
Submitted:
31 March 2024
Posted:
01 April 2024
You are already at the latest version
Abstract
Abstract
Introduction: In the last thirty years, brain neuromodulation techniques have been used as an alternative to pharmacological treatment of neurological disorders. Parkinson's disease (PD) is a neurodegenerative disorder leading to bradykinesia, rest tremor, postural changes, and non-motor symptoms such as depression, anxiety, sleep disorders, pain, and cognitive decline that compromises executive functions (EFs), responsible for the orderly execution of behaviors and tasks of daily life and intentional and directed actions. To this date, a few studies with transcranial direct current stimulation (tDCS) have shown beneficial effects in PD patients concerning specific motor and non-motor symptoms, targeting the motor cortex and/or prefrontal regions. Objective: The main objective of this study was to evaluate the effects of left prefrontal tDCS across a broad spectrum of motor and non-motor symptoms of PD using established validated scales. Method: Single-blind randomized clinical trial with 18 volunteers with PD, aged between 45 and 80 years (66.1 ± 9.65), who met inclusion and exclusion criteria. Participants were submitted to assessments of motor and non-motor functions employing psychometric scales and tests to evaluate EFs and were randomly divided into two groups: control (sham stimulation) and experimental (active stimulation). All participants were involved in three separate tDCS sessions. The anode was positioned over the left dorsolateral prefrontal cortex and the cathode over the right supraorbital region, with a direct current intensity of 2mA, lasting 20 minutes. At the end of the three sessions, all participants were reassessed. Results: Significant effects of tDCS on non-motor functions were observed for cognition (verbal fluency of actions, clock copy test, appointment by visual confrontation, and verbal memory with immediate free recall) and subjective assessment of sleep quality (overall restlessness and discomfort in the arms and legs at night, leg and arm cramps at night and distressing dreams). There was also an improvement in the rate of errors and successes for congruent and incongruent stimuli of the Stroop Test. The beneficial effects on motor function were decreased rigidity, improved gait, and greater agility in the finger-tapping test. Conclusion: Three tDCS sessions showed positive results for participants with PD, producing significant improvements in various motor and non-motor functions, including sleep quality, cognition, and EFs. Additionally, the present results indicate that tDCS neuromodulation of the left dorsolateral prefrontal cortex region is feasible, safe, and provides significant objective benefits for PD patients.
Keywords:
Parkinson’s disease
; neuromodulation
; transcranial direct current stimulation – tDCS
; movement disorders
; mood
; sleep
; cognition
1. Introduction
Transcranial direct current stimulation (tDCS) is a non-invasive neuromodulation technique that allows neuronal plasticity through the delivery of a low-intensity positive (anodal) or negative (cathodal) electric current employing electrodes positioned in a previously established area, leading to changes in neuronal resting membrane potential [1]. Several published studies describe tDCS effects on stimulation or inhibition of the synaptic transmission between neurons. tDCS can be combined with training of cognitive or motor skills to evaluate an improvement in the performance of some tasks. It has also been proposed as a technique with therapeutic effects in clinical protocols for different diseases, including Parkinson’s disease [2,3,4].
Parkinson’s disease (PD) is a neurodegenerative disorder with a progressive loss of dopaminergic neurons, especially those located in the midbrain [5]. In addition to a dopaminergic deficit, the pathogenesis of PD has also been explained by mitochondrial and lysosomal dysfunction, together with alpha-synuclein deposits. These deposits relate to neuronal death in multiple nervous system nuclei, which may explain diverse PD-specific non-motor symptoms [6].
The cardinal signs of PD are mainly of motor nature: bradykinesia, rest tremor, postural changes, and muscular rigidity. However, the non-motor symptoms also require specialized treatment due to the significant impact on quality of life. These include olfactory changes, sleep disorders, postural hypotension, constipation, depression, anxiety, psychosis, and cognitive impairment [6].
Despite the impossibility of ascertaining the etiology of PD, some theories explain the degenerative process in terms of impairment of the affected neurological structures [7]. In this context, PD can be described by its stages, as comprising three main phases: Initially, the premotor phase is characterized by the death of neurons of the lower brainstem (causing sleep disturbance symptoms), progressing through the olfactory bulb (emergence of hyposmia) and the pontine nuclei [6]. Then, in the motor phase, the mesencephalic region is affected (motor symptoms). In the advanced stage, the neuronal deterioration affects the cerebral cortex, impaired impairment cognitive and behavioral functions. In this context, scientists call attention to non-motor predictive signs, which signal the beginning of the pathology and prodromal predictors, indicating the degree of neuronal involvement and prognosis of the disease [7].
To adequately characterize PD symptoms, physicians and researchers use assessment scales and tests that are validated and widely recognized. For instance, there are scales for the screening of signs and symptoms resulting from Parkinson’s disease, such as the Hoehn & Yahr (H&Y) scale, specific for the degree of disease staging; the Unified Parkinson’s Disease Rating Scale (UPDRS), which assesses various domains, including motor function. There is also the Parkinson’s Disease Sleep Scale (PDSS), which identifies the occurrence of sleep disturbances [9], and the Hospital Anxiety and Depression Scale (HADS), a wide-ranging instrument for mood symptoms in PD [8,9].
In addition, the Parkinson’s Disease Cognitive Rating Scale (PD-CRS) is used to assess cognitive impairment and executive function deficits (EFs) [10]. Furthermore, the Stroop Test also provides information about the EFs by measuring the interference effect generated through the evaluation of congruent and incongruent stimuli consisting of color names written in either matching or non-matching colors and presented in pseudo-random order. The applicability of these tools and the Stroop Test for patients with Parkinson’s Disease has been well described in the literature [11,12,13].
Previous studies have investigated the effects of tDCS on motor and non-motor symptoms. Concerning motor symptoms, Ishikuro et al. (2018) identified that anodal stimulation significantly increased scores of motor functions in the Fugl Meyer Assessment set and significantly decreased scores of motor disability in UPDRS-III compared with sham and cathodal stimulation. In another trial, the researchers verified that anodal tDCS improves patients’ walking speed with or without concomitant physical therapy treatment [14].
Regarding the beneficial effects of tDCS on non-motor functions, a study conducted by a group of researchers in Iran showed significant results in the quality of sleep of participants with PD, as well as a decrease in their fatigue symptoms [15,16]. Benusi and collaborators found that participants had a lower incidence of risky decision-making and displayed enhanced executive functions, inhibitory control, and cognitive flexibility. In Australia, a clinical trial with follow-up showed improvement in PD patients’ cognition (language, global memory), and executive functions (working memory, cognitive flexibility), either with cognitive training or with tDCS alone [17,18].
Doruk et al. identified significant results in the Trail Test after tDCS and found that the DLPFC-L group showed a greater reduction in Beck depression inventory scores [2]. It is also important to highlight that using tDCS for depression is common in clinical practice with an anode over the L-DLPFC and a cathode over the right supra-orbital region. The beneficial effects of tDCS have also been identified in other studies [11,19].
Considering that Parkinson’s disease is multi-causal and substantially compromises the patient’s quality of life, studies that offer noninvasive and effective treatments for such symptoms are of great value and potentially relevant. In the present study, we investigate the effects of tDCS stimulation in patients with Parkinson’s disease on motor function, sleep disorders, mood swings, cognition, and executive functions.
2. Material and Methods
2.1. Participants
The study sample included 18 patients, 11 men and 7 women, aged between 45 and 85 years, (mean 66.1 ± 9.65) all diagnosed with Parkinson’s disease by a neurologist. The participants had preserved cognitive status with mild to moderate motor symptoms, according to the MDS-UPDRS-Part III scale. They had no history or current clinical diagnosis of cognitive decline and no legally imposed civil limitations. Inclusion criteria were: a) diagnosis of Parkinson’s disease according to the criteria of the London Brain Bank; b) being under treatment with dopaminergic drugs with a stable total daily dose for at least 30 days; c) being in the on phase and therefore able to more comfortably perform in all tests; d) being able to read and understand instructions; e) having more than 8 years of school education; f) having preserved civil capacity as defined above; g) age between 45 and 85 years. As for the exclusion criteria, the following were considered: a) any contraindication for transcranial stimulation, metallic brain implants near the region to be stimulated, or hypersensitivity to saline or other materials attached to the stimulator; b) illiteracy or less than 8 years of school education; c) history of psychosis, severe vascular diseases, head trauma, and epilepsy; d) uncorrected severe visual or auditory impairment; e) motor function impairment that hinders performance in the evaluation items that require it; f) use of antipsychotics (dopaminergic blockers) or stimulant medications (such as modafinil or methylphenidate); g) use of a pacemaker. The study was carried out in the Laboratory of Neuroscience and Behavior of the Institute of Biology at the University of Brasília and met the requirements of Resolution No. 466/2012 of the National Health Council, which provides ethical standards for research involving human subjects. The study protocol was reviewed and approved by the Research Ethics Committee of the Faculty of Health Sciences of the University of Brasília, under the number CAE:91375218.9.0000.0030.
2.2. Pharmacotherapy for the Treatment of Parkinson`s Disease

Table 1.
Drugs used by the patients in this study.
| Drugs for Parkinson’s Disease therapy | F | % |
|---|---|---|
| Levodopa | 18 | 100% |
| Amantadine | 4 | 22,22% |
| Dopamine Agonists (DA) | 12 | 66,66% |
| Pramipexole | 10 | 55,55% |
| Rotigotine | 2 | 11,11% |
| Monoamine Oxidase (MAO) B inhibitors | 1 | 5,55% |
| Rasagiline | 1 | 5,55% |
| Drugsfor Parkinson’s disease | F | % |
| Amantadine + Prolopa BD + Prolopa HBS | 1 | 5,56% |
| Pramipexole + Amantadine + Prolopa BD 100/25 | 1 | 5,56% |
| Pramipexole Amantadine + Prolopa BD 100/25 + Prolopa HBS | 1 | 5,56% |
| Pramipexole + Levodopa | 1 | 5,56% |
| Pramipexole Prolopa + Prolopa BD | 1 | 5,56% |
| Pramipexole + Prolopa + Prolopa BD + Prolopa HBS | 1 | 5,56% |
| Pramipexole + Prolopa BD | 3 | 16,67% |
| Pramipexole + Prolopa BD + Prolopa HBS 100/25 | 1 | 5,56% |
| Prolopa | 1 | 5,56% |
| Prolopa + Prolopa BD | 1 | 5,56% |
| Prolopa + Prolopa DR | 1 | 5,56% |
| Prolopa + Prolopa HBS 100/25 | 1 | 5,56% |
| Prolopa HBS + Prolopa DR | 1 | 5,56% |
| Rasagiline + Prolopa BD100/25 + Prolopa HBS 100/25 | 1 | 5,56% |
| Rotigotine + Amantadine + Prolopa BD | 1 | 5,56% |
| Rotigotine + Prolopa | 1 | 5,56% |
| Total | 18 | 100,00% |
Regarding other drugs taken by the volunteers for the treatment of comorbidities, 44.8% were antidepressants, 22.4% were anticholinergics, sedatives and/or antihypertensives, 16.1% of the individuals took other drugs of continuous use, such as antidiabetic, neuroleptic, antidyspeptic, antifungal, and anti-inflammatory preparations. On the other hand, 11.1% of the participants used statins or did not use any medication. The distribution of these medications and their frequency by prescription of the participants (Table 2).
2.3. Experimental Protocol
The study was single-blinded since the trained scorer was also involved in the tDCS delivery procedures. The experiment took place in the Laboratory of Neuroscience and Behavior located in the Institute of Biology at the University of Brasilia. In a controlled environment, the selection of the participants was made using a draw with a system of tokens, and the participants did not know whether they would receive “active” or “sham” stimulation.
The patients were randomly assigned to one of two groups (sham control and active stimulation group). They received tDCS with the anode positioned over the left dorsolateral prefrontal cortex region (F3 of the 10-20 international system for electroencephalography electrodes placement) and the cathode over the right supraorbital region (Fp2), either with continuous delivery of electric current at 2mA for 20 minutes (active group), or with the current turned off (sham stimulation control group) after a brief ramp-up stimulation to ensure the patients would experience a tingling effect similar to that perceived during real stimulation. Both groups underwent 3 sessions approximately 24 hours apart. Motor and non-motor assessments were done in the first session (visit 1, day 1) and in the last one (visit 3, day 3).
Selection of tDCS parameters: The most frequently used tDCS protocols in clinical trials with Parkinson’s disease patients have been: 1) excitatory electrode over the left dorsolateral prefrontal cortex (L-DLPFC) and cathode over the right supraorbital region and 2) anode over the motor area (M1) and cathode over the right supraorbital or right dorsolateral prefrontal cortex (R-DLPFC) [1,3,15,17,20,21]. Therefore, our research protocol was chosen according to the prevailing methods described in the literature.
2.4. Transcranial Direct Current Stimulation Apparatus
The tDCS stimulator used was developed especially for research purposes and was calibrated by the Biomedical Engineering Laboratory of the Faculty of Technology at the University of Brasília. It was powered by two 9 V batteries, with current intensity control ranging from a minimum of 0.5mA to a maximum of 2mA. The stimulator had a manual switch that enabled cutting off the current flow during the sham stimulation sessions. The electrodes were made of conductive rubber encased in porous sponges (35cm) soaked in saline solution. The montage sites on the scalp were based on the International 10-20 EEG System.
2.5. Evaluations
2.5.1. Motor Functions
The Unified Parkinson’s Disease Rating Scale (UPDRS), part III (motor examination), was used to evaluate the following cardinal signs: Bradykinesia, either in initiation or performance in which overall body movements were observed [22]; Rigidity, identified by the classical cogwheel sign [16,22]; Rest tremor which is known to increase in situations of emotional stress, mental effort and during gait. It is reduced by active movement of the limb and disappears in sleep [22,23]. Finally, postural instability is a motor symptom expressed by the loss of postural readaptation and the freezing of gait reflexes that becomes evident with the abrupt change of direction in gait or the execution of a rapid movement [22,24].
2.5.2. Non-Motor Functions
2.5.2.1. Mood Swings: Depression and Anxiety
The Hospital Anxiety and Depression Scale (HADS) was the instrument that assessed mood symptoms. It consists of seven items that identify anxiety symptoms (HADS-A) such as tension; fear; excessive worry; agitation; distress; restlessness; and feeling of loss of control [25]. There is also a seven-item questionnaire for symptoms of depression (HADS-D): depressed mood; apathy; reduction to emotional stimuli; lethargy; lack of energy; and anhedonia [9,25].
2.5.2.2. Cognition and Executive Functions
The Parkinson’s Disease Cognitive Rating Scale (PD-CRS) was employed to measure cognition and executive functions. The test consisted of frontal subcortical tasks, with the following items: verbal memory of immediate recall; sustained attention; working memory; spontaneous clock drawing; verbal memory of delayed recall; alternating verbal fluency, and verbal fluency of action [10]. The tasks related to the type of impaired cognition in the higher cortical subtype corresponded to the items: naming by visual confrontation and copying the clock [11]. We also used the Stroop Test in the “reading” and “color naming” versions to further assess executive functions. The Stroop Test protocol allowed the identification of a pattern of responses according to the interference effect in which errors and correct answers provided by congruent and incongruent stimuli were considered [26]. This analysis model and the applicability of the Stroop Test for patients with Parkinson’s disease have been validated [11,12].
2.6. Statistical Analysis
Statistical analysis was performed using the Statistical Package for Social Sciences, SPSS. version 25. Spearman’s correlation test was applied to identify correlations between scale variables, performance in the Stroop Test and demographic and clinical characteristics of the participants at study baseline. Wilcoxon (non-parametric) and paired t-tests (parametric) were performed to check whether there were significant differences between the participants in the sham control and active groups in the pre- and post-stimulation periods. Moreover, the Wilcoxon test was used to analyze the data from the scales, while the paired t-test compared the hit-and-miss rates in the pre- and post-stimulation conditions in the Stroop test. The significance level adopted was p ≤ 0.05.
3. Results
The study sample comprised 18 individuals, all diagnosed with Parkinson’s disease according to the Criteria of the London Brain Bank. The volunteers had preserved cognitive status and some motor impairment. The PD staging score by the Hoehn & Yahr scale shows 7 volunteers classified as stage 1.5, which refers to the initial level with unilateral symptoms associated with axial involvement (craniocervical or trunk).
3.1. Motor Evaluation
In the first analysis, we observed that the sham group did not show significant differences between baseline and post-3-day test evaluation (Table 3).
In the active group, however, we found significant differences pre vs post-evaluation for: finger tapping on the right upper limb (p=0.038), hand movement on the right upper limb (p=0.046), posture (p=0.034) and gait (0.025) (Table 4).
Regarding the total score for the UPDRS scale, the active group presented, from the pre- to the post-stimulation moment, a greater variation in scores when compared to the sham group (Figure 1). The median decreased from 18 to around 15, and there were changes in the percentile levels as well. In the sham group, the median increased slightly. The quartiles kept similar levels from the pre- to the post-phase. In the active group, the median remained below 20 on the full scale, both before and after stimulation. For the sham group, the scale was scored above 20, i.e., the scale levels for the sham group were slightly higher.
3.2. Effects on Mood
The Wilcoxon test did not indicate significant differences for the sham group when comparing the participants’ scores in terms of anxiety and depression measured by the HADS scale in the pre-stimulation and post-stimulation sessions (Table 5).
As for the active group, there was a significant result in item (3): “I get a sort of frightened feeling as if something awful is about to happen” (p= 0,039). (Table 6)
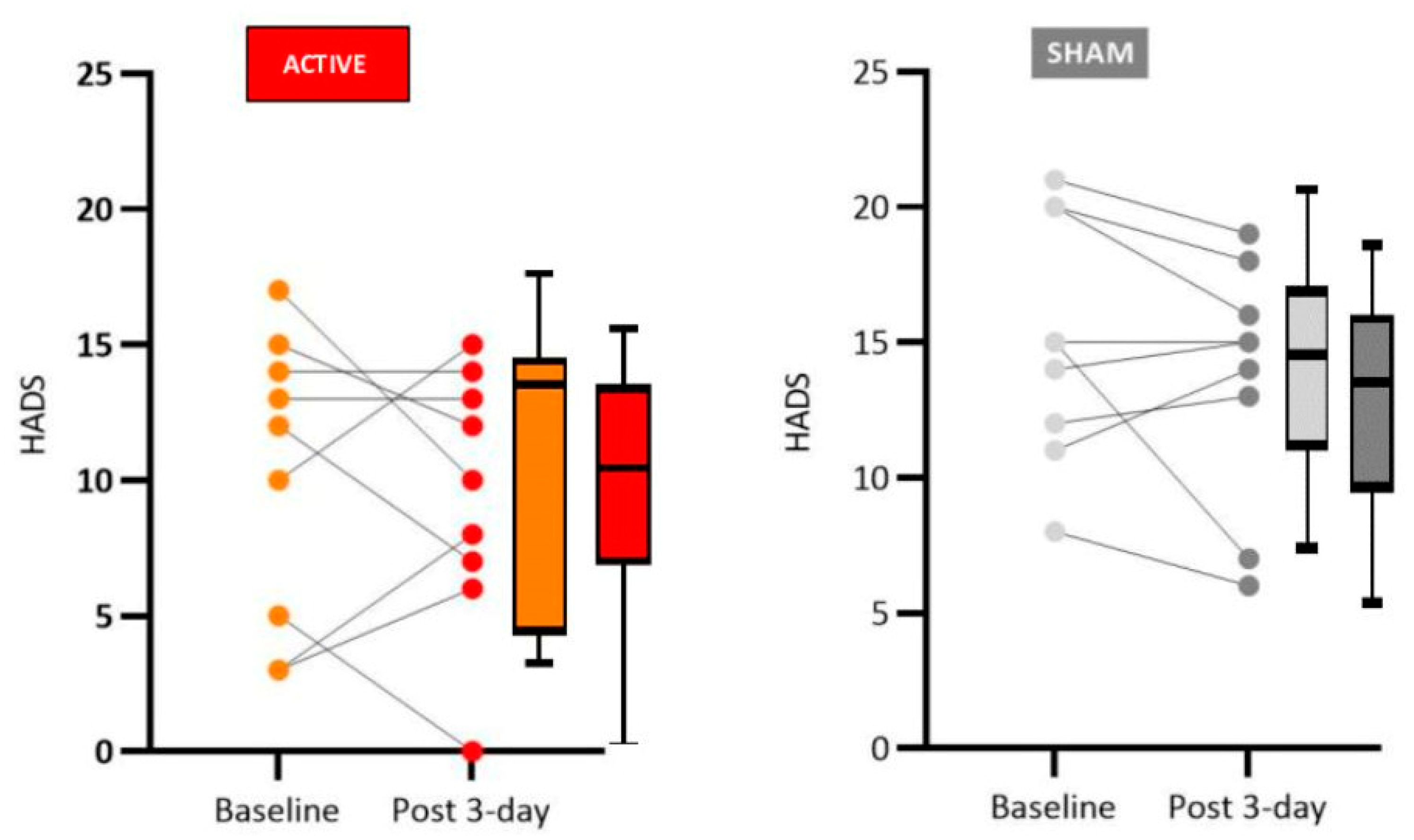
Regarding the percentiles that show the objective results of the scale, there was no discernible pattern of variation between the quartiles in the graphs, either for the sham or the active group (Figure 2).
3.3. Effects on Cognition and Executive Functions
In the PD-CRS scale, the sham group did not show significant differences between baseline and post-3-day test evaluation (Table 7).
In contrast, for the active group, there were significant results concerning the frontal-subcortical tests: (1) immediate free recall verbal memory (p=0,016) and (9) action verbal fluency (p=0,018). Furthermore, results were also significant in the cortical tests: (2) confrontation naming (p=0,011) and (6) copy drawing of a clock (p=0,024) (Table 8).
The results of the total scores of the PD-CRS scale indicated an increase from pre- to post-stimulation levels in both groups. However, the performance of the active group was considerably higher.
Figure 3.
Effects of tDCS on mood for the real and sham groups. A low score on the HADS scale indicates better mood. The mean score for the real group decreased suggesting a mood improvement (although 3 out 8 participants showed an increase). No difference was observed for the mean score in the sham group (although 3 out 8 participants showed a decrease in the HADS score).
Figure 3.
Effects of tDCS on mood for the real and sham groups. A low score on the HADS scale indicates better mood. The mean score for the real group decreased suggesting a mood improvement (although 3 out 8 participants showed an increase). No difference was observed for the mean score in the sham group (although 3 out 8 participants showed a decrease in the HADS score).
The participants’ performance after tDCS sessions for the Color and Word Stroop Test was determined by the Wilcoxon Test. The analysis is based on right answers, errors, and omissions. The p-value between the groups indicated significant results for the correct answers in both groups: sham (p=0.041) and active (p=0.018) (Table 9 and Table 10).
In Figure 4 it is possible to observe the effects of tDCS in the active group when the participants’ performance was better in the post-stimulation tests than at baseline. In the sham group, it was also possible to observe a better result when comparing the baseline to the post-stimulation scores. Statistical analysis shows significant differences in both groups.
In Figure 5 it is possible to observe the effects of tDCS in the active group when the performance of the participants was better in the post stimulation tests than at baseline. In the sham group it was also possible to observe a better result when comparing baseline to the post-stimulation scores. Statistical analysis of the median shows significant differences in both groups.
4. Discussion
Levodopa is a primary treatment for PD with beneficial effects for most patients. However, long-term complications such as motor fluctuations, dyskinesias, major depression, and psychotic symptoms are possible. Moreover, as PD progresses, levodopa effects wear off and other clinical manifestations also occur, both motor and non-motor, such as freezing of gait and dementia [7].
Additional strategies that improve the patient’s symptoms and quality of life are essential. In this regard, recent studies have suggested a possible role for non-invasive electrical stimulation. Transcranial electrical stimulation can modulate resting membrane potentials, therefore generating changes in the polarization and depolarization process that may improve symptoms of neurological diseases [27]. tDCS allows synaptic plasticity while exciting or inhibiting brain regions, an adaptive neural strategy.
Differently from transcranial magnetic stimulation (TMS), tDCS cannot produce motor evoked potentials since the change in resting membrane potential does not reach the threshold for action potential firing. However, prolonged modulation, applied for more than three minutes, can generate changes in glutamatergic and GABAergic receptors [28]. The spatial resolution of tDCS is uncertain since it may also influence deeper brain structures connected to the target cortical region. [29].
Our results have shown significant improvement in motor function in PD patients who received active tDCS anodal stimulation to the left dorsolateral prefrontal cortex region (2mA for 20 min, 3 sessions), particularly regarding rigidity, the finger tapping test, posture, and general gait patterns. Non-significant improvement was observed for participants who received sham tDCS.
It is important to point out that other authors have previously reported both similar and divergent results. Therefore, at the present stage of this field of study, it is important to try to replicate previous results so that meaningful meta-analysis can be done to instruct future controlled clinical trials. An example of these uncertainties concerns studies that investigated the effects of tDCS on PD patients using anodal stimulation to the left dorsolateral prefrontal cortex (L-DLPFC). Doruk et al. [2], in ten neuromodulation sessions with an intensity of 2mA, did not obtain significant improvement in motor function, while Chang et al. [30], with five sessions, employing a current intensity of 1mA for 20 minutes, obtained a satisfactory short-term response for the occurrence of freezing. Swank [31], in a study that employed two sessions, with a current intensity of 2 mA for 20 minutes, obtained moderate evidence of improved motor functions measured by UPDRS.
Studies in which tDCS was applied to the primary motor area presented more agreement regarding satisfactory results. Fregni et al. [28], with a single session and a current intensity of 1mA for 20 minutes, observed significant improvement in motor function, as did Benninger [21] with eight sessions, at 2mA of intensity and 20 minutes of stimulation; Valentino [32], with five sessions, at 2mA intensity for 20 minutes, and Kaski [33] with five sessions, at 2mA intensity for 3 minutes of tDCS, employing a dancing task. The most significant motor effects described in the literature were improvements in gait, rigidity, and bradykinesia, evaluated with the Timed Up and Go motor test, as well as other gait performance assessments [19,34].
Although sleep disorders in PD are known to represent a major aspect of Parkinsonian patients’ complaints, this variable is not a frequently evaluated parameter in tDCS studies. Despite the low rate of sleep assessments, Hadoush and collaborators [28], using a study protocol of anodal tDCS applied to the L-DLPFC, in 20-minute sessions with an electrical current intensity of 2mA, obtained significant improvements in sleep latency, global sleep quality, reduction in sleeping medication, in sleep disorders, as well as a reduction in daytime dysfunction. Forogh and co-workers [16] investigated the effects of anodal tDCS on the L-DLPFC, during 10 sessions, each lasting 20 minutes with a current intensity of 2 mA. The results were reevaluated after three months, and a significant improvement in fatigue was noted, something that was questioned by the researchers as being an effect of improvement in mood and not necessarily in sleep quality.
The results obtained in our study regarding the mood domain align with what the literature shows for anodal L-DLPFC stimulation for mood, which is the most consolidated protocol for depression treatment and is already used in clinical practice. Patients in the active group showed an improvement in mood, particularly clear for a decrease in anxiety. The literature explains the improvement in depressive symptoms and other behavioral effects of tDCS through a process akin to long-term potentiation (LTP) in which there is a permanent increase in synapse strength due to high-frequency stimulation produced by a chemical stimulus. LTP is likely triggered by applying a low-intensity direct current that changes the intracerebral current flow, generating effects compatible with mood improvement [35,36,37].
Moreover, depression in PD is associated with changes in dopaminergic pathways, and cortical and subcortical afferents in which the irregular neuronal excitability reaches L-DLPFC causing psychiatric manifestations in some patients. It is likely that anodal tDCS over the L-DLPFC also produces neuromodulation of the DA system in this area [37].
Again, there is some controversy regarding the mood modulation of PD patients by tDCS. Some studies employing L-DLPFC tDCS with PD patients have shown improvement in anxiety and depression [17,39], while others did not observe mood improvement with a single session of tDCS. Manenti [18] used the neuromodulation protocol with a constant current of 2 mA applied for 7 minutes (with a ramping period of ten seconds at the beginning and end of the stimulation) and observed a slight momentary improvement in the mood of the participants. Lawrence [17] used a protocol with an intensity of 2mA for 20 minutes and the effects on depression were significant when associated with cognitive training for four weeks. Impressive results on mood improvement were observed in the studies by Pereira [39], who conducted a study with a single session of tDCS with the intensity of 2 mA.
Another important aspect related to PD is that, as the pathology progresses, a specific dementia picture, called Parkinson’s Disease Dementia, becomes evident. Therefore, the cognitive profile of patients who develop this dementia has greater impairment in executive functions, attention, and visuospatial memory (which would be associated with subcortical changes) and a lesser impairment in declarative memory, language, and practice (which would be associated with cortical changes) [39].
We found significant improvement in patients who received active tDCS stimulation compared to sham tDCS in cognitive functions related to verbal memory (free and immediate recall), naming by visual confrontation, clock copy test, and verbal fluency. Although the sham group did not present significant changes concerning pre- and post-stimulation tests (Wilcoxon test, see tables in the Results sections for details), the medians were slightly reduced between the phases, suggesting a possible learning effect for repeated tests. Therefore, the difference observed between active and sham control groups is likely due to the tDCS treatment and not only to the learning effects of repeated testing.
Regarding the cognitive effects of anodal tDCS when applied in L-DLPFC of patients with PD, the literature points to the effectiveness of the technique, thus corroborating our results. For instance, Boggio et al. [38] using a 2mA protocol of current intensity applied for 20 minutes in a single session observed an increase in the scores of the response time and working memory test. Pereira et al. [39] identified a significant improvement in phonological verbal fluency after a 20-minute session, applied with a current intensity of 2mA.
The Stroop Test is widely used in evaluating executive functions in patients with PD because it measures an ability commonly impaired in pathology, the inhibitory control [40]. Studies show that the Stroop test is reliable for identifying deficits associated with L-DLPFC and the main motor area [6,41].
The performance of our patients who received real tDCS showed a significant improvement in the number of correct answers and error reduction in the Stroop test, suggesting activation of executive functions with increased inhibition control, cognitive flexibility and working memory.
Regarding executive functions, Doruk [2] reported that anodal tDCS over the L-DLPFC, after 20-minute sessions of 2mA stimulation, improves the performance of the Trail Making Tests. Manenti and collaborators [19] investigated the effects of anodal transcranial direct current stimulation applied over the dorsolateral prefrontal cortex and combined with physical therapy in PD patients. Their results indicated improved motor abilities, reduced depressive symptoms, and increased performance in the Parkinson’s Disease Cognitive Rating Scale and verbal fluency test. Lawrence et al. [17] showed significant improvements across executive function, attention/working memory, memory, language, activities of daily living, and quality of life.
There are some potential limitations in this study, such as the small number of participants and the low number of tDCS sessions and follow-up time. Future cross-over studies would be useful to observe, with greater accuracy, the effects of treatments with the patients as their controls. However, an appropriate wash-out time interval must be determined to prevent the residual effects of previous stimulations. Another limitation was the unblinded condition of the examiners. Since one of the researchers applying tDCS also had to be trained for scoring the patients, the study was not double-blinded, a problem that should also be addressed in future studies.
Another confounding factor is the variable drug regimens of the patients included in the study. However, for medical and ethical reasons, it is impossible to withdraw or standardize drug treatments in all patients. Many patients were receiving benzodiazepines. Many of our patients were on benzodiazepines, which raises the question of possible pharmacological interference with our results. However, neuroplastic after-effects of tDCS are NMDA-receptor dependent [42]. Anodal after-effects can be selectively suppressed by the sodium channel blocker carbamazepine and the calcium channel blocker flunarizine [43]. tDCS after-effects are also thought to be mediated by synaptic modulation similar to those occurring in long-term potentiation studies. In this regard, Xu and Sastry [44] have found that benzodiazepine receptors do not participate in LTP induction. Thus, it is unlikely that the use of benzodiazepines by our patients has had a significant effect on the observed tDCS after-effects.
Finally, larger randomized-controlled trials, using more than one scale to assess motor function and with extended follow-up periods are needed for elucidating the potential role of this new treatment modality in the clinical management of PD patients.
5. Conclusions
This study identified improvement after tDCS neuromodulation on motor functions, especially in gait patterns, posture, and subtests indicative of bradykinesia (hand movements and finger tapping). Regarding mood spectrum, significant improvements were observed for the real group concerning anxiety and depression after tDCS. As to cognition and executive functions, tDCS showed positive effects on the items: verbal memory with immediate free recall, naming pattern by visual confrontation, the clock copy test, and verbal fluency of actions. Finally, the performance on the Stroop test for executive functions showed an improvement for both congruent and incongruent stimuli.
The present results indicate that tDCS neuromodulation of the left dorsolateral prefrontal cortex region is feasible, safe, and might provide significant clinical benefits for PD patients. Further controlled studies with larger numbers of patients are necessary to establish the real potential of this non-pharmacological tool in the management of PD patients.
Author Contributions
Conceptualization, F.P. and M.C.H.T.; methodology, F.P., M.C.H.T. and J.B.N., ; formal analysis, F.P., M.C.H.T., C.T., N.A., P.B. and J.B.N..; investigation, F.P. and M.C.H.T.; writing—original draft, F.P., M.C.H.T., C.T., P.B., N.A. and J.P.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study protocol was reviewed and approved by the Research Ethics Committee of the Faculty of Health Sciences of the University of Brasília, DF, Brazil, under the number CAE:91375218.9.0000.0030.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are contained within the article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Brunoni A, Nitsche MA, Loo C. Transcranial direct current stimulation in neuropsychiatric: clinical principles and management. Switzerland: Springer Nature Switzerland (2016).
- Doruk D, Gray Z, Bravo G, Pascual-Leone A, Fregni F. Effects of tDCS on executive function in Parkinson’s disease. Neurosci. Lett. (2014), 582 (1) 2731-2739. [CrossRef]
- Broeder S, Nackaerts E, Heremans E, Vervoort G, Meesen R, Verheyden G, Nieuwboer A. Transcranial direct current stimulation in Parkinson’s disease: neurophysiological mechanism and behavior effects. Neurosci. Beh. Rev. (2015), 57, p105-117. [CrossRef]
- Tysnes, O.B.; Storstein, A. Epidemiology of Parkinson’s disease. J. Neur. Transm. 2017, 124, 901–905. [Google Scholar] [CrossRef] [PubMed]
- Bhatia KP, Chaudhuri KR, Stamelou M. Parkinson’s Disease. Int. Rev. Neurobiol. (2016), 132, 122-146.
- Braak H, Braak E, Yilmazer D, de Vos RA,Jansen ENH, Bohl J, Jellinger K. Amygdala pathology in Parkinson’s disease. Acta Neuropathol. (1994), 88(6), 493–500. [CrossRef]
- Braak H and Del Tredici, K. Invited Article: Nervous system pathology in sporadic Parkinson disease. Neurol. (2008), 13;70(20):1916–1925. [CrossRef]
- Martinez-Martin P, Rodriguez-Blazquez C, Forjaz MJ, Chaudhuri KR. Guide to assessment scales in Parkinson’s disease. United Kingdom Springer Healthcare (2014), p 14-46.
- Goodarzi Z, Mrklas KJ, Roberts DJ, Jette N, Pringsheim T, Holroyd-Leduc J. Detecting depression in Parkinson disease. Neurol. (2016), 87(4), 426–437. [CrossRef]
- Pagonabarraga J, Kulisevsky J, Llebaria G, Garcia-Sanchez C, Pascual-Sedano B, Gironell A. Parkinson’s disease-cognitive rating scale: a new cognitive scale specific for Parkinson’s disease. Movement disorders: official journal of the Movement Disorder Society. Mov Disord (2008), 23: 998-1005. [CrossRef]
- Bettcher BM, Mungas D, Pate lN, Elofson J, Dutt S, Wynn M, Watson CL, Stephens M, Walsh CM, Kramer J.H. Neuroanatomical substrates of executive functions: Beyond prefrontal structures. J. Neuropsychol. (2016). 85:100-9. [CrossRef]
- Kleiner AFR, Pagnussat AS, diPrisco G, Vagnini A, Stocchi F, De Pandis MF, Galli M. Analyzing gait variability and dual-task interference in patients with Parkinson’s disease and freezing by means of the word-color Stroop test. Ag. Clin. Exp. Res. (2017), 30(9), 1137–1142. [CrossRef]
- Langston RG and Virmani T. Use of a Modified STROOP Test to Assess Color Discrimination Deficit in Parkinson’s Disease. Front. Neurol. (2018). [CrossRef]
- Ishikuro,K. Nobuhiro,D, Nukui,T, Yamamoto M, Nakatsuji, Y, Kuroda, S, Matsushita,I, Nishimaru, I, Araujo,FP, Nishijo, H. Effects of Transcranial Direct Current Stimulation (tDCS) Over the Frontal Polar Area on Motor and Executive Functions in Parkinson’s Disease; A Pilot Study. Front Aging Neurosci (2018)10: 231. [CrossRef]
- Yotnuengnit P, Bhidayasiri R, Donkhan R, Chaluay J, Piravej K. Effects of Transcranial Direct Current Stimulation Plus Physical Therapy on Gait in Patients with Parkinson Disease: A Randomized Controlled Trial. Johannesgatan: American Journal of Physical Medicine & Rehabilitation. (2018), No. 97, pp. 7-15. [CrossRef]
- Forogh B, Rafiei M, Arbabi A, Motamed MR, Madani SP, Sajadi S. Repeated sessions of transcranial direct current stimulation evaluation on fatigue and daytime sleepiness in Parkinson’s disease. Neurol. Sci. (2017), 38(2), 249–254. [CrossRef]
- Benussi, A; Alberici, A; Cantoni, V; Manenti, R; Brambilla, M; Dell’Era, V; Borroni, B. Modulating risky decision-making in Parkinson’s disease by transcranial direct current stimulation. European Journal of Neurology, 2017; 24(5), 751–754.
- Lawrence BJ, Gasson N, Johnson AR, Booth L, Loftus AM. Cognitive Training and Transcranial Direct Current Stimulation for Mild Cognitive Impairment in Parkinson’s Disease: A Randomized Controlled Trial. Parkinson’s Disord. (2018). [CrossRef]
- Manentti R, Brambilla M, Rosini S, Orizio I, Ferrari C, Borroni B, Cottelli M. Time up and go task performance improves after transcranial direct current stimulation in patient affected by Parkinson’s disease. Neurosci. Lett. (2014), Sep 19; 580:74-7. [CrossRef]
- Boggio PS, Ferrucci R Rigonatti, SP, Covre P, Nitsche M, Pascual-Leone A., Fregni F. (2006) Effects of transcranial direct current stimulation on working memory in patients with Parkinson’s disease. J. Neurol. Sci. (2006), 249(1), 31–38. [CrossRef]
- Benninger DH, Lomarev M, Lopez G, Wassermann EM, Li X, Considine E, Hallett M. Transcranial direct current stimulation for the treatment of Parkinson’s disease. J. Neurol. Neurosurg. Psych. (2010), p 81(10), 1105–1111. [CrossRef]
- Goetz CG,Tilley BC, Shaftman RS, Stebbins GT, Fahn S, Martinez-Martin P, Poewe W, Sampaio CV, Stern MB, Dodel R, Dubois B, Holloway R, Jankovic J, Kulisevsky J, Lang AE, Lees A, Leurgans S, LeWitt PA, Nyenhuis D, Olanow W, Rascol O, Schrag A, Teresi JA, J van Hilten J, LaPelle N. Movement Disorder Society-Sponsored. Revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Scale Presentation and Clinimetric Testing Results. Mov. Disord. (2008), Vol. 23, No. 15, pp. 2129–2170. [CrossRef]
- Walter U, Kleinschmidt S, Rimmele F, Wunderlich C, Gemende I, Benecke R, Busse, K. Potential impact of self-perceived prodromal symptoms on the early diagnosis of Parkinson’s disease. J. Neurol. (2013). 260(12), 3077–3085. [CrossRef] [PubMed]
- Skorvanek M, Martinez-Martin P, Kovacs N, Rodriguez-Violante M, Corvol JC, Taba P, Stebbins GT. Differences in MDS-UPDRS Scores Based on Hoehn and Yahr Stage and Disease Duration. Mov. Disord. Clin. Pract. (2017). 4(4), 536–544. [CrossRef]
- Zigmond AS and Snaith, RP. The hospital anxiety and depression scale. Acta Psychiatr. Scand. (1993), Jun; 67(6):361-70. [CrossRef]
- Macleod, CM. John Ridley Stroop: creator of a landmarker cognitive task. Canad. Psychol./Psychol. Canad. (1991), p 32:3. [CrossRef]
- Bear, Mark F., et al. Neuroscience: Exploring the Brain. Fourth edition. Philadelphia, Wolters Kluwer, 2016.
- Fregni F. Boggio PS, Nitsche M, Marcolin MA, Rigonatti SP, Pascual-Leone A. Treatment of major depression with transcranial direct current stimulation. Bipol. Disord (2006), 8, 203–205. [CrossRef]
- Raimundo, R. J. S., Uribe, C. E., & Brasil-Neto, J. P. (2012). Lack of clinically detectable acute changes on autonomic or thermoregulatory functions in healthy subjects after transcranial direct current stimulation (tDCS). Brain stimulation (2012). 5(3), p.196-200. [CrossRef]
- Chang WH, Kim MS, Park E, Cho JW, Youn J, Kim YK, Kim YH. (2017) Effect of Dual-mode and Dual-site Non-invasive Brain Stimulation on Freezing of Gait in Patients with Parkinson’s Disease. Arch. Phys. Med. Rehab. (2017), Jul;98(7):1283-1290. [CrossRef]
- Swank A C, Mehtab J, Criminberc C. Transcranial direct current stimulation lessens dual task cost in people with Parkinson’s disease. Neurosci. Lett. (2016) 626 1–5. [CrossRef]
- Valentino F, Cosentino G, Brighina F. Transcranial direct current stimulation for treatment of freezing of gait: a cross-over study. Mov. Disord. (2014), 29(8):1064–106910. [CrossRef]
- Kaski D, Dominguez R, Allum J, Islam A, Bronstein A. Combining physical training with transcranial direct current stimulation to improve gait in Parkinson’s disease: a pilot randomized controlled study. Clin. Rehab. (2014), 28(11), 1115–1124. [CrossRef]
- Goldman JG and Litvan, I. Mild cognitive impairment in Parkinson’s disease. Minerva Med. (2011), 102(6): 441-59. [CrossRef]
- Brunoni A, R. Princípios da prática do uso da neuromodulação não invasiva em psiquiatria. Porto Alegre: Artmed (2017).
- Miniussi C, Paulus W, Rossini PM. Transcranial Brain Stimulation. Front. Neurosci. United Kingdom: Taylor & Francis Group LLC. (2013). p.56-69.
- Nitsche, MA, Cohen LG, Wassermann EM, Priori A, Lang N, Pascual-Leone A. (2008) Transcranial direct current stimulation: State of the art. Brain Stimul. (2008), 1(3), 206–223. [CrossRef]
- Hadoush K, Al-Sharman A, Khalil S, Banihani A, Al-Jarrah M. Sleep Quality. Depression, and Quality of Life After Bilateral Anodal Transcranial Direct Current Stimulation in Patients with Parkinson’s Disease. Med. Sci. Monit. Basic. Res. (2018); p.24:198-205. [CrossRef]
- Pereira JB, Junqué C, Bartrés-Faz D, Martí MJ, Sala-Llonch R, Compta Y,Falcón C, Vendrell P, Pascual-Leone A, Valls-Solé J, Tolosa E Modulation of verbal fluency networks by transcranial direct current stimulation (tDCS) in Parkinson’s disease. Brain Stimul. (2013) p 16–22. [CrossRef]
- Dinkelbach L, Brambilla M, Manenti R, Brem, A.K. Non-invasive brain stimulation in Parkinson’s disease: Exploiting crossroads of cognition and mood. Neurosci. Biobehav. (2017), Rev.75. p407-418. [CrossRef] [PubMed]
- Ferrucci R, Bocci T, Cortese F, Ruggiero F, Priori A. Cerebellar transcranial direct current stimulation in neurological disease. Cereb. Atax. (2016); 3(1) 58-66. [CrossRef]
- Liebetanz, D., Nitsche, M. A., Tergau, F., & Paulus, W. (2002). Pharmacological approach to the mechanisms of transcranial DC-stimulation-induced after-effects of human motor cortex excitability. Brain, 125, 2238–2247. [CrossRef]
- Nitsche, M. A., Fricke, K., Henschke, U., Schlitterlau, A., Liebetanz, D., et al. (2003). Pharmacological modulation of cortical excitability shifts induced by transcranial direct current stimulation in humans. Journal of Physiology, 553, 293–301. [CrossRef]
- Xu, J.-Y. and Bhagavatula Sree Rama Sastry. Benzodiazepine involvement in LTP of the GABA-ergic IPSC in rat hippocampal CA1 neurons. Brain Research 1062 (2005): 134-143. [CrossRef]
Figure 1.
Effects of tDCS on motor symptoms for the real and sham groups. According to the UPDRS, low scores indicate a lower occurrence of motor symptoms. It is possible to observe a drop in the measured indexes when comparing baseline with post-stimulation. The sham group did not show significant results.
Figure 1.
Effects of tDCS on motor symptoms for the real and sham groups. According to the UPDRS, low scores indicate a lower occurrence of motor symptoms. It is possible to observe a drop in the measured indexes when comparing baseline with post-stimulation. The sham group did not show significant results.
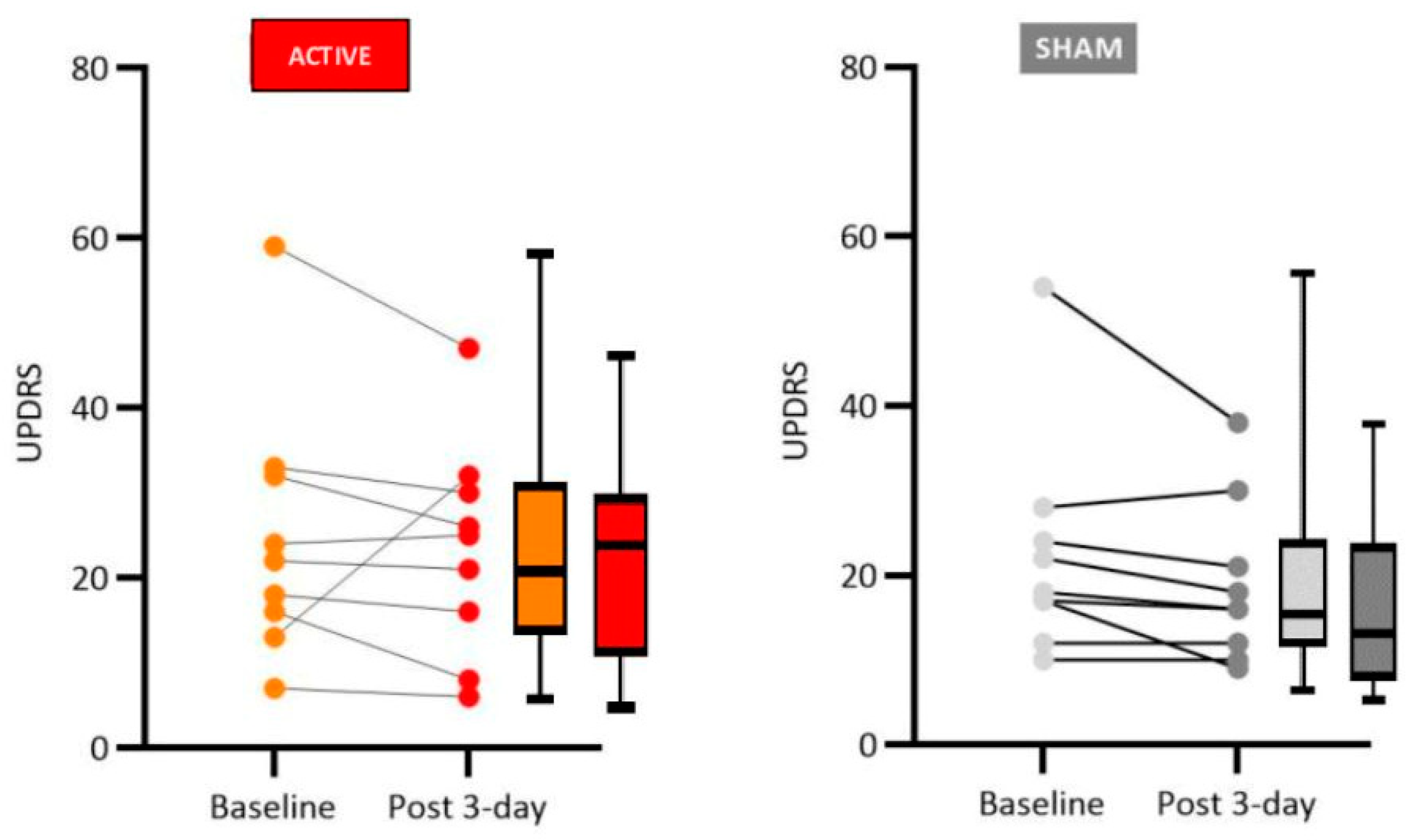
Figure 2.
Effects of tDCS on sleep disorders for the real and sham groups. Low scores indicate more severe sleep disorders. For the real group, we identified a significant increase in the medians of the participants pointing to a positive effect of tDCS. No significant statistical difference was observed for the sham group.
Figure 2.
Effects of tDCS on sleep disorders for the real and sham groups. Low scores indicate more severe sleep disorders. For the real group, we identified a significant increase in the medians of the participants pointing to a positive effect of tDCS. No significant statistical difference was observed for the sham group.
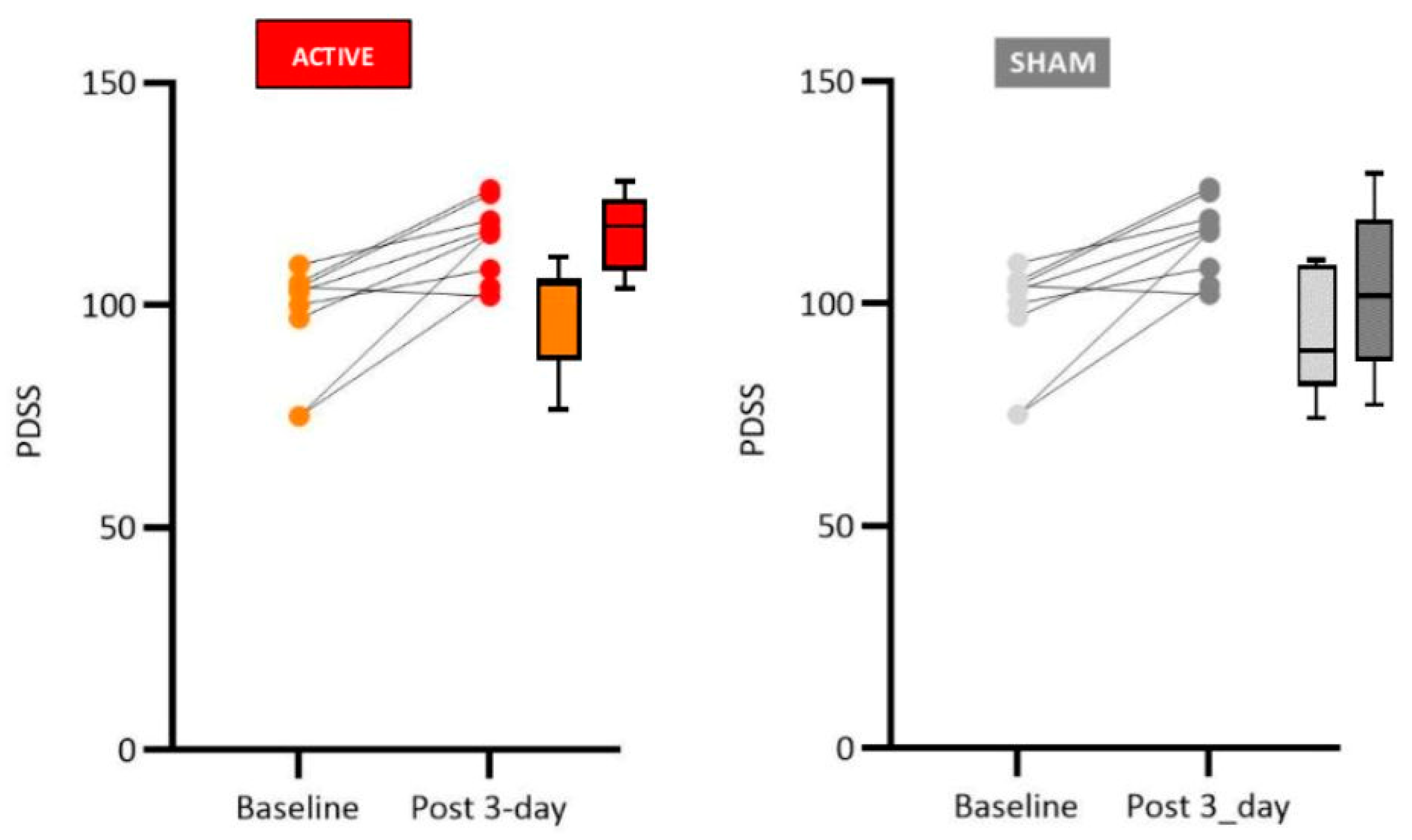
Figure 4.
Effects on executive functions for the real and sham groups. Higher PD-CRS scores indicate better cognitive performance. Total scores of the PD-CRS scale indicated an increase from pre- to post-stimulation levels for both groups, although the performance for the real group was considerably higher.
Figure 4.
Effects on executive functions for the real and sham groups. Higher PD-CRS scores indicate better cognitive performance. Total scores of the PD-CRS scale indicated an increase from pre- to post-stimulation levels for both groups, although the performance for the real group was considerably higher.
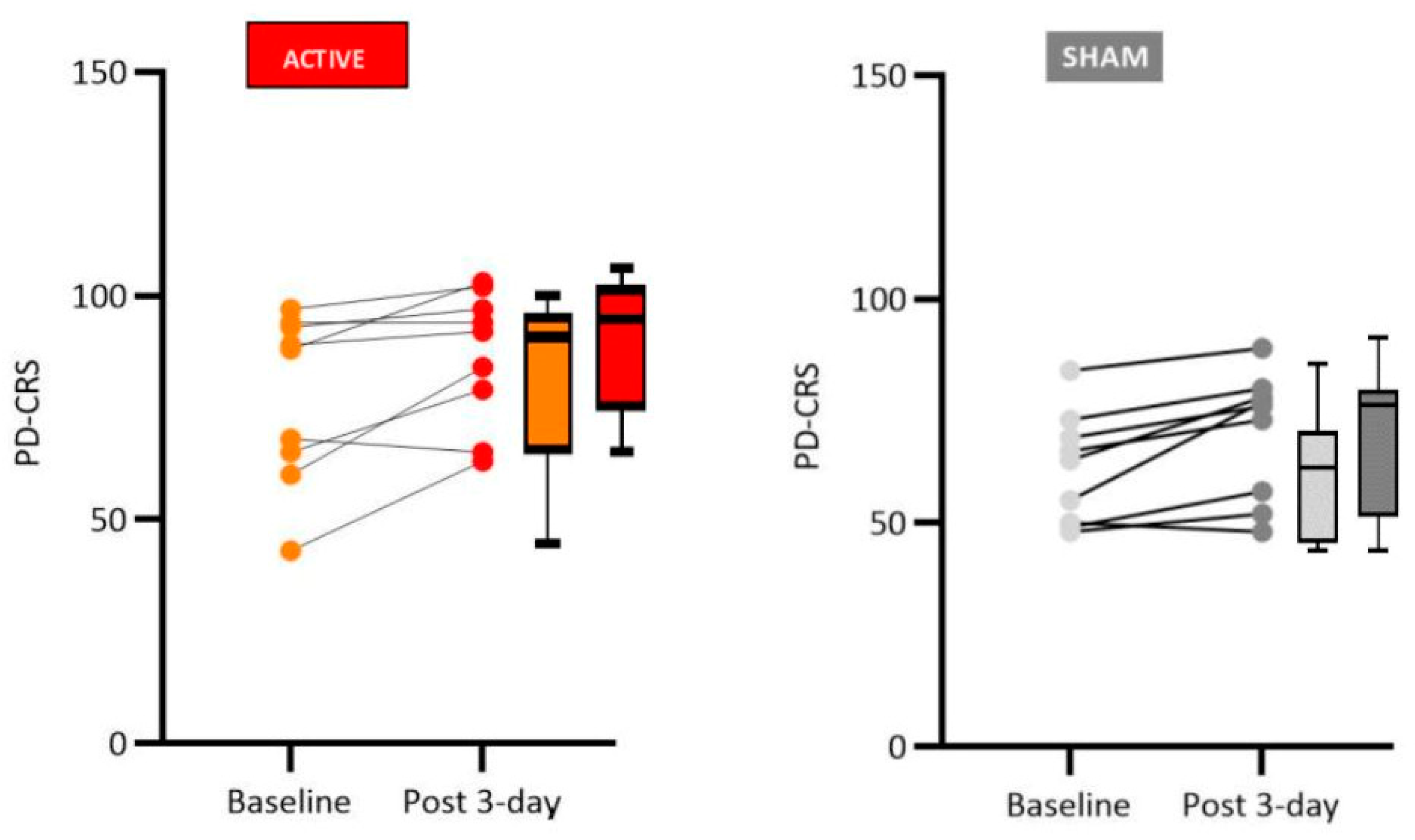
Figure 5.
In the Stroop test, a higher score indicates better performance in the executive functions. As can be seen, both groups show improvement in the performance between baseline and post/stimulation test.
Figure 5.
In the Stroop test, a higher score indicates better performance in the executive functions. As can be seen, both groups show improvement in the performance between baseline and post/stimulation test.
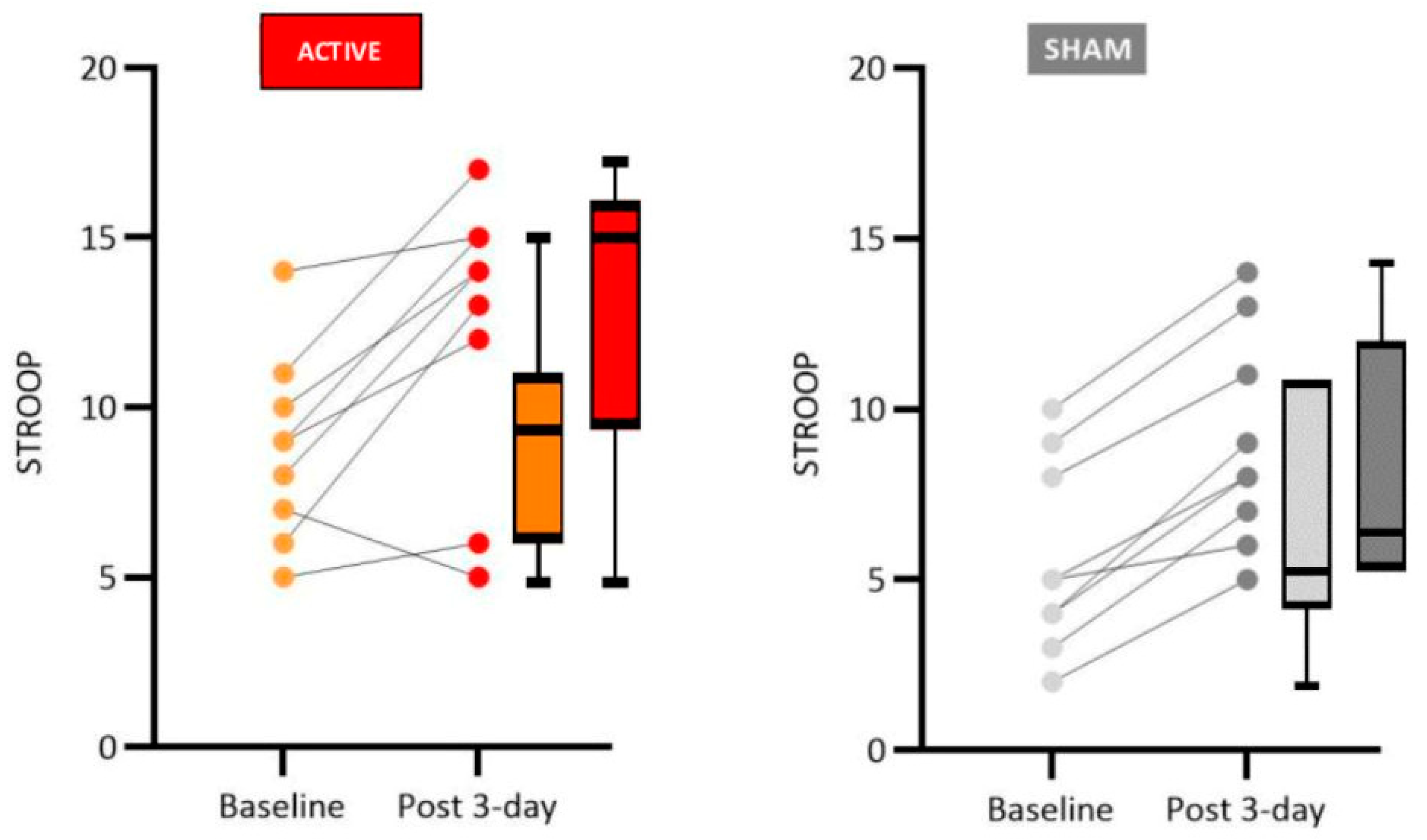
Table 2.
Description of the sample according to drug treatment of comorbidities.
| Other drugs for comorbidities | F | % |
|---|---|---|
| Does not use other medications | 2 | 11,11% |
| Antidepressants | ||
| Mirtazapine | 1 | 5,56% |
| Antidepressants + antihypertensive + Antidiabetic + Antidyslipidemic | ||
| Sertraline + Losartan + Metformin + Simvastatin | 1 | 5,56% |
| Antidepressants + Neuroleptic | ||
| Venlafaxine + Quetiapine | 1 | 5,56% |
| Antidepressants +Sedative | ||
| Mirtazapine + Alprazolam | 1 | 5,56% |
| Antidepressants + Sedative + Anticholinergic | ||
| Sertraline + Alprazolam + Tamsulosin | 1 | 5,56% |
| Antifungal + Anticholinergic | ||
| Fluconazole + Biperiden | 1 | 5,56% |
| Antihypertensive | ||
| Valsartan | 1 | 5,56% |
| Antihypertensive + Antidepressants + Antidyslipidemic | ||
| Hydrochlorothiazide + Amitriptyline + Simvastatin | 1 | 5,56% |
| Antihypertensive + Antidiabetic | ||
| Enalapril + Metformin | 1 | 5,56% |
| Antidyslipidemic + Anticholinergic + Anticholinergic | ||
| Rosuvastatin + Atropine +Tamsulosin | 1 | 5,56% |
| Hormone + Sedative + Bisphosphonate | ||
| Levothyroxine + Alprazolam + Alendronate Sodium | 1 | 5,56% |
| Hormone | ||
| Melatonin | 1 | 5,56% |
| Anti Dyspeptic + Anti-inflammatory | ||
| Omeprazole + Diclofenac Sodium + Paracetamol | 1 | 5,56% |
| Sedative | ||
| Clonazepam | 2 | 11,11% |
| Sedative + Antidepressants | ||
| Clonazepam + Escitalopram | 1 | 5,56% |
| TOTAL | 18 | 100% |
Table 3.
Effects of tDCS on motor symptoms.
| Wilcoxon Test (Baseline X Day 3) - UPDRS Motor Scale | ||||||||||
| Variable | Sham Group | |||||||||
| p-value | Mean_pre | Mean_post | SD_pre | SD_post | Median_pre | Median_post | IQR_pre | IQR_post | ||
| Speech | 1.000 | 0.78 | 0.78 | 0.83 | 0.83 | 1.0 | 1 | 1.00 | 1 | |
| Facial Expression | 0.317 | 0.89 | 0.89 | 0.93 | 0.93 | 1.0 | 1 | 2.00 | 2 | |
| Rest Tremor | Chin | 0.317 | 0.33 | 0.22 | 0.50 | 0.44 | 0.0 | 0 | 1.00 | 0 |
| Rul | 1.000 | 1.33 | 1.44 | 0.50 | 0.53 | 1.0 | 1 | 1.00 | 1 | |
| Lul | 0.564 | 0.89 | 0.89 | 0.78 | 0.93 | 1.0 | 1 | 1.00 | 2 | |
| Ril | 0.577 | 1.00 | 1.00 | 0.71 | 0.71 | 1.0 | 1 | 0.00 | 0 | |
| Lil | 1.000 | 0.89 | 0.78 | 0.78 | 0.67 | 1.0 | 1 | 1.00 | 1 | |
| Postural Tremor | Rul | 1.000 | 0.89 | 0.67 | 0.78 | 0.71 | 1.0 | 1 | 1.00 | 1 |
| Lul | 1.000 | 0.33 | 0.33 | 0.50 | 0.50 | 0.0 | 0 | 1.00 | 1 | |
| Rigidity | Cervical | 0.462 | 1.56 | 1.00 | 1.24 | 0.87 | 1.0 | 1 | 2.00 | 0 |
| Rul | 0.655 | 1.00 | 1.00 | 0.71 | 0.71 | 1.0 | 1 | 0.00 | 0 | |
| Lul | 0.655 | 0.89 | 0.89 | 1.05 | 1.05 | 1.0 | 1 | 1.00 | 1 | |
| Ril | 1.000 | 0.89 | 0.56 | 0.78 | 0.73 | 1.0 | 0 | 1.00 | 1 | |
| Lil | 0.317 | 0.89 | 0.89 | 0.93 | 0.93 | 1.0 | 1 | 2.00 | 2 | |
| Finger Tapping | Rul | 0.102 | 0.89 | 1.00 | 0.78 | 0.71 | 1.0 | 1 | 1.00 | 0 |
| Lul | 0.257 | 0.78 | 0.78 | 0.83 | 0.83 | 1.0 | 1 | 1.00 | 1 | |
| Hand Movement | Rul | 0.102 | 1.11 | 1.00 | 1.05 | 0.87 | 1.0 | 1 | 2.00 | 2 |
| Lul | 0.408 | 1.22 | 0.78 | 0.97 | 0.97 | 2.0 | 0 | 2.00 | 2 | |
| Pronation-Supination | Rul | 0.655 | 1.22 | 1.00 | 0.83 | 0.87 | 1.0 | 1 | 0.00 | 0 |
| Lul | 1.000 | 0.67 | 0.67 | 0.87 | 0.87 | 0.0 | 0 | 1.00 | 1 | |
| Toe Tapping | Ril | 0.705 | 1.33 | 0.89 | 1.00 | 0.93 | 1.0 | 1 | 1.00 | 2 |
| Ril | 0.655 | 0.89 | 0.78 | 0.93 | 0.97 | 1.0 | 0 | 2.00 | 2 | |
| Arising from chair | 0.317 | 1.00 | 0.89 | 0.87 | 0.60 | 1.0 | 1 | 2.00 | 0 | |
| Posture | 0.705 | 1.11 | 0.67 | 0.33 | 0.50 | 1.0 | 1 | 0.00 | 1 | |
| Gait | 0.257 | 1.00 | 0.56 | 0.87 | 0.88 | 1.0 | 0 | 2.00 | 1 | |
| Postural Stability | 0.317 | 1.33 | 1.11 | 0.50 | 0.78 | 1.0 | 1 | 1.00 | 1 | |
| Bradykinesia | 0.157 | 0.89 | 0.44 | 0.93 | 0.53 | 1.0 | 0 | 1.00 | 1 | |
p value <0.05. p value <0,05. Rul: Right upper limb; Lul: Left upper limb; Ril: Right inferior limb; Lil: Left inferior limb.
Table 4.
Effects of tDCS on motor symptoms.
| Wilcoxon Test (Baseline X Day 3) - UPDRS Motor Scale | ||||||||||
| Variable | Active Group | |||||||||
| p-value | Mean_pre | Mean_post | SD_pre | SD_post | Median_pre | Median_post | IQR_pre | IQR_post | ||
| Speech | 1.000 | 0.78 | 0.78 | 0.83 | 0.83 | 1.0 | 1.0 | 1.00 | 1.00 | |
| Facial Expression | 0.083 | 0.44 | 0.22 | 0.73 | 0.44 | 0.0 | 0.0 | 1.00 | 0.00 | |
| Rest Tremor | Chin | 1.000 | 0.44 | 0.33 | 0.53 | 0.50 | 0.0 | 0.0 | 1.00 | 1.00 |
| Rul | 0.655 | 0.89 | 0.89 | 0.60 | 0.60 | 1.0 | 1.0 | 0.00 | 0.00 | |
| Lul | 0.414 | 1.00 | 0.78 | 0.87 | 0.83 | 1.0 | 1.0 | 2.00 | 1.00 | |
| Ril | 0.655 | 1.22 | 1.22 | 0.83 | 0.83 | 1.0 | 1.0 | 1.00 | 1.00 | |
| Lil | 0.414 | 1.00 | 0.78 | 1.12 | 1.09 | 1.0 | 0.0 | 2.00 | 1.00 | |
| Postural Tremor | Rul | 0.564 | 1.00 | 1.00 | 1.00 | 1.00 | 1.0 | 1.0 | 1.00 | 1.00 |
| Lul | 0.102 | 0.89 | 0.89 | 0.33 | 0.33 | 1.0 | 1.0 | 0.00 | 0.00 | |
| Rigidity | Cervical | 0.564 | 0.78 | 0.78 | 1.09 | 0.83 | 0.0 | 1.0 | 1.00 | 1.00 |
| Rul | 0.414 | 0.89 | 1.00 | 0.78 | 0.87 | 1.0 | 1.0 | 1.00 | 2.00 | |
| Lul | 0.414 | 0.89 | 1.00 | 1.05 | 1.00 | 1.0 | 1.0 | 1.00 | 1.00 | |
| Ril | 0.564 | 0.67 | 0.78 | 0.71 | 0.67 | 1.0 | 1.0 | 1.00 | 1.00 | |
| Lil | 0.183 | 1.22 | 1.00 | 1.09 | 0.87 | 1.0 | 1.0 | 2.00 | 2.00 | |
| Finger Tapping | Rul | 0.038 | 0.56 | 0.67 | 0.88 | 1.00 | 0.0 | 0.0 | 1.00 | 2.00 |
| Lul | 0.713 | 1.00 | 1.89 | 1.00 | 3.48 | 1.0 | 1.0 | 1.00 | 1.00 | |
| Hand Movement | Rul | 0.046 | 0.78 | 0.78 | 0.97 | 0.97 | 0.0 | 0.0 | 2.00 | 2.00 |
| Lul | 0.157 | 1.33 | 1.11 | 1.00 | 0.60 | 1.0 | 1.0 | 1.00 | 0.00 | |
| Pronation-Supination | Rul | 0.655 | 0.89 | 0.89 | 0.93 | 0.93 | 1.0 | 1.0 | 2.00 | 2.00 |
| Lul | 0.481 | 1.00 | 0.89 | 0.50 | 0.33 | 1.0 | 1.0 | 0.00 | 0.00 | |
| Toe Tapping | Ril | 1.000 | 0.89 | 0.89 | 1.05 | 1.05 | 1.0 | 1.0 | 1.00 | 1.00 |
| Lui | 0.414 | 0.89 | 0.78 | 0.93 | 0.97 | 1.0 | 1.0 | 1.00 | 1.00 | |
| Arising from chair | 1.000 | 1.00 | 1.00 | 1.32 | 1.32 | 1.0 | 1.0 | 1.00 | 1.00 | |
| Posture | 0.034 | 1.44 | 0.78 | 1.01 | 0.83 | 2.0 | 1.0 | 1.00 | 1.00 | |
| Gait | 0.025 | 1.44 | 0.67 | 0.73 | 0.71 | 2.0 | 1.0 | 1.00 | 1.00 | |
| Postural Stability | 0.564 | 0.56 | 0.67 | 0.73 | 0.87 | 0.0 | 0.0 | 1.00 | 1.00 | |
| Bradykinesia | 0.655 | 1.00 | 1.00 | 0.71 | 0.71 | 1.0 | 1.0 | 0.00 | 0.00 | |
p value <0.05. p value <0,05. Rul: Right upper limb; Lul: Left upper limb; Ril: Right inferior limb; Lil: Left inferior limb.
Table 5.
Effects on mood.
| Wilcoxon Test (Baseline X Day 3) – HADS scale | |||||||||
| Variable | Sham Group | ||||||||
| p-value | Mean_pre | Mean_post | SD_pre | SD_post | Median_pre | Median_post | IQR_pre | IQR_post | |
| Anxiety subscale | |||||||||
| (1) I feel tense or “wound-up” | 0.257 | 1.33 | 1.00 | 0.87 | 0.50 | 1.0 | 1 | 1.00 | 0 |
| (3) I get a sort of frightened feeling as if something awful is about to happen | 1.000 | 0.78 | 0.78 | 0.83 | 0.83 | 1.0 | 1 | 1.00 | 1 |
| (5) Worrying thoughts go through my mind | 0.584 | 0.89 | 1.00 | 0.93 | 0.87 | 1.0 | 1 | 1.00 | 0 |
| (7) I can sit at ease and feel relaxed | 0.317 | 0.89 | 0.67 | 0.78 | 0.71 | 1.0 | 1 | 1.00 | 1 |
| (9) I get a sort of frightened feeling like “butterflies” in my stomach | 0,234 | 1.11 | 0.67 | 1.05 | 0.50 | 1.0 | 1 | 2.00 | 1 |
| (11) I feel restless as if I have to be on the move | 0.48 | 1.33 | 1.67 | 1.00 | 1.22 | 1.0 | 1 | 1.00 | 2 |
| (13) I get sudden feeling of panic | 0.879 | 0.78 | 0.33 | 1.09 | 0.50 | 0.0 | 0 | 1.00 | 1 |
| Depression subscale | |||||||||
| (2) I still enjoy the things I used to enjoy | 0.317 | 1.00 | 0.78 | 0.50 | 0.83 | 1.0 | 1 | 0.00 | 1 |
| (4) I can laugh and see the funny side of things | 0.59 | 0.67 | 1.22 | 0.71 | 0.67 | 1.0 | 1 | 1.00 | 1 |
| (6) I feel cheerful | 0.18 | 1.00 | 0.67 | 0.71 | 0.71 | 1.0 | 1 | 0.00 | 1 |
| (8) I fell as if I am slowed down | 0.141 | 1.78 | 2.00 | 0.83 | 1.00 | 2.0 | 2 | 1.00 | 1 |
| (10) I have lost interest in my appearance | 1.000 | 1.11 | 1.11 | 0.78 | 1.05 | 1.0 | 1 | 1.00 | 2 |
| (12) I look forward with enjoyment to things | 0.785 | 0.67 | 0.56 | 0.71 | 0.73 | 1.0 | 0 | 1.00 | 1 |
| (14) I can enjoy a good book or radio or a TV program | 0.705 | 1.00 | 1.00 | 1.12 | 0.87 | 1.0 | 1 | 2.00 | 2 |
p value <0.05.
Table 6.
Effects on mood.
| Wilcoxon Test (Baseline X Day 3) – HADS scale | |||||||||
| Variable | Active Group | ||||||||
| p-value | Mean_pre | Mean_post | SD_pre | SD_post | Median_pre | Median_post | IQR_pre | IQR_post | |
| Anxiety subscale | |||||||||
| (1) I feel tense or “wound-up” | 0.131 | 1.11 | 1.78 | 0.60 | 1.09 | 1.0 | 2.0 | 0.00 | 2.00 |
| (3) I get a sort of frightened feeling as if something awful is about to happen | 0.039 | 1.33 | 0.44 | 1.00 | 0.73 | 1.0 | 0.0 | 1.00 | 1.00 |
| (5) Worrying thoughts go through my mind | 0.157 | 0.67 | 0.44 | 0.87 | 0.73 | 0.0 | 0.0 | 1.00 | 1.00 |
| (7) I can sit at ease and feel relaxed | 0.257 | 0.89 | 0.56 | 0.78 | 0.53 | 1.0 | 1.0 | 1.00 | 1.00 |
| (9) I get a sort of frightened feeling like “butterflies” in my stomach | 0.234 | 0.44 | 0.44 | 0.53 | 0.73 | 0.0 | 0.0 | 1.00 | 1.00 |
| (11) I feel restless as if I have to be on the move | 0.48 | 0.56 | 0.56 | 0.73 | 1.01 | 0.0 | 0.0 | 1.00 | 1.00 |
| (13) I get sudden feeling of panic | 0.879 | 0.22 | 0.33 | 0.44 | 0.50 | 0.0 | 0.0 | 0.00 | 1.00 |
| Depression subscale | |||||||||
| (2) I still enjoy the things I used to enjoy | 0.141 | 0.67 | 0.44 | 1.00 | 0.53 | 0.0 | 0.0 | 1.00 | 1.00 |
| (4) I can laugh and see the funny side of things | 0.584 | 0.33 | 0.22 | 0.50 | 0.67 | 0.0 | 0.0 | 1.00 | 0.00 |
| (6) I feel cheerful | 1 | 0.33 | 0.33 | 0.50 | 0.50 | 0.0 | 0.0 | 1.00 | 1.00 |
| (8) I fell as if I am slowed down | 0.785 | 1.56 | 1.67 | 1.24 | 1.12 | 1.0 | 1.0 | 2.00 | 2.00 |
| (10) I have lost interest in my appearance | 0.257 | 0.67 | 0.33 | 0.71 | 0.50 | 1.0 | 0.0 | 1.00 | 1.00 |
| (12) I look forward with enjoyment to things | 0.102 | 1.00 | 1.00 | 1.12 | 1.12 | 1.0 | 1.0 | 2.00 | 2.00 |
| (14) I can enjoy a good book or radio or a TV program | 0.705 | 0.44 | 0.67 | 0.73 | 1.00 | 0.0 | 0.0 | 1.00 | 1.00 |
p value <0.05.
Table 7.
Effects of tDCS on cognition and executive functions.
| Wilcoxon Test (Baseline X Day 3) - PD-CRS Scale | |||||||||
| Variable | Sham Group | ||||||||
| p-value | Mean_pre | Mean_post | SD_pre | SD_post | Median_pre | Median_post | IQR_pre | IQR_post | |
| Frontal subcortical Tests | |||||||||
| (1) Immediate free recall verbal memory | 0.12 | 6.33 | 7.67 | 1.94 | 2.00 | 7.0 | 7 | 2.00 | 2 |
| (3) Sustained attention | 0.725 | 6.22 | 7.00 | 2.59 | 2.29 | 8.0 | 7 | 4.00 | 3 |
| (4) Working memory | 0.786 | 4.00 | 3.89 | 2.12 | 1.76 | 4.0 | 4 | 2.00 | 2 |
| (5) Unprompted drawing of a clock | 0.131 | 8.00 | 9.33 | 1.41 | 0.87 | 8.0 | 10 | 2.00 | 1 |
| (7) Delayed free recall verbal memory | 0.152 | 4.11 | 5.11 | 1.69 | 3.82 | 4.0 | 5 | 2.00 | 5 |
| (8) Alternating verbal fluency | 0.832 | 4.78 | 5.11 | 1.56 | 1.90 | 5.0 | 5 | 2.00 | 4 |
| (9) Action verbal fluency | 0.135 | 9.11 | 9.11 | 3.18 | 2.42 | 8.0 | 9 | 4.00 | 3 |
| Cortical Tests | |||||||||
| (2) Confrontation naming | 0.246 | 11.11 | 13.33 | 4.46 | 4.66 | 13.0 | 14 | 5.00 | 2 |
| (6) Copy drawing of a clock | 0.102 | 8.33 | 9.44 | 1.58 | 0.73 | 9.0 | 10 | 1.00 | 1 |
p value <0,05.
Table 8.
Effects of tDCS on cognition.
| Wilcoxon Test (Baseline X Day 3) - PD-CRS Scale | |||||||||
| Variable | Active Group | ||||||||
| p-value | Mean_pre | Mean_post | SD_pre | SD_post | Median_pre | Median_post | IQR_pre | IQR_post | |
| Fronto-subcortical Tests | |||||||||
| (1) Immediate free recall verbal memory | 0.016 | 7.56 | 8.67 | 2.01 | 2.00 | 7.0 | 8.0 | 2.00 | 2.00 |
| (3) Sustained attention | 0.12 | 7.44 | 8.67 | 2.01 | 1.58 | 8.0 | 9.0 | 3.00 | 1.00 |
| (4) Working memory | 0.433 | 5.44 | 6.00 | 1.94 | 1.12 | 6.0 | 6.0 | 2.00 | 0.00 |
| (5) Unprompted drawing of a clock | 0.126 | 9.11 | 9.67 | 1.36 | 0.50 | 10.0 | 10.0 | 2.00 | 1.00 |
| (7) Delayed free recall verbal memory | 0.235 | 3.78 | 5.11 | 2.73 | 1.83 | 3.0 | 4.0 | 4.00 | 2.00 |
| (8) Alternating verbal fluency | 0.322 | 6.22 | 6.33 | 2.17 | 1.58 | 5.0 | 7.0 | 4.00 | 2.00 |
| (9) Action verbal fluency | 0.018 | 14.22 | 17.22 | 5.78 | 5.85 | 14.0 | 20.0 | 8.00 | 7.00 |
| Cortical Tests | |||||||||
| (2) Confrontation naming | 0.011 | 14.22 | 14.89 | 5.04 | 4.51 | 16.0 | 17.0 | 9.00 | 8.00 |
| (6) Copy drawing of a clock | 0.024 | 9.44 | 10.00 | 0.88 | 0.00 | 10.0 | 10.0 | 1.00 | 0.00 |
p value <0.05.
Table 9.
Effects of tDCS on executive functions.
| Wilcoxon Test (Baseline X Day 3) – Stroop Test | |||||||||
| Variable | Sham Group | ||||||||
| p-value | Mean_pre | Mean_post | SD_pre | SD_post | Median_pre | Median_post | IQR_pre | IQR_post | |
| (1) Right answer | 0.041 | 6.11 | 7.22 | 3.06 | 3.60 | 5.0 | 6 | 6.00 | 6 |
| (2) Error | 0.82 | 6.11 | 5.33 | 2.20 | 3.08 | 7.0 | 6 | 3.00 | 5 |
| (3) Omission | 1 | 3.78 | 3.44 | 1.72 | 2.24 | 4.0 | 3 | 2.00 | 3 |
p value <0.05.
Table 10.
Effects of tDCS on executive functions.
| Wilcoxon Test (Baseline X Day 3) – Stroop Test | |||||||||
| Varible | Active Group | ||||||||
| p-value | Mean_pre | Mean_post | SD_pre | SD_post | Median_pre | Median_post | IQR_pre | IQR_post | |
| (1) Right answer | 0.018 | 8.78 | 12.22 | 2.82 | 3.99 | 9.0 | 14.0 | 4.00 | 3.00 |
| (2) Error | 0.076 | 5.22 | 2.22 | 2.64 | 3.35 | 6.0 | 1.0 | 1.00 | 1.00 |
| (3) Omission | 0.087 | 1.89 | 1.56 | 1.76 | 1.88 | 1.0 | 1.0 | 2.00 | 2.00 |
* p value <0,05.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



