
Submitted:
11 March 2025
Posted:
12 March 2025
You are already at the latest version
Abstract
Introduction: Antimicrobial resistance (AMR) is an urgent global public health problem. It threatens effective treatment of infections and leads to prolonged duration of illness, higher morbidity and mortality rates, and an increased cost of health care. The effectiveness of currently available antibiotics is decreasing as a result of increasing resistant strains among clinical isolates. Objective: The aim of this study was to determine the bacterial profile and AMR patterns of bacterial isolates from different clinical specimens at Uttara Adhunik Medical College Hospital (UAMCH), Dhaka. Material and methods: This retrospective study was carried out at UAMCH in Bangladesh from January 2017 to December 2019. In total 32,187 clinical specimens such as urine, blood, stool, wound swab/pus, and sputum were collected and processed at the Microbiology laboratory. Among these, 4232 were positive culture samples. Standard bacteriological methods were employed to identify the bacteria, and Kirby-Bauer disc diffusion methods were used in accordance with CLSI guidelines to assess the bacteria's susceptibility to various antibiotics. Data were entered, cleaned, and analyzed using the WHONET software developed by the WHO Collaborating Centre for Surveillance of Antimicrobial Resistance and the Quick Analysis of Antimicrobial Patterns and Trends (QAAPT) web application. Result: Urine had the highest percentage of positive cultures (47.5%, n=2009), followed by blood (35%, n=1500), wound swab/pus (10.1%, n=426) and sputum (5.3%, n=225). Among positive samples, E. coli was the most frequent isolate accounting for 37.19% (1574) of specimens, followed by Salmonella typhi (25.73%, n=1089), Klebsiella sp. (11.51%, n=487), Salmonella paratyphi A (6.38%, n=270), Staphylococcus aureus (4.21%, n=178), and Enterobacter sp. (3.59%, n=152). Overall, the Gram-negative isolates exhibited a high level of resistance to commonly used antibiotics such as amoxicillin/clavulanic acid, cefixime, and ceftriaxone. The resistance rate was lower in case of gentamicin, amikacin, and meropenem; however, Acinetobacter sp. showed a higher and alarming resistance rate against all antibiotics. Conclusion: This study exposes the antibiotic resistance patterns of bacterial isolates to routinely used antibiotics. The outcomes of this study will assist healthcare professionals in Bangladesh and the area in making informed decisions and providing better care to their patients. Therefore, resistance surveillance studies should be conducted to develop local antibiogram data, which will help to choose the best antibiotic for empirical therapy.
Keywords:
Antibiogram
; antimicrobial susceptibility testing
; antimicrobial resistance
; QAAPT
; WHONET
1. Introduction
Antimicrobials are medicines used to treat infections or diseases which are essential in both human and animal health. Antimicrobial resistance (AMR) occurs when microorganisms change over time and no longer respond to medicines, making infections harder to treat and increasing the risk of severe illness and death [1]. The development of resistance among microorganisms or ‘superbugs’ is a natural phenomenon that will inevitably occur when antimicrobials are used to treat disease [1]. Antimicrobial resistance, especially resistance to antibiotics, has emerged as one of the leading public health threats of the 21st century [1]. Infections caused by resistant bacteria adversely affect treatment outcomes, costs, disease spread and duration of illnesses, posing a serious challenge to future chemotherapies [2].
The World Health Organization (WHO) declared antimicrobial resistance as one of the serious health threats at the global level. Globally, AMR is believed to cause approximately 700,000 deaths per year [6]. In 2019, a total of 4.95 million casualties were associated with AMR, out of which 1.27 million deaths occurred due to bacterial AMR in the world and the six leading pathogens for deaths associated with resistance were Escherichia coli, followed by Staphylococcus aureus, Klebsiella pneumoniae, Streptococcus pneumoniae, Acinetobacter baumannii, and Pseudomonas aeruginosa [7]. It is estimated that failing to tackle AMR could cause 10 million deaths every year by 2050 [6].
The AMR problem is challenging in developing countries because of the widespread misuse of antibiotics, non-human antibiotic use, poor quality of drugs, inadequate surveillance, and factors associated with individual and national poverty indicators [3]. The lack of clinical microbiology laboratories to identify the specific etiologic agents and their antimicrobial susceptibility testing has increased empirical therapy, leading to the emergence of AMR.
Bangladesh, a developing country of Southeast Asia with a high prevalence of antibiotic resistance, poses a regional and global threat. Up-to-date information about the bacterial profile, monitoring AMR patterns, and the leading pathogen–drug combinations contributing to bacterial AMR burden is crucial to guide empiric antibiotic treatment strategies, rational use of the existing antimicrobials, and infection control programs. In this study retrospective data was utilized to analyze a large number of samples over an extended period, for providing an accurate understanding of the patterns and extent of AMR. Therefore, the present study was aimed to determine the bacterial profile and antimicrobial resistance patterns of bacterial isolates from different clinical specimens at Uttara Adhunik Medical College Hospital (UAMCH), Dhaka.
2. Materials and Methods
- Study design and setting
A retrospective study was carried out at UAMCH in Bangladesh to analyze pre-recorded data from the period of January 2017 to December 2019. The Capturing data on Antimicrobial Resistance Patterns and Trends in Use in Regions of Asia (CAPTURA) project funded by the Fleming Fund (a regional grant) supported the digitization of the data. Patients' data were obtained from the Microbiology laboratory at UAMCH for all specimens collected from both inpatients and outpatients. During the study period from September 2020 to December 2022, a total of 32,187 clinical specimens were received. All clinical samples were collected following standard microbiological techniques.
- Isolation and identification of bacteria
Specimens of urine, blood, stool, wound swab/pus, and sputum were carried to the microbiology lab within 2 hours and depending on the source of samples. Therefore, blood, wound swab/pus, and sputum specimens were plated onto MacConkey agar, Blood agar, Chocolate agar, stool samples were inoculated in MacConkey agar, TCBS (Thiosulfate-citrate-Bile salt sucrose) agar and urine specimens inoculated in Cystine lactose electrolyte deficient (CLED) agar and then incubated aerobically at 35 °C for 18-24 hours. Blood specimens were inoculated into blood culture bottles at the collection site immediately after collection, carried to the microbiology laboratory, and BD BACTEC FX40 automated blood culture method was used. In case of a growth, the BD BACTEC FX40 automatically gives an alert. The positive bottles were subcultured on MacConkey’s, blood agar, and chocolate agar media. The chocolate agar plates were incubated inside a candle jar to provide 5–10% CO2, whereas the other two agar plates (blood agar and MacConkey agar) were incubated aerobically for 18–24 h at 35 °C according to SOP. Bacterial species were identified following laboratory SOPs. The bacteria were identified based on morphological characters, Gram’s stain and biochemical tests [12]. Gram-negative bacteria were identified using a series of biochemical tests such as indole, urease, oxidase, triple sugar iron agar, citrate utilization, and motility tests. Gram-positive bacteria were identified based on Gram reaction, hemolytic pattern, catalase, and coagulase tests.
- Antimicrobial susceptibility testing
After bacterial identification, antimicrobial susceptibility tests (AST) were done on Mueller-Hinton using Kirby-Bauer disk diffusion method. Antimicrobials were selected according to Clinical Laboratory Standard Institute guideline (CLSI 2019). Mueller Hinton agar media and antimicrobial discs were procured from Oxoid Ltd., UK.
- Data collection tools
During the specified period (2017-2019), the laboratory maintained manual registers containing patient identifiers, demographic information, and laboratory test results. The WHONET software, developed by the WHO Collaboration Center for AMR Surveillance, was installed and configured in this laboratory. Training was also provided to the laboratory technologists to enable them to collect Antimicrobial Susceptibility Testing (AST) data using the software.
- Data management and statistical analysis
Data was entered, curated, and demographic characteristics were analyzed by using the WHONET software. The patterns and trends were analyzed using the Quick Analysis of Antimicrobial Patterns and Trends (QAAPT) web application.
- Sampling technique and sample size
A convenient sampling technique was employed, resulting in 5,602 individual records in different categories such as growth, mixed bacterial species, normal flora, no pathogen detected, and no Salmonella found (n=1,370). After excluding the contaminated samples, we identified 4,232 culture-positive isolates and 26,585 culture-negative cases (Figure 1).
- Inclusion and exclusion criteria
All isolates from the inpatients and outpatients of the hospital over the study period were included for this study. The incomplete, missing records (age and sex) and other than six specimens were excluded (Figure 1).
- Quality control
To control the quality of culture and drug susceptibility testing, the American Type Culture Collection (ATCC) isolates of E. coli (ATCC25922), S. aureus (ATCC- 25923) and Pseudomonas aeruginosa (ATCC 27853) were used as reference strains. The data was reviewed thoroughly by experienced microbiologists and data management specialists using WHONET standard reports.
3. Results
3.1. Profile of Patients, Clinical Specimens, and Bacterial Isolates
Clinical specimens were collected from 4232 patients; females accounted for 54.22% (n = 2,295). Most of the patients were in the age category of 15-24 years old (19.37%, n = 820). Most of the isolates were from medicine wards (78.3%, n=3,315), followed by surgery (8.72%, n=369), intensive care unit (ICU) (4.96%, n=210) and pediatrics (3.62%, n=153). Among 4,232 patients, a total of 1,063 (25.12%) samples were collected in 2017, 1620 (38.28%) in 2018 and 1,549 (36.60%) in 2019. Their mean age ± standard deviation was 34 years, nearly 76.86% of them were adults, and the majority 54.22% were female (Table 1).
Urine samples made up the majority of specimens (50.8%, n=16363). Similarly, Figure 2b depicts that urine samples had the highest percentage of positive cultures (47.5%, n=2009), followed by blood (35%, n=1500), wound swab/pus (10.1%, n=426) and sputum (5.3%, n=225).
3.1.1. Bacterial Isolates and Frequency of Organisms
Figure 3 demonstrates that E. coli was the most frequent isolate accounting for 37.19% (n=1,574), followed by Salmonella Typhi (25.73%, n=1,089), Klebsiella sp. (11.51%, n=487), Salmonella Paratyphi A (6.38%, n=270), Staphylococcus aureus (4.21%, n=178), and Enterobacter sp. (3.59%, n=152).
Figure 4 shows that E. coli, Salmonella typhi, Staphylococcus aureus, Klebsiella pneumoniae were the top four organisms found in urine, blood, wound swab and sputum respectively.
3.1.2. Most Commonly Found Pathogens
The most frequently isolated organisms among all samples were Escherichia coli (32.48%), Klebsiella sp. (15.50%), Pseudomonas sp. (10.60%), S. aureus (7.76%), and Enterococcus sp. (7.69%) respectively (Table 1). Figure 5 shows the distribution of the most common organisms according to specimen type.
Of the top five pathogens found in urine specimens, E. coli was frequently (n=60790, 52.03%) reported, followed by Klebsiella sp. (n=17487, 14.96%), Enterococcus sp. (n=15339, 13.13%), Pseudomonas sp. (n=5062, 4.33%), and Staphylococcus, coagulase negative (n=3385, 2.89%). Pseudomonas sp. (n=14348, 24.91%) and Staphylococcus aureus (n=11146, 19.35%) were the major isolated pathogens from soft tissue and body fluid samples, followed by other Gram-negative bacteria. The blood culture data showed Salmonella Typhi (n=9101, 32.50%) as the primary pathogen causing bloodstream infections (BSI). Other frequently reported pathogens from BSI included Staphylococcus, coagulase negative (n=3763, 13.44%), E. coli (n=3026, 10.81%), S. aureus (n=1955, 6.98%), and Salmonella paratyphi (n=1767, 6.31%). In respiratory tract infections, Klebsiella sp.(n=7950, 32.22%) was a commonly reported pathogen. Similarly, Candida sp. (n=1138, 32.95%) predominated in genital specimens while E. coli (n=1261, 71.12%) was the most common in stool samples.
3.1.3. Antibiotic Resistance Patterns of Bacterial Isolates
Table 2 reveals the antimicrobial resistance rate of Gram-negative bacteria. In this study, overall resistance pattern of E. coli isolates from various clinical specimens showed high resistance rates to amoxicillin/clavulanic acid (71.49%), cefuroxime (64.17%), cefixime (65.08%), ceftriaxone (60.25%) and ciprofloxacin (54.37%). A lower rate (12.76%, 5.06% and 1.47%) of resistance was observed in case of nitrofurantoin, amikacin, and meropenem respectively. Klebsiella sp. was resistant to amoxicillin/clavulanic acid (65.91%) followed by cefixime (58.59%) and ceftriaxone (55.46%). The resistance rate was lower in case of gentamicin (24.90%), amikacin (19.79%) and meropenem (15.43%). Enterobacter sp. showed higher percentage of resistance to cephalosporine group of drugs. Pseudomonas aeruginosa was found 60.40%, 52.04%, 33.33%, 21.36%, 18.03% and 4.35% resistant to aztreonam, ceftazidime, amikacin, meropenem, cefepime and piperacillin/tazobactam respectively. A higher percentage of resistance was seen in the case of Acinetobacter sp. against ceftriaxone (80.3%), ceftazidime (74.24%), amikacin (53.73%) and meropenem (46.15%) respectively.
Likewise, a higher percentage of strains of Salmonella typhi (85.36%) was found to be resistant to azithromycin. Resistance to ampicillin, chloramphenicol, and cotrimoxazole was 26.99%, 17.11% and 18.88%, respectively, indicating that the resistance trend might have started reversing. Moreover, the resistance rate of Staphylococcus aureus was 78.79% to penicillin, 69.01% to azithromycin, and 50.87% to ciprofloxacin. In addition, 5.93% resistance was observed to cloxacillin and 2.98% to gentamycin in Staphylococcus aureus. In the case of Enterococcus sp., 58.91%, 49.29%, and 42.96% resistance was found against gentamicin, ciprofloxacin, and trimethoprim/sulfamethoxazole.
4. Discussion
Drug-resistant bacterial infections have become a real threat in developing countries, including Bangladesh. But the extent of this antimicrobial resistance is not clear due to a lack of adequate data. In a study performed in Dhaka, Salmonella typhi and Salmonella paratyphi had reduced susceptibility against ciprofloxacin and a high percentage of strains were multidrug-resistant (MDR) [8]. Another study examining a three-year antimicrobial susceptibility trend among bacterial isolates from a tertiary health-care facility in Dhaka conducted from 2016 to 2018 found that the resistance pattern of E. coli, Klebsiella pneumonia, Acinetobacter baumannii and Pseudomonas aeruginosa against meropenem, amikacin, ceftazidime, and cefepime fluctuated in year-to-year pattern, highlighting an increase of resistance among Gram-negative bacteria to commonly used antibiotics [9]. Uropathogenic E. coli and Klebsiella sp. were found very highly resistance to first line drugs in a study conducted in 2018 at a hospital of Bangladesh [10]. The small-scale study on blood culture isolates conducted in this medical college in 2015 revealed 84% and 77% of isolates of Salmonella typhi and Salmonella paratyphi were resistant to azithromycin [31]. Another study conducted in this medical college focused on wound infection showed a high resistance pattern to commonly used antibiotics in the case of Pseudomonas aeruginosa and E. coli [32].
In this study, a total of 32,187 specimens were processed, among which 4,232 (13%) were culture positive. The bacteria isolation rate in this study was 13%, which is comparable with the results from India (11.2%) [33], Tanzania (14.8%) [12], but it was lower than reports from Ethiopia (28%) [13]. The majority of cases required antibiotic treatment prior to hospital admission, which may be the reason. Since antibiotics are frequently sold over the counter, self-medication is also fairly widespread in Bangladesh.
The difference in the pattern of bacterial isolate among different clinical specimens might be due to differences in study subjects, study design, identification method, geographic variation and variation over time within a study population [34]
Among all specimens, E. coli was the most frequent isolate accounting for 37.19% (1,574), followed by Salmonella typhi (25.73%, n=1,089), Klebsiella sp. (11.51%, n=487), Salmonella paratyphi A (6.38%, n=270), Staphylococcus aureus (4.21%, n=178), Enterobacter sp. (3.59%, n=152), and the least frequent was Enterococci sp. which accounted for 3.35% (n=142) of the isolates. The distribution and frequency of bacteria isolated in different clinical specimens were different. In urine, the predominant bacterial isolates were E. coli in agreement with different studies [10,13]. In the case of blood specimens, the predominant organism was Salmonella typhi. Several studies from Bangladesh have identified Salmonella typhi as a common cause of bloodstream infection (BSI) in this region and reported Salmonella sp. to be responsible for almost half of the disease burden associated with BSI in Dhaka [8]. Although the proportion and prevalence of the bacterial agents differed, more or less the same observations were made in cases of bacteremia in several countries [14,15]. As the only source of Salmonella sp. infection in diseased humans is fecal contamination of drinking water and food supplies, the highest percentage of salmonella isolates in this study highlight the importance of adequate waste management and infection control practices [38]. In this study, S. aureus and Klebsiella pneumoniae were the top two organisms found in wound swab and sputum respectively.
Overall resistance patterns of E. coli isolates from various clinical specimens showed high resistance rates to amoxicillin/clavulanic acid (71.49%), cefixime (65.08%), ceftriaxone (60.25%) and ciprofloxacin (54.37%), with lower rate (12.76%, 5.06% and 1.47%) of resistant were observed in case of nitrofurantoin, amikacin, meropenem respectively. In addition, the antimicrobial resistance patterns of Klebsiella sp. showed 65.91% resistant to amoxicillin / clavulanic acid followed by cefuroxime (60.26%), cefixime (58.59%) and ceftriaxone (55.46%). The Resistance rate was lower in case of gentamicin (24.90%), amikacin (19.79%) and meropenem (15.43%). The lower sensitivity of amikacin and meropenem may be due to these drugs being used as an alternate treatment option when first line drugs are ineffective [35].
This study found that the highest overall resistance was against amoxicillin/clavulanic acid; The reason for high resistance in our study could be due to recurrent empirical therapy with these combinations prior to sampling.
In addition, the high resistance percentages against some of the cephalosporin antibiotics cefuroxime (60.26%), cefixime (58%) and ceftriaxone (55%) are an indication of the irrational use of antibiotics for simple infectious or even viral diseases that leads to widespread bacterial resistance to these antibiotics. Different study in Bangladesh on antibiotic prescribing practice and antibiotic use showed that cephalosporin was a commonly prescribed antibiotic group and third-generation cephalosporins, were documented as highly used antibiotics [36,37]. E. coli and Klebsiella pneumoniae showed a lower rate of resistance to gentamicin, amikacin and meropenem which was comparable to the other studies done in Bangladesh 10,18. These findings contrast with those of previous studies in Yemen and India, which found greater rates of gentamycin resistance in E. coli and Klebsiella sp. [19,20].
The majority of bacteria resistant to sulfamethoxazole/trimethoprim and ciprofloxacin were Gram-negative species, such as E. coli, Klebsiella sp., and Enterobacter sp. Ciprofloxacin is a first-line treatment for a variety of diseases, including urinary tract infection (UTI), gastrointestinal infections (GIT), and typhoid. The wide empirical use, excessive and injudicious use of these drugs may have contributed to the high levels of observed resistance. According to the site of the bacterial infection and geographical aspect, the percentages of ciprofloxacin resistance differed. In this study, E. coli. showed 54.37%, Klebsiella pneumoniae showed 40.75% and Enterobacter sp. showed 44.75% resistance to ciprofloxacin which was close to the study from Iran and lower than that in the study from Bangladesh [18, 21]. Possible reasons for the disparity in drug resistance at different sites could be attributed to the differences in the rational use of antibiotics in the study areas.
E. coli isolates in our study showed low resistance (12.76%) against nitrofurantoin which was close to a study conducted by Haque et al in Bangladesh [22]. Although a slightly higher value was observed in the other study10 but still it remains as the most sensitive drug and similar results were also reported in other studies [23,24]. The reason behind this might be due to less use of this drug for a long period considering its toxicity and side effects. Nitrofurantoin might be the only useful oral antibiotic in the treatment of uncomplicated UTI and prophylaxis in the context of gradually decreasing susceptibility of most of the comparatively cheaper anti-UTI drugs.
In our setting, we found higher resistant rates (15.43%, 21.36 and 44.3%) of meropenem in the case of Klebsiella pneumoniae, Pseudomonas sp. and Acinetobacter sp. respectively. Our results were comparable to those obtained in Saudi Arabia, India, and Iran [24,25,16]. Carbapenems were used to treat life threatening infections caused by multidrug resistance (MDR) bacterial pathogens and antibiotics in this class represent the last line of therapy in treatment options against very serious infections such as those caused by extended spectrum beta-lactamases.
Pseudomonas aeruginosa was found 60%, 52% and 33% resistant to aztreonam, ceftazidime and amikacin respectively which suggests that P. aeruginosa was increasingly becoming resistant to antibiotics. Acinetobacter sp. showed 80.3%, 74% and 53.73% resistance against ceftriaxone, ceftazidime and amikacin respectively. Another review study in Iran (2009 to 2015) revealed the emergence of Acinetobacter baumannii in clinical specimens with high resistance to different classes of antibiotics [25]. Acinetobacter sp. and Pseudomonas sp. are well known for their high degree of resistance against all classes of antibiotics, and the emergence of MDR strains makes it very difficult to treat them.
Salmonella sp. showed lower resistance rate to ampicillin, chloramphenicol and cotrimoxazole in this study which is consistent with studies carried out in Nepal and Pakistan [26,27]. A higher percentage of strains of Salmonella typhi was found resistant to azithromycin. Several clinical studies have demonstrated good efficacy of azithromycin for the treatment of common enteric fever in clinical and in vitro studies. In a study in India, 93.2 percent of S. Typhi were found susceptible to azithormycin [28]. In our study, we only used a disc diffusion method for azithromycin, MIC was not done which was one of the limitations. In summary, the study results revealed that first-line anti-typhoidal drugs were becoming less effective against Salmonella, whereas azithromycin resistance was noticeably rising. Use of ceftriaxone should be restricted to patients of enteric fever that are MDR and Extensively drug resistant (XDR). However, understanding the significance of microbiology for accurate reporting, evaluation, and monitoring of antimicrobial therapy is essential [27].
Similarly, among the Gram-positive bacteria high rates of resistance were observed against azithromycin and ciprofloxacin. In contrast to past research where a higher proportion of Methicillin-resistant Staphylococcus aureus (MRSA) was observed, this study found that Staphylococcus aureus had a lower rate of Cloxacillin resistance [12,29,30].
5. Conclusions
Bacterial AMR is a major global health problem. AMR has increased over the years in Bangladesh owing to the country’s poor healthcare standards, along with the misuse and overuse of antimicrobials which poses a regional and global threat. This study reveals the bacterial isolates and their antibiotic resistance patterns for commonly used antibiotics. The outcomes of this study will help healthcare professionals in Bangladesh and the region to make informed decisions and provide better care for their patients. The rise of antibiotic resistance in different clinical isolates emphasizes the importance of sound hospital infection control, proper waste management, rational prescribing policies, and the need for new antimicrobial drugs and vaccines. Also, there is a need for continuous evaluation of the local antibiotic resistance patterns for the formulation of a rational antibiotic policy.
Author Contributions
MN reports lead the data collection, outlined the first version and lead writing of the manuscript. MFB, HTB, ZHH, SMSR, AR, AS, MAH, RK, MSA, NN, MMB, SG, FM, and NP reports to review the manuscript. MJS reports leading the data digitization, management, analysis, interpretation and coordinate with co-authors.
Funding
The “Capturing Data on Antimicrobial Resistance Patterns and Trends in Use in Regions of Asia (CAPTURA)” and SAG-WHONET project funded by the Department of Health and Social Care’s Fleming Fund using UK aid. The views expressed in this publication are those of the authors and not necessarily those of the UK Department of Health and Social Care or its Management Agent, Mott MacDonald.
Institutional Review Board Statement
The CAPTURA project was exempt from ethical review by the Institutional Review Board (IRB) of the IVI because the project did not involve intervention or interaction with individuals and the information collected was not individually identifiable. This exemption is per the IVI IRB SOP D-RB-4-003. The CAPTURA project undertook the retrospective data collection and curation, and the authors used the digitized data to prepare this manuscript.
Informed Consent Statement
The CAPTURA consortium project received official approval from the Communicable Disease Control, DGHS, and MoHFW on May 17, 2020. The reference number is DGHS/DC/ARC/2020/1708. Prior to the data collection, a tri-party collaborative agreement was made among the DGHS, UAMC, and International Vaccine Institute - CAPTURA on 28 September 2020.
Data Availability Statement
The dataset will be shared upon request.
Acknowledgments
We would like to express our gratitude to the microbiologist, data entry operators and laboratory technologists at the microbiology lab. We also acknowledge Md. Dulal Mia, Shah Alam Islam, Mr. Sumon Sarkar, Milon Ahmed, and Zillur Rahman, for for their invaluable assistance in digitizing the data.
Conflicts of Interest
The authors declare no conflicts of interest
Abbreviations
The following abbreviations are used in this manuscript:
| UAMC | Uttara Adhunik Medical College |
| CAPTURA | Capturing Data on Antimicrobial Resistance Patterns and Trends in Use in Regions of Asia |
| IEDCR | Institute of Epidemiology Disease Control & Research |
| CDC | Communicable Disease Control |
| MoHFW | Ministry of Health and Family Welfare |
| QAAPT | Quick Analysis of Antimicrobial Patterns and Trends |
| CLSI | Clinical & Laboratory Standards Institute |
| EUCAST | European Committee for Antimicrobial Susceptibility Testing |
References
- O’Neill, J. Tackling drug-resistant infections globally: final report and recommendations. London: Review on Antimicrobial Resistance, 2016.
- Mulu, W.; Kibru, G.; Beyene, G.; Damtie, M. Postoperative nosocomial infections and antimicrobial resistance pattern of bacteria isolates among patients admitted at FelegeHiwot Referral Hospital, Bahir Dar, Ethiopia. Ethiop J Health Sci. 2012, 22, 7–17. [Google Scholar] [PubMed]
- Ahmed, I.; Rabbi, M.B.; Sultana, S. Antibiotic resistance in Bangladesh: A systematic review. International Journal of Infectious Diseases 2019, 80, 54–61. [Google Scholar] [CrossRef]
- Biswas, R.; Rabbani, R.; Ahmed, H.S.; Sarker MA, S.; Zafrin, N.; Rahman, M.M. Antibiotic sensitivity pattern of urinary tract infection at a tertiary care hospital. Bangladesh Critical Care Journal 2014, 2, 21–24. [Google Scholar] [CrossRef]
- Abera, B.; Kibret, M.; Mulu, W. Knowledge and beliefs on antimicrobial resistance among physicians and nurses in hospitals in Amhara Region, Ethiopia. BMC Pharmacol. Toxicol. 2014, 15, 26. [Google Scholar] [CrossRef]
- WHO, 2019. New report calls for urgent action to avert antimicrobial resistance crisis. World Health Organization website. Available online: https://www. who. int/news-room/detail/29-04-2019-new-reportcalls-for-urgent-action to avert-antimicrobial-resistance-crisis.
- Murray, C.J.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Aguilar, G.R.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; Johnson, S.C. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. The Lancet 2022. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, D; et al. Bacterial etiology of bloodstream infections and antimicrobial resistance in Dhaka, Bangladesh, 2005–2014. Antimicrobial Resistance and Infection Control 2017, 6, 2. [Google Scholar] [CrossRef] [PubMed]
- Hasan MJ, Hosen MS, Bachar SC. The resistance growing trend of common gram-negative bacteria to the potential antibiotics over three consecutive years: a single center experience in Bangladesh. Pharm PharmacolInt J. 2019, 7, 114–9. [Google Scholar]
- Antimicrobial Resistance Pattern of Uropathogenic Escherichia coli and Klebsiella species Isolated in a Tertiary Care Hospital of Sylhet 2018 Volume 30 Number 02 Rahman MM, Chowdhury OA , Hoque MM , Hoque SA , Chowdhury SMR , Rahman MA. 2018 Volume 30 Number 02.
- Deen J, et al. Community-acquired bacterial bloodstream infections in developing countries in south and southeast Asia: a systematic review. Lancet Infect Dis. 2012, 12, 480–7. [Google Scholar] [CrossRef]
- Nicholaus, P; et al. Antibiotic Susceptibility Patterns of Bacterial Isolates from Routine Clinical Specimens from Referral Hospitals in Tanzania: A Prospective Hospital-Based Observational Study. Infection and Drug Resistance 2021, 14, 869–878. [Google Scholar]
- Anteneh, Amsalu; et al. Antimicrobial resistance pattern of bacterial isolates from different clinical specimens in Southern Ethiopia. African Journal of Bacteriology Research: A three year retrospective study 2017, 9, 1–8. [Google Scholar]
- Zenebe T, Kannan S, Yilma D, Beyene G Invasive bacterial pathogens and their antibiotic susceptibility patterns In Jimma University Specialized Hospital, Jimma, Southwest Ethiopia. Ethiop J Health Sci 2011, 21, 1.
- Mulu et al. Bacterial agents and antibiotic resistance profiles of infections from different sites that occurred among patients at Debre Markos Referral Hospital, Ethiopia: a cross-sectional study. BMC Res Notes 2017, 10, 254. [Google Scholar]
- Wafa F., S. Badulla, 1 Mohammed Alshakka,2 and Mohamed Izham Mohamed Ibrahim 3 Antimicrobial Resistance Profiles for Different Isolates in Aden, Yemen: A Cross-Sectional Study in a Resource-Poor Setting. BioMed Research International 2020, 2020, 1810290, 8. [Google Scholar] [CrossRef]
- Fleischmann-Struzek, C.; Goldfarb, D.M.; Schlattmann, P.; Schlapbach, L.J.; Reinhart, K.; Kissoon, N. +e global burden of paediatric and neonatal sepsis: a systematic review. 3e Lancet Sputum Medicine 2018, 6, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Majumder, *!!! REPLACE !!!*; et al. Antibiotic resistance pattern of microorganisms causing urinary tract infection: a 10-year comparative analysis in a tertiary care hospital of Bangladesh. Antimicrobial Resistance & Infection Control 2022, 11, 156. [Google Scholar] [CrossRef]
- Gashe, F.; Mulisa, E.; Mekonnen, M.; Zeleke, G. Antimicrobial Resistance Profile of Different Clinical Isolates against Third- Generation Cephalosporins. Journal of Pharmaceutics 2018, 5070742, 7. [Google Scholar]
- Mhada, T.V.; Fredrick, F.; Matee, M.I.; Massawe, A. Neonatal sepsis at Muhimbili National Hospital, Dar es Salaam, Tanzania; aetiology, antimicrobial sensitivity pattern and clinical outcome. BMC Public Health 2012, 12, 904. [Google Scholar]
- Fallah, F.; Parhiz, S.; Azimi, L. Distribution and antibiotic resistance pattern of bacteria isolated from patients with community-acquired urinary tract infections in Iran: a crosssectional study. International Journal of Health Studies 2019, 4. [Google Scholar]
- Haque R, Akter LM, Salam AM. Prevalence and susceptibility of uropathogens: a recent report from a teaching hospital in Bangladesh. BMC Res Notes. 2015, 8, 416. [Google Scholar]
- Kothari A, Sagar V. Antibiotic resistance in pathogens causing community-acquired urinary tract infections in India: a multicenter study. [Abstract] J Infect Dev Ctries. 2008, 2, 354–358, 30. Sharifian M, Karimi A, Rafiee-Tabatabaei S, Anvaripour N. Microbial Sensitivity Pattern in Urinary Tract Infections in Children: A Single Center Experience of 1177 Urine Cultures. Jpn J Infect Dis. 2006; 59: 380-2.. [Google Scholar]
- Sharifian M, Karimi A, Rafiee-Tabatabaei S, Anvaripour N. Microbial Sensitivity Pattern in Urinary Tract Infections in Children: A Single Center Experience of 1177 Urine Cultures. Jpn J Infect Dis. 2006, 59, 380–2. [Google Scholar]
- R. Nikoo, A. A. Hadi, and J. Mardaneh, Systematic review of antimicrobial resistance of clinical Acinetobacter baumannii isolates in Iran: an update. Microbial Drug Resistance 2017, 23, 744–756. [Google Scholar] [CrossRef]
- Khadka et al. Susceptibility pattern of Salmonella enterica against commonly prescribed antibiotics, to febrile-pediatric cases, in low-income countries. BMC Pediatrics 2021, 21, 38.
- Sattar et al. Current trends in antimicrobial susceptibility pattern of Salmonella typhi and paratyphi. Rawal Medical Journal 2020, 45.
- Sharma, P; et al. Azithromycin resistance mechanisms in typhoidal salmonellae in India: A 25 years analysis. Indian J Med Res. 2019, 149, 404–411. [Google Scholar] [PubMed]
- Wangai FK, Masika MM, Maritim MC, Seaton RA. Methicillinresistant Staphylococcus aureus (MRSA) in East Africa: red alert or red herring. BMC Infect Dis. 2019, 19, 596, 32. Garoy EY, Gebreab YB, Achila OO, et al. Methicillin-Resistant Staphylococcus aureus (MRSA): prevalence and Antimicrobial Sensitivity Pattern among Patients - A Multicenter Study in Asmara, Eritrea. Can J Infect Dis Med Microbiol. 2019; 10.1155/2019/8321834. [Google Scholar] [CrossRef]
- Ali Abdel Rahim KA, Ali Mohamed AM. Prevalence of Extended Spectrum -lactamase-Producing Klebsiella pneumoniae in Clinical Isolates. Jundishapur J Microboil. 2014, 7, 1-5. 26. Varaiya AY, Dogra JD, Kulkarni MH, Bhalekar PN. Extended-spectrum beta-lactamase-producing Escherichia coli and Klebsiella pneumoniae in diabetic foot infections. Indian J PatholMicrobiol. 2008, 51, 370–2. [Google Scholar]
- Nasrin M, Bhuiyan M, Begum MF, Karim R, Bacteriological profile and Antimicrobial susceptibility Patterns of blood culture Isolates in a Referral Hospital. Journal of UttaraAdhunik Medical College 2018, 8, 11–12.
- Begum MF, Nasrin M, Karim R, Alam Shah, Bacteriological profile and antimicrobial susceptibility patterns of wound infections at Uttara Adhunik Medical College Hospital. Bangladesh J Med Microbiol 2020, 14, 15–19.
- Karuna T, Gupta A, Vyas A, et al. Changing Trends in Antimicrobial Susceptibility Patterns of Bloodstream Infection (BSI) in Secondary Care Hospitals of India. Cureus 2023, 15, e37800. [Google Scholar] [CrossRef]
- Zewodie Haile. HylemariamMihiretieMengist,TebelayDilnessa,Bacterial isolates, their antimicrobial susceptibility pattern, and associated factors of external ocular infections among patients attending eye clinic at Debre Markos Comprehensive Specialized Hospital, Northwest Ethiopia. PLoS One 2022, 17, e0277230. [Google Scholar]
- Standard Treatment Guidelines on Antibiotic Use in Common Infectious Diseases of Bangladesh,Version1,CDC,DGHS; Website. Available online: https://play.google.com/store/apps/details?id=stgapp.cdc.gov.bd (accessed on 22 April 2024).
- Laizu, J.; Parvin, R.; Sultana, N.; Ahmed, M.; Sharmin, R.; Sharmin, Z.R. , et al. Prescribing Practice of Antibiotics for Outpatients in Bangladesh: Rationality Analysis. Am J Pharmacol. 2018, 1. [Google Scholar]
- Rashid M et al, Pattern of Antibiotic Use among Hospitalized Patients according to WHO Access, Watch, Reserve (AWaRe) Classification: Findings from a Point Prevalence Survey in Bangladesh. Antibiotics 2022, 11, 810. [CrossRef]
- Saha S et al Enteric Fever and Related Contextual Factors in Bangladesh. Am J Trop Med Hyg. 2018, 99 (Suppl. 3), 20–25. [CrossRef]
Figure 1.
Flow diagram in sampling technique.
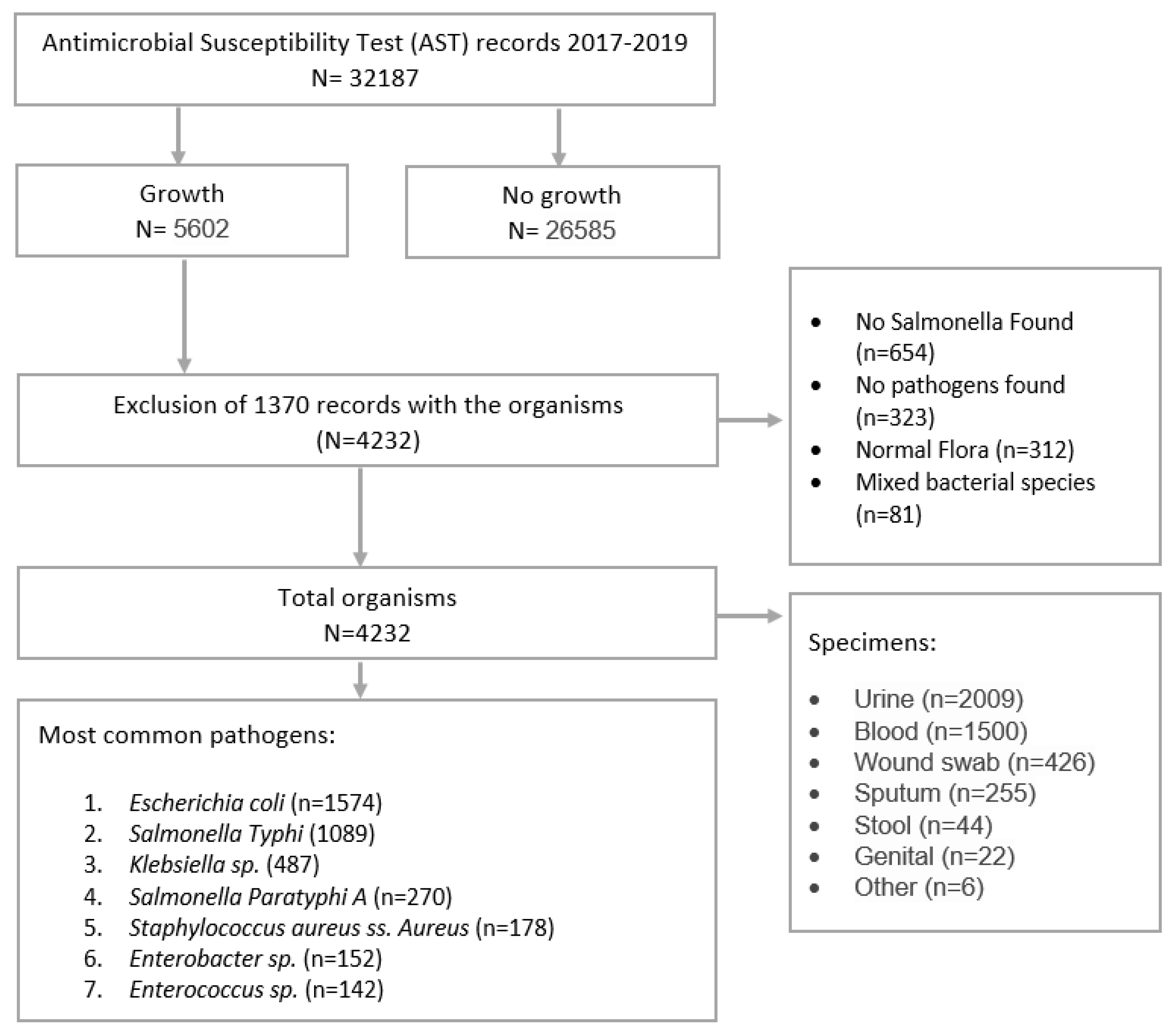
Figure 2.
Sample distribution by type of specimens.
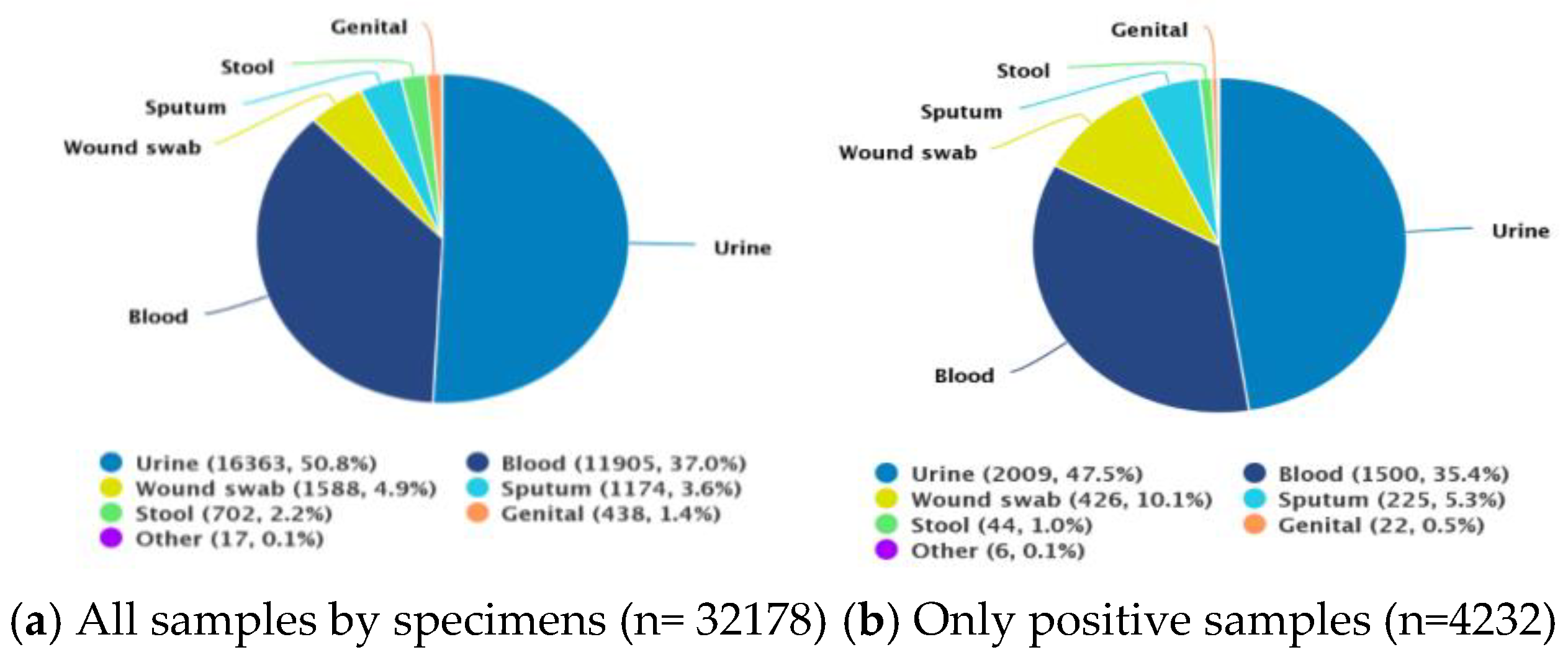
Figure 3.
Most common organisms.
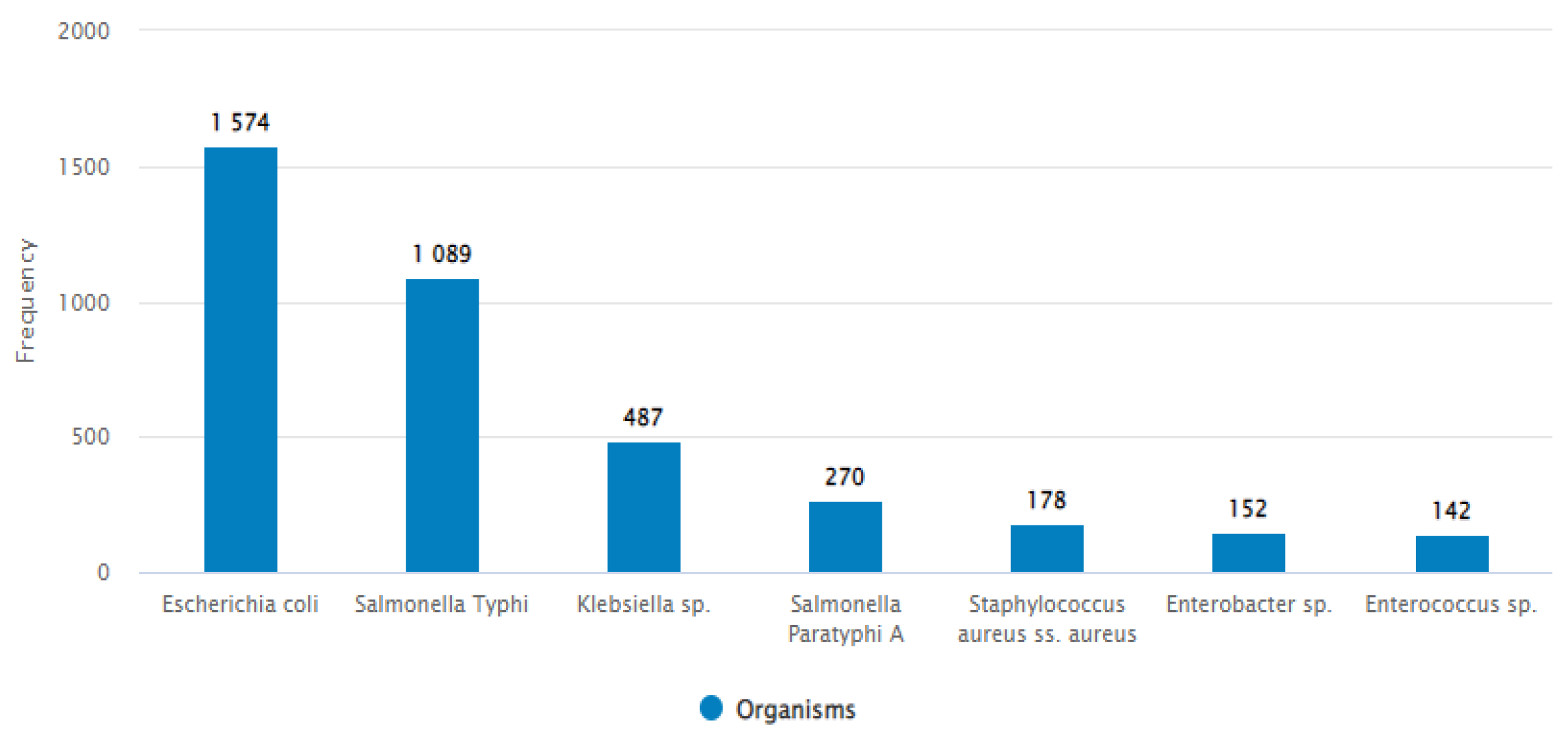
Figure 4.
Top five organisms by specimen.
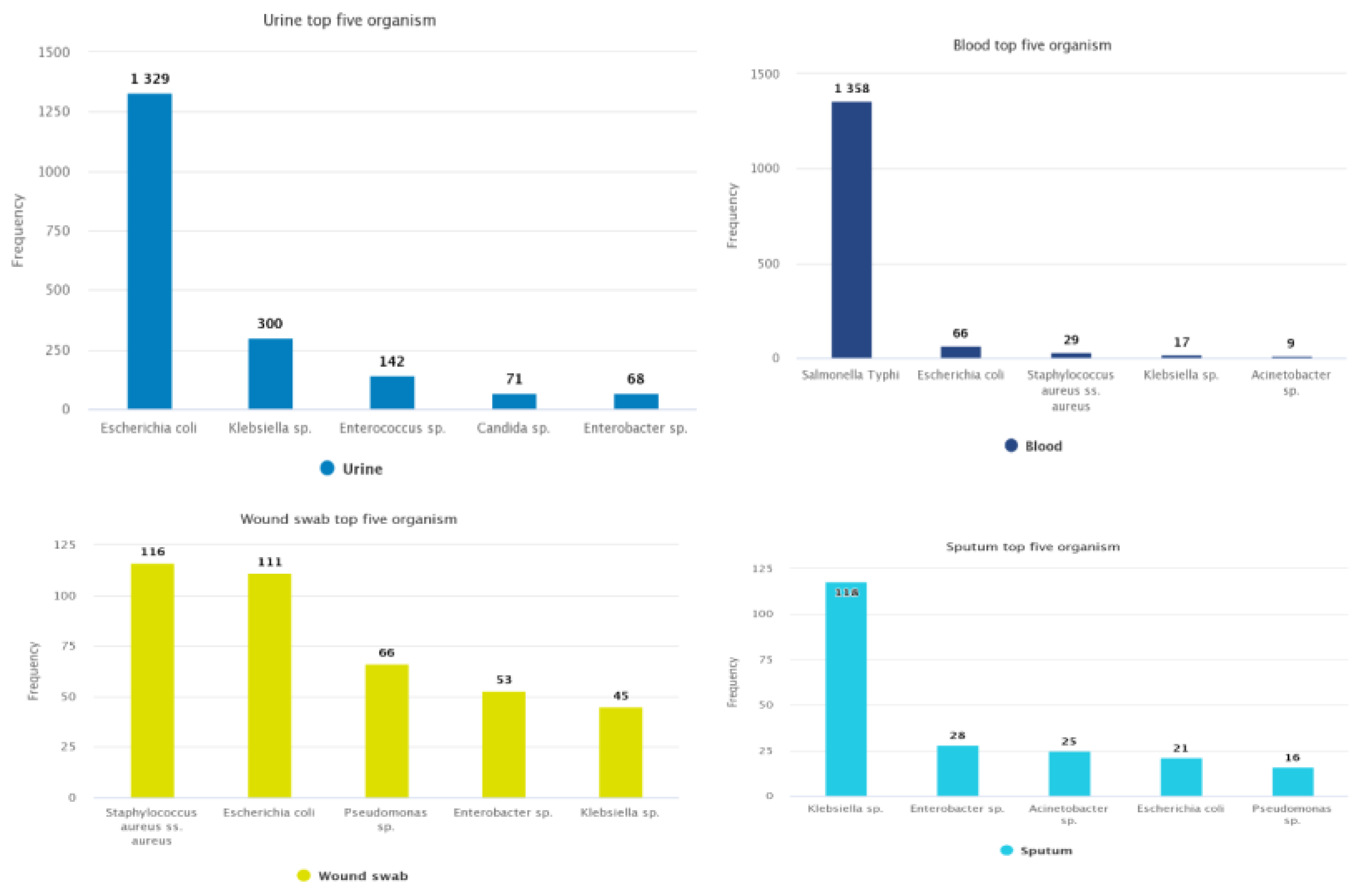

Table 1.
characteristics of the study participants (only positive, n=4,232).
| Characteristics | Frequency N= 4,232 | Percentage (%) |
| Gender | ||
| Male | 1,937 | 45.77 |
| Female | 2,295 | 54.22 |
| Age group | ||
| <1 | 68 | 1.60 |
| 1-4 Years | 157 | 3.71 |
| 5-14 Years | 452 | 10.68 |
| 15-24 Years | 820 | 19.37 |
| 25-34 Years | 603 | 14.25 |
| 35-44 Years | 403 | 9.52 |
| 45-54 Years | 442 | 10.44 |
| 55-69 Years | 768 | 18.15 |
| 70+ Years | 519 | 12.26 |
| Age category | ||
| Adult | 3,253 | 76.86 |
| Pediatric | 979 | 23.13 |
| Yearly AST | ||
| 2017 | 1,063 | 25.12 |
| 2018 | 1,620 | 38.28 |
| 2019 | 1,549 | 36.60 |
| Location type | ||
| Inpatient | 1,971 | 46.57 |
| Outpatient | 2,261 | 53.43 |
| Department | ||
| Medicine | 3,315 | 78.33 |
| Surgery | 369 | 8.72 |
| Intensive Care Unit | 210 | 4.96 |
| Pediatrics | 153 | 3.62 |
| Obstetrics/Gynecology | 73 | 1.72 |
| Neonatal | 67 | 1.58 |
| Coronary Care Unit | 33 | 0.78 |
| Orthopedic | 10 | 0.24 |
| Neonatal Intensive Care Unit | 2 | 0.04 |
| Specimen type | ||
| Urine | 2009 | 47.47 |
| Blood | 1500 | 35.44 |
| Wound swab/pus | 426 | 10.06 |
| Sputum | 225 | 2.36 |
| Stool | 44 | 1.04 |
| Genital | 22 | 0.52 |
| Other | 6 | 0.14 |
Table 2.
Antimicrobial resistance patterns.
| Antibiotics/ Organisms | Gram Negative organism | Gram Positive organism | ||||||
| E. coli (%) | Klebsiella sp. (%) | Enterobacterus sp. (%) | Pseudomonas sp. (%) | Acinetobacter sp. (%) | Salmonella sp. (%) | S. aureus (%) | Enterococcus sp. (%) | |
| Amikacin | 5.06 (76/1501) | 19.79 (94/475) | 22.92 (33/144) | 33.33 (34/102) | 53.73 (36/67) | - | - | - |
| Amoxicillin / Clavulanic acid | 71.49 (1096/1533) | 65.91 (319/484) | - | - | - | |||
| Ampicillin | - | - | - | - | - | 26.77 (166/620) | - | - |
| Azithromycin | - | - | - | - | - | 85.21 (1158/1359) | 69.01 (118/171) | - |
| Aztreonam | 62.11 (900/1449) | 56.37 (261/463) | 62.24 (89/143) | 60.40 (61/101) | - | - | - | |
| Cefepime | 58.06 (72/124) | 61.47 (67/109) | 46.15 (18/39) | 18.03 (11/61) | 75.76 (25/33) | - | - | - |
| Cefixime | 65.08 (1014/1558) | 58.59 (283/483) | 64.90 (98/151) | 90.77 (59/65) | - | - | - | |
| Cloxacillin | - | - | - | - | 5.93(8/135) | - | ||
| Ceftazidime | - | 57.82 (85/147) | 52.04 (51/98) | 74.24 (49/66) | - | - | - | |
| Ceftriaxone | 60.25 (929/1542) | 55.46 (264/476) | 54.97 (83/151) | 80.30 (53/66) | 0.29 (4/1361) | - | - | |
| Cefuroxime | 64.17 (908/1415) | 60.26 (282/468) | 63.89 (92/144) | 81.54 (53/65) | - | - | ||
| Chloramphenicol | - | - | - | - | - | 17.2 (232/1349) | - | - |
| Ciprofloxacin | 54.37 (846/1556) | 40.75 (196/481) | 44.74 (68/152) | 39.42 (41/104) | 57.58 (38/66) | 26.59 (360/1354) | 50.87 (88/173) | 49.29 (69/140) |
| Gentamicin | 17.87 (272/1522) | 24.90 (119/478) | 33.11 (50/151) | 37.00 (37/100) |
56.06 (37/66) | - | 2.98 (5/168) | 58.91 (76/129) |
| Levofloxacin | 52.86 (803/1519) | 34.86 (167/479) | 32.88 (48/146) | 38.61 (39/101) | 51.56 (33/64) | - | - | - |
| Mecillinam (Amdinocillin) | 21.92 (294/1341) | - | 39.71 (27/68) | - | - | - | - | - |
| Meropenem | 1.47 (22/1497) | 15.43 (73/473) | 9.03 (13/144) |
21.36 (22/103) | 46.15 (30/65) | - | - | - |
| Netilmicin | 7.92 (118/1490) | 22.80 (106/465) | 24.49 (36/147) | 29.00 (29/100) | 38.81 (26/67) | - | - | - |
| Nitrofurantoin | 12.76 (168/1317) | 34.01 (100/294) | 41.18 (28/68) | - | - | - | - | 10.37 (14/135) |
| Penicillin | - | - | - | - | - | 78.79 (104/132) | - | |
| Piperacillin/Tazobactam | 56.13 (142/253) | 70.09 (75/107) | 37.14 (13/35) | 4.35 (4/92) | - | - | - | - |
| Trimethoprim/Sulfamethoxazole | 50.80 761/1498 |
54.76 253/462 |
42.96 58/135 |
60.94 39/64 |
18.88 (253/1340) | 20.47 (35/171) | 42.96 (58/135) | |
| Vancomycin | - | - | - | - | - | 1.18 (2/169) | - | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



