Submitted:
22 February 2026
Posted:
25 February 2026
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background/Objectives: Cognitive dysfunction, or “brain fog”, following Covid-19 viral infection is strongly associated with diminished work capacity which disproportionality affects working-age adults. This study examined an existing method of cognitive reha-bilitation training applied to adults struggling with workplace functioning and self-efficacy due to post-Covid brain fog. Methods: Nine adults with post-Covid cognitive dysfunction participated in this single arm pilot trial of a severity-adaptive cognitive training program. Participants completed 45-90 hours of clinician-delivered cognitive training exercises delivered remotely in 60 to 90-minute sessions, 2 or 3 times per week. The primary outcome measure was overall workplace self-efficacy with subskills of perceived workplace functioning, perception of cognitive functioning, and perception of [1–3]home functioning assessed through a pre and post quantitative survey and quali-tative interviews. The secondary outcome was cognitive function operationalized by IQ score administered before and after the intervention. Results: Participants achieved significant improvements in workplace self-efficacy and cognition following cognitive training. The main qualitative themes of self-reported improvements were in executive function, health and energy, daily living activities, productivity, and socioemotional functioning. A cross-case synthesis of pre-intervention struggles and post-intervention improvements revealed subthemes at work or school in cognitive processing and com-prehension, memory, executive function, fatigue, emotional distress, confidence in work or academics, and work/academic performance impairment. As a group, the mean gain in IQ score was 10.5 points. Conclusions: This study adds to the growing body of literature examining how cognitive rehabilitation for post-Covid cognitive sequalae may be im-portant for restoring not only cognitive functioning but also workplace self-efficacy and performance.
Keywords:
cognitive training
; cognitive rehabilitation
; cognition
; memory
; post-Covid syndrome
; long COVID
; neuroplasticity
; attention
; focus
1. Introduction
Post-acute sequelae of COVID-19 (PASC), also referred to as post-acute COVID-19 syndrome (PACS) and long COVID, describes a heterogeneous constellation of persistent symptoms that can affect multiple organ systems following acute SARS-CoV-2 infection. Among these, neurological manifestations – often termed neurological PASC (NC-PASC) - are particularly prevalent and disabling, even in individuals who experience mild initial illness. Reported symptoms span cognitive, autonomic, and affective domains and commonly include cognitive dysfunction (“brain-fog”), impaired attention and memory, slowed processing speed, fatigue, myalgia, headache, and dysautonomia [1,2,3]. The severity and combination of symptoms vary substantially across individuals, contributing to a marked clinical heterogeneity and complicating diagnosis, mechanistic interpretation, and treatment development, consistent with prior post-viral and post-infectious syndromes described after other acute infections [4].
A central controversy in the field concerns the pathophysiological basis of NC-PASC. While SARS-CoV-2 has been shown to access the central nervous system (CNS) through olfactory, vascular, and blood-brain barrier (BBB) associated routes [5,6,7,8,9], current evidence does not suggest widespread, persistent viral infection of the CNS as the primary driver of long-term cognitive symptoms [10,11]. Instead, converging lines of evidence suggest that NC-PASC arises from multiple, interacting mechanisms, including chronic neuroinflammation, endothelial dysfunction, BBB disruption, microvascular injury, immune dysregulation and impaired neural plasticity [12,13,14]. Recent molecular imaging work further suggests that these upstream processes may converge at the synaptic level, with evidence of widespread alterations in postsynaptic glutamatergic signaling associated with cognitive impairment in NC-PASC, consistent with diffuse network-level dysfunction rather than focal pathology [15]. These mechanisms may act synergistically to disrupt large-scale brain networks rather than producing focal deficits, offering one explanation for the diffuse and fluctuating cognitive symptoms reported by patients. Importantly, the diversity of the proposed mechanisms makes the likelihood of a single, mechanism-targeted therapy relatively low.
In parallel with mechanistic research, growing attention has been directed toward the functional consequences of post-COVID cognitive impairment. Large-scale patient-led and longitudinal studies demonstrate that cognitive dysfunction is not only highly prevalent but also a major driver of disability in PASC. In a large, multinational survey spanning over 3,700 individuals with PASC, Davis et al. characterized the prevalence and functional consequences of cognitive dysfunction, reporting cognitive dysfunction and/or memory impairment in approximately 88% of respondents across all age groups and a strong association with impaired occupational functioning, with over 86% of working participants reporting mild to severe difficulty performing their jobs [16]. Consistent with this, nearly half of respondents required reduced work hours, and more than one-fifth were unable to work at the time of survey completion due to NC-PASC. These findings align with broader population-based studies showing that NC-PASC disproportionately affects working-age adults and contributes to significant societal and economic burden [2,17,18].
Within this context, cognitive rehabilitation training interventions have emerged as potentially promising, pragmatic approaches for addressing post-COVID brain fog. However, outcomes have been inconsistent across interventions specifically targeting Covid-related cognitive dysfunction and return-to-work challenges. For example, Garcia-Molina et al. (2022) evaluated a post-Covid rehabilitation program where 44.9% of participants remained unable to perform their workplace functions and 81.2% continued to experience difficulty with activities of daily living following completion of cognitive rehabilitation [19]. Similarly, a 2025 scoping review of return-to-work interventions for individuals living with PASC, the few interventions classified as “promising” emphasized multidisciplinary, clinician-supported approaches, while self-directed digital rehabilitation programs showed limited evidence of effectiveness [20].
Nevertheless, evidence from longitudinal cohorts, systemic reviews, and early-phase intervention studies suggests that cognitive rehabilitation – particularly when adaptive, individualized, and multi-domain – can be associated with improvements in both objective cognitive performance and real-world functioning, including work participation and self-efficacy [21,22,23]. These findings are consistent with broader cognitive neuroscience and rehabilitation literature demonstrating that repeated, targeted cognitive engagement can support recovery through experience-dependent neuroplasticity, even in the presence of ongoing neurobiological vulnerability [24,25,26].
Prior work by our group has demonstrated the feasibility and functional relevance of utilizing the LearningRx Brain Strong (formerly Brain Booster) and ThinkRx cognitive training programs in populations with neurodevelopmental and learning disorders, traumatic brain injury (TBI), and age-related cognitive decline. Across multiple studies, intervention participation was associated with significant improvements in cognitive performance as well as functional outcomes, self-reported confidence in cognitive abilities with evidence of transfer beyond standardized test performance to everyday functioning [27,28,29,30,31,32,33,34]. These findings provide important precedent for applying a severity-tailored, multi-domain cognitive training approach to other heterogeneous neurological conditions characterized by diffuse network dysfunction, including NC-PASC.
Together, this body of work suggests that functionally oriented cognitive interventions, designed to accommodate individual variability and emphasize real-world relevance, may be particularly well suited to addressing post-COVID cognitive sequelae. Accordingly, outcomes that capture confidence, competence, and perceived ability to function in occupational roles, such as workplace self-efficacy, may offer clinically meaningful indicators of recovery in early-phase intervention studies.
The primary aim of this study was to evaluate, using both quantitative and qualitative methods, pre-post changes in workplace self-efficacy following a clinically and commercially available, adaptive, severity-tailored cognitive training intervention in individuals with varying severity of post-COVID brain fog. A secondary aim was to explore changes in objective cognitive performance. Using a single-arm design and a small, intentionally heterogenous sample, analyses were exploratory and intended to identify preliminary signals of functional improvement and inform the design of future, controlled studies rather than establish treatment efficacy [35,36].
2. Materials and Methods
2.1. Study Design and Implementation Considerations
The current study employed a prospective, single-arm, proof-of-concept interventional design to evaluate pre-post changes in workplace self-efficacy and cognitive performance following a clinically and commercially available, adaptive, severity-tailored cognitive training intervention in adults with post-COVID brain fog.
All study procedures – including informed consent, screening, assessment, and intervention delivery – were conducted remotely using a secure videoconferencing platform (e.g., Zoom). The study was designed to protect participant privacy and maximize feasibility for working adults, reflecting real-world conditions under which the intervention would typically be delivered.
Initial recruitment occurred through local dissemination of study flyers and word-of-mouth outreach during early phases of study planning, when pre-post MRI imaging was under consideration. Subsequent sharing of recruitment materials on a long-COVID community message board generated immediate interest and enabled enrollment of a geographically diverse cohort with heterogeneous disease severity.
Given that the intervention is commercially available and deliverable remotely without geographic constraints, geographical diversity was prioritized over inclusion of neuroimaging as a secondary outcome measure. This decision supported feasibility and external validity while maintaining focus on functionally meaningfully clinical outcomes.
2.2. Participants
Inclusion criteria consisted of adults aged ≥18 years with persistent subjective cognitive impairment (“brain fog”) lasting more than 60 days following COVID-19 who were working (including volunteer roles), enrolled in school, or unable to work or attend school due to COVID-19, and were able to provide informed consent and complete study procedures. Exclusion criteria included non-English speakers, incarcerated individuals, those with a history of stroke, individuals with unstable medical or psychiatric conditions, and those pregnant at the time of consent.
2.3. Intervention
The cognitive training intervention used in this study was Brain Strong (formerly Brain Booster), a clinically and commercially available cognitive training program used in LearningRx cognitive training centers across the United States. The training methodology has been extensively tested through a variety of research designs and described in previous studies [27,28,29,30,31,32,33,34] so, therefore, briefly highlighted here.
The Brain Strong intervention is an adult-focused version of the cognitive training methodology created by LearningRx. It consists of sixteen core mental exercises delivered by a cognitive trainer. Each training exercise has 8 to 12 variations sequenced in order of difficulty and complexity and designed to target multiple cognitive domains, including working memory, long-term memory, processing speed, fluid reasoning, visual processing, auditory processing, and attention. Training tasks are hands-on using a variety of manipulatives, cards, shapes, and workboards with grids and diagrams. Crucially, tasks are structured to promote coordinated engagement of multiple cognitive domain networks within a single activity, rather than isolated practice of individual skills. For example, a memory task requiring the participant to reproduce patterns of shapes on a grid also engages visual processing, processing speed, and attention, particularly as the number of shapes increases and the time allotted for the task decreases. See Figure 1 for an illustration of this task.
Each task is also paced using a metronome to increase development of automaticity and to increase the intensity of the training session flow. Participants respond “on beat” to the metronome with oral answers to the actual task or with answers to an unrelated task. For example, on the same memory task where the participant must reproduce a pattern of shapes from memory, he must also answer a math question in the allotted time window.
The Brain Strong program was originally designed to be delivered in a clinic setting in person but has been adapted and rigorously tested in the remote environment as well. In the current study, all the participants were trained remotely over Zoom. At the beginning of the study period, each participant was mailed an external webcam and all hands-on materials needed for training. Training was delivered through one-on-one sessions with a participant’s assigned cognitive trainer who has been trained and certified in the program’s delivery. The intervention was delivered using an adaptive, severity-tailored protocol with total training duration ranging from 45 to 90 training hours. All participants began with a minimum training duration of 45 hours. Participants attended two to three training sessions per week, each lasting 60 or 90 minutes, based on participant preference, tolerance, and schedule. Following completion of the initial 45 hours, additional training hours were assigned in 15-hour increments, determined through ongoing needs assessments and collaborative discussions involving the participant, the cognitive trainer, and the study director. This adaptive and flexible delivery model mirrors standard clinical practice in LearningRx cognitive training centers and therefore supports the ecological validity of the intervention.
2.4. Primary Assessment Measures and Data Collection
The primary outcome for the study was workplace self-efficacy. Two measures were used to assess the construct: Workplace Self-Efficacy Survey and a semi-structured interview. Data from both measures were collected before and after the intervention.
The Workplace Self-Efficacy Survey is a 29-item Likert-style functional rating scale with questions and response options on a scale from 1 to 10 developed by Christina Ledbetter at LSU. The questions are divided into three categories: 1) Perceived performance at work or school (20 items), 2) perceived cognitive functioning at work or school (6 items), and 3) perceived functioning at home (3 items). A composite score on overall workplace self-efficacy is also generated by adding the scores on categories 1 and 2. Appendix A lists the survey items. Each participant completed the survey twice: once at the beginning of the study and again after completing the intervention. When a participant was enrolled in the study and had completed their informed consent documents, the study director emailed the participant a link to the survey using RedCap [37,38], a secure web application for electronic data capture hosted at LSU and compliant with HIPAA and 21CFR Part 11. It’s used by more than 8,000 institutions for administering and collecting survey data.
After receiving the link, each participant was asked to rate themselves on each item as they recall functioning prior to getting Covid. Then, they were asked to rate how they perceive themselves to be functioning on each item currently (after getting Covid but before starting the intervention). After the intervention, the participant was asked to rate their perceived functioning on each item again. To minimize expectancy effects and encourage realistic reporting, they could not see their original responses from the beginning of the study.
The second method for assessing the primary outcome of workplace self-efficacy was through pre and post semi-structured interviews. Each participant in the current study was interviewed two times: once at the beginning of the study and again upon completion of the intervention. The interviews were conducted by doctoral-level researchers in the fields of psychology and neuroscience using the items on the Workplace Self-Efficacy Survey as the interview guide. The interviewer asked the participant to comment on each of their ratings and to give an example of how the item impacts them at work or school or at home. For example, in the baseline interview, Item #3a Ability to maintain workspace order or neatness BEFORE Covid served as a prompt for the question, “Give me an example of your ability to do that. What did that look like for you?” Then, the interviewer would ask for an example of how each ability changed AFTER getting Covid. Item #3b Ability to maintain workspace order or neatness AFTER Covid served as a prompt for the question, “What does that look like for you after getting Covid. How did that ability change?” At the exit interview, the interviewer would ask the participant to comment on their ratings of each item after completing the intervention. For example, Item 3c Ability to maintain workspace order or neatness currently AFTER completing cognitive training served as a prompt for the question, “Tell me about your rating on this item. What does that look like for you now? What has changed since completing cognitive training?”
In addition to asking about the participant’s ratings on the survey, the interviewer also asked the participant to talk about any other changes they noticed since completing cognitive training. To encourage self-reflection, the interviewer was careful to use neutral terms such as “changes” versus “improvements” and asked general questions such as “What have you noticed about ______?” rather than asking leading questions such as “What improvements have you seen in ______?”
Following the interviews, the recordings were transcribed using Descript software. The transcripts were then downloaded for analysis.
2.5. Secondary Assessment Measure and Data Collection
The secondary outcome for the current study was change in overall cognitive function which we operationalized using an IQ score, or the General Intellectual Ability (GIA) composite score from the Woodcock Johnson IV (WJIV) Tests of Cognitive Abilities [39]. The GIA is a weighted composite of 7 subtests measuring the following constructs: fluid reasoning, short-term working memory, long-term memory, visual processing, auditory processing, processing speed, and prior knowledge. The GIA score has a median reliability of .97 across the normative sample [40]. The WJIV was administered either in person or remotely by a doctoral level psychologist. Raw scores were uploaded into Riverside Score, the online scoring system for the assessment, and then the score report was downloaded for analysis.
2.6. Data Analysis
2.6.1. Workplace Self-Efficacy Survey Statistical Analysis
The primary outcome for this study was to quantify change in workplace self-efficacy for the participants. We first assessed this outcome using the scores on the Workplace Self-Efficacy Survey (WSES) completed by the participants. Statistical analysis was conducted using SPSS, Version 29. We performed a within-group group repeated measures MANOVA to determine whether the overall Workplace Self-Efficacy Score as well as ratings of perceived workplace performance, cognitive functioning at work, and home functioning changed over three timepoints: before COVID, after getting COVID, and after cognitive training. We used Time as the independent variable and the four composite scores on the WSES as the dependent variable (with three timepoints). Partial eta squared was the metric used for effect size classified as small ( = .01), medium ( = .06), and large ( .14).
2.6.2. Interview Data Analysis
We analyzed the interview data from pre and post-intervention interviews using a codebook-style thematic analysis based flexibly and pragmatically on Braun and Clark’s 6 phase framework: familiarization, coding, theme development, review, definition, and write-up [41] . We familiarized ourselves with the transcripts, generated an initial coding framework based on the interview guide, and then coded the data from both the pre and post intervention interviews using the codebook to ensure the ability to compare longitudinally. After completing the coding, we created code-by-participant matrices and then put into clusters that addressed like areas of functioning to help develop themes and subthemes. After comparing the themes to the overall dataset, we refined them to ensure clear distinctions between them and then gave them official names.
Then, we developed a cross-case synthesis matrix using pre-intervention subthemes and post-intervention subthemes to look at change over time and across participants. Finally, we conducted descriptive counts of how many participants reported data in each subtheme to show pattern strength and we selected representative examples for the narrative.
2.6.3. IQ Score Data Analysis
The secondary outcome for this study was to quantify change in IQ score for the participants. We assessed this outcome using the General Intellectual Ability (GIA) composite scores on the WJIV. Statistical analysis was conducted using SPSS, Version 29. We performed a paired samples t test on pre-intervention and post-intervention standard scores to determine whether there was a significant change following the intervention. We report Cohen’s d as the metric for effect size classified as small (d = .2), medium (d = .5), and large (d .8).
2.7. Ethics
The study was approved by the Institutional Review Board of Louisiana State University Health Sciences Center Shreveport (IRB Study00001896; original approval July 11, 2022). Written informed consent was obtained from all participants prior to study participation. In accordance with the approved protocol and institutional policies, all assessment data and interview recordings were stored securely, and identifiable information was removed from interview transcripts to protect participant confidentiality.
3. Results
3.1. Participant Characteristics
Eleven participants from across the United States enrolled in the study (8 female, 3 male); however, two participants withdrew early due to unanticipated family needs. The final analytic sample therefore included nine participants (8 female, 1 male). All nine participants completed the training intervention and the workplace self-efficacy survey. Pre-post qualitative interviews and cognitive assessments were available for eight participants, reflecting one instance of incomplete secondary outcome data.
To protect participant privacy, ages were rounded to the nearest half-decade, and occupations were reported in general categories. Participant ages ranged from 20 to 55 years (median = 40, IQR = 35-45). Occupations spanned a range of fields, including military and first responders, legal and personal services, science and industry, small business ownership, writing, and higher education (college students).
The median time between SARS-CoV-2 infection and study participation was 21 months (range = 11-76 months). None of the participants required hospitalization during their acute COVID-19 illness. At the time of enrollment, participants reported persistent post-acute sequelae consistent with NC-PASC. Reported post-COVID symptoms spanned cognitive, autonomic and affective domains and included cognitive dysfunction (“brain fog”), impaired attention and memory, slowed processing speed, fatigue, headache, sleep disturbance, anxiety, dysautonomia, and attention-related difficulties. Several participants also reported ongoing pulmonary manifestations, including dyspnea and reduced exercise tolerance. Four participants reported receiving ongoing care through specialized long-COVID clinics.
Total training exposure varied across participants, reflecting the adaptive delivery model of the intervention. Total training hours ranged from 45 to 90 hours, with participants completing between 30 and 90 training sessions. Session duration was either 60 or 90 minutes, and the total training period spanned 4 to 13 months. Variability was observed in the number of sessions required to complete training as well as in the overall duration of participation. Individual training parameters are summarized in Table 1.
3.2. Primary Outcome: Workplace Self-Efficacy Survey Results
The primary outcome for this study was to quantify change in workplace self-efficacy for the participants. We first assessed this outcome using the scores on the Workplace Self-Efficacy Survey (WSES) completed by the participants. We performed a within-group group repeated measures MANOVA to determine whether the overall Workplace Self-Efficacy Score as well as ratings of perceived workplace performance, cognitive functioning at work, and home functioning changed over three timepoints: before COVID, after getting COVID, and after cognitive training. Ratings on the 29 individual items on the survey are presented in Appendix A and results of the MANOVA on the four composite scores are illustrated in Table 2 and described below:
3.2.1. Workplace Self-Efficacy Score
There was a statistically significant effect of Time on the Workplace Self-Efficacy Score, F(2,16) = 18.28, p < .001, = .69 with a large effect size. Post hoc testing with a Bonferroni correction revealed that the Workplace Self-Efficacy Score was significantly higher at Time 1 before getting COVID (M = 239.56, SD = 4.9) than at Time 2 after getting COVID (M = 119.66, SD = 22.1, p = .002). The Workplace Self-Efficacy Score was also significantly higher at Time 3 after cognitive training (M = 201.22, SD = 22.1) than it was at Time 2 after getting COVID but before training (p = .003). There was no significant difference between the Workplace Self-Efficacy Score at Time 1 before getting COVID and at Time 3 after training (p = .35), indicating a general return to pre-COVID function in workplace self-efficacy after cognitive training.
3.2.2. Work Performance Rating
There was a statistically significant effect of Time on the Work Performance Rating, F(2,16) = 17.66, p < .001, = .69 with a large effect size. Post hoc testing with a Bonferroni correction revealed that the Work Performance Rating was significantly higher at Time 1 before getting COVID (M = 177.56, SD = 3.2) than at Time 2 after getting COVID (M = 90.89, SD = 16.1, p = .002). The Work Performance Rating was also significantly higher at Time 3 after cognitive training (M = 148.11, SD = 15.4) than it was at Time 2 after getting COVID but before training (p = .003). There was no significant difference between the Work Performance Rating at Time 1 before getting COVID and at Time 3 after training (p = .31), indicating a general return to pre-COVID function in perceived work or school performance after cognitive training.
3.2.3. Cognitive Performance Rating
There was a statistically significant effect of Time on the Cognitive Performance Rating, F(2,16) = 17.91, p < .001, = .69 with a large effect size. Post hoc testing with a Bonferroni correction revealed that the Cognitive Performance Rating was significantly higher at Time 1 before getting COVID (M = 62.00, SD = 2.1) than at Time 2 after getting COVID (M = 28.78, SD = 6.3, p = .001). Cognitive Performance Rating was also significantly higher at Time 3 after cognitive training (M = 53.11, SD = 5.2) than it was at Time 2 after getting COVID but before training (p = .006). There was no significant difference between the Cognitive Performance Rating at Time 1 before getting COVID and at Time 3 after training (p = .52), indicating a general return to pre-COVID function in perceived cognitive performance after cognitive training.
3.2.4. Home Functioning Rating
There was a statistically significant effect of Time on the Home Functioning Rating, F(2,16) = 18.23, p < .001, = .69 with a large effect size. Post hoc testing with a Bonferroni correction revealed that the Home Functioning Rating was significantly higher at Time 1 before getting COVID (M = 26.89, SD = .93) than at Time 2 after getting COVID (M = 13.44, SD = 2.43, p = .001). Home Functioning Rating was also significantly higher at Time 3 after cognitive training (M = 23.67, SD = 2.5) than it was at Time 2 after getting COVID but before training (p = .001). There was no significant difference between the Home Functioning Rating at Time 1 before getting COVID and at Time 3 after training (p = .80), indicating a general return to pre-COVID function in perceived home functioning after cognitive training.
3.3. Primary Outcome: Interview Results
Of the 9 participants in the study, 8 completed the pre and post interviews. The qualitative thematic analysis was conducted on the qualitative data from those 8. Five main themes emerged in both intake (pre-intervention) and exit (post-intervention) qualitative interview data: executive function, health and energy, daily living activities, productivity, and socioemotional functioning. Table 3 summarizes these main themes, the percentage of participants who reported them, and examples of items in each theme.
3.3.1. Executive Function
The theme of executive function captures the extensive cognitive challenges, specifically the executive functions, following COVID and subsequent cognitive and executive function improvements after the intervention. It reflects difficulties such as initiating and completing tasks, maintaining attention and focus, processing information (both verbal and visual), problem solving, planning, and memory (short- and long-term). For example, one participant lamented after Covid, “My thoughts were scattered, making organization difficult…my thoughts overlapped, making it hard to categorize and keep them in order.”
And this theme also reflects participants’ post-training perceived improvements in memory, planning, attention, and problem solving. One participant said, “If I’m comparing now with six months ago, it’s night and day. I feel like I’m at about 80% of where I was before I got sick.” Another said, “I have more motivation sometimes,” and “I still struggle with long-term focus, but it’s better.” Other participants describe significant improvements such as, “I can figure things out [now],” and “I know I wouldn’t have been able to do this in the condition I was in before,” and “Memories come back randomly and…it brings me joy when I remember something!” One participant also said, “My attention to detail, short term memory, and ability to not get distracted in loud environments is the best I can remember since before Covid.”
3.3.2. Productivity
The theme of productivity addresses the post-Covid impact on professional, academic, and work-related activities. In pre-intervention interviews, examples included reduced work output, diminished work quality, and challenges in meeting work and/or academic deadlines, lower productivity, frequent errors, and fears of career stagnation, loss of employment, and academic failure. In post-intervention interviews, participants mentioned improvements in work attendance, productivity, planning, and the ability to complete a normal workload. One participant described, “Before Covid I worked 24-hour shifts and I always knew my deadlines and benchmarks. After Covid I had brain fog…my thinking slowed down, I started screwing up dates and times.” After the intervention, the same participant reported “I feel sharp again. I’m driven. I’m going back to college.” Another participant reported a dramatic improved in grades saying, “I’m much more efficient in balancing responsibilities. I can make a plan, stick to it, and get things done…Now I can complete tasks.” Every participant reported some level of improved productivity with work or academics such as, “I stay busy and productive,” and “Now, I’m doing my job well.”
3.3.3. Health and Energy
This theme reflects the widespread physical health challenges and energy constraints experienced after COVID, as well as the strategies participants adopted to manage these issues. At the pre-intervention interview, participants reported post-exertional malaise, lingering lethargy, nerve pain, disrupted sleep, and autonomic dysfunction (e.g., POTS, migraines). One participant stated significant ongoing health issues with shortness of breath, fatigue, and dizziness. They discussed fatigue-related problems with confusion, inattention, and inability to follow conversations stating, “I have no concept of time, no schedules, no thought process; I’m just trying to get through the day... I forget what I’m saying or can’t keep simple conversations.” Another mentioned, “It’s too hard to drive; I get very sleepy and can’t stay focused,” while another said, “Even social interaction drains me.” After completing the intervention, participants described developing structured sleep and exercise routines, and improvements in energy resulting in more motivation, better focus, and feeling more cognitively healthy. One stated, “I stay on task, organize, declutter, and feel like myself again.”
3.3.4. Daily Living Activities
This theme encompasses the post-Covid challenges in Activities of Daily Living (ADLs) and Instrumental Activities of Daily Living (IADLs), such as managing day-to-day living tasks, personal hygiene, and maintaining an orderly home, as well as the post-intervention improvements in these same areas. Prior to the intervention, multiple participants described a post-Covid decline in their ability to keep up with cleanliness, organization, and scheduling of personal activities. One participant stated, “It’s a struggle just to manage basic tasks,” and another said, “Mostly it’s just an inability to focus long enough to finish [household] tasks.” One said, “Initiating tasks is much harder. I procrastinate even small things like ordering pet food…. I forgot to pack my child’s lunch, first time ever. Later, I couldn’t remember what day it was.” After the intervention, participants described specific improvements such as, “My house isn’t like I used to keep it…but I pace myself and do better now,” and “I can help my daughter with her homework again, which I couldn’t do before,” and “Now I can put household tasks down and come back to them [later]…before I couldn’t focus at all.”
3.3.5. Socioemotional Functioning
This theme reflects the emotional and psychological toll of Covid 19 on confidence, personal identity, and social relationships. Prior to the intervention, participants expressed emotional distress, depression, anxiety, and feelings of isolation that affected self-confidence and interpersonal interactions saying, “I get overwhelmed really fast. I struggle with lack of motivation.” Some reported feeling overwhelmed, irritable, unmotivated, impatient, and embarrassed of struggling with memory. For some, conversation and speaking became harder: “It’s overwhelming…I get anxious about forgetting things,” and “I can’t articulate like I used to,” and “I struggle to get words out – it feels like a stutter, but it’s not a speech issue, it’s my brain not working as fast. It’s scary.” After the intervention participants stated that motivation, confidence, memory, focus, and communication skills had improved, such as “I articulate better, process information faster, and stay calm under pressure.” One participant described improved social interactions saying, “I retain conversations better, I hear and understand people again…this training has been life-changing.” Other participants also claimed improved emotional and psychosocial functioning such as, “I have better self-control in interactions,” and “Now I can have a conversation despite what I’m feeling,” and “I can follow discussions better,” and “ I’m closer to my family, and I’m mentally in a better place.”
3.3.5. Work and School Cross-Case Synthesis
Across pre-intervention interviews, all 8 participants who completed the interviews described substantial challenges with their ability to perform at work or school. They reported difficulties with brain fog, reduced attention span, slow verbal processing, reading comprehension struggles, challenges learning and retaining new information, and memory deficits. They also reported issues with planning, prioritizing, time management, task initiation, frequent forgetfulness, follow-through, and even safety. Several described how exhaustion limited their ability to go to work or school or sustain a full day. They reported emotional struggles that impacted their confidence and abilities in work or school. After the intervention, participants described significant improvements in these areas. Table 4 presents this cross-case synthesis in work and school subthemes from pre-intervention to post-intervention.
3.4. Secondary Outcome: IQ Score Results
The secondary outcome measure for the current study was change in overall cognitive function as measured by the Woodcock Johnson IV Tests of Cognitive Abilities. Seven subtests were administered at baseline and again at the end of cognitive training in order to determine change in the participant’s overall General Intellectual Ability (GIA) score. Pretest standard scores ranged from 87 to 114 and post-test standard scores ranged from 99 to 117. Using a paired samples t test on pretest and post-test GIA scores, results revealed a statistically significant improvement from pretest (M = 99.5, SD = 10.15) to post-test (M = 110.0, SD = 7.57; t = -5.42, p < .001, d = 1.9) with a mean change of 10.5 points and a large effect size. Figure 2 illustrates the pretest and post-test range of scores.
4. Discussion
We conducted a prospective, single-arm, proof-of-concept interventional study to evaluate pre-post changes in workplace self-efficacy and cognitive performance following a clinically and commercially available, adaptive, severity-tailored cognitive intervention in adults with post-COVID brain fog. Prior research on the relevance of cognitive rehabilitation for post-covid cognitive dysfunction stressed the importance of remediating deficits impacting daily life [21]. Unfortunately, and to our knowledge, current treatments have not led to pre-Covid levels of recovery. Our study tested a cognitive training methodology which had previously shown both statistically significant and clinically significant improvements in cognitive and daily functioning for populations with TBI, age-related cognitive decline, ADHD, and learning disabilities [27,28,29,30,31,32,33,34]. Therefore, our goal was to examine the applicability of the same methodology to this population as well.
We chose a mixed-methods approach to this pilot examination to assess both quantitative change in overall workplace self-efficacy and cognition but also to capture detailed examples of the perceived changes in those same constructs elucidated by the participants. This approach produced rich data enabling us to identify clear patterns in the participants’ perceptions of change that were consistent with the changes in their overall cognitive abilities operationalized by their IQ scores.
The primary outcome of our study was workplace self-efficacy. Our analysis of the Workplace Self-Efficacy Survey indicated statistically significant change from pre-Covid to post-Covid and again from pre-intervention (after getting Covid) to post-intervention in overall workplace self-efficacy, perceived work performance, perceived cognitive functioning, and perceived functioning at home. As hoped, there were no statistically significant differences between the pre-Covid ratings on those measures and the post-intervention ratings on those measures which suggests a return to pre-Covid levels of functioning.
We wanted to explore specific examples of each participant’s experience, struggles, and recovery in those areas through in-depth intake and exit interviews. As described in the methods section, we used the Workplace Self-Efficacy Survey items as our interview guide. Our thematic analysis of the interview data revealed 5 main themes: executive function, health and energy, daily living activities, productivity, and socioemotional functioning. We also drilled down on the subthemes related to work and school in a cross-case synthesis of pre-intervention struggles and post-intervention improvements. The analysis of that data revealed six subthemes including cognitive processing and comprehension difficulties, memory problems impacting work or school, executive dysfunction in work or school tasks, fatigue that limited performance at work or school, emotional distress and loss of confidence in work or academics, and actual work or academic performance impairments or disruption. We noted that nearly all participants who reported struggles in these areas also reported improvement in these areas following the cognitive training intervention. This was consistent with our team’s prior research and with a doctoral study on adult self-efficacy by Highland (2019) whose participants reports improvements in workplace self-efficacy, achievement, leaderships, emotional control, and problem-solving ability after completing cognitive training with this methodology[42].
Further, we also administered seven subtests from a standardized cognitive skills assessment, the Woodcock Johnson IV Tests of Cognitive Abilities, to generate an overall IQ score called General Intellectual Ability, or GIA, on this test battery. Because self-reported functioning is frequently dismissed as less reliable than objective tests, we opted to add this testing to supplement our workplace self-efficacy data. Consistent with all prior research conducted by our team on this cognitive training methodology, the pretest to post-test changes in IQ score were statistically significant with a very large effect size. And although studies on other types of cognitive rehabilitation programs for post-Covid cognitive dysfunction have reported significant improvement in individual cognitive constructs such as processing speed, executive function, and visual processing, this is the first study to our knowledge that documented significant change on a traditional and widely-accepted IQ test that weights the performance across multiple cognitive constructs: working memory, long-term memory, visual processing, auditory processing, processing speed, fluid reasoning, and comprehension knowledge. We note the significant change in overall IQ score is not surprising in light of the significant change in self-reported cognitive functioning on the survey as well. Further, the comments made by participants in their post-intervention interviews are also consistent with these quantitative changes. Comments such as “My attention to detail, short term memory, and ability to not get distracted in loud environments is the best I can remember since before Covid” certainly align with these findings.
A key strength of this study is its ecological validity and clinical implications. Although this was a lengthy intervention, ranging from 45 to 90 training hours over 5 to 15 months depending on the number of training sessions needed, all participants indicated the effort and time commitment had been worth it, and all but one expressed an interest to continue cognitive training past the study period. The human aspect of this intervention enables the adaptability and flexibility of the methodology without compromising the integrity or consistency of the intervention delivery. Because trainers match the intensity, complexity, and length of the program to the individual’s deficits and strengths, frustration tolerance, willingness to engage, and their work and home schedules, they were able to keep participants in the study motivated with momentum. This practice of dynamic assessment and adaptation mirrors the practices of cognitive trainers in the LearningRx cognitive training centers where this program is delivered. Thus, the adaptive and flexible nature of the intervention delivery in the study was ecologically valid and was informed by the years of prior practice in this program delivery. In fact, the trainers in the study were actual trainers at LearningRx centers. Thus, the clinical implications of this study are encouraging. The methodology is already in widespread use both in centers and remotely anywhere in the world. This study adds to the literature on the potential applicability to this population as well.
This pilot study does have a couple of limitations and implications for future research. First, the small sample size was a function of both grant funding limits but also the importance of examining the intervention’s potential with this population using such in-depth methods. However, the sample size certainly limits generalizability. Future research should be conducted on a larger sample. Additionally, this study’s design did not include a control group which limits any causal conclusions that can be made. However, the results were consistent with prior controlled trials on this methodology which does situate the interpretation of our results within the wider body of literature on this intervention. Yet, future research should include a control group to account for the counterfactual.
5. Conclusions
This pilot study supports the applicability of the Brain Strong cognitive training program for individuals with post-Covid cognitive dysfunction and the trickle-down effect on work and school performance. The study demonstrated significant improvements in workplace self-efficacy and cognition for the participants and serves as a justification for future randomized controlled trials with this population. This study adds to the growing body of literature examining how cognitive training and cognitive rehabilitation for post-Covid cognitive sequalae may be important for restoring not only cognitive function but also workplace performance impacted by Covid and other viral illnesses.
Author Contributions
Conceptualization, J.P., C.L.; methodology, J.P., C.L., A.M.; formal analysis, A.M.; investigation, C.L., A.M., E.J.; resources, A.M., E.J.; data curation, A.M., E.J.; writing—original draft preparation, C.L., A.M.; writing—review and editing, C.L., A.M., E.J., J.P.; supervision, J.P., C.L.; validation, A.M., visualization, A.M.; project administration, C.L.; funding acquisition, J.P., C.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Louisiana State University Health Sciences Center Shreveport Research Council Intramural Grants Program, specifically the Center for Brain Health (CBH) Grant-in-Aid Award. .
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Louisiana State University Health Sciences Center Shreveport (IRB Study00001896; original approval July 11, 2022).:
Informed Consent Statement
Written Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Dataset available on request from the authors.
Acknowledgments
We’d like to thank Teri Miller, MS for her contribution to the qualitative thematic analysis.
Conflicts of Interest
The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results. The authors declare the following COI: J.P. has no conflict of interest to declare. C.L. sits on the Scientific Advisory Board for the intervention used in the study but receives no renumeration for that role or in the outcome of the study. A.M. and E.J. are employed by the research institute founded by the creator of the intervention used in the study.
Abbreviations
The following abbreviations are used in this manuscript:
| ADLs | Activities of Daily Living |
| IADLs | Instrumental Activities of Daily Living |
| WJIV | Woodcock Johnson IV Tests of Cognitive Abilities |
| GIA | General Intellectual Ability |
| IQ | Intelligence Quotient |
| WSES | Workplace Self-Efficacy Survey |
Appendix A
Appendix A.1. Questions on Workplace Self-Efficacy Surveys
Workplace Self-Efficacy Survey Questions
1 being “Poor” and 10 being “Excellent”
1. Ability to maintain your personal hygiene and appearance standards
2. Ability to maintain home order or neatness
3. Ability to maintain workspace order or neatness
4. Ability to balance home and work responsibilities
5. Ability to manage time
6. Ability to make it to work on time
7. Ability to work required hours
8. Ability to plan and prioritize
9. Ability to complete simple tasks
10. Ability to accomplish larger goals
11. Problem solving ability
12. Ability to gain needed knowledge and skills
13. Initiative
14. Productivity
15. Work quality
16. Work accuracy
17. Dependability at work
18. Attention and focus
19. Patience and tolerance
20. Writing ability
21. Ability to orally communicate to peers
22. Ability to communicate to peers in writing
23. Ability to orally communicate to customers/clients
24. Ability to communicate to customers/clients in writing
25. Speed of processing verbal information
26. Speed of processing visual information
27. Speed of processing written information
28. Short-term memory
29. Long-term memory
Scoring
Category 1: Work Performance (Items 3, 5, 6, 7-17, 19-24)
Category 2: Cognitive Function (Items 18, 25-29)
Category 3: Home Function (Items 1, 2, 4)
Total Workplace Self-Efficacy Score = Category 1 + Category 2
References
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-Acute COVID-19 Syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef]
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: Major Findings, Mechanisms and Recommendations. Nat. Rev. Microbiol. 2023, 21, 133–146. [Google Scholar] [CrossRef] [PubMed]
- Proal, A.D.; VanElzakker, M.B. Long COVID or Post-Acute Sequelae of COVID-19 (PASC): An Overview of Biological Factors That May Contribute to Persistent Symptoms. Front. Microbiol. 2021, 12, 698169. [Google Scholar] [CrossRef]
- Choutka, J.; Jansari, V.; Hornig, M.; Iwasaki, A. Unexplained Post-Acute Infection Syndromes. Nat. Med. 2022, 28, 911–923. [Google Scholar] [CrossRef]
- Meinhardt, J.; Radke, J.; Dittmayer, C.; Franz, J.; Thomas, C.; Mothes, R.; Laue, M.; Schneider, J.; Brünink, S.; Greuel, S.; et al. Olfactory Transmucosal SARS-CoV-2 Invasion as a Port of Central Nervous System Entry in Individuals with COVID-19. Nat. Neurosci. 2021, 24, 168–175. [Google Scholar] [CrossRef]
- Greene, C.; Connolly, R.; Brennan, D.; Laffan, A.; O’Keeffe, E.; Zaporojan, L.; O’Callaghan, J.; Thomson, B.; Connolly, E.; Argue, R.; et al. Blood–Brain Barrier Disruption and Sustained Systemic Inflammation in Individuals with Long COVID-Associated Cognitive Impairment. Nat. Neurosci. 2024, 27, 421–432. [Google Scholar] [CrossRef] [PubMed]
- Andrews, M.G.; Mukhtar, T.; Eze, U.C.; Simoneau, C.R.; Ross, J.; Parikshak, N.; Wang, S.; Zhou, L.; Koontz, M.; Velmeshev, D.; et al. Tropism of SARS-CoV-2 for Human Cortical Astrocytes. Proc. Natl. Acad. Sci. 2022, 119, e2122236119. [Google Scholar] [CrossRef] [PubMed]
- Crunfli, F.; Carregari, V.C.; Veras, F.P.; Silva, L.S.; Nogueira, M.H.; Antunes, A.S.L.M.; Vendramini, P.H.; Valença, A.G.F.; Brandão-Teles, C.; Zuccoli, G.D.S.; et al. Morphological, Cellular, and Molecular Basis of Brain Infection in COVID-19 Patients. Proc. Natl. Acad. Sci. 2022, 119, e2200960119. [Google Scholar] [CrossRef]
- Huang, S.; Fishell, G. SARS-CoV-2, Astrocytes Are in It for the Long Haul. Proc. Natl. Acad. Sci. 2022, 119, e2209130119. [Google Scholar] [CrossRef]
- Fernández-Castañeda, A.; Lu, P.; Geraghty, A.C.; Song, E.; Lee, M.-H.; Wood, J.; O’Dea, M.R.; Dutton, S.; Shamardani, K.; Nwangwu, K.; et al. Mild Respiratory COVID Can Cause Multi-Lineage Neural Cell and Myelin Dysregulation. Cell 2022, 185, 2452–2468.e16. [Google Scholar] [CrossRef]
- Douaud, G.; Lee, S.; Alfaro-Almagro, F.; Arthofer, C.; Wang, C.; McCarthy, P.; Lange, F.; Andersson, J.L.R.; Griffanti, L.; Duff, E.; et al. SARS-CoV-2 Is Associated with Changes in Brain Structure in UK Biobank. Nature 2022, 604, 697–707. [Google Scholar] [CrossRef]
- Boldrini, M.; Canoll, P.D.; Klein, R.S. How COVID-19 Affects the Brain. JAMA Psychiatry 2021, 78, 682. [Google Scholar] [CrossRef]
- Yong, S.J. Persistent Brainstem Dysfunction in Long-COVID: A Hypothesis. ACS Chem. Neurosci. 2021, 12, 573–580. [Google Scholar] [CrossRef]
- Monje, M.; Iwasaki, A. The Neurobiology of Long COVID. Neuron 2022, 110, 3484–3496. [Google Scholar] [CrossRef]
- Fujimoto, Y.; Abe, H.; Eiro, T.; Tsugawa, S.; Tanaka, M.; Hatano, M.; Nakajima, W.; Ichijo, S.; Arisawa, T.; Takada, Y.; et al. Systemic Increase of AMPA Receptors Associated with Cognitive Impairment of Long COVID. Brain Commun. 2025, 7, fcaf337. [Google Scholar] [CrossRef]
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re’em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing Long COVID in an International Cohort: 7 Months of Symptoms and Their Impact. eClinicalMedicine 2021, 38, 101019. [Google Scholar] [CrossRef]
- Al-Aly, Z.; Xie, Y.; Bowe, B. High-Dimensional Characterization of Post-Acute Sequelae of COVID-19. Nature 2021, 594, 259–264. [Google Scholar] [CrossRef]
- Graham, E.L.; Clark, J.R.; Orban, Z.S.; Lim, P.H.; Szymanski, A.L.; Taylor, C.; DiBiase, R.M.; Jia, D.T.; Balabanov, R.; Ho, S.U.; et al. Persistent Neurologic Symptoms and Cognitive Dysfunction in Non-hospitalized Covid-19 Long Haulers. Ann. Clin. Transl. Neurol. 2021, 8, 1073–1085. [Google Scholar] [CrossRef] [PubMed]
- García-Molina, A.; García-Carmona, S.; Espiña-Bou, M.; Rodríguez-Rajo, P.; Sánchez-Carrión, R.; Enseñat-Cantallops, A. Neuropsychological Rehabilitation for Post–COVID-19 Syndrome: Results of a Clinical Programme and Six-Month Follow Up. Neurol. Engl. Ed. 2024, 39, 592–603. [Google Scholar] [CrossRef]
- Nagra, G.; Ezeugwu, V.E.; Bostick, G.P.; Branton, E.; Dennett, L.; Drake, K.; Durand-Moreau, Q.; Guptill, C.; Hall, M.; Ho, C.; et al. Return-to-Work for People Living with Long COVID: A Scoping Review of Interventions and Recommendations. PLOS One 2025, 20, e0321891. [Google Scholar] [CrossRef] [PubMed]
- Braga, L.W.; Oliveira, S.B.; Moreira, A.S.; Martins Pereira, M.E.M.D.S.; Serio, A.S.S.; Carneiro, V.D.S.; Freitas, L.D.F.P.; Souza, L.M.D.N. Long COVID Neuropsychological Follow-up: Is Cognitive Rehabilitation Relevant? NeuroRehabilitation 2023, 53, 517–534. [Google Scholar] [CrossRef]
- Weix, N.M.; Shake, H.M.; Duran Saavedra, A.F.; Clingan, H.E.; Hernandez, V.C.; Johnson, G.M.; Hansen, A.D.; Collins, D.M.; Pryor, L.E.; Kitchens, R.; et al. Cognitive Interventions and Rehabilitation to Address Long-COVID Symptoms: A Systematic Review. OTJR Occup. Ther. J. Res. 2026, 46, 74–95. [Google Scholar] [CrossRef]
- Uswatte, G.; Taub, E.; Ball, K.; Mitchell, B.S.; Blake, J.A.; McKay, S.; Biney, F.; Iosipchuk, O.; Hempfling, P.; Harris, E.; et al. Long COVID Brain Fog Treatment: An Early-Phase Randomized Controlled Trial of Constraint-Induced Cognitive Therapy Signals Go. Rehabil. Psychol. 2025. [Google Scholar] [CrossRef] [PubMed]
- Bashir, S.; Mizrahi, I.; Weaver, K.; Fregni, F.; Pascual-Leone, A. Assessment and Modulation of Neural Plasticity in Rehabilitation With Transcranial Magnetic Stimulation. PM&R 2010, 2. [Google Scholar] [CrossRef] [PubMed]
- Lampit, A.; Hallock, H.; Valenzuela, M. Computerized Cognitive Training in Cognitively Healthy Older Adults: A Systematic Review and Meta-Analysis of Effect Modifiers. PLoS Med. 2014, 11, e1001756. [Google Scholar] [CrossRef]
- Gavelin, H.M.; Domellöf, M.E.; Leung, I.; Neely, A.S.; Launder, N.H.; Nategh, L.; Finke, C.; Lampit, A. Computerized Cognitive Training in Parkinson’s Disease: A Systematic Review and Meta-Analysis. Ageing Res. Rev. 2022, 80, 101671. [Google Scholar] [CrossRef]
- Ledbetter, C.; Moore, A.L.; Mitchell, T. Cognitive Effects of ThinkRx Cognitive Rehabilitation Training for Eleven Soldiers with Brain Injury: A Retrospective Chart Review. Front. Psychol. 2017, 8, 825. [Google Scholar] [CrossRef]
- Moore, A.L.; Carpenter, D.M.; James, R.L.; Miller, T.M.; Moore, J.J.; Disbrow, E.A.; Ledbetter, C.R. Neuroimaging and Neuropsychological Outcomes Following Clinician-Delivered Cognitive Training for Six Patients With Mild Brain Injury: A Multiple Case Study. Front. Hum. Neurosci. 2020, 14, 229. [Google Scholar] [CrossRef]
- Moore, A.L.; Carpenter, D.M.; Miller, T.M.; Ledbetter, C. ThinkRx Cognitive Training for Adults over Age 50: Clinician–Caregiver Partners in Delivery as Effective as Clinician-Only Delivery. Psychol. Neurosci. 2019, 12, 291–306. [Google Scholar] [CrossRef]
- Moore, A.L.; Miller, T.M.; Ledbetter, C. Remote vs. In-Person Delivery of LearningRx One-on-One Cognitive Training During the COVID-19 Pandemic: A Non-Inferiority Study. Front. Psychol. 2021, 12, 749898. [Google Scholar] [CrossRef] [PubMed]
- James, R.; Lawson Moore, A.; Carpenter, D.M., Ii; Miller, T.M.; Ledbetter, C. Feasibility of a Functional Medicine Approach to Slowing Clinical Cognitive Decline in Patients over Age 55: A Multiple Case Study Report. OBM Integr. Complement. Med. 2019, 04, 1–36. [Google Scholar] [CrossRef]
- Moore, A.L.; Carpenter, D.M., Ii; Miller, T.M.; Ledbetter, C. Clinician-Delivered Cognitive Training for Children with Attention Problems: Effects on Cognition and Behavior from the ThinkRx Randomized Controlled Trial. Neuropsychiatr. Dis. Treat. 2018, Volume 14, 1671–1683. [Google Scholar] [CrossRef]
- Jedlicka, E.J. LearningRx Cognitive Training for Children and Adolescents Ages 5–18: Effects on Academic Skills, Behavior, and Cognition. Front. Educ. 2017, 2, 62. [Google Scholar] [CrossRef]
- Carpenter, D.M.; Ledbetter, C.; Moore, A.L. LearningRx Cognitive Training Effects in Children Ages 8–14: A Randomized Controlled Trial. Appl. Cogn. Psychol. 2016, 30, 815–826. [Google Scholar] [CrossRef]
- Onken, L.S.; Carroll, K.M.; Shoham, V.; Cuthbert, B.N.; Riddle, M. Reenvisioning Clinical Science: Unifying the Discipline to Improve the Public Health. Clin. Psychol. Sci. 2014, 2, 22–34. [Google Scholar] [CrossRef] [PubMed]
- Eldridge, S.M.; Chan, C.L.; Campbell, M.J.; Bond, C.M.; Hopewell, S.; Thabane, L.; Lancaster, G.A. CONSORT 2010 Statement: Extension to Randomised Pilot and Feasibility Trials. BMJ 2016, i5239. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research Electronic Data Capture (REDCap)—A Metadata-Driven Methodology and Workflow Process for Providing Translational Research Informatics Support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap Consortium: Building an International Community of Software Platform Partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Schrank, F.; McGrew, K.; Mather, N. Woodcock–Johnson IV Tests of Cognitive Abilities, 4th ed.; Riverside: Rolling Meadows, IL.
- McGrew, K.; LaForte, E.; Schrank, F. Woodcock–Johnson IV Technical Manual, 4th ed.; Riverside: Rolling Meadows, IL, 2014. [Google Scholar]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Highland, S. Examining the Self-Efficacy Perceptions of Adults Who Completed a ThinkRx One-on-One Brain Training Program. Doctoral dissertation, Grand Canyon University, Phoenix, AZ, 2019. [Google Scholar]
Figure 1.
Example of a memory task from the Brain Strong program.
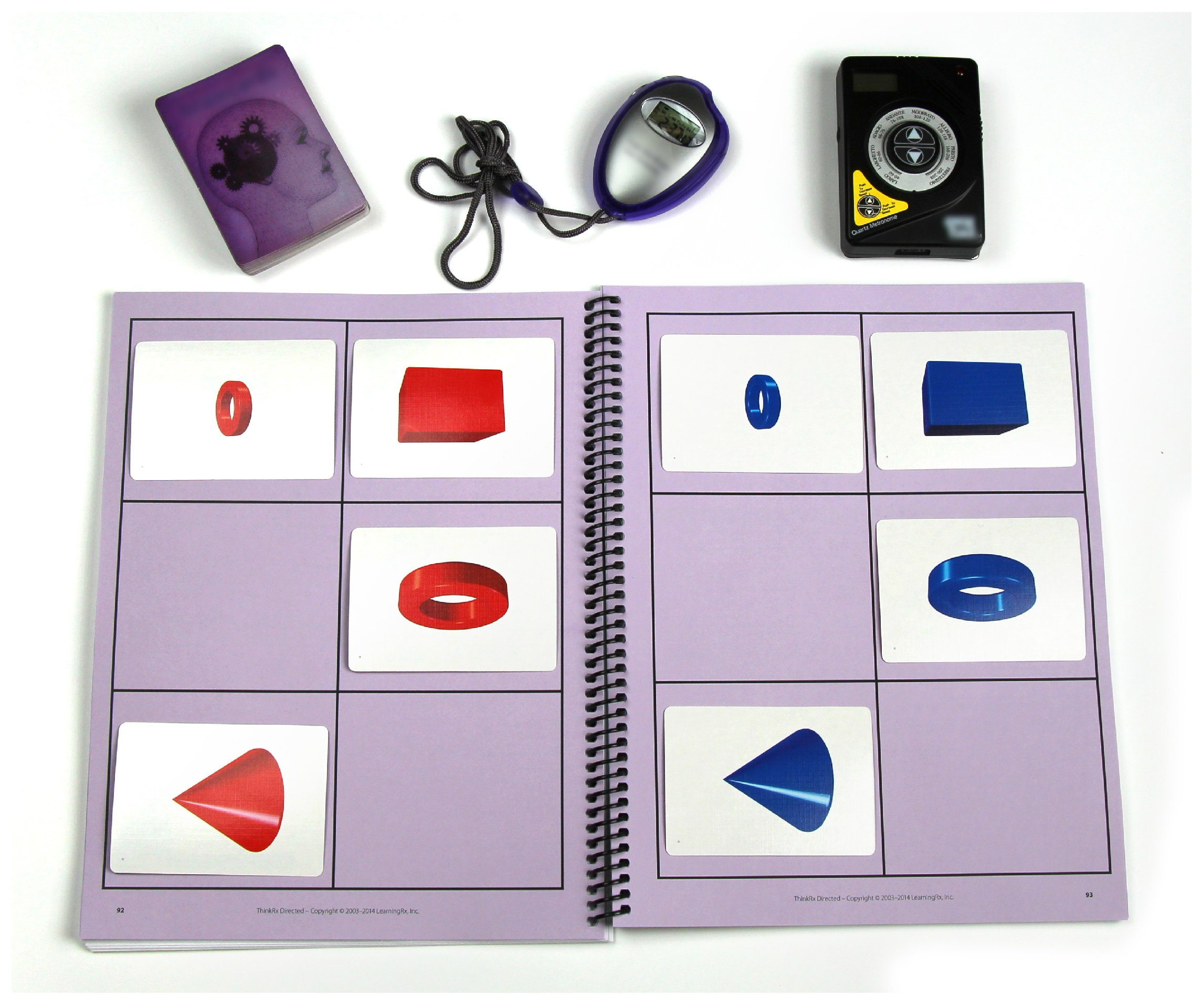
Figure 2.
Box and whisker plot of pre and post GIA scores.
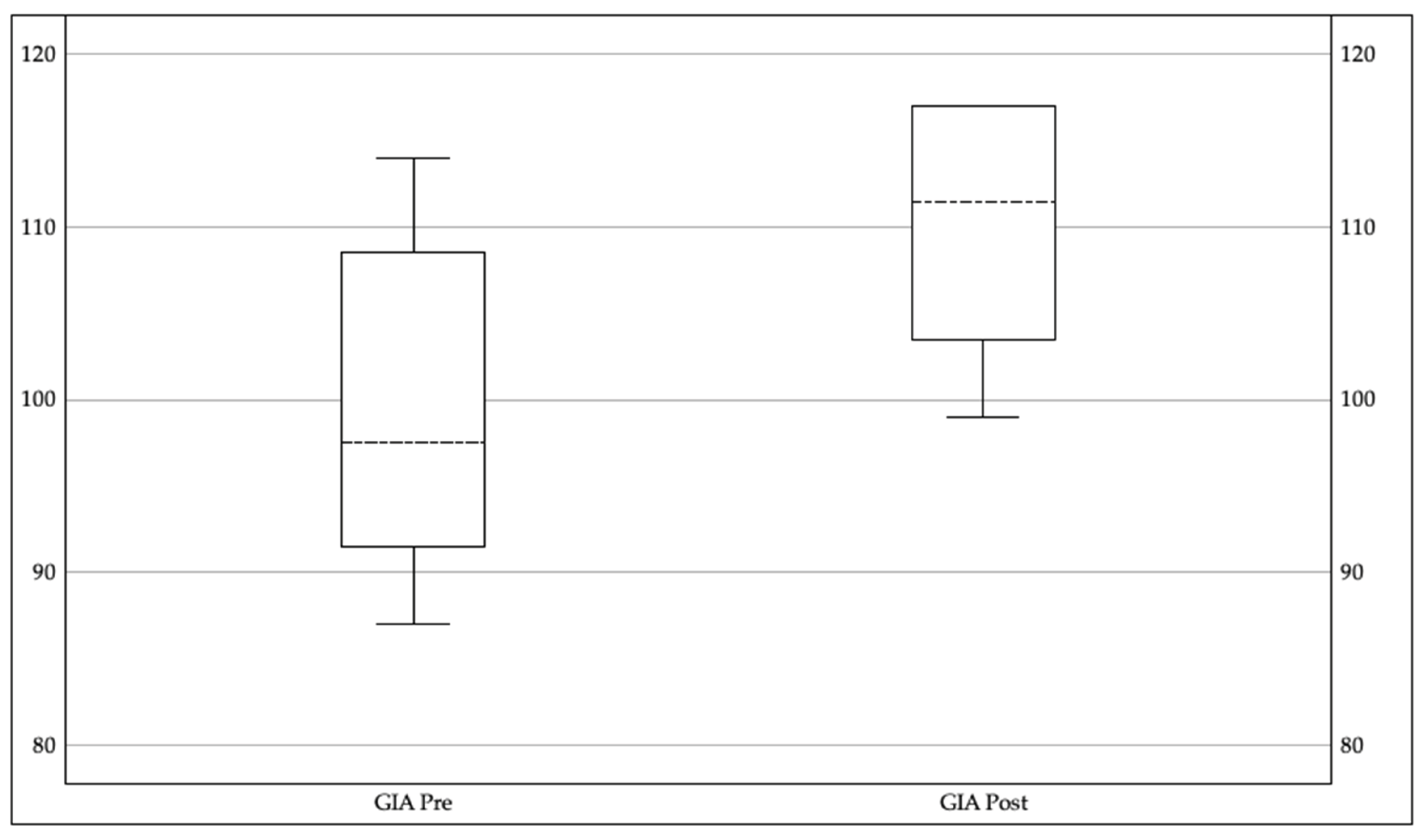

Table 1.
Training exposure parameters for individual participants, including total training hours, number of sessions, session duration, and overall training duration (months).
Table 1.
Training exposure parameters for individual participants, including total training hours, number of sessions, session duration, and overall training duration (months).
| Training Hours | Number of Sessions | Session Duration (min) | Training Months |
| 45 | 30 | 90 | 4 |
| 45 | 45 | 60 | 5 |
| 60 | 43 | 90 | 7 |
| 60 | 59 | 60 | 6 |
| 75 | 63 | 60/90 | 13 |
| 75 | 64 | 60 | 9 |
| 90 | 60 | 90 | 11 |
| 90 | 90 | 60 | 10 |
| 90 | 90 | 90 | 13 |
Table 2.
WSES scores at before COVID, after COVID/pre-intervention, and post-intervention.
| WSES Scores |
Before COVID Mean (SD) |
After COVID (Mean (SD) |
Post Intervention Mean (SD) |
Time Effect Size |
|
Workplace Self-Efficacy Score |
239.55 (4.9) | 119.66 (22.1) | 201.22 (20.6) | .69 |
|
Work Performance Rating |
177.56 (3.2) | 90.89 (16.1) | 147.11 (15.4) | .69 |
|
Cognitive Performance Rating |
62.00 (2.1) | 28.78 (6.3) | 53.11 (5.2) | .69 |
|
Home Functioning Rating |
26.89 (.93) | 13.44 (2.4) | 23.67 (2.5) | .69 |
Table 3.
Main themes of post-Covid brain fog and intervention impact (n =8).
| Theme | Percent Reporting | Examples of Impact |
| Executive Function | 100% | Attention, memory, processing speed, learning, planning, time management |
| Health and Energy | 100% | Fatigue, sleep, endurance, exercise, autonomic dysfunction |
| Daily Living Activities | 87% | Hygiene, home organization, driving, household choirs, caregiving |
| Productivity | 100% | Work hours, punctuality, performance, workload |
| Socioemotional Functioning | 100% | Confidence, emotion regulation, relationships, distress |
Table 4.
Cross-Case Synthesis of Work/School Impacts and Improvements.
| Work/School Subtheme | Examples |
Percent Reporting Difficulty Pre-Intervention |
Percent Reporting Improvements Post-Intervention |
| Cognitive processing and comprehension difficulties |
Difficulty learning new information, trouble comprehending written material, reduced attention span, slow verbal processing | 100% | 100% |
| Memory problems impacting work or school |
Short-term memory lapses, forgetting tasks or appointments, needing extensive lists, difficulty retaining information | 100% | 88% |
| Executive dysfunction in work/school tasks | Procrastination, difficulty initiating or completing tasks, disorganization, poor time management, impaired planning and prioritizing | 100% | 100% |
| Fatigue limits performance |
Exhaustion, mental & physical fatigue, limited ability to stay at work/school a full day |
75% | 63% |
| Emotional distress and confidence loss in work or academics | Anxiety, depression, distress about decline, loss of confidence in ability, loss of identity at work or school roles | 88% | 88% |
| Work/academic performance impairment and disruption |
Reduced productivity or accuracy, missed deadlines, underperformance, employment loss or fear of loss | 100% | 100% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



