
Submitted:
13 February 2026
Posted:
25 February 2026
You are already at the latest version
Abstract
Hospitals play a central role in promoting health and well-being, yet they are also among the most resource-intensive institutions, contributing significantly to environmental degradation through high energy and water consumption, extensive waste generation, and reliance on single-use materials. This conceptual paper explores how principles of the circular economy and green economy can be integrated into hospital operations through a strategic Corporate Social Responsibility (CSR) framework, reframing sustainability as a strategic management issue rather than a compliance-driven activity. Drawing on environmental economics, sustainability studies, and institutional theory, the paper develops an integrated conceptual model structured around the environmental, social, and economic pillars of sustainability. Within this framework, four interconnected operational domains are identified: waste management and circular practices, energy consumption and renewable integration, sustainable procurement and circular supply chains, and economic and policy incentives. The social dimension explicitly encompasses healthcare staff and patients, addressing issues of workforce well-being, health education, safety, quality of life, and equitable care delivery. The paper also examines institutional and cultural barriers that constrain sustainability implementation and highlights the role of strategic leadership, governance, and system-wide innovation in overcoming these challenges. While not empirical, the study provides a theoretical foundation to inform future research, policy development, and strategic decision-making aimed at advancing sustainable, low-carbon, and resilient healthcare systems.
Keywords:
hospital sustainability
; circular economy
; green economy
; Corporate Social Responsibility (CSR)
; strategic CSR
; healthcare management
1. Introduction
Despite their mission to promote health and well-being, hospitals are among the most environmentally impactful institutions worldwide (Kahramanoglu et al., 2025). The global healthcare sector is estimated to account for approximately 4.4% of worldwide greenhouse gas emissions, contributing significantly to the climate crisis through energy and water consumption, supply chains, and waste production (HCWH, 2021; Mirow, Venne, & Brand, 2024). Beyond carbon emissions, hospitals are highly resource intensive, consuming large volumes of energy and water while relying heavily on disposable medical products and packaging (Lehtinen, 2022; Vanderwee et al., 2024). In addition, hospitals generate complex waste streams, including infectious materials, sharps, chemicals, pharmaceuticals, and radioactive waste. This waste burden represents not only a volume challenge but also a source of emissions and contamination risk: biomedical waste is frequently incinerated, generating air pollutants and potentially toxic emissions, while radioactive waste from nuclear medicine typically requires shielded storage until decay and, in some jurisdictions, regulated discharge of limited volumes of liquid radioactive waste into wastewater systems, raising concerns about downstream environmental contamination (HCWH, 2021; WHO, 2014). As a result, hospitals are significant contributors to environmental degradation through their intensive use of energy, water, and materials, yet sustainability research in this sector remains fragmented and unevenly developed (McGain & Naylor, 2014). This situation highlights a fundamental paradox whereby healthcare institutions promote human health while adversely affecting planetary health, underscoring the need for systemic sustainability frameworks (Ranucci, 2025).
Historically, hospitals have operated within a linear economic logic based on the extraction, consumption, and disposal of resources, with limited consideration for environmental impact or systemic efficiency (Chew et al., 2023). While this model supported convenience and short-term cost control, its ecological consequences have become increasingly unsustainable in the context of climate change and escalating waste management challenges (Wyssusek et al., 2019). In response, scholars and policymakers have increasingly turned to alternative frameworks, most notably the circular economy (CE) and the green economy (GE), as pathways for embedding sustainability into institutional design and decision-making (Loiseau et al., 2016; Heshmati, 2017). These approaches emphasize resource circularity, low-carbon infrastructure, and ecological resilience. Despite their growing prominence in policy discourse, however, their application within the healthcare sector remains underdeveloped and fragmented, both theoretically and operationally (Schwab, Schiestl, & Hasenburg, 2025).
At the same time, corporate social responsibility (CSR) has gained increasing visibility within healthcare management, particularly as public expectations of accountability and transparency have intensified (Doherty et al., 2009; Aguinis & Glavas, 2012; Buttigieg et al., 2019). Throughout this paper, we distinguish between traditional, often fragmented Corporate Social Responsibility (CSR) and Strategic CSR (S-CSR), the latter being defined as the deliberate integration of social and environmental value into the hospital’s core business strategy and operational DNA. In many hospital settings, CSR initiatives remain peripheral, driven primarily by compliance requirements, philanthropic activities, or isolated projects rather than strategic integration (Reddy & Mariyappan, 2023). Moreover, the social dimension of sustainability has become increasingly salient in healthcare, given growing workforce shortages and retention challenges, alongside rising pressure to ensure equitable access to care and fair working conditions that support quality of care and population quality of life (WHO, 2020; OECD, 2023; WHO, 2022). This paper argues that meaningful sustainability integration within hospital systems requires CSR to evolve into a strategic orientation that embeds environmental and social commitments into organizational strategy, culture, and performance logic. In this context, Strategic CSR (S-CSR) functions not only as a mechanism for sustainability implementation but also as a driver of innovation, institutional resilience, and long-term legitimacy (Porter & Kramer, 2011).
Against this background, the aim of this paper is to rethink hospital sustainability through the conceptual integration of four theoretical pillars: the circular economy, the green economy, strategic corporate social responsibility, and institutional theory. These pillars form the foundational architecture of the proposed model. Consistent with the established environmental, social, and economic pillars of sustainability, the circular and green economy perspectives primarily reinforce the environmental and economic dimensions through resource efficiency, decarbonization, and value creation, while strategic CSR foregrounds the social dimension, including workforce well-being, equity, and community value. Institutional theory provides the explanatory lens for understanding how these principles can be embedded and sustained through governance structures, norms, and regulatory and cultural pressures within hospital systems.
To enhance practical relevance, the paper further incorporates two operational extensions derived from these theoretical pillars. The first concerns institutional barriers to sustainability, which explains why hospitals often struggle to implement sustainability initiatives despite growing awareness and policy pressure. The second focuses on emerging digital enablers, which provide the technological pathways for operationalizing CE, GE, and S-CSR principles within complex hospital environments.
By integrating these four theoretical pillars with their operational extensions, the paper develops a multi-layered framework that links strategic sustainability principles to actionable implementation pathways in hospital systems. The core contribution lies in articulating a conceptual model that connects sustainability thinking to hospital management practices across four interrelated operational domains: waste management and circular practices; energy consumption and renewable integration; sustainable procurement and circular supply chains; and economic and policy incentives. These domains are examined not as isolated functions but as interdependent components of a broader strategic transformation. By mapping how each domain aligns with circular and green economy principles and how strategic CSR operates as the integrative managerial mechanism, the paper offers a framework for embedding sustainability into healthcare operations at scale.
Ultimately, this work contributes to the growing body of conceptual literature that reframes sustainability as a matter of strategic management and institutional change. It aims to stimulate critical discussion, inform future empirical research, and support hospital administrators and policymakers in treating sustainability not as an external obligation, but as a central principle of organizational performance, ethical leadership, and long-term resilience.
2. Theoretical Background
The conceptual framework of this paper is built on four primary theoretical pillars: the circular economy (CE), the green economy (GE), strategic corporate social responsibility (S-CSR), and institutional theory.
In the hospital sustainability context, two cross-cutting themes are emphasized in the theoretical background. First, institutional barriers to sustainability specify how cultural norms, regulatory requirements, and organizational structures can constrain change, shaping the social and governance conditions under which sustainability initiatives succeed or fail. Second, digital enablers capture the socio-technical capabilities (e.g., data infrastructure, monitoring, decision support and coordination tools) that operationalize circular economy, green economy and strategic CSR principles in day-to-day practice. Together, these four pillars and their two operational extensions form a coherent and multi-dimensional conceptual foundation for reimagining hospital sustainability. These concepts provide the operational lenses through which hospital sustainability can be reimagined. Each offers a unique entry point – ranging from resource flows and ecological impact to governance, stakeholder accountability, and long-term institutional resilience. Defining and contextualizing these concepts is fundamental to establishing the theoretical coherence of the proposed sustainability framework for hospital management.
At the core of this discussion there are two interdependent models for sustainable operations: the Circular Economy (CE) and the Green Economy (GE), which will be explored in more detail in the sections below.
2.1. Circular Economy (CE) in Healthcare: A Regenerative Model
The circular economy (CE), as defined by the Ellen MacArthur Foundation (2013), promotes a regenerative, closed-loop system designed to keep products, components, and materials in use for as long as possible (Kara et al., 2022). Unlike the prevailing linear model of extraction, production, consumption, and disposal, CE aims to minimize waste and reduce ecological harm through long-lasting design and resource efficiency, achieved by slowing, closing, and narrowing material and energy loops (Geissdoerfer et al., 2017). In hospital settings, these goals depend not only on technologies and product redesign but also on behavioral and procedural levers, including staff and patient education, clear protocols, and interoperable hospital information systems that reduce avoidable duplication (e.g., repeated laboratory tests or low-value imaging) and improve resource stewardship (Stewart et al., 2010). Beyond environmental gains, reducing unnecessary investigations can generate patient-safety co-benefits by limiting avoidable exposures and risks, including the use of contrast media in optimized volumes and only when it is clinically justified. In hospital settings, CE directly challenges the traditional “disposable culture” characterized by single-use medical products and high material throughput. Embracing circularity requires a systemic re-evaluation of supply chains and protocols by: (i) redesigning systems to incorporate reusable surgical tools and modular equipment (Bocken et al., 2016); (ii) optimizing waste segregation and reprocessing to maximize material recovery, moving beyond traditional, low-yield recycling efforts (WHO, 2022); (iii) collaborating with suppliers to implement circular product life cycles for medical devices (Sepetis & Parlavantzas, 2025); and (iv) leveraging technological advances in diagnostic services, particularly medical imaging, to reduce material and energy intensity through AI-enabled protocol optimization (e.g., lowering contrast volumes where clinically appropriate) and improved equipment energy management (e.g., automated power-down/standby modes) (Roletto et al., 2024; Ribeiro et al., 2025).By focusing on resource flow and maximizing material value, the CE offers a structural approach to sustainability that reduces material throughput and environmental impact without compromising the quality of patient care.
For hospital leadership and operational managers (ranging from executive teams to clinical and nursing administrators) embracing circularity requires a systemic re-evaluation of supply chains, infrastructure, and day-to-day protocols through the lens of long-term sustainability (Sepetis & Parlavantzas, 2025).
2.2. The Transition to the Green Economy (GE) and Sustainable Healthcare
While CE addresses material and waste flows, GE focuses on the financial and investment strategies required to drive this change. The integration of CE principles must be financially viable, which is where GE provides the economic lens for investing in clean energy, green infrastructure, and sustainable procurement that ultimately reduces operational costs and fosters long-term financial resilience.
The GE is defined as an economic system that promotes environmentally sustainable, socially inclusive, and economically viable development through principles of low carbon emissions and resource efficiency (UNEP, 2011; Foster, 2011). The GE ensures that sustainability is not treated merely as a cost centre but as a driver of economic growth and long-term financial resilience. It is built on principles of low carbon emissions, resource efficiency, and social equity (Foster, 2011). While CE focuses on resource loops, GE encompasses broader structural transitions, including renewable energy adoption, green infrastructure, and eco-innovation in service delivery. Within healthcare, GE calls for hospitals to transition to low-carbon building systems, implement energy-saving technologies (including equipment-level energy management such as switching imaging systems to standby or powering down when in standby), and adopting green procurement practices that reduce the environmental footprint of care delivery (Stevenson et al., 2013; Roletto et al., 2024; Rockall et al., 2025).Applied to hospitals, this would mean shifting towards energy-efficient infrastructure, low-carbon procurement policies, and sustainable resource management. Hospitals that embrace GE principles could integrate renewable energy sources, such as solar and geothermal power, to reduce their carbon footprint while lowering operational costs (Reddy et al., 2024). Additionally, the implementation of eco-friendly hospital designs, including smart energy systems and passive cooling techniques, could further reduce hospitals’ reliance on fossil fuels and excessive resource consumption (Dion et al., 2023). These priorities are also increasingly salient in high-energy clinical areas such as medical imaging, where departmental energy consumption and associated emissions have been documented as significant and where professional bodies have called for operational and technological measures to reduce radiology’s footprint (Roletto et al., 2024; Rockall et al., 2025). Importantly, GE implementation in hospitals is not only technical but also social: it depends on staff and patient education, changes in everyday practices, and mobility initiatives (e.g., telework where feasible, car-pooling, and travel-demand management) that can reduce congestion and transport-related emissions. GE-aligned resource stewardship can also extend to pollution prevention, for example by addressing pharmaceutical and imaging-related contaminants such as contrast agent residuals in wastewater (Zanardo et al., 2023). More broadly, GE principles support system-level redesign, including decentralization of appropriate services into community hubs to improve access and redistribute resources while reducing unnecessary travel and pressure on central hospital sites. System-level redesign should, therefore, be framed not only as a logistical efficiency but as a strategic move toward more equitable and sustainable public value creation. This transition reduces the environmental burden of patient travel while simultaneously increasing the accessibility and resilience of the health system, bridging the gap between clinical excellence and social responsibility. From a strategic management perspective, embracing GE principles represents a fundamental shift towards ethical governance and viewing environmental responsibility as a source of long-term institutional value creation. To ensure these economic and environmental goals translate into broader institutional benefits and stakeholder acceptance, they must be formally integrated into the hospital’s mandate through the framework of S-CSR. Having established the theoretical pillars of CE and GE, the following section articulates how S-CSR acts as the essential management framework required to synthesize these principles into hospital operations.
2.3. Strategic Corporate Social Responsibility
Corporate Social Responsibility (CSR) is broadly defined as an organization’s responsibility for the social and environmental impacts of its activities, particularly as they affect stakeholders such as employees, communities, regulators, and the environment (Aguinis & Glavas, 2012, Tomaselli et al., 2018). Rooted in ethical and stakeholder theory, CSR reflects the expectation that organizations contribute positively to society while minimizing negative externalities. In the healthcare context, CSR takes on added significance: hospitals serve not only as care providers but also as major employers, resource consumers, and environmental actors. CSR commitments in hospitals often include environmental stewardship (e.g., reducing emissions and waste), equitable access to healthcare, ethical labor practices, and community well-being initiatives (Doherty et al., 2009).
However, traditional CSR in healthcare has often been peripheral and focused on compliance, public relations, or philanthropic activities, rather than integrated into the strategic core of hospital operations. This reactive or voluntary model, while valuable, falls short in addressing the structural and systemic sustainability challenges facing hospitals today.
To address this gap, Strategic CSR (S-CSR) has emerged as an evolution of CSR theory and practice. S-CSR refers to the deliberate integration of social and environmental goals into an organization’s core strategy, governance, and operational models (Porter & Kramer, 2011). It is based on the premise that addressing societal challenges, such as environmental degradation, health equity, and resource scarcity, can create shared value for both society and the institution itself (Husted & Allen, 2007; Carroll & Shabana, 2010). Hence, CSR becomes a source of long-term competitive advantage, not just reputational benefit (Tomaselli & Melia, 2014; Tomaselli et al., 2016).
This progression from general CSR to strategic CSR (S-CSR) is particularly relevant in the healthcare sector, where hospitals face increasing expectations to balance patient care and service/efficiency with environmental sustainability and fiscal responsibility (Jamali, 2007; Smith et al., 2013). S-CSR reframes sustainability not as an external obligation but as a source of competitive advantage, driving innovation, operational efficiency, and institutional legitimacy (Husted & Allen, 2007; Porter & Kramer, 2011). For hospitals, this involves embedding sustainability into core operational areas such as: procurement policies, prioritizing reusable, low-impact products and strengthening supplier relationships for continuity of supply (Duque-Uribe et al., 2019; Klein, 2015); infrastructure design, adopting green buildings and energy-efficient systems (Dion et al., 2023); risk mitigation, building resilience to energy shocks, climate-related disruptions and supply constraints associated with critical raw materials and essential health products (Schmidt & Bohnet-Joschko, 2022; WHO, 2023); as well as leadership development, training executives in sustainability governance and environmental ethics (Aguinis & Glavas, 2012; Basu & Palazzo, 2008). These strategic priorities are further amplified by structural pressures facing health systems, including workforce shortages and rising demand from ageing and growing populations, alongside vulnerabilities in global production networks that can affect access to essential medicines and, in specialized services such as nuclear medicine, time-sensitive radiotracers with limited manufacturing capacity (OECD, 2023; WHO, 2023).Therefore, moving from CSR to Strategic CSR (S-CSR) marks a shift from “doing good” to “doing well by doing good” (Porter & Kramer, 2011). It reflects a broader redefinition of social responsibility, not as peripheral altruism but as a core element of institutional strategy and value creation (Husted & Allen, 2007; Jamali, 2007). Within this logic, hospitals are positioned as transformative agents capable of aligning ethical commitments with organizational performance, effectively bridging the gap between moral responsibility and managerial decision-making (Basu & Palazzo, 2008; Aguinis & Glavas, 2012). This repositioning underscores how sustainability, when embedded strategically, can simultaneously serve environmental stewardship, public health, and long-term organizational resilience (Jeyarajasekar et al, 2025).
2.4. Integrating the Models
While each of the models discussed in the previous sub-sections, Circular Economy (CE), Green Economy (GE), and Strategic Corporate Social Responsibility (S-CSR), emerges from distinct disciplinary domains such as environmental economics, sustainability science, and organizational theory, they intersect in critical and complementary ways within the healthcare context. Their convergence offers a robust, multi-layered conceptual architecture for rethinking hospital sustainability which brings together systems innovation, ecological ethics, and strategic governance.
The circular economy, grounded in industrial ecology and ecological economics, provides a practical framework for optimizing material and process flows. It promotes waste prevention, closed-loop systems, and life cycle thinking (Geissdoerfer et al., 2017; Kirchherr et al., 2018). In hospitals, this translates not only into reusing medical equipment where clinically safe, designing modular infrastructure, and collaborating with suppliers for sustainable product design, but also into closing operational loops across utilities and consumables. Examples include the reuse of treated wastewater for non-potable applications, the safe redistribution of unopened and properly labelled pharmaceuticals within appropriate regulatory and quality assurance frameworks, and the recovery and recycling of laboratory solvents following suitable treatment, enhancing resource efficiency without compromising care quality (Bocken et al., 2016; WHO, 2014). Circular practices can also extend to clinical process optimization, for instance by reducing material inputs in diagnostic pathways and using lower volumes of contrast media in imaging when clinically appropriate (Zanardo et al., 2023; Rockall et al., 2025).Building on this, the green economy extends the logic of sustainability beyond materials to encompass infrastructure, energy systems, and broader institutional frameworks. It emphasizes decarbonization, ecological regeneration, and social equity within economic development (Barbier, 2011; UNEP, 2011). Applied to healthcare, GE principles encourage low-carbon hospital design, energy-efficient operations, and integration of renewable energy and thereby aligning clinical excellence with environmental and financial performance (Stevenson et al., 2013).
Rather than being a separate pillar, S-CSR is positioned here as a managerial synthesis, a function of CE and GE principles embedded into organizational strategy. It translates the operational logic of CE and the systemic ambitions of GE into institutional commitment, accountability, and long-term performance (Porter & Kramer, 2011; Husted & Allen, 2007). CSR introduces the normative foundation emphasizing hospitals’ duties not just to patients and regulators, but also to communities, workers, suppliers, and the environment (Aguinis & Glavas, 2012; Matten & Moon, 2008). Yet it is S-CSR that elevates these obligations from principle to practice by integrating them into procurement systems, energy planning, executive governance, and ESG-linked performance metrics (Lyon & Maxwell, 2008; Macassa et al., 2021). In practice, this 'managerial synthesis' is exemplified when a hospital board evaluates a capital investment, such as a transition to a closed-loop medical device reprocessing system, not solely on immediate procurement costs, but through a multi-dimensional matrix. This matrix synthesizes clinical safety (S-CSR), long-term waste reduction (CE), and regional supply chain resilience (GE). Such a synthesis transforms a routine purchasing decision into a strategic act of health system governance. To effectively transition from compliance-based CSR to S-CSR, hospital leadership must treat sustainability as a core component of organizational resilience rather than an auxiliary activity. This requires the development of specific sustainability governance competencies within executive teams to overcome deep-seated bureaucratic inertia and the 'siloization' of clinical versus administrative departments. By embedding ESG-linked performance metrics into the institutional core, hospitals can transform sustainability from a 'moral cost' into a strategic driver of long-term legitimacy and operational excellence. To transition from conceptual commitment to operational reality, hospital boards must cultivate a specific set of sustainability governance competencies. These go beyond traditional healthcare administration and are summarized in Table 1 below.
By viewing S-CSR as a function of CE and GE, this paper proposes an integrated sustainability logic where ethical, operational, and systemic imperatives converge into a unified strategic direction for hospitals. This framing allows hospital administrators to shift from fragmented or compliance-driven initiatives toward a strategic sustainability agenda that reinforces both institutional legitimacy and public value. Whilst synthesizing these approaches, this model provides a multi-dimensional lens for addressing hospital sustainability, balancing environmental ethics, economic pragmatism, and institutional accountability. This integrated approach is especially crucial for hospitals, which are resource-intensive organizations operating within politically and economically complex systems. Through this combination of principles, hospitals can shift from being passive contributors to environmental harm to becoming proactive agents of sustainability, innovation, and public value creation. Although this integrated model provides a comprehensive strategic roadmap for hospitals, the operationalization of these principles is often impeded by inherent institutional barriers, namely organizational, cultural, and regulatory dynamics that resist fundamental change. In this model, institutional barriers and digital enablers are treated not as additional pillars but as operational extensions of the four foundational theoretical pillars, clarifying both the constraints and the mechanisms through which CE, GE, and S-CSR can be implemented in hospital systems.
2.5. Institutional Barriers to Sustainability
While CE, GE and S-CSR offer compelling pathways toward sustainable hospital operations, their implementation is often constrained by institutional barriers. Drawing on institutional theory, this section explores the organizational, cultural, and regulatory dynamics that shape decision-making within healthcare settings. Institutional theory suggests that hospitals often conform to external sustainability pressures primarily to gain social legitimacy. However, if these actions are not fully integrated into core operations, they risk resulting in 'greenwashing' or merely superficial compliance (DiMaggio & Powell, 1983; Marchildon et al., 2021). By reframing these pressures through a strategic management lens, hospitals can move beyond symbolic gestures toward substantive institutional change.
As an operational extension of institutional theory, the analysis of institutional barriers reveals how deeply embedded cultural, regulatory, and structural forces can prevent hospitals from adopting CE, GE and S-CSR practices. Importantly, these constraints may be amplified by geography: in small states and island settings (e.g., Malta, Cyprus or Iceland), infrastructural limits and dependence on overseas supply chains for medicines, consumables, and clinical inputs (including contrast agents) can restrict procurement choices, lengthen lead times, and increase vulnerability to shortages and overstocking, thereby creating additional waste risks and requiring context-specific “island” sustainability planning that accounts for logistics, storage capacity, and end-of-life pathways. Therefore, in small-island states, institutional barriers are compounded by extreme geographical and logistical constraints. The reliance on extended overseas supply chains necessitates a more proactive form of 'island sustainability planning' that prioritizes local storage resilience and waste-minimization protocols to mitigate the risks of both overstocking and supply-chain-induced waste. Consequently, addressing these island-specific barriers provides a rigorous 'stress test' for the universal applicability of the integrated conceptual model proposed in this paper. Strategic leadership in these contexts must focus on regional collaboration and local circular loops to ensure that resource scarcity does not compromise clinical care delivery. Hospitals are complex, risk-averse institutions embedded in highly regulated systems. As such, many sustainability initiatives face internal resistance, not because they lack merit, but because they disrupt established norms or involve upfront costs with long-term returns. Financial constraints, bureaucratic inertia, siloed departments, and rigid procurement policies often inhibit cross-functional sustainability strategies (Marchildon et al., 2021). In addition, infection prevention and control protocols, legal liabilities, and accreditation pressures can make hospital administrators wary of adopting circular practices like reusable materials or decentralized energy solutions.
Moreover, leadership turnover, lack of sustainability expertise, and short-term planning horizons further limit innovation. This institutional resistance is not unique to healthcare, but it is particularly acute in hospitals due to their dual mandate: to deliver life-critical services and to comply with strict regulatory standards. As such, even progressive sustainability models must be filtered through a lens of institutional feasibility (Badanta et al., 2025; Zurynski et al., 2023).
Understanding these institutional dynamics is essential not only for diagnosing barriers but also for effectively operationalizing the principles of CE, GE and S-CSR. The integration of these concepts must account for the cultural and systemic constraints within healthcare organizations. Without addressing institutional inertia, even well-designed sustainability frameworks risk superficial adoption or outright failure. Therefore, any roadmap for hospital sustainability must combine visionary frameworks with practical awareness of the complex institutional ecosystems in which hospitals operate. To actively overcome this institutional inertia and move beyond superficial adoption, the framework must leverage emerging digital enablers that provide the necessary data, automation, and systemic efficiency to make CE, GE, and S-CSR actionable.
2.6. Emerging Digital Enablers
The global imperative for sustainability is driving the adoption of digital technologies, such as the Internet of Things (IoT) and Artificial Intelligence (AI), as essential tools for enhancing environmental performance in energy-intensive healthcare facilities. These technologies enable improvements across operational efficiency, computational resource use, and patient logistics.
A core application is optimizing energy consumption within clinical environments. IoT sensors and smart systems are increasingly used to monitor and manage the electricity utilized by buildings and critical clinical devices, such as CT and MRI scanners. Studies indicate that a substantial percentage (ranging from 40% to 91%) of energy consumed by radiological devices is often classified as non-productive, occurring while equipment is idle (Roletto et al., 2024). Digital solutions, such as automated power management systems and informatics tools (activity trackers), address this by either automatically reducing power or alerting staff to shut down equipment during off-hours, leading to notable energy and cost savings (Büttner et al., 2021; Alshqaqeeq et al., 2020; Roletto et al., 2024). For instance, one department realized annual energy savings of 72,337 kWh by implementing an activity-tracking system to monitor and prompt the shutdown of nonproductive, energy-consuming devices (Heye et al., 2023).
Furthermore, Sustainable AI techniques enhance computational efficiency, which is critical given the high energy demands of large AI models (Alzoubi et al., 2025; Liu & Yin, 2024). Methods like Tiny Machine Learning (TinyML) compress complex models for optimized deployment on low-power edge devices, enabling real-time patient monitoring (e.g., heart rate and oxygen saturation) with minimal energy drain, making the systems sustainable for resource-constrained environments (Alzoubi et al., 2025; Wang et al., 2025; Arthi & Krishnaveni, 2024).
Also important is Virtual Consulting (telemedicine/video conferencing), which fundamentally improves logistical sustainability by eliminating the necessity of patient, carer, and staff travel (Brown et al., 2023; Pickard Strange et al., 2023). This shift to remote consultations results in significant reductions in greenhouse gas (GHG) and harmful particulate matter (PM) emissions (Brown et al., 2023; Pickard Strange et al., 2023). The application of this technology by one virtual hospital service resulted in the avoidance of over 3.1 million km of car travel in a single year, saving an estimated 533,170 kg of carbon dioxide equivalent (CO2e) (Brown et al., 2023). Complementary tools like Online Appointment Scheduling (OAS), especially when combined with automated reminders, optimize resource utilization by reducing missed appointments (“no-shows"), thereby streamlining clinical operations and improving overall system efficiency (Kammrath Betancor et al., 2025). Digital enablers function as cross-cutting mechanisms that operationalize the principles of CE, GE, and S-CSR, allowing hospitals to overcome institutional constraints and translate strategic intentions into measurable outcomes.
Therefore, digital transformation should not be viewed as a standalone technological upgrade but as a strategic facilitator. It acts as the functional layer that operationalizes the 'Managerial Synthesis' discussed in Section 2.4, providing the analytical tools necessary to manage the complex trade-offs between clinical excellence, environmental circularity, and social equity.
3. Rethinking Hospital Operations: Key Areas of Conceptual Analysis
Building on the integration of CE, GE, and S-CSR outlined in Section 2, this section translates these theoretical constructs into four key operational domains for sustainable hospital management (see Figure 1): (i) Waste Management and Circular Practices; (ii) Energy Consumption and Renewable Integration; (iii) Sustainable Procurement and Circular Supply Chains; and (iv) Economic and Policy Incentives for Sustainability.
These domains represent the primary areas where sustainability challenges and opportunities converge – offering hospitals strategic entry points to embed circularity, decarbonization, and long-term value creation. Rather than treating these areas as discrete functions, the framework positions them as interconnected expressions of the broader sustainability logic developed in the previous section (Jamali & Karam, 2018; Eckelman & Sherman, 2016). The four operational domains outlined in this section translate the four theoretical pillars, and their operational extensions of institutional barriers and digital enablers, into concrete areas of hospital practice. Crucially, these operational domains are not merely technical environmental targets; they are social imperatives. Each domain is analyzed through the lens of its impact on workforce well-being, patient safety, and community health, ensuring a balanced 'triple-bottom-line' approach that aligns with the core tenets of healthcare CSR.
Their selection is based on a synthesis of CE and GE principles, namely emphasizing resource efficiency, low-carbon transition, and closed-loop systems, combined with the strategic orientation of S-CSR, which foregrounds stakeholder accountability, institutional legitimacy, and resilience. They also correspond to critical institutional pressure points where sustainability efforts are often constrained by regulatory inertia, fiscal limits, or organizational silos (DiMaggio & Powell, 1983; Marchildon et al., 2021). The derivation of these specific operational domains is rooted in the functional intersections of the theoretical framework. The first domain, Waste Management and Circular Practices, is the direct operationalization of the CE-S-CSR intersection. It moves beyond technical waste reduction to encompass the strategic redefinition of resource value and stakeholder safety. The second domain, Energy Consumption and Renewable Integration, represents the GE-S-CSR intersection, where the systemic transition to low-carbon infrastructure is framed as a strategic necessity for long-term institutional resilience and decarbonization. The third domain, Sustainable Procurement and Circular Supply Chains, emerges from the CE-GE-S-CSR triad, requiring a synthesis of resource circularity (CE), economic viability (GE), and supplier accountability (S-CSR). Finally, the fourth domain, Economic and Policy Incentives, addresses the Institutional-GE intersection, providing the governance and fiscal mechanisms necessary to overcome the identified bureaucratic and financial barriers to implementation
As illustrated in Figure 1, the framework identifies Digital Enablers (such as AI-driven resource optimization and IoT-enabled waste tracking) as the critical operational bridge. These technologies translate the abstract theoretical intersections of CE, GE, and S-CSR into measurable actions within the four operational domains. By providing real-time data and transparency, digital enablers allow management to move beyond theoretical commitment to evidence-based execution, effectively closing the gap between strategic intent and operational output. The sub-sections that follow examine each domain in detail, presenting them as both conceptual levers and practical pathways for rethinking sustainability in hospital operations.
3.1. Waste Management and Circular Practices
Hospitals generate large quantities of diverse waste streams, including medical plastics, single-use packaging, disposable textiles, food waste, pharmaceutical residues, as well as radioactive, biohazard and liquid waste. The World Health Organization estimates that approximately 85% of healthcare waste is non-hazardous, and yet the vast majority of it is treated as infectious and sent for incineration or landfill disposal (WHO, 2022). Globally, the healthcare sector is responsible for up to 5.5 million tonnes of waste annually, with significant portions contributing to greenhouse gas emissions, toxic ash, and the release of microplastics into ecosystems (Eckelman & Sherman, 2016; Voudrias, 2018). The perception that most medical waste is inherently hazardous perpetuates a linear "generate-dispose" model and discourages innovation in waste handling.
Emerging CE frameworks challenge this paradigm by encouraging hospitals to adopt waste hierarchy principles, prioritizing prevention, reuse, and recovery over disposal (Kirchherr et al., 2018). The inclusion of the island context is not merely a specialized case study but a validation of the framework’s universal applicability. By demonstrating that strategic management can bridge the gap between logistical vulnerability and environmental responsibility in small island state settings, this paper argues that the transition to a Green and Circular Economy is achievable in any institutional context, provided there is sufficient strategic leadership and governance. Ultimately, the 'island stress test' confirms that sustainability is not a luxury afforded by resource abundance, but a strategic necessity for institutional survival in the face of global environmental change. CE strategies in the healthcare sector include the reclassification of waste streams to distinguish between genuinely hazardous and potentially reusable materials, the deployment of advanced sterilization technologies (e.g., autoclaving, ozone-based treatment), and the creation of closed-loop recovery systems for materials like surgical instruments, IV bags, and textiles (Deshwal & Parkash, 2018). Hospitals in Sweden, the Netherlands, and Canada have successfully piloted reusable gowns, drapes, and surgical toolkits, demonstrating reductions in both environmental impact and operational costs over time (MacNeill et al., 2020; Campion et al., 2015).
Critically, the social dimension of waste management extends beyond institutional compliance to encompass occupational health and community justice. Effective waste circularity reduces the exposure of healthcare workers to hazardous pathogens and chemical residues associated with traditional disposal methods. Furthermore, by minimizing the incineration of medical waste, which is often disproportionately sited near socio-economically disadvantaged areas, hospitals fulfill their social responsibility to environmental justice, ensuring that 'healing' within the hospital walls does not contribute to the 'harming' of the surrounding community’s public health (Buttigieg et al., 2019).
In addition to environmental considerations, waste management carries strategic, reputational, and ethical implications for hospitals. As public awareness around climate change, plastic pollution, and antimicrobial resistance increases, hospitals are being held to higher standards of environmental accountability. From a S-CSR perspective, sustainable waste practices represent a commitment to public trust, transparency, and long-term value creation (Singh & Trivedi, 2020; Aguinis & Glavas, 2012). For instance, reducing incineration can decrease toxic air emissions that disproportionately affect nearby communities, especially in underserved areas, thus linking waste management to health equity and environmental justice (Koh et al., 2020). These considerations also extend to radioactive waste streams, which require controlled management: solid radioactive waste is typically stored to allow decay and can only be managed in-house once it reaches non-radioactive levels, while liquid radioactive waste disposal is governed by jurisdiction-specific regulations and, in some settings, requires monitoring to ensure discharges remain below permitted limits, making staff education and strict procedures essential for compliance and risk reduction (WHO, 2014). Finally, opportunities to reduce pharmaceutical and chemical waste include targeting contrast agent residues from imaging procedures, given growing concerns about iodinated contrast contamination of water systems and the need for mitigation strategies within hospitals (Dekker, Stroomberg & Prokop, 2022; Zanardo et al., 2023).Moreover, sustainable waste practices can serve as a staff engagement tool, fostering a culture of responsibility and innovation. Beyond waste reduction, the institutionalization of sustainability serves as a critical social pillar by directly enhancing workforce well-being and engagement. In an era of chronic healthcare staff shortages, a visible and authentic commitment to environmental stewardship and social equity, such as reducing community-level incineration emissions, can foster a stronger sense of organizational identity and purpose among frontline workers. This alignment between planetary health and occupational satisfaction is essential for creating a resilient and committed healthcare workforce. Studies suggest that frontline healthcare workers are more likely to participate in sustainability initiatives when these efforts are visibly institutionalized and ethically framed (Rahman et al., 2024). Partnerships with certified medical recycling firms, implementation of real-time waste tracking technologies, and participation in green hospital accreditation programs (such as Practice Greenhealth or the Global Green and Healthy Hospitals Network) can further solidify sustainable waste management as a core strategic pillar of hospital governance.
Sustainable waste management is not merely an operational concern, it is a strategic imperative that intersects with cost savings, regulatory compliance, environmental ethics, and public legitimacy. This approach allows hospitals to reduce their ecological footprint while providing high quality standards of care.
3.2. Energy Consumption and Renewable Integration
Energy consumption represents one of the most significant environmental footprints of hospital operations. Hospitals are energy-intensive by design: they operate 24/7, maintain controlled temperature and air quality conditions for infection prevention and control, and rely on complex, high-powered medical devices and diagnostic systems. In the United States alone, hospitals consume approximately 2.5 times more energy per square foot than standard commercial buildings, contributing substantially to greenhouse gas emissions (U.S. Energy Information Administration, 2022). Globally, healthcare facilities account for roughly 4.4% of net carbon emissions, a large share of which comes from fossil-fuel-based electricity and heat generation (Karliner et al., 2019).
Despite the sector’s high energy demand, the adoption of renewable energy solutions remains limited. Barriers include high upfront investment costs, infrastructural inflexibility, limited access to capital, and short-term budgeting cycles that discourage long-term energy planning (Moner-Girona et al., 2021; Bozic et al., 2022). Moreover, institutional risk aversion, lack of technical expertise, and fragmented decision-making between facility managers, administrators, and clinicians further hinder widespread implementation of green energy technologies (Cohen et al., 2020).
Nevertheless, some promising models demonstrate what is possible. For example, the Gundersen Health System in Wisconsin became the first energy-independent health system in the U.S., relying on a portfolio of solar, wind, biomass, and biogas technologies – generating both economic returns and environmental benefits (Karliner et al., 2019). Similar efforts have been seen in Spain, Australia, and the UK, where hospitals have invested in photovoltaic systems, geothermal heating, and LED retrofits, often supported by government incentives or public-private partnerships (Delgado & Millán, 2020; NHS England, 2020).
From a GE perspective, these initiatives exemplify how healthcare institutions can decouple energy use from emissions while enhancing resilience, cost-efficiency, and climate preparedness. Retrofitting hospital buildings with passive ventilation systems, thermal insulation, on-site renewable generation, and smart energy monitoring platforms represents a core strategy for aligning health infrastructure with sustainable development goals (Schmidt et al., 2021). Studies have shown that hospitals with integrated energy management systems can achieve energy savings of 20–40%, significantly lowering their operating costs over time (Fabbri & Bianchi, 2021).
Here, the role of S-CSR has become particularly critical. When energy sustainability is embedded into hospital governance – as part of capital planning, executive Key Performance Indicators (KPIs), and environmental performance reporting – it moves from a facilities issue to a strategic management priority. S-CSR enables hospitals to frame energy transformation not as a cost but as an investment in long-term organizational value, social legitimacy, and operational resilience (Porter & Kramer, 2011; Lyon & Maxwell, 2008).
Travel (patients and staff) and transportation (consumables and equipment) represent a massive, yet often overlooked, component of a healthcare facility’s environmental impact. These activities account for approximately 16% of the total carbon footprint of healthcare systems (McGain & Naylor, 2014). In departments requiring frequent patient visits, transportation can even emerge as the primary contributor to their carbon profile (Chuter, 2023).
Regarding the transportation of goods, the impact is primarily driven by procurement logistics. Healthcare organizations can leverage their status as "anchor institutions" to mandate that vendors adopt low-emission logistics or "last-mile" electric delivery fleets. Strategically, this shifts the financial burden of the green transition onto the commercial market rather than the hospital’s operational budget. This approach naturally favors local suppliers, who benefit from inherently lower logistical costs and shorter supply chains (Wilburn et al. 2021).
While transitioning to green-energy vehicles is a primary objective, global adoption remains gradual; green alternatives are projected to reach only 30% of the market by 2030 (IEA, 2017). Furthermore, the viability of public transportation and active travel (walking or cycling) is heavily dictated by individual patient needs and urban planning (Sánchez-Barroso et al., 2021; World Health Organization & Health Care Without Harm, 2009a). To mitigate these constraints, healthcare systems must implement clinical solutions such as: telemedicine, reducing the necessity for physical travel for suitable consultations (Soares et al. 2023); efficient treatment planning, utilizing intensive treatment protocols to minimize the total number of patient visits (Bhatia et al., 2024); or decentralising care, allowing care to be provided closer to patients homes (Soares et al. 2023).
From an S-CSR perspective, reducing visits and increasing mass transit usage offers clear financial and sustainability benefits for both hospitals and users. However, the financial sustainability of electric vehicles (EVs) remains a point of academic debate. Some research suggests that EVs are currently viable only with government subsidies (Ganji, 2024) and that gasoline-powered vehicles remain more cost-effective for certain consumers (Rapson et al., 2023). Conversely, other studies indicate that EVs are already achieving financial parity or superiority when accounting for total cost of ownership (Liu et al., 2021), though these findings are highly sensitive to regional variations in taxation, insurance, and energy costs.
Beyond logistics, Strategic CSR encompasses workforce value propositions. Implementing green incentives—such as cycle-to-work schemes, subsidized transit passes, or on-site EV charging—has shown significant employee adherence (Swift et al., 2016; Busch-Geertsema et al., 2021). In a competitive labor market, these ESG-aligned benefits serve as a powerful tool for recruitment and retention, providing a form of "financial sustainability" by reducing the high costs associated with clinical staff turnover (Howard, 2024; Salha, 2022).
Moreover, GE adoption can be linked to community benefits such as improved air quality, lower public health burdens from pollution, and greater energy security during climate-related disruptions (Tait et al., 2019). These co-benefits further enhance the social return on investment of sustainable energy projects, reinforcing the alignment between hospital missions and sustainability. Hence, energy transformation in hospitals is both technically viable and strategically beneficial. Overcoming existing barriers requires a multi-level approach, combining GE incentives, regulatory support, institutional reform, and CSR-driven leadership. to embed sustainability into the energy DNA of healthcare systems.
Hospitals are among the most energy-intensive public institutions, with significant potential to reduce consumption through combined strategies that address both efficiency and renewable energy generation. Evidence from a recent analysis of Farabi Hospital in Iran showed that reducing the use of fossil fuels, recycling waste, and integrating renewable energy sources such as solar power are the most critical elements of sustainable energy management. Complementary measures such as installing water-saving equipment, automatic doors, and rainwater collection systems were also identified as high-impact interventions for optimizing resource use and environmental performance. The findings highlight that environmental criteria outweigh economic and social ones in overall importance, suggesting that energy strategies in healthcare should prioritize emission reduction, waste recycling, and renewable integration to achieve long-term sustainability goals (Jabbari, Feili, & Sorooshian, 2024).
Building on these findings, sustainable energy management should be embedded within hospitals’ broader strategic corporate social responsibility framework to ensure accountability and long-term impact. Establishing dedicated energy and environmental supervisory roles can help integrate technical initiatives, such as renewable energy adoption, energy-efficient building systems, and preventive maintenance programmes; into institutional governance structures. Applying multi-criteria decision-making methods, as demonstrated in the Farabi Hospital study, allows decision-makers to weigh environmental, economic, and social dimensions when prioritizing interventions. This structured approach aligns operational energy management with corporate sustainability goals, ensuring that hospitals balance service quality with environmental stewardship and cost efficiency (Jabbari, Feili, & Sorooshian, 2024).
3.3. Sustainable Procurement and Circular Supply Chains
Procurement is a pivotal area where hospitals either advance or compromise their sustainability objectives. As some of the largest institutional purchasers in the public sector, hospitals acquire massive volumes of goods ranging from pharmaceuticals and diagnostic tools to surgical instruments and facility maintenance supplies. Historically, procurement practices in healthcare have emphasized cost-effectiveness, regulatory compliance, and hygiene, factors that have led to widespread reliance on single-use, disposable products (Rotinen, 2022). While this approach may appear operationally efficient in the short term, it has contributed to significant environmental degradation through the acceleration of material throughput and the generation of non-recyclable waste.
In recent years, however, breakthroughs in material science, digital product traceability, and sterilization technologies have created new opportunities for sustainability in healthcare procurement. Products previously considered non-reusable, such as personal protective equipment, surgical drapes, or diagnostic devices, can now be safely reprocessed and recirculated with appropriate protocols (Rowan et al., 2023). These technological advancements enable hospitals to begin transitioning toward circular procurement models, a core tenet of the circular economy, which emphasize minimizing resource extraction and maximizing product lifespan through reuse, remanufacturing, and recycling (Kirchherr et al., 2018). Circular procurement can also involve redesigning consumable supply models to reduce packaging and product waste. For example, in CT services, multi dose iodinated contrast media packaging and delivery systems have been modeled as offering environmental and financial advantages compared with single dose systems (Lindsey et al., 2023). Unlike traditional procurement approaches, circular procurement encourages life cycle thinking, long-term supplier relationships, and innovative contracting mechanisms. Such model involves shifting from product ownership to performance-based contracts, in which the supplier retains responsibility for the entire lifecycle of the product, including maintenance, recovery, and end-of-life management (Lacy & Rutqvist, 2015). This not only incentivizes suppliers to design more durable and modular products but also reduces the hospital’s operational burden associated with disposal and compliance.
Viewed through the lens of S-CSR, procurement takes on a broader institutional significance. It becomes not merely a financial transaction but a strategic choice that reflects the hospital’s values, mission, and ethical responsibilities. S-CSR urges organizations to align procurement decisions with their long-term environmental, social, and governance goals. In this view, selecting vendors is no longer just about price or functionality, it is about choosing partners who operate with transparency, adhere to ethical labor standards, minimize carbon emissions throughout their logistics chains, and design products with end-of-life recovery in mind (Aguinis & Glavas, 2012; Porter & Kramer, 2011).
In practice, several hospitals and healthcare systems have begun embedding sustainability into procurement processes by adopting green criteria in tendering, supporting supplier training on circular practices, and engaging in industry-wide collaborations. For instance, healthcare networks in the European Union have partnered through initiatives like Health Care Without Harm Europe to push manufacturers toward cleaner production methods and reusable packaging (HCWH Europe, 2021). Similarly, group purchasing organizations (GPOs) in the U.S. and Canada are increasingly incorporating sustainability metrics into their evaluation criteria, thereby magnifying the systemic impact of procurement reforms (Li & Wang, 2022).
Crucially, procurement serves as a connective tissue within the hospital: it bridges clinical operations, facilities management, finance, and external supply chains. As such, it is uniquely positioned to act as a platform for sustainability integration across the institution. When approached strategically, sustainable procurement has the power not only to reduce ecological footprints but also to enhance hospital reputation, foster innovation, and stimulate market demand for cleaner, more ethical medical products. It becomes a site where environmental ethics, operational efficiency, and institutional legitimacy converge.
Ultimately, rethinking procurement through a CE, GE and S-CSR lens enables hospitals to shift from being passive consumers of unsustainable products to proactive agents of supply chain transformation. In doing so, they strengthen both their environmental performance and their social contract with patients, staff, and the broader community.
From a social perspective, sustainable procurement must also integrate ethical labor standards and health equity. A strategic CSR approach requires hospitals to evaluate suppliers not only on their carbon footprint but on their adherence to fair labor practices throughout the global supply chain. By prioritizing locally-sourced and ethically-produced materials, hospitals leverage their significant 'anchor institution' purchasing power to support local economic development and workforce stability. This transforms procurement from a purely transactional administrative function into a strategic tool for promoting social well-being and systemic equity.
3.4. Economic and Policy Incentives for Sustainability
While hospitals may be motivated by environmental and ethical constraints, the economic and policy environment in which they operate plays a critical role in determining whether sustainability goals are realized. Economic and policy incentives are not merely complementary, they are structural enablers or, conversely, barriers to sustainable transformation. Although numerous sustainability investments offer compelling long-term returns, they are frequently inhibited by high capital costs, uncertain payback timelines, and rigid public budgeting systems that prioritize short-term cost containment over long-term value (Chen et al., 2020).
This financial disincentive is particularly acute in public health systems, where administrative structures and funding mechanisms often leave little room for proactive, long-horizon investments. As a result, promising initiatives, (such as retrofitting buildings for energy efficiency or transitioning to circular procurement systems), are deferred or abandoned despite their long-term economic and ecological benefits.
To address this gap, a growing body of research and policy advocacy has emphasized the role of innovative financial instruments. Tools such as green bonds, climate funds, sustainability-linked loans, carbon pricing schemes, and targeted subsidies for energy retrofitting can dramatically improve the financial feasibility of sustainability investments (Zhou et al., 2022; Chien et al., 2022). Green bonds, for example, allow hospitals to raise capital for environmentally friendly infrastructure projects at preferential interest rates, while carbon pricing provides a market signal that incentivizes emissions reductions across operations. In some countries, tax credits for renewable energy installations have made solar and geothermal technologies more attractive to healthcare facilities previously constrained by narrow margins (IEA, 2023).
Policy and regulation, in parallel, provide institutional scaffolding that shapes hospitals' operating environments. Governments and regulatory bodies can accelerate sustainability transitions by introducing mandatory ESG reporting, national sustainability standards, and performance-linked accreditation frameworks. These mechanisms help institutionalize sustainability as a baseline requirement rather than a voluntary or symbolic gesture. A leading example is the UK’s National Health Service (NHS), which launched a sector-wide Net Zero strategy in 2020. This policy is not only backed by ambitious emissions targets but also enforces sustainable procurement rules, carbon accounting protocols, and funding incentives, making the NHS one of the world’s most comprehensive national models for decarbonizing healthcare (NHS England, 2020).
Beyond public funding, public–private partnerships (PPPs) represent a promising model for co-investment in sustainability infrastructure. By sharing costs and risks across sectors, PPPs can catalyse innovation in green construction, clean energy, waste treatment, and digital health platforms (Marx, 2019). Such collaborations are particularly effective in contexts where public funding is limited, yet there is political will and strategic vision for transformation. Moreover, PPPs can drive knowledge exchange and technical capacity-building, which are essential for embedding sustainability in institutional practice.
When these economic and policy mechanisms are aligned with S-CSR, they not only enhance financial viability but also reframe sustainability from a cost centre to a source of long-term value creation. S-CSR encourages hospitals to integrate these incentives into their investment planning, governance processes, and performance measurement systems. Therefore, hospitals can move beyond reactive compliance and embrace sustainability as a form of competitive advantage, institutional legitimacy, and public accountability (Porter & Kramer, 2011; Bansal & DesJardine, 2014).
Economic and policy incentives do not operate in isolation; they are part of a broader ecosystem of enablers that must be actively cultivated. For hospitals, leveraging these tools requires visionary leadership, cross-sector collaboration, and an internal culture that treats sustainability not as an optional add-on, but as a strategic and structural priority.
3.5. Integrated Framework Summary
To consolidate the conceptual insights discussed across the four operational domains – waste management, energy use, procurement, and policy – this sub-section presents an integrative framework that maps each domain to its relevant CE and GE principles, the corresponding S-CSR mechanisms, and the anticipated sustainability outcomes.
Table 2 below offers a synthesized view of how these components interact within hospital management systems. The table illustrates that sustainability in hospitals is not achieved through isolated interventions, but rather through the alignment of institutional strategies with broader ecological and ethical imperatives. It also highlights how S-CSR serves as the bridging mechanism that operationalizes sustainability principles across different functional areas.
By summarizing these interconnections, the framework supports a more holistic and actionable understanding of how hospitals can embed circular and green principles into core decision-making processes. This synthesis provides a foundation for future empirical research and policy design aimed at accelerating sustainability transitions in healthcare settings.
Although digital enablers are not listed as a separate column in the table, they operate across all four domains by providing the data, automation, and monitoring capacity required to implement CE, GE, and S-CSR practices effectively.
4. Contribution and Implications
This paper contributes to the growing literature on hospital sustainability by offering a theoretically grounded and strategically integrated model that aligns environmental, operational, and institutional priorities. Building on the conceptual integration of CE, GE, and S-CSR as developed in Section 2, and operationalized in Section 3, the study reframes hospital sustainability not as a peripheral obligation but as a core element of governance, innovation, and long-term performance. While distinguishing four foundational theoretical pillars from their two operational extensions, the paper offers a structured pathway that links conceptual sustainability logic with real-world implementation challenges and solutions.
A central contribution lies in the redefinition of S-CSR as a strategic function of CE and GE principles. Rather than treating CSR as isolated or philanthropic, the paper positions it as a mechanism that translates circularity and decarbonization into actionable strategies aligned with institutional missions and stakeholder expectations (Porter & Kramer, 2011; Husted & Allen, 2007). This lens empowers hospitals to transform sustainability from a reputational asset into a driver of organizational legitimacy and operational resilience.
Second, the paper identifies and details four operational domains – waste management, energy consumption, procurement, and policy incentives – as strategic entry points through which hospitals can enact this integrated logic (Section 3). These domains embody the technical ambitions of CE (e.g., closed-loop systems), the structural imperatives of GE (e.g., low-carbon infrastructure), and the governance lens of S-CSR (e.g., stakeholder alignment, long-term value creation).
Third, it centers the institutional barriers – including financial rigidity, siloed governance, and short-term planning – that inhibit sustainability implementation in healthcare (Section 2.5). While applying institutional theory (DiMaggio & Powell, 1983), this conceptual paper highlights how deeply embedded cultural and structural factors need to be addressed if conceptual models are to be operationalized at scale (Marchildon et al., 2021).
Furthermore, the specific challenges identified regarding 'island sustainability planning' serve as a critical 'stress test' for the proposed integrated model. Small-island states like Malta, characterized by extreme geographical isolation and external supply-chain dependencies, represent the frontier of resource scarcity. If the synthesis of S-CSR and Circular Economy principles can successfully navigate these high-constraint environments, the framework provides a robust blueprint for larger, mainland health systems. Policy recommendations must therefore prioritize 'resilience-by-design,' ensuring that procurement and waste management protocols are adaptable to both routine operations and the logistical shocks inherent in isolated geographic contexts.
Lastly, as a conceptual paper, the work offers a foundational framework for future empirical and policy research. While it does not present primary data, its synthesis of interdisciplinary literature (2010–2025) provides an initial base for hospital administrators, policymakers, and scholars to further develop, test, and scale the model in diverse healthcare contexts.
5. Strengths and Limitations
A major strength of this conceptual paper lies in its interdisciplinary integration. By synthesizing insights from environmental economics (CE, GE), strategic management (S-CSR), and institutional theory, the paper offers a multi-dimensional lens for understanding the complexity of hospital sustainability. In addition, the incorporation of institutional barriers and emerging digital enablers as operational extensions enhances the model’s practical relevance by clarifying both the constraints that hinder sustainability transitions and the technological pathways to implement the four foundational pillars. This conceptual base, articulated in Section 2, supports a more holistic view of how ecological imperatives intersect with organizational strategy and systemic design.
Another strength is the positioning of Strategic CSR as the managerial mechanism through which CE and GE principles are not only implemented but embedded into hospital identity, decision-making, and leadership development (Porter & Kramer, 2011; Jamali & Karam, 2018; Aguinis & Glavas, 2012). This emphasis moves beyond traditional CSR models and offers a value-driven pathway to sustainability that aligns with long-term institutional legitimacy and competitive advantage.
Moreover, by identifying four operational domains as practical levers (Section 3), this paper bridges theory and action. These domains offer a roadmap for applying sustainability principles to key hospital functions, from waste and energy to procurement and finance, thus providing both an operational and strategic tool for reform (Kirchherr et al., 2018; Singh & Trivedi, 2020). While the model focuses on these four domains for parsimony and clarity, hospital sustainability is inherently multi-dimensional, and additional domains such as water stewardship, food systems, mobility and travel, and building design warrant dedicated examination in future research and context specific applications. With regard to limitations, the conceptual design, while valuable for theory-building, lacks empirical validation. The model’s practical feasibility, scalability, and outcomes remain untested in real-world hospital environments. Moreover, it does not fully address regional or resource disparities, such as those faced by hospitals in low-income or fragile health systems and which could significantly affect implementation (Badanta et al., 2025; Zurynski et al., 2023).
Future research should focus on first conducting a systematic review of the literature on the topic and then empirically testing the model through case studies, cross-national comparisons, or pilot implementations. Despite these limitations, the paper lays an initial conceptual foundation and invites further investigation into one of healthcare’s most pressing challenges.
Conclusion
Embedding sustainability in hospital operations is now a strategic necessity. This paper offers an integrated framework that connects circular economy, green economy and strategic CSR principles with four actionable operational domains: waste, energy, procurement and policy incentives, supported by institutional and digital enablers.
This framework can be implemented in practice through a phased approach. First, hospitals should establish governance and accountability by assigning executive ownership, defining clear sustainability targets and KPIs, and embedding these into risk management, budgeting and reporting. Second, organizations should baseline impacts across the four domains using readily available operational data (waste streams, energy use, procurement spend and emissions, and relevant incentives or compliance requirements), then prioritize interventions using both environmental and clinical criteria. Third, hospitals should translate priorities into standard operating procedures and procurement clauses, for example circular purchasing requirements, supplier take-back arrangements, energy management protocols including equipment standby and shut-down procedures, and waste segregation and treatment pathways aligned with regulation. Fourth, implementation should be supported through staff and patient engagement, training, and continuous improvement cycles that monitor outcomes and iterate.
At system level, policymakers and regulators can accelerate uptake by aligning accreditation standards, reimbursement mechanisms and capital investment criteria with sustainability performance, and by enabling infrastructure and data interoperability that support circular and low-carbon service delivery. Future research should focus on empirical testing of the model across different hospital types and geographic contexts, identifying which combinations of interventions deliver the greatest benefits and how institutional constraints shape outcomes.
Hospitals are well placed to lead this transition. By combining operational redesign with strategic governance, they can reduce environmental harm while strengthening resilience, equity and long-term value in healthcare delivery.
References
- Aguinis, H.; Glavas, A. What we know and don’t know about corporate social responsibility. Journal of Management 2012, 38(4), 932–968. [Google Scholar] [CrossRef]
- Alzoubi, Y. I.; Topcu, A. E.; Elbasi, E. A systematic review and evaluation of sustainable AI algorithms and techniques in healthcare. IEEE Access 13 2025, 139547–139582. [Google Scholar] [CrossRef]
- Badanta, B.; Porcar Sierra, A.; Fernández, S. T.; Rodríguez Muñoz, F. J.; Pérez-Jiménez, J. M.; Gonzalez Cano-Caballero, M.; Ruiz-Adame, M.; de-Diego-Cordero, R. Advancing environmental sustainability in healthcare: Review on perspectives from health institutions. Environments 12 2025, 9. [Google Scholar] [CrossRef]
- Bhatia, R. K.; Lichter, K. E.; Zaorsky, N. G.; Mantz, C. Using hypofractionation to decarbonise radiation oncology. BMJ 2024, 386, e079072. [Google Scholar] [CrossRef] [PubMed]
- Bansal, P.; DesJardine, M. R. Business sustainability: It is about time. Strategic Organization 2014, 12(1), 70–78. [Google Scholar] [CrossRef]
- Barbier, E. B. Capitalizing on nature: Ecosystems as natural assets; Cambridge University Press, 2011. [Google Scholar]
- Bocken, N. M. P.; Bakker, C.; de Pauw, I. Product design and business model strategies for a circular economy. Journal of Industrial and Production Engineering 2016, 33(5), 308–320. [Google Scholar] [CrossRef]
- Brown, M. R. D.; Knight, M.; Peters, C. J.; Maleki, S.; Motavalli, A.; Nedjat-Shokouhi, B. Digital outpatient health solutions as a vehicle to improve healthcare sustainability—A United Kingdom focused policy and practice perspective. Frontiers in Digital Health 5 2023, Article 1242896. [Google Scholar] [CrossRef]
- Busch-Geertsema, A.; Lanzendorf, M.; Klinner, N. Making public transport irresistible? The introduction of a free public transport ticket for state employees and its effects on mode use. Transport Policy 106 2021, 1–9. [Google Scholar] [CrossRef]
- Buttigieg, S. C.; Tomaselli, G.; Byers, V.; Cassar, M.; Tjerbo, T.; Rosano, A. Corporate social responsibility and person-centered care: A scoping review. Journal of Global Responsibility 2019, 10(4), 289–306. [Google Scholar] [CrossRef]
- Buttner, L.; Posch, H.; Auer, T.; et al. Switching off for future—Cost estimate and a simple approach to improving the ecological footprint of radiological departments. European Journal of Radiology Open 8 2021, 100320. [Google Scholar] [CrossRef]
- Campion, N.; Thiel, C. L.; DeBlois, J.; Woods, N. C.; Landis, A. E. Life cycle assessment perspectives on delivering an infant in the US. Journal of Cleaner Production 79 2015, 89–98. [Google Scholar] [CrossRef]
- Chen, T. L.; Kim, H.; Pan, S. Y.; Tseng, P. C.; Lin, Y. P.; Chiang, P. C. Implementation of green chemistry principles in circular economy system towards sustainable development goals: Challenges and perspectives. Science of the Total Environment 716 2020, 136998. [Google Scholar] [CrossRef]
- Chew, X.; Khaw, K. W.; Alnoor, A.; Ferasso, M.; Al Halbusi, H.; Muhsen, Y. R. Circular economy of medical waste: Novel intelligent medical waste management framework based on extension linear Diophantine fuzzy FDOSM and neural network approach. Environmental Science and Pollution Research 2023, 30(21), 60473–60499. [Google Scholar] [CrossRef]
- Chien, F.; Sadiq, M.; Kamran, H. W.; Nawaz, M. A. The role of green financing and carbon pricing in enhancing the sustainability of healthcare infrastructure. Environmental Science and Pollution Research 2022, 29(4), 4567–4581. [Google Scholar]
- Chuter, R.; Stanford-Edwards, C.; Cummings, J.; Taylor, C.; Lowe, G.; Holden, E.; Razak, R.; Glassborow, E.; Herbert, S.; Reggian, G.; Mee, T.; Lichter, K.; Aznar, M. Towards estimating the carbon footprint of external beam radiotherapy. Physica Medica 112 2023, 102652. [Google Scholar] [CrossRef]
- Cohen, A. J.; Brauer, M.; Burnett, R.; et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the Global Burden of Disease Study 2019. The Lancet 2020, 396(10262), 1223–1249. [Google Scholar]
- Dekker, H. M.; Stroomberg, G. J.; Prokop, M. Tackling the increasing contamination of the water supply by iodinated contrast media. Insights into Imaging 13 2022, 30. [Google Scholar] [CrossRef]
- Deshwal, D. R.; Parkash, C. A review on medical waste management: Regulatory framework and practice. Environmental Claims Journal 2018, 30(1), 1–21. [Google Scholar]
- DiMaggio, P. J.; Powell, W. W. The iron cage revisited: Institutional isomorphism and collective rationality in organizational fields. American Sociological Review 1983, 48(2), 147–160. [Google Scholar] [CrossRef]
- Dion, H.; Evans, M.; Farrell, P. Hospitals management transformative initiatives; towards energy efficiency and environmental sustainability in healthcare facilities. Journal of Engineering, Design and Technology 2023, 21(2), 552–584. [Google Scholar] [CrossRef]
- Doherty, B.; Haugh, H.; Lyon, F. Social enterprises as hybrid organizations: A review and research agenda. International Journal of Management Reviews 2009, 16(4), 417–436. [Google Scholar] [CrossRef]
- Duque-Uribe, V.; Sarache, W.; Gutiérrez, E. V. Sustainable supply chain management practices and sustainable performance in hospitals: A systematic review and integrative framework. Sustainability 2019, 11(21), 5949. [Google Scholar] [CrossRef]
- Eckelman, M. J.; Sherman, J. D. Environmental impacts of the U.S. health care system and effects on public health. PLOS ONE 2016, 11(6), e0157014. [Google Scholar] [CrossRef]
- Ellen MacArthur Foundation. Towards the circular economy: Opportunities for the consumer goods sector; Ellen MacArthur Foundation, 2013. [Google Scholar]
- European Commission. A new circular economy action plan: For a cleaner and more competitive Europe; European Commission, 2020. [Google Scholar]
- Fabbri, M.; Bianchi, G. Smart energy systems in hospital facilities: A review of practices and barriers. Journal of Cleaner Production 310 2021, 127397. [Google Scholar]
- Foster, J. The green economy: Environment, sustainable development and the politics of the future; Zed Books, 2011. [Google Scholar]
- Ganji, F. Assessing electric vehicle viability: A comparative analysis of urban versus long-distance use with financial and auditing insights. UJRRA 2023, 3(4). [Google Scholar] [CrossRef]
- Geissdoerfer, M.; Savaget, P.; Bocken, N. M. P.; Hultink, E. J. The circular economy – A new sustainability paradigm? Journal of Cleaner Production 143 2017, 757–768. [Google Scholar] [CrossRef]
- Heshmati, A. A review of the circular economy and its implementation. International Journal of Green Economics 2017, 11(3–4), 251–288. [Google Scholar] [CrossRef]
- HCWH Europe. Sustainable procurement in European healthcare: A practical guide. In Health Care Without Harm; 2021. [Google Scholar]
- Heye, T.; Meyer, M. T.; Merkle, E. M.; Vosshenrich, J. Turn it off! A simple method to save energy and CO₂ emissions in a hospital setting with focus on radiology by monitoring nonproductive energy-consuming devices. Radiology 2023, 307(4), e230162. [Google Scholar] [CrossRef]
- Howard, E. L. Employee turnover in United States companies that embrace green practices to promote employee retention. Doctoral dissertation, Capella University, 2024. [Google Scholar]
- Husted, B. W.; Allen, D. B. Strategic corporate social responsibility and value creation among large firms. Long Range Planning 2007, 40(6), 594–610. [Google Scholar] [CrossRef]
- International Energy Agency. Global EV outlook 2017; International Energy Agency, 2017. Available online: https://www.iea.org/reports/global-ev-outlook-2017.
- International Energy Agency. Global energy efficiency policy toolkit for the health sector; International Energy Agency, 2023. Available online: https://www.iea.org.
- Jabbari, O.; Feili, A.; Sorooshian, S. Sustainable energy management strategies in hospitals: Examination and analysis. Hospital Management Studies Journal 5 2024. [Google Scholar] [CrossRef]
- Jamali, D.; Karam, C. Corporate social responsibility in developing countries as an emerging field of study. International Journal of Management Reviews 2018, 20(1), 32–61. [Google Scholar] [CrossRef]
- Jeyarajasekar, T.; Afzana, S. A.; Anaswara, A. R.; Chandran, B. S.; Santhosh, D. S.; A, S. Sustainability in hospitals: Identifying boosting elements through the triple bottom line framework. International Journal of Environmental Science 2025, 11(23s), 950–961. [Google Scholar]
- Kahramanoglu, I.; Kacperczyk-Bartnik, J.; Nout, R.; de Vries, M.; Oduncu, F. S. Practical strategies for environmentally sustainable practices in gynecologic oncology. International Journal of Gynecology & Obstetrics 2025. [Google Scholar] [CrossRef]
- Kammrath Betancor, P.; Boehringer, D.; Jordan, J.; Lüchtenberg, C.; Lambeck, M.; Ketterer, M. C.; Reinhard, T.; Reich, M. Efficient patient care in the digital age: Impact of online appointment scheduling in a medical practice and a university hospital on the “no-show” rate. Frontiers in Digital Health 7 2025, Article 1567397. [Google Scholar] [CrossRef]
- Kara, S.; Hauschild, M.; Sutherland, J.; McAloone, T. Closed-loop systems to circular economy: A pathway to environmental sustainability? CIRP Annals 2022, 71(2), 505–528. [Google Scholar] [CrossRef]
- Karliner, J.; Slotterback, S.; Boyd, R.; Ashby, B.; Steele, K. Healthcare’s climate footprint: How the health sector contributes to the global climate crisis and opportunities for action. In Health Care Without Harm; 2019. [Google Scholar]
- Kirchherr, J.; Reike, D.; Hekkert, M. Conceptualizing the circular economy: An analysis of 114 definitions. Resources, Conservation and Recycling 127 2018, 221–232. [Google Scholar]
- Kjelle, E.; et al. Sustainability in healthcare by reducing low-value imaging: A narrative review. Radiography 30 2024, 30–34. [Google Scholar] [CrossRef]
- Klein, K. Values-based food procurement in hospitals: The role of health care group purchasing organizations. Agriculture and Human Values 2015, 32(4), 635–648. [Google Scholar] [CrossRef]
- Koh, H. K.; Bantham, A.; Geller, A. C.; Pronk, N. P. Integrating public health and health care delivery to advance health equity: A conceptual framework. Health Affairs 2020, 39(7), 1061–1068. [Google Scholar]
- Lacy, P.; Rutqvist, J. Waste to wealth: The circular economy advantage; Palgrave Macmillan, 2015. [Google Scholar]
- Lehtinen, L. Emerging sustainable materials in the health care industry: Possibilities and challenges of replacing single-use plastics. Bachelor’s thesis, JAMK University of Applied Sciences, Theseus, 2022. [Google Scholar]
- Li, Y.; Wang, X. Greening healthcare procurement: Strategies for circular supply chains. Journal of Cleaner Production 367 2022, 133022. [Google Scholar]
- Lindsey, J. S.; Frederick-Dyer, K.; Carr, J. J.; Cooke, E.; Allen, L. M.; Omary, R. A. Modeling the environmental and financial impact of multi-dose vs. single-dose iodinated contrast media packaging and delivery systems. Academic Radiology 2023, 30(6), 1017–1023. [Google Scholar] [CrossRef]
- Liu, Z.; Song, J.; Kubal, J.; Susarla, N.; Knehr, K. W.; Islam, E.; Nelson, P.; Ahmed, S. Comparing total cost of ownership of battery electric vehicles and internal combustion engine vehicles. Energy Policy 158 2021, 112564. [Google Scholar] [CrossRef]
- Loiseau, E.; Saikku, L.; Antikainen, R.; Droste, N.; Hansjürgens, B.; Pitkänen, K.; Thomsen, M. Green economy and related concepts: An overview. Journal of Cleaner Production 139 2016, 361–371. [Google Scholar] [CrossRef]
- Lyon, T. P.; Maxwell, J. W. Corporate social responsibility and the environment: A theoretical perspective. Review of Environmental Economics and Policy 2008, 2(2), 240–260. [Google Scholar] [CrossRef]
- Macassa, G.; McGrath, C.; Tomaselli, G.; Buttigieg, S. C. Corporate social responsibility and internal stakeholders’ health and well-being in Europe: A systematic descriptive review. Health Promotion International 2021, 36(3), 866–883. [Google Scholar] [CrossRef]
- MacNeill, A. J.; Hopf, H. W.; Khanuja, A.; et al. Transforming the medical device industry: Road map to a circular economy. Health Affairs 2020, 39(12), 2088–2097. [Google Scholar] [CrossRef]
- Marchildon, G. P.; Allin, S.; Merkur, S. Health systems in transition, 3rd ed.; University of Toronto Press, 2021. [Google Scholar]
- Mariampillai, J.; Rockall, A.; Manuellian, C.; et al. The green and sustainable radiology department. In Radiologie; 2023. [Google Scholar] [CrossRef]
- Marx, A. Public-private partnerships for sustainable development: Exploring their design and its impact on effectiveness. Sustainability 2019, 11(4), 1087. [Google Scholar] [CrossRef]
- Matten, D.; Moon, J. “Implicit” and “explicit” CSR: A conceptual framework for a comparative understanding of corporate social responsibility. Academy of Management Review 2008, 33(2), 404–424. [Google Scholar] [CrossRef]
- McGain, F.; Naylor, C. Environmental sustainability in hospitals: A systematic review and research agenda. Journal of Health Services Research & Policy 2014, 19(4), 245–252. [Google Scholar] [CrossRef]
- Mirow, J.; Venne, J.; Brand, A. Green health: How to decarbonise global healthcare systems. Sustain Earth Reviews 7 2024, 28. [Google Scholar] [CrossRef]
- Moner-Girona, M.; Kakoulaki, G.; Falchetta, G.; Weiss, D. J.; Taylor, N. Achieving universal electrification of rural healthcare facilities in sub-Saharan Africa with decentralized renewable energy technologies. Joule 2021, 5(10), 2687–2714. [Google Scholar] [CrossRef]
- NHS England. Delivering a “net zero” National Health Service. In NHS England; 2020. [Google Scholar]
- Patel, S.; Pundge, A.; Akhter, N. Harnessing IoT and artificial intelligence for sustainable healthcare. 2023. [Google Scholar] [CrossRef]
- Pickard Strange, M.; Booth, A.; Akiki, M.; Wieringa, S.; Shaw, S. E. The role of virtual consulting in developing environmentally sustainable health care: Systematic literature review. Journal of Medical Internet Research 25 2023, e44823. [Google Scholar] [CrossRef]
- Porter, M. E.; Kramer, M. R. Creating shared value. Harvard Business Review 2011, 89(1–2), 62–77. [Google Scholar]
- Potting, J.; Hekkert, M.; Hanemaaijer, A. Circular economy: Measuring innovation in the product chain; Netherlands Environmental Assessment Agency, 2017. [Google Scholar]
- Rahman, F. F.; Haris, F.; Febriyanto, K. Organizational support for green hospital initiatives: A case study. Jurnal Medicoeticolegal dan Manajemen Rumah Sakit 2024, 13(3), 304–314. [Google Scholar] [CrossRef]
- Ranucci, R. Delivering health care without degrading health: Factors associated with hospital commitment to environmental sustainability. Health Care Management Review 2025, 50(3), 175–184. [Google Scholar] [CrossRef]
- Rapson, D. S.; Muehlegger, E. The Economics of Electric Vehicles. Review of Environmental Economics and Policy 2023, 17(2), 274–294. [Google Scholar] [CrossRef]
- Reddy, V. J.; Hariram, N. P.; Ghazali, M. F.; Kumarasamy, S. Pathway to sustainability: An overview of renewable energy integration in building systems. Sustainability 2024, 16(2), 638. [Google Scholar] [CrossRef]
- Ribeiro, D. F.; et al. A scoping review of sustainable strategies adopted in nuclear medicine. Radiography 2025, 31(5), 103122. [Google Scholar] [CrossRef]
- Rockall, A.; et al. Sustainability in radiology: Position paper and call to action from ACR, AOSR, ASR, CAR, CIR, ESR, ESRNM, ISR, IS3R, RANZCR, and RSNA. European Radiology 35 2025, 5427–5436. [Google Scholar] [CrossRef]
- Roletto, E.; et al. The environmental impact of energy consumption and carbon emissions in radiology departments: A systematic review. European Radiology Experimental 8 2024, 35. [Google Scholar] [CrossRef]
- Salha, R. The influence of a company’s sustainability initiatives on its employee retention. Master’s thesis, 2022. [Google Scholar] [CrossRef]
- Sánchez-Barroso, G.; González-Domínguez, J.; García-Sanz-Calcedo, J.; Sokol, M. Impact of weather-influenced urban mobility on carbon footprint of Spanish healthcare centres. Journal of Transport & Health 20 2021, 101017. [Google Scholar] [CrossRef]
- Sarchosoglou, A.; Couto, J. G.; Khine, R.; O’Donovan, T.; Pisoni, V.; Bajinskis, A.; England, A.; et al. A European Federation of Radiographer Societies (EFRS) position statement on sustainability for the radiography profession. Radiography 30 2024, 19–22. [Google Scholar] [CrossRef]
- Schmidt, C. W.; Lindgren, S.; Nolan, T. Energy efficiency in healthcare: Challenges and opportunities. Environmental Health Perspectives 2021, 129(2), 025001. [Google Scholar]
- Schwab, R.; Schiestl, L. J.; Hasenburg, A. Greening the future of healthcare: Implementation of sustainability strategies in German hospitals and beyond: A review. In Frontiers in Public Health; 2025. [Google Scholar] [CrossRef]
- Schoen, J.; McGinty, G. B.; Quirk, C. Radiology in our changing climate: A call to action. Journal of the American College of Radiology 2021, 18(7), 1041–1043. [Google Scholar] [CrossRef]
- Sepetis, A.; Parlavantzas, I. Circular economy behavior and sustainable healthcare. In Circular Economy and Sustainability; 2025. [Google Scholar] [CrossRef]
- Shum, P. L.; Kok, H. K.; Maingard, J.; et al. Sustainability in interventional radiology: Are we doing enough to save the environment? CVIR Endovascular 5 2022, Article 36. [Google Scholar] [CrossRef]
- Singh, H.; Trivedi, A. Application of circular economy principles in the healthcare sector: A conceptual analysis. Sustainability 2020, 12(19), 8187. [Google Scholar]
- Soares, A. L.; Buttigieg, S. C.; Bak, B.; McFadden, S.; Hughes, C.; McClure, P.; Couto, J. G.; Bravo, I. A review of the applicability of current green practices in healthcare facilities. International Journal of Health Policy and Management 12 2023, 6947. [Google Scholar] [CrossRef]
- Stevenson, M.; Hendry, L. C.; Kingsman, B. G. Green supply chain practices in healthcare: A comparison between hospitals in the UK and the US. International Journal of Production Economics 2013, 146(2), 589–602. [Google Scholar] [CrossRef]
- Swift, S.; Green, M.; Hillage, J.; Nafilyan, V. Impact of the cycle to work scheme: Evidence report 2016.
- Tait, L.; Wlokas, H.; Garside, B. Benefits and risks of renewable energy in healthcare in developing regions. Energy for Sustainable Development 49 2019, 77–85. [Google Scholar]
- Tomaselli, G.; Garg, L.; Gupta, V.; Xuereb, P. A.; Buttigieg, S. C. Digital and traditional tools for communicating corporate social responsibility: A literature review. In Corporate social responsibility: Concepts, methodologies, tools, and applications; IGI Global, 2019; pp. 679–696. [Google Scholar]
- United Nations Environment Programme. Towards a green economy: Pathways to sustainable development and poverty eradication; UNEP, 2011. [Google Scholar]
- Voudrias, E. A. Healthcare waste management from the perspective of the circular economy. Waste Management 75 2018, 1–2. [Google Scholar]
- Wang, Y.; Yang, Y.; Qin, Z.; Yang, Y.; Li, J. A literature review on the application of digital technology in achieving green supply chain management. Sustainability 2023, 15(11), 8564. [Google Scholar] [CrossRef]
- Wilburn, S.; Jharia, I.; Prabhakaran, P. Sustainable procurement in healthcare. In Sustainable healthcare; 2022. [Google Scholar] [CrossRef]
- World Health Organization; Health Care Without Harm; World Health Organization. Healthy hospitals, healthy planet, healthy people: Addressing climate change in health care settings; 2009. [Google Scholar]
- World Health Organization. WHO guidance for climate-resilient and environmentally sustainable health care facilities; World Health Organization, 2020. [Google Scholar]
- World Health Organization. Global analysis of healthcare waste in the context of COVID-19: Status, impacts and recommendations; World Health Organization, 2022. [Google Scholar]
- Wyssusek, K. H.; Keys, M. T.; van Zundert, A. A. Operating room greening initiatives—the old, the new, and the way forward: A narrative review. Waste Management & Research 2019, 37(1), 3–19. [Google Scholar]
- Zanardo, M.; Cozzi, A.; Cardani, R.; et al. Reducing contrast agent residuals in hospital wastewater: The GREENWATER study protocol. European Radiology Experimental 7 2023, 27. [Google Scholar] [CrossRef]
- Zhou, J.; Zhao, X.; Lin, Y. Green bonds in healthcare: Financing sustainability transitions. Sustainability 2022, 14(3), 1287. [Google Scholar]
- Zurynski, Y.; Ludlow, K.; Testa, L.; et al. Built to last? Barriers and facilitators of healthcare program sustainability: A systematic integrative review. Implementation Science 18 2023, 62. [Google Scholar] [CrossRef]
Figure 1.
Integrated Conceptual Framework for Hospital Sustainability, illustrating Digital Enablers as the strategic bridge between theoretical pillars (CE, GE, S-CSR) and operational domains.
Figure 1.
Integrated Conceptual Framework for Hospital Sustainability, illustrating Digital Enablers as the strategic bridge between theoretical pillars (CE, GE, S-CSR) and operational domains.
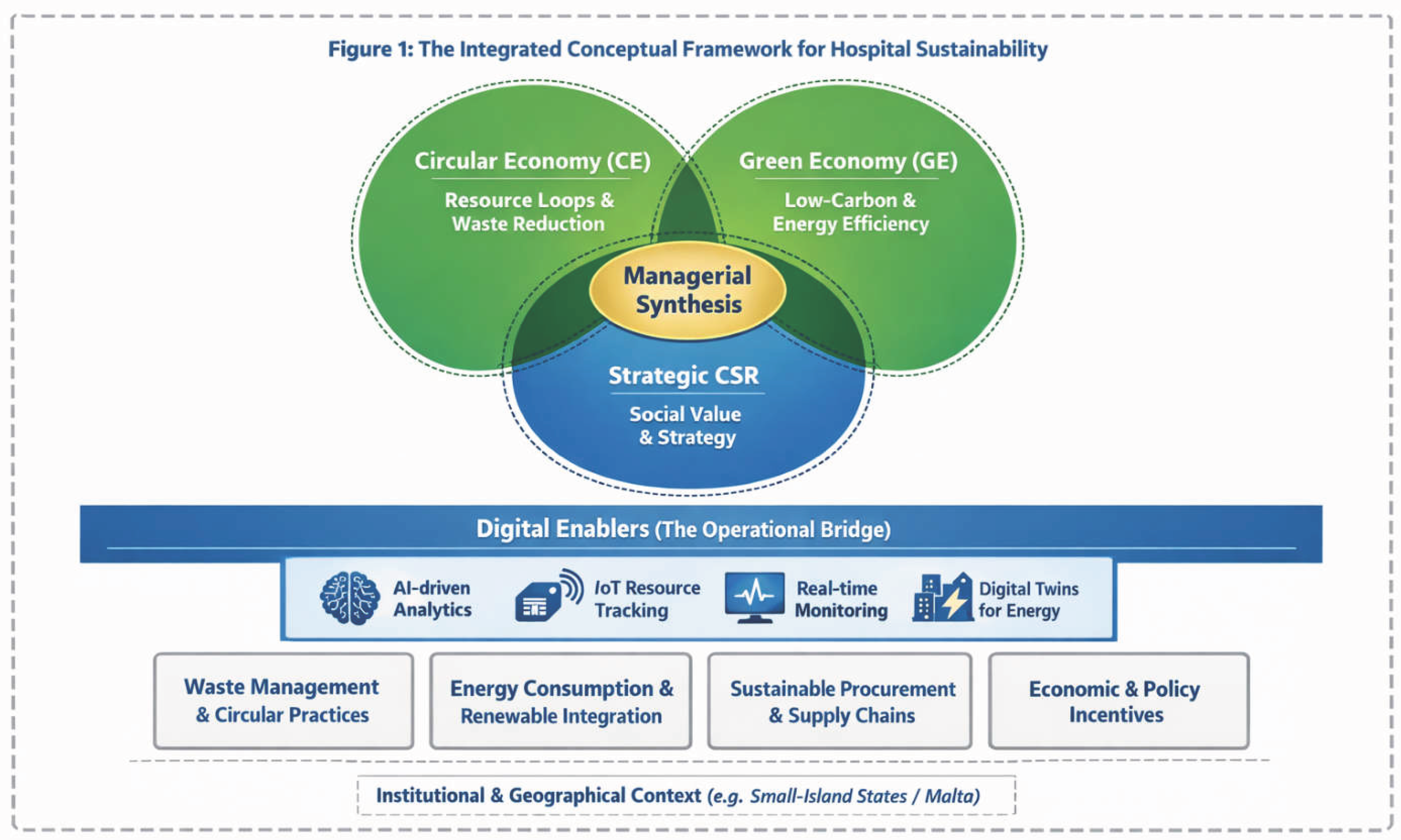

Table 1.
Key Sustainability Governance Competencies for Hospital Leadership.
| Competency | Description | Strategic Impact |
|---|---|---|
| ESG Literacy | Understanding Environmental, Social, and Governance metrics and their impact on hospital rating and funding. | Ensures sustainability is integrated into the hospital’s financial and risk management profile. |
| Systems Thinking | The ability to recognize interdependencies between clinical workflows, supply chains, and environmental health. | Enables leaders to identify how a change in one department (e.g., procurement) reduces waste in another (e.g., clinical wards). |
| Stakeholder Stewardship | Proactive engagement with patients, staff, and the local community regarding the hospital’s environmental footprint. | Enhances institutional legitimacy and aligns hospital operations with public health and community well-being. |
| Ethical Decision-Making | Balancing short-term financial constraints with long-term planetary health and social equity mandates. | Bridges the gap between immediate clinical needs and the "moral responsibility" of the institution. |
Table 2.
Integrated Sustainability Framework for Hospitals.
| Domain | Circular/Green Economy Principle | Strategic CSR Mechanism | Expected Sustainability Outcome |
|---|---|---|---|
| Waste Management & Circular Practices | Material rethink, reuse, repair, and recycle waste hierarchy, closed-loop systems | Investment in reusable products, partnerships with recycling firms, reclassification of waste streams | Reduced landfill waste and incineration, improved resource efficiency, reputational legitimacy, long-term cost savings |
| Energy Consumption & Renewable Integration | Energy decarbonization, energy resilience, resource efficiency | Capital planning for retrofitting, integrating renewable energy into infrastructure, reporting GHG reductions | Lower emissions, long-term cost savings, energy security |
| Sustainable Procurement & Supply Chains | Lifecycle thinking, shared responsibility, supplier engagement | Circular procurement policies, sustainability criteria in tenders, performance-based contracts | Reduced supply chain emissions, ethical sourcing, system-wide circularity |
| Economic and Policy Incentives | Regulatory support, financial instruments, market-based incentives | Leveraging green bonds, engaging in PPPs, compliance with national net-zero strategies | Scaled sustainability adoption, enhanced investment appeal, long-term institutional transformation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



