
Submitted:
26 September 2025
Posted:
30 September 2025
You are already at the latest version
Abstract
Child maltreatment (CM) is a widespread and underreported public health concern with long-term physical and mental consequences. In Europe, access to timely, effective support remains limited. Inadequate responses exacerbate long-term outcomes and influence life course trajectories, with substantial societal and economic costs. The EU-funded SERENA project aims to improve access to health and social care (HSC) services for individuals who experience CM throughout Europe by enhancing detection and interventions, limiting consequences, and reducing societal burdens. SERENA takes an early life course perspective, and will examine HSC pathways before and after CM detection, assess related physical and mental health conditions, and evaluating the societal costs of CM. Two scoping reviews will examine quantitative and qualitative evidence on barriers and facilitators to access to HSC for children who experience CM, and their service pathways. A mixed methods study will combine quantitative analyses of nationwide longitudinal administrative HSC data from seven countries, supplemented by aggregated child protection data from 26 countries, with qualitative analyses of interviews with adult survivors of CM and HSC professionals in three countries. Examination of HSC pathways will enable us to identify the settings and stages where interventions can be targeted to improve outcomes for children with CM. We will also examine societal costs by analysing direct medical expenses, educational costs, and productivity losses in four countries. An interdisciplinary, participatory synthesis involving stakeholders and adult survivors of CM will assess services, define priority actions, and inform recommendations.SERENA, a consortium of 22 partners across Europe, represents the first multi-country, large-scale, cross-sectorial longitudinal initiative to comprehensively examine CM and HSC service use. By addressing critical evidence gaps, SERENA will provide operationally and economically viable recommendations to enhance service access and public health responses in Europe, with findings that are transferable to diverse international contexts.
Keywords:
child health
; child maltreatment
; health and social care
; care inequalities
; mixed methods
; health economics
; child protection
; child welfare
Introduction
The World Health Organisation defines child maltreatment (CM) as a major public health concern [1]. Worldwide, an estimated 60% of children less than five years of age experience physical and/or psychological violence by their caregivers, and about 20% of women and 14% of men report childhood sexual abuse [2,3], with considerable variation between continents and countries [3]. CM has immediate and long-lasting negative effects on health and well-being [2,4,5,6], leading to developmental and health challenges [7]. These adverse experiences can influence life course trajectories, impairing educational achievement and employment, with far-reaching societal and economic impacts [1,8]. Despite considerable European investments in child protection policies and legal frameworks to safeguard children´s rights [9], CM remains under-identified in health and social care (HSC) systems. . For example, among children under five, hospitalisations for physical abuse are estimated at 18/100,000 per year in five European countries [10], although self-report studies estimate the incidence of childhood physical abuse to be much higher [11,12], with sparse comparative data for other forms of CM. Moreover, social care provision for children who experience CM is poorly understood, with limited insights into how needs evolve beyond childhood, including the provision of adequate support during key life transitions such as entering the educational system, the labour market, and parenthood.
Advancing expertise and driving innovation requires comprehensive data collection and analysis on CM and its associated health, social and economic effects [13,14]. Multi-country collaboration, with data-sharing and expert networks across multiple sectors and informants - including adult survivors of CM (ASCM) - is essential to address challenges such as the low numbers of identified individuals in administrative registries, inconsistent definitions of CM across sectors and countries, differences in perspectives between professionals and individuals with lived experience, varying data collection practices, limited national guidelines and training, and restricted systematic data linkage [15,16,17,18]. Consequently, our understanding of European HSC service provision for CM, including disparities and gaps in access, service quality, and long-term effects and service needs, is incomplete, emphasising the need for an expanded surveillance programmes to inform evidence-based policy and practice [3].
Building upon the outcomes and expertise developed through the pan-European initiative Euro-CAN COST Action 19106 (www.euro-can.org)—which laid the groundwork for the SERENA project (Assessing and improving access to health and social care SErvices for children RENdered vulnerable by Abuse)—this project will undertake an early life course approach to identify the settings and stages where interventions can be targeted to improve outcomes for children with CM. The work forms a critical assessment of current HSC service pathways in multiple European countries. By leveraging in-depth, cross-sectoral data collection and incorporating the lived experiences of ASCM, SERENA seeks to identify key structural and procedural barriers to service access, both prior to and following the formal recognition of CM. The overarching aim of SERENA is to enhance access to effective, timely, and contextually appropriate HSC services for individuals impacted by CM. To this end, the project will generate a set of evidence-based, actionable recommendations at the sectoral, national, and European levels. These recommendations will inform improvements in early detection, the optimisation of care pathways, and ultimately contribute to improved short- and long-term outcomes for affected individuals, based on the rigorous analysis of the physical and mental health consequences of CM during childhood, adolescence and early adulthood, alongside an estimation of its societal and economic burden.
Methods/Design
Overall Methodology
SERENA is a large-scale, Horizon Europe-funded research initiative involving 22 partners from multiple European countries (Figure 1), sectors and professions. The project period is from Jan 1, 2025, to Dec 31, 2029. It is coordinated under the standard Horizon Europe framework, with governance overseen in France. The project employs a cross-sectoral, mixed-methods, multi-study design (Figure 2) comprising two scoping reviews, several nationwide quantitative studies from longitudinal HSC data, two multidisciplinary qualitative studies, and a study of the societal costs of CM. These analyses will of course overlap so that the findings from these studies can be combined and analysed to yield an expanded understanding of service availability, provision, benefits and costs. The framework for analysis will involve consultations with HSC professionals and ASCM to ensure that interpretations, insights and recommendations are inclusive, evidence-based, and multifaceted.
Methodology: A Three-Step Process
SERENA follows a three-step process, outlined in Figure 3:
- Step 1: The preparatory phase: country selection and scoping reviews to refine criteria for the subsequent quantitative and qualitative studies.
The selection of countries for SERENA is informed by the methodologies and insights developed during the Euro-CAN project (www.euro-can.org). The quantitative longitudinal studies on healthcare pathways of maltreated children will include seven countries: Austria, Denmark, France, Germany, Sweden, Switzerland, and Wales. We will also conduct a longitudinal study examining the pathways through different administrative systems for children in care through linkage of health, education and social care datasets in Denmark and Wales. These countries were selected as they have already linked these datasets and made them accessible to researchers. . This will allow us to examine trajectories over time, transitions between different systems and longer-term health, social care and educational outcomes from childhood into adolescence and early adulthood. In addition, we will supplement this analysis with the ROCKWOOL-Duke Global Child Welfare Database [19], which aggregates cross-national data on children in welfare systems across 26 countries in Europe. In the absence of a centralised national medico-administrative database on CM data in Austria, data will be sourced from the FOKUS database, a regional tertiary hospital-based child protection unit in Vienna, which represents an umbrella service for all hospital-based CP teams in the region [20]. The qualitative study will include data from Denmark, France, and Wales, the findings from which can be combined with findings from the quantitative studies to give a comprehensive life course approach. Interviews with ASCM and HSC professionals in these countries will explore access to HSC services for maltreated children.
For the quantitative studies, CM will be grouped in three categories: (1) physical abuse, identified via an existing algorithm based on predefined diagnosis codes, according to the International Classification of Diseases 10th Revision (ICD-10); (2) sexual abuse; and (3) psychological abuse, or neglect, for which we will develop new ICD-10-based algorithms through scoping reviews and existing algorithms from Euro-CAN. We have already demonstrated the feasibility of developing such algorithms and carrying out pooled analyses in our initial work on physical abuse [10].
We will conduct two scoping reviews. The first scoping review will examine barriers and facilitators to accessing HSC therapeutic services for children who have experienced child maltreatment and will be conducted in two parts. A review of qualitative studies will include literature from France, Denmark, and the UK. The review of quantitative studies will incorporate 12 countries: Austria, Denmark, France, Germany, Greece, Ireland, the Netherlands, Portugal, Romania, Sweden, Switzerland, and the UK. The findings will inform the designs for the qualitative and quantitative studies. The second scoping review will examine the pathways that children with maltreatment take through services, including health, social care, education and other services. The review will help to complement our analysis conducted in Denmark and Wales and on the ROCKWOOL dataset, by comparing with the findings from other nations.
- Step 2: Mixed-methods analyses involving quantitative and qualitative studies to assess how maltreated children navigate HSC services. A final synthesis of study results will be reviewed by an expert group of ASCM and HSC professionals.
The quantitative studies of healthcare pathways will utilise nationwide medico-administrative data from six countries (Denmark, France, Germany, Sweden, Switzerland and Wales) and a regional tertiary hospital-based data from Austria to compare the healthcare pathways of maltreated children with those not identified as exposed to maltreatment, across three time points: before maltreatment diagnosis, short-term follow-up to two years, and long-term follow-up to ten years. We will use different algorithms to identify each type of abuse in medical-administrative databases. For physical abuse, we will use the algorithm already developed as part of the Euro-CAN project. For other types of abuse, we will develop algorithms in collaboration with all partners. To this end, as for physical abuse, we will organise several meetings to take into account the specific coding practices in each country. To account for these differences, we will use a minimal set of ICD-10 codes available in all participating countries, which will allow us to apply a standardised approach to carry out the planned analyses. For each maltreatment type, we will describe characteristics at the index hospitalisation by gender, age, diagnoses and procedures, length of stay, intensive care unit admission, and in-hospital death.
At the time point before CM diagnosis (Start 1 January 2025, end 31 December 2026), we will identify prior hospitalisations. For physical abuse, this will include birth data such as gestational age, birth weight, small for gestational age, and foetal sex, as well as neonatal conditions such as respiratory disorders and congenital malformations following EUROCAT guidelines [21]. For sexual abuse, psychological abuse, and neglect, we will use data on hospitalisations within four years before the index hospitalisation, including the number of hospitalisations, length of stay, diagnoses, and procedures.
At the short-term (Start 1 January 2026, end 31 December 2027) and long-term (Start 1 January 2027, end 31 December 2028) follow-up time points, we will identify the number of hospitalisations, maltreatment readmissions, diagnosed physical and mental health conditions (e.g. asthma, neurological disorders, suicidal behaviours, anxiety), and in-hospital deaths. Denmark, France and Wales have access to outpatient data which will enable the assessment of consultations with general practitioners and specialists, redeemed prescriptions for drugs, deaths, and socio-economic status.
Matched cohort studies (1:3) will compare maltreated children and children not identified as maltreated, matched mainly on date of index hospitalisation, age at index hospitalisation, gender, and region. The analyses will use identical methods across all countries, and the results will be pooled and weighted by the number of maltreated children per country.
The quantitative studies of social care pathways (Start 1 January 2026, end 31 December 2027) will use linked individual-level child protective services (CPS) registry data from Denmark and Wales to map children’s pathways through HSC systems, comparing maltreated children known to social care services with children not identified as maltreated. These registries include demographics, in- and outpatients hospital contacts and services, general practitioner visits, child protection, education, and justice data. We will conduct analyses by sector, and stratified by age, follow-up time, and country. For other countries, we will use aggregate statistics from the ROCKWOOL-Duke global child welfare database, which includes data on CM investigations, confirmed cases, and out-of-home care data.
The qualitative studies of HSC pathways (Start 1 January 2025, end 31 December 2027) will be based on individual and group interviews with HSC professionals and interviews with ASCM. Participants will be recruited via existing networks (www.euro-can.org), provided with study information, and asked to give written informed consent. Interviews and focus groups will be conducted in 2025 - 2026 by trained interviewers in local languages. Data collection will be informed by findings from the scoping reviews and public consultations (e.g. the Welsh advisory group of young people with lived experience of social care services (CASCADE Voices). CM will be defined as acts of commission and omission (neglect) by permanent or temporary caregivers and exclude victimisation by non-caregivers such as strangers, acquaintances, and peers [17,22]. We will analyse transcripts using thematic analysis, drawing on a mix of pre-specified themes (e.g. barriers to access for available services) and by identifying themes within the data.
In the final stage of Step 2, we will produce a cross-case synthesis using a convergent mixed methods design [23]. We will thematically analyse data from the qualitative and quantitative studies on short-term follow-up after CM identification guided by the frameworks of Boyatzis [24], and Braun and Clarke [25]. The discussion of the analysis will reference the findings of scoping reviews. We will then conduct an interdisciplinary, participatory synthesis, involving HSC professionals and ASCM, to interpret and assess the facilitators of, and barriers to, HSC services and to identify priority actions. Building on the Euro-CAN network, SERENA will establish an ASCM Board, composed of six diverse members selected via snowball sampling. The board will contribute to project design and interpretation of findings, with members receiving training, support, and compensation. Discrepancies between academic and survivor perspectives will be actively discussed and documented. The approach will inform the final analysis to identify patterns, confirmatory and discordant findings from the studies and identify priority actions across countries.
The initial synthesis of findings will be shared with the ASCM board through individual interviews, using an expert guide to minimise bias. Feedback will guide further analyses, overseen by a board member, with updates provided through online exchanges. A revised synthesis will be reviewed by the board, with two virtual meetings and a final in-person meeting. This participatory approach will ensure the recommendations are credible and informed by survivor expertise.
- Step 3: Reaching recommendations
We will use the findings of the studies to develop evidence-based recommendations for improving detection, intervention and follow-up, and administrative data collection on CM. These recommendations, aimed at national and European policymakers and HSC professionals, will be based on the results of the mixed methods analysis, societal cost estimates, and input from ASCM and HSC providers, to ensure impact and acceptability.
The estimate of the societal costs of CM, will include short- and long-term HSC costs and productivity losses. This economic evaluation will allow us to compare implementation costs with expected health and social benefits. Estimates will be based on linked hospital, social care, and educational data, following standard guidelines for economic evaluations [26].
Although data availability varies by country, a comparative analysis approach will be used to estimate direct healthcare costs, other sectoral costs, and indirect costs from productivity losses associated with CM. Direct costs will be calculated by combining healthcare and social care utilisation data multiplied by relevant unit costs. In addition, education and productivity losses will be included to reflect the broader societal impact of CM. We will estimate productivity losses using both the Human Capital Method and the Friction Cost Method [27]. Cost estimates will use non-parametric bootstrapping due to skewed distributions. Multiple regression models will be conducted to address the evaluation of potential effect modifiers such as age, gender, education, and urbanisation. First, average costs for non-identified maltreated children will be estimated using a weighted intercept-only generalised linear model, providing baseline insights into overall cost patterns. Secondly, the impact of each maltreatment type will be assessed by regressing individual maltreatment variables against costs. Finally, population-level costs will be extrapolated by multiplying the adjusted annual per-person excess costs by the prevalence of maltreatment exposure in the population.
Discussion
SERENA is a large-scale research initiative funded by Horizon Europe, designed to enrich the current body of knowledge regarding CM and the role of HSC services and improve evidence-informed practices. The project comprises 22 partners from multiple European countries and operates within the Horizon Europe framework, with governance based in France. Using multi-country, multi-sectoral, mixed-methods, and a longitudinal design, SERENA aims to provide evidence-based recommendations for HSC professionals and policymakers to enhance CM detection and optimise the planning and delivery of HSC services. The project’s novelty is its comprehensive approach, as the recommendations will: (1) be based on a European-wide project on HSC access and barriers for maltreated children; (2) draw on both quantitative and qualitative data from multiple countries; (3) include an economic evaluation of the societal costs of CM; (4) be developed through a participatory process involving key stakeholders including ASCM; and 5) be tailored to national, sector-specific, and European-level contexts, including guidance on capacity building and training to improve both short- and long-term outcomes for children affected by CM.
Strengths and Limitations
Epidemiological studies indicate a lack of research on assessing and improving access to HSC services for maltreated children, which affects decision-making, policy, and practice in child welfare and child protection services. There is a lack of longitudinal, national, register-based studies on CM and HSC utilisation in low and middle-income countries. Even in high-income settings, longitudinal evidence remains scarce [28]. SERENA addresses this gap through a multi-country, cross-sectoral, mixed-methods design, combining longitudinal administrative HSC data, qualitative case studies, and cross-national aggregated child protection data to generate comprehensive insights into HSC utilisation and barriers to accessing services. An additional strength is the use of administrative HSC data, enabling analysis of pooled individual-level and cross-sectoral data across countries. This real-world project will utilise nationwide data from several European countries, allowing large-scale examination of CM and HSC services with sufficient numbers of recorded children with CM for robust outcome analyses.
SERENA will conduct a multinational longitudinal retrospective cohort study using social- and health care linked registry data. The inclusion of longitudinal data, covering a period of up to 10 years, with a recorded timing of maltreatment event will provide valuable insights into early-life trajectories of affected children, enhancing our understanding of how experiences during potentially sensitive developmental periods can influence pathways in health and well-being.
This design addresses a notable gap in the literature, as most studies on maltreated children's health rely on retrospective surveys of adults with medical conditions, which are prone to recall bias and false negatives [6,29]. Longitudinal studies using administrative data can overcome these limitations [6]. Before the submission of this European SERENA project, most longitudinal CM studies were US-based.
Cross-sectoral data linkage studies are an effective methodology to generate information and represent an innovative way of measuring the use of HSC services for vulnerable populations [30]. Regarding cross-sectoral data, the longitudinal study of pathways through services for maltreated children in care will link individual-level social care data from Denmark and Wales with demographic, health, education and justice data. This will allow us to map children’s trajectories through HSC systems, enabling analysis of transitions between systems, and help us to understand the patterns and barriers to access to HSC services. We will supplement this analysis with the ROCKWOOL-Duke Global Child Welfare Database, which aggregates harmonized data from child welfare and statistical agencies across 26 European countries.
SERENA has limitations. Cultural perceptions of CM may lead to the different understandings of the qualitative interview questions. There may be challenges with reporting of abuse-related service experiences due to stigma and recall issues. We will attempt to mitigate these issues through the use of trained and experienced interviewers and multiple participant recruitment strategies. In the quantitative data, national variations in coding practices for CM types will be addressed by applying algorithms for physical abuse from a previous multinational European study [10] and by developing new algorithms for other types of abuse that account for cultural differences in definitions and recording.
Exposure misclassification due to under-reporting and under-identification of CM in medico-administrative data is another weakness, likely leading to an underestimation of the true prevalence. In addition, medico-administrative data capture data on the children most severely affected by CM. While this may limit generalisability to the broader population, the quantitative study using social care data also included in SERENA aims to broaden the scope. By linking social care data with health data, it will be possible to identify children involved with social care services who have not been to hospital, and to study the care pathways of children identified by either sector. Given that a large proportion of CM-affected individuals are not reported to child protection services [31], some misclassification should still be expected. However, by pooling individual-level data across several European countries, SERENA enables the study of CM in one of the largest populations to date. This increases statistical power and makes it possible to detect associations that may previously have gone undetected. To further minimise bias and improve representativeness and interpretive robustness, findings will be synthesised with qualitative results and reviewed by HSC professionals and ASCM stakeholders, who can also recommend additional analyses. Another limitation is that the algorithms used to identify CM types do not explicitly capture the timing or frequency of maltreatment. CM often occurs covertly and may go undetected for long periods, if identified at all. However, the fact that SERENA exploits the databases’ capacity to link healthcare episodes over time on an individual level will enable the identification of recurrent events and patterns among identified children, offering unique insights into recurrence and potential cumulative harm. Nevertheless, the data remains limited to the subset of children identified through HSC administrative data.
System-level challenges in the identification and response to CM may result from limited training among health professionals [32], uncertainty about legal procedures, and concerns about the consequences of misreporting [33]. Coordination and information-sharing across HSC services and judicial systems can be complex and fragmented [17,34], potentially hindering timely and effective responses.
Moreover, the recognition of maltreatment does not necessarily ensure quick access to support [32], due to potential workforce shortages and long waiting times for mental health services. While these challenges are well recognised in the field, they have received limited attention in cross-sectoral and multinational research. SERENA may be in a unique position to address these gaps by examining barriers to identify maltreatment and access care from both quantitative and qualitative perspectives.
Expected Results
SERENA expects to improve access to HSC services for maltreated children by generating robust, multidisciplinary evidence on HSC pathways across Europe and developing European-level recommendations to enhance detection and intervention, ultimately improving short- and long-term outcomes for individuals and society (Table 1).
We expect that the two scoping reviews will map existing HSC pathways for maltreated children and provide insights to refine the subsequent mixed-method studies. In addition, we will develop validated algorithms for identifying physical abuse, sexual abuse, psychological abuse, and neglect in administrative health records, facilitating cross-country comparability and strengthening future research on CM.
From the multi-study mixed-method analyses, we expect to provide a clearer picture of HSC pathways before and after CM identification, thus highlighting existing gaps in access and follow-up. We hypothesise that the quantitative studies will find increased morbidity and more frequent hospital visits among maltreated children compared to the general population, both for acute and chronic conditions. We also expect to gain insight into the types of health conditions that may increase the risk of CM, particularly stress-related conditions such as infections, autoimmune diseases, and mental health diagnoses. Furthermore, we expect to observe patterns of increased healthcare utilisation, help-seeking behaviour, and social care use. Additionally, we hypothesise that early predictors of CM can be identified in HSC data, along with the typical age of identification. The qualitative study is expected to generate in-depth evidence of the scope of health and social care services for children who experience CM, insights into how these services are currently implemented, and how access to these services can be facilitated. Finally, we expect the economic evaluation to reveal an increased financial burden associated with CM, compared to the general population, on a societal level. By incorporating both healthcare and educational costs, we expect to contribute to a more comprehensive understanding of the broader societal impact of CM. Thus, we expect our analysis to provide robust insights into the complex interplay between CM and its short- and long-term outcomes as well as the temporal benefits of HSC interventions in mitigating its negative effects [1,35,36].
Ultimately, we expect that the findings and participatory analysis and interpretation involving HSC professionals and ASCM will lead to evidence-based recommendations that can be implemented by decision-makers for public health policy (Table 1). The key objectives of these recommendations will be to reinforce planning, delivery, and early detection of CM across HSC systems throughout Europe. As a result, evidence-based practices and research in this area will be enhanced, HSC services will be mapped out, and additional intervention services and management strategies will be offered to children and young adults who have been maltreated.
Expected Implications
Based on findings from multiple sources within the SERENA studies, including the economic evaluation of societal costs, we will develop recommendations for policymakers at the European level. These recommendations will emphasize the avoidable costs of CM to society, and promote investment in evidence-based policies and practices for improved detection, intervention, follow-up, and systematic data collection on CM within HSC services. They will also address the introduction of necessary legal provisions, the promotion of multi-sectoral coordination, the creation of safe environments in HSC services, and the capacity-building of frontline professionals, in alignment with the INSPIRE programme, a set of seven evidence-based strategies for countries and communities working to eliminate violence against children, developed by WHO and partners [37].
The results are expected to provide crucial baseline evidence on children who experience CM prior to key life transitions, during which critical and formative periods occur. For example, the transition into adulthood is a stage when prolonged absence from education, social engagement, or support systems can have lasting adverse effects on labour market participation as well as physical and mental health. Early-life adversities, such as maltreatment, may disrupt brain maturation, physiological growth, and social adaptation, increasing the risk of negative health, social, and educational outcomes across the life course. Children and adolescents who have experienced maltreatment are a population at risk, and this early adversity can disturb developmental trajectories, increasing the risk of disengagement from education or employment and other long-term negative outcomes.
The findings from SERENA are expected to have relevance beyond Europe by providing transferable evidence on detection algorithms, critical developmental periods, service coordination, long-term health outcomes, and health behaviour patterns. These insights can guide policymakers and practitioners to adapt detection, intervention, and prevention strategies to local contexts, including high-, middle-, and low-income settings, even where resources or data infrastructure are limited. By highlighting children’s trajectories prior to key life transitions, SERENA will inform prioritisation of early interventions, multi-sectoral collaboration, and cost-effective approaches to mitigate the long-term consequences of CM.
At the European level, SERENA will guide sectoral, national, and European policies to reduce disparities and strengthen early CM detection and intervention within HSC services.
Evidence to support targeted early CM detection and intervention aligns with the World Health Assembly’s public health approach to delivering comprehensive care throughout the life course [38]. The results will guide the development of standardised approaches to data collection and service provision, potentially enabling more timely and equitable responses to CM in Europe.
Although the substantial burden of CM is widely recognised, its societal costs remain poorly quantified. According to the WHO [39], these costs are likely in the tens of billions of euros, with healthcare accounting for a significant portion [36]. For instance, Conti et al. [14] found that short-term somatic and mental health issues in the UK comprise over 40% of CM-related costs. Additionally, CM leads to increased risk of substance abuse, school and work absence, unemployment, and intergenerational violence, contributing to wider social and economic consequences [8,40]. SERENA will address this critical knowledge gap by providing current, cross-country estimates of these costs. This economic analysis will support decision-makers in understanding the long-term societal impact of CM and strengthen the case for investing in effective, preventive, and coordinated care systems, with potential relevance for diverse income settings globally.
Project Feasibility
SERENA is funded by Horizon Europe, Grant agreement ID: 101151854, involving 22 partners from 12 countries and operating under the standard Grant Agreement protocol with structured work packages and strict reporting times.
The project spans 2025–2029 and follows a three-step process that encompasses scoping reviews, quantitative studies, qualitative research, and economic evaluation. While work package interdependence means delays in one component may affect subsequent studies, this risk will be mitigated through strategic planning, interim deadlines, and close collaboration to ensure progress and knowledge transfer. All participating countries are Euro-CAN partners with confirmed data access, strengthening the feasibility of the project and ensuring consistency across national datasets. SERENA builds on strong institutional collaboration and methodological expertise, ensuring scientific rigour and project deliverability.
Conclusion
SERENA will advance the state-of-the-art in the field of CM by generating robust, multi-country evidence regarding CM and related use of HSC services across Europe. The project’s cross-sectoral and mixed-methods approach should considerably improve our understanding of the barriers to service access, allow us to estimate the societal costs of CM and prioritise future actions informed by lived experience and professional expertise.
Our findings will support evidence-based recommendations for early detection, improved service pathways, and policy development on national and European levels. These recommendations will aim to strengthen HSC system responses, promote cross-sector collaboration, and ultimately to improve outcomes for maltreated children and society at large.
Importantly, the evidence generated by SERENA is designed to be transferable beyond Europe, providing insights and methodological frameworks that can inform policy and practice globally, across different economic settings.
Author Contributions
CQ conceptualised the study. All main authors contributed to the design of the study. CQ wrote the manuscript with the help of DOL, YS, NB, MB, JC, LC, TGK, DL, KL, AJ, LH, PF, GN, AN, UN, SB. All authors reviewed and edited the manuscript.
Funding
This work was supported by the European Union under HORIZON Europe SERENA project (Grant agreement 101151854). Views and opinions expressed are however those of the authors only and do not necessarily reflect those of the European Union. Neither the European Union nor the granting authority can be held responsible for them.
Clinical trial number
not applicable.
Consent for publication
Not applicable
Availability of data and materials
In accordance with the rules of the European Commission and the consortium agreement signed between the SERENA project partners, only published information may be shared.
Acknowledgements
SERENA Co-Author Group: Jonathan Ablitt, Imola Antal, Christian Bachmann, Amrita Bandyopadhyay, Marie Berlin, Zoe Bezeczky, Myriam Borel, Lars Brannstrom, Johanne Bundgaard Bak, Olivier Degrand, Thomas Gabriel, Maryse Gadreau, Joel Gautschi, Rolando Granados, Chryssa Grylli, Sally Holland, Bethan Jones, Natasha Kennedy, Emilie Lajeune, Bérénice Lambert, Eva Laszlo, Alice McHale, Eva Mora-Theuer, Yann Mikaeloff, Cynthia Morgny, Stijn Peeters, Aurore Pelissier, Christine Peyron, Maria Roth, Maylis Sposito, Dragan Stoll, Solène Tapia, Frederick Thielen, Sarah Thompson, Christian Torp-Pedersen, Sophie Wallimann Meret.
Competing interests
The authors declare that they have no competing interests.
Ethics approval and consent to participate
SERENA conforms with the EU Horizon Ethics Guidelines. In particular, this protocol underwent ethical evaluation as part of the assessment process for the project SERENA funded under the horizon Europe programme. Following the recommendations of the ethics review, an external independent Ethics Advisor, specialised in research ethics and data protection law, was appointed within the project. A specific work package has been planned, with this Ethics Advisor, to ensure that all ethical rules are respected, and that regulatory, ethical, data access, material/data transfer approvals by the competent bodies are obtained for all research sites, so that ethics approval will be obtained in all participating countries and agencies. Data Management Plans will conform to European GDPR and country-specific regulations. Regarding quantitative studies, the primary individual data are already pseudonymised by the national data servers which comply with the GDPR. The different partners are granted access to the data of their country only once it has been pseudonymised or anonymised, and after obtaining specific authorisations or ethical approvals. They do not have access to re-identification keys, which guarantees that data remain pseudonymised. Regarding qualitative studies, all participants will be asked to give a written informed consent. Data will be systematically pseudonymised during transcriptions of the interviews conducted. Summary notes created from these files will not contain any information intended to make an identification possible. Dissemination processes will engage policymakers and health and social care professionals across the EU. Results will be published in peer-reviewed journals and presented at international meetings.
List of Abbreviations
Child maltreatment (CM)
Health and social care (HSC)
International Classification of Diseases 10th Revision (ICD-10)
Child protective services (CPS)
World health organization (WHO)
References
- Sethi D, Parekh N, Yon Y, Mikkelsen B. Progress in preventing child maltreatment in Europe. Lancet Child Adolesc Health. 2018 Nov;2(11):774–5.
- Scott KM, Smith DR, Ellis PM. Prospectively ascertained child maltreatment and its association with DSM-IV mental disorders in young adults. Arch Gen Psychiatry. 2010 Jul;67(7):712–9. [CrossRef]
- Cagney J, Spencer C, Flor L, Herbert M, Khalil M, O’Connell E, et al. Prevalence of sexual violence against children and age at first exposure: a global analysis by location, age, and sex (1990-2023). Lancet Lond Engl. 2025 May 24;405(10492):1817–36.
- Angelakis I, Gillespie EL, Panagioti M. Childhood maltreatment and adult suicidality: a comprehensive systematic review with meta-analysis. Psychol Med. 2019 May;49(7):1057–78. [CrossRef]
- Vink RM, van Dommelen P, van der Pal SM, Eekhout I, Pannebakker FD, Klein Velderman M, et al. Self-reported adverse childhood experiences and quality of life among children in the two last grades of Dutch elementary education. Child Abuse Negl. 2019 Sep;95:104051. [CrossRef]
- Jud A, Fegert JM, Finkelhor D. On the incidence and prevalence of child maltreatment: a research agenda. Child Adolesc Psychiatry Ment Health. 2016;10:17. [CrossRef]
- Bellis MA, Hughes K, Ford K, Ramos Rodriguez G, Sethi D, Passmore J. Life course health consequences and associated annual costs of adverse childhood experiences across Europe and North America: a systematic review and meta-analysis. Lancet Public Health. 2019 Oct;4(10):e517–28.
- WHO, 2020 WHO. Global status report on preventing violence against children. (2020). Available online: https://www.who.int/publications/i/item/9789240004191.
- European Union Agency for Fundamental Rights. Mapping Child Protection Systems in the EU – Update 2023. FRA - European Union Agency for Fundamental Rights. 2024. Available online: https://fra.europa.eu/en/publication/2024/mapping-child-protection-systems-eu-update-2023?page=8#read-online.
- Quantin C, Cottenet J, Chambers C, Kennedy N, Whelan S, Debelle G, et al. Hospitalisations for physical abuse in infants and children less than 5 years, 2013-2021: a multinational cohort study using administrative data from five European countries. Lancet Reg Health Eur. 2025 May;52:101270.
- Office for National Statistics. Child physical abuse in England and Wales [Internet]. [cited 2025 Sep 3]. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/crimeandjustice/articles/childphysicalabuseinenglandandwales/yearendingmarch2019.
- WHO. Child maltreatment [Internet]. 2024 [cited 2025 Sep 3]. Available online: https://www.who.int/news-room/fact-sheets/detail/child-maltreatment.
- Habetha S, Bleich S, Weidenhammer J, Fegert JM. A prevalence-based approach to societal costs occurring in consequence of child abuse and neglect. Child Adolesc Psychiatry Ment Health. 2012 Nov 16;6(1):35. [CrossRef]
- Conti G, Pizzo E, Morris S, Melnychuk M. The economic costs of child maltreatment in UK. Health Econ. 2021 Dec;30(12):3087–105.
- Connolly M, Katz I. Typologies of Child Protection Systems: An International Approach. Child Abuse Rev. 2019 Sep 1;28:381–94. [CrossRef]
- Fluke JD, Tonmyr L, Gray J, Bettencourt Rodrigues L, Bolter F, Cash S, et al. Child maltreatment data: A summary of progress, prospects and challenges. Child Abuse Negl. 2021 Sep;119(Pt 1):104650. [CrossRef]
- Cowley LE, Lamela D, Drabarek K, Rodrigues LB, Ntinapogias A, Naughton A, et al. Defining child maltreatment for research and surveillance: an international, multi-sectoral, Delphi consensus study in 34 countries in Europe and surrounding regions. Lancet Reg Health Eur. 2025 Mar;50:101196.
- Otterman G, Nurmatov UB, Akhlaq A, Korhonen L, Kemp AM, Naughton A, et al. Clinical care of childhood sexual abuse: a systematic review and critical appraisal of guidelines from European countries. Lancet Reg Health Eur. 2024 Apr;39:100868.
- Roehrkasse AF, Becker L, Wildeman C, Fallesen P. Introducing a new data resource for comparative child welfare research: The ROCKWOOL-Duke global child welfare database. Child Youth Serv Rev. 2023;152:107075. [CrossRef]
- Mora-Theuer EA, Klomfar S, Ramazanova D, Grylli C, Kletecka-Pulker M, Völkl-Kernstock S, et al. Cohort analysis of child abuse and neglect cases treated during the initial 2 years of a programme to support hospital-based child protection work in Austria. BMJ Open. 2023 Jul 14;13(7):e071536. [CrossRef]
- Bergman JEH, Perraud A, Barišić I, Kinsner-Ovaskainen A, Morris JK, Tucker D, et al. Updated EUROCAT guidelines for classification of cases with congenital anomalies. Birth Defects Res. 2024 Feb;116(2):e2314. [CrossRef]
- Nurmatov U, Cowley LE, Rodrigues LB, Naughton A, Debelle G, Alfandari R, et al. Consensus building on definitions and types of child maltreatment to improve recording and surveillance in Europe: protocol for a multi-sectoral, European, electronic Delphi study. BMJ Open. 2023 Dec 12;13(12):e076517. [CrossRef]
- Pluye P, Hong QN. Combining the power of stories and the power of numbers: mixed methods research and mixed studies reviews. Annu Rev Public Health. 2014;35:29–45. [CrossRef]
- Boyatzis CJ, Baloff P, Durieux C. Effects of perceived attractiveness and academic success on early adolescent peer popularity. J Genet Psychol [Internet]. 1998 Sep [cited 2025 Mar 31];159(3). Available online: https://pubmed.ncbi.nlm.nih.gov/9729839/.
- Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3:77–101.
- Hakkaart-van Roijen l, Peeters S, Kanters T. Costing manual: Methods and Reference Prices for Economic Evaluations in Healthcare [Internet]. 2024. (Commissioned by the National Health Care Institute). Available from: file://///chu-dijon/doc/dl/BAGW1802770/Downloads/Module+-+Costing+manual.pdf.
- Koopmanschap MA, Rutten FF, van Ineveld BM, van Roijen L. The friction cost method for measuring indirect costs of disease. J Health Econ. 1995 Jun;14(2):171–89. [CrossRef]
- Jud A, Fluke J, Alink LRA, Allan K, Fallon B, Kindler H, et al. On the nature and scope of reported child maltreatment in high-income countries: opportunities for improving the evidence base. Paediatr Int Child Health. 2013 Nov;33(4):207–15. [CrossRef]
- Baldwin JR, Reuben A, Newbury JB, Danese A. Agreement Between Prospective and Retrospective Measures of Childhood Maltreatment: A Systematic Review and Meta-analysis. JAMA Psychiatry. 2019 Jun 1;76(6):584–93. [CrossRef]
- Pearce LA, Borschmann R, Young JT, Kinner SA. Advancing cross-sectoral data linkage to understand and address the health impacts of social exclusion: Challenges and potential solutions. Int J Popul Data Sci. 2023;8(1):2116. [CrossRef]
- Jud A, Mitrovic T, Portmann R, Gonthier H, Fux E, Koehler J, et al. Multi-sectoral response to child maltreatment in Switzerland for different age groups: Varying rates of reported incidents and gaps in identification. Child Abuse Negl. 2021 Jan;111:104798. [CrossRef]
- Milidou I, Merrild CH, Frost L, Charles AV, Kjeldsen HC, Søndergaard C. Suspicion of child maltreatment: Knowledge and experiences with mandatory reports to social services among general practitioners in Denmark in 2019-20. Child Abuse Negl. 2023 May;139:106132. [CrossRef]
- Kruger, H. “The Discrepancy between the Criminal Capacity and Delictual Accountability of Children: A Children’s Rights Perspective". J Contemp Roman-Dutch Law. 2022;85(1):68–90.
- Herbert JL, Bromfield L. Multi-disciplinary teams responding to child abuse: Common features and assumptions. Child Youth Serv Rev. 2019;106:104467. [CrossRef]
- WHO. Framework to Implement a Life Course Approach in Practice. Geneva: WHO. Licence: CC BY-NC-SA 3.0 IGO [Internet]. [cited 2025 Sep 3]. Available online: https://www.who.int/publications/i/item/9789240112575.
- Gilbert R, Widom CS, Browne K, Fergusson D, Webb E, Janson S. Burden and consequences of child maltreatment in high-income countries. Lancet Lond Engl. 2009 Jan 3;373(9657):68–81.
- World Health Organization. INSPIRE: Seven Strategies for Ending Violence against Children. World Health Organization; 2016. Accessed August 25, 2025. Available online: https://apps.who.int/iris/handle/10665/207717.
- World Health Assembly. Strengthening the role of the health system in addressing violence, in particular against women and girls, and against children. [Internet]. 2014. Report No.: 67. Available online: https://iris.who.int/handle/10665/162855.
- Sethi D, Bellis M, Hughes K, Gilbert R, Mitis F, Galea G. European report on preventing child maltreatment [Internet]. World Health Organization. Regional Office for Europe; 2013 [cited 2025 Apr 1]. Available online: https://iris.who.int/handle/10665/326375.
- Thielen FW, Ten Have M, de Graaf R, Cuijpers P, Beekman A, Evers S, et al. Long-term economic consequences of child maltreatment: a population-based study. Eur Child Adolesc Psychiatry. 2016 Dec;25(12):1297–305. [CrossRef]
Figure 1.
Institutions and countries involved in the SERENA project.

Figure 2.
Interconnected studies from the SERENA collaborative project. The project deals with a cross-sectoral, mixed-methods, multi-study design comprising several nationwide longitudinal quantitative studies, qualitative studies, and a study of the societal costs of CM. These findings and the participatory analysis and interpretation involving HSC professionals and ASCM will lead to evidence-based recommendations.
Figure 2.
Interconnected studies from the SERENA collaborative project. The project deals with a cross-sectoral, mixed-methods, multi-study design comprising several nationwide longitudinal quantitative studies, qualitative studies, and a study of the societal costs of CM. These findings and the participatory analysis and interpretation involving HSC professionals and ASCM will lead to evidence-based recommendations.
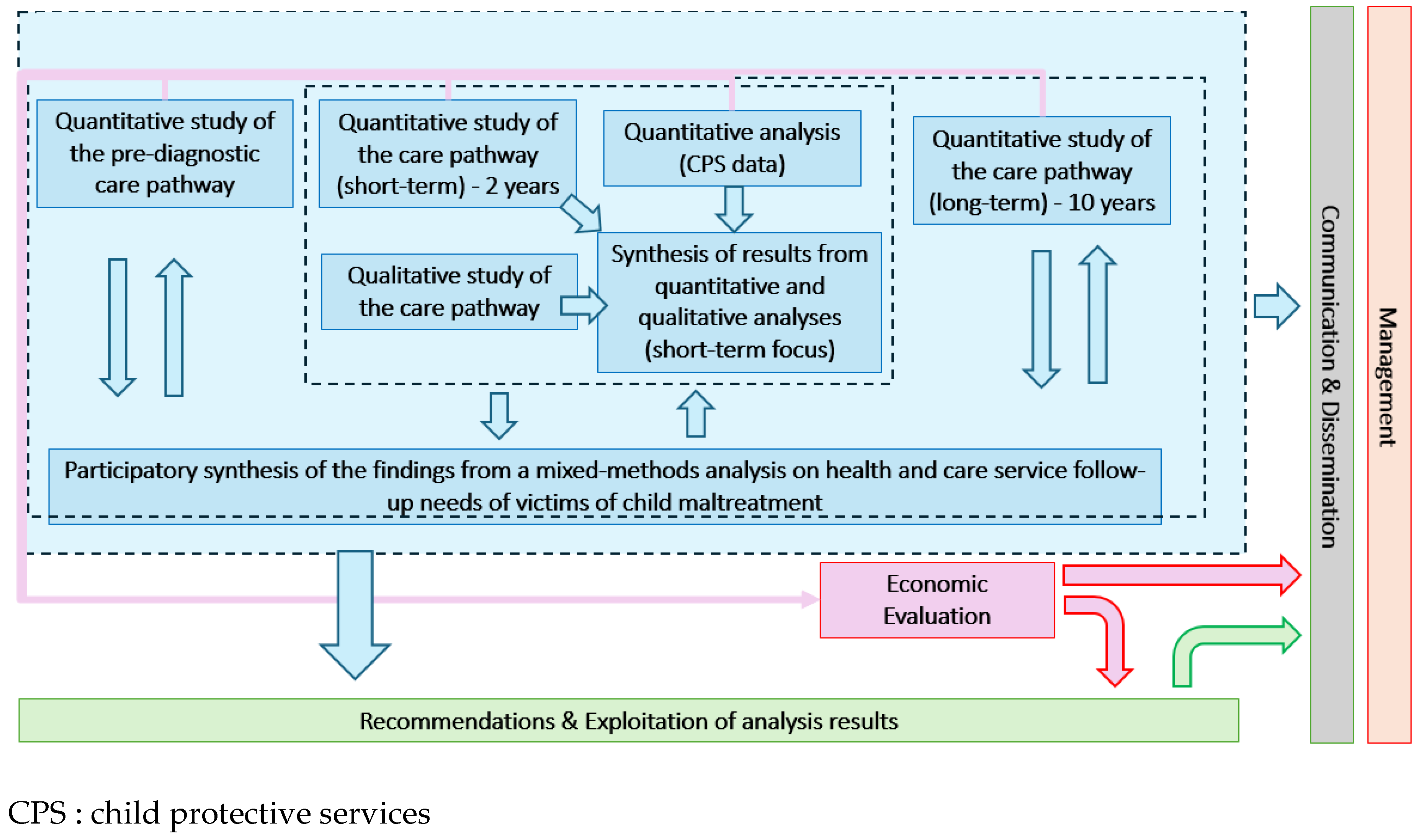
Figure 3.
SERENA’s Three-Step Process. The project follows a sequential three-step approach, which outlines the process from initial scoping reviews and data collection to mixed-method analyses and the development of evidence-based recommendations.
Figure 3.
SERENA’s Three-Step Process. The project follows a sequential three-step approach, which outlines the process from initial scoping reviews and data collection to mixed-method analyses and the development of evidence-based recommendations.
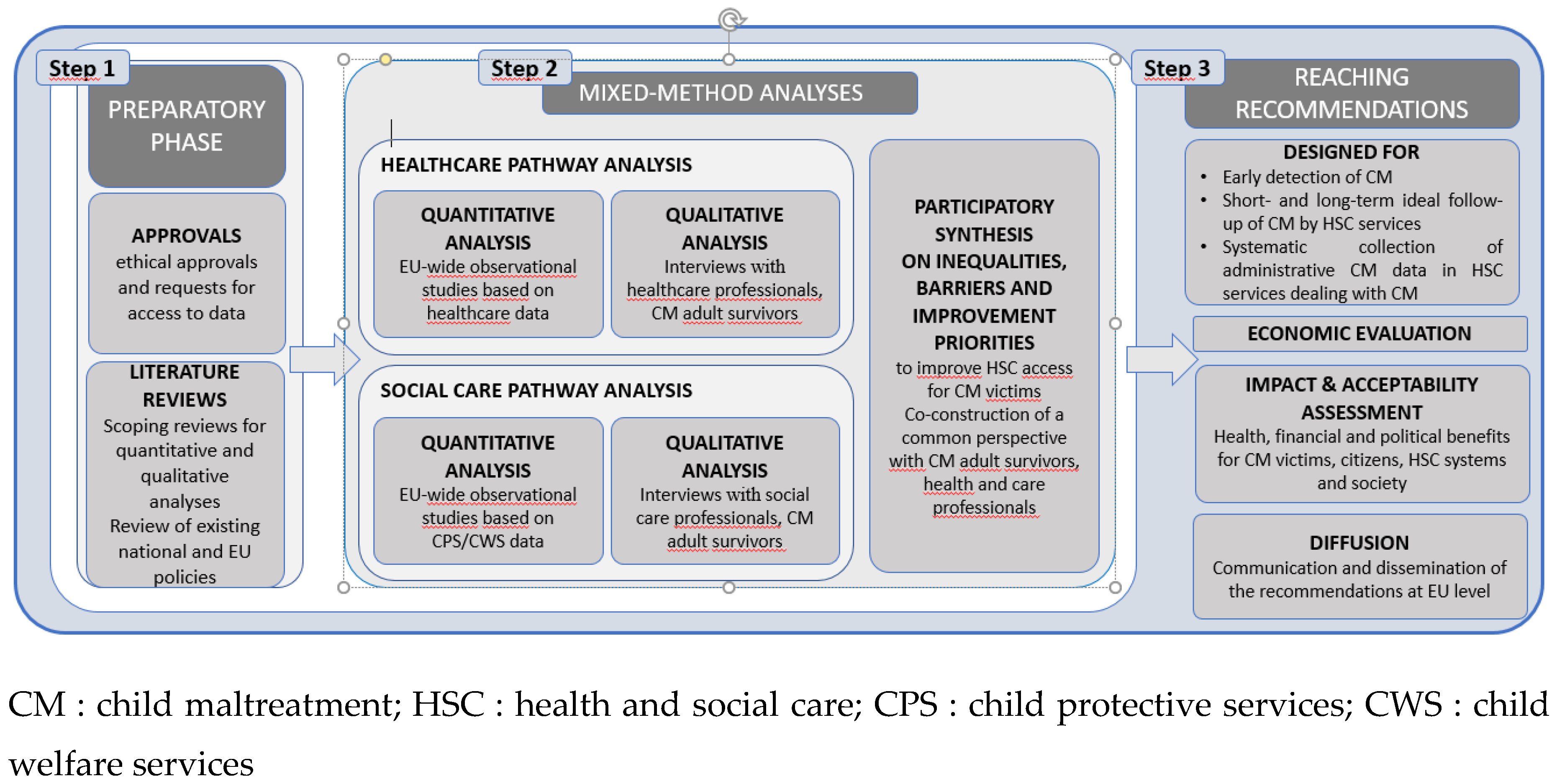

Table 1.
Summary of target groups and expected impact of the SERENA project.
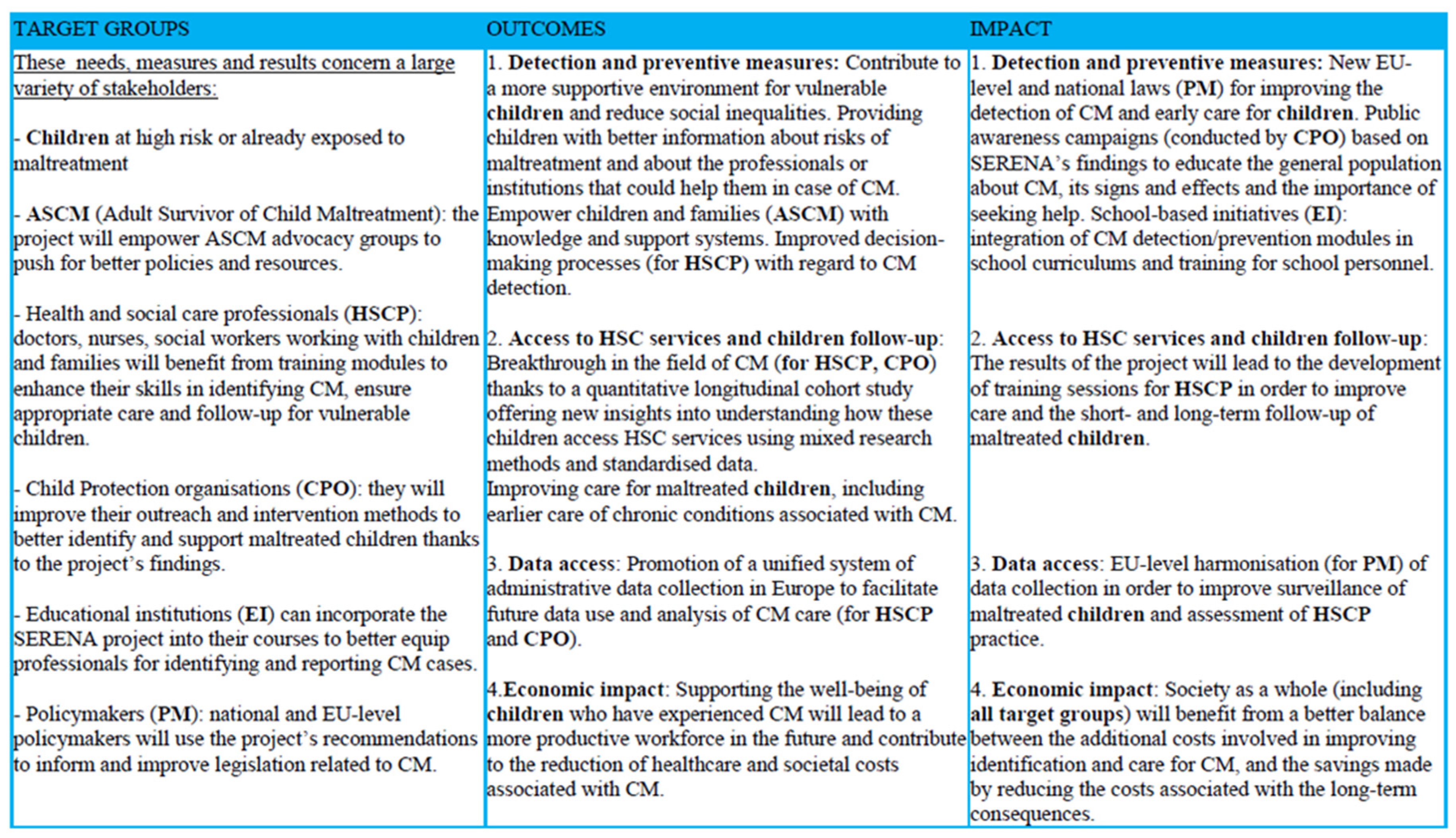 |
CM : child maltreatment; HSC : health and social care; CPS : child protective services; ASCM : adult survivors of child maltreatment.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



