
Submitted:
23 January 2025
Posted:
24 January 2025
You are already at the latest version
Abstract
Background: Prostate cancer consists the second most commonly diagnosed malignancy in men and a global threatening health condition with severe following outcomes. Screening via the digital rectal examination (DRE), prostate-specific antigen (PSA) test, or both is widely used in clinical practice and supported as early detection tools. Although neither of the two tests, PSA and DRE, are appropriate to be used alone for screening of prostate cancer. This meta-analysis aims to find out the role of these techniques used in conjunction in a primary healthcare setting to diagnose prostate cancer(PC).Methods: This meta-analysis was conducted according to (PRISMA) guideline. A comprehensive literature search was performed to PubMed, Cochrane, and Google Scholar from November 2022 to April 2023. Diagnostic studies were retrieved with no restrictions on publication date, country, patient's age or clinical setting. The selection of studies proceeded based on specific inclusion and exclusion criteria without restrictions to particular study designs, language or publication dates and followed by data extraction and statistical analysis. The gold standard reference in the included studies was biopsy for prostate carcinoma.Results: Twelve studies with 175379 patients who underwent DRE Vs Biopsy and fifteen studies with 22006 patients who measured PSA cutoff 4 ng/ml VS biopsy were included in our meta-analysis. Overall, the overall sensitivity, specificity, and PPV of DRE was 57.8% (95% CI 52 -63.6 %), 44.7% (95% CI 37.6 - 51.7%), and 29.8% (95% CI 24.1 - 35.5%) respectively. The diagnostic accuracy of DRE was 48.5% with a Younden index of 2.5%. Also, the sensitivity, specificity, and PPV for PSA cutoff level of more than 4 ng/mL were found to be 57.7 % (95% CI 51.2 - 64.2%) ,82.3% (95% CI 79.7 - 85%), and 67.6% (95% CI 62.7 - 72.6%) respectively. In addition, the diagnostic accuracy of the PSA cutoff level of more than 4 ng/mL was 72.7% with a Younden index of 0.4. Conclusion: The use of DRE and PSA has high diagnostic accuracy in PC, although the lone application of each one is not statistically strong and diagnostically accurate. Their contribution could form an optimistic clue in future updates considering this condition.
Keywords:
digital rectal examination
; DRE AND prostate-specific antigen
; PSA AND prostate cancer
; prostate neoplasm
; prostatic carcinoma
Introduction
Prostate cancer contributes to substantial morbidity and mortality. As a result, screening via the digital rectal examination (DRE), prostate-specific antigen (PSA) test, or both has become the mainstay of clinical practice. Approximately 1.1 million men receive the diagnosis of prostate cancer yearly, making it the second most commonly diagnosed malignancy in men [1], indicating the necessity of an extremely important and efficacious screening method. As prostate cancer contributes to substantial morbidity and mortality, screening via the DRE, PSA test, or both has become the mainstay of clinical practice. In fact, prior to the recent addition of serum PSA testing to DRE, most prostate cancers were diagnosed only after they had become locally advanced or metastatic. [2] Once regional lymph node involvement has occurred, death from prostate cancer has a probability of 70%. [3]
As stated above, screening for prostate cancer by PSA and DRE tests to enhance early detection is widely supported. To support this practice, multiple studies have reported that PSA tests detect a significant number of cancers missed by DRE [4]. However, PSA tests alone missed 11% of patients who had prostate cancer with a normal serum PSA level (<4 ng/ml) [5] thus making an inquest into it’s accuracy a prudent manoeuver to establish more clarity regarding the use of the method. In spite of this, PSA is the most widely used screening test for prostate cancer, and is considered to be the main cause of the stage migration and the decreased cancer specific mortality rates observed in countries where screening is carried out.[6]
Digital rectal examination (DRE) is commonly used to screen for prostate carcinoma. It is the oldest and least invasive test modality. Although false negative and positive exams on DRE may occur, DRE does detect some prostate cancers that are missed by PSA screening [7] That being considered, the proportion of these potentially diagnosable cancers, diagnosed by DRE, remains very low, perhaps because many of these tumors are too small to be palpable by DRE [8]. It is with this evidence that DRE appears to be a test with a high specificity and a high negative predictive value. It may have a place as an initial test when screening for prostate cancer. A negative test result of DRE has a high predictive value. The sensitivity being only moderate, however, should prevent the primary caregiver from drawing conclusions on the sole basis of such a result. Owing to its very low predictive value, a positive test result cannot be advocated as the basis for any important diagnosis without further confirmation. [9]
Having established that neither of the two tests, PSA and DRE, are appropriate to be used alone for screening of prostate cancer, this meta-analysis aims to find out the role of these techniques used in conjunction in a primary healthcare setting to diagnose prostate cancer.
Methods and Results
this meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guideline [10]
Data Sources and Searches
A comprehensive literature search was conducted during the period from November 2022 to April 2023 through these databases: PubMed, Cochrane, and Google Scholar with the search key terms “digital rectal examination “ OR “DRE” AND prostate-specific antigen” OR “PSA” AND “prostate cancer” OR “prostate neoplasm” OR “prostatic carcinoma” with no language or time limitation. Diagnostic studies were retrieved with no restrictions on publication date, country, patient’s age or clinical setting
Study Eligibility Criteria and Selection
The studies included in this meta-analysis are studies in which it was evident that a primary care clinician performed the DRE AND/OR PSA levels in asymptomatic or symptomatic patients. Studies must have sufficient or available numeric information such as a 2 × 2 contingency data table or sensitivity (Sn), specificity (Sp), and positive predictive value (PPV) of the PSA cutoff of more than 4 ng/ml and/or DRE. Studies must include biopsy as a reference standard for prostate carcinoma. Studies of symptomatic patients who presented with lower urinary symptoms (disturbances of urination, hematuria ) suggestive of prostate cancer or benign prostate hyperplasia. The non-English studies, non-human subjects, or invalid data were excluded.
Data Extraction
Two reviewers (Anisa & Abeer) Independently conducted title and abstract screening and full-text review in duplicate to identify eligible studies. A pre-prepared Excel sheet was used for data extraction. Disagreements were resolved by discussion to reach a consensus and, if necessary, by involving a third reviewer (Tayba). Data extracted included general study characteristics (authors, publication year, country, study design, patient number, patients who underwent biopsy, age range), index test (sensitivity, specificity, true positive, true negative, false positive, false negative), and reference standard test.
Statistical Analysis
We performed a meta-analysis of the sensitivity, specificity, and PPV, values obtained from the individual studies using RevMan (Review Manager, version 5.3). . Individual study sensitivity and specificity were plotted on Forest plots and in the receiver operating characteristic (ROC) curve. Heterogeneity for the individual outcomes was detected by Cochran Q and I2 test statistics with a p value <0.1 or I2> 50% was considered to be significant. The random-effects model (DerSimonian-Laird method) was preferred over the fixed-effects model (Mantel-Haenszel method); if there was significant heterogeneity (I2 > 50% or P ≤ .05), otherwise, the fixed-effects model was the first choice.
Risk of Bias and Quality Assessment
We used the validated Quality Assessment of Diagnostic Accuracy Studies 2 (QUADAS-2) tool to assess the quality of included studies. Funnel plot was used to assess the risk of bias.
Results
Study Selection and Characteristics
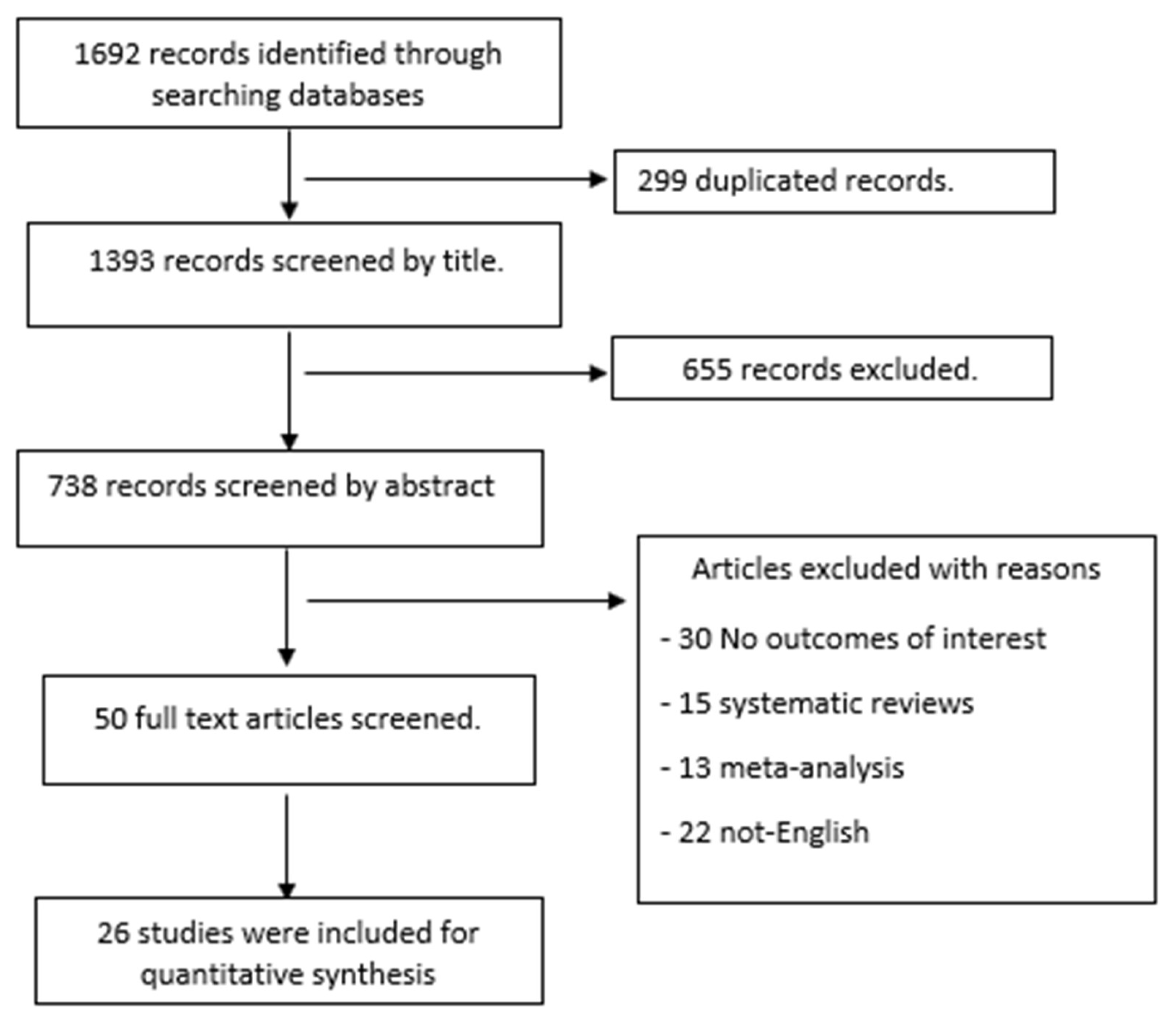
Database searching revealed a total of 1692 studies with only 26 studies meeting the inclusion criteria. We included 12 studies with 175379 patients who underwent DRE Vs Biopsy and 15 studies with 22006 patients who measured PSA cutoff 4 ng/ml VS biopsy. Crawford et al. study was used in common for both DRE and/or PSA.The general characteristics of the included studies are summarized in Table 1. Patients were enrolled prospectively in sixteen studies, nine were retrospective and one was case-control.
Figure 1.
PRISMA Flow Chart.
Diagnostic Accuracy of PSA and DRE
For each of the included studies, we were able to calculate the sensitivity, specificity, and positive predictive value (PPV) for the reference test (biopsy for prostatic cancer) results versus the diagnostic test (PSA OR DRE) as shown on the forest plots (Figure 2). This data was then combined using RevMan to give an overall sensitivity, specificity, and PPV of PSA and/or DRE. Overall, the sensitivity, specificity, and PPV for PSA cutoff level of more than 4 ng/mL as a screening tool for prostatic cancer in 22006 patients of 15 studies were found to be 57.7 % (95% CI 51.2– 64.2%) ,82.3% (95% CI 79.7 – 85%), and 67.6% (95% CI 62.7– 72.6%) respectively. In addition, the diagnostic accuracy of the PSA cutoff level of more than 4 ng/mL was 72.7% with a Younden index of 0.4. There were no other secondary outcomes of adverse events or cost-effectiveness extracted from the studies. However, the overall sensitivity, specificity, and PPV of DRE as a screening tool for prostatic cancer in 12 studies with 175379 patients was found to be 57.8% (95% CI 52 –63.6 %), 44.7% (95% CI 37.6– 51.7%), and 29.8% (95% CI 24.1– 35.5%) respectively. The diagnostic accuracy of DRE was 48.5% with a Younden index of 2.5%.
Figure 3 shows the summary of the ROC curve of both PSA and/or DRE . The area under the curve of PSA is .7000 with a diagnostic odds ratio of 6.346. The area under the ROC curve of DRE is .5122 with a diagnostic odds ratio of 1.105.
The overall diagnostic odds ratio of PSA>=4 was 41.43 and the Index Q* was at 0.8531 with standard error of 0.0969. (Figure 4) The overall diagnostic odds ratio of DRE was 1.93 and the Index Q* was at 0.5602 with standard error at 0.0569.(Figure 5)
The funnel plot shows asymmetry that indicates publications bias for the 15 included PSA>=4 studies (figure 6).The funnel plot of the 12 included studies regarding DRE shows asymmetrical distribution which indicates publication bias(Figure 7).Among the 28 papers, the risk of bias in patient selection was almost low in the majority of the papers 22, and unclear in 6 papers. As well, the index test of 25 papers was low, unclear in one, and high in 2 papers. While the reference standard was low in 12, unclear in 10, and high in 6 papers. However, the risk of bias in flow and timing was low in all papers except one was unclear. Moreover, the applicability concern in patient selection was low, unclear, and high in 17, 8, and 3 papers respectively. Also, the index test was a low risk of bias in 23, 4 unclear, and only one paper high risk of bias. However, the reference standard was low in 10, unclear in 10, and high in 8 papers. (Figure8)
Discussion
In this systematic review and meta-analysis including 26 studies, we found that the DRE as it currently exists, cannot be recommended for prostate cancer detection but it may have a role in screening for the same. The results showed that the pooled sensitivity and specificity values of DRE were approximately 57.8% and 44.7%, respectively. In addition, the overall accuracy of DRE for predicting Prostate Cancer was 48.5%. When PSA levels at a cut off of 4 ng/ml were considered, they yielded a pooled sensitivity of 57.7% and a pooled specificity of 82.3%, with an accuracy of 72.7%. This study was aimed at exploring the weakness, strength and accuracy of these techniques, either alone or in combination for the early and effective diagnosis of prostate cancer.
DRE is cheap and has almost no morbidity, but when performed by non-urologists the number of cancers detected is very low [11]. Even when specialists perform the examination more than half of the tumors detected are found on staging to be locally advanced [12]. Nonetheless, most screening or case finding studies report a proportion of clinically significant cancers which are detected by DRE in spite of a normal PSA level [13] and the fact that the subjects do not find the examination unpleasant unto a degree of discomfort indicate that the test perhaps has a role in screening for the same. In a study conducted in Sweden [14], it was established that digital rectal palpation was readily tolerated, with less than 10% of the men expressing negative attitudes about the screening. The method is noninvasive and fast, and any doctor can learn to perform it, which adds a benefit of convenience in reproducibility for standardization in application of the technique. Furthermore, Lee at al found 30% more suspected cancers by ultrasonic examination than by DRE, but the PPV of both methods was the same. [15]
However, it would be prudent to state that Chadwick et al.‘s pilot study [16] of prostate cancer in general practice yielded much greater variation in findings. It determined that only 3% men out of 407 examined had an abnormal DRE, and no cancer was detected on the basis of DRE alone, a finding which led the authors to question the value of GP-based rectal examinations in the detection of prostate cancer. Another study by Paul R. Bretton in Fort Myers [17]determined that of the 1,027 men in this study, 78 (8%) had abnormal findings on DRE and only 11 of these 78 men (14%) had prostate cancer. Thus, the overall cancer detection rate by DRE was 1%. This can’t help but make one wonder about the utility and futility associated with DRE in the era of modern science and technology in the field of clinical diagnosis.
The World Health Organization has stipulated that screening tests should have scientific evidence to demonstrate their effectiveness and that the overall benefits of screening should outweigh harms [18] As it stands, DRE does not meet these criteria. That itself is a testament to the depleting importance of DRE in the context of its essentiality in diagnosing prostate cancer.
These evidences along with the advent of other reliable diagnostic modalities based on radiology and hematology should determine that DRE has no accurate or independent role in the diagnosis of prostate cancer, and should be applied in a capacity purely associated with screening for cancer, to be always supplemented with more accurate techniques.
PSA levels in the diagnosis and prognosis of prostate cancer represent a modality that is both noninvasive as well as convenient to the physician and patient. In a study performed by Catalona [19], it was found that using the lower PSA cutoff, the great majority of cancers detected had favorable histopathological features, with approximately 80% being pathologically organ confined. This compares with about 70% organ-confined cancers with PSA levels higher than 4ng/mL [20,21] Since 17% were pathologically low-volume and low grade or moderately low-grade tumors, the use of the lower PSA cutoff did not appear to substantially increase the detection of medically unimportant cancers. In the Prostate Cancer Prevention Trial, the specificity of PSA at 4 ng/ml in healthy and asymptomatic men (placebo arm) has been shown to be 92.7% resulting in further lowing of PSA cut-off for biopsy [22]. PSA is a valuable tool for the early detection of PC. One third of patients with a normal DRE are biopsied because of an elevated PSA level [23] However, there is a high false-positive rate of PSA-indicated biopsies resulting in unnecessary invasive diagnostic procedures leading to unnecessary morbidity and psychological problems of patients. PSA also offers the advantage of not being operator dependent like DRE, which showed a higher sensitivity when performed by urologists than by GPs.
However, as evident by a low sensitivity, which would lead to an increasing number of missed cases, it was established that PSA as an independent modality is highly volatile, especially when taking into account the variation prevalence of PC in different ethnicities. Based on that, this study does not recommend the use of PSA alone, at a cut off of 4 ng/ml to be used as a modality in the diagnosis of PC.
Upon further elaboration of the above data, the conjunct use of DRE and PSA was considered as a two pronged approach to diagnosing PC. A very promising study conducted by Bretton, MD [17], yielded a very holistic set of results comparing the use of DRE and PSA as lone modalities as well as when being used in conjunction in a trial observing 1027 men. 78 (8%) had abnormal findings on DRE. 11 of these 78 men (14%) had prostate cancer. Thus, the overall cancer detection rate by DRE was 1%. When both DRE and PSA levels were abnormal, they found a 50% incidence of prostate cancer. However, of the 60 men with abnormal DRE and a normal PSA level, only 2 (3%) had prostate cancer, reflecting the low specificity of DRE. Of the 107 men who had a normal DRE but an abnormal PSA level, 28 (26% ) had prostate cancer, conversely reflecting the higher specificity of PSA levels. It appears that it perhaps would be prudent to use these modalities in conjunction, preferably followed by other confirmatory methods like ultrasound or biopsy, that would lead to a sound diagnostic algorithm for PC, the recommendation of which is beyond the scope of this study.
In conclusion, this study does not advocate the lone application of the stated modalities for the diagnosis of PC in a primary care setting, but in no manner does it discourage their use when followed upon by further confirmatory.
Funding
No financial benefits have been received by any author for this work.
Conflicts of Interest
The authors have no competing interest.
References
- Center, M., Siegel, R., and Jemal, A. (2011). American Cancer Society. Global Cancer Facts and Figures, 2nd Edn. Atlanta, GA: American Cancer Society, 1–58.
- A prospective evaluation of plasma prostate-specific antigen for detection of prostatic cancer - PubMed [Internet]. [cited 2023 Apr 28]. Available from: https://pubmed.ncbi.nlm.nih.gov/7529341/.
- Scardino PT, Weaver R, Hudson MA. Early detection of prostate cancer. Hum Pathol [Internet]. 1992 [cited 2023 Apr 19];23(3):211–22. Available from: https://pubmed.ncbi.nlm.nih.gov/1372877/.
- Brawer MK, Chetner MP, Beatie J, Buchner DM, Vessella RL, Lange PH. Screening for prostatic carcinoma with prostate specific antigen. J Urol [Internet]. 1992 [cited 2023 Apr 28];147(3 Pt 2):841–5. Available from: https://pubmed.ncbi.nlm.nih.gov/1371559/.
- Ekwueme DU, Stroud LA, Chen Y. Peer Reviewed: Cost Analysis of Screening for, Diagnosing, and Staging Prostate Cancer Based on a Systematic Review of Published Studies. Prev Chronic Dis [Internet]. 2007 [cited 2023 Apr 28];4(4). Available from: /pmc/articles/PMC2099265/.
- Smith DS, Catalona WJ, Herschman JD. Longitudinal screening for prostate cancer with prostate-specific antigen. JAMA [Internet]. 1996 Oct 23 [cited 2023 Apr 28];276(16):1309–15. Available from: https://pubmed.ncbi.nlm.nih.gov/8861989/.
- Song JM, Kim CB, Chung HC, Kane RL. Prostate-Specific Antigen, Digital Rectal Examination and Transrectal Ultrasonography: A Meta-Analysis for This Diagnostic Triad of Prostate Cancer in Symptomatic Korean Men. Yonsei Med J [Internet]. 2005 Jun 6 [cited 2023 Apr 28];46(3):414. Available from: /pmc/articles/PMC2815820/.
- Schröder FH, Van Der Maas P, Beemsterboer P, Kruger AB, Hoedemaeker R, Rietbergen J, et al. Evaluation of the Digital Rectal Examination as a Screening Test for Prostate Cancer. JNCI: Journal of the National Cancer Institute [Internet]. 1998 Dec 2 [cited 2023 Apr 28];90(23):1817–23. Available from: https://academic.oup.com/jnci/article/90/23/1817/2520677.
- Hoogendam A, Buntinx F, De Vet HCW. The diagnostic value of digital rectal examination in primary care screening for prostate cancer: a meta-analysis. Fam Pract [Internet]. 1999 Dec 1 [cited 2023 Apr 28];16(6):621–6. Available from: https://academic.oup.com/fampra/article/16/6/621/475662.
- Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009;6(7):e1000100. https://doi.org/10.1371/journal. pmed.1000100).
- Digital rectal examination is not useful to early detect prostate cancers - Uroweb [Internet]. [cited 2023 Apr 28]. Available from: https://uroweb.org/press-releases/digital-rectal-examination-is-not-useful-to-early-detect-prostate-cancers.
- Chodak GW, Keller P, Schoenberg HW. Assessment of screening for prostate cancer using the digital rectal examination. J Urol [Internet]. 1989 [cited 2023 Apr 28];141(5):1136–8. Available from: https://pubmed.ncbi.nlm.nih.gov/2709500/.
- The American Cancer Society National Prostate Cancer Detection Project. Findings on the detection of early prostate cancer in 2425 men - PubMed [Internet]. [cited 2023 Apr 28]. Available from: https://pubmed.ncbi.nlm.nih.gov/1710531/.
- Pedersen K V., Carlsson P, Varenhorst E, Lofman O, Berglund K. Screening for carcinoma of the prostate by digital rectal examination in a randomly selected population. Br Med J [Internet]. 1990 Apr 21 [cited 2023 Apr 28];300(6731):1041–4. Available from: https://www.bmj.com/content/300/6731/1041.
- Lee F, Littrup PJ, Torp-Pedersen ST, Mettlin C, McHugh TA, Gray JM, et al. Prostate cancer: comparison of transrectal US and digital rectal examination for screening. Radiology [Internet]. 1988 [cited 2023 Apr 28];168(2):389–94. Available from: https://pubmed.ncbi.nlm.nih.gov/3293108/.
- Kemple T, Chadwick DJ, Gillatt DA, Abrams P, Gingell JC, Astley JP, et al. Pilot study of screening for prostate cancer in general practice. Lancet [Internet]. 1991 Sep 7 [cited 2023 Apr 28];338(8767):613–6. Available from: https://pubmed.ncbi.nlm.nih.gov/1715503/.
- Bretton PR. Prostate-specific antigen and digital rectal examination in screening for prostate cancer: a community-based study. South Med J [Internet]. 1994 [cited 2023 Apr 28];87(7):720–3. Available from: https://pubmed.ncbi.nlm.nih.gov/7517580/.
- Andermann A, Blancquaert I, Beauchamp S, Déry V. Revisiting Wilson and Jungner in the genomic age: a review of screening criteria over the past 40 years. Bull World Health Organ [Internet]. 2008 Apr [cited 2023 Apr 28];86(4):317–9. Available from: https://pubmed.ncbi.nlm.nih.gov/18438522/.
- Catalona WJ, Smith DS, Ornstein DK. Prostate cancer detection in men with serum PSA concentrations of 2.6 to 4.0 ng/mL and benign prostate examination. Enhancement of specificity with free PSA measurements. JAMA [Internet]. 1997 May 14 [cited 2023 Apr 28];277(18):1452–5. Available from: https://pubmed.ncbi.nlm.nih.gov/9145717/.
- Catalona WJ, Smith DS, Ratliff TL, Basler JW. Detection of Organ-Confined Prostate Cancer Is Increased Through Prostate-Specific Antigen—Based Screening. JAMA [Internet]. 1993 Aug 25 [cited 2023 Apr 28];270(8):948–54. Available from: https://jamanetwork.com/journals/jama/fullarticle/408074.
- Catalona WJ, Richie JP, Ahmann FR, Hudson MA, Scardino PT, Flanigan RC, et al. Comparison of digital rectal examination and serum prostate specific antigen in the early detection of prostate cancer: results of a multicenter clinical trial of 6,630 men. J Urol [Internet]. 1994 [cited 2023 Apr 28];151(5):1283–90. Available from: https://pubmed.ncbi.nlm.nih.gov/7512659/.
- Thompson IM, Ankerst DP, Chi C, Goodman PJ, Tangen CM, Lucia MS, et al. Assessing prostate cancer risk: results from the Prostate Cancer Prevention Trial. J Natl Cancer Inst [Internet]. 2006 Apr 19 [cited 2023 Apr 28];98(8):529–34. Available from: https://pubmed.ncbi.nlm.nih.gov/16622122/.
- Weining C, Semjonow A, Hertle L. Nutzen verschiedener Verfahren zur Verbesserung der Spezifitat von PSA in der Prostatakarzinomdiagnostik. Urologe - Ausgabe B [Internet]. 1997 Apr 8 [cited 2023 Apr 28];37(3):216–20. Available from: https://link.springer.com/article/10.1007/s001310050078.
Figure 2.
Forest plots of PSA cutoff level of more than 4 ng/ml and/or DRE VS biopsy in the detection of prostatic cancer.
Figure 2.
Forest plots of PSA cutoff level of more than 4 ng/ml and/or DRE VS biopsy in the detection of prostatic cancer.
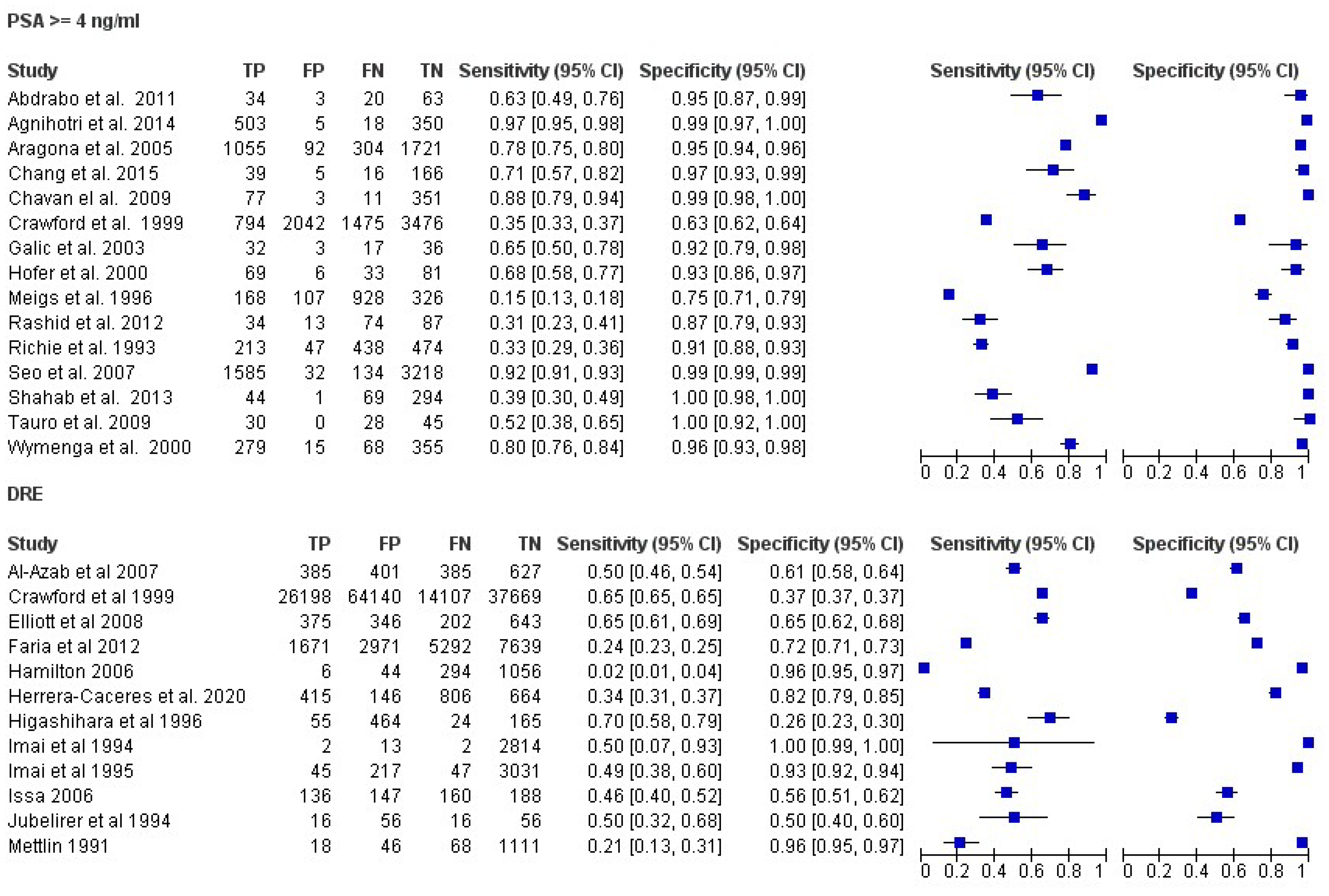
Figure 3.
Summary receiver operating characteristic (ROC) curve for PSA and/or DRE in prostatic cancer in all studies.
Figure 3.
Summary receiver operating characteristic (ROC) curve for PSA and/or DRE in prostatic cancer in all studies.
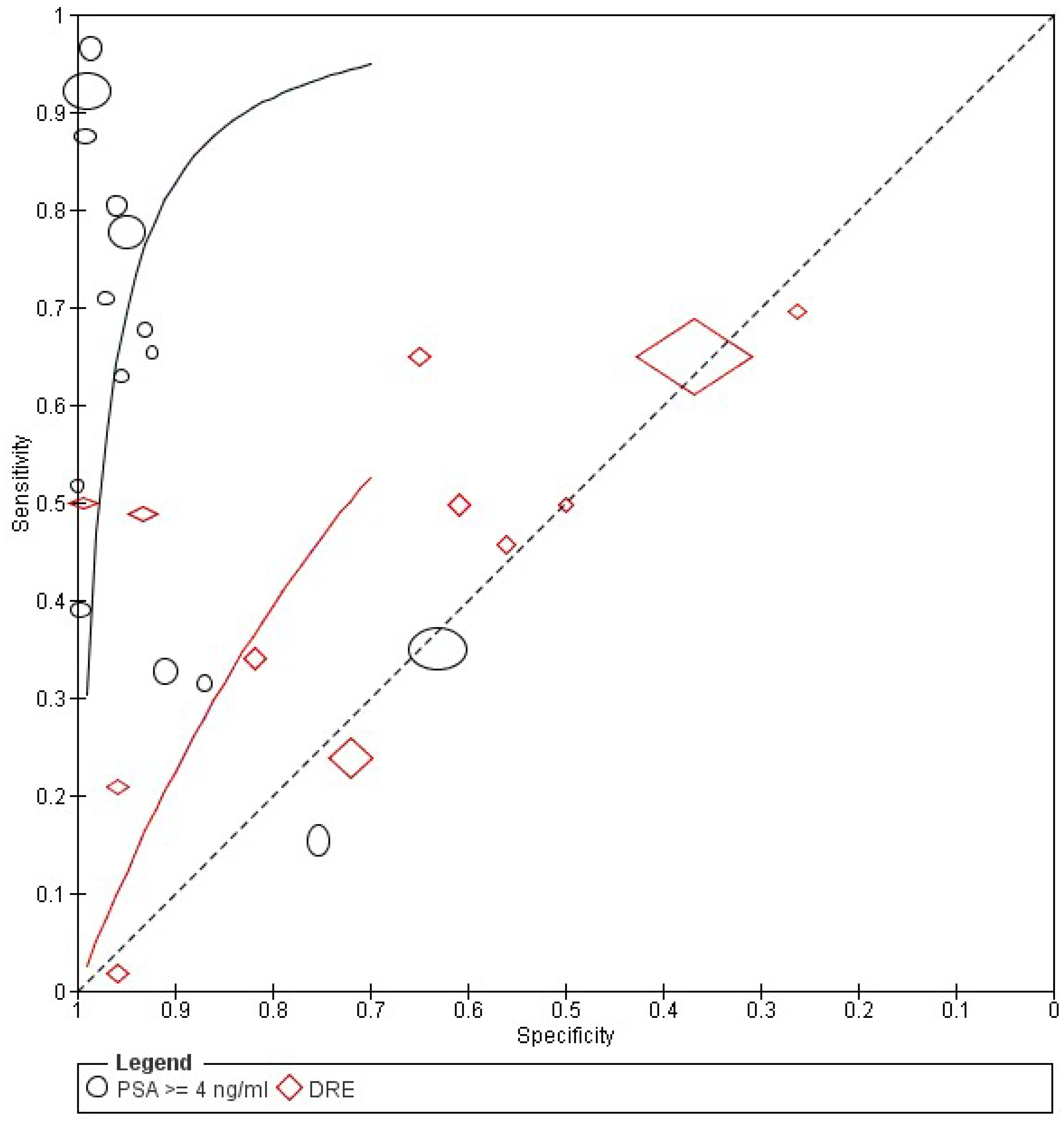
Figure 4.
Forest plot of PSA diagnostic odds ratio.
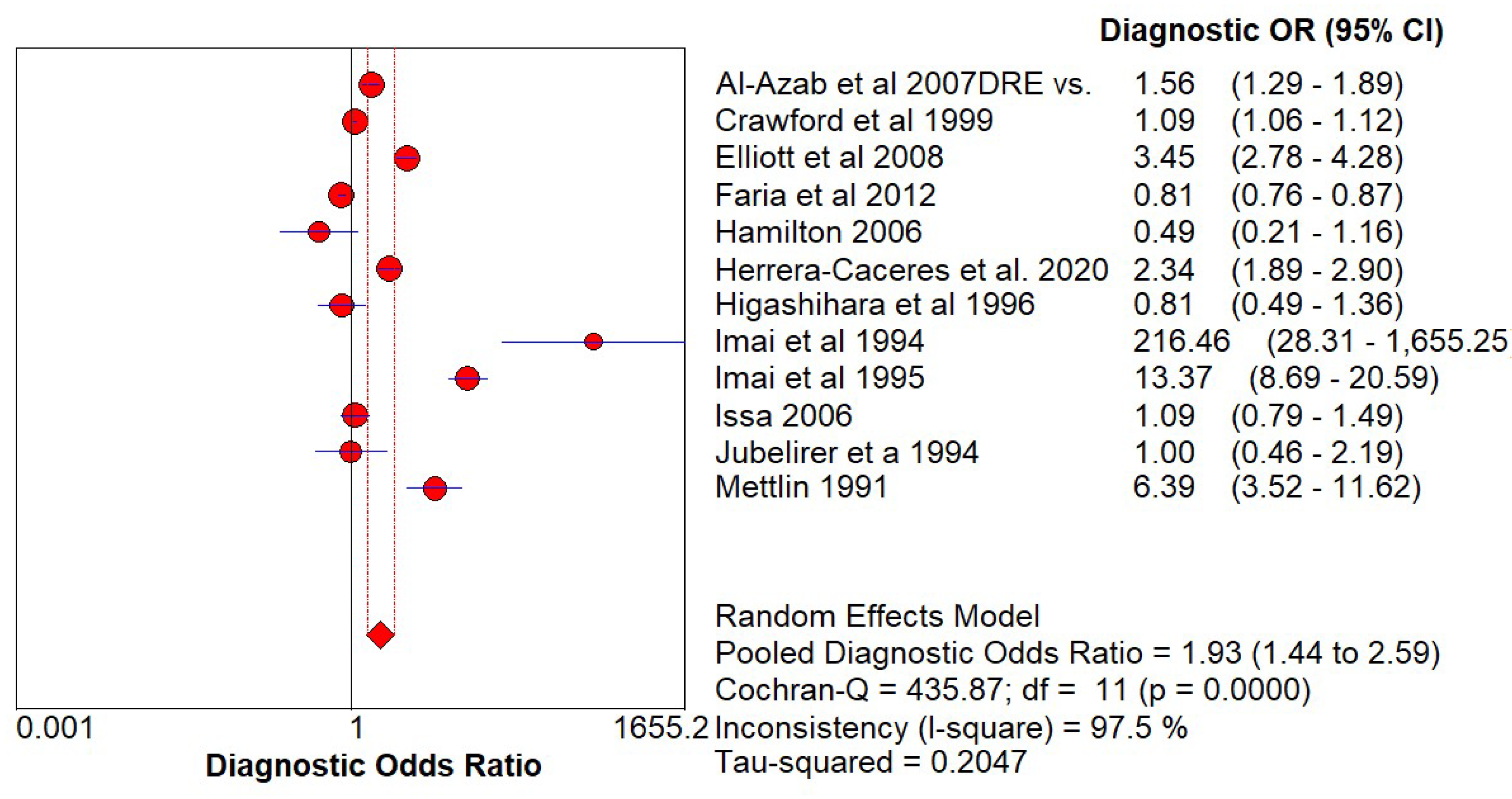
Figure 5.
Forest plot of DRE diagnostic odds ratio.
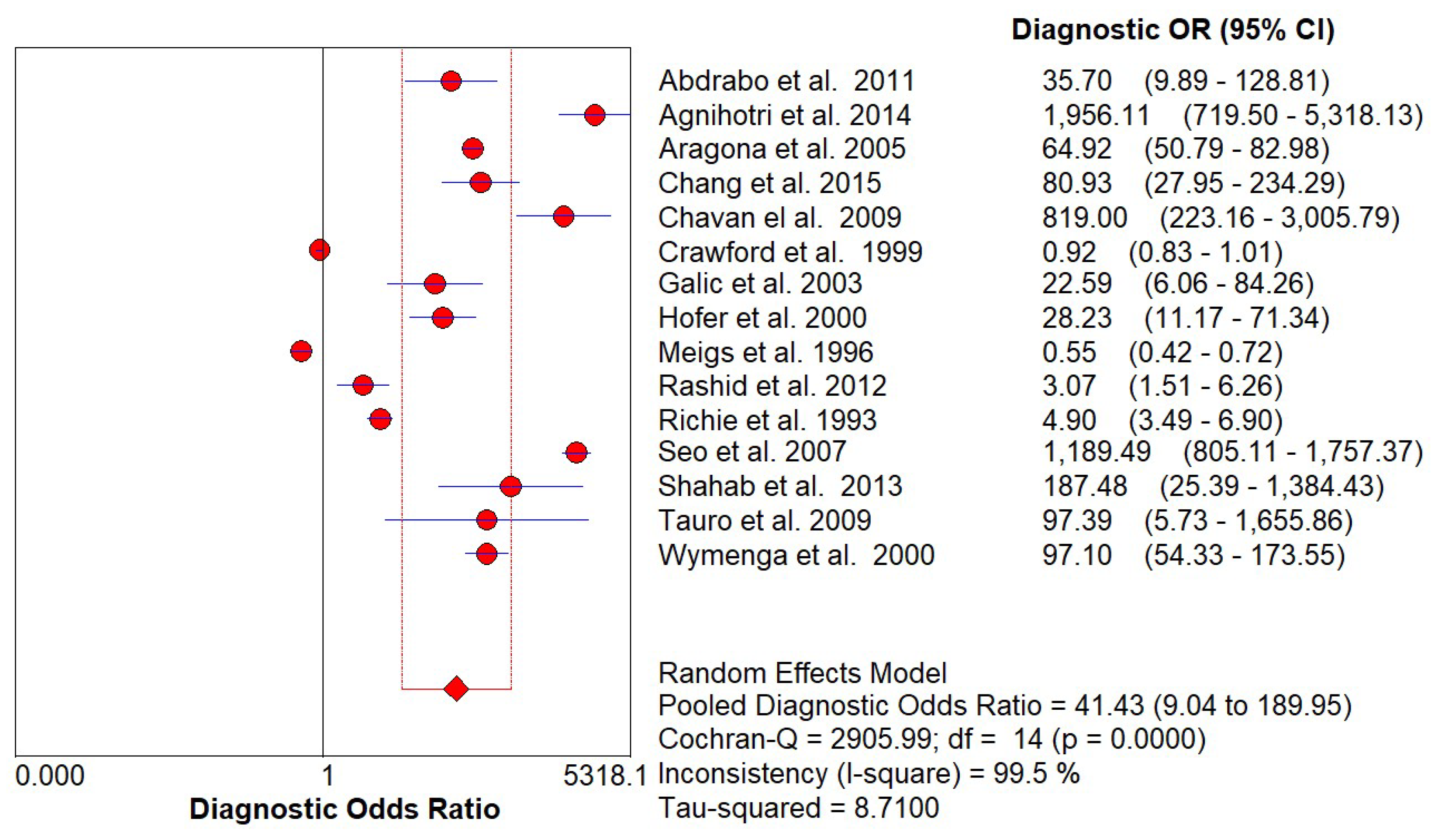
Figure 6.
Funnel plot for publication bias of the 12 PSA included studies.
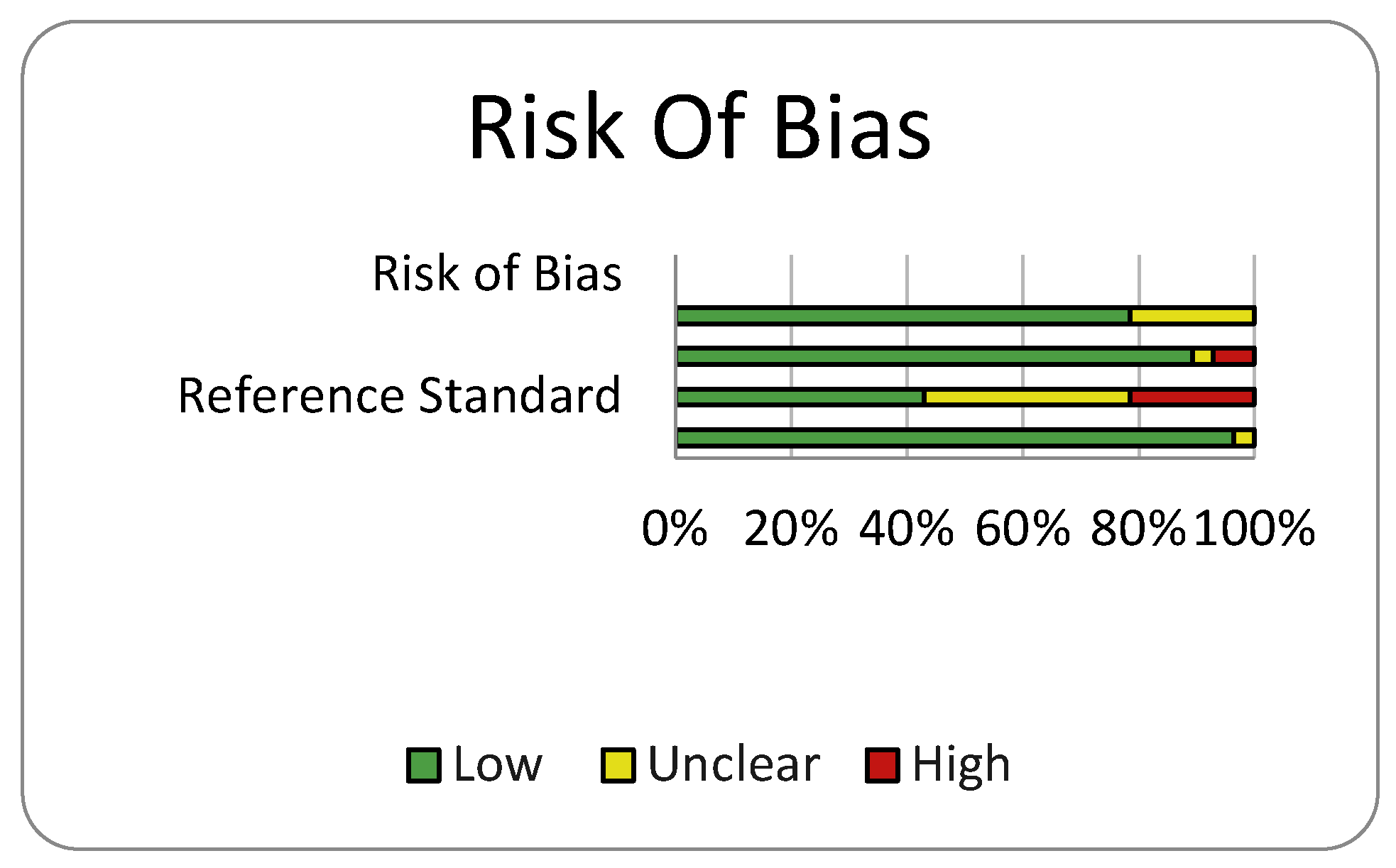
Figure 7.
Funnel plot for publication bias of the 12 DRE included studies.
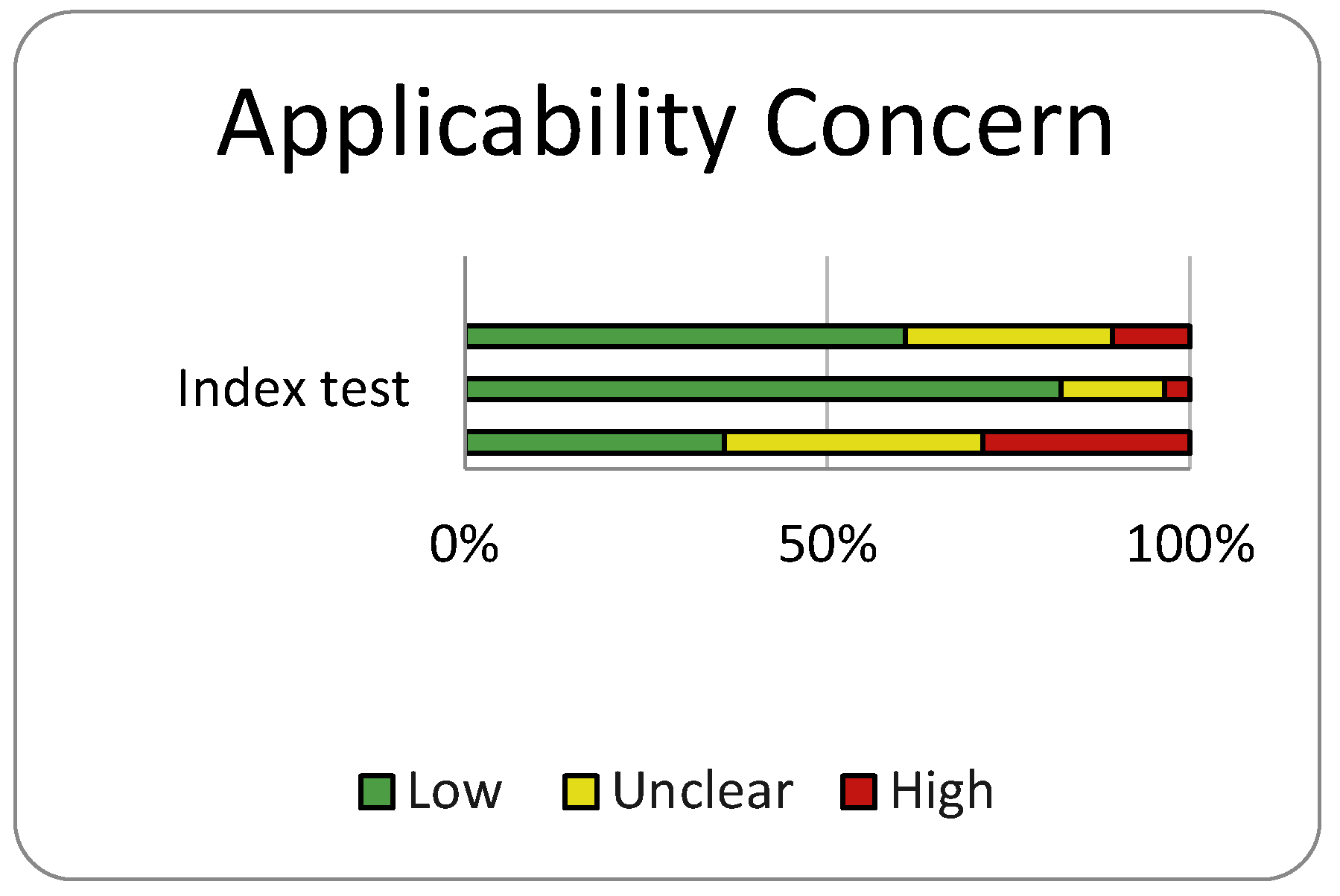
Figure 8.
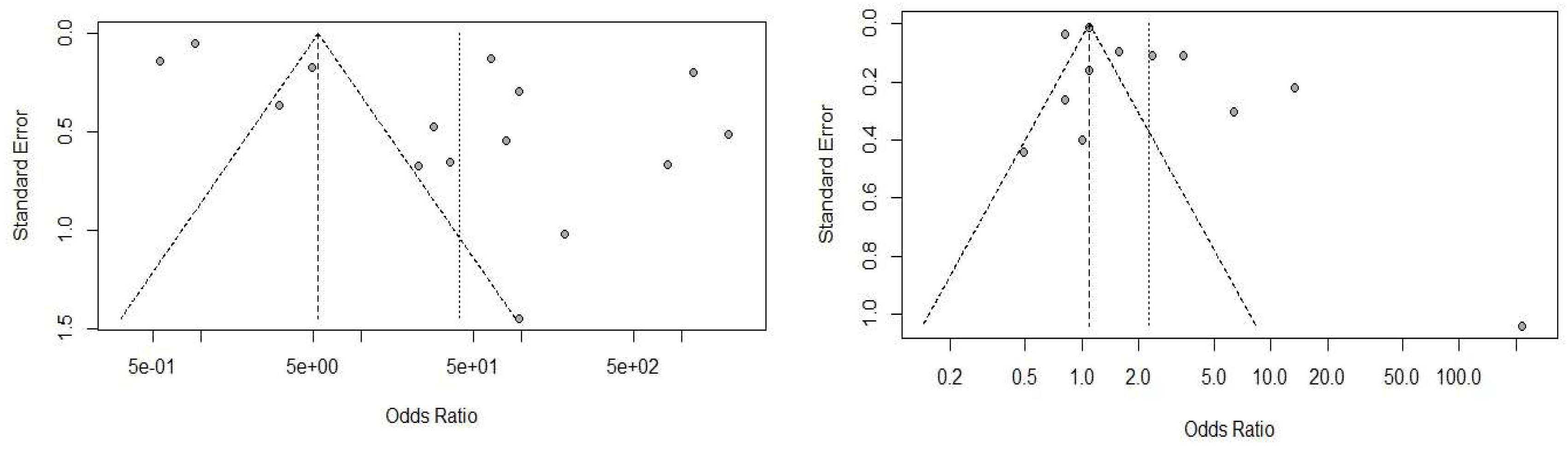

Table 1.
General characteristcis of the studies.
| Study | Year | Country | Design | Patients Number | Patients Underwent Biopsy No | Age Range | Diagnostic Criteris | Reference Test |
|---|---|---|---|---|---|---|---|---|
| Chang et al. | 2015 | Taiwan | Retrospective chart review | 225 | 225 | N/A | PSA ≥ 4 ng/mL | Biopsy |
| Agnihotri et al. | 2014 | India | Prospective study | 4702 | 875 | 50-75 | PSA ≥ 4 ng/mL | Biopsy |
| Shahab et al. | 2013 | Indonesia | Retrospective study | 404 | 404 | 34-84 | PSA ≥ 4 ng/mL | Biopsy |
| Rashid et al. | 2012 | Bangladesh | Prospective study | 206 | 206 | Over50 | PSA ≥ 4 ng/mL | Biopsy |
| Abdrabo et al. | 2011 | Sudan | Prospective study | 118 | 118 | 56-83 | PSA ≥ 4 ng/mL | Biopsy |
| Chavan el al. | 2009 | India | Retrospective study | 922 | 440 | 40-95 | PSA ≥ 4 ng/mL | Biopsy |
| Tauro et al. | 2009 | India | Prospective study | 100 | 100 | 56-75 | PSA ≥ 4 ng/mL | Biopsy |
| Seo et al. | 2007 | Korea | Prospective study | 4967 | 4967 | 40-96 | PSA ≥ 4 ng/mL | Biopsy |
| Aragona et al. | 2005 | Italy | Prospective cohort study | 16298 | 3171 | 40-75 | PSA ≥ 4 ng/mL | Biopsy |
| Galic et al. | 2003 | Croatia | Prospective controlled study | 944 | 88 | Over 50 | PSA ≥ 4 ng/mL | Biopsy |
| Hofer et al. | 2000 | Germany | Prospective study | 188 | 188 | 40-79 | PSA ≥ 4 ng/mL | Biopsy |
| Wymenga et al. | 2000 | The Netherlands | Prospective study | 716 | 716 | N/A | PSA ≥ 4 ng/mL | Biopsy |
| Crawford et al. | 1999 | USA | Retrospective of prospectively collected data. | 142111 | 4160 | 40-79 | PSA ≥ 4 ng/mL/ DRE | Biopsy |
| Meigs et al. | 1996 | USA | Retrospective of prospectively collected data. | 1554 | N/A | 50-79 | PSA ≥ 4 ng/mL | Biopsy |
| Richie et al. | 1993 | USA | Prospective clinical trial. | 6630 | 1167 | 50-96 | PSA ≥ 4 ng/mL | Biopsy |
| Al-Azab et al. | 2007 | Canada | Retrospective chart review | 1796 | 1796 | 40-93 | DRE/PSA | Biopsy |
| Elliott et al. | 2008 | USA | Retrospective review of prospectively collected data | 1564 | 1564 | 60-75 | DRE/PSA | Biopsy |
| Faria et al. | 2012 | Brazil | Prospective cohort study | 17571 | 1647 | 45-98 | DRE/PSA | Biopsy |
| Higashihara et al. | 1996 | Japan | Prospective clinical trial | 701 | 116 | 50-92 | DRE/PSA | Biopsy |
| Imai et al. | 1994 | Japan | Prospective study | 1680 | 132 | 39-89 | DRE/PSA | Biopsy |
| Imai et al. | 1995 | Japan | Prospective study | 3276 | 254 | 40-89 | DRE/PSA | Biopsy |
| Jubelirer et a | 1994 | USA | Prospective study | 142 | 15 | 50-85 | DRE/PSA | Biopsy |
| Mettlin | 1991 | USA | Prospective cohort study | 1218 | 330 | 55-70 | DRE/PSA | Biopsy |
| Hamilton | 2006 | UK | Case-control | 1297 | 217 | Over 40 | DRE/PSA | Biopsy |
| Issa | 2006 | USA | Retrospective cohort study | 628 | 628 | 40-89 | DRE/PSA | Biopsy |
| Herrera-Caceres | 2020 | Canada | Retrospective study | 2031 | 2031 | 60-71 | DRE/PSA | Biopsy |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



