
Submitted:
11 September 2023
Posted:
12 September 2023
You are already at the latest version
Abstract
The definition of Early Cholecystectomy (EC) is still debatable. This paper aims to find whether the timing of EC affects outcomes. This is a multicentric prospective observational study including patients with acute calculous cholecystitis (ACC) who had cholecystectomy within ten days from the onset of symptoms. Kruskall-Wallis test, Fisher’s Exact test and Spearman rank correlation were used for statistical analysis. The patients were divided into three groups depending on the timing of the operation: 0-3 days, 4-7 days, or 8-10 days from the onset of symptoms. 1117 patients were studied over a year. The time from the onset of symptoms to EC did not affect the postoperative complications and mortality, the conversion and the reintervention rate. It was a significant risk factor for intraoperative complications (0-3 days, 2.8%; 4-7 days, 5.6%; 8-10 days, 7.9%; p=0.01) and subtotal cholecystectomies (0-3 days, 2.7%; 4-7 days, 5.6%; 8-10 days, 10.9%; p<0.001). ACC is an evolutive inflammatory process and, as the days go by, the local and systemic inflammation increases which makes surgery more complex and difficult with higher risk of intraoperative complications. We recommend performing EC for ACC as soon as possible within the first ten days of the onset of symptoms.
Keywords:
acute cholecystitis
; cholecystectomy
; surgery
; timing
; complication
; mortality
1. Introduction
Early cholecystectomy (EC) represents the gold standard for treating acute calculous cholecystitis (ACC) [1,2]. It is superior to both intermediate cholecystectomy (performed between 7 days and 6 weeks of hospital admission) and delayed cholecystectomy (performed between 6 weeks and 3 months from hospital admission) [1]. EC has shorter total hospital stay and lower cost, but longer operative time [3,4].
However, the definition of EC is still debatable without available definitive data. The World Society of Emergency Surgery (WSES) guidelines defined “early cholecystectomy” when performed within 7 days of hospital admission and within 10 days of the onset of symptoms [1]. The Japanese guidelines defined EC when performed as soon as possible, preferably within 72 hours from the onset of symptoms, but even after this time [2].
Multiple studies and meta-analyses comparing different timing of EC revealed no significant association between timing of operation and postoperative mortality or morbidity [4,5,6,7], but longer post-operative LOS in the group of patients with longer times from admission to surgery [5,8]. On the other hand, a large retrospective observational study [9] including 43870 patients in England who underwent emergency cholecystectomy on index admission showed a significantly lower biliary complication rate in patients undergoing cholecystectomy within 3 days of admission. Another retrospective study [10] including 34151 cholecystectomies for ACC showed that operations performed on hospital days 3-7 had increased 30-day mortality and morbidity in comparison to hospital day 1 or hospital day 2. On multivariable analysis, the number of days from admission to EC was an independent predictor of mortality.
Focusing on the conversion rate, some observational studies [5] showed that patients who underwent operation later in the course of admission were more likely to require an open procedure. Other studies [8,11] did not find difference in the conversion rate, but an increasing rate of difficult surgical procedures and an increasing operative time. A recent meta-analysis has found that cholecystectomy which was performed within 24 h of admission has not reduced the post-operative complications [7], but has reduced LOS. Many of these studies are not comparable because they consider different time intervals. A recent meta-analysis has shown that cholecystectomies performed within 72 h of symptoms have reduced conversion rate and LOS in comparison to cholecystectomy ≤7 days [4,7]. No differences in complication rate and bile duct injuries have been found [4]. There are three RCTs [12,13,14] and other prospective non-randomized studies [6,11] which compare different timings of EC from the onset of symptoms. Three RCTs randomized patients with ACC to receive EC within 72 hours or after 4-7 days from the onset of symptoms. In these studies no differences in postoperative complication rate and conversion rate were found, but patients who received EC within 72 hours had significantly shorter postoperative LOS. In the studies by Chandler et al. [12] and by Onuk et al. [13] there was no difference in the duration of the surgery, while in the study by Jan et al. [14] the operative time was longer in patients who were operated on after 72h. Furthermore, Jan et al. [14] did not find significant difference in intraoperative complications, while Chandler et al. [12] found significantly greater blood loss in those operated on after 72h. However, none of the RCTs and the prospective non-randomized studies had enough powered sample size. The only study that reported data about sample size calculation [13], had a power of 34%. A Cochrane systematic review [15] highlighted the difficulty of obtaining sufficient data on this topic through RCTs because studies with enough power would involve thousands of patients.
Accordingly, there is lack of high-quality and properly powered studies that stratify the intra and post-operative risks of EC based on the delay of surgery from the onset of symptoms, especially when considering an inclusive time of 10 days from the onset of symptoms. The validation and comparison of Scores for Prediction of Risk for post-operative major Morbidity after cholecystectomy in Acute Calculous Cholecystitis (S.P.Ri.M.A.C.C.) study was conceived as a WSES prospective multicentre observational study on patients with ACC who are candidates for EC aiming to validate different scores in predicting postoperative complications [16]. This current paper is a posthoc analysis of the S.P.Ri.M.A.C.C study aiming to define the effects of different timings of EC (within 10 days from the onset of symptoms) on intra and postoperative outcomes.
2. Materials and Methods
2.1. Ethical considerations
The medical ethics board of the trial coordinating centre IRCCS San Matteo Hospital, Pavia, Italy, approved the S.P.Ri.M.A.C.C. study protocol. All regional ethics committees of the participating centres provided secondary approval. Before enrollment, patients provided both verbal and written informed consent. The S.P.Ri.M.A.C.C. trial was carried out in line with the Helsinki Declaration.
2.2. Design
The S.P.Ri.M.A.C.C. study is an observational multicenter prospective study endorsed by the WSES. 1253 patients from 79 locations in 19 nations were enrolled between September 1, 2021, and September 1, 2022. The study was listed in LegalTrial.gov under case number NCT04995380. 1117 participants were included in the study after patients with incomplete information regarding the timing of EC were excluded. Within 10 days after the onset of symptoms, EC was administered to all patients. The goal of the study was to determine whether there was a statistically significant difference in the rate of intraoperative complications between individuals who underwent surgery at various times after the onset of their symptoms (0-3 days, 4-7 days, 8-10 days).
2.3. Studied variables
The intraoperative complication rate was the primary objective. It included haemorrhage above 500 mL, biliary tree injuries, bowel perforation, major vascular injuries, general anaesthetic respiratory complications, and general anaesthesia cardiac issues. The secondary endpoints were represented by the rate of conversion from laparoscopic to laparotomy, the rate of needing bailout procedures (subtotal cholecystectomy, fundus-first cholecystectomy, laparoscopic drainage only), the operative time, the in-hospital postoperative major complications (defined as complications with Common Terminology Criteria for Adverse Event, CTCAE 3), the 30-day postoperative major complications (CTCAE 3), the post-operative length of stay (LOS), the in-hospital mortality, and the 30-day mortality.
2.4. Inclusion and exclusion criteria
The following criteria had to be met for a patient to be included: 1) have a diagnosis of ACC according to the 2018 Tokyo Guidelines; 2) be a candidate for EC during the index admission; 3) be older than 18 years of age; 4) be stratified for the risk of common bile duct stones and, in case of confirmation, receive preoperative ERCP 5) sign a written informed consent form, inclusive of the date and 6) be willing to comply with all study protocol rules and be available for the duration of the investigation.
Pregnancy or lactation, acute cholecystitis unrelated to a gallstone cause, symptoms appearing more than 10 days before cholecystectomy, concurrent cholangitis or pancreatitis, intraoperative treatment of common bile duct stones, or anything else that would prevent full compliance with or completion of the study were the exclusion criteria.
2.5. Statistical analysis
Sample size: for the sample size calculation, the investigators grounded on the RCT by Jan et al. (14) in which patients with ACC were randomized to receive EC within 72h from the onset of symptoms (group 1) or after 72h up to 7 days from the onset of symptoms (group 2). In the study, the intraoperative complication rate in group 1 was 2%, while in group 2 was 6%. 1,000 patients are required to have a 90% chance of detecting, as significant at the 5% level, an increase in the primary outcome measure. The patients were divided into three different groups depending on the time from onset of symptoms: group I from 0-3 days, Group II from 4-7 days, and Group III from 8-10 days.
Variables comparison: The three groups were compared using the Kruskall-Wallis test for continuous or ordinal data and Fisher’s Exact test for categorical data. Spearman rank correlation was used to study the correlation between the continuous or ordinal data. A P value of less than 0.05 was accepted as significant. SPSS version 26 was used for comparison.
3. Results
58.7% of patients received EC within 3 days, 32.2% from 4 to 7 days and 9.0% from 8 to 10 days from the onset of symptoms. The mean age was 59 and the mean POSSUM (Physiological and Operative Severity Score for the enUmeration of Mortality and morbidity) Physiological score (PS) was 20.7. The intraoperative complication rate was 4.1%. The most frequent complication was intraoperative bleeding >500ml (16 patients). Other intraoperative complications were biliary tree injuries (8 patients), bowel perforation (1 patient), respiratory complications (3 patients), cardiac complications (3 patients) and others (16 patients). 8.4% of patients needed a bail-out procedure (49 subtotal cholecystectomies, 65 patients treated with a fundus-first technique and 1 patient received only laparoscopic drainage). Preoperative characteristics of the three groups of patients are reported in Table 1. Patients were similar in terms of age and BMI. Patients operated after 8-10 days from the onset had a significantly higher POSSUM PS (median (IQR): 0-3 days, 19 (15-24); 4-7 days, 19 (16-24); 8-10 days, 21 (17-26); p=0.012). Patients operated on within 3 days from onset of symptoms had lower ACC severity grades (mean (SD): 1.6 (0.5) for 0-3 days, 1.8 (0.4) for 4-7 days, 1.7 (0.5) for 8-10 days; p=0.012).
Table 2 shows intraoperative outcomes. A higher number of days from the onset of symptoms to EC was a significant risk factor for longer operative times (median (IQR): 0-3 days, 90 (60-120) minutes; 4-7 days, 100 (65-134.5) minutes; 8-10 days, 107 (74-145) minutes; p<0.001), for needing of bail-out procedures (0-3 days, 6.9%; 4-7 days, 9.7%; 8-10 days, 13.9%; p=0.037) and for intraoperative complications (0-3 days, 2.8%; 4-7 days, 5.6%; 8-10 days, 7.9%; p=0.01). Analyzing the kind of bail-out procedures, the rate of subtotal cholecystectomies significantly increased with the increase of days from onset (0-3 days, 2.7%; 4-7 days, 5.6%; 8-10 days, 10.9%; p<0.001). Figure 1 shows the box-and-whisker plot of the operative time by the time between the onset of symptoms and surgery. The time interval from the onset to EC did not affect the conversion rate to open surgery.
Table 3 shows postoperative outcomes. A higher number of days from the onset of symptoms to EC was a significant risk factor for a longer LOS (median (IQR) LOS: 0-3 days, 3 (2-5) days; 4-7 days, 5 (3-7) days; 8-10 days, 8 (3-11) days; p<0.001; patients with a LOS longer than 10 days: 0-3 days, 6.67%; 4-7 days, 10.6%; 8-10 days, 24.8%; p<0.001) (Figure 2). The time from the onset to EC did not affect the reintervention rate, the postoperative complications and mortality.
There was a statistically significant, small positive correlation between days from onset of symptoms and LOS (r=0.26, p<0.001), POSSUM PS (r= 0.01, p<0.001) and operative time (r=0.14, p<0.001) (Table 4).
4. Discussion
The present study is the first prospective study of our knowledge focusing on the ideal timing of EC with a sample size calculated on a high study power. These data showed that the risk of intraoperative complications, the risk of needing a bail-out procedure (e.g., subtotal cholecystectomy), the operative time and, to a lesser degree, the LOS increase for each time interval (0-3 days, 4-7 days, 8-10 days) from the onset of symptoms to EC. The evolution of the inflammatory process, with the passage of days, makes it more difficult to dissect tissues, recognize structures and increases the tendency to bleed. The ACC severity grade and the POSSUM PS rise with the passing of days, due to the exacerbation of the local and systemic inflammation. Despite the greater difficulty of the intervention, the delay in performing EC, if within 10 days from the onset of symptoms, did not affect post-operative complications, postoperative mortality, risk of conversion to open surgery and need for reintervention.
The definition of EC in terms of timing is still debatable [4,5,6,7,8,9,10,11]. Most of the existing studies are unpowered or they are not comparable because they consider different timing definitions. Some consider the time interval from the onset of symptoms while others from hospitalization. Patients can go to the emergency department after very different intervals of time from the onset of symptoms, and then at different stages of the disease. This may depend on age, comorbidities, geographic location, pain tolerance and social class. This can lead to poor population uniformity when the timing is based on the time of admission. Basing the timing on the onset of symptoms allows to create more homogeneous patient groups for the stage of disease and the surgical risk.
Compared with other surgical urgencies, physicians often procrastinate cholecystectomy for ACC. Hospitals and community care often fail to ensure patients with ACC an ideal timing for surgery. General practitioners, emergency doctors and surgeons often try to treat ACC medically before considering surgery. This, combined with the organizational issues of operating rooms, increases the time between the onset of symptoms and EC. It worsens the general and local inflammatory condition, increases the surgical complexity and rises the risk of intraoperative complications.
The time between the onset of symptoms and the presentation of the patient in the emergency department does not depend on the physician. However, the physician, considering the organizational issues within the health care system and availability of the operating rooms, should do everything possible to ensure a patient with ACC has a cholecystectomy performed as early as possible.
Probably a proper surgeon-patient and surgeon-general practitioner knowledge translation could shorten the time between the onset of symptoms and emergency department presentation. Surgeons should recommend symptomatic patients with cholelithiasis during outpatient visits to go to the hospital as soon as possible. Furthermore, the time between the arrival in the emergency room and the surgical visit should be optimized. Clinical examination, blood tests and ultrasound are usually sufficient to diagnose ACC. Emergency doctors should not delay the management by performing uneeded examinations or attempts for medical therapy when there is clear indication for surgery.
Main bile duct stones associated with ACC often delay EC because of the need for MRCP or ERCP to have a clear management plan. Probably, a single-stage intraoperative ERCP or a laparoscopic cholangioscopy combined with laparoscopic cholecystectomy will reduce the time for EC [17].
Our study has some limitations. It is a non-randomized study with possible confounding factors. However, given the large sample size required, it would be difficult to carry out a RCT on this topic. Furthermore, we were interested in the generalizability of the study which will contain more heterogeinity in the data. This included some developing countries with lack of training in research methodology including performing RCTs. To our knowledge, the prospective nature and the large sample size of our study, despite being type II research data, provide the highest quality data available in the literature. An adequate RCT would be possible only through a multicenter study with a high degree of organization and international cooperation.
5. Conclusions
In conclusion, considering that EC is superior to delayed and interval cholecystectomy [1,3,4], this study clarifies the best timing of EC. Our study has shown that delaying EC up to ten days from the onset of symptoms does not affect postoperative complications and mortality. However, ACC is an evolutive inflammatory process and, as the days go by, the local and systemic inflammation increases which makes surgery more complex and difficult with higher risk of intraoperative complications. We recommend performing EC for ACC as soon as possible within the first ten days of the onset of symptoms6.
Author Contributions
LA: PF: study conception; PF, LA, LC, FDM, FMAZ, MC: manuscript conception and draft and contribute to important scientific knowledge; FMAZ statistical analysis of the data. PF, LC, FDM, FMAZ, MT, MC, FC, TD, CNF, SF, VM, BS, JV, FC, LA gave substantial contributions to the interpretation of data for the work and critically revised the manuscript; PF, MT and S.P.Ri.M.A.C.C. Collaborative Group: substantial contributions to the acquisition of data and draft critically revised. All authors gave the final approval and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by Medical Ethics Board of the trial coordinating centre IRCCS San Matteo Hospital, Pavia, Italy (protocol code P20210050641, date of approval 04/06/2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
S.P.Ri.M.A.C.C. Collaborative Group: Goran Augustin (1), Trpimir Morić (1), Selmy Awad (2), Azzah M Alzahrani (2), Mohamed Elbahnasawy (3), Damien Massalou (4), Belinda De Simone (5), Zaza Demetrashvili (6), Athina-Despoina Kimpizi (7), Dimitrios Schizas (8), Dimitrios Balalis (9), Nikolaos Tasis (10), Maria Papadoliopoulou (11), Petrakis Georgios (12), Konstantinos Lasithiotakis (13), Orestis Ioannidis (14), Lovenish Bains (15), Matteo Magnoli (16), Pasquale Cianci (17), Nunzia Ivana Conversano (17), Alessandro Pasculli (18), Jacopo Andreuccetti (19), Elisa Arici (19), Giusto Pignata (19), Guido A.M. Tiberio (20), Mauro Podda (21), Cristina Murru (22), Massimiliano Veroux (23),Costanza Distefano (23), Danilo Centonze (23), Francesco Favi (24), Raffaele Bova (24), Girolamo Convertini (24), Vanni Agnoletti (24), Andrea Balla (25), Diego Sasia (26), Giorgio Giraudo (26), Anania Gabriele (27), Nicola Tartaglia (28), Giovanna Pavone (28), Fabrizio D’Acapito (29), Nicolò Fabbri (30), Francesco Ferrara (31), Stefania Cimbanassi (32), Luca Ferrario (32), Stefano Cioffi (32), Marco Ceresoli (33), Chiara Fumagalli (33), Luca Degrate (33), Maurizio Degiuli (34), Silvia Sofia (34), Leo Licari (35), Andrea Anderloni (36), Tommaso Dominioni (36), Jacopo Viganò (36), Marcello Maestri (36), Camilla Nikita Farè (36), Benedetta Sargenti (36), Mario Improta (36), Valeria Musella (36), Giulia Gambini (36), Alberto Patriti (37),Diego Coletta (37), Luigi Conti (38), Michele Malerba (39), Muratore Andrea (40), Marcello Calabrò (40), Beatrice De Zolt (40), Gabriele Bellio (41), Alessio Giordano (42), Davide Luppi (43), Carlo Corbellini (44),Gianluca Matteo Sampietro (44), Chiara Marafante (45), Stefano Rossi (46), Andrea Mingoli (47), Pierfrancesco Lapolla (47), Pierfranco M Cicerchia (47), Leandro Siragusa (48), Michele Grande (48), Claudio Arcudi (49), Amedeo Antonelli (49), Danilo Vinci (49), Ciro De Martino (50), Mariano Fortunato Armellino (50), Enrica Bisogno (50), Diego Visconti (51), Mauro Santarelli (51), Elena Montanari (51), Alan Biloslavo (52), Paola Germani (52), Claudia Zaghi (53), Naoki Oka (54), Mohd Azem Fathi (55), Daniel Ríos-Cruz (56), Edgard Efren Lozada Hernandez (57), Ibrahim Umar Garzali (58), Liliana Duarte (59), Ionut Negoi (60), Andrey Litvin (61), Sharfuddin Chowdhury (62), Salem M. Alshahrani (62), Silvia Carbonell-Morote (63), Juan J. Rubio-Garcia (63), Claudia Cristina Lopes Moreira (64), Iñigo Augusto Ponce (64), Fernando Mendoza-Moreno (65), Anna Muñoz Campaña (66), Heura Llaquet Bayo (66), Andrea Campos Serra (66), Begoña Estraviz-Mateos (67), Izaskun Markinez-Gordobil (67), Aitor Landaluce-Olavarria (67), Mario Serradilla-Martín (68), Antonio Cano-Paredero (68), Miguel Ángel Dobón-Rascón (68), Hytham Hamid (69), Oussama Baraket (70), Emre Gonullu (71), Sezai Leventoglu (72), Yilmaz Turk (72), Çağrı Büyükkasap (72), Ulaş Aday (73), Yasin Kara (74), Hamit Ahmet Kabuli (75), Semra Demirli Atici (76), Elif Colak (77), Serge Chooklin (78), Serhii Chuklin (78), Elena Martín-Pérez (79), Ángela de la Hoz Rodríguez (79), Marcello Di Martino (80), Salomone Di Saverio (81), Ari Leppäniemi (82), Ernest E. Moore (83), Andrew B. Peitzman (84), Massimo Sartelli (85), Walter Biffl (86).
(1) Department of Surgery, University Hospital Centre Zagreb, Zagreb, Croatia
(2) Department of General Surgery, Mansoura University Hospitals, Mansoura, Egypt
(3) University Faculty of Medicine, Tanta, Egypt
(4) Acute care surgery, CHU de Nice, Nice, France
(5) Dpt of Emergency, Digestive and Metabolic Minimally invasive surgery, Poissy and Saint Germain en Laye Hospitals, Poissy, France
(6) State Medical University, Tbilisi, Georgia
(7) Hippocration General Hospital of Athens, Athens, Greece
(8) National and Kapodistrian University of Athens, Laikon General Hospital, Athens, Greece
(9) Saint Savvas Cancer Hospital, Athens, Greece
(10) Naval and Veterans Hospital, Department of Surgery, Athens, Greece
(11) University General Hospital Attikon-UoA, Chaidari, Greece
(12) Surgery Department, General Hospital of Chania - Saint George, Crete, Greece
(13) Surgery University Hospital of Heraklion, Medical School of Heraklion, Crete, Greece
(14) General Hospital George Papanikolaou, Thessaloniki, Greece
(15) Maulana Azad Medical College, New Delhi, India
(16) Chirurgia generale, Ospedale Monsignor Galliano, Acqui terme, Italy
(17) Lorenzo Bonomo Hospital, Andria, Italy
(18) University of Bari, Bari, Italy
(19) Chirurgia 2, ASST Spedali Civili of Brescia, Brescia, Italy
(20) Surgical Clinic, University of Brescia, Brescia, Italy
(21) Department of Surgical Science, University of Cagliari, Cagliari, Italy
(22) PO Santissima Trinità, Cagliari, Italy
(23) Azienda Policlinico Università di Catania, Catania, Italy
(24) Bufalini Hospital, Cesena, italy
(25) UOC of General and Minimally Invasive Surgery, San Paolo Hospital, Civitavecchia, Italy
(26) Azienda Ospedaliera Santa Croce e Carle, Cuneo, Italy
(27) Azienda Ospedaliero-Universitaria di Ferrara, Arcispedale Sant’Anna, Ferrara, Italy
(28) University Hospital, Foggia, Italy
(29) Ospedale Morgagni Pierantoni, Forlì, Italy
(30) Ospedale del Delta, Lagosanto, italy
(31) ASST Santi Paolo e Carlo, Milano, Italy
(32) Chirurgia generale Trauma team, Ospedale Niguarda, Milano, Italy
(33) General and Emergency Surgery, School of Medicine and Surgery, Milano-Bicocca University, Monza, Italy
(34) Surgical oncology and digestive surgery, A.O.U. San Luigi Gonzaga, Orbassano, Italy
(35) FBF Buccheri La Ferla, Palermo, Italy
(36) Fondazione IRCCS Policlinico San Matteo, Pavia, Italy
(37) AO Ospedali Riuniti Marche Nord, Pesaro, Italy
(38) G, Da Saliceto Hospital, Piacenza, Italy
(39) ASL2 Savonese, Pietra Ligure, Italy
(40) Chirurgia generale Ospedale E. Agnelli, Pinerolo, Italy
(41) Ospedale Immacolata Concezione, Piove di Sacco, Italy
(42) “S.Stefano” New Hospital, Prato, Italy
(43) ASMN, Reggio Emilia, Italy
(44) Ospedale di Rho - ASST Rhodense, Rho, Italy
(45) Chirurgia Generale Ospedale degli Infermi, Rivoli, Italy
(46) San Filippo Neri Hospital, Roma, Italy
(47) Policlinico Umberto I Sapienza, Roma, Italy
(48) University Tor Vergata, Roma, Italy
(49) UOC Chirurgia Bariatrica, Ospedale San Carlo di Nancy, Roma, Italy
(50) University Hospital “S. Giovanni di Dio e Ruggi d’Aragona”, Salerno, Italy
(51) Chirurgia Generale d’Urgenza e PS, AOU Città della Salute e della Scienza, Torino, Italy
(52) General Surgery Department, Cattinara University Hospital, ASUGI, Trieste, Italy
(53) Ospedale San Bortolo, Vicenza, Italy
(54) Kurashiki Central Hospital, Kurashiki, Japan
(55) Department of Surgery, Hospital Universiti Sains Malaysia, Kota Bharu, Malaysia
(56) Instituto Mexicano del seguro social, Ciudad de México, Mexico
(57) Regional Hospital of High Speciality of Bajio, Leon Guanajuato, Mexico
(58) Aminu Kano Teaching Hospital, Kano, Nigeria
(59) Centro Hospitalar Tondela-Viseu, Viseu, Portugal
(60) Emergency Hospital of Bucharest, Bucharest, Romania
(61) Immanuel Kant Baltic Federal University, Regional Clinic Hospital, Kaliningrad, Russia
(62) General Surgery, King Saud Medical City, Riyadh, Saudi Arabia
(63) Department of Surgery and Liver Transplantation. Hospital General Universitario Dr. Balmis, Alicante, Spain
(64) Hospital universitario Donostia, Donostia-San Sebastian, Spain
(65) Hospital Universitario Príncipe de Asturias, Madrid, Spain
(66) Emergency Surgery Unit, Parc Tauli Hospital, Sabadell, Spain
(67) Urduliz Hospital, Urduliz, Spain
(68) Department of Surgery, Miguel Servet University Hospital, Zaragoza, Spain
(69) Kuwaiti Specialized Hospital, Khartoum, Sudan
(70) Bizerte hospital, Bizerte, Tunis
(71) Sakarya Training and Research Hospital, Adapazari/Sakarya, Turkey
(72) Gazi University, School of Medicine, Department of Surgery, Ankara, Turkey
(73) Department of Gastroenterological Surgery, Dicle University School of Medicine, Diyarbakir, Turkey
(74) Kanuni Sultan Süleyman Training and Research Hospital, Instanbul, Turkey
(75) Bakirkoy Dr Sadi Konuk Training and Research Hospital, Instanbul, Turkey
(76) Tepecik Training and Research Hospital, Konak/İzmir, Turkey
(77) Samsun Training and Research Hospital, Samsun, Turkey
(78) Regional Clinical hospital, Lviv, Ukraine
(79) Department of General and Digestive Surgery, Hospital Universitario La Princesa, Instituto de Investigación Sanitaria Princesa (IIS-IP), Universidad Autónoma de Madrid (UAM), Madrid, Spain
(80) Hepato-Biliary and Liver Transplantation Department, AORN Cardarelli, Napoli
(81) Department of Surgery, Madonna Del Soccorso Hospital, San Benedetto del Tronto, Italy
(82) Abdominal Center, Helsinki University Hospital and University of Helsinki, Helsinki, Finland
(83) Denver Health System - Denver Health Medical Center, Denver, USA
(84) Department of Surgery, University of Pittsburgh School of Medicine, UPMC-Presbyterian, Pittsburgh, USA
(85) Department of Surgery, Macerata Hospital, 62100 Macerata, Italy
(86) Division of Trauma/Acute Care Surgery, Scripps Clinic Medical Group, La Jolla, CA, USA
Conflicts of Interest
The authors declare no conflict of interest.
References
- Pisano M, Allievi N, Gurusamy K, Borzellino G, Cimbanassi S, Boerna D, et al. 2020 World Society of Emergency Surgery updated guidelines for the diagnosis and treatment of acute calculus cholecystitis. World J Emerg Surg. 2020, 15, 1–26. [Google Scholar]
- Wakabayashi G, Iwashita Y, Hibi T, Takada T, Strasberg SM, Asbun HJ, et al. Tokyo Guidelines 2018: surgical management of acute cholecystitis: safe steps in laparoscopic cholecystectomy for acute cholecystitis (with videos). J Hepatobiliary Pancreat Sci. 2018, 25, 73–86. [Google Scholar] [CrossRef] [PubMed]
- De, U. Evolution of cholecystectomy: A tribute to Carl August Langenbuch. Indian J Surg. 2004, 66, 97–100. [Google Scholar]
- Coccolini F, Solaini L, Binda C, Catena F, Chiarugi M, Fabbri C, et al. Laparoscopic Cholecystectomy in Acute Cholecystitis: Refining the Best Surgical Timing Through Network Meta-Analysis of Randomized Trials. Surg Laparosc Endosc Percutan Tech. 2022, 32, 755–763. [Google Scholar] [CrossRef] [PubMed]
- Brooks K, Scarborough J, Vaslef S, Shapiro M. No need to wait: An analysis of the timing of cholecystectomy during admission for acute cholecystitis using the American College of Surgeons National Surgical Quality Improvement Program database. J Trauma Acute Care Surg. 2012, 74. [Google Scholar]
- Tzovaras G, Zacharoulis D, Liakou P, Theodoropoulos T, Paroutoglou G, Hatzitheofilou C. Timing of laparoscopic cholecystectomy for acute cholecystitis: A prospective non randomized study. World J Gastroenterol. 2006, 12, 5528–5531. [Google Scholar] [CrossRef] [PubMed]
- Borzellino G, Khuri S, Pisano M, Mansour S, Allievi N, Ansaloni L, et al. Timing of early laparoscopic cholecystectomy for acute calculous cholecystitis: a meta-analysis of randomized clinical trials. World J Emerg Surg. 2021, 16, 1–12. [Google Scholar]
- Al-Mulhim, AA. Timing of early laparoscopic cholecystectomy for acute cholecystitis. J Soc Laparoendosc Surg. 2008, 12, 282–287. [Google Scholar]
- Wiggins T, Markar SR, MacKenzie H, Faiz O, Mukherjee D, Khoo DE, et al. Optimum timing of emergency cholecystectomy for acute cholecystitis in England: population-based cohort study. Surg Endosc [Internet]. 2019, 33, 2495–2502. [Google Scholar] [CrossRef] [PubMed]
- Alore EA, Ward JL, Todd SR, Wilson CT, Gordy SD, Hoffman MK, et al. Ideal timing of early cholecystectomy for acute cholecystitis: An ACS-NSQIP review. Am J Surg [Internet]. 2019, 218, 1084–1089. [Google Scholar] [CrossRef] [PubMed]
- Brunée L, Hauters P, Closset J, Fromont G, Puia-Negelescu S. Assessment of the optimal timing for early laparoscopic cholecystectomy in acute cholecystitis: a prospective study of the Club Coelio. Acta Chir Belg [Internet]. 2019, 119, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Chandler CF, Lane JS, Ferguson P, Thompson JE, Ashley SW. Prospective evaluation of early versus delayed laparoscopic cholecystectomy for treatment of acute cholecystitis. Am Surg. 2000, 66, 896–900. [Google Scholar] [CrossRef]
- Arslan onuk zinet asuman. The timing of laparoscopic cholecystectomy in acute cholecystitis: importance of first 72 hours and oxidative stress markers. Turkish J Trauma Emerg Surg. 2019, 25, 440–446. [Google Scholar]
- Jan Y, Shah M, Hussain S, Din W, Khan A. Variables affecting outcome of laparoscopic cholecystectomy in acute cholecystitis. Pak J Surg. 2016, 32, 16–21. [Google Scholar]
- Gurusamy KS, Davidson C, Gluud C, Davidson B. Early versus delayed laparoscopic cholecystectomy for people with acute cholecystitis (Review). Cochrane Database Syst Rev. 2013;(6).
- Fugazzola P, Cobianchi L, Di Martino M, Tomasoni M, Dal Mas F, Abu-Zidan FM, Agnoletti V, Ceresoli M, Coccolini F, Di Saverio S, Dominioni T, Farè CN, Frassini S, Gambini G, Leppäniemi A, Maestri M, Martín-Pérez E, Moore EE, Musella V, Peitzman AB, de la Hoz Rodríguez Á, Sargenti B, Sartelli M, Viganò J, Anderloni A, Biffl W, Catena F, Ansaloni L; S.P.Ri.M.A.C.C. Collaborative Group. Prediction of morbidity and mortality after early cholecystectomy for acute calculous cholecystitis: results of the S.P.Ri.M.A.C.C. study. World J Emerg Surg. 2023 Mar 18;18(1):20. PMID: 36934276; PMCID: PMC10024826. [CrossRef]
- Liao Y, Cai Q, Zhang X, Li F. Single-stage intraoperative ERCP combined with laparoscopic cholecystectomy versus preoperative ERCP Followed by laparoscopic cholecystectomy in the management of cholecystocholedocholithiasis: A meta-analysis of randomized trials. Med (United States). 2022, 101, E29002. [Google Scholar]
Figure 1.
Box-and-whisker plot of the operative time for the patients who were operated on for acute cholecystitis from September 2021 to September 2022 from 79 centres in 19 countries by the time between the onset of symptoms and surgery, n=117. The box represents the 25th to the 75th percentile IQR. The horizontal line within each box represents the median. ***p < 0.001, Kruskal-Wallis test.
Figure 1.
Box-and-whisker plot of the operative time for the patients who were operated on for acute cholecystitis from September 2021 to September 2022 from 79 centres in 19 countries by the time between the onset of symptoms and surgery, n=117. The box represents the 25th to the 75th percentile IQR. The horizontal line within each box represents the median. ***p < 0.001, Kruskal-Wallis test.
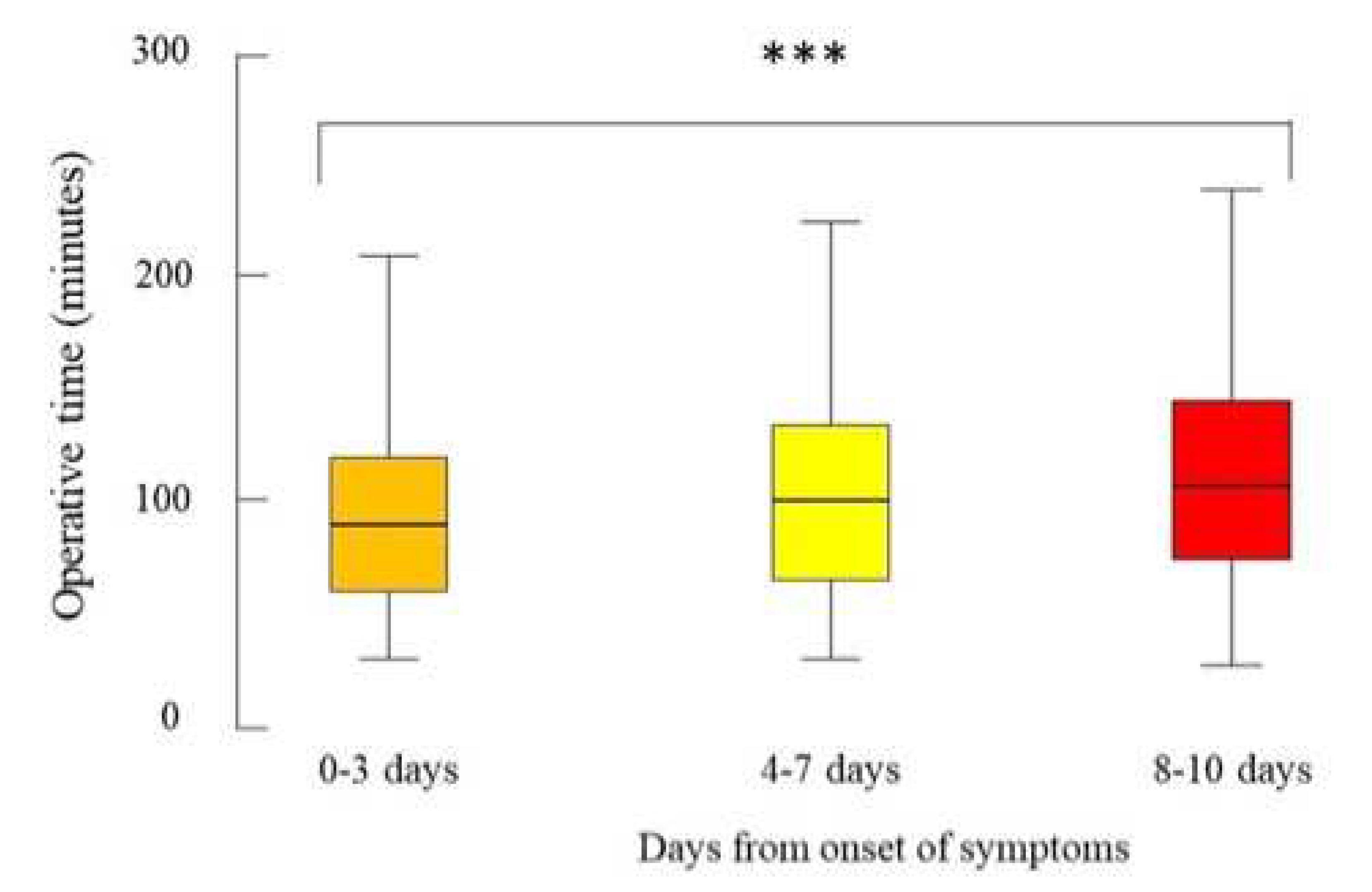
Figure 2.
Box-and-whisker plot of the length of hospital stay (days) of the patients who were operated on for acute cholecystitis from September 2021 to September 2022 from 79 centres in 19 countries by the time between the onset of symptoms and surgery, n=117. The box represents the 25th to the 75th percentile IQR. The horizontal line within each box represents the median. ***p < 0.001, Kruskal-Wallis test.
Figure 2.
Box-and-whisker plot of the length of hospital stay (days) of the patients who were operated on for acute cholecystitis from September 2021 to September 2022 from 79 centres in 19 countries by the time between the onset of symptoms and surgery, n=117. The box represents the 25th to the 75th percentile IQR. The horizontal line within each box represents the median. ***p < 0.001, Kruskal-Wallis test.
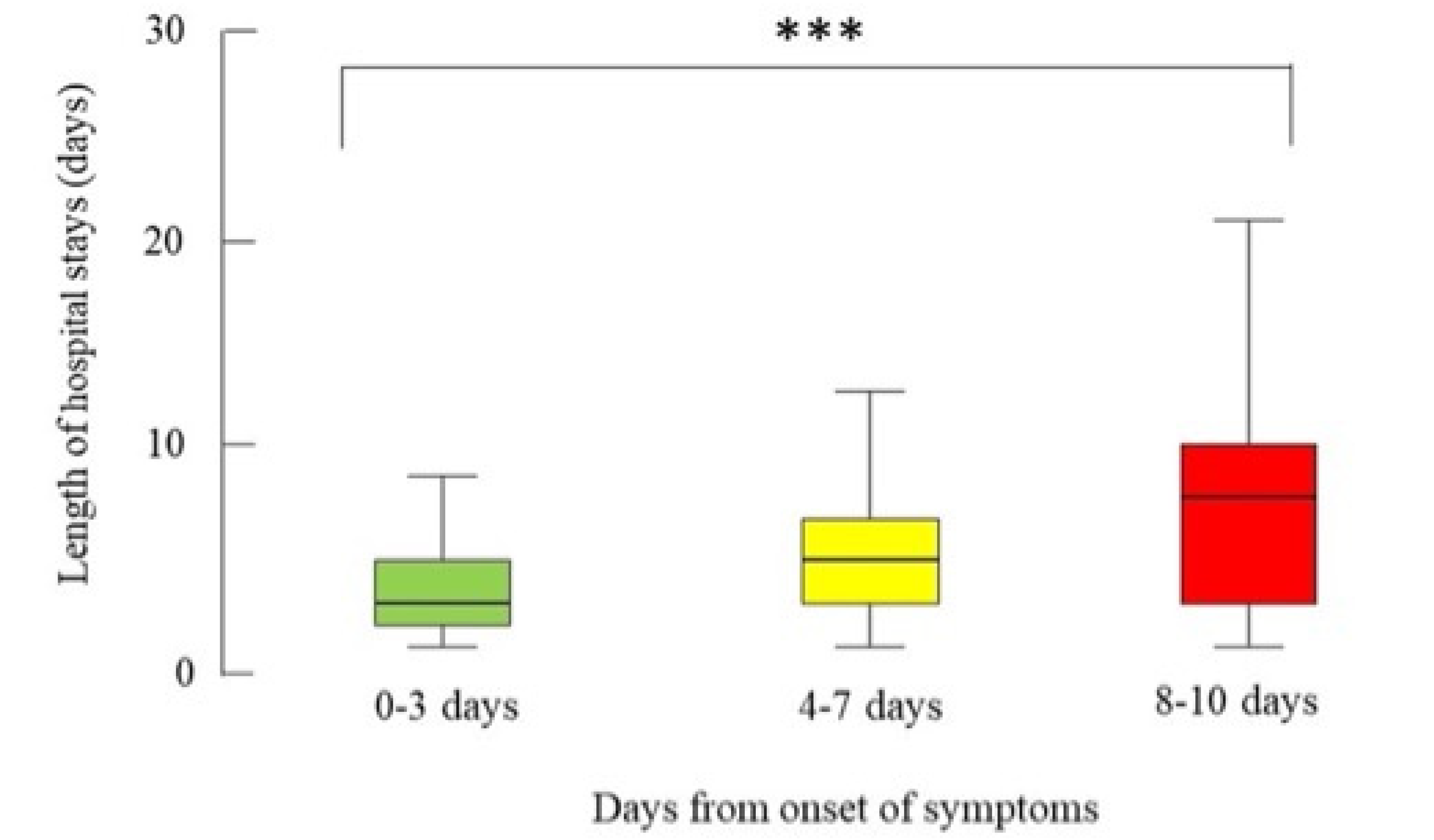

Table 1.
Preoperative characteristics of the patients who were operated on for acute cholecystitis from September 2021 to September 2022 from 79 centres in 19 countries by the time between the onset of symptoms and surgery, n=117.
Table 1.
Preoperative characteristics of the patients who were operated on for acute cholecystitis from September 2021 to September 2022 from 79 centres in 19 countries by the time between the onset of symptoms and surgery, n=117.
| Onset of Symptoms | ||||
|---|---|---|---|---|
| Variables | 0-3 days n=656 |
4-7 days n=360 |
8-10 days n=101 |
P value |
| Age (years) | 59 (46-72) | 62 (50-74) | 61 (46-74) | 0.14 |
| BMI | 26.7 (24.3-29.4) | 26.7 (24.2-29.4) | 26.3 (23.6-28.9) | 0.4 |
| ACC severity grade | 2 (1-2)* | 2 (2-2)* | 2 (1-2)* | <0.001 |
| POSSUM physiological score | 19 (15-24) | 19 (16-24) | 21(17-26) | 0.012 |
| Days from admission to surgery | 1 (0-1) | 2 (0-3) | 6 (2-8) | <0.001 |
BMI: Body Mass Index, ACC: Acure Cholecystitis, POSSUM: Physiological and Operative Severity Score for the enUmeration of Mortality and morbidity, PS: physiological score. Data are presented as median (IQR). P value Kruskall Wallis test. * mean (SD) of ACC severity grade: 1.6 (0.5) for 0-3 days, 1.8 (0.4) for 4-7 days, 1.7 (0.5) for 8-10 days.
Table 2.
Intraoperative outcome of the patients who were operated on for acute cholecystitis from September 2021 to September 2022 from 79 centres in 19 countries by the time between the onset of symptoms and surgery, n=117.
Table 2.
Intraoperative outcome of the patients who were operated on for acute cholecystitis from September 2021 to September 2022 from 79 centres in 19 countries by the time between the onset of symptoms and surgery, n=117.
| Onset of Symptoms | ||||
|---|---|---|---|---|
| Variables | 0-3 days n=656 |
4-7 days n=360 |
8-10 days n=101 |
P value |
| Operative time (minutes) | 90 (60-120) | 100 (65-134.5) | 107 (74-145) | <0.001 |
| Conversion to open surgery | 48 (7.9%) | 32 (9.9%) | 9 (9.5%) | 0.54 |
|
Bail-out procedure: Subtotal cholecystectomy Fundus-first technique Drainage only |
45 (6.9%) 18 (2.7%) 34 (5.2%) 1 (0.2%) |
35 (9.7%) 20 (5.6%) 24 (6.7%) 0 (0.0%) |
14 (13.9%) 11 (10.9%) 7 (6.9%) 0 (0%) |
0.037 <0.001 0.52 0.99 |
| Intraoperative complications | 18 (2.8%) | 20 (5.6%) | 8 (7.9%) | 0.01 |
Data are presented as median (IQR) or number (%). Percentages were calculated from valid available data. P value Kruskall Wallis test of Fisher’s Exact test as appropriate.
Table 3.
Postoperative outcomes of the patients who were operated on for acute cholecystitis from September 2021 to September 2022 from 79 centres in 19 countries by the time between the onset of symptoms and surgery, n=117.
Table 3.
Postoperative outcomes of the patients who were operated on for acute cholecystitis from September 2021 to September 2022 from 79 centres in 19 countries by the time between the onset of symptoms and surgery, n=117.
| Onset of Symptoms | ||||
|---|---|---|---|---|
| Variables | 0-3 days n=656 |
4-7 days n=360 |
8-10 days n=101 |
P value |
| Reintervention | 16 (2.4%) | 6 (1.7%) | 0 (0%) | 0.29 |
| Inhospital major complication | 38 (5.8%) | 15 (4.2%) | 6 (5.9%) | 0.49 |
| 30-day major complications | 48 (7.3%) | 22 (6.2%) | 7 (7.1%) | 0.78 |
| Inhospital mortality | 5 (0.8%) | 5 (1.4%) | 1 (1%) | 0.52 |
| 30-day mortality | 5 (0.8%) | 7 (1.9%) | 1 (1%) | 0.25 |
| LOS>10 days | 43 (6.6%) | 38 (10.6%) | 25 (24.8) | <0.001 |
| LOS (days) | 3 (2-5) | 5 (3-7) | 8 (3-11) | <0.001 |
LOS: length of stay. Data are presented as median (IQR) or number (%). P value Kruskall Wallis test of Fisher’s Exact test as appropriate.
Table 4.
Correlations between different continuous and ordinal data of the patients who were operated on for acute cholecystitis from September 2021 to September 2022 from 79 centres in 19 countries by the time between the onset of symptoms and surgery, n=117.
Table 4.
Correlations between different continuous and ordinal data of the patients who were operated on for acute cholecystitis from September 2021 to September 2022 from 79 centres in 19 countries by the time between the onset of symptoms and surgery, n=117.
| Length of stay | Days from admission to EC | POSSUM PS | Operative time | ||
|---|---|---|---|---|---|
| Days from onset to EC | Correlation | 0.26 | 0.53 | 0.01 | 0.14 |
| P value | <.001 | <.001 | 0.002 | <.001 | |
| Length of stay | Correlation | ------- | 0.35 | 0.31 | 0.33 |
| P value | ------- | <.001 | <.001 | <.001 | |
| Days from admission | Correlation | ------- | ------- | 0.06 | .167 |
| P value | ------- | ------- | 0.049 | <.001 | |
| POSSUM score | Correlation | ------- | ------- | ------- | 0.16 |
| P value | ------- | ------- | ------- | <.001 |
EC: early cholecystectomy, POSSUM: Physiological and Operative Severity Score for the enUmeration of Mortality and morbidity, PS: physiological score. P value= Pearson rank correlation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



