant difference between the measurements. A graphical representation of the results is provided in Figure 5.
Table 6 presents the results of the post-hoc analysis of the Traveled Distance parameter. This analysis compares individual measurements with each other and evaluates statistically significant differences observed when comparing the 1st, 2nd, and 3rd measurements with the 4th. No statistically significant differences were observed when comparing the other measurements with each other.
Table 7 provides the basic statistical evaluation of the Traveled Distance parameter when comparing men and women. The results suggest that the average values of this parameter are higher in men, which implies that the male population overall reacts to therapy with the Icaros® system in VR with worsened coordination.
4. Discussion
In this study, we tested the response of a healthy human organism to the Icaros® system combined with VR immediately after exercise, a study that has not yet been described. The statistical analysis of the obtained data confirmed that a 15-minute training session on this system significantly affects the coordination and stability of a healthy person, causing one of the symptoms of VR sickness. After completing the training on Icaros®, participants subjectively felt unstable, and this subjective assessment was confirmed by objective measurements on the pressure platform, which we performed four times with 5-minute breaks. Statistically significant differences were observed in both monitored parameters, Ellipse Area (p=0.000) and Traveled Distance (p=0.000) (Tab. 2, Tab. 5). In the detailed post-hoc analysis, which aimed to determine the differences between individual measurements, statistically significant differences were confirmed only when comparing the first, second, and third measurements with the fourth (Tab. 3, Tab. 6). Similar results were observed in studies that recorded changes in static balance after playing VR games with a fixed or non-fixed background, where significant deterioration in balance was observed [24]. In our study, the exercise was performed during a VR game with a non-fixed background, which may have contributed to the deterioration of stability after exercise.
A variety of VR systems are globally utilized, particularly in rehabilitation, sports, and fitness environments [25]. In rehabilitation, the primary focus is on neurorehabilitation for patients with neurological diagnoses (such as Multiple Sclerosis, Parkinson’s Disease, or Stroke), aimed at improving overall quality of life and cognitive functions in elderly patients [13,14,16,18,26]. Another major area where VR therapy is significantly utilized is in pain management [8,9,10,11,27]. Athletes use VR systems due to their broad range of gaming scenarios and experiences to enhance performance and as injury prevention [28,29]. The advantage lies in the numerous active sports games that VR offers, which can engage individuals and consequently improve their physical health [25,30,31,32]. VR tools were also employed during the global Covid-19 pandemic, where athletes used them for home training [33]. However, there are studies that provide various training plans [34,35] or reference systems and methodological frameworks [36] to prevent nausea, oculomotor deficits, disorientation, and VR sickness caused by using other VR systems [37]. These studies, however, yield conflicting results.
Virtual Reality (VR) sickness and its symptoms are most explained through two main theories: the sensory conflict theory and the postural instability theory. According to the sensory conflict theory, motion sickness occurs due to a conflict between visual perception and signals from the vestibular system, leading to perceptual mismatch [38]. On the other hand, the postural instability theory attributes the feeling of instability to difficulties in maintaining a stable body position [39]. Beginners in virtual reality are therefore more likely to experience VR sickness symptoms due to their lower ability to maintain a stable posture. Based on these theories, several studies have been conducted to alleviate VR-induced sickness, often through software solutions. One such approach involves visual effects. Groth et al. (2021) implemented techniques such as peripheral blur and narrowing of the field of view within the content, and experimental results confirmed their effectiveness in reducing VR sickness [40]. In a study by Nie et al. (2019), a dynamically changing blur effect was introduced in first-person perspective games, which, based on experimental data, proved to be an effective solution to reduce VR sickness [41]. Another study presents design elements aimed at alleviating cybersickness, such as movement styles, panel placement, laser use, and the background of panels [42].
The use of the Icaros® system combined with VR shows to be an effective approach for training and therapy of the deep muscular system. Furthermore, this training system significantly impacts the balance abilities and stability of healthy individuals immediately after the therapy. We hypothesize that the feeling of instability experienced by participants on the Icaros® system is due to a combination of factors, as described by the theories of VR sickness, such as the initial VR experience, the use of VR goggles, prolonged engagement in the plank position, and the exercise involved in controlling the Icaros® system. By engaging in the exercise on the Icaros® system in combination with VR, we influenced both components described in the theories of VR sickness symptoms. On one hand, the sensory component was affected using VR goggles, where the participants were exposed to multiple sensory stimuli that could impact the function of their vestibular system. On the other hand, participants remained in the plank position throughout the exercise, which required significant activity from the deep muscular system, thus influencing the second theory related to postural instability. The prolonged stay in the plank position subjected the deep muscular system to demanding conditions, as the recommended duration for holding this position for healthy individuals aged 18-25 years typically ranges from 60 to 100 seconds [43,44].
An important question that remains is how real patients with specific diagnoses would respond to a similar exercise routine on this system within a VR environment. Further research involving patients with neurological or musculoskeletal disorders, such as those with chronic low back pain, sciatica, or even post-stroke rehabilitation, would be necessary to determine whether the therapeutic effect seen in healthy individuals translates to clinical populations. Additionally, examining the adaptation process to the plank position and VR could help in designing tailored therapies for different patient groups.
5. Conclusions
In conclusion, we can state that after exercising on the Icaros® system in a VR environment, changes in motor control and imbalance occur. It is essential to allow clients who are using this system in VR for the first time to sit or lie down for at least 15 minutes after completing the training. The positive effects of VR therapy have been proven in both adult and paediatric patients with specific diagnoses or pain conditions. One of the significant advantages of VR is its ability to combine therapy or training with experiential therapy, which motivates athletes and patients to engage in repeated exercises. Another benefit is the ability to introduce the client to various gaming scenarios and virtual environments, where they have specific tasks or goals to achieve. In our study, we tested a specific deep muscular system therapy system, Icaros®, in a VR environment, assessing its impact on motor control and stability immediately after therapy in healthy individuals. We demonstrated its effect on the body's physiology, enabling us to use this therapy more effectively while also preventing falls or injuries that could arise from a loss of balance.
6. Limitations of the Study
One of the limitations of this study could be the participants' first experience with the Icaros® system and VR. Another limitation is the lack of reference values for the posturographic parameters being monitored, meaning we can only compare the changes in these parameters as a result of the therapy. The study also did not account for the participants' fatigue during the measurements. However, the therapy itself was not physically strenuous, and the fatigue experienced was considered acceptable. Another limitation is the absence of a control group and the sample size. To achieve broader generalizability, groups of 100 or more participants would be necessary. The results of this study are applicable to the population with characteristics described in the research sample section.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was approved by the institutional ethics committee of Faculty of Health Care under approval number 02/2024. The research protocol was conducted in accordance with the principles of the Declaration of Helsinki and other applicable data protection regulations.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Lederman, E. Mýty o stabilizačním systému. Rehabil. Fyz. Lék. 2008, 15, 63–73. [Google Scholar]
- Bačová, I.; Cicholesová, T.; Dziaková, M.; Šulla, I.; Kitka, M.; Petrovicová, J. Význam rehabilitácie hlbokého stabilizačného systému pri liečbe vertebrogénnych ochorení. Rehabilitácia, 2015, 52, 67–77. [Google Scholar]
- Kolář, P.; Lewit, K. Význam hlubokého stabilizačního system v rámci vertebrogenních obtíží. Neurol. praxi. 2005, 6, 270–275. [Google Scholar]
- Jebavý, R.; Baláš, J.; Jalovcová, M. Komparace silových cvičení na nestabilních a stabilních plochách jako prostředek pro zlepšení činnosti hlubokého stabilizačního systému. Rehabilitácia. 2016, 53, 85–93. [Google Scholar]
- Akuthota, V.; Nadler, S.F. Core strengthening. Arch. Phys. Med. Rehabil. 2004, 85, 86–92. [Google Scholar] [CrossRef]
- Pappas, E.; Panou, H.; Souglis, A. The effect of Pilates training on balance and falls of the elderly: A literature review. J. Phys. Educ. Sport. 2013, 13, 392–400. [Google Scholar]
- Hao, J.; Buster, T.; Cesar, G.; Burnfield, J. Virtual reality augments effectiveness of treadmill walking training in patients with walking and balance impairments: A systematic review and meta-analysis of randomized controlled trials. Clin. Rehabil. 2023, 37, 603–619. [Google Scholar] [CrossRef]
- Ahmadpour, N.; Randall, H.; Choksi, H.; Gao, A.; Vaughan, C.; Poronnik, P. Virtual Reality interventions for acute and chronic pain management. Int. J. Biochem. Cell Biol. 2019, 114, 105568. [Google Scholar] [CrossRef]
- Pourmand, A.; Davis, S.; Marchak, A.; Whiteside, T.; Sikka, N. Virtual reality as a clinical tool for pain management. Curr. Pain Headache Rep. 2018, 22, 53. [Google Scholar] [CrossRef]
- Gumaa, M.; Rehan, Y.A. Is virtual reality effective in orthopedic rehabilitation? A systematic review and meta-analysis. Phys. Ther. Rehabil. J. 2019, 99, 1304–1325. [Google Scholar] [CrossRef]
- Mallari, B.; Spaeth, E.K.; Goh, H.; Boyd, B.S. Virtual reality as an analgesic for acute and chronic pain in adults: A systematic review and meta-analysis. J. Pain Res. 2019, 12, 2053–2085. [Google Scholar] [CrossRef]
- Bahat, S.H.; Takasaki, H.; Chen, X.; Bet-Or, Y.; Treleaven, J. Cervical kinematic training with and without interactive VR training for chronic neck pain - a randomized clinical trial. Man. Ther. 2015, 20, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Booth, V.; Masud, T.; Connell, L.; Bath-Hextall, F. The effectiveness of virtual reality interventions in improving balance in adults with impaired balance compared with standard or no treatment: a systematic review and meta-analysis. Clin. Rehabil. 2013, 28, 419–431. [Google Scholar] [CrossRef]
- Wang, B.; Shen, M.; Wang, Y.; He, Z.; Chi, S.; Yang, Z. Effect of virtual reality on balance and gait ability in patients with Parkinson’s disease: a systematic review and meta-analysis. Clin. Rehabil. 2019, 33, 1130–1138. [Google Scholar] [CrossRef] [PubMed]
- Libak, A.; Malala, V.D.; Yarnot, R.; Alluri, A.; Rice, L.A. Effects of virtual reality therapy on gait and balance among individuals with spinal cord injury: a systematic review and meta-analysis. Neurorehabil. Neural Repair. 2020, 34, 375–388. [Google Scholar]
- Zhen, L.; Xiu-Guo, H.; Jing, S.; Shao-Jun, M. Virtual reality for improving balance in patients after stroke: A systematic review and meta-analysis. Clin. Rehabil. 2015, 30, 432–440. [Google Scholar]
- Gemert van, T.; Nilsson, N.Ch.; Hirzle, T.; Bergström, J. Sicknificant Steps: A Systematic Review and Meta-analysis of VR Sickness in Walking-based Locomotion for Virtual Reality. In CHI '24: Proceedings of the 2024 CHI Conference on Human Factors in Computing Systems, Honolulu, Hawai, USA, 11.-16. May; Mueller, F.F., Kyburz, P., Williamson, J.R., Sas, C., Wilson, M.L., Dugas, P.T., Shklovski, I., Eds.; Association for Computing Machinery: New York, NY, United States, 2024; 632, pp. 1–36. [Google Scholar]
- Casuso-Holgado, M.J.; Martín-Valero, R.; Carazo, A.F.; Medrano-Sánchez, E.M.; Cortés-Vega, M.D.; Montero-Bancalero, F.J. Effectiveness of virtual reality training for balance and gait rehabilitation in people with multiple sclerosis: a systematic review and meta-analysis. Clin. Rehabil. 2018, 32, 1220–1234. [Google Scholar] [CrossRef]
- He, Y.J.; Zheng, X.L.; Wang, D.F.; Mu, Z.Z.; Li, G.Y.; Fang, Z.Z.; Fei, W.; Huan, K. Static and dynamic plantar pressure distribution in 94 patients with different stages of unilateral knee osteoarthritis using the footscan platform system: an observational study. Med. Sci. Monit. 2023, 12, 938485. [Google Scholar] [CrossRef]
- Xu, C.; Wen, X.X.; Huang, L.Y.; Shang, L.; Cheng, X.X.; Yan, Y.B.; Lei, W. Normal foot loading parameters and repeatability of the Footscan platform system. J. Foot Ankle Res. 2017, 10, 30. [Google Scholar] [CrossRef]
- Eo, H.; Park, D.; Jun, K.; Woo, S.; Koo, W.M.; Kim, J.M.; Lee, B.J.; Chang, M.C. Comparison of travel distance of center of pressure using the footscan system in individuals with and without flatfoot. J. Back Musculoskelet. Rehabil. 2025, 0, 1–6. [Google Scholar] [CrossRef]
- Jun, K.; Eo, H.; Koo, W.M.; Woo, S.; Lee, J.; Kim, J.M.; Lee, B.J.; Nam, T.W. Long-term changes of standing balance after lateral ankle sprain using Footscan system: A case report. Medicine (Baltimore). 2023, 102, 36058. [Google Scholar] [CrossRef]
- Wang, Z.; Mao, X.; Guo, Z.; Zhao, R.; Feng, T.; Xiang, C. Comparison of walking quality variables between end-stage osteonecrosis of femoral head patients and healthy subjects by a footscan plantar pressure system. Medicina (Kaunas). 2023, 59, 59. [Google Scholar] [CrossRef]
- Park, S.; Lee, G. Full-immersion virtual reality: Adverse effects related to static balance. Neurosci. Lett. 2020, 733, 134974. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.G.; Wang, X.; Li, P.; Jung, Y.; Bi, L. A systematic review: Virtual-reality-based techniques for human exercises and health improvement. Front. Public Health. 2023, 11, 1143947. [Google Scholar] [CrossRef]
- Maheta, B.; Kraft, A.; Interrante, N.; Fereydooni, S.; Bailenson, J.; Beams, B.; Keny, C.; Osborne, T.; Giannitrapani, K.; Lorenz, K. Using virtual reality to improve outcomes related to quality of life among older adults with serious illnesses: systematic review of randomized controlled trials. J. Med. Internet Res. 2025, 27, 54452. [Google Scholar] [CrossRef] [PubMed]
- Manca, O.; Kozinc, Ž.; Ivezic, D. Effects of virtual reality on pain, disability and kinesiophobia in patients with chronic low back pain: A systematic review with meta-analysis. Physiotherapy Practice and Research. 2024, 45, 107–132. [Google Scholar]
- Mohamed, Z.; Ngali, M.Z.; Sudin, S.; Ibrahim, M.F.; Casson, A. Proceedings of the 2nd International Conference on Innovation and Technology in Sports, ICITS 2023; Springer: Heidelberg, Germany, 2023. [Google Scholar]
- Cmentowski, S.; Karaosmanoglu, S.; Nacke, L.E.; Steinicke, F.; Krüger, J.H. Never skip leg day again: training the lower body with vertical jumps in a virtual reality exergame. In CHI '23: Proceedings of the 2023 CHI Conference on Human Factors in Computing Systems, Hamburg, Germany, 23.-28. April; Schmidt, A., Väänänen, K., Goyal, T., Kristensson, P.O., Peters, A., Mueller, S., Williamson, J.R., Wilson, M.L., Eds.; Association for Computing Machinery: New York, NY, United States, 2023; 786, pp. 1–18. [Google Scholar]
- Hu, Z. Virtual reality-based cooperative learning in physical education: ways to improve physical performance and motivation of students. Int. J. Hum-Comput. Int. 2023, 41, 242–253. [Google Scholar] [CrossRef]
- Schmidt, S.; Ehrenbrink, P.; Weiss, B.; Voigt-Antos, JN.; Kojic, T.; Johnston, A.; Möller, S. Impact of virtual environments on motivation and engagement during exergames. Tenth International Conference on Quality of Multimedia Experience (QoMEX), Cagliari, Italy, 29. May-01. June; IEEE: Piscataway, United States, 2018; p. 8463389. [Google Scholar]
- Debska, M.; Polechonski, J.; Mynarski, A.; Polechonski, P. Enjoyment and intensity of physical activity in immersive virtual reality performed on innovative training devices in compliance with recommendations for health. Int. J. Environ. Res. Public Health. 2019, 16, 3673. [Google Scholar] [CrossRef]
- Washif, J.A.; Hettinga, F.J.; Ammar, A.; van Resburg, D.Ch.J.; Materne, O.; Trabelsi, K.; Romdhani, M.; Farooq, A.; Pyne, D.B.; Chamari, K. Supporting athletes during a challenging situation: recommendations from a global insight of COVID-19 home-based training experience. BMC Sports Sci. Med. Rehabil. 2024, 16, 83. [Google Scholar] [CrossRef]
- Won, J.; Na, Ch.H.; Kim, Y.S. A New Training Method for VR Sickness Reduction. Appl. Sci. 2024, 14, 3485. [Google Scholar] [CrossRef]
- Chang, E.; Kim, H.T.; Yoo, B. Virtual Reality Sickness: A Review of Causes and Measurements. Int. J. Hum-Comput. Int. 2020, 36, 1658–1682. [Google Scholar] [CrossRef]
- Rouhani, R.; Umatheva, N.; Brockerhoff, J.; Keshavarz, B.; Kruijff, E.; Gugenheimer, J.; Riecke, B.E. Towards benchmarking VR sickness: A novel methodological framework for assessing contributing factors and mitigation strategies through rapid VR sickness induction and recovery. Displays. 2024, 84, 102807. [Google Scholar] [CrossRef]
- Dopsaj, M.; Tan, W.; Perovic, V.; Stajic, Z.; Milosavljevic, N.; Paessler, S.; Makishima, T. Novel neurodigital interface reduces motion sickness in virtual reality. Neurosci. Lett. 2024, 825, 137692. [Google Scholar] [CrossRef] [PubMed]
- LaViola, J.J.; Joseph, J. A discussion of cybersickness in virtual environments. ACM Sigchi Bull. 2000, 32, 47–56. [Google Scholar] [CrossRef]
- Riccio, G.E.; Stoffregen, T.A. An ecological theory of motion sickness and postural instability. Ecol. Psychol. 1991, 3, 195–240. [Google Scholar] [CrossRef]
- Groth, C.; Tauscher, J.P.; Heesen, N.; Castillo, S.; Magnor, M. Visual techniques to reduce cybersickness in virtual reality. In Proceedings of the 2021 IEEE Conference on Virtual Reality and 3D User Interfaces Abstracts and Workshops, Lisbon, Portugal, 27 March–1 April 2021; pp. 486–487. [Google Scholar]
- Nie, G.Y.; Duh, H.B.L.; Liu, Y.; Wang, Y. Analysis on mitigation of visually induced motion sickness by applying dynamical blurring on a user’s retina. IEEE Trans. Vis. Comput. Graph. 2019, 26, 2535–2545. [Google Scholar] [CrossRef]
- Jang, W.J.; Bae, J.H.; You, H.B.; Bak, S.H. Content Design Research to Improve Motion Sickness in Extended Reality (XR). Digit. Contents Soc. 2024, 25, 49–55. [Google Scholar]
- Chase, K.A.; Brigham, C.E.; Peterson, J.T.; Coste, S.C. Fitness norms for the plank exercise. Int. J. Exerc. Sci. 2014, 8. [Google Scholar]
- Aleais, D.S.; Sullivan, K.; Ferreira, P.; Marchetti, P.N.; Marchetti, P. H. Acute dose-response of duration during the plank exercise on muscle thickness, echo-intensity, peak force, and perception of effort in recreationally-trained participants. Int. J. Exerc. Sci. 2014, 15, 676–685. [Google Scholar]
Figure 1.
Posturographic Diagnostics - Ellipse Area and Traveled Distance.
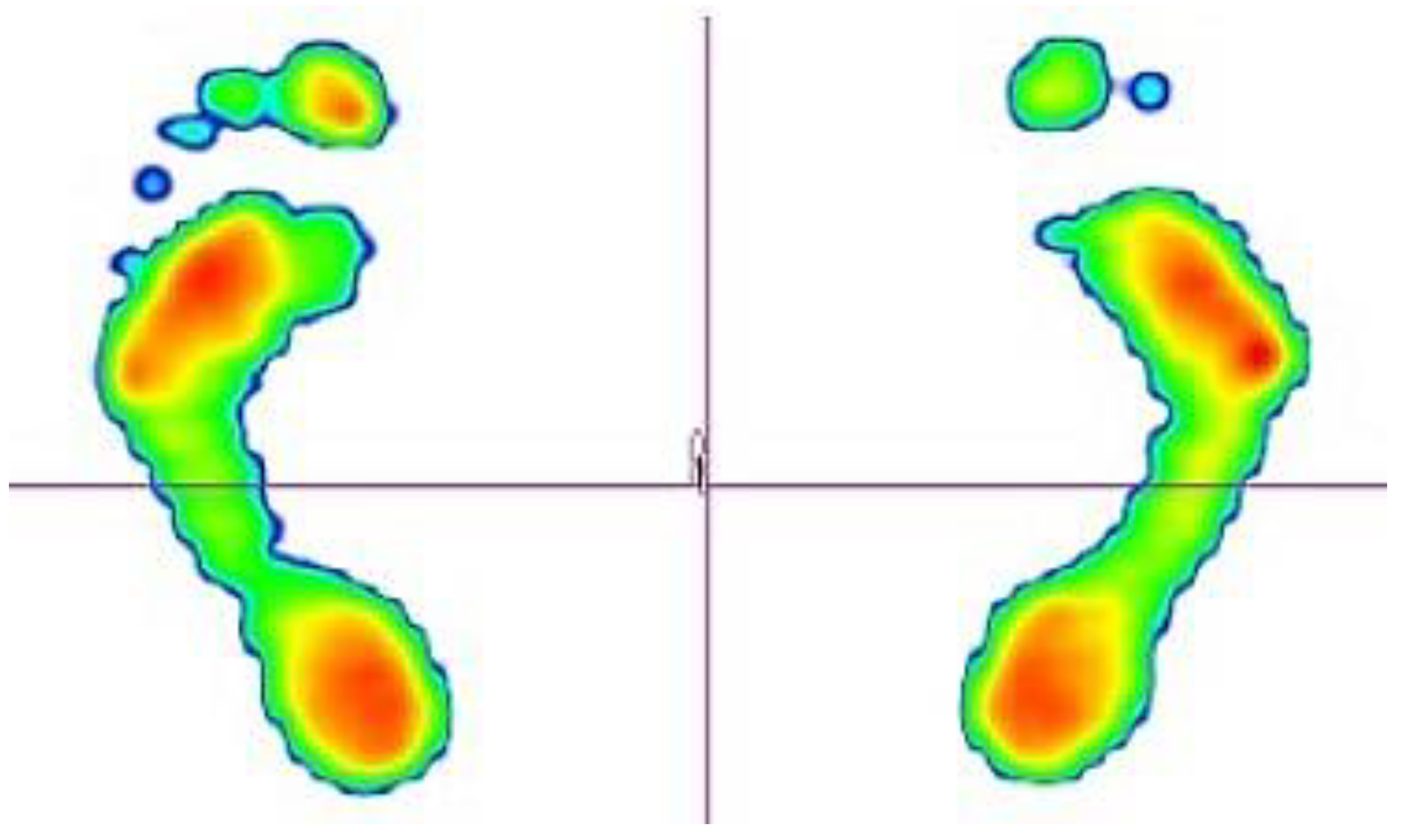
Figure 2.
Therapy on Icaros® in VR environment.

Figure 3.
Footscan® measurement.
Figure 4.
Graphical representation of the average Ellipse Area values of all participants across individual measurements.
Figure 4.
Graphical representation of the average Ellipse Area values of all participants across individual measurements.
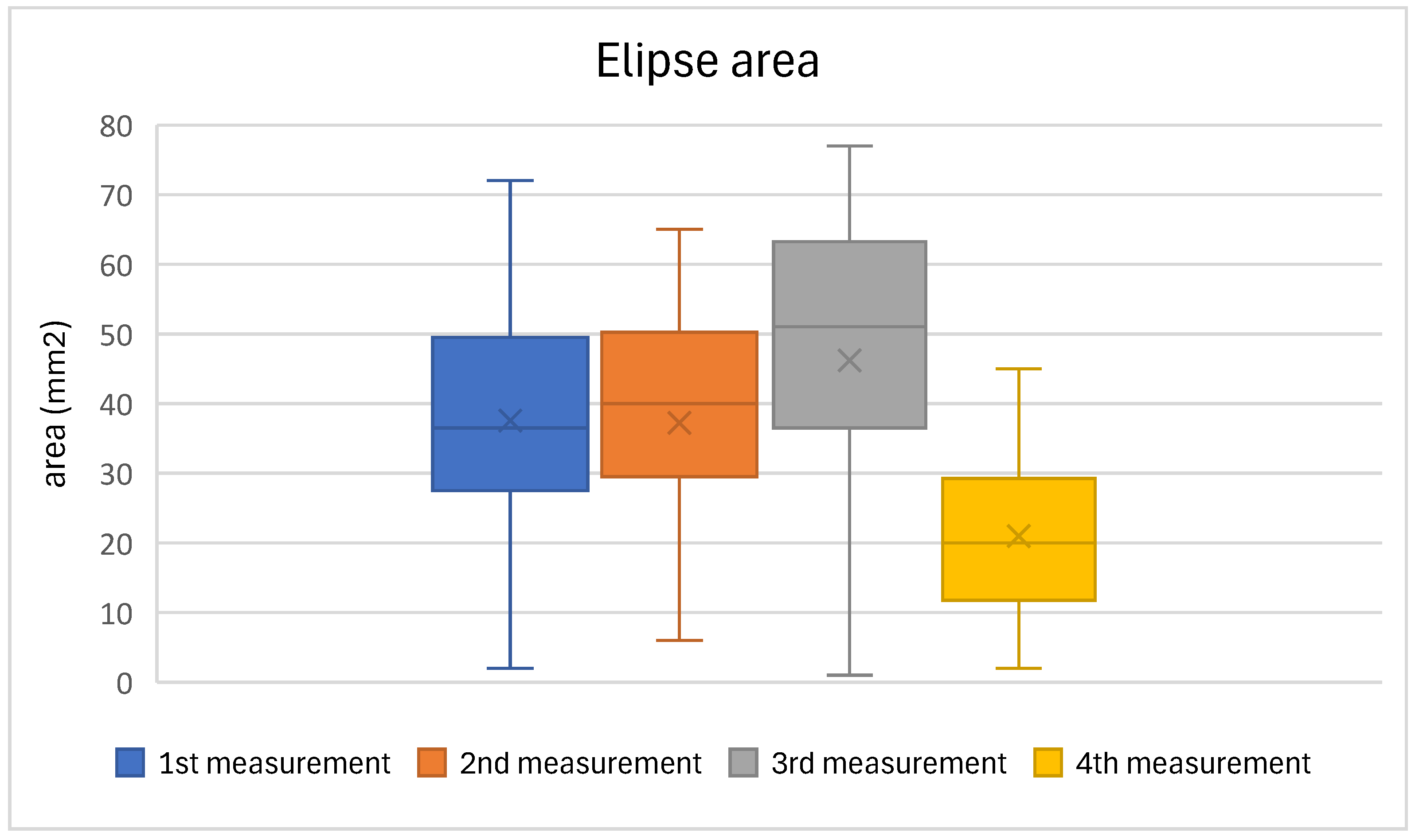
Figure 5.
Graphical representation of the mean Traveled Distance values of all participants in individual measurements.
Figure 5.
Graphical representation of the mean Traveled Distance values of all participants in individual measurements.
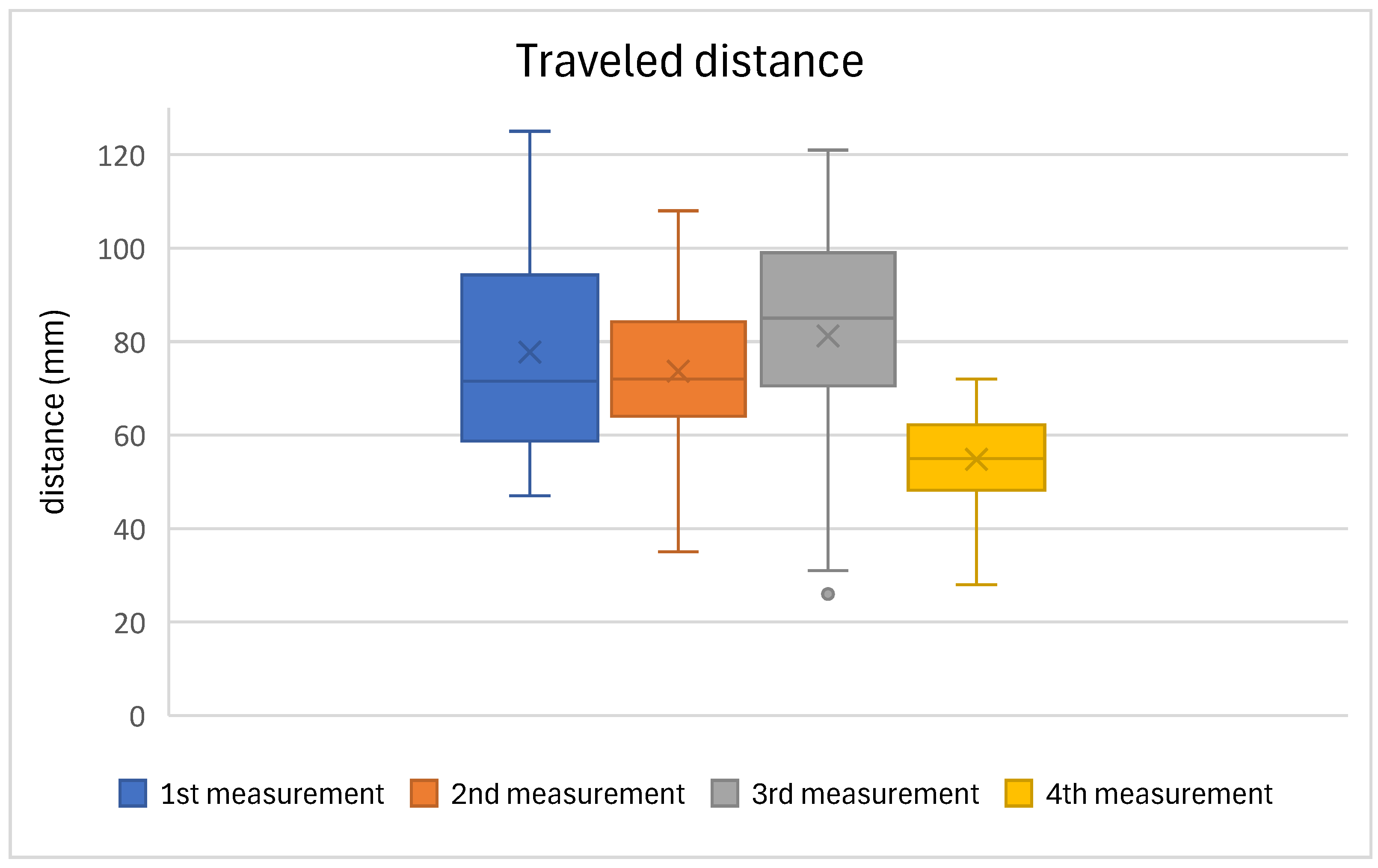

Table 1.
Data normality testing results.
| n = 30 | Ellipse area (mm2) | Traveled distance (mm) | ||
|---|---|---|---|---|
| 1. measurement | p = 0.951 | normality confirmed | p = 0.023 | normality unconfirmed |
| 2. measurement | p = 0.119 | normality confirmed | p = 0.964 | normality confirmed |
| 3. measurement | p = 0.094 | normality confirmed | p = 0.456 | normality confirmed |
| 4. measurement | p = 0.320 | normality confirmed | p = 0.475 | normality confirmed |
Table 2.
Results of post urography evaluation (ellipse area mm2) of all participants.
| Ellipse area (mm2); n = 30 | ||||
|---|---|---|---|---|
| measurements | 1st | 2nd | 3rd | 4th |
| average | 37,5 | 37,2 | 46,2 | 20,9 |
| median | 36,5 | 40 | 51 | 20 |
| max | 72 | 65 | 77 | 45 |
| min | 2 | 6 | 1 | 2 |
| sd | 16,6 | 16,9 | 20,6 | 11,9 |
| pvalue | 0,000 | |||
| F value | 11,38 | |||
Table 3.
Results of post-hoc test of Elipse area.
| Compared measurements | p value |
|---|---|
| 1. measurement vs. 4. measurement | 0,001 |
| 2. measurement vs. 4. measurement | 0,002 |
| 3. measurement vs. 4. measurement | 0,001 |
Table 4.
Comparison of ellipse area (mm2) results between men and women.
| women | men | |||||||
|---|---|---|---|---|---|---|---|---|
| measurements | 1st | 2nd | 3rd | 4th | 1st | 2nd | 3rd | 4th |
| average | 39,3 | 34,1 | 36,6 | 13,6 | 36,2 | 39,5 | 53,4 | 26,5 |
| median | 44 | 35 | 38 | 12 | 36 | 40 | 55 | 25 |
| max | 72 | 63 | 71 | 30 | 62 | 65 | 77 | 45 |
| min | 2 | 6 | 1 | 2 | 7 | 10 | 15 | 4 |
| sd | 19,2 | 19,8 | 22, 5 | 7,9 | 14,2 | 13,7 | 15,4 | 11,4 |
Table 5.
Results of posturography evaluation (traveled distance) of all participants.
| Traveled distance (mm); n=30 | ||||
|---|---|---|---|---|
| measurements | 1st | 2nd | 3rd | 4th |
| average | 77,8 | 73,6 | 81,2 | 54,8 |
| median | 71,5 | 72 | 85 | 55 |
| max | 125 | 108 | 142 | 72 |
| min | 47 | 35 | 26 | 28 |
| sd | 21,4 | 16,2 | 26,2 | 10,3 |
| pvalue | 0,000 | |||
| Test statistic value | 46,52 | |||
Table 6.
Results of post-hoc test of Traveled distance.
| Compared measurements | p value |
|---|---|
| 1. measurement vs. 4. measurement | 0,000 |
| 2. measurement vs. 4. measurement | 0,002 |
| 3. measurement vs. 4. measurement | 0,000 |
Table 7.
Comparison of traveled area results between men and women.
| women | men | |||||||
|---|---|---|---|---|---|---|---|---|
| measurements | 1st | 2nd | 3rd | 4th | 1st | 2nd | 3rd | 4th |
| average | 85,1 | 70,3 | 65,7 | 49,7 | 72,1 | 76,2 | 93,1 | 58,7 |
| median | 85 | 70 | 66 | 52 | 66 | 75 | 89 | 61 |
| max | 125 | 105 | 121 | 64 | 125 | 108 | 142 | 72 |
| min | 47 | 35 | 26 | 28 | 54 | 51 | 74 | 44 |
| sd | 23,8 | 17,7 | 28,4 | 10,6 | 17,4 | 14,4 | 16,4 | 8,2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



