
Submitted:
30 August 2023
Posted:
30 August 2023
You are already at the latest version
Abstract
Psychological readiness following Anterior Cruciate ligament Reconstruction (ACLR) correlates with different return to sport outcomes. However, the relationship between strength and power and psychological readiness remains unexplored. The aim of this study was to investigate the relationship between the Anterior Cruciate Ligament Return to Sport After Injury (ACL-RSI) scores and various hamstrings and quadriceps strength and power variables. Twelve participants (20.7±2.5 years old; 174.2±7.5 cm; 70.2±8.5 kg; 18.2±8.3% of body fat) who had an ACLR nine months or more before the study completed the ACL-RSI questionnaire and isokinetic strength testing of the hamstrings and quadriceps (60°.s-1 and 180°.s-1). Based on ACL-RSI scores, they were divided into “cases” and “controls”, deemed not psychologically ready and psychologically ready to return to previous sport performance (PILOS), respectively. The main findings are that quadriceps’ and hamstrings’ rate of torque development (RTD) and time since surgery were determinants of psychological readiness following ACLR. Furthermore, compared to controls cases showed significantly lower angle-specific quadriceps and hamstrings torque close to extension and lower RTD, but no difference in peak torque. These results suggest that physiotherapists should facilitate athletes’ RTS by focusing on the restoration of RTD and strength at angles close to full knee extension.
Keywords:
angle-specific torque
; rate of force development
; time since surgery
; rehabilitation
Introduction
Anterior Cruciate Ligament Injury (ACLI) is a common and incapacitating knee injury often sustained during sport participation and treated with ACL reconstruction (ACLR) followed by rehabilitation [1]. Return to sport (RTS) following ACLR is a major concern, with 73% of athletes able to participate in sport at some point following surgery, but only 49% returning to their pre-injury level of sport (PILOS), [2].
While the reasons behind which an athlete may not resume participation to their PILOS is multifactorial, the role played by psychological factors seems crucial [3]. Indeed, pooled data from 28 studies identified that out of 2918 participants, 65% cited a psychological reason for not returning to sport [4]. The most significant factor consistently reported being that of fear of re-injury with 24%-50% of athletes reporting fear/ lack of confidence as their primary concern surrounding participation [5,6,7,8]. Physiological factors also play an important role in RTS, and in an attempt to understand the extent of the problem and synthesise current evidence for RTS decision making, a group of expert clinicians produced a consensus statement in which a Biopsychosocial model for RTS was developed [3]. This model emphasizes in particular the modifiable nature of athlete’s psychological perceptions through relationships with the physiological determinants that may underpin an athlete’s confidence [3].
The main physiological determinant of RTS following ACLR is the restoration of strength in both the knee flexors and extensors of the operated knee, with deficits commonly reported in athletes both at RTS and in the years following [9,10,11,12]. The hamstrings role as a synergist for the ACL is important in managing anterior tibial translation (ATT) during landing, with maximal strength deficits reported as a risk factor for ACLI or re-injury in a number of prospective studies [13,14]. Quadriceps contractions help to absorb ground reaction forces (GRF) during performance, in turn, attenuating loads on lower extremities such as the ACL during landing [15]. Deficits in quadriceps maximal strength have been associated with the incidence of re-injury following ACLI [16]. For both these muscle groups, it is commonly accepted that a Limb Symmetry Index (LSI) greater than 90% between operated and non-operated legs should be sufficiently reduce the risk of future damage to the surgical graft [16]. Despite this stipulation, many athletes still RTS with strength deficits in both muscle groups at RTS and in the years following, making appropriate rehabilitation essential [9,11,12].
More recently, authors have investigated quadriceps and hamstring force produced close to knee extension as risk factors because ACLI seem to occur at these angles [17,18], while peak values occur mid-range [19]. Hammond [20] identified that within a cohort of previously injured athletes who met initial criteria of LSI >90% for maximal strength of the quadriceps and hamstrings, strength deficiencies were still observed in 72% of them, in particular at 10°- 40° from full extension.
In addition to the level of strength of the hamstring, its capacity to quickly produce force (rate of force or torque development, RFD or RTD) is a strong predictor of ACLI [21]. Indeed, most ACLI occurs within 0-61ms of initial contact with the ground [22]. The use of RFD, despite its relevance, remains very limited for RTS testing following ACLR [23]. Yet deficits in RFD are commonly seen following ACLR [24,25].
To our knowledge, only one study has examined the relationship between strength performance and psychological variables following ACLR, utilising the ACL-RSI to quantify patient psychological readiness to RTS [26]. This study showed a significant association between ACL-RSI scores and hamstring peak torque, but not quadriceps, in a cohort of male athletes at 9 months post-surgery [26]. Additional findings from this study were the absence of significant differences in peak strength variables between a group with a low ACL-RSI score (<65) and a group with a high ACL-RSI score (>85). However this study only measured peak strength and there is currently no investigations on the association between ACL-RSI scores and other strength parameters, such as RFD or angle-specific torque.
Therefore the primary aim of the present study was to investigate the strength and power determinants of athletes’ psychological readiness to RTS. A secondary aim was to compare strength and power performance of a group deemed psychologically ready for a return to PILOS against those deemed not psychologically ready to return to PILOS.
Materials and Methods
Participants
Twelve participants, including six male and six females (20.7±2.5 years old; 174.2±7.5 cm; 70.2±8.5 kg; 18.2±8.3% of body fat) volunteered to take part in the study. They were recruited from various University teams competing at regional to national levels (football, volleyball, netball, lacrosse, tennis and triathlon). Inclusion criteria were having a primary ACLR more than 9 months prior to the start of the study because most athletes are cleared for RTS support between 6-9-month post-surgery. To be included in the study participants should also have already returned to some form of sport participation or have been officially cleared to do so by a qualified physiotherapist. Exclusion criteria were any current lower limb injury, any history of contralateral ACLI or recurrent ipsilateral ACLR and any mental health condition, such as depression and anxiety that could influence ACLI-RSI scores [27]. Participants gave written informed consent and the study was approved by the local University ethics committee (reference number 191305), in accordance with the principles set in the Helsinki declaration.
Procedures
The study design was cross-sectional, with participants attending the laboratory on one occasion only to perform psychological assessments first, followed by strength testing.
Psychological assessment consisted in the ACL-RSI questionnaire. This questionnaire was chosen for its very good validity and reliability [28,29]. In addition, its use was recommended in the 2015 consensus statement following ACLI [3]. The total score out of 100 was recorded, and it was also used to separate participants into one group deemed not psychologically ready to return to PILOS (cases) and a group deemed psychologically ready to return to PILOS (controls). The threshold used for these groups was a total score of 81.4%, as a previous study reported an association between scores <81.4% and the inability for athletes to return to this level [28].
Strength testing was undertaken on an isokinetic dynamometer (Biodex system 4; Biodex, Shirley, NY). A standardised warm up was implemented prior to the initiation of isokinetic testing. This consisted of 8 minutes on a Monark cycle ergometer (874E; Monark, Vanberg, Sweden) at an intensity of 100W, with three intermittent 6-s maximal effort sprints at minutes 6,7 and 8. This was followed by five body weight squats, two submaximal and three maximal counter movement jumps [26]. After the warm-up, participants were instructed to sit upright on the chair with their hips flexed at 90°. Straps were secured to immobilise movement at the thigh, hips and trunk in order to limit the influence of extraneous joint and muscle involvement. Straps were secured at the proximal tibia from which participants would initiate/ resist movement. Alignment of the lateral femoral condyle was made with the axis of the dynamometer level arm, with the proximal lever arm secured at the lateral malleolus. Participants were tested on both operated and non-operated legs and at two angular velocities, with all these conditions randomised. The range of motion was from 0° (full knee extension) to 90° of knee flexion and participants were given verbal encouragement to provide maximal effort throughout the range. The test consisted of concentric contractions of the quadriceps and hamstrings and eccentric contraction of the hamstrings at 60°·s-1 (three repetitions) and 180°·s-1 (five repetitions). These velocities are characterised by excellent test-retest reliability (Intraclass correlation coefficients of 0.95-0.98, [30]. Each condition was preceded by a familiarisation set.
The following variables were calculated as the average of the two best contractions at 60°·s-1 and the three best contractions at 180°·s-1:
- Concentric peak torque of the quadriceps relative to body weight (Qcon, N.m.kg-1).
- Eccentric peak torque of the hamstrings relative to body weight (Hecc, N.m.kg-1).
- Peak Hecc:Qcon.
- Angle-specific Hecc, Qcon and Hecc:Qcon at 10° (Hecc10, Qcon10, Hecc:Qcon10), 20° (Hecc20, Qcon20, Hecc:Qcon20), 30° (Hecc30, Qcon30, Hecc:Qcon30), and 40° (Hecc40, Qcon40, Hecc:Qcon40) from full knee extension. These were calculated as averages between 0°-10°, 11°-20°, 21°-30° and 31°-40°, respectively [31].
- Quadriceps and hamstrings rate of torque development in the first 50 ms and the first 100 ms (RTD50 and RTD100, N·m·s-1) for Hecc, Qcon and Hecc/Qcon, calculated as the ratio between the change in torque and the corresponding change in time in the first 50ms and 100 ms of contraction, respectively. The onset of contraction was defined as a torque value of 1% of the peak torque produced during the same contraction [32]. The time windows of 50 ms and 100 ms were chosen as the best compromise between reliability and ecological validity. Indeed, ACL injuries usually occur in the first 50ms after initial ground contact [33]. However, Mentiplay et al. [34] showed greater reliability of RFD at 100 ms than 50ms. The same time windows were previously used in similar research [32].
- Limb symmetry index (LSI) for all parameters: = ([(operated-non-operated)/non-operated] x 100.
Statistical Analyses
All data was presented as mean ± standard deviation with 95% confidence interval (CI). Statistical analyses were conducted using IBM SPSS V.29. The normality of data was assessed using the Shapiro-Wilk test. A stepwise linear regression was conducted on the entire sample to identify if strength data from the operated leg could be determinants of the ACL-RSI score. Subsequently, participants were divided into a ready to return to PILOS group and not ready to return to PILOS group. A student-t test for independent samples was used to assess differences between groups in all outcome variables. Effect sizes were calculated as Cohen’s d (d) and interpreted as small (>0.2), medium (>0.5) and large (>0.8), [35]. The P-value was set at P<0.05.
Results
Seven participants were identified as cases with ACL-RSI scores <81.4% and five participants were identified as controls with ACL-RSI scores >81.5. Participant Demographics are summarised in Table 1.
The linear regression identified that three variables, namely quadriceps RTD100 at 60°.s-1, time since surgery and hamstrings RTD50 at 60°.s-1, were significant predictors of the ACL-RSI score (r2=0.915). The statistics associated with each factor were Beta=0.583, t=5.077 (P<0.001) for quadriceps RTD100 at 60°.s-1, Beta=0.620, t=5.855 (P<0.001) for time since surgery and Beta=0.411, t=3.498 (P=0.008) for hamstrings RTD50 at 60°.s-1.
Between group differences were shown on Qcon40 at 60°.s-1, with significantly lower values in cases than controls (t(df)=-2.71(9.846), 95% CI: -0.68 to -0.07, d=1.46, p=0.011), Figure 1. A significantly lower Qcon30 at 60°.s-1 was also shown in cases compared to controls (t(df)=2.62(10), 95% CI: -0.54 to -0.04, d= 1.54, p= 0.013, Figure 1). No statistically significant differences were seen for hamstring torque values at any angle or angular velocity (P>0.05, Figure 2).
RTD values showed that cases were characterised by significantly lower Quadriceps RTD100 at 60°.s-1 (t(df)=2.32(10), 95% CI: -447.34 to -9.56, d= 1.36, p=0.021, Figure 3) and at 180°.s-1 (t(df)=1.85(10), 95% CI: -449.81 to 42.37, d= 1.08, p=0.047, Figure 3) compared to controls. In the hamstrings, the only significant RTD difference observed was a significantly lower RTD100 at 60°.s-1 in the cases compared to controls (t(df=2.04(10), 95% CI: -175.4 to 7.7, d= 1.2, p=0.034, Figure 4).
Regarding asymmetry between limbs, LSI for the quadriceps RFD50 LSI at 180°.s-1 showed a significantly higher score in the cases than controls (1.05±0.11 vs. 0.95±0.04, respectively for cases and controls, t(df=1.87(10), 95% CI: -0.02 to 0.29, d=1.1, p=0.045). In addition, cases had a significantly lower hamstring RFD50 LSI at 60°.s-1 than controls (0.51±0.32 vs. 2.06±1.61, respectively for cases and controls, t(df)= 2.12 (4.222), 95% CI: -3.54 to 0.44, d=1.48, p=0.049) and a significantly lower hamstring RFD100 LSI at 60°.s-1 than controls (0.57±0.30 vs. 1.61±1.12, respectively for cases and controls, t(df)= 1.95 (4.222), 95% CI: -2.01 to -0.06, d= 1.39, p=0.019).
Discussion
This study is one of very few observing the relationship between strength and power parameters and psychological readiness following ACLR. The main findings are that the RTD of the quadriceps and hamstrings, as well as time since surgery were the main determinants of psychological readiness following ACLR. In addition, compared to controls, cases showed significantly lower angle-specific quadriceps and hamstrings torque close to extension and lower RTD, but no difference in peak torque values.
A novel finding identified within this study is the extent to which RTD has been identified as both a determinant for psychological readiness and as a statistically significant difference between groups. This is the first study to examine the relationships between muscle RTD scores and psychological readiness and therefore comparison of results cannot be made against previous literature. The prevalence of rate of force development (RFD) as a power deficit following ACLR however, is well reported in the injured limb in the short- [24,25] but also longer-term [36]. Deficits in RFD following ACLR could be due to both neural and peripheral muscular factors [36,37] and seem to reflect closely athletes’ rehabilitation status [36]. Several training modalities can improve RFD; for example, ballistic training performed around RTS [38] has shown greater increases in RFD against traditional strength and endurance training [39]. Sprint training also increased RFD (+29% in week weeks) in a recent study, while strength training did not [40]. With a potential overreliance on isolated maximal muscle strength after ACLR within traditional RTS training [38], results from this study indicate a greater focus should be given to RFD in the facilitation of a successful RTS. To explain the impact of RTD on psychological outcomes shown in the present study, the functional role played by the hamstrings and quadriceps in providing stability at the knee needs to be considered [41,42]. The ability of muscles to generate force within an early critical window (0-100ms) is essential in stabilising the leg, attenuating GRF [15],and aligning landing mechanics within the period of time in which ACLI occur [22]. With residual movement impairments during RTS, it may be theorised that such neuromuscular deficits will affect the quality of movement athletes display [38], which may be negatively perceived by athletes, subsequently altering their ACL-RSI scores. These assumptions rely on the biopsychosocial framework, where an athlete’s physiological factors have a mediating role on their psychological perceptions [3]. However, further experimental studies should be conducted to confirm these associations.
The role of peak torque as a determinant of ACL-RSI scores was not identified in the present study. This is partly in line with the findings of the only study in this area, reporting no significant relation between quadriceps peak torque at 60°.s-1 and ACL-RSI scores in athletes 9 months post surgery [26]. However, the same authors also showed a small but significant correlation (r=0.14) between hamstrings peak torque at 60°.s-1 and ACL-RSI scores [26], which in contrast with our results. The study of O’Connor et al. [26] also separated participants according to their ACL-RSI scores, similarly to the present study and found no significant between group differences in quadriceps or hamstrings peak torque, in accordance with our results. The contrasting results on hamstrings peak torque between the present study and the study of O’Connor et al. [26] could be explained by the different criteria used to separate groups (low (<65) and high (>85) ACL-RSI scores for cases and controls in the study by O’Connor et al. [26] compared to <81.4% and >81.4% in the present study). Having some individuals from different groups but with very close ACL-RSI scores in the present study could have biased the results towards a lack of between group differences. Other differences between studies are the significantly larger sample size in O’Connor [26]’s study (n=452), and their cut-off at 9 months post-surgey, compared to the range of longitudinal time frames examined within this study. It can be hypothesized that athlete perceptions within O’Connor’s [26] study are more of a reflection of their rehabilitation process. In contrast, for our participants who have returned to sport and thus benefit from greater sporting exposures, ACL-RSI scores illustrate the development of psychological barriers for athletes in the pursuit of a return to PILOS, which is novel element of the current study. Finally, our data analysis was based on a linear regression, in contrast to correlations in the study of O’Connor et al. [26], which may explain the lack of association between some parameters and the ACL-RSI scores.
A novel finding of the present study is the significantly lower quadriceps torque at angles from 20° and 40° from full extension in cases compared to controls (differences of 21% and 23%, respectively at these angles). The role of the quadriceps at these shallow flexion angles is significant in relation to the number of ACLI that occur within them [17]. Previous studies have shown that individuals with weaker quadriceps have altered sagittal plane kinematics during landing and subsequently incur higher GRF upon a stiff legged landing [15]. Similarly to our comments on RTD, this process may result in a perception of instability during sport participation that could be reflected in the ACL-RSI scores. During rehabilitation, restoration of joint ROM is targeted during the early phases [43], yet, little consideration is noted regarding muscular strength specifically in the functionally important ranges that non-contact ACLI occur (Hammond [20]). Our findings on angle-specific torque, together with the absence of significant differences between groups in peak torque, highlights the importance for physiotherapists to address strength deficits across the full range of motion and consider sport-specific mechanics. Supporting stipulations made by Hammond [20] who similarly reported strength deficits between specific angles, where >90% LSI was achieved during PT assessments. The importance of the capacity to produce high torque when the knee is close to full extension has also been highlighted in a study on fatigue in female footballers, showing that Hecc:Qcon was significantly reduced after a simulated match only between 0 and 10° from full knee extension [31]. This highlights a reduced capacity of the hamstring to stabilise the knee joint close to extension in a fatigue state, where ACLI occur, and highlights the importance to address residual strength deficits at these angles during rehabilitation.
Limb symmetry index has been cited as a risk factor for lower limb injuries in previous literature [44], although there are contrasting results in the literature [45]. Our findings did not identify it as a major determinant of psychological readiness to RTS, suggesting that it might not be sensitive enough to affect athletes’ perception during exercise. However we found that LSI for RTD50 in the quadriceps at both testing speeds was greater in cases than controls. This highlights one more time that power, rather than strength is an important factor that could play a role on athletes’ decision to RTS.
The main limitations of the present study are the lack of control on our participants’ rehabilitation and subsequent sport experience. In addition, we chose to focus on psychological parameters as our main outcome and explore the role of strength and power variables as potential determinants of this. However an argument can be made that constructs such as fear and confidence may instead impact physiological parameters through the avoidance of high-intensity rehabilitation required in order to efficiently address them. Finally, our sample size was small, which could limit the interpretation of our findings, however this is counteracted by the fact that we observed relatively large effect sizes.
In conclusion, our findings showed that one of the main determinants of psychological readiness to RTS following ACLR was the rate of torque development of the quadriceps and hamstrings. In addition, compared to controls, cases showed significantly lower angle-specific quadriceps and hamstrings torque close to extension and lower RTD, but no difference in peak torque values. The importance of muscular strength across all angles of function were also identified, with quadriceps strength of particular importance at angles of functional relevance between 20° and 40°. These findings highlight the importance for physiotherapists to address muscular deficits across their full range and develop power and explosiveness in addition to strength in rehabilitation. Future studies with larger sample sizes are needed to further investigate the relationship between strength and power and psychological factors playing a role in RTS.
Author Contributions
OL did the data collection, statistical analysis and write-up. AD designed the study and supervised statistical analysis and write-up. MW designed the study and helped with the write-up. CS helped with the write-up and analysis.
Funding Information
The authors did not receive any external funding for this study.
Ethics Statements
The study was approved by the local University ethics committee (reference number 191305).
Conflicts of Interest
The authors do not have to report any conflict of interest.
References
- Ardern, C.L.; Webster, K.E.; Taylor, N.F.; Feller, J.A. Return to sport following anterior cruciate ligament reconstruction surgery: a systematic review and meta-analysis of the state of play. British journal of sports medicine 2011, 45, 596–606. [Google Scholar] [CrossRef] [PubMed]
- DeFazio, M.W.; Curry, E.J.; Gustin, M.J.; Sing, D.C.; Abdul-Rassoul, H.; Ma, R.; Fu, F.; Li, X. Return to sport after ACL reconstruction with a BTB versus hamstring tendon autograft: a systematic review and meta-analysis. Orthopaedic journal of sports medicine 2020, 8, 2325967120964919. [Google Scholar] [CrossRef] [PubMed]
- Ardern, C.L.; Glasgow, P.; Schneiders, A.; Witvrouw, E.; Clarsen, B.; Cools, A.; Gojanovic, B.; Griffin, S.; Khan, K.M.; Moksnes, H.; Mutch, S.A. 2016 Consensus statement on return to sport from the First World Congress in Sports Physical Therapy. Bern. British journal of sports medicine 2016, 50, 853–864. [Google Scholar] [CrossRef]
- Nwachukwu, B.U.; Adjei, J.; Rauck, R.C.; Chahla, J.; Okoroha, K.R.; Verma, N.N.; Allen, A.A.; Williams, RJ., III. ‘How much do psychological factors affect lack of return to play after anterior cruciate ligament reconstruction? A systematic review. Orthopaedic journal of sports medicine 2019, 7, 2325967119845313. [Google Scholar] [CrossRef]
- Ardern, C.L.; Österberg, A.; Tagesson, S.; Gauffin, H.; Webster, K.E.; Kvist, J. The impact of psychological readiness to return to sport and recreational activities after anterior cruciate ligament reconstruction. British journal of sports medicine 2014, 48, 1613–1619. [Google Scholar] [CrossRef] [PubMed]
- Kvist, J.; Ek, A.; Sporrstedt, K.; Good, L. Fear of re-injury: a hindrance for returning to sports after anterior cruciate ligament reconstruction. Knee surgery, sports traumatology, arthroscopy 2005, 13, 393–397. [Google Scholar] [CrossRef]
- Lentz, T.A.; Zeppieri Jr, G.; Tillman, S.M.; Indelicato, P.A.; Moser, M.W.; George, S.Z.; Chmielewski, T.L. Return to preinjury sports participation following anterior cruciate ligament reconstruction: contributions of demographic. knee impairment, and self-report measures. journal of orthopaedic & sports physical therapy 2012, 42, 893–901. [Google Scholar] [CrossRef]
- McCullough, K.A.; Phelps, K.D.; Spindler, K.P.; Matava, M.J.; Dunn, W.R.; Parker, R.D.; Moon Group Reinke, E.K. Return to high school–and college-level football after anterior cruciate ligament reconstruction: a Multicenter Orthopaedic Outcomes Network (MOON) cohort study. The American journal of sports medicine 2012, 40, 2523–2529. [Google Scholar] [CrossRef]
- Csapo, R.; Hoser, C.; Gföller, P.; Raschner, C.; Fink, C. Fitness, knee function and competition performance in professional alpine skiers after ACL injury. Journal of science and medicine in sport 2019, 22, S39–S43. [Google Scholar] [CrossRef]
- Fischer, F.; Fink, C.; Herbst, E.; Hoser, C.; Hepperger, C.; Blank, C.; Gföller, P. Higher hamstring-to-quadriceps isokinetic strength ratio during the first post-operative months in patients with quadriceps tendon compared to hamstring tendon graft following ACL reconstruction. Knee Surgery, Sports Traumatology, Arthroscopy 2018, 26, 418–425. [Google Scholar] [CrossRef]
- Guney-Deniz, H.; Harput, G.; Kaya, D.; Nyland, J.; Doral, M.N. Quadriceps tendon autograft ACL reconstructed subjects overshoot target knee extension angle during active proprioception testing. Knee Surgery, Sports Traumatology, Arthroscopy 2020, 28, 645–652. [Google Scholar] [CrossRef]
- Lee, J.K.; Lee, S.; Lee, M.C. Outcomes of anatomic anterior cruciate ligament reconstruction: bone–quadriceps tendon graft versus double-bundle hamstring tendon graft. The American journal of sports medicine 2016, 44, 2323–2329. [Google Scholar] [CrossRef] [PubMed]
- Myer, G.D.; Ford, K.R.; Foss, K.D.B.; Liu, C.; Nick, T.G.; Hewett, T.E. The relationship of hamstrings and quadriceps strength to anterior cruciate ligament injury in female athletes. Clinical journal of sport medicine 2009, 19, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Wild, C.Y.; Steele, J.R.; Munro, B.J. Insufficient hamstring strength compromises landing technique in adolescent girls. Medicine & Science in Sports & Exercise 2013, 45, 497–505. [Google Scholar]
- Ward, S.H.; Blackburn, J.T.; Padua, D.A.; Stanley, L.E.; Harkey, M.S.; Luc-Harkey, B.A.; Pietrosimone, B. Quadriceps neuromuscular function and jump-landing sagittal-plane knee biomechanics after anterior cruciate ligament reconstruction. Journal of athletic training 2018, 53, 135–143. [Google Scholar] [CrossRef]
- Grindem, H.; Snyder-Mackler, L.; Moksnes, H.; Engebretsen, L.; Risberg, M.A. Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction: the Delaware-Oslo ACL cohort study. British journal of sports medicine 2016, 50, 804–808. [Google Scholar] [CrossRef]
- Beynnon, B.D.; Fleming, B.C.; Johnson, R.J.; Nichols, C.E.; Renström, P.A.; Pope, M.H. Anterior cruciate ligament strain behavior during rehabilitation exercises in vivo. The American journal of sports medicine 1995, 23, 24–34. [Google Scholar] [CrossRef]
- Yu, B.; Garrett, W.E. Mechanisms of non-contact ACL injuries. British journal of sports medicine 2007, 41, 47–51. [Google Scholar] [CrossRef]
- Cohen, D.D.; Zhao, B.; Okwera, B.; Matthews, M.J.; Delextrat, A. ‘Angle-specific eccentric hamstring fatigue after simulated soccer. International Journal of Sports Physiology and Performance 2015, 10, 325–331. [Google Scholar] [CrossRef]
- Hammond, J.A. Strength profiling using isokinetic dynamometry following anterior cruciate ligament reconstruction: Implications for rehabilitation and return to sport decision making. PhD thesis, University of Gloucestershire, 2022, 10 November 2022. [Google Scholar]
- Zebis, M.K.; Aagaard, P.; Andersen, L.L.; Hölmich, P.; Clausen, M.B.; Brandt, M.; Husted, R.S.; Lauridsen, H.B.; Curtis, D.J.; Bencke, J. First-time anterior cruciate ligament injury in adolescent female elite athletes: A prospective cohort study to identify modifiable risk factors. Knee Surgery and Sports Traumatology and Arthroscopy 2021, 30, 1341–1351. [Google Scholar] [CrossRef]
- Bates, N.A.; Schilaty, N.D.; Ueno, R.; Hewett, T.E. Timing of strain response of the ACL and MCL relative to impulse delivery during simulated landings leading up to ACL failure. Journal of applied biomechanics 2020, 36, 148–155. [Google Scholar] [CrossRef]
- Burgi, C.R.; Peters, S.; Ardern, C.L.; Magill, J.R.; Gomez, C.D.; Sylvain, J.; Reiman, M.P. Which criteria are used to clear patients to return to sport after primary ACL reconstruction? A scoping review. British journal of sports medicine 2019, 53, 1154–1161. [Google Scholar] [CrossRef] [PubMed]
- Kadija, M.; Knežević, O; Milovanović, D; Nedeljković, A; Mirkov, D.M. The effect of anterior cruciate ligament reconstruction on hamstring and quadriceps muscle function outcome ratios in male athletes. Srpski arhiv za celokupno lekarstvo 2016, 144, 151–157. [Google Scholar] [CrossRef]
- Mirkov, D.M.; Knezevic, O.M.; Maffiuletti, N.A.; Kadija, M.; Nedeljkovic, A.; Jaric, S. Contralateral limb deficit after ACL-reconstruction: an analysis of early and late phase of rate of force development. Journal of sports sciences 2017, 35, 435–440. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, R.F.; King, E.; Richter, C.; Webster, K.E.; Falvey, É.C. No relationship between strength and power scores and anterior cruciate ligament return to sport after injury scale 9 months after anterior cruciate ligament reconstruction. The American journal of sports medicine 2020, 48, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Carolan, D.; King, E.; Richter, C.; Franklyn-Miller, A.; Moran, R.; Jackson, M. Differences in strength, patient-reported outcomes, and return-to-play rates between athletes with primary versus revision ACL reconstruction at 9 months after surgery. Orthopaedic Journal of Sports Medicine 2020, 8, 2325967120950037. [Google Scholar] [CrossRef] [PubMed]
- Webster, K.E.; Feller, J.A. Development and validation of a short version of the anterior cruciate ligament return to sport after injury (ACL-RSI) scale. Orthopaedic journal of sports medicine 2018, 6, 2325967118763763. [Google Scholar] [CrossRef]
- Webster, K.E.; Feller, *!!! REPLACE !!!*; J.A., *!!! REPLACE !!!*. Who passes return-to-sport tests, and which tests are most strongly associated with return to play after anterior cruciate ligament reconstruction? Orthopaedic journal of sports medicine 2020, 8, 2325967120969425. [Google Scholar] [CrossRef]
- Drouin, J.M.; Valovich-mcLeod, T.C.; Shultz, S.J.; Gansneder, B.M.; Perrin, D.H. Reliability and validity of the Biodex system 3 pro isokinetic dynamometer velocity, torque and position measurements. European journal of applied physiology 2004, 91, 22–29. [Google Scholar]
- De Ste Croix, M.; Priestley, A.; Lloyd, R.; Oliver, J. () ‘Age-Related Differences in Functional Hamstring/Quadriceps Ratio Following Soccer Exercise in Female Youth Players: An Injury Risk Factor. ’ Pediatrics and Exercise Science 2018, 30, 376–382. [Google Scholar] [CrossRef]
- Zhang, Q.; Morel, B.; Trama, R.; Hautier, C. Influence of Fatigue on the Rapid Hamstring/Quadriceps Force Capacity in Soccer Players. Frontiers in Physiology 2021, 12, 627674. [Google Scholar] [CrossRef] [PubMed]
- Krosshaug, T.; Nakamae, A.; Boden, B.P.; Engebretsen, L.; Smith, G.; Slauterbeck, J.R.; Hewett, T.E.; Bahr, R. Mechanisms of anterior cruciate ligament injury in basketball: Video analysis of 39 cases. American Journal of Sports Medicine 35, 359–367. [CrossRef] [PubMed]
- Mentiplay, B.F.; Perraton, L.G.; Bower, K.J.; Adair, B.; Pua, Y.H.; Williams, G.P.; McGaw, R.; Clark, R.A. Assessment of Lower Limb Muscle Strength and Power Using Hand-Held and Fixed Dynamometry: A Reliability and Validity Study. PLoS One 2015, 10, e0140822. [Google Scholar] [CrossRef]
- Cohen, J. () Statistical Power Analysis for the behavioural sciences. 1988, 19–66. [Google Scholar]
- Turpeinen, J.T.; Freitas, T.T.; Rubio-Arias, J.Á.; Jordan, M.J.; Aagaard, P. Contractile rate of force development after anterior cruciate ligament reconstruction—a comprehensive review and meta-analysis. Scandinavian Journal of Medicine & Science in Sports 2020, 30, 1572–1585. [Google Scholar]
- Maffiuletti, N.A.; Aagaard, P.; Blazevich, A.J.; Folland, J.; Tillin, N.; Duchateau, J. Rate of force development: physiological and methodological considerations. European journal of applied physiology 2016, 116, 1091–1116. [Google Scholar] [CrossRef]
- Buckthorpe, M. Optimising the late-stage rehabilitation and return-to-sport training and testing process after ACL reconstruction. Sports Medicine 2019, 49, 1043–1058. [Google Scholar] [CrossRef]
- Vila-Chã, C.; Falla, D.; Farina, D. Motor unit behaviour during submaximal contractions following six weeks of either endurance or strength training. Journal of Applied Physiology 2010, 109, 1455–1466. [Google Scholar] [CrossRef]
- Sancese, A.; Taylor, L.; Walsh, G.; Byrd, E.; Delextrat, A. ‘Effects of sprint versus strength training on risk factors for hamstring injury in football players. Journal of Sports Medicine and Physical Fitness 2023, 63, 580–587. [Google Scholar] [CrossRef]
- Birchmeier, T.; Lisee, C.; Kane, K.; Brazier, B.; Triplett, A.; Kuenze, C. Quadriceps muscle size following ACL injury and reconstruction: a systematic review. Journal of Orthopaedic Research 2020, 38, 598–608. [Google Scholar] [CrossRef]
- Buckthorpe, M.; Danelon, F.; La Rosa, G.; Nanni, G.; Stride, M.; Della Villa, F. Recommendations for hamstring function recovery after ACL reconstruction. Sports Medicine 2021, 51, 607–624. [Google Scholar] [CrossRef] [PubMed]
- Cavanaugh, J.T.; Powers, M. ACL rehabilitation progression: where are we now? Current reviews in musculoskeletal medicine 2017, 10, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Bourne, M.N.; Opar, D.A.; Williams, M.D.; Shield, A.J. Eccentric Knee Flexor Strength and Risk of Hamstring Injuries in Rugby Union: A Prospective Study. American Journal of Sports Medicine 2015, 43, 663–2670. [Google Scholar] [CrossRef] [PubMed]
- Collings, T.J.; Diamond, L.E.; Barrett, R.S.; Timmins, R.G.; Hickey, J.T.; DUMoulin, W.S.; Williams, M.D.; Beerworth, K.A.; Bourne, M.N. Strength and Biomechanical Risk Factors for Noncontact ACL Injury in Elite Female Footballers: A Prospective Study. Medicine and Science in Sports and Exercise 2022, 54, 1242–1251. [Google Scholar] [CrossRef]
Figure 1.
Concentric peak torque and angle-specific torque values of the quadriceps (Qcon, N.m.kg-1) in cases (white) and controls (black).
Figure 1.
Concentric peak torque and angle-specific torque values of the quadriceps (Qcon, N.m.kg-1) in cases (white) and controls (black).
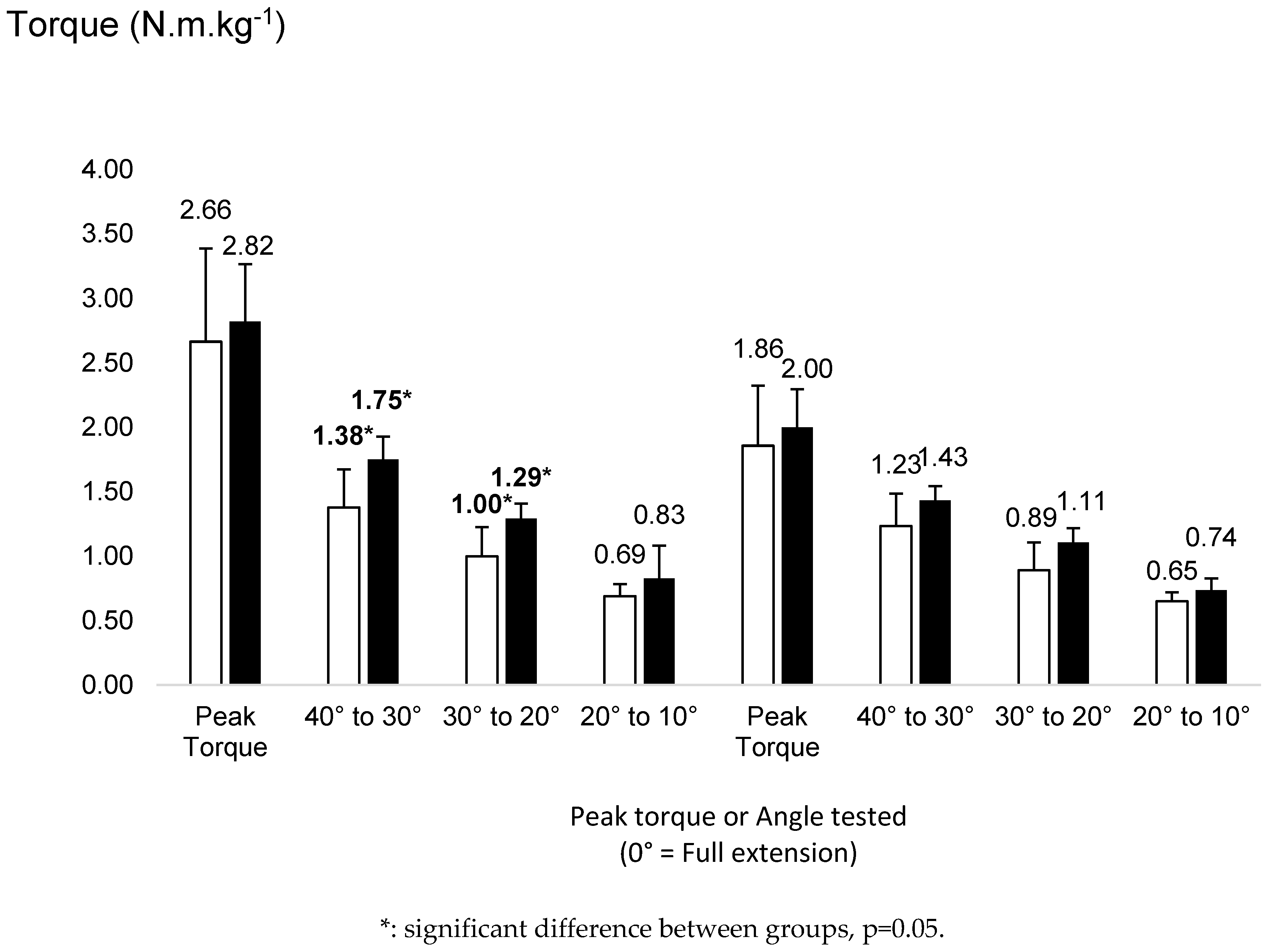
Figure 2.
Eccentric peak torque and angle-specific torque values of the hamstrings (Hecc, N.m.kg-1) in cases (white) and controls (black).
Figure 2.
Eccentric peak torque and angle-specific torque values of the hamstrings (Hecc, N.m.kg-1) in cases (white) and controls (black).
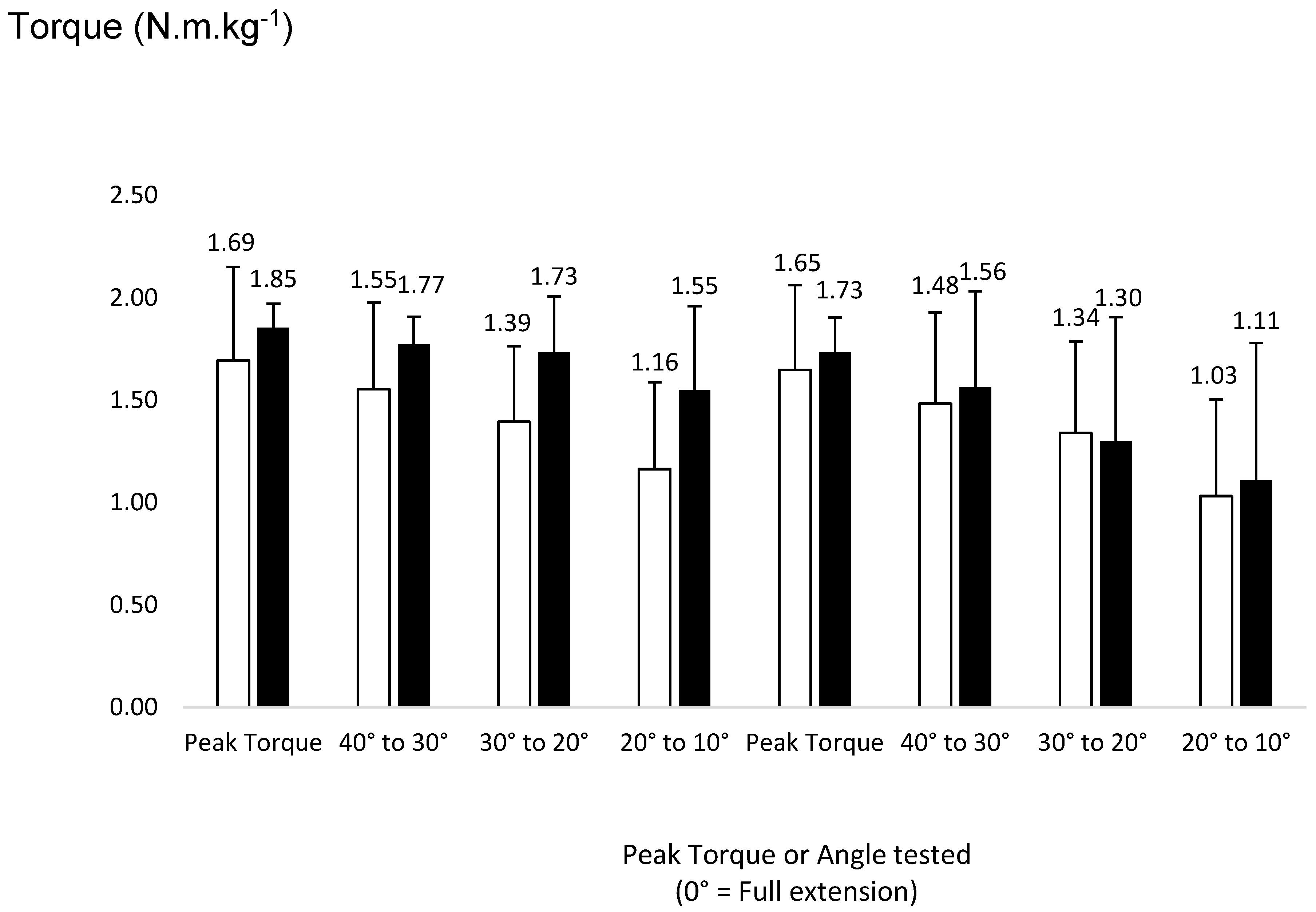
Figure 3.
Rate of torque development (RTD) for the quadriceps concentric (Qcon) contractions (N.m.s-1) between cases (white) and controls (black).
Figure 3.
Rate of torque development (RTD) for the quadriceps concentric (Qcon) contractions (N.m.s-1) between cases (white) and controls (black).
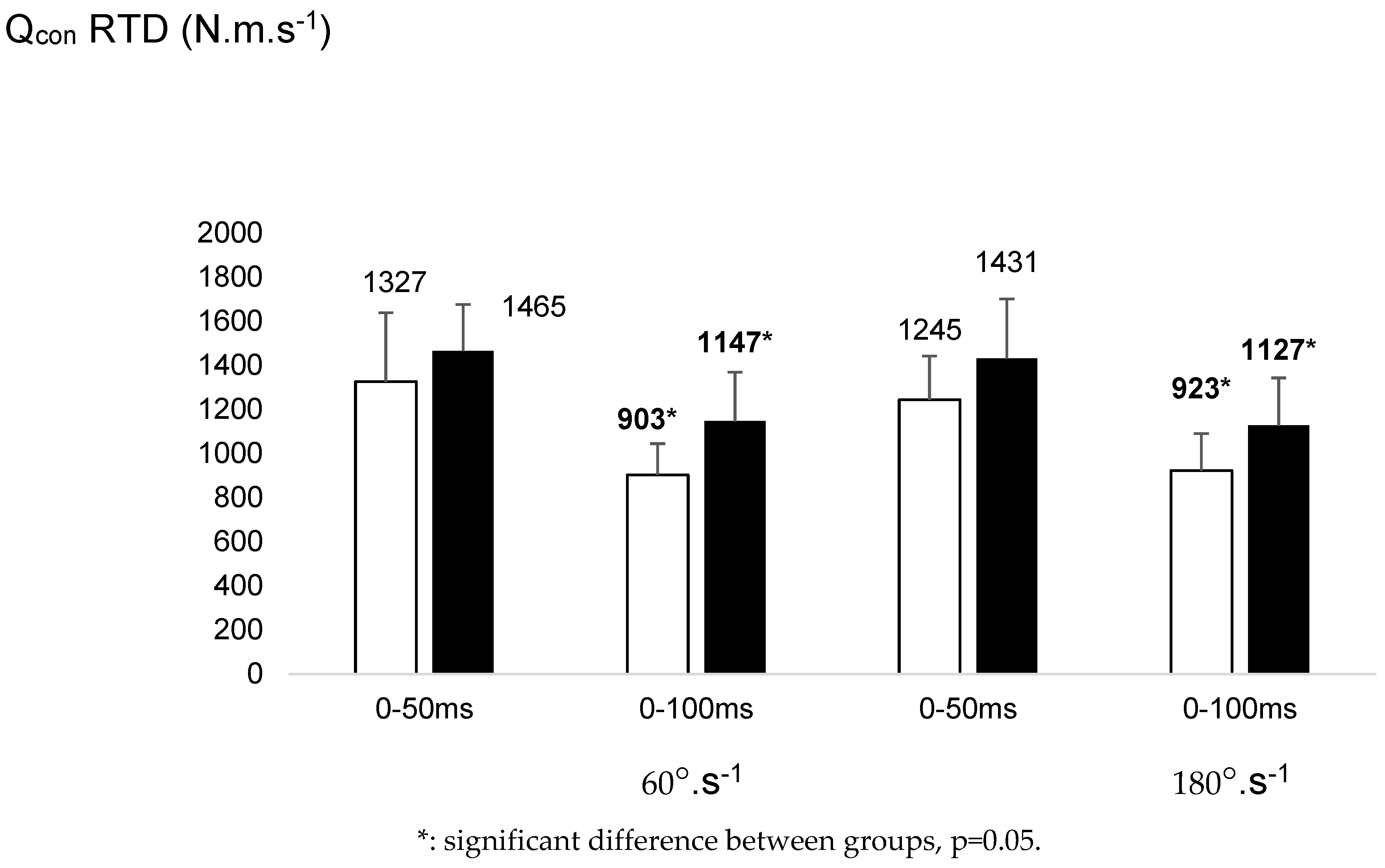
Figure 4.
Rate of torque development (RTD) for the hamstrings eccentric (Hecc) contractions (N.m.s-1) between cases (white) and controls (black).
Figure 4.
Rate of torque development (RTD) for the hamstrings eccentric (Hecc) contractions (N.m.s-1) between cases (white) and controls (black).
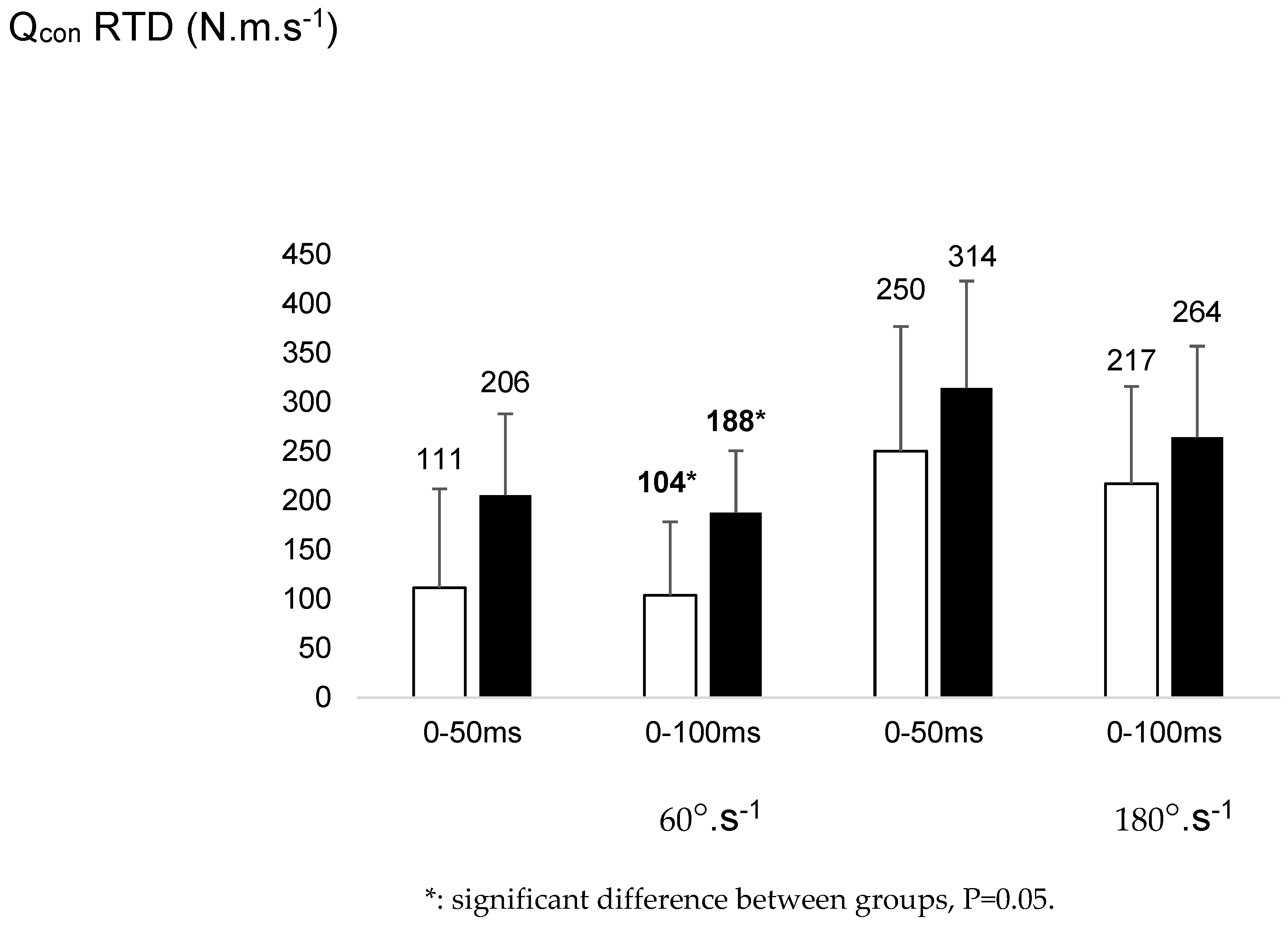

Table 1.
Participants demographics (mean ± SD). Triad is reported with injury to each of the ACL, Meniscus and associated Medial Collateral Ligament or Lateral Collateral Ligament. HTG: Hamstring Tendon Graft, PTG :Patella Tendon Graft.
Table 1.
Participants demographics (mean ± SD). Triad is reported with injury to each of the ACL, Meniscus and associated Medial Collateral Ligament or Lateral Collateral Ligament. HTG: Hamstring Tendon Graft, PTG :Patella Tendon Graft.
|
All Participants (n=12) |
Cases ACL-RSI Scores <81.4% (n=7) |
Controls ACL-RSI Scores >81.4% (n=5) |
|
|---|---|---|---|
| Age | 20.7 ± 2.5 | 20 ± 2.2 | 21.6 |
| Sex, male: female | 6:6 | 3:4 | 3:2 |
| Operated Side, right: left | 7:5 | 4:3 | 3:2 |
| Height (cm) | 174 ±8 | 170 ±5 | 179 ± 8 |
| Weight (Kg) | 70.2 ±8.5 | 68.7 ±7.5 | 72.26 ±10.3 |
| Body fat % | 18.2 ±8.3 | 20.9±9.9 | 14.32 ± 3.5 |
| Time Since Injury (months) | 38 ±21 | 33 ±18 | 46 ± 24 |
| Time Since Surgery (months) | 31 ±19 | 24 ±13 | 41 ±23 |
| Time Since RTS (months) Reported to have returned to PILOS, yes:no |
15 ±15 5:8 |
11 ±9 1:6 |
21 ±21 4:1 |
| Combined Injury, none: meniscal tear: Triad | 3:6:3 | 3:3:1 | 0:3:2 |
| Graft Type, HTG: PTG | 12:0 | 7:0 | 5:0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



