
Submitted:
22 January 2026
Posted:
22 January 2026
You are already at the latest version
Abstract
This paper explores innovation and accountability in spiritual and pastoral care for frontline personnel facing chronic stress, trauma, and moral injury. Police and emergency service psychologists and chaplains operate within stressful and morally charged environments where trauma, psychosocial safety and recovery are constant challenges. Amid such pressures, there is a vital need for credible, evidence-informed, yet deeply human psycho-spiritual frameworks that protect confidentiality while promoting care and wellbeing. Using a Critical Interpretive Synthesis enriched by heuristic and bricolage perspectives, this study integrates recent research across psycho-spirituality, positive psychology, and occupational health. It demonstrates how pastoral carers—particularly chaplains—co-lead moral repair, meaning-making, and value realignment within a biopsychosocial-spiritual (BPSS) framework. From this synthesis emerges a new psycho-spiritual self-care model anchored in humility, self-compassion, and meaningful detachment as virtues that buffer burnout, reduce harsh self-talk, and foster relational safety. Key innovations include early, embedded pastoral interventions; clear referral pathways with clinical partners; and virtue-based micro-skills that complement psychology and medicine while maintaining the integrity of spiritual presence, ritual, and trust. The paper also addresses the enduring tension between institutional demands for measurable outcomes and the ineffable nature of pastoral impact. It proposes blended evaluation indicators such as moral-injury scales (MIOS/MISS-M), spiritual wellbeing tools (FACIT-Sp-12), alliance markers, and organizational climate measures, interpreted heuristically to safeguard authenticity and confidentiality.By reframing pastoral care and chaplaincy as both evidence-informed and spiritually grounded, this paper offers a transformative model for psycho-spiritual care that renews moral resilience and meaning in high-risk professions. Finally, future research possibilities and limitations are also discussed.
Keywords:
self-compassion
; emergency/police chaplaincy
; meaningful detachment
; humility
; stress
; positive psychology
; trauma
Introduction
Frontline emergency response work and policing exposes officers to repeated psychological, moral, and physical harms arising from high-stakes decision-making, traumatic incidents, and sustained public scrutiny. Research consistently highlights elevated risks of post-traumatic stress, moral injury, burnout, and erosion of meaning among emergency response and police personnel (Papazoglou & Tuttle, 2018; Phelps et al., 2023). These harms are not only operational but existential, often leaving officers struggling to reconcile professional duty with personal wellbeing. Within this context, pastoral care and chaplaincy care offers a distinct contribution: a relational, spiritually-attuned presence that provides confidential support, rituals of meaning-making, and pathways for recovery and resilience. Alongside psychologists, chaplains are positioned to help officers process trauma, restore dignity, and reconnect with self-care and human dignity. This complements medical and organisational responses.
Spirituality in its broadest sense, beyond formal religion but not excluding it, and however subjective it is, is recognized as protective against stress and linked to better mental health outcomes (Lusk et al., 2018). Then, by integrating pastoral care into policing cultures, chaplaincy can buffer against the cumulative toll of frontline exposure and sustain both individual wellbeing, spirituality and institutional integrity.
While chaplains provide confidential, relational, spiritually grounded care, crisis support, grief care, and assist in moral repair, complementing clinical services, research is by no means definitive let alone comprehensive (Carey, Hodgson, & Koenig, 2022). Moreover, emergency and police organizations expect measurable outcomes from chaplaincy investments. Chaplains’ impact often lies in intangible even spiritual action and qualities, tender compassion, prayer, presence, trust and meaning-making that resist traditional metrics (Miller & Stephens, 2024). The challenge is to preserve spiritual care and pastoral authenticity while developing credible evaluation aligned with organizational expectations and interdisciplinary practice (Best, Leach, Layson, & Carey, 2024; Devenish-Meares, 2025).
There is also a need to recognize that innovative, structured and evidence-informed emergency/police chaplaincy practices need to integrate well with psychological responses to stress, PTSD, moral injury, and trauma by closing care gaps and integrating spiritual–moral domains into standard biopsychosocial care (Smith-MacDonald et al., 2017). This is because chaplains are often the first trusted contact for distressed service members and can triage, educate, and refer those reluctant to seek clinical help, reducing stigma and accelerating entry to evidence-based treatments (Nieuwsma et al., 2014).
Where possible it is relevant to draw on military and veteran chaplaincy research and practice. So, turning to a military example, programmatic Veteran Affairs (VA)/Defense work has mapped practical pathways for this collaboration, defining chaplains’ roles alongside clinicians, building shared screening and referral protocols, and upskilling chaplains through the Mental Health Integration for Chaplain Services (MHICS) curriculum (VA Mental Health & Chaplaincy, 2021; Nieuwsma et al., 2014). Further, quality-improvement collaboratives across multiple VA/DoD facilities show that integrated chaplain–mental health teams are feasible and improve coordination of care (Nieuwsma et al., 2017).
Finally, emerging models and trials of spiritually integrated care for moral injury are beginning to show how military chaplains co-lead meaning-making, forgiveness, and values-repair work that complements PTSD therapies rather than duplicating them (Cenkner et al., 2021). One wonders if this could be adapted by police chaplains too. Additionally, chaplaincy innovation needs to deepen its connections with and refer to police-related medicine. This is because pastoral care can be a clinically aligned force multiplier that helps more members receive the right care, sooner, with better fit to their moral and spiritual needs.
Aim and research questions
This paper explores innovations and effects of police chaplaincy on stress reduction, meaning-making, and organizational outcomes. It synthesizes innovations and outcomes, addressing tensions between pastoral authenticity and accountability, including balancing confidentiality with organizational reporting.
Research Questions
Against this background, the study has two main questions related to understanding chaplaincy innovation and chaplaincy’s effect:
- What contemporary police chaplain innovation fosters healing, resilience and moral repair among personnel exposed to trauma, stress and moral injury?
- How can chaplains’ effectiveness, noting the deeply personal and subjective nature of pastoral care, be understood and where possible, evaluated in terms of organizational need?
Methodological Approach
The study uses Critical Interpretive Synthesis (CIS), an interpretive, reflexive, theory-generating method suited to chaplaincy’s relational, spiritual, and moral outcomes that resist narrow quantification (Dixon-Woods et al., 2006). CIS acknowledges literature’s disciplinary biases and positions the researcher as an active interpreter within spiritual and psycho-spiritual domains.
In terms of definition, the term spirituality is used more broadly than just religious practice. It is about “lifestyles and practices that embody a vision of human existence and of how the human spirit is to achieve its full potential… embracing an aspirational approach to the meaning and conduct of human life” (Robinson-Edwards & Kewley, 2018, p. 3). This wider focus aligns with both contemporary police and police chaplaincy, where pastoral care seeks to support people spiritually while addressing moral meaning, identity, and belonging often in the context of psychological distress.
CIS proceeds through iterative searching, reviewing, and synthesizing toward conceptual saturation, purposively sampling evidence illuminating innovation and effect. The process involves: (1) systematic database searches; (2) critical appraisal of conceptual contributions; (3) development of synthetic constructs and themes. Overall, the study uses a heuristic lens, drawing on the researcher’s chaplaincy experiences and uses a bricolage approach emphasizing intuition and reflective engagement (Devenish-Meares, 2020; Douglass & Moustakas, 1985; Moustakas, 1990). Here, bricolage is relevant to chaplaincy because pastoral carers often adapt and draw themes and ideas and practices from many sources so long as they are personally relevant to those being care for. This combination grounds findings in lived chaplaincy realities while critically evaluating literature. It is a:
“a tapestry of ideas, themes and possibilities cobbled together to produce creative outcomes. It adapts and co-opts whatever information from whichever discipline that is necessary. This approach appears well suited to the subjective, intuitive nature of workplace stress and suffering and especially where interdisciplinary approaches to self-care are warranted” (Devenish-Meares, 2020, 1).
Literature Review
Building on foundational reflective practice (Schön, 1983) and health professions research on structured reflection supporting healing and reasoning (Mamede & Schmidt, 2004), recent studies (2019–2025) examine chaplaincy outcomes related to moral suffering, spiritual wellbeing, relational alliance, and organisational climate.
Jones et al. (2022) highlighted integration and collaboration between chaplains and mental health providers addressing moral injury. Then, despite growing measurement research, chaplaincy effects remain difficult to quantify. Peery (2012) and Handzo et al. (2014) emphasize the necessity of outcome research for quality and funding. However, chaplaincy’s work with trust, spirituality, and subjective suffering defies conventional metrics (Damen et al., 2020).
Police and emergency personnel value chaplains for confidential counsel, unit presence, and family support (Best et al., 2024). Personnel face chronic operational and organizational stressors increasing burnout and moral injury risk; embedded chaplains provide rapid relational and ethical support (Blumberg, 2022; Correia et al., 2023). In these contexts, scholars call for multidimensional evaluation models integrating spiritual outcomes, relational trust, and moral resilience, noting chaplains’ preference over other care professionals in police settings (Best, Leach, Layson, & Carey, 2024; Carey et al., 2023).
Chaplains are also expected to work in conjunction with those who support people’s medical, social and psychological health. They also encounter negative self-talk so often to do with harsh inner critics, spiritual degradation and the loss of purpose and hope. Moreover, some care frameworks have omitted religious and spiritual elements of moral suffering and distress not only as interventions but as stress response and prevention strategies. So, noting the need for a more holistic perspectives for distress and moral suffering the biopsychosocial-spiritual (BPSS) framework was developed to include spirituality and meaning making. In fact:-
“Current moral models of distress such as moral injury, moral distress, and perceived injustice are aggregated into a larger anthropological model called moral suffering. The BPSS framework addresses the omission of religious and spiritual elements of moral suffering to produce holistic organisational and leadership interventions as primary prevention strategies” (Layson, 2023, 1).
Chaplains are expected to be proactive first responders but are vulnerable to burnout themselves (Braswell & Beamer, 2023). Reflective self-care, mindfulness, and meaning-making sustain chaplain wellbeing as much as they are assisting those who are suffering or ruminating painfully often with negative self-talk and who may have lost hope (Hotchkiss & Lesher, 2018).
Innovations include early interventions, person-centered approaches that specifically address an inability to detach self-caringly. (Devenish-Meares, 2025; Best, Leach, Layson & Carey, 2024).
Research suggests that in these contexts, Chaplains need to be aware of self-compassion, which arises from positive psychology, which plays a crucial protective and therapeutic role in addressing moral injury by fostering acceptance, kindness, and understanding towards oneself and the difficult experiences that constitute moral injury. It counteracts the self-blame, shame, and guilt common in moral injury, promoting well-being and resilience (Udovicich & McLaren, 2025). This in some ways is an innovation for chaplains who while they may have spoken of self-love often, may not be aware of Neff’s (2003) seminal work and related self-administered Self-Compassion Scale (SCS).
Developing self-compassion as a key positive psychological practice, can help individuals to process morally injurious events without harsh self-criticism, encouraging a more realistic and warm response to hardship, which is essential for recovery. This involves encouraging kindness, reduced negative self-talk and a non-judgmental approach to one's own experiences of suffering, failure, and inadequacy (Smith-MacDonald, Morin & Brémault-Phillips, 2018).
In their pastoral practice, chaplains triage often and then support individuals grappling with moral injury by helping them find space to find new meaning after profound ethical breaches and fostering meaningful detachment from the trauma through spiritual and values-based reflection, fostering a path toward acceptance and renewed purpose. This process involves listening and providing a safe space for expression, alongside theological reflection and spiritual care to help individuals process guilt, shame, and betrayal and to reorient themselves toward their core values (Phoenix, 2023). By integrating their experience into a broader spiritual framework, chaplains facilitate a crucial process of life review, reestablishing boundaries and meaning-making allowing for a release from the negative emotional and cognitive burden of the moral injury and even support its repair.
Humility is related to self-compassion and it not about self-deprecation. It can buffer against workplace burnout by fostering a resilient mindset George, Wallace, Snider & Suh, 2024). It is also about having a realistic understanding of one’s reality. Such are better able to cope with setbacks by reframing negative experiences, enhancing their self-regulatory and coping skills. This internal resource helps to prevent the depletion of personal resources that leads to exhaustion, cynicism, and feelings of inefficacy, key components of burnout.
In terms of moral injury and distress, Carey et al. (2023) evaluated Pastoral Narrative Disclosure (PND), a chaplain-led trauma and moral injury intervention, reporting positive usability and user perception. Recent reviews identify three wellbeing domains for clergy and chaplains: individual, relational, and institutional. Chaplain presence correlates with reduced burnout and improved professional fulfillment among health professionals (Gaines et al., 2023). Chaplains support colleagues through brief reflective conversations, moral distress support, enable realistic knowledge and bereavement rituals, especially during critical incidents (Knapp et al., 2025).
Then, while not an emergency services nor police example but of relevance, the Australian Royal Commission into Defence and Veteran Suicide (2024) called for cultural reform, transition support, and research to prevent deaths. In terms of this, chaplaincy programs which emphasise interdisciplinary collaboration and proactivity support system reforms They also requires chaplain to be proactive in triaging, screening for moral injury and enabling self-care (Devenish-Meares, 2025).
Moral Injury: Concepts, Prevalence, and Consequences
Moral injury (MI) is central to pastoral care and to chaplaincy, in particular in military and police settings. In terms of this, Litz et al. (2022) introduced the Moral Injury Outcome Scale (MIOS), the first validated intervention outcome measure. Mensink et al. (2022) found distinct MI profiles in police and veterans, underscoring tailored chaplaincy responses. Crucially too it must be noted that approximately 44% of treatment-seeking veterans and police met MI symptom profiles, often comorbid with PTSD (Mensink et al., 2022). Therefore, routine MI screening is recommended, recognizing MI extends beyond guilt and shame to existential loss, spiritual crisis, and moral disorientation (Griffin et al., 2019).
Military care programs like Moral Injury Skills Training and Pastoral Narrative Disclosure help in occupational MI and bereavement (Carey, 2025; Liuski & Ubani, 2020; Oosterhuis, Olsman & Vos, 2025). More particularly in a police setting but of use to moral injury responses, Phelps et al. (2023) proposed a holistic police chaplain model emphasizing confidentiality, ritual leadership, and organizational support. Generic mental health metrics may miss MI’s spiritual dimensions; targeted instruments include MIES (Nash et al., 2013), MISS-M (Koenig et al., 2018), Expressions of Moral Injury Scale (Tao et al., 2023), and MIOS (Litz et al., 2022). Finally, MIOS is also emerging as a benchmark for recovery assessment.
Police chaplaincy research is closing gaps between conceptual frameworks and measurable practice (Phelps et al., 2023). Complementary measures include FACIT-Sp-12 for spiritual wellbeing (Peterman et al., 2002). The U.S. Department of Veterans Affairs notes moral-injury-specific interventions are nascent but growing, with chaplains co-leading group modalities focused on moral repair, forgiveness, and meaning-making (Beech et al., 2024; Cenkner et al., 2021; Nieuwsma et al., 2025). It must also be noted here that these are inherently subjective and deeply personal issues where chaplains are expected to support people who may not be able to detach self-lovingly let alone get new perspectives. Rather they engage in harsh, negative self-talk (Devenish-Meares, 2018).
Again, Australian and New Zealand police research shows chaplains are accessible and aligned with officers’ preferences for support after morally transgressive events, valued for narrative repair, spiritual care, and pragmatic accompaniment (Phelps et al., 2023). This is relevant too because organizational justice and identification correlate with lower burnout; chronic demands predict higher burnout and turnover (Correia, Romão, Almeida & Ramos, 2023; Baker et al., 2023). Then, the International Association of Chiefs of Police (IACP) defines chaplaincy’s role within integrated wellness systems emphasizing confidentiality and boundary clarity (IACP, 2023; Amundson, 2023).
Overall, authentic, discretionary, whole-person care fosters positive perceptions (Gaines et al., 2023). However, this will require a chaplain to support self-care, boundary-setting and confidentiality while maintaining accountability (Devenish-Meares, 2025).
Self-Reflection: Formative but Insufficient
Reflective practice aids adaptive reasoning, moral awareness, and growth (Schön, 1983; Mamede & Schmidt, 2004; Doehring, 2015). However, self-assessment is prone to bias and inaccuracies (Eva & Regehr, 2005, 2008; Mann et al., 2009). Reliable evaluation requires augmenting reflection with supervision, peer review, and external data triangulation. Despite subjectivity, reflective capacity remains essential for professional competence (Mann et al., 2009).
Measurement: Instruments and Multi-Level Indicators.
Individual-level measures include ProQOL-5 (compassion satisfaction, burnout, secondary traumatic stress) (Stamm, 2010), Maslach Burnout Inventory (Maslach et al., 2016), FACIT-Sp-12 for spiritual wellbeing (Peterman et al., 2002) and Working Alliance Inventory for pastoral relationship (Horvath & Greenberg, 1989). MI-specific tools include MIES, MISS-M/SF, EMI-M, and MIOS (Nash et al., 2013; Koenig et al., 2018; Litz et al., 2022). Then, police research recently has used qualitative-quantitative hybrids mapping MI phenomenology and help-seeking, often employing MIOS (Phelps et al., 2023).
Implementation Approaches and Real-World Learning
Again, chaplains are trusted points of contact for veterans facing moral injury and suicidality (Smigelsky et al., 2020). They must be continually open to learning and innovation which includes MHICS which provides chaplains with a structured curriculum in mental health concepts and evidence-based practices). This fosters collaboration with mental health professionals (MIRECC & CoE, 2021). Further, Acceptance and Commitment Therapy (ACT) relates to self-compassion (Neff, 2003). This is because ACT strengthens workers’ psychological flexibility, while self-compassion ensures that this flexibility is underpinned by kindness rather than self-criticism. Together, they create a powerful approach to help workers manage stress, reduce negative thoughts and recover from setbacks. Improved workplace psychological climate may also result from such integrated approaches (Wolgast, Sandeberg, et al. 2024).
Virtues in Practice: Humility, Meaningful Detachment, and Self-Compassion
Building on the foregoing research on self-kindness, addressing negative thoughts, taking self-responsibility, innovative chaplaincy fosters confidential, relational, proactive, and healing-focused support that enhances resilience and counters policing cultures of stoicism and emotional suppression (American Police University, 2023; Devenish-Meares, 2025). These cultures often discourage vulnerability, increasing burnout and moral injury risk.
Earlier, too the recent work on how religious and spiritual elements of moral suffering and distress are being responded to in a healing way with self-criticism and loss of hope were identified. What arose from an intuitive literature search, a focus on an integrated BPSS model and the need to respond holistically to suffering, were three themes related to self-awareness, the risk of harsh self-criticism, lack of self-kindness especially in terms of moral injury and workplace stress and burnout. These three themes are:
• Humility: Accurate self-view, compassion-focused self-knowledge (even when failure is perceived), openness, and non-dominating presence foster trust and psychological safety (Devenish-Meares, 2021; Chintakananda et al., 2024; Luo et al., 2022). It can be taught and modeled, reducing stigma and encouraging help-seeking (Rego et al., 2021; Amundson, 2023). The Comprehensive Intellectual Humility Scale measures this virtue (Krumrei-Mancuso & Rouse, 2016).
• Meaningful Detachment: Tender emotional distancing that allows processing without rumination or enmeshment (Devenish-Meares, 2021; Neff, 2003a). Occupational measures like the Recovery Experience Questionnaire and detachment indices assist assessment (Sonnentag & Fritz, 2007; Sonnentag & Kühnel, 2016).
• Self-Compassion: Defined by self-kindness, common humanity, and mindful awareness, it enables chaplains to model grace and sustain resilience (Neff, 2003; Devenish-Meares, 2018, 2021). Self-compassion buffers compassion fatigue and burnout (Neff & Germer, 2013; Zessin et al., 2015). The Self-Compassion Scale (SCS) correlates with wellbeing and emotion regulation (Neff, 2023). Mindful Self-Compassion training shows benefits for helping professionals (Neff & Germer, 2013).
These virtues are self-determining yet relational catalysts that support personal care while fostering organisational psychological safety and openness to moral repair (Luo et al., 2022; Chintakananda et al., 2024). Research cautions that psychometrics like the SCS must be paired with heuristic interpretations to avoid misrepresentation. In fact Lopez et al (2015) challenged the common practice of reporting a single total SCS score and argued that self-compassion and self-criticism are separate constructs best measured distinctly. Specifically too, the SCS can be subject to substantial conscious and unconscious bias and be at least in part be determined by social not personal factors Muris & Otgaar, 2020).
Conclusion
Recent literature supports evaluating chaplaincy effectiveness in terms honouring its unique contributions to moral repair, spiritual care, and relational safety, especially in defence and policing where moral stressors are chronic and systemic. In innovative terms, the field is progressing toward outcome targets aligned with chaplaincy (MIOS, MISS-M/SF, spiritual wellbeing, alliance), self-compassion, enhancements to how a suffering person detaches emotionally and implementation models embedding chaplains in multidisciplinary systems and psychosocial safety climate action. However, emergency services/police chaplaincy research remains limited compared to police contexts. More research on innovations, effects, policy, and evaluation is needed (Best, Leach, Layson & Carey, 2024; Devenish-Meares, 2025; Liuski & Ubani, 2020).
Discussion
Using CIS and heuristic perspectives, some aspects of chaplaincy are both empirically evaluable and a vocational practice embedded in relational, moral, and spiritual realities (Devenish-Meares, 2018, 2021, 2025). Yet, a central tension exists between organisational demands for measurable outcomes and chaplaincy’s subjective, person-centred spiritual and pastoral support (Schön, 1983; Doehring, 2015). Outcome tools like MIOS and FACIT-Sp-12 provide benchmarks but risk reducing chaplaincy to clinical analogues if used without interpretive care.
Chaplains may discern change, such as increased self-acceptance even healing through subtle shifts in trust, relationships, moral orientation, coping, propensity to seek help or renewed hope. Chaplaincy practice must be highly adaptable and this requires innovation. Thinking heuristically, this could be consider activating a bricolage of spiritual care, modelling improved self-talk, prayer, ritual, narrative, humour, silence, and ethical accompaniment, integrating referrals as needed noting that it all needs to work within a BPSS framework (Devenish-Meares, 2025). This resists linear evaluation but produces trust, resilience, relational safety, and moral repair (Carey, Hodgson & Koenig, 2022; Phelps et al., 2023). In all this, a multi-faceted approach is needed. This is the use of validated outcome tools which can demonstrate reality, while pastoral care fosters hope, meaning-making, self-compassion, and trust. Innovation need to resist binary empirical-experiential distinctions and heuristic inquiry keeps chaplains’ intuitive and embodied knowing at the centre of their practice.
Integrating Moral Injury and Organizational Determinants
MI has transformed chaplaincy in both police and military contexts (Mensink et al., 2022; Phoenix Australia, 2023). Chaplain responses focus on shame, betrayal, trust loss, and spiritual crisis (Griffin et al., 2019). Tools like MIES, MISS-M, and MIOS enable effective screening and response (Koenig et al., 2018; Nash et al., 2013; Litz et al., 2022). However, relational and spiritual processes—rituals, lament, narrative repair—are essential chaplain competencies (Carey et al., 2023; Smigelsky et al., 2022).
Again, chaplains discern progress through embodied knowing and subtle signs such as sighs, reduced rumination, storytelling and reengagement with relationships and even community return. Burnout, role conflict, justice perceptions, and psychosocial safety climate also drive chaplaincy innovation (Correia, Romão, Almeida & Ramos, 2023; Hydinger et al., 2024).
Three central virtues, humility, meaningful detachment, and self-compassion, help define effective chaplaincy and support those with moral injury and can assist in caring for those with burnout by fostering trust, self-care, and mindfulness (Devenish-Meares, 2018, 2021; Hydinger et al., 2024; Khatib et al., 2022; Rego et al., 2021).
Humility enables non-dominating awareness, meaningful detachment protects against enmeshment and rumination, and self-compassion sustains self-care even resilience. These virtues also foster organizational psychological safety (Luo et al., 2022; Chintakananda et al., 2024). To assist, validated measures such as Recovery Experience Questionnaire, detachment indices, and the Self-Compassion Scale, offer opportunities to care yet require heuristic interpretation to avoid misrepresentation (Lopez et al., 2015; Muris & Otgaar, 2020).
New Conceptual Framework
Recalling, the biopsychosocial-spiritual (BPSS) framework developed to include spirituality and meaning making, the literature review and synthesis produced concepts such as meaningful detachment, humility and self-compassion which serve as ways, even enablers, to address stress and assist in moral repair. This is about supporting safe space for expression, alongside improved and non-judgmental self-talk and reflection and spiritual care which may help individuals process guilt, shame, and betrayal and to reorient themselves toward their core values.
In the context of confidentiality, which is also an enabler, chaplains have so often focussed on self-love but not necessarily on self-compassion (Neff, 2003). In actuality, virtues, practices and choices offered by an innovative chaplain could lead to individual, relational and organisational outcomes. Specifically, in the context of listening to narratives and helping to ensure psychological safety, moral repair may begin and negative self-talk reduction occur.
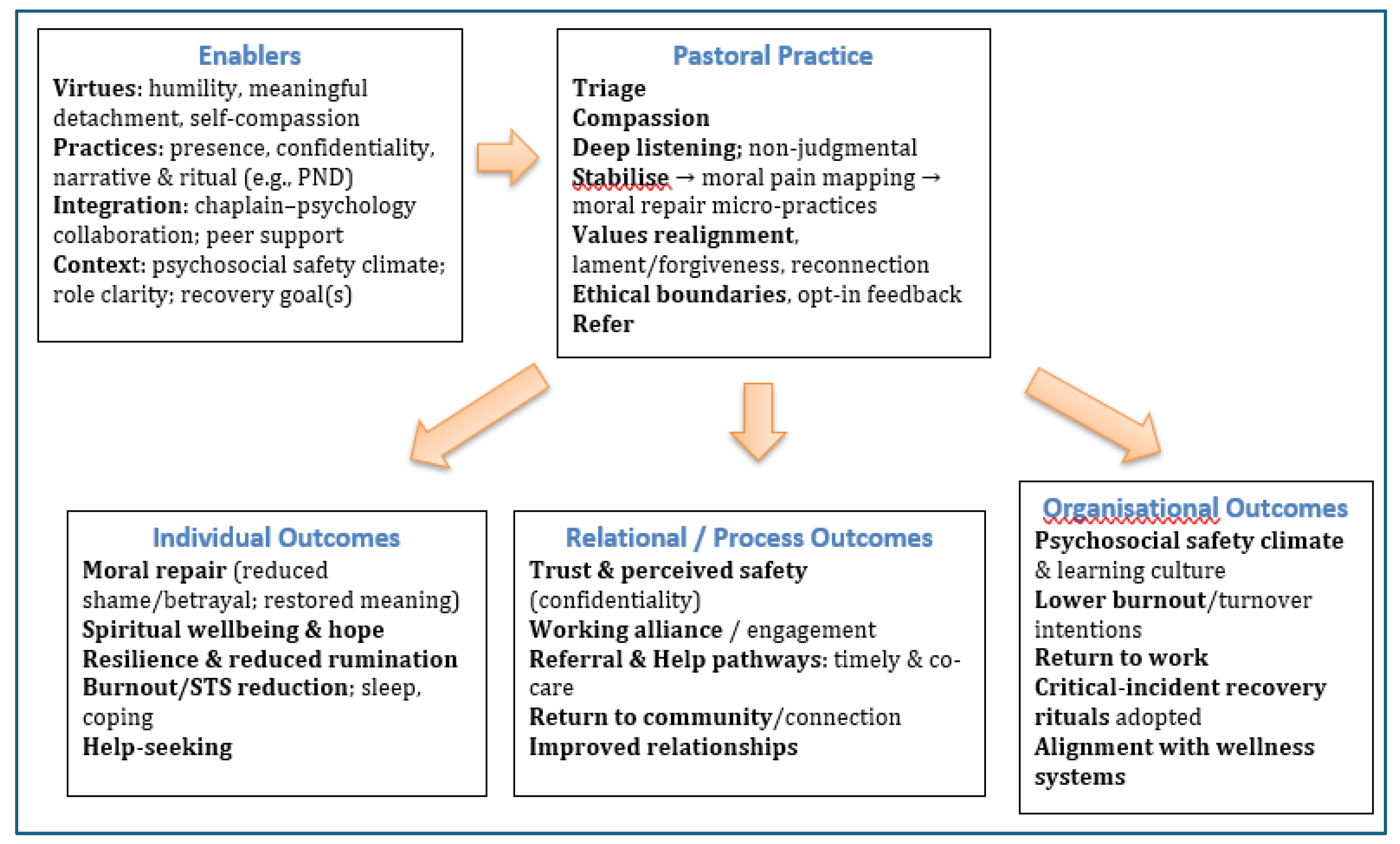
Relationally, it may lead to renewed trust, necessary and holistic referrals to other carers and some return to relationships even to community. Finally, in the organisation, safety, addressing the adverse effects of critical incidents and strengthening wellbeing may occur with the right mix of actions and interventions. To assist, these multi-faceted enablers, practices and outcomes (individual, relational and organisational) are illustrated in a Pastoral Action Concept Map. It is hoped that this draft map could also assist in building inter-disciplinary collaboration between chaplains, psychologists and medical doctors working in the treatment of emergency service and police-related, mental health injury and illness, trauma and stress and burnout.
Figure 1.
Pastoral Action Concept Map: enablers, practices and outcomes
Re-Imagining Chaplaincy Effectiveness
Chaplains operate within institutional climates where justice, workload, and psychosocial safety shape wellbeing and impact (Baker et al., 2023). It also needs to integrate well with police-related medicine’s response to PTSD, moral injury, and trauma. Evaluation can erode authenticity if imposed too narrowly or quickly, or if managerial language alienates care recipients (Miller & Stephens, 2024). Flexible, bricolage-informed methods—delayed, opt-in feedback, aggregate reporting, de-identified narratives—respect confidentiality while generating actionable insights (Devenish-Meares, 2025).
Chaplaincy effectiveness in police contexts is best understood as an interpretive bricolage integrating personal pastoral care with tender compassion and where relevant, validated outcome tools (MIOS, FACIT-Sp-12, ProQOL-5), process indicators (Working Alliance, supervision), organizational metrics (psychosocial safety climate, burnout), and heuristic insights (pastoral intuition, ritual efficacy, narrative repair). This hybrid approach legitimizes chaplaincy to organizations while preserving pastoral authenticity. Irrespective, without external feedback, structured outcome measurement, and reference to empirical literature, reflective insights risk remaining subjective impressions rather than validated improvements.
Finally, to assist chaplaincy practitioners and inform related mental health and medical professionals, a playbook guide, distilled from this paper’s synthesis and findings is shown in the Appendix called; Police Pastoral Guide: Innovative Chaplaincy for Stress & Moral Injury: A (brief) pragmatic playbook. It is hoped that this guide may also enable professional cooperation and improved understanding between caring disciplines.
We must also bear in mind that reflection alone does not guarantee effective, safe care; it must be supplemented by external feedback, structured measurement, and empirical reference to avoid subjective bias (Schön, 1983; Mamede & Schmidt, 2004).
Limitations
This synthesis is limited by the fact that CIS relies heavily on researcher interpretation, which can introduce subjectivity and reflexivity bias; the study acknowledges this and attempts to mitigate it through methodological transparency. There was also a relative scarcity of contemporary police chaplaincy research compared to police contexts. This limits the breadth of evidence available for synthesis, a limitation inherent to the field rather than the method. Moreover, while CIS is flexible, it may lack the replicability and rigor of more structured systematic reviews, but this trade-off is justified given the study’s exploratory and theory-building goals.
Many studies use qualitative or cross-sectional designs, limiting causal inference. Heuristic and bricolage methods, while insightful, carry subjectivity and reflexivity bias (Devenish-Meares, 2020). Longitudinal research tracking chaplaincy impact over careers or deployments is scarce, leaving durability of outcomes under-evaluated.
Future Research
Significant gaps remain in police chaplaincy research (Phelps et al., 2023). Future studies should prioritize pragmatic, multisite trials using mixed methods combining quantitative indicators with qualitative narratives and reflective journals (Eva & Regehr, 2005; Mann et al., 2009). Praxis can be enhanced through interprofessional collaboration, as exemplified by VA’s MHICS training integrating clinical modalities with pastoral care (MIRECC & CoE, 2025).
Future research should be supported by expanded methodological and contextual scope, employing mixed-methods and longitudinal designs combining validated instruments with qualitative narrative and reflective data. Embedding chaplaincy within organizational climate frameworks like psychosocial safety climate is essential (Dollard & Bakker, 2010). Greater focus on pastoral virtues such as humility, detachment, self-compassion, as self-care and care-enhancing practices is recommended (Devenish-Meares, 2018, 2021; Neff & Germer, 2013). Intervention studies should examine how training and supervision in these virtues improve chaplain wellbeing and support capacity.
Summary and Conclusion
Chaplains in police settings provide indispensable, complex care at the nexus of moral injury, organizational wellbeing, and spiritual care. Their unique psycho-spiritual contributions cannot be replaced by clinical or managerial services. Despite evaluation challenges, emerging research shows chaplains and their modelled virtues enhance resilience, facilitate moral repair, and safeguard psychosocial safety in high-risk institutions (Gaines et al., 2023; Phelps et al., 2023).
Moral injury is a central organizing framework linking chaplaincy to lived moral and spiritual struggles (Mensink et al., 2022; Carey, Hodgson & Koenig, 2022). Pastoral stances of humility, meaningful detachment, and self-compassion are foundational (Devenish-Meares, 2021; Neff, 2003). Integrating these virtues into practice and measurement offers an innovative approach to professional effectiveness, equipping chaplains with theological, pastoral, and resilience-sustaining skills.
Balancing authenticity, relationality, and virtue-driven care with credible outcome measures and organizational expectations is essential. A bricolage approach expands evaluation beyond technical metrics to include empirical evidence and pastoral wisdom (Devenish-Meares, 2020). Chaplaincy effectiveness cannot be reduced to clinical or managerial outcomes alone.
Embedding chaplains within psychosocial safety initiatives, adopting mixed-methods evaluation, and safeguarding confidentiality preserve chaplaincy authenticity. Evaluation is not a threat but a necessary means to refine practice, demonstrate value, and sustain chaplaincy’s trusted role in institutions marked by trauma, moral stress, and operational intensity.
Police Pastoral Care Guide:
Innovative Chaplaincy for Stress: A (brief) pragmatic playbook1
--------------------------------------------------------------------------------------------------------------------
1) Quick-start: what matters in your first 24–48 hours
Your posture: be present, open, humble, boundaried, trustworthy.
Your aim: stabilise, protect dignity, surface meaning, and connect to supports.
Your guardrails: confidentiality (within policy), “do no harm,” informed consent,
opt-in. Constantly check with other mental health professionals
Rapid contact checklist (10–15 minutes)
- Make contact where they are (parade ground, station, patrol room, mess, family setting).
- Micro-grounding (60–90 sec): “Feet on the floor, slow breath in… out. Right now you’re safe with me.”
- Name the moral or distress signal (guilt, shame, betrayal, moral confusion, grief, anger).
- Normalize + permission: “Many in your role feel this; you don’t have to carry it alone.”
- Confidentiality script (adapt locally): “I’m here as your chaplain. Our conversation is confidential except for immediate risk to life or mandated reporting. I don’t write performance reports nor tell your team or team leader. This space is for you.”
- Triage decision: Immediate risk? If yes → activate emergency protocol; if no/unsure → continue chaplaincy care pathway while seeking help, advice and assistance.
2) Core pathway for moral injury & high moral stress
- Purpose: offer a repeatable, humane sequence blending pastoral care, light-touch measurement, and collaboration.
Step A - Stabilise & locate the wound (15–30 min)
- Containment: posture, breath, quiet room; “We’ll take this slowly.”
- Name the moral pain: “What value feels violated? Whose trust feels broken?”
- Offer solidarity, not solutions: “You’re not broken; you’ve been hurt in a moral way.”
Step B - Screen & choose a lane (5–10 min)
Use brief, acceptable tools (select one per domain; keep it light):
- Moral injury exposure/symptoms: brief items from MIES / MISS-M(SF) / MIOS.
- Spiritual well-being: FACIT-Sp-12 short.
- General distress (if needed): DASS-21 short.
- Alliance/process: one Working Alliance item (“Do you feel this time is helpful?”).
Decision lanes:
- Lane 1 - Watchful Waiting + Pastoral Care: mild burden; schedule follow-up.
- Lane 2 - Chaplain-led Moral Repair: moderate MI load; offer Pastoral Narrative Disclosure (PND) elements, lament/forgiveness ritual, meaning-mapping, values repair.
- Lane 3 - Co-facilitation / Referral: severe symptoms or safety issues; coordinate with psychology/GP/peer support; remain spiritually present.
Step C — Moral repair micro-practices (15–40 min)
- Narrative repair: invite the story, pace the hardest parts, mark turning points.
- Lament & acknowledgement: “What needs naming out loud?” (ritual optional: candle, coin, soil, scripture/prayer/poem).
- Re-alignment: surface core values; one small act to realign life with values this week.
- Forgiveness work (when approp): responsibility, remorse, repair, release—never rush it.
- Community re-link: partner, family, trusted colleague, faith group, veteran peer group.
Step D — Close & plan (5–10 min)
- Self-compassion practice (60-120 sec): hand on chest, slow breath, phrase: “This is painful. Others at work know this pain. May I be kind to myself & do what’s wise next
- Meaningful detachment for next shift: Stop ritual at gate; Body reset (walk, shower); Re-entry intention (who/what matters after work).
- Book the next contact and, with consent, note a tiny outcome marker (e.g., slept 5 hours, told partner, attended ritual).
3) Micro-skills that lift effectiveness
Humility (relational safety amplifier)
- Behaviours: ask before advising; honour the person’s wisdom; admit your limits; invite collaboration
- Phrases: “You’re the expert on your experience; I can walk with you.” / “If this doesn’t help, tell me and we’ll try something else.”
Meaningful detachment (boundary-keeping with warmth)
“We must take the risk of legitimate attachment (fully feeling the emotion), learn its important message, and then have the presence and purpose to detach from that fascinating emotion after it has done its work. This is the gift and power of an emotionally mature person”. Richard Rohr
- Behaviours: empathic presence + clear edges; time-bound sessions; deliberate handover when risk rises.
- Phrases: “I’m with you in this, and I’ll also help you connect with X for the parts outside my lane.” / “Let’s hold the story here for today; we’ll pick it up safely next time.”
Self-compassion (burnout buffer & modelling tool
- Daily 3-minute reset: breathe, name a stressor, offer kind words, choose a wise next step
- After-care for you (post-critical event): peer check-in, brief reflection note, hydrating/food, movement, sleep target, micro-Sabbath. Seek regular supervision.
4) Working with the system (PSC) so chaplaincy can actually work
- Brief leadership (10 minutes): top 3 moral stressors; one practice helping; one barrier command can remove; ask for one Psychosocial Safety Climate (PSC) action this month.
- Integrate, don’t compete: monthly touchpoint with peer support, psychology, welfare etc.
- Protect confidentiality: reaffirm in every commander changeover and incident review.
5) Documentation & evaluation without killing the soul of the work - ethical, light-touch
- Log (de-identified where possible): contacts, themes, lane chosen, brief outcome at follow-up, referrals, rituals.
- Avoid logging identifying moral content without consent.
- Use delayed, opt-in feedback (2–6 weeks) with a one-item pulse (“Did chaplain support help you move one step toward what matters?”).
A minimalist measurement bundle (pick 2–3)
- MI focus: brief items adapted from MIOS or MISS-M(SF) (local approvals).
- Spiritual well-being: FACIT-Sp-12 short.
- Burnout/STS: ProQOL-5.
- Alliance/process: 1–2 Working Alliance items.
6) Longer term care (7–30 days)
- Narrative & Ritual: embed a simple lament/meaning ritual after hard calls; co-design language; train 2 peer champions; success = officers ask for it next time.
- Detachment at the Gate: end-of-shift 3-minute protocol; cue card at locker; success = earlier switch-off reports.
- Chaplain + Psych 2-hander”: 4–6 session MI group; agenda: values, lament, forgiveness, reconnection; closing ritual; success = shame reduction, renewed belonging.
7) Personal sustainability for chaplains (non-negotiables)
- Regular supervision (spiritual/clinical).
- Peer round (15 min) after tough call: what I noticed / carried / am setting down.
- Borders: fixed off-duty windows; say “not now—tomorrow 0900?” and keep it.
- Three anchors: movement, presence/prayer/quiet, friendship.
- Red flags: persistent cynicism, sleep collapse, secrecy about coping ..escalate.
8) One-page scripts & prompts
- Opening: “What’s the part of this that hurts most to remember?” / “If a trusted mate had lived this, what would you say to them?”
- Values repair: “Which value got bent or broken—loyalty, fairness, duty, care, truth?” / “Name one small act this week that honours that value.”
- Forgiveness (when appropriate): “Is there anything to ask or offer in forgiveness—toward yourself, another, God?” / “What would repair look like, even one small step?”
- Close: “Between now and our next chat, what would kindness to yourself look like?” / “Who could safely walk with you for the next few days?”
9) Rapid Chaplaincy Pathway (flow chart) – see attached
Print and place in notebook or duty folder.
10) Leader briefing card (for commander ‘catch-ups’)
- What we’re seeing: 2–3 moral stressors.
- What’s working: (one) 1 pastoral/peer practice.
- What blocks impact: (one) 1 system friction (rostering, space, role confusion).
- One PSC action to authorise this month (specific, small, public).
| 1 | This brief guide is for ‘information purposes’ only and meant to stimulate the reader to seek professional training and development. It is not intended to offer clinical instructions. Every personal circumstance is different and requires clinical and medical triage and assessment by qualified mental health and medical practitioners. |
References
- American Police University. (2023). The stoic cop: A philosophy for law enforcement. https://www.amu.apus.edu/area-of-study/arts-and-humanities/resources/the-stoic-cop/.
- Ames, D., Erickson, Z. D., Geise, C., Tiwari, S., Sakhno, S., Sones, A. C., Tyrrell, C. G., Mackay, C. R. B., Steele, C. W., Van Hoof, T., Weinreich, H., & Koenig, H. G. (2021). Treatment of moral injury in U.S. veterans with PTSD using a structured chaplain intervention. Journal of Religion and Health, 60, 3052–3060. [CrossRef]
- Amundson, G. J. (2023). Law enforcement chaplains: A confidential resource. FBI Law Enforcement Bulletin. https://leb.fbi.gov/articles/featured-articles/law-enforcement-chaplains-a-confidential-resource.
- Baker, L. D., Richardson, E., Fuessel-herrmann, D., Ponder, W., & Smith, A. (2023). Police burnout and organizational stress: job and rank associations. Policing: An international Journal, 46(4), 682-693.
- Beech E. H., Mackey, K. M., Parr, N. J., Baltich Nelson, B., Young, S & Belsher B. E. (2024). Moral Injury and Mental Health Among US Police Service Members and Veterans: A Systematic Review and Evidence Overview. Evidence Synthesis Program, Health Systems Research, Office of Research and Development, Department of Veterans Affairs.
- Best, M., Leach, K., Layson, M. & Carey, L. (2024). Police Perspectives on the Provision of Spiritual Care in the Australian Defence Force: A Cross-Sectional Study. Journal of Religion and Health, 63(1). 289-308. [CrossRef]
- Blumberg, D. M. (2022). What Should Clinicians Who Care for Police Officers Know About Moral Injury? AMA Journal of Ethics, 24(2), E126-E132.
- Braswell, R., Beamer, A. (2023). Role of the Chaplaincy. In: Bourke, M.L., Van Hasselt, V.B., Buser, S.J. (eds) First Responder Mental Health. Springer, Cham. [CrossRef]
- Carey, L. B., & Hodgson, T. J. (2018). Chaplaincy, Spiritual Care and Moral Injury: Considerations Regarding Screening and Treatment. Frontiers in Psychiatry, 9, Article 619. DOI: 10.3389/fpsyt.2018.00619.
- Carey, L. B. (2025). Police Chaplaincy, Moral Injury, Pastoral Narrative Disclosure, Bereavement and Spiritual Research Contamination, Health and Social Care Chaplaincy, 12(3).
- Carey, L. B., Bambling, M., Hodgson, T. J., Jamieson, N., Bakhurst M. G., & Koenig, H. G. (2023). Pastoral Narrative Disclosure: The Development and Evaluation of an Australian Chaplaincy Intervention Strategy for Addressing Moral Injury. Journal of Religion and Health, 62(6), 4032-4071.
- Carvalho, K. B. (2024). Law enforcement trauma: Can chaplains help? Christianity Today, May. https://www.christianitytoday.com/2024/05/law-enforcement-trauma-can-chaplains-help/.
- Chintakananda, K., Diefendorff, J. M., Oc, B., Daniels, M. A., Greguras, G. J., & Bashshur, M. R. (2024). Leader-Expressed Humility: Development and Validation of Scales Based on a Comprehensive Conceptualization. Journal of Business Ethics, 192(1), 129-146. [CrossRef]
- Correia, I., Romão, Â., Almeida, A. E., & Ramos, S. (2023). Protecting Police Officers Against Burnout: Overcoming a Fragmented Research Field. Journal of Police and Criminal Psychology, 38(3), 622-638.
- Damen, A., Schuhmann, C., Leget, C., & Fitchett, G. (2020). Can outcome research respect the integrity of chaplaincy? A review of outcome studies. Journal of Health Care Chaplaincy, 26(4), 131-158.
- Devenish-Meares, P. (2018). A newer form of psycho-spiritual detachment to support those suffering at work. Journal of Spirituality in Mental Health, 20(2), 140-166.
- Devenish-Meares, P. (2020). The ‘tapestry’ of bricolage: Extending interdisciplinary approaches to psycho-spiritual self-care research. Methodological Innovations, 13(1), 2059799119898410.
- Devenish-Meares, P. (2021). Humility at work: a dynamic personal and leadership choice and strategic multiplier! Academia Letters, Article 1553. [CrossRef]
- Devenish-Meares, P. (2025). Strengthening Workplace Pastoral Care in Police, Paramedic and Police Settings: Chaplaincy Confidentiality, Proactivity, Proximity & Referral Options. International Journal of Academic Research in Business and Social Sciences, 15(3), 1134-1154.
- Dixon-Woods, M., Cavers, D., Agarwal, S., Annandale, E., Arthur, A., Harvey, J., ... & Sutton, A. J. (2006). Conducting a critical interpretive synthesis of the literature on access to healthcare by vulnerable groups. BMC Medical Research Methodology, 6(1), 35. [CrossRef]
- Doehring, C. (2015). The practice of pastoral care (revised). Westminster John Knox Press.
- Dollard, M. F., & Bakker, A. B. (2010). Psychosocial safety climate as a precursor to conducive work environments, psychological health problems, and employee engagement. Journal of Occupational and Organizational Psychology, 83(3), 579-599. [CrossRef]
- Douglass, B. G., & Moustakas, C. (1985). Heuristic inquiry: The internal search to know. Journal of Humanistic Psychology, 25(3), 39-55. [CrossRef]
- Eva, K. W., & Regehr, G. (2005). Self-assessment in the health professions: A reformulation and research agenda. Academic Medicine, 80(10), S46–S54. [CrossRef]
- Gaines, A. F., Rangel, T. L., Freedberg, R., Doucette, S., Stengem, D., Timmerman, R., ... & Colorafi, K. (2023). Relationships between perceived importance of chaplain presence and health professionals’ emotional well-being in the United States. Journal of religion and health, 62(3), 1546-1560.
- George, L., Wallace, J. C., Snider, J. B., & Suh, H. (2024). Self-compassion, performance, and burnout: Surfacing an unknown work construct. Group & Organization Management, 49(5), 1280-1324.
- Griffin, B. J., Purcell, N., Burkman, K., Litz, B. T., Bryan, C. J., Schmitz, M., ... Maguen, S. (2019). Moral injury: An integrative review. Journal of Traumatic Stress, 32(3), 350-362. [CrossRef]
- Handzo, G. F., Cobb, M., Holmes, C., Kelly, E., & Sinclair, S. (2014). Outcomes for professional health care chaplaincy: An international call to action. Journal of Health Care Chaplaincy, 20(2), 43-53. [CrossRef]
- Hodgson T. J., Carey L. B., & Koenig H. G. (2022). Moral Injury, Betrayal and Retribution: Australian Veterans and the Role of Chaplains. Journal of Religion and Health, 61(2), 993-1021. [CrossRef]
- Hotchkiss, J. T., & Lesher, R. (2018). Factors predicting burnout among chaplains: Compassion satisfaction, organizational factors, and the mediators of mindful self-care and secondary traumatic stress. Journal of Pastoral Care & Counseling, 72(2), 86-98. [CrossRef]
- Horvath, A. O., & Greenberg, L. S. (1989). Development and validation of the Working Alliance Inventory. Journal of Counseling Psychology, 36(2), 223-233.
- Hydinger, K. R., Wu, X., Captari, L.E. et al. (2024). Burnout, Trauma Impacts, and Well-Being Among Clergy and Chaplains: A Systematic Review and Recommendations to Guide Best Practice. Pastoral Psychol 73, 587-608. [CrossRef]
- International Association of Chiefs of Police. (2023). Officer safety and wellness: Chaplaincy resources (web resource). https://www.theiacp.org.
- Jones, K. A., Freijah, I., Carey, L., Carleton, R. N., Devenish-Meares, P., Dell, L., Rodrigues, S., Madden, K., Johnson, L., Hosseiny, F., & Phelps, A. J. (2022). Moral injury, chaplaincy and mental health provider approaches to treatment: A scoping review. Journal of Religion and Health, 61(2), 1051-1094. [CrossRef]
- Khatib, L., Glaser-Reich, J., Mosbey, D., Oliva, V., Riegner, G., Dean, J. G., ... & Zeidan, F. (2022). Mindfulness meditation training reduces aggression and improves well-being in highly stressed law enforcement officers. Journal of Police and Criminal Psychology, 37(4), 972-983. [CrossRef]
- Knapp, S., Schaefer, B., Stratton, R. G., Usset, T. J., K Yadav, S., & Fitchett, G. (2025). Chaplain care for health care colleagues: a scoping review. Journal of Health Care Chaplaincy, 31(1), 1-30. [CrossRef]
- Koenig, H. G., Ames, D., Youssef, N. A., Oliver, J. P., Volk, F., Teng, E. J., ... Pearce, M. (2018). The Moral Injury Symptom Scale–Police Version: Reliability and validity. Journal of Religion and Health, 57(1), 249-265. [CrossRef]
- Krumrei-Mancuso, E. J., & Rouse, S. V. (2016). The development and validation of the Comprehensive Intellectual Humility Scale. Journal of Personality Assessment, 98(2), 209–221. [CrossRef]
- Layson, M. (2023). Developing a Biopsychosocial-Spiritual Framework to Prevent Moral Suffering (Moral Injury) in Trauma-Exposed First Responder Communities. [Doctoral Thesis, Charles Sturt University]. Charles Sturt University.
- Litz, B. T., Plouffe, R. A., Nazarov, A., Murphy, D., Phelps, A., Coady, A., ... & Consortium, M. I. O. S. (2022). Defining and assessing the syndrome of moral injury: Initial findings of the Moral Injury Outcome Scale Consortium. Frontiers in Psychiatry, 13, 923928. [CrossRef]
- Liuski, T., & Ubani, M. (2020). How is Police Chaplaincy in Europe Portrayed in European Scientific Journal Articles between 2000 and 2019? A Multidisciplinary Review. Religions, 11(10). [CrossRef]
- Luo, Y., Zhang, Z., Chen, Q., Zhang, K., Wang, Y., & Peng J. (2022). Humble leadership and its outcomes: A meta-analysis. Frontier Psychology, 13:980322. PMID: 36619057; PMCID: PMC9811147. [CrossRef]
- Lusk, J. L., Dobscha, S., Kopacz, M., Ritchie, M., & Ono, S. (2018). Spirituality, religion and suicidality among veterans: A qualitative study. Archives of Suicide Research, 22(2), 311-326.
- Mamede, S., & Schmidt, H. G. (2004). The Structure of Reflective Practice in Medicine. Medical Education, 38(12), 1302-1308.
- Mann, K., Gordon, J., & MacLeod, A. (2009). Reflection and reflective practice in health professions education: A systematic review. Advances in Health Sciences Education, 14(4), 595-621. [CrossRef]
- Maslach, C., Jackson, S. E., & Leiter, M. P. (2016). Maslach Burnout Inventory manual (4th ed.). Mind Garden.
- Mensink, B., van Schagen, A., van der Aa, N., & ter Heide, F. J. J. (2022). Moral Injury in Trauma-Exposed, Treatment-Seeking Police Officers and Police Veterans: Latent Class Analysis. Frontiers in Psychiatry, 13, 904659.
- Miller, S., & Stephens, C. W. B. (2024). Assessing Impact Amongst Chaplains in a University Setting: Phase Two of an Action Research Project. Journal of Pastoral Care & Counseling, 78(1-2), 35-46. (Original work published 2024). [CrossRef]
- MIRECC & CoE (2025). MHICS training program overview 2025–2026. Department of Veterans Affairs. https://www.mirecc.va.gov/IMH/Docs_and_Images/ MHICS_Overview_2025.pdf?utm_source=chatgpt.com.
- Moustakas, C. (1990). Heuristic research: Design, methodology, and applications. Sage.
- Muris, P., & Otgaar, H. (2020). The process of science: A critical evaluation of 15 years of research on self-compassion with the Self-Compassion Scale. Mindfulness, 11(6), 1469-1482.
- Nash, W. P., Marino Carper, T. L., Mills, M. A., Au, T., Goldfinger, J., & Litz, B. T. (2013). Psychometric evaluation of the Moral Injury Events Scale. Police Medicine, 178(6), 646-652. [CrossRef]
- Neff, K. D. (2003). The development and validation of a scale to measure self-compassion. Self and Identity, 2(3), 223-250. [CrossRef]
- Neff, K. D. (2003a). Self-compassion: An alternative conceptualization of a healthy attitude toward oneself. Self and Identity, 2(2), 85-101. [CrossRef]
- Neff, K. D., & Germer, C. K. (2013). A pilot randomized controlled trial of the Mindful Self-Compassion program. Journal of Clinical Psychology, 69(1), 28-44. [CrossRef]
- Nieuwsma, J. A., Jackson, G. L., DeKraai, M. B., Bulling, D. J., Cantrell, W. C., Rhodes, J. E., Bates, M. J., Ethridge, K., Lane, M. E., Tenhula, W. N., Batten, S. V., & Meador, K. G. (2014). Collaborating across the Departments of Veterans Affairs and Defense to integrate mental health and chaplaincy services. Journal of General Internal Medicine, 29(Suppl 4), 885–894. [CrossRef]
- Nieuwsma, J. A., King, H. A., Jackson, G. L., Bidassie, B., Wright, L. W., Cantrell, W. C., Bates, M. J., Rhodes, J. E., White, B. S., Gatewood, S. J. L., & Meador, K. G. (2017). Implementing integrated mental health and chaplain care in a national quality improvement initiative. Psychiatric Services, 68(12), 1213–1215. [CrossRef]
- Nieuwsma, J. A., Smigelsky, M. A., Wortmann, J. H., & Meador, K. G. (2025). Piecing it Together: Collaborative Group Care for Moral Injury (Accepted). Current Treatment Options in Psychiatry, 12(1). [CrossRef]
- Norris, N. & Altic, J. (2023). How peer support and police chaplains build wellness in law enforcement. Police1. https://www.police1.com/police-products/firearms/accessories/ammunition/how-peer-support-and-police-chaplains-build-wellness-in-law-enforcement/.
- Oosterhuis, T., Olsman, H., & Vos, P. (2025). The contribution of chaplaincy classes to the moral formation of future police leaders: an ethnographic study in Dutch police chaplaincy. British Journal of Religious Education, 47(3), 369-388. [CrossRef]
- Papazoglou, K., & Tuttle, B. M. (2018). Fighting police trauma: Practical approaches to addressing psychological needs of officers. SAGE Open, 8(3), 1-12. [CrossRef]
- Peery, B. (2012). Outcome oriented chaplaincy: Intentional caring. In S. Roberts (ed.), Professional spiritual and pastoral care: A practical clergy and chaplain’s handbook (pp. 342-361). Woodstock, VT: SkyLight Paths Publishing.
- Peterman, A. H., Fitchett, G., Brady, M. J., Hernandez, L., & Cella, D. (2002). Measuring spiritual well-being in people with cancer: The FACIT-Sp. Annals of Behavioral Medicine, 24(1), 49-58. [CrossRef]
- Phelps, A. J., Madden, K., Carleton, R. N., Johnson, L., Carey, L. B., Mercier, J. M., ... & Dell, L. (2023). Towards a holistic model of care for moral injury: An Australian and New Zealand investigation into the role of police chaplains in supporting police members following exposure to moral transgression. Journal of Religion and Health, 62(6), 3995-4015.
- Phoenix Australia Centre for Posttraumatic Mental Health and the Atlas Institute for Veterans and Families. (2023). The role of chaplains in supporting police members impacted by moral stressors: A guide for chaplains and other wellbeing service providers. Phoenix Australia – Centre for Posttraumatic Mental Health and Atlas Institute for Veterans and Families.
- Rego, A., Melo, A. I., Bluhm, D. J., e Cunha, M. P., & Júnior, D. R. (2021). Leader-expressed humility predicting team psychological safety: A personality dynamics lens. Journal of Business Ethics, 174(3), 669-686. [CrossRef]
- Robinson-Edwards, S and Kewley, S (2018) Faith-Based Intervention: Prison, Prayer, and Perseverance. Religions, 4(9). ISSN 2077-1444.
- Royal Commission into Defence and Veteran Suicide. (2024). Final report (Australia). https://www.defenceveteransuicide.royalcommission.gov.au.
- Schön, D. A. (1983). The reflective practitioner: How professionals think in action. Basic Books.
- Smigelsky, M. A., Nieuwsma, J. A., Meador, K., Vega, R. J., Henderson, B., & Jackson, G. L. (2020). Dynamic diffusion network: advancing moral injury care and suicide prevention using an innovative model. Healthcare, 8(3), Epub. Elsevier.
- Smigelsky, M. A., Trimm, V., Meador, K. G., Jackson, G. L., Wortmann, J. H., & Nieuwsma, J. A. (2022). Core components of moral injury groups co-facilitated by mental health providers and chaplains. Spirituality in Clinical Practice, 9(3), 159-174.
- Smith-MacDonald L. A., Morin J. S., & Brémault-Phillips S. (2018). Spiritual Dimensions of Moral Injury: Contributions of Mental Health Chaplains in the Canadian Armed Forces. Frontier Psychiatry, 9, 592. 30487762; PMCID: PMC6246733. [CrossRef]
- Smith-MacDonald, L., Norris, J. M., Raffin-Bouchal, S., & Sinclair, S. (2017). Spirituality and mental well-being in combat veterans: A systematic review. Police Medicine, 182(11–12), e1920–e1940. [CrossRef]
- Sonnentag, S., & Fritz, C. (2007). The Recovery Experience Questionnaire: Development and validation of a measure for assessing recuperation and unwinding from work. Journal of Occupational Health Psychology, 12(3), 204-221.
- Sonnentag, S., & Kühnel, J. (2016). Coming back to work in the morning: Psychological detachment and reattachment as day-level predictors of work engagement. Journal of Occupational Health Psychology, 21(4), 379–390. [CrossRef]
- Stamm, B. H. (2010). The concise ProQOL manual (2nd ed.). ProQOL.org.
- Tao, H, Nieuwsma, J. A., Meador, K. G., Harris, S. L., & Robinson, P. S. (2023). Validation of the Moral Injury Outcome Scale in acute care nurses. Frontier Psychiatry, 14. PMID: 38094593; PMCID: PMC10716276. [CrossRef]
- Udovicich, B. E., & McLaren, S. (2025). Beyond the badge: Understanding the link between moral injury, self-compassion, and suicide risk in retired police officers. The Police Journal, 0(0). [CrossRef]
- VA Mental Health & Chaplaincy. (2021). Mental Health Integration for Chaplain Services (MHICS): Description and course overviews [PDF]. U.S. Department of Veterans Affairs. https://www.mirecc.va.gov/IMH/Docs/MHICS_Overview_2021.pdf.
- Vovkotecha, O., Horenkov, D., Kravchuk, M., Aparov, A., & Kravchenko, K. (2025). Legal and Paedagogical Principles of the formation of Professional Competencies of Police Chaplains: Domestic and Foreign Experience. Pharos Journal of Theology,106(2). Online.
- Wolgast, S.N., Wolgast, M., Sandeberg, K.A. et al. (2024). Psychological Flexibility and Compassion Training for Equality in Organizations: A Randomized Controlled Trial of a Diversity and Inclusion Intervention. Mindfulness 15, 2875-2887. [CrossRef]
- Wu, Q., Qi, T., Wei, J. et al. (2023). Relationship between psychological detachment from work and depressive symptoms: indirect role of emotional exhaustion and moderating role of self-compassion. BMC Psychol 11, 344. [CrossRef]
- Zessin, U., Dickhäuser, O., & Garbade, S. (2015). The relationship between self-compassion and well-being: A meta-analysis. Applied Psychology: Health and Well-Being, 7(3), 340–364. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



