
Submitted:
04 December 2024
Posted:
05 December 2024
You are already at the latest version
Abstract
Background: Due to its anatomy and function, the rotator cuff (RC) is vulnerable to considerable morbidity. The prevalence of RC diseases (RCD) in the general population is of 5–39%, and it increases with age, reaching over 30% in patients over 60 years old. The aim of the present systematic review is to investigate the effects of collagen injections use for the treatment of RCD.
Methods: A systematic search of scientific electronic databases was performed up to October 2023, following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Two independent authors performed the search and evaluated the articles. The inter-rater reliability in the quality assessment was evaluated using the Cohen’s kappa coefficient; while the Modified Coleman Methodology Score (CMS) was used to evaluate the methodological quality of the articles included in this systematic review.
Results: A total of seven articles were included with the overall quality of the included articles being evaluated as fair. Despite the use of different types of collagen and injections protocols, and different scores applied, each of the included study showed clinically relevant improvements. However, given the high grade of heterogeneity of the included studies, we cannot draw conclusions regarding which type of collagen and injection protocol is the best for the RCD treatment.
Discussion: Collagen administration for RCD seem to be effective in reducing pain, improving function, as well as improving tendon structure, especially in partial tears and RC tendinopathy. High-quality and prospective long-term follow-up studies are needed to confirm the outcomes of the articles included in this systematic review.
Keywords:
rotator cuff
; rotator cuff tendinopathy
; supraspinatus tendinopathy
; rotator cuff partial-thickness tear
; collagen
; collagen injections
1. Introduction
Rotator cuff (RC) consists in subscapularis, supraspinatus, infraspinatus tendons and teres minor muscle, and its function is of dynamically stabilizing the glenohumeral joint, avoiding the humeral head migration and contributing to initial phase of shoulder abduction, internal and external rotation[1]. Due to its anatomy and function, the RC is vulnerable to considerable morbidity [2], usually for a combination of both extrinsic (such as anatomic variables like acromial morphologic characteristics, os acromialis, and acromial spurs that compress the RC by bony impingement or direct pressure from the surrounding soft tissue) and intrinsic factors (that arise from the tendon itself, such as tensile overload, aging, microvascular supply, traumatisms, or degeneration) [3].
RC diseases (RCD) rank third in the population prevalence among musculoskeletal pathologies after low back pain and knee pain. The prevalence of RCD is of 5–39% in the general population, and it increases with age, reaching over 30% in patients over 60 years old, with a great majority described as RC tendinopathy (RCTP), and partial- or full-thickness RC tears (PTRCTs or FTRCTs) [4,5,6,7].
PTRCTs can be divided into bursal, intra-tendinous and articular tears, and are more common and painful compared to FTRCTs, with a prevalence of 13% to 32% in the adult population [8,9,10]. Several studies demonstrated that the 80% of PTRCTs progress into FTRCTs despite conservative treatment [11].
Treatment of choice for RCD is still debated and relies on several factors, including tear degree and size, patient symptoms and needs, and functional loss [12,13].
The arthroscopic cuff repair is the most common and accepted surgical treatment with proven satisfactory results [14,15], but post-operative re-tears represent an impor tant complication with an incidence between 34.2% and 40% [16], seriously influencing the rehabilitation process and patients’ quality of life [17,18]. Given the risks related to surgery (such as reduced strength of RC tendons) and a significant risk of recurrence, conservative treatment is usually the first choice, especially in older adults [19,20], with different studies showing good results for the management of both PTRCTs and FTRCTs [4,21], with surgical option usually being considered when the conservative treatment has not effect within the first six–12 weeks [22,23].
Conservative options include pharmacotherapy (such as the use of non-steroidal anti-inflammatory drugs and analgesics), physiotherapy [24,25,26], therapeutic exercise [27,28,29], and injections using different drugs such as corticosteroids (CS), platelet-rich plasma (PRP), hyaluronic acid (HA), and collagen [30,31,32,33,34].
CS injections provide transient pain relief: anyway, their use does not modify the natural history of disease, with recent evidence showing a potential role in accelerating the degenerative tendon process [35].
PRP alleviate symptoms and slow tendon degeneration better than CS administration and prolotherapy [36,37,38,39,40], HA has anti-inflammatory and adhesion prevention activities [41] and play an important role in promoting cell differentiation and growth, improving type-I collagen expression in tendon-derived cells, and contributing to tendon and bone healing [42,43,44,45,46,47]. The use of injectable collagen into the tendon itself or in the subacromial bursa showed a positive effect reducing collagen degenerative process [48].
Several types of collagens (types I, II, III, and V) can be found in fibrous tissues such as tendons, ligaments, and skin. Type-I collagen, the major component of the tendon extracellular matrix (ECM), directly influence the structural and mechanical properties of tendons [21,49]. In the RC’s ECM, type-I collagen represents more than the 95% of the total amount of collagen, whereas the remaining 5% consists of collagen types III and V [50,51].
The most frequently used injectable collagen is atelocollagen, a soluble type-I collagen with good biocompatibility, minor immunogenicity, long half-life and high resistance to enzymatic degradation [52,53,54]. Several advantages have been reported with the use of highly purified atelocollagen in terms of collagen-cell interactions and few adverse effects [48]. Collagen injections induce regenerative pathways by stimulating tenocyte proliferation and migration, by the synthesis of endogenous collagen, and by the restoration of collagen fibers in damaged tendons [23,35,55,56]. The administration of collagen at the target site activates the integrin receptors in fibroblast cell membranes [57]; consequently, the growth factor cascade initiates the synthesis of endogenous collagen [58]. Finally, this pathway heals the damaged collagen fibers and leads to proper alignment [59,60,61].
In animal models, the administration of atelocollagen directly into the site of RC tear led to better tendon healing and remodelling stages based on immunohisto chemistry or histopathological analyses [48,62]; a possible explanation of this effect may be a facilitation to re-create tendon continuity in the injured site, decreasing peritendinous adhesions and improving muscle activity.
Collagen injections were also used, with good reported outcomes, for the treatment of large and massive RC tears with collagen patches implanted arthroscopically [48,63], as well as for the treatment of tennis elbow [64,65] and plantar fasciitis [58,66].
Evidence reported synergic effects of collagen and PRP, suggesting that PRP may positively affect the cell’s mitogenic activity, collagen production, and the collagen I/III ratio [67]. Furthermore, injections with combined drugs such as collagen and PRP or collagen and HA may promote regeneration of the na tive insertion site, prevent scar tissue formation and increase biomechanical strength [9,68,69,70]. The aim of the present study is to systematically review the use of collagen injections for the treatment of RCD in humans. We hypothesised that the use of collagen injections allows to achieve better clinical and functional results in patients with RCTP, PTRCTs and FTRCTs. To date, this is the first systematic review conducted using PRISMA guidelines regarding the use of collagen injections for RCD.
2. Materials and Methods
2.1. Study Design
The present systematic review and its procedures were organized and conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [71,72,73]. The PRISMA flow diagram can be retrieved in Figure 1, while the PRISMA checklist has been added as Supplementary Materials. The research protocol has been registered in the International Prospective Register of Systematic Reviews (PROSPERO), registration number CRD42023470461.
2.2. Eligibility Criteria
This review includes included randomized clinical trials (RCTs), prospective and case-series studies, with a minimum follow-up of one month. Comparative studies with other injections therapies such as PRP were also included.
Articles such as editorials, technical notes, letters to authors, narrative reviews, systematic review, case reports, animal or cadaveric studies that did not report clinical outcomes about the use of collagen for RCD were excluded.
2.3. Information Sources
Potential studies were identified by searching electronic databases, including Cochrane Central Register of Controlled Trials (CENTRAL), EMBASE, MEDLINE, PEDro, Web of Science, Scopus, PubMed, ad CINAHL. A systematic search of all databases was performed from their inception to November 2024, with no language limitations. Reference lists of relevant studies were also screened for additional possible studies.
2.4. Search Strategy
The strategy had two components including terms for collagen and RCD. Keywords for population were “Rotator cuff” [MeSH] OR rotator cuff disease*[all fields] OR rotator cuff tendinopathy*[all fields] OR rotator cuff tear*[all fields]; keywords for intervention were “collagen” [MeSH] OR “atelocollagen” [MeSH].
2.5. Types of Participants
This study included patients with diagnosis of RCD, defined as RCTP, PTRCTs and FTRCTs.
2.6. Types of Interventions
For inclusion, collagen had to be administered to at least one group in the RCTs. Studies in which the effects of collagen alone could not be evaluated (such as a mixture of collagen and another drug compared with collagen alone or another drug) would not be included.
2.7. Types of Comparison Controls
Comparison groups were classified into active and inactive controls according to the Cochrane handbook for systematic reviews of interventions [74]. Inactive control was defined as no injection or arthroscopic repair without collagen injection. Active control was defined as the use of different injection solutions such as PRP [70] or acellular dermal matrix allograft [75].
2.8. Outcomes Measures
The primary outcome was pain reduction measured by Numeric Analogue Scale (NAS, 0-10) or Visual analogue scale (VAS, 0-10). Secondary outcomes included the Constant score (CoS) and the American Shoulder and Elbow Surgeons Shoulder Score (ASES), where available. Other scores were evaluated on a case-by-case basis depending on the ones used in the included studies. The outcomes were evaluated at baseline and at final follow-up for each of the included studies.
2.9. Study Selection and Data Extraction
Two independent authors (R.A. and D.T.) performed the search and evaluated the articles. Experienced researchers in systematic reviews (E.S., B.C., F.S., R.P., C.R.,) solved cases of doubt. At the beginning, investigators read the articles’ abstracts, selected the relevant ones according to both inclusion and exclusion criteria, and then compared results with the other investigators. After two weeks, the same studies were read again to confirm the agreement. No disagreement was observed among the investigators.
One investigator (R.A.) extracted the data from the full-text articles to Excel spreadsheet structured tables to analyse each study in a descriptive fashion. Number of sample size, type of management and collagen used, time of follow-up, clinical and functional outcome before and after treatment, adverse events and complication were extracted from the retrieved articles and collected in Table 1. A second investigator (E.S.) independently double-checked the extraction of primary data from all the articles. Doubts and inconsistencies were grouped and solved. All the authors participated in the drafting of the text. All results that were compatible with each outcome domain in each study were sought. A p-value <0.05 was considered statistically significant. Results are presented in Table 1 for comparison of progression from baseline to the last follow-up. All results were reported at baseline and at the last follow-up, highlighting the significant differences. Level of evidence analysis was determined using the Oxford Centre for Evidence-Based Medicine Levels of Evidence [76].
2.10. Quality Assessment
The Modified Coleman Methodology Score (MCMS) was used to evaluate the quality of the articles included in this PRISMA systematic review [77]. MCMS was used to assess the quality of the articles found in the present study, assessing methodology with 10 criteria, with a total score between 0 and 100 (which indicates that the study largely avoids chance, various biases, and confounding factors). Final score was categorized as excellent (85-100 points), good (70-84 points), fair (55-69 points), and poor (<55 points).
MCMS’ criteria were modified to make them reproducible and relevant for the present systematic review. We changed, for example, the “description of surgical technique” criterion with “description of injection technique”. More details about the MCMS (such as the definition for each criterion along with the scoring system, etc) are reported in the Supplementary Materials[78]. Two authors (D.T. and R.A.) independently applied the MCMS, and a final score was reached by consensus. The MCMS is calculated using ten different criteria (study size, follow-up, number of procedures, type of study, diagnostic certainty, description of the injection technique, rehabilitation and compliance, outcome criteria, outcome assessment, and selection process), with a maximum total possible score of 100 [79]. Then, the agreement in the quality assessment between the two reviewers was evaluated using Cohen’s kappa coefficient.
3. Results
3.1. Eligible Studies
After the initial literature search, a total of 299 potentially relevant citations were identified. After removal of duplicate records, 83 articles were identified. Then, following a first check of titles and abstracts, 67 articles were not included, since they did not investigate outcomes in the use of collagen injections for RCD. Finally, after a further screening, other nine articles were excluded as not conform to inclusion criteria, and a total of seven articles were included in the present systematic review (Figure 1).
Among the nine excluded studies, two were case-report studies, so their outcomes could not be considered as reliable. One article was also excluded because combined collagen with HA, so the effects of the sole collagen could not be evaluated.
3.2. Quality of the Included Studies
The inter-rater (R.A. and D.T.) reliability in the quality assessment, evaluated using the Cohen’s K coefficient, was optimal (0.9). The raters were blinded to the other reviewer’s ratings.
The results of the MCSMS are reported in Table 2.
3.3. Characteristics of Included Studies
Detailed descriptions of the characteristics of the included studies are summarised in Table 1. Of the seven articles retrieved, four studies were retrospective [12,35,75,80], two were prospective studies [81,82], reporting results after a different number of collagen injections (from one to four), while a single study was a RCT [70].
Three studies evaluated the effects of collagen injections for PTRCTs [70,80,81], with one of these being a RCT in which patients were treated using collagen injections alone or combined with PRP or PRP alone [70]. One prospective studies [81] evaluated the use of collagen for PTRCTs at different concentration or no injection therapy, while a retrospective [80] study evaluated collagen injections alone.
Two retrospective studies reported the outcomes of patients managed with arthroscopic rotator cuff repair for FTRCTs and that received a single collagen injection [12], or a single acellular dermal matrix injection [75], or no injections after surgery.
Effects of collagen injections on RCTPs were investigated in one case-series and one prospective studies [35,82]: Buda et al.[82] divided patients on the basis of the simple shoulder test (SST), showing better outcomes in patients managed with two single injection, in approximately two weeks, with the worst SST at the first time.
3.4. Clinical Assessment
The initial assessment of patients was performed in all the included studies through an US or magnetic resonance imaging (MRI) assessment that confirmed the presence of PTRCTs, FTRCTs or RCTPs, and three studies also considered clinical signs and symptoms of RC pathology [35,70,81]. Only one study reported the use of specific tests for the clinical assessment of RCD such as Neer’s and Jobe’s tests [35].
3.5. Injection Technique
Four studies used an in-plane, ultrasound (US)-guided injection technique [35,70,80,81], while in the studies in which collagen injection followed the arthroscopic repair, it was delivered through an arthroscopic visualization [12,75].
3.6. Adverse Events
3.7. Rehabilitation
In one study, the rehabilitation protocol after the injection consisted in progressive stretching exercises and posterior capsular stretching, comfortable passive ROM, and strengthening exercises with resistance bands [81], while in another study, pain-free ROM, postural exercises, and scapular stabilisation exercise were allowed [70]. In the study in which collagen was injected after the arthroscopic repair [12], the shoulder was immobilized for six weeks using an abduction brace, with early passive ROM permitted within a tolerable range, and active assisted ROM exercises started after six weeks, while strengthening exercise were started after three months.
3.8. Primary and Secondary Outcomes Evaluation
Different outcomes were assessed, such as range of motion (ROM) [80,81], VAS, NAS, numeric rating scale (NRS) [12,70,80,81], ASES [80,81], the Korean Shoulder Score (KSS) [12,80], CoS and Constant-Murley (CM) scores [35,80], the Disabilities of the Arm, Shoulder, and Hand (DASH) and Quick- Disabilities of the Arm, Shoulder, and Hand (Q-DASH) scores [35,70], Simple Shoulder Test (SST) [80,82], and the EQ-5D-5L (descriptive part – Utility Index and EQ-VAS 0–100) questionnaire [70].
In three out of four study in which VAS or NRS were evaluated, the scores decreased at final follow-up when compared to baseline more than the threshold for minimal clinically important difference (MCID) [83], especially in the short-term [12,70]. Regarding other scores evaluated for shoulder function such as DASH, Q-DASH, ASES or CoS, in some studies [35,70,81] scores increased significantly from baseline to final follow-up more than the respective MCID [84,85,86].
3.9. Collagen Versus Active Controls
In the study by Godek et al.[70] in which collagen injections for PTRCTs were compared to collagen plus PRP and PRP alone injections, the comparison of NRS evolution between the groups revealed a reduction in pain intensity mostly in the first six weeks of follow-up (p< 0.001), but no significant statistical differences between groups were noticed (p =0.870). The comparison of Q-DASH results between the groups at each measurement point also showed a similar pattern of mean value reduction (p < 0.001) without significant statistical differences between groups (p =0.997). The comparison of EQ-5D-5L (regarding the VAS subscore) results between the groups at each measurement point demonstrated no statistically significant differences. The dynamics of changes six weeks after the last injection were similarly more intense (p< 0.001).
Despite no statistical differences were found between groups in primary outcomes, there was a trend towards improvement in the collagen plus PRP and PRP alone groups between 12 and 24 weeks. The following outcomes were also retrieved: rotator cuff discontinuity (n= 3, one case in each group) and rotator cuff regeneration (n= 22 in the collagen plus PRP group, n= 20 in the collagen group, and n= 23 in the PRP group). The Authors finally stated that a combined therapy of collagen and PRP in PTRCTs is not more effective than monotherapies in reducing pain and improving mobility, self-care, and usual activities.
In the study by Aldhafian et al.[75], patients with FTRCTs were treated by arthroscopic repair only or arthroscopic repair together with collagen or acellular dermal matrix allograft injection. Functional outcomes of the three groups, including VAS for pain, ASES score, KSS, and CS score, were improved in all three groups compared with the preoperative assessment at final follow-up, with the most consistent improvement at 12-month follow-up. However, there was no significant difference between the three groups.
4. Discussion
The aim of the present study was to systematically review the use of collagen injections for RCD, reporting their functional outcomes, alone or in combination with other management modalities. The outcomes of the included studies highlighted the paucity of evidence on the effectiveness and safety of collagen injections for RCD.
Despite the use of different types of collagen and injection protocols, and different scores applied, each study evaluated in this systematic review showed that the administration of collagen for the treatment of RCD is effective in reducing pain and improving function.
RCD are one of the most common disabling musculoskeletal disorders with high prevalence rate, and the appropriate treatment is still under debate [87,88,89]. Among conservative treatments, different injection therapies have been proposed in the last years for the treatment of RCD, but they have achieved controversial effectiveness according to the scientific literature [90]. Since very few injection therapies have proven effective for RCD [31,91], collagen injections may represent an effective therapeutic option.
All the evaluation tools scored differently among the included studies, with statistically significant improvements found in all the scores [35,70,75,81] or just in some of them [12,80].
US [35,70,80] and MRI [12,81] evaluations were also performed during the follow-up to assess RC repair integrity, showing a significant decrease of the tear size in three studies [35,70,81].
Four studies [35,70,81,82] showed both clinical and radiological improvements for PTRCTs and RCTP with the use of collagen, while non-significant changes were found only in one article [80] on PTRCTs. When patients treated with collagen injections were compared to non-treated patients, outcomes were significantly better [75,81]. These outcomes were also observed in two case-reports on the use of injectable collagen for PTRCTs [23,57] in which a complete healing of the tendon tear at the last follow-up, along with improvements in shoulder pain and function, were reported. Therefore, the use of collagen injections for PTRCTs and RCTPs appears to be reasonable, especially for patients with worse starting baseline [82], even if the quality of the studies is relatively low, so several questions still need to be addressed.
Kim et al. [12] compared patients treated with a single collagen injection after RC arthroscopic repair for FTRCTs to patients who underwent only arthroscopic repair, and although patients treated with collagen resulted in reduced pain two weeks after surgery, no significant difference in the healing rate of the RC tear at six months postoperatively was found. Surprisingly, a 11.5% re-tear rate in the group treated with collagen versus a 6.7% in the non-collagen group was found, even if the difference was statistically not significant.
These outcomes disagree with those found by Jeong al. [9] who compared patients managed, after RC arthroscopic repair for FTRCTs, with combined collagen and HA to patients treated with HA alone or with no injections, reporting no difference in terms of clinical outcomes at 1-year follow-up, but an higher rate of RC tears in the groups treated with HA alone and with no injections, while no re-tears were found in the group treated with combined collagen and HA. Therefore, the authors stated that the co-administration of collagen and HA effectively improved healing of the RC and increased the integrity of the RC repair site. In the same study, at the 3-month follow-up, the authors performed in tra-articular CS injection to patients with shoulder pain and ROM limitation and, interestingly, they administered a significantly lower number of CS injections in the group treated with combined collagen and HA. This finding could be of some importance since recently growing evidence indicated that CS can have tenotoxic effects, increasing the risk of tendon rupture, increasing tenocytes necrosis, and decreased cell viability [92,93,94].
Despite the good outcomes reported in the included studies in this review, the use of collagen for RCD remains questionable, since some studies reported conflicting results. For this reason, other types of injections, such as PRP, may be preferred according to two recent systematic review about the efficacy of injections for RC tears [31,91]: anyway, in one of the included studies [70], patients were treated with either combined collagen and PRP or collagen alone or PRP alone for PTRCTs, and no statistical differences were found between groups in primary outcomes, with combined therapy of collagen and PRP presenting similar effectiveness to monotherapies with collagen or PRP.
Study limitations
The present review is not free from limitations. First, the quality of the included studies is relatively low, with only one level-I study [70], one level-III [81] and five level-IV studies [12,35,75,80,82], preventing definitive recommendations regarding the indication for the use of collagen for RCD. Furthermore, there was a great heterogeneity about the type of collagen used and the number of injections performed, and even when the same type of collagen was administered, the injection protocol was different [35,70,82]. Even in the studies in which the same specific RC issue was addressed [70,80,81], the type of collagen used was different. For this reason, we cannot draw any conclusions about which collagen and injection protocol is the best choose for the conservative treatment of RCD.
Finally, the heterogeneity of the study population with the absence of a control group in many investigations is an important limitation.
5. Conclusions
Despite a relatively low number of studies and low quality of the evidence, collagen administration for conservative treatment of RCD showed a positive trend in reducing pain and improving function during follow-ups, as well as improving tendon structure, with the most satisfactory results seen in PTRCTs and RCTP when patients at baseline experienced worse shoulder symptomatology.
In each study, all the evaluated scores, or at least some of them, improved significantly with good, reported outcomes, but given the low level of evidence, recommendations regarding the correct indication for the use of collagen in case of RCD cannot be defined. High quality studies with long-term follow-ups, such as RCTs, are needed to confirm the outcomes of the included articles.
Supplementary Materials
The following supporting information can be downloaded at: www.mdpi.com/xxx/s1, Table S1: PRISMA checklist; Table S2: The Modified Coleman Methodology Score.
Author Contributions
Conceptualization, D.T. and R.A.; writing—original draft preparation, D.T., R.A., R.M., D.D., R.T., L.R.; writing—review and editing, D.T., R.A., E.S., R.M., B.C., F.S., D.D., R.T., R.P.; supervision, D.T., R.A., E.S., B.C., F.S., R.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
Data are available on request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Dugas, J.R.; Campbell, D.A.; Warren, R.F.; Robie, B.H.; Millett, P.J. Anatomy and Dimensions of Rotator Cuff Insertions. J. Shoulder Elbow Surg. 2002, 11, 498–503. [Google Scholar] [CrossRef] [PubMed]
- Nho, S.J.; Yadav, H.; Shindle, M.K.; Macgillivray, J.D. Rotator Cuff Degeneration: Etiology and Pathogenesis. Am. J. Sports Med. 2008, 36, 987–993. [Google Scholar] [CrossRef] [PubMed]
- Maffulli, N.; Longo, U.G.; Berton, A.; Loppini, M.; Denaro, V. Biological Factors in the Pathogenesis of Rotator Cuff Tears. Sports Med. Arthrosc. Rev. 2011, 19, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Berton, A.; Papapietro, N.; Maffulli, N.; Denaro, V. Epidemiology, Genetics and Biological Factors of Rotator Cuff Tears. Med. Sport Sci. 2012, 57, 1–9. [Google Scholar] [CrossRef]
- Pellegrino, R.; Di Iorio, A.; Del Prete, C.M.; Barassi, G.; Paolucci, T.; Tognolo, L.; Fiore, P.; Santamato, A. Efficacy of Ultrasound-Guided Percutaneous Lavage and Biocompatible Electrical Neurostimulation, in Calcific Rotator Cuff Tendinopathy and Shoulder Pain, A Prospective Pilot Study. Int. J. Environ. Res. Public. Health 2022, 19, 5837. [Google Scholar] [CrossRef]
- Tuè, G.; Masuzzo, O.; Tucci, F.; Cavallo, M.; Parmeggiani, A.; Vita, F.; Patti, A.; Donati, D.; Marinelli, A.; Miceli, M.; et al. Can Secondary Adhesive Capsulitis Complicate Calcific Tendinitis of the Rotator Cuff? An Ultrasound Imaging Analysis. Clin. Pract. 2024, 14, 579–589. [Google Scholar] [CrossRef]
- Farì, G.; Megna, M.; Ranieri, M.; Agostini, F.; Ricci, V.; Bianchi, F.P.; Rizzo, L.; Farì, E.; Tognolo, L.; Bonavolontà, V.; et al. Could the Improvement of Supraspinatus Muscle Activity Speed up Shoulder Pain Rehabilitation Outcomes in Wheelchair Basketball Players? Int. J. Environ. Res. Public. Health 2022, 20, 255. [Google Scholar] [CrossRef]
- Fukuda, H. Partial-Thickness Rotator Cuff Tears: A Modern View on Codman’s Classic. J. Shoulder Elbow Surg. 2000, 9, 163–168. [Google Scholar] [CrossRef]
- Jeong, J.Y.; Khil, E.K.; Kim, T.S.; Kim, Y.W. Effect of Co-Administration of Atelocollagen and Hyaluronic Acid on Rotator Cuff Healing. Clin. Shoulder Elb. 2021, 24, 147–155. [Google Scholar] [CrossRef]
- Ricci, V.; Özçakar, L. The Dodo Bird Is Not Extinct: Ultrasound Imaging for Supraspinatus Tendinosis. Am. J. Phys. Med. Rehabil. 2019, 98, e8–e9. [Google Scholar] [CrossRef]
- Yamanaka, K.; Matsumoto, T. The Joint Side Tear of the Rotator Cuff. A Followup Study by Arthrography. Clin. Orthop. 1994, 68–73. [Google Scholar]
- Kim, I.B.; Kim, E.Y.; Lim, K.P.; Heo, K.S. Does the Use of Injectable Atelocollagen during Arthroscopic Rotator Cuff Repair Improve Clinical and Structural Outcomes? Clin. Shoulder Elb. 2019, 22, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Ricci, V.; Özçakar, L. Looking into the Joint When It Is Frozen: A Report on Dynamic Shoulder Ultrasound. J. Back Musculoskelet. Rehabil. 2019, 32, 663–665. [Google Scholar] [CrossRef] [PubMed]
- Jost, B.; Pfirrmann, C.W.; Gerber, C.; Switzerland, Z. Clinical Outcome after Structural Failure of Rotator Cuff Repairs. J. Bone Joint Surg. Am. 2000, 82, 304–314. [Google Scholar] [CrossRef]
- Ricci, V.; Chang, K.-V.; Güvener, O.; Mezian, K.; Kara, M.; Leblebicioğlu, G.; Stecco, C.; Pirri, C.; Ata, A.M.; Dughbaj, M.; et al. EURO-MUSCULUS/USPRM Dynamic Ultrasound Protocols for Shoulder. Am. J. Phys. Med. Rehabil. 2022, 101, e29–e36. [Google Scholar] [CrossRef]
- Sugaya, H.; Maeda, K.; Matsuki, K.; Moriishi, J. Repair Integrity and Functional Outcome after Arthroscopic Double-Row Rotator Cuff Repair. A Prospective Outcome Study. J. Bone Joint Surg. Am. 2007, 89, 953–960. [Google Scholar] [CrossRef]
- Oh, J.H.; Kim, S.H.; Ji, H.M.; Jo, K.H.; Bin, S.W.; Gong, H.S. Prognostic Factors Affecting Anatomic Outcome of Rotator Cuff Repair and Correlation with Functional Outcome. Arthrosc. J. Arthrosc. Relat. Surg. Off. Publ. Arthrosc. Assoc. N. Am. Int. Arthrosc. Assoc. 2009, 25, 30–39. [Google Scholar] [CrossRef]
- Ricci, V.; Mezian, K.; Chang, K.-V.; Özçakar, L. Clinical/Sonographic Assessment and Management of Calcific Tendinopathy of the Shoulder: A Narrative Review. Diagn. Basel Switz. 2022, 12, 3097. [Google Scholar] [CrossRef]
- Abtahi, A.M.; Granger, E.K.; Tashjian, R.Z. Factors Affecting Healing after Arthroscopic Rotator Cuff Repair. World J. Orthop. 2015, 6, 211–220. [Google Scholar] [CrossRef]
- Khazzam, M.; Sager, B.; Box, H.N.; Wallace, S.B. The Effect of Age on Risk of Retear after Rotator Cuff Repair: A Systematic Review and Meta-Analysis. JSES Int. 2020, 4, 625–631. [Google Scholar] [CrossRef]
- Thankam, F.G.; Dilisio, M.F.; Gross, R.M.; Agrawal, D.K. Collagen I: A Kingpin for Rotator Cuff Tendon Pathology. Am. J. Transl. Res. 2018, 10, 3291–3309. [Google Scholar] [PubMed]
- Ryösä, A.; Laimi, K.; Äärimaa, V.; Lehtimäki, K.; Kukkonen, J.; Saltychev, M. Surgery or Conservative Treatment for Rotator Cuff Tear: A Meta-Analysis. Disabil. Rehabil. 2017, 39, 1357–1363. [Google Scholar] [CrossRef] [PubMed]
- Corrado, B.; Bonini, I.; Alessio Chirico, V.; Rosano, N.; Gisonni, P. Use of Injectable Collagen in Partial-Thickness Tears of the Supraspinatus Tendon: A Case Report. Oxf. Med. Case Rep. 2020, 2020, omaa103. [Google Scholar] [CrossRef] [PubMed]
- Conaire, E.Ó.; Delaney, R.; Lädermann, A.; Schwank, A.; Struyf, F. Massive Irreparable Rotator Cuff Tears: Which Patients Will Benefit from Physiotherapy Exercise Programs? A Narrative Review. Int. J. Environ. Res. Public. Health 2023, 20, 5242. [Google Scholar] [CrossRef] [PubMed]
- Dominguez-Romero, J.G.; Jiménez-Rejano, J.J.; Ridao-Fernández, C.; Chamorro-Moriana, G. Exercise-Based Muscle Development Programmes and Their Effectiveness in the Functional Recovery of Rotator Cuff Tendinopathy: A Systematic Review. Diagn. Basel Switz. 2021, 11, 529. [Google Scholar] [CrossRef]
- Vita, F.; Pederiva, D.; Tedeschi, R.; Spinnato, P.; Origlio, F.; Faldini, C.; Miceli, M.; Stella, S.M.; Galletti, S.; Cavallo, M.; et al. Adhesive Capsulitis: The Importance of Early Diagnosis and Treatment. J. Ultrasound 2024, 27, 579–587. [Google Scholar] [CrossRef]
- Paraskevopoulos, E.; Plakoutsis, G.; Chronopoulos, E.; Maria, P. Effectiveness of Combined Program of Manual Therapy and Exercise Vs Exercise Only in Patients With Rotator Cuff-Related Shoulder Pain: A Systematic Review and Meta-Analysis. Sports Health 2023, 15, 727–735. [Google Scholar] [CrossRef]
- Ortega-Castillo, M.; Cuesta-Vargas, A.; Luque-Teba, A.; Trinidad-Fernández, M. The Role of Progressive, Therapeutic Exercise in the Management of Upper Limb Tendinopathies: A Systematic Review and Meta-Analysis. Musculoskelet. Sci. Pract. 2022, 62, 102645. [Google Scholar] [CrossRef]
- Farì, G.; Megna, M.; Fiore, P.; Ranieri, M.; Marvulli, R.; Bonavolontà, V.; Bianchi, F.P.; Puntillo, F.; Varrassi, G.; Reis, V.M. Real-Time Muscle Activity and Joint Range of Motion Monitor to Improve Shoulder Pain Rehabilitation in Wheelchair Basketball Players: A Non-Randomized Clinical Study. Clin. Pract. 2022, 12, 1092–1101. [Google Scholar] [CrossRef]
- DeClercq, M.G.; Fiorentino, A.M.; Lengel, H.A.; Ruzbarsky, J.J.; Robinson, S.K.; Oberlohr, V.T.; Whitney, K.E.; Millett, P.J.; Huard, J. Systematic Review of Platelet-Rich Plasma for Rotator Cuff Repair: Are We Adhering to the Minimum Information for Studies Evaluating Biologics in Orthopaedics? Orthop. J. Sports Med. 2021, 9, 23259671211041971. [Google Scholar] [CrossRef]
- Giovannetti de Sanctis, E.; Franceschetti, E.; De Dona, F.; Palumbo, A.; Paciotti, M.; Franceschi, F. The Efficacy of Injections for Partial Rotator Cuff Tears: A Systematic Review. J. Clin. Med. 2020, 10, 51. [Google Scholar] [CrossRef] [PubMed]
- Prodromos, C.C.; Finkle, S.; Prodromos, A.; Chen, J.L.; Schwartz, A.; Wathen, L. Treatment of Rotator Cuff Tears with Platelet Rich Plasma: A Prospective Study with 2 Year Follow-Up. BMC Musculoskelet. Disord. 2021, 22, 499. [Google Scholar] [CrossRef] [PubMed]
- Palermi, S.; Gnasso, R.; Belviso, I.; Iommazzo, I.; Vecchiato, M.; Marchini, A.; Corsini, A.; Vittadini, F.; Demeco, A.; De Luca, M.; et al. Stem Cell Therapy in Sports Medicine: Current Applications, Challenges and Future Perspectives. J. Basic Clin. Physiol. Pharmacol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Lalli, A.; Medina, G.; Maffulli, N. Conservative Management of Partial Thickness Rotator Cuff Tears: A Systematic Review. Sports Med. Arthrosc. Rev. 2023, 31, 80–87. [Google Scholar] [CrossRef]
- Corrado, B.; Bonini, I.; Chirico, V.; Filippini, E.; Liguori, L.; Magliulo, G.; Mazzuoccolo, G.; Rosano, N.; Gisonni, P. Ultrasound-Guided Collagen Injections in the Treatment of Supraspinatus Tendinopathy: A Case Series Pilot Study. J. Biol. Regul. Homeost. Agents 2020, 34, 33–39. [Google Scholar]
- Kim, S.J.; Yeo, S.M.; Noh, S.J.; Ha, C.-W.; Lee, B.C.; Lee, H.S.; Kim, S.J. Effect of Platelet-Rich Plasma on the Degenerative Rotator Cuff Tendinopathy According to the Compositions. J. Orthop. Surg. 2019, 14, 408. [Google Scholar] [CrossRef]
- Cross, J.A.; Cole, B.J.; Spatny, K.P.; Sundman, E.; Romeo, A.A.; Nicholson, G.P.; Wagner, B.; Fortier, L.A. Leukocyte-Reduced Platelet-Rich Plasma Normalizes Matrix Metabolism in Torn Human Rotator Cuff Tendons. Am. J. Sports Med. 2015, 43, 2898–2906. [Google Scholar] [CrossRef]
- Sari, A.; Eroglu, A. Comparison of Ultrasound-Guided Platelet-Rich Plasma, Prolotherapy, and Corticosteroid Injections in Rotator Cuff Lesions. J. Back Musculoskelet. Rehabil. 2020, 33, 387–396. [Google Scholar] [CrossRef]
- de Sire, A.; Lippi, L.; Mezian, K.; Calafiore, D.; Pellegrino, R.; Mascaro, G.; Cisari, C.; Invernizzi, M. Ultrasound-Guided Platelet-Rich-Plasma Injections for Reducing Sacroiliac Joint Pain: A Paradigmatic Case Report and Literature Review. J. Back Musculoskelet. Rehabil. 2022, 35, 977–982. [Google Scholar] [CrossRef]
- Vascellari, A.; Demeco, A.; Vittadini, F.; Gnasso, R.; Tarantino, D.; Belviso, I.; Corsini, A.; Frizziero, A.; Buttinoni, L.; Marchini, A.; et al. Orthobiologics Injection Therapies in the Treatment of Muscle and Tendon Disorders in Athletes: Fact or Fake? Muscles Ligaments Tendons J. 2024, 14, 239–246. [Google Scholar] [CrossRef]
- Mitsui, Y.; Gotoh, M.; Nakama, K.; Yamada, T.; Higuchi, F.; Nagata, K. Hyaluronic Acid Inhibits mRNA Expression of Proinflammatory Cytokines and Cyclooxygenase-2/Prostaglandin E(2) Production via CD44 in Interleukin-1-Stimulated Subacromial Synovial Fibroblasts from Patients with Rotator Cuff Disease. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2008, 26, 1032–1037. [Google Scholar] [CrossRef] [PubMed]
- Honda, H.; Gotoh, M.; Kanazawa, T.; Ohzono, H.; Nakamura, H.; Ohta, K.; Nakamura, K.; Fukuda, K.; Teramura, T.; Hashimoto, T.; et al. Hyaluronic Acid Accelerates Tendon-to-Bone Healing After Rotator Cuff Repair. Am. J. Sports Med. 2017, 45, 3322–3330. [Google Scholar] [CrossRef] [PubMed]
- Manferdini, C.; Guarino, V.; Zini, N.; Raucci, M.G.; Ferrari, A.; Grassi, F.; Gabusi, E.; Squarzoni, S.; Facchini, A.; Ambrosio, L.; et al. Mineralization Behavior with Mesenchymal Stromal Cells in a Biomimetic Hyaluronic Acid-Based Scaffold. Biomaterials 2010, 31, 3986–3996. [Google Scholar] [CrossRef] [PubMed]
- Osti, L.; Berardocco, M.; di Giacomo, V.; Di Bernardo, G.; Oliva, F.; Berardi, A.C. Hyaluronic Acid Increases Tendon Derived Cell Viability and Collagen Type I Expression in Vitro: Comparative Study of Four Different Hyaluronic Acid Preparations by Molecular Weight. BMC Musculoskelet. Disord. 2015, 16, 284. [Google Scholar] [CrossRef] [PubMed]
- Pellegrino, R.; Brindisino, F.; Barassi, G.; Sparvieri, E.; DI Iorio, A.; de Sire, A.; Ruosi, C. Combined Ultrasound Guided Peritendinous Hyaluronic Acid (500-730 Kda) Injection with Extracorporeal Shock Waves Therapy vs. Extracorporeal Shock Waves Therapy-Only in the Treatment of Shoulder Pain Due to Rotator Cuff Tendinopathy. A Randomized Clinical Trial. J. Sports Med. Phys. Fitness 2022, 62, 1211–1218. [Google Scholar] [CrossRef]
- Pellegrino, R.; Paolucci, T.; Brindisino, F.; Mondardini, P.; Di Iorio, A.; Moretti, A.; Iolascon, G. Effectiveness of High-Intensity Laser Therapy Plus Ultrasound-Guided Peritendinous Hyaluronic Acid Compared to Therapeutic Exercise for Patients with Lateral Elbow Tendinopathy. J. Clin. Med. 2022, 11, 5492. [Google Scholar] [CrossRef]
- Pellegrino, R.; Di Iorio, A.; Brindisino, F.; Paolucci, T.; Moretti, A.; Iolascon, G. Effectiveness of Combined Extracorporeal Shock-Wave Therapy and Hyaluronic Acid Injections for Patients with Shoulder Pain Due to Rotator Cuff Tendinopathy: A Person-Centered Approach with a Focus on Gender Differences to Treatment Response. BMC Musculoskelet. Disord. 2022, 23, 863. [Google Scholar] [CrossRef]
- Suh, D.-S.; Lee, J.-K.; Yoo, J.-C.; Woo, S.-H.; Kim, G.-R.; Kim, J.-W.; Choi, N.-Y.; Kim, Y.; Song, H.-S. Atelocollagen Enhances the Healing of Rotator Cuff Tendon in Rabbit Model. Am. J. Sports Med. 2017, 45, 2019–2027. [Google Scholar] [CrossRef]
- Aicale, R.; Tarantino, D.; Maffulli, N. Basic Science of Tendons. In Bio-orthopaedics: A New Approach; Gobbi, A., Espregueira-Mendes, J., Lane, J.G., Karahan, M., Eds.; Springer: Berlin, Heidelberg, 2017; pp. 249–273. ISBN 978-3-662-54181-4. [Google Scholar]
- Thankam, F.G.; Dilisio, M.F.; Agrawal, D.K. Immunobiological Factors Aggravating the Fatty Infiltration on Tendons and Muscles in Rotator Cuff Lesions. Mol. Cell. Biochem. 2016, 417, 17–33. [Google Scholar] [CrossRef]
- Thankam, F.G.; Evan, D.K.; Agrawal, D.K.; Dilisio, M.F. Collagen Type III Content of the Long Head of the Biceps Tendon as an Indicator of Glenohumeral Arthritis. Mol. Cell. Biochem. 2019, 454, 25–31. [Google Scholar] [CrossRef]
- Lynn, A.K.; Yannas, I.V.; Bonfield, W. Antigenicity and Immunogenicity of Collagen. J. Biomed. Mater. Res. B Appl. Biomater. 2004, 71, 343–354. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, I.; Mishra, D.; Das, T.; Maiti, S.; Maiti, T.K. Caprine (Goat) Collagen: A Potential Biomaterial for Skin Tissue Engineering. J. Biomater. Sci. Polym. Ed. 2012, 23, 355–373. [Google Scholar] [CrossRef] [PubMed]
- Tarantino, D.; Mottola, R.; Palermi, S.; Sirico, F.; Corrado, B.; Gnasso, R. Intra-Articular Collagen Injections for Osteoarthritis: A Narrative Review. Int. J. Environ. Res. Public. Health 2023, 20, 4390. [Google Scholar] [CrossRef] [PubMed]
- Randelli, F.; Menon, A.; Giai Via, A.; Mazzoleni, M.G.; Sciancalepore, F.; Brioschi, M.; Gagliano, N. Effect of a Collagen-Based Compound on Morpho-Functional Properties of Cultured Human Tenocytes. Cells 2018, 7, 246. [Google Scholar] [CrossRef]
- Martinello, T.; Bronzini, I.; Volpin, A.; Vindigni, V.; Maccatrozzo, L.; Caporale, G.; Bassetto, F.; Patruno, M. Successful Recellularization of Human Tendon Scaffolds Using Adipose-Derived Mesenchymal Stem Cells and Collagen Gel. J. Tissue Eng. Regen. Med. 2014, 8, 612–619. [Google Scholar] [CrossRef]
- Jo, Y.; Kim, W.-J.; Lee, H. Healing of Partial Tear of the Supraspinatus Tendon after Atelocollagen Injection Confirmed by MRI. Medicine (Baltimore) 2020, 99. [Google Scholar] [CrossRef]
- Corrado, B.; Bonini, I.; Tarantino, D.; Sirico, F. Ultrasound-Guided Collagen Injections for Treatment of Plantar Fasciopathy in Runners: A Pilot Study and Case Series. 2020. [CrossRef]
- Canty, E.G.; Kadler, K.E. Procollagen Trafficking, Processing and Fibrillogenesis. J. Cell Sci. 2005, 118, 1341–1353. [Google Scholar] [CrossRef]
- Hynes, R.O. Integrins: Bidirectional, Allosteric Signaling Machines. Cell 2002, 110, 673–687. [Google Scholar] [CrossRef]
- Massoud, E.I.E. Healing of Subcutaneous Tendons: Influence of the Mechanical Environment at the Suture Line on the Healing Process. World J. Orthop. 2013, 4, 229–240. [Google Scholar] [CrossRef]
- Im, G.-I.; Ahn, J.-H.; Kim, S.-Y.; Choi, B.-S.; Lee, S.-W. A Hyaluronate-Atelocollagen/Beta-Tricalcium Phosphate-Hydroxyapatite Biphasic Scaffold for the Repair of Osteochondral Defects: A Porcine Study. Tissue Eng. Part A 2010, 16, 1189–1200. [Google Scholar] [CrossRef]
- Thon, S.G.; O’Malley, L.; O’Brien, M.J.; Savoie, F.H. Evaluation of Healing Rates and Safety With a Bioinductive Collagen Patch for Large and Massive Rotator Cuff Tears: 2-Year Safety and Clinical Outcomes. Am. J. Sports Med. 2019, 47, 1901–1908. [Google Scholar] [CrossRef] [PubMed]
- Farkash, U.; Avisar, E.; Volk, I.; Slevin, O.; Shohat, N.; El Haj, M.; Dolev, E.; Ashraf, E.; Luria, S. First Clinical Experience with a New Injectable Recombinant Human Collagen Scaffold Combined with Autologous Platelet-Rich Plasma for the Treatment of Lateral Epicondylar Tendinopathy (Tennis Elbow). J. Shoulder Elbow Surg. 2019, 28, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Corrado, B.; Mazzuoccolo, G.; Liguori, L.; Chirico, V.A.; Costanzo, M.; Bonini, I.; Bove, G.; Curci, L. Treatment of Lateral Epicondylitis with Collagen Injections: A Pilot Study. Muscle Ligaments Tendons J. 2019, 09, 584. [Google Scholar] [CrossRef]
- Kim, M.; Choi, Y.S.; You, M.-W.; Kim, J.S.; Young, K.W. Sonoelastography in the Evaluation of Plantar Fasciitis Treatment: 3-Month Follow-Up After Collagen Injection. Ultrasound Q. 2016, 32, 327–332. [Google Scholar] [CrossRef]
- Baksh, N.; Hannon, C.P.; Murawski, C.D.; Smyth, N.A.; Kennedy, J.G. Platelet-Rich Plasma in Tendon Models: A Systematic Review of Basic Science Literature. Arthrosc. J. Arthrosc. Relat. Surg. Off. Publ. Arthrosc. Assoc. N. Am. Int. Arthrosc. Assoc. 2013, 29, 596–607. [Google Scholar] [CrossRef]
- Kovacevic, D.; Rodeo, S.A. Biological Augmentation of Rotator Cuff Tendon Repair. Clin. Orthop. 2008, 466, 622–633. [Google Scholar] [CrossRef]
- de Albornoz, P.M.; Aicale, R.; Forriol, F.; Maffulli, N. Cell Therapies in Tendon, Ligament, and Musculoskeletal System Repair. Sports Med. Arthrosc. Rev. 2018, 26, 48–58. [Google Scholar] [CrossRef]
- Godek, P.; Szczepanowska-Wolowiec, B.; Golicki, D. Collagen and Platelet-Rich Plasma in Partial-Thickness Rotator Cuff Injuries. Friends or Only Indifferent Neighbours? Randomised Controlled Trial. BMC Musculoskelet. Disord. 2022, 23, 1109. [Google Scholar] [CrossRef]
- Padulo, J.; Oliva, F.; Frizziero, A.; Maffulli, N. Basic Principles and Recommendations in Clinical and Field Science Research: 2018 Update. Muscle Ligaments Tendons J 2018, 8, 305–307. [Google Scholar] [CrossRef]
- Padulo, J.; De Giorgio, A.; Oliva, F.; Frizziero, A.; Maffulli, N. I Performed Experiments and I Have Results. Wow, and Now? Muscles Ligaments Tendons J. 2017, 7, 403. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. J. Clin. Epidemiol. 2009, 62, e1-34. [Google Scholar] [CrossRef] [PubMed]
- Cochrane Handbook for Systematic Reviews of Interventions. Available online: https://training.cochrane.org/handbook/current (accessed on 25 August 2023).
- Aldhafian, O.R.; Choi, K.-H.; Cho, H.-S.; Alarishi, F.; Kim, Y.-S. Outcome of Intraoperative Injection of Collagen in Arthroscopic Repair of Full-Thickness Rotator Cuff Tear: A Retrospective Cohort Study. J. Shoulder Elbow Surg. 2023, 32, e429–e436. [Google Scholar] [CrossRef] [PubMed]
- Durieux, N.; Vandenput, S.; Pasleau, F. [OCEBM levels of evidence system]. Rev. Med. Liege 2013, 68, 644–649. [Google Scholar] [PubMed]
- Coleman, B.D.; Khan, K.M.; Maffulli, N.; Cook, J.L.; Wark, J.D. Studies of Surgical Outcome after Patellar Tendinopathy: Clinical Significance of Methodological Deficiencies and Guidelines for Future Studies. Victorian Institute of Sport Tendon Study Group. Scand. J. Med. Sci. Sports 2000, 10, 2–11. [Google Scholar] [CrossRef]
- Mancino, F.; Di Matteo, V.; Mocini, F.; Cacciola, G.; Malerba, G.; Perisano, C.; De Martino, I. Survivorship and Clinical Outcomes of Proximal Femoral Replacement in Non-Neoplastic Primary and Revision Total Hip Arthroplasty: A Systematic Review. BMC Musculoskelet. Disord. 2021, 22, 933. [Google Scholar] [CrossRef]
- Coleman, B.D.; Khan, K.M.; Maffulli, N.; Cook, J.L.; Wark, J.D. Studies of Surgical Outcome after Patellar Tendinopathy: Clinical Significance of Methodological Deficiencies and Guidelines for Future Studies. Victorian Institute of Sport Tendon Study Group. Scand. J. Med. Sci. Sports 2000, 10, 2–11. [Google Scholar] [CrossRef]
- Chae, S.H.; Won, J.Y.; Yoo, J.C. Clinical Outcome of Ultrasound-Guided Atelocollagen Injection for Patients with Partial Rotator Cuff Tear in an Outpatient Clinic: A Preliminary Study. Clin. Shoulder Elb. 2020, 23, 80–85. [Google Scholar] [CrossRef]
- Kim, J.-H.; Kim, D.-J.; Lee, H.-J.; Kim, B.-K.; Kim, Y.-S. Atelocollagen Injection Improves Tendon Integrity in Partial-Thickness Rotator Cuff Tears: A Prospective Comparative Study. Orthop. J. Sports Med. 2020, 8, 2325967120904012. [Google Scholar] [CrossRef]
- Buda, M.; Dlimi, S.; Parisi, M.; Benoni, A.; Bisinella, G.; Di Fabio, S. Subacromial Injection of Hydrolyzed Collagen in the Symptomatic Treatment of Rotator Cuff Tendinopathy: An Observational Multicentric Prospective Study on 71 Patients. JSES Int. 2023, 7, 799–804. [Google Scholar] [CrossRef]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of Adult Pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011, 63 Suppl 11, S240–252. [Google Scholar] [CrossRef]
- Franchignoni, F.; Vercelli, S.; Giordano, A.; Sartorio, F.; Bravini, E.; Ferriero, G. Minimal Clinically Important Difference of the Disabilities of the Arm, Shoulder and Hand Outcome Measure (DASH) and Its Shortened Version (QuickDASH). J. Orthop. Sports Phys. Ther. 2014, 44, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Malavolta, E.A.; Yamamoto, G.J.; Bussius, D.T.; Assunção, J.H.; Andrade-Silva, F.B.; Gracitelli, M.E.C.; Ferreira Neto, A.A. Establishing Minimal Clinically Important Difference for the UCLA and ASES Scores after Rotator Cuff Repair. Orthop. Traumatol. Surg. Res. OTSR 2022, 108, 102894. [Google Scholar] [CrossRef] [PubMed]
- Louwerens, J.K.G.; van den Bekerom, M.P.J.; van Royen, B.J.; Eygendaal, D.; van Noort, A.; Sierevelt, I.N. Quantifying the Minimal and Substantial Clinical Benefit of the Constant-Murley Score and the Disabilities of the Arm, Shoulder and Hand Score in Patients with Calcific Tendinitis of the Rotator Cuff. JSES Int. 2020, 4, 606–611. [Google Scholar] [CrossRef] [PubMed]
- Urwin, M.; Symmons, D.; Allison, T.; Brammah, T.; Busby, H.; Roxby, M.; Simmons, A.; Williams, G. Estimating the Burden of Musculoskeletal Disorders in the Community: The Comparative Prevalence of Symptoms at Different Anatomical Sites, and the Relation to Social Deprivation. Ann. Rheum. Dis. 1998, 57, 649–655. [Google Scholar] [CrossRef]
- Roquelaure, Y.; Ha, C.; Leclerc, A.; Touranchet, A.; Sauteron, M.; Melchior, M.; Imbernon, E.; Goldberg, M. Epidemiologic Surveillance of Upper-Extremity Musculoskeletal Disorders in the Working Population. Arthritis Rheum. 2006, 55, 765–778. [Google Scholar] [CrossRef]
- Brindisino, F.; Garzonio, F.; DI Giacomo, G.; Pellegrino, R.; Olds, M.; Ristori, D. Depression, Fear of Re-Injury and Kinesiophobia Resulted in Worse Pain, Quality of Life, Function and Level of Return to Sport in Patients with Shoulder Instability: A Systematic Review. J. Sports Med. Phys. Fitness 2023, 63, 598–607. [Google Scholar] [CrossRef]
- Lin, M.-T.; Chiang, C.-F.; Wu, C.-H.; Huang, Y.-T.; Tu, Y.-K.; Wang, T.-G. Comparative Effectiveness of Injection Therapies in Rotator Cuff Tendinopathy: A Systematic Review, Pairwise and Network Meta-Analysis of Randomized Controlled Trials. Arch. Phys. Med. Rehabil. 2019, 100, 336–349.e15. [Google Scholar] [CrossRef]
- Jiang, X.; Zhang, H.; Wu, Q.; Chen, Y.; Jiang, T. Comparison of Three Common Shoulder Injections for Rotator Cuff Tears: A Systematic Review and Network Meta-Analysis. J. Orthop. Surg. 2023, 18, 272. [Google Scholar] [CrossRef]
- Nuelle, C.W.; Cook, C.R.; Stoker, A.M.; Cook, J.L.; Sherman, S.L. In Vivo Toxicity of Local Anesthetics and Corticosteroids on Supraspinatus Tenocyte Cell Viability and Metabolism. Iowa Orthop. J. 2018, 38, 107–112. [Google Scholar]
- Khoury, M.; Tabben, M.; Rolón, A.U.; Levi, L.; Chamari, K.; D’Hooghe, P. Promising Improvement of Chronic Lateral Elbow Tendinopathy by Using Adipose Derived Mesenchymal Stromal Cells: A Pilot Study. J. Exp. Orthop. 2021, 8, 6. [Google Scholar] [CrossRef]
- Zhang, A.Z.; Ficklscherer, A.; Gülecyüz, M.F.; Paulus, A.C.; Niethammer, T.R.; Jansson, V.; Müller, P.E. Cell Toxicity in Fibroblasts, Tenocytes, and Human Mesenchymal Stem Cells—A Comparison of Necrosis and Apoptosis-Inducing Ability in Ropivacaine, Bupivacaine, and Triamcinolone. Arthroscopy 2017, 33, 840–848. [Google Scholar] [CrossRef]
Figure 1.
Flowchart of included studies.
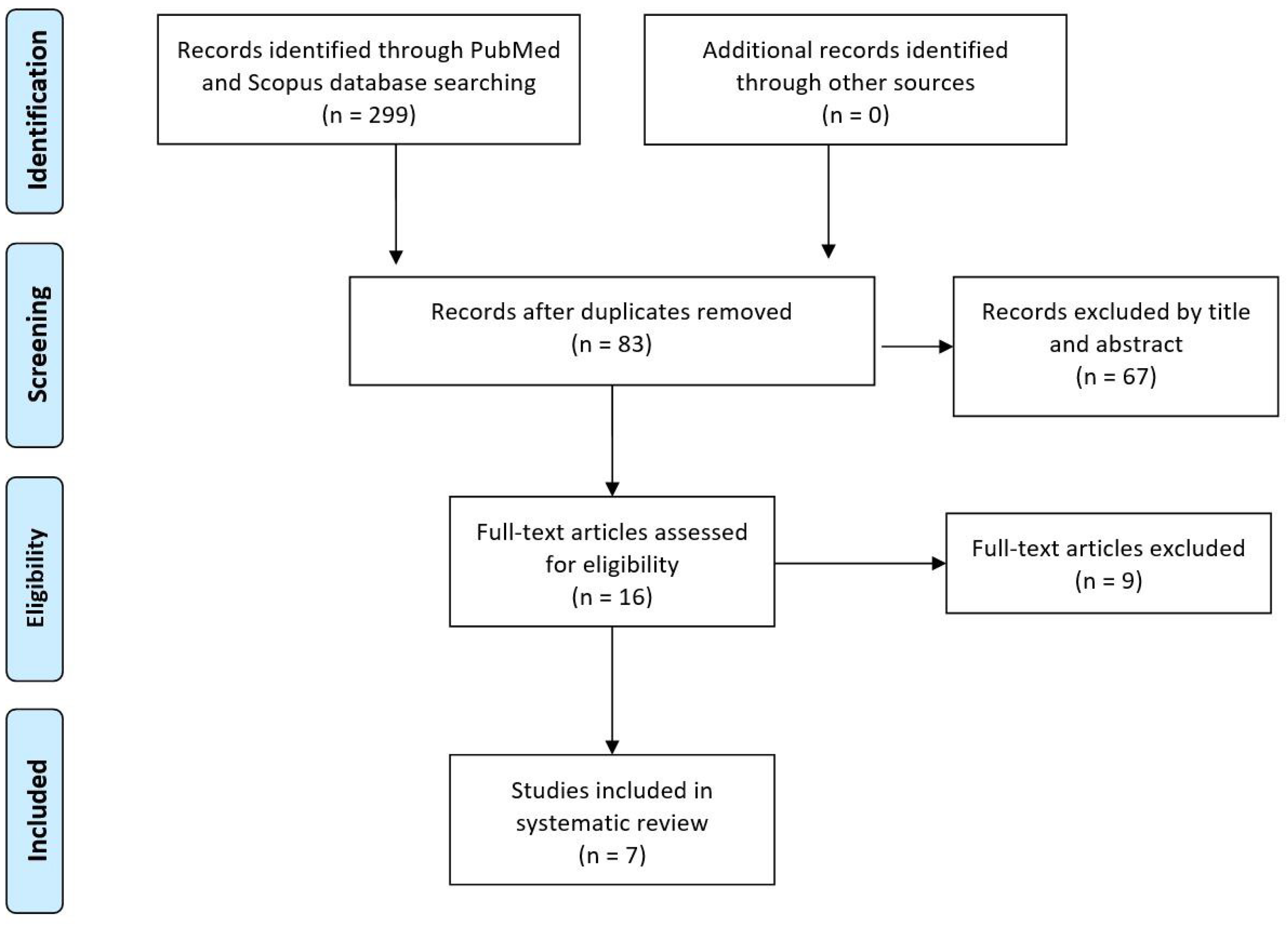

Table 1.
Main results and outcomes of each study.
| Study name | N. patient | Follow-ups | Groups | Collagen used | Intervention | Scores at baseline | Scores at last follow-up | Complications |
|---|---|---|---|---|---|---|---|---|
|
Kim et al. (2019) |
121 |
VAS: 3 days, 1 and 2 weeks KSS: 3, 12, 24 months |
Arthroscopic repair plus collagen injection (Group I, n=61) Arthroscopic repair alone (Group II, n=60). FTRCT |
3mL of 3% porcine type-I atelocollagen | Single injection at baseline (after arthroscopy) |
Group I VAS: 5.3 ± 2.1 KSS: 63.0 ± 15.1 Group II VAS: 6.3 ± 1.7 KSS: 61.5 ± 15.2 |
Group I VAS: 1.2 ± 1.0 KSS: 80.1 ± 9.4 Group II VAS: 3.2 ± 1.7 KSS:82.3 ± 11.2 |
Group I: 7 re-tears (11.5%) Group II: 4 re-tears (6.7%) |
|
Significant improvement in pre-op and last follow-up; VAS significantly better in Group I than Group II; No differences for KSS at final follow-up. |
||||||||
|
Kim et al. (2020) |
94 | 3, 12 and 24 months | 0.5 mL collagen injection (Group I, n=32) 1mL collagen injection (Group II, n=30) No injection (Group III, n=32) PTRCT |
0.5 or 1mL of 3%, porcine type-I atelocollagen | Single injection at baseline |
Group I VAS: 4.1 ASES: 61.9 CoS: 68.1 Group II VAS: 3.6 ASES: 63.5 CoS: 65.8 Group III VAS: 3.4 ASES: 62.9 CoS: 68.4 |
Group I VAS: 2.1 ± 1.2 ASES: 82.5 ± 12.3 CoS: 89.0 ± 6.9 Group II VAS: 1.4 ± 1.1 ASES: 79.3 ± 8.3 CoS: 82.0 ± 10.1 Group III VAS: 3.3 ± 2.5 ASES: 65.5 ± 8.5 CoS: 62.5 ± 11.5 |
Not reported |
|
Significant improvement pre-op and last follow-up only in Group I and II; Scores significantly better in Group I and II than III; No differences between Group I and II. |
||||||||
|
Chae et al. (2020) |
15 | 2 months | Collagen injection PTRCT |
1mL atelocollagen + 1mL of lidocaine | Single injection at baseline | ASES: 57.0 KSS: 64.6 CoS: 56.4 VAS: 4.2 SST: 6.6 FVAS: 6.3 |
ASES: 60.4 KSS: 68.5 CoS: 58.9 VAS: 3.7 SST: 6.9 FVAS: 7.1 |
Post-injection pain (57%, 8/15) |
| Significant improvement in pre-op and last follow-up only for SST and FVAS. | ||||||||
| Corrado et al. (2020) | 18 | 2 weeks, 1 and 3 months | Collagen injections RCTP |
2mL, porcine type-I atelocollagen | 4 injections (one a week for 4 weeks in a row) | CoS: 53.11 ± 12.7 DASH: 37.72 ± 19 |
CoS: 75 ± 12.9 DASH: 18.67 ± 13 |
Not reported |
| Statistically significant improvement. | ||||||||
|
Godek et al. (2022) |
82 | 6 weeks, 3 and 6 months | Collagen plus PRP injections (Group I, n=28) Collagen injections (Group II, n=27) PRP injections (Group III, n=27) PTRCT |
2mL, porcine type-I atelocollagen | 3 injections (one a week for 3 weeks in a row) |
Group I VAS: 74% QuickDASH: 37 NRS: 5 Group II VAS: 68% QuickDASH: 42 NRS: 5,5 Group III VAS: 71% QuickDASH: 41 NRS: 6 |
Group I VAS: 82% QuickDASH: 15 NRS: 1,5 Group II VAS: 80% QuickDASH: 20 NRS: 2 Group III VAS. 86% QuickDASH: 20 NRS: 1,8 |
No complications |
| No differences between groups at final follow-up. | ||||||||
| Aldhafian et al. (2023) | 129 | 3, 6 and 12 months for all groups Last follow-up (months): Group I: 21.6±5.1 Group II: 20±6.3 Group III: 18.3±3.2 |
Arthroscopic repair only (Group I, n=36) Arthroscopic repair plus collagen injection (Group II, n=44) Arthroscopic repair with acellular dermal matrix allograft injection (Group III, n=49) FTRCT |
1ml atelocollagen | Single injection at baseline (after arthroscopy) |
Group I VAS: 4 ASES: 58 CoS: 62 KSS: 61 Group II VAS: 4 ASES: 61 CoS: 68 KSS: 68 Group III VAS: 4 ASES: 62 CoS: 68 KSS: 68 |
Group I VAS: 2 ASES: 80 CoS: 76 KSS: 75 Group II VAS: 3 ASES: 74 CoS: 79 KSS: 81 Group III VAS: 3 ASES: 76 CoS: 73 KSS: 73 |
Re-tear rates after 12 months: Group I: 19.4% (7 of 36) Group II: 13.6% (6 of 44) Group III: 20.4% (10 of 49) Adverse events were not detected in any groups. |
|
Improved in all 3 groups compared to preoperative assessment at final follow-up. No significant difference among the 3 groups. |
||||||||
|
Buda et al. (2023) |
71 | 1 and 6 months | Collagen injections Group I (SST<42, n=23) Group II (43< SST<74, n=28) Group III (SST>75, n=20) RCTP |
4mg/2ml, bovine collagen, low molecular weight (<3kDa) | 2 injections (one at baseline and one between nine and 17 days after the first one) |
Overall population VAS at rest: 4.25 ± 3.10 VAS during movement: 6.56 ± 1.47 VAS at night: 5.33 ± 2.98 CoS: 63.76 ± 12.50 SST: 54.14 ± 20.16 Group I VAS at rest: 6.35 ± 2.29 VAS during movement: 7.26 ± 4.09 VAS at night: 6.56 ± 4.48 CoS: 51.52 ± 59.17 SST: 30.43 ± 40.58 Group II VAS at rest: 4.28 ± 2.07 VAS during movement: 6.57 ± 3.96 VAS at night: 5.03 ± 3.04 CoS: 65.32 ± 74.10 SST: 56.79 ± 72.58 Group III VAS at rest: 1.90 ± 0.95 VAS during movement: 5.85 ± 4.30 VAS at night: 4.55 ± 2.75 CoS: 75.1 ± 81.85 SST: 77.49 ± 81.24 |
Overall population VAS at rest: 0.39 ± 0.77 VAS during movement: 1.87 ± 1.85 VAS at night: 0.7 ± 1.32 CoS: 84.07 ± 11.47 SST: 87.15 ± 14.99 Group I VAS at rest: 0.86 ± 0.99 VAS during movement: 1.77 ± 1.87 VAS at night: 0.91 ± 1.27 CoS: 75.10 ± 10.06 SST: 77.27 ± 16.7 Group II VAS at rest: 0.18 ± 0.56 VAS during movement: 1.89 ± 1.82 VAS at night: 0.59 ± 1.15 CoS: 85.37 ± 10.24 SST: 90.74 ± 13.34 Group III VAS at rest: 0.15 ± 0.49 VAS during movement: 1.9 ± 1.97 VAS at night: 0.65 ± 1.63 CoS: 92.45 ± 7.19 SST: 94.18 ± 7.69 |
No complications |
| Significant improvement in the overall population and Group I, no differences in Group II and III. | ||||||||
RCTP=rotator cuff tendinopathy; PTRCT=partial-thickness rotator cuff tear; FTRCT=full-thickness rotator cuff tear; CoS=Constant score; ASES=American Shoulder and Elbow Surgeons Shoulder Score; VAS=Visual analogue score; KSS=Korean Shoulder Scoring System; SST=Simple Shoulder Test; FVAS=Function-VAS; PVAS=Pain-VAS; NRS=Numerical Rating Scale; DASH= Disability of the Arm, Shoulder, and Hand.
Table 2.
Results of the Modified Coleman Methodology Score (MCMS) used to assess the quality of the included articles.
Table 2.
Results of the Modified Coleman Methodology Score (MCMS) used to assess the quality of the included articles.
| References | Study size | Follow-up | N procedures | Type of study | Diagnostic certainty | Description of injection technique | Rehabilitation and compliance | Outcome criteria | Outcome assessment | Selection process | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Kim et al 2019 | 10 | 4 | 7 | 0 | 5 | 10 | 5 | 10 | 12 | 5 | 68 |
| Kim et al 2020 | 7 | 4 | 7 | 10 | 5 | 10 | 5 | 10 | 12 | 5 | 75 |
| Chae et al 2020 | 0 | 0 | 10 | 0 | 5 | 10 | 5 | 10 | 12 | 5 | 57 |
| Corrado et al 2020 | 0 | 0 | 10 | 0 | 5 | 5 | 5 | 10 | 12 | 5 | 52 |
| Godek et al 2022 | 7 | 0 | 7 | 15 | 5 | 5 | 5 | 10 | 12 | 5 | 71 |
| Aldhafian et al 2023 | 10 | 4 | 10 | 0 | 5 | 5 | 5 | 10 | 12 | 5 | 54 |
| Buda et al. 2023 | 7 | 0 | 10 | 10 | 5 | 5 | 0 | 10 | 12 | 5 | 76 |
| Maximum Score Possible | 10 | 10 | 10 | 15 | 5 | 10 | 10 | 10 | 15 | 10 | 100 |
| Mean ± Standard Deviation | 5,8 ± 4,2 | 1,7 ± 2,1 | 8,7 ± 1,6 | 5 ± 6,4 | 5 ± 0 | 7,1 ± 2.6 | 4,2 ± 1,8 | 10 ± 0 | 12 ± 0 | 5 ± 0 | 63,3 ± 8,9 |
There was a large range of MCMS values, from 52 to 76, with a mean of 63.3 ± 8.9 regarded as fair (55-69 points). Some of the selected studies reported a relatively small cohort of patients, unclear outcome criteria and assessments and poor patient selection processes and low quality of evidence. For this reason, a meta-analysis was not performed.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



