Submitted:
06 February 2026
Posted:
06 February 2026
You are already at the latest version
Abstract
Objective: The effectiveness of available wound debridement strategies, including endogenous autolysis, enzymatic, larval, and surgical approaches, is often limited by poor wound-bed biology, cost, and invasiveness. Although copper oxide–containing dressings (COD) have demonstrated broad wound-healing activity in basic science and clinical studies, their potential to modulate debridement has not been specifically characterized. Methods: We retrospectively analyzed five extreme clinical cases involving six limbs with diverse etiologies, extensive necrosis, impaired perfusion, and frequently compromised systemic conditions. Sequential clinical imaging and detailed follow-up were used to assess wound-bed dynamics. Observations were interpreted in the context of relevant published basic science. Results: In five of six limbs, major amputation or revision to a higher level had been indicated prior to COD initiation. In all cases, application of COD was associated with rapid and extensive clearance of devitalized tissue, suggesting augmentation of endogenous autolytic mechanisms. Review of the literature supports copper-dependent pathways (CDPs), including the MMP–TIMP axis, inflammatory signaling via NF-κB, and macrophage polarization. Analysis of serial photographs demonstrated concurrent emergence of granulation tissue and vascularization, supporting synergism between angiogenesis, granulation tissue formation, and debridement, all induced by COD. Conclusions: The findings support the hypothesis that copper ions and COD may amplify autolytic tissue clearance through CDPs, with concurrent synergistic interaction between angiogenesis and debridement.
Keywords:
debridement
; copper
; copper oxide
; wound dressings
; angiogenesis
; matrix metalloproteinases
; copper dressings
1. Introduction
Good tissue quality is essential for wound healing, yet many wounds are characterized by compromised viability and necrosis that impede repair [1]. Debridement is therefore a cornerstone of wound management, aiming to remove non-viable tissue and restore a healing-permissive environment [2]. Although surgical debridement is effective, it is not always feasible and may damage viable tissue, leaving many wounds reliant on endogenous autolytic and enzymatic mechanisms [2].
Copper cations appear to engage multiple interconnected molecular and cellular pathways involved in necrotic tissue autolysis. By modulating extracellular matrix remodeling via the MMP–TIMP axis, activating controlled inflammatory signaling via NF-κB, and polarizing macrophages, copper cations enhance the debridement response [3,4,5,6,7,8].
These physiological debridement processes are often insufficient in the presence of extensive necrosis, impaired perfusion, hypoxia, or systemic illness, leading to insufficient inflammation, bacterial persistence, and delayed healing [9,10]. This creates a clear clinical need for therapies that directly enhance, rather than merely support, native debridement pathways.
Copper-oxide dressings (COD) represent a novel approach[11]. Experimental and clinical studies show that copper cations activate key wound-healing pathways, including antimicrobial activity, modulation of inflammation, angiogenesis, and enzymatic tissue remodeling [3,11,12,13]. Copper stabilizes hypoxia-inducible factor (HIF-1α), leading to upregulation of pro-angiogenic and reparative mediators such as VEGF and PDGF, thereby promoting granulation tissue formation and epithelialization [3,14]. Nevertheless, debridement was not declared a property of copper-containing dressings.
Clinically, COD was observed to induce rapid clearance of devitalized tissue, prompting a search for mechanistic explanations to bridge the gap [15,16,17,18,19,20,21] . We analyze five extreme cases to demonstrate preclinical concepts in clinical practice. We have analyzed sequential images, paying special attention to the inter-relationship between the disappearance of necrotic tissue and angiogenesis and granulation tissue formation.
2. Materials and Methods
Beginning in May 2019, COD were introduced into clinical practice at Rambam Health Care Campus. Initial use was limited to stable patients with hard-to-heal wounds, primarily diabetic foot ulcers. With accumulating clinical experience and emerging supportive evidence, indications were progressively expanded to include complex and severe wounds, including cases with extensive necrosis, compromised perfusion, and failure of conventional surgical and non-surgical treatments.
This report analyzes a retrospective case series of five patients and six limbs with diverse wound etiologies, treated inpatient (n=4) or outpatient (n=1). Attention was paid to cover all the surfaces and cavities of the wounds, as well as the normal skin surrounding the wound. Dressing was changed once or twice weekly throughout all stages of wound healing. No adjunctive enzymatic or chemical debridement agents were used.
Clinical analysis using high-quality sequential images taken every dressing change, focused on the extent and rate of necrotic tissue clearance, granulation tissue formation, local inflammatory signs, wound demarcation, and readiness for definitive closure or grafting.
All patients, or their legal representatives when applicable, provided informed consent for treatment with COD and for the use of anonymized clinical data and images for academic publication, in accordance with institutional ethical standards and the Declaration of Helsinki. No electronic laboratory notebook platform was used.
3. Results
Case 1—Chronic Venous Leg Ulcer in a Patient with APLA Syndrome
A 48-year-old male with antiphospholipid antibody syndrome (APLA) and chronic venous insufficiency following recurrent venous thrombosis presented with a chronic venous leg ulcer of approximately eight years’ duration. Over this period, the patient had been treated by experienced multidisciplinary wound care teams without meaningful clinical improvement, and amputation was offered to him.
On examination, the ulcer was extensive, measuring 185 × 120 mm, and was characterized by near-complete coverage with nonviable tissue and minimal to absent granulation tissue. Peripheral arterial pulses were palpable and symmetrical, with no clinical signs of arterial insufficiency. Treatment with COD (changed weekly) was initiated. Progressive autolytic debridement was observed, accompanied by early granulation tissue formation. After four weeks of COD treatment, the wound bed demonstrated complete clearance of devitalized tissue and 100% granulation tissue coverage. The progression of the wound is depicted in Figure 1.
Case 2—Debridement of Marginal Wound (Stump) Necrosis
A 60-year-old woman with diabetes mellitus was admitted following a supracondylar femoral fracture. Initial management was prolonged and non-operative. Due to failure of fracture healing and ongoing wound complications, a transfemoral amputation above the fracture level was ultimately performed. Postoperatively, the amputation stump failed to heal and required revision surgery, which in turn failed to heal, and hip disarticulation was considered. At presentation, the stump demonstrated partial central granulation tissue surrounded by necrotic and ischemic wound margins. Within several days, early granulation tissue was observed centrally, with a clear demarcation between viable and non-viable tissue at the wound margins. After 4 weeks (day 27), bedside sharp marginal debridement was performed without anesthesia, limited to approximately 2 mm from the necrotic wound edges, thereby eliminating pain and minimizing damage to viable skin. Four days later, most residual necrotic tissue had been resolved. Within two to three weeks, the wound demonstrated fully viable margins and complete granulation tissue coverage, allowing delayed primary closure at day 52. The progression of the wound is depicted in Figure 2.
Case 3—Biological Reactivation of a Critically Ischemic Amputation Stump
A 71-year-old male, one month after coronary artery bypass grafting, during which a saphenous vein graft was harvested from the lower limb, presented with complications at the graft harvest site. The harvest site became severely infected and ischemic, ultimately necessitating below-knee amputation followed by progression to an above-knee amputation. Due to ischemia, the stump was closed loosely but failed to heal. The patient was critically ill, mechanically ventilated, and systemically compromised, with additional pressure-related wounds. The thigh was not warm or edematous (failure to raise an inflammatory response). The sutures were removed, revealing an entirely non-viable stump with no inflammatory response, including erythema or edema. COD were then applied and replaced twice weekly. Already at the first dressing change, early granulation tissue was observed, with progressive autolytic debridement and granulation tissue growth during subsequent changes. At the fourth dressing change, 14 days after initiation of COD therapy, a significant purulent discharge appeared without associated thigh swelling, erythema, or systemic deterioration. Three days later, no purulent discharge was observed, and the wound bed appeared dry, with organized, cauliflower-like granulation tissue and clean margins. The patient succumbed shortly afterward due to his cardiovascular condition. The progression of the wound is depicted in Figure 3.
Case 4—Debridement of Extensive Eschar Following Electrical Burn
A 19-year-old patient sustained an electrical injury, resulting in a burn to the left foot. Initial treatment with betadine-soaked dressing, followed by chlorine-based solutions and sulfurous application. The devitalized tissue, mainly on the dorsum of the foot and toes, underwent denaturation to necrotic eschar or dry gangrene of the toes. The use of COD began on the 10th day after injury. The left foot demonstrated extensive necrosis of the toes, including the 1st metatarsal head and the dorsum of the foot. Surgical resection of the necrotic middle toes was performed two weeks after injury, leaving the definitive amputation (and skin grafting) to a later stage. of the hallux and the fifth toe was deferred to a later stage. COD was changed once weekly T Progressive autolytic debridement was observed, with gradual and steady replacement of necrotic tissue by thick, red granulation tissue. The surgical intervention consisted of a trans metatarsal amputation to preserve good-quality plantar skin at the forefoot, and a split-thickness skin graft was applied onto the dense, well-vascularized granulation tissue. The graft demonstrated complete take, consistent with prior successful wound bed preparation. The progression of the wound is depicted in Figure 4.
Case 5—Debridement and Revascularization of Extensive Devitalized Tissue Following an Open Fracture
A 73-year-old man with a 25-year history of diabetes mellitus was injured in a farming accident, causing a high-energy open fracture of the left femur and an open dislocation of the right knee. The injury was accompanied by extensive contamination of the deep soft tissues with earth and animal fecal material.
Urgent CT angiography demonstrated patent major arteries in both limbs. Emergency surgery included irrigation and sharp debridement, and the application of external fixators. In the ICU and then in the orthopedic ward, the wounds were managed with chlorine-based solutions, which were temporarily changed to sulfamylon and then resumed. Routine antibiotics (cefazolin and gentamicin) were used initially, followed by minocycline, levofloxacin, and piperacillin/tazobactam.
At two weeks post-injury, the wounds remained extensively devitalized without clinical progression. Given the extent of necrosis and long-standing diabetes, bilateral trans-femoral amputation was planned. Instead, wound management was changed to COD, applied twice weekly directly to the wounds and surrounding skin. At the first dressing change, a significant purulent discharge was observed. As in Case 3, this was interpreted as a productive inflammatory response rather than a sign of treatment failure (e.g., infection), and COD treatment was continued.
Subsequent dressing changes showed progressive autolytic debridement, with necrotic tissue replaced by abundant, well-vascularized granulation tissue and complete resolution of purulent discharge. Within three weeks of COD therapy, approximately 90% of the wound bed was covered by granulation tissue. Split-thickness skin grafting was performed at 8-10 weeks post injury. At the two-year follow-up, the patient walks with a walker due to arthritic changes in the knee, but the skin is intact. The progression of the wound is depicted in Figure 5.
4. Discussion
Most wounds, except for clean surgical wounds, involve tissue injury, manifesting as compromised, devitalized, or necrotic tissue. Good tissue quality is a prerequisite for effective wound healing. Within the well-established TIME framework for wound healing, tissue management is the first and most critical therapeutic priority [22]. Debridement, the removal of devitalized tissue to restore a healing-conducive wound environment, is the first and probably most fundamental part of wound bed preparation [2]. This fact led some wound specialists to use the acronym DIME instead of TIME, replacing Tissue with Debridement [23,24]. On one hand, surgical debridement provides rapid and effective removal of necrotic tissue but is inherently limited by patient tolerance, clinical context, and the risk of collateral damage to viable tissue [2,10]. On the other hand, physiological selective debridement, although more patient-friendly, is slower and dormant in stagnated wounds. Available solutions for wound bed preparation include agents that condition the wound for physiologic debridement (e.g., hydrocolloids, hydrogels), enzymatic dressings (e.g., collagenase), or biological debridement (maggot therapy) [2,9].
Each of these approaches has its pros and cons. In stagnant wounds, one cannot rely on physiological wound debridement; direct stimulation of the debridement mechanisms is mandatory. Copper induces autolytic and enzymatic mechanisms that rely on endogenous proteolytic enzymes, macrophage activity, and regulated inflammatory signaling[10] as shown in the current cases, right after initiating COD therapy.
Figure 6 depicts the molecular and cellular mechanisms through which COD promote active physiological wound debridement.
At the extracellular level, copper ions modulate matrix metalloproteinase activity, particularly MMP-2 (gelatinase A) and MMP-9 (gelatinase B), enzymes central to the degradation of denatured collagen, fibrin, and necrotic extracellular matrix components. Copper exposure shifts the balance between MMPs and their endogenous inhibitors, tissue inhibitors of metalloproteinases (TIMP-1 and TIMP-2), favoring regulated proteolysis required for effective clearance of devitalized tissue while preventing excessive matrix destruction [3,25,26,27].
Concurrently, copper ions are taken up by macrophages predominantly via the high-affinity copper transporter CTR1 (SLC31A1). Intracellular copper trafficking is mediated by the chaperone ATOX1 and the ATP-dependent copper exporters ATP7A and ATP7B, enabling copper-dependent macrophage activation and functional polarization. This process enhances the expression of key phagocytic receptors, including CD36, MARCO, and Fcγ receptors (FcγR), thereby facilitating efficient recognition and engulfment of necrotic debris and opsonized tissue fragments. At the signaling level, copper modulates inflammatory pathways essential for effective debridement [28,29,30,31].
Copper-dependent regulation of NF-κB signaling leads to controlled induction of downstream cytokines such as TNF-α and IL-1β, supporting macrophage recruitment and protease activation without excessive inflammatory amplification. This regulated inflammatory milieu promotes the activation of additional proteolytic enzymes involved in early wound cleaning, including neutrophil elastase and lysosomal cathepsins, particularly cathepsin B and cathepsin K [3,32,33,34,35,36].
Collectively, these convergent pathways result in efficient physiological wound debridement, characterized by controlled clearance of necrotic tissue and preservation of the wound environment necessary for subsequent healing.
This constellation of enzymatic and receptor-mediated effects is consistent with active initiation of physiological debridement, rather than secondary autolysis resulting from passive wound bed conditioning. Whereas conventional dressings primarily optimize environmental parameters, such as moisture balance and exudate control, to permit endogenous debridement when host biology is intact, we propose that COD actively modulates the wound microenvironment to promote proteolytic activity and macrophage-mediated clearance. This mechanistic distinction provides a biologically grounded explanation for COD's ability to induce effective debridement even in ischemic or biologically inactive wounds, as demonstrated in the presented cases.
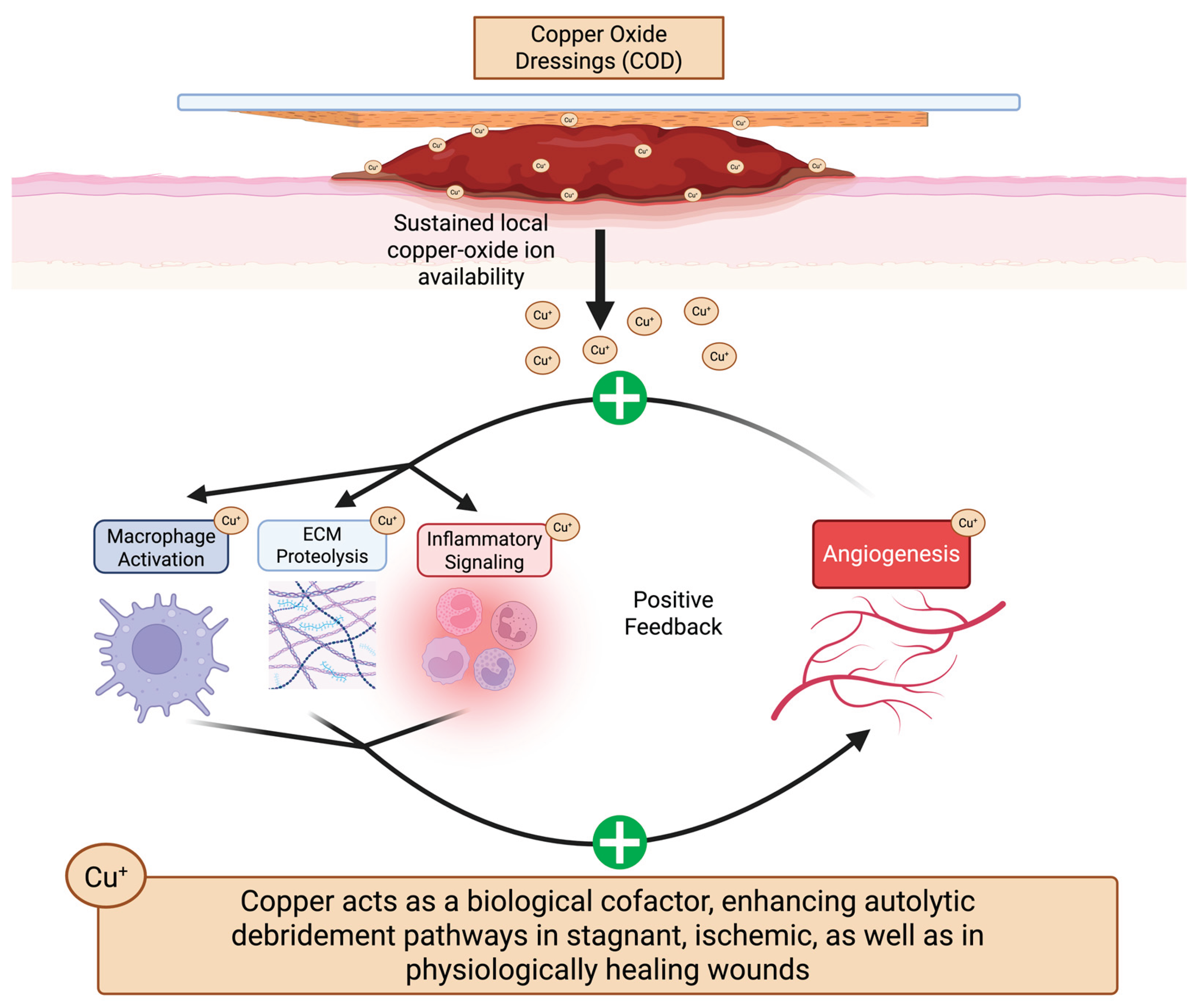
As shown in Figure 7, the present case series suggests that COD induce a coupled, positive feedback loop in which the components of wound debridement (macrophage activation, ECM remodeling, and inflammatory signaling control) and tissue regeneration (angiogenesis) amplify each other. Clinically, this is most clearly reflected by the consistent observation that extensive devitalized tissue is eliminated concurrently with the emergence of dense, well-vascularized granulation tissue, as seen in Cases 2–5 and most strikingly in the ischemic stump in Case 3. This synergy is reflected in the rapid emergence of dense granulation tissue and extracellular matrix formation, which, in turn, provides the biological substrate for the continued production and secretion of autolytic enzymes. This positive feedback loop is reinforced by several copper-dependent biological programs, including matrix remodeling (e.g., MMP–TIMP regulation), controlled inflammatory activation (e.g., NF-κB–mediated signaling), macrophage-mediated clearance, and hypoxia-responsive angiogenesis (e.g., HIF-1α–VEGF signaling) [3,7,8]. The emergence of a systems-level behavior in which COD synchronously reactivate both sides of wound biology, tissue clearance and tissue reconstruction, is probably the reason for the ability of COD to overcome the deadlock typical of hard-to-heal wounds.
The clinical evolution depicted in case 3 supports the concept that COD actively reinitiate physiological debridement in wounds otherwise locked in biological arrest. The baseline condition (Figure 3A–B) reflects a state of complete tissue non-viability, profound ischemia, and absence of inflammatory signaling, a milieu in which endogenous autolysis and immune-mediated clearance are inactive. Following initiation of COD therapy, the early treatment phase (Figure 3C–E) demonstrates reactivation of coordinated wound-healing pathways, with progressive granulation tissue formation occurring alongside enzymatic degradation and removal of necrotic tissue, consistent with concurrent angiogenesis, matrix remodeling, and immune engagement. Nevertheless, at the following dressing change (Figure 3F), we observed increased volumes of thick exudate resembling pus, with no local signs of infection, indicating a positive sign of robust immune response in the wound bed. In the subsequent phase (Figure 3H), the wound stabilizes into a uniformly granulating bed with peripheral displacement of residual debris, indicating resolution of active debridement and restoration of organized tissue regeneration. Collectively, the sequential biological states depicted in Figure 3A–H illustrate a copper-driven synergy capable of reactivating wound biology despite severe ischemic constraints.
Case 4 demonstrates a similar pattern, with progressive replacement of eschar and necrotic tissue by granulation tissue over time. A comparable synergistic interaction between debridement and granulation tissue formation is further illustrated in Case 5, depicting a patient with long-standing diabetes mellitus and mangled extremities. No wound progression was observed with abundant devitalized tissue; after two weeks, despite conventional surgical and medical treatment, bilateral lower-limb amputation was mandated. COD therapy was initiated, and healing progressed rapidly, showing >90% granulation tissue in both legs after two weeks. Notably, at the first dressing change, thick exudate resembling pus was noted, representing emergence from stagnation.
Large and complex wounds are increasingly treated with negative pressure wound therapy (NPWT), which primarily promotes angiogenesis and exudate management but lacks inherent debridement activity. In such wounds, COD may offer enhanced biological activity by directly augmenting debridement. Although a randomized controlled study showed COD to be non-inferior to NPWT, it included diabetic foot patients after surgical debridement (partial foot amputation) [16]. It may be hypothesized that in wounds containing nonviable tissue, COD could confer an advantage over NPWT due to its debridement capabilities.
Limitations
The conclusions presented in this manuscript are derived from a retrospective analysis of a small number of extreme clinical cases and are therefore descriptive in nature; and causal inference cannot be established. Although the prolonged period of wound stagnation prior to initiation of COD provided an internal comparison, this does not substitute for formal controls. Proposed mechanistic interpretations are grounded in established biological literature and inferred from observed clinical behavior rather than direct molecular or histological measurements and should be regarded as hypothesis-generating. Prospective controlled studies are required to further validate the proposed biological model.
5. Conclusions
COD appear to actively enhance autolytic debridement through engagement of endogenous enzymatic and cellular pathways, rather than passively conditioning the wound environment. Debridement is coupled with angiogenesis and granulation tissue formation, creating a self-reinforcing biological loop in which improved perfusion further amplifies tissue clearance. This multimodal mechanism enables effective debridement in severely compromised wounds, including those with extensive necrosis, ischemia, or poor systemic reserve. Clinically, COD may reduce or partially substitute the need for sharp or surgical debridement, offering a non-surgical therapeutic option in complex wound management.
Author Contributions
Conceptualization, E.M.; methodology, E.M.; validation, E.M. and I.C.; formal analysis, E.M. and I.C.; investigation, E.M.; resources, E.M.; data curation, I.C.; writing—original draft preparation, E.M. and I.C.; writing—review and editing, E.M. and I.C.; visualization, I.C.; supervision, E.M.; project administration, E.M.; funding acquisition, not applicable. All authors have read and agreed to the published version of the manuscript.
Funding
The study has received no financial funding. MedCu Provided dressing samples for use during routine clinical care at an early stage of clinical availability.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to the retrospective case report nature of the publication. Nevertheless, all patients, or their legal representatives when applicable, provided informed consent for treatment with COD and for the use of anonymized clinical data and images for academic publication, in accordance with institutional ethical standards and the Declaration of Helsinki. No electronic laboratory notebook platform was used.
Informed Consent Statement
All patients, or their legal representatives when applicable, provided informed consent for treatment with COD and for the use of anonymized clinical data and images for academic publication.:
Data Availability Statement
not applicable.
Acknowledgments
The authors would like to thank Dr. Jihad Dabbah for sharing with us cases 4 and 5.
Conflicts of Interest
Eyal Melamed is a medical member of the advisory board and a minor shareholder of MedCu, the manufacturer of the copper oxide dressings discussed in this manuscript. Ithamar Cheyne declares no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| APLA | Antiphospholipid Antibody Syndrome |
| ATP7A | ATPase Copper Transporting Alpha |
| ATP7B | ATPase Copper Transporting Beta |
| ATOX1 | Antioxidant Protein 1 (Copper Chaperone) |
| CD36 | Cluster of Differentiation 36 |
| CDP | Copper-Dependent Pathways |
| COD | Copper Oxide Dressings |
| CTR1 (SLC31A1) | Copper Transporter 1 |
| ECM | Extracellular Matrix |
| FcγR | Fc Gamma Receptor |
| HIF-1α | Hypoxia-Inducible Factor 1 Alpha |
| ICU | Intensive Care Unit |
| IKK | IκB Kinase |
| IL-1β | Interleukin 1 Beta |
| MARCO | Macrophage Receptor with Collagenous Structure |
| MMP | Matrix Metalloproteinase |
| MMP-2 | Matrix Metalloproteinase-2 (Gelatinase A) |
| MMP-9 | Matrix Metalloproteinase-9 (Gelatinase B) |
| NF-κB | Nuclear Factor Kappa B |
| NPWT | Negative Pressure Wound Therapy |
| PDGF | Platelet-Derived Growth Factor |
| TIMP | Tissue Inhibitor of Metalloproteinases |
| TIMP-1 | Tissue Inhibitor of Metalloproteinases-1 |
| TIMP-2 | Tissue Inhibitor of Metalloproteinases-2 |
| TNF-α | Tumor Necrosis Factor Alpha |
| VEGF | Vascular Endothelial Growth Factor |
References
- Halim, A.S.; Khoo, T.L.; Saad, A.Z. Wound Bed Preparation from a Clinical Perspective. Indian Journal of Plastic Surgery 2012, 45, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.C.; Tsu, C.L.; Nain, R.A. The Role of Debridement in Wound Bed Preparation in Chronic Wound: A Narrative Review. Annals of Medicine and Surgery 2021, 71, 102876. [Google Scholar] [CrossRef]
- Borkow, G.; Gabbay, J.; Dardik, R.; Eidelman, A.I.; Lavie, Y.; Grunfeld, Y.; Ikher, S.; Huszar, M.; Zatcoff, R.C.; Marikovsky, M. Molecular Mechanisms of Enhanced Wound Healing by Copper Oxide-Impregnated Dressings. Wound Repair and Regeneration 2010, 18, 266–275. [Google Scholar] [CrossRef]
- White, C.; Lee, J.; Kambe, T.; Fritsche, K.; Petris, M.J. A Role for the ATP7A Copper-Transporting ATPase in Macrophage Bactericidal Activity. Journal of Biological Chemistry 2009, 284, 33949–33956. [Google Scholar] [CrossRef] [PubMed]
- Uriu-Adams, J.Y.; Keen, C.L. Copper, Oxidative Stress, and Human Health. Mol. Aspects Med. 2005, 26, 268–298. [Google Scholar] [CrossRef]
- Percival, S. Copper and Immunity. Am. J. Clin. Nutr. 1998, 67, 1064S–1068S. [Google Scholar] [CrossRef] [PubMed]
- Borkow, G.; Cheyne, I.; Melamed, E. Copper Dressings as Part of the Armamentarium in the Fight against Wounds – Much More than an Antimicrobial. Wound Healing Southern Africa 2024, 17, 38–40. [Google Scholar] [CrossRef]
- Cheyne, I.; Rybka, M.; Mazurek, Ł.; Jurak, J.; Konop, M. Shifting the Clinical Paradigm: Copper versus Silver Wound Dressings - Where We Are and What We Are Looking For. J. Biomater. Appl. 2025. [Google Scholar] [CrossRef]
- Amadeh, A.; Mohebbi, N.; Amadeh, Z. others Comparative Efficacy of Autolytic and Collagenase-Based Enzymatic Debridement in Chronic Wound Healing: A Comprehensive Systematic Review. Int. Wound J. 2025, 22, e70177. [Google Scholar] [CrossRef]
- Atkin, L. Understanding Methods of Wound Debridement. British Journal of Nursing 2014, 23, S10–S15. [Google Scholar] [CrossRef]
- Borkow, G.; Melamed, E. The Journey of Copper-Impregnated Dressings in Wound Healing: From a Medical Hypothesis to Clinical Practice. Biomedicines 2025, 13, 562. [Google Scholar] [CrossRef]
- Borkow, G.; Melamed, E. Copper, an Abandoned Player Returning to the Wound Healing Battle. In Recent Advances in Wound Healing; IntechOpen, 2022. [Google Scholar]
- Borkow, G.; Melamed, E. Multi-Function Modality of Copper Dressings in Managing Hard-to-Heal Wounds. J. Wound Care 2026. [Google Scholar] [CrossRef]
- Bogadi, S.; Uddin, M.E.; Karri, V. others Therapeutic Potential of Copper II Oxide in Treating Diabetic Wounds: An Emerging Approach for Enhanced Healing. Acta Diabetol. 2025. [Google Scholar] [CrossRef] [PubMed]
- Melamed, E.; Borkow, G. Continuum of Care in Hard-to-Heal Wounds by Copper Dressings: A Case Series. J. Wound Care 2023, 32, 788–796. [Google Scholar] [CrossRef]
- Melamed, E.; Dabbah, J.; Israel, T.; Kan, I.; Pinzur, M.S.; Roth, T.; Borkow, G. Noninferiority of Copper Dressings Than Negative Pressure Wound Therapy in Healing Diabetic Wounds: A Randomized Clinical Trial. In Adv. Wound Care (New Rochelle).; 2025. [Google Scholar] [CrossRef]
- Melamed, E.; Kiambi, P.; Okoth, D.; Honigber, I.; Tamir, E.; Borkow, G. Healing of Chronic Wounds by Copper Oxide-Impregnated Wound Dressings—Case Series. Medicina (B Aires). 2021, 57, 296. [Google Scholar] [CrossRef]
- Melamed, E.; Rovitsky, A.; Roth, T.; Assa, L.; Borkow, G. Stimulation of Healing of Non-Infected Stagnated Diabetic Wounds by Copper Oxide-Impregnated Wound Dressings. Medicina (B Aires). 2021, 57, 1129. [Google Scholar] [CrossRef]
- Melamed, E.; Rovitsky, A.; Roth, T.; Borkow, G. Anterior Ankle Full Thickness Skin Necrosis Treated with Copper Oxide Dressings without Debridement and Skin Grafting – A Case Report. Arch. Clin. Med. Case Rep. 2022, 06. [Google Scholar] [CrossRef]
- Gorel, O.; Hamuda, M.; Feldman, I.; Kucyn-Gabovich, I. Enhanced Healing of Wounds That Responded Poorly to Silver Dressing by Copper Wound Dressings: Prospective Single Arm Treatment Study. Health Sci. Rep. 2024, 7. [Google Scholar] [CrossRef] [PubMed]
- Chausha Weitman, C.; Roth, T.; Borkow, G. Copper Dressings to the Wound Rescue after Everything Else Failed: Case Report. Arch. Clin. Med. Case Rep. 2022, 06. [Google Scholar] [CrossRef]
- Harries, R.L.; Bosanquet, D.C.; Harding, K.G. Wound Bed Preparation: TIME for an Update. Int. Wound J. 2016, 13, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Giaquinto-Cilliers, M.G.C.; Nair, A.; Von Pressentin, K.B.; others. A “Game of Dressings”: Strategies for Wound Management in Primary Health Care. South African Family Practice 2022, 64, e1–e8. [Google Scholar] [CrossRef] [PubMed]
- Lauerman, M.H.; Scalea, T.M.; Eglseder, W.A. others Efficacy of Wound Coverage Techniques in Extremity Necrotizing Soft Tissue Infections. American Surgeon 2018, 84, 1790–1795. [Google Scholar] [CrossRef] [PubMed]
- Philips, N.; Hwang, H.; Chauhan, S.; Leonardi, D.; Gonzalez, S. Stimulation of Cell Proliferation and Expression of Matrixmetalloproteinase-1 and Interluekin-8 Genes in Dermal Fibroblasts by Copper. Connect. Tissue Res. 2010, 51, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Ogen-Shtern, N.; Chumin, K.; Silberstein, E.; Borkow, G. Copper Ions Ameliorated Thermal Burn-Induced Damage in Ex Vivo Human Skin Organ Culture. Skin Pharmacol. Physiol. 2021, 34, 317–327. [Google Scholar] [CrossRef]
- Caley, M.P.; Martins, V.L.C.; O’Toole, E.A. Metalloproteinases and Wound Healing. Adv. Wound Care (New Rochelle). 2015, 4, 225–234. [Google Scholar] [CrossRef]
- Fukai, T.; Ushio-Fukai, M.; Kaplan, J.H. Copper Transporters and Copper Chaperones: Roles in Cardiovascular Physiology and Disease. American Journal of Physiology-Cell Physiology 2018, 315, C186–C201. [Google Scholar] [CrossRef]
- Stafford, S.L.; Bokil, N.J.; Achard, M.E.S.; Kapetanovic, R.; Schembri, M.A.; McEwan, A.G.; Sweet, M.J. Metal Ions in Macrophage Antimicrobial Pathways: Emerging Roles for Zinc and Copper. Biosci. Rep. 2013, 33. [Google Scholar] [CrossRef]
- Flemming, A. Copper Boosts Pro-Inflammatory State of Macrophages. Nat. Rev. Immunol. 2023, 23, 344–344. [Google Scholar] [CrossRef]
- White, C.; Lee, J.; Kambe, T.; Fritsche, K.; Petris, M.J. A Role for the ATP7A Copper-Transporting ATPase in Macrophage Bactericidal Activity. Journal of Biological Chemistry 2009, 284, 33949–33956. [Google Scholar] [CrossRef]
- Vidak, E.; Javoršek, U.; Vizovišek, M.; Turk, B. Cysteine Cathepsins and Their Extracellular Roles: Shaping the Microenvironment. Cells 2019, 8, 264. [Google Scholar] [CrossRef]
- Chevriaux, A.; Pilot, T.; Derangère, V.; Simonin, H.; Martine, P.; Chalmin, F.; Ghiringhelli, F.; Rébé, C. Cathepsin B Is Required for NLRP3 Inflammasome Activation in Macrophages, Through NLRP3 Interaction. Front. Cell Dev. Biol. 2020, 8. [Google Scholar] [CrossRef] [PubMed]
- Korkmaz, B.; Horwitz, M.S.; Jenne, D.E.; Gauthier, F. Neutrophil Elastase, Proteinase 3, and Cathepsin G as Therapeutic Targets in Human Diseases. Pharmacol. Rev. 2010, 62, 726–759. [Google Scholar] [CrossRef] [PubMed]
- Ganapathy, N.; Venkataraman, S.S.; Daniel, R.; Aravind, R.J.; Kumarakrishnan, V.B. Molecular Biology of Wound Healing. J. Pharm. Bioallied Sci. 2012, 4, S334–7. [Google Scholar] [CrossRef]
- Guo, H.; Jing, L.; Xia, C.; Zhu, Y.; Xie, Y.; Ma, X.; Fang, J.; Wang, Z.; Zuo, Z. Copper Promotes LPS-Induced Inflammation via the NF-КB Pathway in Bovine Macrophages. Biol. Trace Elem. Res. 2024, 202, 5479–5488. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Sequential images demonstrate progressive debridement of a chronic (eight-year) venous leg ulcer in a patient with antiphospholipid antibody syndrome (APLA). (A) Baseline appearance of the wound, measuring approximately 185 × 120 mm, predominantly covered by fibrinous and devitalized tissue. (B) One week after initiation of copper oxide dressings (COD). Partial clearance of non-viable tissue with early foci of granulation tissue is observed. (C) Four weeks after COD initiation, the wound bed is largely covered by granulation tissue, with thin residual fibrinous tissue over the medial malleolus.
Figure 1.
Sequential images demonstrate progressive debridement of a chronic (eight-year) venous leg ulcer in a patient with antiphospholipid antibody syndrome (APLA). (A) Baseline appearance of the wound, measuring approximately 185 × 120 mm, predominantly covered by fibrinous and devitalized tissue. (B) One week after initiation of copper oxide dressings (COD). Partial clearance of non-viable tissue with early foci of granulation tissue is observed. (C) Four weeks after COD initiation, the wound bed is largely covered by granulation tissue, with thin residual fibrinous tissue over the medial malleolus.
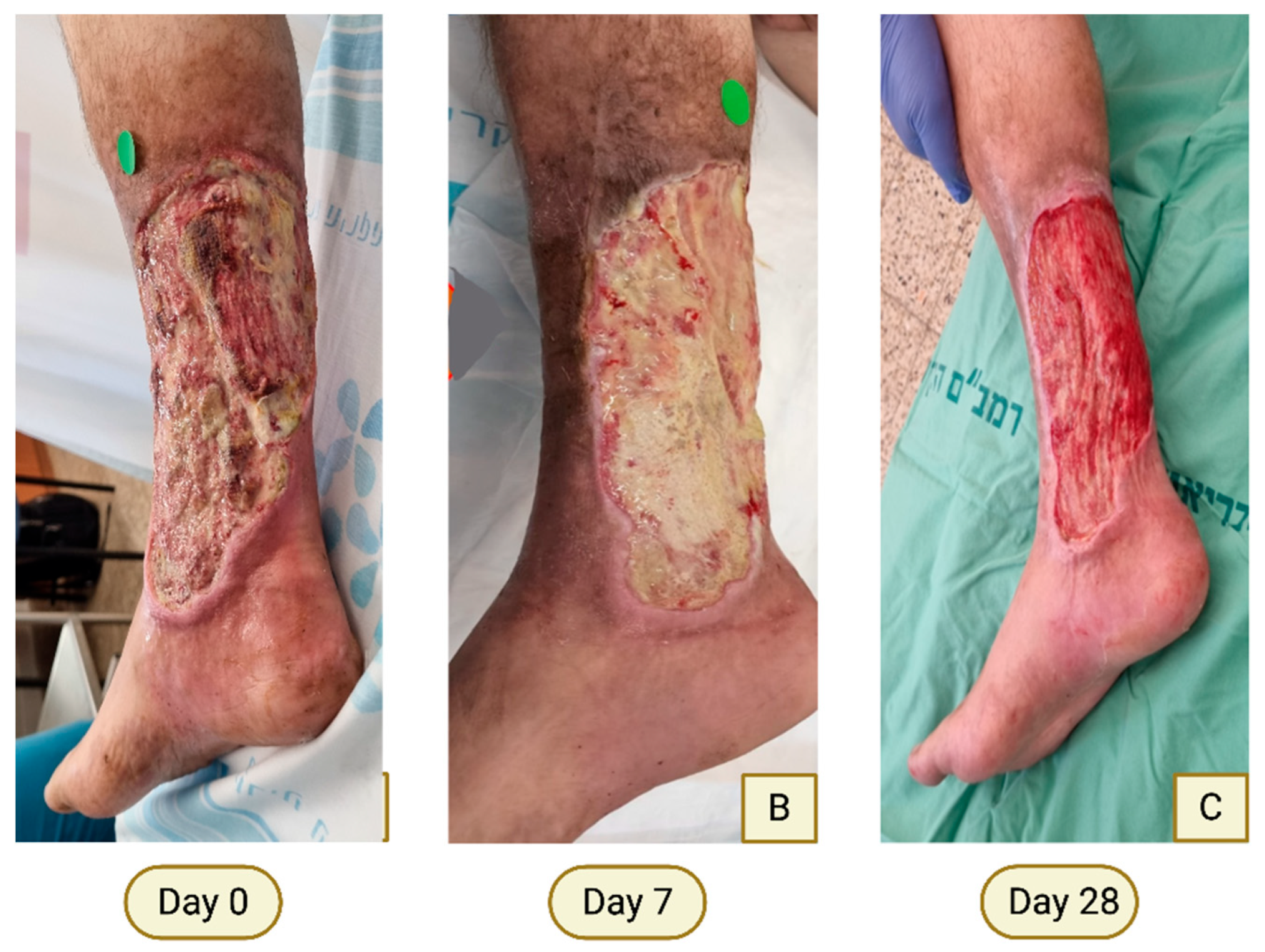
Figure 2.
Progressive marginal and central debridement with granulation following COD therapy. (A) At presentation, the amputation stump shows partial central granulation surrounded by necrotic and ischemic wound margins. (B–C) Early changes within several days of COD initiation, including increased central granulation and clearer demarcation between viable and non-viable tissue. (D) Day 27: White dashed lines outline necrotic wound margins prior to bedside intervention. (E) Immediate appearance following limited bedside sharp marginal debridement (~2 mm) to prevent pain and preserve viable skin. (F) Resolution of previously necrotic areas (dashed lines). (G) Day 50: Fully viable wound margins with complete granulation tissue coverage, allowing delayed primary closure (H).
Figure 2.
Progressive marginal and central debridement with granulation following COD therapy. (A) At presentation, the amputation stump shows partial central granulation surrounded by necrotic and ischemic wound margins. (B–C) Early changes within several days of COD initiation, including increased central granulation and clearer demarcation between viable and non-viable tissue. (D) Day 27: White dashed lines outline necrotic wound margins prior to bedside intervention. (E) Immediate appearance following limited bedside sharp marginal debridement (~2 mm) to prevent pain and preserve viable skin. (F) Resolution of previously necrotic areas (dashed lines). (G) Day 50: Fully viable wound margins with complete granulation tissue coverage, allowing delayed primary closure (H).
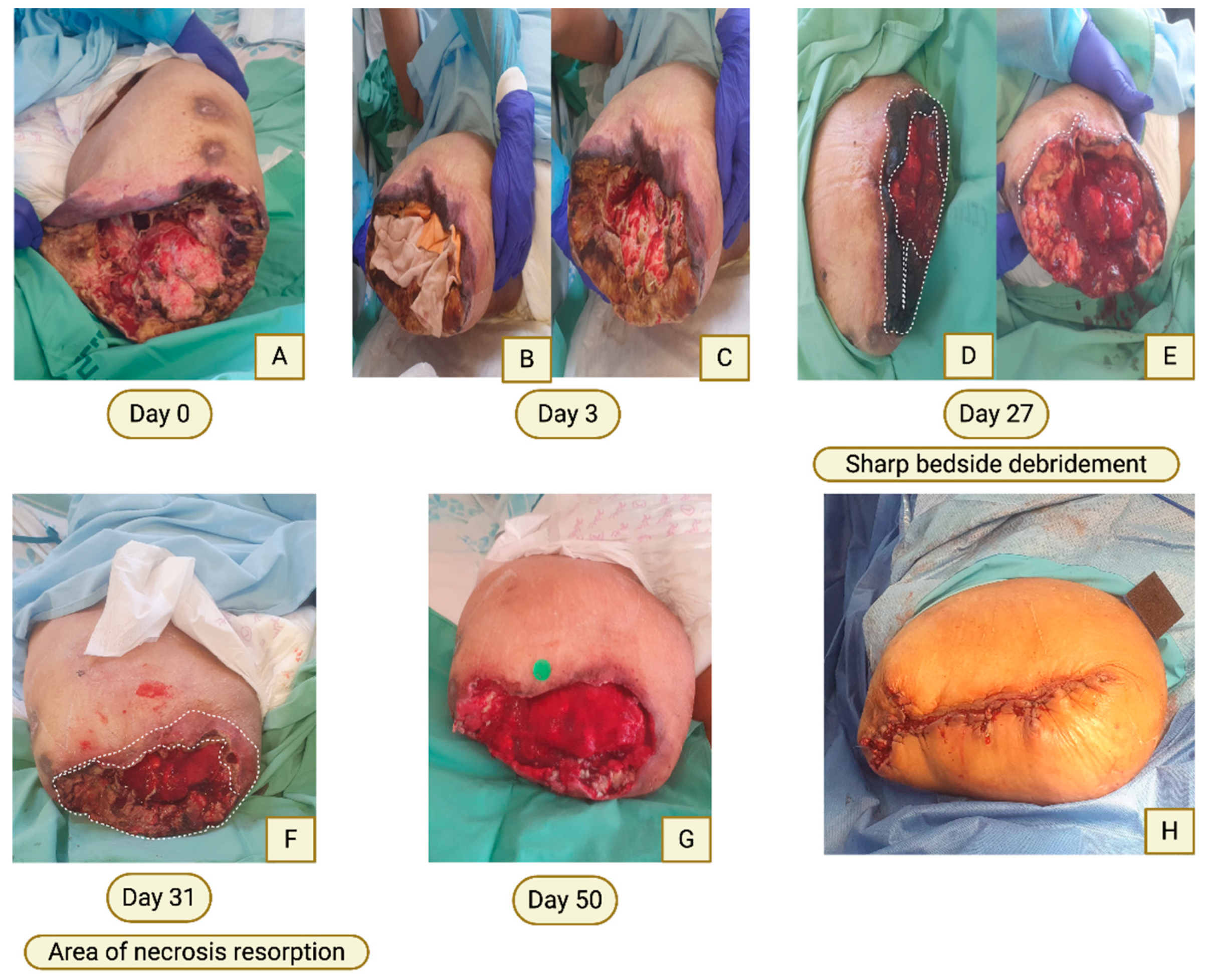
Figure 3.
Sequential images demonstrate a transition from ischemic, biologically inactive tissue to robust granulation with a controlled inflammatory response. (A–B) Trans-femoral amputation stump in a critically ill patient following coronary artery bypass surgery. Before and after suture removal, showing an entirely non-viable stump with extensive devitalized tissue, exposed bone, and absence of surrounding erythema or edema. (C–E) Bi-weekly COD dressing changes demonstrating progressive replacement of necrotic tissue by granulation tissue, including involvement of exposed bone marrow (arrowheads). (F-G) Day 14 (fourth dressing change): Purulent-appearing discharge within the wound bed, without accompanying clinical signs of infection (no thigh swelling or erythema; white arrows indicate preserved skin wrinkling). (H) Three days later, resolution of discharge with a dry wound bed, solid and organized granulation tissue, and clean, viable margins. Residual surface debris, presumed microbial, appears displaced toward the wound margins (white arrows).
Figure 3.
Sequential images demonstrate a transition from ischemic, biologically inactive tissue to robust granulation with a controlled inflammatory response. (A–B) Trans-femoral amputation stump in a critically ill patient following coronary artery bypass surgery. Before and after suture removal, showing an entirely non-viable stump with extensive devitalized tissue, exposed bone, and absence of surrounding erythema or edema. (C–E) Bi-weekly COD dressing changes demonstrating progressive replacement of necrotic tissue by granulation tissue, including involvement of exposed bone marrow (arrowheads). (F-G) Day 14 (fourth dressing change): Purulent-appearing discharge within the wound bed, without accompanying clinical signs of infection (no thigh swelling or erythema; white arrows indicate preserved skin wrinkling). (H) Three days later, resolution of discharge with a dry wound bed, solid and organized granulation tissue, and clean, viable margins. Residual surface debris, presumed microbial, appears displaced toward the wound margins (white arrows).
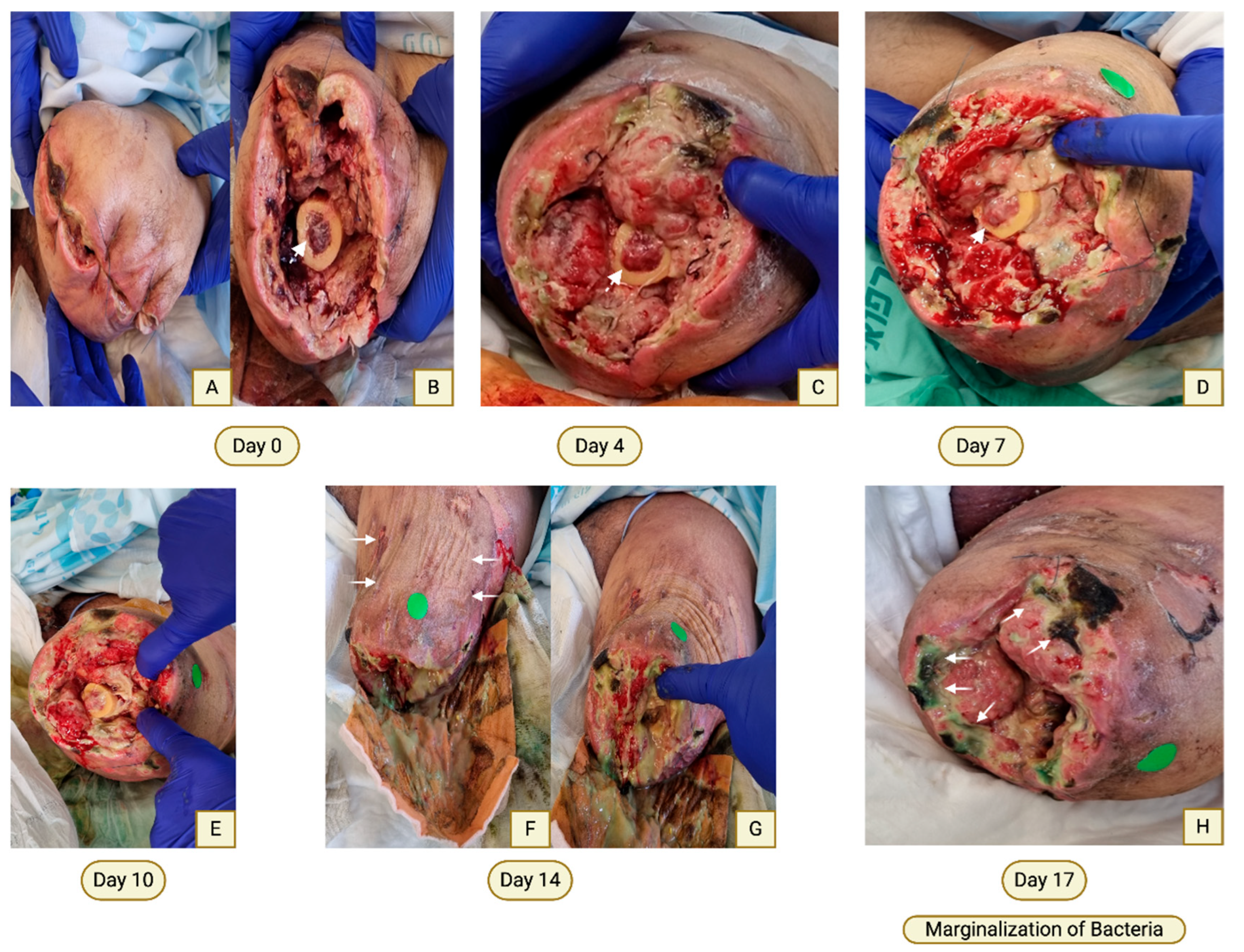
Figure 4.
Clinical course following electrical injury to the left foot. (A) Two weeks post-injury, extensive necrosis involving the dorsal foot and toes. COD treatment was initiated. (B) Evolution to eschar formation with subsequent middle toes amputation. (C) After four additional weeks of COD therapy, progressive autolytic debridement with replacement by dense, well-vascularized granulation tissue. (D) Definitive surgical management: Trans- metatarsal amputation with preservation of plantar skin and split-thickness skin grafting onto a well-prepared wound bed. (E–F) Complete graft take at two weeks and two months post-grafting. (G) Corresponding radiographic image.
Figure 4.
Clinical course following electrical injury to the left foot. (A) Two weeks post-injury, extensive necrosis involving the dorsal foot and toes. COD treatment was initiated. (B) Evolution to eschar formation with subsequent middle toes amputation. (C) After four additional weeks of COD therapy, progressive autolytic debridement with replacement by dense, well-vascularized granulation tissue. (D) Definitive surgical management: Trans- metatarsal amputation with preservation of plantar skin and split-thickness skin grafting onto a well-prepared wound bed. (E–F) Complete graft take at two weeks and two months post-grafting. (G) Corresponding radiographic image.
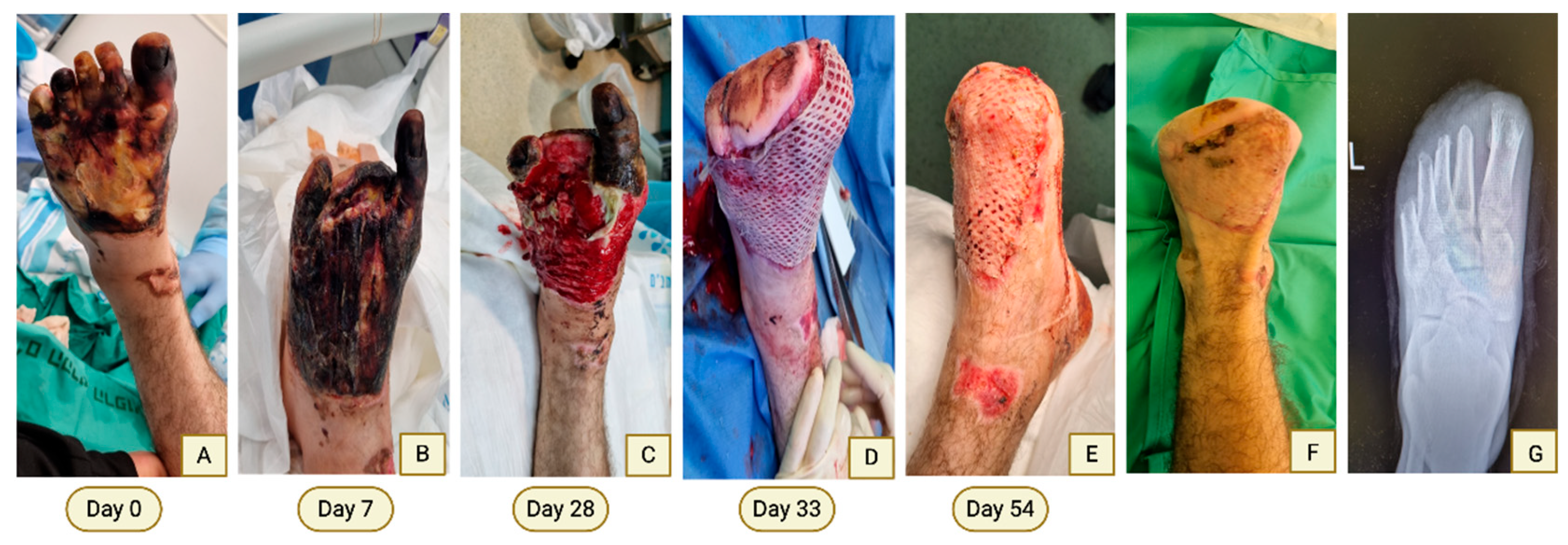
Figure 5.
Progressive debridement and wound bed reactivation following COD therapy in a contaminated open fracture. (A) Day 0: Extensive soft tissue devitalization following high- energy open fracture with severe contamination. (B) CT angiography demonstrates skeletal injury with preserved arterial perfusion. (C) Day 14: Persistent devitalized tissue despite prior surgical debridement and antiseptic wound care. (D) Day 28: Marked replacement of necrotic tissue by dense granulation tissue following COD therapy. (E) Day 40: Well- vascularized wound bed suitable for skin grafting. (F) Long-term follow-up demonstrating stable wound closure and limb preservation.
Figure 5.
Progressive debridement and wound bed reactivation following COD therapy in a contaminated open fracture. (A) Day 0: Extensive soft tissue devitalization following high- energy open fracture with severe contamination. (B) CT angiography demonstrates skeletal injury with preserved arterial perfusion. (C) Day 14: Persistent devitalized tissue despite prior surgical debridement and antiseptic wound care. (D) Day 28: Marked replacement of necrotic tissue by dense granulation tissue following COD therapy. (E) Day 40: Well- vascularized wound bed suitable for skin grafting. (F) Long-term follow-up demonstrating stable wound closure and limb preservation.

Figure 6.
Schematic representation of proposed mechanisms by which copper oxide dressings (COD) promote active physiological wound debridement. COD provide sustained local release of copper ions (Cu⁺), which modulate extracellular matrix proteolysis through regulation of MMP–TIMP balance, enhance macrophage activation and phagocytic clearance of necrotic tissue via copper-dependent transport pathways, and regulate NF-κB–mediated inflammatory signaling. Collectively, these coordinated processes facilitate controlled clearance of devitalized tissue while preserving a wound environment conducive to subsequent healing.
Figure 6.
Schematic representation of proposed mechanisms by which copper oxide dressings (COD) promote active physiological wound debridement. COD provide sustained local release of copper ions (Cu⁺), which modulate extracellular matrix proteolysis through regulation of MMP–TIMP balance, enhance macrophage activation and phagocytic clearance of necrotic tissue via copper-dependent transport pathways, and regulate NF-κB–mediated inflammatory signaling. Collectively, these coordinated processes facilitate controlled clearance of devitalized tissue while preserving a wound environment conducive to subsequent healing.
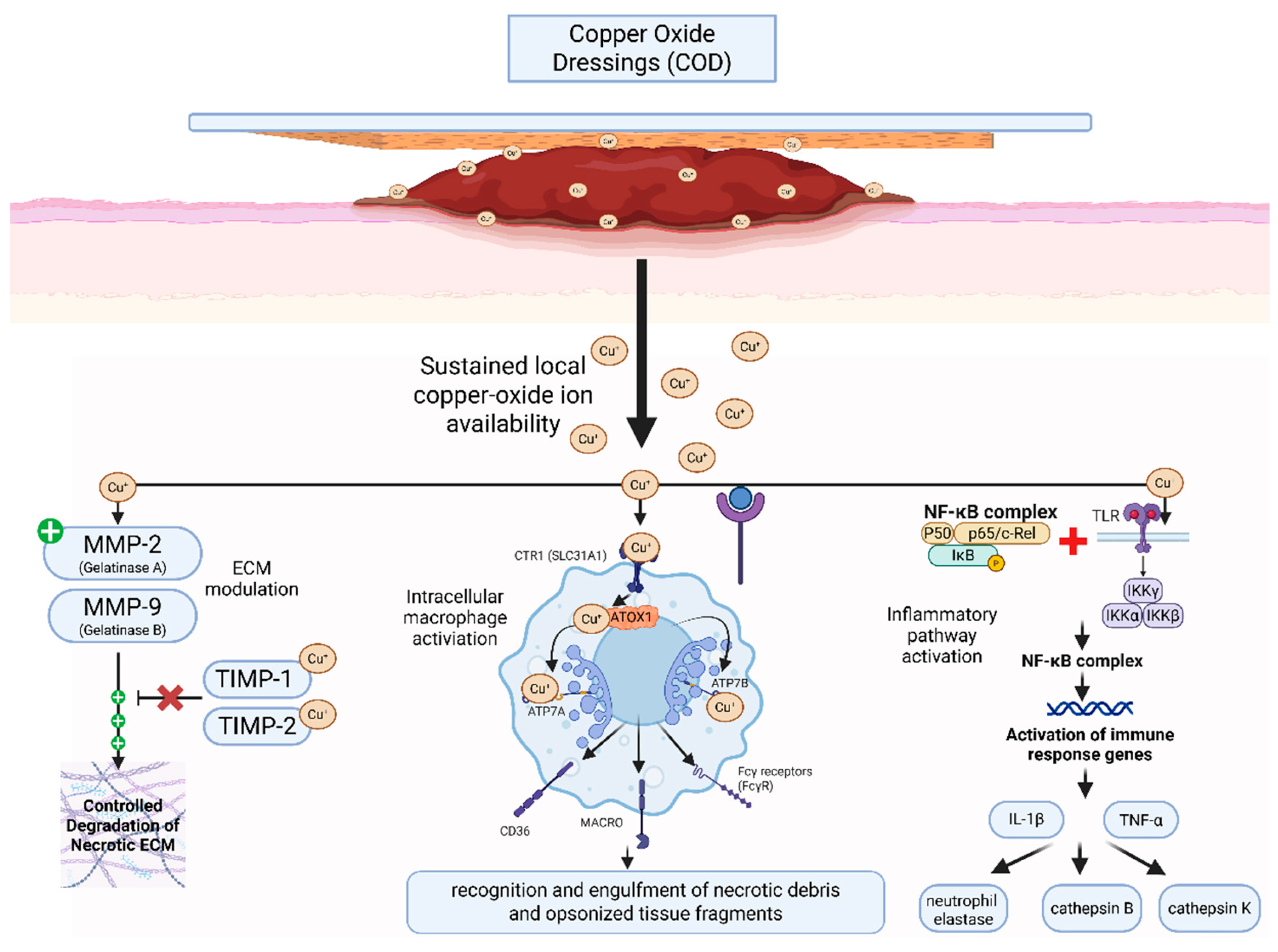
Figure 7.
Copper cations appear to engage multiple interconnected molecular and cellular pathways involved in necrotic tissue autolysis. By modulating extracellular matrix remodeling via the MMP–TIMP axis, activating controlled inflammatory signaling via NF-κB, and polarizing macrophages, copper cations enhance the debridement response. Beyond their direct role in physiological debridement, COD and copper cations promote angiogenesis, creating a synergistic interaction in which improved perfusion and tissue regeneration further amplify autolytic tissue clearance. In contrast, conventional debriding dressings (e.g., hydrocolloids) only permit passive autolysis, which is usually insufficient in hard-to-heal wounds, and act slowly in physiological wounds.
Figure 7.
Copper cations appear to engage multiple interconnected molecular and cellular pathways involved in necrotic tissue autolysis. By modulating extracellular matrix remodeling via the MMP–TIMP axis, activating controlled inflammatory signaling via NF-κB, and polarizing macrophages, copper cations enhance the debridement response. Beyond their direct role in physiological debridement, COD and copper cations promote angiogenesis, creating a synergistic interaction in which improved perfusion and tissue regeneration further amplify autolytic tissue clearance. In contrast, conventional debriding dressings (e.g., hydrocolloids) only permit passive autolysis, which is usually insufficient in hard-to-heal wounds, and act slowly in physiological wounds.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



