
Submitted:
25 July 2025
Posted:
29 July 2025
You are already at the latest version
Abstract
Background/Objectives: Anterior cruciate ligament (ACL) injuries continue to present significant clinical and rehabilitative challenges. Despite advances in surgical techniques and rehabilitation protocols, persistent reinjury rates and increased pressure for early return to sport require a critical reassessment of current practices. This narrative review provides a comprehensive overview of the evolution, current standards, and future directions of ACL treatment and rehabilitation. Additionally, we present original data evaluating the effectiveness of brace-free rehabilitation following ACL reconstruction (ACL-R). Methods: The review synthesizes developments in surgical techniques and rehabilitation strategies, including blood flow restriction training, anti-gravity treadmill use, and return-to-play criteria. Complementary to the literature, we report results from a controlled, longitudinal study (n = 137) comparing isokinetic strength and functional outcomes between brace-based and brace-free early rehabilitation after ACL-R using hamstring grafts. Results: The literature reflects a shift from time-based to criteria-driven rehabilitation, emphasizing individualization and functional readiness. Our original data revealed no significant differences in quadriceps and hamstring torque production between groups at 16, 26, and 52 weeks postoperatively. Statistical parametric mapping confirmed the non-inferiority of brace-free rehabilitation in terms of isokinetic performance. Conclusions: ACL therapy has evolved toward personalized, function-oriented rehabilitation. Our findings suggest that postoperative bracing may be unnecessary in many cases, supporting a more progressive approach. Future developments may include markerless motion analysis, AI-supported rehabilitation, and digital health tools to further individualize care.
Keywords:
ACL reconstruction
; brace-free rehabilitation
; isokinetic strength
; return to sport
; statistical parametric mapping
1. Introduction
Injuries to the anterior cruciate ligament (ACL) remain among the most significant challenges in sports, not only due to their immediate impact on physical performance but also because of their long-term implications for joint health and function. Over the past decades, advancements in surgical techniques and rehabilitation protocols have substantially shaped treatment outcomes. Besides that, new challenges emerged, driven by evolving athletic demands, especially at both younger and older ages, and high pressure for an early return to sports, work, and social participation. To understand where ACL therapy and rehabilitation stand today – and where they might go in the future – it is essential to take a step back and examine the development of clinical approaches in this field. This paper aims to provide a comprehensive perspective on how far we have come and what lies ahead in the treatment of ACL injuries.
This article combines a narrative review of the evolution, current practice, and future perspectives of ACL surgery and rehabilitation with a controlled study investigating the role of postoperative bracing in ACL reconstruction. While the review sections aim to contextualize the clinical development in the field, the data section contributes new evidence regarding the effectiveness of brace-free rehabilitation protocols.
ACL injuries are common in both athletes and the general population. The highest incidence rates are observed among athletes aged 15 to 40 who participate in pivoting sports such as soccer, handball, volleyball, and alpine skiing [1]. Most ACL injuries result from non-contact events, particularly during change of direction and landing [2]. Female athletes have an approximately 1 in 10,000 athlete-exposure risk of ACL injury, which is 1.5 times higher than that of male athletes [3]. Unfortunately, the risk of reinjury remains significant [4]. Approximately 35% of athletes do not return to preinjury sport level within two years following anterior cruciate ligament reconstruction (ACL-R) [5,6,7]. Furthermore, recent research indicates that within the first five years after ACLR, 3-22% of athletes experience re-rupture of the reconstructed ACL and 3-24% sustain a rupture of their contralateral ACL [1].
2. Current Evidence and Future Directions in ACL Surgery and Rehabilitation
From Past to Present
Therapy of ACL Injuries: Development of Arthroscopic Surgery
The transition from open to minimally invasive ACL surgery was completed mainly 25 years ago [8,9,10,11,12]. At that time, the patellar tendon was the graft of choice [8,11,13,14,15], while hamstring tendon grafts were continuously gaining popularity [16,17,18,19]. The additional augmentation with a synthetic ligament showed poor results and was abandoned [20]. In parallel, new fixation techniques for anchoring the ACL grafts were developed [16,21,22,23].
One of the most significant developments of the past 25 years was the focus on anatomical ACL-R, based on the knowledge of the bundle structure of the ACL [24]. As a result, the double-bundle reconstruction of the anteromedial and posterolateral bundles temporarily became the focus of scientific interest [25,26,27]. However, in many studies, the double-bundle technique did not lead to significantly better functional and clinically subjective outcomes compared to the single-bundle technique [24,28,29].
Awareness of concomitant injuries to lateral extracapsular knee structures in ACL ruptures paved the way for the next developmental step [30,31,32,33] and led to the establishment of additional anterolateral tenodesis techniques [34,35,36,37,38]. This reduced the rate of recurrent ruptures [39,40,41]. In recent years, an increased posterior tibial slope has been identified as a risk factor for ACL rupture and graft failure following ACL reconstruction. Therefore, slope-reducing surgical techniques have been developed, which are currently used after failed ACL reconstruction [42,43,44].
Rehabilitation of ACL Injuries: Development of Treatment Protocols
From an evolutionary perspective, the treatment of ACL injuries has not only been driven by advances in arthroscopy. Rehabilitation after ACL-R has also changed significantly over the past 25 years. These changes affect various areas and include differences in early-stage rehabilitation, e.g., updated recommendations for post-operative bracing or the overall duration of rehabilitation. In addition, ACL-R treatment methods have been further developed and optimized, particularly regarding open vs. closed kinetic chain exercise, the use of innovative training tools such as anti-gravity treadmills or blood flow restriction training, prehabilitation approaches, options for conservative management, and the criteria-based return-to-sports (RTS) process. The following sections provide a brief overview of the development of each of the areas mentioned above.
Early-Stage Rehabilitation
Traditional approaches to ACL-R rehabilitation were characterized by delayed weight-bearing and phases of immobilization [45]. In 1990, Shelbourne and Nitz [45] already advocated for accelerated rehabilitation, including immediate weight-bearing and full knee extension on the first postoperative day. Before 1986, full weight-bearing was permitted only after eight weeks, and active range of motion (ROM) was restricted during the same period [45]. Subsequent studies demonstrated that accelerated rehabilitation is not harmful and can be effective for patients with certain graft types [46,47,48]. This is further supported by recent guidelines from Van Melick et al. (2016), which emphasize that immediate weight-bearing does not compromise knee laxity and is associated with a reduced incidence of anterior knee pain [1].
Duration of the Rehabilitation Process
Earlier approaches to ACL-R rehabilitation commonly used fixed timeframes—typically around six months—until the end of rehabilitation. These protocols lacked individualization and did not incorporate objective criteria to guide return-to-sport decisions. While conceptual frameworks for criterion-based rehabilitation were proposed relatively early, they were not widely implemented in clinical practice [49]. Current guidelines emphasize the use of functional criteria to guide the rehabilitation process and recommend longer rehabilitation timeframes, delaying return to sport until 9-12 months post-surgery to accommodate the biological healing of the graft [1,50,51]. Recent research indicates that critical biological healing processes are still ongoing at the time when athletes traditionally resume sports activities [52]. Claes et al. (2011) reported that the timeframe for ligamentization (the biological process where a tendon graft, used to replace a torn or damaged ligament, transforms and remodels to resemble the original ligament tissue) is not well-defined and may extend beyond 12 months after surgery [53]. Evidence suggests that delaying RTS, which promotes graft integration and maturation, significantly decreases the risk of reinjury [54]. More specifically, every one-month delay in RTS up to nine months after surgery was associated with a 51% reduction in knee re-injury rates [54].
Prehabilitation
Over the years, preoperative rehabilitation, termed prehabilitation, has gained increasing attention in the context of ACL-R. According to a review by Brinlee et al. (2022), the success of ACL-R depends on both preoperative and postoperative rehabilitation [51]. The preoperative phase should focus on eliminating knee effusion, restoring full active and passive ROM, and achieving at least 90% quadriceps strength symmetry [52]. Van Melick et al. (2016) reported predictive factors, including a preoperative knee extension deficit and a preoperative quadriceps strength deficit of >20%, that are associated with significantly poorer self-reported outcomes two years after ACL-R [1]. In addition to these physiological goals, mental preparation is also essential. Educating patients about the postoperative rehabilitation process and the expected timeline helps create realistic expectations [51]. Future research will determine whether improved surgical techniques and rehabilitation algorithms, including prehabilitation programs, can meet these expectations.
Open vs. Closed Kinetic Chain Exercises
Debate continues over open vs. closed kinetic chain exercises in ACL rehab. Early protocols favoured closed chain exercises, but Wright et al. (2008) found that adding open chain exercises from six weeks post-surgery may be safe and beneficial, though more research was needed. [55]. Further studies compared early (4 weeks) versus late (12 weeks) start of open kinetic chain exercises and compared ACL-R with bone-patellar tendon-bone graft (BPTB) and hamstring graft (HS). The HS group with an early start had more knee laxity 7 months after surgery in comparison to the other group [56]. Therefore, Fukuda et al. (2013) limited the ROM in their study and concluded that open kinetic chain can be started from week 4 after ACL-R with HS, but only within a “safe-zone” ROM of 90°-45° knee flexion [57].
Therefore, a more recent guideline from 2016 provides specific recommendations for integrating open kinetic chain [1]. The authors suggest that both open and closed kinetic chain exercises can be used to restore quadriceps strength. In ACL-R, using BPTB, open kinetic chain exercises can be performed from the fourth postoperative week onward within a restricted ROM (90-45°) and extra resistance [1]. For HS, open kinetic chain exercises can also be started from the fourth postoperative week onward within a restricted ROM (90-45°). However, no additional weight should be applied within the first 12 weeks to prevent graft elongation [1]. For both graft types, ROM can be increased to 90-30° in week 5, to 90-20° in week 6, to 90-10° in week 7 and to full ROM in week 8 [1].
Innovative Training Tools
In recent years, several innovative training tools have been implemented in ACL-R rehabilitation and routinely applied in clinical practice in addition to traditional training means. These include special devices that enable anti-gravity treadmill (AGT) and blood flow restriction (BFR) training. Both methods have promising effects on the outcome after ACL-R, as they allow early functional treatment under controlled training loads that counteract the negative consequences of unloading or immobilization.
AGT-Training is a therapeutic option that enables partial body weight support of up to 80% of the patient’s body weight during functional movement activities such as walking, running, or even jumping. AGT devices use air blown into an airtight chamber installed above a standard treadmill, with patients wearing special shorts attached to the airbag. This creates a positive pressure below the patient’s waist which can be used to specifically reduce body weight, allowing for controlled, weight-supported locomotion according to the surgeon’s post-treatment recommendations [58].. The AGT-induced reduction of impact forces and metabolic demand enables early mobilization without overloading healing tissues during the immediate postoperative period, when complete weight-bearing activities are often not clinically recommended or tolerated by the patient [59]. In addition, by decreasing the mechanical load on joints and muscles, AGT-Training can promote pain-free movement, maintain cardiorespiratory fitness, support muscle activation, alleviate the effects of muscle atrophy, and preserve gait and running mechanics [59,60]. Furthermore, AGT-Training can even contribute to faster mental recovery and higher motivation by exposing patients to functional and sport-specific tasks more quickly in the rehabilitation process. In summary, AGT-Training is an effective method for targeted weight-supported mobilization with movement stimuli similar to ground locomotion.
By applying low mechanical loads, BFR training is becoming increasingly important as a safe and effective method for muscle preservation or for promoting early muscle growth and strength as part of a preoperative or rehabilitative training program [61,62]. BFR stimuli can be administered either passively without voluntary muscle activation (e.g. immediately after ACL surgery, bed rest) [63] or actively during aerobic exercise (e.g., cycling) or low-load resistance training (e.g., knee extensions, squats). During BFR training, pneumatic cuffs are placed proximally on the limbs to reduce arterial inflow and block venous return, inducing distal ischemia and hypoxia [64]. This triggers anaerobic metabolite buildup and energy depletion in muscles [65]. The resulting metabolic stress and cell swelling activate anabolic pathways and satellite cells, promoting hypertrophy and angiogenesis [66]. Additional mechanisms may include increased anabolic hormone release and enhanced neural drive with preferential recruitment of type II fibres [62].
To optimize muscle hypertrophy, moderate training loads of 60 to 80% of the individual maximum strength (one-repetition maximum, 1 RM) are recommended in training practice, with gains in maximum strength even benefiting from higher loads (> 80% 1 RM) [67]. However, such training loads are initially contraindicated after surgery [68]. BFR-Training, therefore, provides a valuable alternative to high-load strength training, as only low mechanical loads between 20-40% 1RM are utilized [64]. Recent meta-analytic evidence suggests that BFR training has similar effects on muscle hypertrophy as high-load strength training in healthy subjects. At the same time, there are mixed results regarding the BFR-related muscle strength response [69].
Evidence on preoperative BFR training before ACL-R is mixed. Some studies show improved knee extensor strength and endurance before surgery and up to four weeks post-op [70,71]. However, others report no significant benefits on muscle strength or volume pre-surgery or within 12 weeks post-op [71,72,73]. Methodological differences and limited data make definitive conclusions difficult.
In the context of ACL-R rehabilitation, passive BFR interventions in intermittent mode have been shown to preserve muscle strength after immobilization [74] and prevent knee extensor muscle atrophy in the first two weeks after ACL-R [63], especially when combined with neuromuscular electrical stimulation [75]. However, using similar BFR training protocols, Iversen et al. (2016) did not observe a reduction in muscle atrophy in the early phase after ACL-R [76].
Regarding active BFR interventions, Hughes et al. (2017) showed that low-load BFR training led to higher gains in muscle strength than classical resistance training with the same load, but is less effective compared to high-load strength training [75]. However, subjects were more compliant in the BFR group, justifying the temporary use of BFR training when patients are unable to tolerate heavy loads. In a subsequent study, the same authors demonstrated that an 8-week BFR intervention induced similar hypertrophy and strength effects compared to high-intensity strength training (70% 1RM) after ACL-R, with BFR subjects reporting higher scores in subjective knee function and less pain and swelling [77]. Furthermore, Ohta et al. (2003) even observed superior effects of a 16-week BFR intervention on muscle strength and muscle hypertrophy after ACL-R compared to a control training group [78]. In contrast, Curran et al. (2020) could not demonstrate any additional hypertrophy and strength gains from an 8-week BFR intervention after ACL-R when BFR training was applied at high loads (70% 1RM) compared to high-load strength training without BFR [79]. Beneficial effects of BFR-Training therefore only seem to occur in combination with low loads (20 to 40% 1RM). In summary, most studies show that BFR interventions can mitigate early strength loss and muscle atrophy and can induce similar hypertrophy and strength effects during ACL-R rehabilitation compared to high-intensity strength training. Therefore, BFR training seems to be a helpful method that should be regularly implemented in ACL-R rehabilitation.
Conservative Management
Recent studies show that conservative management can be effective for some patients [80]. Especially activity demands, rather than knee stability, may be the primary factor in treatment decisions [81]. It is recommended that ACL-R should be considered when the patient suffers from functional instability, has high activity demands, and/or has a concomitant injury that should be treated with initial surgery [82]. A systematic review comparing conservative vs. surgical treatment observed higher stability and more extended recovery periods in patients undergoing surgery [80].
Return-to-Play Process
The development of progression guidelines and return-to-play (RTP) criteria represented an essential advance in ACL-R rehabilitation. Since the late 1990s, there has been a shift from strictly time-based approaches to comprehensive, objective, and individualized assessments to optimize clinical decision-making regarding an athlete’s RTP readiness following ACL-R [51]. Typically, an RTP test battery using predefined criteria is recommended, including strength, jump, and hop tests as well as movement quality assessments and psychological evaluations [1]. Psychological readiness, in particular, is increasingly recognized as a crucial factor in RTP decisions [83]. There is evidence that meeting specific clinical discharge criteria before RTP is associated with a reduced risk of knee re-injury ranging between 60 to 84 % [54,84,85]. In addition, Grindem et al. (2016) showed that delaying RTP until 9 months after ACL-R contributes to further risk reduction [54]. However, it remains controversial whether the decrease in injury risk is due to improved biological healing or enhanced physiological and psychological readiness, or a combination of both. Considering biological healing time and objective RTP cut-off criteria currently appears to be the best-practice strategy for successful RTP [51].
The RTP process is usually broken down into different stages or phases of rehabilitation, structured in a hierarchical order [86]. Various terms and definitions of phases can differ considerably in their meaning and objectives for the injured athlete [87]. Therefore, there should be clear coding of the different RTP phases in each setting. A typical classification of the RTP continuum is shown in Table 1. Following clinical care (RFS) and restoration of activities of daily living (RTA), ACL-R rehabilitation can generally be divided into three consecutive sporting phases that include different training goals. The Return-to-Running (RTR) phase focuses on the regeneration and intensification of the linear running pattern and the development of the energy systems. The Return-to-Sports (RTS) phase refers to the initiation of sport-specific training loads as part of the individual on-field rehabilitation and restricted team training. The RTS phase is therefore an essential link between general and sport-specific training interventions. The goals are to further increase muscle and strength levels, re-educate and stabilize athletic movement patterns, intensify plyometric and speed stimuli, and develop endurance capacity. Other approaches define RTS as the unrestricted return to the pre-injury sport, but at a lower level of performance [87]. In some cases, this can be a satisfactory outcome and not an unrealistic scenario, especially for amateur athletes [86]. The RTP phase marks the start of full team training, which prepares for gradual reintegration into competitive match play. In addition to maintaining physical qualities, the objectives are to restore sport-specific performance until a full return to competition (RTC) can occur.
Current RTP approaches favor a criteria-based rehabilitation algorithm based on knee function and physical performance [1]. To enter the next phase, specific progression criteria must be met, as purely time-based rehabilitation programs do not consider the athlete’s individual recovery process [88,89,90]. This is important since the severity of the injury, concomitant pathologies, injury history, and patient-specific functional deficits require an individualized training prescription with consistent monitoring of performance progress throughout the RTP process. Table 2 shows an example of a time- and criteria-based rehabilitation scheme, based on the empirical data and the RTP phase model [1,49,88,89,90,91,92,93,94,95,96].
Athletes who return to pivoting sports have a higher risk of ACL re-injury than those who did not [54], especially young athletes within the first two years after ACL-R [97]. This group would benefit from a precise analysis of the movement quality and the resulting joint loading during jump and change-of-direction tasks. The latter is strongly related to the mechanism of ACL injury [98]. Of particular interest is the knee valgus moment (KVM) as a function of the angle of change of direction. The KVM characterizes the medio-lateral force effects and thus serves as an indirect indicator of coronary joint and ligament loading. Specifically, angles of shift in direction between 45° and 105° induce the highest KVMs due to increasing rotational and deceleration loads. Therefore, a thorough 3D movement analysis of jump and change of direction competencies should be carried out to identify athletes with faulty movement patterns and to counteract possible worst-case scenarios during training and competition. The current gold standard method for accurately measuring joint kinematics and kinetics is a 3D marker-based motion analysis system. Figure 1 shows an example of the knee valgus moment during a planned 90° change of direction task in a professional soccer player 9 months after ACL-R. There is an increased knee valgus loading on the operated (blue line) compared to the non-operated leg (red line). In addition, the rotational instability of the core (i.e., lack of alignment with the intended direction of travel) may further contribute to an increased knee valgus loading. Consequently, the athlete should primarily optimize the change of direction technique before RTP.
Bracing
Limiting post-surgical range of motion (ROM) by bracing after ACL-R has been a common practice during the early phases of rehabilitation. Rigid frame orthoses are believed to prevent loss of extension, decrease pain, and protect the graft from excessive strain [99]. However, evidence suggests that postoperative bracing after ACL-R may not provide significant clinical benefit and improve subjective outcome, even in the presence of relevant concomitant knee injuries [100]. Some authors also describe detrimental effects of orthoses use such as delayed time to full weight bearing or decreased muscle activation and joint swelling [100,101,102]. In summary, multiple systematic reviews have found no support for routine use of braces to reduce pain, improve function, and stability [47,48,99,103,104]. This is underlined by the authors’ workgroup recent work, which also demonstrated the non-inferiority of a brace-free rehabilitation protocol after ACL-R regarding self-reported knee function (e.g., International Knee Document committee, IKDC; Lysholm Score) and objective assessments such as peak isokinetic knee strength or limb asymmetry in joint kinematics during gait, running and jumping tasks [105].
Summary of the Current State
In summary, rehabilitation after ACLR over the last decades has shifted from being primarily dictated by surgical limitations to being driven by rehabilitation requirements. Advances in surgical techniques now enable more robust reconstructions that tolerate early mobilization and strengthening, promoting faster functional recovery and improved patient outcomes. As a result, modern rehabilitation protocols focus on individualized, criteria-based progression rather than rigid, time-based schedules. This evolution underscores the importance of integrating surgical innovation with evidence-based rehabilitation strategies to optimize long-term success.
Fom Present to Future
After reflecting on the developments of the past quarter-century, we now have a look on the future of ACL therapy and rehabilitation. In the coming decades, this field will likely undergo relevant shifts driven by scientific, technological, and clinical innovation. Broader societal trends – such as digitalization, data-driven decision-making, and a growing emphasis on prevention – might influence both surgical and rehabilitative strategies. This forward-looking section focuses on the prevention of ACL injury, the future of arthroscopic surgery, marker-less movement analysis, digital health applications, and the use of AI.
Prevention of ACL Injury
Despite aiming to optimize the surgical technique and rehabilitation, an ACL injury remains a significant burden for the patient. Even following successful surgical intervention, long-term consequences such as persistent functional impairments, an increased risk of osteoarthritis, and the likelihood of early degenerative knee surgery remain significant concerns [106]. From a health-economic perspective, ACL injuries result in substantial direct and indirect costs, including expenses for ACL-R and rehabilitation, productivity losses due to time off work, and the potential for premature end of career [106].
Therefore, understanding the primary risk of an ACL injury is of high importance. Over the last years, it has been shown that prevention programs can effectively reduce ACL injuries. Webster and Hewett [107] were able to show an overall reduction of 50% in the risk of ACL injuries by ACL injury prevention training programs [107]. Several evidence-based prevention programs have been developed and successfully implemented. Among the most established are the FIFA 11+, the PEP (Prevent Injury and Enhance Performance) Program, and the ESSKA-ESMA’s “Prevention for All” [108,109]. Despite knowing that a substantial reduction in ACL injury risk is possible, there remains a problem regarding the implementation of these programs. In the next 25 years, prevention programs should be integrated comprehensively into sports club and schools as soon as possible. However, one of the greatest challenges in sports medicine is turning scientific evidence into effective real-world practice. Currently, the prevention of ACL injuries is predominantly implemented on an individual level – for example, when a coach or a specific club chooses to adopt preventive measures. However, in the coming years, it will be essential that the importance of implementing these prevention strategies is recognized at a significantly higher level. This includes institutions such as sports federations, schools, and other organizational bodies. Only when prevention is embraced and supported at these broader structural levels can it be effectively and widely implemented.
Therapy of ACL Injuries: Development in ACL Surgery
Technical Innovations
Surgical errors still occur in the execution of ACL surgeries, for example in tunnel placement, graft harvesting, or graft fixation [110]. Inadequate training and lack of experience are possible causes. In line with this, good outcomes correlate with the number of ACL reconstructions performed by the respective surgeon [111]. Therefore, innovative training concepts are needed. In addition to the already established use of simulators, VR headsets may further optimize surgical training in ACL procedures in the future [112]. It remains to be seen whether new intraoperative navigation technologies can improve quality while also considering time and cost factors [113]. At the same time, it is the responsibility of policymakers to initiate a quality campaign by mandating minimum case volumes.
Development of ACL Repair
The body’s natural repair processes following an ACL rupture typically result in the formation of insufficient scar tissue that does not provide lasting ligament stability. Although innovative suture techniques can achieve good outcomes in selected patients (depending on tear pattern, patient age, accompanying injuries, and activity level) [114,115], the replacement of the ruptured ACL remains the gold standard.
Tissue engineering in the context of ACL repair is still experimental and has not yet demonstrated in situ improvement of the healing process [116,117]. Promising – though still lacking clinical application – is the therapeutic (non-viral or adenoviral) gene transfer (e.g., TGF-β, miRNA, BMP-12) using biomaterials such as type I collagen gel. In the future, this approach could potentially redefine the current limitations of biological ACL healing [116].
Rehabilitation of ACL Injuries
Markerless Motion Capture
The current gold standard for non-invasive video-based motion capture is bi-planar videography. However, this method is associated with high costs, small capture volume, and an exposure to radiation which makes it impractical for clinical or sporting application [118]. Instead, marker-based motion capture is often being treated as a gold standard due to its low errors in comparison. Marker-less motion capture (MMC) systems are emerging as promising tools for assessing movement both in clinical and sports setting. In comparison to marker-based methods they offer advantages such as reduced setup and processing time, as well as no soft-tissue artefacts [119]. In MMC standard video (single or multiple cameras) is used to record movement without markers. To identify the positions and orientations of the body segments, deep learning-based software is used [118].
Currently, measuring temporo-spacial parameters in MMC seems to have a good accuracy compared to marker-based motion capture, however, joint center locations and joint angles are yet not sufficiently accurate for clinical applications [118]. Existing open-source pose estimation algorithms were not originally developed for biomechanical purposes, leading to inconsistently and inaccurately labelled training datasets. To advance the field, future work must focus on improving the quality of these datasets and validating marker-less motion capture systems against gold-standard methods. In the next 25 years, MMC is expected to evolve from an experimental tool into a practical, AI-driven, and personalized rehabilitation technology, with significant relevance for the treatment and long-term management of ACL injuries.
Digital Health Application
Digital health applications are increasingly recognized as effective tools in ACL-R rehabilitation, showing promising results when used alongside standard care. For instance, a randomized controlled trial demonstrated that combining the Orthopy app with conventional therapy led to significant improvements in pain, symptoms, and quality of life for post-ACL surgery patients [120]. Similarly, the TRAK web-based platform was well-received by both patients and physiotherapists, contributing to increased confidence and motivation during the rehabilitation process [121]. As access to internet-connected devices becomes more widespread, digital technologies such as eHealth and mHealth (mobile-based eHealth) are playing a growing role in sports medicine [122]. These digital solutions have the potential to enhance both the efficiency and quality of care, underscoring their likely importance in the future of ACL rehabilitation.
The Use of AI in Rehabilitation
AI marks the fourth industrial revolution and represents the next frontier in medicine, with the potential to transform orthopaedics and sports medicine. However, a full understanding of its core principles and seamless integration into clinical practice are still in the early stages [123].
The following section comprises recent advances in the integration of AI methodology in
- Injury and Treatment Outcome Prediction
- Diagnostic
- Rehabilitation
- Limitations and ethical concerns
Injury and Treatment Outcome Prediction
Machine learning (ML) is well-suited for predicting ACL injury/reinjury risk and optimizing peri- and postoperative care [124]. Early applications included pattern recognition in radiology. Pedoia et al. trained an AI to distinguish healthy from ACL-injured knees via tibial and femoral bone morphology, identifying condylar distance and tibial plateau slope as key markers. Tamimi et al. extended this to injury prediction using MRI-derived measurements of bone and meniscal slopes, achieving >90% accuracy[125].
ML also excels in analyzing 3D motion data. Taborri et al. developed an algorithm using inertial sensors and optoelectronics to assess jump mechanics and predict injury risk, with high correlation to expert human scoring [126]. Johnson et al. used a convolutional neural network (CNN) to analyze 3D knee kinematics during athletic tasks, showing strong correlation (r = 0.8895) during sidestepping compared to traditional regression models[127]. Richter et al.’s neural network predicted injury risk from drop jumps with up to 81% accuracy [128].
Martin et al. externally validated an ML model using data from national registries (NKLR, DKLR) to predict ACL revision risk with moderate accuracy based on five variables, noting the need for more comprehensive datasets [129]. Kakavas et al. highlighted the promise of deep learning (DL) in improving injury screening and return-to-sport assessments [130,131]. The literature increasingly supports AI’s utility in predicting both initial and recurrent ACL injuries [124].
In perioperative management, Anderson et al. developed an AI model to predict prolonged opioid use post-ACL surgery (AUC = 0.77), offering a patient-friendly risk score [132]. Additional models trained on military data support clinical decision-making for opioid overuse. Other ML tools incorporating patient factors (e.g., sex, tobacco use, perioperative drugs) predict the need for femoral nerve block (FNB) with AUCs up to 0.7 [133]
Diagnostic
AI, DL, and neural networks have shown high accuracy in orthopaedic image interpretation, such as detecting proximal humeral fractures and ACL or meniscal injuries in MRI [134,135]. Some algorithms reached specificity levels of 0.968 for ACL tears, comparable to radiologists (0.933), and can analyze 120 MRIs in 2 minutes—work equivalent to 3 hours for a radiologist [124]. Rather than replacing clinicians, AI serves as a diagnostic aid, improving sensitivity by 5% and enhancing overall performance in identifying ACL tears.
Stajduhar et al. used a support vector machine (SVM) to detect both partial and complete ACL tears, achieving AUCs of 0.894 and 0.943, respectively [136]. Li et al. reported DL models with sensitivity (96.78%), specificity (90.62%), and accuracy (92.17%) comparable to arthroscopy in classifying ACL integrity [137].
Diagnosing ACL injuries remains clinically challenging. SVMs interpreting pivot-shift tests offer objectivity in a variable assessment, distinguishing low- from high-grade injuries with 86% sensitivity and 90% specificity [138]. Intraoperatively, AI helps identify anatomical landmarks and improves tunnel placement accuracy in ACL reconstruction [139,140]. Real-time segmentation during arthroscopy may enhance both surgical training and future robotic procedures [124].
AI’s potential also extends to tissue engineering. Though not yet applied to ACL repair, AI has successfully predicted cell differentiation in cardiac tissue, and may help replace empirical methods in complex tissue modeling [141].
Rehabilitation
Nearly 30 years ago, Dye et al. envisioned AI’s role in post-surgical rehab through motion capture and wearable sensors to detect deviations from expected recovery and suggest adjustments [142]. More recently, Gokeler [95,143] highlighted AI’s ability to analyze biomechanical data, classify movement patterns as safe or at-risk, and aid clinicians in interpreting complex datasets. Wearable sensors can now detect movement discrepancies between lab and field environments during return-to-sport assessments in near real-time.
AI-assisted telerehabilitation has shown superior short-term outcomes compared to conventional programs. In-person sessions also benefit from AI-driven biofeedback systems that support motor control recovery by identifying abnormal movement patterns [144]. DL algorithms can enhance load management and rehabilitation monitoring after ACL injury, enabling frequent, objective, and personalized assessments [145].
Emerging applications include brain-computer interfaces (BCI) to promote neuroplasticity and relearn movement patterns. BCI translates brain activity into control signals, and its effectiveness may be improved through AI-enhanced signal processing. Though successful in stroke rehabilitation, its utility in sports injury recovery remains under investigation [146].
Limitations and Ethical Concerns
The integration of AI into clinical care raises significant ethical concerns, including patient privacy, data security, algorithmic bias, and the risk of clinician deskilling. Ensuring fairness, transparency, and informed consent is crucial. While AI offers substantial benefits in diagnosis, surgery, and rehabilitation, it requires clear regulatory standards and ongoing human oversight to mitigate risks and ensure safe, equitable care [123].
Despite the increasing digitalization and personalization of rehabilitation strategies outlined above, many aspects of ACL rehabilitation are still based on longstanding conventions rather than robust evidence. One such example is the routine use of postoperative bracing. Although widely practiced, the clinical benefit of early immobilization via orthoses remains controversial. Our research group conducted a controlled, longitudinal study to evaluate whether brace-free rehabilitation after ACL reconstruction is functionally equivalent to conventional brace-based protocols. The following section outlines the methodology and results of this investigation.
3. Materials and Methods
The methods described in the following section refer exclusively to the original data component of this work.
This randomized controlled trial with a 1:1 allocation was conducted at a tertiary trauma centre in Germany. Ethical approval was granted by the Institutional Review Board of Witten/Herdecke University (Ref. 14/2015) on July 7, 2015. Eligible participants were adults aged 18–60 years (BMI < 35 kg/m²) undergoing primary ACL reconstruction using ipsilateral hamstring tendons. Written informed consent was obtained. Minor meniscal lesions not requiring repair and previous contralateral injuries without functional impairment did not lead to exclusion. Patients with additional ligament injuries, prior ligament surgeries, advanced osteoarthritis (Kellgren–Lawrence ≥ 3), cartilage procedures, or required meniscal repair were excluded [105].
Details regarding surgical procedure can be found elsewhere [105]. In this study a total of 138 patients of the general public was assigned in either intervention group (n=69), receiving the initial 6-weeks of post-surgical rehabilitation without orthosis, or control group (n=68) which was treated with orthosis to limit ROM to extension/flexion 0-0-90° during the first 4 weeks with no further limitation for another 2 weeks. Both groups showed a statistically comparable profile regarding demographics, injury, and sports level. They were tested at baseline (t0), 6- (t1), 16- (t2), and 26- (t3) weeks postoperatively, with the 52- (t4) weeks follow-up appointment being the primary study endpoint.
Isokinetic strength testing was collected at a frequency of 100 Hz on a Biodex System 3 device (Biodex Medical Systems, Inc., Shirley, New York, NY, USA). Data was corrected for gravity and normalized to body weight, reported as mean relative peak torque filtered by a second-order 5 Hz Butterworth low-pass bidirectional filter.
Instead of interpreting inter-limb differences based on peak or mean values, we further used statistical parametric mapping (SPM) as a means of analyzing kinetic data in this study. Previous studies have used this approach to evaluate kinematic and kinetic data, such as joint angular motion and ground reaction forces, following ACL-R. SPM has recently emerged as a promising alternative to traditional statistical methods, as it better captures the continuous, waveform-like characteristics of time-dependent data [147].
Technically, the SPM procedure consists of a SPM two-tailed t-test that compares the torque-time trajectory between the braced and unbraced conditions. A critical threshold was computed, beyond which the null hypothesis is rejected, and a significant difference is assumed. Due to waveform smoothness and temporal correlation, significant regions often span multiple adjacent points, forming so-called "supra-threshold clusters" (STCs). Where appropriate, we report cluster-specific p-values, indicating the likelihood that these STCs could arise by chance. In the case of significant group differences, we also report the effect size (Cohen’s d ± CI), with thresholds of 0.2, 0.5, and 0.8 representing small, medium, and significant effects, respectively.
4. Results
The following section presents results from our original study on postoperative bracing in ACL rehabilitation. These findings complement the broader context discussed in the narrative part of this work.
Our data show a complete longitudinal comparison between the groups regarding their isokinetic force production profile for slow (60°/s) and fast (240°/s) isokinetic testing velocities (see Table 3).
Figure 2.
Knee extension and flexion torque [Nm/kg] at 60°/sec and 240°/s (c, d) angular velocity for the brace-free (black line) and braced group (red line) 16-weeks, 26-weeks and 52-weeks after surgery (mean torque ± SD). The respective shaded areas show the groupwise standard deviation.
Figure 2.
Knee extension and flexion torque [Nm/kg] at 60°/sec and 240°/s (c, d) angular velocity for the brace-free (black line) and braced group (red line) 16-weeks, 26-weeks and 52-weeks after surgery (mean torque ± SD). The respective shaded areas show the groupwise standard deviation.
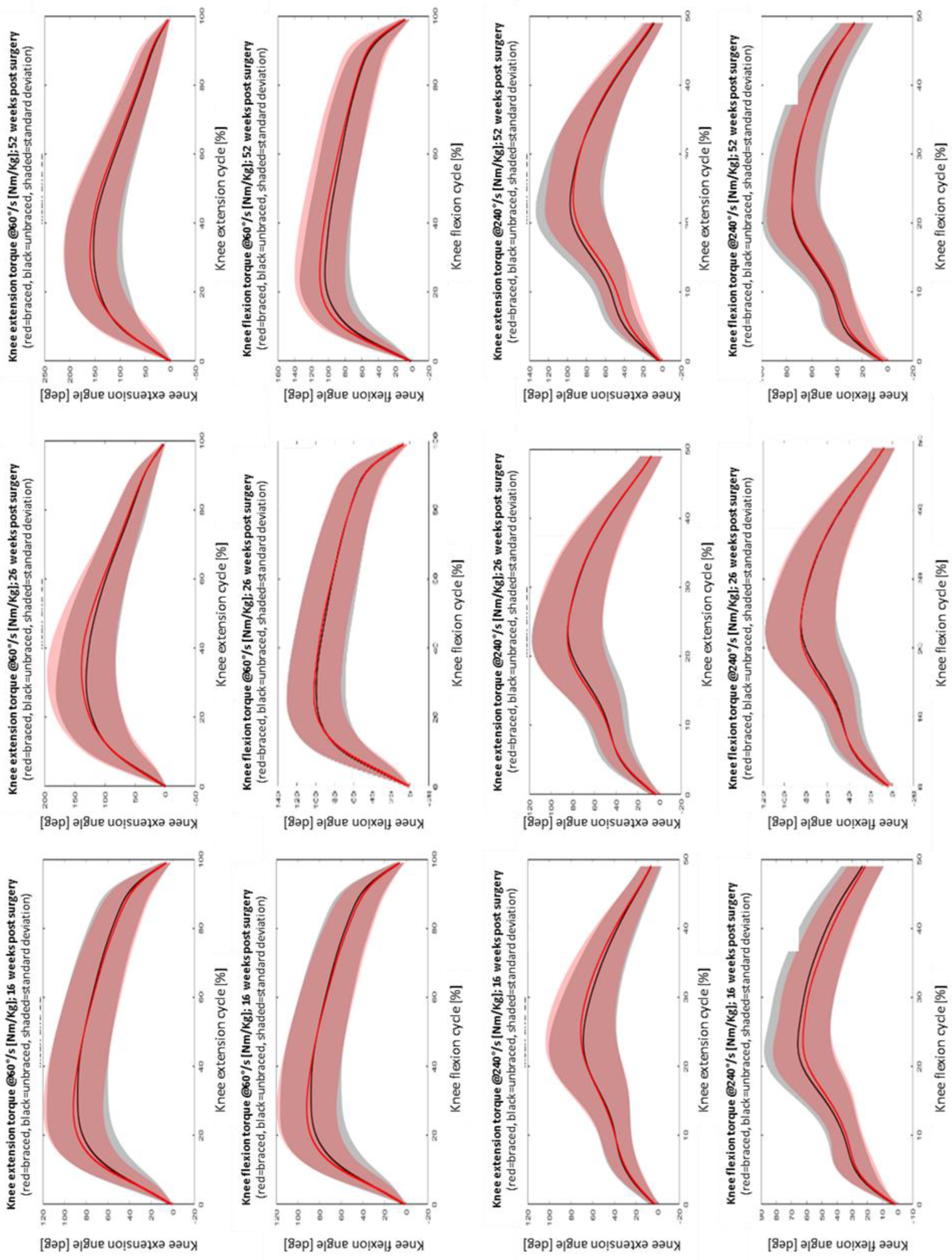
In our sample, no group differences were found for isokinetic torque production at any time point during the first year of rehabilitation. Adhering to a level of significance threshold of 0.05, SPM did not see "supra-threshold clusters" that would indicate a portion of the torque-time trajectory where knee extension or flexion differed; therefore, it is statistically unlikely that our observations are compatible with chance.
5. Discussion
This manuscript integrates a narrative review of the evolution and future of ACL surgery and rehabilitation with original data on the clinical effectiveness of brace-free rehabilitation after ACL reconstruction. Taken together, the findings support a broader shift in clinical practice toward more individualized, evidence-based, and function-oriented rehabilitation strategies.
Our original data provide a focused contribution to the ongoing discussion around the necessity of postoperative bracing. To our knowledge, no study focusing on postoperative bracing has so far analyzed isokinetic torque production after hamstring ACL-R longitudinally using statistical parametric mapping. The SPM procedure generates more precise information on angle-specific strength deficits during crucial phases of the isokinetic motion cycle, e.g., around maxima or minima of knee flexion, where the ability to produce force rapidly is a key factor in maintaining joint stability and safeguarding functional performance. Comparing our results to results published by other researchers we found that the mean torque production during both isokinetic testing velocities were highly similar for the orthosis-based rehabilitation group and the orthosis-free rehabilitation group [148,149,150,151,152,153,154,155]. This is in line with previously published recent work by the author’s group, which also demonstrated the non-inferiority of a brace-free rehabilitation protocol after ACL-R regarding self-reported knee function (e.g., International Knee Document committee, IKDC; Lysholm Score). Based on these results, we conclude that routine postoperative bracing may not offer functional benefits and could potentially be omitted.
Beyond the specific topic of bracing, our narrative review highlights how ACL rehabilitation has evolved substantially over the past 25 years. The transition from time-based to criteria-based rehabilitation, the integration of innovative tools such as BFR training or AGT-training, and the increased attention to prehabilitation and return-to-play decision-making reflect a clear trend toward personalization and functional outcome orientation. However, several practices – such as bracing, early exercise selection, and loading strategies – are still influenced by tradition, surgeon preference, or insurance guidelines rather than robust clinical data.
This review also underlines a critical gap between technological possibility and clinical implementation. Although tools such as markerless motion analysis, wearable sensor technology, and AI-supported rehabilitation systems are rapidly advancing, their real-world integration into ACL rehabilitation remains limited. Additionally, psychological readiness and return-to-sport behavior are still insufficiently addressed in many rehabilitation models, even though they are known predictors of re-injury risk.
Looking ahead, the next 25 years of ACL rehabilitation may be shaped by data-driven decision-making, automated monitoring of load and movement quality, and a stronger focus on preventive strategies embedded in youth sports and public health policy. To achieve this, a paradigm shift is needed – not only in research and clinical routines but also in how evidence is translated into standardized care across health systems.
6. Conclusions
In conclusion, the field of ACL treatment has moved toward individualized and function-oriented rehabilitation strategies. The integration of literature-based insights with our own findings supports the idea that routine bracing may not be necessary in all patients following ACL reconstruction. Combining established surgical advances with progressive, evidence-based rehabilitation protocols may further improve outcomes – especially when aligned with future tools such as AI-assisted analysis and digital health applications.
Author Contributions
Conceptualization, C.S., J.T., A.P. and C.R.; methodology, C.S., J.T., A.P. and C.R.; formal analysis, C.S., J.T., A.P. and C.R.; investigation, A.P. and C.R.; data curation, A.P.; writing—original draft preparation, C.S., J.T., A.P., M.D. and C.R.; writing—review and editing, C.S., J.T., A.P. and C.R.; visualization, C.S., J.T., A.P. and C.R.; supervision, C.S.; project administration, A.P.; funding acquisition, C.S. All authors have read and agreed to the published version of the manuscript.
Funding
The original data presented in this manuscript were collected as part of a research project funded by the German Statutory Accident Insurance (Deutsche Gesetzliche Unfallversicherung, DGUV) under the project reference identifier FF-FR 0251. The funding body had no role in the design, analysis, interpretation, or publication of this manuscript.
Institutional Review Board Statement
Ethical approval was obtained for the original data collection component of this work. The study was approved by the Institutional Review Board (IRB) of the University Witten/Herdecke, Witten, Germany (Reference-No. 14/2015). All procedures were conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants prior to study enrollment.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study
Data Availability Statement
Dataset available on request from the authors
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ACL | Anterior Cruciate Ligament |
| ACL-R | Anterior Cruciate Ligament Reconstruction |
| AGT | Anti-Gravity Training |
| BFR | Blood Flow Restriction |
| BPTB | Bone-patellar tendon-bone graft |
| DL | Deep Learning |
| HS | Hamstring graft |
| KVM | Knee Valgus Moment |
| ML | Machine Learning |
| MMC | Marker-less Motion Capture |
| RFS | Recovery from Surgery |
| RTA | Return-to-Activity |
| RTR | Return-to-Running |
| RTS | Return-to-Sports |
| RTP | Return-to-Play |
| RTC | Return-to-Competition |
| ROM | Range of motion |
| RTS | Return-to-sports |
| STC | Supra-threshold cluster |
| SPM | Statistical Parametric Mapping |
| SVM | Support Vector Machine |
References
- van Melick, N.; van Cingel, R.E.; Brooijmans, F.; Neeter, C.; van Tienen, T.; Hullegie, W.; Nijhuis-van der Sanden, M.W. Evidence-based clinical practice update: practice guidelines for anterior cruciate ligament rehabilitation based on a systematic review and multidisciplinary consensus. Br J Sports Med 2016, 50, 1506–1515. [Google Scholar] [CrossRef]
- Yu, B.; Garrett, W.E. Mechanisms of non-contact ACL injuries. British journal of sports medicine 2007, 41, i47–i51. [Google Scholar] [CrossRef]
- Bram, J.T.; Magee, L.C.; Mehta, N.N.; Patel, N.M.; Ganley, T.J. Anterior cruciate ligament injury incidence in adolescent athletes: a systematic review and meta-analysis. The American journal of sports medicine 2021, 49, 1962–1972. [Google Scholar] [CrossRef]
- Kamath, G.V.; Murphy, T.; Creighton, R.A.; Viradia, N.; Taft, T.N.; Spang, J.T. Anterior cruciate ligament injury, return to play, and reinjury in the elite collegiate athlete: analysis of an NCAA Division I cohort. The American journal of sports medicine 2014, 42, 1638–1643. [Google Scholar] [CrossRef]
- Ardern, C. Fifty-five per cent return to competitive sport fo. 2014.
- Ardern, C.L.; Webster, K.E.; Taylor, N.F.; Feller, J.A. Return to sport following anterior cruciate ligament reconstruction surgery: a systematic review and meta-analysis of the state of play. British journal of sports medicine 2011, 45, 596–606. [Google Scholar] [CrossRef]
- Shah, V.M.; Andrews, J.R.; Fleisig, G.S.; McMichael, C.S.; Lemak, L.J. Return to play after anterior cruciate ligament reconstruction in National Football League athletes. The American journal of sports medicine 2010, 38, 2233–2239. [Google Scholar] [CrossRef]
- Boszotta, H. Arthroscopic anterior cruciate ligament reconstruction using a patellar tendon graft in press-fit technique: surgical technique and follow-up. Arthroscopy 1997, 13, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Brandsson, S.; Faxén, E.; Eriksson, B.I.; Swärd, L.; Lundin, O.; Karlsson, J. Reconstruction of the anterior cruciate ligament: comparison of outside-in and all-inside techniques. Br J Sports Med 1999, 33, 42–45. [Google Scholar] [CrossRef] [PubMed]
- Cameron, S.E.; Wilson, W.; St Pierre, P. A prospective, randomized comparison of open vs arthroscopically assisted ACL reconstruction. Orthopedics 1995, 18, 249–252. [Google Scholar] [CrossRef] [PubMed]
- Deehan, D.J.; Salmon, L.J.; Webb, V.J.; Davies, A.; Pinczewski, L.A. Endoscopic reconstruction of the anterior cruciate ligament with an ipsilateral patellar tendon autograft. A prospective longitudinal five-year study. J Bone Joint Surg Br 2000, 82, 984–991. [Google Scholar] [CrossRef]
- Fu, F.H.; Bennett, C.H.; Ma, C.B.; Menetrey, J.; Lattermann, C. Current trends in anterior cruciate ligament reconstruction. Part II. Operative procedures and clinical correlations. Am J Sports Med 2000, 28, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Jomha, N.M.; Pinczewski, L.A.; Clingeleffer, A.; Otto, D.D. Arthroscopic reconstruction of the anterior cruciate ligament with patellar-tendon autograft and interference screw fixation. The results at seven years. J Bone Joint Surg Br 1999, 81, 775–779. [Google Scholar] [CrossRef]
- Shelbourne, K.D.; Urch, S.E. Primary anterior cruciate ligament reconstruction using the contralateral autogenous patellar tendon. Am J Sports Med 2000, 28, 651–658. [Google Scholar] [CrossRef]
- Fu, F.H.; Schulte, K.R. Anterior cruciate ligament surgery 1996. State of the art? Clin Orthop Relat Res 1996, 19–24. [Google Scholar] [CrossRef]
- Muneta, T.; Sekiya, I.; Yagishita, K.; Ogiuchi, T.; Yamamoto, H.; Shinomiya, K. Two-bundle reconstruction of the anterior cruciate ligament using semitendinosus tendon with endobuttons: operative technique and preliminary results. Arthroscopy 1999, 15, 618–624. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, D.B. Arthroscopically assisted reconstruction of the anterior cruciate ligament. A prospective randomized analysis of three techniques. J Bone Joint Surg Am 1996, 78, 803–813. [Google Scholar] [CrossRef] [PubMed]
- Pinczewski, L.A.; Clingeleffer, A.J.; Otto, D.D.; Bonar, S.F.; Corry, I.S. Integration of hamstring tendon graft with bone in reconstruction of the anterior cruciate ligament. Arthroscopy 1997, 13, 641–643. [Google Scholar] [CrossRef]
- Rosenberg, T.D.; Deffner, K.T. ACL reconstruction: semitendinosus tendon is the graft of choice. Orthopedics 1997, 20, 396–398. [Google Scholar] [CrossRef]
- Kumar, K.; Maffulli, N. The ligament augmentation device: an historical perspective. Arthroscopy 1999, 15, 422–432. [Google Scholar] [CrossRef]
- Abate, J.A.; Fadale, P.D.; Hulstyn, M.J.; Walsh, W.R. Initial fixation strength of polylactic acid interference screws in anterior cruciate ligament reconstruction. Arthroscopy 1998, 14, 278–284. [Google Scholar] [CrossRef]
- Brand, J., Jr.; Weiler, A.; Caborn, D.N.; Brown, C.H., Jr.; Johnson, D.L. Graft fixation in cruciate ligament reconstruction. Am J Sports Med 2000, 28, 761–774. [Google Scholar] [CrossRef]
- Clark, R.; Olsen, R.E.; Larson, B.J.; Goble, E.M.; Farrer, R.P. Cross-pin femoral fixation: a new technique for hamstring anterior cruciate ligament reconstruction of the knee. Arthroscopy 1998, 14, 258–267. [Google Scholar] [CrossRef]
- Meredick, R.B.; Vance, K.J.; Appleby, D.; Lubowitz, J.H. Outcome of single-bundle versus double-bundle reconstruction of the anterior cruciate ligament: a meta-analysis. Am J Sports Med 2008, 36, 1414–1421. [Google Scholar] [CrossRef] [PubMed]
- Buoncristiani, A.M.; Tjoumakaris, F.P.; Starman, J.S.; Ferretti, M.; Fu, F.H. Anatomic double-bundle anterior cruciate ligament reconstruction. Arthroscopy 2006, 22, 1000–1006. [Google Scholar] [CrossRef] [PubMed]
- Fu, F.H.; Shen, W.; Starman, J.S.; Okeke, N.; Irrgang, J.J. Primary anatomic double-bundle anterior cruciate ligament reconstruction: a preliminary 2-year prospective study. Am J Sports Med 2008, 36, 1263–1274. [Google Scholar] [CrossRef]
- Marcacci, M.; Molgora, A.P.; Zaffagnini, S.; Vascellari, A.; Iacono, F.; Presti, M.L. Anatomic double-bundle anterior cruciate ligament reconstruction with hamstrings. Arthroscopy 2003, 19, 540–546. [Google Scholar] [CrossRef]
- Aga, C.; Risberg, M.A.; Fagerland, M.W.; Johansen, S.; Trøan, I.; Heir, S.; Engebretsen, L. No Difference in the KOOS Quality of Life Subscore Between Anatomic Double-Bundle and Anatomic Single-Bundle Anterior Cruciate Ligament Reconstruction of the Knee: A Prospective Randomized Controlled Trial With 2 Years’ Follow-up. Am J Sports Med 2018, 46, 2341–2354. [Google Scholar] [CrossRef]
- Hussein, M.; van Eck, C.F.; Cretnik, A.; Dinevski, D.; Fu, F.H. Prospective randomized clinical evaluation of conventional single-bundle, anatomic single-bundle, and anatomic double-bundle anterior cruciate ligament reconstruction: 281 cases with 3- to 5-year follow-up. Am J Sports Med 2012, 40, 512–520. [Google Scholar] [CrossRef] [PubMed]
- Claes, S.; Vereecke, E.; Maes, M.; Victor, J.; Verdonk, P.; Bellemans, J. Anatomy of the anterolateral ligament of the knee. J Anat 2013, 223, 321–328. [Google Scholar] [CrossRef]
- Claes, S.; Luyckx, T.; Vereecke, E.; Bellemans, J. The Segond fracture: a bony injury of the anterolateral ligament of the knee. Arthroscopy 2014, 30, 1475–1482. [Google Scholar] [CrossRef]
- Kennedy, M.I.; Claes, S.; Fuso, F.A.; Williams, B.T.; Goldsmith, M.T.; Turnbull, T.L.; Wijdicks, C.A.; LaPrade, R.F. The Anterolateral Ligament: An Anatomic, Radiographic, and Biomechanical Analysis. Am J Sports Med 2015, 43, 1606–1615. [Google Scholar] [CrossRef]
- Getgood, A.; Brown, C.; Lording, T.; Amis, A.; Claes, S.; Geeslin, A.; Musahl, V. The anterolateral complex of the knee: results from the International ALC Consensus Group Meeting. Knee Surg Sports Traumatol Arthrosc 2019, 27, 166–176. [Google Scholar] [CrossRef] [PubMed]
- Hollyer, I.; Sholtis, C.; Loughran, G.; Raji, Y.; Akhtar, M.; Smith, P.A.; Musahl, V.; Verdonk, P.C.M.; Sonnery-Cottet, B.; Getgood, A.; et al. Trends in lateral extra-articular augmentation use and surgical technique with anterior cruciate ligament reconstruction from 2016 to 2023, an ACL study group survey. J isakos 2024, 9, 100356. [Google Scholar] [CrossRef]
- Inderhaug, E.; Stephen, J.M.; Williams, A.; Amis, A.A. Biomechanical Comparison of Anterolateral Procedures Combined With Anterior Cruciate Ligament Reconstruction. Am J Sports Med 2017, 45, 347–354. [Google Scholar] [CrossRef]
- McAleese, T.; Murgier, J.; Cavaignac, E.; Devitt, B.M. A review of Marcel Lemaire’s original work on lateral extra-articular tenodesis. J isakos 2024, 9, 431–437. [Google Scholar] [CrossRef]
- Herbort, M.; Abermann, E.; Feller, J.A.; Fink, C. [Anterolateral stabilization using the modified ellison technique-Treatment of anterolateral instability and reduction of ACL re-rupture risk]. Oper Orthop Traumatol 2022, 34, 231–238. [Google Scholar] [CrossRef]
- Neri, T.; Dabirrahmani, D.; Beach, A.; Grasso, S.; Putnis, S.; Oshima, T.; Cadman, J.; Devitt, B.; Coolican, M.; Fritsch, B.; et al. Different anterolateral procedures have variable impact on knee kinematics and stability when performed in combination with anterior cruciate ligament reconstruction. J isakos 2021, 6, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Rezansoff, A.; Firth, A.D.; Bryant, D.M.; Litchfield, R.; McCormack, R.G.; Heard, M.; MacDonald, P.B.; Spalding, T.; Verdonk, P.C.M.; Peterson, D.; et al. Anterior Cruciate Ligament Reconstruction Plus Lateral Extra-articular Tenodesis Has a Similar Return-to-Sport Rate to Anterior Cruciate Ligament Reconstruction Alone but a Lower Failure Rate. Arthroscopy 2024, 40, 384–396.e381. [Google Scholar] [CrossRef] [PubMed]
- Sonnery-Cottet, B.; Thaunat, M.; Freychet, B.; Pupim, B.H.; Murphy, C.G.; Claes, S. Outcome of a Combined Anterior Cruciate Ligament and Anterolateral Ligament Reconstruction Technique With a Minimum 2-Year Follow-up. Am J Sports Med 2015, 43, 1598–1605. [Google Scholar] [CrossRef]
- van der Wal, W.A.; Meijer, D.T.; Hoogeslag, R.A.G.; LaPrade, R.F. The Iliotibial Band is the Main Secondary Stabilizer for Anterolateral Rotatory Instability and both a Lemaire Tenodesis and Anterolateral Ligament Reconstruction Can Restore Native Knee Kinematics in the Anterior Cruciate Ligament Reconstructed Knee: A Systematic Review of Biomechanical Cadaveric Studies. Arthroscopy 2024, 40, 632–647.e631. [Google Scholar] [CrossRef]
- Imhoff, F.B.; Mehl, J.; Comer, B.J.; Obopilwe, E.; Cote, M.P.; Feucht, M.J.; Wylie, J.D.; Imhoff, A.B.; Arciero, R.A.; Beitzel, K. Slope-reducing tibial osteotomy decreases ACL-graft forces and anterior tibial translation under axial load. Knee Surg Sports Traumatol Arthrosc 2019, 27, 3381–3389. [Google Scholar] [CrossRef]
- Mabrouk, A.; Kley, K.; Jacquet, C.; Fayard, J.M.; An, J.S.; Ollivier, M. Outcomes of Slope-Reducing Proximal Tibial Osteotomy Combined With a Third Anterior Cruciate Ligament Reconstruction Procedure With a Focus on Return to Impact Sports. Am J Sports Med 2023, 51, 3454–3463. [Google Scholar] [CrossRef] [PubMed]
- Weiler, A.; Gwinner, C.; Wagner, M.; Ferner, F.; Strobel, M.J.; Dickschas, J. Significant slope reduction in ACL deficiency can be achieved both by anterior closing-wedge and medial open-wedge high tibial osteotomies: early experiences in 76 cases. Knee Surg Sports Traumatol Arthrosc 2022, 30, 1967–1975. [Google Scholar] [CrossRef]
- Shelbourne, K.D.; Nitz, P. Accelerated rehabilitation after anterior cruciate ligament reconstruction. The American journal of sports medicine 1990, 18, 292–299. [Google Scholar] [CrossRef]
- Beynnon, B.D.; Uh, B.S.; Johnson, R.J.; Abate, J.A.; Nichols, C.E.; Fleming, B.C.; Poole, A.R.; Roos, H. Rehabilitation after anterior cruciate ligament reconstruction: a prospective, randomized, double-blind comparison of programs administered over 2 different time intervals. The American journal of sports medicine 2005, 33, 347–359. [Google Scholar] [CrossRef] [PubMed]
- Kruse, L.M.; Gray, B.; Wright, R.W. Rehabilitation after anterior cruciate ligament reconstruction: a systematic review. J Bone Joint Surg Am 2012, 94, 1737–1748. [Google Scholar] [CrossRef] [PubMed]
- Glattke, K.E.; Tummala, S.V.; Chhabra, A. Anterior cruciate ligament reconstruction recovery and rehabilitation: a systematic review. JBJS 2022, 104, 739–754. [Google Scholar] [CrossRef]
- Manal, T.J.; Snyder-Mackler, L. Practice guidelines for anterior cruciate ligament rehabilitation: a criterion-based rehabilitation progression. Operative techniques in orthopaedics 1996, 6, 190–196. [Google Scholar] [CrossRef]
- Kotsifaki, R.; Korakakis, V.; King, E.; Barbosa, O.; Maree, D.; Pantouveris, M.; Bjerregaard, A.; Luomajoki, J.; Wilhelmsen, J.; Whiteley, R. Aspetar clinical practice guideline on rehabilitation after anterior cruciate ligament reconstruction. British Journal of Sports Medicine 2023, 57, 500–514. [Google Scholar] [CrossRef]
- Brinlee, A.W.; Dickenson, S.B.; Hunter-Giordano, A.; Snyder-Mackler, L. ACL Reconstruction Rehabilitation: Clinical Data, Biologic Healing, and Criterion-Based Milestones to Inform a Return-to-Sport Guideline. Sports Health 2022, 14, 770–779. [Google Scholar] [CrossRef]
- Filbay, S.R.; Grindem, H. Evidence-based recommendations for the management of anterior cruciate ligament (ACL) rupture. Best Pract Res Clin Rheumatol 2019, 33, 33–47. [Google Scholar] [CrossRef] [PubMed]
- Claes, S.; Verdonk, P.; Forsyth, R.; Bellemans, J. The “ligamentization” process in anterior cruciate ligament reconstruction: what happens to the human graft? A systematic review of the literature. The American journal of sports medicine 2011, 39, 2476–2483. [Google Scholar] [CrossRef]
- Grindem, H.; Snyder-Mackler, L.; Moksnes, H.; Engebretsen, L.; Risberg, M.A. Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction: the Delaware-Oslo ACL cohort study. British journal of sports medicine 2016, 50, 804–808. [Google Scholar] [CrossRef]
- Wright, R.W.; Preston, E.; Fleming, B.C.; Amendola, A.; Andrish, J.T.; Bergfeld, J.A.; Dunn, W.R.; Kaeding, C.; Kuhn, J.E.; Marx, R.G. A systematic review of anterior cruciate ligament reconstruction rehabilitation–part II: open versus closed kinetic chain exercises, neuromuscular electrical stimulation, accelerated rehabilitation, and miscellaneous topics. The journal of knee surgery 2008, 21, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Heijne, A.; Werner, S. Early versus late start of open kinetic chain quadriceps exercises after ACL reconstruction with patellar tendon or hamstring grafts: a prospective randomized outcome study. Knee Surgery, Sports Traumatology, Arthroscopy 2007, 15, 402–414. [Google Scholar] [CrossRef]
- Fukuda, T.Y.; Fingerhut, D.; Moreira, V.C.; Camarini, P.M.F.; Scodeller, N.F.; Duarte Jr, A.; Martinelli, M.; Bryk, F.F. Open kinetic chain exercises in a restricted range of motion after anterior cruciate ligament reconstruction: a randomized controlled clinical trial. The American journal of sports medicine 2013, 41, 788–794. [Google Scholar] [CrossRef] [PubMed]
- Saxena, A.; Granot, A. Use of an anti-gravity treadmill in the rehabilitation of the operated achilles tendon: a pilot study. J Foot Ankle Surg 2011, 50, 558–561. [Google Scholar] [CrossRef]
- Vincent, H.K.; Madsen, A.; Vincent, K.R. Role of Antigravity Training in Rehabilitation and Return to Sport After Running Injuries. Arthrosc Sports Med Rehabil 2022, 4, e141–e149. [Google Scholar] [CrossRef]
- Cutuk, A.; Groppo, E.R.; Quigley, E.J.; White, K.W.; Pedowitz, R.A.; Hargens, A.R. Ambulation in simulated fractional gravity using lower body positive pressure: cardiovascular safety and gait analyses. J Appl Physiol (1985) 2006, 101, 771–777. [Google Scholar] [CrossRef]
- Minniti, M.C.; Statkevich, A.P.; Kelly, R.L.; Rigsby, V.P.; Exline, M.M.; Rhon, D.I.; Clewley, D. The Safety of Blood Flow Restriction Training as a Therapeutic Intervention for Patients With Musculoskeletal Disorders: A Systematic Review. Am J Sports Med 2020, 48, 1773–1785. [Google Scholar] [CrossRef]
- Franz, A.; Praetorius, A.; Raeder, C.; Hirschmüller, A.; Behringer, M. Blood flow restriction training in the pre-and postoperative phases of joint surgery. Arthroskopie 2023, 1–9. [Google Scholar] [CrossRef]
- Takarada, Y.; Takazawa, H.; Ishii, N. Applications of vascular occlusion diminish disuse atrophy of knee extensor muscles. Medicine & Science in Sports & Exercise 2000, 32, 2035–2039. [Google Scholar] [CrossRef]
- Colapietro, M.; Portnoff, B.; Miller, S.J.; Sebastianelli, W.; Vairo, G.L. Effects of Blood Flow Restriction Training on Clinical Outcomes for Patients with ACL Reconstruction: A Systematic Review. Sports health 2023, 15, 260–273. [Google Scholar] [CrossRef] [PubMed]
- García-Rodríguez, P.; Pecci, J.; Vázquez-González, S.; Pareja-Galeano, H. Acute and Chronic Effects of Blood Flow Restriction Training in Physically Active Patients With Anterior Cruciate Ligament Reconstruction: A Systematic Review. Sports Health 2024, 16, 820–828. [Google Scholar] [CrossRef]
- Rodríguez, S.; Rodríguez-Jaime, M.F.; León-Prieto, C. Blood Flow Restriction Training: Physiological Effects, Molecular Mechanisms, and Clinical Applications. Critical Reviews™ in Physical and Rehabilitation Medicine 2024, 36. [Google Scholar] [CrossRef]
- Schoenfeld, B.J.; Grgic, J.; Van Every, D.W.; Plotkin, D.L. Loading recommendations for muscle strength, hypertrophy, and local endurance: a re-examination of the repetition continuum. Sports 2021, 9, 32. [Google Scholar] [CrossRef] [PubMed]
- Fraca-Fernandez, E.; Ceballos-Laita, L.; Hernandez-Lazaro, H.; Jimenez-Del-Barrio, S.; Mingo-Gomez, M.T.; Medrano-de-la-Fuente, R.; Hernando-Garijo, I. Effects of Blood Flow Restriction Training in Patients before and after Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-Analysis. Healthcare (Basel) 2024, 12. [Google Scholar] [CrossRef]
- Lixandrão, M.E.; Ugrinowitsch, C.; Berton, R.; Vechin, F.C.; Conceição, M.S.; Damas, F.; Libardi, C.A.; Roschel, H. Magnitude of muscle strength and mass adaptations between high-load resistance training versus low-load resistance training associated with blood-flow restriction: a systematic review and meta-analysis. Sports medicine 2018, 48, 361–378. [Google Scholar] [CrossRef]
- Kacin, A.; Drobnic, M.; Mars, T.; Mis, K.; Petric, M.; Weber, D.; Tomc Zargi, T.; Martincic, D.; Pirkmajer, S. Functional and molecular adaptations of quadriceps and hamstring muscles to blood flow restricted training in patients with ACL rupture. Scand J Med Sci Sports 2021, 31, 1636–1646. [Google Scholar] [CrossRef]
- Žargi, T.; Drobnič, M.; Stražar, K.; Kacin, A. Short–term preconditioning with blood flow restricted exercise preserves quadriceps muscle endurance in patients after anterior cruciate ligament reconstruction. Frontiers in physiology 2018, 9, 1150. [Google Scholar] [CrossRef]
- Tramer, J.S.; Khalil, L.S.; Jildeh, T.R.; Abbas, M.J.; McGee, A.; Lau, M.J.; Moutzouros, V.; Okoroha, K.R. Blood Flow Restriction Therapy for 2 Weeks Prior to Anterior Cruciate Ligament Reconstruction Did Not Impact Quadriceps Strength Compared to Standard Therapy. Arthroscopy: The Journal of Arthroscopic & Related Surgery 2023, 39, 373–381. [Google Scholar]
- Zargi, T.G.; Drobnic, M.; Jkoder, J.; Strazar, K.; Kacin, A. The effects of preconditioning with ischemic exercise on quadriceps femoris muscle atrophy following anterior cruciate ligament reconstruction: a quasi-randomized controlled trial. 2016.
- Kubota, A.; Sakuraba, K.; Sawaki, K.; Sumide, T.; Tamura, Y. Prevention of disuse muscular weakness by restriction of blood flow. Medicine & Science in Sports & Exercise 2008, 40, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Hughes, L.; Paton, B.; Rosenblatt, B.; Gissane, C.; Patterson, S.D. Blood flow restriction training in clinical musculoskeletal rehabilitation: a systematic review and meta-analysis. British journal of sports medicine 2017, 51, 1003–1011. [Google Scholar] [CrossRef]
- Iversen, E.; Røstad, V.; Larmo, A. Intermittent blood flow restriction does not reduce atrophy following anterior cruciate ligament reconstruction. Journal of sport and health science 2016, 5, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Hughes, L.; Rosenblatt, B.; Haddad, F.; Gissane, C.; McCarthy, D.; Clarke, T.; Ferris, G.; Dawes, J.; Paton, B.; Patterson, S.D. Comparing the Effectiveness of Blood Flow Restriction and Traditional Heavy Load Resistance Training in the Post-Surgery Rehabilitation of Anterior Cruciate Ligament Reconstruction Patients: A UK National Health Service Randomised Controlled Trial. Sports Med 2019, 49, 1787–1805. [Google Scholar] [CrossRef]
- Ohta, H.; Kurosawa, H.; Ikeda, H.; Iwase, Y.; Satou, N.; Nakamura, S. Low-load resistance muscular training with moderate restriction of blood flow after anterior cruciate ligament reconstruction. Acta Orthopaedica Scandinavica 2003, 74, 62–68. [Google Scholar] [CrossRef]
- Curran, M.T.; Bedi, A.; Mendias, C.L.; Wojtys, E.M.; Kujawa, M.V.; Palmieri-Smith, R.M. Blood flow restriction training applied with high-intensity exercise does not improve quadriceps muscle function after anterior cruciate ligament reconstruction: a randomized controlled trial. The American Journal of Sports Medicine 2020, 48, 825–837. [Google Scholar] [CrossRef]
- Papaleontiou, A.; Poupard, A.M.; Mahajan, U.D.; Tsantanis, P. Conservative vs Surgical Treatment of Anterior Cruciate Ligament Rupture: A Systematic Review. Cureus 2024, 16, e56532. [Google Scholar] [CrossRef]
- Grevnerts, H.T.; Sonesson, S.; Gauffin, H.; Ardern, C.L.; Stålman, A.; Kvist, J. Decision making for treatment after ACL injury from an orthopaedic surgeon and patient perspective: results from the NACOX study. Orthopaedic Journal of Sports Medicine 2021, 9, 23259671211005090. [Google Scholar] [CrossRef]
- Grevnerts, H.T.; Krevers, B.; Kvist, J. Treatment decision-making process after an anterior cruciate ligament injury: patients’, orthopaedic surgeons’ and physiotherapists’ perspectives. BMC musculoskeletal disorders 2022, 23, 782. [Google Scholar] [CrossRef]
- Webster, K.E.; Feller, J.A. Who Passes Return-to-Sport Tests, and Which Tests Are Most Strongly Associated With Return to Play After Anterior Cruciate Ligament Reconstruction? Orthop J Sports Med 2020, 8, 2325967120969425. [Google Scholar] [CrossRef]
- Kyritsis, P.; Bahr, R.; Landreau, P.; Miladi, R.; Witvrouw, E. Likelihood of ACL graft rupture: not meeting six clinical discharge criteria before return to sport is associated with a four times greater risk of rupture. Br J Sports Med 2016, 50, 946–951. [Google Scholar] [CrossRef]
- Capin, J.J.; Snyder-Mackler, L.; Risberg, M.A.; Grindem, H. Keep calm and carry on testing: a substantive reanalysis and critique of ’what is the evidence for and validity of return-to-sport testing after anterior cruciate ligament reconstruction surgery? A systematic review and meta-analysis’. Br J Sports Med 2019, 53, 1444–1446. [Google Scholar] [CrossRef]
- Ardern, C.L.; Glasgow, P.; Schneiders, A.; Witvrouw, E.; Clarsen, B.; Cools, A.; Gojanovic, B.; Griffin, S.; Khan, K.M.; Moksnes, H.; et al. 2016 Consensus statement on return to sport from the First World Congress in Sports Physical Therapy, Bern. Br J Sports Med 2016, 50, 853–864. [Google Scholar] [CrossRef]
- Doege, J.; Ayres, J.M.; Mackay, M.J.; Tarakemeh, A.; Brown, S.M.; Vopat, B.G.; Mulcahey, M.K. Defining Return to Sport: A Systematic Review. Orthop J Sports Med 2021, 9, 23259671211009589. [Google Scholar] [CrossRef]
- Buckthorpe, M. Optimising the Late-Stage Rehabilitation and Return-to-Sport Training and Testing Process After ACL Reconstruction. Sports Med 2019, 49, 1043–1058. [Google Scholar] [CrossRef]
- Buckthorpe, M.; Della Villa, F. Optimising the ’Mid-Stage’ Training and Testing Process After ACL Reconstruction. Sports Med 2020, 50, 657–678. [Google Scholar] [CrossRef] [PubMed]
- Buckthorpe, M.; Gokeler, A.; Herrington, L.; Hughes, M.; Grassi, A.; Wadey, R.; Patterson, S.; Compagnin, A.; La Rosa, G.; Della Villa, F. Optimising the Early-Stage Rehabilitation Process Post-ACL Reconstruction. Sports Med 2024, 54, 49–72. [Google Scholar] [CrossRef] [PubMed]
- Adams, D.; Logerstedt, D.; Hunter-Giordano, A.; Axe, M.J.; Snyder-Mackler, L. Current concepts for anterior cruciate ligament reconstruction: a criterion-based rehabilitation progression. journal of orthopaedic & sports physical therapy 2012, 42, 601–614. [Google Scholar]
- Davies, G.J.; McCarty, E.; Provencher, M.; Manske, R.C. ACL Return to Sport Guidelines and Criteria. Curr Rev Musculoskelet Med 2017, 10, 307–314. [Google Scholar] [CrossRef]
- Davies, W.T.; Myer, G.D.; Read, P.J. Is It Time We Better Understood the Tests We are Using for Return to Sport Decision Making Following ACL Reconstruction? A Critical Review of the Hop Tests. Sports Med 2020, 50, 485–495. [Google Scholar] [CrossRef]
- Dingenen, B.; Gokeler, A. Optimization of the Return-to-Sport Paradigm After Anterior Cruciate Ligament Reconstruction: A Critical Step Back to Move Forward. Sports Med 2017, 47, 1487–1500. [Google Scholar] [CrossRef]
- Gokeler, A.; Dingenen, B.; Hewett, T.E. Rehabilitation and Return to Sport Testing After Anterior Cruciate Ligament Reconstruction: Where Are We in 2022? Arthrosc Sports Med Rehabil 2022, 4, e77–e82. [Google Scholar] [CrossRef] [PubMed]
- Rambaud, A.J.M.; Ardern, C.L.; Thoreux, P.; Regnaux, J.P.; Edouard, P. Criteria for return to running after anterior cruciate ligament reconstruction: a scoping review. Br J Sports Med 2018, 52, 1437–1444. [Google Scholar] [CrossRef] [PubMed]
- Paterno, M.V. Incidence and Predictors of Second Anterior Cruciate Ligament Injury After Primary Reconstruction and Return to Sport. J Athl Train 2015, 50, 1097–1099. [Google Scholar] [CrossRef]
- McBurnie, A.J.; Dos’ Santos, T. Multidirectional speed in youth soccer players: theoretical underpinnings. Strength & Conditioning Journal 2022, 44, 15–33. [Google Scholar]
- Wright, R.W.; Fetzer, G.B. Bracing after ACL reconstruction: a systematic review. Clin Orthop Relat Res 2007, 455, 162–168. [Google Scholar] [CrossRef]
- Di Miceli, R.; Marambio, C.B.; Zati, A.; Monesi, R.; Benedetti, M.G. Do Knee Bracing and Delayed Weight Bearing Affect Mid-Term Functional Outcome after Anterior Cruciate Ligament Reconstruction? Joints 2017, 5, 202–206. [Google Scholar] [CrossRef]
- Lowe, W.R.; Warth, R.J.; Davis, E.P.; Bailey, L. Functional Bracing After Anterior Cruciate Ligament Reconstruction: A Systematic Review. J Am Acad Orthop Surg 2017, 25, 239–249. [Google Scholar] [CrossRef]
- Moller, E.; Forssblad, M.; Hansson, L.; Wange, P.; Weidenhielm, L. Bracing versus nonbracing in rehabilitation after anterior cruciate ligament reconstruction: a randomized prospective study with 2-year follow-up. Knee Surg Sports Traumatol Arthrosc 2001, 9, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Grant, J.A. Updating recommendations for rehabilitation after ACL reconstruction: a review. Clinical Journal of Sport Medicine 2013, 23, 501–502. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Merchán, E.C. Knee bracing after anterior cruciate ligament reconstruction. Orthopedics 2016, 39, e602–e609. [Google Scholar] [CrossRef]
- Schoepp, C.; Ohmann, T.; Martin, W.; Praetorius, A.; Seelmann, C.; Dudda, M.; Stengel, D.; Hax, J. Brace-free rehabilitation after isolated anterior cruciate ligament reconstruction with hamstring tendon autograft is not inferior to brace-based rehabilitation—A randomised controlled trial. Journal of Clinical Medicine 2023, 12, 2074. [Google Scholar] [CrossRef] [PubMed]
- Prill, R.; Janosky, J.; Bode, L.; van Melick, N.; Della Villa, F.; Becker, R.; Karlsson, J.; Gudas, R.; Gokeler, A.; Jones, H. Prevention of ACL injury is better than repair or reconstruction-Implementing the ESSKA-ESMA’Prevention for All’ACL programme. Knee Surgery and Arthroscopy 2025. [Google Scholar] [CrossRef]
- Webster, K.E.; Hewett, T.E. Meta-analysis of meta-analyses of anterior cruciate ligament injury reduction training programs. Journal of Orthopaedic Research® 2018, 36, 2696–2708. [Google Scholar] [CrossRef]
- Bizzini, M.; Dvorak, J. FIFA 11+: an effective programme to prevent football injuries in various player groups worldwide—a narrative review. British journal of sports medicine 2015, 49, 577–579. [Google Scholar] [CrossRef]
- Jones, H.; Patt, T.; Thoureux, P.; Della Villa, F. ACL Prevention for All. The ESSKA-ESMA prevention programme in children and adolescents.
- Wang, K.C.; Keeley, T.; Lansdown, D.A. Anterior Cruciate Ligament Reconstruction: Common Intraoperative Mistakes and Techniques for Error Recovery. Curr Rev Musculoskelet Med 2025. [Google Scholar] [CrossRef]
- Rizvanovic, D.; Waldén, M.; Forssblad, M.; Stålman, A. Influence of Surgeon Experience and Clinic Volume on Subjective Knee Function and Revision Rates in Primary ACL Reconstruction: A Study from the Swedish National Knee Ligament Registry. Orthop J Sports Med 2024, 12, 23259671241233695. [Google Scholar] [CrossRef]
- Bitschi, D.; Fürmetz, J.; Gilbert, F.; Jörgens, M.; Watrinet, J.; Pätzold, R.; Lang, C.; Neidlein, C.; Böcker, W.; Bormann, M. Preoperative Mixed-Reality Visualization of Complex Tibial Plateau Fractures and Its Benefit Compared to CT and 3D Printing. J Clin Med 2023, 12. [Google Scholar] [CrossRef]
- Figueroa, F.; Figueroa, D.; Guiloff, R.; Putnis, S.; Fritsch, B.; Itriago, M. Navigation in anterior cruciate ligament reconstruction: State of the art. J isakos 2023, 8, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Rilk, S.; Goodhart, G.C.; van der List, J.P.; Von Rehlingen-Prinz, F.; Vermeijden, H.D.; O’Brien, R.; DiFelice, G.S. Anterior cruciate ligament primary repair revision rates are increased in skeletally mature patients under the age of 21 compared to reconstruction, while adults (>21 years) show no significant difference: A systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc 2025, 33, 29–58. [Google Scholar] [CrossRef] [PubMed]
- Vermeijden, H.D.; van der List, J.P.; O’Brien, R.J.; DiFelice, G.S. Primary Repair of Anterior Cruciate Ligament Injuries: Current Level of Evidence of Available Techniques. JBJS Rev 2021, 9. [Google Scholar] [CrossRef]
- Amini, M.; Venkatesan, J.K.; Liu, W.; Leroux, A.; Nguyen, T.N.; Madry, H.; Migonney, V.; Cucchiarini, M. Advanced Gene Therapy Strategies for the Repair of ACL Injuries. Int J Mol Sci 2022, 23. [Google Scholar] [CrossRef]
- Gögele, C.; Hahn, J.; Schulze-Tanzil, G. Anatomical Tissue Engineering of the Anterior Cruciate Ligament Entheses. Int J Mol Sci 2023, 24. [Google Scholar] [CrossRef]
- Wade, L.; Needham, L.; McGuigan, P.; Bilzon, J. Applications and limitations of current markerless motion capture methods for clinical gait biomechanics. PeerJ 2022, 10, e12995. [Google Scholar] [CrossRef]
- Ito, N.; Sigurðsson, H.B.; Seymore, K.D.; Arhos, E.K.; Buchanan, T.S.; Snyder-Mackler, L.; Silbernagel, K.G. Markerless motion capture: What clinician-scientists need to know right now. JSAMS plus 2022, 1, 100001. [Google Scholar] [CrossRef]
- Schmidt, S.; Krahl, D.; Podszun, J.; Knecht, S.; Zimmerer, A.; Sobau, C.; Ellermann, A.; Ruhl, A. Combining a digital health application with standard care significantly enhances rehabilitation outcomes for ACL surgery patients. Knee Surg Sports Traumatol Arthrosc 2025, 33, 1241–1251. [Google Scholar] [CrossRef]
- Dunphy, E.; Hamilton, F.L.; Spasic, I.; Button, K. Acceptability of a digital health intervention alongside physiotherapy to support patients following anterior cruciate ligament reconstruction. BMC Musculoskelet Disord 2017, 18, 471. [Google Scholar] [CrossRef]
- Verhagen, E.A.; Clarsen, B.; Bahr, R. A peek into the future of sports medicine: the digital revolution has entered our pitch. Br J Sports Med 2014, 48, 739–740. [Google Scholar] [CrossRef] [PubMed]
- Andriollo, L.; Picchi, A.; Sangaletti, R.; Perticarini, L.; Rossi, S.M.P.; Logroscino, G.; Benazzo, F. The Role of Artificial Intelligence in Anterior Cruciate Ligament Injuries: Current Concepts and Future Perspectives. Healthcare (Basel) 2024, 12. [Google Scholar] [CrossRef] [PubMed]
- Corban, J.; Lorange, J.P.; Laverdiere, C.; Khoury, J.; Rachevsky, G.; Burman, M.; Martineau, P.A. Artificial Intelligence in the Management of Anterior Cruciate Ligament Injuries. Orthop J Sports Med 2021, 9, 23259671211014206. [Google Scholar] [CrossRef] [PubMed]
- Tamimi, I.; Ballesteros, J.; Lara, A.P.; Tat, J.; Alaqueel, M.; Schupbach, J.; Marwan, Y.; Urdiales, C.; Gomez-de-Gabriel, J.M.; Burman, M.; et al. A Prediction Model for Primary Anterior Cruciate Ligament Injury Using Artificial Intelligence. Orthop J Sports Med 2021, 9, 23259671211027543. [Google Scholar] [CrossRef]
- Taborri, J.; Molinaro, L.; Santospagnuolo, A.; Vetrano, M.; Vulpiani, M.C.; Rossi, S. A Machine-Learning Approach to Measure the Anterior Cruciate Ligament Injury Risk in Female Basketball Players. Sensors (Basel) 2021, 21. [Google Scholar] [CrossRef]
- Johnson, W.R.; Mian, A.; Lloyd, D.G.; Alderson, J.A. On-field player workload exposure and knee injury risk monitoring via deep learning. J Biomech 2019, 93, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Richter, C.; King, E.; Strike, S.; Franklyn-Miller, A. Objective classification and scoring of movement deficiencies in patients with anterior cruciate ligament reconstruction. PLoS One 2019, 14, e0206024. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.K.; Ley, C.; Pareek, A.; Groll, A.; Tischer, T.; Seil, R. Artificial intelligence and machine learning: an introduction for orthopaedic surgeons. Knee Surg Sports Traumatol Arthrosc 2022, 30, 361–364. [Google Scholar] [CrossRef]
- Kakavas, G.; Malliaropoulos, N.; Pruna, R.; Traster, D.; Bikos, G.; Maffulli, N. Neuroplasticity and Anterior Cruciate Ligament Injury. Indian J Orthop 2020, 54, 275–280. [Google Scholar] [CrossRef]
- Kakavas, G.; Malliaropoulos, N.; Bikos, G.; Pruna, R.; Valle, X.; Tsaklis, P.; Maffulli, N. Periodization in Anterior Cruciate Ligament Rehabilitation: A Novel Framework. Med Princ Pract 2021, 30, 101–108. [Google Scholar] [CrossRef]
- Anderson, A.B.; Grazal, C.F.; Balazs, G.C.; Potter, B.K.; Dickens, J.F.; Forsberg, J.A. Can Predictive Modeling Tools Identify Patients at High Risk of Prolonged Opioid Use After ACL Reconstruction? Clin Orthop Relat Res 2020, 478, 0–1618. [Google Scholar] [CrossRef]
- Tighe, P.; Laduzenski, S.; Edwards, D.; Ellis, N.; Boezaart, A.P.; Aygtug, H. Use of machine learning theory to predict the need for femoral nerve block following ACL repair. Pain Med 2011, 12, 1566–1575. [Google Scholar] [CrossRef]
- Chen, J.H.; Asch, S.M. Machine Learning and Prediction in Medicine - Beyond the Peak of Inflated Expectations. N Engl J Med 2017, 376, 2507–2509. [Google Scholar] [CrossRef] [PubMed]
- Bien, N.; Rajpurkar, P.; Ball, R.L.; Irvin, J.; Park, A.; Jones, E.; Bereket, M.; Patel, B.N.; Yeom, K.W.; Shpanskaya, K.; et al. Deep-learning-assisted diagnosis for knee magnetic resonance imaging: Development and retrospective validation of MRNet. PLoS Med 2018, 15, e1002699. [Google Scholar] [CrossRef]
- Štajduhar, I.; Mamula, M.; Miletić, D.; Ünal, G. Semi-automated detection of anterior cruciate ligament injury from MRI. Comput Methods Programs Biomed 2017, 140, 151–164. [Google Scholar] [CrossRef]
- Zhang, L.; Li, M.; Zhou, Y.; Lu, G.; Zhou, Q. Deep Learning Approach for Anterior Cruciate Ligament Lesion Detection: Evaluation of Diagnostic Performance Using Arthroscopy as the Reference Standard. J Magn Reson Imaging 2020, 52, 1745–1752. [Google Scholar] [CrossRef]
- Swain, M.S.; Henschke, N.; Kamper, S.J.; Downie, A.S.; Koes, B.W.; Maher, C.G. Accuracy of clinical tests in the diagnosis of anterior cruciate ligament injury: a systematic review. Chiropr Man Therap 2014, 22, 25. [Google Scholar] [CrossRef]
- Luites, J.W.; Wymenga, A.B.; Blankevoort, L.; Eygendaal, D.; Verdonschot, N. Accuracy of a computer-assisted planning and placement system for anatomical femoral tunnel positioning in anterior cruciate ligament reconstruction. Int J Med Robot 2014, 10, 438–446. [Google Scholar] [CrossRef]
- Shafizadeh, S.; Balke, M.; Wegener, S.; Tjardes, T.; Bouillon, B.; Hoeher, J.; Baethis, H. Precision of tunnel positioning in navigated anterior cruciate ligament reconstruction. Arthroscopy 2011, 27, 1268–1274. [Google Scholar] [CrossRef]
- Sopilidis, A.; Stamatopoulos, V.; Giannatos, V.; Taraviras, G.; Panagopoulos, A.; Taraviras, S. Integrating Modern Technologies into Traditional Anterior Cruciate Ligament Tissue Engineering. Bioengineering (Basel) 2025, 12. [Google Scholar] [CrossRef] [PubMed]
- Dye, S.F. The future of anterior cruciate ligament restoration. Clin Orthop Relat Res 1996, 130–139. [Google Scholar] [CrossRef] [PubMed]
- Gokeler, A.; Grassi, A.; Hoogeslag, R.; van Houten, A.; Bolling, C.; Buckthorpe, M.; Norte, G.; Benjaminse, A.; Heuvelmans, P.; Di Paolo, S.; et al. Return to sports after ACL injury 5 years from now: 10 things we must do. J Exp Orthop 2022, 9, 73. [Google Scholar] [CrossRef]
- Sarlis, V.; Papageorgiou, G.; Tjortjis, C. Injury patterns and impact on performance in the NBA League Using Sports Analytics. Computation 2024, 12, 36. [Google Scholar] [CrossRef]
- Daggett, M.C.; Witte, K.A.; Cabarkapa, D.; Cabarkapa, D.V.; Fry, A.C. Evidence-Based Data Models for Return-to-Play Criteria after Anterior Cruciate Ligament Reconstruction. Healthcare (Basel) 2022, 10. [Google Scholar] [CrossRef]
- Patel, H.H.; Berlinberg, E.J.; Nwachukwu, B.; Williams, R.J., 3rd; Mandelbaum, B.; Sonkin, K.; Forsythe, B. Quadriceps Weakness is Associated with Neuroplastic Changes Within Specific Corticospinal Pathways and Brain Areas After Anterior Cruciate Ligament Reconstruction: Theoretical Utility of Motor Imagery-Based Brain-Computer Interface Technology for Rehabilitation. Arthrosc Sports Med Rehabil 2023, 5, e207–e216. [Google Scholar] [CrossRef] [PubMed]
- Pataky, T.C. One-dimensional statistical parametric mapping in Python. Computer methods in biomechanics and biomedical engineering 2012, 15, 295–301. [Google Scholar] [CrossRef]
- McDevitt, E.R.; Taylor, D.C.; Miller, M.D.; Gerber, J.P.; Ziemke, G.; Hinkin, D.; Uhorchak, J.M.; Arciero, R.A.; Pierre, P.S. Functional bracing after anterior cruciate ligament reconstruction: a prospective, randomized, multicenter study. Am J Sports Med 2004, 32, 1887–1892. [Google Scholar] [CrossRef] [PubMed]
- Harilainen, A.; Sandelin, J. Post-operative use of knee brace in bone-tendon-bone patellar tendon anterior cruciate ligament reconstruction: 5-year follow-up results of a randomized prospective study. Scand J Med Sci Sports 2006, 16, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Harilainen, A.; Sandelin, J.; Vanhanen, I.; Kivinen, A. Knee brace after bone-tendon-bone anterior cruciate ligament reconstruction. Randomized, prospective study with 2-year follow-up. Knee Surg Sports Traumatol Arthrosc 1997, 5, 10–13. [Google Scholar] [CrossRef]
- Muellner, T.; Alacamlioglu, Y.; Nikolic, A.; Schabus, R. No benefit of bracing on the early outcome after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 1998, 6, 88–92. [Google Scholar] [CrossRef]
- Ito, Y.; Deie, M.; Adachi, N.; Kobayashi, K.; Kanaya, A.; Miyamoto, A.; Nakasa, T.; Ochi, M. A prospective study of 3-day versus 2-week immobilization period after anterior cruciate ligament reconstruction. Knee 2007, 14, 34–38. [Google Scholar] [CrossRef]
- Birmingham, T.B.; Bryant, D.M.; Giffin, J.R.; Litchfield, R.B.; Kramer, J.F.; Donner, A.; Fowler, P.J. A randomized controlled trial comparing the effectiveness of functional knee brace and neoprene sleeve use after anterior cruciate ligament reconstruction. Am J Sports Med 2008, 36, 648–655. [Google Scholar] [CrossRef]
- Birmingham, T.B.; Kramer, J.F.; Kirkley, A. Effect of a functional knee brace on knee flexion and extension strength after anterior cruciate ligament reconstruction. Arch Phys Med Rehabil 2002, 83, 1472–1475. [Google Scholar] [CrossRef] [PubMed]
- Birmingham, T.B.; Kramer, J.F.; Kirkley, A.; Inglis, J.T.; Spaulding, S.J.; Vandervoort, A.A. Knee bracing after ACL reconstruction: effects on postural control and proprioception. Med Sci Sports Exerc 2001, 33, 1253–1258. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Knee valgus moment during a planned 90° change of direction task in a professional soccer player, 9 months after ACL-R using 3D marker-based motion analysis.
Figure 1.
Knee valgus moment during a planned 90° change of direction task in a professional soccer player, 9 months after ACL-R using 3D marker-based motion analysis.
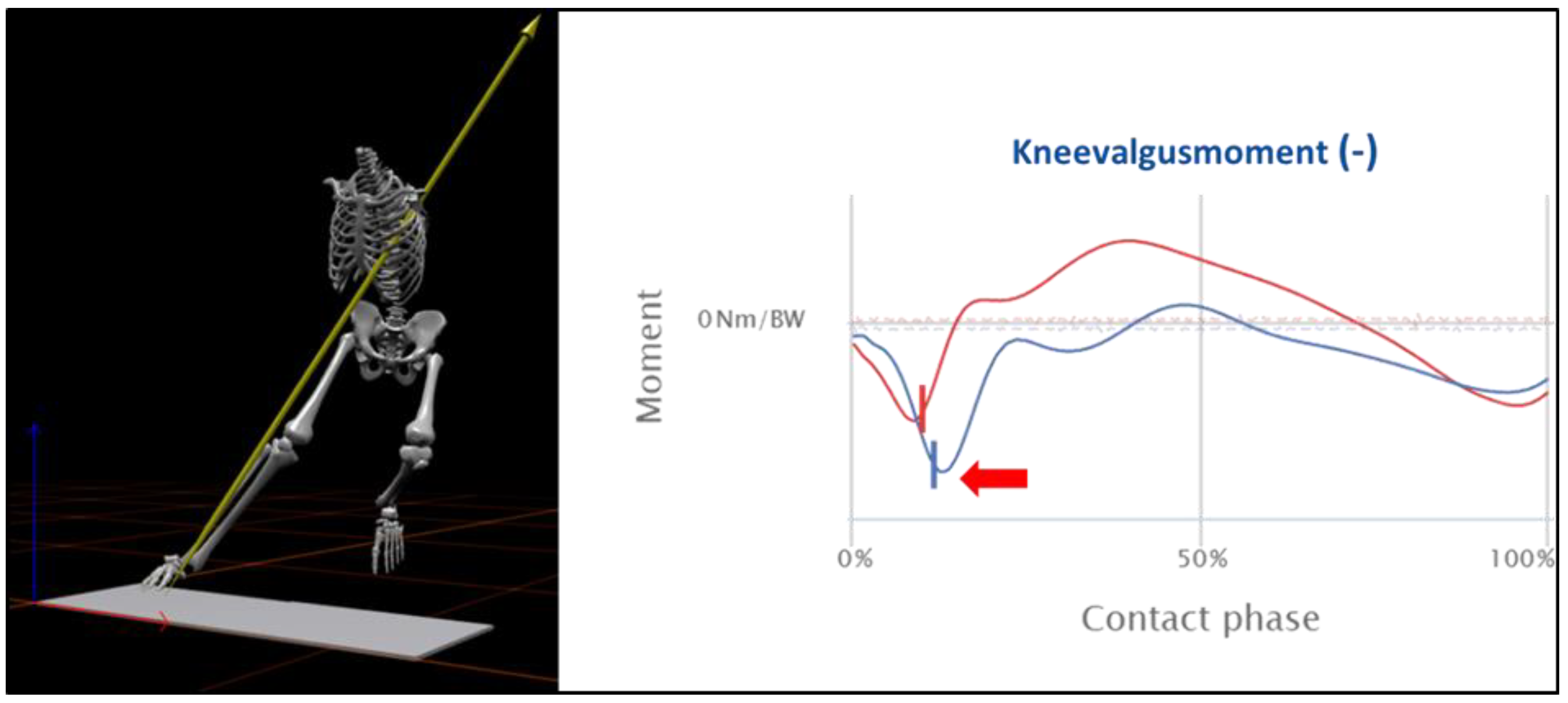

Table 1.
The RTP continuum encompasses various phases of rehabilitation.
| Phase | Training Goals |
| Prehabilitation: | “Quiet Knee”, Development of Muscle Strength |
| Recovery from Surgery (RFS) | Clinical Care and Inflammatory Management |
| Return-to-Activity (RTA): | Neuromuscular Control and Resistance Training |
| Return-to-Running (RTR): | Strength, Power, and Energy Systems Training |
| Return-to-Sports (RTS): | Speed, Agility, and High-Intensity Interval Training (On-Field and Restricted Team Training) |
| Return-to-Play (RTP): | Readiness to Play and Compete (Full Team Training) |
| Return-to-Competition (RTC) | Competitive Performance & Injury Prevention |
Table 2.
Time- and criteria-based rehabilitation algorithm following ACL-R.
| Phase | Goals | Intervention | Progression Criteria |
|---|---|---|---|
|
RFS – Recovery of Surgery Week 1 to 2 |
Reduction of pain and swelling Optimization of knee mobility and activation Pain-adapted increase of daily activities |
Passive & active knee mobilization, patella mobilization Gait training (initially partial weight-bearing if necessary) Decongestive exercises, electrical stimulation and quadriceps isometrics, mobilization of adjacent joints Core and hip stabilizer training Balance & perturbation training, 30° mini squats Strength training of the contralateral limb and upper extremity |
Passive ROM (P-ROM): 0-0–90° Modified stroke effusion test: moderate 1+ Quadriceps activation with proximal patella glide (visibly observable) Straight leg raise test without extension lag Active knee extension during walking possible KOS-ADL ≥ 85% |
|
RTA – Return-to-Activity Week 3 to 12 |
Normalization of knee mobility Optimization of strength and movement coordination Normalization of gait pattern, stair climbing, cycling |
Passive & active knee mobilization, scar mobilization Intensive gait training BFR-Training, NMES, intensified perturbation training Closed-kinetic chain resistance training: Week 5: 0–60° ROM, Week 7: 0–90° ROM, Week 9: full ROM (focus on fundamental movement patterns) Open kinetic chain resistance training = from week 9: 90–40° ROM (10° weekly increase; no restrictions from week 13) Week 11: running drills, bi- and unilateral jumps (landing) Gait-running progression, upper extremity strength training |
P-ROM: 0-0-120° (6 weeks), 0-0-LSI [°] ≤ 10 (12 weeks) Modified stroke effusion test: none to minimal Y-Balance LSI [cm] ≥ 95%, Composite Score > 94% Knee extension/flexion strength LSI [Nm] ≥ 70% 10-minute jog at 10–12 km/h possible Jump and hop tests LSI [N, cm] ≥ 70% Single-leg 60° squat and jump-landing pattern with stable trunk-pelvis-leg axis |
|
RTR – Return-to-Running Week 14 to 24 |
Performance optimization in short and long SSC (stretch-shortening cycle) Development of running resilience and performance | Intensified running drills, bi- and unilateral plyometric & jump training Technique training for lateral & multidirectional locomotion Machine-based strength training in open & closed kinetic chain (15–8 RM) Strength training with free weights (12–6 RM; focus on fundamental patterns), eccentric strength training Core strength training (focus on force transfer, e.g., medicine ball throws) Linear running progression, HIIT sequences, on-field technique sessions |
Knee extension/flexion strength LSI [Nm] ≥ 80% Flexion-extension ratio ≥ 60% Jump and hop tests LSI [N, cm] ≥ 80% Stable trunk-pelvis-leg axis in planned jumping and cutting maneuvers |
|
RTS – Return-to-Sports Week 25 to 34 |
Performance optimization of speed actions Sport-specific movement patterns Restricted team training |
Progressive sprint development, short intense HIIT sessions (45–15 sec) Intensification of multidirectional locomotion (to fatigue) Development of technical-tactical performance prerequisites Technique stabilization in bi- and unilateral plyometrics (to fatigue) Technique stabilization of intense COD actions (to fatigue) Optimization of maximal and explosive strength (6–4 RM) Eccentric strength training (in end-range joint positions) |
Knee extension/flexion strength LSI [Nm] ≥ 90% Knee extension > 2.5 Nm/kg body weight Jump and hop tests LSI [N, cm] ≥ 90–95% Stable trunk-pelvis-leg axis in unplanned jumping and cutting actions ♂: VIFT ≥ 20 km/h, ♀: VIFT ≥ 18 km/h ACL-RSI Score > 65% |
|
RTP – Return-to-Play From week 35 |
Sport-specific training and competitive exposure (full team training) | Pressing & tackling, gradual increase of competitive match minutes Development of individual prevention routines, e.g., FIFA 11+, PEP, KIPP Maintenance of maximal & explosive strength, endurance performance |
|
| ROM = Range of Motion, KOS-ADL = Knee Outcome Survey – Activities of Daily Living, LSI = Limb Symmetry Index, Nm = Newton meter, Comp. Score = Composite Score, SAS = Sports Activity Scale, COD = change of direction, VIFT = Final velocity in the 30-15 Intermittent Fitness Test (IFT), ACL-RSI = ACL – Return to sport after injury scale. | |||
Table 3.
Isokinetic torque 60/s and 240°/s for knee extension/flexion ([Nm/kg] mean ±SD), 16-, 26- and 52-weeks post ACL-R, brace-free and brace-based.
Table 3.
Isokinetic torque 60/s and 240°/s for knee extension/flexion ([Nm/kg] mean ±SD), 16-, 26- and 52-weeks post ACL-R, brace-free and brace-based.
| Extension | Flexion | ||||
|---|---|---|---|---|---|
| Brace-free | braced | Brace-free | Braced | ||
| 16 weeks | 240°/sec | 0.89±0.38 | 0.89±0.35 | 0.87±0.22 | 0.86±0.17 |
| 60°/sec | 1.55±0.59 | 1.50±0.50 | 1.14±0.29 | 1.14±0.25 | |
| 26 weeks | 240°/sec | 1.10±0.37 | 1.05±0.29 | 0.99±0.22 | 0.96±0.18 |
| 60°/sec | 1.74±0.65 | 1.75±0.51 | 1.27±0.33 | 1.28±0.26 | |
| 52 weeks | 240°/sec | 1.27±0.44 | 1.20±0.33 | 1.03±0.29 | 0.98±0.25 |
| 60°/sec | 2.09±0.74 | 2.05±0.59 | 1.38±0.36 | 1.37±0.34 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



