
Submitted:
04 November 2024
Posted:
05 November 2024
You are already at the latest version
Abstract
The ever-increasing problem of chronic, non-healing wound treatment is a challenge in contemporary medicine. The study aims to verify the effect of a designed dressing containing coating involving oxygenating factors on promoting wound healing in all healing phases in a single clinical case. The alginate-based coating, which incorporates the oxygenating factor, was produced. The obtained surface physicochemical features were examined using FTIR and AFM microscopy. The bandage support was modified with elaborated coating and applied to the patients who suffered from chronic wounds (treated with non-modified commercially available bandage) and required treatment at least 3 months before starting the study. During bandage application, the chosen characteristics of the wound healing process were examined. Histological evaluation of granulation tissue confirmed the presence of fibroblasts, hemorrhage, and lymphocytes during the second week of treatment. Moreover, epithelization tissue in the third week of treatment exhibited the presence of keratinocytes. The 100% wound reduction was observed between 3-4 weeks of treatment with modified dressing. The applied coating, which provides a smooth surface of contact with the wound, inducing the remodeling phase in up to 4 weeks of treatment, can be recommended to be developed for hard-to-heal wound treatment.
Keywords:
polyelectrolyte coating
; oxygenating factor
; platelet-rich plasma
; dressing
; non-healing wound
; granulation
; epithelialization
1. Introduction
Modern medicine is struggling with the ever-increasing problem of chronic, non-healing wound treatment [1]. It is associated with aging societies, the lifestyle of people in developed countries, and constantly increasing urbanization, resulting in a growing number of injuries, including traffic ones [2]. In addition, chronic wounds are the reason for professional absenteeism, cause individuals to withdraw from social life, and, in extreme cases, may lead to psychiatric disorders headed by depression [3]. Furthermore, considering the high cost of long-term – often lasting several months – outpatient treatment [4,5], whose efficacy varies between patients, it is critical to provide fast-acting, effective dressing that significantly supports ulcer healing.
Chronic wounds are difficult-to-heal, physiologically impaired wounds/ulcers in which the normal healing process has been disrupted at one or more phases [6,7]. In addition, the underlying pathology (e.g., comorbidities like cardiovascular disease or diabetes) usually cause a delay in the healing process. Moreover, non-physiological factors (quality of healthcare services, social context, or patient mental state) are also identified as the ones influencing wound healing [8]. Contemporary medicine applies several approaches to heal chronic wounds, including treatment based on managing controllable process factors (e.g., nutritional support, infections removal, and mechanical protection) [9], target delivery of active agents [10], or hyperbaric oxygen therapy [11,12], and the usage of sub-atmospheric pressure dressings [13]. On the opposite sites are methods based on the tissue-engineering, like human skin equivalents [14] or autologous skin transplantation [15]. Other strategies might be the usage of platelet-rich plasma (PRP) [16] or the application of recombinant growth factors [17].
As a result, in therapies based on PRP, the time of patients' hospitalization can be reduced [18]. Nonetheless, due to the variable concentration of PRP and lack of standardized procedures for application, studies' pieces of evidence can be unreliable, which impedes clinical usage in patients [19,20].
Oxygen is essential in wound healing as it participates in many processes leading to tissue restoration, including angiogenesis, fibroplasia, or cell proliferation [21,22]. On the other hand, limiting the oxygen supply to a wound area impedes and delays healing [23]. Furthermore, it has been shown that oxygen transport to the tissue is disturbed in chronic wounds, which results in high hypoxia [21,24], wherein extreme hyperoxia can promote the formation of reactive oxygen species, causing oxidative stress, mitochondrial apoptosis and growth retardation [23]. Thus, it cannot be surprising that scientists try to improve wound healing by enhancing tissue oxygenation, such as employing special dressings that maintain adequate oxygen levels by continuous delivery [25,26,27]. Incorporating oxygenating factors into the plasters aimed at wound care is another possible option. Perfluorocarbons (PFCs), known for absorbing large amounts of oxygen, can be used for that purpose. PFCs have been previously applied in wound healing. For example, Li and coworkers described a perfluorodecalin-based supersaturated oxygen emulsion supporting eye regeneration after chemical injuries [28]. The works on improving dressing construction for wound healing are still been developed [29,30,31,32,33].
Herein, we report the cases of applying the dressing containing oxygenating factors to promote hard-to-heal wound healing and its effect. A subassembly of the dressing was qualified for the clinical trial to cooperate with the previously developed platform containing platelet growth factor, constructed of bandage support with oxygenating coating.
The study aims to assess the effectiveness and clinical usefulness of modified dressings in combination with autologous platelet-rich plasma. The work addresses the treatment of chronic, non-healing wounds in which the healing process has been disrupted at one or more phases. The system involving an oxygenating layer- patient platelet-rich plasma interface has been constructed. The coatings, incorporating oxygenating factors, were prepared on the bandage support for that purpose. The patient platelet-rich plasma was transferred to the patient's previously prepared wound area. The wound was covered with a designed bandage, and the dressing was changed every 7 days.
It should be noted that the bioethics committee approved the studies. In addition, the patients participating in the study were informed in detail about the methodology and purpose of the experiment and then gave written informed consent to participate.
2. Materials and Methods
2.1. Materials
Reagents: 1-Bromoheptadecafluorooctane (Sigma-Aldrich, Munchen, Germany); phosphate-buffered saline (PBS) (Biomed Lublin, Lublin, Poland); MilliQ water; bandage support AQUACEL (ConvaTec, UK); sodium alginate (Sigma-Aldrich (St. Louis, MO, USA); FluoSpheres carboxylate modified microspheres 0.2µm, yellow-green fluorescent (Invitrogen Molecular Probes, Eugene, Oregon, USA).
2.2. Methods
2.2.1. Preparation of Polyelectrolyte Layer Coating
The following solutions were used to prepare the layer coatings for spectroscopic and microscopic assessment and/or to modify the bandage support: 2.2% sodium alginate in PBS (ALG); 1-Bromoheptadecafluorooctane liquid in the original liquid concentration from the brand bottle (PFC); 2.5% CaCl2.
The polyelectrolyte layer coating forming was described previously [34]. Briefly, a 2.2% solution of sodium alginate in PBS (ALG) or alginate–perfluorooctyl (ALG-PFC)—made from the mixture of 1-Bromoheptadecafluorooctane and alginate (2.2%) in a 1:9 volume ratio layers cross-linking using 2.5% CaCl2 or not were produced. Afterward, dried under atmospheric pressure for 45 minutes.
Applied coatings: alginate (ALG)—made of 2.2% sodium alginate; alginate cross-linked (ALG)net—made of ALG cross-linked with 2.5% CaCl2; alginate–perfluorooctyl (ALG-PFC)—made from the mixture ALG-PFC; alginate–perfluorooctyl cross-linked ((ALG-PFC)net)—made by cross-linking ALG-PFC using 2.5% CaCl2.
The coatings were tested regarding roughness changes after applying an oxygenating agent within the coating. For this purpose, the polyelectrolyte layer coating ALG and ALG-PFC were examined using AFM. Furthermore, the coating material was examined in terms of durability during long-term storage, which is essential in case of the need for long-term storage of coating-modified dressings. For this purpose, the coating material after 10 months of storage (4◦C) was examined using FT-IR.
Furthermore, microscopic confirmation of oxygenating elements within the coating was performed.
2.2.2. PFC Labeling
The suspension of fluorescent microspheres (µB-FITC) was incubated with PFC solution in a 1:100 (v/v) ratio for 4 minutes. Afterward, PFC was washed twice in PBS at 1600 rpm for 3 minutes to remove unabsorbed µB-FITC. PFC coated with µB-FITC was obtained (PFC_µB-FITC).
2.2.3. Bandage Modification
For clinical trial purposes, a square bandage support with an area of around 25 cm2 was covered with a coating layer of (ALG-PFC)net. Bandages modified in this way were applied to the patients in combination with autologous platelet-rich plasma according to the presented model (Figure 1).
The use of an autologous plasma layer is intended to increase the adhesion forces between the dressing and the wound bed, facilitating direct contact with the regenerated tissue. Some authors observed that encapsulation of PFC with amphiphilic biopolymers (e.g., charged proteins like albumin) enhances PFC biocompatibility and prevents coalescence and flocculation [35,36].
Figure 2 shows a view of modified dressings packaged sterile for use on patients.
2.2.4. AFM Evaluation
A Multimode 8 Nanoscope atomic force microscope (AFM, Bruker, Billerica, MA, U.S.A.) was used to image the samples' surfaces. Silicon cantilevers with a spring constant of ca. 5 Nm-1 (TapDLC-150, BudgetSensors, Sofia, Bulgaria) were applied for imaging in PeakForce TappingTM microscopy mode. The sample preparation procedure includes the application of 150 L of solution on the clean mica plate, V1 grade (NanoAndMore GmbH, Wetzlar, Germany). After 10 min, the plates were rinsed with deionized water and dried under a gentle stream of argon.
2.2.5. Fourier Transform Infrared (FT-IR) Spectroscopy
The samples' measurement was performed with FT-IR spectroscopy using an attenuated total reflection accessory with diamond crystal. The measurements were performed with a resolution of 4 cm−1; typically, 32 scans were taken for each sample. A 10µl drop of solution was deposited in the crystal and left to dry under a gentle air stream.
2.2.6. Scanning Electron Microscopy and Fluorescence Microscopy Evaluation
For scanning electron microscopy evaluation, the prepared samples of coatings were lyophilized and deposited on microscope tables. After that, the specimens were sputtered with gold and placed in a microscope measuring chamber. The samples were assessed by scanning electron microscope TM-1000 (Hitachi, Tokyo, Japan).
For fluorescence observation, the layer coatings were placed in the wells of a culture plate in a physiological saline solution and photographed using an Olympus IX70 (Olympus, Tokyo, Japan) fluorescence microscope.
2.2.7. Confocal Microscopy
For confocal microscopy evaluation, the samples of layer coatings prepared on microscopic glass were examined. The measurements were performed using Olympus FV4000 microscope (Evident Europe GMBH), equipped with 30xsilicone lens-zoom 2.84, laser 488. The detection at 500-580nm was applied.
2.2.8. Evaluation of the Wettability Angle of Polyelectrolyte Shells
The wettability angle of the water positioned on the polypropylene support coatings, or the support alone (as a control) was analyzed. The fluid was dispensed from a manually controlled syringe. The sessile drop method was used to measure the contact angle using the SEO Phoenix 300 assembly and a DLT-Cam Pro 5MP USB 2.0 camera with dedicated software. The recorded water droplet images were then analyzed using ImageJ software applying a wave function algorithm.
2.2.9. Histopathology
The study was carried out according to the following procedure:
(1) the skin sample of a square shape of about 1 cm2 was immersed in 10% formalin.
(2) The samples were embedded in paraffin
(3) The material was cut into pieces with a thickness of 4 μm.
(4) Paraffin sections were stained by the routine hematoxylin-eosin method.
A chosen patient's skin samples were analyzed using microscopic evaluation.
2.2.10. Patients & Methods
Study design: The modified cross-over design of randomized clinical trials (RCT) was applied. The trial was done on patients who suffered from chronic wounds. Due to the specificity of wound healing, the order in which the patient receives interventions was not randomized. Thus, in this design, participants start with a non-modified bandage and switch to a modified one. The results are then compared within the same case.
The most common chronic diseases in patients were permanent atrial fibrillation, arterial hypertension, type II diabetes, and obesity. The causes of ulceration in the examined cases were post-traumatic, postoperative changes, generalized scleroderma, and chronic venous ulcer.
The participants were the patients treated with unmodified bandages who still suffered from chronic wounds during treatment over 3 months and more and who received, after that, the modified bandage.
Inclusion criteria
The criterion for inclusion in the study was the presence of a non-healing wound for more than 3 months despite treatment with an unmodified bandage used at the local center.
Exclusion criteria
- Patients with leg ulcers during atherosclerosis of the lower limbs and chronic venous insufficiency before treatment of the underlying disease.
- Patients with chronic end-stage heart failure NYHA4 addicted to alcohol and psychoactive substances,
- Patients with severe mental disorders were not promising to comply with medical recommendations.
Patients' characteristics
Five patients participated in the study: four men and one woman. The average age was: 65.8.
Preliminary examination
Each patient qualified for the clinical trial has undergone basic laboratory tests and an ultrasound examination of the arteries of the lower limbs and the veins of the lower limbs to assess their efficiency.
Procedure
After the standard wound cleaning of necrotic tissue, fibrin, and disinfection of its surface, about 5 ml of peripheral venous blood was collected and then centrifuged at 3,000 revolutions per minute for 5 minutes. Then, the upper layer of platelet-rich plasma was collected from the test tube and transferred to the patient's previously prepared wound. Finally, the wound was covered with a bandage prepared as described above. The dressing was changed in the above manner once every 7 days in the Wolski Hospital.
Ethics approval and consent to participate
The research bioethics committee of the Medical Centre of Postgraduate Education approved the trial protocol Number 31/2022 on March 9, 2022. Each patient participating in the clinical trial was informed in detail about the type and purpose of the study, the possible benefits of participating in the experiment, and the possible side effects. In addition, each patient signed an informed consent form to participate in the study. Successively admitted outpatients with non-healing wounds were included in the trial.
2.2.11. Statistical Analysis
Statistica 7.1 software was used to perform statistical calculations. Each time, mean values, the significance of the difference, and standard deviations were determined. Values with a p-value below 0.05 were considered to indicate significance.
3. Results
3.1. AFM Evaluation of Morphology of Oxygenated Coating Layer
Topography analysis can indirectly confirm the presence of functional elements within the coating. In order to characterize the surface topography of the prepared coating at the production level, atomic force microscopy (AFM) was applied. AFM visualization of the ALG and ALG-PFC layer deposited onto gold-covered mica substrate is presented in Figure 3.
The ALG and ALG—PFC layers (with root mean square average of profile height deviations from the mean line (Rms) equal to 0.88 and 2.33 [nm], respectively) show the structure with evenly marked active centers over the entire surface.
In the case of PFC incorporation in the ALG sample, a 62% increase in Rms was observed, which might be caused by the appearance of additional centers compared with ALG alone. Figure 4 presents the ALG-PFC profile.
3.2. Fourier Transform Infrared (FT-IR) Spectroscopic Evaluation
The presence of functional elements within the coating was confirmed using FT-IR spectroscopy. It can be noted that in ALG-PFC, besides the characteristic bands for ALG-like stretching vibrations of O–H bonds, which appear in the range of 3000–3600 cm−1, the bands appeared at 1600 and 1414 cm-1, which can be attributed to stretching vibrations of the carboxylate group can be observed. Due to PFC involvement, the bands at 1143 and 1200 cm-1 appeared, which can be attributed to C-F bonds (Figure 5).
3.3. Microscopic Evaluation of Morphology of Coating and Oxygenating Elements Presence
The SEM examination of the morphology of coating with incorporated oxygenating elements was performed to visualize the oxygenating elements. The exemplary images of the analysis are presented in Figure 6.
Within the ALG-PFC, the PFC elements of spherical shape were observed (Figure 6AB). The oxygenating element of about 260 µm can be observed in the field of view in Figure 6B.
Moreover, fluorescence microscopy was applied to assess coating layer morphology. In Figure 7. the exemplary ALGnet and (ALG-PFC)net coating morphology can be observed. The ALGnet layer represents a relatively even structure (Figure 7A). On the other hand, (ALG-PFC)net exhibits the presence of elements of spherical shape within the layer structure (Figure 7B).
In addition to physicochemical methods, fluorescence microscopy was used to confirm oxygenating elements' presence within the layer coating structure. For this purpose, the PFC_µB-FITC obtained using the method described above was applied. Figure 8 shows the fluorescent microscopic picture of the (ALG—PFC_µB-FITC)net within the layer coating structure.
The spherical elements with fluorescent coating can be observed within the coating structure, confirming the oxygenating elements' involvement in it (Figure 8A,B). The magnitude of the oxygenating element can be observed in Figure 8B. Due to the interaction between fluor present in PFC and oxygen present in carboxyl groups of µB-FITC, the PFC spherical elements are coated by 0,2 µm fluorescent microspheres.
Furthermore, confocal microscopy was applied to confirm oxygenating elements' presence within the coating layer structure. Figure 9A,B. presents the exemplary images of the assessment.
3.4. Water Contact Angle Evaluation
The coating wettability was assessed by measurement of the contact angle for water based on the relationship between the specific surface energy of the solid, interfacial energy between the solid and liquid, and surface energy of water, according to Young's equation. The coatings ALG and ALG-PFC deposited on the polypropylene support were tested (Figure 10 and Figure 11).
It was found that the involvement of PFC in the ALG layer did not significantly change the wettability compared to the ALG layer alone. Moreover, the placement of tested coatings did not significantly change the wettability parameters of the applied support.
3.5. Wound Treatment
The patients' data and wound characteristics before treatment with modified bandages are presented in Table 1 and Table 2, respectively.
The pictures of the patients' wounds during treatment with modified bandages are presented in Figure 12, Figure 13, Figure 14, Figure 15 and Figure 16. The results of the patients' wounds examination are listed below:
Patient 001M: the wound area of 13 cm2 exhibited granulation tissue covering during 14-day treatment (after that time, the patient discontinued treatment).
Patient 002M: the wound of 7 cm length exhibited granulation tissue covering for one week; during the next two weeks, epithelial cells grow, and during the fourth week, the resistant epidermis can be observed (100% epithelialization at 29 days of treatment).
Patient 003M: the wound of the area of 3 cm2 exhibited granulation tissue covering for one week; during the next two weeks, epithelial cells grew, and the resistant epidermis during the 22-day treatment.
Patient 004M: the wound of the area of 8 cm2 exhibited granulation tissue covering for one week; during the second week, epithelial cells grew; during the third week, the resistant epidermis can be observed with 100% epithelialization at 21 days of treatment.
Patient 005F: an oblong wound of 3 cm2 with a length of the longer side of 3 cm exhibited granulation tissue covering for two weeks; during the next two weeks, epithelial cells grew, and the resistant epidermis formed during 28-day treatment.
In the case of all treated wounds with accomplished treatment, it was observed that the wound shrinks, and the granulation tissue transforms into scar tissue. It can be observed that the granulation tissue covers the bottom and walls of the wound, gradually filling it completely. Epithelial cells grow from the edges to the center of the wound and eventually form a durable, resistant epidermis. In Figure 12-2., Figure 13-2, Figure 14-2, Figure 15-2, Figure 16-2C, 3C, a newly formed epidermis can be observed.
Figure 16 presents pictures of the wounds of selected patients. At 1-2 weeks of treatment, granulation tissue is visible, indicating the hemostasis phase (Figure 16-1B, 1C; 16-2B, 2C). Epithelialization is visible at two weeks of treatment, indicating that the remodeling phase is progressing.
The percent linear reduction of wound size during individual weeks of treatment was assessed using the following formula:
where: ln- a maximum wound size after n-week of treatment, n = 1,2,3…
Table 3 summarizes R values for patients 002M, 003M, 004M, and 005F during the following weeks of treatment.
No significant differences were observed in the R-value for treatment in the first and second weeks. Moreover, no significant differences in the R-value for treatment in the third and fourth weeks were observed. However, a difference was observed in the rate of wound size reduction between the first two weeks and the following two weeks of treatment.
The mean percent linear reduction of Patients' (002M-005F) wound size during individual weeks of treatment with a trend line is presented in Figure 17. It can be observed that the R rate achieves a 100% value between 3-4 weeks with a correlation rate of 0.878.
In some approaches, different materials are recommended for each phase of healing, which is made possible by the dressings available on the market. During the hemostasis and inflammation phases, bacteria and debris are eliminated, exudates are coagulated, and blood clots [37,38].
In the inflammatory phase of wound healing (with a difficult-to-heal wound), dressings should be used which, unlike dressings like e.g., gauze, absorb a large part of the wound exudates, causing quick drying of the wound surface [39,40], stimulate cleansing without removing moisture, often containing an antimicrobial agent [27,41,42,43].
Different studies indicated the role of growth factors in wound healing processes, including chronic wounds. Platelet-derived growth factors may play a role in the regulation of cellular response [44,45] among other biologically active polypeptides (like epidermal growth factor, transforming growth factor-β, vascular endothelial growth factor) in hemostasis and inflammation, e.g., stimulating the chemotaxis of macrophages, neutrophils, and fibroblasts, supporting the initiation of the inflammatory response, what brings to a conception of synergic application along with the bandage. It can be noted that there are reports on recombinant platelet-derived growth factor Becaplermin application for supporting the treatment of ulcers resulting from calciphylaxis as well as the treatment of nondiabetic chronic ulcers of various etiologies [46]. On the other side, despite the indisputable increase in the healing rate, due to the high cost of treatment and the long list of adverse reactions, including the risk of malignancy occurrence (US Food and Drug Administration warning from 2008) [47] the application of this therapeutic is limited [48].
In the next healing phase – proliferation, the granulation process may begin when the inflammation disappears, and the wound is clean. It is the production of the base necessary for the regeneration of the surface layers of the skin and the epidermis.
In this case, it is also favored to maintain a humid environment, e.g., using dressings containing hydrogel.
The last stage of wound healing is the remodeling (maturation) phase. The wound shrinks, and the granulation tissue transforms into scar tissue. Maintaining a humid environment with a low absorption capacity is still advantageous. The task of the dressing is also to secure the recently formed epidermis.
Some dressings provide wound healing in all overlapping phases (hemostasis and inflammation, proliferation, remodeling); however, in the case of chronic wounds, the action stops at the inflammatory phase (e.g., Endoform® - The Natural Dermal Template), which is a natural extracellular matrix obtained from the tissues of the sheep stomach (KIKGEL, EU) [49]. Our dressing provides chronic wound healing, including the remodeling phase. The image of a wound healing against the background of the granulation and epithelization model [50] is presented in Figure 18.
The time of appearance of phases of proliferation involving granulation and remodeling involving epithelialization of treated chronic wounds was close to the time expected to heal non-chronic wounds [51], which is presented with representative histopathological photographs of the preparations in these phases in Figure 19. The histopathology of granulation tissue was presented during the second week of treatment, and it shows fibroblasts, hemorrhage, and lymphocytes' presence. Histopathology of epithelization tissue in the third week of treatment exhibits keratinocytes' presence.
The applied design of dressings, which involves maintaining a humid environment and oxygenation-enhancing coating, allows for the healing of non-healing wounds in treated patients for up to 4 weeks.
However, due to the limited group of patients, it is impossible to assess the impact of chronic diseases on wound healing time using a modified dressing at this study stage.
5. Conclusions
The oxygenating layer coating for dressing modification can be developed for non-healed wound treatment. The system involving an oxygenating coating layer – patients' platelet-rich plasma interface allowed to heal wounds that had not healed so far in the examined patients, regardless of their etiology and size. Moreover, performing the dressing and further care of the wound while using the tested system excludes the patient's contribution, might reduce the number of errors made during unprofessional dressing changes, and may enhance the comfort of a patient's life.
Author Contributions
Conceptualization, T.M., A.G., A.L. and L.H.G.; methodology, T.M., A.G., A.L. and L.H.G.; soft-ware, X.X.; validation, T.M., and L.H.G.; formal analysis, T.M., A.K. and L.H.G.; investigation, T.M., A.G., A.L., M.M., L.O., M.S., M.D., and L.H.G.; writing—original draft preparation, A.K. and L.H.G.;. writing—review and editing, T.M., L.H.G.; visualization, A.K.; supervision, T.M., L.H.G.All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Eriksson, E.; Liu, P.Y.; Schultz, G.S.; Martins-Green, M.M.; Tanaka, R.; Weir, D.; Gould, L.J.; Armstrong, D.G.; Gibbons, G.W.; Wolcott, R.; et al. Chronic wounds: Treatment consensus. Wound Repair Regen. 2022, 30, 156–171. [Google Scholar] [CrossRef] [PubMed]
- Sen, C.K. Human Wound and Its Burden: Updated 2020 Compendium of Estimates. Adv. Wound Care 2021, 10, 281–292. [Google Scholar] [CrossRef] [PubMed]
- Olsson, M.; Järbrink, K.; Divakar, U.; Bajpai, R.; Upton, Z.; Schmidtchen, A.; Car, J. The humanistic and economic burden of chronic wounds: A systematic review. Wound Repair Regen. 2019, 27, 114–125. [Google Scholar] [CrossRef] [PubMed]
- Chan, B.; Cadarette, S.; Wodchis, W.; Wong, J.; Mittmann, N.; Krahn, M. Cost-of-illness studies in chronic ulcers: A systematic review. J. Wound Care 2017, 26 (Suppl. 4), S4–S14. [Google Scholar] [CrossRef]
- Nussbaum, S.R.; Carter, M.J.; Fife, C.E.; DaVanzo, J.; Haught, R.; Nusgart, M.; Cartwright, D. An Economic Evaluation of the Impact, Cost, and Medicare Policy Implications of Chronic Nonhealing Wounds. Value Health 2018, 21, 27–32. [Google Scholar] [CrossRef]
- Bowers, S.; Franco, E. Chronic Wounds: Evaluation and Management. Am. Fam. Physician 2020, 101, 159–166. [Google Scholar]
- Falanga, V.; Isseroff, R.R.; Soulika, A.M.; Romanelli, M.; Margolis, D.; Kapp, S.; Granick, M.; Harding, K. Chronic wounds. Nat. Rev. Dis. Prim. 2022, 8, 1–21. [Google Scholar] [CrossRef]
- Murray, R.Z.; West, Z.E.; McGuiness, W. The multifactorial formation of chronic wounds. Wound Pract. Res. 2018, 26, 38–46. [Google Scholar]
- Leaper, D.J.; Schultz, G.; Carville, K.; Fletcher, J.; Swanson, T.; Drake, R. Extending the TIME concept: What have we learned in the past 10 years? Int. Wound J. 2012, 9, 1–19. [Google Scholar] [CrossRef]
- Monti, D.; Tampucci, S.; Tiwari, R.; Pathak, K. Local Drug Delivery Strategies towards Wound Healing. Pharmaceutics 2023, 15, 634. [Google Scholar] [CrossRef]
- Andrade, S.M.; Santos, I.C. Hyperbaric oxygen therapy for wound care. Rev. Gauch. Enferm. 2016, 37, e59257. [Google Scholar] [CrossRef]
- Vinkel, J.; Holm, N.F.R.; Jakobsen, J.C.; Hyldegaard, O. Effects of adding adjunctive hyperbaric oxygen therapy to standard wound care for diabetic foot ulcers: A protocol for a systematic review with meta-analysis and trial sequential analysis. BMJ Open 2020, 10, e031708. [Google Scholar] [CrossRef] [PubMed]
- Rosadi Seswandhana, M.; Anzhari, S.; Dachlan, I.; Widodo Wirohadidjojo, Y.; Aryandono, T. A case series of negative pressure wound therapy as a promising treatment in patients with burn injury. Int. J. Surg. Case Rep. 2020, 69, 64–67. [Google Scholar] [CrossRef]
- Stiefel, D.; Schiestl, C.; Meuli, M. Integra Artificial Skin® for burn scar revision in adolescents and children. Burns 2010, 36, 114–120. [Google Scholar] [CrossRef]
- Schlottmann, F.; Bucan, V.; Vogt, P.M.; Krezdorn, N. A short history of skin grafting in burns: From the gold standard of autologous skin grafting to the possibilities of allogeneic skin grafting with immunomodulatory approaches. Med. 2021, 57, 225. [Google Scholar] [CrossRef]
- Driver, V.R.; Hanft, J.; Fylling, C.P.; Beriou, J.M. Autologel Diabetic Foot Ulcer Study Group. A prospective, randomized controlled trial of autologous platelet-rich plasma gel for the treatment of diabetic foot ulcers. Ostomy. Wound Manag. 2006, 52, 68–87. [Google Scholar]
- Gilligan, A.M.; Waycaster, C.R.; Motley, T.A. Cost-effectiveness of becaplermin gel on wound healing of diabetic foot ulcers. Wound Repair Regen. 2015, 23, 353–360. [Google Scholar] [CrossRef]
- Mazzucco, L.; Medici, D.; Serra, M.; Panizza, R.; Rivara, G.; Orecchia, S.; Libener, R.; Cattana, E.; Levis, A.; Betta, P.G.; et al. The use of autologous platelet gel to treat difficult-to-heal wounds: A pilot study. Transfusion 2004, 44, 1013–1018. [Google Scholar] [CrossRef]
- Dohan Ehrenfest, D.M.; Rasmusson, L.; Albrektsson, T. Classification of platelet concentrates: From pure platelet-rich plasma (P-PRP) to leucocyte- and platelet-rich fibrin (L-PRF). Trends Biotechnol. 2009, 27, 158–167. [Google Scholar] [CrossRef]
- Grigore, T.V.; Cozma, C. Platelet-rich plasma as a site-targeted approach in wound healing: A molecular perspective. Discoveries 2018, 6, e87. [Google Scholar] [CrossRef]
- Schreml, S.; Szeimies, R.M.; Prantl, L.; Karrer, S.; Landthaler, M.; Babilas, P. Oxygen in acute and chronic wound healing. Br. J. Dermatol. 2010, 163, 257–268. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, P.G.; Felix, F.N.; Woodley, D.T.; Shim, E.K. The Role of Oxygen in Wound Healing: A Review of the Literature. Dermatologic Surg. 2008, 34, 1159–1169. [Google Scholar] [CrossRef]
- Castilla, D.M.; Liu, Z.-J.; Velazquez, O.C. Oxygen: Implications for Wound Healing. Adv. Wound Care 2012, 1, 225–230. [Google Scholar] [CrossRef]
- Sen, C.K. Wound healing essentials: Let there be oxygen. Wound Repair Regen. 2009, 17, 1–18. [Google Scholar] [CrossRef]
- Chandra, P.K.; Ross, C.L.; Smith, L.C.; Jeong, S.S.; Kim, J.; Yoo, J.J.; Harrison, B.S. Peroxide-based oxygen generating topical wound dressing for enhancing healing of dermal wounds. Wound Repair Regen. 2015, 23, 830–841. [Google Scholar] [CrossRef]
- Ochoa, M.; Rahimi, R.; Zhou, J.; Jiang, H.; Yoon, C.K.; Maddipatla, D.; Narakathu, B.B.; Jain, V.; Oscai, M.M.; Morken, T.J.; et al. Integrated sensing and delivery of oxygen for next-generation smart wound dressings. Microsystems Nanoeng. 2020, 6, 46. [Google Scholar] [CrossRef]
- Shiekh, P.A.; Singh, A.; Kumar, A. Exosome laden oxygen releasing antioxidant and antibacterial cryogel wound dressing OxOBand alleviate diabetic and infectious wound healing. Biomaterials 2020, 249, 120020. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Pang, K.; Zhu, S.; Pate, K.; Yin, J. Perfluorodecalin-based oxygenated emulsion as a topical treatment for chemical burn to the eye. Nat. Commun. 2022, 13, 1–14. [Google Scholar] [CrossRef]
- Mousavi, S.M.; Zarei, M.; Hashemi, S.A.; Ramakrishna, S.; Chiang, W.H.; Lai, C.W.; Gholami, A.; Omidifar, N.; Shokripour, M. Asymmetric membranes: A potential scaffold for wound healing applications. Symmetry 2020, 12, 1100. [Google Scholar] [CrossRef]
- Kwiatkowska, A.; Drabik, M.; Lipko, A.; Grzeczkowicz, A.; Stachowiak, R.; Marszalik, A.; Granicka, L.H. Composite Membrane Dressings System with Metallic Nanoparticles as an Antibacterial Factor in Wound Healing. Membranes (Basel). 2022, 12. [Google Scholar] [CrossRef]
- Graça, M.F.P.; de Melo-Diogo, D.; Correia, I.J.; Moreira, A.F. Electrospun Asymmetric Membranes as Promising Wound Dressings: A Review. Pharmaceutics 2021, 13, 183. [Google Scholar] [CrossRef] [PubMed]
- Xia, J.; Zhang, H.; Yu, F.; Pei, Y.; Luo, X. Superclear, Porous Cellulose Membranes with Chitosan-Coated Nanofibers for Visualized Cutaneous Wound Healing Dressing. ACS Appl. Mater. Interfaces 2020, 12, 24370–24379. [Google Scholar] [CrossRef]
- Bagrov, V.V.; Bukhtiyarov, I.V.; Volodin, L.Y.; Zibarev, E.V.; Kamrukov, A.S.; Kondratiev, A.V.; Krylov, V.I.; Nikonova, S.M.; Novikov, D.O.; Semenov, K.A. Preclinical Studies of the Antimicrobial and Wound-Healing Effects of the High-Intensity Optical Irradiation “Zarnitsa-A” Apparatus. Appl. Sci. 2023, Vol. 13, Page 10794 2023, 13, 10794. [Google Scholar] [CrossRef]
- Miłek, T.; Grzeczkowicz, A.; Lipko, A.; Oleksinski, L.; Kwiatkowska, A.; Strawski, M.; Drabik, M.; Stachowiak, R.; Goliszewski, J.; Granicka, L.H. A Functionalized Membrane Layer as Part of a Dressing to Aid Wound Healing. Membranes (Basel). 2022, 12, 936. [Google Scholar] [CrossRef]
- Mayer, D.; Ferenz, K.B. Perfluorocarbons for the treatment of decompression illness: How to bridge the gap between theory and practice. Eur. J. Appl. Physiol. 2019, 119, 2421–2433. [Google Scholar] [CrossRef]
- Jägers, J.; Wrobeln, A.; Ferenz, K.B. Perfluorocarbon-based oxygen carriers: From physics to physiology. Pflügers Arch. - Eur. J. Physiol. 2020, 473, 139–150. [Google Scholar] [CrossRef]
- Guo, S.; DiPietro, L.A. Factors Affecting Wound Healing. J. Dent. Res. 2010, 89, 219–221. [Google Scholar] [CrossRef]
- Wilkinson, H.N.; Hardman, M.J. Wound healing: Cellular mechanisms and pathological outcomes. Open Biol. 2020, 10, 200223. [Google Scholar] [CrossRef]
- Shi, C.; Wang, C.; Liu, H.; Li, Q.; Li, R.; Zhang, Y.; Liu, Y.; Shao, Y.; Wang, J. Selection of Appropriate Wound Dressing for Various Wounds. Front. Bioeng. Biotechnol. 2020, 8, 00182. [Google Scholar] [CrossRef]
- Boateng, J.S.; Matthews, K.H.; Stevens, H.N.E.; Eccleston, G.M. Wound healing dressings and drug delivery systems: A review. J. Pharm. Sci. 2008, 97, 2892–2923. [Google Scholar] [CrossRef]
- Zhu, J.; Cheng, H.; Zhang, Z.; Chen, K.; Zhang, Q.; Zhang, C.; Gao, W.; Zheng, Y. Antibacterial Hydrogels for Wound Dressing Applications: Current Status, Progress, Challenges, and Trends. Gels 2024, Vol. 10, Page 495 2024, 10, 495. [Google Scholar] [CrossRef] [PubMed]
- Yousefian, F.; Hesari, R.; Jensen, T.; Obagi, S.; Rgeai, A.; Damiani, G.; Bunick, C.G.; Grada, A. Antimicrobial Wound Dressings: A Concise Review for Clinicians. Antibiot. 2023, 12, 1434. [Google Scholar] [CrossRef] [PubMed]
- Lemnaru, G.M.; Motelica, L.; Trusca, R.D.; Ilie, C.I.; Croitoru, A.M.; Ficai, D.; Oprea, O.; Stoica-Guzun, A.; Ficai, A.; Ditu, L.M.; et al. Antimicrobial Wound Dressings based on Bacterial Cellulose and Independently Loaded with Nutmeg and Fir Needle Essential Oils. Polymers 2023, 15. [Google Scholar] [CrossRef]
- Vaidyanathan, L. Growth factors in wound healing ⇓ a review. Biomed. Pharmacol. J. 2021, 14, 1469–1480. [Google Scholar] [CrossRef]
- Yamakawa, S.; Hayashida, K. Advances in surgical applications of growth factors for wound healing. Burn. Trauma 2019, 7, 1–13. [Google Scholar] [CrossRef]
- Twu, O.; Mednik, S.; Scumpia, P.; Doaty, S.; Worswick, S. Use of Becaplermin for nondiabetic ulcers: Pyoderma gangrenosum and calciphylaxis. Dermatol. Ther. 2016, 29, 104–108. [Google Scholar] [CrossRef]
- Papanas, N.; Maltezos, E. Benefit-risk assessment of becaplermin in the treatment of diabetic foot ulcers. Drug Saf. 2010, 33, 455–461. [Google Scholar] [CrossRef]
- Barrientos, S.; Brem, H.; Stojadinovic, O.; Tomic-Canic, M. Clinical application of growth factors and cytokines in wound healing. Wound Repair Regen. 2014, 22, 569–578. [Google Scholar] [CrossRef] [PubMed]
- Simcock, J.; May, B.C.H. Ovine Forestomach Matrix as a Substrate for Single-Stage Split-Thickness Graft Reconstruction. Eplasty 2013, 13, e58. [Google Scholar]
- Alven, S.; Peter, S.; Mbese, Z.; Aderibigbe, B.A. Polymer-Based Wound Dressing Materials Loaded with Bioactive Agents: Potential Materials for the Treatment of Diabetic Wounds. Polymers (Basel). 2022, 14, 724. [Google Scholar] [CrossRef]
- Witte, M.B.; Barbul, A. General principles of wound healing. Surg. Clin. North Am. 1997, 77, 509–528. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The coating (ALG—PFC)net – patient platelet-rich plasma interface model in configuration with treated tissue. Key to the symbol: (ALG—PFC)net – alginate–perfluorooctyl cross-linked.
Figure 1.
The coating (ALG—PFC)net – patient platelet-rich plasma interface model in configuration with treated tissue. Key to the symbol: (ALG—PFC)net – alginate–perfluorooctyl cross-linked.
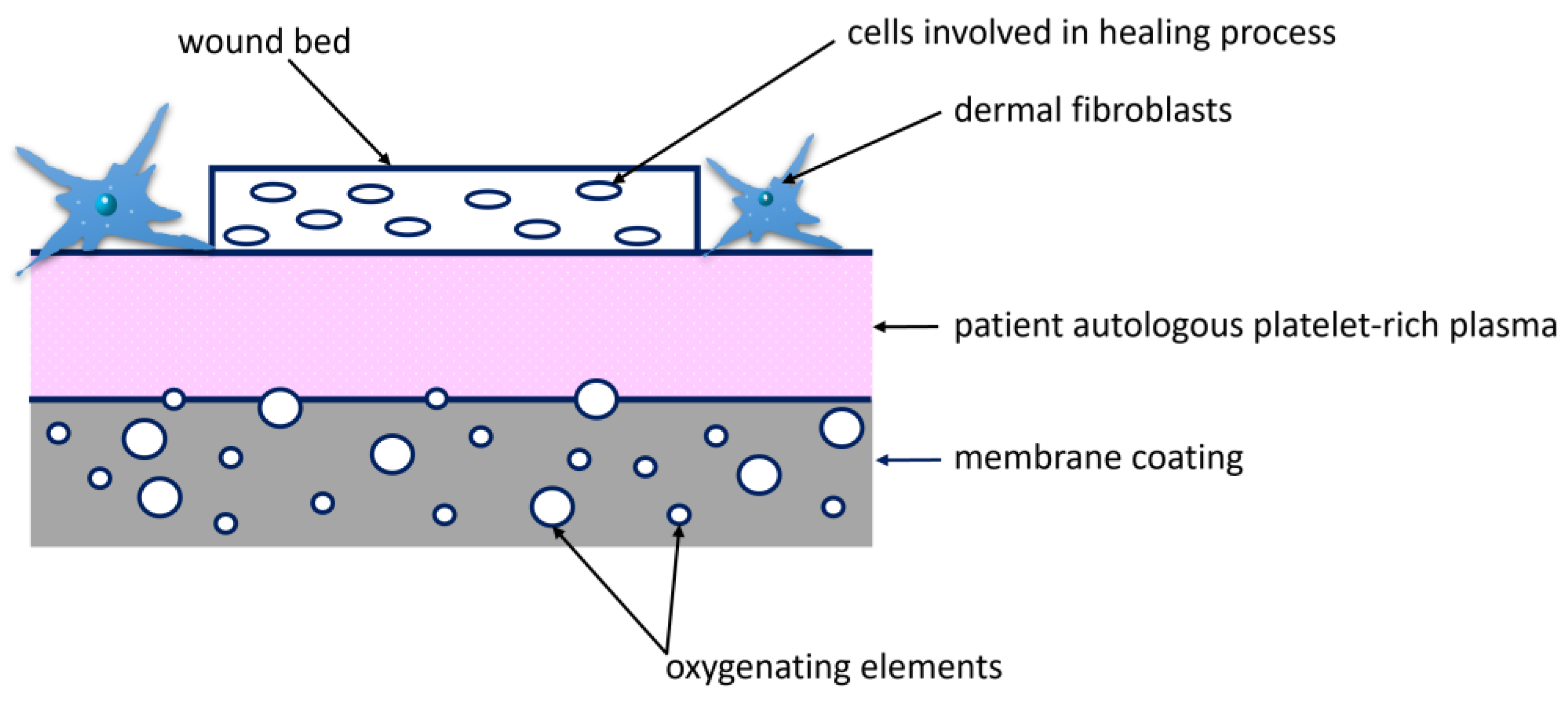
Figure 2.
The package modified with (ALG–PFC)net coating dressings. Key to the symbol: (ALG—PFC)net –alginate–perfluorooctyl cross-linked.
Figure 2.
The package modified with (ALG–PFC)net coating dressings. Key to the symbol: (ALG—PFC)net –alginate–perfluorooctyl cross-linked.

Figure 3.
AFM visualization of (ALG) and (ALG—PFC) layers on the gold-covered mica substrate. Key to the symbols: ALG – alginate, ALG—PFC – alginate with oxygenating factor.
Figure 3.
AFM visualization of (ALG) and (ALG—PFC) layers on the gold-covered mica substrate. Key to the symbols: ALG – alginate, ALG—PFC – alginate with oxygenating factor.
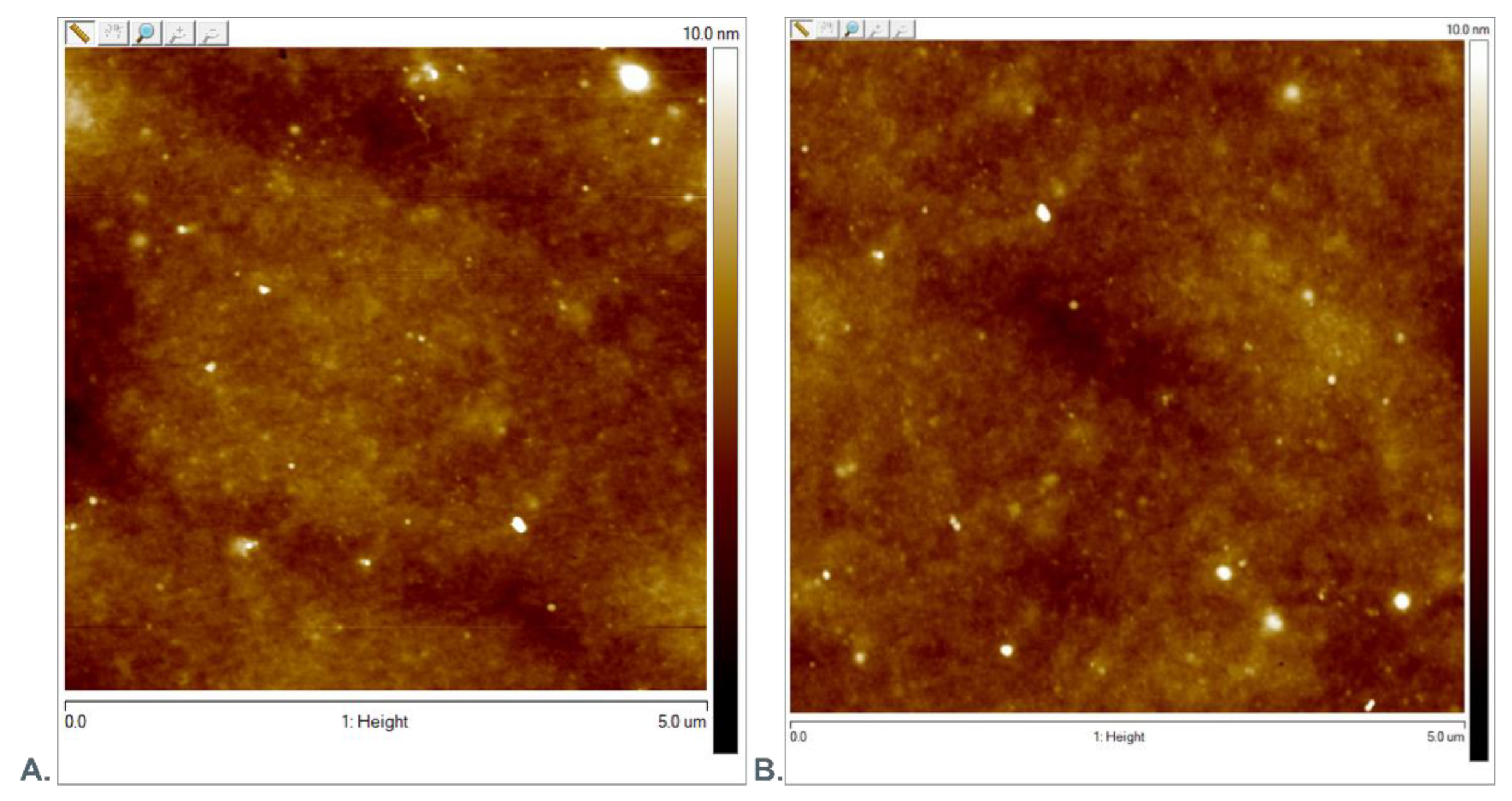
Figure 4.
AFM visualization of the profile of the ALG-PFC layer deposited on the gold mica substrate cover. Key to the symbol: ALG—PFC – alginate with oxygenating factor.
Figure 4.
AFM visualization of the profile of the ALG-PFC layer deposited on the gold mica substrate cover. Key to the symbol: ALG—PFC – alginate with oxygenating factor.
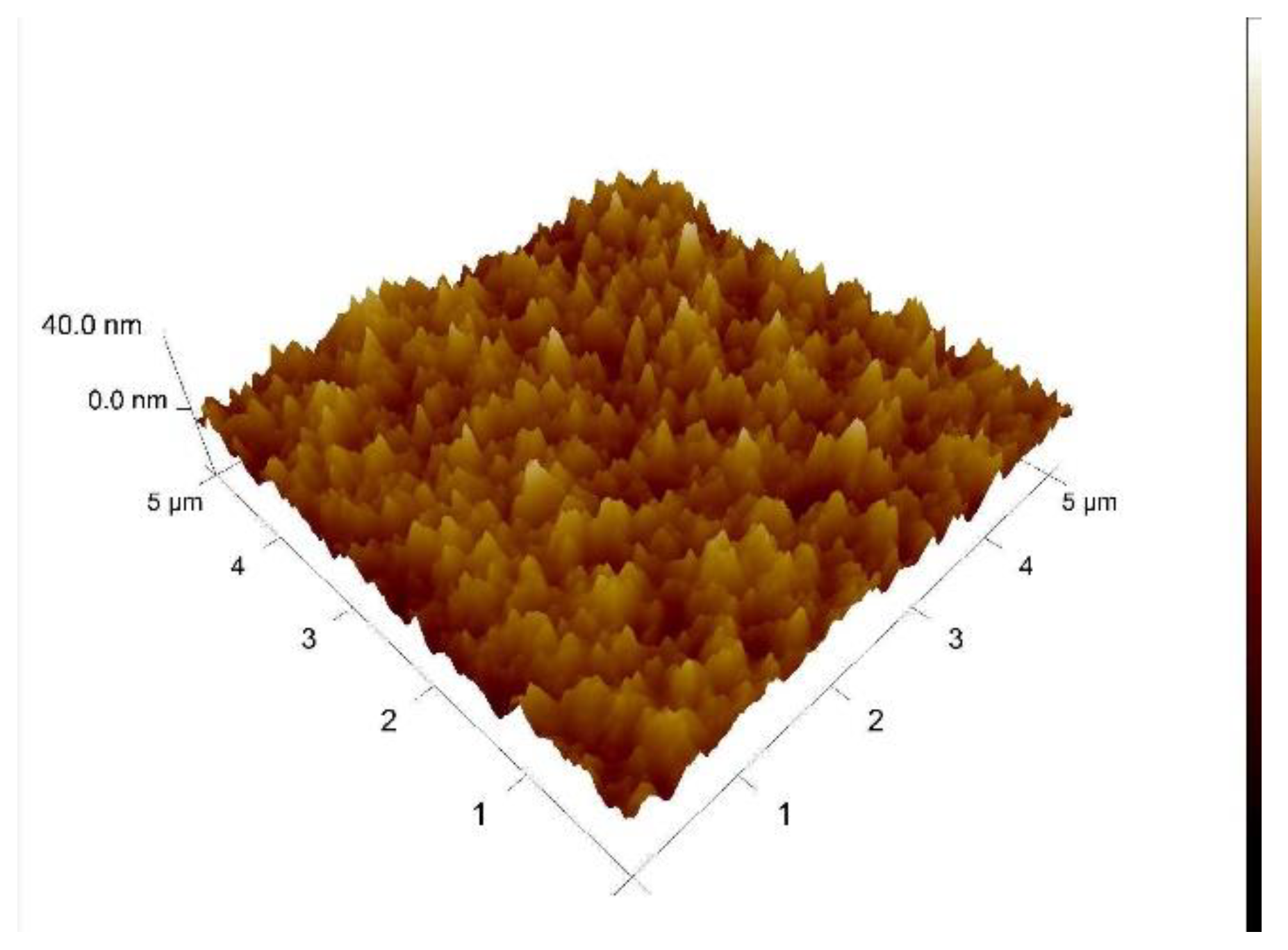
Figure 5.
FT-IR spectra of ALG, ALG—PFC. Key to the symbols: ALG– alginate; ALG—PFC –alginate–perfluorooctyl.
Figure 5.
FT-IR spectra of ALG, ALG—PFC. Key to the symbols: ALG– alginate; ALG—PFC –alginate–perfluorooctyl.
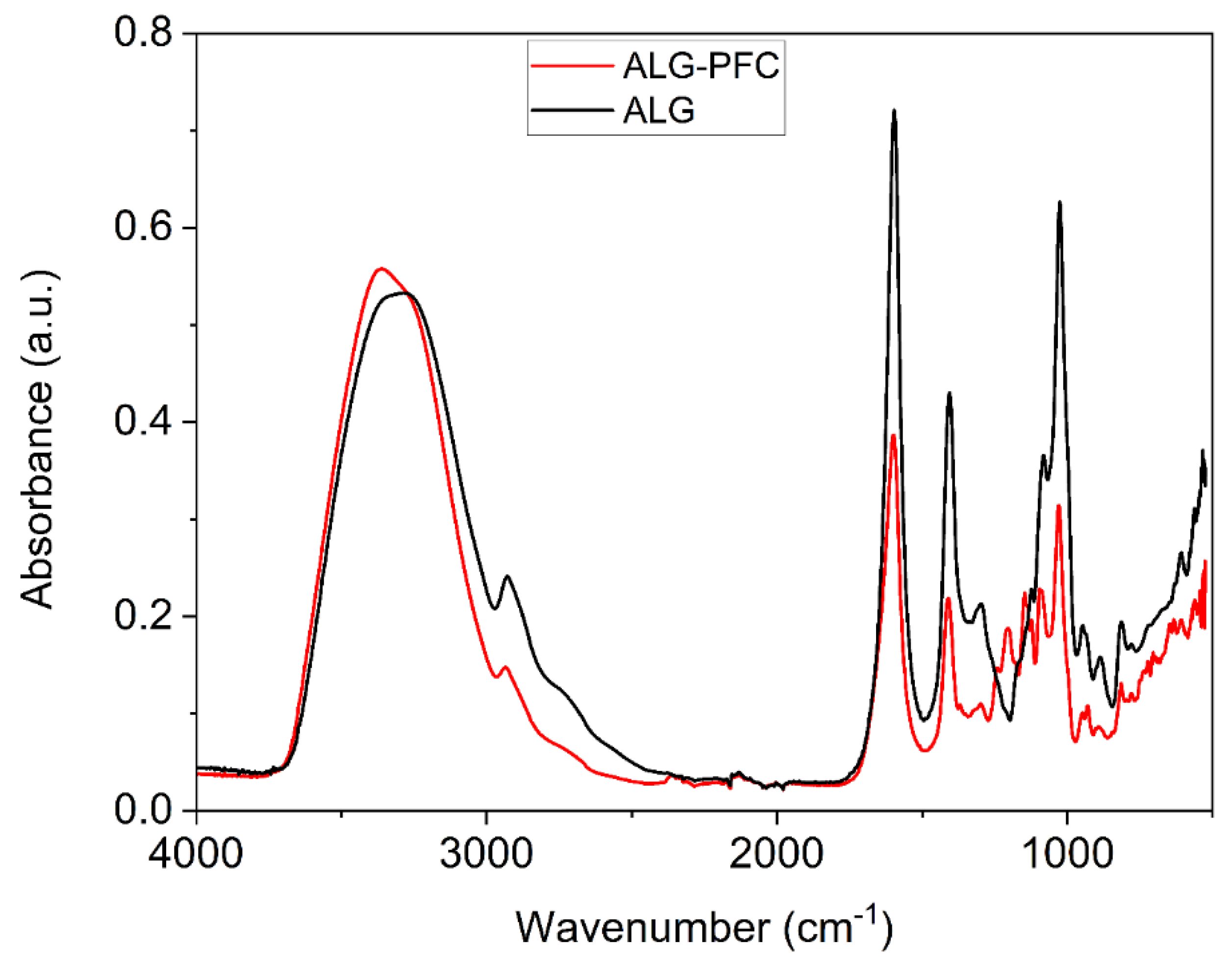
Figure 6.
SEM visualization of the surface of (ALG-PFC)net coating. Key to the symbol: (ALG—PFC)net – alginate–perfluorooctyl cross-linked.
Figure 6.
SEM visualization of the surface of (ALG-PFC)net coating. Key to the symbol: (ALG—PFC)net – alginate–perfluorooctyl cross-linked.
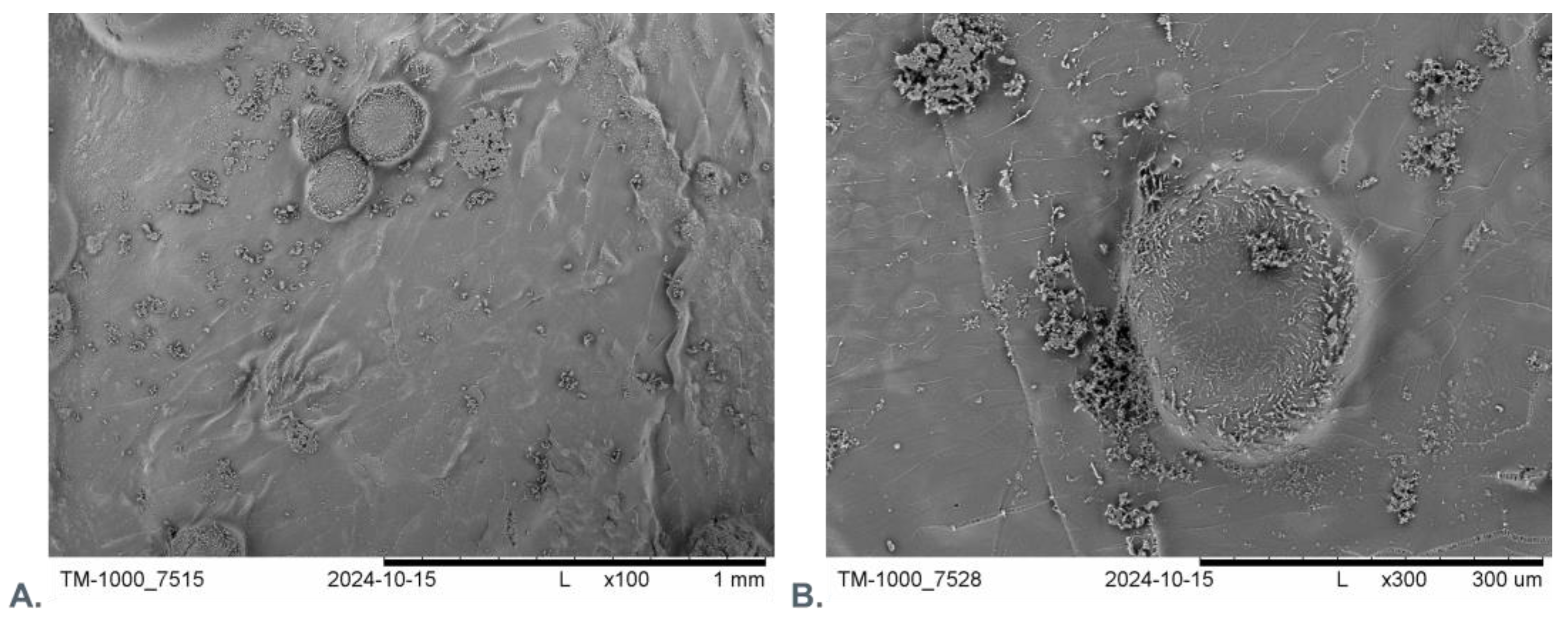
Figure 7.
Visualization of the surface of the: A) ALGnet coating; B) (ALG-PFC)net coating. Key to the symbols: ALGnet – alginate cross-linked; (ALG—PFC)net –alginate–perfluorooctyl cross-linked.
Figure 7.
Visualization of the surface of the: A) ALGnet coating; B) (ALG-PFC)net coating. Key to the symbols: ALGnet – alginate cross-linked; (ALG—PFC)net –alginate–perfluorooctyl cross-linked.
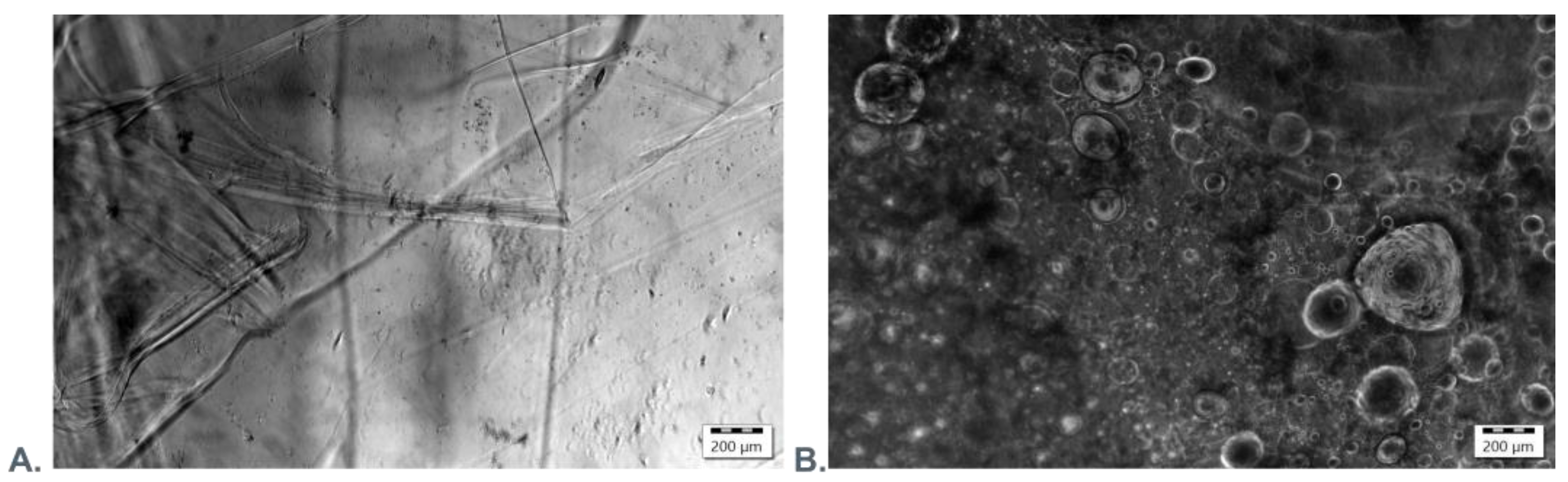
Figure 8.
Fluorescence microscopic picture of (ALG—PFC_µB-FITC)net layer coating. Key to the symbol: (ALG—PFC_µB-FITC)net – alginate–perfluorooctyl labeled with fluorescent microbeads, cross-linked.
Figure 8.
Fluorescence microscopic picture of (ALG—PFC_µB-FITC)net layer coating. Key to the symbol: (ALG—PFC_µB-FITC)net – alginate–perfluorooctyl labeled with fluorescent microbeads, cross-linked.
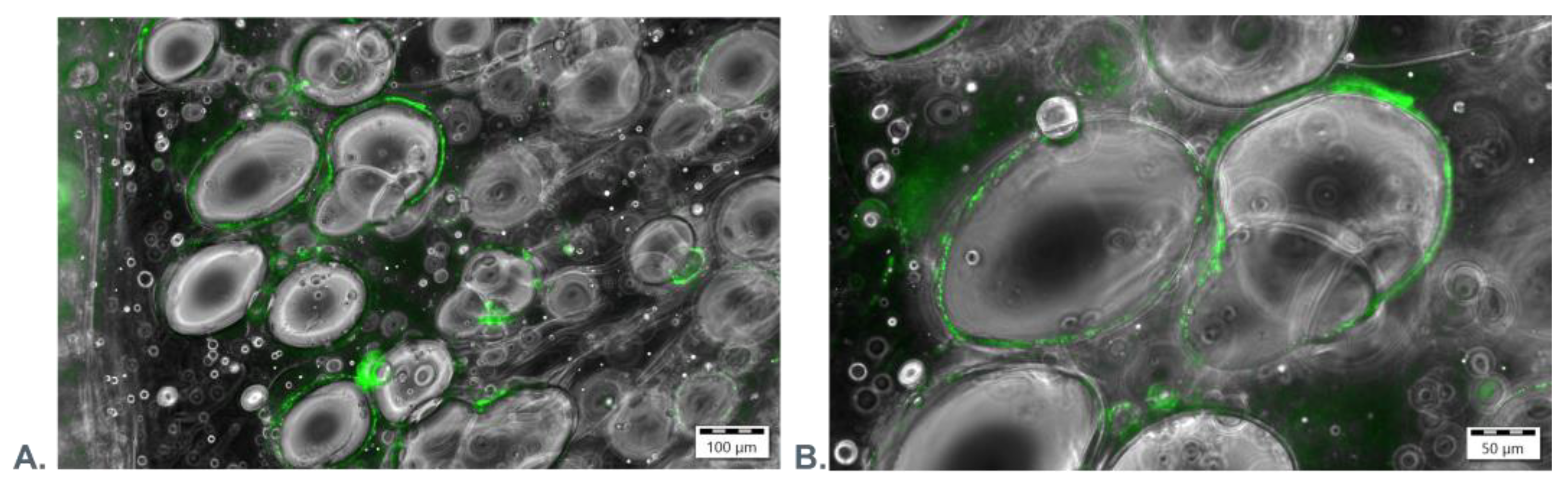
Figure 9.
3D view in the coordinate system of the oxygenating layer (ALG—PFC_µB-FITC)net in confocal microscope. Key to the symbol: (ALG—PFC_µB-FITC)net – alginate–perfluorooctyl labeled with fluorescent microbeads, cross-linked.
Figure 9.
3D view in the coordinate system of the oxygenating layer (ALG—PFC_µB-FITC)net in confocal microscope. Key to the symbol: (ALG—PFC_µB-FITC)net – alginate–perfluorooctyl labeled with fluorescent microbeads, cross-linked.
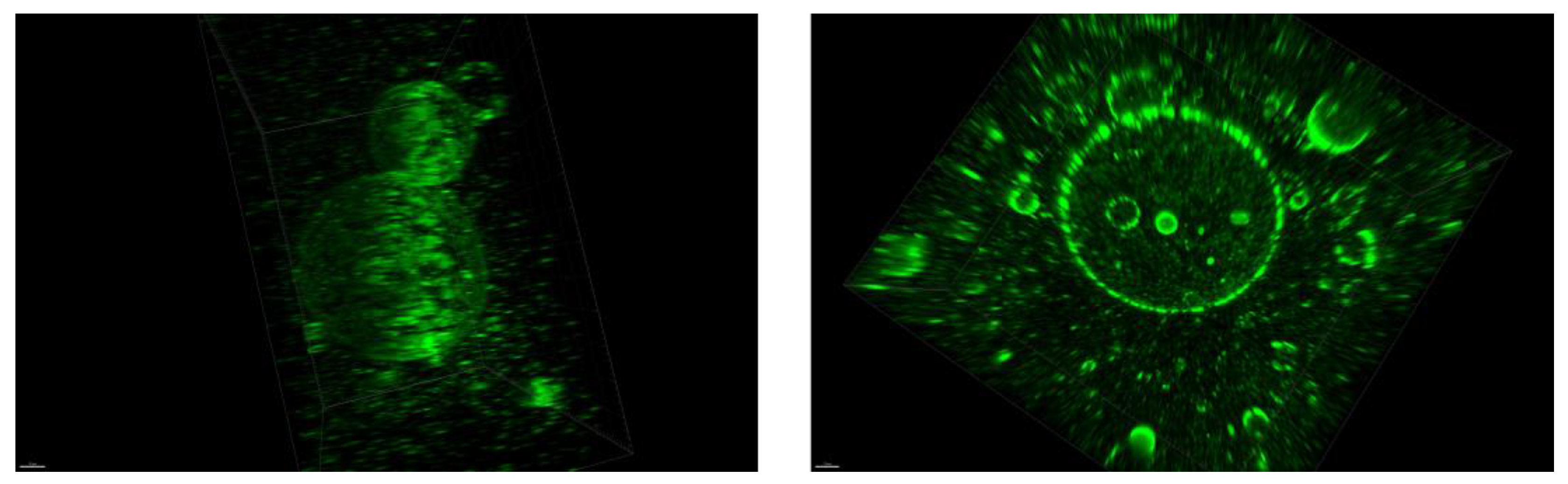
Figure 10.
The water contact angle. Key to the symbols: ALG – alginate, ALG_PFC – alginate–perfluorooctyl.
Figure 10.
The water contact angle. Key to the symbols: ALG – alginate, ALG_PFC – alginate–perfluorooctyl.
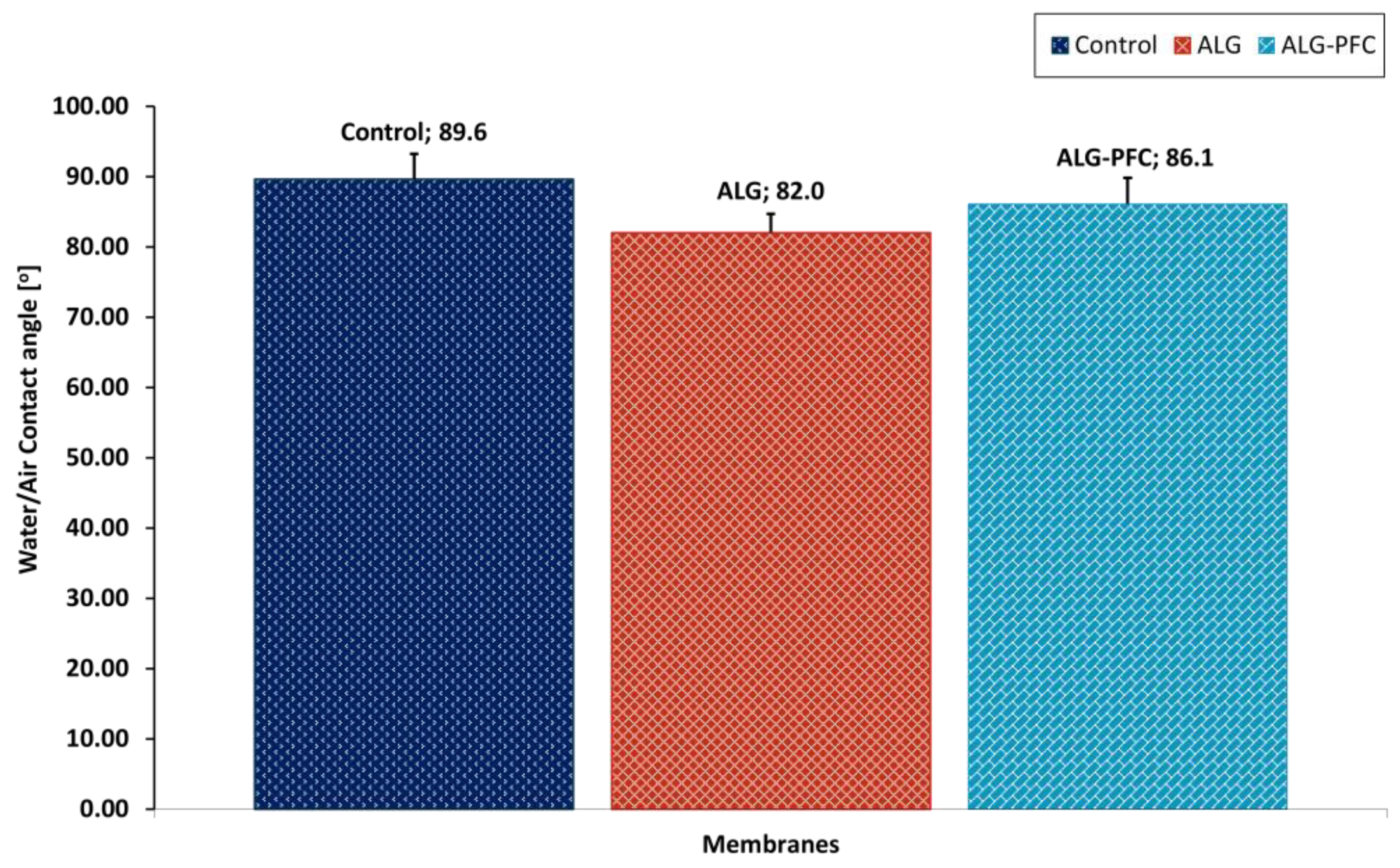
Figure 11.
The representing images of the droplets of water exhibiting the contact angles for assessed layer coatings. A) support; B) alginate; C) alginate–perfluorooctyl.
Figure 11.
The representing images of the droplets of water exhibiting the contact angles for assessed layer coatings. A) support; B) alginate; C) alginate–perfluorooctyl.

Figure 12.
Wound treatment with the designed system (Patient 002M).
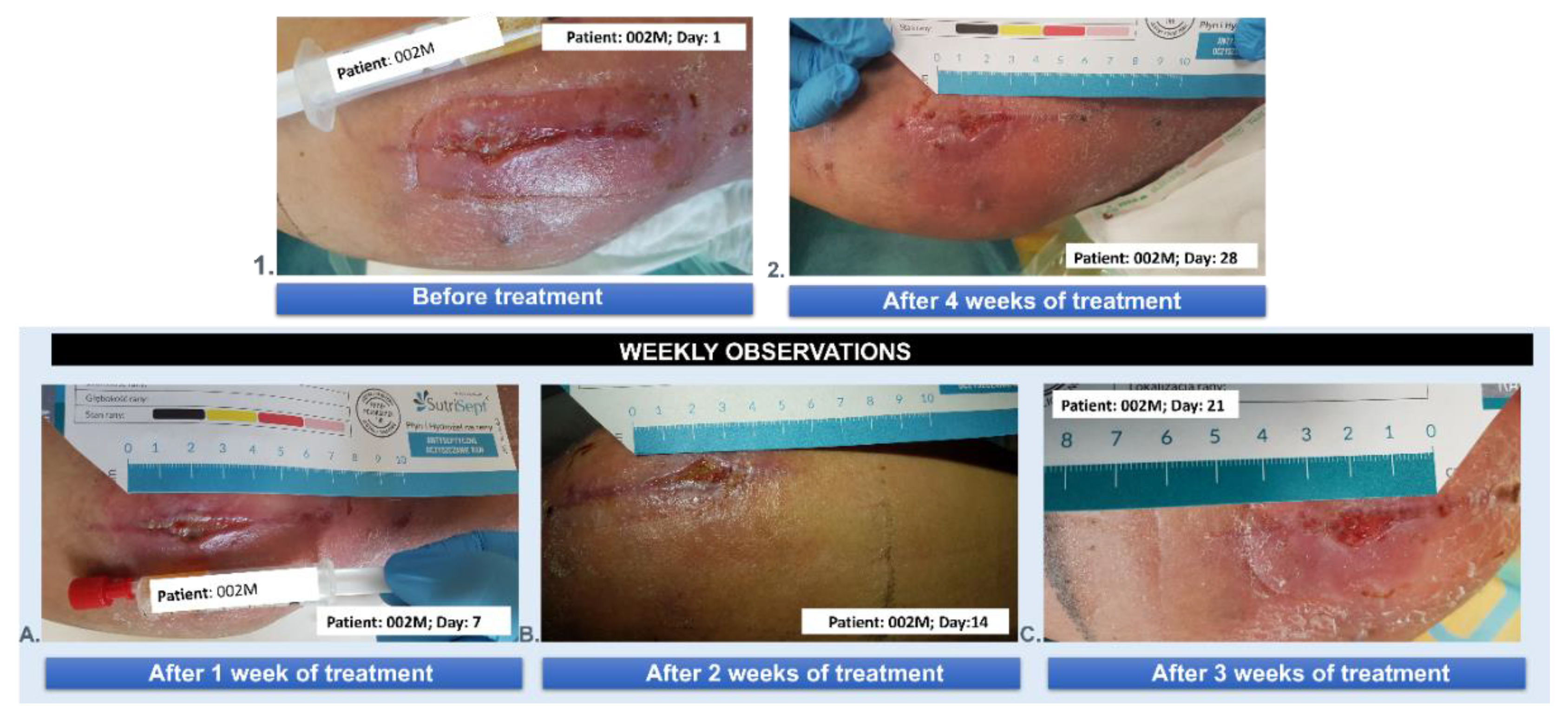
Figure 13.
Wound treatment with the designed system (Patient 003M).

Figure 14.
Wound treatment with the designed system (Patient 004M).

Figure 15.
Wound treatment with the designed system (Patient 005F).

Figure 16.
Compilation of the wound treatment effects in time for three different patients (001M, 002M, 003M): (A) before the treatment, (B) after 1 week of the treatment, and (C) after 2 weeks of the treatment.
Figure 16.
Compilation of the wound treatment effects in time for three different patients (001M, 002M, 003M): (A) before the treatment, (B) after 1 week of the treatment, and (C) after 2 weeks of the treatment.
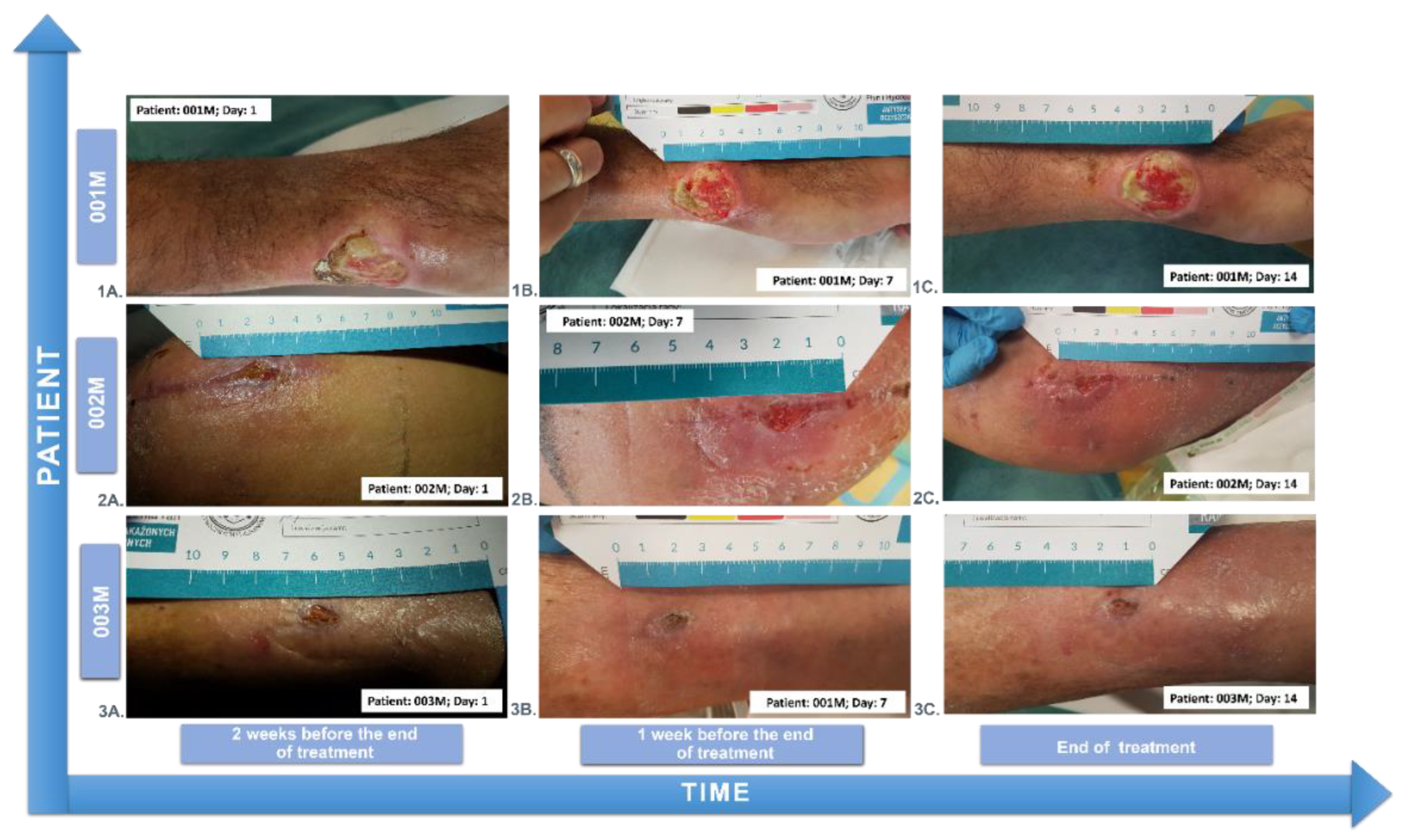
Figure 17.
The mean percent linear reduction of wound size during individual weeks of treatment calculated for Patients 002M, 003M, 004M, and 005F.
Figure 17.
The mean percent linear reduction of wound size during individual weeks of treatment calculated for Patients 002M, 003M, 004M, and 005F.
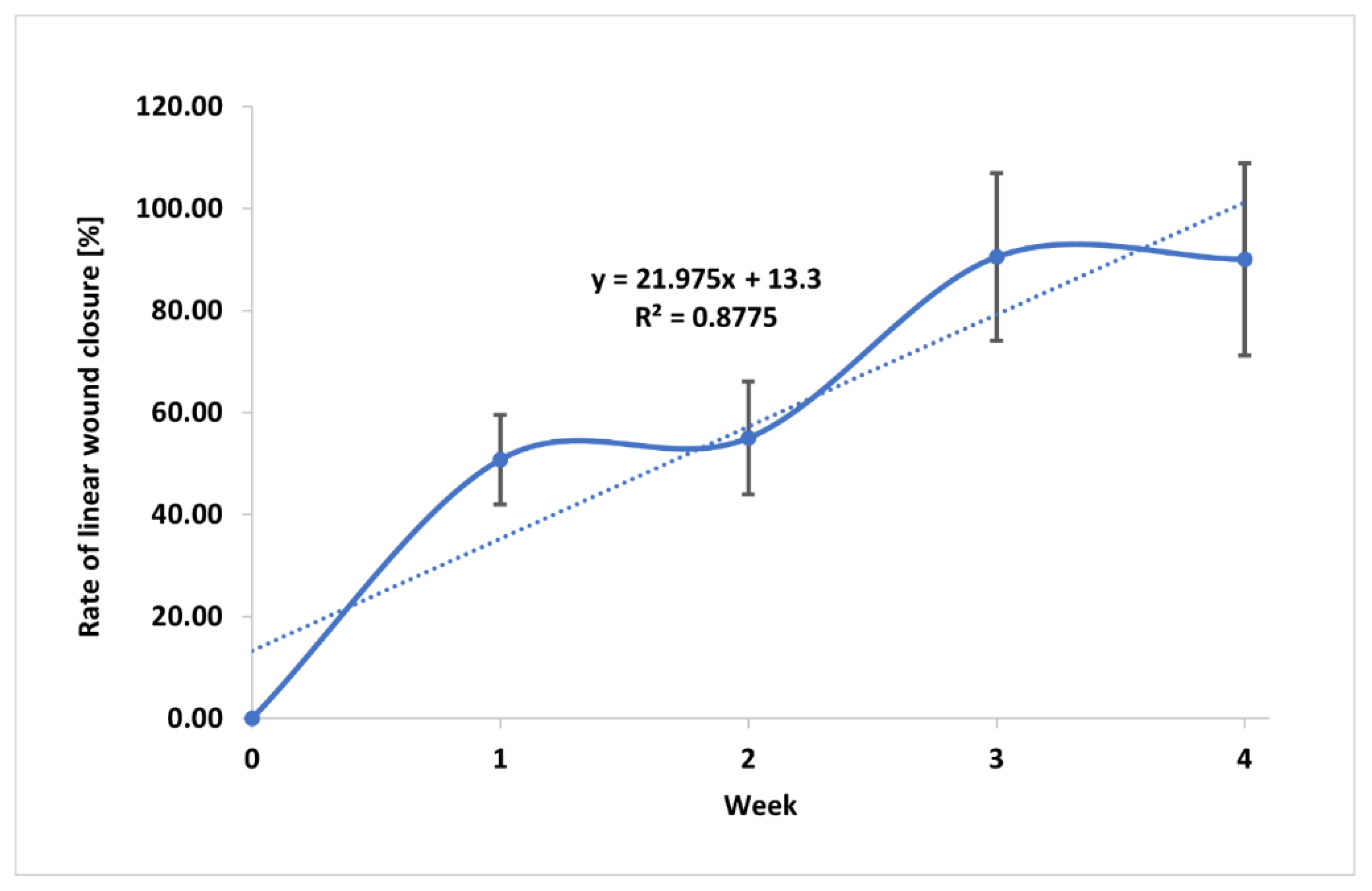
Figure 18.
Illustration of wound healing with visible granulation and epithelization. Granulation and epithelization models based on Alven et al. 2022 [50]. ROS-reactive oxygen species.
Figure 18.
Illustration of wound healing with visible granulation and epithelization. Granulation and epithelization models based on Alven et al. 2022 [50]. ROS-reactive oxygen species.
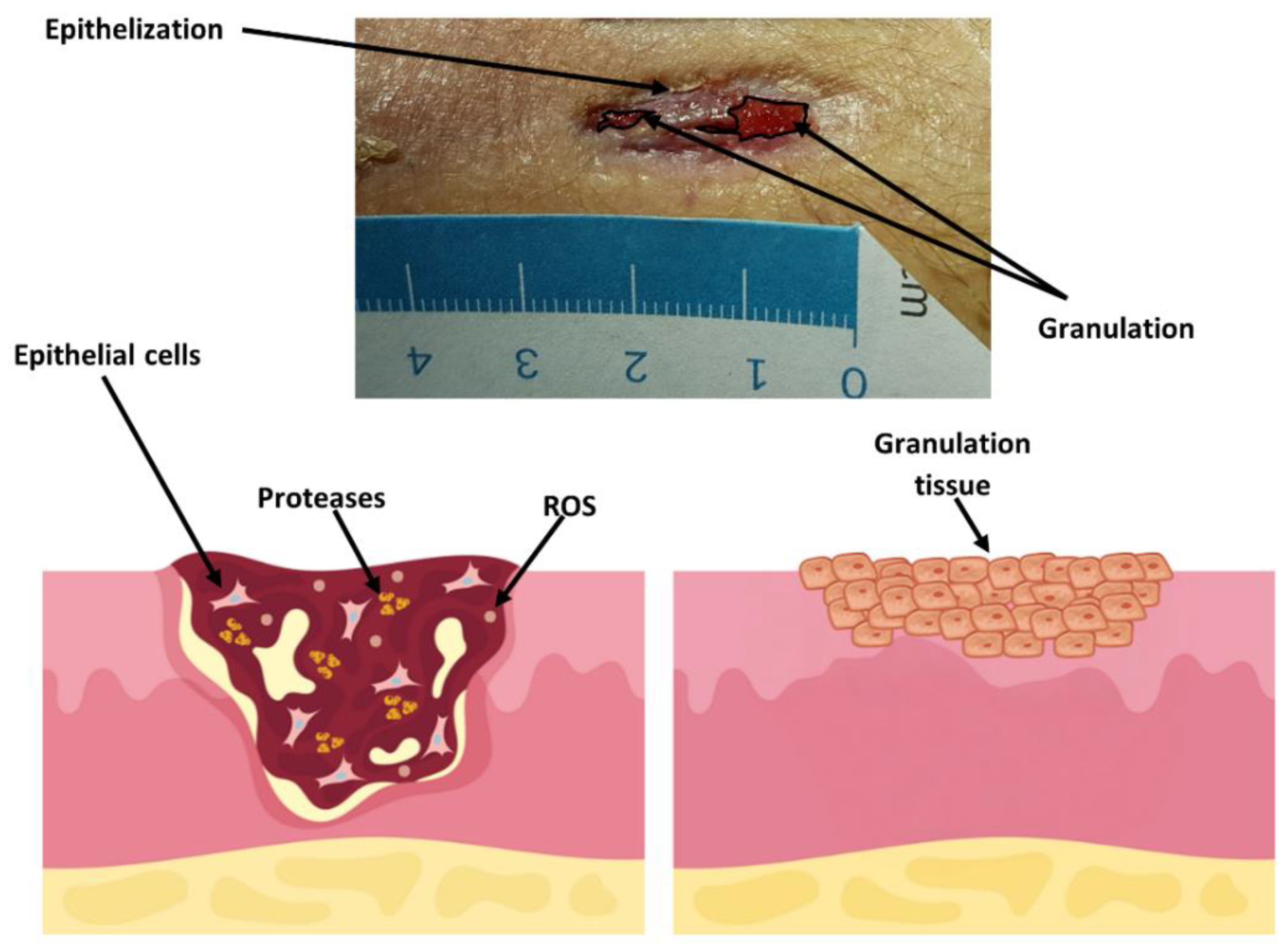
Figure 19.
Theoretical (for normally healing wounds) and experimental duration of phases of proliferation and maturation. The histological pictures visualize the time range of granulation, indicating the proliferation phase, and epithelialization, indicating the maturation stage during healing of treated non-healing wounds.
Figure 19.
Theoretical (for normally healing wounds) and experimental duration of phases of proliferation and maturation. The histological pictures visualize the time range of granulation, indicating the proliferation phase, and epithelialization, indicating the maturation stage during healing of treated non-healing wounds.
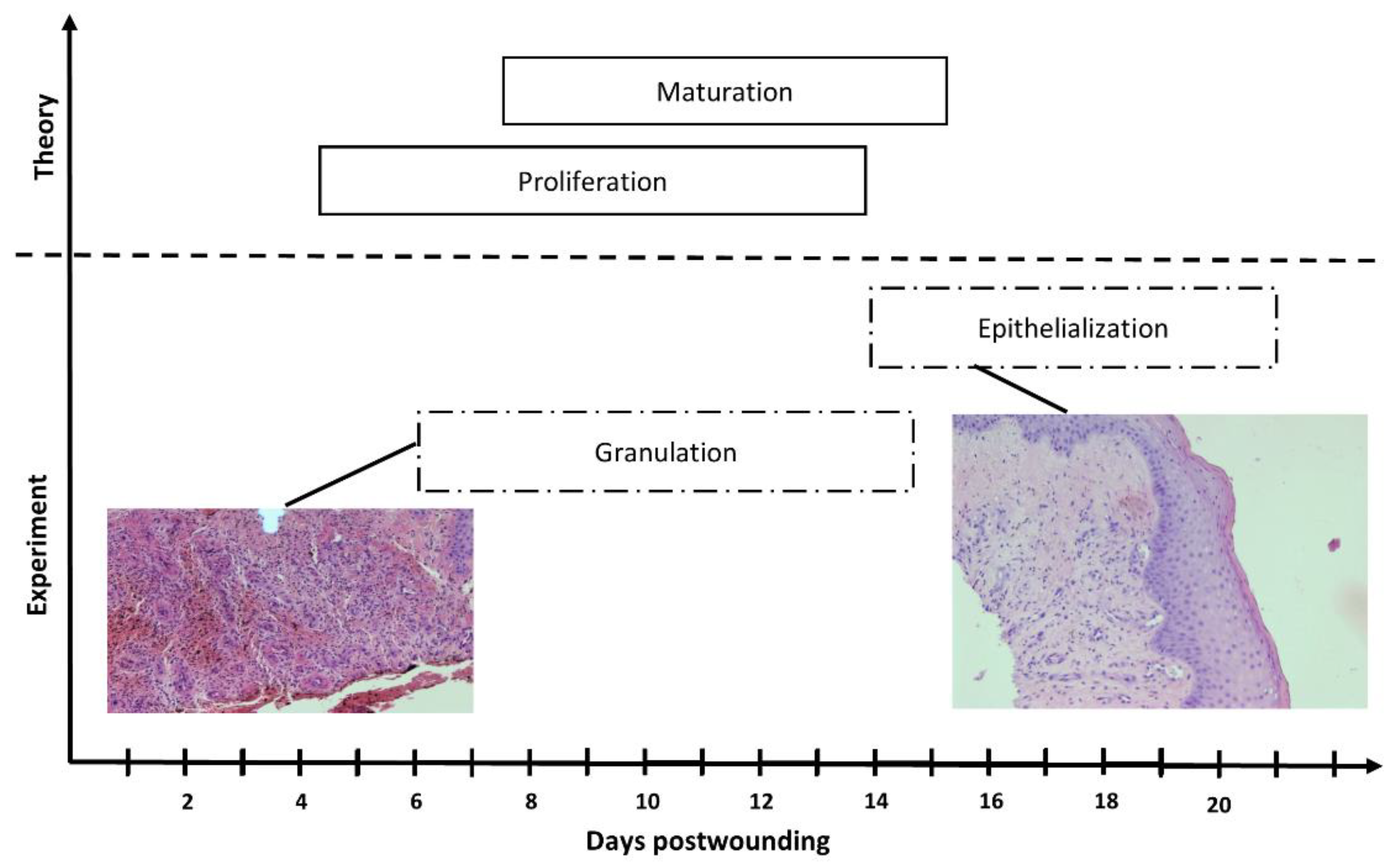

Table 1.
Patients in the trial.
| Code | Age | Ulceration time [months] | Gender | Diabetes | Treatment [weeks] |
|---|---|---|---|---|---|
| 001M | 54 | 4 | male | YES | 2 |
| 002M | 62 | 3 | male | NO | 4 |
| 003M | 84 | 8 | male | NO | 3 |
| 004M | 71 | 5 | male | YES | 3 |
| 005F | 58 | 3 | female | NO | 4 |
Table 2.
Patients' wounds characteristics.
| Code | Age | Gender | Wound characteristics |
|---|---|---|---|
| 001M | 54 | male | |
| generalized scleroderma wound of the wrist | |||
| 002M | 62 | male | the postoperative wound of liposarcoma of the lower leg |
| 003M | 84 | male | the post-traumatic wound of the lower leg |
| 004M | 71 | male | chronic venous ulcer wound of the lower leg |
| 005F | 58 | female | the post-traumatic wound of the lower leg |
Table 3.
The percent linear reduction of wound size value (R) during individual weeks of treatment.
| Time of treatment/treated Patients | R [%] |
|---|---|
| 1 week/Patients 002M, 003M, 004M, 005F | 50.75±8.8 |
| 2 week/Patients 002M, 003M, 004M, 005F | 55.0±11.1 |
| 3 week/Patients 002M, 003M, 004M, 005F | 90.50±16.5 |
| 4 week/Patients 002M, 003M, 005F | 86.70±18.8 |
The values are presented as mean±SD.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



