
Submitted:
22 January 2025
Posted:
22 January 2025
You are already at the latest version
Abstract
Most people living with HIV (PLWH) are co-infected with syphilis or other sexually transmitted infections (STIs) and experience frequent reactivations of syphilis. Thus, syphilis or other STIs are highly prevalent in most regions experiencing severe HIV epidemics. In sub-Saharan Africa, the region most heavily affected by HIV, the prevalence of syphilis among PLWH is approximately 7.3%. This region accounts for 40% of global STIs and 70% of HIV cases, highlighting the need for targeted research. Despite the high prevalence of syphilis among PLWH in the region, the impact of syphilis on HIV transmission and HIV disease progression has not been well-studied. In this manuscript, we evaluated if syphilis facilitates HIV acquisition and HIV disease progression in the region. We used retrospective data from 53,915 adult participants enrolled through Population-based HIV Impact Assessment (PHIA) surveys conducted in Zambia and Tanzania. Logistic regression models were used to assess the impact of syphilis on HIV acquisition and disease progression. Our findings indicated that syphilis infection was associated with higher odds of HIV acquisition. Moreover, co-infection with syphilis was associated with higher odds of HIV disease progression among PLWH treated with antiretroviral therapy (ART). Our findings suggested that the recognition, treatment, and prevention of syphilis to reduce the risk of HIV transmission and HIV disease progression should be a public health priority in sub-Saharan Africa, where ART may not be readily available.
Keywords:
HIV/AIDS
; Syphilis
; Propensity Score Matching
; ART
; Acquisition
; Progression
1. Introduction
Syphilis is still a modern-day pandemic that affects millions of individuals globally and is becoming more common [1]. Treponema pallidum is the bacterium that causes syphilis [2,3]. Syphilis mainly spreads through sexual activity (anal, genital, or oral) [1]. The infection progresses through four stages (primary, secondary, latent, and tertiary), with signs and symptoms varying at each stage [2,3]. If left untreated, syphilis can impact multiple organs over the years or even decades as it advances through its various stages [1,2,3]. It can also be transmitted from mother to fetus, leading to congenital syphilis, which may result in complications such as stillbirth, miscarriage, and low birth weight [2,3,4,5]. In 2022, the World Health Organization (WHO) projected that 8 million people aged 15 to 49 contracted syphilis globally, with an additional 700,000 cases of congenital syphilis [6,7]. New syphilis cases among adults aged 15 to 49 rose from 7.1 million in 2020 to 8.0 million in 2022 [8]. The global prevalence rate of syphilis was reported to be 0.6% [95%CI, 0.5%–0.7%] in both men and women, and congenital syphilis at a rate of 523/100,000 live births [3,6,7]. Notably, certain countries that systematically track syphilis have reported significant increases, particularly among MSM and cases of congenital syphilis [6]. An estimated 7.5% of MSM worldwide are infected with syphilis, compared to just 0.6% of men in the general population [6]. The World Health Organization (WHO) has set two goals for 2030: (1) to reduce the global incidence of syphilis by 90% and (2) to decrease the rate of congenital syphilis to ≤50 cases per 100,000 live births [6,9]. Penicillin or doxycycline medication is the conventional treatment for syphilis [1,2,3]. However, the requirement for injections, medication shortages, and allergies are obstacles to taking penicillin, and doxycycline is not recommended for pregnant women [1,2,3].
Syphilis and other sexually transmitted infections (STIs) worldwide are most common among PLWH[1,2,4]. HIV infection is complex on its own, but when it coexists with syphilis or other STIs, the severity of each infection increases and can lead to treatment failure [1,10,11]. Syphilis and HIV share common risk factors like lower education level, having multiple sexual partners, and alcohol consumption [12,13,14]. Syphilis and HIV have a bi-directional relation where syphilis could increase the risk of HIV transmission, and HIV could also accelerate the progression of syphilis [11,15,16]. Prior studies have indicated that the serious side effects linked to untreated syphilis may contribute to HIV infection transmission and acquisition [12]. The presence of syphilitic sores or ulcers, particularly in genital or anal areas, creates entry points for HIV, facilitating easier transmission during unprotected sexual contact. The inflammatory response caused by syphilis also increases immune cells like CD4 T cells in affected tissues, which are the primary targets for HIV, heightening the risk of infection [2]. The risk of HIV infection doubles in individuals with syphilis, as does the likelihood of contracting other STIs, such as gonorrhea, chlamydia, and genital herpes [3]. Thus, screening and treating syphilis play a key role in reducing HIV incidence [12]. In individuals co-infected with HIV and syphilis, HIV could alter syphilis symptoms, making it more challenging to diagnose and treat accurately, sometimes resulting in false positive or negative serology results [11,15,16,17]. Preventative strategies like doxycycline postexposure prophylaxis (doxy-PEP), which refers to taking the antibiotic doxycycline after exposure to STIs, have shown promise in reducing syphilis incidence in high-risk populations [18,19]. Several studies have shown that doxy-PEP led to a nearly 70% reduction in syphilis among MSM using HIV preexposure prophylaxis (PrEP) [18,20,21].
Antiretroviral therapy (ART) has proven to be highly effective in managing HIV in PLWH. Early ART initiation and adherence to ART reduce disease progression and death while also preventing new cases from spreading [22]. While there is compelling evidence of the effect of ART on HIV viral load (VL) suppression, the impact of STIs like syphilis on the efficacy of ART has not been well studied, especially in sub-Saharan Africa, where HIV-syphilis co-infection is common. Frequent activation of syphilis can reoccur among PLWH. A recent study found that syphilis prevalence among PLWH in the sub-Saharan African region was approximately 7.3% [95% CI, 6.3%–8.5%] [4]. Another study has shown that around 45% of PLWH with suppressed VL were still diagnosed with syphilis [23]. Research on HIV-positive men with secondary syphilis, for example, found significant increases in HIV VL during syphilis infection, particularly in those not on ART [24,25]. Even among those on ART, syphilis caused detectable increases in VL in some cases [24,25]. In PLWH, untreated syphilis is linked to substantial neurologic and cardiovascular consequences as well as significant morbidity and mortality [3,4]. Some studies suggest that syphilis co-infection in PLWH can cause temporary increases in HIV VL, which may lead to a sustained loss of VL suppression [26]. Thus, reducing the risk of recurrent syphilis among PLWH enhances their ability to maintain HIV VL suppression. Additionally, other research indicates that individuals on highly active antiretroviral therapy (HAART) may experience an improved serological response to syphilis [26,27]. These findings suggest that incorporating doxy-PEP as part of a broader HIV prevention strategy may enhance the efficacy of ART treatment among PLWH.
HIV-syphilis co-infection causes challenges in the treatment and prevention of HIV, especially in sub-Saharan Africa, where ART is not readily available and the region that bears 40% of the global burden of STIs and 70% of the global HIV burden [8]. In this paper, we used retrospective data from 53,915 adult participants to study the role syphilis plays in HIV acquisition, transmission, and disease progression. The participants were enrolled through population-based surveys in Zambia and Tanzania.
2. Materials and Methods
Study Design and Participants: In this study, we did a secondary analysis of retrospective cross-sectional data collected through the Population-based HIV Impact Assessment (PHIA) surveys conducted in Zambia and Tanzania. The PHIA project was funded by the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) and technically supported by the International Center for AIDS Care and Treatment Programs (ICAP) at Columbia University through the U.S. Centers for Disease Control and Prevention (CDC) [28,29,30,31]. Written informed consent was obtained at every survey stage (head of the household interview, individual interview, and blood sample collection). All survey materials, including questionnaires and consent forms, were translated from English into local languages. The survey covered various aspects, including a household questionnaire, individual interviews addressing HIV care and treatment, HIV knowledge, behavioral risk factors associated with HIV incidence and prevalence, and questions on co-infections such as syphilis, tuberculosis, hepatitis B, and cervical cancer. Eligible participants aged 15 years and more completed a standardized questionnaire and provided blood samples for HIV and syphilis testing [31,32]. HIV home-based testing and counseling (HBTC) was conducted following national guidelines, using a sequential rapid-test algorithm that included the Determine HIV-1/2 test (Abbott Molecular Inc., Des Plaines, Illinois, US) as the screening test and the Uni-Gold test (Trinity Biotech, Wicklow, Ireland) as the confirmatory test. Individuals with reactive results on both tests were identified as HIV-positive and referred to HIV care and treatment services. Whereas syphilis testing was conducted using Chembio DPP Syphilis Screen & Confirm Assay (Chembio Diagnostic Systems, Inc, Medford, NY, U.S.) to detect antibodies against treponemal and non-treponemal antigens. Active syphilis infection is defined as the presence of both treponemal and non-treponemal antibodies, whereas a history of syphilis is defined as the presence of only treponemal antibodies. The methodology, including survey questionnaires, study design, and testing procedures, was described previously [31,32,33].
Study Outcome and Covariates: The primary outcomes of interest in this paper were HIV acquisition and HIV disease progression. HIV disease progression was assessed among the ART-treated PLWH by lack of HIV RNA VL suppression, defined as ≥ 1000 copies/mL. The covariates we considered include socio-demographic factors (such as age and gender), STI (co-infection) status, and clinical variables (such as duration on ART, ART initiation 12 months or more before the survey, and CD4 T cell count).
Statistical Analysis: Descriptive measures and statistical graphs were used to summarize data. Continuous variables such as age and CD4 T-cell count were summarized using medians and interquartile ranges (IQRs), while categorical variables were presented as frequencies and percentages. Categorical variables were compared between groups using Fisher’s exact test, whereas the nonparametric Wilcoxon rank-sum test was used for comparing continuous study variables. The main objectives of our analyses were twofold: The first objective was to evaluate the impact of syphilis on HIV disease acquisition. Logistic regression models were used to assess the impact of syphilis on HIV acquisition after adjusting for the effect of other factors such as age and gender. The second objective was to evaluate the impact of syphilis on HIV disease progression in ART-treated PLWH. HIV disease progression was defined by the failure of HIV RNA viral load (VL) suppression. We used propensity score matching (PSM) to reduce potential confounding and ascertain the independent impact of syphilis on HIV disease progression. HIV patients co-infected with syphilis were matched for age and gender with HIV patients without syphilis co-infection. The matching was done in R using the MatchIt package. HIV RNA VL suppression rates were analyzed by comparing participants co-infected with syphilis with age-gender-matched HIV participants without syphilis co-infection. Logistic regression models were used to assess the impact of syphilis on VL suppression after adjusting for the effect of other confounding variables such as CD4 T cell count, duration on ART treatment, and ART initiation 12 months or more before the survey.
3. Results
We analyzed data from 21,280 participants in Zambia and 32,635 participants in Tanzania who took part in the surveys. Participant’s ages ranged from 15 to 59 years in Zambia and 15 to 64 years in Tanzania. Table 1 provides an overview of the participant characteristics. The median age of the participants was 29 [IQR= 21-39] years in Zambia and 31 [IQR= 22-45] years in Tanzania. In both countries, female participation was higher than male, with females making up 57% (n=12,109) in Zambia and 56% (n=18,172) in Tanzania. A total of 19,157 (90%) participants from Zambia and 32,634 (99%) from Tanzania were tested for syphilis. Of those tested, 2.8% (n=591) in Zambia and 1% (n=328) in Tanzania were tested positive for an active syphilis. More than 6% of participants in both countries had a history of syphilis, with 6.4% (n=1,361) in Zambia and 6.2% (n=2,026) in Tanzania. A total of 19,115 participants in Zambia and all participants in Tanzania were screened for HIV. Among those screened, 11.6% (n=2,467) in Zambia and 5.8% (n=1,895) in Tanzania were tested positive for HIV. Of those who tested positive for HIV and started ART, 7% (n=1,465) in Zambia and 3% (n=994) in Tanzania achieved VL suppression.

Table 1.
Characteristics of participants in the survey in Zambia and Tanzania.
| Zambia (n=21,280) | Tanzania (n=32,635) | |
|---|---|---|
| Variable | N (%) | N (%) |
| Age | 29 (IQR: 21-39) | 31 (IQR: 22-45) |
| Female Gender | 12,109 (56.9%) | 18,172 (55.7%) |
| Male | 9,171 (43.1%) | 14,463 (44.3 %) |
| Active syphilis | ||
| Yes | 591 (2.8%) | 328 (1%) |
| No | 18,566 (87.2%) | 32,306 (99%) |
| Ever syphilis | ||
| Yes | 1,361 (6.4%) | 2,026 (6.2%) |
| No | 17,796 (83.6%) | 30,608 (93.8%) |
| HIV Acquired | 2,467 (11.6%) | 1,895 (5.8%) |
| Viral Load suppressed | 1,465 (6.9%) | 994 (3%) |
Table 2 outlines the characteristics of the study participants by HIV acquisition status in Zambia and Tanzania. Among those screened for HIV, 13% (n=2,467) in Zambia and 6% (n=1,895) in Tanzania were tested positive for HIV. The median age of the participants was notably higher among PLWH, with a median age of 38 years [ IQR= 30-45] in Zambia and 39 years [IQR: 30-47] in Tanzania, suggesting that older individuals were more susceptible to acquiring HIV (p <0.001). In both countries, most of the PLWH were females: 69% (n=1,688) in Zambia and 69% (n=1,297) in Tanzania. Moreover, participants with active syphilis or a history of syphilis were found to be at increased risk of HIV acquisition. Among participants with active syphilis, 9.1% (n=225) tested positive, and 2.2% (n=366) tested negative for HIV in Zambia. Similarly, in Tanzania, among the participants with active syphilis, 4.0% (n=76) tested positive, and 0.8% (n=252) tested negative for HIV. As with the case of active syphilis, a history of syphilis was also significantly (p<0.001) associated with an increased risk of HIV acquisition in both countries. In Zambia, among the participants with a history of syphilis infection, 16.4% (n=406) were HIV positive compared to 5.7%(n=955) of HIV negative. Similarly, in Tanzania, among the participants having a history of syphilis, 14.3% (n=271) were tested as HIV positive compared to 5.7%(n=1,755) as HIV negative (p<0.001). In conclusion, our analysis indicates that older age, female gender, and active syphilis infection or history of syphilis were associated with an increased risk of HIV acquisition.
Table 2.
Characteristics of participants by HIV acquisition status in Zambia and Tanzania.
| Zambia | Tanzania | |||||
|---|---|---|---|---|---|---|
| Variable | HIV positive (n=2,467, 12.9%) | HIV negative (n=16,648, 87.1%) | P-Value | HIV positive (n=1,895, 5.8%) | HIV negative (n=30,740, 94.2%) | P-Value |
| N (%) | N (%) | N (%) | N (%) | |||
| Age | 38 (IQR: 30-45) | 27 (IQR: 20-38) | < 0.001 | 39 (IQR: 30-47) | 30 (IQR: 21-44) | < 0.001 |
| Female Gender | 1,688 (68.4%) | 9,285 (55.8%) | < 0.001 | 1,297 (68.4%) | 16,875 (54.9%) | < 0.001 |
| Active syphilis | ||||||
| Yes | 225 (9.1%) | 366 (2.2%) | < 0.001 | 76 (4%) | 252 (0.8%) | < 0.001 |
| No | 2,242(90.9%) | 16281(97.8%) | 1,819(96%) | 30,487(99.2%) | ||
| Ever syphilis | ||||||
| Yes | 406 (16.4%) | 955 (5.7%) | < 0.001 | 271 (14.3%) | 1,755 (5.7%) | < 0.001 |
| No | 2,061(83.6%) | 15,692(94.3%) | 1,624(85.7%) | 28,984(94.3%) | ||
In both countries, less than 20% of the PLWH were co-infected with syphilis. For this reason, we used propensity score matching (PSM) to select age-gender-matched PLWH without syphilis for each co-infected subject. Table 3 displays the patient characteristics by HIV VL suppression status for co-infected PLWH and the matched PLWH without syphilis infection. Among PLWH, 61.5% (n=487) in Zambia and 55% (n=299) in Tanzania achieved VL suppression after receiving ART treatment. In Zambia, the proportion of PLWH who achieved VL suppression was lower in those with active syphilis (26.1%, n=127) compared to those without active syphilis (73.9%, n=360). Similarly, in Tanzania, the proportion of PLWH and active syphilis achieved VL suppression is lower (12.0%, n=36) compared to those without active syphilis (88%, n=263). However, this difference was not statistically significant (p=0.123 in Zambia and p=0.171 in Tanzania). In Zambia, PLWH with a history of syphilis also achieved less VL suppression (49.7%, n=242) compared to those without any history of syphilis (50.3%, n=245), though the difference was not too high. On the contrary, in Tanzania, the proportion of PLWH with a history of syphilis achieved higher VL suppression rates (52.5%, n=157) compared to those without any history of syphilis (47.5%, n=142). This difference was also not statistically significant (p=0.715 in Zambia and p=0.226 in Tanzania). Hence, PLWH infected with co-infections like syphilis are less likely to achieve VL suppression, making it a contributing factor for HIV disease progression. Table 3 also compares other covariates by suppression status. In Zambia, PLWH who achieved VL suppression were older (median = 40 years, IQR = 32–46) than those without suppression (median = 32 years, IQR = 28–42). A similar trend was observed in Tanzania, where the median age of those with VL suppression was 43 years (IQR: 36–52), compared to those without suppression (median= 40 years, IQR: 32-49), making age a significant factor in achieving VL suppression (p <0.001). In both countries, participants with VL suppression had higher CD4 T-cell counts. In Zambia, the median CD4 T-cell count was higher among virally suppressed participants with 475 cells/µL [IQR: 344-635] compared to those without suppression at 333 cells/µL [IQR: 207-492.5], which was statistically significant (p <0.001). A similar trend was observed in Tanzania, where participants with VL suppression have a higher median CD4 T-cell count of 483.5 cells/µL [IQR: 346.8-655] compared to those without suppression at 328 cells/µL [IQR: 191-485] which was statistically significant (p<0.001). Although a higher proportion of females achieved VL suppression in both countries, gender was not statistically significant (p=0.07 in Zambia and p=0.06 in Tanzania) in achieving viral suppression. In Zambia, participants taking ART medication achieved higher VL suppression rates (93.8%, n=457) compared to those without suppression (10.8%, n=33). Similarly, in Tanzania, 88.6% (n=265) of the PLWH taking ART medication achieved VL suppression compared to 13.6%(n=33) without suppression, and it was statistically significant (p<0.001). In Zambia, PLWH achieved higher VL suppression (70.4%, n=343) who had started ART treatment 12 months or more before the survey, compared to those without suppression (11.1%, n=34),) and it was not statistically significant (p =0.29). A similar trend is observed in Tanzania, with 56.5% (n=169) of PLWH achieving higher VL suppression in those who had started ART 12 months or more before the survey compared to the 11.1%(n=27) without suppression, and it was also not statistically significant (p=0.219). The duration on ART is divided into four categories (not on ART, less than 12 months on ART, 12-23 months, and 24 months or more duration on ART). In Zambia, a lower proportion of PLWH achieved VL suppression (14.2%, n=69) who were not receiving ART treatment compared to those who were not virally suppressed (86.5%, n=264). A similar trend is seen in Tanzania, with 11% (n=33) of PLWH who were not on ART achieved VL suppression compared to 81.9%(n=199) without viral suppression. Whereas, in Zambia, PLWH who are on ART treatment for 24 months or more achieved higher VL suppression (57.3%, n=279) when compared to PLWH on ART treatment for 12-23 months (11.5%, n=56) and less than 12 months (13.5%, n=66). Similarly, in Tanzania, higher VL suppression was achieved among PLWH and on ART treatment for 24 months or more (62.2%, n=186) when compared to PLWH on ART treatment for 12-23 months (9%, n=27) and less than 12 months (0%). ART Duration was statistically significant in achieving VL suppression (p<0.001) in both countries. In summary, our analysis indicated that in PLWH, active syphilis and a history of syphilis were associated with a lack of VL suppression or HIV disease progression.
Table 3.
Characteristics of participants by HIV progression status in Zambia and Tanzania.
| Zambia | Tanzania | |||||
|---|---|---|---|---|---|---|
| Variable | HIV suppressed (n=487, 61.5%) | HIV not suppressed (n=305, 38.5%) | P-Value | HIV suppressed (n=299, 55.1%) | HIV not suppressed (n=243, 44.8%) | P-Value |
| N (%) | N (%) | N (%) | N (%) | |||
| Age | 40 (IQR: 32-46) | 32 (IQR: 28-42) | < 0.001 | 43 (IQR: 36-52) | 40 (IQR: 32-49) | < 0.001 |
| CD4 count | 475 (IQR: 344-635) | 333 (IQR:207-492.5) | < 0.001 | 483.5 (IQR: 346.8-655) | 328 (IQR: 191-485) | < 0.001 |
| Female Gender | 332 (68.2%) | 189 (62%) | 0.07 | 196 (65.5%) | 140 (57.6%) | 0.06 |
| Active syphilis | ||||||
| Yes | 127 (26.1%) | 95 (31.1%) | 0.1235 | 36 (12.0%) | 40 (16.5%) | 0.171 |
| No | 360(73.9%) | 210(68.9%) | 263(88%) | 203(83.5%) | ||
| Ever syphilis | ||||||
| Yes | 242 (49.7%) | 156 (51.1%) | 0.7153 | 157 (52.5%) | 114 (46.9%) | 0.2266 |
| No | 245(50.3%) | 149(48.9%) | 142(47.5%) | 129(53.1%) | ||
| ART status | 457 (93.8%) | 33 (10.8%) | < 0.001 | 265 (88.6%) | 33 (13.6%) | < 0.001 |
| ART initiation | 343 (70.4%) | 34 (11.1%) | 0.29 | 169 (56.5%) | 27 (11.1%) | 0.219 |
| ART duration | ||||||
| Not on ART | 69 (14.2%) | 264 (86.5%) | < 0.001 | 33 (11.0%) | 199 (81.9%) | < 0.001 |
| On ART <12 months | 66 (13.5%) | 10 (3.3%) | 0 (0%) | 0 (0%) | ||
| On ART 12-23 months | 56 (11.5%) | 4 (1.3%) | 27 (9%) | 5 (2%) | ||
| On ART 24 months or more | 279 (57.3%) | 26 (8.5%) | 186 (62.2%) | 25 (10.3%) | ||
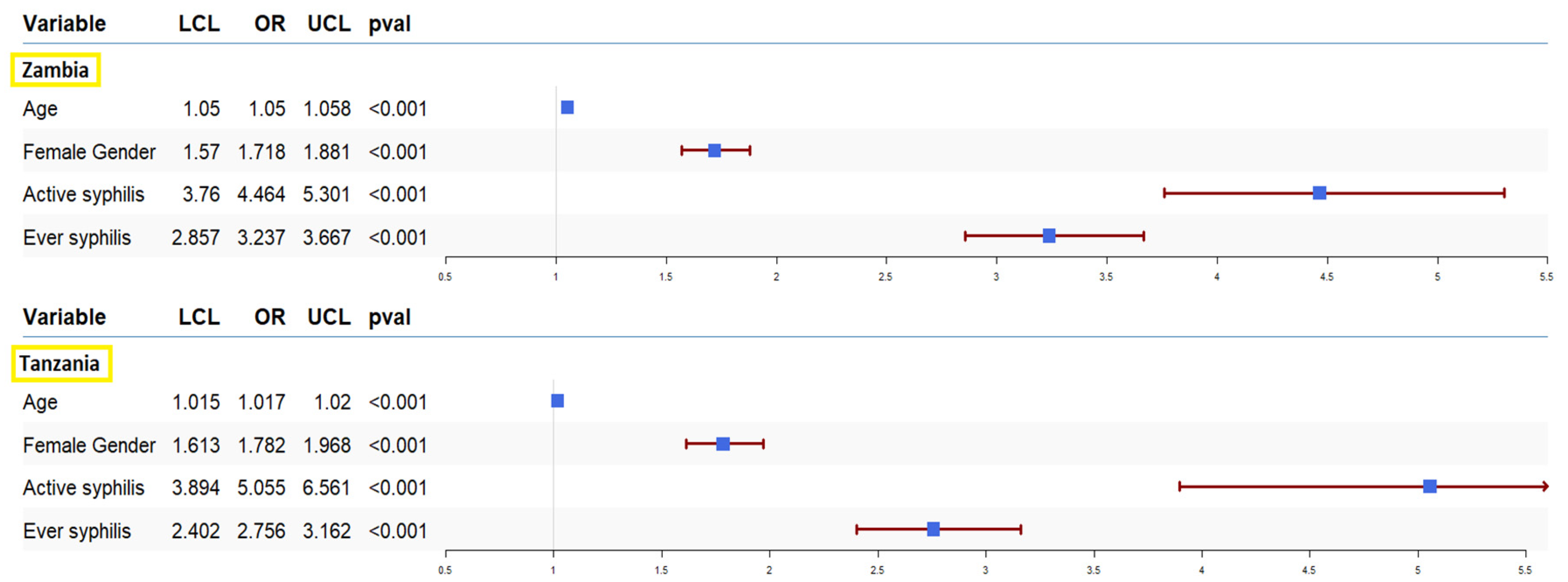
We ran univariate and multivariate logistic regression to assess the effect of syphilis on the odds of HIV acquisition and progression. The results of our analysis for HIV acquisition are presented in Figure 1. In our sample data from both countries, syphilis infection was associated with higher odds of HIV acquisition. The odds of HIV acquisition in participants with active syphilis infection in Zambia and Tanzania were [OR=4.46, 95% CI:3.76-5.30, p < 0.001] and [OR=5.05, 95% CI:3.89-6.56, p < 0.001], respectively. Moreover, the odds of HIV acquisition in participants with a history of syphilis in Zambia and Tanzania were [OR=3.23, 95% CI:2.85-3.66, p < 0.001] and Tanzania [OR=2.75, 95% CI:2.40-3.16, p < 0.001] respectively. We also ran multivariate logistic regression to estimate the impact of syphilis on HIV acquisition after adjusting for the effect of other covariates, including gender and age. These results also showed that both active syphilis: Zambia [OR=2.37, 95%CI: 1.86-3.02, p<0.001] and Tanzania [OR=2.58, 95% CI:1.91-3.48, p<0.001] and a history of syphilis infection: Zambia[OR=1.77, 95% CI: 1.48-2.12, p<0.001] and Tanzania[OR=1.94, 95% CI: 1.65-2.29, p<0.001] were associated with higher odds of HIV acquisition regardless of the other covariates. our data showed no significant association between co-infections and VL suppression.
Figure 1.
Forest plot of odds ratio (OR) together with their 95% confidence intervals for HIV acquisition in Zambia and Tanzania. The blue box represents the point estimate of the analysis, while horizontal lines represent the confidence interval (CI). The ends of the lines mark the boundaries of the CI, and the arrow mark indicates the extended CI beyond the x-axis limits.
Figure 1.
Forest plot of odds ratio (OR) together with their 95% confidence intervals for HIV acquisition in Zambia and Tanzania. The blue box represents the point estimate of the analysis, while horizontal lines represent the confidence interval (CI). The ends of the lines mark the boundaries of the CI, and the arrow mark indicates the extended CI beyond the x-axis limits.
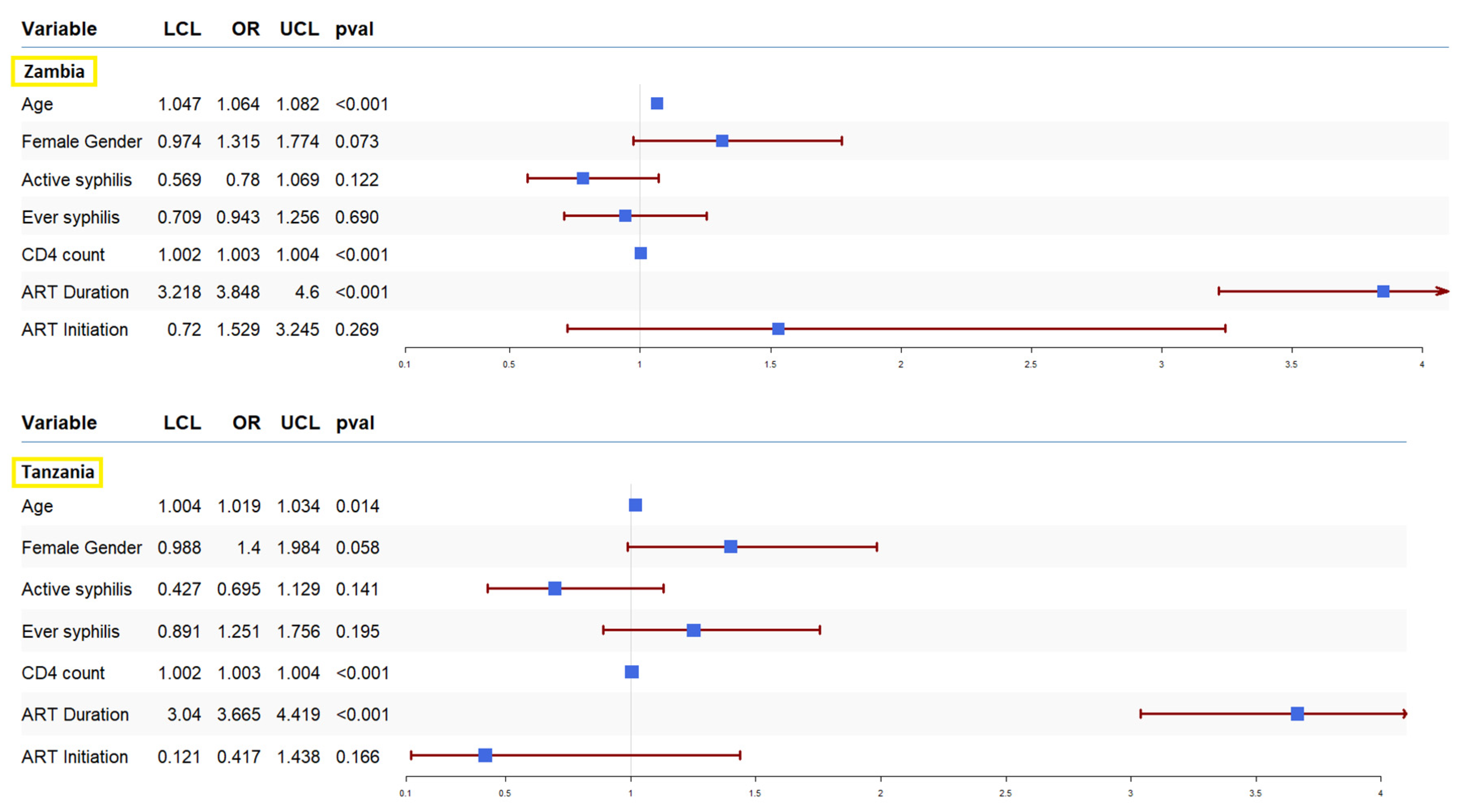
To understand the impact of syphilis on HIV progression, we ran a univariate and multivariate logistic regression, and the results are presented in Figure 2. In our sample data from both countries, syphilis infection was associated with a lack of VL suppression in ART-treated PLWH. In both countries, active syphilis was associated with a lack of VL suppression, though it did not reach statistical significance: Zambia [OR=0.78, 95% CI:0.56-1.06, p=0.1225] and Tanzania [OR=0.695, 95% CI:0.427-1.129, p=0.141]. Similarly, a history of syphilis was associated with a lack of viral suppression in Zambia [OR=0.94, 95% CI: 0.70-1.25, p=0.690] but a trend toward suppression in Tanzania [OR=1.25, 95% CI:0.89-1.75, p=0.195]. Figure 2 also displays the effect of the other covariates on VL suppression. In both countries, ART duration: Zambia [OR=3.84, 95% CI:3.21-4.60, p<0.001] and Tanzania [OR=3.66, 95% CI:3.04-4.41, p<0.001] and CD4 count: Zambia [OR=1.003, 95% CI:1.002-1.004, p<0.001] and Tanzania [OR=1.003, 95% CI:1.002-1.004, p<0.001] were associated with VL suppression. Similarly, older age in Zambia [OR=1.064, 95% CI:1.04-1.08, p<0.001] was also associated with VL suppression. Though not statistically significant, older age in Tanzania [OR=1.01, 95% CI: 1.00-1.03, p=0.014] and female gender in both Zambia [OR=1.31, 95% CI:0.97-1.77, p=0.073] and Tanzania [OR=1.4, 95% CI:0.98-1.98, p=0.058] were also associated with VL suppression. In both countries, ART initiation 12 months or more before the survey was not statistically significant, but it was associated with VL in Zambia [OR=1.52, 95% CI: 0.72-3.24, p=0.26] and showed a tendency towards lack of VL suppression in Tanzania [OR=0.41,95% CI:0.12-1.43, p=0.16].
Figure 2.
Forest plot of odds ratio (OR) together with their 95% confidence intervals for HIV progression among PLWH in Zambia and Tanzania. The blue box represents the point estimate of the analysis, while horizontal lines represent the confidence interval (CI). The ends of the lines mark the boundaries of the CI and arrow mark indicate the extended CI beyond the x-axis limits.
Figure 2.
Forest plot of odds ratio (OR) together with their 95% confidence intervals for HIV progression among PLWH in Zambia and Tanzania. The blue box represents the point estimate of the analysis, while horizontal lines represent the confidence interval (CI). The ends of the lines mark the boundaries of the CI and arrow mark indicate the extended CI beyond the x-axis limits.
4. Discussion
The major focus of our paper was twofold: to assess the impact of syphilis on HIV acquisition and HIV disease progression in sub-Saharan Africa. The presence of co-infections like syphilis can complicate the health of PLWH, as it makes managing HIV and maintaining immune system function more challenging [10,34,35]. Syphilis, being an STI, causes lesions in the genital area, which serve as an entry point for HIV, thereby increasing the likelihood of HIV transmission [12]. Despite the high prevalence of syphilis among PLWH in the region, the impact of syphilis on HIV transmission and HIV disease progression has not been well-studied in sub-Saharan Africa. Previous studies on the interplay between HIV and syphilis have often been constrained by either limited sample size [15,36] or were focused on very specific subgroups, such as MSM [12,37,38], female sex workers [39], and pregnant women [40]. As a result, the insights gained from these studies may not be widely generalizable to the broader HIV population. In this manuscript, we used retrospective data from 53,915 adult participants enrolled through population-based studies in Zambia and Tanzania. In our Zambia data, 11.6% of the participants were PLWH, 2.8% had active syphilis infection, and 6.4% had a history of syphilis. Similarly, in our Tanzania data, 5.9% of the study participants were PLWH, 1% had active syphilis infection, and 6.2% had a history of syphilis. These figures align with findings from previous studies in sub-Saharan Africa [13,32]. In both countries, the prevalence of HIV was markedly higher among individuals with either active syphilis or a history of syphilis infection, which is consistent with previous studies [13,32,41]. The proportion of syphilis (active or history of syphilis) among PLWH was 25.5% (n=631) and 18.3% (n=347) in Zambia and Tanzania, respectively. These rates exceeded those reported in earlier research, such as a study in Tanzania which reported prevalence of 9.6% and a study in Uganda reporting 10% [42,43]. In both countries, people with active syphilis are more than four times more likely to have HIV infection, which is consistent with prior findings in sub-Saharan Africa [32]. The history of syphilis was associated with more than a two-fold increase in HIV acquisition in both countries, which is consistent with a previous study in sub-Saharan Africa [42]. Moreover, our findings indicate that older adults and females were at an increased risk of acquiring HIV in both countries, consistent with previous research from the region [13,44].
The second objective of our manuscript was to evaluate the impact of syphilis on HIV disease progression in ART-treated PLWH. Since not all the PLWH had syphilis, we matched a syphilis-negative HIV-positive subject, by age and gender using propensity score methods, for each co-infected subject. We then compared the association of syphilis with HIV-disease progression among ART-treated PLWH. HIV disease progression was defined by the failure of HIV RNA VL suppression. Our analyses revealed that in both countries, active syphilis was associated with a lack of VL suppression, though it did not reach statistical significance: Zambia [OR=0.78, 95% CI:0.56-1.06, p=0.1225] and Tanzania [OR=0.695, 95% CI:0.427-1.129, p=0.141]. Similarly, a history of syphilis was associated with a lack of viral suppression in Zambia [OR=0.94, 95% CI: 0.70-1.25, p=0.690] but a trend toward suppression in Tanzania [OR=1.25, 95% CI:0.89-1.75, p=0.195]. Our findings align with a previous study from China, which reported virological failure due to co-infection with syphilis in PLWH [10]. Moreover, a study from Spain observed an increase in HIV RNA VL among HAART-treated PLWH due to syphilis infection [45]. Further, several studies from different parts of the world have reported that co-infection with syphilis increases HIV RNA VL in ART-treated PLWH, leading to HIV disease progression, which is consistent with our findings [43,45,46,47]. Co-infections with syphilis and other STIs can weaken the immune system and interfere with the ability of ART to suppress HIV-1 RNA VL, particularly among individuals who struggle with adherence to treatment or those who experience suboptimal responses to ART [10,34,35]. Thus, identifying and treating co-infections in PLWH is a crucial factor for achieving ART treatment success and controlling HIV disease progression.
The results of our analysis provide valuable insights that can help policymakers understand the effects of co-infections, like syphilis, on HIV acquisition and progression. The higher odds of HIV acquisition among syphilis co-infected patients emphasize the importance of integrating syphilis diagnosis and treatment services in HIV prevention programs. Furthermore, the association between syphilis and HIV disease progression suggests that syphilis co-infection interferes with ART treatment, thereby resulting in the failure of HIV RNA VL suppression. Compared with previous related studies, our study has many advantages. Unlike many previous studies, which were based either on a smaller sample size or specific groups such as female sex workers, MSM, or pregnant women, we utilized a large population-based study, reducing the potential biases associated with small sample sizes and sampling specific groups of participants. However, it is important to interpret these findings cautiously due to certain limitations. One significant limitation is the use of retrospective cross-sectional data, which may not account for changes over time in key variables such as healthcare access or high-risk behavioral factors. Additionally, our data cannot determine the sequence of infections (whether syphilis preceded HIV or vice versa) or whether participants received treatment for syphilis. Future studies should consider a prospective longitudinal cohort to better understand the relationship between syphilis and HIV acquisition and progression.
5. Conclusions
In this paper, we utilized retrospective cross-sectional data from Zambia and Tanzania and used regression models to identify the impact of syphilis on HIV acquisition and progression. Our analysis revealed that participants with syphilis infection (active or history) were more susceptible to HIV acquisition. Moreover, co-infection with syphilis was associated with HIV disease progression assessed by failure of HIV RNA viral load suppression. These findings emphasize the importance of integrating syphilis screening and treatment in HIV prevention programs. By offering syphilis testing alongside HIV testing, healthcare systems could enhance early detection and improve patient outcomes [44]. Moreover, early identification and treatment of syphilis not only improves patient outcomes but also reduces the burden and cost of managing these co-infections [44]. Integrating syphilis screening and treatment programs can strengthen public health responses to combat both HIV and syphilis.
Author Contributions
S.G. wrote the manuscript. R.N. analyzed data and wrote the manuscript. R. K. reviewed the manuscript. F.S. reviewed the manuscript. M.G. conceived the study, wrote the manuscript, and provided guidance on data analyses and interpretation of the findings. All authors read and approved the final manuscript.
Funding
The research was supported by grants from the Harvard University Center for AIDS Research (HU CFAR NIH/NAIDS P30-AI 060354) and the Ragon Institute of MGH, MIT, and Harvard.
Institutional Review Board Statement
All PHIA survey protocols, consent forms, screening forms, refusal forms, referral forms, recruitment materials, and questionnaires were reviewed and approved by in-country ethics and regulatory bodies and the institutional review boards of Columbia University Medical Center, Westat, and the U.S. Centers for Disease Control and Prevention. External monitoring was conducted twice per survey. Survey management teams conducted continuous surveillance for protocol deviations and adverse events, which were promptly reported to institutional review boards.
Informed Consent Statement
Not applicable.
Data Availability Statement
The dataset used in the manuscript is available from the Population-based HIV Impact Assessment (PHIA) Center: https://phia.icap.columbia.edu/ (accessed on 11th October 2024).
Acknowledgments
We want to thank the participants who gave their time to participate in ZAMPHIA 2016 and THIS (2016 -2017). We would also like to thank all the survey teams, laboratory personnel, and other key members involved in the surveys.
Conflicts of Interest
The authors do not have a commercial or other association that might pose a conflict of interest, i.e., the authors declare that they have no competing interests to disclose.
References
- Tudor ME, Al Aboud AM, Leslie SW, et al. Syphilis. [Updated 2024 Aug 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available online: https://www.ncbi.nlm.nih.gov/books/NBK534780/ (accessed on 5 October 2024).
- Centers for Disease Control and Prevention- Syphilis -fact sheet; Available online: https://www.cdc.gov/syphilis/about/index.html (accessed on 7 October 2024).
- World Health Organization (WHO) Syphilis- overview, Available online: https://www.who.int/health-topics/syphilis#tab=tab_1 (accessed on 8 October 2024).
- Mussa A, Jarolimova J, Ryan R, Wynn A, Ashour D, Bassett IV, Philpotts LL, Freyne B, Morroni C, Dugdale CM. Syphilis Prevalence Among People Living With and Without HIV in Sub-Saharan Africa: A Systematic Review and Meta-Analysis. Sex Transm Dis. 2024, 51, e1–e7. [CrossRef] [PubMed] [PubMed Central]
- Godfrey, J.A. Walker, Damian G. Walker,Congenital syphilis: A continuing but neglected problem,Seminars in Fetal and Neonatal Medicine,Volume 12, Issue 3,2007,Pages 198 206,ISSN 1744-165X. https://www.sciencedirect.com/science/article/pii/S1744165X07000200. [CrossRef]
- World Health Organization (WHO) Data on Syphilis, Available online: https://www.who.int/data/gho/data/themes/topics/data-on-syphilis (accessed on 8 October 2024).
- World Health Organization (WHO) Sexually transmitted infections (STIs): Strategic information. Available online: https://www.who.int/teams/global-hiv-hepatitis-and-stis-programmes/stis/strategic-information (accessed on 9 October 2024).
- World Health Organization. (2024). Implementing the global health sector strategies on HIV, viral hepatitis and sexually transmitted infections, 2022–2030: report on progress and gaps 2024, 2nd ed. World Health Organization. Available online: https://iris.who.int/handle/10665/378246 (accessed on 9 October 2024).
- World Health Organization, global health sector strategy on sexually transmitted infections 2016–2021 towards ending STIs. Available online: https://iris.who.int/bitstream/handle/10665/246296/WHO-RHR-16.09-eng.pdf?sequence=1 (accessed on 10 October 2024).
- Fan L, Yu A, Zhang D, Wang Z, Ma P. Consequences of HIV/Syphilis Co-Infection on HIV Viral Load and Immune Response to Antiretroviral Therapy. Infect Drug Resist. 2021, 14, 2851–2862. [CrossRef] [PubMed] [PubMed Central]
- Wu Y, Zhu W, Sun C, Yue X, Zheng M, Fu G and Gong X. Prevalence of syphilis among people living with HIV and its implication for enhanced coinfection monitoring and management in China: A meta-analysis. Front. Public Health 2022, 10, 1002342. [CrossRef]
- Wu MY, Gong HZ, Hu KR, Zheng HY, Wan X, Li J. Effect of syphilis infection on HIV acquisition: a systematic review and meta-analysis. Sex Transm Infect. 2021, 97, 525–533. [CrossRef] [PubMed] [PubMed Central]
- Gilbert L, Dear N, Esber A, Iroezindu M, Bahemana E, Kibuuka H, Owuoth J, Maswai J, Crowell TA, Polyak CS, Ake JA; AFRICOS Study Group. Prevalence and risk factors associated with HIV and syphilis co-infection in the African Cohort Study: a cross-sectional study. BMC Infect Dis. 2021, 21, 1123. [CrossRef] [PubMed] [PubMed Central]
- Solomon H, Moraes AN, Williams DB, Fotso AS, Duong YT, Ndongmo CB, et al. Prevalence and correlates of active syphilis and HIV co-Infection among sexually active persons aged 15–59 years in Zambia: Results from the Zambia Population-based HIV Impact Assessment (ZAMPHIA) 2016. PLoS ONE 2020, 15, e0236501. [CrossRef]
- Wu Y, Lu L, Song X, Liu X, Yang Y, Chen L, Tang J, Han Y, Lv W, Cao W, Li T. Clinical and immunological characteristics of HIV/syphilis co-infected patients following long-term antiretroviral treatment. Front Public Health. 2024, 11, 1327896. [CrossRef] [PubMed] [PubMed Central]
- Ren M, Dashwood T, Walmsley S. The Intersection of HIV and Syphilis: Update on the Key Considerations in Testing and Management. Curr HIV/AIDS Rep. 2021, 18, 280–288. [CrossRef] [PubMed] [PubMed Central]
- Wang CL, Gao S, Li XZ, Martcheva M. Modeling Syphilis and HIV Coinfection: A Case Study in the USA. Bull Math Biol. 2023, 85, 20. [CrossRef] [PubMed] [PubMed Central]
- Luetkemeyer AF, Donnell D, Dombrowski JC, Cohen S, Grabow C, Brown CE, Malinski C, Perkins R, Nasser M, Lopez C, Vittinghoff E, Buchbinder SP, Scott H, Charlebois ED, Havlir DV, Soge OO, Celum C; DoxyPEP Study Team. Postexposure Doxycycline to Prevent Bacterial Sexually Transmitted Infections. N Engl J Med. 2023, 388, 1296–1306. [CrossRef] [PubMed] [PubMed Central]
- Molina JM, Charreau I, Chidiac C, et al. Post-exposure prophylaxis with doxycycline to prevent sexually transmitted infections in men who have sex with men: an open-label randomised substudy of the ANRS IPERGAY trial. Lancet Infect Dis 2018, 18, 308–317.
- La Ruche G, Goubard A, Bercot B, Cambau E, Semaille C, Sednaoui P. Gonococcal infections and emergence of gonococcal decreased susceptibility to cephalosporins in France, 2001 to 2012. Euro Surveill 2014, 19, 20885–20885.
- Bolan RK, Beymer MR, Weiss RE, Flynn RP, Leibowitz AA, Klausner JD. Doxycycline prophylaxis to reduce incident syphilis among HIV-infected men who have sex with men who continue to engage in high-risk sex: a randomized, controlled pilot study. Sex Transm Dis 2015, 42, 98–103.
- He L, Pan X, Yang J, Zheng J, Luo M, Cheng W, Chai C. Current syphilis infection in virally suppressed people living with HIV: a cross-sectional study in eastern China. Front Public Health. 2024, 12, 1366795. [CrossRef] [PubMed] [PubMed Central]
- Billock RM, Samoff E, Lund JL, Pence BW, Powers KA. HIV Viral Suppression and Pre-exposure Prophylaxis in HIV and Syphilis Contact Tracing Networks: An Analysis of Disease Surveillance and Prescription Claims Data. J Acquir Immune Defic Syndr. 2021, 88, 157–164. [CrossRef] [PubMed] [PubMed Central]
- Nicola, M. Zetola, Jeffrey D. Klausner, Syphilis and HIV Infection: An Update, Clinical Infectious Diseases, Volume 44, Issue 9, 1 May 2007, Pages 1222–1228. 1 May. [CrossRef]
- Buchacz K, Patel P, Taylor M, Kerndt PR, Byers RH, Holmberg SD, Klausner JD. Syphilis increases HIV viral load and decreases CD4 cell counts in HIV-infected patients with new syphilis infections. AIDS. 2004, 18, 2075–9. [CrossRef] [PubMed] [PubMed Central]
- Ghanem KG, Moore RD, Rompalo AM, Erbelding EJ, Zenilman JM, Gebo KA. Antiretroviral therapy is associated with reduced serologic failure rates for syphilis among HIV-infected patients. Clin Infect Dis. 2008, 47, 258–65. [CrossRef] [PubMed] [PubMed Central]
- Ghanem, Khalil G; Moore, Richard D; Rompalo, Anne M; Erbelding, Emily J; Zenilman, Jonathan M; Gebo, Kelly A. Neurosyphilis in a clinical cohort of HIV-1-infected patients. AIDS 22, p 1145-1151, June 19, 2008. |. [CrossRef]
- Population-based HIV Impact Assessment (PHIA) project. Available online: https://phia.icap.columbia.edu/ (accessed on 11 October 2024).
- Tanzania Commission for AIDS (TACAIDS), Zanzibar AIDS Commission (ZAC). Tanzania HIV Impact Survey (THIS) 2016-2017: Final Report. Dar es Salaam, Tanzania. December 2018, Available online:. Available online: https://phia.icap.columbia.edu/tanzania-final-report/ (accessed on 15 October 2024).
- Ministry of Health, Zambia. Zambia Population-based HIV Impact Assessment (ZAMPHIA) 2016: Final Report. Lusaka, Ministry of Health. February 2019, Available online:. Available online: https://phia.icap.columbia.edu/zambia-final-report/ (accessed on 15 October 2024).
- PHIA Data Use Manual, Available online: https://phia-data.icap.columbia.edu/storage/Country/28-09-2021-22-01-17-615390ad6a147.pdf (accessed on 16 October 2024).
- Farahani M, Killian R, Reid GA, Musuka G, Mugurungi O, Kirungi W, Nuwagaba-Biribonwoha H, El-Sadr WM, Justman J. Prevalence of syphilis among adults and adolescents in five sub-Saharan African countries: findings from Population-based HIV Impact Assessment surveys. Lancet Glob Health. 2024, 12, e1413–e1423. [CrossRef] [PubMed]
- Sachathep K, Radin E, Hladik W, Hakim A, Saito S, Burnett J, Brown K, Phillip N, Jonnalagadda S, Low A, Williams D, Patel H, Herman-Roloff A, Musuka G, Barr B, Wadondo-Kabonda N, Chipungu G, Duong Y, Delgado S, Kamocha S, Kinchen S, Kalton G, Schwartz L, Bello G, Mugurungi O, Mulenga L, Parekh B, Porter L, Hoos D, Voetsch AC, Justman J. Population-Based HIV Impact Assessments Survey Methods, Response, and Quality in Zimbabwe, Malawi, and Zambia. J Acquir Immune Defic Syndr. 2021, 87(Suppl 1), S6-S16. [CrossRef] [PubMed] [PubMed Central]
- Getaneh Y, Getnet F, Amogne MD, Liao L, Yi F, Shao Y. Burden of hepatitis B virus and syphilis co-infections and its impact on HIV treatment outcome in Ethiopia: nationwide community-based study. Ann Med. 2023, 55, 2239828. [CrossRef] [PubMed] [PubMed Central]
- Shimelis T, Tassachew Y, Tadewos A, Hordofa MW, Amsalu A, Tadesse BT, Tadesse E. Coinfections with hepatitis B and C virus and syphilis among HIV-infected clients in Southern Ethiopia: a cross-sectional study. HIV AIDS (Auckl). 2017, 9, 203–210. [CrossRef] [PubMed] [PubMed Central]
- Yuindartanto, A. , Hidayati, A. N., Indramaya, D. M., Listiawan, M. Y., Ervianti, E., & Damayanti, D. Risk Factors of Syphilis and HIV/AIDS Coinfection. Berkala Ilmu Kesehatan Kulit Dan Kelamin 2022, 34, 114–119. [Google Scholar] [CrossRef]
- Mahmud S, Mohsin M, Muyeed A, Islam MM, Hossain S, Islam A. Prevalence of HIV and syphilis and their co-infection among men having sex with men in Asia: A systematic review and meta-analysis. Heliyon. 2023, 9, e13947. [CrossRef] [PubMed] [PubMed Central]
- Parmley LE, Chingombe I, Wu Y, Mapingure M, Mugurungi O, Samba C, Rogers JH, Hakim AJ, Gozhora P, Miller SS, Musuka G, Harris TG. High Burden of Active Syphilis and Human Immunodeficiency Virus/Syphilis Coinfection Among Men Who Have Sex With Men, Transwomen, and Genderqueer Individuals in Zimbabwe. Sex Transm Dis. 2022, 49, 111–116. [CrossRef] [PubMed] [PubMed Central]
- Musema, G. M. A. , Mapatano, A. M., Tshala, D. K. and Kayembe, P. K. HIV-1-syphilis co-infection associated with high viral load in female sex workers in the Democratic Republic of the Congo. International Journal of Translational Medical Research and Public Health 2020, 4, 93–102. [Google Scholar] [CrossRef]
- Anteneh, D. E. , Taye, E. B., Seyoum, A. T., Abuhay, A. E., & Cherkose, E. A. Seroprevalence of HIV, HBV, and syphilis co-infections and associated factors among pregnant women attending antenatal care in Amhara regional state, northern Ethiopia: A hospital-based cross-sectional study. Plos one 2024, 19, e0308634. [Google Scholar]
- Katamba C, Chungu T, Lusale C. HIV, syphilis and hepatitis B coinfections in Mkushi, Zambia: a cross-sectional study. F1000Res. 2019, 8, 562. [CrossRef] [PubMed] [PubMed Central]
- Haule A, Msemwa B, Mgaya E, Masikini P, Kalluvya S. Prevalence of syphilis, neurosyphilis and associated factors in a cross-sectional analysis of HIV infected patients attending Bugando Medical Centre, Mwanza, Tanzania. BMC Public Health. 2020, 20, 1862. [CrossRef] [PubMed] [PubMed Central]
- Mboowa G, Inda DA. Seroprevalence of syphilis among human immunodeficiency virus positive individuals attending immune suppressed syndrome clinic at international hospital Kampala, Uganda. Int STD Res Rev. 2015, 3, 84–90.
- Ruangtragool L, Silver R, Machiha A, Gwanzura L, Hakim A, Lupoli K, Musuka G, Patel H, Mugurungi O, Tippett Barr BA, Rogers JH. Factors associated with active syphilis among men and women aged 15 years and older in the Zimbabwe Population-based HIV Impact Assessment (2015-2016). PLoS One 2022, 17, e0261057. [CrossRef] [PubMed] [PubMed Central]
- Palacios R, Jiménez-Oñate F, Aguilar M, Galindo MJ, Rivas P, Ocampo A, Berenguer J, Arranz JA, Ríos MJ, Knobel H, Moreno F, Ena J, Santos J. Impact of syphilis infection on HIV viral load and CD4 cell counts in HIV-infected patients. J Acquir Immune Defic Syndr. 2007, 44, 356–9. [CrossRef] [PubMed]
- Buchacz K, Patel P, Taylor M, Kerndt PR, Byers RH, Holmberg SD, Klausner JD. Syphilis increases HIV viral load and decreases CD4 cell counts in HIV-infected patients with new syphilis infections. AIDS. 2004, 18, 2075–9. [CrossRef] [PubMed] [PubMed Central]
- Kofoed K, Gerstoft J, Mathiesen LR, et al. Syphilis and human immunodeficiency virus (HIV)-1 coinfection: influence on CD4 T-cell count, HIV viral load, and treatment response. Sex Transm Dis. 2006, 33, 143–148.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



