
Submitted:
29 May 2025
Posted:
30 May 2025
You are already at the latest version
Abstract
Sexually transmitted infections (STIs) are common infections globally, posing significant public health challenges and financial strain, especially in low- and middle-income countries. Sub-Saharan Africa (SSA) accounts for 40% of global STI prevalence, with South Africa having the highest rates of curable STIs and human immunodeficiency virus (HIV), both of which are closely linked to increasing HIV transmission risk and other STIs. Genital ulcer disease (GUD), primarily caused by HSV-1, HSV-2, and Treponema pallidum, and less frequently by Haemophilus ducreyi, Klebsiella granulomatis, and Chlamydia trachomatis, exemplifies the complex interplay of STIs. This study analysed GUD and coinfection with HIV, testing patterns, and co-occurrence trends among public clinic attendees in Mthatha, South Africa, to identify demographic, behavioural, and occupational disparities. Gender-specific analysis revealed higher HIV prevalence among females (47.00 %) compared to males (22.00%), alongside notable testing gaps and disparities in diseases such as syphilis, genital herpes, and lymphogranuloma venereum (LGV). Age-specific trends indicated the highest HIV prevalence in individuals aged 30–49, with peaks at 66.67% (30–39) and 76.47% (40–49). Treponema pallidum and HSV-2 prevalence were most pronounced in younger age groups (<20 and 20–29), while older demographics (50+) exhibited significant diagnostic gaps. Occupation-based analysis highlighted elevated HIV (65.91%) and HSV-2 (19.61%) prevalence among unemployed individuals, reflecting socioeconomic vulnerabilities. Co-occurrence analysis revealed notable overlaps, such as HIV and HSV-2 (6.67%) and Chlamydia trachomatis with HSV-1 (5.71%) and HSV-2 (4.76%), driven by shared risk factors. Correlation analysis identified strong links between HSV-1 and Haemophilus ducreyi (0.64) and between Chlamydia trachomatis and HSV-1 (0.56), underscoring the potential for integrated diagnostic strategies. These findings emphasize the need for targeted public health interventions addressing gender, age, and occupational disparities while improving diagnostic coverage and prevention efforts for co-occurring infections.
Keywords:
disease prevalence
; testing coverage
; gender disparities
; age-specific trends
; co-occurrence analysis
; GUD
; public health interventions
1. Introduction
Sexually transmitted infections (STIs), among the most common acute infectious conditions globally, pose a significant public health challenge, straining household and national health budgets while adversely affecting individuals' quality of life despite rarely being life-threatening [1]. Low- and middle-income countries continue to bear a disproportionate burden, with sub-Saharan Africa (SSA) contributing to 40% of the global prevalence of STIs. Within SSA, South Africa has the highest rates of curable STIs and human immunodeficiency virus (HIV), with the two epidemics closely linked, as STIs significantly heighten the risk of HIV transmission and acquisition [2]. Dhar et al (2024) define genital ulcer disease (GUD) as ulcerations resulting from STIs, primarily due to genital herpes caused by herpes simplex virus types 1 and 2 (HSV-1 and -2) and syphilis caused by Treponema pallidum [3]. Less frequently, it is associated with chancroid caused by Haemophilus ducreyi, granuloma inguinale (donovanosis), caused by Klebsiella granulomatis, and lymphogranuloma venereum (LGV) caused by Chlamydia trachomatis [3].
Understanding disease prevalence and testing patterns is essential for developing targeted public health interventions. This study analyses gender, age, occupation, and co-occurrence trends among clinic attendees, highlighting critical disparities in disease distribution and diagnostic coverage. Gender-specific analysis reveals a higher prevalence of HIV and syphilis among females compared to males, while testing gaps for multiple diseases are more pronounced in females [4]. A study conducted in Zambia also recorded a HIV prevalence among young women aged 15–24, which is significantly higher (5.6%) compared to their male counterparts (1.8%) [5]. Conversely, with syphilis statistics, another study reported that 97.9% of syphilis-positive individuals were male, with 66.3% identifying as men who have sex with men (MSM) [6]. Age-based trends show that HIV and syphilis prevalence peak in middle-aged groups, with younger populations exhibiting elevated rates of HSV2 and Chlamydia trachomatis [4]. Gilbert et al. (2021) found that the median age of individuals with HIV and syphilis co-infection was 38 years, suggesting higher prevalence in middle-aged groups [7]. Older adults face significant testing gaps across multiple conditions, emphasizing the need for improved diagnostic efforts in this demographic.
Occupation-based analysis identifies unemployed individuals as particularly vulnerable, with higher prevalence rates for HIV, syphilis, HSV-1, and HSV-2 compared to employed or student groups, indicating socioeconomic disparities in disease burden [8,9]. Studies have demonstrated that unemployed individuals exhibit higher prevalence rates of STIs, including HIV, syphilis, HSV-1, and HSV-2, compared to their employed or student counterparts. This disparity underscores the influence of socioeconomic status on disease burden[10]. Significant overlaps, such as between HIV and HSV-2 and between Chlamydia trachomatis and HSV-1/HSV-2, suggest shared risk factors and transmission pathways [11]. The co-infection of HIV and HSV-2 is well-documented, with HSV-2 infection increasing susceptibility to HIV acquisition. Additionally, co-infections involving Chlamydia trachomatis and HSV-1/HSV-2 are prevalent, suggesting shared risk factors and transmission routes [12]. Conversely, diseases like syphilis and granuloma inguinale show minimal overlap, reflecting distinct epidemiological profiles [13]. Research indicates minimal overlap between infections like syphilis and HSV-2, reflecting distinct epidemiological profiles and transmission dynamics [10].
This study's additional analysis extends the original study’s findings of [4] by addressing gaps in knowledge regarding GUD in the Eastern Cape Province of South Africa, particularly in the King Sabata Dalindyebo local municipality. By providing a deeper understanding of epidemiological patterns, the new analysis focuses on gender, age, and occupational disparities in GUD prevalence and co-occurring HIV infection. Furthermore, it emphasizes the relationship between GUD and other STIs such as HIV, genital herpes, and syphilis, offering a detailed examination of co-occurrence trends among public clinic attendees. This provides insights into overlapping infection risks and potential transmission pathways, which were not explored in-depth in the original study. Additionally, the extended analysis highlights critical socioeconomic and demographic insights, identifying specific groups, such as unemployed individuals, who exhibit a higher burden of disease, underscoring the need for targeted public health interventions. By examining disease testing coverage and identifying diagnostic gaps, this analysis supports improved public health strategies aimed at enhancing STI diagnostic efforts, particularly for vulnerable groups like older adults and women. The incorporation of statistical and correlation analysis between different pathogens, such as HSV-1 and Haemophilus ducreyi, further emphasizes the importance of integrated diagnostic strategies, providing a more comprehensive understanding of disease co-occurrence patterns. This level of analysis supports more effective resource allocation for GUD and HIV prevention and treatment in the region.
This comprehensive approach aims to inform future efforts to reduce the burden of GUD and its associated infections, ultimately improving health outcomes in the region.
2. Materials and Methods
A retrospective cross-sectional analysis was conducted using data from Tshaka et al., (2022) study, in which data was generated between May 2018 and July 2019 from public clinic attendees in Mthatha, South Africa. All available data were used, which included demographic variables (gender, age, residence, occupation, and education), behavioural factors (substance abuse, number of sexual partners), and laboratory results for the following diseases: HIV, syphilis, genital herpes, lymphogranuloma venereum, chancroid, and granuloma inguinale. Participants were included in the study if they presented with visible, unhealed genital ulcers during routine visits to public CHCs in Mthatha, Eastern Cape, South Africa, and self-reported signs and symptoms of GUD. Eligible participants were required to provide written informed consent to participate in the study. They also underwent a private interview to collect socio-demographic and clinical information, followed by a clinical examination and sample collection. Furthermore, blood and genital ulcer swab samples were collected from each participant and tested for the presence of HIV, HSV-1, HSV-2, Chlamydia trachomatis, Treponema pallidum, Haemophilus ducreyi, and Klebsiella granulomatis to ensure comprehensive analysis and accurate diagnosis of GUD and associated infections. Participants were excluded from the study if they did not present with visible or unhealed genital ulcers, as the study specifically targeted individuals with clinical symptoms of GUD. Additionally, individuals who refused to provide written informed consent were not included, as consent was a prerequisite for participation. Those whose blood or swab samples were insufficient or unsuitable for laboratory testing were also excluded to ensure the integrity of the diagnostic results. Furthermore, participants with incomplete socio-demographic or clinical information were excluded, as comprehensive data was essential for the study’s analysis and conclusions.
2.1. Data Collection
Data for the study were obtained from a study by Tshaka et al (2022). The clinic records collected from May 2018 to July 2019, with inclusion criteria requiring complete demographic and clinical records. Disease test results were categorized into three groups: positive, negative, and missing data. The study recruited 105 participants due to the inclusion of additional participants who met the selection criteria for epidemiology of GUD but were not part of the original study of aetiology of GUD, resulting in a broader and more comprehensive dataset for analysis.
2.2. Data Processing
Categorical variables, such as gender and substance abuse, were coded for analysis, while "not done" test results were analyzed separately to identify testing gaps. Age was grouped into categories (<20, 20–29, 30–39, 40–49, 50–59, and 60+) for a more detailed examination of demographic trends.
2.3. Statistical Analysis
The results included descriptive statistics calculating prevalence rates for each disease across demographic and behavioral factors. Python (version 3.8) and R (version 4.1.1) software were used for data analysis. Correlation analysis, using Pearson correlation coefficients, examined relationships between diseases, age, and substance abuse. Additionally, co-occurrence analysis computed rates of simultaneous positivity for multiple diseases, providing insights into patterns of disease overlap.
3. Results
3.1. Gender-Based Prevalence
The analysis of gender-specific disease distribution among clinic attendees revealed distinct patterns. Females exhibited a higher prevalence of HIV (47.00%) compared to males (22.00%), with males showing relatively higher negative test rates, underscoring gender-specific differences in exposure and testing outcomes. For syphilis (Rapid Plasma Reagin (RPR) results), both genders predominantly tested negative, females at 5.0% and males at 3.0%. Negative results were also common for HSV-1 and HSV-2 (Herpes Simplex Viruses 1 & 2), though females had marginally higher testing rates. Similarly, Chlamydia trachomatis testing showed a predominance of negative results with minimal positive cases, yet females were tested more frequently, albeit with persistent disparities in coverage. For Treponema pallidum, Haemophilus ducreyi, and Klebsiella granulomatis, the results were largely negative or with missing data, with females showing slightly higher rates of "missing data" entries, highlighting gaps in comprehensive testing across both genders. These findings emphasize the need for targeted interventions to address gender-specific disparities in disease prevalence and diagnostic coverage. The prevalence of positive results for HIV and syphilis was notably higher among females, highlighting a potential gender disparity in exposure or susceptibility to these conditions.
3.2. Age Trends
The analysis revealed age-specific trends in disease prevalence and testing coverage. HIV prevalence was highest in the 30–49 age group, with rates peaking at 66.67% in those aged 30–39 and 76.47% in the 40–49 age group. Syphilis prevalence was most pronounced in the 30–39 age group (12.12%), while younger individuals (<20 and 20–29) demonstrated elevated rates of HSV-2 and Chlamydia trachomatis.
Figure 1 indicates that HIV is the most prominent infection across almost all age groups, reflecting a widespread burden of the disease. The percentage of HIV-positive cases appears to increase with age, suggesting prolonged exposure or cumulative risk factors, such as multiple sexual partners and a lack of early intervention. In contrast, younger individuals, particularly those in their 20s and 30s, exhibit a higher proportion of HSV-2 and Chlamydia trachomatis, both of which are common STIs. This suggests that younger populations may engage in riskier sexual behaviours, such as unprotected sex and multiple partners, increasing their vulnerability to these infections. Syphilis, as indicated by RPR results, shows a relatively low burden across all age groups, suggesting either effective screening and treatment efforts or underdiagnosis in some cases. Furthermore, Haemophilus ducreyi appears in minimal proportions, while Klebsiella granulomatis, was not detected in any of the age groups. This suggests that these pathogens are not major contributors to GUD within this population, consistent with the declining prevalence of chancroid and donovanosis reported in other studies. These results highlight age-related variations in STI distribution, with younger populations more affected by HSV-2 and Chlamydia trachomatis, while HIV remains a significant concern across all age groups.
3.3. Infection Trends by Age
The analysis of disease testing across age groups revealed consistent patterns. Negative RPR results dominated all age groups, with few positive cases; however, "missing data" results were more common among older individuals, highlighting gaps in testing. Similarly, negative results for HSV-1 and HSV-2 were predominant, particularly in younger cohorts, while older age groups had more incomplete testing. Chlamydia trachomatis testing showed consistent negative results across age groups, with minimal positive cases, yet testing gaps mirrored those of HSV, particularly in older populations. Older age groups exhibited higher rates of unperformed tests, indicating inconsistencies in diagnostic efforts for GUD. Key trends emerged, with the 20–39 age group showing a higher prevalence of positive HIV results, marking it as a priority for targeted interventions. Conversely, older age groups (50+) demonstrated significant testing gaps for multiple diseases, underscoring the need for improved diagnostic coverage in this demographic. Our study also enrolled a few participants in this group.
The analysis of disease prevalence across age groups highlighted distinct patterns. HIV prevalence peaked in the 40–49 age group (76.47%), followed by the 30–39 age group (66.67%), with a noted prevalence in the 20–29 age group (37.50%). Syphilis prevalence, measured through RPR results, was highest in the 30–39 age group (12.12%), with no positive cases reported in individuals <20, 50–59, or 60+. For HSV-1 and HSV-2, HSV-1 prevalence peaked in the 40–49 age group (17.65%), with notable rates in those <20 (10.00%) and 30–39 (6.06%). HSV-2 showed steady prevalence across younger and middle age groups, peaking in the 20–29 cohort (15.63%). Chlamydia trachomatis exhibited higher prevalence in the 40–49 (11.76%) and 20–29 (9.38%) age groups. Treponema pallidum and Haemophilus ducreyi were generally rare but appeared more frequently in younger and middle-aged adults. Klebsiella granulomatis showed no detected cases across any age group. These findings underscore age-specific disease trends, with younger and middle-aged groups being more affected, and the need for targeted health interventions across these demographics.
3.4. Occupation-Based Prevalence
The analysis of GUD patterns by occupation revealed notable trends. HIV prevalence was highest among employed individuals (65.91%), potentially linked to mobility or workplace exposure, followed by unemployed individuals (50.98%), reflecting socioeconomic vulnerabilities. Students had a lower prevalence (17.24%), likely due to younger age demographics. Chlamydia trachomatis showed a significantly higher prevalence among unemployed individuals (17.65%), highlighting a critical need for targeted interventions in this group. For syphilis, unemployed individuals had the highest prevalence (7.84%), while employed and student groups exhibited moderate rates (~4.50–6.90%). HSV-1 and HSV-2 were more prevalent among unemployed individuals (HSV-1: 11.76%, HSV-2: 19.61%), marking this group as particularly at risk, whereas students and employed individuals showed lower rates. Treponema pallidum was more frequent among students (17.24%), and Haemophilus ducreyi demonstrated a unique 100% prevalence in the self-employed group, though this may be skewed by a limited sample size. These findings emphasize the occupational disparities in disease prevalence, with unemployed individuals consistently showing higher rates for multiple conditions, signaling a need for focused public health interventions tailored to at-risk occupational groups.
The analysis of co-occurrence and correlation rates among diseases in Figure 2 revealed significant patterns. High co-occurrence was observed for HIV and HSV-2 (6.67%), highlighting shared risk factors or overlapping populations, while Chlamydia trachomatis showed notable overlap with HSV-1 (5.71%) and HSV-2 (4.76%), likely due to common transmission routes. Similarly, Haemophilus ducreyi co-occurred with HSV-1 and Chlamydia trachomatis (5.71%), indicating potential co-infection patterns. Low or zero co-occurrence rates were notable for RPR results, which rarely overlapped with other diseases, and Klebsiella granulomatis, which showed no co-occurrence across all conditions in the dataset. Correlation analysis revealed strong links between HSV-1 and Haemophilus ducreyi (0.64) and between Chlamydia trachomatis and HSV-1 (0.56), suggesting shared risk factors. Conversely, weak or negative correlations were found for RPR results and HSV2 (-0.13), HIV status, and Treponema pallidum (-0.19), indicating limited overlap between these conditions. Minimal relationships were observed for diseases like HIV and syphilis (RPR results), reflecting low co-dependence. These findings underscore the need for integrated diagnostics for diseases with high co-occurrence, such as HIV and genital herpes, and targeted prevention strategies addressing common pathways for infections Chlamydia trachomatis and HSV-1/HSV-2. Additionally, the lack of overlap in some diseases highlights the importance of investigating testing gaps and population-specific risks to refine public health interventions.
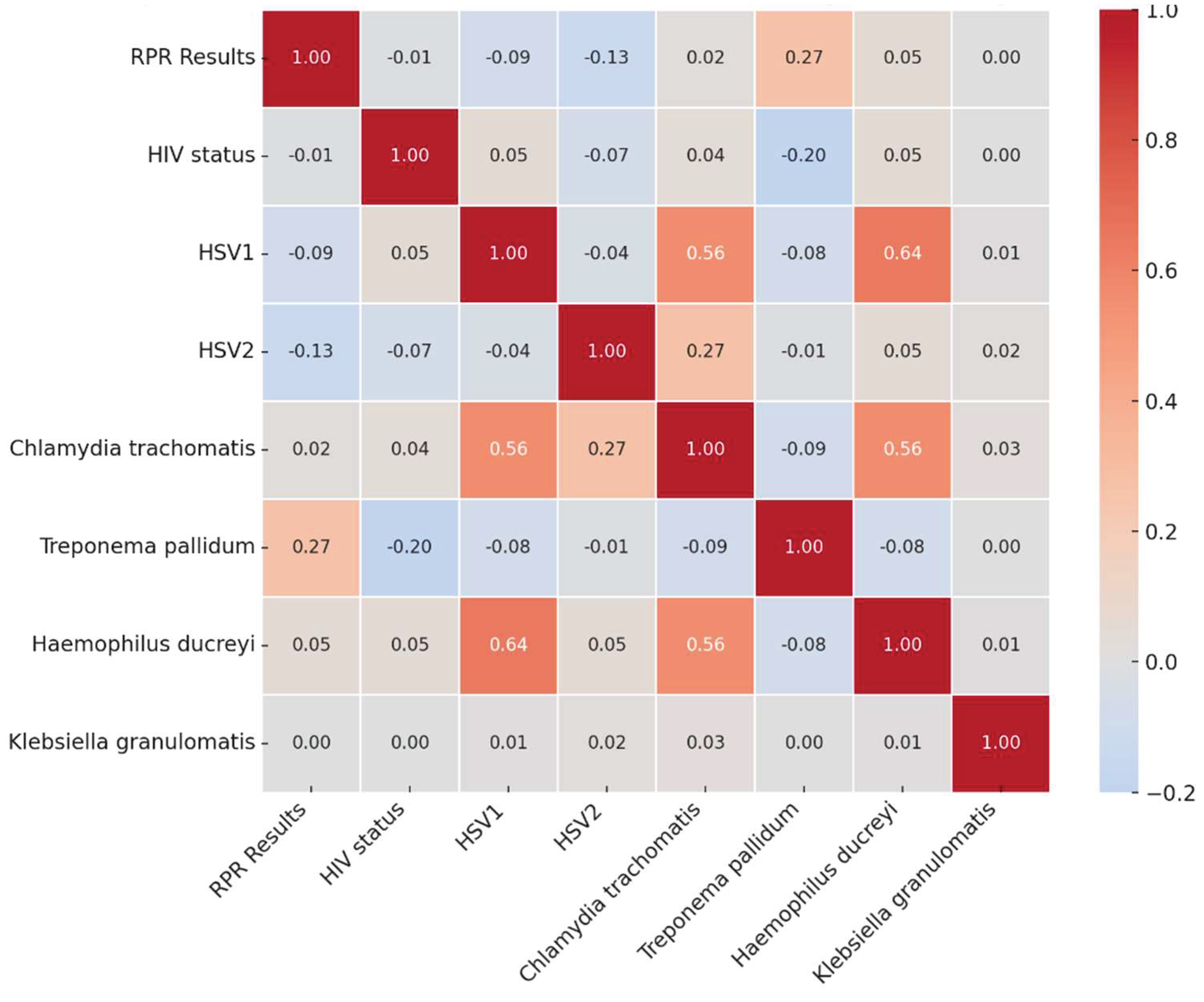
The correlation analysis of STIs in Figure 2 revealed key patterns of disease co-occurrence and independence. Strong positive correlations were observed between HSV-1 and Haemophilus ducreyi (0.64), Chlamydia trachomatis and HSV-1 (0.56), and Chlamydia trachomatis and Haemophilus ducreyi (0.56), suggesting shared transmission routes and behavioral risk factors such as unprotected sexual contact. Additionally, HSV-2 and Chlamydia trachomatis (0.27) showed a moderate correlation, indicating potential overlap due to common transmission pathways. Conversely, weak or negative correlations were noted between HIV status and Treponema pallidum (-0.20) and RPR results and HSV2 (-0.13), indicating that these infections do not frequently co-occur, possibly due to differing risk factors, testing interventions, or distinct transmission dynamics. Minimal relationships were found between HIV status and other STIs, as well as Treponema pallidum and other diseases, suggesting these infections often occur independently. Klebsiella granulomatis exhibited nearly zero correlation with all other infections, reinforcing its rarity in this study population and the distinct epidemiology of donovanosis. These findings underscore the importance of integrated diagnostic strategies for strongly correlated infections while emphasizing the need for targeted screening and prevention efforts for infections with independent transmission patterns.
4. Discussion
The observed gender disparities in HIV prevalence and testing outcomes highlight significant public health concerns. Females exhibited a notably higher prevalence of HIV (47.00%) compared to males (22.00%), which aligns with findings that indicate women often face unique vulnerabilities that increase their risk of HIV infection. Factors contributing to this heightened risk include social determinants such as intimate partner violence, economic instability, and limited access to healthcare services, which disproportionately affect women [14,15]. Furthermore, the stigma surrounding HIV can deter individuals from seeking testing, with studies indicating that women may have more access to testing through antenatal care services, thereby influencing the observed prevalence rates [15].
Regarding testing outcomes, males demonstrated relatively higher negative test rates, suggesting that they may be less likely to engage in testing behaviors than females. This aligns with research indicating that men, particularly in certain cultural contexts, may avoid testing due to stigma or perceived masculinity norms that discourage vulnerability [16,17]. The slight difference in syphilis positivity rates, with females at 5.00% compared to males at 3.00%, further underscores the need for gender-specific approaches to sexual health education and testing initiatives [18].
The gender-specific differences in HIV prevalence and testing outcomes necessitate tailored public health strategies that address the unique challenges faced by different populations. Efforts should focus on increasing awareness, reducing stigma, and improving access to testing services, particularly for women and marginalized groups, to enhance overall health outcomes and reduce the incidence of HIV.
The prevalence of negative test results for STIs such as HIV, herpes simplex virus (HSV-1 and HSV-2), and Chlamydia trachomatis, alongside the higher testing rates among females, underscores the complexities of STI screening and public health strategies. In the context of herpes simplex virus (HSV), both HSV-1 and HSV-2 testing results predominantly reflect negative outcomes, although females tend to have slightly higher testing rates. This trend may be attributed to increased awareness and proactive health-seeking behaviors among women, particularly in reproductive health contexts where routine screenings are more common [19].
Chlamydia trachomatis testing also reveals a predominance of negative results, with a significant proportion of positive cases reported among high-risk populations. Studies indicate that while the infection can often be asymptomatic, the overall testing rates among females are higher, reflecting a targeted approach to screening in populations at risk [20,21]. The literature suggests that age and socioeconomic factors significantly influence the prevalence of Chlamydia infections, particularly among younger women aged 20-24, who are at greater risk due to various behavioral and biological factors [22,23]. Furthermore, disparities in access to testing services continue to persist, highlighting the need for improved outreach and education efforts to ensure equitable coverage across different demographics [24].
For other pathogens such as Treponema pallidum (causing syphilis), Haemophilus ducreyi (causing chancroid), and Klebsiella granulomatis (causing donovanosis), the results are largely negative, indicating low prevalence in the tested populations. The negative results for Treponema pallidum, in particular, are significant as they reflect the effectiveness of public health interventions aimed at reducing syphilis transmission rates. While negative test results for STIs are common across various pathogens, the higher testing rates among females highlight the importance of gender-specific health strategies. Continued efforts to enhance testing accessibility and education, particularly for high-risk populations, are essential in addressing the disparities in STI prevalence and ensuring comprehensive sexual health services.
The analysis of age-specific trends in disease prevalence and testing coverage reveals significant disparities in the rates of HIV, Treponema pallidum, HSV-2, and Chlamydia trachomatis across different age groups. Notably, HIV prevalence peaks in the 30–49 age group, with alarming rates reported in various studies, although specific figures such as 66.67% among those aged 30–39 and 76.47% in the 40–49 age group require further verification. The importance of targeted interventions for these age groups to achieve the 95-95–95 targets for HIV treatment and care is emphasized in the literature, including findings from Marinda et al., who reported high awareness and treatment rates among HIV-positive individuals [25]. Furthermore, the prevalence of syphilis is most pronounced in the 30–39 age group, where rates have been reported to be significant, indicating a need for enhanced screening and treatment protocols for STIs in this demographic [25]. In contrast, younger individuals, particularly those under 30, exhibit elevated rates of HSV2 and Chlamydia trachomatis, suggesting a different pattern of sexual health risks that necessitates age-appropriate educational and preventive measures [25]. The findings align with studies indicating that younger populations often engage in riskier sexual behaviors, leading to higher STI rates [25].
A critical concern highlighted in the analysis is the significant testing gaps observed in older age groups (50+), underscoring the urgent need for improved diagnostic coverage in this demographic. Hlongwane and Madiba emphasize that healthcare providers often overlook the HIV risk among older adults, leading to late diagnoses and advanced disease stages at the time of detection [26]. This is further supported by research from Kiplagat et al., which illustrates the dual stigma faced by older adults living with HIV, complicating their access to care and testing services [27]. The lack of awareness and targeted outreach for older populations contributes to these gaps, as many older adults do not perceive themselves as at risk for HIV, leading to underutilization of testing services and detection [26,27].
Moreover, the COVID-19 pandemic has exacerbated these issues, as testing rates have declined significantly due to healthcare disruptions, particularly affecting older adults who are already at higher risk for severe outcomes from both HIV and COVID-19 [28,29] The need for comprehensive strategies to enhance testing and treatment access for older adults is critical, as indicated by the findings of Gebremeskel et al., which highlight the disparities in HIV testing uptake among older adults in Sub-Saharan Africa [30].
The analysis of HIV status across different age groups reveals significant trends in prevalence and testing outcomes, particularly highlighting the high rates of positive results in the 20–29 and 30–39 age groups. This observation aligns with findings from Vandormael et al. (2019), who documented a notable decline in HIV incidence among older populations, suggesting that younger individuals are more frequently diagnosed with HIV due to higher exposure risks and behavioral factors [31]. The systematic review by Frank et al. further supports this by providing a comprehensive overview of global HIV trends, indicating that younger age groups consistently show higher prevalence rates compared to older cohorts [32].
In contrast, negative HIV test results appear to be relatively stable across all age groups, although they are less common among both younger and older populations. This pattern suggests that while younger individuals may engage in riskier behaviors leading to higher infection rates, older adults may also experience lower testing rates, which could contribute to the observed decline in prevalence in these age groups [33]. The consistency of negative results across age groups may reflect a broader trend of increased awareness and preventive measures among the general population, as noted by Birdthistle et al., who highlighted the importance of targeted interventions to reduce HIV incidence among young women [34].
Moreover, the age-related variations in HIV exposure and testing outcomes can be attributed to several factors, including social stigma, access to healthcare, and the effectiveness of public health campaigns. For instance, Haeuser et al. pointed out that local shifts in HIV prevalence are influenced by demographic changes and the scale-up of antiretroviral therapy (ART), which has been more effectively implemented in younger populations [35]. This is corroborated by the findings of Akullian et al., who noted significant age shifts in HIV incidence patterns, indicating that younger cohorts are more affected by the epidemic [36].
The implications of these trends are critical for public health strategies aimed at improving testing and treatment access. As highlighted by Patel et al., there is a pressing need to enhance HIV testing among younger populations while also addressing the barriers that older adults face in accessing care [37]. The literature suggests that comprehensive approaches, including education and outreach tailored to specific age groups, are essential for reducing HIV prevalence and improving health outcomes across all demographics [38,39].
The analysis of disease testing across various age groups reveals notable patterns in the prevalence of STIs and the associated testing outcomes. Negative results for the RPR test for syphilis were predominant across all age groups, indicating a low prevalence of positive cases. However, a concerning trend emerged with "Not done" results being more prevalent among older individuals, suggesting significant gaps in testing coverage in this demographic [40,41,42]. This finding is consistent with the broader literature, which indicates that older adults often face barriers to accessing STI testing, including stigma and healthcare provider biases [43]. Moreover, Klebsiella granulomatis yielded negative results, the data suggest that while younger and middle-aged groups are more frequently tested and diagnosed with certain STIs, older populations face significant barriers to adequate testing, which may contribute to undiagnosed cases and ongoing transmission within these age groups [44].
A critical observation from the analysis is the elevated prevalence of positive HIV results in the 20–39 age group, marking this cohort as a priority for targeted health interventions. Specifically, the 40–49 age group exhibited the highest HIV prevalence at 76.47%, followed closely by the 30–39 age group at 66.67%, with a significant presence in the 20–29 group at 37.50% [45,46]. Conversely, older age groups (50+) displayed significant gaps in testing across multiple diseases, underscoring the urgent need for improved diagnostic coverage and health service accessibility for this demographic [44,47]. The disparities in testing practices and disease prevalence across age groups highlight a critical area for public health initiatives aimed at reducing STI transmission and improving overall health outcomes [43].
The analysis of disease patterns by occupation reveals significant disparities in the prevalence of STIs across different employment statuses. The findings indicate that HIV prevalence is notably highest among employed individuals, reported at 65.91%. This elevated rate may be attributed to factors such as increased mobility, workplace exposure, and potentially higher engagement in risk-taking behaviors associated with occupational environments [42,43]. In contrast, the prevalence among unemployed individuals stands at 50.98%, which reflects the socioeconomic vulnerabilities that often accompany unemployment, including limited access to healthcare services and education regarding safe practices [46]. Students, representing a younger demographic, exhibited a significantly lower HIV prevalence of 17.24%, likely due to their age and possibly lower engagement in high-risk behaviors [48].
Chlamydia trachomatis prevalence presents a critical concern, particularly among unemployed individuals, where it reaches 17.65%. This statistic underscores the urgent need for targeted public health interventions for this group, as they may lack access to preventive healthcare and education [44]. The prevalence of syphilis also mirrors this trend, with unemployed individuals reporting the highest rates at 7.84%. In comparison, employed individuals and students exhibited moderate rates of syphilis, ranging from approximately 4.5% to 6.9% [45].
The HSV-1 and HSV-2 further illustrate the occupational disparities in disease prevalence. Unemployed individuals demonstrated higher rates of HSV-1 (11.76%) and HSV-2 (19.61%), indicating that this group is particularly at risk for these infections. Conversely, students and employed individuals reported lower prevalence rates, suggesting a potential correlation between employment status and exposure risk [47].
Interestingly, Treponema pallidum, the causative agent of syphilis, was found to be more prevalent among students at 17.24%. This finding may reflect specific behavioral patterns within this demographic, such as increased sexual activity or lack of awareness regarding STI risks. Additionally, Haemophilus ducreyi, responsible for chancroid, exhibited a striking 100% prevalence in the self-employed group; however, this statistic may be skewed due to a limited sample size, necessitating caution in interpretation.
The analysis of co-occurrence and correlation rates among various STIs reveals significant patterns that underscore the interconnectedness of these diseases. The data indicate a high co-occurrence rate between HIV and HSV-2, recorded at 6.67%. This finding suggests shared risk factors or overlapping populations, which is consistent with existing literature that highlights the role of HSV-2 as a significant risk factor for HIV acquisition [49,50]. The prevalence of HSV-2 infection is known to disrupt the genital mucosa, thereby providing a portal for HIV entry, which may explain the observed co-occurrence [51,52].
Chlamydia trachomatis also exhibited notable overlap with HSV-1 and HSV-2, likely due to common transmission routes and risk behaviors associated with these infections [53,54]. The co-occurrence of Haemophilus ducreyi with both HSV-1 and Chlamydia trachomatis further indicates potential co-infection patterns that warrant attention in public health strategies [55]. The presence of multiple infections within the same population can complicate treatment and prevention efforts, highlighting the need for integrated diagnostic approaches.
Conversely, low or zero co-occurrence rates were observed for RPR test results for syphilis, which rarely overlapped with other diseases. Similarly, Klebsiella granulomatis showed no co-occurrence across all conditions in the dataset, suggesting that these infections may have distinct epidemiological profiles that do not frequently intersect [56]. This lack of overlap emphasizes the importance of targeted screening and prevention strategies for these specific infections.
Correlation analysis further elucidates the relationships between these diseases. Strong correlations were identified between HSV-1 and Haemophilus ducreyi and between Chlamydia trachomatis and HSV-1, indicating shared risk factors and potential pathways for transmission [57]. In contrast, weak or negative correlations were found for RPR results and HSV-2 and between HIV status and Treponema pallidum, suggesting limited overlap between these conditions [58]. The minimal relationships observed for diseases like HIV and RPR results reflect a low co-dependence, indicating that interventions targeting one may not necessarily impact the other.
The analysis of disease correlations within the context of STIs reveals distinct patterns that can inform public health strategies and clinical practices. Strong correlations were identified between HSV-1 and Haemophilus ducreyi (correlation coefficient of 0.64), suggesting a potential for co-occurrence or shared risk factors between these two infections [59]. This correlation may be attributed to overlapping transmission routes, as both infections are often associated with sexual activity and can occur in similar populations.
Additionally, a significant correlation was observed between Chlamydia trachomatis and HSV-1 (0.56), further indicating a link likely driven by common transmission pathways [59,60]. The presence of Chlamydia trachomatis, a prevalent bacterial STI, may increase susceptibility to HSV-1 infection due to mucosal disruption during sexual contact. This finding highlights the importance of considering multiple infections in the same patient population, as co-infections can complicate treatment and management strategies.
Conversely, weak or negative correlations were noted between RPR results and HSV-2 (-0.13), reflecting minimal overlap between these two conditions. This suggests that individuals who test positive for one may not necessarily be at increased risk for the other, indicating distinct epidemiological profiles [61,62]. Similarly, the correlation between HIV status and Treponema pallidum (-0.19) suggests a lower likelihood of concurrent infections in the dataset, which may be influenced by differing risk factors and transmission dynamics associated with each infection [63]. Moreover, several diseases, such as HIV and RPR results, demonstrated minimal or negligible correlations with other conditions, indicating limited interdependence. This lack of correlation underscores the necessity for tailored public health interventions that address the unique characteristics and risk factors associated with each STI [64,65].
5. Conclusions
The analysis highlights the intricate interplay of age-specific trends in disease prevalence and testing coverage, revealing critical implications for public health strategies. It underscores the necessity of targeted interventions to address the unique needs and barriers faced by different demographics, particularly older adults, while improving testing rates and diagnostic coverage for all age groups. The higher rates of positive results among younger individuals, alongside stable negative outcomes across age groups, suggest complex factors influencing exposure and testing behaviors. These findings emphasize the importance of integrated diagnostics for co-occurring infections, such as HIV and HSV-2, and tailored prevention strategies for diseases with shared transmission pathways, like Chlamydia trachomatis and HSV-1/HSV-2. Furthermore, the occupational disparities in disease prevalence, particularly among unemployed individuals, signal an urgent need for focused outreach, education, and testing programs targeting at-risk populations. Investigating testing gaps and population-specific risks for infections with low correlation remains vital for developing effective interventions. Overall, the results call for comprehensive, demographically informed public health efforts to enhance health outcomes and reduce transmission rates across diverse populations
Author Contributions
Conceptualization, T.T. and T.A.; methodology, T.T.; formal analysis, T.T.; investigation, T.T.; resources, T.A.; data curation, T.T.; writing—original draft preparation, T.T. and L.M.F.; writing—review and editing, Z.Z.A.M.; visualization, T.T. and L.M.F.; supervision, Z.Z.A.M. and T.A.; project administration, T.T.; funding acquisition, T.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Walter Sisulu University’s University Capacity Development Grant Research Fund (TRT), and the APC was funded by Walter Sisulu University
Institutional Review Board Statement
The study was conducted following the Declaration of Helsinki and approved by the Research Ethics and Biosafety Committee of the Faculty of Medicine and Health Sciences of Walter Sisulu University (ref. No. 015/2016) and Eastern Cape Department of Health (ref. No. EC_2016RP26_934).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data can be requested from the corresponding author.
Acknowledgments
The authors wish to acknowledge Sister Z.N. Jafta for participants’ enrolment and sample collection, the staff of the CHCs for use of their facilities, and the Nelson Mandela Academic Clinical Research Unit for using their facilities for sample storage.
Conflicts of Interest
The authors declare no conflicts of interest
References
- Zheng, Y.; Yu, Q.; Lin, Y.; Zhou, Y.; Lan, L.; Yang, S.; Wu, J. Global burden and trends of sexually transmitted infections from 1990 to 2019: an observational trend study. The Lancet Infectious Diseases. 2022, 22, 541–551. [Google Scholar] [CrossRef]
- Huyveneers, L.E.; Maphanga, M.; Umunnakwe, C.N.; Bosman-de Boer, L.; Moraba, R.S.; Tempelman, H.A.; Wensing, A.M.; Hermans, L.E. Prevalence, incidence, and recurrence of sexually transmitted infections in HIV-negative adult women in a rural South African setting. Tropical Medicine & International Health. 2023, 28, 335–342. [Google Scholar]
- Dhar, C.P.; Feuerstein, J.L.; Salas-Humara, C. Overview of Vaginal Ulcerative Disease. Pediatric Annals. 2024, 53, e10–e16. [Google Scholar] [CrossRef] [PubMed]
- Tshaka, T.R.; Singh, R.; Apalata, T.R.; Mbulawa, Z.Z.A. Aetiology of genital ulcer disease and associated factors among Mthatha public clinic attendees. S Afr J Infect Dis. 2022, 37, a444. [Google Scholar] [CrossRef]
- Musonda, P.; Halwiindi, H.; Kaonga, P.; Ngoma-Hazemba, A.; Simpungwe, M.; Mweemba, M.; Tembo, C.; Zyambo, C.; Chisoso, J.; Munakampe, M.; Choonga, P. HIV, syphilis and sexual-risk behaviours’ prevalence among in-and out-of-school adolescent girls and young women in Zambia: A cross-sectional survey study. Plos one. 2024, 19, e0294545. [Google Scholar] [CrossRef] [PubMed]
- KORKUSUZR, *!!! REPLACE !!!*; ŞENOĞLUS, *!!! REPLACE !!!*. Syphilis Seroprevalence and Associated Risk Factors in HIV-infected Individuals. Mediterranean Journal of Infection, Microbes & Antimicrobials 2020, 9. [Google Scholar]
- Gilbert, L.; Dear, N.; Esber, A.; Iroezindu, M.; Bahemana, E.; Kibuuka, H.; Owuoth, J.; Maswai, J.; Crowell, T.A.; Polyak, C.S.; Ake, J.A. Prevalence and risk factors associated with HIV and syphilis co-infection in the African Cohort Study: a cross-sectional study. BMC Infectious Diseases. 2021, 21, 1–7. [Google Scholar] [CrossRef]
- Kularatne, R.S.; Muller, E.E.; Maseko, D.V.; Kufa-Chakezha, T.; Lewis, D.A. Trends in the relative prevalence of genital ulcer disease pathogens and association with HIV infection in Johannesburg, South Africa, 2007–2015. PLoS One 2018, 13, e0194125. [Google Scholar] [CrossRef]
- Abdallah, I.; Armstrong-Mensah, E.; Alema-Mensah, E.; Cheryl, J. Demographic and behavioural risk factors associated with Trichomonas vaginalis among South African HIV-positive men with genital ulcer disease: a cross-sectional study. BMJ Open 2017, 7, e013486. [Google Scholar] [CrossRef]
- Smith, J.S.; Robinson, N.J. Age-specific prevalence of infection with herpes simplex virus types 2 and 1: a global review. The Journal of Infectious Diseases. 2002, 186 (Supplement_1), S3–S28. [Google Scholar] [CrossRef]
- Wand, H.; Reddy, T.; Dassaye, R.; Moodley, J.; Naidoo, S.; Ramjee, G. Estimating prevalence and incidence of sexually transmitted infections among South African women: Implications of combined impacts of risk factors. Int J STD AIDS. 2020, 31, 1093–1101. [Google Scholar] [CrossRef] [PubMed]
- Mathias, B.A.; Muñoz, T.I.; Guaicha, E.P.; Quinde, A.P.; Herrera, M.F. Side effects of Sexually Transmitted Infections (STIs) on female fertility: diagnostic and treatment strategies–a literature review. Ibero-American Journal of Health Science Research. 2024, 4, 84–92. [Google Scholar] [CrossRef]
- Kojima, N.; Klausner, J.D. An Update on the Global Epidemiology of Syphilis. Curr Epidemiol Rep. 2018, 5, 24–38. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Malama, K.; Logie, C.H.; Sokolovic, N.; Skeritt, L.; O'Brien, N.; Cardinal, C.; Gagnier, B.; Loutfy, M.; Kaida, A.; de Pokomandy, A. Pathways from HIV-related stigma, racial discrimination, and gender discrimination to HIV treatment outcomes among women living with HIV in Canada: longitudinal cohort findings. JAIDS Journal of Acquired Immune Deficiency Syndromes. 2023, 94, 116–123. [Google Scholar] [CrossRef] [PubMed]
- Ha, J.H.; Van Lith, L.M.; Mallalieu, E.C.; Chidassicua, J.; Pinho, M.D.; Devos, P.; Wirtz, A.L. Gendered relationship between HIV stigma and HIV testing among men and women in Mozambique: a cross-sectional study to inform a stigma reduction and male-targeted HIV testing intervention. BMJ Open. 2019, 9, e029748. [Google Scholar] [CrossRef]
- Smith, P.J.; Davey, D.J.; Green, H.; Cornell, M.; Bekker, L.G. Reaching underserved South Africans with integrated chronic disease screening and mobile HIV counselling and testing: A retrospective, longitudinal study conducted in Cape Town. Plos one. 2021, 16, e0249600. [Google Scholar] [CrossRef]
- Turan, J.M.; Elafros, M.A.; Logie, C.H.; Banik, S.; Turan, B.; Crockett, K.B.; Pescosolido, B.; Murray, S.M. Challenges and opportunities in examining and addressing intersectional stigma and health. BMC Medicine. 2019, 17, 1–5. [Google Scholar] [CrossRef]
- Klein, P.W.; Psihopaidas, D.; Xavier, J.; Cohen, S.M. HIV-related outcome disparities between transgender women living with HIV and cisgender people living with HIV served by the Health Resources and Services Administration’s Ryan White HIV/AIDS Program: a retrospective study. PLoS Medicine. 2020, 17, e1003125. [Google Scholar] [CrossRef]
- Naeem, A.; Waseem, H.; Ali, S.; Usman, J.; Hanif, F.; Furqan, W. CHLAMYDIA TRACHOMATIS INFECTION IN PELVIC INFLAMMATORY DISEASE PATIENTS–A SNAP SHOT. Infectious Diseases Journal of Pakistan. 2023, 32, 93–98. [Google Scholar] [CrossRef]
- Chen, H.; Luo, L.; Wen, Y.; He, B.; Ling, H.; Shui, J.; He, P.; Hou, X.; Tang, S.; Li, Z. Chlamydia trachomatis and human papillomavirus infection in women from southern Hunan Province in China: a large observational study. Frontiers in Microbiology. 2020, 11, 827. [Google Scholar] [CrossRef]
- Li, T.; Liu, Z.; Zhang, D.; Liao, Q.; Fan, S.; Hao, M.; Hong, Y.; Huang, X.; Wang, H.; Xiong, Z.; Xu, H. Prevalence of and risk factors for chlamydia in female outpatients with genital tract infections: a nationwide multi-center, cross-sectional study in China. Frontiers in Public Health. 2023, 11, 1182108. [Google Scholar] [CrossRef] [PubMed]
- Yan, R.L.; Ye, Y.F.; Fan, Q.Y.; Huang, Y.H.; Wen, G.C.; Li, L.M.; Cai, Y.M.; Feng, T.J.; Huang, Z.M. Chlamydia trachomatis infection among patients attending sexual and reproductive health clinics: a cross-sectional study in Bao'an district, Shenzhen, China. PLoS One. 2019, 14, e0212292. [Google Scholar] [CrossRef]
- Dombrowski, J.C.; Wierzbicki, M.R.; Newman, L.M.; Powell, J.A.; Miller, A.; Dithmer, D.; Soge, O.O.; Mayer, K.H. Doxycycline versus azithromycin for the treatment of rectal chlamydia in men who have sex with men: a randomized controlled trial. Clinical Infectious Diseases. 2021, 73, 824–831. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Chow, E.P.; Ong, J.J.; Hoebe, C.J.; Zou, Z.; Hocking, J.S.; Fairley, C.K.; Zhang, L. Chlamydia trachomatis transmission between the oropharynx, urethra and anorectum in men who have sex with men: a mathematical model. BMC medicine. 2020, 18, 1–0. [Google Scholar] [CrossRef]
- Marinda, E.; Simbayi, L.; Zuma, K.; Zungu, N.; Moyo, S.; Kondlo, L.; Jooste, S.; Nadol, P.; Igumbor, E.; Dietrich, C.; Briggs-Hagen, M. Towards achieving the 90–90–90 HIV targets: results from the south African 2017 national HIV survey. BMC Public Health. 2020, 20, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Hlongwane, N.; Madiba, S. Navigating life with HIV as an older adult in South African communities: A phenomenological study. International Journal of Environmental Research and Public Health. 2020, 17, 5797. [Google Scholar] [CrossRef]
- Kiplagat, J.; Mwangi, A.; Chasela, C.; Huschke, S. Challenges with seeking HIV care services: perspectives of older adults infected with HIV in western Kenya. BMC Public Health. 2019, 19, 1–2. [Google Scholar] [CrossRef]
- Huang, G.; Cheng, W.; Xu, Y.; Yang, J.; Jiang, J.; Pan, X.; Zhou, X.; Jiang, J.; Chai, C. Spatiotemporal Pattern and Its Determinants for Newly Reported HIV/AIDS Among Older Adults in Eastern China From 2004 to 2021: Retrospective Analysis Study. JMIR Public Health and Surveillance. 2024, 10, e51172. [Google Scholar] [CrossRef]
- Waterfield, K.C.; Shah, G.H.; Etheredge, G.D.; Ikhile, O. Consequences of the COVID-19 crisis for persons with HIV: the impact of social determinants of health. BMC Public Health. 2021, 21, 1–7. [Google Scholar] [CrossRef]
- Gebremeskel, A.T.; Gunawardena, N.; Omonaiye, O.; Yaya, S. Sex Differences in HIV Testing among Older Adults in Sub-Saharan Africa: A Systematic Review. BioMed Research International. 2021, 2021, 5599588. [Google Scholar] [CrossRef]
- Vandormael, A.; Akullian, A.; Siedner, M.; de Oliveira, T.; Bärnighausen, T.; Tanser, F. Declines in HIV incidence among men and women in a South African population-based cohort. Nature Communications. 2019, 10, 5482. [Google Scholar] [CrossRef] [PubMed]
- Frank, T.D.; Carter, A.; Jahagirdar, D.; Biehl, M.H.; Douwes-Schultz, D.; Larson, S.L.; Arora, M.; Dwyer-Lindgren, L.; Steuben, K.M.; Abbastabar, H. and Abu-Raddad, L.J., 2019. Global, regional, and national incidence, prevalence, and mortality of HIV, 1980–2017, and forecasts to 2030, for 195 countries and territories: a systematic analysis for the Global Burden of Diseases, Injuries, and Risk Factors Study. The Lancet HIV 2017, 6, e831–e859. [Google Scholar]
- Hayes, R.J.; Donnell, D.; Floyd, S.; Mandla, N.; Bwalya, J.; Sabapathy, K.; Yang, B.; Phiri, M.; Schaap, A.; Eshleman, S.H.; Piwowar-Manning, E. Effect of universal testing and treatment on HIV incidence—HPTN 071 (PopART). New England Journal of Medicine. 2019, 381, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Birdthistle, I.; Tanton, C.; Tomita, A.; de Graaf, K.; Schaffnit, S.B.; Tanser, F.; Slaymaker, E. Recent levels and trends in HIV incidence rates among adolescent girls and young women in ten high-prevalence African countries: a systematic review and meta-analysis. The Lancet Global Health. 2019, 7, e1521–40. [Google Scholar] [CrossRef]
- Haeuser, E.; Serfes, A.L.; Cork, M.A.; Yang, M.; Abbastabar, H.; Abhilash, E.S.; Adabi, M.; Adebayo, O.M.; Adekanmbi, V.; Adeyinka, D.A.; Afzal, S. Mapping age-and sex-specific HIV prevalence in adults in sub-Saharan Africa, 2000–2018. BMC medicine. 2022, 20, 488. [Google Scholar] [CrossRef] [PubMed]
- Akullian, A.; Vandormael, A.; Miller, J.C.; Bershteyn, A.; Wenger, E.; Cuadros, D.; Gareta, D.; Bärnighausen, T.; Herbst, K.; Tanser, F. Large age shifts in HIV-1 incidence patterns in KwaZulu-Natal, South Africa. Proceedings of the National Academy of Sciences. 2021, 118, e2013164118. [Google Scholar] [CrossRef]
- Patel, D.; Johnson, C.H.; Krueger, A.; Maciak, B.; Belcher, L.; Harris, N.; DiNenno, E.A. Trends in HIV testing among US adults, aged 18–64 years, 2011–2017. AIDS and behavior. 2020, 24, 532–539. [Google Scholar] [CrossRef]
- Havlir, D.; Lockman, S.; Ayles, H.; Larmarange, J.; Chamie, G.; Gaolathe, T.; Iwuji, C.; Fidler, S.; Kamya, M.; Floyd, S.; Moore, J. What do the Universal Test and Treat trials tell us about the path to HIV epidemic control? Journal of the International AIDS Society. 2020, 23, e25455. [Google Scholar] [CrossRef]
- Govender, R.D.; Hashim, M.J.; Khan, M.A.; Mustafa, H.; Khan, G. Global epidemiology of HIV/AIDS: a resurgence in North America and Europe. Journal of epidemiology and global health. 2021, 11, 296–301. [Google Scholar] [CrossRef]
- Workowski, K.A. Sexually Transmitted Infections Treatment Guidelines. MMWR. Recommendations and Reports. 2021, 2021, 70. [Google Scholar]
- Willemstein, I.J.; Götz, H.M.; Visser, M.; Heijne, J.C. HIV and syphilis testing for women and heterosexual men aged above 25 years in the Netherlands: possibilities for targeted testing at sexual health centres. BMJ open. 2023, 13, e072862. [Google Scholar] [CrossRef] [PubMed]
- Effendi, I.; Rosana, Y.; Yasmon, A.; Indriatmi, W. Multiplex nested polymerase chain reaction for Treponema pallidum using blood is more sensitive than using serum. Universa Medicina. 2018, 37, 75–84. [Google Scholar] [CrossRef]
- Bristow, C.C.; Leon, S.R.; Huang, E.; Ramos, L.B.; Vargas, S.K.; Flores, J.A.; Konda, K.A.; Caceres, C.F.; Klausner, J.D. Field evaluation of a dual rapid immunodiagnostic test for HIV and syphilis infection in Peru. Sexually transmitted diseases. 2016, 43, 57–60. [Google Scholar] [CrossRef]
- Mosen, D.M.; Banegas, M.P.; Dickerson, J.F.; Fellows, J.L.; Pihlstrom, D.J.; Kershah, H.M.; Scott, J.L.; Keast, E.M. Evaluating the Effectiveness of Medical–Dental Integration to Close Preventive and Disease Management Care Gaps. Frontiers in dental medicine. 2021, 2, 670012. [Google Scholar] [CrossRef]
- Song, Y.; Liu, Y.S.; Talarico, F.; Zhang, Y.; Hayward, J.; Wang, M.; Stroulia, E.; Dixon, R.A.; Greiner, R.; Li, X.; Greenshaw, A. Associations between differential aging and lifestyle, environment, current, and future health conditions: Findings from Canadian Longitudinal Study on Aging. Gerontology. 2023, 69, 1394–1403. [Google Scholar] [CrossRef] [PubMed]
- Nkansah, C.; Serwaa, D.; Osei-Boakye, F.; Owusu-Ampomah, R. Magnitude and trend of HIV and Treponema pallidum infections among blood donors in Offinso-North District, Ghana: a nine-year retrospective, cross-sectional study. African health sciences. 2022, 22, 465–474. [Google Scholar] [CrossRef]
- Liu, W.S.; You, J.; Ge, Y.J.; Wu, B.S.; Zhang, Y.; Chen, S.D.; Zhang, Y.R.; Huang, S.Y.; Ma, L.Z.; Feng, J.F.; Cheng, W. Association of biological age with health outcomes and its modifiable factors. Aging Cell. 2023, 22, e13995. [Google Scholar] [CrossRef]
- Corebima, B.I.; Almiradani, A.; Sulistijono, E. Importance of Serological Tests in the Diagnosis of Asymptomatic Congenital Syphilis in Neonates: A Case Report. Archives of Pediatric Infectious Diseases. 2020, 9. [Google Scholar] [CrossRef]
- Bradley, J.; Floyd, S.; Piwowar-Manning, E.; Laeyendecker, O.; Young, A.; Bell-Mandla, N.; Bwalya, J.; Bock, P.; Fidler, S.; Ayles, H.; Hayes, R.J. Sexually transmitted bedfellows: exquisite association between HIV and herpes simplex virus type 2 in 21 communities in southern Africa in the HIV prevention trials network 071 (PopART) study. The Journal of Infectious Diseases. 2018, 218, 443–452. [Google Scholar] [CrossRef]
- Reinheimer, C.; Doerr, H.W. Prevalence of herpes simplex virus type 2 in different risk groups: Thirty years after the onset of HIV. Intervirology. 2012, 55, 395–400. [Google Scholar] [CrossRef]
- Barnabas RV, Wasserheit JN, Huang Y, Janes H, Morrow R, Fuchs J, Mark KE, Casapia M, Mehrotra DV, Buchbinder SP, Corey L; NIAID HIV Vaccine Trials Network. Impact of herpes simplex virus type 2 on HIV-1 acquisition and progression in an HIV vaccine trial (the Step study). J Acquir Immune Defic Syndr. 2011, 57, 238–244. [CrossRef] [PubMed] [PubMed Central]
- Sunur, S.; Purwoko, I.H.; Yahya, Y.F.; Pamudji, R. Genital Herpes in Human Immunodeficiency Virus Infected Patients. Bioscientia Medicina: Journal of Biomedicine and Translational Research. 2021, 5, 758–772. [Google Scholar]
- Ajani, T.A.; Oluwasola, T.A.; Anaedobe, C.G.; Ajani, M.A.; Fayemiwo, S.A.; Bakare, R.A. Correlates of genital Chlamydial trachomatis infection in a cohort of infertile women in Ibadan, Nigeria. Int J Reprod Contracep Obstet Gynecol. 2017, 6, 3754–3759. [Google Scholar] [CrossRef]
- Beyuo, T.; Oppong, S.A.; Samba, A.; Beyuo, V.M. Chlamydia trachomatis infection among Ghanaian women undergoing hysterosalpingography for suspected tubal factor infertility. International Journal of Gynecology & Obstetrics. 2019, 146, 200–205. [Google Scholar]
- Shukla, D.; Kalyan, R.K.; Gupta, P.; Venkatesh, V.; Agarwal, A. The socio-demographic profile and clinical correlation of Chlamydia trachomatis among infertile women at a tertiary care center in North India. International Journal of Reproduction, Contraception, Obstetrics and Gynecology. 2024, 13, 332–339. [Google Scholar] [CrossRef]
- Lautenschlager, S.; Kemp, M.; Christensen, J.J.; Mayans, M.V.; Moi, H. 2017 European guideline for the management of chancroid. Int J STD AIDS. 2017, 28, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Martinelli, E.; Tharinger, H.; Frank, I.; Arthos, J.; Piatak Jr, M.; Lifson, J.D.; Blanchard, J.; Gettie, A.; Robbiani, M. HSV-2 infection of dendritic cells amplifies a highly susceptible HIV-1 cell target. PLoS pathogens. 2011, 7, e1002109. [Google Scholar] [CrossRef]
- Adejumo, B.I.; Oronsaye, F.E.; Drisu, U.I.; Adebowale, M.O.; Oke, O.M.; Dimkpa, U.; Omosor, K.I.; Abdulrahman, O.N.; Ukatu, E.N.; Michael, E.A. The Level of CD4+ T Cell Count among Reproductive Age Women Coinfected with Human Immune Virus, Hepatitis Surface Antigen and Herpes Simplex Virus in Kogi State, Nigeria. Health. 2018, 10, 1449–1458. [Google Scholar] [CrossRef]
- Popoola, V.O.; Kagaayi, J.; Ssekasanvu, J.; Ssekubugu, R.; Kigozi, G.; Ndyanabo, A.; Nalugoda, F.; Chang, L.W.; Lutalo, T.; Tobian, A.A.; Kabatesi, D. Prevalence of untreated HIV and HIV incidence among occupational groups in Rakai, Uganda: a population-based longitudinal study, 1999-2016. medRxiv. 2022, 2022–06. [Google Scholar]
- Adegbosin, A.P.; Adegbosin, A.E. A review of socioeconomic inequalities in HIV infections among women in Low and Middle-income countries. medRxiv. 2022, 2022–07. [Google Scholar]
- Abdulkarim, S.; John, S.; Garba, T.; Basason, H.; Balogun, P.; Kuye, J. Perceptions of TB-HIV comorbidity among the Nomads in Adamawa State, Nigeria. BMC Public Health. 2024, 24, 1208. [Google Scholar] [CrossRef]
- Kimaro, L.; Adinan, J.; Damian, D.J.; Njau, B. Prevalence of occupational injuries and knowledge of availability and utilization of post exposure prophylaxis among health care workers in Singida District Council, Singida Region, Tanzania. PLoS One. 2018, 13, e0201695. [Google Scholar] [CrossRef] [PubMed]
- Nwalozie, R.; Kareem, J.A.; Ikpo, P.E. Epidemiological Distribution of Human Immunodeficiency Virus (HIV) among Residents of Port Harcourt Metropolis in Rivers State Nigeria. Asian Journal of Research in Infectious Diseases. 2024, 15, 1–1. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, X.; Huang, Y.; Gao, L.; Gao, Z.; He, M. The prevalence of Human Immunodeficiency Virus infection among voluntary blood donors in mainland China: A systematic review and meta-analysis. Journal of Medical Virology. 2024, 96, e29599. [Google Scholar] [CrossRef] [PubMed]
- Hanke, D.; Freuling, C.M.; Fischer, S.; Hueffer, K.; Hundertmark, K.; Nadin-Davis, S.; Marston, D.; Fooks, A.R.; Bøtner, A.; Mettenleiter, T.C.; Beer, M. Spatio-temporal analysis of the genetic diversity of arctic rabies viruses and their reservoir hosts in Greenland. PLoS neglected tropical diseases. 2016, 10, e0004779. [Google Scholar] [CrossRef]
Figure 1.
Distribution of GUD by age group.
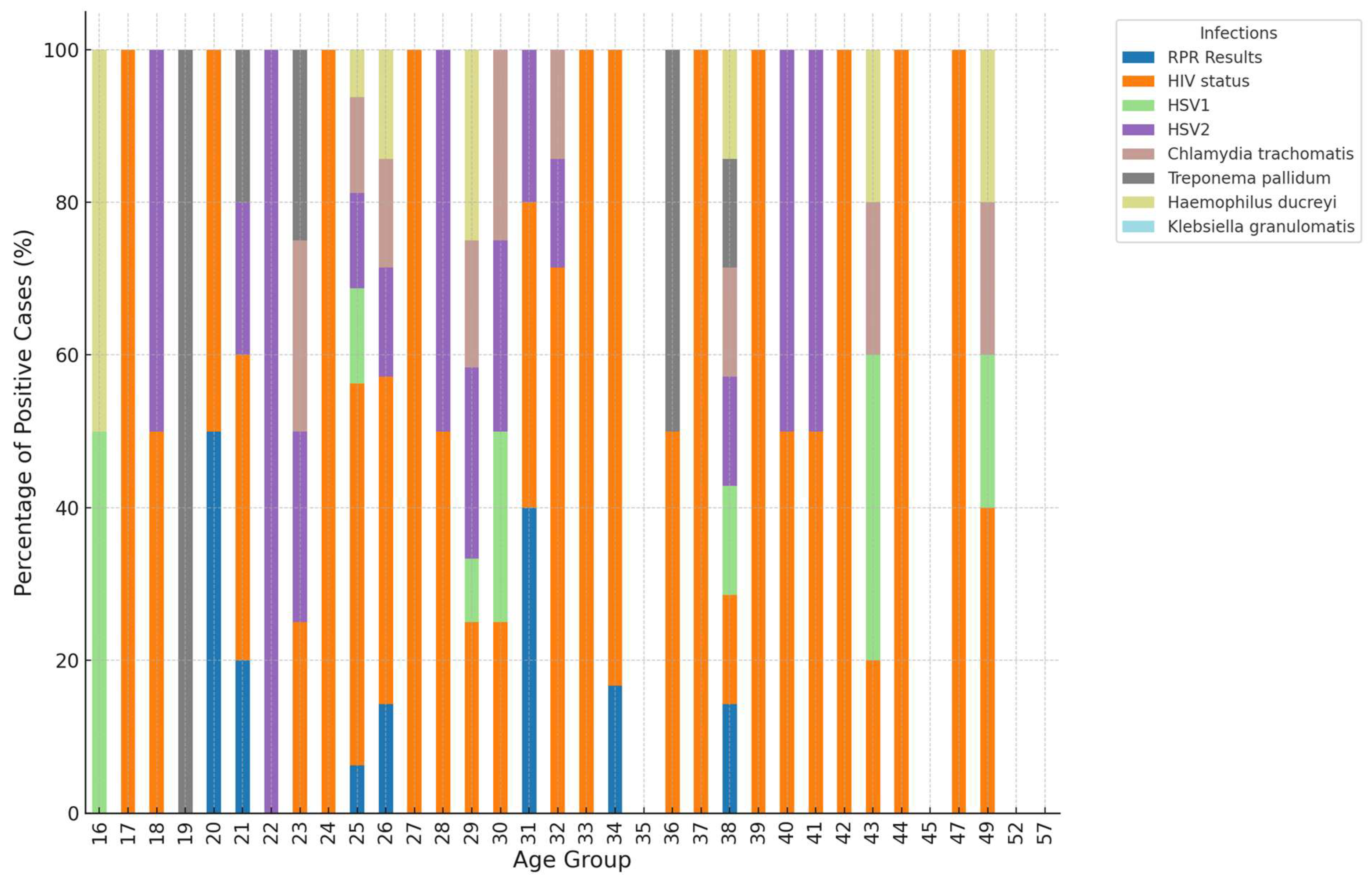
Figure 2.
Co-occurrence and correlation rates among genital ulcer diseases.
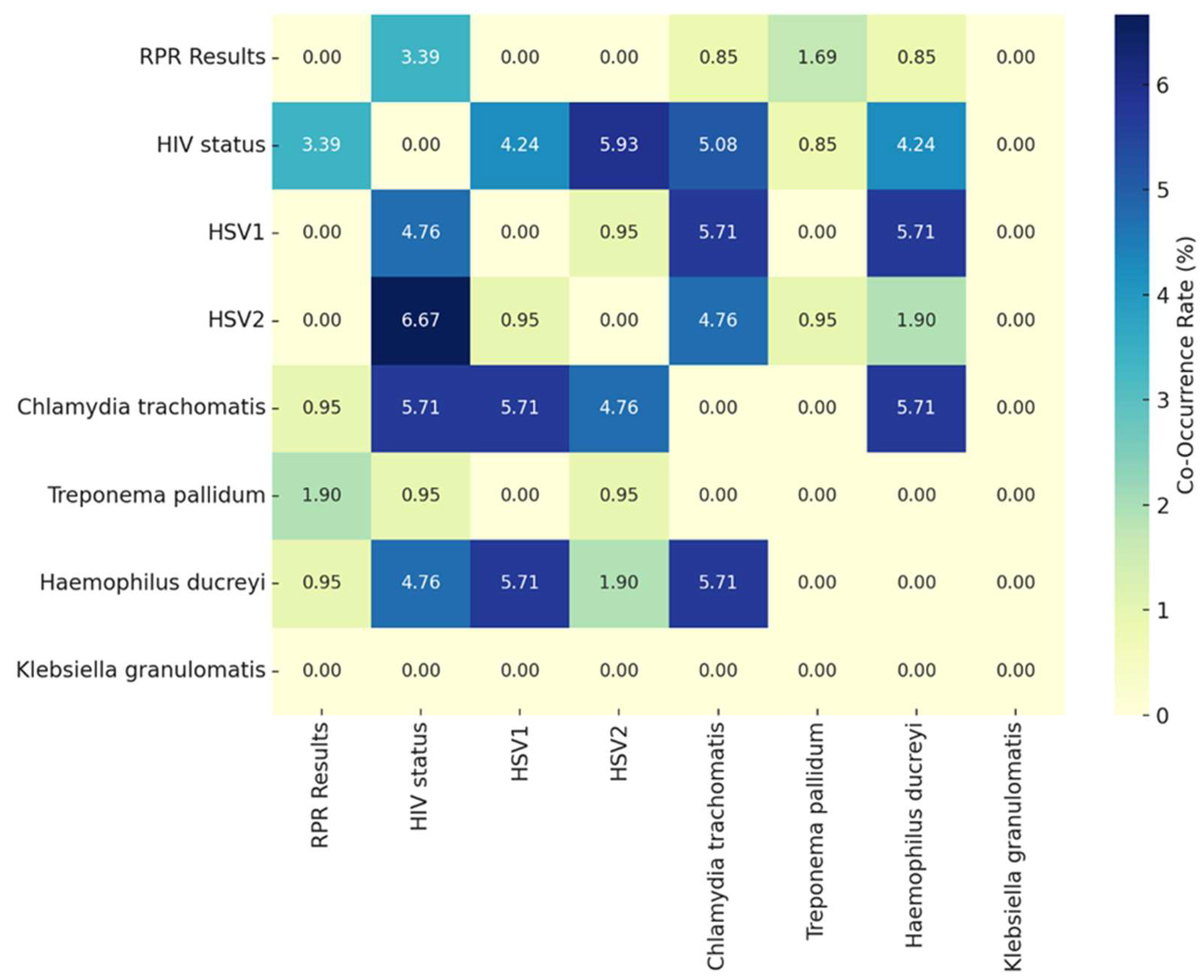
Figure 3.
Correlation patterns and co-occurrence of sexually transmitted infections.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



