Submitted:
22 February 2026
Posted:
23 February 2026
You are already at the latest version
Abstract
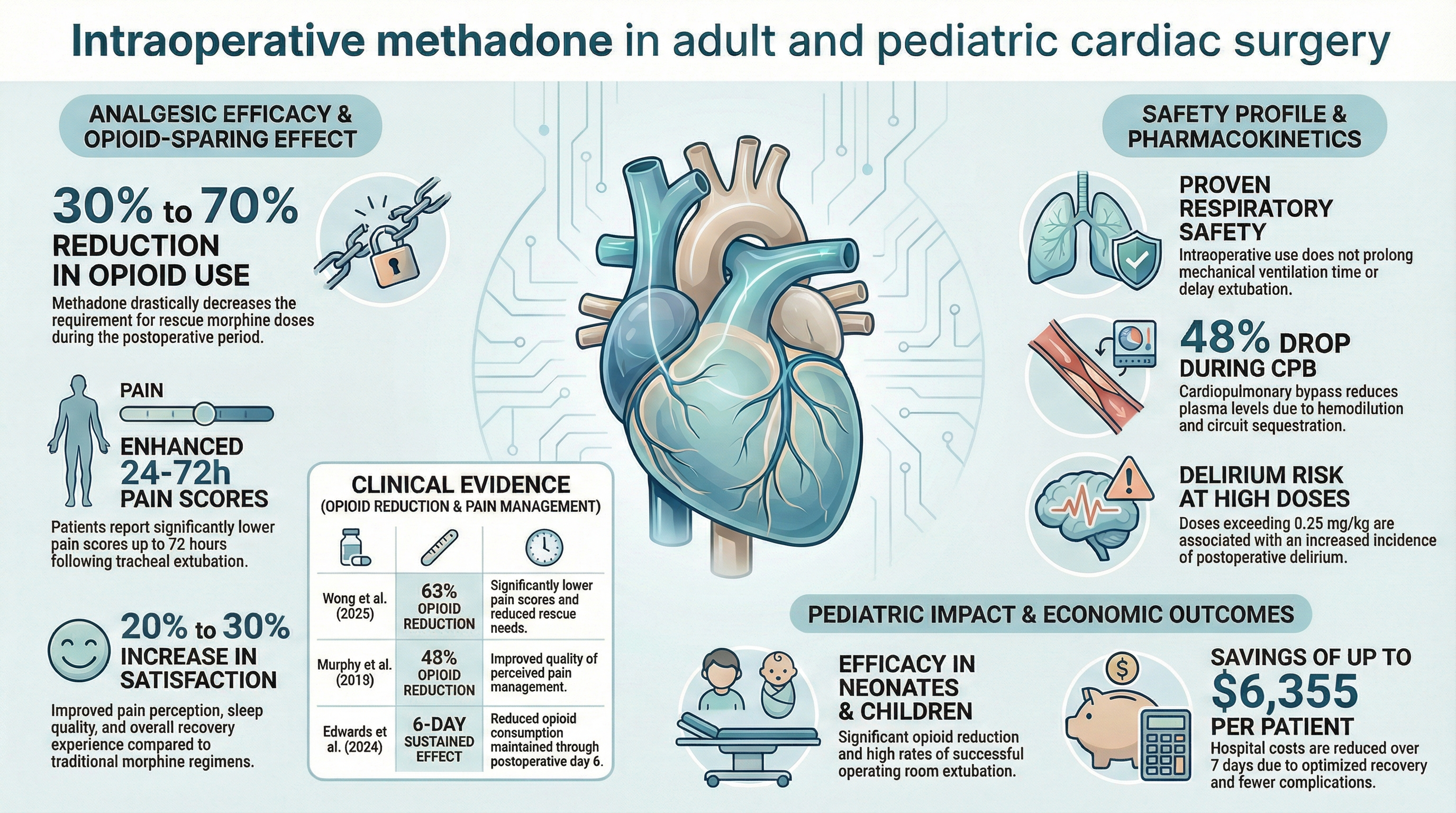
Background/Objectives: Intraoperative methadone has emerged as a significant pharmacological strategy in cardiac surgery to improve postoperative analgesic outcomes and reduce the reliance on rescue short action opioids. This review aims to synthesize evidence regarding the safety and efficacy of intravenous methadone compared to other strategies for postoperative pain control in adult and pediatric cardiac surgeries. Methods: This scoping review relied on electronic searches in PubMed, Web of Science, Cochrane Library, and EMBASE up to January 2026. From 199 articles retrieved, 41 were included, focusing on analgesic efficacy, safety, pharmacokinetic variations during cardiopulmonary bypass (CPB), and cost-effectiveness. Results: The implementation of methadone results in a 30% to 70% reduction in postoperative opioid requirements. Patients experience significantly lower pain scores from 24 to 72 hours and a 20% to 30% improvement in satisfaction regarding their recovery. In pediatric populations (neonates and children), the use of methadone leads to a significant reduction in opioid needs and a high rate of extubation in the operating room. Pharmacokinetically, a 48% drop in methadone concentration occurs during CPB due to hemodilution and sequestration. Safety data confirms that intraoperative use does not prolong mechanical ventilation; however, doses exceeding 0.25 mg/kg are linked to an increased incidence of delirium. Economically, optimized recovery generates savings of up to $6,355 per patient within seven days. Conclusions: Intraoperative methadone is a robust and safe analgesic option for cardiac surgery, including pediatric cases. It offers profound opioid-sparing effects and significant cost reductions, if dosages are carefully managed to minimize delirium risks.
Keywords:
methadone
; cardiac surgical procedures
; postoperative pain
; pharmacokinetics
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



