
Submitted:
26 January 2026
Posted:
27 January 2026
You are already at the latest version
Abstract
Background. Cardiorenometabolic syndrome (CRMS) reflects the interaction between heart failure (HF), chronic kidney disease, and metabolic disorders. Its prognostic impact during the acute phase of HF remains poorly defined. The primary objective of this study was to assess whether severe CRMS (sCRMS: estimated glomerular filtration rate < 45 mL/min/1.73 m² associated with type 2 diabetes mellitus and/or obesity) predicts worse clinical outcomes.
Methods. Retrospective observational study of a prospective cohort including 2,228 patients admitted for acute HF between 2015 and 2025. Clinical characteristics and outcomes (mortality, HF readmission, and the composite endpoint) were compared between patients with and without sCRMS.
Results. sCRMS was present in 486 patients (21,8%) who were older, had worse functional class, and a higher burden of cardiovascular comorbidities. They presented more frequently with systemic congestion and less often with de novo HF. During follow-up, sCRMS was associated with higher mortality (29.4% vs 18.4%), HF readmissions (56.2% vs 33.5%), and the composite endpoint (85.6% vs 51.9%) (all p< 0.001). In multivariable analysis, sCRMS remained an independent predictor of mortality (HR 1.25), readmissions (HR 1.24), and overall morbidity and mortality (HR 1.20).
Conclusions. In patients hospitalized for acute HF, sCRMS consistently identified a high-risk clinical phenotype with an unfavorable prognosis. These findings support the value of sCRMS as a simple and reproducible prognostic marker and highlight the need for integrated cardiorenometabolic strategies during post-discharge follow-up.
Keywords:
acute heart failure
; cardiorenometabolic syndrome
; cardiorenal syndrome
; prognosis
1. Introduction
Cardiorenometabolic syndrome (CRMS) describes the bidirectional and self-perpetuating interaction among the cardiovascular, renal, and metabolic systems. In 2023, the American Heart Association (AHA) unified this concept under the term Cardiovascular–Kidney–Metabolic (CKM) syndrome, established staging criteria, and emphasized that the coexistence of heart failure (HF), chronic kidney disease (CKD), and metabolic factors (type 2 diabetes mellitus [T2DM] and obesity) markedly increases mortality and hospital readmissions [1,2]. Recent reviews confirm that these three axes share inflammatory, neurohormonal, and oxidative stress pathways, which explains how frequently they coexist in the same patient [2].
Acute cardiorenal syndrome (CRS type 1), defined as acute kidney injury secondary to cardiac decompensation, is common (≈30–50%) among patients hospitalized for acute HF and is associated with a worse prognosis [3]. In the setting of acute HF, convergence of CRMS is not uncommon: contemporary registries report CKD in approximately 40% of patients and T2DM or obesity in more than 50% of admissions [4,5], with a negative impact on survival and quality of life.
However, despite the growing relevance of this integrated view in prevention and outpatient management, important knowledge gaps remain in the acute phase of HF, and most CRMS series derive from outpatient or CKD cohorts. There is a lack of analyses specifically focused on the in-hospital phase, where pathophysiology and therapeutic opportunities differ. Moreover, most studies continue to evaluate renal dysfunction and metabolic factors in isolation, without assessing their combined effect, and with heterogeneity in the definition of CRMS.
The study hypothesis was that, in patients with acute HF, the severe CRMS phenotype (sCRMS) would be associated with a higher frequency of major outcomes (mortality and readmissions) compared with patients without this combined metabolic and renal profile, and that specific clinical characteristics might allow risk stratification and help guide future therapeutic interventions during follow-up.
The primary objective of the study was to assess whether the sCRMS phenotype (glomerular filtration rate [GFR] <45 mL/min/1.73 m² plus T2DM or obesity) predicts worse clinical outcomes (mortality or HF readmission) in a large cohort of patients with acute HF. Secondary objectives were to determine the prevalence of sCRMS in acute HF, compare clinical, laboratory, and therapeutic characteristics between patients with and without this phenotype, and analyze predictors of morbidity and mortality.
2. Materials and Methods
This was a retrospective study based on a database of patients consecutively admitted for an episode of acute HF to the Cardiology Department of a tertiary care hospital. Data were collected prospectively during hospitalization and subsequently extracted and curated by a team of cardiologists specialized in HF. Recruitment was consecutive over a 10-year period (July 2015–July 2025), with a total of 3,406 episodes of acute HF recorded. Elective admissions for planned procedures, transfers from other hospitals, and episodes with insufficient data to calculate estimated glomerular filtration rate (eGFR), ascertain the presence of T2DM, or determine body mass index (BMI) were excluded.
A total of 2,228 patients were included in the analysis: 486 with sCRMS and 1,742 without this syndrome.
For the present analysis, the sCRMS phenotype was defined as an eGFR <45 mL/min/1.73 m² at admission together with the presence of T2DM or a diagnosis of obesity (BMI ≥30 kg/m² or documented in the medical record).
The diagnosis of acute HF was established according to European guideline criteria, based on the presence of signs and/or symptoms of congestion with objective evidence of cardiac dysfunction and the need for intravenous therapy [6].
Variables of interest included clinical, laboratory, and therapeutic data at admission. The main outcome measures were mortality, readmission, and overall morbidity and mortality during follow-up. Patients were censored at death for the readmission analysis.
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Biomedical Research Ethics Committee of Hospital Universitari i Politècnic La Fe, Valencia (protocol code/acronym: SCRMs-HF).
Statistical Analysis
Categorical variables are expressed as percentages, and continuous variables as mean (standard deviation) or median (interquartile range), depending on whether they followed a normal distribution, as assessed by the Kolmogorov–Smirnov test. Group comparisons were performed using the chi-square test with Yates’ correction when appropriate for categorical variables, and Student’s t test or the Mann–Whitney U test for continuous variables with non-normal distribution.
Survival was analyzed using Kaplan–Meier curves, with comparisons performed using the log-rank test. Multivariable survival analysis was conducted using Cox proportional hazards regression, with the sCRMS variable entered as a dichotomous factor. A forward conditional method was used for variable selection. Variables included were those showing statistical significance in univariable analysis or considered clinically relevant. A p value <0.05 was considered statistically significant.
Statistical analyses were performed using IBM SPSS Statistics version 27® and Stata® Statistics/Data Analysis version 16.1. Figures were generated using SPSS and subsequently edited with PowerPoint (Microsoft Office).
3. Results
3.1. Medical History and Clinical Profile
Patients with sCRMS were significantly older, with no relevant differences observed in sex distribution. Regarding underlying heart disease, sCRMS was associated with a higher prevalence of ischemic heart disease and a greater overall burden of cardiovascular comorbidities. In contrast, de novo HF was more frequent among patients without sCRMS.
With respect to prior HF history, patients with sCRMS had a higher number of previous hospitalizations, worse baseline functional class, and a slightly longer length of hospital stay. In addition, the hemodynamic presentation pattern differed between groups: patients with sCRMS more frequently exhibited systemic or mixed congestion, whereas isolated pulmonary congestion predominated in patients without sCRMS (Table 1).
3.2. Prior Treatment and Admission Laboratory Findings
Analysis of prior treatment revealed relevant differences between groups. Although no significant differences were observed in the use of angiotensin-converting enzyme inhibitors (ACEIs), angiotensin II receptor blockers (ARBs), angiotensin receptor–neprilysin inhibitors (ARNIs), or mineralocorticoid receptor antagonists (MRAs), patients with sCRMS more frequently received beta-blockers. Consistently, diuretic use was significantly higher in the sCRMS group, including loop diuretics and other strategies for intensification of diuretic therapy. In addition, these patients showed greater use of antiplatelet agents, nitrates, statins, and calcium channel blockers.
In the metabolic and renal domains, patients with sCRMS had higher use of oral antidiabetic agents, sodium–glucose cotransporter 2 inhibitors (SGLT2i), potassium supplements, hypokalemia-inducing agents, and allopurinol (Table 2).
At the laboratory level, patients with sCRMS had significantly higher values of urea, uric acid, N-terminal pro–B-type natriuretic peptide (NT-proBNP), and high-sensitivity troponin T. On complete blood count, lower hemoglobin and hematocrit levels were observed, with a higher prevalence of anemia. In contrast, no significant differences were found in certain renal and congestion biomarkers, such as carbohydrate antigen 125 (CA-125), cystatin C, or microalbuminuria (Table 3).
3.3. Diagnostic Criteria and Morbidity–Mortality Data
Analysis of diagnostic criteria confirmed that sCRMS is inherently associated with a higher burden of metabolic comorbidities, with a markedly higher prevalence of T2DM and obesity. From a renal function perspective, patients with sCRMS had significantly higher creatinine levels and clearly lower eGFR, with all patients in this group having an eGFR <45 mL/min/1.73 m².
3.4. Survival Curves and Multivariable Analysis
Survival analysis confirmed the adverse prognostic impact of sCRMS. In the unadjusted analysis, sCRMS was associated with a higher risk of mortality, HF readmissions, and the combined endpoint. After multivariable adjustment for relevant clinical variables, these associations were attenuated but remained statistically significant (Table 5).
Kaplan–Meier curves demonstrated a lower cumulative probability of survival in patients with sCRMS throughout follow-up, with progressively diverging curves (Figure 2). Stratified analysis according to the individual components of sCRMS revealed that certain components of the syndrome contribute differentially to mortality risk. Notably, patients with obesity showed a better prognosis compared with those of normal weight (Figure 3).
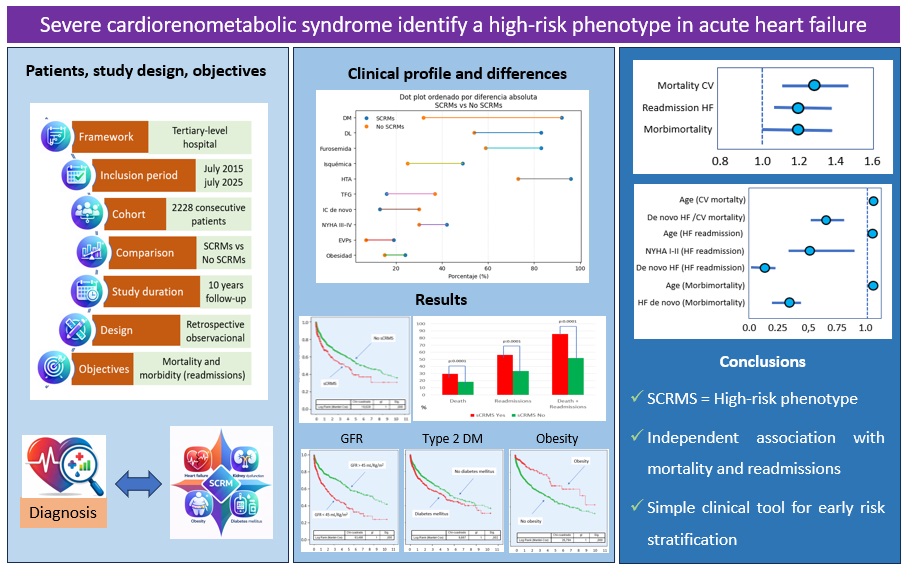
A graphical summary of the study is presented in Figure 4.
4. Discussion
Acute HF represents a clinical scenario in which hemodynamic decompensation and congestion act as triggers for multiorgan dysfunction, particularly at the renal and metabolic levels. In this context, the coexistence of CKD, T2DM, and obesity constitutes a substrate of clinical vulnerability that can amplify both the severity of the index episode and the risk of subsequent events during follow-up [1,2].
Despite increasing recognition, evidence on CRMS phenotypes has been generated predominantly in stable or outpatient populations, leaving a knowledge gap in the hospitalized acute HF setting [7]. In this study, the prevalence of sCRMS in this context was 22%, corresponding to a patient profile with a higher burden of cardiovascular comorbidity, worse functional class, and a greater history of prior hospitalizations. Even the pattern of acute decompensation differed, with a higher prevalence of systemic congestion in these patients.
Furthermore, it was observed that patients with sCRMS experienced greater HF-related morbidity and mortality (readmissions and HF-related death) during follow-up, and that the presence of sCRMS at admission was an independent predictor of HF-related morbidity and mortality.
Patients with sCRMS were older, had a higher prevalence of ischemic heart disease, and carried a greater overall burden of cardiovascular comorbidity. Conversely, de novo HF was less frequent in this group, suggesting distinct clinical profiles between the two cohorts. Indeed, patients with sCRMS had a higher number of previous hospitalizations and worse baseline functional class. These findings are consistent with the literature, which reports that, in the context of acute HF, the accumulation of renal and metabolic comorbidities typically identifies older patients with a higher atherosclerotic burden, supporting the notion that sCRMS represents a more “advanced” disease phenotype rather than a single, isolated episode [8,9,10].
From a pathophysiological standpoint, this pattern aligns with cardiorenal syndrome, where renal dysfunction participates in a vicious cycle of congestion, neurohormonal activation, and disease progression [11]. Beyond these clinical differences, the hemodynamic presentation pattern differed between groups: patients with sCRMS more frequently exhibited systemic or mixed congestion, whereas isolated pulmonary congestion predominated in patients without sCRMS. This observation is consistent with the literature describing cardiorenal syndrome as a phenotype strongly influenced by venous congestion and elevated right-sided pressures (right ventricular dysfunction/venous hypertension), which is associated with worse renal function and greater need for combined diuretic therapy [12,13,14].
In line with this, patients with sCRMS had higher use of loop diuretics and diuretic intensification strategies, reflecting the predominance of systemic congestion and, very likely, a reduced diuretic response—a situation particularly common when renal dysfunction coexists with HF [15]. Beyond diuretic therapy, in general, patients with sCRMS had greater exposure to treatments targeting HF and cardiovascular, metabolic, and renal comorbidities. This therapeutic pattern reflects greater complexity in management, consistent with a more advanced stage of HF and the presence of cardiorenal syndrome [16,17].
When analyzing laboratory findings, we observed that sCRMS is associated with a profile indicative of greater clinical severity, characterized by worse renal function, higher neurohormonal activation, increased myocardial injury, electrolyte disturbances, and anemia. This reinforces its value as a marker of risk and clinical complexity in patients hospitalized for HF [11,18].
Notably, NT-proBNP levels were higher in the sCRMS group, reflecting greater organ involvement and a higher degree of systemic congestion, a pattern particularly described in the literature among patients with impaired renal function [19,20]. However, no differences were found between groups in CA-125 levels, despite the predominance of systemic congestion in patients with sCRMS. These findings have been previously reported by our group, showing that approximately 25% of patients with acute HF and marked systemic congestion present normal CA-125 levels—especially women, patients with preserved ejection fraction, and those with >50% inspiratory collapse of the inferior vena cava [21,22].
Based on these biomarker findings, several research groups have advocated for the implementation of an integrated cardiorenometabolic laboratory profile to optimize clinical care, reduce healthcare costs, and improve patient outcomes [23,24,25].
Regarding clinical outcomes, patients with sCRMS showed a markedly higher incidence of mortality, HF readmissions, and the combined endpoint. Several studies have demonstrated that the coexistence of T2DM in the setting of acute HF is associated with higher in-hospital mortality and a higher-risk profile, likely mediated by a greater burden of ischemic heart disease and associated comorbidities. Likewise, the development or coexistence of cardiorenal syndrome during episodes of decompensated HF has been robustly linked to worse clinical outcomes, including mortality and early events, becoming established as a marker of systemic vulnerability and severity of the acute episode. Taken together, these data support the concept that sCRMS represents a phenotype of increased cardiorenal and metabolic frailty, with reduced physiological reserve in the face of decompensating events and a higher risk of adverse outcomes during follow-up [26,27,28].
Survival analysis additionally demonstrated a progressive divergence of the curves over time, suggesting that the prognostic impact of sCRMS is sustained and extends beyond the acute phase of hospitalization. These findings have been reported in the literature, where patients with sCRMS not only experience higher in-hospital mortality but also worse long-term outcomes [29,30]. Importantly, follow-up duration was comparable between groups, ruling out differences in exposure time as an explanation and supporting the presence of an intrinsically higher risk associated with this syndrome [31]. In multivariable analysis, sCRMS remained an independent predictor of mortality and HF readmissions, reinforcing its prognostic value beyond traditional clinical risk determinants such as age, baseline functional class, or presentation as de novo HF. This finding suggests that sCRMS does not act solely as an indirect marker of disease severity or comorbidity burden, but rather identifies a phenotype with inherent systemic vulnerability, characterized by the interaction between renal dysfunction, metabolic disturbances, and increased cardiovascular complexity.
Overall, these results support the usefulness of integrating renal and metabolic variables into prognostic stratification in acute HF, particularly in a context in which classical models may underestimate risk in patients with cardiorenometabolic multimorbidity [26,32].
Finally, stratified analysis by individual components of the syndrome revealed relevant prognostic heterogeneity, highlighting a relatively better prognosis among patients with obesity, in line with the so-called “obesity paradox” [30,33,34]. This finding may be related to factors such as frailty, which is highly prevalent in patients with advanced stages of HF [35].
This study has several limitations that should be considered when interpreting the results. First, its retrospective observational design precludes the establishment of causal relationships and does not exclude the influence of residual confounding from unmeasured variables. Second, this is a single-center study; therefore, extrapolation of the findings to other healthcare systems or levels of care should be undertaken with caution. In addition, the definition of sCRMS is based on simple clinical and laboratory parameters obtained at admission, which, while enhancing applicability, may not fully capture the pathophysiological complexity of the syndrome or its dynamic nature during hospitalization and follow-up. Finally, the long inclusion period may have introduced some heterogeneity related to temporal changes in therapeutic strategies and standards of HF management. Nevertheless, these limitations are counterbalanced by relevant strengths that underscore the robustness of the results. Notably, the large sample size, with consecutive inclusion over a prolonged period, minimizes selection bias and provides a realistic picture of routine clinical practice. Furthermore, the prospective and structured collection of clinical data by a team specialized in HF ensures high data quality and contributes to the internal validity of the study. From a conceptual standpoint, the integrative sCRMS approach goes beyond the isolated analysis of comorbidities and aligns with current cardiorenometabolic disease paradigms, offering a syndromic perspective that more closely reflects clinical reality. Moreover, the use of a simple, reproducible, and admission-applicable definition facilitates immediate translation into practice, enabling early identification of patients at higher risk.
In summary, in the analyzed cohort, the presence of sCRMS was associated with a high-risk clinical profile with a clear increase in morbidity and mortality. This finding suggests that sCRMS does not act merely as an indirect marker of disease severity or comorbidity burden, but rather identifies a phenotype with inherent systemic vulnerability. The results support the usefulness of integrating renal and metabolic variables into prognostic stratification in acute HF. Early identification of this phenotype may allow more accurate risk stratification, guide more intensive follow-up strategies, and facilitate the development of integrated therapeutic interventions along the cardiorenometabolic axis, particularly after hospital discharge, when clinical vulnerability remains high.
5. Conclusions
In a large contemporary cohort of patients hospitalized for acute HF, the presence of sCRMS consistently identifies a high-risk clinical phenotype, characterized by older age, a greater burden of cardiovascular and metabolic comorbidities, a more advanced clinical course, and a more complex hemodynamic profile. From a prognostic standpoint, sCRMS is associated with a significantly higher incidence of HF-related mortality, HF readmissions, and the combined endpoint, acting as an independent predictor of worse clinical outcomes.
References
- Ndumele CE, Rangaswami J, Chow SL, Neeland IJ, Tuttle KR, Khan SS, et al; American Heart Association. Cardiovascular-Kidney-Metabolic Health: A Presidential Advisory From the American Heart Association. Circulation. 2023 Nov 14;148(20):1606-1635. https://doi.org/10.1161/CIR.0000000000001184. Epub 2023 Oct 9. Erratum in: Circulation. 2024 Mar 26;149(13):e1023. [CrossRef]
- Kittelson KS, Junior AG, Fillmore N, da Silva Gomes R. Cardiovascular-kidney-metabolic syndrome - An integrative review. Prog Cardiovasc Dis. 2024 Nov-Dec;87:26-36. Epub 2024 Oct 30. [CrossRef]
- Schaubroeck HA, Gevaert S, Bagshaw SM, Kellum JA, Hoste EA. Acute cardiorenal syndrome in acute heart failure: focus on renal replacement therapy. Eur Heart J Acute Cardiovasc Care. 2020 Oct;9(7):802-811. Epub 2020 Jun 29. [CrossRef]
- Ahmed A, Campbell RC. Epidemiology of chronic kidney disease in heart failure. Heart Fail Clin. 2008 Oct;4(4):387-99. [CrossRef]
- Parissis J, Farmakis D, Kadoglou N, Ikonomidis I, Fountoulaki E, Hatziagelaki E, et al. Body mass index in acute heart failure: association with clinical profile, therapeutic management and in-hospital outcome. Eur J Heart Fail. 2016 Mar;18(3):298–305. Epub 2016 Jan 28. [CrossRef]
- McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al; ESC Scientific Document Group. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021 Sep 21;42(36):3599-3726. https://doi.org/10.1093/eurheartj/ehab368. Erratum in: Eur Heart J. 2021 Dec 21;42(48):4901. [CrossRef]
- Ndumele CE, Rangaswami J, Chow SL, Neeland IJ, Tuttle KR, Khan SS, et al; American Heart Association. A synopsis of the evidence for the science and clinical management of cardiovascular-kidney-metabolic (CKM) syndrome: a scientific statement from the American Heart Association. Circulation. 2023 Nov 14;148(20):1636-1664. [CrossRef]
- Spinar J, Parenica J, Vitovec J, Linhart A, Widimsky P, Fedorco M, et al. Baseline characteristics and hospital mortality in the Acute Heart Failure Database (AHEAD) Main registry. Crit Care. 2011;15(6):R291. Epub 2011 Dec 7. [CrossRef]
- Parissis JT, Rafouli-Stergiou P, Mebazaa A, Ikonomidis I, Bistola V, Nikolaou M, et al. Acute heart failure in patients with diabetes mellitus: Clinical characteristics and predictors of in-hospital mortality (ALARM-HF). Int J Cardiol. 2012;157(1):108-113. Epub 2011 Dec 15. [CrossRef]
- Lee KS, Park DI, Lee J, Oh O, Kim N, Nam G. Relationship between comorbidity and health outcomes in patients with heart failure: a systematic review and meta-analysis. BMC Cardiovasc Disord. 2023 Oct 10;23(1):498. [CrossRef]
- Rangaswami J, Bhalla V, Blair JEA, Chang TI, Costa S, Lentine KL, et al; American Heart Association Council on the Kidney in Cardiovascular Disease and Council on Clinical Cardiology. Cardiorenal Syndrome: Classification, Pathophysiology, Diagnosis, and Treatment Strategies: A Scientific Statement From the American Heart Association. Circulation. 2019 Apr 16;139(16):e840-e878. [CrossRef]
- Mullens W, Abrahams Z, Francis GS, Sokos G, Taylor DO, Starling RC, et al. Importance of venous congestion for worsening of renal function in advanced decompensated heart failure. J Am Coll Cardiol. 2009;53(7):589-596. [CrossRef]
- Espinosa B, Llorens P, Gil V, Rossello X, Jacob J, Herrero P, et al; ICA-SEMES group. Prognosis of acute heart failure based on clinical data of congestion. Rev Clin Esp (Barc). 2022 Jun-Jul;222(6):321-331. Epub 2021 Oct 29. [CrossRef]
- López-Vilella R, Guerrero Cervera B, Donoso Trenado V, Martínez Dolz L, Almenar Bonet L. Clinical profiling of patients admitted with acute heart failure: a comprehensive survival analysis. Front Cardiovasc Med. 2024 May 21;11:1381514. [CrossRef]
- Emmens JE, Ter Maaten JM, Damman K, van der Meer P, Voors AA, Butler J, et al. Worsening renal function in acute heart failure in the context of diuretic response. Eur J Heart Fail. 2022;24(1):182-192. [CrossRef]
- Galindo Ortego G, Esteve IC, Gatius JR, Santiago LG, Lacruz CM, Soler PS. Pacientes con el diagnóstico de insuficiencia cardiaca en Atención Primaria: envejecimiento, comorbilidad y polifarmacia [Heart failure patients in Primary Care: aging, comorbidities and polypharmacy]. Aten Primaria. 2011 Feb;43(2):61-7. Spanish. Epub 2010 Dec 22. [CrossRef]
- Frigola-Capell E, Verdú-Rotellar JM, Comin-Colet J, Davins-Miralles J, Hermosilla E, Wensing M, Suñol R. Prescription in patients with chronic heart failure and multimorbidity attended in primary care. Qual Prim Care. 2013;21(4):211-9.
- Akbari T, Hammersley DJ, May CY, Halliday BP, Prasad SK. The Impact of Cardio-Renal-Metabolic Profile in Dilated Cardiomyopathy. Curr Cardiol Rep. 2025 May 23;27(1):89. [CrossRef]
- Palazzuoli A, Ruocco G, Pellegrini M, Martini S, Del Castillo G, Beltrami M, et al. Patients with cardiorenal syndrome revealed increased neurohormonal activity, tubular and myocardial damage compared to heart failure patients with preserved renal function. Cardiorenal Med. 2014;4:257–268. [CrossRef]
- McCullough PA, Neyou A. Comprehensive review of the relative clinical utility of B-type natriuretic peptide and N-terminal pro-B-type natriuretic peptide assays in cardiovascular disease. Open Heart Fail J. 2009;3:6–17. [CrossRef]
- López-Vilella R, Guerrero Cervera B, Donoso Trenado V, Martínez-Solé J, Huélamo Montoro S, Soriano Alfonso V, et al. Paradox of Low CA-125 in Patients with Decompensated Congestive Heart Failure. Biomedicines. 2025 Jul 9;13(7):1679. [CrossRef]
- López-Vilella R, González-Vílchez F, Guerrero Cervera B, Donoso Trenado V, Saura Carretero Z, Martínez-Solé J, et al. Predictive Factors of Non-Elevation of Carcinoembryonic Antigen 125 in Acute Heart Failure. Life (Basel). 2025 Mar 18;15(3):494. [CrossRef]
- Montes LF. Cardio-Renal-Metabolic Laboratory Profile: An Integrated Strategy for the Prevention and Management of Chronic Non-Communicable Diseases. EJIFCC. 2025 Dec 5;36(4):564-574.
- Almenar Bonet L, Blasco Peiró MT, Laiz Marro B, Camafort Babkowski M, Buño Soto A, Casado Cerrada J, Crespo-Leiro MG. Specific test panels for patients with heart failure: implementation and use in the Spanish National Health System. Adv Lab Med. 2022 Mar 7;3(1):65-78. [CrossRef]
- Almenar Bonet L, Blasco Peiró MT, Laiz Marro B, Camafort Babkowski M, Buño Soto A, Casado Cerrada J, Crespo-Leiro MG. Preconfigured analytical profiles for the management of patients with heart failure: a consensus-driven study. REC: CardioClinics. 2023;58(3):219-227. [CrossRef]
- Rushton CA, Satchithananda DK, Jones PW, Kadam UT. Non-cardiovascular comorbidity, severity and prognosis in non-selected heart failure populations: A systematic review and meta-analysis. Int J Cardiol. 2015 Oct 1;196:98-106. Epub 2015 Jun 4. [CrossRef]
- Parissis JT, Rafouli-Stergiou P, Mebazaa A, Ikonomidis I, Bistola V, Nikolaou M, et al. Acute heart failure in patients with diabetes mellitus: clinical characteristics and predictors of in-hospital mortality. Int J Cardiol. 2012;157(1):108-113. Epub 2011 Dec 15. [CrossRef]
- Ferreira JP, Rossignol P, Zannad F. Cardiorenal syndrome in acute heart failure: a vicious cycle? Rev Port Cardiol. 2014;33(12):787-793.
- Birkeland KI, Bodegard J, Eriksson JW, Norhammar A, Haller H, Linssen GCM, et al. Heart failure and chronic kidney disease manifestation and mortality risk associations in type 2 diabetes: A large multinational cohort study. Diabetes Obes Metab. 2020 Sep;22(9):1607-1618. Epub 2020 Jun 3. [CrossRef]
- Cherney DZI, Repetto E, Wheeler DC, Arnold SV, MacLachlan S, Hunt PR, et al. Impact of Cardio-Renal-Metabolic Comorbidities on Cardiovascular Outcomes and Mortality in Type 2 Diabetes Mellitus. Am J Nephrol. 2020;51(1):74-82. Epub 2019 Dec 6. [CrossRef]
- Drozd M, Relton SD, Walker AMN, Slater TA, Gierula J, Paton MF, et al. Association of heart failure and its comorbidities with loss of life expectancy. Heart. 2021 Sep;107(17):1417-1421. . Epub 2020 Nov 5. PMID: 33153996. [CrossRef]
- Butler J, Chirovsky D, Phatak H, McNeill A, Cody R. Renal function, health outcomes, and resource utilization in acute heart failure: a systematic review. Circ Heart Fail. 2010;3(6):726-745. PMID: 21081740. [CrossRef]
- Donataccio MP, Vanzo A, Bosello O. Obesity paradox and heart failure. Eat Weight Disord. 2021 Aug;26(6):1697-1707. Epub 2020 Aug 26. [CrossRef]
- Cassadó-Valls P, Enjuanes C, Anguita M, Formiga F, Almenar L, Crespo-Leiro MG, et al. No Obesity Paradox for Health-Related Quality of Life in Patients with Heart Failure and Reduced Ejection Fraction: Insights from the VIDA Multicenter Study. J Clin Med. 2024 Dec 12;13(24):7558. [CrossRef]
- Matsue Y, Kamiya K, Saito H, Saito K, Ogasahara Y, Maekawa E, et al. Prevalence and prognostic impact of the coexistence of multiple frailty domains in elderly patients with heart failure: the FRAGILE-HF cohort study. Eur J Heart Fail. 2020 Nov;22(11):2112-2119. Epub 2020 Jul 14. [CrossRef]
Figure 1.
Mortality and readmissions. Abbreviations: sCRMS: Severe cardiorenometabolic syndrome.
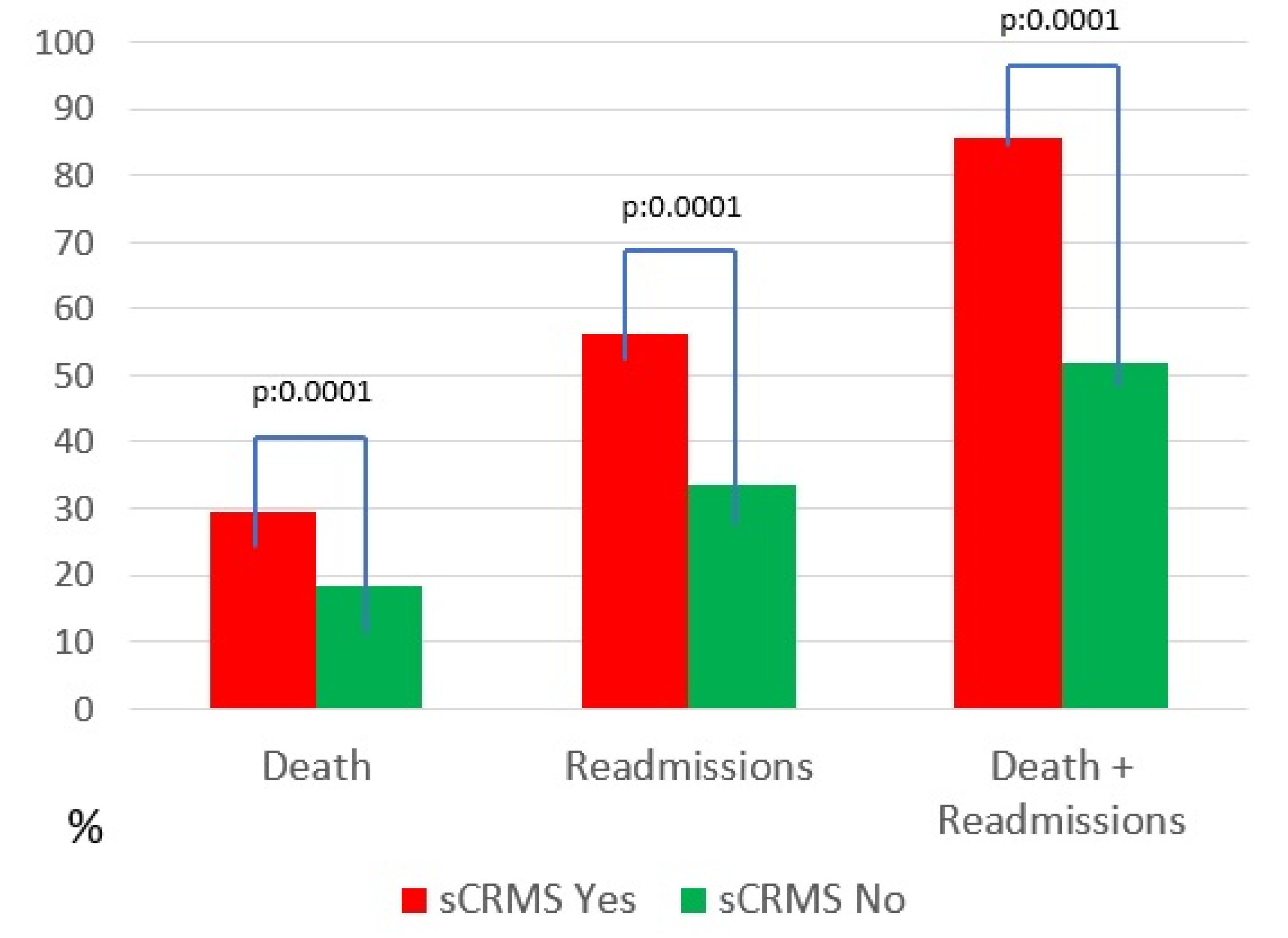
Figure 2.
Survival probability of sCRMS. Abbreviations: sCRMS: Severe cardiorenometabolic syndrome.
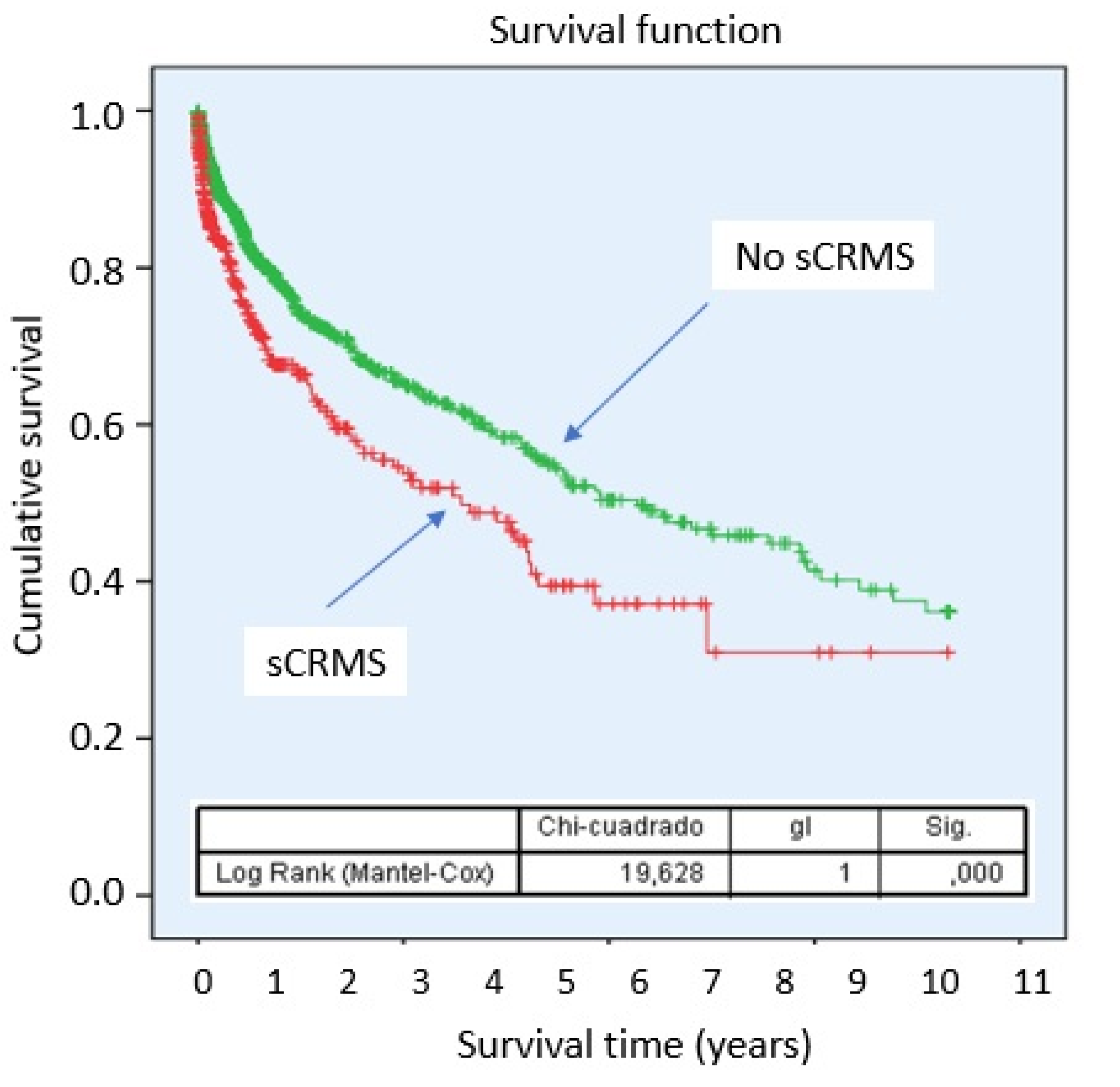
Figure 3.
Survival probability according to sCRMS component. Abbreviations: sCRMS: Severe cardiorenometabolic syndrome. Left: Glomerular filtration rate < 45 mL/min/1.73 m²; Center: Diabetes mellitus; Right: Obesity.
Figure 3.
Survival probability according to sCRMS component. Abbreviations: sCRMS: Severe cardiorenometabolic syndrome. Left: Glomerular filtration rate < 45 mL/min/1.73 m²; Center: Diabetes mellitus; Right: Obesity.
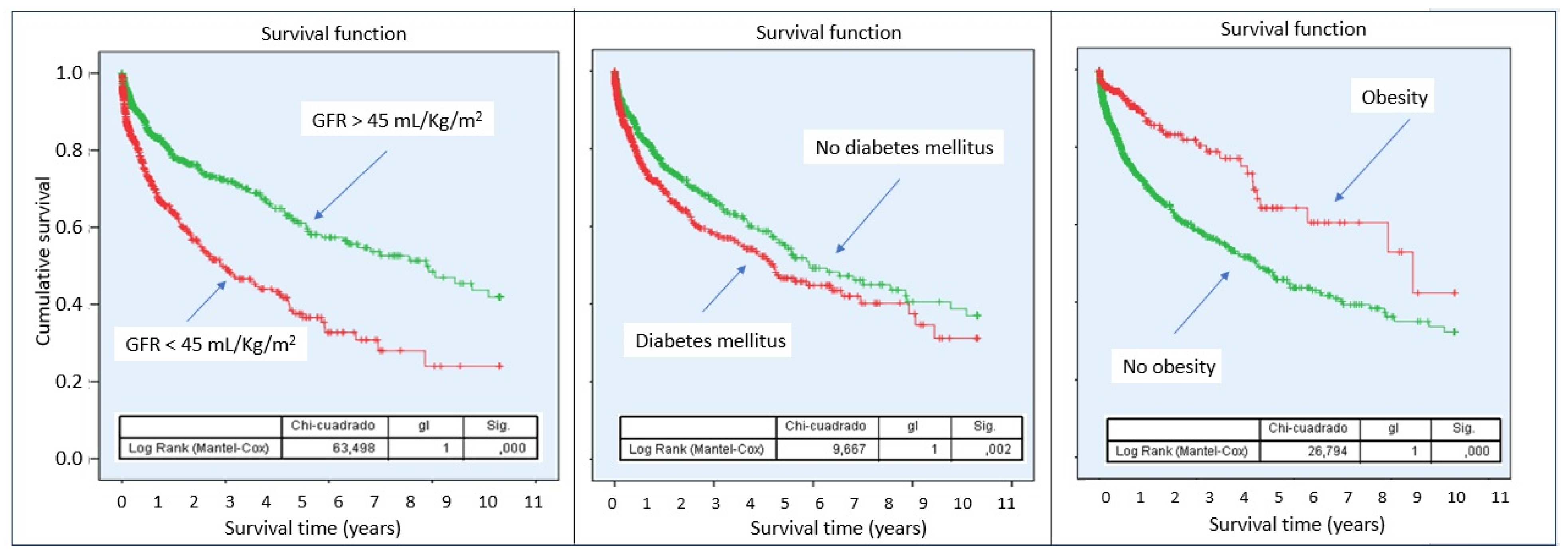
Figure 4.
Graphical abstract. Abbreviations: sCRMS: Severe cardiorenometabolic syndrome.
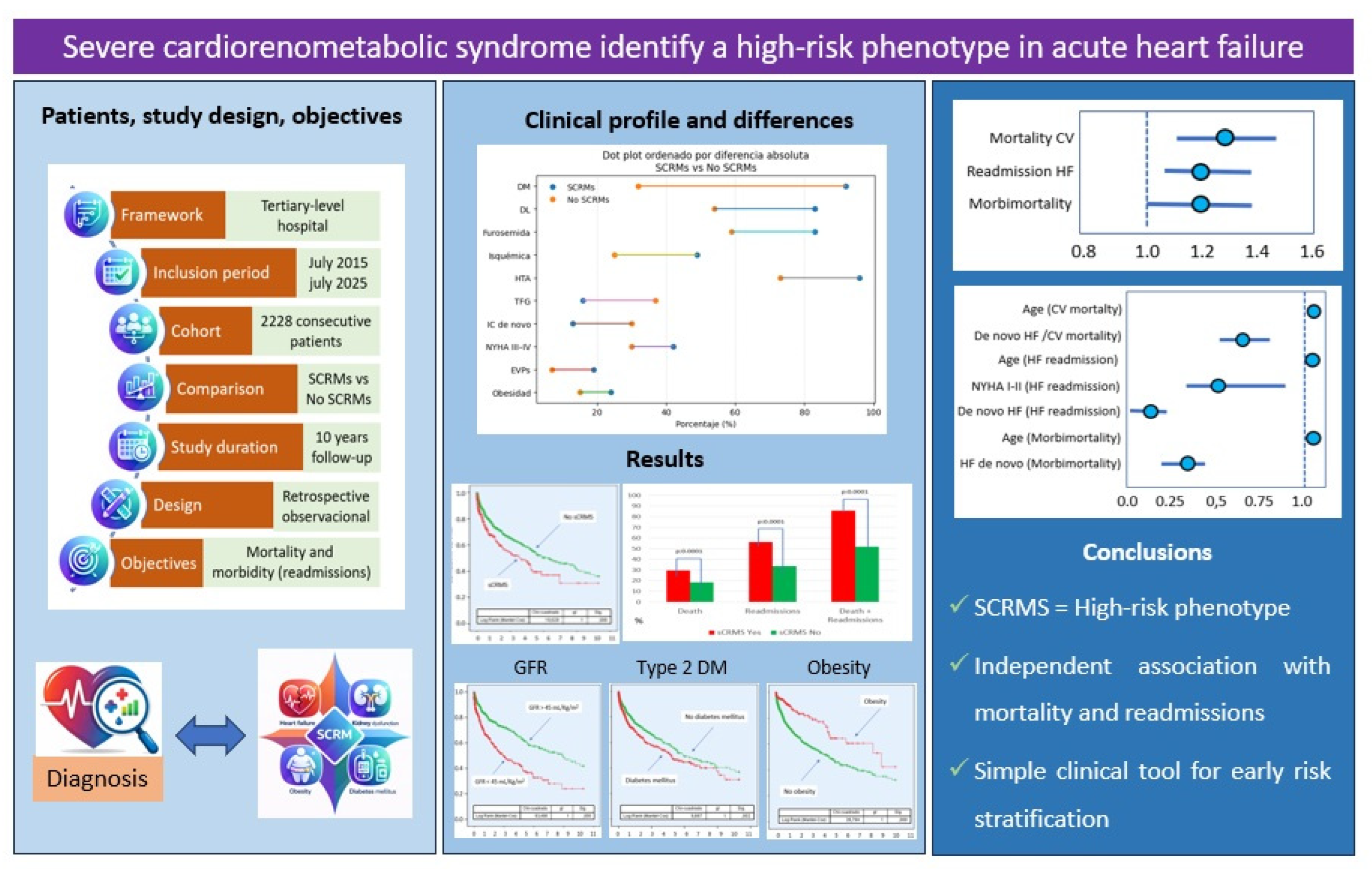

Table 1.
Medical history and clinical profile.
| sCRMS Yes (n=486) | sCRMS No (n=1742) | p-value | Total (n=2228) | |
| Age* | 77 (12) | 73 (19) | 0.0001 | 74 (17) |
| Male sex | 304 (62.6) | 1039 (59.6) | 0.249 | 1343 (3) |
| Underlying heart disease - AF/Flutter - Hypertension - Ischemic heart disease - Non-ischemic DCM - Valvular heart disease - Other causes |
21 (4.3) 73 (15) 237 (48.8) 29 (6) 97 (20) 29 (5.9) |
158 (9.1) 209 (12) 436 (25) 223 (12.8) 510 (29.3) 206 (11.8) |
0.0001 |
179 (8) 282 (12.7) 673 (30.2) 252 (11.3) 607 (27.2) 235 (10.6) |
| Previous CV surgery | 107 (22.2) | 377 (21.7) | 0.803 | 484 (21.8) |
| HT | 464 (95.7) | 1270 (72.9) | 0.0001 | 1734 (77.9) |
| Dyslipidemia | 401 (82.5) | 938 (53.9) | 0.0001 | 1339 (60.1) |
| Smoking# | 218 (44.9) | 680 (39.1) | 0.012 | 898 (40.4) |
| Alcoholism | 29 (6) | 139 (8) | 0.081 | 168 (7.5) |
| COPD | 77 (15.8) | 256 (14.7) | 0.289 | 333 (15) |
| Sleep apnea | 80 (19.6) | 160 (11.7) | 0.0001 | 240 (13.5) |
| Hypothyroidism | 44 (9.4) | 146 (8.6) | 0.319 | 190 (8.8) |
| AF | 277 (57.1) | 1004 (58) | 0.755 | 1281 (57.8) |
| Stroke | 44 (10.5) | 143 (9.8) | 0.712 | 187 (10) |
| Peripheral vascular disease | 76 (18.5) | 99 (7.2) | 0.0001 | 175 (9.8) |
| Number of previous hospitalizations ^ | 2 (2) | 1 (1) | 0.0001 | 1 (1) |
| De novo HF | 64 (13.3) | 521 (30.2) | 0.0001 | 585 (26.5) |
| Days of hospitalization | 8 (7) | 7 (7) | 0.015 | 7 (7) |
| Baseline NYHA I, II III, IV |
280 (57.6) 206 (42.4) |
1212 (69.6) 530 (30.4) |
0.0001 |
1492 (67) 736 (33) |
| Hemodynamic pattern Low output Pulmonary congestion Mixed congestion@ Systemic congestion |
23 (4.1) 254 (52.3) 132 (27.2) 77 (16.4) |
101 (5.8) 1075 (61.7) 378 (21.7) 188 (10.8) |
0.001 |
124 (5.6) 1329 (59.6) 510 (22.9) 265 (11.9) |
| CRT | 52 (10.7) | 139 (8) | 0.073 | 191 (8.6) |
| ICD | 79 (16.3) | 213 (12.2) | 0.028 | 292 (13.1) |
| Preserved LVEF | 186 (38.3) | 708 (40.6) | 0.058 | 894 (40.1) |
| Normal RVEF | 319 (65.6) | 1082 (62.1) | 0.253 | 1401 (63) |
| Dilated right ventricle | 165 (34) | 610 (35) | 0.440 | 775 (34.8) |
* Kolmogorov-Smirnov: 0.0001. Median and interquartile range. Values are expressed as absolute numbers and percentages (in parentheses). #Current smoker or ex-smoker <10 years. ^Includes the hospitalization of the study. @Pulmonary and systemic congestion. Abbreviations: AF: atrial fibrillation; CV: cardiovascular; COPD: chronic obstructive pulmonary disease; CRT: Cardiac resynchronization therapy; DCM: dilated cardiomyopathy; HF: Heart failure; HT: hypertension; ICD: implantable cardioverter-defibrillator; LVEF: left ventricle ejection fraction; NYHA: New York Heart Association; RV: right ventricle; sCRMS: Severe cardiorenometabolic syndrome.
Table 2.
Prior treatment.
| sCRMS Yes (n=486) | sCRMS No (n=1742) | p-value | Total (n=2228) | |
| ACEI/ARB/ARNI | 245 (50.4) | 928 (53.3) | 0.257 | 1173 (52.6) |
| Beta-blocker | 326 (67.1) | 1000 (57.4) | 0.0001 | 1326 (59.5) |
| MRA | 160 (32.9) | 521 (29.9) | 0.198 | 681 (30.6) |
| Ivabradine | 27 (5.6) | 103 (5.9) | 0.905 | 130 (5.8) |
| Digoxin | 19 (3.9) | 118 (6.8) | 0.024 | 137 (6.1) |
| Loop diuretic | 403 (82.9) | 1033 (59.3) | 0.0001 | 1436 (64.5) |
| Thiazide | 123 (25.3) | 300 (17.2) | 0.0001 | 423 (19) |
| Tolvaptan | 22 (4.5) | 30 (1.7) | 0.001 | 52 (2.3) |
| Acetazolamide | 23 (4.7) | 14 (0.8) | 0.0001 | 37 (1.7) |
| Antiaplatelet | 195 (40.1) | 481 (27.6) | 0.0001 | 676 (30.3) |
| Anticoagulant | 267 (54.9) | 873 (50.1) | 0.071 | 1140 (51.2) |
| Nitrates | 71 (14.6) | 110 (6.3) | 0.0001 | 181 (8.1) |
| Oral antidiabetics | 325 (66.9) | 441 (25.3) | 0.0001 | 766 (34.4) |
| SGLT2 inhibitor | 170 (35) | 387 (22.2) | 0.0001 | 557 (25) |
| Potassium binder | 18 (3.7) | 3 (0.2) | 0.0001 | 21 (0.9) |
| Potassium supplement | 41 (8.4) | 96 (5.5) | 0.018 | 137 (6.1) |
| Antiarrhytmics | 89 (18.3) | 228 (13.1) | 0.011 | 317 (14.2) |
| Statins | 370 (76.1) | 904 (51.9) | 0.0001 | 1274 (57.2) |
| Calcium channel blockers | 218 (44.9) | 404 (23.2) | 0.0001 | 622 (27.9) |
| Pulmonary vasodilator | 12 (2.5) | 42 (2.4) | 0.853 | 54 (2.4) |
| Allopurinol | 208 (42.8) | 314 (18) | 0.0001 | 522 (23.4) |
| Vericiguat | 17 (3.5) | 21 (1.2) | 0.048 | 38 (1.7) |
Values are expressed as absolute numbers and percentages (in parentheses). Abbreviations: ACEI: angiotensin-converting enzyme inhibitor; ARB: angiotensin II receptor blocker; ARNI: angiotensin receptor-neprilysin inhibitors; MRA: mineralocorticoid receptor antagonist; sCRMS: Severe cardiorenometabolic syndrome; SGLT2: sodium–glucose cotransporter 2.
Table 3.
Laboratory findings at admission.
| sCRMS Yes (n=486) | sCRMS No (n=1742) | p-value | Total (n=2228) | |
| Urea (mg/dL) | 97 (65) | 49 (32) | 0.0001 | 55 (44) |
| Bilirubin (mg/dL) | 0.67 (0.55) | 0.87 (0.76) | 0.0001 | 0.81 (0.7) |
| AST (U/L) | 22 (14) | 25 (18) | 0.0001 | 24 (17) |
| ALT (U/L) | 17 (15) | 21 (19) | 0.0001 | 20 (18) |
| High-sensitivity Troponin T (ng/L) | 57.8 (62.2) | 40.5 (55.6) | 0.0001 | 45 (62) |
| NT-proBNP (pg/mL) | 10147 (17255) | 4622 (7156) | 0.0001 | 5465 (8662) |
| Sodium (mEq/L) | 138 (6) | 140 (5) | 0.0001 | 139 (5) |
| Potassium (mEq/L) | 4.6 (1) | 4.3 (0.8) | 0.0001 | 4.3 (0.8) |
| Hemoglobin (g/dL) | 11.5 (3.2) | 12.7 (2.8) | 0.0001 | 12.3 (3) |
| Hematocrit (%) | 36.7 (9) | 40.1 (8.8) | 0.0001 | 38.4 (8.8) |
| Platelets (µL, ÷100) | 198 (85) | 218 (105) | 0.014 | 213 (104) |
| Uric acid (mg/dL) | 8.4 (3.3) | 7.7 (3.1) | 0.0001 | 7.8 (3.2) |
| TSI (%) | 18 (12) | 17 (12) | 0.636 | 17 (12) |
| Ferritin (ng/mL) | 195 (324) | 152 (230) | 0.0001 | 159 (250) |
| HbA1c (%) | 6.4 (1.3) | 5.9 (1) | 0.0001 | 6 (1) |
| CA125 (U/mL) | 60 (71) | 49 (189) | 0.535 | 75.4 (142.4) |
| Cystatin C (mg/L) | 2.12 (1.33) | 1.43 (1.2) | 0.056 | 2.07 (1.4) |
| Urinary creatinine (mg/dL) | 43.5 (29.2) | 52.4 (58.2) | 0.207 | 50.8 (42.9) |
| Microalbuminuria (mg/g) | 2 (7.4) | 12.7 (12.5) | 0.975 | 2.65 (10.78 |
* Kolmogorov-Smirnov 0.0001. Median and interquartile range. Abbreviations: ALT: alanine aminotransferase; AST: aspartate aminotransferase; CA125: Carbohydrate antigen 125; HbA1c: glycated hemoglobin; NT-proBNP: N-terminal pro–B-type natriuretic peptide; sCRMS: Severe cardiorenometabolic syndrome; TSI: transferrin saturation index.
Table 4.
Diagnostic and study criteria.
| sCRMS Yes (n=486) | sCRMS No (n=1742) | p-value | Total (n=2228) |
|
| Creatinine (mg/dL)# | 2.04 (1.01) | 1.1 (0.52) | 0.0001 | 1.24 (0.83) |
| GFR (ml/min/1.73 m2)# | 30.65 (16.38) | 64.5 (36.5) | 0.0001 | 54.85 (42.28) |
| GFR < 45 ml/min/1.73m2 | 486 (100) | 349 (20) | 0.0001 | 835 (37.5) |
| Diabetes mellitus | 448 (92.2) | 565 (32.4) | 0.0001 | 1013 (45.5) |
| Obesity | 116 (23.9) | 257 (14.8) | 0.0001 | 373 (16.7) |
| HF mortality | 143 (29.4) | 320 (18.4) | 0.0001 | 463 (20.8) |
| HF readmission | 273 (56.2) | 584 (33.5) | 0.0001 | 857 (38.5) |
| HF mortality+readmission | 416 (85.6) | 904 (51.9) | 0.0001 | 1320 (59.2) |
| Follow-up Time# | 116.5 (356) | 111 (325) | 0.186 | 110 (332) |
# Kolmogorov-Smirnov 0.0001. Median and interquartile range. Values are expressed as absolute numbers and percentages (in parentheses). Abbreviations: GFR: glomerular filtration rate; HF: heart failure; sCRMS: Severe cardiorenometabolic syndrome.
Table 5.
Event analysis.
| sCRMS Phenotype | Unadjusted | Adjusted& | ||||
| HR | CI95% | p | HR | CI95% | p | |
| Mortality | 1.558 | 1.278-1.898 | 0.0001 | 1.252 | 1.016-1.544 | 0.035 |
| HF Readmissions | 2.541 | 2.070-3.119 | 0.0001 | 1.235 | 1.061-1.438 | 0.006 |
| Mortality + Readmissions | 1.516 | 1.328-1.730 | 0.0001 | 1.201 | 1.045-1.381 | 0.01 |
&: Adjusted for age, sex, baseline NYHA class, de novo heart failure, ischemic etiology, and variables clinically relevant or significant in univariable analysis. They were also significant for mortality: Age (HR: 1.031, 95% CI: 1.022–1.040) and de novo HF (HR: 0.625, 95% CI: 0.474–0.826). For readmission: Age (HR: 1.014, 95% CI: 1.007–1.020), baseline functional class I–II vs III–IV (HR: 0.501, 95% CI: 0.259–0.972), and de novo HF (HR: 0.049, 95% CI: 0.026–0.091). For mortality + readmissions: Age (HR: 1.019, 95% CI: 1.013–1.025) and de novo HF (HR: 0.278, 95% CI: 0.217–0.356). Abbreviations: CI: confidence interval; HF: heart failure; sCRMS: Severe cardiorenometabolic syndrome.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



