
Submitted:
15 July 2025
Posted:
16 July 2025
You are already at the latest version
Abstract
Objective: To analyze the characteristics of patients with heart failure (HF) in an internal medicine department (IMD), define their clinical trajectories and develop a risk algorithm to predict mortality/rehospitalization. Meth-ods: Retrospective cohort study of 410 hospitalizations (28% readmissions / 280 patients) with acute HF discharged from our MID during 2023. Clinical diagnosis was reassured using the European Society of Cardiology age-related N-terminal proBNP (NT-proBNP) thresholds. Results: The cohort (mean age 82 years, 54% women) predomi-nantly had nonischemic heart disease (80%), HF with preserved ejection fraction (HFpEF, 69%), and a mean left ventricular EF of 53.7%. The most frequent comorbidities included hypertension (85%), diabetes (45%), atrial fibril-lation (44%) and almost half had ≥3 pre-existing non-cardiac diseases. In-hospital mortality reached 19.6% with a 30-day readmission rate of 9.9%. Three clinical trajectories were identified: single hospitalizations (n:169), rehospi-talizations with or without deaths (n :73), and deaths during the index admission (n:38). Markers of severity in-cluded advanced age, elevated NT-proBNP levels, secondary causes of HF, and the degree of reduction in renal function and hemoglobin value. The risk stratification model used was based on NT-proBNP, hemoglobin, LVEF, and gender (accuracy level of 72.7%). Conclusions: This internal medicine HF population was elderly, predomi-nantly female, with multiple comorbidities and high HFpEF prevalence. Severity indicators included renal function, hemoglobin, NT-proBNP, and the proportion of secondary HF causes. The developed algorithm may help identify patients at elevated risk for poor outcomes.
Keywords:
heart failure
; hospitalization
; rehospitalization
; mortality
; NT-proBNP
1. Introduction
Heart failure (HF) represents one of the most significant challenges in contemporary cardiovascular medicine with an estimated prevalence in developed countries ranging from 1–2% of the adult population [1,2]. On the other hand, acute heart failure (AHF) represents the main cause of hospitalization in patients over 65 years of age, who also usually present multiple comorbidities [3,4]. In this context, patients admitted to an internal medicine department (IDM) tend to be older, frailer, and have higher morbidity than those admitted to cardiology ones [5,6].
This paper presents a single-center descriptive study examining AHF patients hospitalized in an IMD. We analyze baseline demographics and identify three distinct clinical trajectories from the initial hospitalization. Additionally, we develop a predictive model using clinical variables to identify patients at elevated risk for in-hospital mortality or readmission.
2. Materials and Methods
2.1. Study Design Ethics Approval
This retrospective, observational study received approval from the hospital’s clinical research committee. All clinical data were processed with patient confidentiality measures in place, in accordance with the Declaration of Helsinki. Written informed consent was waived under national legislation and institutional requirements.
2.2. Patients’ Categorization
The study analyzed all patients discharged with AHF from our IMD during 2023 (January 1 to December 31), including both primary (cardiac-related) and secondary (non-cardiac-related) diagnoses. Case selection involved reviewing all discharge summaries, encompassing both single hospitalizations and readmissions. All data was obtained from the hospital’s clinical information system.
2.3. Heart Failure Diagnosis
A total of 567 hospitalizations were analyzed, allowing the identification of 410 confirmed discharges due to AHF. To validate the diagnosis, a positive clinical assessment was required, conducted collaboratively by specialists in internal medicine and cardiology. Additionally, baseline N-terminal proBNP (NT-proBNP) levels had to meet the age-specific thresholds recommended by the European Society of Cardiology for diagnosing AHF [1].
2.4. Collected Information
A total of 280 patients accounted for 410 hospitalizations, including readmissions, allowing for baseline demographic analysis. Data collected included sex, age, body mass index (BMI), HF etiology (ischemic or non-ischemic), left ventricular ejection fraction (LVEF), HF phenotype, and heart rhythm categorized as sinus rhythm, atrial fibrillation (AF), or pacemaker-dependent rhythm. Data was also collected on comorbidities including hypertension, diabetes mellitus, chronic obstructive pulmonary disease (COPD), sleep apnea syndrome, active cancer, hypothyroidism, stroke, and chronic kidney disease (CKD). To recognize each condition, the use of specific treatments was verified. Stroke was only included if the patient had previous hospitalization for this condition. Pre-existing CKD required an estimated glomerular filtration rate ≤30 mL/min/1.73 m² during a stable phase for inclusion.
Based on each patient’s initial hospitalization of the year (index hospitalization), three progressive severity profiles were established according to clinical trajectory: patients with a single hospitalization, those with rehospitalizations (including deaths during subsequent admissions), and those who died during their first hospitalization. This analysis incorporated admission values of blood pressure, NT-proBNP, hemoglobin, creatinine, and eGFR, along with classification of HF as primary or secondary. Finally, a predictive algorithm was developed using various clinical variables to estimate the risk of in-hospital mortality or rehospitalization
2.5. Statistical Analysis
All categorical variables are presented as absolute numbers (n) and percentages (%), while continuous variables are expressed as mean ± standard deviation (SD) and range. NT-proBNP values, due to their significant skewness and dispersion, are reported as median and interquartile range (IQR, 25–75%). To compare qualitative data between groups, the Student’s t-test was used, while the ANOVA median test was applied for multiple group comparisons. Odds ratios (OR) with 95% confidence intervals (95% CI) were calculated, and all statistical tests were two-sided, considering a p-value < 0.05 as statistically significant. A multivariate analysis was conducted using the non-parametric CHAID (Chi-square Automatic Interaction Detection) decision tree technique, which enabled the development of a predictive model to identify clinical variables associated with in-hospital mortality and rehospitalization. All statistical analyses were performed using Microsoft Excel 2021®, except for the CHAID technique, which was implemented with IBM SPSS Statistics®.
3. Results
3.1. Baseline Demographics
During 2023, our IMD recorded 410 AHF hospitalizations (primary and secondary) involving 280 patients (Table 1).
This population was elderly (mean age 82), predominantly female (54%), and typically overweight (mean BMI 28.1). Women were generally older than men (84.5 vs 79.4 years) with nearly triple the proportion of nonagenarians (29% vs 10%). Our cohort showed high prevalence of hypertension (85%), DM (45%), and AF (44%), with relatively low coronary artery disease (CAD) incidence (20%). This LVEF profile corresponded with predominantly (69%) HF with preserved ejection fraction (HFpEF) versus a minority of patients (20%) exhibiting HF with reduced ejection fraction (HFrEF). Men had higher CAD rates (25% vs. 16%), lower mean LVEF (50.2% vs.56.5%), and more HFrEF (30% vs 12%) (Table 2).
Nearly half (49%) of patients had three or more non-cardiac comorbidities and men showed higher rates of chronic respiratory diseases (58% vs 35%) and sleep disorders (24% vs 14%), while hypothyroidism was more common in women (16% vs 6%).(Table 3).
3.2. Index Hospitalization: Patient Profiles & Clinical Trajectories
Taking the first annual hospitalization for HF (primary or secondary) as the index episode, three distinct clinical trajectories were identified (Table 4): single admission (n=169), rehospitalizations with possible deaths (n=73), and death during initial hospitalization (n=38). Across these groups, worsening outcomes correlated with increased age (80.5, 83.8, 85.9 years; p=0.0018)), higher NT-proBNP levels (8,264, 10,084, 17,001 pg/ml; p<0.0001), reduced kidney function (eGFR: 50.9, 45.3, 38.9 mL/min/1.73m²; p<0.0001), lower hemoglobin values (11.9, 11.3, 11.2 g/dl; p=0.0447), and a higher proportion of secondary causes of HF (63%, 75%, 84%; p=0.0134). This suggests secondary HF carries a worse prognosis than primary HF
3.3. Mortality and Re-Hospitalization Rate
The all-cause mortality rates during hospitalization at 1, 3, and 6 months were 19.6% (n=55), 26% (n=73), and 30% (n=84), respectively. In our cohort of 280 patients, a total of 410 hospitalizations were recorded, including 113 (28%) rehospitalizations. The readmission rates were 9.9% within 30 days and 22.7% within 100 days. Specifically, 69 patients experienced a first readmission (second hospitalization), 27 underwent a second readmission (third hospitalization), 13 had a third readmission (fourth hospitalization), and 4 patients experienced a fourth readmission (fifth hospitalization).
3.4. Multivariable Analysis
The CHAID algorithm classified baseline NT-proBNP levels into three ranges, identifying the highest range (≥15,000 pg/ml) as a categorical indicator of poor prognosis (rehospitalization or in-hospital death). In the lowest NT-proBNP range (≤5,000 pg/ml), hemoglobin levels were identified as a key differentiating factor, categorizing patients into intermediate (≤11.5 g/dl) or low (>11.5 g/dl) risk of death or readmission. For patients with NT-proBNP levels between 5,001 and 14,999 pg/ml, the algorithm initially identified reduced LVEF (≤40%) as an indicator of low risk. Among those with mildly reduced (41-49%) or preserved LVEF (≥50%), gender further stratified patients into intermediate (female) or high (male) risk groups (Figure 1). The model demonstrated a certainty of 72.7% with an error rate of 27.3% (Figure 2)
Predictive model based on the nonparametric CHAID decision tree technique. This method allowed for the determination of the most hierarchical clinical variables for predicting in-hospital mortality and rehospitalization. Consequently, patients were classified as low, intermediate and high risk. Each box contains the corresponding total number of patients (n) and the percentage (%) of them who were rehospitalized or who died during hospitalization. NT-proBNP (N-terminal pro-brain type natriuretic peptide); Hb (hemoglobin); LVEF (left ventricular ejection fraction).
The model achieved an accuracy rate of 72.7% with an error rate of 27.3% when classifying low- and high-risk patients. For intermediate-risk patients, clinical assessment and judgment should be used to reassign them to the low- or high-risk category (considering other clinical factors).
4. Discussion
Summary of Main Results and Comparison with Published References
In general, patients hospitalized for HF in IMDs tend to be older, predominantly women, with a higher prevalence of comorbidities and HFpEF, alongside a lower proportion of CAD compared to those admitted to cardiology units. [5,6,7,8,9]. This prevalent HF phenotype shows a conditional relationship with gender and age, as it is more common in women and its incidence increases with advancing age [10]. The structural basis of this phenomenon lies in the characteristics of the female myocardium, which has a higher content of extracellular fibrosis and a lower rate of myocyte loss throughout life compared to the male myocardium. Consequently, this explains why the left ventricle in women is generally smaller and stiffer than in men. [11,12].
As previously mentioned, our population was elderly (mean age: 82 years), predominantly female (54%), with a high prevalence of hypertension (85%), DM (45%), and AF (44%), along with a lower incidence of CAD (20%) and HFrEF (20%). Similar patterns have been documented in other series of decompensated patients admitted to internal medicine departments. In the PRECIC study (Oporto, Portugal), which included 479 patients (62% women; mean age: 79 years), the prevalence of hypertension, DM, and AF was notably high at 87%, 48%, and 51%, respectively, while the prevalence CAD was relatively low at 35% [9]. Similarly, in the SMIT study (Tuscany, Italy), involving 770 individuals (55% women; mean age: 82 years), hypertension, DM, and AF were also prominent at rates of 73%, 36%, and 47%, respectively, within a context of reduced prevalence of HFrEF at 18% [13].
Data from both a small single-center study in Lodz, Poland, with 75 patients (61% women; mean age: 81 years) and a large single-center registry in Rome, Italy, with 6,930 individuals (51% women; mean age: 81 years), demonstrated a consistent pattern. In the former, the prevalence rates were 72% for hypertension, 44% for diabetes mellitus (DM), and 48% for atrial fibrillation (AF), while in the latter, these rates were 53%, 30%, and 45%, respectively [8,14]. Conversely, the prospective observational registry ESC-HF-LT, which included 4,449 patients (mean age: 69 years), illustrated a clear trend: the lower the mean age of patients hospitalized for AHF, the higher the proportions of men, CAD, and HFrEF, with rates of 63%, 53%, and 67%, respectively [15].
On the other hand, it is well known that the coexistence of comorbidities significantly exacerbates the morbidity and mortality of patients with HF [1,2,4]. Our documented all-cause in-hospital mortality rate was 19.6%, significantly exceeding those reported in other multicenter studies or registries, including the KaRen study (2.4%) [16], the OPTIMISE-HF study (3.8%) [17], the ADHERE registry (4.0%) [18], the SMIT study (5.9%) [13], the PRECIC study (7.9%) [9], and the JROADHF registry (7.7%) [19]. Despite these differences, our results are aligned more closely with data from individual centers. For example, a mortality rate of 20% was reported in the series by Chuda et al. (Lodz, Poland) [14], 12.7% in the study by Dolokupil et al. (Prague, Czech Republic) (20), 12% in the cohort analyzed by Jhon et al. (Vellore, India) (21), and 19% in the geriatric cohort from the ATENA trial (Florence, Italy) [22].
As previously described, three clinical trajectories were identified (based on the index hospitalization): patients with a single hospitalization, patients rehospitalized (including some who died), and patients who died during the initial hospitalization. As severity increased within the groups, a progressive increase in mean age, renal dysfunction, NT-proBNP levels, and the proportion of secondary causes of HF was observed. Patients with primary (cardiac) causes of decompensation showed better outcomes, with lower rates of rehospitalization and in-hospital mortality. In addition, a multivariate analysis was conducted using an algorithmic predictive model to assess in-hospital mortality and rehospitalization based on various clinical variables. The model first categorized baseline NT-proBNP levels into three ranges, identifying the highest level (≥15,000 pg/ml) as an indicator of poor prognosis. For the lowest NT-proBNP range (≤5,000 pg/ml), hemoglobin levels served as the differentiating factor, stratifying patients into intermediate (≤11.5 g/dl) or low (≥11.6 g/dl) risk groups. Lastly, for patients with intermediate NT-proBNP values (5,001–14,999 pg/ml), a reduced LVEF (≤40%) was sufficient to classify patients as low risk, while for those with LVEF ≥41%, gender was used to distinguish between intermediate (female) and high (male) risk categories.
In general, the risk indicators identified in our experience are consistent with those reported in the literature, albeit with nuances and variations depending on the source. De Matteis et al. (Rome, Italy) observed that in-hospital mortality among patients with AHF was 2.5 times higher (p<0.001) in individuals aged ≥85 years, particularly in the presence of cerebrovascular disease or dementia [8]. Similarly, the PRECIC study revealed a significant increase in one-year mortality (univariate analysis) among patients aged ≥80 years (p=0.001) or those with active cancer (p=0.008), dementia (p<0.001), functional dependence (p<0.001), or AF (p=0.004) [9].
Furthermore, the Japanese JROADHF registry (n=13,238; 47% women; mean age: 78 years) identified several independent predictors of in-hospital mortality (multivariate analysis), including older age, aortic valve stenosis, hypertension, CKD; stage IV-V, and elevated baseline peptide levels (all p<0.001) [19]. On the other hand, the previously referenced ESC-HF-LT registry identified the main predictors of annual all-cause mortality (23.6%) in patients with HF as follows: older age (per 5-year increment; p<0.0001), low blood pressure (per 5 mmHg decrement; p<0.0001), reduced LVEF (per 5% decrement; p<0.0001), hepatic or renal dysfunction (p<0.0001), prior stroke (p=0.0225), DM (p=0.0192), COPD (p=0.0043), and aortic stenosis (p=0.0001) [15].
Rehospitalizations represent a significant turning point in the clinical course of HF patients, with the highest risk occurring within 30-90 days post-discharge. However, reported rehospitalization rates vary considerably across different sources [5,6,23,24].
As previously mentioned, our series reported a notably high overall readmission rate (28% of 410 hospitalizations), alongside elevated 30-day (9.9%) and 100-day (22.7%) rehospitalization rates. Comparatively, Dharmarajan et al. (New York, USA) and Sharma et al. (Adelaide, Australia) documented 30-day readmission rates of 24.8% [24] and 23.8% [7], respectively, while Davidge et al. (Halmstad, Sweden) reported a 100-day readmission rate of 33% [6].
Sager et al. (Lund, Sweden) reported a significant 30-day mortality and readmission rate among elderly patients with AHF who were treated with intravenous furosemide. Mortality and readmission rates were 40% and 24% respectively, for those receiving the diuretic as an infusion, compared to 20% and 40%, respectively, for those receiving it as a bolus injection [25]. Meanwhile, Wideqvist et al. (Gothenburg, Sweden) conducted a real-world study that documented 30-day and 90-day readmission rates for AHF of 11.4% and 21%, respectively, figures that closely align with our findings [26]. Chuda et al. (Lodz, Poland) identified several factors associated with an increased risk of rehospitalization in patients with AHF compared to those with a single hospitalization. These included a higher prevalence of HFrEF; CAD, CKD, and more than three comorbidities (all p<0.05) [14]. Similarly, Davidge et al. (Halmstad, Sweden) reported that the risk of rehospitalization due to AHF significantly increased in patients aged >75 years, those with hospital stays >7 days, elevated NT-proBNP levels (all p<0.001), or an eGFR <30 ml/min (p=0.005) [6]. Additionally, Al Omary et al. (Newcastle, Australia) identified their main univariate predictors of annual readmission for AHF as older age (per 10-year increment; p<0.001), CAD (p<0.001), CKD (p=0.082), COPD (p=0.046), and DM (p=0.462) [27]. In the same way, Wideqvist et al. (Gothenburg, Sweden) found that patients readmitted for AHF, compared to those with a single hospitalization, had significantly higher rates of CKD (p=0.001), COPD (p=0.010), and psychiatric diseases (p=0.001). Moreover, the number of comorbidities was strongly associated with the annual rehospitalization rate for any cause (p<0.001) and for AHF specifically (p=0.012) [26].
Baseline NT-proBNP levels in our study served as both a severity marker and predictor of mortality and rehospitalization outcomes. This relationship between higher NT-proBNP values and worse prognosis is well-established in literature and widely used as a prognostic indicator in clinical practice [1,2,3].
Udani et al. (Myrtle Beach, USA) conducted a retrospective study stratifying 21,445 patients with AHF into four quartiles based on their NT-proBNP levels at admission: group 1 (<1,669 pg/ml), group 2 (1,670–4,274 pg/ml), group 3 (4,275–10,499 pg/ml), and group 4 (>10,500 pg/ml). The study revealed that patients in group 4 had a significantly higher all-cause readmission rate at 60 days compared to group 1 (p=0.013) and group 2 (p=0.014). Over the 90 days, this difference remained significant only when compared to group 1 (p=0.021). In-hospital mortality was observed to rise progressively with increasing baseline NT-proBNP levels: 0.9%, 1.4%, 2.5%, and 4.7% for groups 1, 2, 3, and 4, respectively (all p<0.0005). Notably, in this context, mortality in group 4 was consistently significant when compared to any of the other three groups (p<0.0005) [28].
In the previously mentioned series by Sager et al. (Lund, Sweden), 30-day mortality among two groups of elderly patients with acute heart failure (AHF) treated with different diuretic regimens was 20% in the group with a mean NT-proBNP value of 9,640 pg/ml (n=20), compared to 40% in the group with a mean value of 15,901 pg/ml (n=20) [25].
In addition, the BIOSTAT-CHF clinical research program (n=2,516) identified the five most significant predictors of mortality in patients with HF. These included older age (>70 years), elevated blood urea nitrogen levels (>11 mmol/L) or NT-proBNP (>4,000 pg/ml), reduced hemoglobin levels (<12 g/dl), and the absence of a beta-blocker prescription [29].
Finally, and aligning with our findings, Huang et al. (Luodong, ROC, Taiwan) reported in a retrospective study (n=269) that patients with AHF who died during hospitalization had significantly higher mean baseline NT-proBNP levels compared to survivors (15,942 pg/ml vs. 6,013 pg/ml; p<0.001). Furthermore, they determined that the probability of mortality began to rise from an NT-proBNP cut-off level of 8,100 pg/ml [30].
Therefore, we can conclude that, overall, our series aligns with the data reported in the literature regarding the baseline demographics and characteristics of patients with AHF hospitalized in IMDs. Moreover, our findings are consistent with the established association of worse prognosis in this context, particularly in relation to advanced age, comorbidities, renal dysfunction, low hemoglobin levels, and elevated baseline NT-proBNP values.
5. Limitations
The present study has several limitations that warrant consideration. First, the retrospective design of our analysis is inherently subject to multiple biases. Second, the single-center nature of this series introduces an additional bias. Third, there is a low representation of younger patients, individuals with CAD or heart HFrEF, as the study was conducted within an internal medicine department (not in a cardiology one). Fourth, the diagnosis of HF relied on clinical criteria, baseline NT-proBNP levels and LVEF determination.
6. Conclusions
This study provides a real-world depiction of patients admitted with AHF in the internal medicine department of an urban hospital. Our findings highlight a challenging clinical scenario characterized by an elderly population (predominantly female), with numerous cardiac and non-cardiac comorbidities, a low prevalence of CAD and HFrEF, as well as elevated rates of rehospitalization and in-hospital mortality. Clinical data from index hospitalizations—including mean patient age, renal dysfunction, hemoglobin and NT-proBNP levels, and the proportion of secondary versus primary causes of HF were identified as markers of progressive severity. Furthermore, we developed an algorithm based on commonly assessed clinical variables to predict in-hospital mortality and readmissions in patients hospitalized for HF (both primary and secondary). This algorithm has the potential to be replicated and validated in prospective studies. In conclusion, we believe it is crucial to bring visibility to such experiences, as they emphasize the complexity of this clinical scenario, provide valuable lessons, and encourage the implementation of strategies to improve the treatment and care of HF patients, who are often extremely vulnerable.
Author Contributions
All authors have contributed significantly to the manuscript, meeting the criteria for authorship and approving its final version. EK was responsible for study design, data analysis and article writing. SMC, JTM, ASI, DCG, FPA and LZ were responsible for screening articles, data collection and clinical performance GTW, EMA and CCP were responsible for theoretical guidance and decision-making in case of disagreement and AFC was responsible for the statistical analysis.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, B.; Ahmad, T.; Alexander, K.M.; Baker, W.L.; Bosak, K.; Breathett, K.; Fonarow, G.C.; Heidenreich, P.; Ho, J.E.; Hsich, E.; et al. Heart Failure Epidemiology and Outcomes Statistics: A Report of the Heart Failure Society of America. J Card Fail. 2023, 29, 1412–1451. [Google Scholar] [CrossRef] [PubMed]
- Cheema, B.; Ambrosy, A.P.; Kaplan, R.M.; Senni, M.; Fonarow, G.C.; Chioncel, O.; Butler, J.; Gheorghiade, M. Lessons learned in acute heart failure. Eur J Heart Fail. 2018, 20, 630–641. [Google Scholar] [CrossRef] [PubMed]
- Shoaib, A.; Farag, M.; Nolan, J.; Rigby, A.; Patwala, A.; Rashid, M.; Kwok, C.S.; Perveen, R.; Clark, A.L.; Komajda, M.; Cleland, J.G.F. Mode of presentation and mortality amongst patients hospitalized with heart failure? A report from the First Euro Heart Failure Survey. Clin Res Cardiol. 2019, 108, 510–519. [Google Scholar] [CrossRef]
- Labrosciano, C.; Horton, D.; Air, T.; Tavella, R.; Beltrame, J.F.; Zeitz, C.J.; Krumholz, H.M.; Adams, R.J.T.; Scott, I.A.; Gallagher, M.; et al. Frequency, trends and institutional variation in 30-day all-cause mortality and unplanned readmissions following hospitalization for heart failure in Australia and New Zealand. Eur J Heart Fail. 2021, 23, 31–40. [Google Scholar] [CrossRef]
- Davidge, J.; Halling, A.; Ashfaq, A.; Etminani, K.; Agvall, B. Clinical characteristics at hospital discharge that predict cardiovascular readmission within 100 days in heart failure patients—An observational study. Int J Cardiol Cardiovasc Risk Prev. 2023, 16, 200176. [Google Scholar] [CrossRef]
- Sharma, Y.; Horwood, C.; Hakendorf, P.; Thompson, C. Characteristics and outcomes of patients with heart failure discharged from different specialty units in Australia: An observational study. QJM 2022, 115, 727–734. [Google Scholar] [CrossRef]
- De Matteis, G.; Covino, M.; Burzo, M.L.; Della Polla, D.A.; Franceschi, F.; Mebazaa, A.; Gambassi, G. Clinical Characteristics and Predictors of In-Hospital Mortality among Older Patients with Acute Heart Failure. J Clin Med. 2022, 11, 439. [Google Scholar] [CrossRef]
- Marques, I.; Lopes Ramos, R.; Mendonça, D.; Teixeira, L. One-year mortality after hospitalization for acute heart failure: Predicting factors (PRECIC study subanalysis). Rev Port Cardiol. 2023, 42, 505–513. [Google Scholar] [CrossRef]
- Kawai, A.; Nagatomo, Y.; Yukino-Iwashita, M.; Nakazawa, R.; Yumita, Y.; Taruoka, A.; Takefuji, A.; Yasuda, R.; Toya, T.; Ikegami, Y.; et al. Sex Differences in Cardiac and Clinical Phenotypes and Their Relation to Outcomes in Patients with Heart Failure. J Pers Med. 2024, 14, 201. [Google Scholar] [CrossRef]
- Olivetti, G.; Giordano, G.; Corradi, D.; Melissari, M.; Lagrasta, C.; Gambert, S.R.; Anversa, P. Gender differences and aging: Effects on the human heart. J. Am. Coll. Cardiol. 1995, 26, 1068–1079. [Google Scholar] [CrossRef] [PubMed]
- Dworatzek, E.; Baczko, I.; Kararigas, G. Effects of aging on cardiac extracellular matrix in men and women. Proteom. Clin. Appl. 2016, 10, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Verdiani, V.; Panigada, G.; Fortini, A.; Masotti, L.; Meini, S.; Biagi, P. The heart failure in internal medicine in Tuscany: The SMIT study. Italian Journal of Medicine 2015, 9, 349–355. [Google Scholar] [CrossRef]
- Chuda, A.; Berner, J.; Malgorzata, L. The journey of the heart failure patient based on data from a single center. Adv Clin Exp Med 2019, 28, 489–498. [Google Scholar] [CrossRef]
- Crespo-Leiro, M.G.; Anker, S.D.; Maggioni, A.P.; Coats, A.J.; Filippatos, G.; Ruschitzka, F.; Ferrari, R.; Piepoli, M.F.; Delgado Jimenez, J.F.; Metra, M.; et al. European Society of Cardiology Heart Failure Long-Term Registry (ESC-HF-LT): 1-year follow-up outcomes and differences across regions. Eur J Heart Fail. 2016, 18, 613–625. [Google Scholar] [CrossRef]
- Donal, E.; Lund, L.H.; Oger, E.; Hage, C.; Persson, H.; Reynaud, A.; Ennezat, P.V.; Bauer, F.; Sportouch-Dukhan, C.; Drouet, E.; et al. Baseline characteristics of patients with heart failure and preserved ejection fraction included in the Karolinska Rennes (KaRen) study. Arch Cardiovasc Dis. 2014, 107, 112–121. [Google Scholar] [CrossRef]
- Abraham, W.T.; Fonarow, G.C.; Albert, N.M.; Stough, W.G.; Gheorghiade, M.; Greenberg, B.H.; O’Connor, C.M.; Sun, J.L.; Yancy, C.W.; Young, J.B.; Young, J.B.; OPTIMIZE-HF Investigators and Coordinators. Predictors of in-hospital mortality in patients hospitalized for heart failure: Insights from the Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF). J Am Coll Cardiol. 2008, 52, 347–356. [Google Scholar]
- Adams, K.F.Jr.; Fonarow, G.C.; Emerman, C.L.; LeJemtel, T.H.; Costanzo, M.R.; Abraham, W.T.; Berkowitz, R.L.; Galvao, M.; Horton, D.P. ADHERE Scientific Advisory Committee and Investigators. Characteristics and outcomes of patients hospitalized for heart failure in the United States: Rationale, design, and preliminary observations from the first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE). Am Heart J. 2005, 149, 209–216. [Google Scholar]
- Ide, T.; Kaku, H.; Matsushima, S.; Tohyama, T.; Enzan, N.; Funakoshi, K.; Sumita, Y.; Nakai, M.; Nishimura, K.; Miyamoto, Y.; et al. Clinical characteristics and outcome of hospitalized patients with heart failure from the large-scale Japanese registry of acute decompensated heart failure (JROADHF). Circ J. 2021, 85, 1438–1450. [Google Scholar] [CrossRef]
- Dokoupil, J.; Hrečko, J.; Čermáková, E.; Adamcová, M.; Pudil, R. Characteristics and outcomes of patients admitted for acute heart failure in a single-centre study. ESC Heart Fail. 2022, 9, 2249–2258. [Google Scholar] [CrossRef]
- John, F.M.; Joy, A.; Nellimala, N.J.; Bharathy, K.M.; Prakash, T.V.; John, K.V.; Mathuram, A.J.; Sathyendra, S.; Abraham, O.C.; Ramya, I.; et al. Predictors of in-hospital mortality in patients admitted with Congestive Heart failure (HF) in a general medical ward—A case-control study from a tertiary care centre in South India. CHRISMED Journal of Health and Research 2021, 8, 125–130. [Google Scholar] [CrossRef]
- Orso, F.; Pratesi, A.; Herbst, A.; Baroncini, A.C.; Bacci, F.; Ciuti, G.; Berni, A.; Tozzetti, C.; Nozzoli, C.; Pignone, A.M.; et al. Acute heart failure in the elderly: Setting related differences in clinical features and management. J Geriatr Cardiol. 2021, 18, 407–415. [Google Scholar] [PubMed]
- Ambrosy, A.P.; Fonarow, G.C.; Butler, J.; Chioncel, O.; Greene, S.J.; Vaduganathan, M.; Nodari, S.; Lam, C.S.P.; Sato, N.; Shah, A.N.; Gheorghiade, M. The global health and economic burden of hospitalizations for heart failure: Lessons learned from hospitalized heart failure registries. J Am Coll Cardiol. 2014, 63, 1123–1133. [Google Scholar] [CrossRef] [PubMed]
- Dharmarajan, K.; Hsieh, A.F.; Lin, Z.; Bueno, H.; Ross, J.S.; Horwitz, L.I.; Barreto-Filho, J.A.; Kim, N.; Bernheim, S.M.; Suter, L.G.; et al. Diagnoses and timing of 30-day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA 2013, 309, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Sager, R.; Lindstedt, I.; Edvinsson, L.; Edvinsson, M.L. Increased mortality in elderly heart failure patients receiving infusion of furosemide compared to elderly heart failure patients receiving bolus injections. J Geriatr Cardiol. 2020, 17, 359–364. [Google Scholar]
- Wideqvist, M.; Cui, X.; Magnusson, C.; Schaufelberger, M.; Fu, M. Hospital readmissions of patients with heart failure from real world: Timing and associated risk factors. ESC Heart Fail. 2021, 8, 1388–1397. [Google Scholar] [CrossRef]
- Al-Omary, M.S.; Khan, A.A.; Davies, A.J.; Fletcher, P.J.; Mcivor, D.; Bastian, B.; Oldmeadow, C.; Sverdlov, A.L.; Attia, J.R.; Boyle, A.J. Outcomes following heart failure hospitalization in a regional Australian setting between 2005 and 2014. ESC Heart Fail. 2018, 5, 271–278. [Google Scholar] [CrossRef]
- Udani, K.; Patel, D.; Mangano, A. A Retrospective Study of Admission NT-proBNP Levels as a Predictor of Readmission Rate, Length of Stay and Mortality. HCA Healthc J Med. 2021, 2, 207–214. [Google Scholar] [CrossRef]
- Voors, A.A.; Ouwerkerk, W.; Zannad, F.; van Veldhuisen, D.J.; Samani, N.J.; Ponikowski, P.; Ng, L.L.; Metra, M.; Ter Maaten, J.M.; Lang, C.C.; et al. Development and validation of multivariable models to predict mortality and hospitalization in patients with heart failure. Eur J Heart Fail. 2017, 19, 627–634. [Google Scholar] [CrossRef]
- Huang, Y.T.; Tseng, Y.T.; Chu, T.W.; Chen, J.; Lai, M.Y.; Tang, W.R.; Shiao, C.C. N-terminal pro b-type natriuretic peptide (NT-pro-BNP) -based score can predict in-hospital mortality in patients with heart failure. Sci Rep 2016, 6, 29590. [Google Scholar] [CrossRef]
Figure 1.
Predictive algorithm for patient outcomes during a heart failure hospitalization.
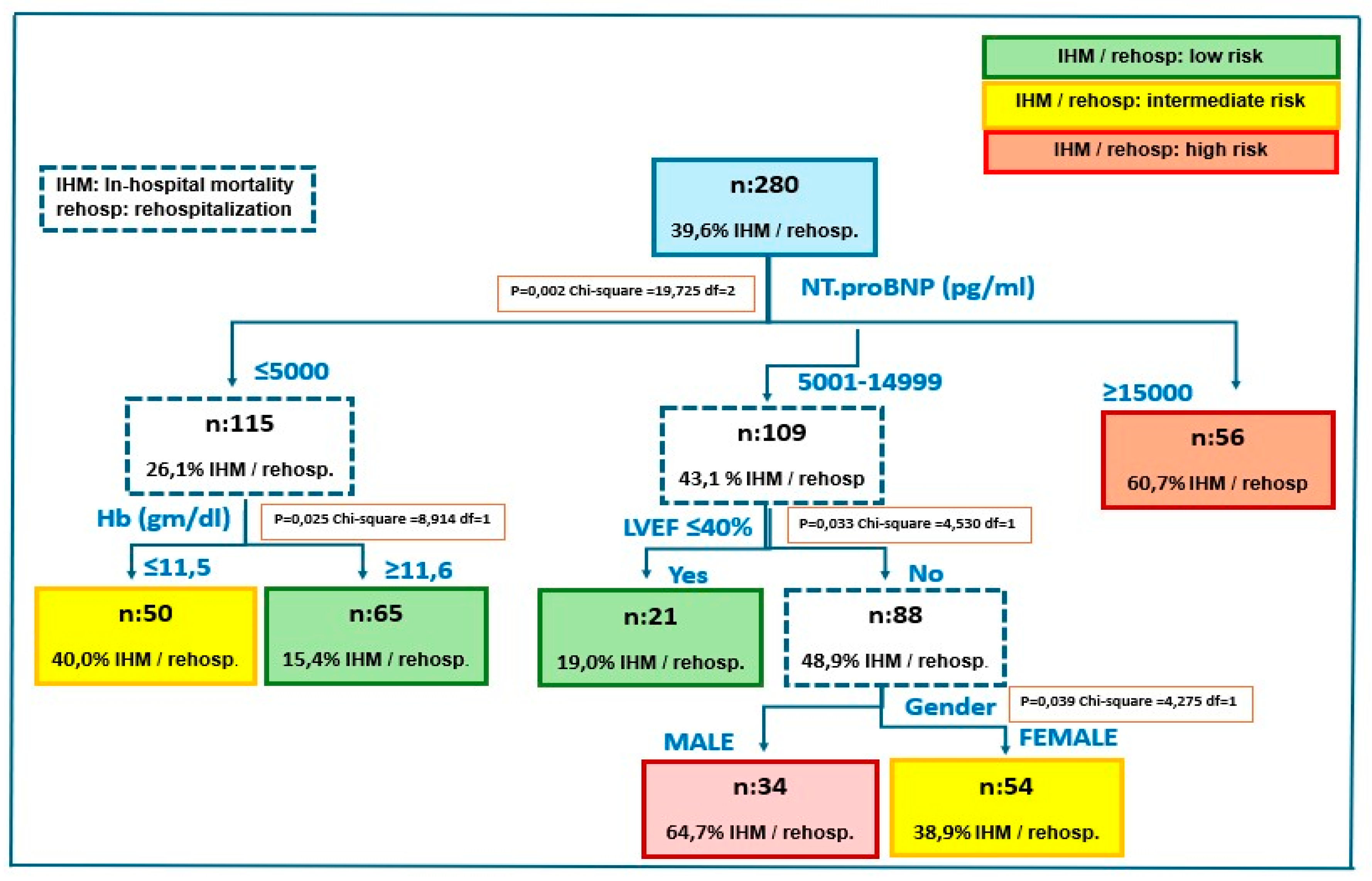
Figure 2.
Error rate and accuracy assessment of the risk prediction model.
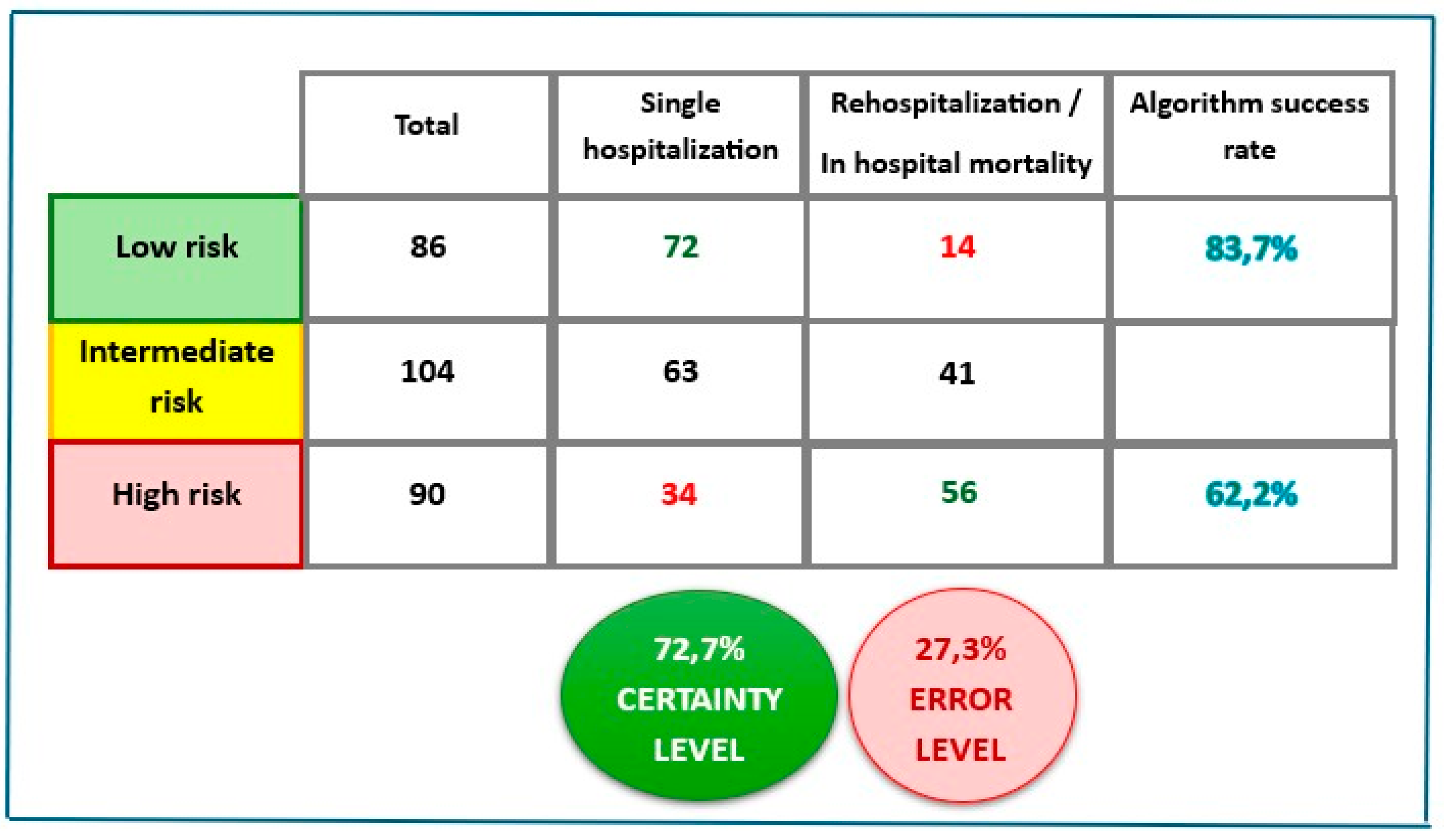

Table 1.
Primary and secondary causes of heart failure.
| Total HFH (n: 420) | |||
|---|---|---|---|
| Primary HF (n/%) | 109 (27%) | Secondary HF (n/%) | 301 (73%) |
| Causes (n/%): | Causes (n/%): | ||
| • New-onset AF | 29 (26%) | • Respiratory infection5 | 116 (39%) |
| • Valvular disease1 | 22 (20%) | • Respiratory insufficiency6 | 60 (20%) |
| • Non-compliance 2 | 17 (16%) | • Worsening renal function7 | 49 (16%) |
| • ACS | 14 (13%) | • Sepsis8 | 27 (9%) |
| • Worsening AF3 | 9 (8%) | • Urinary infection | 19 (6%) |
| • Bradyarrhythmia | 8 (7%) | • Anemia/GI bleeding | 11 (4%) |
| • Cardiac amyloidosis 4 | 6 (6%) | • Hip fractures | 7 (2%) |
| • Pulmonary embolism | 3 (3%) | • Ascitic decompensation | 5 (1,6%) |
| • Aortic dissection | 1 (1%) | • Stroke | 5 (1,6%) |
| • Other | 2 (0,8%) |
HFH (heart failure hospitalizations); HF (heart failure); AF (atrial fibrillation); ACS (acute coronary syndromes); GI (gastrointestinal). 1: advanced valvular pathology (including prosthetic valve dysfunctions). 2: alcoholism, abandonment of treatment, low awareness of illness and social isolation. 3: permanent AF exacerbation. 4: transthyretin cardiac amyloidosis detection. 5: proven viral or bacterial etiology (sepsis not included). 6: partial pressure of oxygen <60 mmHg (no proven infectious origin). 7: Marked increase in serum creatinine compared to basal level (conditioning issue). 8: from any origin. Categorical variables are expressed as absolute number and percentage.
Table 2.
Characteristics of the study population.
| Item | All patients | Female | Male | p between genders |
|---|---|---|---|---|
| Demography | ||||
| n | 280 (100%) | 152 (54%) | 128 (46%) | |
| Age: years± SD, (range) | 82,11 ± 9,9 (41-99) | 84,51 ± 8,6 (46-99) | 79,26 ±10,5 (41-96) | <0,0001 |
| BMI: Kg/m2± SD, (range) | 28,4 ± 5,6 (16 -49,1) | 28,4 ± 5,8 (16 -49,1) | 28,5 ± 5,3 (17,6 -44,1) | 0,9486 |
| Age distribution | ||||
| ≤ 59 years: n (%) | 10 (4%) | 2 (1%) | 8 (6%) | |
| 60-69 years: n (%) | 18 (6%) | 8 (5%) | 10 (8%) | |
| 70-79 years: n (%) | 65 (23%) | 31 (20%) | 34 (27%) | |
| 80-89 years: n (%) | 130 (46%) | 68 (45%) | 62 (48%) | |
| ≥90 years: n (%) | 57 (20%) | 43 (28%) | 14 (11%) | |
| Etiology | ||||
| CAD n (%) | 55 (20%) | 22 (14%) | 33 (26%) | 0,0199 |
| Non-CAD n (%) | 225 (80%) | 130 (86%) | 95 (74%) | |
| Cardiac rhythm | ||||
| SR: n (%) | 134 (48%) | 73 (48%) | 61 (48%) | 0,9510 |
| AF: n (%) | 119 (43%) | 67 (44%) | 52 (41%) | 0,5619 |
| Pacemaker: n (%) | 27 (9%) | 12 (8%) | 15 (11%) | 0,2892 |
| LVEF: % ± SD, (range) | 53,7 ± 12,3 (19-76) | 56,8 ±10,2 (20-76) | 50,0 ± 13,5 (19-76) | |
| HFrEF: n (%) | 57 (20%) | 17 (11%) | 40 (31%) | <0,0001 |
| HFmrEF: n (%) | 30 (11%) | 13 (9%) | 17 (13%) | 0,2115 |
| HFpEF: n (%) | 193 (69%) | 122 (80%) | 71 (55%) | <0,0001 |
BMI (body mass index); SD (standard deviation); CAD (coronary artery disease); SR (sinus rhythm); AF (atrial fibrillation); LVEF. (left ventricular ejection fraction); HFrEF (heart failure with reduced ejection fraction); HFmrEF (heart failure with mildly reduced rejection fraction); HFpEF (heart failure with preserved ejection fraction). All categorical variables are expressed as absolute number and percentage and all continuous variables are expressed as mean ± SD, (range). Significant p values are in bold.
Table 3.
Main non-cardiac comorbidities of the studied population.
| Comorbidity | All Patients | Female | Male | p between genders |
|---|---|---|---|---|
| Hypertension | 242 (86%) | 133 (88%) | 109 (85%) | 0,5724 |
| DM | 130 (46%) | 63 (41%) | 67 (52%) | 0,0694 |
| COPD | 127 (45%) | 53 (35%) | 74 (58%) | 0,0001 |
| SAS | 52 (19%) | 21 (14%) | 31 (24%) | 0,0287 |
| Stroke | 50 (18%) | 30 (20%) | 20 (16%) | 0,3689 |
| CKD | 42 (15%) | 22 (14%) | 20 (16%) | 0,7896 |
| Hypothyroidism | 33 (12%) | 25 (16%) | 8 (6%) | 0,0063 |
| Active cancer | 19 (7%) | 7 (5%) | 12 (9%) | 0,1251 |
| ≥3 comorbidities | 136 (49%) | 68 (45%) | 68 (53%) | 0,1631 |
DM (diabetes mellitus); COPD (chronic obstructive pulmonary disease), SAS (sleep apnea syndrome), CKD (chronic kidney disease). Categorical variables are expressed as absolute number and percentage, and significant p values are in bold.
Table 4.
Patient profiles and trajectories according to index hospitalization.
| Items | All Patients |
Single Hospitalization |
Rehospitalizations | Death first hospitalization |
p between hospitalizations |
|---|---|---|---|---|---|
| Total | 280 (100%) | 169 (60%) | 73 (26%) | 38 (14%) | |
| Female: n (%) | 152 (54%) | 97 (57%) | 33 (45%) | 22 (58%) | 0,1952 |
| Male: n (%) | 128 (46%) | 72 (43%) | 40 (55%) | 16 (42%) | |
| Clinical findings | |||||
| Age: years, ± SD, (range) | 82,1 ± 9,9 (41-99) | 80,5 ± 10,9 (41-99) | 83,8 ± 7,4 (55-98) | 85,9 ± 7,2 (69-96) | 0,0018 |
| BMI: Kg/m2± SD, (range) | 28,4 ± 5,5 (16-49,1) | 28,5 ± 5,9 (17,3-49,1) | 28,2 ± 5,1 (16,0 -40,0) | 28,3 ± 4,6 (20,1-42,3) | 0,8858 |
| SBP: mmHG, ± SD, (range) | 135,3 ± 26,9 (60-230) | 136,6 ± 27,0 (65-230) | 134,3 ± 27,1 (60-195) | 131,2 ± 26,4 (70-200) | 0,4984 |
| DBP: mmHG, ± SD, (range) | 76,3 ± 14,4 (30-115) | 77,4 ± 14,2 (40-110) | 75,3 ± 14,9 (30-115) | 73,3 ± 14,0 (40-100) | 0,2226 |
| Cr: mg/dl, ± SD, (range) | 1,52 ± 1,0 (0,42-6,63) | 1,40 ± 0,9 (0,42-6,24) | 1,55 ± 0,8 (0,47-5,09) | 2,01 ± 1,5 (0,48-6,63) | 0,0022 |
| eGFR: mL/min/1.73 m2, ± SD, (range) | 47,8 ± 21,9 (15-90) | 50,9 ± 21,8 (15-90) | 45,3 ± 20,8 (15-90) | 38,9 ± 22,2 (15-90) | 0,0047 |
| Hb: mg/dl ± SD, (range) | 11,6 ± 2,2 (3,5-17,3) | 11,9 ± 2,3 (4,8-17,3) | 11,3 ± 2,2 (3,5-16,4) | 11,2 ± 2,0 (7,0-16,5) | 0,0447 |
| NT-proBNP (pg/ml) median (IQR) | 9938 (8841-11035) | 8264 (6981-9547) | 10084 (8083-12085) | 17101 (13623-20579) | <0,0001 |
| Etiology | |||||
| CAD | 55 (20%) | 33 (20%) | 19 (26%) | 4 (8%) | 0,0742 |
| Non-CAD | 225 (80%) | 136 (80%) | 54 (74%) | 35 (92%) | |
| Cardiac rhythm | |||||
| SR: n (%) | 134 (48%) | 90 (53%) | 25 (34%) | 19 (50%) | 0,0237 |
| AF: n (%) | 119 (43%) | 68 (40%) | 38 (52%) | 13 (34%) | 0,1264 |
| Pacemaker: n (%) | 27 (9%) | 11 (7%) | 10 (14%) | 6 (16%) | 0,0854 |
| LVEF: % ± SD, (range) | 53,7 ±12,3 (19-76) | 53,4 ± 12,9 (20-72) | 54,8 ± 11,3 (19-76) | 53,1 ± 11,4 (34-76) | |
| HFrEF: n (%) | 57 (20%) | 38 (22%) | 10 (14%) | 9 (24%) | 0,2577 |
| HFmrEF: n (%) | 30 (11%) | 14 (8%) | 11 (15%) | 5 (13%) | 0,2578 |
| HFpEF: n (%) | 193 (69%) | 117 (69%) | 52 (71%) | 24 (63%) | 0,6798 |
| HF cause | |||||
| Primary: n (%) | 87 (31%) | 63 (37%) | 18 (25%) | 6 (16%) | 0,0134 |
| Secondary: n (%) | 193 (69%) | 106 (63%) | 55 (75%) | 32 (84%) |
SBP (systolic blood pressure); DBP (diastolic blood pressure); BMI (body mass index); Cr (creatinine), eGFR (estimated glomerular filtration rate); NT-proBNP (N-terminal pro-brain type natriuretic peptide); CAD (coronary artery disease); SR (sinus rhythm); AF (atrial fibrillation); SD (standard deviation); LVEF (left ventricular ejection fraction); HFrEF (heart failure with reduced ejection fraction); HFmrEF (heart failure with mildly reduced ejection fraction); HFpEF (heart failure with preserved ejection fraction). All categorical variables are expressed as absolute number and percentage and all continuous variables are expressed as mean ± SD, (range) except NT-proBNP which is expressed as median and 25-75% IQR (interquartile range). Significant p values are in bold.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



