
Submitted:
26 December 2024
Posted:
27 December 2024
You are already at the latest version
Abstract
Background/Objectives: Dietary supplements are commonly used in Japan. Although some dietary supplements can affect perioperative conditions due to abnormalities in the blood coagulation system, there are no reports examining the duration of withdrawal and the risk of complications during bronchoscopy. We aimed to retrospectively review the safety and withdrawal periods of supplements prior to bronchoscopy in patients who regularly consumed dietary supplements.
Methods: This single-center retrospective observational study was conducted at Tottori University Hospital. Patients who underwent bronchoscopy between January 2019 and December 2019 were validated and examined. We examined patient backgrounds, in-cluding age, sex, underlying conditions, use of antithrombotic agents, consumption of di-etary supplements and the specific types of dietary supplements consumed, and the type of bronchoscopy procedure. Data regarding the duration of dietary supplement with-drawal and complications during and after bronchoscopy were also collected.
Results: A total of 351 bronchoscopy procedures were performed during the observation period. Of these, 69 (23.3%) bronchoscopies were performed on patients who regularly used dietary supplements. There were 19 cases of invasive bronchoscopy in patients who regularly used dietary supplements with bleeding risk. The median withdrawal period for the dietary supplements was 14 days. The incidence of bleeding complications from inva-sive bronchoscopy did not differ significantly among the groups divided according to whether they took antithrombotic agents or dietary supplements with bleeding risk.
Conclusions: Based on this retrospective analysis, dietary supplements may be considered safe if there is sufficient time to avoid taking them before undergoing invasive bronchoscopy.
Keywords:
dietary supplements
; bronchoscopy
; complication risk
1. Introduction
Recently, dietary supplements have become more commonly used in Japan as people become more health conscious, and according to the 2019 National Health and Nutrition Survey by the Ministry of Health, Labour and Welfare, 34.4% of people aged 20 and older consume dietary supplements [1]. A wide range of dietary supplements exists, yet their potential side effects and interactions with medications have not been sufficiently validated. Some dietary supplements have ingredients that can affect perioperative conditions due to abnormalities in the blood coagulation system, cardiovascular system, electrolytes, and prolonged anesthetic effects [2].
The American Society of Anesthesiologists (ASA) recommends discontinuing healthy foods for at least 2 weeks before surgery. Healthy foods from the ASA that affect the perioperative period include ephedra, garlic, ginkgo, ginseng, kava, St. John’s wort, valerian, and vitamin E [3]. In addition, Hatfield et al. reported that garlic, hawthorn, cordyceps, echinacea, and aloe vera are associated with surgical bleeding independent of anticoagulants, while ginkgo biloba, chondroitin-glucosamine, melatonin, turmeric, bilberry, chamomile, fenugreek, milk thistle, peppermint, cinnamon, and ginger are associated with anticoagulant-related bleeding. Additionally, fish oil, ginseng, and saw palmetto also are thought to be associated with bleeding events, but randomized control trials (RCT) have not demonstrated an increased bleeding risk [4].
Bronchoscopy is often conducted after discontinuation of dietary supplements. However, there is a lack of research investigating the optimal time of withdrawal and its impact on the risk of problems during bronchoscopy. We, therefore, aimed to determine the safety and withdrawal period for dietary supplements for patients undergoing bronchoscopy, with a particular focus on bleeding complications.
2. Methods
2.1. Study Design and Patients
This single-center retrospective observational study was conducted at Tottori University Hospital. The medical records of patients who underwent bronchoscopy between January 2019 and December 2019 were validated and examined. All patients who underwent bronchoscopy during the study period were enrolled to avoid selection bias; however, patients who refused to participate by opting out were excluded from enrollment. Medical information about patients were collected from electronic medical records. This study examined patient backgrounds, including age, sex, underlying conditions, use of antithrombotic agents, consumption of dietary supplements and the specific types of dietary supplements consumed, and the type of bronchoscopy procedure. Data regarding the duration of dietary supplement withdrawal and complications during and after bronchoscopy were also collected. Since the presence or absence of antithrombotic agents and dietary supplements is expected to strongly influence bleeding complications, the frequency of complications was compared among patients who used dietary supplements with bleeding risk, and did not use antithrombotic agents; used dietary supplements without bleeding risk, and did not use antithrombotic agents; used antithrombotic agents, and did not use dietary supplements; used antithrombotic agents and dietary supplements with bleeding risk; used antithrombotic agents and dietary supplements without bleeding risk; and patients who used neither dietary supplements nor antithrombotic agents. The severity of bleeding was assessed according to the criteria of the British Thoracic Society [5]. We followed the STROBE guidelines for the report of this study [6].
2.2. Dietary Supplements
The dietary supplements listed in the ASA recommendation and the report by Hatfield et al [4]. were considered “dietary supplements with bleeding risk” in this study. Fish oil, ginseng, and saw palmetto are associated with bleeding; however, fish oil did not increase the risk of bleeding in a systematic review and meta-analysis of several RCTs, and no RCTs have examined the risk of bleeding in patients who underwent bronchoscopy [4,7,8,9,10,11,12,13,14,15,16]. Similar to fish oil, ginseng and saw palmetto have been reported in RCTs to be unrelated to bleeding, but have not been examined for bleeding risk in bronchoscopy [17,18,19]. Generally, there are fewer procedures to control bleeding during bronchoscopy than during surgery. Moreover, there is a risk of respiratory deterioration and asphyxia in cases of massive hemorrhage during bronchoscopy. Hence, in this study, fish oil, ginseng, and saw palmetto were included among the dietary supplements with bleeding risks.
2.3. Statistical Analysis
Patient backgrounds and complications were analyzed using the chi-squared test or Fisher’s exact test to compare patient groups based on medication and dietary supplement usage. Binary logistic regression analysis was performed to examine the factors influencing bleeding complications. Statistical analyses were performed using SPSS Statistics for Windows (version 22, IBM Corp., Armonk, NY). Statistical significance was set at p < 0.05.
3. Results
3.1. Patient Characteristics
A total of 322 patients underwent bronchoscopies during the observation period. As some patients underwent multiple examinations, a total of 381 bronchoscopies were recorded. Among them, the description of bronchoscopy was inadequate and the details of bronchoscopy were unknown in three patients (four cases). Medication information was lacking for five patients (six cases), and information on dietary supplement use was lacking for 12 patients (14 cases). In six patients (six cases), the ingredients of the dietary supplements consumed were unknown. The reasons for the unknown ingredients were as follows: in three cases, the patient did not know the names of the dietary supplements that they regularly took; in two patients, the details of the ingredients were not provided by the manufacturer; and in one patient, the type of herb in the herbal tea that the patient regularly used was not recorded by medical staff. Patients with insufficient information were excluded from the analysis; thus, 296 patients (351 cases) were analyzed (Figure 1). Among them, 69 (23.3%) were regular users of dietary supplements and 76 (21.6 %) used dietary supplements prior to their bronchoscopy. The median age was 71.0 years old (range 23–91), 206 patients had malignant disease (69.6%), and 70 patients (23.6%) received antithrombotic agents. Fifty-one patients (17.2%) were regular users of dietary supplements without a bleeding risk, and 18 patients (6.1%) were regular users of dietary supplements with a bleeding risk (Table 1). Forty-two patients (60.9%) were regular users of one type of dietary supplement, and 27 patients (39.1%) were regular users of multiple types (Figure 2).
3.2. Bronchoscopy Procedures
A total of 351 bronchoscopies were divided into six groups based on the medication status and dietary supplement usage of the patients (Table 2). Transbronchial lung biopsy, transbronchial biopsy, transbronchial needle aspiration, endobronchial biopsy, bronchial scraping, tumor removal, and photodynamic therapy were considered invasive bronchoscopies. Among the 281 invasive bronchoscopies, 19 were regular users of dietary supplements with a bleeding risk. The ingredients in the dietary supplements associated with bleeding risk were garlic in 13 cases (68.4%), fish oil in five cases (26.3%), and turmeric in one case (5.3%) (Table 3). In the invasive bronchoscopies, there were nine cases in which the patient was a regular user of chondroitin-glucosamine, but none of them were treated with warfarin; therefore, they were not included in the list of dietary supplements with bleeding risk. All patients who regularly used antithrombotic agents were withdrawn from the antithrombotic agents for a sufficient period before invasive bronchoscopy.
3.3. Duration of Withdrawal of Supplements with Bleeding Risk
Dietary supplements with bleeding risk that were used by patients regularly before invasive bronchoscopy included garlic, fish oil, and turmeric. We examined the withdrawal period for these dietary supplements. The median durations of garlic and fish oil withdrawal before invasive bronchoscopy were 16.5 and 13 days, respectively (range: 4–31 and 7–30 days, respectively) (Table 4). In one patient taking garlic, the duration of withdrawal was unknown, but it had been suspended for at least 13 days. Almost all patients had not consumed their supplements for >7 days (Figure 3A). One patient underwent bronchoscopy after only a 4-day withdrawal of garlic because rapid examination and treatment of lung cancer were required (Figure 3B). All patients who regularly used fish oil stopped it for at least 7 days prior to bronchoscopy (Figure 3C). In the case of a patient who was a regular user of turmeric, the patient did not know the name of the dietary supplement and was unable to identify it before bronchoscopy. Therefore, use of the dietary supplement containing turmeric could not be stopped before bronchoscopy.
3.4. Complications
We examined whether there was a difference in complications from invasive bronchoscopy among the six groups divided by medication status and dietary supplement usage. Regarding patient characteristics, there were significant differences in age and sex between the groups; however, no significant differences in disease type or bronchoscopy procedures were observed (Table 5). No serious bleeding was observed as a complication in any group. A total of 54 cases had moderate bleeding (19.2%), which tended to be more common in the group including “antithrombotic agents and dietary supplement with bleeding risk (28.6%)”; however, there was no significant difference in incidence among the six groups. No severe bleeding was observed in the patient who had been taking a dietary supplement containing turmeric ingredients or in the patient who stopped the dietary supplement containing garlic for 4 days before invasive bronchoscopy. No significant differences were found in other complications (Table 6). Binary logistic analysis was performed on factors such as sex, age, disease, bronchoscopic procedure, antithrombotic agent medication status, and dietary supplement usage to examine the factors that influence bleeding complications. Cramer’s measure of association was preliminarily calculated for these variables; however, no strong correlations were found among the factors. Binary logistic regression showed that only the bronchoscopic procedure was an independent factor affecting bleeding complications, while antithrombotic agents, dietary supplement medication status, and other factors did not (Table 7).
4. Discussion
Some dietary supplements can affect perioperative conditions and require a preoperative withdrawal period to avoid bleeding complications. Invasive bronchoscopy could have complications; in particular, dietary supplements with a bleeding risk should be noted. In this study, the 19 patients who underwent invasive bronchoscopy were regular users of dietary supplements with a risk of bleeding, including garlic ingredients, fish oil, and turmeric.
Raw garlic has not been found to reduce platelet function when consumed as part of a regular diet. Still, some garlic powders and garlic extracts derived from garlic or processed garlic oil contain allicin, alliin, ajoene, methyl allyl trisulfide, diaryl trisulfide, dimethyl trisulfide, vinyl disulfide, and non-sulfur steroid saponins, which all have anticoagulant effects [20]. Because of the many case reports of surgical bleeding associated with garlic ingredients and RCTs in which garlic has been shown to reduce platelet function, garlic ingredients seem to have a bleeding risk with strong evidential support [4,21]. Fish oil contains high doses of the polyunsaturated omega-3 fatty acids eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) and is commonly used to reduce cardiovascular events. In a large RCT, a group of patients with hypercholesterolemia who regularly used EPA had significantly fewer coronary events but more bleeding events than a group of patients who did not use EPA. Therefore, withdrawal of fish oil is recommended before surgery or invasive procedures [5,22,23,24,25]. Conversely, a recent systematic review concluded that fish oil has antiplatelet effects in several RCTs but does not increase bleeding events [26]. However, no RCTs have reported the bleeding risk related to fish oil use in bronchoscopy. Considering the risk of respiratory deterioration and asphyxiation due to massive bleeding during bronchoscopy, withdrawal of fish oil before bronchoscopy is strongly recommended.
In this study, we performed an invasive bronchoscopy in one patient who had taken a turmeric dietary supplement. The patient did not know the name of the supplement and could not identify it before the bronchoscopy, which was performed without suspending the supplement. It was later discovered during a medical interview with a pharmacist, when the patient was hospitalized for lung cancer surgery, that this dietary supplement contained various ingredients, including turmeric, maria thistle, and black pepper, which are suspected of having a bleeding risk [4]. Turmeric, often used as a spice and coloring agent, contains a bioactive substance called curcumin [27], reported to have properties such as antioxidant, hepatoprotective, cardioprotective, neuroprotective, anti-microbial, anti-tumor, and amelioration of dyslipidemia and ischemia–reperfusion disease [27,28]. Curcumin also inhibits platelet activity and aggregation [27]. Turmeric has not been studied regarding its risk before bronchoscopy, and it should be withdrawn before bronchoscopy. In this case, we observed no severe complications; however, clinicians should be aware of dietary supplements containing turmeric and of supplements with unknown ingredients.
Chondroitin-glucosamine has been shown to cause prolonged prothrombin time when combined with warfarin in two cases, and over 40 cases showed an interaction between glucosamine and warfarin, reported by various drug-monitoring agencies [4,29,30,31]. In this study, there were nine cases in which the patient was a regular user of chondroitin-glucosamine undergoing invasive bronchoscopy. However, none of these patients were administered warfarin; therefore, these nine cases were not included in the list of dietary supplements with bleeding risk. No severe bleeding was observed in patients administered chondroitin-glucosamine.
Recommendations from the ASA and a report by Hodges and Kam indicate that the withdrawal period for dietary supplements should be no less than 2 weeks [32]. Wong and Townley recommend a 7-day pause for garlic and ginseng, 2 weeks for echinacea and ginger, and 36 hours for ginkgo biloba before surgery [33]. However, because there are so many ingredients that are considered dietary supplements, it is difficult to verify each regarding the risk of perioperative complications such as bleeding and their duration of withdrawal. The duration of withdrawal has not been adequately studied and no reports have examined the duration of dietary supplement withdrawal before bronchoscopy. In this study, of the 19 patients who were regular users of dietary supplements with a risk of bleeding and who underwent invasive bronchoscopy, 18 discontinued dietary supplements before bronchoscopy. In one of these cases, the patient who regularly used a supplement with a garlic ingredient had only a 4-day withdrawal period before invasive bronchoscopy because of the urgent need to diagnose and treat lung cancer. The other 17 cases were performed with a withdrawal of at least 7 days, meeting the duration of withdrawal recommended for garlic components [33]. As for fish oil, at least 1 or 2 weeks of withdrawal is recommended [23,24,25]. The withdrawal period for fish oil in this study was at least 7 days in all patients.
Complications of bronchoscopy include minor bleeding (hemoptysis < 50 mL) in 0.19% and severe bleeding (hemoptysis > 50 mL) in 0.26% of cases [34]; in transbronchial biopsy, the incidence of moderate bleeding is 1.7% [5]. In a prospective cohort study, Herth et al. reported that transbronchial lung biopsies in patients taking aspirin showed moderate bleeding in 1.1% and severe bleeding in 0.9% of patients, but no significant difference was seen in incidence between a group of patients not taking aspirin and a group of patients taking aspirin [35]. In a prospective cohort study conducted by Ernst et al., transbronchial lung biopsies in patients who were continuing to take clopidogrel or clopidogrel plus aspirin resulted in 34% incidence of moderate bleeding and 27% incidence of severe bleeding with a significantly higher rate than that of control group [36]. A retrospective study reported that endobronchial ultrasound-guided transbronchial needle aspiration in patients taking clopidogrel and aspirin resulted in a drop in hemoglobin (> 2 g) or rehospitalization within 48 hours due to bleeding or anemia in 8.7% of patients [37]. Among the patients in this study who were regular users of dietary supplements and underwent invasive bronchoscopy, were taking antithrombotic medications but all had been off their medication for a sufficient period of time prior to bronchoscopy. There was no severe bleeding in any of the groups; however, 19.2% of the patients had moderate bleeding. The incidence of bleeding complications in this study was higher than that in previous reports on transbronchial lung biopsies and ultrasound-guided transbronchial needle aspiration in patients taking antiplatelet drugs [35,37]. However, this may be due to the small number of cases in this study, differences in patient backgrounds, and differences in the evaluation criteria for bleeding severity. The incidence of bleeding complications during bronchoscopy was not significantly different between the groups divided according to medication status and dietary supplement usage, suggesting that dietary supplements with bleeding risks, such as garlic and fish oil, have a similar risk of bleeding as patients who do not consume these dietary supplements when they are withdrawn for at least 7 days. However, the number of cases was small, and the inclusion of further cases is required.
We could not identify the ingredients of the dietary supplements in six cases. The reason for this inadequate information was the lack of knowledge from the patient or healthcare provider. The patient did not know the name of the dietary supplement, and the healthcare provider did not ask enough about it. While healthcare providers need to be aware that some dietary supplements pose a bleeding risk, patients also need to be aware that some dietary supplements contain ingredients that might induce bleeding complications. Additionally, some dietary supplements contain more than one type of ingredient or the ingredients are unclear because of inadequate labeling. Before invasive bronchoscopy, it is crucial to pay close attention in collaboration with pharmacists and to stop using dietary supplements when there is uncertainty about their ingredients.
The limitations of this study that should be considered are its single-center retrospective design and the small number of patients taking dietary supplements with bleeding risk. Therefore, case bias may have affected the results. Further studies with larger numbers of patients from multiple facilities are needed.
5. Conclusion
The duration of withdrawal of dietary supplements with bleeding risk before invasive bronchoscopy was 7 days or more in almost all patients. The incidence of complications such as bleeding during or after invasive bronchoscopy in patients taking dietary supplements with a bleeding risk was not significantly higher than that in other patients, suggesting that the withdrawal period was appropriate and adequate to not increase the risk of bleeding complications. Further case studies are required to confirm this hypothesis.
Author Contributions
Conceptualization, Naoki Kinoshita; Data curation, Naoki Kinoshita; Investigation, Naoki Kinoshita; Methodology, Naoki Kinoshita; Project administration, Akira Yamasaki; Resources, Kosuke Yamaguchi, Tomoya Harada, Tomohiro Sakamoto, Yoshihiro Funaki, Masaaki Yanai, Yasuhiko Teruya, Yuki Hirayama, Takafumi Nonaka, Hiroki Ishikawa, Genki Inui and Masahiro Kodani; Supervision, Akira Yamasaki; Writing – original draft, Naoki Kinoshita. All authors approved the manuscript for submission.
Funding
This research received no funding
Institutional Review Board Statement
This study was approved by the Ethical Review Board of the Faculty of Medicine at Tottori University. (Approval number: 22A041).
Informed Consent Statement
Because study was retrospective and non-interventional, we did not obtain patient consent forms. Instead, an opt-out method was used with the opportunity to refuse to participate.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available due to the storage of patient data is restricted in order to protect personal information but are available from the corresponding author on reasonable requests.
Acknowledgments
We thank the pharmacists at our hospital for their contributions to the medication status interviews and risk assessment of complications.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ASA | American Society of Anesthesiologists |
| RCT | Randomized control trial |
References
- Statistics Bureau of Japan. e-Stat: Portal Site of Official Statistics of Japan; Statistics Bureau of Japan. Available online: https://www.e-stat.go.jp/ (accessed on 2 December, 2024).
- Ang-Lee, M.K.; Moss, J.; Yuan, C.S. Herbal medicines and perioperative care. JAMA 2001, 286(2), 208–216. [CrossRef]
- American Society of Anesthesiologists. Herbal and dietary supplements and anesthesia, October 2020; American Society of Anesthesiologists. Available online: https://www.asahq.org/madeforthismoment/wp-content/uploads/2020/10/ASA_Supplements-Anesthesia_Updated-1.pdf (accessed on 3 December, 2024).
- Hatfield, J.; Saad, S.; Housewright, C. Dietary supplements and bleeding. Proc. (Bayl. Univ. Med. Cent.) 2022, 35(6), 802–807. [CrossRef]
- Du Rand, I.A.; Blaikley, J.; Booton, R.; Chaudhuri, N.; Gupta, V.; Khalid, S.; Mandal, S.; Martin, J.; Mills, J.; Navani, N.; Rahman, N.M.; Wrightson, J.M.; Munavvar, M.; British Thoracic Society Bronchoscopy Guideline Group. British Thoracic Society guideline for diagnostic flexible bronchoscopy in adults: accredited by NICE. Thorax 2013, 68 (Suppl. 1), i1–i44. [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet 2007, 370(9596), 1453–1457. [CrossRef]
- Javaid, M.; Kadhim, K.; Bawamia, B.; Cartlidge, T.; Farag, M.; Alkhalil, M. Bleeding risk in patients receiving Omega-3 polyunsaturated fatty acids: A systematic review and meta-analysis of randomized clinical trials. J. Am. Heart Assoc. 2024, 13(10), e032390. [CrossRef]
- Yokoyama, M.; Origasa, H.; Matsuzaki, M.; Matsuzawa, Y.; Saito, Y.; Ishikawa, Y.; Oikawa, S.; Sasaki, J.; Hishida, H.; Itakura, H.; Kita, T.; Kitabatake, A.; Nakaya, N.; Sakata, T.; Shimada, K.; Shirato, K.; Japan EPA lipid intervention study (JELIS) Investigators. Effects of eicosapentaenoic acid on major coronary events in hypercholesterolaemic patients (JELIS): a randomised open-label, blinded endpoint analysis. Lancet 2007, 369(9567), 1090–1098. [CrossRef]
- Tavazzi, L.; Maggioni, A.P.; Marchioli, R.; Barlera, S.; Franzosi, M.G.; Latini, R.; Lucci, D.; Nicolosi, G.L.; Porcu, M.; Tognoni, G.; Gissi-HF Investigators. Effect of n-3 polyunsaturated fatty acids in patients with chronic heart failure (the GISSI-HF trial): a randomised, double-blind, placebo-controlled trial. Lancet 2008, 372(9645), 1223–1230. [CrossRef]
- ORIGIN Trial Investigators; Bosch, J.; Gerstein, H.C.; Dagenais, G.R.; Díaz, R.; Dyal, L.; Jung, H.; Maggiono, A.P.; Probstfield, J.; Ramachandran, A.; Riddle, M.C.; Rydén, L.E.; Yusuf, S. n-3 fatty acids and cardiovascular outcomes in patients with dysglycemia. N. Engl. J. Med. 2012, 367(4), 309–318. [CrossRef]
- Writing Group for the AREDS2 Research Group; Bonds, D.E.; Harrington, M.; Worrall, B.B.; Bertoni, A.G.; Eaton, C.B.; Hsia, J.; Robinson, J.; Clemons, T.E.; Fine, L.J.; Chew, E.Y. Effect of long-chain omega-3 fatty acids and lutein + zeaxanthin supplements on cardiovascular outcomes: results of the Age-Related Eye Disease Study 2 (AREDS2) randomized clinical trial. JAMA Intern. Med. 2014, 174(5), 763–771. [CrossRef]
- ASCEND Study Collaborative Group; Bowman, L.; Mafham, M.; Wallendszus, K.; Stevens, W.; Buck, G.; Barton, J.; Murphy, K.; Aung, T.; Haynes, R.; Cox, J.; Murawska, A.; Young, A.; Lay, M.; Chen, F.; Sammons, E.; Waters, E.; Adler, A.; Bodansky, J.; Farmer, A.; McPherson, R.; Neil, A.; Simpson, D.; Peto, R.; Baigent, C.; Collins, R.; Parish, S.; Armitage, J. Effects of n-3 fatty acid Supplements in diabetes mellitus. N. Engl. J. Med. 2018, 379(16), 1540–1550. [CrossRef]
- Manson, J.E.; Cook, N.R.; Lee, I.M.; Christen, W.; Bassuk, S.S.; Mora, S.; Gibson, H.; Albert, C.M.; Gordon, D.; Copeland, T.; D’Agostino, D.; Friedenberg, G.; Ridge, C.; Bubes, V.; Giovannucci, E.L.; Willett, W.C.; Buring, J.E.; VITAL Research Group. Marine n-3 Fatty Acids and Prevention of cardiovascular Disease and Cancer. N. Engl. J. Med. 2019, 380(1), 23–32. [CrossRef]
- Bhatt, D.L.; Steg, P.G.; Miller, M.; Brinton, E.A.; Jacobson, T.A.; Ketchum, S.B.; Doyle, R.T.; Juliano, R.A.; Jiao, L.; Granowitz, C.; Tardif, J.C.; Ballantyne, C.M.; REDUCE-IT Investigators. Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia. N. Engl. J. Med. 2019, 380(1), 11–22. [CrossRef]
- Nicholls, S.J.; Lincoff, A.M.; Garcia, M.; Bash, D.; Ballantyne, C.M.; Barter, P.J.; Davidson, M.H.; Kastelein, J.J.P.; Koenig, W.; McGuire, D.K.; Mozaffarian, D.; Ridker, P.M.; Ray, K.K.; Katona, B.G.; Himmelmann, A.; Loss, L.E.; Rensfeldt, M.; Lundström, T.; Agrawal, R.; Menon, V.; Wolski, K.; Nissen, S.E. Effect of high-dose omega-3 fatty acids vs corn oil on major adverse cardiovascular events in patients at high cardiovascular risk: the STRENGTH randomized clinical trial. JAMA 2020, 324(22), 2268–2280. [CrossRef]
- Bischoff-Ferrari, H.A.; Vellas, B.; Rizzoli, R.; Kressig, R.W.; da Silva, J.A.P.; Blauth, M.; Felson, D.T.; McCloskey, E.V.; Watzl, B.; Hofbauer, L.C.; Felsenberg, D.; Willett, W.C.; Dawson-Hughes, B.; Manson, J.E.; Siebert, U.; Theiler, R.; Staehelin, H.B.; de Godoi Rezende Costa Molino, C.; Chocano-Bedoya, P.O.; Abderhalden, L.A.; Egli, A.; Kanis, J.A.; Orav, E.J.; DO-HEALTH Research Group. Effect of vitamin D supplementation, omega-3 fatty acid supplementation, or a strength-training exercise program on clinical outcomes in older adults: the DO-HEALTH randomized clinical trial. JAMA 2020, 324(18), 1855–1868. [CrossRef]
- Fung, F.Y.; Wong, W.H.; Ang, S.K.; Koh, H.L.; Kun, M.C.; Lee, L.H.; Li, X.; Ng, H.J.; Tan, C.W.; Zhao, Y.; Linn, Y.C. A randomized, double-blind, placebo- controlled study on the anti-haemostatic effects of Curcuma longa, Angelica sinensis and panax ginseng. Phytomedicine 2017, 32, 88–96. [CrossRef]
- Tuncel, A.; Ener, K.; Han, O.; Nalcacioglu, V.; Aydin, O.; Seckin, S.; Atan, A. Effects of short-term dutasteride and Serenoa repens on perioperative bleeding and microvessel density in patients undergoing transurethral resection of the prostate. Scand. J. Urol. Nephrol. 2009, 43(5), 377–382. [CrossRef]
- Pecoraro, S.; Annecchiarico, A.; Gambardella, M.C.; Sepe, G. [Efficacy of pretreatment with Serenoa repens on bleeding associated with transurethral resection of prostate]. Minerva Urol. Nefrol. 2004, 56(1), 73–78.
- Scharbert, G.; Kalb, M.L.; Duris, M.; Marschalek, C.; Kozek-Langenecker, S.A. Garlic at dietary doses does not impair platelet function. Anesth. Analg. 2007, 105(5), 1214–1218. [CrossRef]
- Steiner, M.; Li, W. Aged garlic extract, a modulator of cardiovascular risk factors: a dose-finding study on the effects of AGE on platelet functions. J. Nutr. 2001, 131(3s), 980S–984S. [CrossRef]
- Yokoyama, M.; Origasa, H.; Matsuzaki, M.; Matsuzawa, Y.; Saito, Y.; Ishikawa, Y.; Oikawa, S.; Sasaki, J.; Hishida, H.; Itakura, H.; Kita, T.; Kitabatake, A.; Nakaya, N.; Sakata, T.; Shimada, K.; Shirato, K.; Japan EPA lipid intervention study (JELIS) Investigators. Effects of eicosapentaenoic acid on major coronary events in hypercholesterolaemic patients (JELIS): a randomised open-label, blinded endpoint analysis. Lancet 2007, 369(9567), 1090–1098. [CrossRef]
- Akintoye, E.; Sethi, P.; Harris, W.S.; Thompson, P.A.; Marchioli, R.; Tavazzi, L.; Latini, R.; Pretorius, M.; Brown, N.J.; Libby, P.; Mozaffarian, D. Fish oil and perioperative bleeding. Circ. Cardiovasc. Qual. Outcomes 2018, 11(11), e004584. [CrossRef]
- Rowe, D.J.; Baker, A.C. Perioperative risks and benefits of herbal supplements in aesthetic surgery. Aesthetic Surg. J.; Baker: AC, Brazil 2009, 29(2), 150–157. [CrossRef]
- Health Sciences Institute. These excellent supplements need to be sidelined before surgery, 7 October, 2013; Health Sciences Institute. Available online: https://hsionline.com/2013/10/07/the-most-dangerous-supplements/ (accessed on 3 December, 2024).
- Begtrup, K.M.; Krag, A.E.; Hvas, A.M. No impact of fish oil supplements on bleeding risk: a systematic review. Dan. Med. J. 2017, 64(5), A5366.
- Hussain, Y.; Abdullah; Khan, F.; Alsharif, K.F.; Alzahrani, K.J.; Saso, L.; Khan, H. Regulatory effects of curcumin on platelets: an update and future directions. Biomedicines 2022, 10(12), 3180. [CrossRef]
- Salehi, B.; Stojanović-Radić, Z.; Matejić, J.; Sharifi-Rad, M.; Anil Kumar, N.V.; Martins, N.; Sharifi-Rad, J. The therapeutic potential of curcumin: a review of clinical trials. Eur. J. Med. Chem. 2019, 163, 527–545. [CrossRef]
- Knudsen, J.F.; Sokol, G.H. Potential glucosamine-warfarin interaction resulting in increased international normalized ratio: case report and review of the literature and MedWatch database. Pharmacotherapy 2008, 28(4), 540–548. [CrossRef]
- Rozenfeld, V.; Crain, J.L.; Callahan, A.K. Possible augmentation of warfarin effect by glucosamine-chondroitin. Am. J. Health Syst. Pharm. 2004, 61(3), 306–307. [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Statement on the safety of glucosamine for patients receiving coumarin anticoagulants. E.F.S.A. J. 2011, 9(12). [CrossRef]
- Hodges, P.J.; Kam, P.C. The peri-operative implications of herbal medicines. Anaesthesia 2002, 57(9), 889–899. [CrossRef]
- Wong, A.; Townley, S.A. Herbal medicines and anaesthesia. Contin. Educ. Anaesth. Crit. Care Pain 2011, 11(1), 14–17. [CrossRef]
- Facciolongo, N.; Patelli, M.; Gasparini, S.; Lazzari Agli, L.; Salio, M.; Simonassi, C.; Del Prato, B.; Zanoni, P. Incidence of complications in bronchoscopy. Multicentre prospective study of 20,986 bronchoscopies. Monaldi Arch. Chest Dis. 2009, 71(1), 8–14. [CrossRef]
- Herth, F.J.F.; Becker, H.D.; Ernst, A. Aspirin does not increase bleeding complications after transbronchial biopsy. Chest 2002, 122(4), 1461–1464. [CrossRef]
- Ernst, A.; Eberhardt, R.; Wahidi, M.; Becker, H.D.; Herth, F.J.F. Effect of routine clopidogrel use on bleeding complications after transbronchial biopsy in humans. Chest 2006, 129(3), 734–737. [CrossRef]
- Swiatek K, Guthrie, R.; Elliott, J.O.; Jordan, K. Antiplatelet exposure and bleeding events in patients undergoing EBUS-TBNA. Int. J. Respir. Pulm. Med. 2017, 4(3).
Figure 1.
Flow diagram of the study methodology.
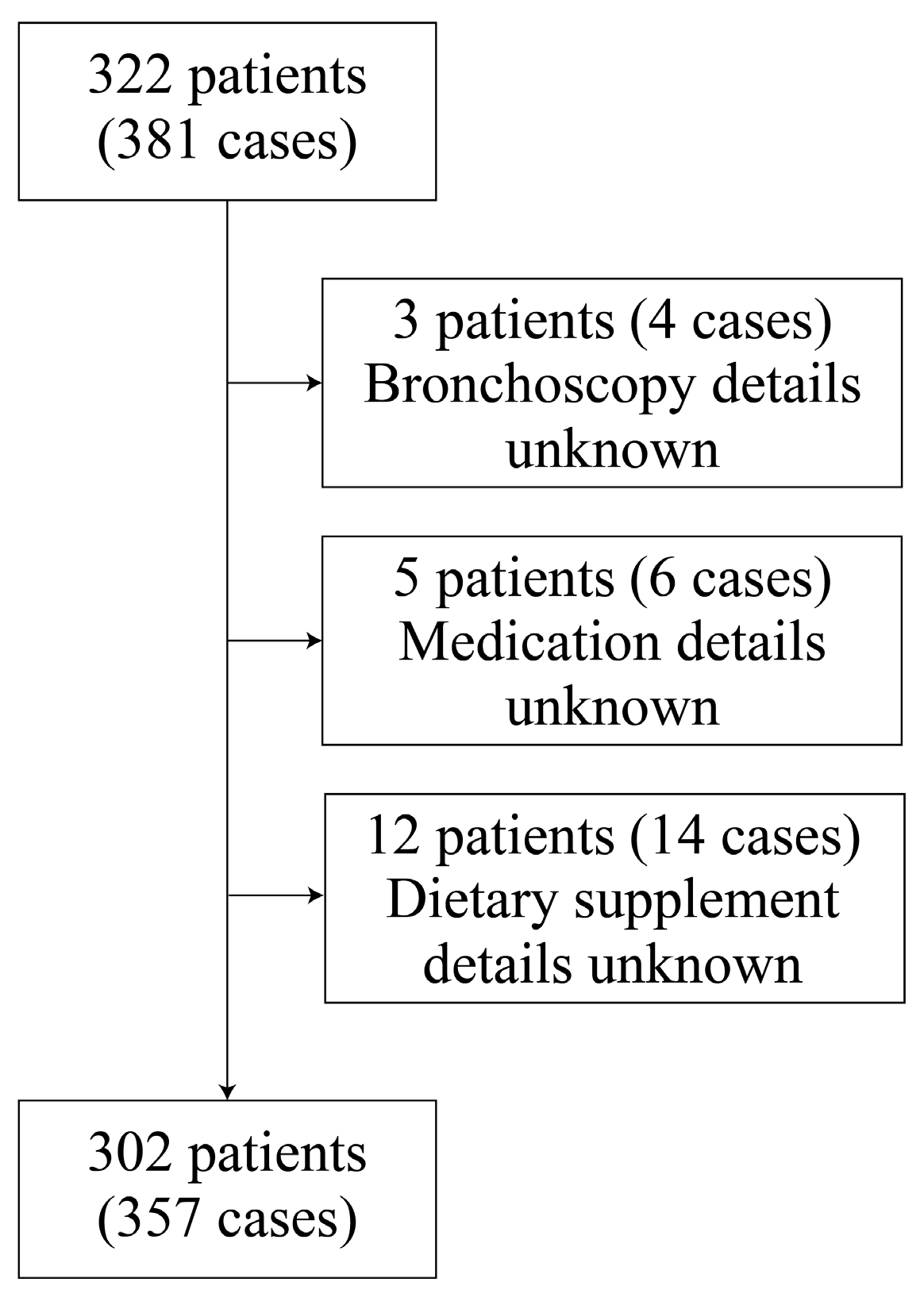
Figure 2.
Number of dietary supplements used by each patient.
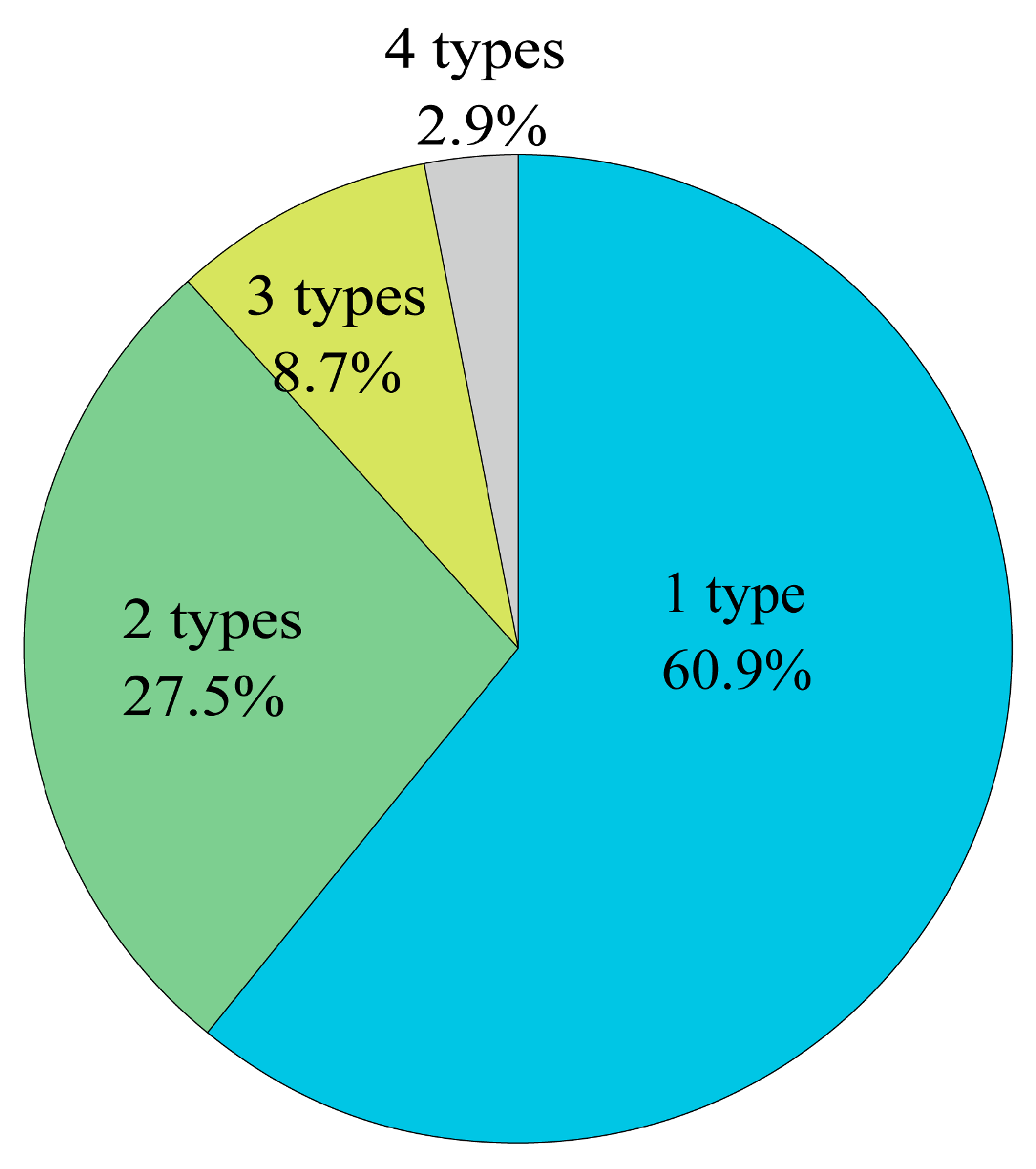
Figure 3.
Number of patients in each withdrawal period. A: Total ingredients. B: Garlic ingredients. C: Fish oil ingredients. Abbreviation: NW, no withdrawal.
Figure 3.
Number of patients in each withdrawal period. A: Total ingredients. B: Garlic ingredients. C: Fish oil ingredients. Abbreviation: NW, no withdrawal.
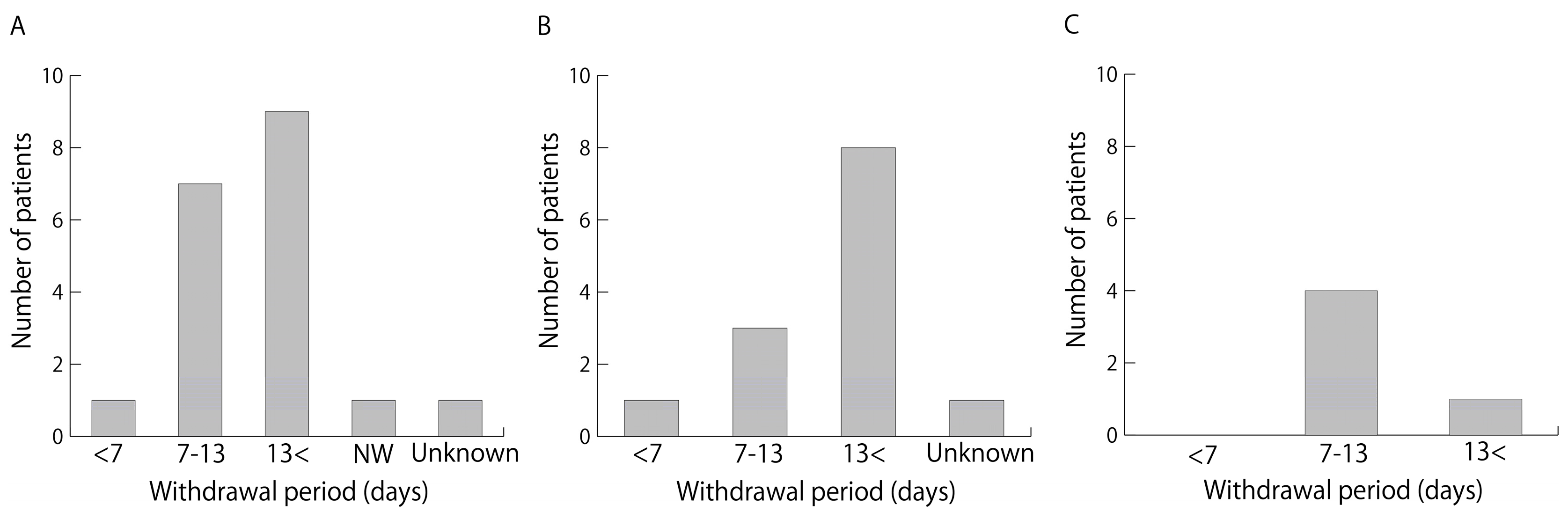

Table 1.
Patient characteristics.
| n = 296 | |
| Age | 71 (23–91) |
| Gender | |
| Male/Female | 191/105 |
| Disease | |
| Malignancy/Benign | 206/90 |
| Antithrombotic agent usage | 70 (23.6) |
| Dietary supplement usage | 69 (23.3) |
| Without bleeding risk | 51 (17.2) |
| With bleeding risk | 18 (6.1) |
| Number of dietary supplement usage each patient | 1 (1–4) |
Data are presented as median(range) or number(%).
Table 2.
Bronchoscopy procedures.
| Total | DS with BR | DS without BR | ATA | ATA and DS with BR | ATA and DS without BR | No ATA and DS | ||||||||
| n = 351 | (%) | n = 13 | (%) | n = 42 | (%) | n = 66 | (%) | n = 8 | (%) | n = 13 | (%) | n = 209 | (%) | |
| Exploration of the bronchus | 31 | (8.7) | 0 | (0) | 1 | (2.4) | 11 | (16.7) | 0 | (0) | 0 | (0) | 19 | (9.1) |
| Bronchial lavage | 21 | (6.0) | 0 | (0) | 4 | (9.5) | 3 | (4.5) | 0 | (0) | 1 | (7.7) | 13 | (6.2) |
| BAL | 11 | (3.1) | 0 | (0) | 0 | (0) | 3 | (4.5) | 1 | (12.5) | 0 | (0) | 7 | (3.3) |
| BAL+TBLB | 8 | (2.2) | 0 | (0) | 1 | (2.4) | 1 | (1.5) | 0 | (0) | 1 | (7.7) | 5 | (2.4) |
| EBUS-GS/UT-TBB | 170 | (48.4) | 10 | (76.9) | 26 | (61.9) | 26 | (39.4) | 5 | (62.5) | 8 | (61.5) | 95 | (45.5) |
| EBUS-TBNA | 68 | (19.4) | 2 | (15.4) | 6 | (14.3) | 16 | (24.2) | 0 | (0) | 2 | (15.4) | 42 | (20.1) |
| EBB | 23 | (6.4) | 0 | (0) | 3 | (7.1) | 3 | (4.5) | 1 | (12.5) | 0 | (0) | 16 | (7.7) |
| EBUS-GS-TBB+EBB | 2 | (0.6) | 0 | (0) | 0 | (0) | 0 | (0) | 1 | (12.5) | 1 | (7.7) | 0 | (0) |
| Mucus plug removal | 1 | (0.3) | 0 | (0) | 1 | (2.4) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) |
| Implantation of the gold marker | 3 | (0.8) | 1 | (7.7) | 0 | (0) | 1 | (1.5) | 0 | (0) | 0 | (0) | 1 | (0.5) |
| REBUS-TBNA | 1 | (0.3) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 1 | (0.5) |
| Bronchial scraping | 4 | (1.1) | 0 | (0) | 0 | (0) | 1 | (1.5) | 0 | (0) | 0 | (0) | 3 | (1.4) |
| BAL+TBLB+EBB | 1 | (0.3) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 1 | (0.5) |
| Implantation of the gold marker+EBB | 1 | (0.3) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 1 | (0.5) |
| Tumor removal | 1 | (0.3) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 1 | (0.5) |
| Foreign body removal | 1 | (0.3) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 1 | (0.5) |
| PDT | 1 | (0.3) | 0 | (0) | 0 | (0) | 1 | (1) | 0 | (0) | 0 | (0) | 0 | (0) |
| EBUS-TBNA+EBB | 1 | (0.3) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 1 | (0.5) |
| EWS | 2 | (0.6) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 2 | (1.0) |
Abbreviations: BAL, bronchoalveolar lavage, TBLB, transbronchial lung biopsy, EBUS, endobronchial ultrasound, GS, guide sheath, UT, ultrathin, TBB, transbronchial biopsy, TBNA, transbronchial needle aspiration, EBB, endobronchial biopsy, REBUS, radial probe endobronchial ultrasound, PDT, photodynamic therapy, EWS, endobronchial Watanabe spigot, DS, dietary supplements, BR, bleeding risk, ATA, antithrombotic agent. Shaded cells refer to invasive bronchoscopy.
Table 3.
Supplementation of ingredients is associated with bleeding during invasive bronchoscopy.
| n = 19 | (%) | |
| Garlic | 13 | (68.4) |
| Fish oil | 5 | (26.3) |
| Turmeric | 1 | (5.3) |
Table 4.
Withdrawal period of dietary supplements.
| Median (days) | [range] | |
| Garlic | 16.5 | 4–31 |
| Fish oil | 13 | 7–30 |
| Turmeric | No withdrawal |
Table 5.
Characteristics of patients who underwent invasive bronchoscopy.
| Total | DS with BR | DS without BR | ATA | ATA and DS with BR | ATA and DS without BR | No ATA and DS | |||||||||
| n = 281 | (%) | n = 12 | (%) | n = 36 | (%) | n = 48 | (%) | n = 7 | (%) | n = 12 | (%) | n = 166 | (%) | p | |
| Age <75 years/≥75 years | 187/94 | 9/3 | 28/8 | 23/25 | 2/5 | 5/7 | 120/46 | 0.001 | |||||||
| Sex, Male/Female | 180/101 | 10/2 | 18/18 | 40/8 | 6/1 | 8/4 | 98/68 | 0.007 | |||||||
| Disease, Malignancy/Benign | 223/58 | 8/4 | 29/7 | 40/8 | 7/0 | 9/3 | 130/36 | 0.587 | |||||||
| Bronchoscopy procedure | 0.600 | ||||||||||||||
| BAL+TBLB | 8 | (2.8) | 0 | (0) | 1 | (2.8) | 1 | (2.1) | 0 | (0) | 1 | (8.3) | 5 | (3.0) | |
| EBUS-GS-TBB、EBUS-UT-TBB | 170 | (60.5) | 10 | (83.3) | 26 | (72.2) | 26 | (54.2) | 5 | (71.4) | 8 | (66.7) | 95 | (57.2) | |
| EBUS-TBNA | 68 | (24.2) | 2 | (16.7) | 6 | (16.7) | 16 | (33.3) | 0 | (0) | 2 | (16.7) | 42 | (25.3) | |
| EBB | 23 | (8.2) | 0 | (0) | 3 | (8.3) | 3 | (6.3) | 1 | (14.3) | 0 | (0) | 16 | (9.6) | |
| EBUS-GS-TBB+EBB | 2 | (0.7) | 0 | (0) | 0 | (0) | 0 | (0) | 1 | (14.3) | 1 | (8.3) | 0 | (0) | |
| REBUS-TBNA | 1 | (0.4) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 1 | (0.6) | |
| Bronchial scraping | 4 | (1.4) | 0 | (0) | 0 | (0) | 1 | (2.1) | 0 | (0) | 0 | (0) | 3 | (1.8) | |
| BAL+TBLB+EBB | 1 | (0.4) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 1 | (0.6) | |
| Implantation of the gold marker+EBB | 1 | (0.4) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 1 | (0.6) | |
| Tumor removal | 1 | (0.4) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 1 | (0.6) | |
| PDT | 1 | (0.4) | 0 | (0) | 0 | (0) | 1 | (2.1) | 0 | (0) | 0 | (0) | 0 | (0) | |
| EBUS-TBNA+EBB | 1 | (0.4) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 1 | (0.6) | |
Abbreviations: TBLB, transbronchial lung biopsy; EBUS, endobronchial ultrasound; GS, guide sheath; UT, ultrathin; TBB, transbronchial biopsy; TBNA, transbronchial needle aspiration; EBB, endobronchial biopsy; REBUS, radial probe endobronchial ultrasound; PDT, photodynamic therapy; DS, dietary supplements; BR, bleeding risk; ATA, antithrombotic agent.
Table 6.
Complications during and after invasive bronchoscopy.
| Total | DS with BR | DS without BR | ATA | ATA and DS with BR | ATA and DS without BR | No ATA and DS | |||||||||
| Adverse event | n = 281 | (%) | n = 12 | (%) | n = 36 | (%) | n = 48 | (%) | n = 7 | (%) | n = 12 | (%) | n = 166 | (%) | p |
| Bleeding | |||||||||||||||
| Severe bleeding | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | |
| Moderate bleeding | 54 | (19.2) | 1 | (8.3) | 4 | (11.1) | 7 | (14.6) | 2 | (28.6) | 3 | (25.0) | 37 | (22.3) | 0.445 |
| Elevation of blood pressure | 34 | (12.1) | 2 | (16.7) | 5 | (13.9) | 3 | (6.3) | 1 | (14.3) | 2 | (16.7) | 21 | (12.7) | 0.821 |
| Decrease of SpO2 (<85%) | 27 | (9.6) | 0 | (0) | 2 | (5.6) | 5 | (10.4) | 0 | (0) | 0 | (0) | 20 | (12.0) | 0.398 |
| Pneumonia, lung abscess | 4 | (1.4) | 1 | (8.3) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 3 | (1.8) | 0.332 |
| Pneumothorax | 7 | (2.5) | 1 | (8.3) | 0 | (0) | 1 | (2.1) | 1 | (14.3) | 0 | (0) | 4 | (2.4) | 0.224 |
| Tachycardia, arrhythmia | 3 | (1.1) | 0 | (0) | 0 | (0) | 1 | (2.1) | 0 | (0) | 1 | (8.3) | 1 | (0.6) | 0.193 |
| Decrease of blood pressure | 4 | (1.4) | 0 | (0) | 0 | (0) | 1 | (2.1) | 0 | (0) | 0 | (0) | 3 | (1.8) | 0.936 |
| Vomiting | 3 | (1.1) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 1 | (8.3) | 2 | (1.2) | 0.211 |
| Laryngeal edema | 7 | (2.5) | 0 | (0) | 0 | (0) | 1 | (2.1) | 0 | (0) | 1 | (8.3) | 5 | (3.0) | 0.652 |
| Fever | 2 | (0.7) | 0 | (0) | 1 | (2.8) | 1 | (2.1) | 0 | (0) | 0 | (0) | 0 | (0) | 0.433 |
Severe Bleeding: Placement of a bronchus blocker or catheter and application of fibrin sealant; resuscitation, blood transfusion, admission to the critical care unit, or death Moderate Bleeding: Intubation of the biopsied segment with the bronchoscope in the wedge position; the use of adrenaline or cold saline to stop bleeding; elevated blood pressure required the use of antihypertensive drugs. Abbreviations: DS, dietary supplement; BR, bleeding risk; ATA, antithrombotic agent
Table 7.
Binary logistic regression analysis of bleeding complications.
| Factor | p |
| Age (<75 y.o./ ≥75 y.o.) | 0.708 |
| gender (Male/Female) | 0.052 |
| Disease (Malignancy/Benign) | 0.667 |
| Bronchoscopy procedure | 0.005 |
| Medication status and dietary supplement usage | 0.591 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



