
Submitted:
15 November 2024
Posted:
18 November 2024
You are already at the latest version
Abstract
Background/Objectives: Childhood trauma has a documented impact on development, which may also affect functioning and well-being in transition-age youth (TAY). There is a need to explore approaches, such as trauma-informed care (TIC), to enhance services provided during the transition to adulthood. The objective of this scoping review was to explore the extent of the literature on the potential of TIC for supporting TAY. Methods: We focused on initiatives grounded in TIC to support TAY between the ages of 14 and 25 who have histories of trauma. The search strategy involved nine databases and gray literature. The titles, abstracts and full text were screened in duplicate by reviewers, and then data were extracted. Results: A total of 19 references were included and classified into three categories: (1) importance of TIC to support TAY (k=5); (2) description of TIC initiatives (k=6); and (3) evaluation of TIC initiatives supporting TAY (k=2). Seven references were classified into more than one category. The references documented 10 TIC models or initiatives, half of which were evaluated and showed promising results. Important components of TIC initiatives supporting TAY included staff training and support; collaborative and multidisciplinary work; systemic changes; addressing trauma and its impacts; and a strength-based and youth-focused approach. Conclusions: Strengths, limitations, as well as future lines of work are discussed. Overall, the literature is emerging and needs to be expanded to ascertain the efficacy of TIC in supporting TAY. TIC is at least promising in terms of transforming services and supporting TAY with histories of trauma.
Keywords:
trauma-informed care
; transition to adulthood
; trauma
; foster care
; scoping review
1. Introduction
Adverse childhood experiences (ACEs), such as abuse, neglect, household dysfunction, poverty, and exposure to community violence or peer victimization, are undoubtedly common [1]. A meta-analysis from Madigan et al. [2] revealed that 66% of adults report they have had ACEs, and rates are even higher among child welfare or foster care samples [3,4]. Cyr et al. [4] found that 90% of children and youth in a child welfare sample disclosed at least one form of victimization and that 54% reported polyvictimization in the past year. Similarly, Collin-Vézina et al. [3] showed that half of youth in a foster care sample revealed that they had experienced four or more forms of maltreatment, as well as clinical levels of depression, anger, post-traumatic stress, and dissociation. Children and youth in child welfare or foster care may also experience system-induced trauma from being separated from family, friends and community; placement instability; or violence [5,6,7]. Thus, a proportion of children and youth, especially those in the child welfare or foster care systems, have histories of cumulative childhood trauma.
Childhood trauma is associated with mental health issues, social-emotional difficulties, cognitive and language problems, educational challenges, as well as difficulties related to identity and self-esteem throughout development, including during the transition to adulthood (TA) [8,9,10,11,12,13]. The TA is a developmental period characterized by change, exploration and challenges in multiple interrelated aspects of development and functioning, when the ultimate goal is to achieve autonomy [14,15,16]. Trauma has a documented impact on development, which may also affect functioning and well-being in transition-age youth (TAY) [13,17,18,19,20,21]. Involvement in the child welfare or the foster care systems could impact the TA because of the reduction or cessation of services combined with the lack of social support from family, friends, and community that is documented among youth exiting those systems (i.e., aging out of care) [22].
1.1. TA Outcomes Among Trauma-Exposed Youth
Studies indicate that trauma-exposed TAY – including those in the child welfare or foster care systems – have poor outcomes in multiple aspects of functioning, including education and employment, economic and living situation, and mental health and social functioning [18,19,20,23,24]. For example, youth with child welfare involvement are found to have poorer educational outcomes than youth from the general population [20] or youth from low-income backgrounds [25]. A study of over 63,000 high school students revealed that youth with child welfare involvement had lower rates of high school completion and college enrollment, poorer educational performance, and greater academic challenges (i.e., special education–qualifying disabilities, school district changes, underperforming school districts) than youth from low-income backgrounds with no child welfare involvement [25]. A review showed that 38% to 83% of former foster youth have a high school diploma, 28% to 56% enroll in post-secondary education, and 17% to 49% are not in education, employment, or training [20]. Notably, when these youth are employed, the jobs are likely to be less stable with lower pay and to require low qualifications [18,20,23]. Thus, trauma-exposed youth show overall poor educational and employment outcomes.
Economic hardship and stress due to educational or employment challenges may in turn impact living situation and mental health, and conversely, homelessness, housing instability and mental health problems may cause additional educational and employment challenges [23]. Not having a high school diploma, having low educational attainment, and being unemployed have been found to be critical risk factors for homelessness, housing instability, and mental health issues [18,23,26]. A prospective longitudinal study of more than 2,500 foster youth showed that one-third experienced at least one episode of homelessness and that one-fifth experienced housing instability at age 21 [27]. This study also showed that 32% (age 17) and 39% (age 19) of them reported mental health issues, including depression, anxiety, attention deficit hyperactivity disorder symptoms, or suicidal behaviors [28].
In sum, trauma-exposed youth and, to a greater extent, youth with involvement in the child welfare or foster care systems are at risk of poor TA outcomes in terms of multiple interrelated aspects of development and functioning [29], hence the need to explore initiatives aimed at supporting the TA of these youth.
1.2. Services and Programs Aiming to Support the TA
A systematic review of eight studies on the effects of services and programs aiming to support the TA yielded mixed results [30], while a meta-analysis of eight studies showed that they had significant but small effects on outcomes related to education, employment, and living situations [31]. Program differences and methodological limitations somewhat precluded comparisons and the drawing of conclusions about the effects of the services and programs studied in this review and meta-analysis [30,31,32]. The most present and empirically supported initiatives include services and programs providing youth support past the age of majority [17,20,23,30,33,34,35]. However, they are not consistently available in the child welfare or the foster care systems [20,30,31,33], and it is agreed that services should aim to prepare youth to TA early, well before they reach the age of majority or exit the child welfare or foster care systems [20]. Thus, existing services or programs – when available – may not be sufficient to fully support TA outcomes among youth with histories of trauma, highlighting the need to explore complementary approaches, such as trauma-informed care, to enhance services [17].
One limitation of the programs and services reviewed is that they do not formally or specifically acknowledge and respond to trauma and its impact. Given that childhood and system-induced trauma may impact functioning and well-being during the TA, services and programs aiming to support education and employment, economic and living situation, or mental health and social functioning in TAY should address trauma [17,18,19,20]. Trauma-informed care (TIC) is a promising approach that may address this limitation.
1.3. Trauma-Informed Care
TIC involves systemic changes in both organizational policies and clinical practices to “realize the widespread impact of trauma and understand potential paths for recovery; recognize the signs and symptoms of trauma in clients, families, staff, and others involved with the system; and respond by fully integrating knowledge about trauma into policies, procedures, and practices, and seek to actively resist re-traumatization” [5] (p. 9). While inclusive of trauma-focused interventions emphasizing the assessment and treatment of trauma symptoms, TIC integrates six principles (safety; trustworthiness and transparency, peer support; collaboration and mutuality; empowerment; and cultural, historical, and gender issues) into policies, procedures, and practices to respond to the needs of individuals with histories of trauma [5]. As such, by acknowledging and responding to trauma and its impact (e.g., mental health issues, socio-emotional difficulties, cognitive and language problems, and difficulties related to identity and self-esteem), a trauma-informed lens creates the opportunity to understand and respond to the needs of youth to support them in multiple aspects of development and functioning, and in turn, improve their education and employment, economic and living situation, and mental health and social functioning outcomes during the TA. As such, TIC is believed to be a promising avenue for supporting the TA [20].
A meta-analysis showed TIC interventions have significant and moderate effects on trauma symptoms, behaviors, and well-being in children and youth [36] . Several studies on trauma-exposed TAY recommend TIC [e.g., [21,37,38,39]], and the Child Welfare League of Canada [35] affirms that foster youth must have the right to receive TIC interventions. The Child Welfare League of Canada also identified eight pillars that support the TA of foster youth. The pillars (education, employment, basic needs, social support and relationships, conduct and victimization, health and well-being, general living skills, and resilience and psychological empowerment) align with TIC principles and are corroborated in the literature as targets for supporting the TA [5,32,40]. While there is growing recognition and implementation of TIC across child welfare and foster care systems [41], most initiatives do not specifically aim to support the TA, although some programs or services are available. A preliminary search of databases was conducted, and no ongoing or available review of such initiatives was identified. This scoping review was therefore undertaken to fill this gap in knowledge and explore the extent of the literature on the potential of TIC to support the TA of trauma-exposed youth. The research questions were as follows:
- What are the existing needs and TIC approaches to specifically support the TA of trauma-exposed youth?
- What are the effects of implementing TIC approaches?
2. Materials and Methods
This scoping review was conducted following the JBI methodology for scoping reviews [42], as well as the PRISMA extension for scoping reviews [43].
2.1. Eligibility Criteria
2.1.1. Participants
The review focused on TAY with histories of trauma. The review adopted an inclusive approach and targeted all youth with child welfare or foster care involvement, or with histories of ACEs or interpersonal traumatic events. Although youth aging out of the child welfare or foster care systems may face additional challenges [22], experiencing childhood trauma in itself is likely to affect the TA so all youth with histories of trauma could require TA support and therefore were considered [17,21]. Thus, to be included in the review, references had to target youth who have been exposed to ACEs or interpersonal traumatic events (e.g., abuse, neglect, household dysfunction, poverty, peer victimization, peer isolation/rejection, and community violence exposure) or who are or have been involved with the child welfare or foster care systems. Non-interpersonal traumatic events (e.g., natural disasters, traumatic brain injuries) or war were not considered in this review to ensure a degree of homogeneity and because the impacts and mechanisms involved in those cases are somewhat different [44].
The age range for the TA period varies across studies and authors. Arnett [14] identifies emerging adulthood as the late teens to the early twenties (18 to 25 years old), whereas the Spinelli et al. [21] sample of TAY includes those aged 14 to 21 years old. Again, we adopted a more inclusive approach, and, as a general rule, we focused on youth between the ages of 14 and 25 years old. This general age band is in line with the acknowledgement that services should aim to prepare youth for the TA before they reach the age of majority, and that the TA period may exceed the twenties. Participants could be youths or other persons involved with TAY with histories of trauma (e.g., researchers, policy-makers, practitioners, service providers).
2.1.2. Concept
References had to focus on outcomes related to education and employment, economic and living situation, or mental health and functioning during the TA.
2.1.3. Context
References also had to focus on services, programs or initiatives grounded in TIC, whether they highlighted the need for a TIC approach to support the TA, described a TIC approach aimed at supporting the TA or evaluated a TIC approach. We used the Substance Abuse and Mental Health Services Administration’s (SAMHSA) definition of TIC in which TIC involves systemic changes in both organizational policies and clinical practices to “realize the widespread impact of trauma and understand potential paths for recovery; recognize the signs and symptoms of trauma in clients, families, staff, and others involved with the system; and respond by fully integrating knowledge about trauma into policies, procedures, and practices, and seek to actively resist re-traumatization” [5] (p.9). When a reference included an intervention focusing on the assessment and treatment of trauma symptoms (e.g., trauma-focused cognitive-behavioral therapy [TF-CBT]) [45], it was included only if the intervention was part of a wider implementation of TIC aimed at changing organizational policies and clinical practices. Otherwise, it was not included.
2.2. Types of Sources
This scoping review did not limit study design (e.g., observational, cross-sectional, program evaluation) or methods (qualitative, quantitative, mixed, review) to broadly explore the extent of the literature on the topic. Previous reviews that met inclusion criteria were considered, as well as text and opinion papers and other types of references (e.g., websites, conference proceedings, government or organization documents). Only documents in English or French were included, and only one study was excluded because of language [46]. A date limit was not applied because a previous review has not been done on the topic.
2.3. Search Strategy
The goal of the search strategy was to locate both published and unpublished documents and other types of references. A preliminary search of PsycINFO (Ovid) was undertaken to identify articles on the topic. Words in titles and abstracts, keywords, and index terms of the relevant articles identified through this preliminary search were used to develop the search strategy for PsycINFO (Ovid) with the assistance of a university librarian (see supplementary material, Table S1 for the search strategy for PsycINFO). The search strategy was then adapted to eight other databases: Medline (Ovid), ERIC (ProQuest), PTSDpubs (ProQuest), Sociological Abstracts (ProQuest), Social Services Abstracts (ProQuest), Social Sciences Abstracts (EBSCOhost), Social Work Abstracts (EBSCOhost and Ovid), and CINAHL Plus with Full Text (EBSCOhost). The search was first conducted in the summer of 2022 and then updated in July 2023.
The reference list of all included sources of evidence was screened for additional references. A search of relevant sources that cited the included references was also done. Unpublished or gray literature was searched using keywords in Analysis & Policy observatory, Information for practice news, new scholarship & more from around the world, OpenAIRE, Publications of the Government of Canada, Policy Commons, Intergovernmental Organization Search Engine – Google, Non-governmental Organization Search Engine – Google, Bielefeld Academic Search Engine, and Google Scholar.
2.4. Sources of Evidence Selection
All references were uploaded into Covidence, a platform that streamlines evidence synthesis with a gold standard process [47]. Duplicates were removed. Titles and abstracts were screened in duplicate by three independent reviewers using the eligibility criteria. The reviewers were two social sciences undergraduates and one graduate student working closely with the principal investigator who specializes in trauma and TIC. The full texts of relevant references were then retrieved and imported into Covidence. Similarly, the full texts were assessed in duplicate by two of the three independent reviewers. Any disagreements between the reviewers at each stage of the selection process were resolved through discussion with the principal investigator. Reasons for exclusion were recorded at each stage. The results of the search and the selection process are reported in a flow diagram (see Figure 1) in the Results section. The search yielded 4320 references (2748 duplicates removed), from which a total of 19 were included. The inter-rater reliability indices indicated quasi-substantial agreement for title and abstract screening (ĸ = .59) and full-text assessment (ĸ = .56) [48].
2.5. Data Extraction
Data were extracted by two reviewers using a tool adapted from the tool provided by Covidence (supplementary material, Table S2). It was adjusted to suit the objective and research questions. The draft adapted tool was pre-tested and then revised to allow information about the following to be extracted: context of the work (e.g., country, type of document, aim), methods (e.g., data collection, sample description, outcome measurement), definitions of main concepts (TIC, ACEs/trauma, TA), analyses, results, limitations, and the TIC services, programs or initiatives. Data extraction was verified by the principal investigator.
2.6. Data Analysis and Presentation
References were classified into three categories based on aim and content: (1) need for or importance of a TIC approach to support the TA; (2) description of a TIC approach aimed at supporting the TA; (3) or the evaluation of a TIC initiative. These categories reflect the usual sequence of program development, implementation and evaluation.
3. Results
3.1. Description of Included References
A total of 19 references were included in this scoping review (see Figure 1). About a third were peer-reviewed articles (k=6), while most were gray literature, including reports (k=4), dissertations (k=3), government or organization documents (k=3), conference proceedings (k=2), and a book chapter (k=1). Most of the work was carried out in the United States (k=12), while the rest originated from Canada (k=3), Australia (k=2), the United Kingdom (k=1) or were international (k=1). The earliest reference dates from 2012, while the most recent is from 2021. As stated above, references included were classified into three categories: (1) need for or importance of a TIC approach to support the TA (k=5); description of TIC practices and policies aimed at supporting the TA (k=5); (3) the evaluation of a TIC initiative (k=2); with some references classified into more than one category (k=7). Table 1 summarizes by category key details about and objectives and methods of included references. Note that information included in Table 1 is based on the information provided in the references, as well as on the category of the document.
3.1.1. Need for or Importance of TIC
References in this category prioritized qualitative (k=4) or mixed methods (k=1) to highlight the importance of or need for a TIC approach to support the TA of youth with histories of trauma. In the qualitative studies [49,50,51,52] youth, service providers and key stakeholders were consulted through photovoice, interviews and focus groups. A last reference in this category was a review [49]. As for the mixed method study [53], an online survey including self-report questionnaires and open-ended questions was administered to service providers working with TAY to assess the providers’ training needs.
3.1.2. Description of Practices and Policies
A total of five references described TIC practices and policies for supporting the TA of youth. While some references presented models or adaptations of models grounded in TIC (Housing First for youth [54]; Therapeutic Family Model of Care [TFMC] [55]; Families Over Coming Under Stress [FOCUS] [56]), others identified trauma-informed principles or guidelines to support the TA of youth [57]. One reference reviewed models that support policy and practice related to youth aging out of care, with some including TIC principles [58].
3.1.3. Evaluation of TIC
One mixed method and one quantitative study assessed the effects of TIC implementation. The mixed method study [59] conducted a three-year evaluation of the LEADS (Learn – Educate – Achieve – Dream – Succeed) program to describe the characteristics and perceptions of the youth served, the types of services provided, the factors associated with success, and the TA outcomes. The quantitative study [60] used census data from the Detroit Jobs for Michigan Graduates (JMG) program to assess youth’s educational and employment achievements at three points (at intake, and during and after the program). JMG comprises three different programs, including LEAP (Learn and Earn to Achieve Potential), which advances a TIC approach.
3.1.4. Importance, Description and Evaluation of TIC
Seven references using qualitative (k=1), mixed (k=3) or other types of methods (k=3), pertained to more than one of the above reference categories. To promote the TA for youth aging out of care, Harder et al. [61] proposed principles grounded in TIC from a qualitative process that considered implications for practice as well as research support. Similarly, a critical review of data and a consultation of stakeholders [62] led to the identification of best practices (which included trauma-informed ones) to support the TA of youth. One mixed method study consulted youth through surveys, interviews, and focus groups to underline the importance of a TIC approach for supporting the TA and to evaluate youth’s experiences and outcomes [63]. Another mixed method study used surveys and focus groups to consult youth and service providers; assess needs, strengths, barriers and strategies while coping with trauma; and document the implementation of a TIC approach and its most effective components [64]. The other mixed method study surveyed and interviewed staff to assess the development and implementation of the Trauma Recovery Model (TRM) [65]. Finally, the study on the LEAP initiative, which involved interviewing youth and reviewing program participation and financial data, described the implementation of the initiative, youth engagement and perspectives, and program costs [66,67].
3.2. Results of Included References
Supplementary material, Table S3 presents the main results from the included references. This section synthesizes results and focuses on findings relevant to the research questions.
3.2.1. Evidence of the Importance of or Need for TIC to Support the TA
Although the included references indicated that services aimed at supporting the TA need to be trauma-informed, Harder et al. [61] highlighted that TIC may not be present enough in services, and that staff need trauma-informed training, support and supervision, which is in line with other accounts [53]. While youth indicated that service providers could benefit from training [64], service providers also communicated training needs related to culture, behavioral and mental health, and youth support and empowerment [53]. Other studies underlined training needs related to trauma, its triggers and its impact [49,64], and to culturally adapted [50], and intersectionally focused services [51]. Butters [62] and Harder et al. [61] highlighted the importance of changes at the organizational and systemic level. Schubert [52] indicated that organizational changes could involve the presence of reference people within organizations to provide information and support through a trauma-informed lens.
The reviewed references highlighted the TA-related needs of youth with histories of trauma and indicated that a TIC approach could be a promising avenue for responding to those needs. The evidence showed that youth could benefit from extended services, collaboration between organizations, a strength-based approach, and support towards education, employment, housing, etc. [49,50,51].
3.2.2. Description of Existing TIC Practices and Policies Supporting the TA
A few services, programs and initiatives grounded in TIC are described in the literature, although they have not been assessed. Those initiatives are reviewed here as they may provide guidance on practices and policies that may support the TA of trauma-exposed youth. Three references aimed to identify principles or recommend best practices [57,61,62]. Butters [62] recommended that practices should be trauma-informed to acknowledge the interrelation between trauma and its impact, and to facilitate recovery [62]. Harder et al. [61] underlined 10 principles for promoting the successful TA of youth aging out of care (e.g., access to education, relationship continuity and safety nets, working through trauma, ensuring access to services). Six supplementary principles were highlighted by Kisiel et al. [57], including understanding trauma and its impact on youth and service providers (secondary traumatic stress).
The review of the Child Protection Project Committee [58] identified at least two models including TIC principles (i.e., The New Zealand’s Oranga Tamariki/Ministry for Children’s policy and The Independent Youth Housing Program). The models adopted were strength-based and described as trauma-informed, youth-centered, holistic and culturally adapted. The Independent Youth Housing Program, an evidence-based program, offers services ranging from rental assistance and case management to helping youth with housing and independence through a trauma-informed lens [58].
Three other models were described [54,55,56]. The first, Housing First for Youth, is used as a philosophy or a guideline by organizations working with homeless TAY [54]. It is based on TIC and aims to support youth with health and well-being by prioritizing awareness and understanding of trauma, and by responding to it at a systemic level (including the organizational structure, the treatment framework, and ongoing training). The second, the TFMC, was developed to assist TAY with histories of trauma with education, employment, development, social relationships and well-being [55]. It focuses on relationships between youth and carers to help youth develop interpersonal relationships and skills. The third, the FOCUS model, is a resilience-based model that assists foster families and youth in college with family functioning and routines, mental health, social skills, and understanding reactions to stress [56]. Thus, the TIC initiatives reviewed in this section, although they have not been assessed, aim ultimately to support the TA of youth with histories of trauma.
3.2.3. Results of Evaluations of TIC Practices and Policies
The results of some evaluations provided information on implementation and on youth’s and staff’s perceptions. LEAP (Jobs for America’s Graduates [JAG] and Back on Track [BoT]) seeks to address trauma in youth and help them get a high school equivalency or a job, gain life skills and create a support system. The evaluation of LEAP implementation revealed a few takeaways for implementing TIC initiatives: find and retain staff to whom youth can relate; partner with organizations as a recruitment strategy for youth and as a way to connect them to services; and flexibility when delivering programs to promote youth engagement [66,67].
The TRM, anchored in attachment, trauma, criminology, and neurology, identifies and addresses with a trauma-informed lens the needs of TAY aging out of care by establishing connections between youth and agencies and ensuring staff understand trauma and its impact. Staff perceived that it helped youth develop confidence and self-esteem, think independently and improve their life skills [65]. While staff found the TRM helped, they mentioned they lacked confidence in applying the model, which underscores the importance of training, according to Baker and Barragan [65].
As for staff training, staff expressed that time for reflection, open dialogue and awareness of ‘success stories’ are important [64]. Staff suggested that the following themes should also be part of trauma-informed training: understanding triggers, conflict resolution skills and positive coping mechanisms, supporting self-regulation, de-escalation techniques, communication, staff burnout considerations, vicarious trauma, and self-care [64]. Furthermore, staff found that techniques shared during TIC training for supporting self-regulation and de-escalation were effective [64].
Effects of TIC initiatives on TA outcomes and costs. First, the evaluation of the LEADS program indicated that intensive services positively influenced educational progress and academic success in youth [59]. Similarly, the two evidence-based models from the LEAP initiative revealed positive effects on youth’s educational and social functioning outcomes. More precisely, youth participating in BoT showed an increased likelihood of pursuing post-secondary education, while those involved in JAG had an increased understanding of career pathways and job credentials [66,67]. As such, most youth involved in JAG (76%) engaged in school or work in the first six months of the follow-up phase, and some obtained high school credentials. In addition, results indicated that JAG helped youth create a support system and gain life skills [66,67].
Assessment of transitional living programs (TLPs) based on the Sanctuary model, a trauma-informed organizational approach [68], revealed positive results in terms of educational and employment outcomes in youth, but findings were very mixed for mental and social functioning [63]. Over a six-month period, participating youth’s scores trended upward on the Achenbach System of Empirically Based Assessment (ASEBA) Adaptive Functioning scales for jobs and friends, and their positive perceptions of community living environments increased. Most youth involved in TLPs reached their employment, housing, and financial goals towards the end of the six-month study [63]. However, the assessment of the TLPs also showed an increase in social withdrawal symptoms and increasing trends for substance use and for all ASEBA DSM-oriented scales – though they remained in the normal range – except for the depression symptoms scale for which a decreasing trend was observed over the six-month period studied [63]. Lastly, only one study evaluated the costs of a TIC initiative (LEAP) that supports the TA. The estimated cost for all phases ranged from $5,300 and $7,300 per youth [66,67]. However, costs could not be compared with those of other initiatives, and cost-benefit or cost-effectiveness was not evaluated.
4. Discussion
The objective of this scoping review was to explore the extent of the literature on the potential of TIC to support the TA of trauma-exposed youth. We identified 19 references (1) highlighting the need for or importance of a TIC approach to support the TA; (2) describing TIC practices and policies supporting the TA; and (3) evaluating TIC initiatives supporting the TA. We propose a schematic figure to summarize the extent of the literature on the topic (see Figure 2). References documented a total of 10 models or initiatives, half of which underwent evaluation. We also noted recurrent or important components of TIC initiatives aimed at supporting the TA: staff training and support; collaborative and multidisciplinary work; systemic and organizational changes; acknowledgment of the interrelation between trauma and its impacts; and a strength-based and youth-focused approach, which are discussed below. While the review gives an overview of current empirical knowledge on the potential of TIC for supporting the TA, it also points out future lines of work.
4.1. Acknowledging and Responding to Trauma
The reviewed literature strongly supports that acknowledging and responding to trauma is essential [57]. TAY [50,51,56,63], foster families [56] and service providers [52,53,56] report there is a need for trauma-informed services and programs to support the TA [54,61,62], despite the fact they may not be widely available (Harder et al., 2020). Many of the included references indicate that youth need to receive services that acknowledge the interrelation between trauma and its impacts on development and functioning and that treat trauma symptoms in a way that is developmentally sensitive, strength-based and youth-focused [50,51,56,63,65]. This could, in turn, positively support education and employment; economic and living situation; and mental health and social functioning during the TA [19,20]. Moreover, given that TIC actively seeks to resist re-traumatization, it could prevent or reduce system-induced trauma.
4.2. The Definition of TIC and Its Systemic Nature: Strengths and Challenges
Although the SAMHSA’s definition of TIC is widely accepted, we uncovered that, while services and programs may define themselves as trauma-informed, TIC may be inconsistently applied. In addition, it may include a variety of components or principles, making it complex to define and operationalize within the context of the TA, although the review led to the identification of “core” components in Figure 2, one of which is the systemic nature of TIC. Although this systemic nature may create challenges when it comes to operationalizing TIC into models and programs [69,70,71], the reviewed references emphasize that organizational changes are key to the systemic nature of TIC and important for supporting the TA of trauma-exposed youth [54,59,61,62]. Systemic and organizational changes in the context of TIC would notably encompass collaborative and multidisciplinary work [63,66,67]. The references reviewed highlighted the importance of collaboration and partnerships among stakeholders [62,67] and among different types of organizations (e.g., education and housing organizations, institution and community organizations) [49]. Partnerships could help to connect youth with services [49]. Accordingly, a review of scoping reviews [72] indicated that trusting relationships and partnerships between youth and service providers, and between service providers, are key to successful TIC initiatives. Yet, trusting service providers is a challenge for youth who have experienced system-induced trauma. Phillips et al. [7] add that multidisciplinary work is best suited to addressing youths’ complex and multiple needs related to childhood trauma. Thus, although the references reviewed bring attention to the importance of systemic and organizational changes, notably through collaborative and multidisciplinary work, they also acknowledge the challenges it poses for operationalization and therefore for evaluation [54,59,61,62,65].
4.3. Implementation of TIC Initiatives Through Staff Training and Support
We reviewed 10 TIC models or programs that aimed to support the TA of trauma-exposed youth, as well as three documents outlining principles or recommendations for best practices [57,61,62]. Most models and programs involved some type of staff training to support implementation [e.g., [54,58,656667]]. This is typical in the field [6,69,70,71,73] and, interestingly, could further support collaborative work and partnerships [72]. This review provides indications of what and how staff training could eventually support the TA of trauma-exposed youth. Moreover, in addition to staff training, the importance of ongoing training, supervision and support is highlighted in many of the references reviewed [52,53,61], as well as in previous reviews on TIC [69,70].
4.4. Effects of TIC Initiatives
While we reviewed 10 TIC models of programs, half of them were not evaluated and those that were evaluated only once [59,60,63,65,66,67]. Therefore, at the moment, there is no one TIC model or program that is deemed effective or recommended for supporting the TA of trauma-exposed youth based on our review. Rather, models and programs show positives and promising effects on TA outcomes, and we have identified key components that were found to be important (see Figure 2). Studies indicate positive effects on youth outcomes related to education and employment and, to a lesser extent, to economic and living situation, and mental health and social functioning. Implementation initiatives also resulted in positive effects on professional knowledge, attitudes and practices [65]. However, some of the models and programs that have been evaluated revealed some mixed findings [66,67]. Results of evaluations are to be considered in light of the fact that implementation of TIC initiatives is seldom described or assessed. This makes it difficult to determine whether mixed findings reflect the actual efficacy of the programs or services evaluated, or stem from issues with implementation.
4.5. Strengths, Limitations and Future Directions
This review drew upon a recent and comprehensive literature search (including gray literature and nine databases). The extensive search for gray literature yielded 43 additional references, of which eight were included, thus the search for gray literature was deemed crucial in this review to increasing our pool of references, to broadening our scope, and to incorporating available empirical knowledge on TIC within the context of TA. Despite its innovative research questions and strengths (e.g., search strategy, gray literature search, duplicate screening), this scoping review also has limitations. It does not include an assessment of the methodological quality of the references, though this assessment is typically not expected in scoping reviews [42,43]. While screening was performed in duplicate, extraction was not. However the tool was pre-tested, and the extraction was verified by the principal investigator in accordance with Pollock et al. [74].
The included references present strengths and limitations as well, giving indications for future studies on the topic. Some references relied on alternative methods to explore the potential of TIC for supporting the TA (e.g., formulation of principles, clinical perspective) [56,57,61], and most did not adopt quasi-experimental or experimental design, precluding any initial affirmations on the efficacy of TIC to support the TA. Although some studies were not experimental, they included repeated measures of outcomes [63,66,67], and the outcomes considered were multidimensional – education, life skills, employment, housing, sense of community – which is in accordance with the TA literature and reiterates the importance of multidisciplinary work when working with TAY.
We observed that some types of methods were more common for some reference categories. References discussing the importance of or need for TIC were mostly qualitative (none was solely quantitative); those describing practices or policies were mostly descriptive only; and references that assessed TIC initiatives were mostly mixed (none was solely qualitative). Although qualitative and quantitative methods are expected and deemed appropriate for exploring TAY’s needs and assessing initiatives, respectively, one can argue that we only have a partial account of the phenomena. We also note small samples, notably in references using qualitative methods. Although some of the studies relying on quantitative methods included large samples, information provided on methods or outcomes were very limited in some cases [e.g., [59]].
Most of the work reviewed was recent but mainly from the U.S., which limits the generalization of findings for other socio-cultural contexts where systems and policies for TAY are different. Studies conducted in a variety of socio-cultural contexts are paramount, given that the TA is influenced by the context in which it occurs [75,76]. Overall, the literature would benefit from adopting quasi-experimental or experimental design, increasing sample sizes in studies, and providing detailed information on methods and results, as well as on TIC operationalization and implementation. Implementation and results of programs could be evaluated using the Bargeman et al. [77] term “intervention methodology” to specify to what extent they could be effective or recommended for supporting the TA of trauma-exposed youth.
In conclusion, it is interesting to note that the main findings from this review are, overall, in line with the key components of successful TIC implementation in youth settings identified by Bryson et al. [69] in a systematic review, that is: (1) the importance of organizational leadership; (2) the need to support staff; (3) the relevance of listening to individuals and families; (4) the importance of reviewing data and outcome towards improvement; and (5) the need to align policy and practice. Our findings in the context of TA echo these components, though the importance of families and data and outcome review are themes that are less present in the reviewed references. This review shows that the literature on the potential of TIC for supporting the TA is emerging and needs to be expanded to ascertain the efficacy of TIC for this specific purpose. At the moment, TIC is at least promising in terms of transforming services and supporting trauma-exposed youth through the challenges they face during the TA.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Search strategy for PsychINFO (Ovid); Table S2: Data extraction tool; Table S3: Main results of included references.
Author Contributions
Conceptualization, A. Matte-Landry and V. Fournier; methodology, A. Matte-Landry and V. Fournier; validation, A. Matte-Landry; formal analysis, A. Matte-Landry, A. Lemire-Harvey and A. de Serres-Lafontaine; investigation, A. Lemire-Harvey; resources, A. Matte-Landry; data curation, A. Lemire-Harvey; writing—original draft preparation, A. Matte-Landry, A. Lemire-Harvey and A. de Serres-Lafontaine; writing—review and editing, all; supervision, A. Matte-Landry; project administration, A. Matte-Landry.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Contact the corresponding author for data supporting reported results.
Acknowledgments
We acknowledge the contribution of the Centre de recherche universitaire sur les jeunes et les familles (CRUJeF) for hiring undergraduate student, Noémie Girard-Bouchard, who contributed to the investigation and data curation. We thank Noémie Girard-Bouchard for her interest in and contribution to this work. We extend our gratitude to Maxime Pedneault, a clinical professional working with TAY, and Marie Dumollard, assistant professor at Université de Montréal, for their insightful comments and suggestions on previous versions of this manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
| 1 | Both references were included on the same line because they were related to the same evaluation. |
References
- Finkelhor, D.; Shattuck, A.; Turner, H.; Hamby, S. A Revised Inventory of Adverse Childhood Experiences. Child Abuse Negl., 2015, 48, 13–21. [Google Scholar] [CrossRef]
- Madigan, S.; Deneault, A.-A.; Racine, N.; Park, J.; Thiemann, R.; Zhu, J.; Dimitropoulos, G.; Williamson, T.; Fearon, P.; Cénat, J. M.; et al. Adverse Childhood Experiences: A Meta-Analysis of Prevalence and Moderators among Half a Million Adults in 206 Studies. World Psychiatry, 2023, 22, 463–471. [Google Scholar] [CrossRef] [PubMed]
- Collin-Vézina, D.; Coleman, *!!! REPLACE !!!*; Milne, L.; Sell, J.; Daigneault, I. Trauma Experiences, Maltreatment-Related Impairments, and Resilience Among Child Welfare Youth in Residential Care. Int. J. Ment. Health Addict., 2011, 9, 577–589. [Google Scholar] [CrossRef]
- Cyr, K.; Chamberland, C.; Lessard, G.; Clément, M.-È.; Wemmers, J.-A.; Collin-Vézina, D.; Gagné, M.-H.; Damant, D. Polyvictimization in a Child Welfare Sample of Children and Youths. Psychol. Violence, 2012, 2, 385–400. [Google Scholar] [CrossRef]
- Substance Abuse and Mental Health Services Administration. SAMHSA’s Concept of Trauma and Guidance for a Trauma-Informed Approach.; Substance Abuse and Mental Health Services Administration, 2014; p 27.
- Matte-Landry, A.; Collin-Vézina, D. Restraint, Seclusion and Time-out among Children and Youth in Group Homes and Residential Treatment Centers: A Latent Profile Analysis. Child Abuse Negl., 2020, 109, 104702. [Google Scholar] [CrossRef] [PubMed]
- Phillips, A. R.; Hiller, R. M.; Halligan, S. L.; Lavi, I.; Macleod, J. A. A.; Wilkins, D. A Qualitative Investigation into Care-Leavers’ Experiences of Accessing Mental Health Support. Psychol. Psychother. Theory Res. Pract., 2024, 97, 439–455. [Google Scholar] [CrossRef]
- Haahr-Pederson, I.; Ershadi, A. E.; Hyland, P.; Hansen, M.; Perera, C.; Sheaf, G.; Bramsen, R. H.; Spitz, P.; Vallières, F. Polyvictimization and Psychopathology among Children and Adolescents: A Systematic Review of Studies Using the Juvenile Victimization Questionnaire. Child Abuse Negl., 2020, 107. [Google Scholar] [CrossRef]
- Lund, J. I.; Toombs, E.; Radford, A.; Boles, K.; Mushquash, C. Adverse Childhood Experiences and Executive Function Difficulties in Children: A Systematic Review. Child Abuse Negl., 2020, 106, 104485. [Google Scholar] [CrossRef]
- Marcotte, J.; Richard, M.-C.; Dufour, I.F.; Plourde, C. Les récits de vie des jeunes placés : vécu traumatique, stratégies pour y faire face et vision d’avenir. Criminologie 2023, 56, 163–186. [Google Scholar] [CrossRef]
- Op den Kelder, R.; Van den Akker, A. L.; Geurts, H. M.; Lindauer, R. J. L.; Overbeek, G. Executive Functions in Trauma-Exposed Youth: A Meta-Analysis. Eur. J. Psychotraumatology, 2018, 9. [Google Scholar] [CrossRef]
- Tarren-Sweeney, M. The Mental Health of Adolescents Residing in Court-Ordered Foster Care: Findings from a Population Survey. Child Psychiatry Hum. Dev., 2018, 49, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Warmingham, J. M.; Handley, E. D.; Rogosch, F. A.; Manly, J. T.; Cicchetti, D. Identifying Maltreatment Subgroups with Patterns of Maltreatment Subtype and Chronicity: A Latent Class Analysis Approach. Child Abuse Negl., 2019, 87, 28–39. [Google Scholar] [CrossRef] [PubMed]
- Arnett, J. J. Emerging Adulthood: A Theory of Development from the Late Teens through the Twenties. Am. Psychol., 2000, 55, 469–480. [Google Scholar] [CrossRef] [PubMed]
- De Singly, F. Penser Autrement La Jeunesse. Lien Soc. Polit. 2000, 43, 9–21. [Google Scholar] [CrossRef]
- Supeno, E.; Bourdon, S. Bifurcations, Temporalités et Contamination Des Sphères de Vie. Parcours de Jeunes Adultes Non Diplômés et En Situation de Précarité Au Québec. Agora DébatsJeunesses, 2013, 65, 109–123. [Google Scholar] [CrossRef]
- Becker-Blease, K.; Kerig, P. K. Emerging Adulthood. Child Maltreatment Dev. Psychopathol. Approach 2016, 91–102. [Google Scholar] [CrossRef]
- Courtney, M. E. The Difficult Transition to Adulthood for Foster Youth in the US: Implications for the State as Corporate Parent. Soc. Policy Rep., 2009, 23, 3–19. [Google Scholar] [CrossRef]
- Gaetz, S.; O’Grady, B.; Kidd, S.; Schwan, K. Without a Home: The National Youth Homelessness Survey; Canadian Observatory on Homelessness, 2016; p 126.
- Fournier, V.; Matte-Landry, A. L’insertion Professionnelle Des Jeunes Ayant Vécu Un Placement En Protection de La Jeunesse: Une Revue de La Portée; Centre de recherche universitaire sur les jeunes et les familles (CRUJeF). Centre intégré universitaire de santé et de services sociaux de la Capitale-Nationale, 2023; p 84.
- Spinelli, T. R.; Bruckner, E.; Kisiel, C. L. Understanding Trauma Experiences and Needs through a Comprehensive Assessment of Transition Age Youth in Child Welfare. Child Abuse Negl., 2021, 122, 105367. [Google Scholar] [CrossRef]
- Leaving Care and the Transition to Adulthood: International Contributions to Theory, Research, and Practice Get Access Arrow; Mann-Feder, V. R., Goyette, M., Eds.; Oxford University Press: New York, 2019. [Google Scholar]
- Longo, M. E.; Goyette, M.; Dumollard, M.; Ziani, M.; Picard, J. Portrait des jeunes ayant été placés sous les services de la protection de la jeunesse et leurs défis en emploi; INRS - Urbanisation Culture Société: Québec, 2024. [Google Scholar]
- Sacker, A.; Lacey, R. E.; Maughan, B.; Murray, E. T. Out-of-Home Care in Childhood and Socio-Economic Functioning in Adulthood: ONS Longitudinal Study 1971–2011. Child. Youth Serv. Rev., 2022, 132, 106300. [Google Scholar] [CrossRef]
- Font, S.; Palmer, L. Left behind? Educational Disadvantage, Child Protection, and Foster Care. Child Abuse Negl., 2024, 149, 106680. [Google Scholar] [CrossRef]
- Clemens, A. Mental Health and Homelessness Among Youth Aging Out of Foster Care: An Integrated Review. J. Stud. Res., 2022, 11, 1–9. [Google Scholar] [CrossRef]
- Goyette, M.; Blanchet, A.; Bellot, C.; Boisvert-Viens, J.; Fontaine, A. Itinérance, Judiciarisation et Marginalisation Des Jeunes Ex-Placés Au Québec. Chaire de Recherche Sur l’évaluation Des Actions Publiques à l’égard Des Jeunes et Des Populations Vulnérables., 2022.
- Goyette, M.; Blanchet, A.; Bellot, C. The Covid-19 Pandemic and Needs of Youth Who Leave Care.; Chaire de recherche du Canada sur l’évaluation des actions publiques à l’égard des jeunes et des populations vulnérables, 2020; p 14.
- Pauzé, M.; Audet, M.; Pauzé, R. Soutenir l’intégration sociale de jeunes vulnérables devant composer avec les défis de transition vers l’âge adulte. Cah. Crit. Thérapie Fam. Prat. Réseaux, 2020, 64, 107–127. [Google Scholar] [CrossRef]
- Bussières, E. L.; Dubé, M.; St-Germain, A.; Lacerte, D.; Bouchard, P.; Allard, M. L’efficacité et l’efficience Des Programmes d’accompagnement Des Jeunes Vers l’autonomie et La Préparation à La Vie d’adulte; UETMISS, CIUSSS de la Capitale-Nationale, installation Centre jeunesse de Québec, 2015; p 170.
- Heerde, J. A.; Hemphill, S. A.; Scholes-Balog, K. E. The Impact of Transitional Programmes on Post-Transition Outcomes for Youth Leaving out-of-Home Care: A Meta-Analysis. Health Soc. Care Community, 2018, 26, e15–e30. [Google Scholar] [CrossRef]
- Alderson, H.; Smart, D.; Kerridge, G.; Currie, G.; Johnson, R.; Kaner, E.; Lynch, A.; Munro, E.; Swan, J.; McGoverrn, R. Moving from ‘What We Know Works’ to ‘What We Do in Practice’: An Evidence Overview of Implementation and Diffusion of Innovation in Transition to Adulthood for Care Experienced Young People. Child Fam. Soc. Work, 2023, 28. [Google Scholar] [CrossRef]
- Institut national d’excellence en santé et en services sociaux (INESSS). Portrait Des Pratiques Visant La Transition à La Vie Adulte Des Jeunes Résidant En Milieu de Vie Substitut Au Québec; Institut national d’excellence en santé et en services sociaux (INESSS), 2018; p 120.
- Goyette, M.; Blanchet, A.; Tardif-Samson, A.; Gauthier-Davies, C. Rapport Sur Les Jeunes Participants Au Programme Qualification Jeunesse; Rapport de recherche; Chaire de recherche du Canada sur l’évaluation des actions publiques à l’égard des jeunes et des populations vulnérables, 2022; p 45.
- Child Welfare League of Canada. Equitable Standards for Transitions to Adulthood for Youth in Care; Child Welfare League of Canada, 2021; p 39.
- Zhang, S.; Conner, A.; Lim, Y.; Lefmann, T. Trauma-Informed Care for Children Involved with the Child Welfare System: A Meta-Analysis. Child Abuse Negl., 2021, 122, 105296. [Google Scholar] [CrossRef] [PubMed]
- Kaminer, D.; Bravo, A. J.; Mezquita, L.; Pilatti, A.; Bravo, A. J.; Conway, C. C.; Henson, J. M.; Hogarth, L.; Ibáñez, M. I.; Kaminer, D.; et al. Adverse Childhood Experiences and Adulthood Mental Health: A Cross-Cultural Examination among University Students in Seven Countries. Curr. Psychol., 2022, 42, 18370–18381. [Google Scholar] [CrossRef]
- Piel, M. H.; Lacasse, J. R. Responsive Engagement in Mental Health Services for Foster Youth Transitioning to Adulthood. J. Fam. Soc. Work, 2017, 20, 340–356. [Google Scholar] [CrossRef]
- Strolin-Goltzman, J.; Woodhouse, V.; Suter, J.; Werrbach, M. A Mixed Method Study on Educational Well-Being and Resilience among Youth in Foster Care. Child. Youth Serv. Rev., 2016, 70, 30–36. [Google Scholar] [CrossRef]
- Agnihotri, S.; Park, C.; Jones, R.; Goodman, D.; Patel, M. Defining and Measuring Indicators of Successful Transitions for Youth Aging out of Child Welfare Systems: A Scoping Review and Narrative Synthesis. Cogent Soc. Sci., 2022, 8. [Google Scholar] [CrossRef]
- Matte-Landry, A.; Brend, D.; Collin-Vézina, D. Le Pouvoir Transformationnel Des Approches Sensibles Au Trauma Dans Les Services à l’enfance et à La Jeunesse Au Québec. Trav. Soc., 2023, 69, 1–5. [Google Scholar] [CrossRef]
- Peters, M. D. J.; Marnie, C.; Tricco, A. C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C. M.; Khalil, H. Updated Methodological Guidance for the Conduct of Scoping Reviews. JBI Evid. Synth., 2020, 18. [Google Scholar] [CrossRef]
- Tricco, A. C.; Lillie, E.; Zarin, W.; O’Brien, K. K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M. D. J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med., 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Forbes, D.; Fletcher, S.; Parslow, R.; Phelps, S.; O’Donnell, M.; Bryant, R. A.; McFarlane kake, A.; Silove, D.; Creamer, M. Trauma at the Hands of Another: Longitudinal Study of Differences in the Posttraumatic Stress Disorder Symptom Profile Following Interpersonal Compared with Noninterpersonal Trauma. J Clin Psychiatry, 2012, 73, 372–376. [Google Scholar] [CrossRef] [PubMed]
- Peters, W.; Rice, S.; Cohen, J.; Murray, L.; Schley, C.; Alvarez-Jimenez, M.; Bendall, S. Trauma-Focused Cognitive–Behavioral Therapy (TF-CBT) for Interpersonal Trauma in Transitional-Aged Youth. Psychol. Trauma Theory Res. Pract. Policy, 2021, 13, 313–321. [Google Scholar] [CrossRef]
- Gestsdottir, S.; Gisladottir, T.; Stefansdottir, R.; Johannsson, E.; Jakobsdottir, G.; Rognvaldsdottir, V. Health and Well-Being of University Students before and during COVID-19 Pandemic: A Gender Comparison. PloS One, 2021, 16. [Google Scholar] [CrossRef]
- Covidence Systematic Review Software, 2023.
- Cohen, J. A Coefficient of Agreement for Nominal Scales. Educ. Psychol. Meas., 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Hallett, R. E.; Westland, M. A.; Mo, E. A Trauma-Informed Care Approach to Supporting Foster Youth in Community College. In New Directions for Community Colleges; 2018; Vol. 2018, pp 49–58.
- Mendes, P.; Standfield, R.; Saunders, B.; McCurdy, S.; Walsh, J.; Turnbull, L.; Armstrong, E. Indigenous Care Leavers in Australia: A National Scoping Study; Report; Monash University, 2020; p 249.
- Mountz, S.; Capous-Desyllas, M.; Perez, N. Speaking Back to the System: Recommendations for Practice and Policy from the Perspectives of Youth Formerly in Foster Care Who Are LGBTQ. Child Welfare, 2020, 97, 117–140. [Google Scholar]
- Schubert, A. Supporting Youth Aging out of Government Care with Their Transition to College. Thesis, Western University, 2019.
- Jivanjee, P.; Grover, L.; Thorp, K.; Masselli, B.; Bergan, J.; Brennan, E. M. Training Needs of Peer and Non-Peer Transition Service Providers: Results of a National Survey. J. Behav. Health Serv. Res., 2020, 47, 4–20. [Google Scholar] [CrossRef]
- Gaetz, S. A Safe and Decent Place to Live: Towards a Housing First Framework for Youth; Canadian Homelessness Research Network, 2014; p 64.
- Gonzalez, R.; Cameron, C.; Klendo, L. The Therapeutic Family Model of Care: An Attachment and Trauma Informed Approach to Transitional Planning. Dev. Pract. Child Youth Fam. Work J., 2012, 32, 13–23. [Google Scholar]
- Marlotte, L. 68.4 Bouncing Back: Resilience-Building in Foster Families and Youth. J. Am. Acad. Child Adolesc. Psychiatry, 2017, 56. [Google Scholar] [CrossRef]
- Kisiel, C.; Pauter, S.; Ocampo, A.; Stokes, C.; Bruckner, E. Trauma-Informed Guiding Principles for Working with Transition Age Youth: Provider Fact Sheet, 2021.
- Child Protection Project Committee. Study Paper on Youth Aging into the Community; Study Paper 11; British Columbia Law Institute: Rochester, NY, 2021. [Google Scholar]
- Hill, S. L. 49.2 Impact of the Leads (Learn - Educate - Achieve - Dream - Succeed) Program. J. Am. Acad. Child Adolesc. Psychiatry, 2021, 60. [Google Scholar] [CrossRef]
- Camp, J. K.; Hall, T. S.; Chua, J. C.; Ralston, K. G.; Leroux, D. F.; Belgrade, A.; Shattuck, S. Toxic Stress and Disconnection from Work and School among Youth in Detroit. J. Community Psychol., 2022, 50, 876–895. [Google Scholar] [CrossRef] [PubMed]
- Harder, A. T.; Mann-Feder, V.; Oterholm, I.; Refaeli, T. Supporting Transitions to Adulthood for Youth Leaving Care: Consensus Based Principles. Child. Youth Serv. Rev., 2020, 116, 1–9. [Google Scholar] [CrossRef]
- Butters, C. Best Practice Recommendations for Transitioning Adolescent Foster Girls. Scholarly Project, University of Utah, 2013.
- Ausikaitis, A. E. Empowering Homeless Youth in Transitional Living Programs: A Transformative Mixed Methods Approach to Understanding Their Transition to Adulthood. Dissertation, Loyola University: Chicago, 2014.
- Spinelli, T. R.; Riley, T. J.; St Jean, N. E.; Ellis, J. D.; Bogard, J. E.; Kisiel, C. Transition Age Youth (TAY) Needs Assessment : Feedback from TAY and Providers Regarding TAY Services, Resources, and Training. Child Welfare, 2019, 97, 89–116. [Google Scholar]
- Baker, D. C.; Berragan, D. L. 1625 Independent People. Trauma Recovery Model Pilot; Evaluation report; University of Gloucestershire: Gloucester, 2020. [Google Scholar]
- Manpower Demonstration and Research Corporation (MDRC). Lessons from the Implementation of Learn and Earn to Achieve Potential, s.d. Manpower Demonstration and Research Corporation (MDRC). Lessons from the Implementation of Learn and Earn to Achieve Potential, s.d.
- Trekson, L.; Wasserman, K.; Ho, V. Connecting to Opportunity; Manpower Demonstration and Research Corporation (MDRC), 2019; p 150.
- Esaki, N.; Benamati, J.; Yanosy, S.; Middleton, J. S.; Hopson, L. M.; Hummer, V. L.; Bloom, S. L. The Sanctuary Model: Theoretical Framework. Fam. Soc., 2013, 94, 87–95. [Google Scholar] [CrossRef]
- Bryson, S. A.; Gauvin, E.; Jamieson, A.; Rathgeber, M.; Faulkner-Gibson, L.; Bell, S.; Davidson, J.; Russel, J.; Burke, S. What Are Effective Strategies for Implementing Trauma-Informed Care in Youth Inpatient Psychiatric and Residential Treatment Settings? A Realist Systematic Review. Int. J. Ment. Health Syst., 2017, 11, 1–16. [Google Scholar] [CrossRef]
- Lowenthal, A. Trauma-Informed Care Implementation in the Child- and Youth-Serving Sectors: A Scoping Review. Int. J. Child Adolesc. Resil., 2020, 7, 178–194. [Google Scholar] [CrossRef]
- Turcotte, M.-E.; Matte-Landry, A.; Hivon, M.; Julien, G. La Pédiatrie Sociale En Communauté En Tant Qu’approche Sensible Au Trauma : Une Voie Légitime Vers La Transformation Des Services à l’enfance Au Québec. Trav. Soc., 2023, 69, 7–23. [Google Scholar] [CrossRef]
- Brown, J. D.; King, M. A.; Wissow, L. S. The Central Role of Relationships With Trauma-Informed Integrated Care for Children and Youth. Acad. Pediatr., 2017, 17, S94–S101. [Google Scholar] [CrossRef]
- Barnett, E. R.; Yackley, C. R.; Licht, E. S. Developing, Implementing, and Evaluating a Trauma-Informed Care Program within a Youth Residential Treatment Center and Special Needs School. Resid. Treat. Child. Youth, 2018, 35, 95–113. [Google Scholar] [CrossRef]
- Pollock, D.; Peters, M. D. J.; Khalil, H.; McInerney, P.; Alexander, L.; Tricco, A. C.; Evans, C.; de Moraes, É. B.; Godfrey, C. M.; Pieper, D.; et al. Recommendations for the Extraction, Analysis, and Presentation of Results in Scoping Reviews. JBI Evid. Synth., 2023, 21, 520–532. [Google Scholar] [CrossRef] [PubMed]
- Moulin, S. L’émergence de l’âge Adulte: De l’impact Des Référentiels Institutionnels En France et Au Québec 1. SociologieS 2012. [Google Scholar] [CrossRef]
- Velde, C. V. de. Devenir adulte: sociologie comparée de la jeunesse en Europe, 1re éd.; Lien social; Presses universitaires de France: Paris, 2008. [Google Scholar]
- Bargeman, M.; Smith, S.; Wekerle, C. Trauma-Informed Care as a Rights-Based “Standard of Care”: A Critical Review. Child Abuse Negl., 2021, 119 Pt 1. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
PRISMA flow diagram.
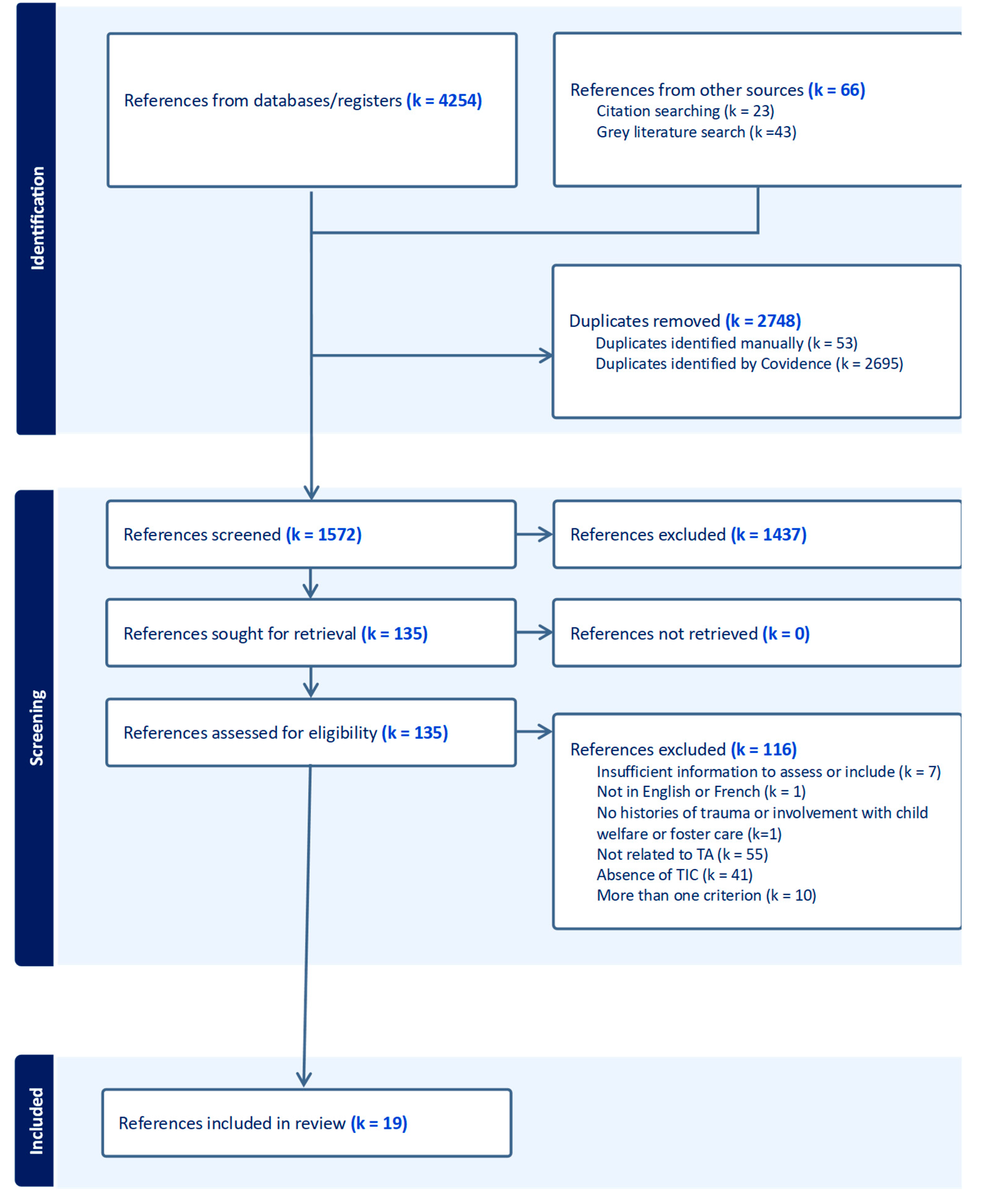
Figure 2.
Schematic representation of the review key findings. Note. Full lines indicate positive effects, whereas dashed lines indicate whether negative or null effects (for models assessed) or that the model targets that outcome but was not assessed. BoT (Back on Track); FOCUS (Families Over Coming Under Stress); JAG (Jobs for America's Graduate); JMG (Jobs for Michigan Graduates); LEADS (Learn – Educate – Achieve – Dream – Succeed); LEAP (Learn and Earn to Achieve Potential); TAY (Transition Age Youth); TFMC (Therapeutic Family Model of Care); TLP (Transitional Living Program); TRM (Trauma Recovery Model).
Figure 2.
Schematic representation of the review key findings. Note. Full lines indicate positive effects, whereas dashed lines indicate whether negative or null effects (for models assessed) or that the model targets that outcome but was not assessed. BoT (Back on Track); FOCUS (Families Over Coming Under Stress); JAG (Jobs for America's Graduate); JMG (Jobs for Michigan Graduates); LEADS (Learn – Educate – Achieve – Dream – Succeed); LEAP (Learn and Earn to Achieve Potential); TAY (Transition Age Youth); TFMC (Therapeutic Family Model of Care); TLP (Transitional Living Program); TRM (Trauma Recovery Model).
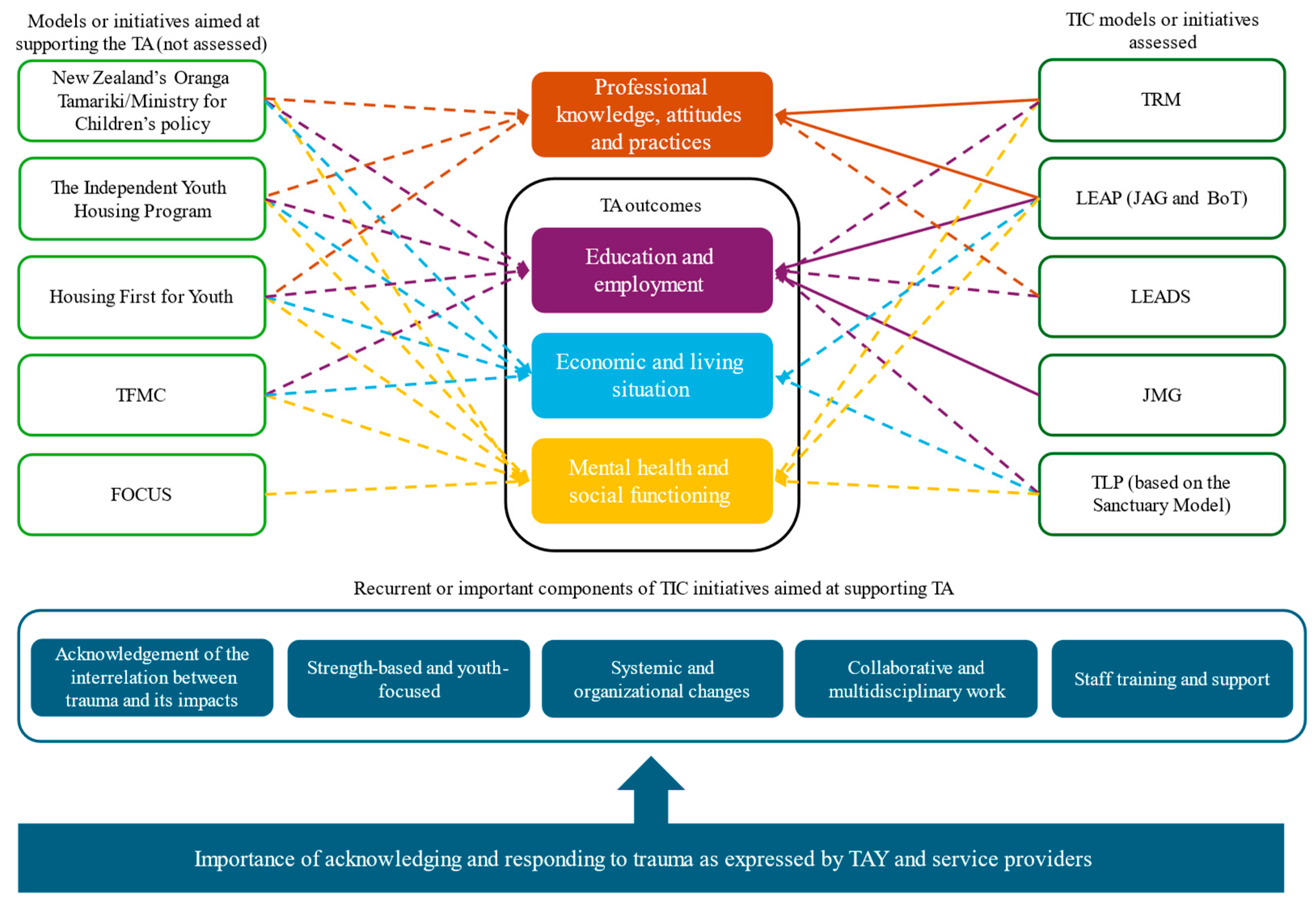

Table 1.
Information, objectives and methods of included references.
| Authors [reference number] | Date | Type of document | Category of document | Objective | Methods |
|---|---|---|---|---|---|
|
Ausikatis, A. E. [63] |
2014 | Thesis or dissertation | Importance or need for TIC; Assessment of TIC to support transition to adulthood | Explore the experiences of homeless young adults in transitional living programs (TLP). | Design and/or type of methods: Multiphase combination design; Mixed methods Methods: Surveys, questionnaires, interviews, and focus groups Time points: 2 time points (6 months delay) for surveys, questionnaires, and interviews; focus groups conducted in the 6 months delay. Participants: Homeless young adults including unaccompanied youth, runaways, throwaways, street-living youth, and youth aging out of foster care (18-21 years old) living in TLP. Participants took part in interviews (N=8) and focus groups (N=10). TIC approach: TLP based on the Sanctuary model which focuses on basic needs, independent living skills, educational and/or employment skills, increases in savings/income, clinical concerns, self-sufficiency and developmental growth, and transition to permanent housing. Program duration: The average length of stay is 6 months, but youth are allowed to stay up to two years. Outcomes: Mental and occupational health; sense of social support, independence, and belonging; support and services; goals; experiences in TLP. |
|
Baker, C., & Berragan, L. [65] |
2020 | Research report | Description of practices and policies; Assessment of TIC to support TA | Investigate the efficacy of the TRM model in helping practitioners to support care leavers and improve practice, knowledge, confidence, and understanding of a trauma-informed approach. | Design and/or type of methods: Mixed methods Methods: Self-report surveys (open-ended questions) and interviews with staff Time points: 2 for the surveys: initial and 3 months follow-up Participants: Staff members involved in the development and implementation of TRM in an organization serving young people leaving care or custody or at risk of entering custody. The initial survey was completed by 15 staff members, while the follow-up survey and interview were completed by 4 staff members. TIC approach: TRM draws together knowledge of attachment, trauma, criminology, and neurology to formulate interventions for children and young people with complex needs. Outcomes: Staff practice and knowledge, staff reflection on the impact of TRM on clients’ experiences and outcomes (e.g., mental health, life skills, independence, positive relationships). |
|
Butters, C. [62] |
2013 | Thesis or dissertation | Importance or need for TIC; Description of practices and policies | Present best practice recommendations for transitioning adolescent foster girls. | Design and/or type of methods: Review. Methods: Critical review of data, systematic reviews, meta-analysis, randomized controlled trials, and clinical practice guidelines relevant to adolescent foster girls transitioning to adulthood; Interviews and communication with stakeholders. |
|
Camp, J. K., Hall, T. S., Chua, J. C., Ralston, K. G., Leroux, D. F., Belgrade, A., & Shattuck, S. [60] |
2021 | Peer-reviewed article | Assessment of TIC to support TA | Determine if toxic stress exposure affected educational attainment and employment among youth. | Design and/or type of methods: Quantitative Methods: Secondary analysis of census data from the Detroit Jobs for Michigan Graduates (JMG) program. Time points: 1) intake; 2) during program enrollment; 3) following program completion. Participants: Youth (n=1934; 13-26 years old) who participated in the JMG program; 93.7% were from homes with low incomes; 4.9% were identified as “systems-involved”. To be enrolled in the JMG program, youth must have a minimum of four barriers across eight domains: educational; employment; disability and health; interpersonal and emotional; childcare and parenting; family; intergenerational; and basic needs. TIC approach: JMG comprises three different programs: in-school, out-of-school, and the LEAP program. It includes intake evaluations, specialized education/training courses, case management services, and job skills/career coaching. The LEAP program complements the out-of-school program for youth who have been identified as “system-involved” with a TIC approach, where cross-systems partnerships allow to meet gaps and unmet basic needs as well as providing additional leadership and skills-based training. Program duration: 2-3 years Outcomes: Achievement of one or more educational or employment goals such as graduating from high school, enrolling in college, earning a general education diploma, and/or becoming employed. |
|
Child Protection Project Committee [58] |
2021 | Government or organization document | Description of practices and policies | Review and compare legislative models that support policy and practice related to youth aging into the community. | Design and/or type of methods: Review Methods: Reviews of models (some including TIC principles) that support policy and practice related to youth aging out into the community. |
|
Gaetz, S. [54] |
2014 | Research report | Description of practices and policies | Provide a clear understanding of what Housing First is, and how it can work to support young people who experience or are at risk of homelessness. | Design and/or type of methods: NA (description of a program) Methods: Review of research, consultation, and interviews with key service providers and young people who have experienced homelessness. TIC approach: Housing First for youth with five kinds of supports (housing; health and wellbeing [including TIC]; access to income and education; complementary supports; and opportunities for meaningful engagement) to support housing and to facilitate TA. |
|
Gonzalez, R., Cameron, C., & Klendo, L. [55] |
2012 | Peer-reviewed article | Description of practices and policies | Examine how to ensure a successful TA for young people in care, relying on the Lighthouse Foundation TFMC. | Design and/or type of methods: NA (description of a model) Methods: NA TIC approach: The TFMC is an integrated model of therapeutic care where TAY in care during are encouraged to be active in education, work, and personal development, and participate in programs to address their psychological wellbeing. |
|
Hallett, R. E., Westland, M. A., & Mo, E. [49] |
2018 | Book chapter | Importance or need for TIC | Increase completion of community college and transition to four-year institutions; explore the importance of embedding a TIC approach for college students aging out of care. | Design and/or type of methods: Qualitative; constant comparative analysis Methods: Semi-structured interviews and documents review. Participants: 7 foster youth attending a community college and 8 stakeholders. |
|
Harder, A. T., Mann-Feder, V., Oterholm, I., & Refaeli, T. [61] |
2020 | Peer-reviewed article | Importance or need for TIC; Description of practices and policies | Propose principles that can support practice and policy in promoting successful TA for young care leavers. | Design and/or type of methods: Qualitative Methods: Participants nominated a principle that had significant implications for practice as well as strong research support. A smaller group reviewed and refined the principles in relation to research and eliminated redundancies. Participants: A network of researchers (15 academics from 14 countries) concerned with the transition experienced by TAYfrom public care participated in the nomination of principles. |
|
Hill, S. L. [59] |
2021 | Conference proceeding | Assessment of TIC to support transition to adulthood | Assess LEADS (Learn –Educate – Achieve – Dream – Succeed) and provide data on characteristics of the youth served, types of services provided, factors associated with success, and overall outcomes. | Design and/or type of methods: Mixed methods Methods: A 3-year evaluation of the LEADS program allowed to describe characteristics of the youth served, types of services provided, factors associated with success, and overall outcomes. Participants' perception of the program was also of interest. Time points: 1 Participants: Foster youth between the ninth and 12th grade or pursuing their General Educational Diploma (GED). TIC approach: LEADS, a trauma-informed, resiliency-based approach, which coordinates youth education assessments, creates individualized action plans, and advocates for support to meet academic demands. Program duration: Not specified Outcomes: Not specified |
|
Jivanjee, P., Grover, L., Thorp, K., Masseli, B., Bergan, J. & Brennan, E. M. [53] |
2019 | Peer-reviewed article | Importance or need for TIC | Assess service providers’ training needs and preferences to better serve TAY with mental health difficulties. | Design and/or type of methods: Cross-sectional participatory action research; Mixed methods Methods: Online survey (self-report questionnaires and open-ended questions) to assess service providers’ training needs and preferences. Time points: 1 Participants: 254 service providers working with TAY with mental health challenges and other needs. |
|
Kisiel, C., Pauters, S., Ocampo, A., Stokes, C., & Bruckner, E. [57] |
2021 | Government or organization document | Description of practices and policies | Recognize the impact of trauma on TAY by offering foundational principles for understanding and working with TAY. | Design and/or type of methods: NA (formulation of principles) Methods: Principles are informed from a range of perspectives, including NCTSN’s 12 Core Concepts, and experiences of youth, caregivers, and professionals. TIC approach: TIC principles for understanding and working with youth approaching transition from the child-serving system(s) (child welfare, juvenile justice, education, behavioral health, etc.) due to “aging out” or other circumstances. |
|
Manpower Demonstration and Research Corporation [66] ; Trekson, L., Wasserman, K. & Ho, V.[1] [67] |
n.d.; 2019 | Government or organization document; Research report | Description of practices and policies; Assessment of TIC to support transition to adulthood | Description and evaluation of LEAP initiatives models (JAG and BoT) to serve youth. | Design and/or type of methods: Program evaluation; Mixed methods Methods: Site visits; interviews with participants; program participation data; financial data. Time points: 2 time points; years 2 and 3 or 4 of implementation for JAG, and years 2 and 3 of implementation for BoT Participants: 9 organizations offering JAG and 5 offering BoT comprising to up to 5000 participants (14-26 years old) with past or current experience in the foster care or juvenile or justice systems or with homelessness. TIC approach: The LEAP initiative aims to improve education and employment outcomes for youth who have a history of involvement in the foster care and/or justice systems, or who are experiencing homelessness. Two evidence-based models (JAG and BoT) were adapted to meet their needs, including support to address trauma they may have experienced in their lives as well as help to connect with postsecondary resources and programs. Outcomes: Implementation; Participants perspectives on their program experiences; Youth engagement; Factors facilitating or constraining participation; Education and employment; Cost. |
|
Marlotte, L. [56] |
2017 | Conference proceeding | Description of practices and policies | Explore the adaptation of FOCUS. | Design and/or type of methods: NA (clinical perspective) TIC approach: FOCUS (Families Over Coming Under Stress) is an evidence-based, skill-building preventive intervention for foster families and foster youth in college. |
|
Mendes, P., Sandfield, R., Saunders, B., McCurdy, S., Walsh, J., Turnbull, L., & Armstrong, E. [50] |
2020 | Research report | Importance or need for TIC | Investigate the numbers, needs, and outcomes of Indigenous care leavers and examine relevant funding, policy and practice. | Design and/or type of methods: Cross-sectional; Qualitative Methods: Focus groups and semi-structured interviews. Time points: 1 Participants: 53 key representatives of government departments (n=9), non-government organizations (n=32), and Aboriginal and Torres Strait Islander community-controlled organizations (n=12) in the leaving care sector. |
|
Mountz, S., Capous-Desyllas, M., & Perez, N. [51] |
2020 | Peer-reviewed article | Importance or need for TIC | Gain a deeper understanding of the experiences of youth formerly in foster care who are LGBTQ. | Design and/or type of methods: Cross-sectional community-based participatory research; Qualitative Methods: Photovoice and interviews on several themes related to TA (e.g., family history, transitioning out of care, mental health, substance use, identity, resilience). Time points: 1 Participants: 25 LGBTQ youth (18–26 years old) formerly in foster care. |
|
Schubert, A. [53] |
2019 | Thesis or dissertation | Importance or need for TIC | Create support and services that will foster college success. | Design and/or type of methods: Qualitative Methods: Consultation with youth and institutions. Participants: Youth in and aging out of care, post-secondary institutions with successful youth-in-care initiatives, community agencies, and alternate high school programs. |
|
Spinelli, T. R., Riley, T. J., St. Jean, N. E., Ellis, J. D., Bogard, J. E., & Kisiel, C. L. [64] |
2019 | Peer-reviewed article | Importance or need for TIC; Assessment of TIC to support transition to adulthood | Improve the quality of services, resources, and training for TAY providers. | Design and/or type of methods: Cross-sectional design; Mixed methods Methods: Written survey and focus groups assessing TAY and providers’ needs, strengths, barriers, and strategies for coping with trauma, as well as TIC resources and services, and perspectives on the most effective components of TIC staff training. Time points: 1 Participants: 95 providers who work with TAY and 34 TAY receiving services in child welfare (14-21 years old) TIC approach: TIC training (not otherwise specified). Program duration: Not specified Outcomes: Not specified |
Note. BoT (Back on Track) ; FOCUS (Families Over Coming Under Stress) ; GED (General Educational Diploma) ; JAG (Jobs for America’s Graduates); JMG (Jobs for Michigan Graduates) ; LEADS (Learn – Educate – Achieve – Dream – Succeed) ; LEAP (Learn and Earn to Achieve Potential) ; LGBTQ (lesbian, gay, bisexual, transgender, and queer) ; NCTSN (The National Child Traumatic Stress Network) ; TA (Transition to adulthood) ) ; TAY (Transition Age Youth) ; TFMC (Therapeutic Family Model of Care); TIC (Trauma-informed care) ; TLP (Transitional Living Program) ; TRM (Trauma Recovery Model).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



