
Submitted:
05 December 2024
Posted:
05 December 2024
You are already at the latest version
Abstract
Background/Objectives: Polygenic risk scores (PRSs) have been extensively studied and are in-creasingly applied in healthcare. One of the most studied and developed areas is predictive med-icine for breast cancer, but there is no wider consensus on the indications for the clinical use of PRSs for breast cancer. Current guidance endeavours to articulate the scientific evidence under-pinning the clinical utility of PRS in stratifying breast cancer risk, with a particular emphasis on clinical application.
Methods: The guidance has been prepared by a group of experts who have been active in breast cancer PRS research and development, combining a review of the evidence base with expert opin-ion for indications for clinical use.
Results: Based on data from various studies and existing breast cancer prevention and screening services, the indications for clinical use of breast cancer PRS can be divided into the following scenarios: 1) Management of cancer-free women with a family history of cancer; 2) Individual personalised breast cancer prevention and screening in healthcare services; 3) Breast cancer screening programs for more personalised screening.
Conclusions: The integration of PRS into clinical practice enables healthcare providers to deliver more accurate risk assessments, personalised prevention strategies, and optimised screening programmes, thereby improving patient outcomes and enhancing the effectiveness of breast cancer care. PRS testing represents a novel component in clinical breast cancer risk assessment, support-ing a personalised, risk-based approach to breast cancer prevention and screening.
Keywords:
breast cancer
; polygenic risk score
; genetic predisposition
; prevention
; screening
; personalised medicine
1. Introduction
Polygenic risk scores (PRSs) have been extensively studied and are increasingly applied in healthcare. One of the most researched and developed areas for this is predictive medicine for breast cancer, but so far, there is no wider consensus on the indications for the clinical use of PRSs for breast cancer. The American College of Medical Genetics and Genomics (ACMG) has published the statement about the clinical application of PRSs with points to consider in applications [1]. The authors state that although being rapidly incorporated into health care, there are currently no clinical guidelines available for the use of this technology. Current guidance endeavours to articulate the scientific evidence underpinning the clinical utility of PRS in stratifying breast cancer risk, with a particular emphasis on clinical application. It delineates pertinent scenarios wherein its clinical application is relevant and deliberates on the methodologies through which these principles can be pragmatically instituted within a clinical environment. The guidance has been prepared by a group of experts who have been active in breast cancer research, including PRS research and other relevant projects, as well as in clinical use. The AnteNOR and BRIGHT projects have investigated and clinically developed the application of PRS in personalised breast cancer prevention and screening [2,3].
To the extent that the contexts of cancer prevention and PRS can be different in different healthcare systems, we will discuss it primarily in the context of European healthcare systems.
2. Background
2.1. Breast Cancer Prevention and Screening
Breast cancer is the leading cause of cancer deaths in women. Every year adds 2.3 million new diagnoses and more than 660,000 deaths worldwide [4]. Breast cancer morbidity and mortality can be reduced through primary and secondary prevention.
Primary breast cancer prevention involves lifestyle modifications such as a healthy diet, weight control, regular exercise, and limiting alcohol intake and prolonged breastfeeding, alongside medical interventions including hormonal preventive medication and risk-reducing surgery in very high-risk cases, all tailored to individual risk factors and developed in consultation with healthcare providers [5].
Secondary breast cancer prevention with mammography screening reduces mortality risk from breast cancer by 20-30% [6,7,8]. Breast cancer incidence rates vary significantly across different age groups and populations globally; therefore, we describe the background in the European context. European breast cancer screening programs typically target women aged 50 to 69 years and are mostly based on age only [9,10]. The primary method used is mammography, performed biennially or triennially in the United Kingdom. Some countries also include women aged 40 or 45 to 74 in their screening programs, recognizing the potential benefits in slightly younger and older populations. European guidelines on breast cancer screening and diagnosis from the “European Commission Initiative on Breast and Colorectal Cancer” recommends for asymptomatic women with an average risk of breast cancer screening from age 45 [10]. Such an approach does not, however, account for the wide variation in individual women’s breast cancer risks and disregards younger women with a higher risk, but also women over age 45 or 50 with higher risk levels who could benefit from intensified screening. The traditional one-size-fits-all approach to breast cancer screening does not account for individual variations in risk factors such as genetic predisposition, family history, breast density, and lifestyle factors. Risk-stratified screening aims to tailor screening strategies to individual risk profiles, enhancing the benefits while minimizing the harms. Risk-based screening, in which an individualized risk assessment is used to inform screening practices, has been proposed as an alternative to age-based screening [11,12].
Around one third of the total breast cancer risk has been shown as hereditary/familial [13]. Therefore, genetic predisposition followed by a genetic risk assessments are an extremely important component in risk-based, or personalised, breast cancer prevention. Genetic factors include rare monogenic pathogenic variants (MPVs) in high and moderate-risk cancer predisposition genes. Their effects are large enough to warrant monogenic variant testing. However, only a fraction (5-10%) of breast cancer cases are contributed to by these rare MPVs [14]. Indeed, only around 1.7% of people and 5.7% of those with breast cancer currently are known to carry MPVs in the 12-13 actionable breast cancer genes conferring at least a reported 2-fold risk [15]. A considerable part of breast cancer risk variation is explained by variants outside these high/moderate-risk genes in the form of breast cancer associated common single-nucleotide polymorphisms (SNPs), identified by genome-wide association studies (GWAS) [16,17]. A polygenic risk score (PRS) is the combined effect of individual breast cancer susceptibility SNPs. Although individual associated SNPs may confer only modest disease risk, the combined effect of all known associated SNPs on risk can be substantial. An additional component of genetic susceptibility is also family history without known MPV and PRS data.
2.2. Monogenic Breast Cancer Risk
Certain monogenic pathogenic variants (MPVs) in individual genes result in a significantly higher predisposition to breast cancer. Recent analyses have specified MPVs in the genes ATM, BARD1, BRCA1, BRCA2, CDH1, CHEK2, PALB2, RAD51C, RAD51D, TP53, PTEN, and STK11, all associated with higher breast cancer risk levels [18,19,20,21].
Testing for MPVs requires panel sequencing of selected genes or sequencing of the entire exome or genome. Indications for MPV testing in healthy individuals, but also in breast cancer patients are usually defined by international and national guidelines using family cancer history and/or age at onset and cancer pathology [22,23,24,25,26]. For instance, in the UK all patients with triple negative breast cancer qualify for testing [27].
Carriers of MPVs associated with an increased risk of breast cancer are recommended to undergo more intensive surveillance and may also be offered additional preventative options. The specifics of how carriers are followed can vary based on individual risk factors, family history, and the type of variant.
2.3. Polygenic Breast Cancer Risk
A considerable part of breast cancer variation is explained by variants outside high-risk or moderate-risk genes in the form of breast cancer-associated common SNPs [16]. PRS in general is an estimate of an individual’s susceptibility to develop a specific disorder, based upon the weighted association of single-nucleotide variants (formerly single-nucleotide polymorphisms) or risk variants identified in genome-wide association studies [28]. A breast cancer PRS is the combined effect of individual breast cancer susceptibility variants identified by genome-wide association studies which have demonstrated their ability to assess individual breast cancer risk levels [17,29,30,31,32,33].
PRS is the strongest independent risk factor for breast cancer development on a population basis [34,35] outweighing MPVs. Breast cancer PRSs identify differences in genetic risks and providing a basis for designing personalised screening programs by accounting for individual genetic susceptibility [36]. In particular, in contrast to MPV testing, they identify a low-risk population. Modelling studies have suggested that risk profile informed preventive activities could provide cost savings and health benefits [37,38,39]. High-risk estimation could be also an indication for the use of hormonal preventive medication [40].
Assessment of the performance of PRSs is commonly performed using hazard ratios (HRsd) or odds ratios (ORsd) for an increment of one standard deviation in the score and the area under the receiver operating characteristic curve (AUC) [41]. AUC is the statistic indicator for assessing the discriminative ability of the PRSs. It is defined as the probability that an individual with a disease will be assigned a higher risk than an individual without the disease. An AUC of 0.5 indicates no discrimination and 1 indicates perfect discrimination. Breast cancer PRSs alone can be considered to exhibit modest discrimination at around 0.6-0.65 [42], however, when considering PRS use in the clinical context of asymptomatic women, the added information provided by PRSs has the potential to detect a large portion of the population at increased risk of breast cancer [43].
It is common to report HRs for the PRS top quintile, top decile or for top 5%, 2% or 1% percentiles compared to an average or low PRS category while modelling breast cancer. In addition, incidence rates of breast cancer in PRS categories are informative. In a landmark study, Mavaddat with colleagues developed several PRSs for breast cancer, from the largest available genome-wide association dataset and empirically validated the PRSs in prospective studies [29]. For the best PRSs (313 SNPs), the OR for overall disease per 1 standard deviation in 10 prospective studies was ORsd=1.61 (95%CI: 1.57–1.65) with the area under the receiver-operator curve (AUC) = 0.630 (95%CI: 0.618–0.651). The lifetime risk of overall breast cancer in the top centile of the PRSs was 32.6%. Compared with women in the middle quintile, those in the highest 1% of risk had a 4.37-fold risk of developing oestrogen receptor-positive disease and a 2.78-fold risk of developing oestrogen receptor-negative disease. The corresponding numbers for those in the lowest 1% of risk were 0.16- and 0.27-fold risks, respectively. Goodness-of-fit tests indicated that this PRS was well calibrated and predicted disease risk accurately in the tails of the distribution. The authors concluded that breast cancer PRS is a powerful and reliable predictor of breast cancer risk that may improve prevention programmes [29].
The development of a clinical grade level breast cancer PRS test and the first clinical implementation outside of research settings have been described by Padrik et al. [44]. The authors aimed to develop a clinical-grade PRS test suitable for breast cancer risk-stratified screening with clinical recommendations for implementation in clinical practice. In the first phase of the development, the authors gathered previously published PRS models for predicting breast cancer risk from the literature and validated them using the Estonian Biobank and UK Biobank data sets. The best-performing model was chosen based on prevalence data and independently validated in both incident data sets. The best performing PRS included 2803 SNPs (PRS2803). The C-index of the Cox regression model associating breast cancer status with PRS was 0.656 (SE=0.05) with a HRof 1.66. The PRS can stratify individuals with more than a three-fold risk increase. Following absolute risk simulations, risk-based recommendations were developed, the test was registered as a CE-marked in vitro device, and implemented into clinical practice [44].
PRSs are distinct from monogenic tests. Single gene or gene panel tests focus on loci and variants with large effects, whereas PRSs evaluate a cumulative risk of multiple loci. In contrast to monogenic diseases, multifactorial, complex diseases require non-family-based approaches, such as a PRS. In clinical practice, it is important to consider the impact of both types of genetic predisposition.
2.4. Possibilities to Combine Breast Cancer PRS with Other Risk Factors
Several combined risk prediction models incorporate traditional risk factors such as demographics, reproductive history, menopausal status, family history, previous biopsies, mammographic density, and carrier status of MPV and PRS [35,45,46,47,48]. For comprehensive breast cancer risk predictions, PRS test information can be used within combined risk models such as CanRisk or Tyrer-Cuzick[47,49]. In these models, the use of other known risk factors in combination with PRS has been shown to enhance the prediction of combined models[42,50,51].
Lee et al. showed that a combined risk model using the CanRisk model with PRS, family history, breast density and other risk factors was estimated to identify ∼13% of the population at moderate or high risk of developing breast cancer according to the UK National Institute for Health and Care Excellence (NICE) guidelines [22,35]. Using the Tyrer-Cuzick model this can rise to as high as 20% [50]. As expected, the variation in risk is greatest when including all risk factors in the model [35].
PRS alone has been shown to predict the risk of breast cancer in European descent individuals more accurately than current clinical models [52]. Van den Broek et al. have assessed the clinical utility of a first-degree breast cancer family history and PRS to inform screening decisions among women aged 30-50 years [53]. Results suggested that breast cancer family history and PRS could guide screening decisions before age 50 years among women at increased risk for breast cancer with the potential to prevent more breast cancer deaths for identifiable groups of women at high risk due to their breast cancer family history and polygenic risk. An analysis by Wolfson et al. concluded that population-wide programs for breast cancer screening that seek to stratify women by their genetic risk should focus first on PRS, not on more highly penetrant but rarer variants, or family history [34]. The PROCAS study also showed that the main factor influencing risk stratification was increasing the number of SNPs in the PRS rather than adding a gene panel (41). The PRS was most predictive for identifying women at high risk, while family history was the weakest.
The results of the clinically available AnteBC test (PRS2803, OÜ Antegenes, Estonia) can be used in the CanRisk combined breast cancer risk assessment model by entering the z-score from the AnteBC test report and the alpha value of 0.437 or in Tyrer-Cuzick using the non-logarithmic OR.
3. Utilising Breast Cancer Polygenic Risk Scores in Clinical Practice
Based on published research evidence, breast cancer PRSs have become an increasingly relevant tool in the landscape of breast cancer risk-stratified prevention and screening. Here are the primary clinical scenarios where the use of PRS can be particularly impactful:
1) Management of healthy women with a family history of cancer in hereditary cancer clinics [54,55,56,57,58,59,60,61,62,63,64,65,66].
3) Breast cancer screening programs to make screening more precise and effective [34,53,68,69,70,71].
If non-genetic risk data is available, and the process is feasible, then it is possible to use PRS test results combined with other risk factors within combined risk prediction models such as CanRisk [49].
3.1. Personalised Breast Cancer Risk-Based Management of Cancer-Free Women with a Family History of Cancer in Hereditary Cancer Clinics
3.1.1. Women with Negative Breast Cancer MPV Test Findings
Family history is an essential factor guiding screening strategies of family members of breast cancer patients. Testing of rare pathogenic variants is already standard practice for women with significant breast and ovarian cancer family history or known diagnosed MPVs in relatives, and with already demonstrated clinical benefit. Approaches in the case of MPVs are summarized in different guidelines and include earlier more intense screening methods (yearly mammography and MRI), but also risk-reducing surgeries [23]. However, for women in whom MPV testing did not detect the presence of MPVs in them or their families, PRS testing is recommended to fully assess their genetic risk [55,56,57,58,72]. PRS identifies women at a genetically higher risk of breast cancer who tested negative for monogenic risk genes [73].
A study by Evans et al. demonstrated that PRS gave additional risk modification information for women with familial breast cancer history who received combined risk estimation using the Tyrer-Cuzick model [54]. The authors concluded that PRS may be used to refine risk assessment for women at increased familial risk who test negative/have a low likelihood of BRCA1/2 mutations [54]. A study by Dite et al. analysed how much breast cancer risk prediction models can be improved by including information on known susceptibility SNPs. The study showed that for women under the age of 50 according to the population-based Australian Breast Cancer Family Registry data, a 77 SNP-based PRS improved risk prediction by >20% in combined risk prediction models [56]. A study by Li et al. examined the utility of PRS in familial but non-BRCA-associated breast cancer cases, demonstrating that according to their PRS-based predicted risk, management for up to 23% of women could be altered [57]. A study by Mars et al. showed that the PRS improved risk assessment of first-degree relatives of women with breast cancer, with pronounced stratification particularly for family history of early-onset disease [59]. A study by Lakeman et al. showed that including the PRS in the BOADICEA combined risk model for family-based risk prediction changed screening recommendations in up to 27%, 36% and 34% of cases according to breast cancer screening guidelines from the USA, UK and the Netherlands, respectively [58]. A study by Stiller et al. aimed to assess the clinical value of incorporating a PRS into breast cancer risk calculations in a cohort of German women with suspected hereditary breast and ovarian cancer syndrome [60]. The PRS led to changes in risk stratification based on 10-year risk calculations in 13.6% of individuals. Furthermore, the inclusion of the PRS in breast cancer risk predictions resulted in clinically significant changes in 12.0% of cases, impacting the prevention recommendations established by the German Consortium for Hereditary Breast and Ovarian Cancer. These findings support the implementation of the PRS in genetic counselling for personalised breast cancer risk assessment [74]. A study by Tüchler et al. assessed estimated lifetime risks and estimated 10-year risks of 425 cancer-free women with family history of cancer. They used the CanRisk model, including germline MPV status, non-genetic risk factors, and a 306 variant-based PRS, and analysed impact to the proportions of women changing country-specific European risk categories for intensified breast screening [75]. The study findings showed that for women with non-informative MPV status, inclusion of PRS and non-genetic risk factors changed clinical recommendations in up to 31.0% of cases, whereas for women tested negative for a MPV observed in their family, clinical recommendations changed in up to 16.7% of cases. This study provided additional rationale for considering PRS and non-genetic risk factors for individualized breast cancer risk prediction in routine clinical care [75].
This data shows that for women with a family history of breast cancer, but with negative findings in MPV testing, individual risk assessments and corresponding clinical recommendations are incomplete without PRS information and therefore not the most complete clinical practice anymore.
3.1.2. Women with Breast Cancer MPV Findings
PRSs have been shown in several studies to modify risk evaluations associated with MPVs in high- and moderate-risk breast cancer genes. Incorporating PRS into genetic testing for MPVs can improve the accuracy of risk estimation and aid risk management decisions for women who are MPV carriers, especially for MPVs in moderate risk genes ATM and CHEK2 [62,63,64,65].
A study by Kuchenbaecker et al. showed that breast cancer PRSs are predictive of cancer risk in BRCA1 and BRCA2 carriers, and that incorporation of the PRS into risk prediction models better informs decisions on cancer risk management [62]. A study by Fahed et al. estimated that among carriers of a MPV the disease risk based on the polygenic background ranged from 13% to 76% by age 75 years. This showed that accounting for the polygenic background increased the accuracy of risk estimation for individuals who inherit a MPV [63]. A study by Gallagher et al. demonstrated that the 86-SNP PRS modified the breast cancer risk for carriers of BRCA1, BRCA2, CHEK2, ATM, and PALB2 MPVs [64]. Results from the study by Gao et al. revealed that PRS facilitates the personalization of breast cancer risk among carriers of MPVs in predisposition genes. Incorporating PRS into breast cancer risk estimation may help identify > 30% of CHEK2 and nearly half of ATM carriers below the 20% lifetime risk threshold, suggesting the addition of PRS may prevent overscreening and enable more personalised risk management approaches [65]. A study by Mars et al. analysed how the PRS modifies breast cancer risk in mutation carriers [59]. For both PALB2 and CHEK2, a high PRS further increased the breast cancer risk. In terms of the lifetime risk for breast cancer by age 80, women with the PALB2 mutation and an average PRS (10–90th percentile) had a lifetime risk of 55.3% (95% CI 49.4–61.2%), which increased to 83.9% (71.2–96.6%) among women with a high PRS (>90th percentile) and decreased to 49.1% (30.6–67.6%) in women with a low PRS (<10th percentile). Women with CHEK2 and an average PRS had a lifetime risk of 29.3% (95% CI 26.8–31.8%) which doubled to 59.2% (52.1–66.3%) in women with a high PRS and decreased to 9.3% (4.5–14.1%) in women with a low PRS [59]. A study by Lakeman et al. showed that among carriers of MPVs in known moderate breast cancer susceptibility genes, the PRS had higher impact on CHEK2 and ATM than in the high risk MPVs [58]. A study by Schreurs et al. analysed the changes in surveillance category by adding a polygenic risk score based on 311 breast cancer-associated variants (PRS311), questionnaire-based risk factors and breast density on personalised breast cancer risk in unaffected women from Dutch CHEK2 c.1100delC families [66]. The surveillance advice was reclassified in 20 (34.5%) heterozygotes and 21 (35.6%) non-carriers after adding PRS311. Overall, most heterozygotes were reclassified to a less intensive surveillance, while non-carriers would require intensified surveillance. The addition of PRS, questionnaire-based risk factors and breast density to family history resulted in a more personalised breast cancer surveillance advice in CHEK2-families, which may lead to more efficient use of surveillance [66]. In the current Cancer Research UK funded study called Precision HBOC a SNP313 PRS is being used to stratify risk in BRCA1 and BRCA2 carriers [76].
Summarising the data, we can conclude that the addition of PRS impact gives additional information for more informed decisions regarding the management of breast cancer risk from MPVs, especially in the case of MPVs in the moderate-risk genes CHEK2 and ATM.
3.2. Individual Personalised Breast Cancer Prevention and Screening
Many healthcare providers and wellness programs offer more comprehensive and personalised health controls and monitoring than the usual population-based public screening programs. Additionally, such programs are also implemented by employer organizations (corporate wellness). As breast cancer is the most common malignancy among women, screening and prevention of breast cancer might be included in these services. Consideration of genetic risks, including MPV- and PRS-testing may be an important part of such services to increase the precision level of relevant clinical recommendations. A PRS is not directly inherited and is a risk factor independent of family history. Whilst MPVs on a population basis only substantially impact risk in the 1.7% of women who carry them, around 50% get a meaningful change in risk from a PRS [50]. Breast cancer individual personalised prevention and screening using the PRS is implemented currently in Estonian and the United Kingdom private healthcare [44].
3.3. Enhancement of Systematic Public breast Cancer Screening Programs
Screening with mammography reduces breast cancer mortality by 20-40% [6,7,77]. Current population-based breast cancer screening programs are based on age only. The European Commission Initiative on Breast Cancer (ECIBC) gives recommendations for breast cancer screening in women with an average risk of breast cancer, but each country has their own program [10,78]. Current European guidelines recommend for breast cancer screening [10]:
- women aged 40-44: no screening;
- women aged 45-49: screening every 2 or 3 years;
- women aged 50-69: screening every 2 years;
- women aged 70-74: screening every 3 years.
However, breast cancer in younger women tends to be more aggressive, with higher rates of metastasis and poorer survival rates compared to older women with breast cancer. Therefore, early detection and diagnosis may be particularly important for this age group.
Age-based population screening fails to include younger individuals already at risk-levels exceeding those defined to enter the screening program, e.g., women with higher genetic risk who can develop breast cancer much earlier than the defined age of the screening program. The application of personalised risks is necessary to identify those women who could benefit from an earlier start of the screening. Also, for high-risk women over age 50 current screening with 2-year intervals might not be considered optimal and miss many interval cases that would otherwise be detected earlier. Therefore, breast cancer screening might benefit from a better adaptation to the individual risk level of a woman.
With the help of the PRS, women can be divided into groups with different levels of risk based on which different recommendations for starting a mammography screening or other preventive measures can be given [50,51,79,80]. PRS identifies women at higher genetic risk who reach the threshold for population screening at a younger age, equivalent to risk for a woman at age 50 years who is eligible for population screening.
A study by Wolfson et al. suggests that population-wide programs for breast cancer screening that seek to stratify women by their genetic risk should focus first on PRS, not on more highly penetrant but rarer variants, nor family history [34]. An analysis by Lee et al., demonstrated that PRS is a stronger independent breast cancer risk factor than family history or mammographic density [35]. This finding is supported by other studies [81,82]. A thorough analysis by van den Broek et al. has assessed the clinical utility of a first-degree breast cancer family history and PRS to inform screening decisions among women aged 30-50 years [53]. The analysis results suggest that a combination of family history of breast cancer and PRS could guide screening decisions before age 50 years among women at increased risk for breast cancer. However, this increases in overdiagnoses, and false positives should be expected. The combined use of family history and PRS versus biennial screening from 50 to 74 years had the greatest increase in life-years gained (29%) and breast cancer deaths averted (18%) [53]. Benefits increased steeply relative to the USPSTF guideline as the PRS increased, so that women with 3 times or higher risk than average could begin screening at age 30 or 35 years, and those with greater than average risk (but <3 times the risk) could initiate screening at age 40 years. In addition, the lowest risk group could be screened triennially from ages 50 to 74 years [53]. Mars et al. evaluated PRS, family history, and MPVs for stratified screening [68]. Using FinnGen data (N = 117,252), linked to the Mass Screening Registry for breast cancer, the authors assessed the screening performance of a breast cancer PRS and compared its performance with family history of breast cancer and MPVs in moderate- (CHEK2)- to high-risk (PALB2) susceptibility genes. A high PRS conferred an elevated risk of interval breast cancers, and women with a low PRS had a low risk for both interval- and screen-detected breast cancers. Using real-life screening data, this study demonstrated the effectiveness of a breast cancer PRS for risk stratification, both alone and when combined with family history and MPVs [68]. A modelling analysis by Huntley et al. has shown that under favourable assumptions, the use of PRS use in UK cancer screening suggests a modest potential efficiency gain in breast cancer case detection and deaths averted [69]. Bolze et al. assessed breast cancer incidence and age of onset among women at low PRS risk compared with women at average risk and evaluated the potential to delay mammography based on genetic risk stratification[83]. In this case-control study of 25,591 women, 9.1% were classified as having low genetic risk for breast cancer; these women exhibited significantly later onset of breast cancer compared with average-risk or high-risk counterparts, indicating a potential to defer mammogram screening by 5 to 10 years with optimisation of health care resource allocation [83].
Personalised breast cancer screening based on hereditary risks for women at age 35-49 has been tested in the Estonian branch of the BRIGHT project using the family cancer history questionnaire, the PRS test AnteBC risk estimates for all women, and MPV testing based on family cancer history [84]. Amongst 799 participants, 90 (11.3%) had MPVs tested after consultations by clinical geneticists, resulting in 4 (4.4%) MPV diagnoses. PRS testing of all participants identified 330 (41.3%) women with elevated polygenic risk, with 124 (37.6%) women already at higher risk than the average 50-year-old [84]. The BRIGHT study demonstrated the feasibility of genetics-based precision prevention, facilitating earlier BC screening for younger women with elevated genetic risks. The predominantly digital service minimised the burden on healthcare personnel [84]. The BRIGHT study also assessed the cost-effectiveness of risk-stratified breast cancer screening in Estonia for women starting at age 35 versus standard mammography screening for ages 50-69, focusing on the PRS test's isolated impact[85]. Risk-stratified screening led to a redistribution of breast cancer stages, with more early (0-I) and fewer advanced stages (II-IV) and averted 1.5 breast cancer deaths per 1,000 women screened. Risk-stratified screening resulted in larger net costs of €145,235 (mainly related to PRS test and counselling costs), and a gain of 3.85 QALYs, with an ICER of €37,755 per QALY gained [85]. The conclusion was that a PRS-tailored breast cancer screening has clinical benefit and is cost-effective in Estonia.
The accumulated evidence clearly shows that age-based screening is probably not the best solution, screening could rather be organized based on women's individual risks. For this purpose, PRS, family history of cancer, MPV testing and, if feasible, the use of combined risk assessment models are important components of risk assessment.
4. Possibilities for Clinical Recommendations for Personalised Prevention and Screening of Breast Cancer Based on PRS Results
There are three foundations for the implementation of clinical recommendations based on PRSs.
4.1. Comparison with the Average Risk of the Same Population at the Same Age, Combined with a Comparison to the Average Risk upon Initiation of Mammographic Screening
Principally, societies have agreed that the average risk level at age 50 in most European countries is suitable to start public mammography screening [78]. It may be logical to start screening at a younger age for women if their PRS driven risk level achieves the same level or is higher than the average risk at age 50. This is according to principles of equitability and equivalence of risks. Figure 1 describes the age difference for women at high PRS risk in reaching same risk level compared to women at average risk at baseline for the start of current screening (age 50).
This approach is used in the WISDOM study for women aged 40 to 49 years, where screening is recommended when a women’s five-year risk equals or exceeds that of the average woman aged 50 years [86]. WISDOM study uses thresholds on five-year risk given that screening and prevention are most impactful in those at immediate risk of cancer, and five-year risk thresholds are standardly used to guide chemoprevention. The 5-year risk estimate in the WISDOM study for women aged 50 was 1.3%.
4.2. Comparison with Similar Risk MPVs
Like elevated polygenic risk, moderately elevated risk level (lifetime risks 25-30%) applies to MPVs in genes ATM and CHEK2[23], Figure 2. Accordingly, on the same PRS risk level, similar clinical recommendations can be given as in the case of moderate-risk MPVs. A comparative modelling analysis has shown that for women with ATM, CHEK2, and PALB2 pathogenic variants annual MRI screening starting at 30 to 35 years followed by annual MRI and mammography at 40 years may reduce breast cancer mortality by more than 50% [87]. A similar approach is feasible for women at the same risk level using PRS testing.
Breast cancer risk management in the case of moderate-risk MPVs is included for example in the NCCN guidelines. NCCN Guidelines for Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic, Version 3.2024 [88]: “In the case of MPVs in ATM and CHEK2 is recommended annual mammography at age 40 years and consider MRI with contrast starting at age 30-53”.
4.3. Comparison with Already Existing National Guidelines Based on Other Risk Factors (not Including PRSs) for Risk-Stratified Breast Cancer Screening According to Different Risk Levels
In this context, it is possible to use PRS isolated risk information as well as total risk estimation using combined models. The current guidelines for breast risk-stratified screening and surveillance of selected countries are reflected below, primarily based on the current practice of the authors of the article.
4.3.1. Guidelines in the United Kingdom
UK National Institute for Health and Care Excellence (NICE) guidelines for the management of women with familial breast cancer risk are using thresholds for risk categories [22], Table 1.
The NICE guideline refers to three levels of risk for developing breast: general population risk, moderate risk, and high risk [22]. Women whose risk is the same as the general population have about an 11% chance of developing breast cancer in their lifetime 23). Women with a moderate risk have a lifetime risk of developing breast cancer of greater than 17% but less than 30%. Women with a high risk have a 30% or greater chance of developing breast cancer in their lifetime. Accordingly, the UK NICE Guidelines have defined a moderate risk as 1.5 to 2.7 times higher than average risk, and a high risk as more than 2.7 times higher than average.
Breast cancer PRS can allocate risk groups based on this accordingly [44]:
- general population risk: 1.–79. percentiles;
- moderate risk: 80.–97. percentiles;
- high risk: 98.–99. percentiles.
- The NICE guideline also gives recommendations on surveillance for high- and moderate-risk groups of different ages, recommending annual mammography from age 40 for increased-risk groups.
4.3.2. Guidelines in Germany
German guidelines for breast cancer management, including screening are characterized in “Interdisziplinäre S3-Leitlinie für die Früherkennung, Diagnostik, Therapie und Nachsorge des Mammakarzinoms” [89]. The current German breast cancer guidelines recommend that women aged 40–49 undergo a mammogram screening every two years, but the guidelines suggest that the decision to undergo mammography screening in this age group should be based on an individual assessment of the potential benefits and harms, taking into account the woman's personal risk factors for breast cancer and her preferences[89]. There are in place principles and guidelines for “Breast Cancer Risk, Genetics and Prevention” by Arbaitsgemeinschaft Gynäkologische Onkologie (AGO) [90].
In Germany, genetic testing for breast cancer is primarily offered to individuals with a personal or family history of breast or ovarian cancer. The current guidelines for genetic testing in Germany are based on recommendations from the German Society of Human Genetics (GfH) and the German Consortium for Hereditary Breast and Ovarian Cancer (GC-HBOC) - Deutsches Konsortium Familiärer Brust- und Eierstockkrebs [91] GC-HBOC recommends for moderate MPV carriers’ annual clinical examination, breast ultrasonography and MRI from age 30 and mammography annually or biannually from age 40.
4.3.3. Guidelines in Norway
In Norway, national guidelines and recommendations exist for risk-stratified BC prevention [92]. Women with a family history of breast cancer and considered being at increased risk after assessment by medical geneticists, with no pathogenic variants in high-risk breast cancer genes, are offered annual 2-plane mammography from the age of 40-60. In families with cases of breast cancer before the age of 40, it may be considered to start mammography checks from the age of 30 [92]. Inclusion of PRS information may add value and give possibilities for more systematic implementation of risk-stratified prevention and screening.
4.3.4. Guidelines in Sweden
In Sweden, the National Board of Health and Welfare recommends population-based mammography screening for ages 40–74 with screening intervals 18 to 24 months [26]. For people with a hereditary increased risk, other intervals or methods may be relevant[26]. Swedish guidelines recommend MPV testing for cancer-free women according to family history, but the risk of primary breast cancer in a woman with healthy breasts can also be roughly estimated using epidemiological risk models. If applicable, the CanRisk model is recommended in the first place [26]. For women with moderately increased risk (based on the presence of pathogenic variant in gene associated with moderately increased risk, alternatively women with an epidemiologically greater than 20% lifetime risk), annual imaging (breast) from about 5 years before the lowest age of onset in the family or at the latest from the age of 40 up to about the age of 74 is recommended [26].
4.3.5. Guidelines in Portugal
According to the National Screening Program in Portugal, 50–69 years old women are invited to breast cancer screening every two years [93]. National guidelines for MPV testing for women without a cancer diagnosis, are based on specific criteria that focus on identifying those at higher risk due to family history or other factors [93]. These guidelines are intended to identify individuals who may benefit most from genetic testing due to an increased risk of hereditary breast cancer, allowing for personalised risk management and preventive strategies. Women with high-risk breast cancer MPVs (e.g., BRCA1, BRCA2), moderate-risk MPVs (e.g., CHEK2, ATM, PALB2), or other increased risk factors such as a strong family history or previous breast conditions, are advised to start screening earlier, typically around 30–40 years, with annual mammograms and breast MRI depending on their specific risk profile. These women receive genetic counselling and personalised management plans.
4.3.6. Guidelines in Estonia
In Estonia, women aged 50–74 years are invited to breast cancer screening at two-year intervals. Risk-based management of hereditary cases is performed according to healthcare institution internal guidelines. Estonia has conducted a national clinical feasibility project investigating the implementation of PRS and MPV based breast cancer risk stratified screening for women younger than current standard screening programme[94]. Breast cancer PRS testing for cancer-free women is currently implemented in healthcare services[67]. Estonian Health Insurance Fund is preparing a PRS based risk stratified screening for women at age 40, the programme is aimed to start early 2025 [95].
5. The Regulatory and Legal Status of Breast Cancer Risk Estimation Tools in the European Union in the Context of Polygenic Risk Score Testing
As the regulatory understanding of PRS in the scientific literature and clinical practice seems somewhat unclear, we also examine the current regulatory background in the European Union. PRS tests for disease predispositions are regulated under the EU In Vitro Diagnostic Regulation (IVDR) 2017/746 because they are considered in vitro diagnostic (IVD) medical devices [96]. According to the regulation, an IVD medical device is any device which, whether used alone or in combination, is intended by the manufacturer for the in vitro examination of specimens derived from the human body solely or principally to provide information on a physiological or pathological state, or a congenital abnormality, or to monitor therapeutic measures. Accordingly, PRS tests are classified as in vitro diagnostic (IVD) medical devices and must comply with the EU's IVDR 2017/746. These tests must demonstrate clinical validity and utility, with a clear demonstration of performance characteristics and safety. They are subject to pre-market scrutiny and must fulfil post-market surveillance obligations. Providers must ensure the tests are not discriminatory and consider the diversity of the population, including genetic variations across different ancestries.
Another option in the EU is to perform PRS tests as Laboratory Developed Tests (LDTs) under EU IVDR 2017/746 with relevant restrictions [96]. The IVDR imposes more stringent requirements on LDTs than the previous directive, aiming to align their safety and performance standards with commercially available IVDs. There is a health institution exemption under Article 5(5), but it requires LDTs to be justified, documented, and notified to national competent authorities. LDTs must be manufactured and used within the same EU member state health institution, under a quality management system. Performance evaluations and compliance with the general safety and performance requirements are mandatory. These regulations ensure a high standard of quality and safety for diagnostic tests, including PRS tests, whether they are commercial kits or developed in-house within EU health institutions. Lab-developed tests cannot be used for public screening programs (on an industrial scale).
6. Conclusions
In conclusion, the adoption of breast cancer PRS testing represents a significant advancement in personalised medicine, namely in personalised screening. By incorporating PRS into clinical practice, healthcare providers can offer more precise risk assessments, tailored prevention strategies, and optimized screening programs, ultimately improving patient outcomes and enhancing the efficiency of breast cancer care.
Author Contributions
All authors have read and agreed to the published version of the manuscript.
Funding
The development of the guidance was supported by the BRIGHT consortium by European Commission via EIT Health BRIGHT innovation activity (project #230121). The AnteNOR consortium was sponsoring the development of the guidance through a grant from the Norwegian Grants 2014-2021 Green ICT programme (Project No 2014-2021.1.02.20-0113). D Gareth Evans is supported by the Manchester National Institute for Health Research (NIHR) Biomedical Research Centre (IS-BRC-1215-20007). Sander Pajusalu is supported by the Estonian Research Council grant (PSG774).
Data Availability Statement
N/A.
Acknowledgments
The authors acknowledge Oslo Cancer Cluster for facilitating discussions on the topic during AnteNOR consortium work and University of Tartu organizing topic-specific discussions during the work of the BRIGHT consortium.
Conflicts of Interest
Peeter Padrik has ownership in OÜ Antegenes. D Gareth Evans is a non-executive director of Everything Genetic Ltd and Is an advisor to OÜ Antegenes. Siim Sõber owns an option for shares in OÜ Antegenes. Krista Kruuv-Käo owns an option for shares in OÜ Antegenes.
References
- Abu-El-Haija, A.; Reddi, H.V.; Wand, H.; Rose, N.C.; Mori, M.; Qian, E.; Murray, M.F.; Practice, A.P.; Guidelines Committee. Electronic address, d.a.n. The clinical application of polygenic risk scores: A points to consider statement of the American College of Medical Genetics and Genomics (ACMG). Genetics in medicine : official journal of the American College of Medical Genetics 2023, 100803, doi:10.1016/j.gim.2023.100803. [CrossRef]
- AnteNOR Project. Available online: https://antegenes.com/antenor/ (accessed on 01.10.2024).
- BRIGHT Project. Available online: https://brightscreening.eu (accessed on 01.10.2024).
- Ferlay J, E.M., Lam F, Laversanne M, Colombet M, Mery L, Piñeros M, Znaor A, Soerjomataram I, Bray F. Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer. Available from: https://gco.iarc.fr/today. Available online: (accessed on 15.09.2024).
- NCCN Clinical Practice Guidelines in Oncology. Breast Cancer Risk Reduction. Version 2. 2024. Available online: https://www.nccn.org/professionals/physician_gls/pdf/breast_risk.pdf (accessed on 30.05.2024).
- Myers, E.R.; Moorman, P.; Gierisch, J.M.; Havrilesky, L.J.; Grimm, L.J.; Ghate, S.; Davidson, B.; Mongtomery, R.C.; Crowley, M.J.; McCrory, D.C.; et al. Benefits and Harms of Breast Cancer Screening. Jama 2015, doi:10.1001/jama.2015.13183. [CrossRef]
- Tabár, L.; Dean, P.B.; Chen, T.H.-H.; Yen, A.M.-F.; Chen, S.L.-S.; Fann, J.C.-Y.; Chiu, S.Y.-H.; Ku, M.M.-S.; Wu, W.Y.-Y.; Hsu, C.-Y.; et al. The incidence of fatal breast cancer measures the increased effectiveness of therapy in women participating in mammography screening. Cancer 2018, doi:10.1002/cncr.31840. [CrossRef]
- Independent, U.K.P.o.B.C.S. The benefits and harms of breast cancer screening: an independent review. Lancet 2012, 380, 1778-1786, doi:10.1016/S0140-6736(12)61611-0. [CrossRef]
- In WHO Position Paper on Mammography Screening; WHO Guidelines Approved by the Guidelines Review Committee; Geneva, 2014.
- European guidelines on breast cancer screening and diagnosis. Available online: https://healthcare-quality.jrc.ec.europa.eu/ecibc/european-breast-cancer-guidelines (accessed on 30.08.2024).
- Schousboe, J.T.; Kerlikowske, K.; Loh, A.; Cummings, S.R. Personalizing mammography by breast density and other risk factors for breast cancer: analysis of health benefits and cost-effectiveness. Ann Intern Med 2011, 155, 10-20, doi:10.7326/0003-4819-155-1-201107050-00003. [CrossRef]
- Shieh, Y.; Eklund, M.; Sawaya, G.F.; Black, W.C.; Kramer, B.S.; Esserman, L.J. Population-based screening for cancer: hope and hype. Nature reviews. Clinical oncology 2016, 13, 550-565, doi:10.1038/nrclinonc.2016.50. [CrossRef]
- Mucci, L.A.; Hjelmborg, J.B.; Harris, J.R.; Czene, K.; Havelick, D.J.; Scheike, T.; Graff, R.E.; Holst, K.; Moller, S.; Unger, R.H.; et al. Familial Risk and Heritability of Cancer Among Twins in Nordic Countries. Jama 2016, 315, 68-76, doi:10.1001/jama.2015.17703. [CrossRef]
- Apostolou, P.; Fostira, F. Hereditary breast cancer: the era of new susceptibility genes. BioMed research international 2013, 2013.
- Rowlands, C.F.; Allen, S.; Balmaña, J.; Domchek, S.M.; Evans, D.G.; Hanson, H.; Hoogerbrugge, N.; James, P.A.; Nathanson, K.L.; Robson, M.; et al. Population-based germline breast cancer gene association studies and meta-analysis to inform wider mainstream testing. Annals of oncology : official journal of the European Society for Medical Oncology / ESMO 2024, 35, 892-901, doi:10.1016/j.annonc.2024.07.244. [CrossRef]
- Ghoussaini, M.; Pharoah, P.D. Polygenic susceptibility to breast cancer: current state-of-the-art. Future oncology 2009, 5, 689-701.
- Mavaddat, N.; Pharoah, P.D.; Michailidou, K.; Tyrer, J.; Brook, M.N.; Bolla, M.K.; Wang, Q.; Dennis, J.; Dunning, A.M.; Shah, M.; et al. Prediction of breast cancer risk based on profiling with common genetic variants. J Natl Cancer Inst 2015, 107, doi:10.1093/jnci/djv036. [CrossRef]
- Breast Cancer Risk Genes — Association Analysis in More than 113,000 Women. New England Journal of Medicine 2021, 384, 428-439, doi:doi:10.1056/NEJMoa1913948. [CrossRef]
- Hu, C.; Hart, S.N.; Gnanaolivu, R.; Huang, H.; Lee, K.Y.; Na, J.; Gao, C.; Lilyquist, J.; Yadav, S.; Boddicker, N.J.; et al. A Population-Based Study of Genes Previously Implicated in Breast Cancer. The New England journal of medicine 2021, 384, 440-451, doi:10.1056/NEJMoa2005936. [CrossRef]
- Foulkes, W.D. The ten genes for breast (and ovarian) cancer susceptibility. Nature reviews. Clinical oncology 2021, 18, 259-260, doi:10.1038/s41571-021-00491-3. [CrossRef]
- McDevitt, T.; Durkie, M.; Arnold, N.; Burghel, G.J.; Butler, S.; Claes, K.B.M.; Logan, P.; Robinson, R.; Sheils, K.; Wolstenholme, N.; et al. EMQN best practice guidelines for genetic testing in hereditary breast and ovarian cancer. European Journal of Human Genetics 2024, 32, 479-488, doi:10.1038/s41431-023-01507-5. [CrossRef]
- Familial breast cancer: classification, care and managing breast cancer and related risks in people with a family history of breast cancer. Available online: https://www.nice.org.uk/guidance/cg164/chapter/recommendations#breast-cancer-risk-category (accessed on 11.06.2017).
- Sessa, C.; Balmana, J.; Bober, S.L.; Cardoso, M.J.; Colombo, N.; Curigliano, G.; Domchek, S.M.; Evans, D.G.; Fischerova, D.; Harbeck, N.; et al. Risk reduction and screening of cancer in hereditary breast-ovarian cancer syndromes: ESMO Clinical Practice Guideline. Annals of oncology : official journal of the European Society for Medical Oncology / ESMO 2023, 34, 33-47, doi:10.1016/j.annonc.2022.10.004. [CrossRef]
- Wappenschmidt, B.; Hauke, J.; Faust, U.; Niederacher, D.; Wiesmuller, L.; Schmidt, G.; Gross, E.; Gehrig, A.; Sutter, C.; Ramser, J.; et al. Criteria of the German Consortium for Hereditary Breast and Ovarian Cancer for the Classification of Germline Sequence Variants in Risk Genes for Hereditary Breast and Ovarian Cancer. Geburtshilfe Frauenheilkd 2020, 80, 410-429, doi:10.1055/a-1110-0909. [CrossRef]
- Rhiem, K.; Auber, B.; Briest, S.; Dikow, N.; Ditsch, N.; Dragicevic, N.; Grill, S.; Hahnen, E.; Horvath, J.; Jaeger, B.; et al. Consensus Recommendations of the German Consortium for Hereditary Breast and Ovarian Cancer. Breast care (Basel, Switzerland) 2022, 17, 199-207, doi:10.1159/000516376. [CrossRef]
- Bröstcancer. Nationellt vårdprogram. 2024-02-07. Version: 4.4.
- NHS National Genomic Test Directory. Testing Criteria for Rare and Inherited Disease. Version 6, 2024. Available online: https://www.england.nhs.uk/wp-content/uploads/2018/08/Rare-and-inherited-disease-eligibility-criteria-version-6-January-2024.pdf (accessed on 08.06.2024).
- Reddi, H.V.; Wand, H.; Funke, B.; Zimmermann, M.T.; Lebo, M.S.; Qian, E.; Shirts, B.H.; Zou, Y.S.; Zhang, B.M.; Rose, N.C.; et al. Laboratory perspectives in the development of polygenic risk scores for disease: A points to consider statement of the American College of Medical Genetics and Genomics (ACMG). Genetics in medicine : official journal of the American College of Medical Genetics 2023, 100804, doi:10.1016/j.gim.2023.100804. [CrossRef]
- Mavaddat, N.; Michailidou, K.; Dennis, J.; Lush, M.; Fachal, L.; Lee, A.; Tyrer, J.P.; Chen, T.H.; Wang, Q.; Bolla, M.K.; et al. Polygenic Risk Scores for Prediction of Breast Cancer and Breast Cancer Subtypes. American journal of human genetics 2019, 104, 21-34, doi:10.1016/j.ajhg.2018.11.002. [CrossRef]
- Michailidou, K.; Lindstrom, S.; Dennis, J.; Beesley, J.; Hui, S.; Kar, S.; Lemacon, A.; Soucy, P.; Glubb, D.; Rostamianfar, A.; et al. Association analysis identifies 65 new breast cancer risk loci. Nature 2017, 551, 92-94, doi:10.1038/nature24284. [CrossRef]
- Sieh, W.; Rothstein, J.H.; McGuire, V.; Whittemore, A.S. The role of genome sequencing in personalized breast cancer prevention. Cancer Epidemiol Biomarkers Prev 2014, 23, 2322-2327, doi:10.1158/1055-9965.EPI-14-0559. [CrossRef]
- Hughes, E.; Judkins, T.; Wagner, S.; Wenstrup, R.J.; Lanchbury, J.S.; Gutin, A. Development and validation of a residual risk score to predict breast cancer risk in unaffected women negative for mutations on a multi-gene hereditary cancer panel. Journal of Clinical Oncology 2017, 35, 1579-1579, doi:10.1200/JCO.2017.35.15_suppl.1579. [CrossRef]
- Khera, A.V.; Chaffin, M.; Aragam, K.G.; Haas, M.E.; Roselli, C.; Choi, S.H.; Natarajan, P.; Lander, E.S.; Lubitz, S.A.; Ellinor, P.T.; et al. Genome-wide polygenic scores for common diseases identify individuals with risk equivalent to monogenic mutations. Nature genetics 2018, 50, 1219-1224, doi:10.1038/s41588-018-0183-z. [CrossRef]
- Wolfson, M.; Gribble, S.; Pashayan, N.; Easton, D.F.; Antoniou, A.C.; Lee, A.; van Katwyk, S.; Simard, J. Potential of polygenic risk scores for improving population estimates of women's breast cancer genetic risks. Genetics in medicine : official journal of the American College of Medical Genetics 2021, 23, 2114-2121, doi:10.1038/s41436-021-01258-y. [CrossRef]
- Lee, A.; Mavaddat, N.; Wilcox, A.N.; Cunningham, A.P.; Carver, T.; Hartley, S.; Babb de Villiers, C.; Izquierdo, A.; Simard, J.; Schmidt, M.K.; et al. BOADICEA: a comprehensive breast cancer risk prediction model incorporating genetic and nongenetic risk factors. Genetics in medicine : official journal of the American College of Medical Genetics 2019, 21, 1708-1718, doi:10.1038/s41436-018-0406-9. [CrossRef]
- Lewis, C.M.; Vassos, E. Prospects for using risk scores in polygenic medicine. Genome medicine 2017, 9, 96, doi:10.1186/s13073-017-0489-y. [CrossRef]
- Pashayan, N.; Morris, S.; Gilbert, F.J.; Pharoah, P.D. Cost-effectiveness and benefit-to-harm ratio of risk-stratified screening for breast cancer: a life-table model. JAMA oncology 2018, 4, 1504-1510.
- Maas, P.; Barrdahl, M.; Joshi, A.D.; Auer, P.L.; Gaudet, M.M.; Milne, R.L.; Schumacher, F.R.; Anderson, W.F.; Check, D.; Chattopadhyay, S.; et al. Breast Cancer Risk From Modifiable and Nonmodifiable Risk Factors Among White Women in the United States. JAMA oncology 2016, 2, 1295-1302, doi:10.1001/jamaoncol.2016.1025. [CrossRef]
- Wright, S.J.; Eden, M.; Ruane, H.; Byers, H.; Evans, D.G.; Harvie, M.; Howell, S.J.; Howell, A.; French, D.; Payne, K. Estimating the Cost of 3 Risk Prediction Strategies for Potential Use in the United Kingdom National Breast Screening Program. MDM Policy Pract 2023, 8, 23814683231171363, doi:10.1177/23814683231171363. [CrossRef]
- Owens, D.K.; Davidson, K.W.; Krist, A.H.; Barry, M.J.; Cabana, M.; Caughey, A.B.; Doubeni, C.A.; Epling, J.W.; Kubik, M.; Landefeld, C.S.; et al. Medication Use to Reduce Risk of Breast Cancer: US Preventive Services Task Force Recommendation Statement. Jama 2019, 322, 857-867, doi:10.1001/jama.2019.11885. [CrossRef]
- Lambert, S.A.; Gil, L.; Jupp, S.; Ritchie, S.C.; Xu, Y.; Buniello, A.; McMahon, A.; Abraham, G.; Chapman, M.; Parkinson, H.; et al. The Polygenic Score Catalog as an open database for reproducibility and systematic evaluation. Nature genetics 2021, 53, 420-425, doi:10.1038/s41588-021-00783-5. [CrossRef]
- Roberts, E.; Howell, S.; Evans, D.G. Polygenic risk scores and breast cancer risk prediction. Breast 2023, 67, 71-77, doi:10.1016/j.breast.2023.01.003. [CrossRef]
- Chatterjee, N.; Shi, J.; Garcia-Closas, M. Developing and evaluating polygenic risk prediction models for stratified disease prevention. Nat Rev Genet 2016, 17, 392-406, doi:10.1038/nrg.2016.27. [CrossRef]
- Padrik, P.; Puustusmaa, M.; Tõnisson, N.; Kolk, B.; Saar, R.; Padrik, A.; Tasa, T. Implementation of Risk-Stratified Breast Cancer Prevention With a Polygenic Risk Score Test in Clinical Practice. Breast Cancer (Auckl) 2023, 17, 11782234231205700, doi:10.1177/11782234231205700. [CrossRef]
- Costantino, J.P.; Gail, M.H.; Pee, D.; Anderson, S.; Redmond, C.K.; Benichou, J.; Wieand, H.S. Validation studies for models projecting the risk of invasive and total breast cancer incidence. Journal of the National Cancer Institute 1999, 91, 1541-1548, doi:10.1093/jnci/91.18.1541. [CrossRef]
- Gail, M.H.; Brinton, L.A.; Byar, D.P.; Corle, D.K.; Green, S.B.; Schairer, C.; Mulvihill, J.J. Projecting individualized probabilities of developing breast cancer for white females who are being examined annually. J Natl Cancer Inst 1989, 81, 1879-1886, doi:10.1093/jnci/81.24.1879. [CrossRef]
- Tyrer, J.; Duffy, S.W.; Cuzick, J. A breast cancer prediction model incorporating familial and personal risk factors. Stat Med 2004, 23, 1111-1130, doi:10.1002/sim.1668. [CrossRef]
- Lee, A.; Mavaddat, N.; Cunningham, A.; Carver, T.; Ficorella, L.; Archer, S.; Walter, F.M.; Tischkowitz, M.; Roberts, J.; Usher-Smith, J.; et al. Enhancing the BOADICEA cancer risk prediction model to incorporate new data on RAD51C, RAD51D, BARD1 updates to tumour pathology and cancer incidence. J Med Genet 2022, 59, 1206-1218, doi:10.1136/jmedgenet-2022-108471. [CrossRef]
- Carver, T.; Hartley, S.; Lee, A.; Cunningham, A.P.; Archer, S.; Babb de Villiers, C.; Roberts, J.; Ruston, R.; Walter, F.M.; Tischkowitz, M.; et al. CanRisk Tool-A Web Interface for the Prediction of Breast and Ovarian Cancer Risk and the Likelihood of Carrying Genetic Pathogenic Variants. Cancer Epidemiol Biomarkers Prev 2021, 30, 469-473, doi:10.1158/1055-9965.EPI-20-1319. [CrossRef]
- Evans, D.G.R.; van Veen, E.M.; Harkness, E.F.; Brentnall, A.R.; Astley, S.M.; Byers, H.; Woodward, E.R.; Sampson, S.; Southworth, J.; Howell, S.J.; et al. Breast cancer risk stratification in women of screening age: Incremental effects of adding mammographic density, polygenic risk, and a gene panel. Genetics in medicine : official journal of the American College of Medical Genetics 2022, 24, 1485-1494, doi:10.1016/j.gim.2022.03.009. [CrossRef]
- Brentnall, A.R.; van Veen, E.M.; Harkness, E.F.; Rafiq, S.; Byers, H.; Astley, S.M.; Sampson, S.; Howell, A.; Newman, W.G.; Cuzick, J.; et al. A case-control evaluation of 143 single nucleotide polymorphisms for breast cancer risk stratification with classical factors and mammographic density. International journal of cancer. Journal international du cancer 2020, 146, 2122-2129, doi:10.1002/ijc.32541. [CrossRef]
- Martin, A.R.; Kanai, M.; Kamatani, Y.; Okada, Y.; Neale, B.M.; Daly, M.J. Clinical use of current polygenic risk scores may exacerbate health disparities. Nature genetics 2019, 51, 584-591, doi:10.1038/s41588-019-0379-x. [CrossRef]
- van den Broek, J.J.; Schechter, C.B.; van Ravesteyn, N.T.; Janssens, A.; Wolfson, M.C.; Trentham-Dietz, A.; Simard, J.; Easton, D.F.; Mandelblatt, J.S.; Kraft, P.; et al. Personalizing Breast Cancer Screening Based on Polygenic Risk and Family History. J Natl Cancer Inst 2021, 113, 434-442, doi:10.1093/jnci/djaa127. [CrossRef]
- Evans, D.G.; Brentnall, A.; Byers, H.; Harkness, E.; Stavrinos, P.; Howell, A.; Newman, W.G.; Cuzick, J. The impact of a panel of 18 SNPs on breast cancer risk in women attending a UK familial screening clinic: a case-control study. J Med Genet 2017, 54, 111-113, doi:10.1136/jmedgenet-2016-104125. [CrossRef]
- Lakeman, I.M.M.; Hilbers, F.S.; Rodriguez-Girondo, M.; Lee, A.; Vreeswijk, M.P.G.; Hollestelle, A.; Seynaeve, C.; Meijers-Heijboer, H.; Oosterwijk, J.C.; Hoogerbrugge, N.; et al. Addition of a 161-SNP polygenic risk score to family history-based risk prediction: impact on clinical management in non-BRCA1/2 breast cancer families. J Med Genet 2019, 56, 581-589, doi:10.1136/jmedgenet-2019-106072. [CrossRef]
- Dite, G.S.; MacInnis, R.J.; Bickerstaffe, A.; Dowty, J.G.; Allman, R.; Apicella, C.; Milne, R.L.; Tsimiklis, H.; Phillips, K.A.; Giles, G.G.; et al. Breast Cancer Risk Prediction Using Clinical Models and 77 Independent Risk-Associated SNPs for Women Aged Under 50 Years: Australian Breast Cancer Family Registry. Cancer Epidemiol Biomarkers Prev 2016, 25, 359-365, doi:10.1158/1055-9965.EPI-15-0838. [CrossRef]
- Li, H.; Feng, B.; Miron, A.; Chen, X.; Beesley, J.; Bimeh, E.; Barrowdale, D.; John, E.M.; Daly, M.B.; Andrulis, I.L.; et al. Breast cancer risk prediction using a polygenic risk score in the familial setting: a prospective study from the Breast Cancer Family Registry and kConFab. Genetics in medicine : official journal of the American College of Medical Genetics 2017, 19, 30-35, doi:10.1038/gim.2016.43. [CrossRef]
- Lakeman, I.M.M.; Rodriguez-Girondo, M.D.M.; Lee, A.; Celosse, N.; Braspenning, M.E.; van Engelen, K.; van de Beek, I.; van der Hout, A.H.; Gomez Garcia, E.B.; Mensenkamp, A.R.; et al. Clinical applicability of the Polygenic Risk Score for breast cancer risk prediction in familial cases. J Med Genet 2022, doi:10.1136/jmg-2022-108502. [CrossRef]
- Mars, N.; Widen, E.; Kerminen, S.; Meretoja, T.; Pirinen, M.; Della Briotta Parolo, P.; Palta, P.; FinnGen; Palotie, A.; Kaprio, J.; et al. The role of polygenic risk and susceptibility genes in breast cancer over the course of life. Nat Commun 2020, 11, 6383, doi:10.1038/s41467-020-19966-5. [CrossRef]
- Stiller, S.; Drukewitz, S.; Lehmann, K.; Hentschel, J.; Strehlow, V. Clinical Impact of Polygenic Risk Score for Breast Cancer Risk Prediction in 382 Individuals with Hereditary Breast and Ovarian Cancer Syndrome. Cancers (Basel) 2023, 15, doi:10.3390/cancers15153938. [CrossRef]
- Tuchler, A.; De Pauw, A.; Ernst, C.; Anota, A.; Lakeman, I.M.M.; Dick, J.; van der Stoep, N.; van Asperen, C.J.; Maringa, M.; Herold, N.; et al. Clinical implications of incorporating genetic and non-genetic risk factors in CanRisk-based breast cancer risk prediction. Breast 2024, 73, 103615, doi:10.1016/j.breast.2023.103615. [CrossRef]
- Kuchenbaecker, K.B.; McGuffog, L.; Barrowdale, D.; Lee, A.; Soucy, P.; Dennis, J.; Domchek, S.M.; Robson, M.; Spurdle, A.B.; Ramus, S.J.; et al. Evaluation of Polygenic Risk Scores for Breast and Ovarian Cancer Risk Prediction in BRCA1 and BRCA2 Mutation Carriers. J Natl Cancer Inst 2017, 109, doi:10.1093/jnci/djw302. [CrossRef]
- Fahed, A.C.; Wang, M.; Homburger, J.R.; Patel, A.P.; Bick, A.G.; Neben, C.L.; Lai, C.; Brockman, D.; Philippakis, A.; Ellinor, P.T.; et al. Polygenic background modifies penetrance of monogenic variants for tier 1 genomic conditions. Nat Commun 2020, 11, 3635, doi:10.1038/s41467-020-17374-3. [CrossRef]
- Gallagher, S.; Hughes, E.; Wagner, S.; Tshiaba, P.; Rosenthal, E.; Roa, B.B.; Kurian, A.W.; Domchek, S.M.; Garber, J.; Lancaster, J.; et al. Association of a Polygenic Risk Score With Breast Cancer Among Women Carriers of High- and Moderate-Risk Breast Cancer Genes. JAMA Netw Open 2020, 3, e208501, doi:10.1001/jamanetworkopen.2020.8501. [CrossRef]
- Gao, C.; Polley, E.C.; Hart, S.N.; Huang, H.; Hu, C.; Gnanaolivu, R.; Lilyquist, J.; Boddicker, N.J.; Na, J.; Ambrosone, C.B.; et al. Risk of Breast Cancer Among Carriers of Pathogenic Variants in Breast Cancer Predisposition Genes Varies by Polygenic Risk Score. Journal of clinical oncology : official journal of the American Society of Clinical Oncology 2021, 39, 2564-2573, doi:10.1200/JCO.20.01992. [CrossRef]
- Schreurs, M.A.C.; Ramón Y Cajal, T.; Adank, M.A.; Collée, J.M.; Hollestelle, A.; van Rooij, J.; Schmidt, M.K.; Hooning, M.J. The benefit of adding polygenic risk scores, lifestyle factors, and breast density to family history and genetic status for breast cancer risk and surveillance classification of unaffected women from germline CHEK2 c.1100delC families. Breast 2024, 73, 103611, doi:10.1016/j.breast.2023.103611. [CrossRef]
- Padrik, P.; Puustusmaa, M.; Tonisson, N.; Kolk, B.; Saar, R.; Padrik, A.; Tasa, T. Implementation of Risk-Stratified Breast Cancer Prevention With a Polygenic Risk Score Test in Clinical Practice. Breast Cancer (Auckl) 2023, 17, 11782234231205700, doi:10.1177/11782234231205700. [CrossRef]
- Mars, N.; Kerminen, S.; Tamlander, M.; Pirinen, M.; Jakkula, E.; Aaltonen, K.; Meretoja, T.; Heinävaara, S.; Widén, E.; Ripatti, S.; et al. Comprehensive Inherited Risk Estimation for Risk-Based Breast Cancer Screening in Women. Journal of clinical oncology : official journal of the American Society of Clinical Oncology 2024, 42, 1477-1487, doi:10.1200/JCO.23.00295. [CrossRef]
- Huntley, C.; Torr, B.; Sud, A.; Rowlands, C.F.; Way, R.; Snape, K.; Hanson, H.; Swanton, C.; Broggio, J.; Lucassen, A.; et al. Utility of polygenic risk scores in UK cancer screening: a modelling analysis. The Lancet. Oncology 2023, 24, 658-668, doi:10.1016/S1470-2045(23)00156-0. [CrossRef]
- Huntley, C.; Torr, B.; Sud, A.; Houlston, R.S.; Hingorani, A.D.; Jones, M.E.; Turnbull, C. The impact of risk stratification by polygenic risk and age on breast cancer screening in women aged 40-49 years: a modelling study. Lancet 2023, 402 Suppl 1, S54, doi:10.1016/S0140-6736(23)02103-7. [CrossRef]
- Tamm, M.; Padrik, P.; Paas, A.; Lepland, A.; Kruuv-Käo, K.; Sõber, S.; Roht, L.; Ojamaa, K.; Pajusalu, S.; Padrik, A.; et al. Implementation of Genetics-Based Precision Prevention in Breast Cancer: Results from the Estonian Arm of the BRIGHT Study. Poster P18.048.C. In Proceedings of the European Society of Human Genetics Conference, Berlin, 2024.
- Sawyer, S.; Mitchell, G.; McKinley, J.; Chenevix-Trench, G.; Beesley, J.; Chen, X.Q.; Bowtell, D.; Trainer, A.H.; Harris, M.; Lindeman, G.J.; et al. A role for common genomic variants in the assessment of familial breast cancer. Journal of clinical oncology : official journal of the American Society of Clinical Oncology 2012, 30, 4330-4336, doi:10.1200/JCO.2012.41.7469. [CrossRef]
- Bahcall, O. Common variation and heritability estimates for breast, ovarian and prostate cancers. Nature genetics 2013, doi:10.1038/ngicogs.1. [CrossRef]
- Allemani, C.; Matsuda, T.; Di Carlo, V.; Harewood, R.; Matz, M.; Niksic, M.; Bonaventure, A.; Valkov, M.; Johnson, C.J.; Esteve, J.; et al. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 2018, 391, 1023-1075, doi:10.1016/s0140-6736(17)33326-3. [CrossRef]
- Tuchler, A.; De Pauw, A.; Ernst, C.; Anota, A.; Lakeman, I.M.M.; Dick, J.; van der Stoep, N.; van Asperen, C.J.; Maringa, M.; Herold, N.; et al. Clinical implications of incorporating genetic and non-genetic risk factors in CanRisk-based breast cancer risk prediction. Breast 2024, 73, 103615, doi:10.1016/j.breast.2023.103615. [CrossRef]
- Precision-HBOC. Stratifying Risk for Early Detection in Hereditary Breast and Ovarian Cancer. Available online: https://www.hra.nhs.uk/planning-and-improving-research/application-summaries/research-summaries/precision-hboc/ (accessed on 08.06.2024).
- The benefits and harms of breast cancer screening: an independent review. Lancet (London, England) 2012, doi:10.1016/S0140-6736(12)61611-0. [CrossRef]
- Peintinger, F. National Breast Screening Programs across Europe. Breast care (Basel, Switzerland) 2019, 14, 354-358, doi:10.1159/000503715. [CrossRef]
- Evans, D.G.R.; Harkness, E.F.; Brentnall, A.R.; van Veen, E.M.; Astley, S.M.; Byers, H.; Sampson, S.; Southworth, J.; Stavrinos, P.; Howell, S.J.; et al. Breast cancer pathology and stage are better predicted by risk stratification models that include mammographic density and common genetic variants. Breast Cancer Res Treat 2019, 176, 141-148, doi:10.1007/s10549-019-05210-2. [CrossRef]
- Hurson, A.N.; Pal Choudhury, P.; Gao, C.; Husing, A.; Eriksson, M.; Shi, M.; Jones, M.E.; Evans, D.G.R.; Milne, R.L.; Gaudet, M.M.; et al. Prospective evaluation of a breast-cancer risk model integrating classical risk factors and polygenic risk in 15 cohorts from six countries. Int J Epidemiol 2022, 50, 1897-1911, doi:10.1093/ije/dyab036. [CrossRef]
- Lakeman, I.M.M.; Rodriguez-Girondo, M.; Lee, A.; Ruiter, R.; Stricker, B.H.; Wijnant, S.R.A.; Kavousi, M.; Antoniou, A.C.; Schmidt, M.K.; Uitterlinden, A.G.; et al. Validation of the BOADICEA model and a 313-variant polygenic risk score for breast cancer risk prediction in a Dutch prospective cohort. Genetics in medicine : official journal of the American College of Medical Genetics 2020, 22, 1803-1811, doi:10.1038/s41436-020-0884-4. [CrossRef]
- Vachon, C.M.; Scott, C.G.; Tamimi, R.M.; Thompson, D.J.; Fasching, P.A.; Stone, J.; Southey, M.C.; Winham, S.; Lindström, S.; Lilyquist, J.; et al. Joint association of mammographic density adjusted for age and body mass index and polygenic risk score with breast cancer risk. Breast Cancer Res 2019, 21, 68, doi:10.1186/s13058-019-1138-8. [CrossRef]
- Bolze, A.; Cirulli, E.T.; Hajek, C.; Schnell Blitstein, J.M.; Grzymski, J.J. The Potential of Genetics in Identifying Women at Lower Risk of Breast Cancer. JAMA oncology 2024, 10, 236-239, doi:10.1001/jamaoncol.2023.5468. [CrossRef]
- Tamm, M.; Padrik, P.; Ojamaa, K.; Paas, A.; Lepland, A.; Kruuv-Käo, K.; Leitsalu, L.; Sõber, S.; Roht, L.; Pajusalu, S.; et al. An implementation study of the service model for genetic risk-based stratified breast cancer screening – Estonian results of the BRIGHT project. medRxiv 2024, 2024.2010.2022.24315198, doi:10.1101/2024.10.22.24315198. [CrossRef]
- Sampaio, F.; Padrik, P.; Kruuv-Käo, K.; Lutsar, K.; Tõnisson, N.; Feldman, I. Cost-Effectiveness of a Polygenic Risk Score Based Breast Cancer Screening Program in Estonia. Poster P18.018.A. In Proceedings of the European Society of Human Genetics Conference, Berlin, 2024.
- Shieh, Y.; Eklund, M.; Madlensky, L.; Sawyer, S.D.; Thompson, C.K.; Stover Fiscalini, A.; Ziv, E.; Van't Veer, L.J.; Esserman, L.J.; Tice, J.A. Breast Cancer Screening in the Precision Medicine Era: Risk-Based Screening in a Population-Based Trial. J Natl Cancer Inst 2017, 109, doi:10.1093/jnci/djw290. [CrossRef]
- Lowry, K.P.; Geuzinge, H.A.; Stout, N.K.; Alagoz, O.; Hampton, J.; Kerlikowske, K.; de Koning, H.J.; Miglioretti, D.L.; van Ravesteyn, N.T.; Schechter, C.; et al. Breast Cancer Screening Strategies for Women With ATM, CHEK2, and PALB2 Pathogenic Variants: A Comparative Modeling Analysis. JAMA Oncol 2022, 8, 587-596, doi:10.1001/jamaoncol.2021.6204. [CrossRef]
- NCCN Clinical Practice Guidelines in Oncology. Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic. Version 3.2024. Available online: (accessed on 30.05.2024).
- Interdisziplinäre S3-Leitlinie für die Früherkennung, Diagnostik, Therapie und Nachsorge des Mammakarzinoms. Available online: https://register.awmf.org/assets/guidelines/032-045OLl_S3_Mammakarzinom_2021-07.pdf (accessed on.
- AGO Breast Cancer Risk, Genetics and Prevention. Available online: https://www.ago-online.de/fileadmin/ago-online/downloads/_leitlinien/kommission_mamma/2024/englisch/Einzeldateien_Literatur/AGO_2024E_02_Genetics_REF.pdf (accessed on 30.05.20204).
- Deutsches Konsortium Familiärer Brust- und Eierstockkrebs. Available online: https://www.konsortium-familiaerer-brustkrebs.de/ (accessed on 30.06.2024).
- Nasjonalt handlingsprogram med retningslinjer for diagnostikk, behandling og oppfølging av pasienter med brystkreft. Available online: https://www.helsebiblioteket.no/innhold/nasjonal-faglig-retningslinje/brystkreft-handlingsprogram (accessed on 30.05.2024).
- Sociedade Portuguesa de Oncologia. Available online: https://www.sponcologia.pt/web/home.php (accessed on 15.10.2024).
- Personaalmeditsiini juhtprojekti eeluuring. Available online: https://www.sm.ee/personaalmeditsiini-juhtprojekti-eeluuring (accessed on 30.08.2024).
- Estonian Health Insurance News. Eestis on Kanda kinnitamas uued sõeluuringud. Available online: https://www.tervisekassa.ee/uudised/eestis-kanda-kinnitamas-uued-soeluuringud (accessed on 05.06.2024).
- Regulation (EU) 2017/746 of the European Parliament and of the Council of 5 April 2017 on in vitro diagnostic medical devices. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX:32017R0746 (accessed on 30.06.2024).
Figure 1.
10-year risk of developing breast cancer according to woman’s age and PRS2803 percentile [44]. 99th percentile – red, 90th percentile – blue, population average – green. Population background is from breast cancer incidence data for Norway 2018-2020 (from Nordcan 2.0).
Figure 1.
10-year risk of developing breast cancer according to woman’s age and PRS2803 percentile [44]. 99th percentile – red, 90th percentile – blue, population average – green. Population background is from breast cancer incidence data for Norway 2018-2020 (from Nordcan 2.0).
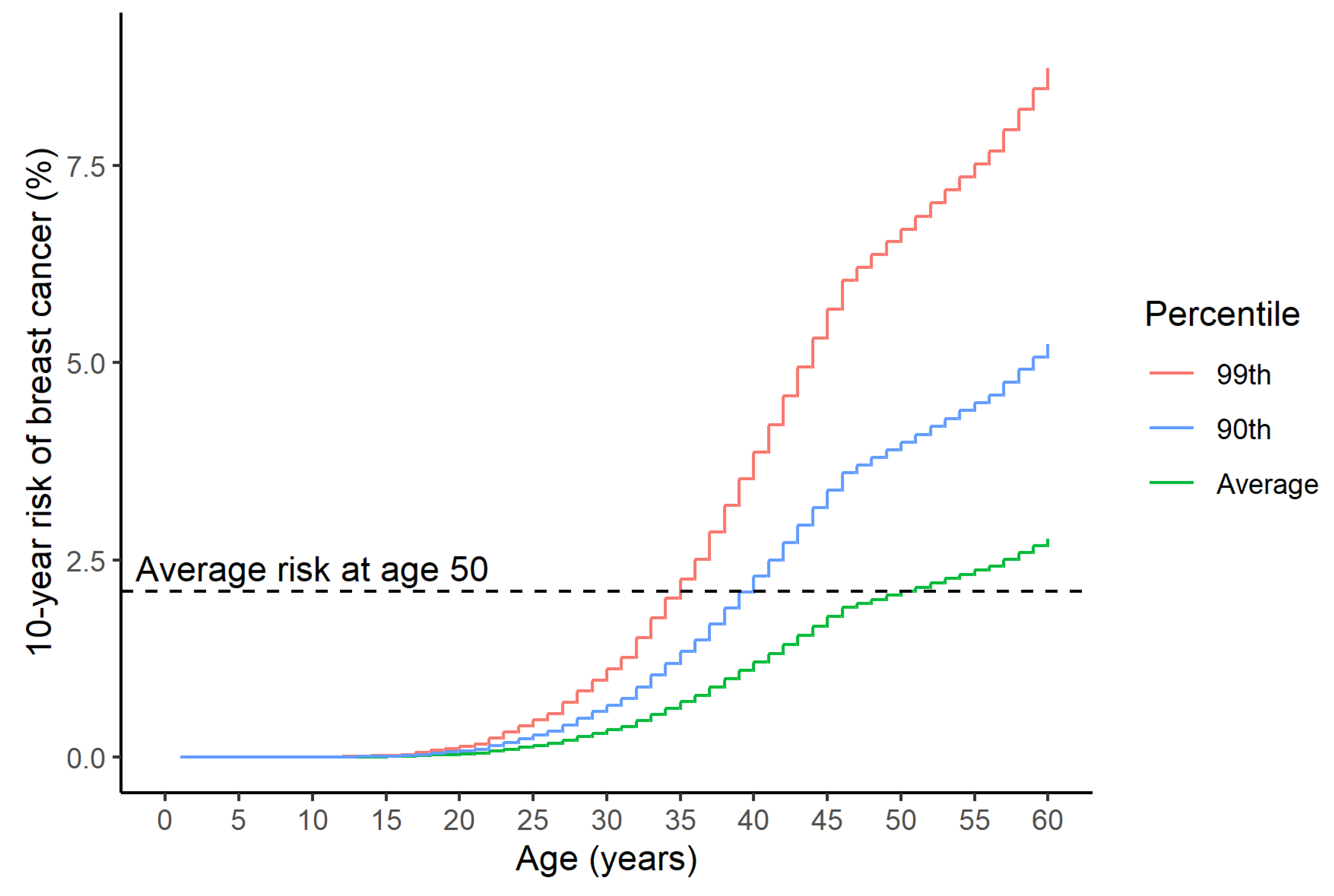
Figure 2.
Cumulative lifetime breast cancer risks of carriers of protein truncating pathogenic variants in breast cancer risk genes compared to women in PRS2803 upper decile (blue). Breast cancer risks of pathogenic variant carriers are from the analysis by the Breast Cancer Association Consortium [18]. Population background is from breast cancer incidence data for Norway 2018-2020 (from Nordcan 2.0).
Figure 2.
Cumulative lifetime breast cancer risks of carriers of protein truncating pathogenic variants in breast cancer risk genes compared to women in PRS2803 upper decile (blue). Breast cancer risks of pathogenic variant carriers are from the analysis by the Breast Cancer Association Consortium [18]. Population background is from breast cancer incidence data for Norway 2018-2020 (from Nordcan 2.0).
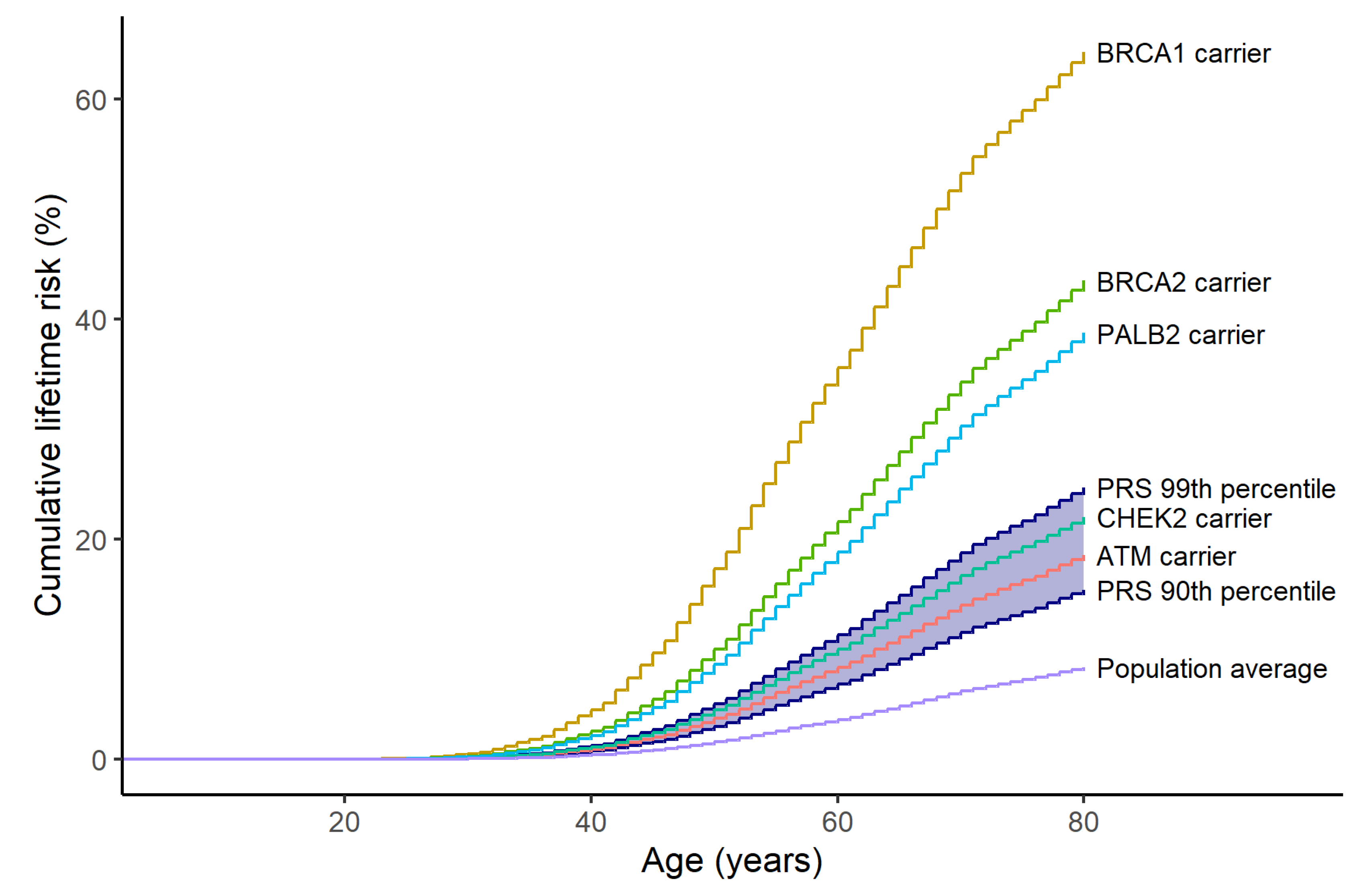

Table 1.
Breast cancer risk categories by the UK NICE guidelines [22].
Table 1.
Breast cancer risk categories by the UK NICE guidelines [22].
| Breast cancer risk category | |||
| Near population risk | Moderate risk | High risk | |
| Lifetime risk from age 20 | Less than 17% | 17% or greater but less than 30% | 30% or greater |
| Risk between ages 40 and 50 | Less than 3 % | 3-8% | Greater than 8% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



