
Submitted:
19 January 2026
Posted:
21 January 2026
You are already at the latest version
Abstract
Background: The history of radical hernia repair was a period of great activity and may have been influenced by factors of the time. Subcutaneous surgery was modified after the introduction of antisepsis, leading to dissection surgery.
Objective: Analyze the publications from the period of radical hernia cure using current methodology, verifying when and how the transition occurred from subcutaneous surgery to dissection surgery.
Methods: Literature review of the databases PubMed, LILACS, Cochrane Library; “Google” and university libraries. The following keywords have been used: “anatomy and surgery”. A critical analysis of the known literature about this historical figure is carried out.
Results: Under-vision dissection surgery, through incision of the aponeurosis of the external oblique muscle, began in England (Durham, 1866), almost 20 years before it was performed in France (Lucas-Ch., 1885). Recurrences decreased after the introduction of the principle of closing the walls of the inguinal canal (Wood, 1860). This surgeon-anatomist should be considered the first specialist in abdominal wall surgery, due to his extensive contributions from the pre-antiseptic era. The evolution of the radical cure of hernias was made possible by combining the knowledge of several countries: England, Germany, and Italy.
Conclusions: There are errors in the references to the period of radical hernia repair. Dissection surgery was initiated in England, Germany, and Italy, not in France. The influence of French literature on the history of hernias is evident, to the detriment of the contributions of surgeons from other countries.
Keywords: radical cure of hernias; subcutaneous operation; dissection operation; hernia; surgical treatment; hernia history.
Keywords:
radical cure of hernias
; subcutaneous operation
; dissection operation
; hernia
; surgical treatment
; hernia history
“Whoever discovers a safe and harmless surgical method could rightly be considered a benefactor of humanity. Thousands of people would be spared great inconveniences; thousands would avoid the dangers and horrific suffering of strangulation.” (Reverdin, 1881)
1. Introduction
The history of radical hernia repair involves numerous surgeons and every country in the world. The literature has presented us with a history that may be biased by factors of the time, such as limited access to texts published by universities, local hospital journals, or language barriers, among others. For example, the literature often refers to Lucas-Champagne (Lucas-Ch.) as the first to open the aponeurosis of the external oblique muscle (AEOM), but a thorough review refutes this "classic" claim [1,2,3,4]. Currently, easy access to digitized works and translation by computer programs allows us to complete this stage of surgery. Our study analyzes all digitized publications and theses in any language.
At the beginning of the 19th century, surgery generally yielded very poor results. In 1835, Gerdy published his incisionless scrotal invagination (subcutaneous operation) as a technique for the radical cure of hernias, reviving interest in this condition. From then on, theses were published every year, and discussions in scientific societies became commonplace. However, after his death (1856), the surgery was abandoned and fell into disrepute in France, and interest shifted to England, Germany, and Italy [5,6,7,8]. Around 1860, Wood's proposal, by a surgeon and anatomist whose work had been largely forgotten in specialized texts, stood out. He described a truly anatomical operation with sutures, rekindling interest in this condition. But it was the dissemination of Lister's antiseptic method (1865) that finally made the development of radical surgery through dissection possible.
2. Materials and Methods
A thorough literature search was carried out, Medline (PubMed) databases, Embase, LILACS (SciELO), Cochrane Library, Current contens, etc., using the following keywords: “radical cure of hernias”, “hernia surgery”, “subcutaneous operation”, dissection operation” and “hernia treatment history”. A targeted search was carried out for the texts and atlases mentioned in a historical analysis and a critical analysis of the articles, theses, books or monographs found on the authors up to the present day. A complementary search was also carried out using “Google” (Google play), university libraries, and bookstores (Archiveorg., Boston Medical Library and Medical Heritage Library). Manuscripts obtained from any country, institution or researcher and in any language were studied. All texts have been stored in digital pdf format to preserve their originality, printed and bound. In our institution this research was deemed low risk and did not require research and ethics approval.
3. Results
3.1. Lister and the Antiseptic Method
In the first half of the 19th century, only Conrad Martin Johann Langenbeck (1776-1851) dared to treat hernias with open surgery. He described two techniques: 1) with a small scrotal incision over the external inguinal ring, exposure of the sac, and ligation, taking care not to entrap the spermatic cord (without excision); 2) with a one-inch-wide quadrilateral skin flap, with an adherent base at the level of the inguinal ring and its lower edge located on the anterior thigh, dissected from bottom to top, inserted into the canal, and sutured along the edges of the defect. He successfully operated on at least 12 cases of the three main types of hernia using the first technique; and on two femoral hernia cases (obturation with an autoplastic flap), also successfully. Langenbeck believed that obliteration of the canal was definitive after a period of three to six months [9] (Figure 1) (Table 1).
Despite the extensive knowledge of anatomist surgeons, mortality exceeded 30%, leading to surgery being considered both useless and dangerous [10,11]. The revolutionary era of surgery arrived with three innovations: 1) the use of ether as a general anesthetic (Morton, 1846) and chloroform (Simpson, 1847); 2) the acceptance of the germ theory of disease as opposed to spontaneous generation (Pasteur, 1860); and 3) antisepsis, published by Lister in 1867. The principles of antisepsis in surgical practice involved washing wounds, hands, surgical instruments, gauze, and sutures with a phenolic solution [12]. Until then, the guiding principle had been to avoid incision, dissection, and the peritoneum. Following the acceptance of Listerism, the fear of the peritoneum diminished, the boundaries of the abdominal cavity were opened, and surgeons began to design operations to treat all types of hernias. Despite this, Lister's great advance was not immediately accepted. In France, it was introduced by Lucas-Ch., who was exemplarily involved for many years; in Germany, Czerny was its greatest advocate; and in the USA, it was Marcy who first performed hernia repair using antisepsis, suturing the deep ring with catgut in 1871 [13,14]. The literature maintains that it was Steele in England (1874) who first performed it by closing only the external inguinal ring [15,16].
3.2. From Subcutaneous Surgery to Dissection: When Is the AOEM Incised?
Initially, all hernia repair procedures were called subcutaneous and were performed "blindly" because the aponeurosis of the external oblique muscle (AEOM) was not exposed. Therefore, anatomical knowledge and experience were essential for the procedures to be safe and effective. There was an overreliance on tactile feedback to avoid vascular and intestinal injuries. Clearly, this approach was not accessible to every surgeon. The profession needed to find a way to simplify hernia surgery so that it would be accepted by all general surgeons. Today, we see the AEOM as a normal and necessary step in every hernia operation, a prerequisite for proper exposure of the hernia sac. But reaching this stage was not so obvious for surgeons with the mindset and traditions of the 19th century. The opening of the anterior epithelium and the exposure of the canal changed everything. The literature states that Lucas-Ch. was the first to take this step in 1881, leaving subcutaneous operations behind. This date does not coincide with any publication by the author, but rather with a case commentary in Segond's thesis [5]. In reality, Lucas-Ch. appears to have performed it as early as 1885, but did not publish it until 1892, after Bassini [16,17,18]. This maneuver-initiated dissection surgery, giving all surgeons direct access to local anatomy, replacing reliance on the sense of touch with direct visualization of anatomical structures, making the operation safer and eliminating the need for extensive experience or prior training. But let us analyze the development of the literature systematically, with greater scientific rigor and current resources.
1860, London. John Wood (1825-1891) published his invasive suturing technique, based on sound anatomical principles, after a long period of training in the operating room and surgical suites. He introduced complete closure of the inguinal canal walls into the radical operation: he sutured Poupart's ligament (inferior and anterior wall) to the conjoint tendon (superior and posterior wall) [19]. His experience was probably the greatest of any surgeon of his time, and his method was widely used. He acknowledged the difficulty of the technique, as it was performed with an incision of less than 2 cm. (3/4” or 1.9 cm), guided almost exclusively by touch. He warns of the need to know all the “guide” anatomical structures to avoid injury and obtain a good result. The technique fails if the sac is not brought up into the abdominal ring, the sutures are applied too low or are poor and do not grasp the posterior wall deeply. Wood's operation represented the first major advance in radical cure by lowering mortality to 2% and recurrence to 20%, incredible results in the pre-antiseptic era [20,21] (Table 1).
It is true that the operation was performed using traditional methods and required considerable skill, but it came to be considered the safest and most effective option of the time. A thorough analysis of his publications allows us to consider him the first "specialist surgeon" in hernias, based on: 1) his lifelong, dedicated interest in the field of hernias; 2) dissecting cadavers to enhance his knowledge and verify his theory; 3) describing a technique that he refined over more than 30 years; 4) designing and perfecting the instruments necessary for the technique; 5) publishing his results and complications in medical journals; 6) presenting the most extensive personal experience of the 19th century, surpassing Bassini; 7) publishing a monograph updating the topic; and 8) demonstrating his technique publicly at meetings and before the College of Surgeons. 9) to demonstrate the benefit of early surgery by comparing its mortality rate with the overall rate in London hospitals for symptomatic and/or complicated operations, 10) to be a pioneer in giving a multidisciplinary character to the specialty by designing the groin flap for abdominal wall defects, and 11) to teach colleagues and students through courses and lectures [19,20,21]. His influence in the field of hernia was the greatest of the 19th century (* epitaph at the end of the text) [22]: Why has he fallen into oblivion from history? Why is he not cited in current texts of the specialty? (Figure 2).
1866, London. Arthur Edward Durham (1834-1895), a surgeon at Guy's Hospital known for performing the first nephrectomy in England (1872), published a case of radical repair of an inguinal hernia and described it as follows: … after administering chloroform and reducing the hernia, an incision 5.5 cm long is made through the skin and superficial fascia, perpendicular to Poupart's ligament and just above the inner edge of the internal or deep abdominal ring, “the tendon of the external oblique muscle is divided in a similar direction, but to a lesser extent”, the lower fibers of the internal abdominal oblique or cremaster are separated longitudinally and the internal spermatic fascia is exposed. The description leaves no room for doubt: he opens the AEOM by dissection layer by layer until reaching the spermatic cord, for the first time, in a case of scrotal hernia, and publishes and presents it to the Medical Society. For repair, he employs a deep ligation of the hernial sac, which he ties firmly as high as possible, precisely at the internal ring (before Marcy, 1871, according to the literature) [23]. The case is cited in Reverdin's thesis, but overlooked and dismissed as "classic and outdated" [24]. We do not know if this is because he was not French. The author, prophetically, concludes that his method "is more scientific than any other adopted until then (from a safe surgical point of view), and hopes that it may have more success in practice." Despite this, the history of hernias has forgotten him (Figure 3).
1875, Halle (Germany). Otto Riesel, head of the Halle Hospital, attends a lecture by Auguste-Dominique Valette (1821-1876) in Lyon, where Valette presents his results with Gerdy's technique, modified by using coagulated needles to introduce small amounts of zinc chloride paste into the cavity of the invaginated hernial sac, with the aim of inducing inflammation and fibrosis. Riesel begins operating on hernias using this method, but through a direct approach by opening the entire abdominal wall. In 1877, he published his experience: “I exposed the hernial sac by making an incision corresponding to the course of the inguinal canal, separating the skin and fascia, and a portion of the anterior wall of the inguinal canal layer by layer, and I isolated it from the spermatic cord…”. After dissecting the inguinal wall, he fixed the sac with sutures without closing either the ring or the canal, an insufficient procedure. He closed the wound with an interrupted suture that encompassed both the skin and the musculotendinous layer (AEOM) and covered it with a Lister-type compression dressing in the form of a bathing suit. With his experience, he improved the technique by introducing high ligation of the neck of the sac, wide suturing of the pillars (following Czerny's advice), and closure of the inguinal canal with several buried button sutures (following Wood). It is described as follows: exposure of the ring is widened by an incision in the aponeurotic and muscular plane, extending beyond the abdominal end of the inguinal canal. This offers the advantage of allowing complete closure with sutures below the eye. This extensive debridement exposes the sac to its entry into the abdomen. To be fair, the use of sutures or ligatures to close the hernial cavity will only be possible after extensive dissection of the inguinal canal… His account leaves no room for doubt. Direct or dissecting surgery began in Germany with the so-called Riesel method, published in his second article of the same year: a wide incision of the AEOM and, if necessary, an extension beyond the abdominal ring. This procedure ensures complete excision of the sac and suturing of the ring, and should be recommended both for extracting the sac and for hermetically closing the canal by suturing layer by layer under direct vision and control. Reverdin's thesis unequivocally reflects his contribution to the radical cure of hernias in 1881 [24,25,26]. In addition to this contribution, Riesel emphasizes the importance of wound cleansing. The careful removal of any remaining cellular or adipose tissue from the surgical field promotes secure closure of the wound by primary intention. In these measures, he clearly anticipates the postulates of Halsted (1890). Possibly, being a German publication, it did not achieve widespread dissemination compared to the prestige of the more influential French literature in Europe. Riesel concludes by leaving us with a task to complete: to operate, evaluate our results through further experiments, and adapt the surgical technique accordingly.
1881, Geneva (Switzerland). Jacques-Louis Reverdin (1842-1929), a proponent of antisepsis and ether anesthesia (due to its superior dosage compared to chloroform), improved the natural recovery of the operated patient by reducing pain and fever. His contribution, aimed at avoiding tension on the sutures of the pillars and during contraction of the external oblique muscle, was to make small incisions in the external abdominal wall (EAW), 1-2 cm in length, above and parallel to the internal pillar, in the AEOM overlapping, alternating series [24]. He acknowledged that his technique, like most described methods, had the drawback of only treating the external ring of the inguinal canal, leaving the abdominal opening and the canal untreated, a fact already noted as insufficient by Wood.
1881, Boston (USA). Henry O. Marcy (1837-1924) began publishing his work in 1871 with two initial cases of hernia repair and closure of the canal using three catgut sutures. In 1877, he operated on another case, and in 1878, two more, publishing them in 1881 [13,27]. In 1887, he published a series of 30 operations, highlighting high ligation of the sac, excision of the redundant tissue, and deep closure of the pillars. He was the first American surgeon to reconstruct the posterior floor of the inguinal canal, although his figures and text are difficult to interpret. He began the closure from the posterior border of Poupart's ligament on its outer side, toward the transversalis fascia anteriorly, a muscular and tendinous structure on the deep side of the canal, continuing downward over the spermatic cord to the external ring, to fix the structures of the floor and restore the obliquity [28] (Figure 4).
1885, London. Wood states that, following the introduction of aerosols in operating rooms and the use of antiseptic dressings, he no longer opposes dissection surgery, but rather employs it frequently. He recommends its use in irreducible hernias or those with large sacs. The AOEM incision dissection facilitates the tedious, invasive, and difficult maneuver of completely removing the sac. In all other cases, he continues to prefer the subcutaneous approach with minimal incision due to less bleeding and tissue damage. It is worth noting that most authors, such as Stokes, Ball, Banks, Nussbaum, Macewen, Czerny, etc., continue to avoid it. Despite acknowledging that the open method allows the surgeon to visualize the operated areas, he warns that it causes greater bleeding, forcing him to rely on touch to suture securely. Therefore, he sees no significant advantages in his 5cm scrotal incision. And the skin's elasticity allows it to reach the dilated inguinal ring and treat the sac without needing to divide the intercolumnar fascia, which weakens the abdominal wall [21].
1886, Paris. Just-Marie-Marcellin Lucas-Championnière (1843-1913), the leading French exponent of antiseptic surgery participated in a debate on hernias at the Amsterdam Congress (1879), performed his first operation which he presented to the Surgical Society (1881), reported his initial experience at the first French Congress of Surgery (1885), and in 1886 published an initial series of ten operations. At the third congress, he presented 81 cases, which were published in the Journal de Médecine et de Chirurgie pratiques in 1888. He advised against routine surgery, recommending instead the most suitable approach for each patient and case. To this end, he proposed a formula outlining the necessary requirements: 1) modifying the conditions of the hernial canal to eliminate the initial predisposition to herniation, and 2) finding the point of support that would withstand the force of the viscera and seal the abdominal wall. He reduced everything to the scar, which must resist the force of the viscera. To achieve this, the incision must extend as high as possible, be long and wide, and therefore the operation must be performed through a large incision. This new precept opposed the traditional one: small incision, minimal mobilization, etc. But if a good result is desired, extensive tissue modification is required, that is, extensive dissection surgery.
Despite this, he initially did not perform the opening of the AEOM. Although Segond's thesis (1883) describes his first case from 1881, in this case, the aponeurosis was not incised [5]. The literature has erroneously maintained the status of this thesis [17,18]. By 1892, the incision of the canal was published, indicating that it began in 1885 (Figure 5). The technique is described in the following steps: exposure of the sac; incision of the external abdominal wall along the entire length of the canal to expose the neck of the sac and clearly visualize the internal ring; suturing the sac 1 cm above the abdominal ring, the internal ring, the canal, and the external ring, the entire cavity occupied by the hernial sac; and imbrication of the roof during closure (the sutures are arranged so that the two lips of the inguinal canal cleft overlap each other). The incision of the ovarian sac is made between two special forceps, which span the entire thickness of the wall, anterior to the spermatic cord, opening beyond the deep ring [18,29]. This maneuver had been published by Riesel in 1877, in German. Despite this, the literature has maintained that he was the first to point out the need to open the AEOM in such a way that the sac is removed under direct vision, as Riesel described it (“with eyes”).
1884, Padua (Italy). Edoardo Bassini (1844-1924) began his apprenticeship using the techniques of Wood and Czerny. When the results were poor, he devised a new operation based on the concept of dissection: extensive dissection of the spermatic cord, the hernial sac with high ligation, and the canal by opening the transversalis fascia (original technique) from the internal inguinal ring to the pubic tubercle, after dividing the cremaster muscle and ligating the hernial sac. He then performed a three-layer fascial repair to restore the integrity of the inguinal floor and the inguinal canal. The only drawback was that he left the hernial rings intact. In 1884, he began a personal series, publishing results first in Italian (1888; 1889) and then in German (1890), lowering the mortality rate to 0.5% and the recurrence rate to 3.3% in uncomplicated hernias [30,31,32]. He incorporated Wood's anatomical and repair concepts, but while this anatomist surgeon used the subcutaneous approach (a pre-Lister mindset), the Italian fully embraced the dissection approach through the entire inguinal wall, opening the transversalis fascia and accessing the preperitoneal space. This complete sectioning of the pre-peritoneal region was a proposal of the Italian school, accepted early on by Bassini [11]. Furthermore, he was familiar with Marcy's work with sutures. In his publications, the illustrations and text are uniform, unlike Marcy's. This fact, and possibly the European prestige compared to the new American surgery, influenced Bassini's being credited as the first surgeon to repair the posterior floor, a claim supported by Halsted in 1924 (Figure 6).
3.3. Participation of the Founding Fathers
The intense surgical activity during the second half of the 19th century transformed hernia surgery into a scientific technique. As we have seen, this period saw the overcoming of the three barriers responsible for high postoperative mortality: pain, hemorrhage, and infection. Hernia surgery, due to its frequency and accessibility, was the perfect operation for training and skill development. All the gestures and maneuvers of a major surgical procedure are performed during hernia surgery: tissue incisions, ligatures, hemostasis, identification of anatomical structures, sutures, knot tying, etc. It is not surprising that the great figures of surgery, the founding fathers and pioneers of many surgical specialties, began their careers repairing hernias and describing some new technique or personal maneuver. Among them, the following stand out: Marcy and Lucas-Ch. in obstetrics; Kocher and Reverdin in thyroid surgery; Durham and Macewen in neurology; Steele in esophageal surgery; Czerny and Halsted in oncology; and Schede in thoracic surgery. Langenbeck and Buchanan in facial surgery, etc. One of the best examples of this era is Kocher, who began by designing a technique for hernias (lateral placement of the spermatic cord) with a 19th-century mindset (no open the AEOM), and later became a pioneer in endocrinology and thyroid surgery, winning the Nobel Prize in Medicine in 1909 [33] (Figure 7).
4. Conclusion
Regarding the period of radical inguinal hernia repair, we can conclude that:
4.1. Direct surgical dissection under vision, through incision of the aponeurosis of the external oblique muscle, began in England (Durham, 1866), almost 20 years before it was performed in France (Lucas-Ch., 1885), despite what was reported in the specialty literature.
4.2. The reduction in recurrence, or the increase in the effectiveness of radical hernia repair, was made possible by the introduction of the principle of closing the walls of the inguinal canal (Wood, 1860). All operations based on closing the sac or the pillars were ineffective. Likewise, this surgeon-anatomist should be considered the first specialist in abdominal wall surgery due to his extensive contributions to this pathology, from the pre-antiseptic era.
4.3. The evolution of radical hernia repair incorporated knowledge from several countries, from England to Germany, and was finally completed in Italy.
Regarding the history of surgery, we have verified that:
4.4. There are numerous errors in historical references, validating comments based on publications, and these have been reused year after year without verification of the original source.
4.5. Full dissection surgery, involving opening the abdominal wall layer by layer to reach the hernial sac, was initiated by anatomist surgeons in England and Germany, not in France.
4.6. The influence of French literature on the history of hernia surgery is undeniable, to the detriment of the notable contributions of English, German, and American surgeons, primarily.
*“No one can write anything about the subject of hernias without referring to Wood’s work, and although his original operation is no longer practiced, modifications to it are simply the natural result of the introduction of antiseptics into surgery.” (The Lancet, 1892)
Author Contributions
A. M-E.: Conceptualization; funding adquisition; methodology; project administration; investigation; resources; supervision; validation; visualization; writing – original draft; writing – review & editing. C. M. L.: methodology; validation; supervision; writing – original draft and writing – review & editing. A. M. L.: methodology; validation; investigation; validation; writing – original draft and writing – review & editing. All authors have read and approved the final manuscript and agree to be accountable for all aspects of the work in ensuring its integrity and accuracy.:.
Funding
This research received no specific grant from public, commercial, or not-for-profit funding agencies.
Institutional Review Board Statement
Not applicable for this review article.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflict of Interest
The authors declare no conflicts of interest or financial ties to disclose.
Conflicts of Interest
The authors have no conflict of interest to declare.
References
- Watson, LF. Hernia. Mosby Co. St. Louis, 1924.
- Sachs, M.; Damm, M.; Encke, A. Historical evolution of inguinal hernia repair. World J. Surg. 1997, 21, 218–223. [CrossRef]
- Malangoni, M.A.; Rosen, M.J. Hernias. En: Townsend CM, Beauchamp RD, Evers BM, Mattox KL. Sabiston. Tratado de cirugía. 20a ed. Elsevier. Madrid, 2018.
- Bittner, R.R.; Felix, E.L. History of inguinal hernia repair, laparoendoscopic techniques, implementation in surgical praxis, and future perspectives: Considerations of two pioneers. Int J of Abd Wall and Hernia Surg. 2021, 4(4), 133-155. DOI: 10.4103/ijawhs.ijawhs_85_21. [CrossRef]
- Segond, P. Cure radicale des hernies. These présentee au concours de l´agrégation (section de chirurgie et d´accouchements). Masson. Paris, 1883.
- Thierry, A. Des diverses méthodes operatoires pour la cure radicale des hernies. Thése, Faculté de Medecine de Paris. Moquet et Compagnie, 1841.
- Roustan, A. De la hernie interstitielle.Thése pour le Doctorat en Médecine. Faculté de Medecine de Paris. Fonderie de Rignoux, Paris, 1843.
- Boinet, A.A. De la cure radicale des hernies. Thése, Concours d'agrégation. Faculté de Medecine de Paris. Maulde et Renou. Paris, 1839.
- Moreno-Egea, A.; Moreno-Latorre, C.; Moreno-Latorre, A. El Último Cirujano Anatomista: Conrad Martin Johann Langenbeck (1776-1851). Inter J of Morphol. 2024, 42, 1328-1337. 10.4067/S0717-95022024000501328. [CrossRef]
- Ashhurst, J. The International Encyclopaedia of Surgery: A Systematic Treatise on the Theory and Practice of Surgery. William Wood & Co. New York, 1883-85.
- Le Dentu, J.F.K.; Delbet, P. Traité de chirurgie clinique et opératoire. J. B. Bailliere et Fils. Paris, 1898.
- Lister, B.J. On the antiseptic principle in the practice of surgery. The Lancet 1867, 90(2299), 353-356.
- Marcy, H.O. Carbolized catgut sutures (buried in the tissues) for the cure of hernia. Boston Med. Surg. J. 1871, 85, 315-316. DOI: 10.1056/NEJM187111160852002. [CrossRef]
- Biographical sketch of Dr. Henry O. Marcy. Physicians and Surgeons of America, 1896.
- Steele, C. On Operations For The Radical Cure Of Hernia. Brit Med J. 1874, 2(723), 584-584. http://www.jstor.org/stable/25239741.
- Stoppa, R. Survol historique de la chirurgie des hernies De la castration à la haute technologie. Histoire des Sciences Mëdicales 2001, 35(1), 57-70.
- Lucas-Championnière, J. Sur la cure radicale des hernies. Bull. et Mem. Soc. Chir (Paris). 1887, 13, 737-742.
- Lucas-Championnière, J. Chirurgie opératorie. Cure radicale des hernies; avec une etude statistique de deux cents soixante-quinze operations. Paris, Rueff et Cie, 1892.
- Wood, J. On a new method of operation for the radical cure of hernia. Medico-Chirurg Transactions 1860, 43, 71. [CrossRef]
- Wood, J. On Rupture Inguinal, crural, and umbilical: the anatomy, pathology, diagnosis, cause and prevention with new methods of effecting a radical and permanent cure embodying the Jacksonian prize essay of the Royal College of Surgeons. John W. Davies. London, 1863.
- Wood, J. Lectures on Hernia and its Radical Cure: Delivered at the Royal College of Surgeons of England in June, 1885 - with A Clinical Lecture on Trusses and Their Application to Ruptures. Henry Renshaw. London, 1886.
- Death of professor John Wood. The Lancet 1892, 139(3566), 39. DOI: 10.1016/S0140-6736(02)13946-8 . [CrossRef]
- Alderson, J.; Toynbee, J.; Durham, A.E.; Smith, W.T. Reports Of Societies. Brit Med J. 1866, 1(286), 674-677. http://www.jstor.org/stable/25205725.
- Reverdin, J-L. Des opérations modernes de cure radicale des hernies. Revue Médicale de la suisse romande. Libraire-Editeur H. George. Genéve, 1881.
- Riesel, O. Versuche zur Radicalheilung freier Hernien. Dtsch Med Wochenschr. 1877, 3(38), 449-452. DOI: 10.1055/s-0029-1194032. [CrossRef]
- Riesel, O. Versuche zur Radicalheilung freier Hernien (Schluss aus No. 38.). Dtsch Med Wochenschr. 1877, 3(39), 467-469. DOI: 10.1055/s-0029-1194045. [CrossRef]
- Marcy, H.O. The cure of hernia by the antiseptic use of animal ligature. Trans Int Med Congr. 1881, 2, 446.
- Marcy, H.O. A treatise on hernia. The radical cure by the use of the buried antiseptic animal suture. GS Davis. Detroit, 1889.
- Lucas-Championnière, J. Cure radicale des hernies. Avec une étude statistique de deux cent soixante-quinze opérations, et 50 figures intercalées dans le texte. Rueff & Cie. Paris, 1892.
- Bassini, E. Sopra 100 casi di cura radicale dell’ernia inguinale operata col metodo dell-autore. Arch ed Atti Sot ltal Chir. 1888, 5, 315-9.
- Bassini, E. Nuovo metodo per la cura radicale dell’ernia inguinale. Padua: Prosperini, 1889.
- Bassini, E. Ueber de behandlung des leistenbruches. Arch Klin Chir. 1890, 40, 429-476.
- Kocher, E.Th. Zur radicalcur der hernien. Cor. Bl. für Schweiz. Aerzte (Basel), 1892, 18, 12.
- Czerny, V. Studien zur radikalbe-handlung der hernien. Wein Med Wschr. 1877, 27, 497-500.
- Macewen, W.I. On the Radical Cure of Oblique Inguinal Hernia by Internal Abdominal Pad and the Restoration of the Valved Form of the Inguinal Canal. Ann Surg. 1886, 4(2), 89-119. doi: 10.1097/00000658-188612000-00010. [CrossRef]
Figure 1.
A: Portrait of Conrad Johann Martin Langenbeck (1776 -1851). Photograph by Ludwig Emil Grimm, 1826 (Philadelphia, Museum of Art). B: Tabula II. C: Tabula IV, Structura peritonaei testiculorum tunicis, Gottingae, 1817.
Figure 1.
A: Portrait of Conrad Johann Martin Langenbeck (1776 -1851). Photograph by Ludwig Emil Grimm, 1826 (Philadelphia, Museum of Art). B: Tabula II. C: Tabula IV, Structura peritonaei testiculorum tunicis, Gottingae, 1817.
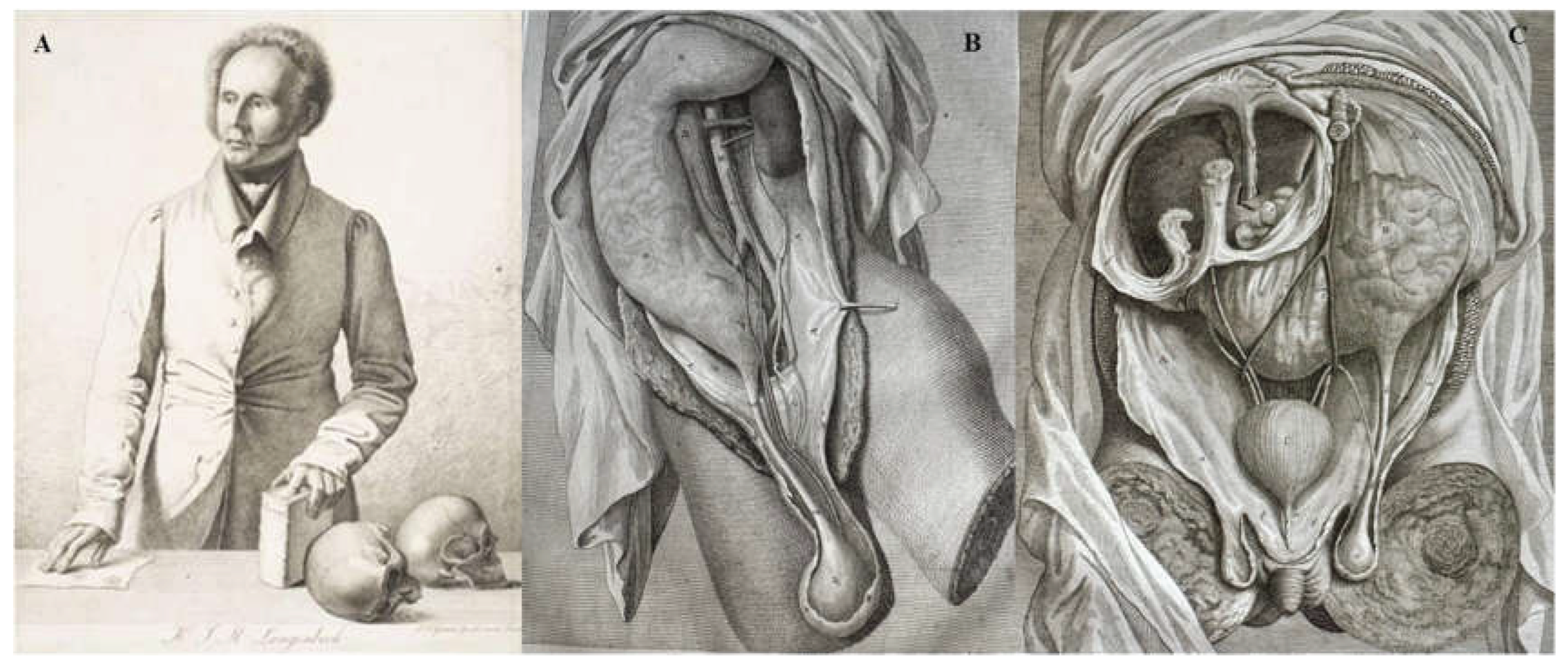
Figure 2.
A: Portrait of John Wood (1825-1891). Photograph by Crellin (Wellcome Collection). B: radical cure of inguinal hernia. C: instruments designed for the Wood technique. D: radical cure of crural hernia. E: radical cure of umbilical hernia.
Figure 2.
A: Portrait of John Wood (1825-1891). Photograph by Crellin (Wellcome Collection). B: radical cure of inguinal hernia. C: instruments designed for the Wood technique. D: radical cure of crural hernia. E: radical cure of umbilical hernia.
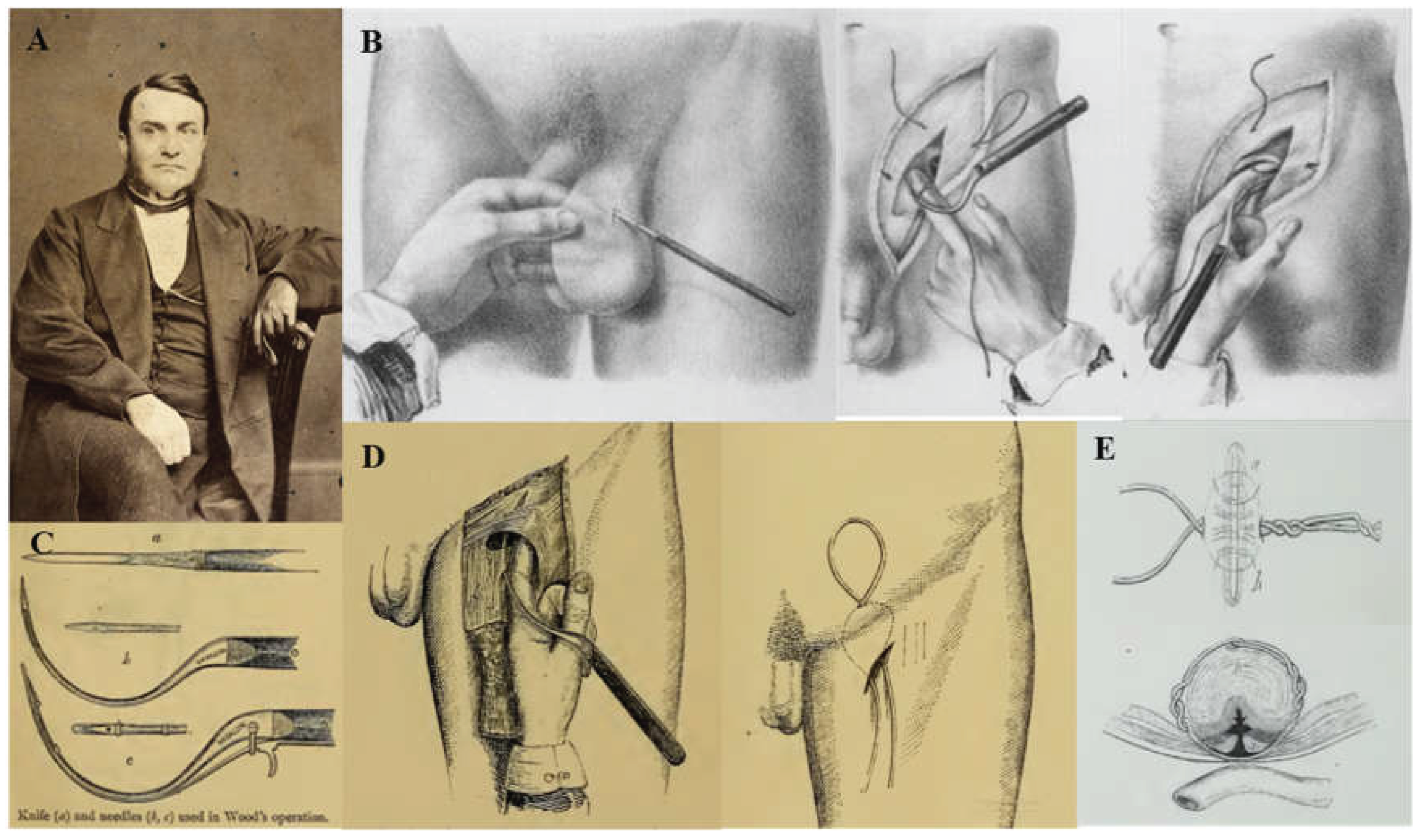
Figure 3.
A: Portrait in memorium, Arthur Edward Durham (1834-1895). Photograph by W.H.A. Jacobson, 1895. B: The past surgeons and physicians of Guy's Hospital, Southwark, London, with views of the building. Colour lithograph by Beynon & Company after M. Hanhart. Portraits of Arthur E Durham, Sir Astley Cooper, John Hilton, Charles Aston Key, and others (Wellcome library).
Figure 3.
A: Portrait in memorium, Arthur Edward Durham (1834-1895). Photograph by W.H.A. Jacobson, 1895. B: The past surgeons and physicians of Guy's Hospital, Southwark, London, with views of the building. Colour lithograph by Beynon & Company after M. Hanhart. Portraits of Arthur E Durham, Sir Astley Cooper, John Hilton, Charles Aston Key, and others (Wellcome library).
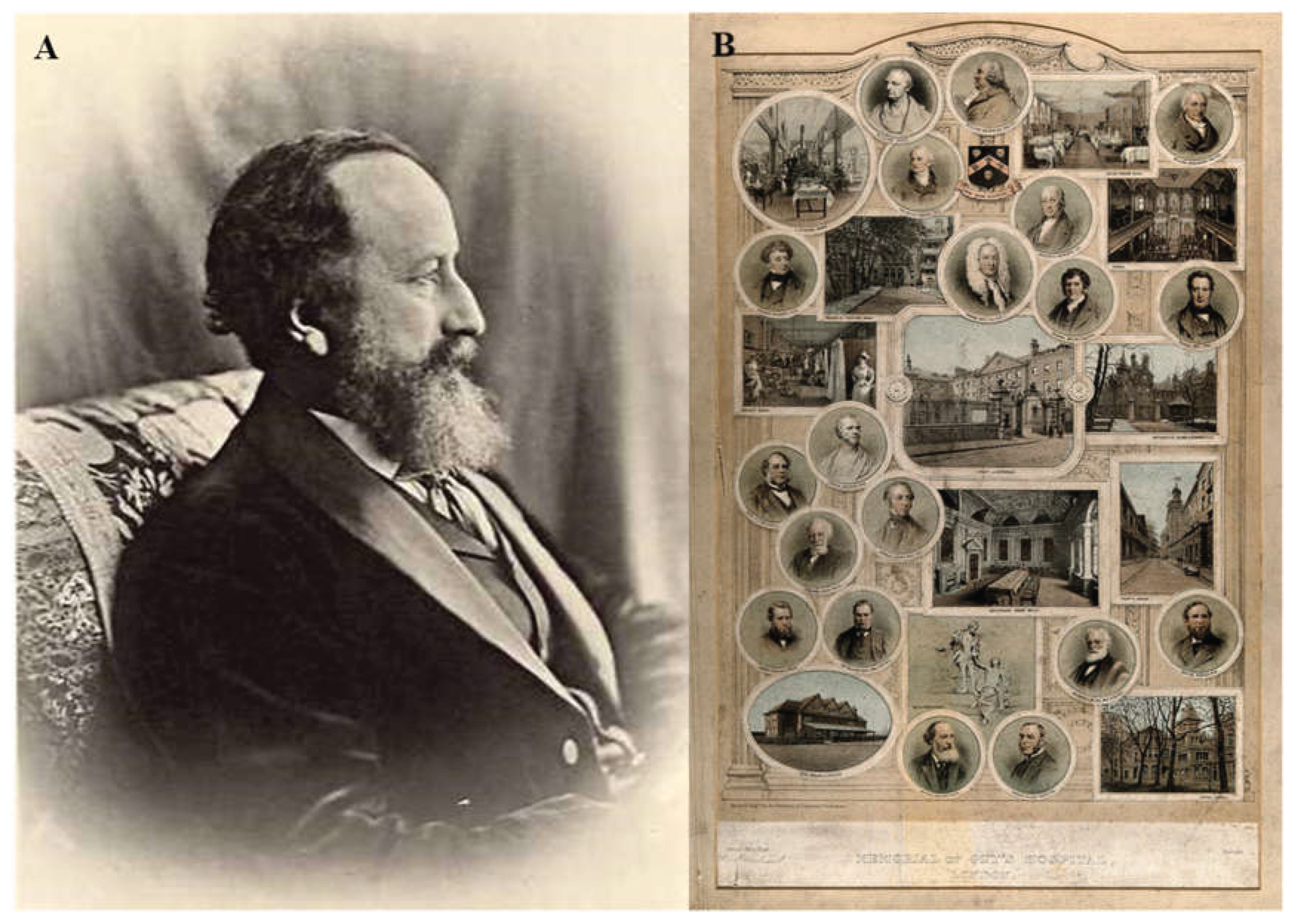
Figure 4.
A: Portrait of Henry O. Marcy (1837-1924) (1896, Physicians and Surgeons of America). B: The first stitch of the deep inguinal ring closure (up) and the closure using a double, continuous stitch (down) are shown. C: Method of folding the transversalis fascia to initiate closure of the posterior floor (up) and suturing by elevating the spermatic cord (down).
Figure 4.
A: Portrait of Henry O. Marcy (1837-1924) (1896, Physicians and Surgeons of America). B: The first stitch of the deep inguinal ring closure (up) and the closure using a double, continuous stitch (down) are shown. C: Method of folding the transversalis fascia to initiate closure of the posterior floor (up) and suturing by elevating the spermatic cord (down).
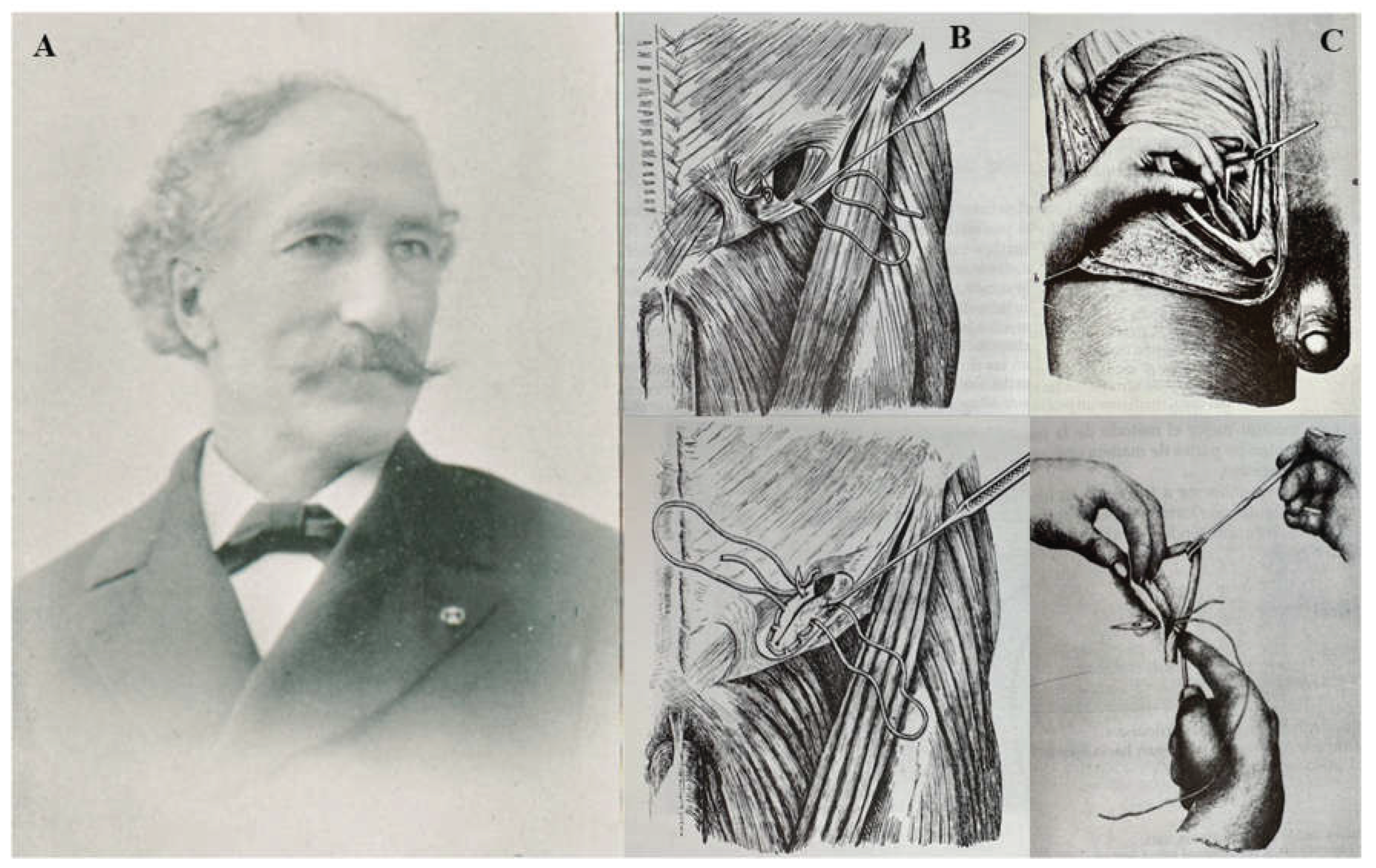
Figure 5.
A: Portrait of Just-Marie-Marcellin Lucas-Championnière (1843-1913) by Eugéne Pirou, 1906 (Bibliothèque interuniversitaire de santé). B: Cover of his great work of 1892. C: diagrams of their concept for treating the sac (up) and repairing the wall (down). D: AEOM opening shape between clamps.
Figure 5.
A: Portrait of Just-Marie-Marcellin Lucas-Championnière (1843-1913) by Eugéne Pirou, 1906 (Bibliothèque interuniversitaire de santé). B: Cover of his great work of 1892. C: diagrams of their concept for treating the sac (up) and repairing the wall (down). D: AEOM opening shape between clamps.
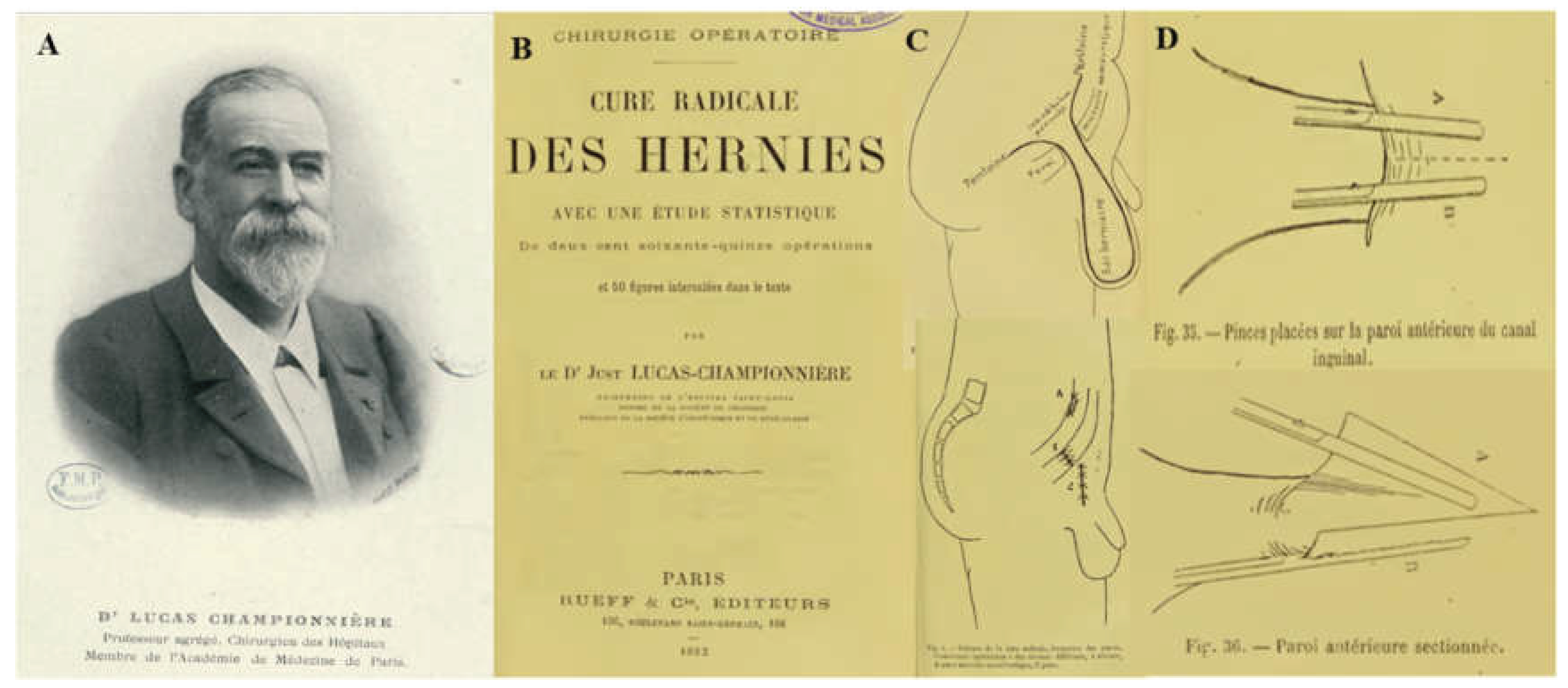
Figure 6.
A: Portrait of Edoardo Bassin. Wellcome collection (Number: M0017969). B: Shows the three-layer (F) with the transversalis fascia open. C: shows the suture of the trilaminar layer. D: the cord is left in place and the AEOM is closed with a continuous suture.
Figure 6.
A: Portrait of Edoardo Bassin. Wellcome collection (Number: M0017969). B: Shows the three-layer (F) with the transversalis fascia open. C: shows the suture of the trilaminar layer. D: the cord is left in place and the AEOM is closed with a continuous suture.
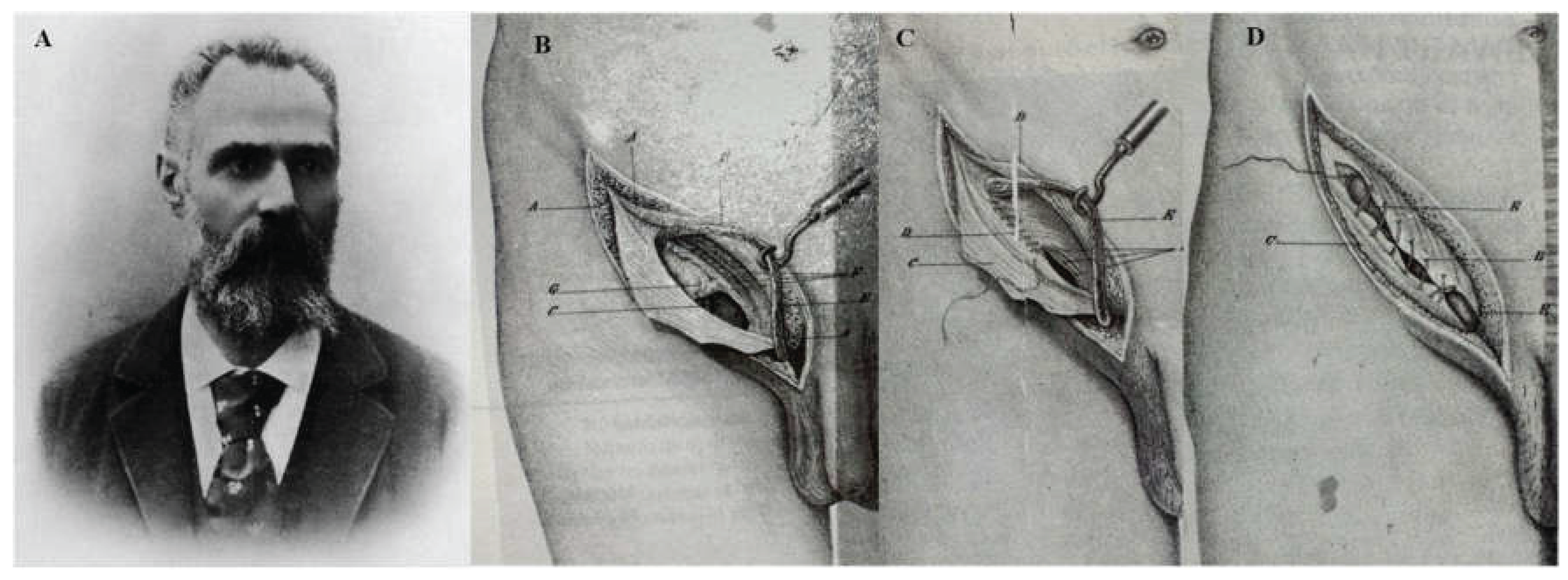
Figure 7.
A: Portrait of Emil Theodor Kocher, and lateral placement technique of the hernial sac. B: After identifying the AEOM, make a 1cm incision over the internal inguinal ring, through which a clamp is passed until it exits through the external ring, grasp the sac and retract it. C: Fix the neck of the sac to the edges of the incision with a silk suture and resect the rest of the sac.
Figure 7.
A: Portrait of Emil Theodor Kocher, and lateral placement technique of the hernial sac. B: After identifying the AEOM, make a 1cm incision over the internal inguinal ring, through which a clamp is passed until it exits through the external ring, grasp the sac and retract it. C: Fix the neck of the sac to the edges of the incision with a silk suture and resect the rest of the sac.
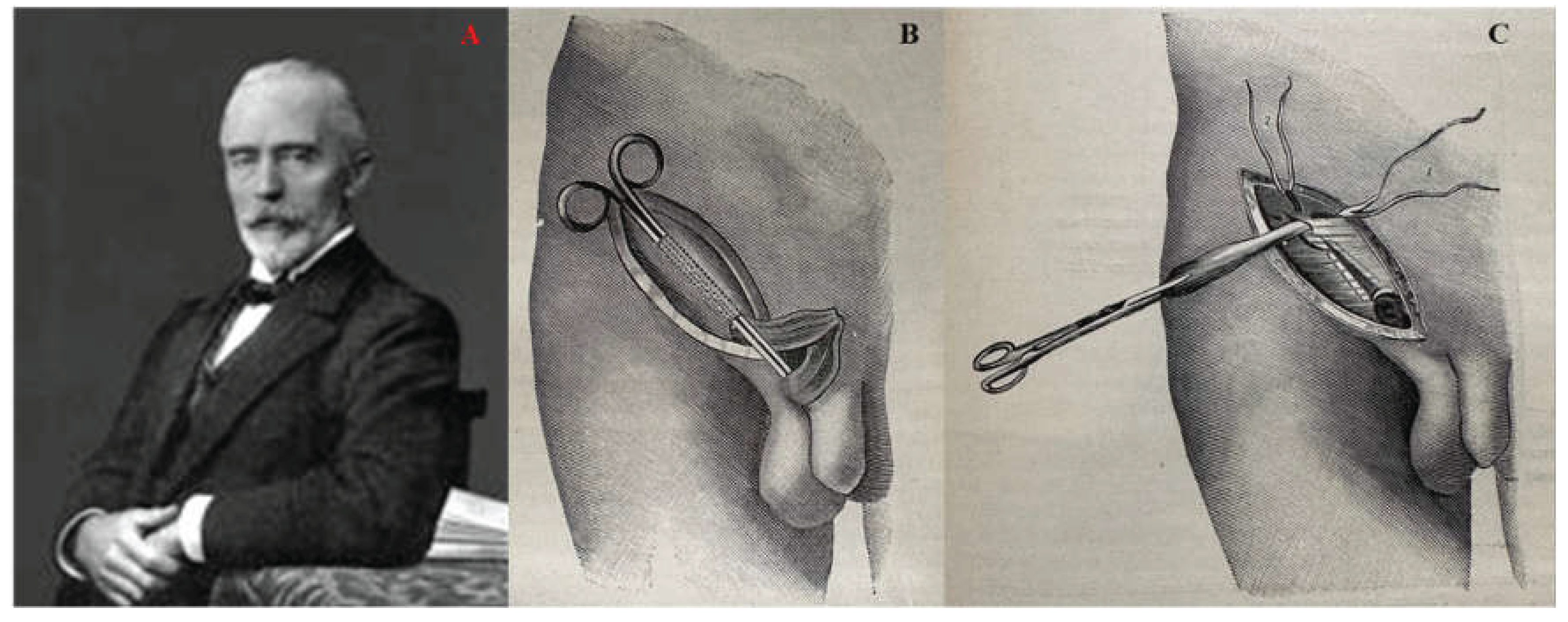

Table 1.
Historical development of the radical cure of inguinal hernia: from Lister to Bassini.
| Year | Technique | Author (country) | Reference |
|---|---|---|---|
| 1808 | Open surgery: 1) Sac dissection and ligation 2) Autoplastic flap obturation |
Langenbeck (Hanover, Germany)) | [9] |
| 1835 | Closed or subcutaneous surgery: Intussusception operation | Gerdy (Paris, France) | [6,7] |
| 1846 | Anesthesia | Morton (Boston, EEUU) | [9] |
| 1858 | Open surgery: closure of the inguinal canal (invasive suture) | Wood (London, England) | [21] |
| 1865 | Antisepsis | Lister (Glasgow, England) | [12] |
| 1866 | Dissection surgery: open the AEOM | Durham (London, England) | [23] |
| 1871 | Open surgery: closure of the abdominal ring | Marcy (Boston, EEUU) | [13] |
| 1874 | Open surgery: closure of the superficial ring | Steele (Bristol, England) | [15] |
| 1877 | Dissection surgery: open the AEOM (Riesel method) | Riesel (Halle, Germany) | [26] |
| 1877 | Open surgery: tamponade of the IIR with the folded sac, suture of the EIR pillars, reinforcement of the AEOM (without opening it) | Czerny (Berlín, Germany)) | [34] |
| 1881 | Open surgery: incisions in the AEOM, in two alternating and overlapping series | Reverdin (Geneva, Switzerland) | [24] |
| 1885 | Open surgery: transplant the remodeled sac laterally under the AEOM | Kocher (Bern, Switzerland) | [33] |
| 1885 | Dissection surgery: opening of the inguinal canal; resection of peritoneal diverticulum (Lucas-Ch. concept); overlap of the AEOM | Lucas-Ch. (Paris, France) | [17] |
| 1886 | Open surgery: valve closure of the canal with the sac as a plug | Macewen (Glasgow, England) | [35] |
| 1888 | Total dissection surgery: Posterior floor closure triple layer | Bassini (Padua, Italy)) | [30] |
(AEOM: aponeurosis of the external oblique muscle; IIR: internal inguinal or abdominal ring; EIR: external inguinal or superficial ring).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



