
Submitted:
25 June 2025
Posted:
26 June 2025
You are already at the latest version
Abstract
Background: Regional anaesthesia techniques allow postoperative pain control while reducing opioid con-sumption. Ketamine is another viable option for minimising perioperative opioid use. We evaluated the ef-ficacy of a perioperative multimodal analgesia protocol incorporating paravertebral block (PVB) and keta-mine infusion in patients undergoing video-assisted thoracic surgery (VATS).
Methods: This retrospective single-centre study divided patients into two groups: the opioid-sparing (OS) group receiving PVB and ketamine (n = 41), and the control group (n = 21) treated with postoperative morphine infusion. The primary outcome was the need for rescue opioid therapy; secondary outcomes in-cluded postoperative pain scores assessed at multiple time points over 48 hours using the Numeric Rating Scale (NRS), prevalence of chronic postoperative pain at three months, perioperative haemodynamics, and hospital length of stay.
Results: Rescue opioid administration was significantly lower in the OS group (19.5% vs. 47.6%, p = 0.021). Upon awakening, pain control was lower in the OS group (1 [1–2] vs 4 [3–4], p < 0.001); however, pain scores did not differ afterwards. Chronic postoperative pain was less common in the OS group (n = 10/41; 23.8% vs n = 11/21, 52.4%; p = 0.028). No differences in haemodynamics were reported, nor were there any ketamine/PVB-related complications. No difference in length of hospital stay was observed between the groups. Ketamine starting dose and postoperative morphine requirements were inversely correlated (rho = -0.380; p = 0.002).
Conclusion: A multimodal analgesia protocol integrating PVB and ketamine infusion in patients undergoing VATS may effectively reduce postoperative opioid consumption, improving analgesia in the initial postop-erative period.
Keywords:
Chronic Pain
; Morphine consumption
; Locoregional Anesthesia
; Video Assisted Thoracoscopy
Introduction
Patients undergoing thoracic surgery frequently experience severe acute postoperative pain (APOP), even after minimally invasive surgical approaches such as video-assisted thoracic surgery (VATS) [1]. Inadequate pain control may lead to delayed recovery, impaired respiratory function, and a higher incidence of postoperative complications including infections, and prolonged hospital stays with increased costs [2,3,4]. Opioids have been a mainstay of APOP management after major surgery, with administration ranging from intravenous to transdermal [5]. However, their use can be associated with adverse effects such as nausea, vomiting, constipation, sedation, delayed mobilisation, and respiratory depression [5,6]; hence, there is a constant search for alternatives in the management of APOP, aimed at enhancing recovery and minimising side effects. In this context, APOP can be effectively controlled by multimodal analgesia approaches[3,4,5]. Multimodal analgesia refers to a variety of strategies aimed at optimising analgesia through the combination of different pharmacological and regional techniques. Such combinations aspire to achieve synergistic effects while minimising systemic opioid consumption and its inevitable side effects [3,4,5,6].
Regional anaesthesia techniques include thoracic epidural anaesthesia (TEA), which has historically been the gold standard for reducing opioid consumption in the management of APOP in thoracic surgery. However, TEA is now less frequently used due to the development of ultrasound-guided thoracic wall blocks, which provide similar outcomes with the advantage of being less invasive. The development of ultrasound-guided thoracic wall blocks has gained interest and wide clinical application[7,8], even in the setting of cardiac surgery [9]. Among the thoracic wall blocks, the paravertebral block (PVB) may offer advantages over other regional anaesthesia techniques. Indeed, compared to the erector spine or serratus anterior plane blocks, PVB targets the origin of the intercostal nerves and provides unilateral analgesia by blocking somatic and sympathetic nerves already in the paravertebral space, making it particularly effective for unilateral thoracic procedures [10,11,12,13]. As part of enhanced recovery after surgery (ERAS) protocols for thoracic procedures, PVB seems to offer comparable analgesia to TEA while reducing the risk of opioid-related respiratory complications [14], contributing to a smoother recovery process[15,16,17]. Recent ERAS guidelines encourage the use of regional anaesthesia techniques to improve postoperative outcomes and reduce opioid consumption [14,16,17]. Conversely, an aspect that requires further research is the implementation of opioid-sparing (OS) multimodal analgesia protocols in which regional anaesthesia is combined with adjuvant drugs such as ketamine[17,18,19,20].
In this retrospective study, we aimed to assess the efficacy of a multimodal analgesia protocol combining ultrasound-guided thoracic PVB and perioperative intravenous ketamine infusion in reducing postoperative opioid consumption and improving pain control in patients undergoing thoracic surgery.
2. Materials and Methods
2.1. Study Population
This retrospective study utilised prospectively collected data as part of an internal audit on the management of APOP in patients undergoing VATS between March and October 2020 at the Thoracic Surgery Unit of the University Hospital of Siena. Ethical approval for using these data was obtained from the local ethical committee (Comitato Etico Regionale per la Sperimentazione Clinica della Regione Toscana; Protocol 18862).
Our audit included all adult patients undergoing VATS lung resection. We excluded patients younger than 18 years, pregnant individuals, those requiring postoperative intensive care unit monitoring, re-do surgeries or emergency procedures, those with known allergies to local anaesthetics, and individuals with a history of neuro-psychiatric conditions that could preclude accurate pain assessment. Patients receiving chronic opioid therapy or regular non-steroidal anti-inflammatory drugs before surgery were also excluded to avoid confounding effects on postoperative analgesia.
Patients were grouped according to their usage of OS, in particular, in intraoperative PVB and ketamine infusion (case group), or the intra- and postoperative use of opioids (control group). General anaesthesia induction was identical in both groups and was performed in all patients with propofol (1–3 mg/kg), fentanyl (1–2 mcg/kg), and rocuronium (0.5 mg/kg) boluses. Endotracheal intubation was achieved with a double-lumen tube (Robertshaw type), and intraoperatively, general anaesthesia was maintained in all patients with sevoflurane (1.0–1.5 minimum alveolar concentration). The control group received intraoperative fentanyl boluses (0.1–0.3mcg/kg every 30 to 45 minutes). Conversely, the OS group did not receive intraoperative opioids (apart from the induction of anaesthesia) and was managed with PVB and ketamine. Specifically, the thoracic PVB was performed before inducing general anaesthesia with the patient in the lateral decubitus position [21]. The T4 paravertebral space was identified using a high-frequency (6–18 MHz) linear ultrasound probe (Epiq 5-Philips® Eindhoven, Amsterdam, Netherlands) with an in-plane approach, placing the probe parallel to the vertebral column [22]. The block consisted of a single injection of 0.5% ropivacaine, titrated based on the patient’s ideal body weight (0.1 ml/kg or a maximum of 15 ml total volume), using a 100-mm nerve block needle (Stimuplex A' B. Braun). At the end of surgery, sedation was discontinued, and patients were extubated upon being neurologically appropriate and demonstrating adequate spontaneous ventilation.
2.2. Postoperative Analgesia
At the end of surgery, both groups received intravenous paracetamol (1 gram) and ketorolac (30 mg), which were also administered perioperatively at regular intervals. Specifically, intravenous paracetamol was administered at doses of 1 gram every 8 hours, and ketorolac 30 mg was given every 12 hours, except in cases of contraindications (allergies, chronic kidney disease stage > 2, or a history of gastrointestinal bleeding). Apart from the use of paracetamol and ketorolac (common to both arms), the control group received intravenous morphine (starting dose of 0.1 mg/kg followed by an infusion of 0.2 mg/kg over 24 hours for 30 hours), while the OS group received a starting dose of ketamine (variable dose of 0.20–0.25 mg/kg) just before extubation, followed by continuous infusion at a dose of 20 mcg/kg/h for 30 hours via an elastomeric pump.
Whenever the nurse's assessment of analgesia revealed uncontrolled pain (defined as Numeric Rating Scale (NRS) > 4), a rescue analgesic dose (oral morphine 10 mg) was administered. The ward nurse on duty was unaware of the contents of the elastomeric pump (ketamine or morphine), nor of the execution of PVB. Assignment to one of the two groups was related to the ability or otherwise of the anaesthetist on duty to perform the PVB.
2.3. Data Collection and Analysis
Demographic characteristics, including age, sex, BMI, and ASA classification, were recorded for all patients. Additionally, detailed perioperative data were gathered, encompassing the type and duration of surgery, haemodynamic parameters (systolic, diastolic, and mean blood pressure, SpO2, and heart rate), and the administration of anaesthetic and analgesic drugs. Postoperative pain scores were assessed using the NRS and documented immediately after extubation and subsequently at six other postoperative time points (every 8 hours for 48 hours). The need for rescue opioid therapy (intravenous morphine 0.01 mg/kg) was also recorded, along with any reported complications (such as postoperative nausea and vomiting–PONV, respiratory depression, or itching) and the total length of hospital stay (LOS).
The primary outcome was the incidence of the rescue dose of oral morphine (10 mg), which was administered when the NRS score was above 4. The assessment according to the NRS and the administration of rescue doses were by a nurse blinded to the intraoperative management to ensure an unbiased evaluation. The secondary objectives included 1) postoperative pain intensity (NRS), recorded immediately after surgery and then every 8 hours up to 48 hours; 2) the development of chronic postoperative pain, which was assessed three months later via telephone interview; 3) the differences in oxygen saturation (SpO2) and blood pressure; and 4) the LOS.
2.4. Statistical Analysis
A minimum sample size of 59 patients was estimated considering a Fisher exact test, with the first type error set at 0.05 and a power of 85%, using an estimated relative difference in rescue opioid dose administration between groups of 30% with a between-group ratio of 1:2. This ratio was determined according to the local availability of anaesthesiologists rotating in the thoracic surgery theatre and their ability to provide PVB and willingness to use ketamine infusion in the context of an OS approach. Power analyses were performed using G*Power. Categorical variables were summarised using absolute numbers and percentage frequencies, while quantitative variables were summarised using median and interquartile range as the Kolmogorov-Smirnov test showed that the distribution of data was not normal. Hence, we used the non-parametric Mann-Whitney tests. Differences between categorical variables were tested with Fisher’s exact test. A p-value of < 0.05 was considered statistically significant. Analyses were carried out with R (The R Foundation for Statistical Computing 2023, version 4.3.2).
3. Results
3.1. Sudy Population
A total of 62 consecutive patients were included in the study (Figure 1), 39% of whom were male (n = 24). Patients underwent VATS lung resection, specifically enrolling 55 lobectomies and 7 segmentectomies. Among the enrolled patients, 41 were assigned to the OS group and 21 to the control group. Descriptive preoperative and perioperative characteristics are presented in Table 1. No differences were observed between groups in the intraoperative parameters, and no complications directly attributable to the PVB or the administration of analgesic drugs during the perioperative period were reported.
Outcome
As shown in Table 2, the incidence of rescue oral morphine administration within 48 hours after surgery was significantly lower in the OS group (n = 8/41, 19.5%) compared to the control group (n = 10/21, 47.6%, p = 0.021). Particularly, eight doses were given to eight patients in the OS group (one rescue each), while 22 doses were given to the 10 patients in the control group (eight patients received two doses and two patients received three doses of rescue analgesia; p < 0.001). Considering the overall number of APOP evaluations (seven per patient), the occurrence of rescue dose administrations was significantly lower in the OS group (n = 8/287 vs 22/147, p < 0.0001). A post-hoc exploratory analysis was conducted according to the different starting doses of ketamine and showed a negative correlation between the ketamine starter dose and the need for rescue oral morphine (Spearman’s Rho = -0.380; p = 0.002).
Patients in the OS group reported significantly lower NRS scores upon awakening (Table 2 and Figure 2), but no statistically significant differences in NRS scores were detected at later time points (from the 8th until the 48th postoperative hour) with median values consistently ranging between 1 and 2 points of the NRS (Table 2).
Upon telephone interview three months after surgery, chronic postoperative pain was reported with significantly lower prevalence in the OS group (n = 10/41, 23.8%) compared to the control group (n = 11/21, 53.4%, p = 0.028; Table 2).
We found no differences in haemodynamic values and SpO2, apart from higher SpO2 levels and lower heart rate at awakening in the OS group. Similarly, there was no statistically significant difference in the hospital LOS between the two groups (OS group vs control group 5 [5,6,7,8]vs 6 [5,6,7] days; p = 0.541) (Table 3).
4. Discussion
In this retrospective study, we report data from an internal audit of patients undergoing VATS with the aim of evaluating the potential benefits of an OS approach. We applied a multimodal analgesia protocol that included a thoracic PVB and an OS analgesia regimen with intravenous ketamine supported by paracetamol and ketorolac at the end of the surgical procedure.
Our findings support the hypothesis of clinical benefits from our multimodal intervention with PVB and ketamine. Indeed, this approach significantly reduced the need for postoperative rescue doses (oral morphine); interestingly, we also noted a possible dose-dependent effect of the ketamine starting dose on opioid-sparing, with a greater initial dose correlated to a lower number of rescue doses. The latest ERAS guidelines in the context of lung surgery recommend a standardised multimodal pain management strategy incorporating locoregional anaesthesia to minimise postoperative opioid consumption[16]. Reducing opioid use is crucial due to the well-documented adverse effects including PONV, paralytic ileus, excessive sedation, and prolonged hospital stays [23,24]. Additionally, multimodal analgesia incorporating locoregional techniques shortens the duration of postoperative mechanical ventilation, facilitates early mobilisation and physiotherapy, and reduces the risk of atelectasis and pneumonia [25]. Our results align with the available evidence, adding scientific information on the value of combining a locoregional anaesthesia approach (PVB in our cohort) with ketamine. Our study demonstrates that multimodal analgesia incorporating both PVB and ketamine might be superior to an opioid-based protocol, with improved pain scores on awakening and reduced rescue doses, although the NRS scores between groups were not significantly different at later time points [26]. This finding highlights the potential of enhancing OS strategies not only with the implementation of locoregional anaesthesia but also with the addition of intravenous ketamine to achieve comparable pain relief while mitigating opioid-related side effects.
Ketamine, an N-methyl-D-aspartate (NMDA) receptor antagonist, is also a known and effective adjuvant for analgesia in the perioperative period, reducing opioid use and preventing opioid tolerance and central sensitisation to nociceptive signalling [23,24,25,26,27]. However, its optimal dosing regimen remains controversial [23], and the drug is not easy to handle due to its possible side effects. Suzuki and colleagues reported reduced pain at three months postoperatively when ketamine was combined with preoperative TEA [28], whereas Dualè et al. found improvements only in immediate postoperative pain, with no long-term benefits [29]. The OS effect of ketamine observed in our study aligns with existing literature and current ERAS recommendations for thoracic surgery. Chumbley et al. conducted a randomised study on 70 patients undergoing thoracotomy, comparing a ketamine infusion (0.1 mg/kg/min preceded by a 0.1 mg/kg bolus) with a control group receiving placebo. Patients in both groups received TEA, patient-controlled analgesia with morphine, or PVB infusion. Opioid use and numeric pain scores at 24 and 48 hours were significantly lower in the ketamine group [30], suggesting its positive modulation on APOP. Furthermore, Jouguelet et al. reviewed the available literature concluding that five meta-analyses and 39 clinical trials were published on this topic with a total of 2482 patients enrolled, 1403 of whom received ketamine[31]. Their summary of the evidence indicated that among the studies reporting a dose of ketamine similar to our approach, six reported a significant reduction in APOP and in opioid consumption within the first 24 hours.
Importantly, unlike previous studies, we did not find evidence of ketamine-related side effects, such as hypertension, tachycardia, hallucinations, or delirium. This finding highlights that ketamine could be well tolerated in the context of a multimodal analgesia protocol, reinforcing its potential as an adjuvant and OS strategy.
According to our study protocol, ketamine infusion was preceded by an ultrasound-guided PVB immediately after the induction of general anaesthesia [32,33]. As emphasised by ERAS guidelines, regional anaesthesia is strongly recommended to reduce postoperative opioid use, with PVB providing analgesia equivalent to TEA, particularly for VATS [16,32,33]. Numerous studies have compared PVB and TEA for thoracic surgery pain management. In a recent narrative review, Hamilton et al. concluded that these techniques provide equivalent analgesia for thoracotomy, although TEA could still be considered the gold standard [25]. However, in the case of VATS, the APOP is of a lower degree, and PVB is preferred as it offers comparable pain relief with fewer perioperative complications. A randomised study by Turhan et al. compared the erector spinae plane block, PVB, and intercostal nerve block after VATS. The authors found that all three techniques provided adequate analgesia, though PVB demonstrated superior pain control and reduced morphine consumption [33].
Interestingly, we observed a significant, albeit weak, inverse correlation between the ketamine starting dose and the need for postoperative rescue morphine (p = 0.002). Indeed, patients receiving a higher initial dose of ketamine (0.25 mg/kg) exhibited superior pain control compared to those receiving (0.20 mg/kg).
In our study, patients in both groups remained haemodynamically stable throughout surgery, with no need for vasopressors or advanced haemodynamic monitoring, and a lower heart rate at awakening may be the result of better-controlled APOP. Overall, it seems that the PVB did not induce clinically relevant sympatholytic effects. Additionally, no complications related to the locoregional technique (e.g., bleeding, pneumothorax, LAST syndrome, inadvertent intrathecal or intravenous local anaesthetic injection) were observed.
An interesting finding in our study was the reduced incidence of chronic pain at three months after surgery, with the incidence more than halved in the OS group (23.8% compared to 52.4%). This finding further highlights the value of reducing exposure to perioperative opioids, which is a hot topic in anaesthesia. The incidence of chronic pain after thoracic surgery varies between 29% and 35% of patients [34,35]. Huan et al. studied 159 patients undergoing VATS and showed that the opioid-free group (in which a postoperative analgesic block was performed) had a reduced incidence of chronic pain compared to the group in which anaesthesia was conducted with opioids only [36]. However, in a meta-analysis pooling data on 1018 patients, Hyo-Seok et al. did not find a decrease in chronic pain in patients who received PVB or other types of thoracic wall blocks compared to those treated without a block [37]. We had similar findings to Yan et al., but it should be noted that in our study, the intervention group received PVB before surgery, which was associated with ketamine infusion. We believe our encouraging results may be partly due to the execution of PVB before the surgical stimulation, reducing neuronal firing and nociceptive activation following surgical stress [34,38].
Our study has several limitations that should be acknowledged. First, it was conducted in a single-centre setting, which may limit the generalisability of the findings to other institutions with different perioperative management protocols. Second, although we prospectively collected data as part of an audit, its retrospective nature introduces potential selection and information biases, which could affect the robustness of our conclusions. Third, the sample size was limited and unbalanced with a ratio of 2:1. This limitation does not allow for the detection of smaller positive effects from the protocol (i.e., reduction of APOP at time points after awakening) nor complications related to ketamine or PVB. Larger, multicentre studies would be necessary to confirm our results and offer external validity. Fourth, our study evaluated chronic postoperative pain over a longer timeframe with only a telephone interview, without a structured questionnaire that may be more appropriate for assessing the development of chronic post-thoracotomy pain syndrome. We believe that future studies should incorporate longer follow-up periods and adequate assessment of chronic post-surgical pain to determine whether the sustained benefits of ketamine and regional anaesthesia extend beyond the immediate postoperative phase. Fifth, while we compared a multimodal OS protocol (PVB and ketamine) to a conventional opioid-based regimen, we did not include control groups with the use of each of the two components of our protocol. This exclusion limits our ability to distinguish the specific contributions of the two strategies in reducing opioid consumption.
5. Conclusions
A multimodal analgesia protocol integrating ultrasound-guided PVB and perioperative ketamine infusion may reduce the need for postoperative rescue doses of opioids while providing effective pain control in the context of an OS approach. Such an approach aligns with the ERAS guidelines for OS strategies in thoracic surgery. However, larger randomised studies are needed to determine the clinical benefits of this association and the incidence of ketamine-related side effects.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org, Figure S1: title; Table S1: title; Video S1: title.
Author Contributions
Conceptualization, D.M. and F.G..; methodology, F.S., F.F.; software, A.C.; validation, F.F. and D.M.; formal analysis, C.B.; investigation, E.M.; resources, F.S.; data curation, R.C.; writing—original draft preparation, D.M.; writing—review and editing, F.S., L.L.; visualization, P.P.; supervision, S.S., F.F.; project administration, F.F. All authors have read and agreed to the published version of the manuscript.” Please turn to the CRediT taxonomy for the term explanation. Authorship must be limited to those who have contributed substantially to the work reported.
Funding
This research received no external funding.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
We encourage all authors of articles published in MDPI journals to share their research data. In this section, please provide details regarding where data supporting reported results can be found, including links to publicly archived datasets analyzed or generated during the study. Where no new data were created, or where data is unavailable due to privacy or ethical restrictions, a statement is still required. Suggested Data Availability Statements are available in section “MDPI Research Data Policies” at https://www.mdpi.com/ethics.
Acknowledgments
In this section, you can acknowledge any support given which is not covered by the author contribution or funding sections. This may include administrative and technical support, or donations in kind (e.g., materials used for experiments). Where GenAI has been used for purposes such as generating text, data, or graphics, or for study design, data collection, analysis, or interpretation of data, please add “During the preparation of this manuscript/study, the author(s) used [tool name, version information] for the purposes of [description of use]. The authors have reviewed and edited the output and take full responsibility for the content of this publication.”.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| APOP | Acute Post Operative Pain |
| ERAS | Enhanced Recovery After Surgery |
| VATS | Video-Assisted Thoracic Surgery |
| TEA | Thoracic Epidural Anaesthesia |
| PVB | ParaVertebral Block |
| OS | Opioid-Sparing |
| MHz | Mega Hertz |
| mg | Milligram |
| kg | Kilogram |
| NRS | Numeric Rating Scale |
| BMI | Body Mass Index |
| PONV | Postoperative Nausea And Vomiting |
| LOS | Length Of Hospital Stay |
| SpO2 | Blood Oxygen Saturation |
| ASA | American Society Of Anetshesiologists |
| SBP | Systolic Blood Pressure |
| DBP | Diastolic Blood Pressure |
| HR | Heart Rate |
| bpm | beat per minute |
| NMDA | Ketamine, an N-methyl-D-aspartate |
| LAST | Local Anesthetic Sytemic Toxicity |
References
- Gerner, P. Postthoracotomy Pain Management Problems. Anesthesiol. Clin. 2008, 26, 355–367. [Google Scholar] [CrossRef]
- Maxwell, C.; Nicoara, A. New developments in the treatment of acute pain after thoracic surgery. Curr. Opin. Anaesthesiol. 2014, 27, 6–11. [Google Scholar] [CrossRef]
- Elmore, B.; Nguyen, V.; Blank, R.; Yount, K.; Lau, C. Pain Management Following Thoracic Surgery. Thorac. Surg. Clin. 2015, 25, 393–409. [Google Scholar] [CrossRef] [PubMed]
- Ghanty, I.; Schraag, S. The quantification and monitoring of intraoperative nociception levels in thoracic surgery: a review. J. Thorac. Dis. 2019, 11, 4059–4071. [Google Scholar] [CrossRef] [PubMed]
- Setti, T.; Sanfilippo, F.; Leykin, Y. Transdermal buprenorphine for postoperative pain control in gynecological surgery: a prospective randomized study. Curr. Med Res. Opin. 2012, 28, 1597–1608. [Google Scholar] [CrossRef] [PubMed]
- Marshall, K.; McLaughlin, K. Pain Management in Thoracic Surgery. Thorac Surg Clin. 2020, 30, 339–346. [Google Scholar] [CrossRef]
- Baldi, C.; Bettinelli, S.; Grossi, P.; Fausto Sardanelli, A.F.; Cavalloro, F.; Allegri, M.; Brasch, A. Ultrasound guidance for locoregional anesthesia: a review. Minerva Anestesiol. 2007, 73, 587–593. [Google Scholar]
- Biuzzi, C.; Marianello, D.; Wellens, C.; Bidi, B.; DI Chiaro, A.; Remiddi, F.; Franchi, F.; Scolletta, S. Multimodal analgesic strategies in polytraumatized patients. Minerva Anestesiol. 2024, 90, 1029–1040. [Google Scholar] [CrossRef]
- Sepolvere, G.; Marianello, D.; Santonocito, C.; Messina, S.; Silvetti, S.; Franchi, F.; Paternoster, G.; Sanfilippo, F. Perspectives On The Role Of Thoracic Fascial Blocks In Cardiac Anaesthesia: Will They Represent A New Era? J Clin Med. 2025, 14, 973. [Google Scholar] [CrossRef]
- Joshi, G.P.; Bonnet, F.; Shah, R.; Wilkinson, R.C.; Camu, F.; Fischer, B.; Neugebauer, E.A.M.; Rawal, N.; Schug, S.A.; Simanski, C.; et al. A Systematic Review of Randomized Trials Evaluating Regional Techniques for Postthoracotomy Analgesia. Anesthesia Analg. 2008, 107, 1026–1040. [Google Scholar] [CrossRef]
- Davies, R.G.; Myles, P.S.; Graham, J.M. A comparison of the analgesic efficacy and side-effects of paravertebral vs epidural blockade for thoracotomy—a systematic review and meta-analysis of randomized trials. Br. J. Anaesth. 2006, 96, 418–426. [Google Scholar] [CrossRef] [PubMed]
- Yeung, J.H.Y.; Gates, S.; Naidu, B.V.; Wilson, M.J.A.; Gao Smith, F. Paravertebral block versus thoracic epidural for patients undergoing thoracotomy. Cochrane Database Syst Rev. 2016, 2, CD009121. [Google Scholar] [CrossRef] [PubMed]
- D’Erco Hle, F.; Harendra Arora, H.; Kumar, P. Paravertebral block for Thoracic Surgery. Journal of Cardiothoracic and Vascular Anesthesia 2018, 32, 915–927. [Google Scholar] [CrossRef]
- Crumley, S.; Schraag, S. The role of local anaesthetic techniques in ERAS protocols for thoracic surgery. J. Thorac. Dis. 2018, 10, 1998–2004. [Google Scholar] [CrossRef] [PubMed]
- George, M.J. The site of action of epidurally administered opioids and its relevance to postoperative pain management. Anaesthesia 2006, 61, 659–664. [Google Scholar] [CrossRef]
- Batchelor, T.J.P.; Rasburn, N.J.; Abdelnour-Berchtold, E.; Brunelli, A.; Cerfolio, R.J.; Gonzalez, M.; Ljungqvist, O.; Petersen, R.H.; Popescu, W.M.; Slinger, P.D.; et al. Guidelines for enhanced recovery after lung surgery: recommendations of the Enhanced Recovery After Surgery (ERAS®) Society and the European Society of Thoracic Surgeons (ESTS). Eur. J. Cardio-Thoracic Surg. 2018, 55, 91–115. [Google Scholar] [CrossRef]
- Cook, T.M.; Counsell, D.; Wildsmith, J.A.W. Major complications of central neuraxial block: report on the Third National Audit Project of the Royal College of Anaesthetists. Br. J. Anaesth. 2009, 102, 179–190. [Google Scholar] [CrossRef]
- Ding, X.; Jin, S.; Niu, X.; Ren, H.; Fu, S.; Li, Q.; Landoni, G. A Comparison of the Analgesia Efficacy and Side Effects of Paravertebral Compared with Epidural Blockade for Thoracotomy: An Updated Meta-Analysis. PLOS ONE 2014, 9, e96233. [Google Scholar] [CrossRef]
- Helms, O.; Mariano, J.; Hentz, J.-G.; Santelmo, N.; Falcoz, P.-E.; Massard, G.; Steib, A. Intra-operative paravertebral block for postoperative analgesia in thoracotomy patients: a randomized, double-blind, placebo-controlled study. Eur. J. Cardio-Thoracic Surg. 2011, 40, 902–906. [Google Scholar] [CrossRef]
- Eason, M.; Wyatt, R. Paravertebral thoracic block—a reappraisal. Anaesthesia 1979, 34, 638–642. [Google Scholar] [CrossRef]
- Luyet, C.; Herrmann, G.; Ross, S.; et al. Ultrasound-guided thoracic paravertebral puncture and placement of catheters in human cadavers: where do catheters go? Br J Anaesth. 2011, 106, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Fortier, S.; Hanna, H.A.; Bernard, A.; Girard, C. Comparison Between Systemic Analgesia, Continuous Wound Catheter Analgesia And Continuous Thoracic Paravertebral Block: A Randomised, Controlled Trial Of Post thoracotomy Pain Management. Eur J Anaesthesiol. 2012, 29, 524–530. [Google Scholar] [CrossRef]
- Radvansky, B.M.; Shah, K.; Parikh, A.; Sifonios, A.N.; Le, V.; Eloy, J.D. Role of Ketamine in Acute Postoperative Pain Management: A Narrative Review. BioMed Res. Int. 2015, 2015, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Chumbley, G.M.; Thompson, L.; Swatman, J.E.; Urch, C. Ketamine infusion for 96 hr after thoracotomy: Effects on acute and persistent pain. Eur. J. Pain 2019, 23, 985–993. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, C.; Alfille, P.; Mountjoy, J.; Bao, X. Regional anesthesia and acute perioperative pain management in thoracic surgery: a narrative review. J. Thorac. Dis. 2022, 14, 2276–2296. [Google Scholar] [CrossRef]
- Chen, X.; Liu, Q.; Fan, L. Effects of thoracic paravertebral block combined with s-ketamine on postoperative pain and cognitive function after thoracoscopic surgery. Heliyon 2022, 8, e12231. [Google Scholar] [CrossRef]
- Michelet, P.; Guervilly, C.; Hélaine, A.; Avaro, J.P.; Blayac, D.; Gaillat, F.; Dantin, T.; Thomas, P.; Kerbaul, F. Adding ketamine to morphine for patient-controlled analgesia after thoracic surgery: influence on morphine consumption, respiratory function, and nocturnal desaturation. Br. J. Anaesth. 2007, 99, 396–403. [Google Scholar] [CrossRef]
- Suzuki, M.; Haraguti, S.; Sugimoto, K.; Kikutani, T.; Shimada, Y.; Sakamoto, A. Low-dose Intravenous Ketamine Potentiates Epidural Analgesia after Thoracotomy. Anesthesiology 2006, 105, 111–119. [Google Scholar] [CrossRef]
- Dualé, C.; Gayraud, G.; Taheri, H.; Bastien, O.; Schoeffler, P. A French Nationwide Survey on Anesthesiologist-Perceived Barriers to the Use of Epidural and Paravertebral Block in Thoracic Surgery. J. Cardiothorac. Vasc. Anesthesia 2015, 29, 942–949. [Google Scholar] [CrossRef]
- Chumbley, G.M.; Thompson, L.; Swatman, J.E.; Urch, C. Ketamine infusion for 96 hr after thoracotomy: Effects on acute and persistent pain. Eur. J. Pain 2019, 23, 985–993. [Google Scholar] [CrossRef]
- Jouguelet-Lacoste, J.; La Colla, L.; Schilling, D.; Chelly, J.E. The Use of Intravenous Infusion or Single Dose of Low-Dose Ketamine for Postoperative Analgesia: A Review of the Current Literature. Pain Med. 2015, 16, 383–403. [Google Scholar] [CrossRef] [PubMed]
- Nesher, N.; Serovian, I.; Marouani, N.; Chazan, S.; Weinbroum, A. Ketamine spares morphine consumption after transthoracic lung and heart surgery without adverse hemodynamic effects☆. Pharmacol. Res. 2008, 58, 38–44. [Google Scholar] [CrossRef]
- Turhan, Ö.; Sivrikoz, N.; Sungur, Z.; Duman, S.; Özkan, B.; Şentürk, M. Thoracic Paravertebral Block Achieves Better Pain Control Than Erector Spinae Plane Block and Intercostal Nerve Block in Thoracoscopic Surgery: A Randomized Study. J. Cardiothorac. Vasc. Anesthesia 2021, 35, 2920–2927. [Google Scholar] [CrossRef] [PubMed]
- Feray, S.; Lemoine, A.; Aveline, C.; Quesnel, C. Pain management after thoracic surgery or chest trauma. Minerva Anestesiol. 2023, 89, 1022–1033. [Google Scholar] [CrossRef] [PubMed]
- Dualé, C.; Ouchchane, L.; Schoeffler, P.; Dubray, C.; Soule-Sonneville, S.; Decoene, C.; Baylot, D.; Lefebvre-Kuntz, D.; Reynier, P.; Sokolo, B.; et al. Neuropathic Aspects of Persistent Postsurgical Pain: A French Multicenter Survey With a 6-Month Prospective Follow-Up. J. Pain 2014, 15, 24.e1–24.e20. [Google Scholar] [CrossRef]
- Huan, Y.; Wannan, C.; Youwen, C.; Huayuan, G.; Yu, F.; Mingxiang, F.; Xiaoming, W.; Han, T.; Jiacheng, Y.; Yunjia, Q.; Ming, D.; Jing, C.; Changhong, M.; Hao, W. Opioid-Free Versus Opioid-Based Anesthesia on Postoperative Pain After Thoracoscopic Surgery: The Use of Intravenous and Epidural Esketamine. Anesthesia & Analgesia. 2023, 137, 399–408. [Google Scholar]
- Na, H.-S.; Koo, C.-H.; Koo, B.-W.; Ryu, J.-H.; Jo, H.; Shin, H.-J. Effect of the Paravertebral Block on Chronic Postsurgical Pain After Thoracic Surgery: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Cardiothorac. Vasc. Anesthesia 2022, 37, 252–260. [Google Scholar] [CrossRef]
- Bugada, D.; Ghisi, D.; Mariano, E.R. Continuous regional anesthesia: a review of perioperative outcome benefits. Minerva Anestesiol. 2017, 83, 1089–1100. [Google Scholar] [CrossRef]
Figure 2.
NRS.NRS after surgery was lower in OS-group (1 [1-2]) referred to Control group (4[3-4]; p>0.001).
Figure 2.
NRS.NRS after surgery was lower in OS-group (1 [1-2]) referred to Control group (4[3-4]; p>0.001).
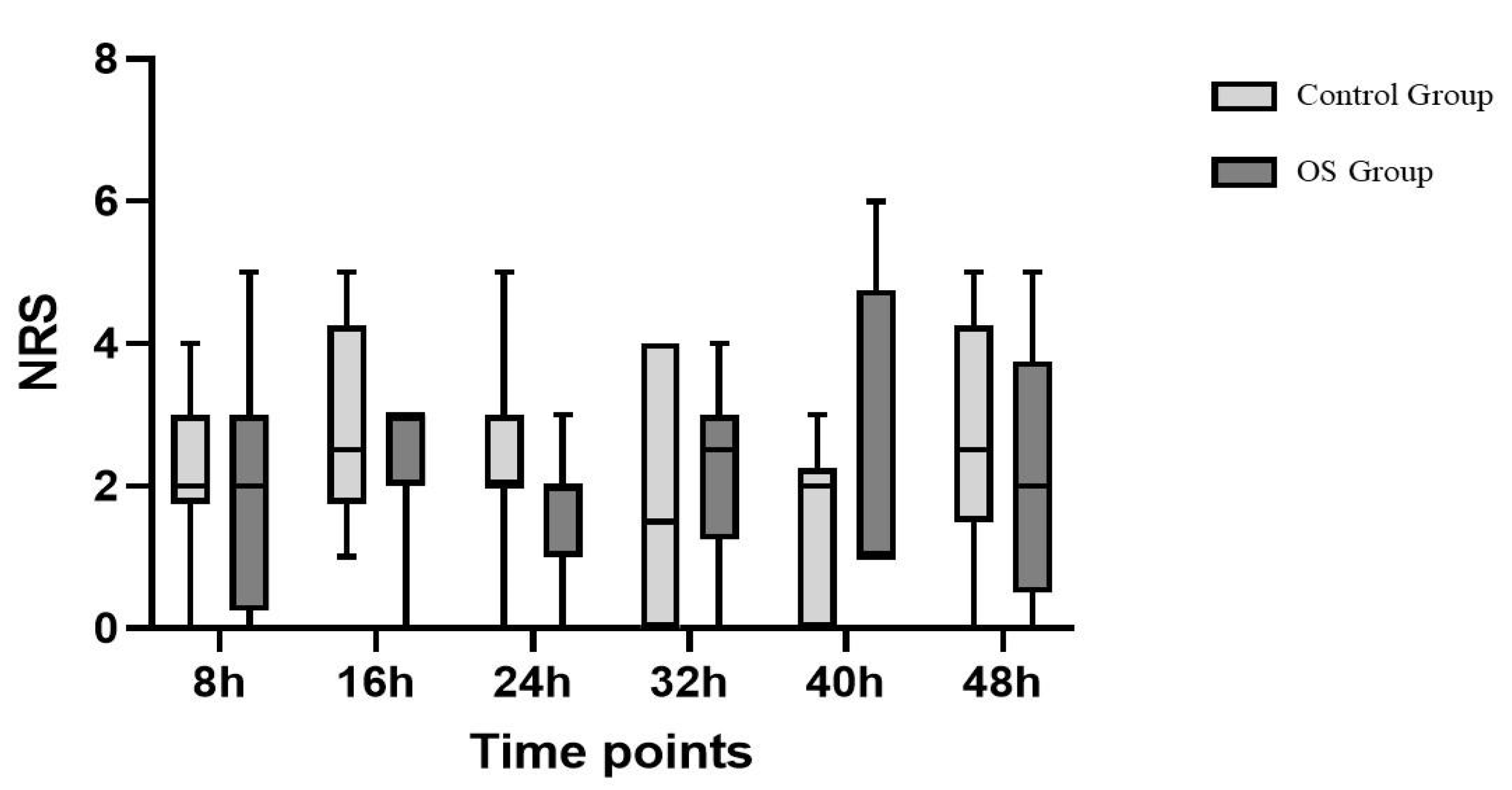

Table 1.
Characteristics of the study population. Results are presented as median and interquartile range, and absolute numbers with percentages.
Table 1.
Characteristics of the study population. Results are presented as median and interquartile range, and absolute numbers with percentages.
| Variables | Overall Population (N =62) |
OS Group (n=41) |
Control Group (n=21) |
p Value |
|---|---|---|---|---|
| Age, years | 68 [64-73] | 71 [65-74] | 67 [61-73] | 0.16 |
| Sex (M), N (%) | 24 (39) | 18 (44) | 6 (29) | 0.25 |
| Weight, kg | 70 [58-79] | 70 [60-80] | 65 [55-70] | 0.13 |
| Height, cm | 166 [160-172] | 166 [162-180] | 165 [159-175] | 0.60 |
| ASA Score | 2 [2-2] | 2 [2-2] | [2-2] | 0.07 |
ASA, American Society of Anesthesiologists; OS: Opioid Sparing. .
Table 2.
Differences in morphine rescue dose use and NRS scale trend in the two groups during the first 48 hours after surgery. Results are presented as median and interquartile range, and absolute numbers with percentages.
Table 2.
Differences in morphine rescue dose use and NRS scale trend in the two groups during the first 48 hours after surgery. Results are presented as median and interquartile range, and absolute numbers with percentages.
| Variables | Overall Population (n=62) | OS Group (n=41) |
Control Group (n=21) |
p |
|---|---|---|---|---|
| Morphine rescue (by 48 h) | 18 (29%) | 8 (19.5%) | 10 (47.6%) | 0.021 |
| NRS after surgery | 2 [1-3] | 1 [1-2] | 4 [3-4] | <0.001 |
| NRS 8h | 2 [1-2] | 2 [1-2] | 2 [1-2] | 0.66 |
| NRS 16h | 2 [1-3] | 1 [1-2] | 2 [1-2] | 0.50 |
| NRS 24h | 2 [1-2] | 2 [1-2] | 2 [1-3] | 0.24 |
| NRS 32h | 1 [1-2] | 0 [0-2] | 2 [1-3] | 0.12 |
| NRS 40h | 1 [0-2] | 1 [1-2] | 1 [0-2] | 0.37 |
| NRS 48h | 1 [0-2] | 1 [0-2] | 0 [0-3] | 0.11 |
| Chronic Pain, n (%) | 21 (33,9%) | 10 (23,8%) | 11 (52,4%) | 0.028 |
NRS, Numeric Range Scale; OS group, Opioid Sparing Group.
Table 3.
Hemodynamics and respiratory parameters during the time of observation between the two groups. Results are presented as median and interquartile range.
Table 3.
Hemodynamics and respiratory parameters during the time of observation between the two groups. Results are presented as median and interquartile range.
| Overall Population (n=62) |
OS Group (n=41) |
Control Group (n=21) |
p | |
|---|---|---|---|---|
| SBP after surgery, mmHg | 120 [110-135] | 120 [110-135] | 120 [115-140] | 0.28 |
| SBP 8h | 130 [120-140] | 130 [120-140] | 130 [115-140] | 0.71 |
| SBP 16h | 125 [115-135] | 123 [115-135] | 125 [112-135] | 0.80 |
| SBP 24h | 125 [115-145] | 130 [115-150] | 125 [110-130] | 0.11 |
| SBP 32h | 125 [116-140] | 130 [120-140] | 120 [110-130] | 0.06 |
| SBP 40h | 125 [115-145] | 125 [115-145] | 120 [115-125] | 0.58 |
| SBP 48h | 130 [120-145] | 130 [120-150] | 133 [115-140] | 0.54 |
| DBP after surgery, mmHg | 70 [61-80] | 70 [60-80] | 70 [65-75] | 0.83 |
| DBP 8h, mmHg | 75 [70-85] | 80 [70-85] | 75 [60-80] | 0.26 |
| DBP 16h, mmHg | 75 [65-83] | 80 [65-83] | 70 [65-80] | 0.64 |
| DPB 24h, mmHg | 70 [65-80] | 75 [65-85] | 70 [60-80] | 0.07 |
| DBP 32h, mmHg | 72 [65-80] | 75 [68-87] | 70 [65-75] | 0.15 |
| DBP 40h, mmHg | 75 [65-85] | 75 [67-90] | 75 [65-80] | 0.24 |
| DBP 48h, mmHg | 80 [65-85] | 80 [65-90] | 75 [67-80] | 0.13 |
| HR after surgery, bpm | 75 [68-80] | 70 [67-75] | 85 [76-86] | <0.001 |
| HR 8h, bpm | 74 [70-78] | 75 [70-79] | 74 [67-76] | 0.32 |
| HR 16h, bpm | 75 [70-80] | 76 [68-81] | 75 [72-80] | 0.87 |
| HR 24h, bpm | 78 [70-85] | 78 [68-85] | 78 [75-84] | 0.67 |
| HR 32h, bpm | 74 [70-78] | 74 [70-80] | 75 [70-78] | 0.93 |
| HR 40h, bpm | 77 [70-80] | 77 [70-80] | 77 [70-80] | 0.64 |
| HR 48h, bpm | 78 [70-83] | 76 [70-80] | 80 [76-90] | 0.11 |
| SpO2 after surgery, % | 95 [94-97] | 95 [94-97] | 95 [94-95] | 0.02 |
| SpO2 8h, % | 96 [94-97] | 96 [94-97] | 95 [94-96] | 0.20 |
| SpO2 16h, % | 96 [94-97] | 96 [94-97] | 96 [94-97] | 0.96 |
| SpO2 24h, % | 95 [93-97] | 96 [93-98] | 95 [93-96] | 0.12 |
| SpO2 32h, % | 95 [93-97] | 95 [94-97] | 94 [92-96] | 0.14 |
| SpO2 40h, % | 95 [92-96] | 95 [93-96] | 93 [91-96] | 0.18 |
| SpO2 48h, % | 94 [93-96] | 94 [93-96] | 94 [91-96] | 0.29 |
SPB, systolic blood pressure; DPB, diastolic blood pressure; HR, Heart Rate; bpm, beat per minute.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



