
Submitted:
08 September 2023
Posted:
11 September 2023
You are already at the latest version
Abstract
Quality of life (QOL) is based on their perception of their position in life in respect to their goals, expectations, standards, and concerns, as well as their culture and value systems, their workflow and workplace situations while it influences quality of services. In this study we aim to report on dental and nursing academians’ QOL and well-being at the end of the third year of the COVID-19 pandemic. The World Health Organization Quality of Life-BREF Scale (WHOQOL-BREF) tool, recording Physical, Psychological, Social and Environmental dimensions of QOL, was used. The WHOQOL-BREF was modified on a spiritual, coaching/mentoring approach in a two-step designing and validated procedure. The modified SHQOL-BREF (Spiritual Healthcare version) designed for this study, was uploaded, and filled in online during April-June 2023. Staff (N=120, 75% female) of both departments of Dentistry (44.2%) and Nursing (55.8%) of the National and Kapodistrian university of Athens, participated in anonymity. QOL in terms of physical health was reported at a higher level (M=72.2 points) compared to social relationships (M=69 points), psychological health (M=65 points) and environment (M=59 points) (scores reported in 0-100 score). Overall QOL was rated at 66 points while satisfaction from health at 72 points. Job satisfaction (M1=3.2) and spirituality (M2=3.0) were reported at a medium level in a 5-point scale, while personal beliefs and values were reported at a high level (M3=4.0). Participants age presented a significant, moderate to strong effect on physical health [F(3,97)=2.89, p<.05, η2p=.08] and on environment [F(3,97)=2.80, p<.05, η2p=.08] and marital status on social relationships [F(1,97)=9.66, p<.05, η2p=.09]. Married participants reported consistently higher levels of QOL compared to single participants, for all age groups. Department had a significant moderate effect on social relationships (F(1,97)=5.10, p<.05, η2p=.05) and education a significant moderate to strong effect on psychological health (F(2,97)=3.74, p<.05, η2p=.07). PhD level participants in both departments presented higher levels of psychological health compared to lower educational levels. Also, participants from the department of Dentistry reported higher levels of social relationships QOL in all educational groups, compared to the department of Nursing. Strategic planning on sustainability and QOL initiatives should be introduced after the COVID-19 pandemic for dental and nursing academic personnel to promote resilience and QOL scores.
Keywords:
healthcare
; quality of life
; WHOQOL questionnaire
; WHOQOL BREF version
; resilience
; values
; spirituality
; coach
; mentor
; academians
; academic personnel
; dentistry
; nursing
; sustainability in healthcare
; health Care Sector
1. Introduction
Employees 's perception of their position in life in respect to their goals, expectations, standards, and concerns, as well as their culture and value systems are a part of what the World Health Organization (WHO) defines as their quality of life (QOL). As a result, QOL is a wide concept that encompasses all human essential characteristics, such as the amount of independence, mental health, level of physical health, and personal values [1]. Individual facets of people’s perspective of their health and well-being define this description.
QOL is a multifaceted concept that incorporates psychological, sociocultural, and physical factors. It encompasses both subjective and objective assessments of the physical, mental, emotional, social, and spiritual health of an individual [2]. The QOL has a significant impact on how a person thinks, acts, feels, and approach challenges. It may impair one's performance and result in job loss, which worsens one's physical and mental health [1]. Further, effective function, precision, tolerance, patient care, and satisfaction from work are all impacted by sleep quality, which influences quality of life [3,4,5]. Also, there is an inverse tension in the relationship between QOL, employment, and family [6].
As of June 7, 2023, the World Health Organization (WHO) had received reports of more than 767 million COVID-19 illnesses and 6.94 million fatalities since the SARS-CoV-2 virus was originally discovered in December 2019. Data from the 5th of June 2023, reveal that a total of more than 13.39 billion vaccine doses have been administered [7]. This pandemic's unparalleled scope has an impact on every element of people's lives, encompassing their economical, emotional, and physical health. The COVID-19's psychological effects on Health Care Professionals (HCPs) were consistently recorded in different nations throughout the world.
Compared to the general population, COVID-19 patients and HCPs had a higher prevalence of sleep issues [8,9]. According to HCPs, there is a significant level of perceived stigma and burnout [10], which may be a factor in the increased frequency of psychological morbidities. Additionally, it has been noted that HCPs are more likely than people in general to experience psychiatric issues [11,12]. Moderate levels of QOL (62.4%), social relationship satisfaction (42.4%), mental health (59.4%), work environment and workplace safety perceptions (55.9%), in relation to stated quality of life were also reported [13]. According to another study in Greece, more than one-third of nurses, report having mild to severe symptoms of stress, depression, and anxiety [14]. The demanding and stressful nature of the profession can put nurses in danger and diminish their QOL. Low QOL may have an impact on the standard of care that nurses must give to their patients [15].
The continuous COVID-19 outbreak has caused nurses to be overloaded and under a great deal of stress. These demands can be balanced by improving one's quality of life, including one's work [16]. While secondary traumatic stress was more prevalent in nurses with traumatic life events, compassion satisfaction was higher in those with higher scores on religion and meaning. All participants viewed the change from fear to compassion satisfaction as a challenging but valuable trip [17]. According to research, resilience may operate as a protective factor against burnout and is a strong predictor of secondary traumatic stress, burnout, and compassion satisfaction [18,19].
Resilience is a crucial attribute that enables healthcare professionals to overcome obstacles in the face of the COVID-19 pandemic, according to recent studies [20]. In a study of 1210 HCPs from Iran, Germany, Italy and Netherlands, no matter the setting, HCPs and mainly female nurses, experienced stress, and anxiety. This led to poorer sleep and a decreased QOL [21]. In a cross-sectional study involving 218 HCPs, Abdelghani et al. [22] discovered that all QOL dimensions were negatively connected with health anxiety due to the COVID-19 virus. Furthermore, according to a study in 804 Greek dentists, men were more likely than women to experience low QOL and be dissatisfied with how their careers and personal lives were integrated during Covid-19 pandemic [23]. Personal resources including tight relationships with others, higher education, beliefs, and values might act as a resilience buffer against professional challenges during times of unplanned stressful situations. Dental professionals experienced extremely high levels of physical and mental weariness, which increased by 5.5 and 8.5 times, respectively, during the pandemic [24].
Although the pandemic's effects on health and QOL of are well known [25,26], there is less examination on how the pandemic has affected academic HCPs QOL. Healthcare academic workplace is ever more demanding, as scientific staff has clinical training, teaching and administrative work to fulfill while technical and administrative personnel perform duties with great responsibility towards students and patients corresponding to multiple roles each day. In the third year of the Covid-19 pandemic, there is a dearth of evidence for these personnel. Thus, this study aims to investigate Greek dental and nursing academians’ QOL and additional well-being elements (working conditions, job satisfaction, personal beliefs and values, spirituality) that affect their welfare and quality of services in their line of work during the third year of the Covid-19 pandemic. To design effective strategic resilience programs for healthcare professionals, it is crucial to additionally comprehend how the pandemic has impacted HCPs' QOL, their opinions on “well-being” footprint in workflow and workspace, as well as their suggestions on the most important risk factors associated with low QOL. We also aim to report on the relationship between sustainability in healthcare, well-being of professionals and QOL, since these terms affect productivity as well as patient care quality and safety [27,28,29,30,31]. Finally, we overall search for resilience improvement actions based on participants’ responses that would enable them to show a sustainable behavior in future stressful events and emergency situations.
2. Research Methods
2.1. Background of the study
The assessment of QOL has become progressively important in the healthcare sector even before Covid-19 pandemic. A related concept, gathering also attention lately is subjective well-being. Despite some commonalities, QOL and well-being are usually discussed in the relevant literature as separate concept and not as synonyms. In short, QOL refers to the cognitive appraisal which a person makes about the impact of certain factors on their daily life, whilst well-being concerns a person’s emotional response to these factors [32]. Defininition and measuring of well-being comes in many forms, has multiple dimensions and defines also certain parameters of QOL [33,34,35]. It is suggested that well-being at work concerns an overall sense of happiness, physical and mental health of the workforce [36]. The term has three dimensions: the psychological dimension (satisfaction, attitudes, and emotions in relation to work), the physical dimension (health and safety at work) and the social dimension (interpersonal relations, teamwork, management/administrative style) [34]. Recently a more broader and holistic explanation of well-being in the workplace has been developed including sixteen individual, group and organizational well-being domains [33,35,37,38,39,40,41,42] (Figure 1).
2.2. Identification of Factors Influencing QOL
QOL has been a key pillar in medical research for more than twenty years, supporting many clinical trials and research approaches regarding both the condition of the provider-doctor-professional of the field and the patient and how the relationship between them can affect the QOL of both [43,44,45,46] and the quality of services [30]. QOL has been already explored through philoshophic, psycologic and spiritual approaches on a research level through exploration of well-being status as described before [47,48].
Of course, QOL, by definition, contains subjective elements that are not easy to capture with quantitative measurements [49]. For this reason, the World Health Organization (WHO) has weighted a quality of life assessment questionnaire (analytical and short form) in which facts and values are essentially mixed at an unsystematic level in order to allow some quantitative assessments of the phenomenon [50,51,52]. The World Health Organization Quality of Life-BREF Scale (WHOQOL-BREF), a 26-item instrument, is a general QOL measurement tool that records four areas of QOL (Physical, Psychological, Social and Environmental dimensions) and is expressed officially by WHO in different languages [53]. Further, we used WHOQOL-SRPB field-test instrument (WHOQOL spirituality, religiousness and personal beliefs (SRPB) that is based on WHOQOL-100 questions plus 32 SRPB questions [54], addressing an additional domain of QOL, that of spirituality (Figure 2).
In our study we used the english and greek original version of the WHOQOL-BREF and WHOQOL-SRPB. Providing an opportunity to contrast QOL with other conditions or with various population patterns, values and factors, the current study had four objectives: 1) to assess whether the tool can be weighted for Greek academic healthcare professionals (dental and nursing personnel, 2) to reach an overall score for their QOL, 3) to capture and redifine factors addressed by WHOQOL-BREF as well as to add others from our pilot study, 4) to search on the impact of these factors on the QOL of Greek healthcare academic staff, and 5) to validate a modified SHQOL-BREF (Spiritual Healthcare QOL-BREF version) for healthcare professionals.
2.3. Methodology of Designing the Study Questionnaire
In this study, we used a previously reliable study technique, based on questionnaire data selection on QOL [52,55,56]. We performed the tecnhique in two rounds as has been described before [57,58].Prior to undertaking the main data collection, a pilot study was carried out, on March 2023 on a small sample in order to test the preliminary questionnaire. The initial questionnaire was based on the original Greek version of the WHOQOL-BREF in which 20 more open-ended questions were added according to WHOQOL-SRPB and findings of previous research on the field [35,59,60,61,62,63,64]. (Appendix I). We gave the list randomly to ten employees from the Department of Dentistry and ten employees from the Departement of Nursing of the School of Health Sciences of the National and Kapodistrian University of Athens, who volunteered in filling the questionnaire in person withing the settings of the two schools. During this procedure explanations were given when necessary according to the comprehensibility of the questions and the suggestions of participants to form the additional close-ended questions of the final questionnaire of the study. The additional questions were finally discussed with participants on site to determine comprehensibility, avoid bias interpretations and promote significance of additional factors, and their impact on stakeholders in both schools. This practice is suggested elsewhere too [35,55].
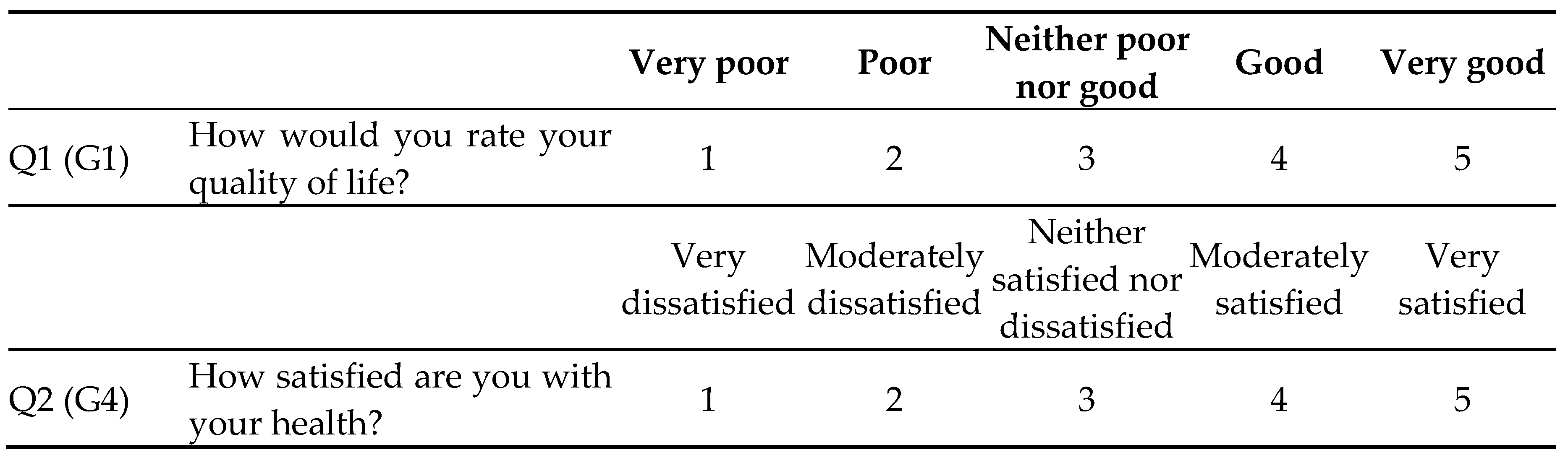
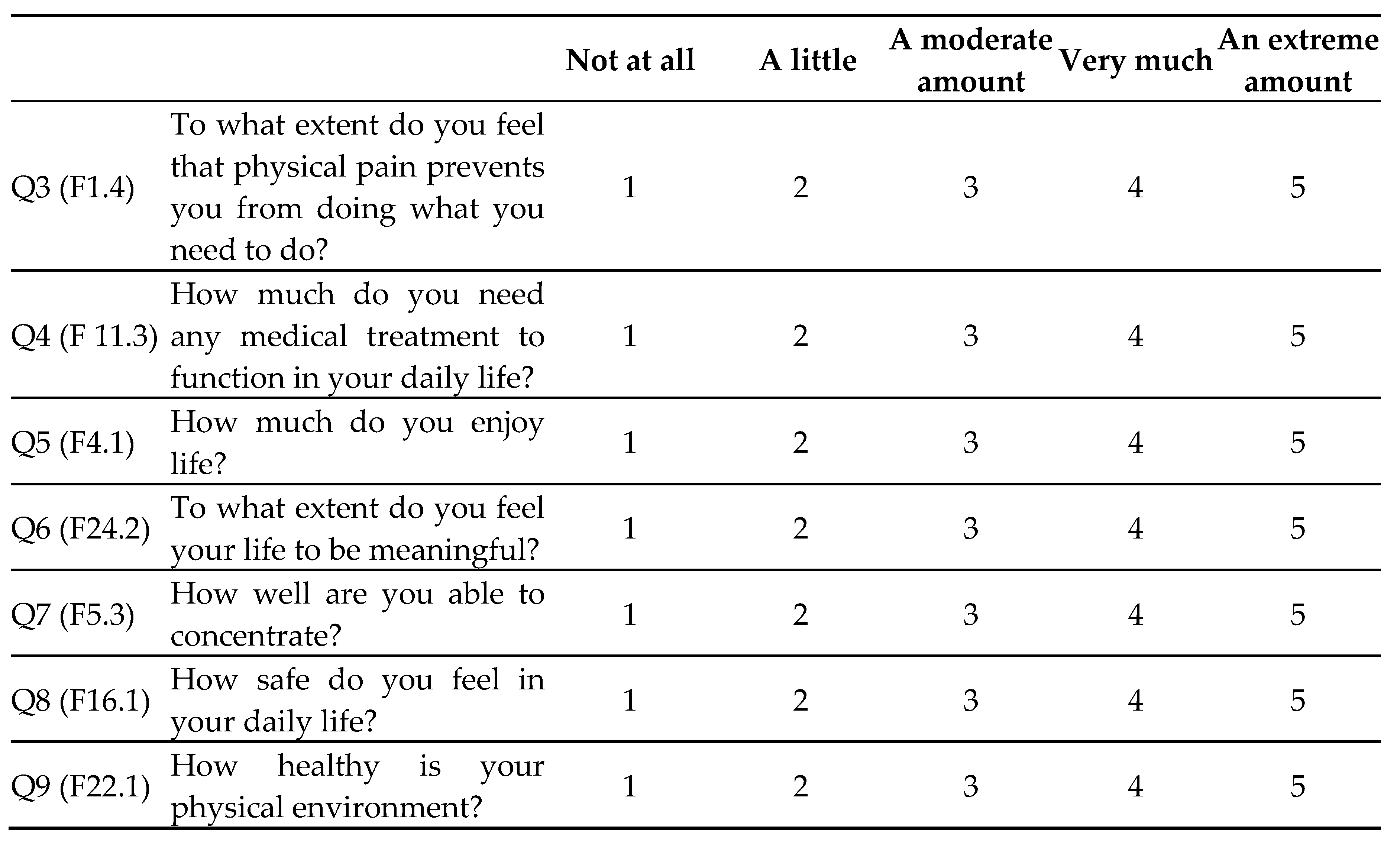
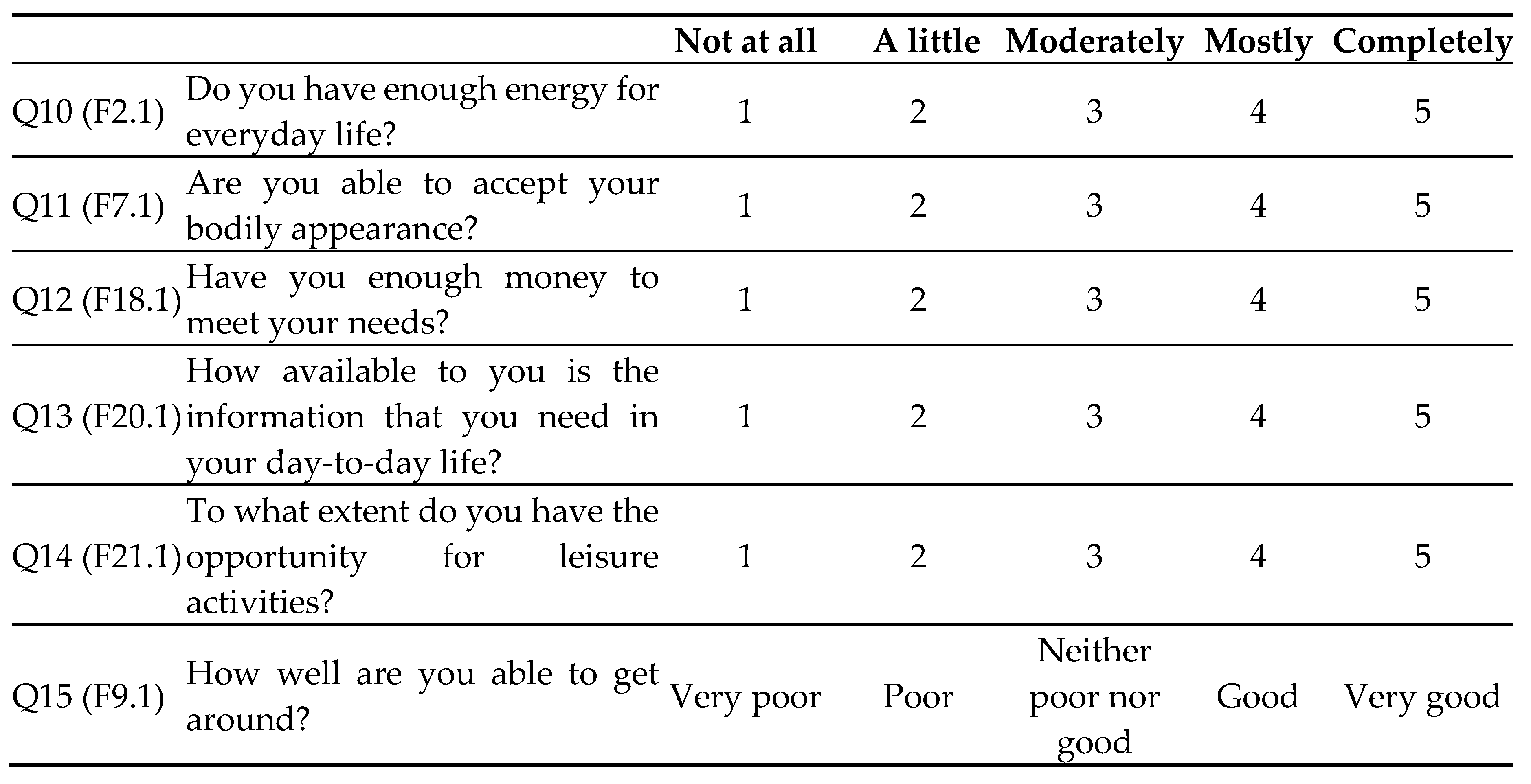
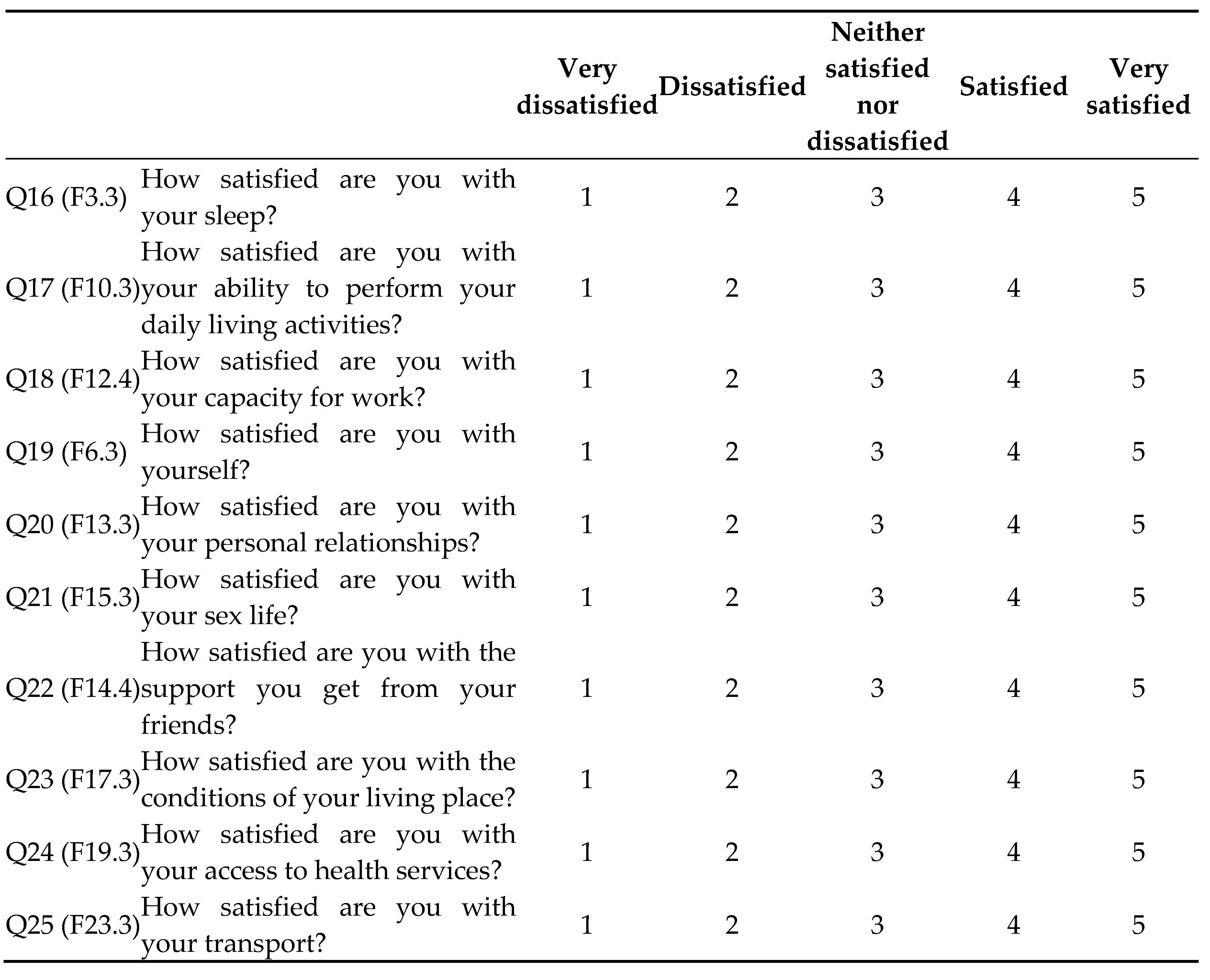
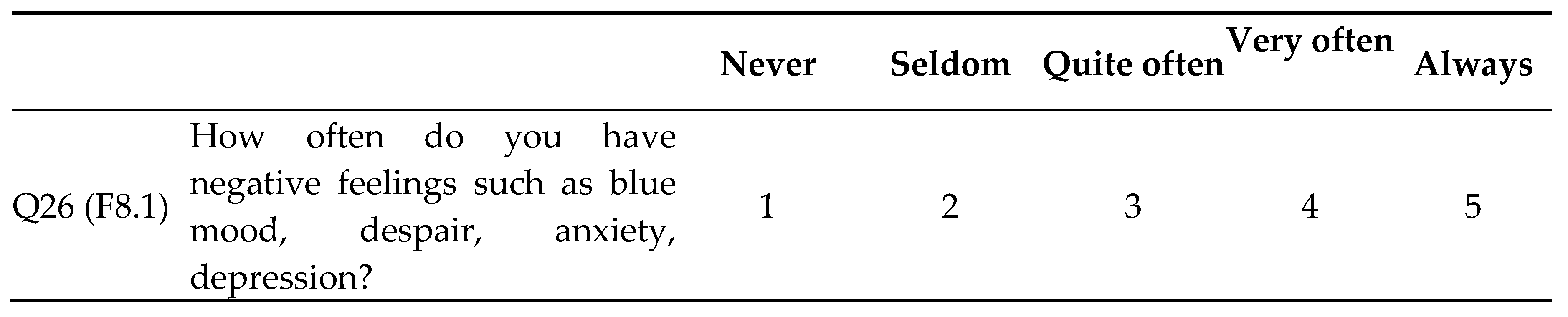
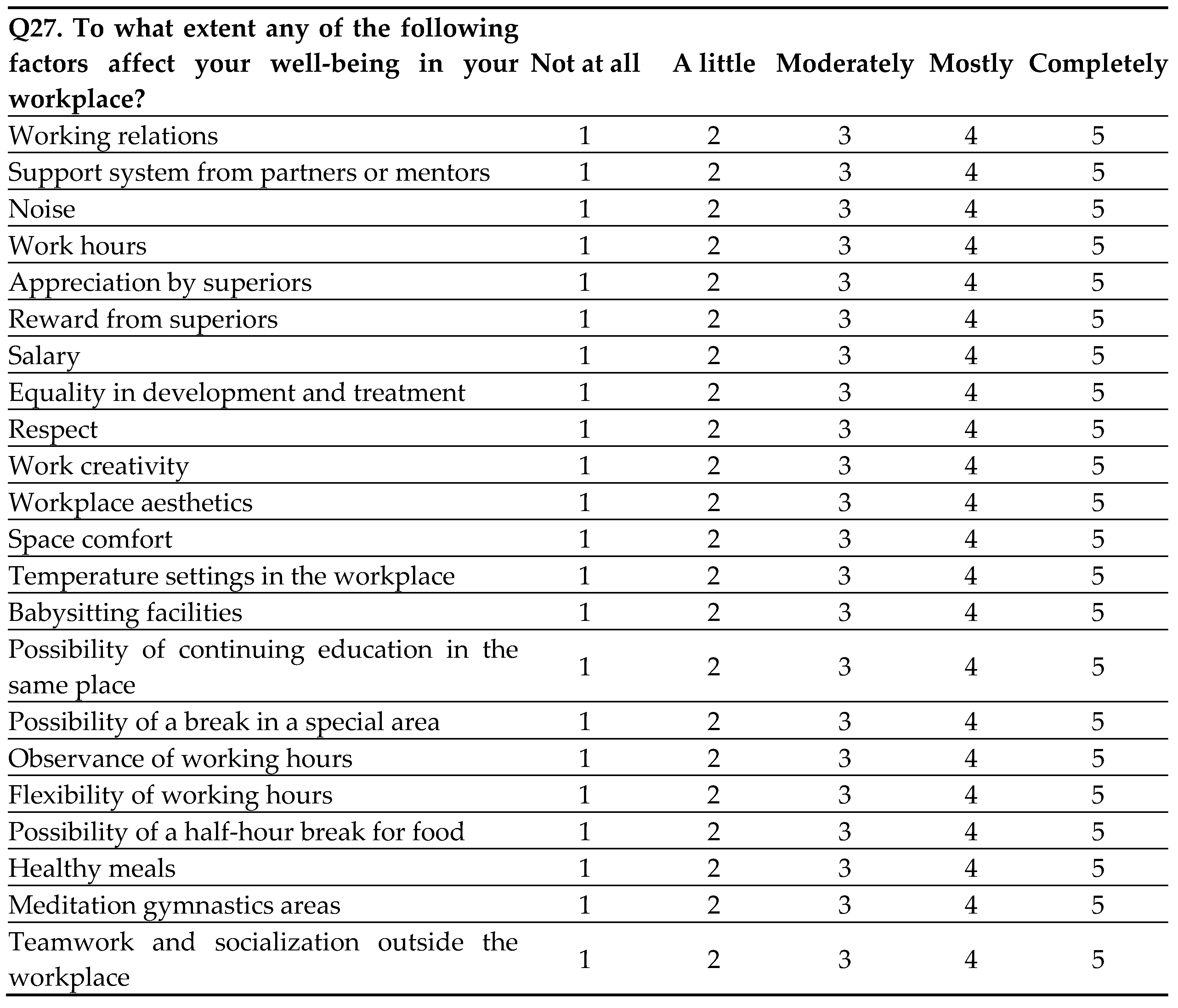
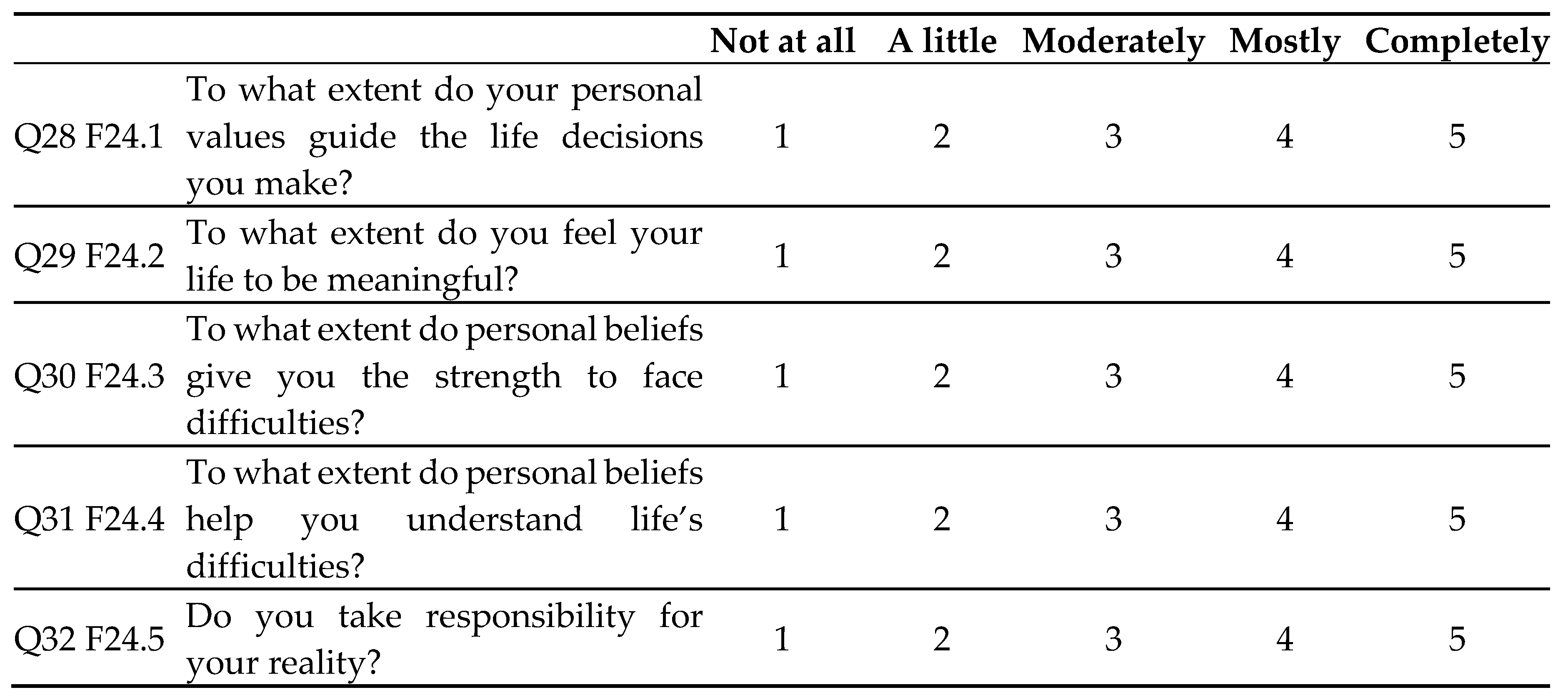
The final questionnaire was named SHQOL-BREF (Spiritual Healthcare QOL-BREF). It investigated: (a) the demographic characteristics of the sample (Demographic Part, Q1–Q12), including gender, age, marital and educational status, type of work employment, current status of health, also described partly elsewhere [58], (b) PART A (Q1-Q2), the overall QOL status and satisfaction level from health status, c) PART B (Q3-Q9) the experiences affecting QOL, d) PART C (Q10-Q15) the extent of importance of certain experiences in QOL e) PART D (Q16-Q26) the satisfaction from certain aspects of QOL, f) PART E (Q27) the additional factors affecting well-being, g) PART F (Q28-Q32) the intensity of personal beliefs and values affecting well-being, h) PART G (Q33-Q38) the religious and spiritual factors affecting well-being, i) PART H (Q39-Q40) the suggestions and personal opinions on ways to promote QOL and well-being at work and personal life. Parts E-G (Q27-Q38) had additional questions derived from the pilot study.
The descriptive part had multiple choice answers, Parts A-G used a five-point Likert scale to evaluate participants attitudes and preferences for QOL and well-being factors used in the study. Part H (Q39-Q40) had open-ended questions where participants could fill in their proposals and express their overall view on the topic.
The design and validity of the final questionnaire was further examined by 5 participants from each subgroup, while an independent panel of 3 experts (2 professors of the Department of Dentistry and 1 from the department of Nursing) reviewed and revised the final version of SHQOL-BREF questionnaire. At first, experts filled in the final version and discussed all questions with the authors in person to affirm validity. No issues regarding misconceptions of the terms or the expressions used were mentioned.
The steps followed to design the SHQOL-BREF questionnaire can be seen in Figure 3.
Two categories of participants were included in the second round (main study) of the data collection: (a) staff members of the Department of Dentistry and b) staff members of the Department of Nursing of the School of Health Sciences of the National and Kapodistrian University of Athens, Greece. The sample frame was made up of the total population within the two schools comprising of 1039 employees (485 in the department of Dentistry and 554 in the department of Nursing) which corresponds to previous research protocols suggesting that it is possible to survey an entire population if it is of a manageable size [65]. The final e-questionnaire version of SHQOL-BREF was designed according to the previously mentioned methodology and uploaded in google forms. Participants could follow a specific QR code to provide direct access through smartphones. Link and instructions were then distributed to staff members through the internal email system of each department, four times in a period of one month (once per week) during April 2023. The questionnaire incorporated an introductory message describing the purpose of the study and specifically mentioning that participation was voluntary, and confidentiality guaranteed. Participants had the right to refuse to participate. Consent was obtained by asking participants to confirm that they agreed to complete the questionnaire by marking a “Yes, I agree to participate” box. The Board of Ethics of the Department of Dentistry gave approval (No 547/21.11.2022) and of the Department of Nursing (No 426/9.1.2023). To submit the form, all questions needed to be answered. Only one submission was allowed. The questionnaires required approximately 15-18 min to complete. All staff members were given the same access and opportunity to complete the questionnaire. The questionnaire remained open for three months in total.
2.4. Statistical analysis
Data collected from the survey was analyzed with IBM SPSS v.28. Absolute and relative frequencies were calculated to summarize demographic characteristics of the study sample. Principal Component Analysis (PCA) and Varimax rotation with Kaiser normalization was applied to group items of working conditions scale into components. Cronbach’s alpha indices were calculated to examine the reliability of the scales and subscales of the survey. Quantitative variables were summarized with descriptive statistics (M, SD, median) and the distributions were examined in terms of normality via skewness and kurtosis [66]. Since variables were considered normally distributed, the parametric Pearson correlation coefficient was used to detect significant associated between QOL domains, job satisfaction, working conditions, personal beliefs, and spirituality, whereas the combined effects of gender, age, marital status, educational level, and department on QOL domains were examined with the use of Multivariate Analysis of Variance (MANOVA), [67].
3. Results
3.1. Sample
The sample consisted of 120 participants, (75% female), working in the department of Nursing (55.8%) and Dentistry (44.2%). Total staff members in the department of Dentistry (485) and Nursing (554) give an overall response rate of 11,54). Most participants (58.4%) were up to 40 years old, 45% were single and 62.5% had no children. Forty percent (40%) had a postgraduate degree and 23.3% a PhD, 20.8% were faculty members, 56.7% were postgraduate students, while 22.5% consisted of other administrative and technical staff. Most participants reported either 1-10 years (42.7%) or 10-20 years (29.1%) of working experience. Approximately 80% of participants maintained a professional activity outside of the academic community, while 68.8% reported an annual family income up to 25.000€. The sample was representative of all employees with respect to the demographic profile of the workforce in each department and has been described also elsewhere [23,24,58]. Closed questions about socio-demographic data (e.g. gender, age, marital status, length of service and job title) provided sufficient detail to compare the characteristics of the sample with the characteristics of the entire population of employees as recorded by the organization’s computerized personnel system. Detailed information on demographic characteristics is presented in Table 1.
Table 2 presents the component derived from the working conditions’ items as well as their loadings in the respective components, because of Principal Component Analysis (PCA). Three components were extracted, explaining 59.5% of the initial variability. The items “Respect from superiors”, “Respect from colleagues” and “Possibility of temperature adjustments in the space” have been removed because they loaded on more than one component. The first component with 9 items refers to working conditions and benefits, including items such as breaks for food in a suitable place, healthy meals, flexibility in working hours, babysitting, ability to socialize with colleagues, spaces for exercise, relaxation, or meditation etc., and explains 39.6% of the variability. The second component with 7 items refers to work relationships, rewards, and compensation (appreciation and recognition from superiors, business relations, reward from superiors, support system from colleagues or mentors, equality in development and treatment, noise, salary) and explains 12.7% of the variability and the third component with 4 items refers to workspace and nature of work (workplace aesthetics, work creativity, feeling of giving, space comfort) and explains 7.2% of the variability.
Descriptive statistics and reliability indicators of the study variables are presented in Table 3. QOL domain variables have been reported in 0-100 scores. Quality of life in terms of physical health was reported at a higher level (M=72.2 points) compared to social relationships (M=69 points), psychological health (M=65 points) and environment (M=59 points). Overall QOL was rated at 66 points while satisfaction from health at 72 points. The importance of the three working conditions’ components (Working conditions and benefits, Work relationships, rewards, and compensation and Workspace and nature of work) presented medium to high ratings (scores between 3 and 4 in a 5-point scale), job satisfaction was moderate (M=3.2 points in a 5-point scale), spirituality was also reported at a medium level (M=3.0 points in a 5-point scale), while personal beliefs and values were reported at a high level (M=4.0 points in a 5-point scale).
Pearson correlation coefficients between study variables are presented in Table 4. QOL in terms of physical health was positively correlated with job satisfaction (r=.377, p<.01) and personal beliefs (r=.332, p<.01). Moreover, psychological health was associated with higher levels of personal beliefs (r=.595, p<.01) and spirituality (r=.262, p<.01). Social relationships were positively related to workspace and nature of work (r=.293, p<.01), job satisfaction (r=.319, p<.01), and personal beliefs (r=.304, p<.01). Environmental QOL was related to higher levels of job satisfaction (r=.504, p<.01), personal beliefs (r=.282, p<.01) and spirituality (r=.223, p<.01). Overall, our findings show that the four areas of QOL are associated with job satisfaction, personal beliefs, and spirituality, so that the higher these are, the better the quality of life in those four domains. Also, the dimension of the Workspace and nature of work is positively associated with the quality of social relations, i.e. in a creative environment where people feel that they offer and are accepted, there is better quality in social relationships.
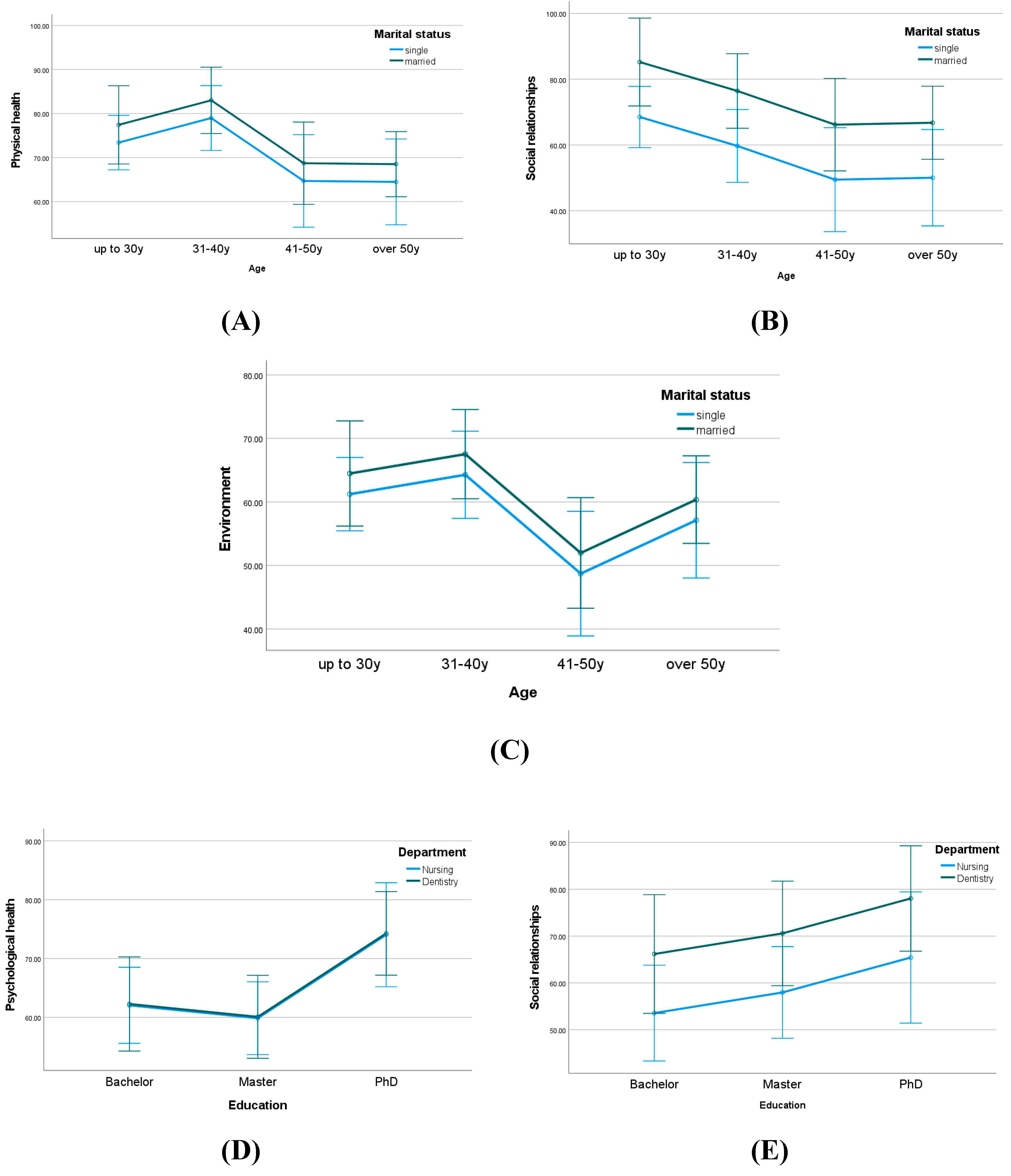
MAVONA results of tests of between-subjects effects of gender, age, marital status, department, and education level on the four QOL domains are presented in Table 5. Participants age presented a significant, moderate to strong effect on physical health [F(3,97)=2.89, p<.05, η2p=.08] and on environment [F(3,97)=2.80, p<.05, η2p=.08]. Marital status presented a significant, moderate to strong effect on social relationships [F(1,97)=9.66, p<.05, η2p=.09].
Specifically, as presented in Figure 3A, both married and single participants under 40 years of age reported higher levels of physical health compared to older participants. In terms of social relationships (Figure 3B), married participants reported consistently higher levels of QOL compared to single participants, for all age groups. Despite the non-significant differences between marital status groups, participants under 40 years of age reported higher levels of environmental QOL compared to older participants (Figure 3C).
Following, department also had a significant moderate effect on social relationships (F(1,97)=5.10, p<.05, η2p=.05) and education a significant moderate to strong effect on psychological health (F(2,97)=3.74, p<.05, η2p=.07). As presented in Figure 3D, PhD level participants in both departments presented higher levels of psychological health compared to lower educational levels. Also, Figure 3E shows that participants from the department of Dentistry reported higher levels of social relationships QOL in all educational groups, compared to the department of Nursing.
Figure 3.
Estimated marginal means of the MANOVA model for the domains of QoL: A) physical health against age groups and marital status, B) social relationships against age groups and marital status, C) environment against age groups and marital status, D) physical health against department and educational level, E) social relationships against department and educational level.
Figure 3.
Estimated marginal means of the MANOVA model for the domains of QoL: A) physical health against age groups and marital status, B) social relationships against age groups and marital status, C) environment against age groups and marital status, D) physical health against department and educational level, E) social relationships against department and educational level.
Almost half of the participants, at a percentage of 57.5%, answered positively at Q28: “To what extent do you think a coach/mentor/spiritual guide would help you in your self-awareness and development?” (27 people answered, “A moderate amount”, 27 “Very much” and 15 “an extreme amount”). Data from the open-ended question Q39 “What would you like to change in your workplace to be more satisfied?” revealed that 29.2% of the participants suggest changes in administrative issues (stable timetable, breaks, organization, change position, respect of employees rights, evolution in the hierarchy), 25% of them would expect better salary, 24.2% would rather experience better behavior from superiors, (respect, recognition, reward, equality, meritocracy, justice and common values), 17.5% would prefer better staff relations (team working, responsibility, respect), 14.2% need adequacy of staff, 13.1% discuss improvements in esthetics and infrastructure (improvement of space, equipment, privacy, noise hygiene, software). Only 2.5% discussed education on site and 1.6% other practical issues such as distance from home and transportation issues.
From question Q40 “What would you like to change in your life to be happier?”, we can report that most of the participants (48.3%) would prefer sufficient personal time to relax, do gymnastics, travel, spend time with friends and family, do hobbies or be more educated. Only 10.8% of them would rather change personality issues (be more positive, open, and resilient, less of a thinker, reduce stress, change worldview). Further, 10% of them would prefer to resolve economic issues to be happier and 7.5% would like to improve human relations (intimate and friendly). Additionally, a 6.7% of the participants would like to solve home issues (residence, house, distances), 5.8% of them would rather improve health issues to be happier (health, body image, healthier food, access to health modalities) and 5.8% would prefer to improve work conditions (stable timetable, relevant position to education, no work οut of working hours (e.g., on Saturdays and Sundays etc.). Finally, 3.3% suggest improvements in security issues and 3.3% discuss societal issues (environment, state status, society’s profile).
We could mention further some written approaches of the participants in the pilot and main study that give their overview of the topic. “There is a need to improve working conditions at all levels: Quality, safety, ensuring necessary resources for adequate operation, personnel, hygiene. Retraining, ensuring sufficient staff for the services, improving bureaucracy, effective management systems of an organization by ensuring people related to the subjects they are called to manage, rationalization of division of labor, opportunities for the promotion of qualifications, benefits to employees, etc.” and “well-being for me is to be happy most of the day..and in order to be happy, I need time for myself, qood people around me to work or chat, respect and reward at work, a family dinner without stress, time with friends and money to spend in order to be educated, travel, enjoy nature and silence!..”
4. Discussion
In this study we derived data on QOL and well-being of a sample of Greek dental and nursing academic personnel, three years after COVID-19 was declared a pandemic. To our knowledge this is the first study to evaluate the QOL of academic personnel. In Greece, frontline healthcare workers' quality of life and presence of negative emotions were assessed before [13,23]. In our study, the overall QOL was rated at 66 points. The importance of the three working conditions components presented medium to high ratings. The level of physical health was reported to be higher (M=72.2) compared to social relationships (M=69), psychological health (M=65) and environment (M=59). Similarly, in the study of Ghazy et al. [68], investigating health care professionals' QOL two years after the COVID-19 outbreak in Arab nations, the highest mean score was at the physical domain (M=68), indicating adequate energy, the capacity to deal with fatigue, pain, and discomfort, as well as adequate sleep and rest. Previous studies have also shown the association between pre-existing medical issues (negative self-perceived health status or being diagnosed with systemic illnesses) and poor physical health QOL [25,26,69]. Chronic diseases may significantly affect one's ability to participate in the workforce owing to physical, emotional, or social problems [70] and chronic pain or illnesses are associated with less compassion satisfaction, absenteeism and presenteeism [71]. In our study, most participants (58.4%) aged up to 40 years old and both married and single participants under 40 years of age reported higher levels of physical health compared to older participants thus explaining the overall QOL of this study.
Physical health dimension and QOL
In our study physical health QOL was rated at 72 points and was positively correlated with job satisfaction and personal beliefs meaning that professionals that are satisfied with work and have a stable value system feel physically healthy. Quality of life in terms of physical health was reported at a higher level than all other QOL dimensions (social relationships, psychological health, and environment) suggesting that physical health is obviously first in importance for QOL in our sample. Only 5.8% of our participants would like to make changes in health issues to be happier. In the study of Zaylea et al. [72], where healthcare workers in the second year of the pandemic had experienced changes in their working hours, and the majority had reduced their physical activity frequency (42.5%) and duration (42.8%), 29.4% reported that their physical well-being has been negatively affected. This fact though is not presented in the study of Teixeira et al. [73], in the first year of the pandemic where most of the participants were reporting health issues. Of course, except for the pandemic there are other chronic health problems not directly attributed to the pandemic but mainly to ergonomic working conditions that can somehow affect general health in healthcare professionals [74]. These differences during the pandemic could be attributed to our sample, to the gradual return to normality in the period of our study and the unevenness of our sample consisting not only of clinicians but also of administrative personnel. We also found that age is also affecting physical health QO, something that comes in accordance with findings suggesting that aging nursing personnel due to heavy physical tasks have more health issues than physicians [75]. Oppositely, age was not a significant factor in the Ghazy et al. [68] study for determining the physical activity score while in the study of Hawlader et al., [76], people over 45 years of age have a 52% lower likelihood of being in good physical condition as was the case in our study too.
Psychological health dimension and QOL
Our data reveal that psychological health was associated with higher levels of importance of personal beliefs and spirituality while education had a significant moderate to strong effect on psychological health. We can also report that marital status can enhance psychological health. Our findings correspond to findings from the study of Suryavanshi et al. [77] that demonstrated a high prevalence of symptoms of depression and anxiety and low QOL among Indian HCPs during the COVID-19 pandemic. Also, in that study, combined depression and anxiety were found to be 2.37 times higher among single HCPs compared to married. Overall, our findings correspond to findings of other studies too, demonstrating a high prevalence of symptoms of depression and anxiety and low QOL in healthcare professionals working with COVID-19 patients, where gender, marital status, and age significantly predicted depressive symptoms, posttraumatic stress symptoms, and psychological distress respectively [24,78]. More specifically, it is mentioned that during the pandemic, factors associated with psychological distress for dentists were lower income, burnout, high job stress, career-choice regret, and lack of sufficient personal time, and for dental nurses were age, lower income, longer working hours per week, burnout, high job stress, low job satisfaction, lack of sufficient personal time, and poor medical environment [78]. In our study though, lack of sufficient personal time was attributed to 48.3% of our participants as a basic factor of low psychological health. Further, being female and not in a relationship were found elsewhere to be associated with higher levels of depressive symptoms, whereas being female and older were found to be related to higher levels of posttraumatic syndrome [79], as was the case in our study too. Also, in dental population, male professionals were having more phycological problems than their female colleagues during the pandemic due to the reverse of roles in their routines [24]. Our data show though that gender is not directly correlated to QOL possibly due to the different job distribution among academic personnel, the distance working during the pandemic and the overload program of academic work for all participants, despite of gender in the period recovering from the pandemic when the study had taken place.
Environmental dimension and QOL
The three working conditions’ components revealed by our analysis (Working conditions and benefits, Work relationships, rewards, and compensation and Workspace and nature of work) are of medium to high importance for environmental QOL in our sample. Elsewhere is also suggested that environmental QOL consists of a variety of different relationships and working conditions in the workplace. In the study by Omidi et al. [80], nurses who worked more than 36–40 hours a week had a poorer score in the environment category. The environmental domain findings covered topics including physical security, leisure time activities, and transit options. In the Ghazy et al. study [68], also low mean scores were found for the environmental and psychological domains, indicating poor home environment satisfaction, poor participation in leisure activities, comprised activities of daily living, general law and order situations, less mobility and greater discomfort, fatigue, and reduced work capacity. In our study though, environmental QOL was related to higher levels of job satisfaction, personal beliefs, and spirituality meaning that a strong value and existential base could go hand in hand with environmental QOL. Although it is not specified whether these bases initiate higher environmental QOL or it is the good environmental QOL that enhance values and spirituality, the correlation among these parameters is not to be denied. Other researchers agree that feeling comfortable at work is associated with a positive perception of the supportiveness of the organizational climate since insecurity is a key dimension of negative well-being and low quality of services [81]. If work environment is not exciting, fulfilling, rewarding stimulating and enjoyable [38] and there is not a compassionate culture demonstrating support and a caring and empathetic culture, there is no promotion of employees’ well-being, people are disappointed, even angry, and thus performance is low, and services are of questionable quality [35]. On the opposite, people who feel well and valued perform better than those who feel rejected [82]. We should further mention that when people feel that they have been unfairly treated they experience a series of injustices, they feel hurt slighted and, in many cases, frustrated because feelings of inferiority preoccupy the mind and dominate one’s thoughts [83]. Perceived unfairness is a significant demotivator [84]. Hopefully, only 24.2% in our sample would rather experience better behavior from superiors, (respect, recognition, reward, equality, meritocracy, justice, and common values) and 17.5% would prefer better staff relations (team working, responsibility, respect) possibly showing that not such issues are important in both departments. So, quality relationships between employees and counsellors, mentors/coaches and customers are important for employees’ well-being at work [33]. Employees want to be convinced about ethical practice and corporate social responsibility that includes fairness, compassionate leadership, fair work practices [35] to perform better in their position. In our study only three employees argued about the irrelevance of their job or the need to change position. Of course, we must consider that this study has taken place in a public university where people are being paid by the state a fixed amount and most of them have a permanent position in the organization that at least argues any doubt about job insecurity.
Working conditions concerning hours of work, timetable, breaks, seem also to be significant factors on QOL in our sample. This means that not having staff adequacy thus not having time for breaks and work overload, has a negative impact on care, teaching, administrative or technical support quality and services as mentioned elsewhere too [84]. It is already reported that low nurse staffing levels in local care settings are associated with poorer user experiences [85], hospital readmissions [86] and less continuity of care [87,88]. We must consider from one part, the number of staff and the distribution of staff groups (staff ratio) and from the other, the skill-mix to provide the care that is needed [89,90]. In our study, 14.2% of the participants commented on the staff ratio adequacy and 5.8% of them discussed the right position according to education and skills. As suggested elsewhere, not being in the right position, working overloaded and overtime due to inadequacy of staff results in high levels of sickness, absence and part-time work or retirement for dentist too [23,24]. Long hours of working is an important factor in our study too as it was already reported that it had driven to a burnout blast among dentists and nurses before and during the pandemic [23,24,91,92,93,94], with a negative impact on employees’ health fatigue and relationships, resulting in absences, more accidents and errors, reduced satisfaction psychological well-being and job performance [95,96,97,98].
Finally, work-life conflict is mentioned as a negative factor for QOL and well-being. It is not unusual in the relevant literature to reveal high needs for personal time from employees in the healthcare sector [68,84]. The fact that most individuals are continuously striving to balance work and personal lives is the big challenge of today [99]. In the study of Shivakumar & Pujar [95], an approximately 40% of the staff expressed they are unable to spend enough time with family while most of the staff agree that there should be flexible working hours and compensatory holidays to maintain work life balance. In our study 48.3% of our participants needed more free personal time and time to spend with family and friends, also discussing flexibility in the timetable but also avoidance of overtime on Saturdays and Sundays. This situation can drive to less commitment, discipline, and performance as has been mentioned already [95]. Also, in our study, 5.8% of the employees would rather have changes in administrative issues concerning working hours. Employees working overtime experience negative work-life balance, health issues, family disturbance that ultimately leads to de-motivation and scope of turnover. Moore [100] has indicated that those employers who can provide supportive policies to create long term work life balance, can create a culture where employees are positive, productive, and loyal will be addressed as “good cases” for work.
We can also comment in our study, that participants under 40 years of age reported higher levels of environmental QOL compared to older participants signalizing that millennials and Z-ers give a further attribute to natural environments and esthetics in the workplace as also mentioned elsewhere [101]. In the study of Schell et al. [101], a” high rank” needs for aesthetic improvement were associated to psychologically demanding work, negative work stress, sleep disturbances, problems at work, musculoskeletal pain, and lower age. We did not find such a correlation with only 13.1% of our participants worrying about esthetics, infrastructure, equipment, and maintenance. Of course, environmental QOL has more to do than just esthetics. It also discusses the matter of privacy in the workplace, which is another important issue associated with the concept of confidentiality [102]. Privacy refers to the right to be left alone and free from intrusion, having an independent workspace, including the right to make independent decisions based on personal beliefs, feelings, or attitudes; the right to control bodily integrity; and the right to decide when and how sensitive information is shared [102,103,104]. Only two of our participants discussed privacy issues to be more satisfied in the workplace, possibly because privacy is well controlled in both departments. Noise and hygiene issues were mentioned by only four people in our study as negative factors affecting QOL and well-being as discussed elsewhere too [105].
Environmental QOL is further related to financial issues of both individual employees as well as of the organization itself. It is mentioned that the environment in which individuals live, and work has a major and significant influence on how individuals respond to their own feelings of well-being [82]. So, an emotionally healthy workplace, oriented financially sound has better perspectives to flourish, offer better services, enhances motivation and effort, and can afford to be optimistic about its future [106]. This has a serious effect on employees as in our case that more than 50% of the sample discussed about the need for organizational changes that most of them would be afforded if the economic status of the two departments was better (better salaries, adequate staff). If the financial well-being of an organization is not healthy and administration and managers need to function with limited budgets and expenditure reduction ideology, there are implications such as job insecurity, increased workloads, job-related stress and strain, mental ill health [35]. Then the success of an organization is judged based on its financial performance and its ability to provide high-quality goods and services over time [30,107]. On the other way round, a joy-filled workplace is said to improve financial performance and ensure positivity and meaning in the work done [108], thus improving QOL and quality of services. This should be an administrative strategic plan for both departments in our study.
Social relationships dimension and QOL
A significant relationship between marital status and QOL was reported in the study of Han et al. [109] with this relationship to be affected by gender and age. Further in the study of Puciato et al. [110], there was a dependence between marital status, perceived health condition and QOL. In that study male sex, higher education, being an entrepreneur, college student or white-collar worker, and good financial status were associated with the highest assessments of QOL and perceived health condition. In our study, although married participants also reported consistently higher levels of QOL compared to single participants, there were no differences among age groups or sex. In a sample of Greek dentists though during pandemic QOL was significantly lower for men than women [23]. Overall, social relationships in our study were positively related to workspace and nature of work, job satisfaction, and personal beliefs as reported elsewhere too [23,24]. Also, dentists reported a better QOL in social relationships than nurses. In the “Harvard Study of Adult Development” which started in Boston in 1938, following 2000 volunteers for 85 years and covering already three generations: grandparents, parents and children revealed that the happiest people did two main things during those 85 years: taking care of their health and cultivating meaningful relationships with others [109]. This is suggested by others too in between this lifespan [110,111,112,113,114].
Proposals on academic QOL
Initiatives to enhance QOL and well-being should be embraced by organizations as a priority otherwise they could be found marginalized in the future. On the opposite part healthcare facilities that foster well-being are perceived as employers of “best practice” and are recognized by current and prospective employees as offering a desirable place to work [30,34]. There is a universal agreement that the healthcare industry is one of the most hazardous environments to work in. Employees in this industry are constantly exposed to a complex variety of health and safety hazards, noise, constant human contact, ergonomic issues and standing for long periods. Long working hours, overload and shift work add to the stress of work [115]. Our findings agree with the description of this hard-working environment [116,117] and changes should be incorporated in future administrative plans. According to participants’ suggestions, the timetable should be reorganized to fulfill a stable but rather flexible timetable of morning shifts (8.00-16.00 hours), lunch breaks, avoid overtime or weekends work, and have access to healthy food. Spaces of relaxation, gym and meditation should be designed too in the facilities of both departments. Communication and teamworking should be enhanced to cultivate trust. International collaborations could reinforce the openness of the departments and bring the sense of creativity, knowledge excitement and work meaning to employees. Finally, periodical educational seminars on resilience themes should be incorporated for all personnel. The role of employee’s coach or mentor within both the departments should be enhanced as more than 55% of staff members would like a coach assistance to further help them in their self-awareness effort and self-development as has been already suggested before [118]. Overall, it seems from our findings that professional success alone does not guarantee happiness, although it can be enjoyable. The study revealed that happier people were not isolated. In fact, the happiest people valued and nurtured human relationships. Education and cultural awareness levels, which tended to be higher among those with higher salaries, were also important factors in adopting healthy habits (promoted more frequently since the 1960s) and in better access to healthcare. Loneliness, which is becoming more and more frequent, causes anxiety [119,120,121,122]. It is therefore necessary to have someone to whom we can get rid of it. We also recommend cultivating, strengthening, and expanding human relationships, in fact maintaining social ties, which, just like fitness, also requires constant practice. Friendships and relationships in Academia need regular commitment with just a simple phone call, to keep them from slackening. Engaging in activities that bring joy and encourage companionship, such as sports, hobbies, and volunteer work, can broaden the network of relationships especially among academic personnel that do not have the time to expand relationships outside academia. However, the truth is that no one's life is free of difficulties and challenges, but social skills contribute to resilience. Administrators of the two departments and especially of the nursing department should encourage social events where all personnel could have access to and enjoy common leisure time.
Limitations of the study
This study has some strengths and some limitations. First, the data were directed in specific healthcare sectors of a public university, making it less possible to understand the QOL and health of individual professionals or establish health policies based on generalized evidence. Above all, these data reflect the experiences of academic personnel in only one institution which although is supposed to be in a high-ranking position (NKUA is ranked 252nd worldwide among 12,000 Universities, 55th among the 3465 Universities of the European Union and respectively 1st in Greece among the Greek Universities included in the ranking) [123], QOL of staff members is not reaching a high level (less than 80 points). Further estimation of values, culture and regions or work positions could promote more differences in QOL as suggested also elsewhere [120] providing a better insight of the correlation between academic effort and willingness to promote QOL with physical, psychological, and mental health environment and working/administrative issues. Additionally, the study used a rather limited (although efficient sample) that could then be augmented in future studies to allow for a wider simulation of the respective population. The unwillingness to participate in this study is relevant to behavior reported elsewhere too [58] and could be addressed with a personal interview future approach.
This study was cross-sectional in nature, hence there is limitation in interpreting the causal relationship between certain demographic characteristics and QOL or specify the physical health disorders that are involved in the estimation of Health QOL due to the generic nature of the information collected as is the case elsewhere too [75,124]. The questions were asked for the current time and the question about QOL was on the day the participant filled out the questionnaire. Therefore, we believe that we are working on a one-way relationship. Thus, it is unlikely that the participants’ previous QOL resulted in the current estimation of factors addressed here. Further, to measure the relationship more accurately between QOL, work well-being, demographic characteristics in healthcare academic personnel and quality of services, other issues must be considered. For instance, more studies are needed about the positive impact of marital satisfaction, educational and economic status on quality of life of academic personnel, about work relationships quality by gender or age group, and about the increase in well-being due to ethical, religious, and spiritual values and practices such as regular breaks, gym exercise or meditation on work site. Privacy and its various dimensions in the occupational health context should also be examined in connection with QOL as suggested elsewhere too [102,104].
Despite these limitations and up to the best of our knowledge this is the first study on the relationship between QOL, demographic characteristics, well-being factors and healthcare personnel in a public academic environment and even more between two different healthcare departments. Further estimation of QOL in other departments could give more information to design resilience strategies for future emergency situations. Finally, the SHQOL-BREF although validated in our study could be further tested in other public or private healthcare departments.
5. Conclusions
In this study the modified SHQOL_BREF (Spiritual Healthcare version) was administered in personnel of Dentistry and Nursing Faculty of National and Kapodistrian University of Athens. Overall QOL was rated at a medium to high level. Physical health was rated as having the highest QOL of the four domains, while the environment had the lowest. Personal values and beliefs were indicated at a high level, whereas job satisfaction and spirituality were recorded at a medium level. Higher levels of QOL were correlated with marital status, a PhD education, and young age (under 40). Social interactions were also very somewhat influenced by department.
Understanding the role that sociodemographic, individual, interpersonal, and workplace traits play in staff members' quality of life, overall wellbeing, and academic performance is crucial. More attention has to be paid to the role that resilience and spirituality play in quality of life and job satisfaction. The QOL delivers creative work practises that impact both the performance of the person and the entire organisation. at addition to being crucial for creating health promotion initiatives at universities, enhancing the QOL of academic staff can also improve staff and student performance. After the COVID-19 pandemic, dental and nursing academic staff should begin strategic planning on sustainability and QOL activities to foster resilience and QOL scores.
Author Contributions
Conceptualization, M.A.; methodology, M.A.; software, M.A.; validation, M.A., P.M. and P.M.; formal analysis, M.A.; investigation, M.A., P.M. and P.M.; resources, M.A., and P.M.; data curation, M.A.; writing—original draft preparation, M.A., and P.M.; writing—review and editing, M.A., P.M. and P.M; visualization, M.A., and P.M; supervision, M.A.; project administration, M.A.; funding acquisition, M.A., P.M. and P.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research was partly financed by the Specific Account for Grant Research of the National and Kapodistrian University of Athens (ELKE). The funding source was not involved in the study.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Board of Ethics of the Department of Dentistry (No 547/21.11.2022) and of the Department of Nursing (No 426/9.1.2023).
Informed Consent Statement
Informed consent was obtained from all participants when the questionnaires were filled out.
Data Availability Statement
Not applicable.
Acknowledgments
The authors would like to thank all participants who filled out the questionnaires used in the study.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A. (pilot study)
The following questions were asked additionally to the questions of the WHOQOL (greek version):
- 1)
- In your opinion, what do you understand by the term employee well-being?
- 2)
- What sort of practices had implemented either the administration of the department or that of the university to promote employee wellbeing?
- 3)
- If you have to use words to define your individual well-being at work in the department what would they be? Please explain
- 4)
- Do you have time for breaks at work in the department? Please explain
- 5)
- What are your views about training received within the department the last 12 months? What would you like to suggest for improvement?
- 6)
- How do you feel about having a coach or mentor within the workplace to support you? Please explain
- 7)
- Do you think relationships between administration and staff are harmonious? Please explain
- 8)
- What are your views about team working in the department?
- 9)
- What are your views about recruitment and selection strategies used in the department? Please explain
- 10)
- How satisfied are you with your job? Please explain
- 11)
- What are your views on being able to use your own initiative?
- 12)
- Do you feel that your job is secure? Please explain
- 13)
- What are your views about being adequately compensated for the amount of work and effort that you put into your job?
- 14)
- What are your views about ethical code and reward policy used in the department? Please explain
- 15)
- What are your views on being involved in decision making in the department?
- 16)
- If you were offered more money in another department/university would you think about changing job? Please explain
- 17)
- In terms of work-life balance what are your views on work-life balance practices that should be implemented or enforced within the department?
- 18)
- How has changes within the department affected your well-being? Please explain
- 19)
- How supportive are your colleagues and administration with non-work issues? Please explain
- 20)
- Can you describe what things you would like to see improved in the department to promote your well-being at work?
Appendix B. (main study)
Introductory message
Dear colleagues,
You are invited to participate in an interdepartmental research activity of the Department of Dentistry and the Department of Nursing of the School of Health Sciences of the National and Kapodistrian University of Athens.
In your capacity as employees (faculty members, technical and administrative staff members, scientific associates, and postgraduate students) of these two departments, you are welcome to fill in the following questionnaire.
This questionnaire examines how you judge your quality of life, your health, and other aspects of your life at the present time. Please answer all questions. You should read each question, think about, and evaluate your feelings by noting the number on the scale that gives the most appropriate answer for you. If you are unsure of the answer to a question, please choose the one you think is the most correct. Often, the most correct one may be the first answer you thought of. Please consider your own criteria, your own expectations, what gives you joy as well as what may concern you. We would like you to remember the last two weeks of your life.
The questionnaire is anonymous and in no way leads to the collection of personal data. Participation is voluntary and no reward is provided for your participation. Each employee can complete the questionnaire ONLY once. The completion of the questionnaire implies acceptance of the rules of personal data protection. The results of this study will be used for scientific publications and actions to improve working conditions in the departments involved.
Time to complete the questionnaire: 15 minutes.
The study is carried out under the auspices and approval of the Board of Ethics of the Department of Dentistry (No 547/21.11.2022) and of the Department of Nursing (No 426/9.1.2023).
The final version of the questionnaire
DESCRIPTIVE PART
1. What is your gender? a. Male, b. Female, c. Other
2. How old are you? a. Up to 30 years old, b. 31-40 years old, c. 41-50 years old, d. 51-60 years old, e. 60 years and over
3. What is your marital status? a. Single, b. Married, c. In cohabitation, d. Separated, e. Divorced, F. Widower, g. Other
4. Which category do you belong to? a. Faculty Member, b. Member of EDIP, c. EIB staff, d. Administrative staff of IDAX, e. IDOX administrative staff, F. IDAX technical staff, g. IDOX technical staff, h. Scientific associates (paid), i. Unpaid scientific associates, j. Postgraduate students.
5. If you maintain professional activity outside academic hours, what form does it take? a. Sole proprietorship, b. Sole proprietorship with 1 employee, c. Sole proprietorship with more than 2 employees, d. Company (member or director), e. Provision of services with block without individual headquarters, f. Hospital occupation, g. Provision with block without individual headquarters
6. What is the highest education you received? A. Primary education, b. Secondary education, c. University, d. postgraduate degree
7. Do you have children? a. 0 none b. 1-2 children c. 3-4 children, d. 5 and over children
8. How many years do you receive a salary in the department? a. 1-10 years b. 11-20 years c. 21-30 years d. 31 and over
9. What is your annual family income? Under 15.000, 15.001- 25.000, €25.001 € - 50.000, €50.001 € - 100.000 €, 100.001€ and above
10. How is your health? Pretty poor (1) - Poor (2) - Neither poor nor good (3) – Good (4) -Very good (5)
11. Do you consider yourself currently ill? Yes......No....................
12. If there is something wrong with you, what do you think it is? ________________________
Instructions: This questionnaire examines how you judge your quality of life, your health, and other aspects of your life. Please answer all questions. If you are unsure of the answer to a question, please choose the one you think is the most correct. Often, the most correct may be the first answer you thought of. Please consider your own criteria, your own expectations, what gives you joy and what may concern you. We would like you to remember the last two weeks of your life. For example, thinking back to the last two weeks, one question might be:
| How well are you able to concentrate? | Not at all 1 |
A little 2 |
A moderate amount 3 |
Very much 4 |
Extremely 5 |
- You should circle the number that best fits how well you are able to concentrate over the last two weeks. So, you would
- circle the number 4 if you were able to concentrate very much. You would circle number 1 if you were not able to
- concentrate at all in the last two weeks.
PART A
Please read each question, think about, and evaluate your feelings, and circle the number of the scale that gives the most appropriate answer to each question.
PART B
The following questions look at the extent to which you have had certain experiences or situations during the last two weeks.
PART C
The following questions look at the extent to which you have had certain experiences or been able to do certain things during the last two weeks.
PART D
The next questions look at how good you felt or how satisfied you have been in various aspects of your life over the past two weeks.
The next question looks at how often you’ve had certain feelings over the past two weeks.
PART E
The following questions address the factors that may affect your well-being in your workplace and the extent to which they are considered important. They relate to general working conditions prevailing over your work environment for the last 6 months.
PART F
The following questions are about your personal beliefs and values and how much they affect your quality of life. Once again, these questions refer to the last two weeks.
PART H
The following questions are about spiritual pursuits that may be affecting your quality of life. These questions refer to religion, spirituality, and any other beliefs you may have. Once again, these questions refer to the last two weeks.
PART G
The last session has two open -ended questions where you can explain your opinions more.
- -
- How long did it take to fill this form out? ………………………….. minutes
- -
- Did someone help you to fill out this form? YES…………NO…………………
Thank you for your participation!
Abbreviations: Health Care Professionals (HCPs), Quality of life (QOL), Principal Component Analysis (PCA).
References
- The WHOQOL Group. The World Health Organization Quality of Life assessment (WHOQOL): Position paper from the World Health Organization. Soc. Sci. Med. 1995, 41, 1403–1409. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Fernández, M. D.; Ortega-Galán, Á. M.; Fernández-Sola, C.; Hernández-Padilla, J. M.; Granero-Molina, J.; Ramos-Pichardo, J.D. Occupational factors associated with health-related quality of life in nursing professionals: A multi-centre study. Int. J. Environ. Res. Public Health 2020, 17, 982. [Google Scholar] [CrossRef] [PubMed]
- Coiro, M.J.; Asraf, K.; Tzischinsky, O.; Hadar-Shoval, D.; Tannous-Haddad, L.; Wolfson, A.R. Sleep quality and COVID-19-related stress in relation to mental health symptoms among Israeli and U.S. adults. Sleep Heal. 2021, 7, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Korkmaz, S.; Kazgan, A.; Çekiç, S.; Tartar, A.S.; Balci, H.N.; Atmaca, M. The anxiety levels, quality of sleep and life and problem-solving skills in healthcare workers employed in COVID-19 services. J. Clin. Neurosci. 2020, 80, 131–136. [Google Scholar] [CrossRef]
- Olagunju, A.T.; Bioku, A.A.; Olagunju, T.O.; Sarimiye, F.O.; Onwuameze, O.E.; Halbreich, U. Psychological distress and sleep problems in healthcare workers in a developing context during COVID-19 pandemic: implications for workplace wellbeing. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 110, 110292. [Google Scholar] [CrossRef]
- Rabiei, M.; Shirani, S.; Sharifi, T. Study the effectiveness of cognitive-behavioral intervention on the quality of life, job satisfaction, and nurses’ organizational performance. J. Clin. Nurs. Midwifery 2018, 4, 3. [Google Scholar]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 12 June 2023).
- Alimoradi, Z.; Brostro, M.A.; Tsang, H.W.H.; Griffiths, M.D.; Haghayegh, S.; Ohayon, M.M.; Lin, C.Y.; Pakpour, A.H. Sleep problems during COVID-19 pandemic and its’ association to psychological distress: A systematic review and meta-analysis. EClinicalMedicine 2021, 36, 100916. [Google Scholar] [CrossRef]
- Jahrami, H.A.; Alhaj, O.A.; Humood, A.M.; Alenezi, A.F.; Fekih-Romdhane, F.; AlRasheed, M.M.; Saif, Z.Q.; Bragazzi, N.L.; Pandi-Perumal, S.R.; et al. Sleep disturbances during the COVID-19 pandemic: A systematic review, meta-analysis, and meta-regression. Sleep Med. Rev. 2022, 62, 101591. [Google Scholar] [CrossRef]
- Patel, B.; Khanpara, B.; Mehta, P.; Patel, K.; Marvania, N. Evaluation of perceived social stigma and burnout, among health-care workers working in covid-19 designated hospital of India: A cross-sectional study. Asian J. Soc. Health Behav. 2021, 4, 156–62. [Google Scholar] [CrossRef]
- Krishnamoorthy, Y.; Nagarajan, R.; Saya, G.K.; Menon, V. Prevalence of psychological morbidities among general population, healthcare workers and COVID-19 patients amidst the COVID-19 pandemic: A systematic review and meta-analysis. Psychiatry Res. 2020, 293, 113382. [Google Scholar] [CrossRef]
- Alimoradi, Z.; Ohayon, M.M.; Griffiths, M.D.; Lin, C.Y.; Pakpour, A.H. Fear of COVID-19 and its association with mental health-related factors: systematic review and meta-analysis. BJPsych Open 2022, 8, e73. [Google Scholar] [CrossRef] [PubMed]
- Aslanidis, V.; Tsolaki, V.; Papadonta, M. E.; Amanatidis, T.; Parisi, K.; Makris, D.; Zakynthinos, E. The Impact of the COVID 19 Pandemic on Mental Health and Quality of Life in COVID 19 Department Healthcare Workers in Central Greece. J. Pers. Med. 2023, 13, 250. [Google Scholar] [CrossRef] [PubMed]
- Dafogianni, C.; Pappa, D.; Koutelekos, I.; Mangoullia, P.; Ferentinou, E.; Margari, N. Stress, anxiety and depression in nurses during COVID-19 pandemic: Evaluation of coping strategies. Int. J. Nurs. 2021, 8, 1–10. [Google Scholar] [CrossRef]
- Cruz, J. Quality of life and its influence on clinical competence among nurses: A self-reported study. J. Clin. Nurs. 2016, 26, 388–399. [Google Scholar] [CrossRef]
- Niu, A.; Li, P.; Duan, P.; Ding, L.; Xu, S.; Yang, Y.; Guan, X.; Shen, M.; Jiang, Y.; Luo, Y. Professional quality of life in nurses on the frontline against COVID-19. J. Nurs. Manag. 2022, 30, 1115–1124. [Google Scholar] [CrossRef]
- Missouridou, E.; Mangoulia, P.; Pavlou, V.; Kritsotakis, E.; Stefanou, E.; Bibou, P.; Kelesi, M.; Fradelos, E. Wounded healers during the COVID-19 syndemic: Compassion fatigue and compassion satisfaction among nursing care providers in Greece. Perspect. Psychiatr. Care 2022, 58, 1422–1432. [Google Scholar] [CrossRef]
- Luceño-Moreno, L.; Talavera-Velasco, B.; García-Albuerne, Y.; Martín-García, J. Symptoms of posttraumatic stress, anxiety, depression, levels of resilience and burnout in spanish health personnel during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 5514. [Google Scholar] [CrossRef]
- Jackson, D.; Firtko, A.; Edenborough, M. Personal resilience as a strategy for surviving and thriving in the face of workplace adversity: A literature review. J Adv. Nurs. 2007, 60, 1–9. [Google Scholar] [CrossRef]
- Santarone, K.; McKenney, M.; Elkbuli, A. Preserving mental health and resilience in frontline healthcare workers during COVID-19. Am. J. Emerg. Med. 2020, 38, 1530. [Google Scholar] [CrossRef]
- Zangeneh Soroush, M.; Tahvilian, P.; Koohestani, S.; Maghooli, K.; Jafarnia Dabanloo, N.J.; Sarhangi Kadijani, M.; Jahantigh, S.; Zangeneh Soroush, M.; Saliani, A. Effects of COVID-19-related psychological distress and anxiety on quality of sleep and life in healthcare workers in Iran and three European countries. Front. Public Health 2022, 10, 997626. [Google Scholar] [CrossRef]
- Abdelghani, M.; Mahdy, R.; El-Gohari, H. Health anxiety to COVID-19 virus infection and its relationship to quality of life in a sample of health care workers in Egypt: A cross-sectional study. Arch. Psychiatry Psychother. 2021, 1, 19–28. [Google Scholar] [CrossRef]
- Antoniadou, M. Quality of life and satisfaction from career and work-life integration of Greek dentists before and during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2022, 19, 9865. [Google Scholar] [CrossRef] [PubMed]
- Antoniadou, M. Estimation of factors affecting burnout in Greek dentists before and during the Covid-19 pandemic. Dent J. 2022, 10, 108. [Google Scholar] [CrossRef] [PubMed]
- Mroczek, B.; Łubkowska, W.; Jarno, W.; Jaraczewska, E.; Mierzecki, A. Occurrence and impact of back pain on the quality of life of healthcare workers. Ann. Agric. Environ. Med. 2020, 27, 36–42. [Google Scholar] [CrossRef]
- Woon, L.S.C.; Mansor, N.S.; Mohamad, M.A.; Teoh, S.H.; Leong Bin Abdullah, M.F.I. Quality of life and Its predictive factors among healthcare workers after the end of a movement lockdown: The salient roles of COVID-19 stressors, psychological experience, and social support. Front. Psychol. 2021, 12, 652326. [Google Scholar] [CrossRef]
- Pfeffer, J. Producing sustainable competitive advantage through effective management of people. Academy Management Exe 2005, 19, b95–108. [Google Scholar] [CrossRef]
- Kowitlawkul, Y.; Yap, S.F; Makabe, S.; Chan, S.; Takagai, J.; Tam, W.W.S. , Nurumal, M.S. Investigating nurses’ quality of life and work-life balance statuses in Singapore. Int. Nurs. Rev. 2019, 66, 61–69. [Google Scholar] [CrossRef]
- Antoniadou, M. Application of the humanities and basic principles of coaching in health sciences. www.ekdoseis-tsotras.gr Athens, 2021.
- Antoniadou, Μ. Quality management in health services. The dental model of quality_Μateriam superabat opus. www.ekdoseis-tsotras.gr, Athens, 2022.
- Antoniadou, M. Leadership and managerial skills in Dentistry: Characteristics and challenges based on a preliminary case study. Dent. J. 2022, 10, 146. [Google Scholar] [CrossRef]
- Upton, D.; Upton, P. Quality of Life and Well-Being. In: Psychology of Wounds and Wound Care in Clinical Practice. Springer: Cham, 2015, pp. 85–111. [CrossRef]
- Baptiste, N.R. Fun and well-being: Insights from senior managers in a local authority. 2009 Empl. Relat. 2009, 31, 600–612. [Google Scholar]
- Grant, A.; Christianson, M.; Price, R. Happiness, health or relationships? Managerial practices and employee well-being tradeoffs. Acad. Manag. Perspect. 2007, 21, 51–63. [Google Scholar] [CrossRef]
- Cvenkel, N. Well-being in the workplace: governance and sustainability insights to promote workplace health. Springer Nature Singapore Pte Ltd, 2020.
- Peccei, R. Human resources management and the search for the happy workplace. Erasmus research institute of management, Rotterdam School of management, Rotterdam school of economics, 2004.
- Chen, P.; Cooper, C. Work and well-being: a complete reference guide (vol III), John Wiley & Sons, 2014.
- Tehrani, N.; Humpage, S.; Willmott, B.; Haslam, I. What’s happening with well-being at work? Change agenda. London: Chartered institute of personnel development, 2007.
- Chechak, D.; Csiernik, R. Canadian perspectives on conceptualizing and responding to workplace violence. J. Workplace Behav. Health 2014, 29, 55–74. [Google Scholar] [CrossRef]
- Poorkvavoos, M. Compassionate leadership: What is it and why do organizations need moreof ot? Research Chapter Roffey Park, 2016. www.roffeypark.com.
- Meechan, F. Compassion at work toolkit. Alliance Manchester Business School, University of Manchester. Available at https://www.researchgate.net/publication/322404395_Compassion_aat_Work_Toolkit. 2018. [Google Scholar]
- CIPD. Health and well-being at work. In partnership with Simply Health, April 2019 championing better work and working lives. London: Chartered Institute of personnel and development. 2019. 20 April.
- Azevedo, W.F.; Mathias, L.A.D.S.T. Work addiction and quality of life: a study with physicians. Einstein (Sao Paulo), 2017, 15, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Caillault, P.; Bourdon, M.; Hardouin, J.B.; Moret, L. How do doctors perceive and use patient quality of life? Findings from focus group interviews with hospital doctors and general practitioners. Qual. Life Res. 2020, 29, 1895–1901. [Google Scholar] [CrossRef] [PubMed]
- Cesar, F.C.R.; Oliveira, L.M.A.C.; Ribeiro, L.C.M.; Alves, A.G.; Moraes, K.L.; Barbosa, M.A. Quality of life of master's and doctoral students in health. Rev. Bras. Enferm. 2021, 74, e20201116. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, S.K. Professional quality of life, burnout and alexithymia. Radiother Oncol. 2021, 155, e5. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, D. Philosophische Grundlagen der Psychologie. Darmstadt: Wissenschaftliche Buchgesellschaft, 1998.
- La qualità di vita conta più della quantità della vita [Quality of life counts more than the quantity of life.]. Recenti Prog Med. 2019, 110, 269–270. [CrossRef]
- Williams, M. Generalization in interpretative research. In T. May (Ed.), Qualitative research in action. London, Sage 2002.
- Development of the World Health Organization WHOQOL-BREF quality of life assessment. The WHOQOL Group. Psychol. Med. 1998, 28, 551–558. [Google Scholar] [CrossRef]
- Skevington, S.M.; Lotfy, M.; O'Connell, K.A. WHOQOL Group. The World Health Organization's WHOQOL-BREF quality of life assessment: psychometric properties and results of the international field trial. A report from the WHOQOL group. Qual. Life Res. 2004, 13, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.C.; Yao, G. Validation of the factor structure of the WHOQOL-BREF using meta-analysis of exploration factor analysis and social network analysis. Psychol. Assess. 2022, 34, 660–670. [Google Scholar] [CrossRef]
- WHOQOL BREF version. Available online: https://www.who.int/tools/whoqol/whoqol-bref.
- WHOQOL-SRPB. (2012 revision, WHOQOL-SRPB)( https://www.who.int/publications/i/item/WHO-MSD-MER-Rev-2012-04).
- Oppenheim, A.N. Questionnaire design interviewing and attitudes measurement (New Ed.). Continuum International: London, 2000.
- Bowling, A. Measuring Disease. A Review of Disease-specific Quality of Life Measurement Scales. Open University Press: Buckingham, 2001.
- Moser, C.; Kalton, G. Survey methods in social investigation (2nd ed.). Gower: Hants, 1992.
- Antoniadou, M.; Chrysochoou, G.; Tzanetopoulos, R.; Riza, E. Green Dental Environmentalism among Students and Dentists in Greece. Sustainability 2023, 15, 9508. [Google Scholar] [CrossRef]
- Haworth, J.; Hart, G. Wellbeing: individual, community and social perspectives. Palgrave MacMillan: Basingstoke, 2007.
- Silcox, S. Health work and well-being: rising to the public sector attendance management challenge. ACAS policy discussion paper, 2007, 6.
- Silverman, D. Interpreting qualitative data: methods for analysing talk, text and interaction. Sage: London, 1993.
- O’Donnell, M.; Shields, J. Performance management and the psychological contract in the Australian federal public sector. J. Industrial. Rel. 2002, 44, 435–457. [Google Scholar] [CrossRef]
- Noblet, A.J.; Rodwell, J.J. Integrating job stress and social exchange theories to predict employee strain in reformed public sector contexts. J. Public Admin. Res. Theory Adv. Acc. 2009, 19, 555–624. [Google Scholar] [CrossRef]
- Whitfield, K. (Ed). Employee well-being and working life: towards an evidence based policy agenda. An ESRC/HSE public policy project, report on a public policy seminar held at HSEE, London, 2009.
- Saunders, M.; Lewis, P.; Thornhill, A. research methods for business students (5th ed.). Pearson Education, Financial Times, Prentice Hall: London, 2009.
- George, D.; Mallery, P. IBM SPSS Statistics 25 Step by Step: A Simple Guide and Reference (15th ed.). Routledge: New York, 2019.
- Field, A. Discovering Statistics Using IBM SPSS Statistics Ed. 5. SAGE Publications, 2017.
- Ghazy, R.M.; Abubakar Fiidow, O.; Abdullah, F.S.A.; Elbarazi, I.; Ismail, I.I.; Alqutub, S.T.; Bouraad, E.; Hammouda, E.A.; Tahoun, M.M.; Mehdad, S.; Ashmawy, R.; Zamzam, A.; Elhassan, O.M.; Al Jahdhami, Q.M.; Bouguerra, H.; Kammoun Rebai, W.; Yasin, L.; Jaradat, E.M.; Elhadi. Y.A.M.; Sallam, M. Quality of life among health care workers in Arab countries 2 years after COVID-19 pandemic. Front. Public Health 2022, 10, 917128. [Google Scholar] [CrossRef] [PubMed]
- Teles, M.A.B.; Barbosa, M.R.; Vargas, A.M.D.; Gomes, V.E.; Ferreira, E.F.; Martins, A.M.E.; Ferreira, R.C. Psychosocial work conditions and quality of life among primary health care employees: a cross sectional study. Health Qual. Life Outcomes 2014, 12, 72. [Google Scholar] [CrossRef] [PubMed]
- de Boer, A.G.; Geuskens, G.A.; Bültmann, U.; Boot, C.R.; Wind, H.; Koppes, L.L.; Frings-Dresen, M.H.W. Employment status transitions in employees with and without chronic disease in the Netherlands. Int. J. Public Health 2018, 63, 713–22. [Google Scholar] [CrossRef]
- Mangoulia, P. The influence of secondary traumatic stress on the productivity of health professionals focus on ICU and psychiatric nurses. 2011, Doctoral Dissertation. Faculty of Nursing, National and Kapodistrian University of Athens, Greece. Available online: http://hdl.handle.net/10442/hedi/26088 (accessed 6 September 2023).
- Kua, Z.; Hamzah, F.; Tan, P.T.; Ong, L.J.; Tan, B.; Huang, Z. Physical activity levels and mental health burden of healthcare workers during COVID-19 lockdown. Stress Health 2022, 38, 171–179. [Google Scholar] [CrossRef]
- Teixeira, C.F.S.; Soares, C.M.; Souza, E.A.; Lisboa, E.S.; Pinto, I.C.M.; Andrade, L.R.; Espiridião, M.A. The health of healthcare professionals coping with the Covid-19 pandemic. Cien. Saude. Colet. 2020, 25, 3465–3474. [Google Scholar] [CrossRef] [PubMed]
- Soo, S.Y.; Ang, W.S.; Chong, C.H.; Tew, I.M.; Yahya, N.A. Occupational ergonomics and related musculoskeletal disorders among dentists: A systematic review. Work 2023, 74, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Garzaro, G.; Clari, M.; Ciocan, C.; Albanesi, B.; Guidetti, G.; Dimonte, V.; Sottimano, I. Physical Health and Work Ability among Healthcare Workers. A Cross-Sectional Study. Nurs. Rep. 2022, 12, 259–269. [Google Scholar] [CrossRef]
- Hawlader, M.D.H.; Rashid, M.U.; Khan, M.A.S.; Ara, T.; Nabi, M.H.; Haque, M.M.A.; Matin, K.F.; Hossain, M.A.; Rahman, M.A.; Hossian, M.; Saha, S.; Manna, R.M.; Arafat, M.Y.; Barsha, S.Y.; Maliha, R.; Khan, J.Z.; Kha, S.; Hasan, S.M.R.; Hasan, M.; Siddiquea, S.R.; Khan, J.; Islam, A.M.K.; Rashid, R.; Nur, N.; Khalid, O.; Bari, F.; Rahman, M.L. Quality of life of COVID-19 recovered patients in Bangladesh. PLoS ONE 2021, 16, e0257421. [Google Scholar] [CrossRef]
- Suryavanshi, N.; Kadam, A.; Dhumal, G.; Nimkar, S.; Mave, V.; Gupta, A.; Cox, S.R.; Gupte, N. Mental health and quality of life among healthcare professionals during the COVID-19 pandemic in India. Brain Behav. 2020, 10(11), e01837. [Google Scholar] [CrossRef]
- Zhang, Y.; Yan, L.; Long, H.; Yan, L.; Wang, J.; Liu, Y.; Pu, J.; Liu, L.; Zhong, X.; Jin, X. Occupational Differences in Psychological Distress Between Chinese Dentists and Dental Nurses. Front. Psychol. 2022, 13, 923626. [Google Scholar] [CrossRef] [PubMed]
- Di Tella, M.; Romeo, A.; Benfante, A.; Castelli, L. Mental health of healthcare workers during the COVID-19 pandemic in Italy. J. Eval. Clin. Pract. 2020, 26, 1583–1587. [Google Scholar] [CrossRef] [PubMed]
- Omidi, Z.; Khanjari, S.; Saleji, T.; Haghani, S. Association between burnout and nurses’ quality of life in neonatal intensive care units: During the COVID-19 pandemic. J. Neonatal Nurs. 2023, 29, 144–148. [Google Scholar] [CrossRef] [PubMed]
- Hilton, M.F.; Whiteford, H.A.; Sheridan, J.S.; Cleary, C.M.; Chant, D.C.; Wang, P.S. The prevalence of psychological distress in employees and associated occupational risk factors. J. Occ. Environm. Med. 2008, 50, 746–757. [Google Scholar] [CrossRef] [PubMed]
- Wilson, F. Organizational behaviour and work: a critical introduction. Oxford: Oxford University Press, 2010.
- Ryff, C.; Singer, B. Psychological well-being: meaning, measurement and implications for psychotherapy research. Psychother. Psychosom. 1996, 65, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Veenstra, M.; Gautun, H. Nurses' assessments of staffing adequacy in care services for older patients following hospital discharge. J. Adv. Nurs. 2021, 77, 805–818. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, P.; Ball, J.; Drennan, J.; Dall'Ora, C.; Jones, J.; Maruotti, A.; Pope, C.; Recio Saucedo, A.; Simon, M. Nurse staffing and patient outcomes: Strengths and limitations of the evidence to inform policy and practice. A review and discussion paper based on evidence reviewed for the National Institute for Health and Care Excellence Safe Staffing guideline development. Int. J. Nurs. Studies, 2016, 63, 213–225. [Google Scholar] [CrossRef]
- Glette, M. K.; Roise, O.; Kringeland, T.; Churruca, K.; Braithwaite, J.; Wiig, S. Nursing home leaders' and nurses' experiences of resources, staffing and competence levels and the relation to hospital readmissions – A case study. BMC Health Serv. Res., 2018, 18, 955. [Google Scholar] [CrossRef]
- Belling, R.; Whittock, M.; McLaren, S.; Burns, T.; Catty, J.; Jones, I.; R. ; Rose, D.; Wykes, T. ECHO Group. Achieving continuity of care: Facilitators and barriers in community mental health teams. Implement. Sci., 2011, 6, 23. [Google Scholar] [CrossRef]
- Koopmans, L.; Damen, N.; Wagner, C. Does diverse staff and skill mix of teams impact quality of care in long-term elderly health care? An exploratory case study. BMC Health Serv. Res. 2018, 18, 988. [Google Scholar] [CrossRef]
- Dubois, C.A.; Singh, D. From staff-mix to skill-mix and beyond: Towards a systemic approach to health workforce management. Human Resources for Health 2009, 19, 87. [Google Scholar] [CrossRef] [PubMed]
- Bing-Jonsson, P.C.; Foss, C.; Bjørk, I. T. (2016). The competence gap in community care: Imbalance between expected and actual nursing staff competence. Nord. J. Nurs. Res., 2016, 36, 27–37. [Google Scholar] [CrossRef]
- Mangoulia, P.; Koukia, E.; Alevizopoulos, G.; Fildissis, G.; Katostaras, T. Prevalence of Secondary Traumatic Stress Among Psychiatric Nurses in Greece. Arch Psychiatr Nurs 2015, 29, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, S.P. , Adair, K.C.; Bae, J.; Rehder, K.J.; Shanafelt, T.D.; Profit, J.; Sexton, J.B. Work-life balance behaviours cluster in work settings and relate to burnout and safety culture: a cross-sectional survey analysis. BMJ Qual. Saf. 2019, 28, 142–150. [Google Scholar] [CrossRef]
- Bodendieck, E.; Jung, F.U.; Conrad, I.; Riedel-Heller, S.J.; Hussenoeder, F. The work-life balance of general practitioners as a predictor of burnout and motivation to stay in the profession. BMC Prim. Care 2022, 23, 218. [Google Scholar] [CrossRef]
- Pulcrano, M.; Evans, S.R.; Sosin, M. Quality of Life and Burnout Rates Across Surgical Specialties: A Systematic Review. JAMA Surg. 2016, 151, 970–978. [Google Scholar] [CrossRef]
- Shivakumar, K.; Pujar, V. Work Life Balance in the Health Care Sector. Amity J. Healthc. Manag. 2016, 1, 45–54. [Google Scholar] [CrossRef]
- White, M.; Hill, S.; McGovern, P.; Mills, C.; Smeaton, D. High performance management practices, working hours and work-life balance. Br. J. Ind. Relations 2003, 4, 175–195. [Google Scholar] [CrossRef]
- Wiig S, Fahlbruch B, editors. Exploring resilience: a scientific journey from practice to theory. Springer Open: Cham, 2019.
- Haraldstad, K.; Wahl, A.; Andenæs, R.; Andersen, J.R.; Beisland, E.; Borge, C.R.; Engebretsen, M; Eisemann, L.; Halvorsrud, T.A.; Hanssen, A.; et al. Helseth A systematic review of quality of life research in medicine and health sciences. Qual Life Res. 2019, 28, 2641–50. [Google Scholar] [CrossRef]
- Parida, S.; Aamir, A.; Alom, J.; Rufai, T.A.; Rufai, S.R. British doctors' work-life balance and home-life satisfaction: A cross-sectional study. Postgrad Med. J. 2023, 19, 198–206. [Google Scholar] [CrossRef]
- Michel, J.S.; Kotrba, L.M.; Mitchelson, J.K. Antecedents of work-family conflict: a meta-analytic review. J. Organ. Behav. 2011, 32, 689–725. [Google Scholar] [CrossRef]
- Schell, E.; Theorell, T.; Saraste, H. Workplace aesthetics: Impact of environments upon employee health? Work 2011, 39(3), 203–13. [Google Scholar] [CrossRef] [PubMed]
- Pinch, W.J.E. Confidentiality: concept analysis and clinical application. Nurs. Forum 2000, 35, 5–16. [Google Scholar] [CrossRef] [PubMed]
- Badzek, L.; Gross, L. Confidentiality, and privacy: at the forefront for nurses. Am. J. Nurs. 1999, 99, 52–54. [Google Scholar] [CrossRef]
- Heikkinen, A.; Launis, V.; Wainwright, P.; Leino-Kilpi, H. Privacy and occupational health services. J. Med. Ethics. 2006, 32, 522–525. [Google Scholar] [CrossRef]
- Antoniadou, M.; Tziovara, P.; Antoniadou, C. The Effect of Sound in the Dental Office: Practices and Recommendations for Quality Assurance—A Narrative Review. Dent. J. 2022, 10, 228. [Google Scholar] [CrossRef]
- Youssef, C.M.; Luthans, F. Positive organizational behavior in the workplace: The impact of hope, optimism, and resilience. Journal of Management 2007, 33, 774–800. [Google Scholar] [CrossRef]
- Cho, J.; Laschinger, H.K.S.; Wong, C. Workplace empowerment, work engagement and organizational commitment of new graduate nurses. Nurs. Leadersh. (Tor Ont), 2006, 19, 43–60. [Google Scholar] [CrossRef]
- Bosch, G. Towards a new standard employment relationship in Western Europe. Br. J. Industrial Relations 2004, 42, 617–636. [Google Scholar] [CrossRef]
- Waldinger, R.; Schulz, M.; Waldinger, R.; Schulz, M. Harvard study of adult development. https://www.adultdevelopmentstudy.
- Puciato, D.; Rozpara, M.; Bugdol, M. Socio-economic correlates of quality of life in single and married urban individuals: a Polish case study. Health Qual. Life Outcomes 2022, 20, 58. [Google Scholar] [CrossRef]
- Borges, C.C.; dos Santos, P.R.; Alves, P.M.; Borges, R.C.M.; Lucchetti, G.; Barbosa, M.A.; Porto, C.C.; Fernandes, M.R. Association between spirituality/ religiousness and quality of life among healthy adults: a systematic review. Health Qual Life Outcomes 2021, 19, 246. [Google Scholar] [CrossRef]
- Ibrahim, N.K.; Alzahrani, N.A.; Batwie, A.A.; Abushal, R.A.; Almograti, G.G.; Sattam, M.A.; Hussin, B.K. Quality of life, job satisfaction and their related factors among nurses working in king Abdulaziz University Hospital, Jeddah, Saudi Arabia. Contemp. Nurse 2016, 52, 486–498. [Google Scholar] [CrossRef]
- Barmanpek, N.K.; Şahin, A.; Demirel, C.; Kiliç, S.P. The relationship between nurses’ job satisfaction levels and quality of life. Perspect Psychiatr Care 2022, 58, 2310–2320. [Google Scholar] [CrossRef]
- Cruz, J.P.; Alquwez, N.; Mesde, J.H.; Almoghairi, A.M.A.; Altukhays, A.I.; Colet, P.C. Spiritual climate in hospitals influences nurses' professional quality of life. J. Nurs. Manag. 2020, 28, 1589–1597. [Google Scholar] [CrossRef]
- Joseph, B.; Joseph, M. The health of the healthcare workers. Indian J. Occup. Environ. Med. 2016, 20, 71–72. [Google Scholar] [CrossRef]
- Matos, M.; McEwan, K.; Kanovský, M.; Halamová, J.; Steindl, S.R.; Ferreira, N.; Linharelhos, M.; Rijo, D.; Asano, K.; et al. Fears of compassion magnify the harmful effects of threat of COVID-19 on mental health and social safeness across 21 countries. Clin. Psychol. Psychother. 2021, 28, 1317–1333. [Google Scholar] [CrossRef]
- Missouridou, E.; Mangoulia, P.; Pavlou, V.; Kritsotakis, E.; Stefanou, E.; Bibou, P.; Kelesi, M.; Fradelos, E.C. Wounded healers during the COVID-19 syndemic: Compassion fatigue and compassion satisfaction among nursing care providers in Greece. Perspect. Psychiatr. Care 2022, 58, 1421–1432. [Google Scholar] [CrossRef]
- Penconek, T.; Tate, K.; Bernardes, A.; Lee, S.; Micaroni, S.P.M.; Balsanelli, A.P.; de Moura, A.A.; Cummings, G.G. Determinants of nurse manager job satisfaction: A systematic review. Int. J. Nurs. Stud. 2021, 118, 103906. [Google Scholar] [CrossRef] [PubMed]
- Benham-Clarke, S.; Ewing, J.; Barlow, A.; Newlove-Delgado, T. Learning how relationships work: a thematic analysis of young people and relationship professionals’ perspectives on relationships and relationship education. BMC Public Health 2022, 22, 2332. [Google Scholar] [CrossRef]
- Han, K.T.; Park, E.C.; Kim, J.H.; Park, S. Is marital status associated with quality of life? Health Qual. Life Outcomes 2014, 12, 109. [Google Scholar] [CrossRef]
- Suryavanshi, N.; Kadam, A.; Dhumal, G.; Nimkar, S.; Mave, V.; Gupta, A.; Cox, S.R.; Gupte, N. Mental health and quality of life among healthcare professionals during the COVID-19 pandemic in India. Brain Behav. 2020, 10, e01837. [Google Scholar] [CrossRef] [PubMed]
- Achangwa, C.; Lee, T.J.; Park, J.; Lee, M.S. Quality of life and associated factors of international students in South Korea: A cross-sectional study using the WHOQOL-BREF instrument. Healthcare 2022, 10, 1262. [Google Scholar] [CrossRef] [PubMed]
- Webometrics Ranking Web of Universities, 2023. Available online: https://www.webometrics.info/en/world. (accessed on 6 September 2023).
- Diener, E. Assessing subjective wellbeing. Progress and opportunities. Social Indicators Res. 1994, 31, 103–157. [Google Scholar] [CrossRef]
Figure 1.
Domains of well-being in workplace according to review analysis.
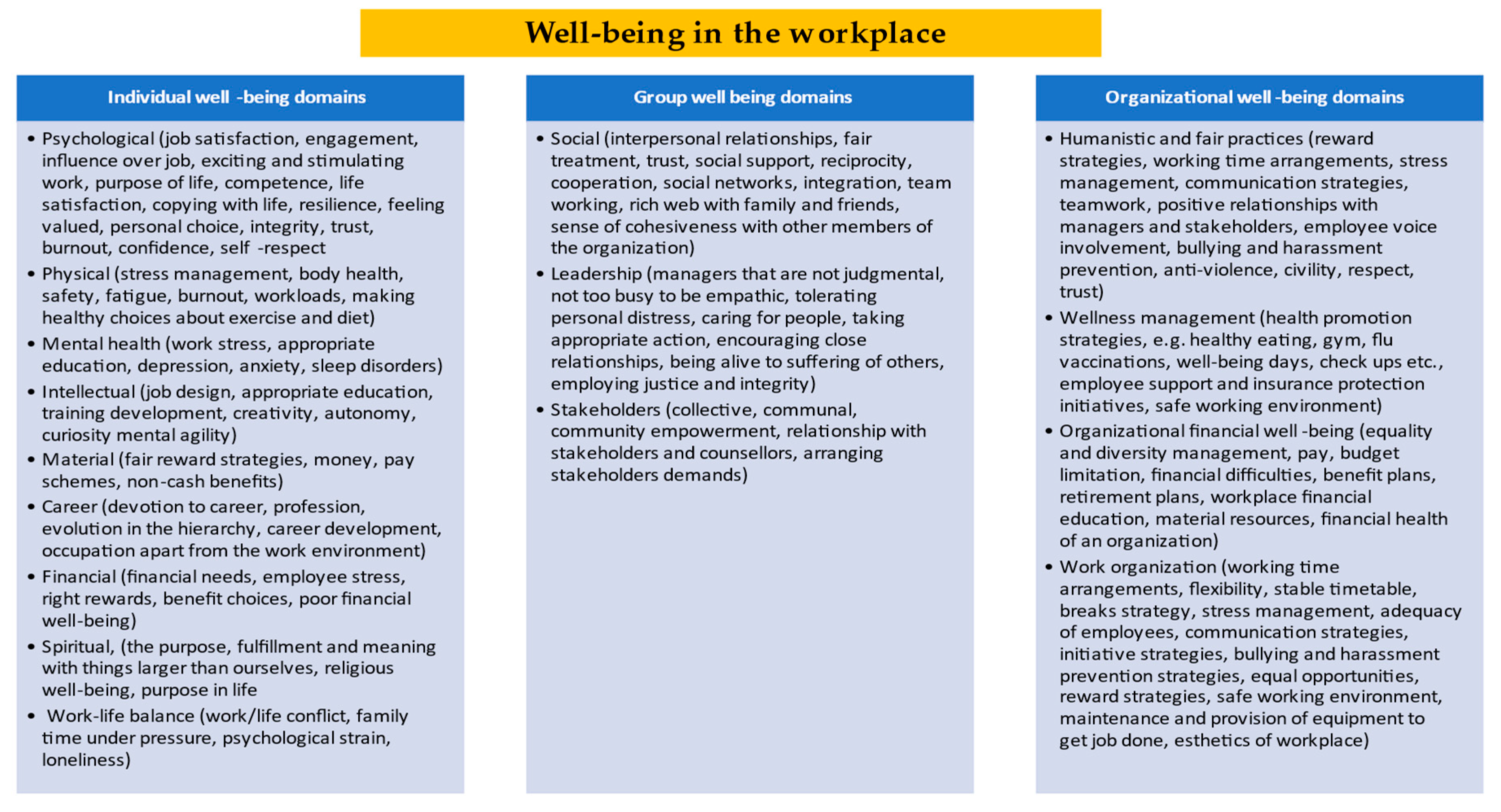
Figure 2.
Domains of WHOQOL-BREF [Physical (pain & discomfort, energy and fatigue, sleep and rest, mobility, activities of daily life, medication, working capacity), Psychological (positive feelings, thinking, memory, concentration, self-esteem, body image and appearance,negative feelings, spirituality), social relationships (personal relationships, social support, sexual activity), environment (physical safety and security, home environment, financial rsources, availiability and quality of health and social care,information access, leisyre, physical environment, transportation)], and WHOQOL-SRPB [Spirituality (spirituality, religion, personal beliefs)].
Figure 2.
Domains of WHOQOL-BREF [Physical (pain & discomfort, energy and fatigue, sleep and rest, mobility, activities of daily life, medication, working capacity), Psychological (positive feelings, thinking, memory, concentration, self-esteem, body image and appearance,negative feelings, spirituality), social relationships (personal relationships, social support, sexual activity), environment (physical safety and security, home environment, financial rsources, availiability and quality of health and social care,information access, leisyre, physical environment, transportation)], and WHOQOL-SRPB [Spirituality (spirituality, religion, personal beliefs)].
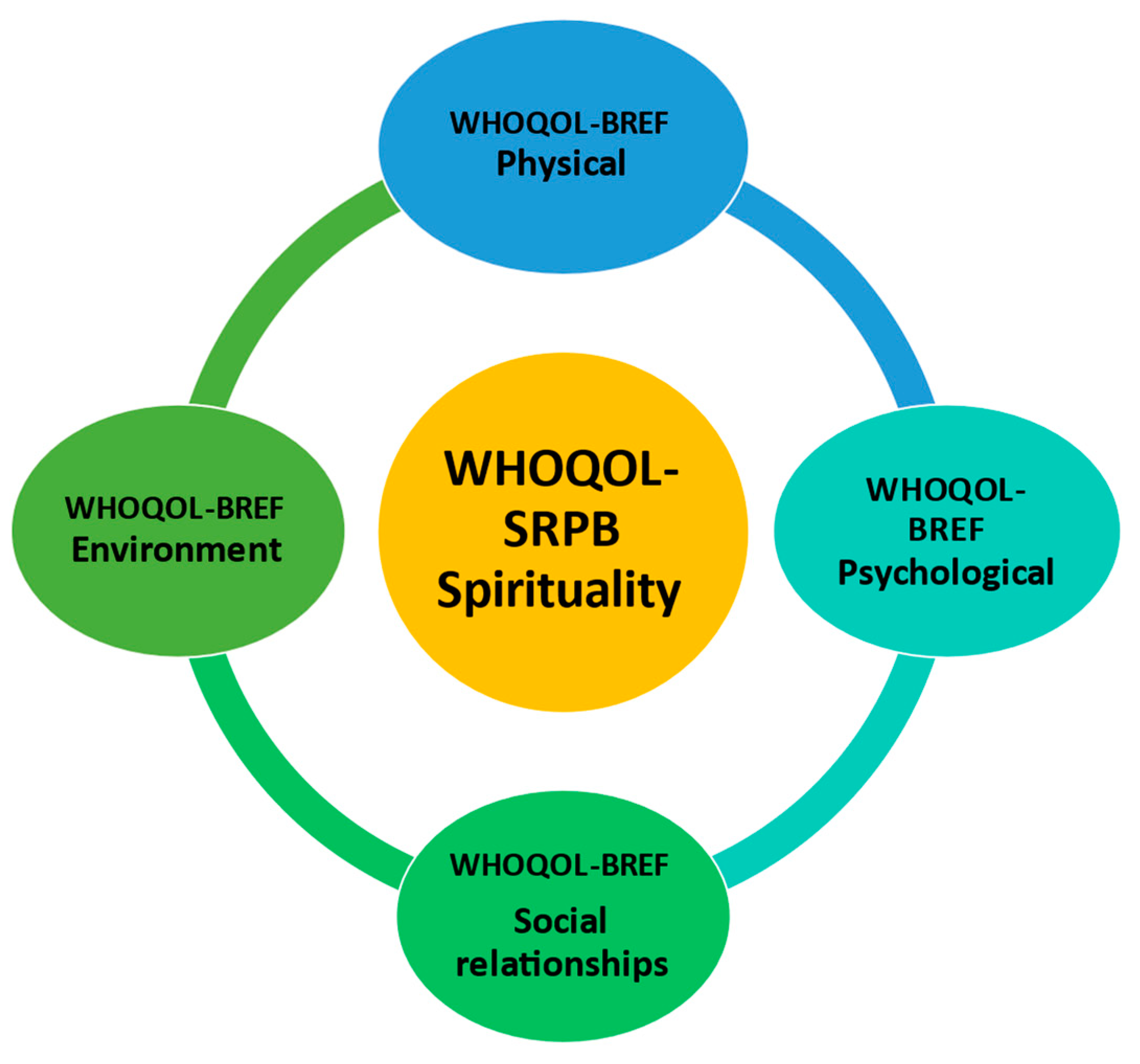
Figure 3.
Procedure followed for the design of the study questionnaire.
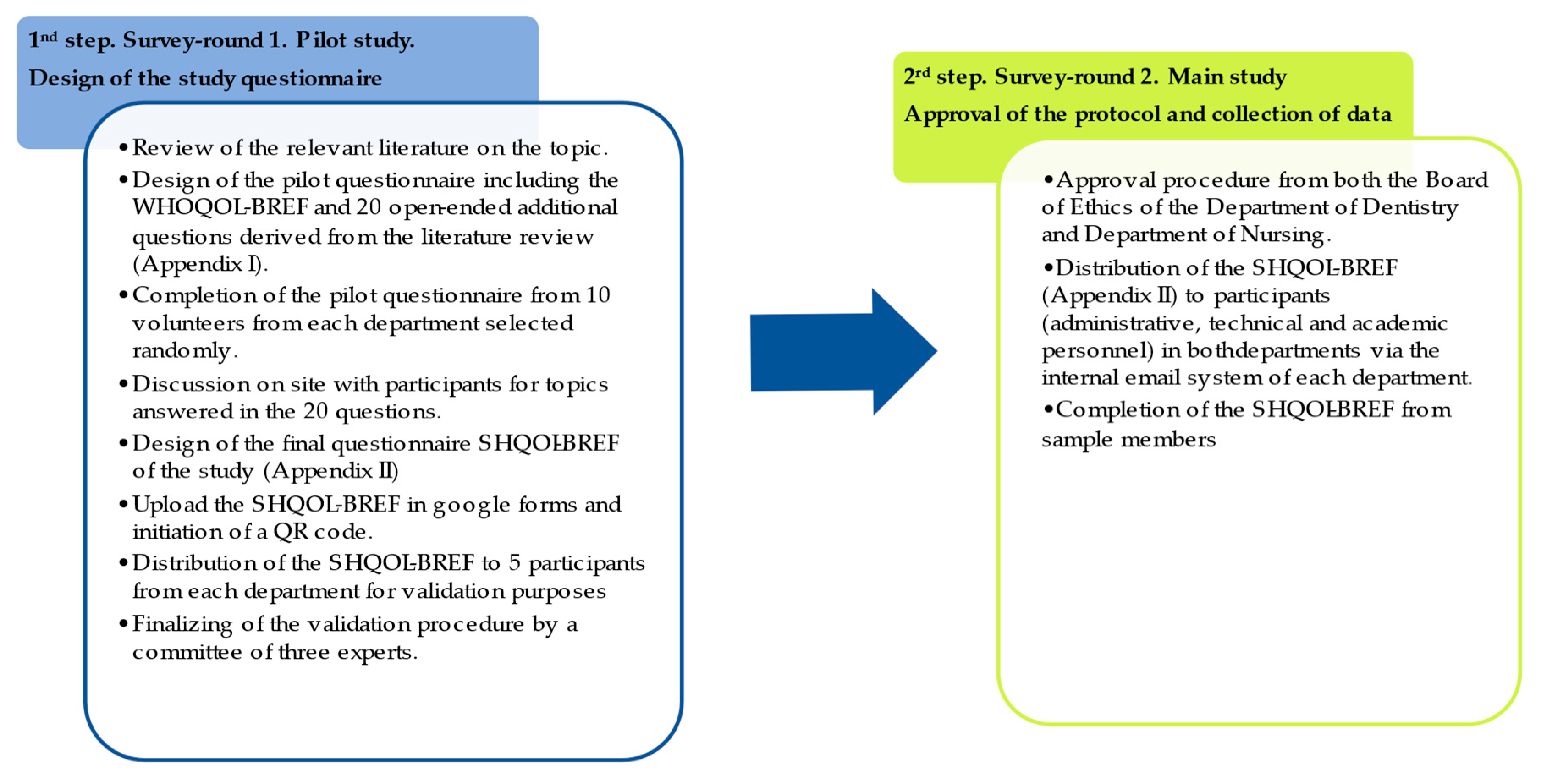

Table 1.
Demographic characteristics of the study sample (N=120).
| Ν | % | ||
|---|---|---|---|
| Gender | Male | 30 | 25.0% |
| Female | 90 | 75.0% | |
| Age | Up to 30 years old | 41 | 34.2% |
| 31-40 | 29 | 24.2% | |
| 41-50 | 18 | 15.0% | |
| 51-60 | 24 | 20.0% | |
| 61 and above | 8 | 6.7% | |
| Marital status | Single | 54 | 45.0% |
| Living like married | 11 | 9.2% | |
| Married | 49 | 40.8% | |
| Widowed | 1 | 0.8% | |
| Divorced | 5 | 4.2% | |
| Number of children | No children | 75 | 62.5% |
| 1-2 children | 43 | 35.8% | |
| 3-4 children | 2 | 1.7% | |
| Education | Secondary (high school, technical school) | 9 | 7.5% |
| Tertiary (Bachelor) | 35 | 29.2% | |
| Postgraduate (Master) | 48 | 40.0% | |
| Ph.D | 28 | 23.3% | |
| Job position | IDAX administrative staff (administrative) | 8 | 6.7% |
| Administrative staff IDOH (administrative) | 7 | 5.8% | |
| Research Associates (Unpaid) (scientific) | 6 | 5.0% | |
| Research Associates (paid) (scientific) | 2 | 1.7% | |
| Faculty members (scientific) | 25 | 20.8% | |
| Postgraduate students (scientific) | 68 | 56.7% | |
| EIB staff (technical) | 1 | 0.8% | |
| Technical staff IDOH (technical) | 3 | 2.5% | |
| Work experience | 1-10 years | 50 | 42.7% |
| 10-20 years | 34 | 29.1% | |
| 21-30 years | 20 | 17.1% | |
| Over 31 | 13 | 11.1% | |
| Department | Nursing | 67 | 55.8% |
| Dentistry | 53 | 44.2% | |
| Non- academic professional activity | sole proprietorship with more than 2 employees | 6 | 5.0% |
| sole proprietorship | 5 | 4.2% | |
| sole proprietorship with one employee | 11 | 9.2% | |
| I don't know/I don't answer | 17 | 14.2% | |
| I do not maintain a professional activity outside of academic hours | 26 | 21.7% | |
| company (member or director) | 9 | 7.5% | |
| hospital employment | 40 | 33.3% | |
| provision of services without an individual seat | 6 | 5.0% | |
| Annual family income | under 15,000 euros | 47 | 42.0% |
| 15,001-25,000 euros | 30 | 26.8% | |
| 25,001-50,000 euros | 25 | 22.3% | |
| 50,001-100,000 euros | 9 | 8.0% | |
| 100,001 and above euros | 1 | 0.9% | |
Table 2.
Working conditions item loadings in the respective component of working conditions.
| Component | |||
|---|---|---|---|
| Working conditions and benefits | Work relationships, rewards, and compensation | Workspace and nature of work | |
| Possibility of a half hour break for food | .867 | ||
| Possibility of a break in a suitable place | .845 | ||
| Possibility of receiving healthy meals | .744 | ||
| Flexibility of working hours | .727 | ||
| Possibility of babysitting | .668 | ||
| Working hours compliance | .616 | ||
| Possibility of continuing education in the same area | .607 | ||
| Ability to socialize with colleagues | .569 | ||
| Spaces for exercise, relaxation, or meditation | .569 | ||
| Appreciation and recognition from superiors | .800 | ||
| Business relations | .798 | ||
| Reward from superiors | .773 | ||
| Support system from colleagues or mentors | .658 | ||
| Equality in development and treatment | .536 | ||
| Noise | .515 | ||
| Salary | .508 | ||
| Workplace aesthetics | .832 | ||
| Work creativity | .805 | ||
| Feeling of giving | .747 | ||
| Space comfort | .701 | ||
* 1. Extraction Method: Principal Component Analysis, Rotation Method: Varimax with Kaiser Normalization, 2. The items Respect from superiors, Respect from colleagues and Possibility of temperature adjustments in the space have been removed because they loaded on more than one component.
Table 3.
Descriptive statistics and reliability indicators of the study variables.
| N items | Cronbach’s a | M | SD | Median | Skewness | Kurtosis | |
|---|---|---|---|---|---|---|---|
| QoL Domain Scores (0-100) | |||||||
| 1. Physical health | 7 | .736 | 72.17 | 15.75 | 75.00 | -0.545 | -0.213 |
| 2. Psychological health | 5 | .741 | 64.58 | 15.31 | 66.67 | -0.616 | 0.221 |
| 3. Social relationships | 3 | .847 | 68.89 | 24.08 | 75.00 | -0.813 | 0.014 |
| 4. Environment | 8 | .756 | 58.72 | 15.54 | 59.38 | -0.359 | -0.176 |
| Overall QoL | 1 | - | 65.63 | 18.64 | 75.00 | -0.501 | 0.713 |
| Satisfaction from health | 1 | - | 72.08 | 22.96 | 75.00 | -0.493 | -0.233 |
| Working conditions and benefits | 9 | .891 | 3.21 | .90 | 3.33 | -0.324 | -0.579 |
| Work relationships, rewards, and compensation | 7 | .840 | 3.42 | .76 | 3.57 | -0.563 | -0.104 |
| Workspace and nature of work | 4 | .869 | 3.64 | .82 | 3.75 | -0.765 | 0.759 |
| Job satisfaction | 4 | .829 | 3.17 | .97 | 3.25 | -0.122 | -0.747 |
| Personal beliefs and values | 4 | .818 | 4.04 | .62 | 4.00 | -0.500 | 0.889 |
| Spirituality | 6 | .621 | 3.01 | .70 | 3.08 | -0.273 | -0.059 |
Table 4.
Pearson correlation coefficients between study variables.
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Physical health | -- | |||||||||
| 2. Psychological health | .652** | -- | ||||||||
| 3. Social relationships | .544** | .464** | -- | |||||||
| 4. Environment | .673** | .605** | .511** | -- | ||||||
| 5. Working conditions and benefits | 0.066 | 0.059 | .217* | -0.044 | -- | |||||
| 6. Work relationships, rewards, and compensation | 0.007 | 0.024 | 0.172 | -0.018 | .473** | -- | ||||
| 7. Workspace and nature of work | 0.158 | 0.176 | .293** | 0.134 | .539** | .557** | -- | |||
| 8. Job satisfaction | .377** | 0.17 | .319** | .504** | 0.077 | -0.002 | 0.142 | -- | ||
| 9. Personal beliefs and values | .332** | .595** | .304** | .282** | .234* | 0.145 | .377** | 0.113 | -- | |
| 10. Spirituality | 0.108 | .262** | 0.132 | .223* | .194* | .321** | .324** | .221* | .418** | -- |
Table 5.
MANOVA results of tests of Between-Subjects Effects of gender, age, marital status, department and education level on QoL domains.
Table 5.
MANOVA results of tests of Between-Subjects Effects of gender, age, marital status, department and education level on QoL domains.
| Source | Dependent Variable | Type III SS | Df | MSE | F | p | η2p |
|---|---|---|---|---|---|---|---|
| Corrected Model | Physical health | 2863.914a | 8 | 357.99 | 1.56 | 0.148 | 0.11 |
| Psychological health | 4547.003b | 8 | 568.38 | 2.74 | 0.009 | 0.18 | |
| Social relationships | 11181.755c | 8 | 1397.72 | 2.68 | 0.010 | 0.18 | |
| Environment | 4036.145d | 8 | 504.52 | 2.52 | 0.016 | 0.17 | |
| Intercept | Physical health | 361283.10 | 1 | 361283.10 | 1570.91 | <.001 | 0.94 |
| Psychological health | 295091.40 | 1 | 295091.40 | 1420.64 | <.001 | 0.94 | |
| Social relationships | 293787.22 | 1 | 293787.22 | 563.79 | <.001 | 0.85 | |
| Environment | 243657.41 | 1 | 243657.41 | 1216.65 | <.001 | 0.93 | |
| Gender | Physical health | 39.61 | 1 | 39.61 | 0.17 | 0.679 | 0.00 |
| Psychological health | 118.42 | 1 | 118.42 | 0.57 | 0.452 | 0.01 | |
| Social relationships | 763.33 | 1 | 763.33 | 1.47 | 0.229 | 0.02 | |
| Environment | 447.38 | 1 | 447.38 | 2.23 | 0.138 | 0.02 | |
| Age | Physical health | 1995.74 | 3 | 665.25 | 2.89 | 0.039 | 0.08 |
| Psychological health | 1187.74 | 3 | 395.91 | 1.91 | 0.134 | 0.06 | |
| Social relationships | 2802.83 | 3 | 934.28 | 1.79 | 0.154 | 0.05 | |
| Environment | 1681.32 | 3 | 560.44 | 2.80 | 0.044 | 0.08 | |
| Marital status | Physical health | 291.79 | 1 | 291.79 | 1.27 | 0.263 | 0.01 |
| Psychological health | 659.86 | 1 | 659.86 | 3.18 | 0.078 | 0.03 | |
| Social relationships | 5032.72 | 1 | 5032.72 | 9.66 | 0.002 | 0.09 | |
| Environment | 190.44 | 1 | 190.44 | 0.95 | 0.332 | 0.01 | |
| Department | Physical health | 139.89 | 1 | 139.89 | 0.61 | 0.437 | 0.01 |
| Psychological health | 0.88 | 1 | 0.88 | 0.00 | 0.948 | 0.00 | |
| Social relationships | 2659.13 | 1 | 2659.13 | 5.10 | 0.026 | 0.05 | |
| Environment | 128.29 | 1 | 128.29 | 0.64 | 0.425 | 0.01 | |
| Education | Physical health | 794.56 | 2 | 397.28 | 1.73 | 0.183 | 0.03 |
| Psychological health | 1553.88 | 2 | 776.94 | 3.74 | 0.027 | 0.07 | |
| Social relationships | 1061.42 | 2 | 530.71 | 1.02 | 0.365 | 0.02 | |
| Environment | 888.58 | 2 | 444.29 | 2.22 | 0.114 | 0.04 | |
| Error | Physical health | 22308.40 | 97 | 229.984 | |||
| Psychological health | 20148.52 | 97 | 207.717 | ||||
| Social relationships | 50545.84 | 97 | 521.091 | ||||
| Environment | 19426.14 | 97 | 200.269 | ||||
| Total | Physical health | 581403.06 | 106 | ||||
| Psychological health | 465746.52 | 106 | |||||
| Social relationships | 549652.77 | 106 | |||||
| Corrected total | Environment | 394560.54 | 106 | ||||
| Physical health | 25172.31 | 105 | |||||
| Psychological health | 24695.52 | 105 | |||||
| Social relationships | 61727.59 | 105 | |||||
| Environment | 23462.28 | 105 |
a R2= .114 (Adj. R2= .041), b R2= .184 (Adj. R2= .117), c R2= .181 (Adj. R2= .114), d R2= .172 (Adj. R2= .104).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



