Submitted:
17 October 2025
Posted:
20 October 2025
You are already at the latest version
Abstract
Introduction: There are many well described approaches to symptomatic hernia management; however, there remains a significant patient population with limited options for a durable ventral hernia repair with reasonable risk of infection and recurrence. Drawing from orthopedic literature, we changed our approach to this clinical problem and developed a palliative ventral herniorrhaphy pathway.
Methods: An IRB approved retrospective review (January 2017-June 2019) of patients’ palliative ventral herniorrhaphy was performed.
Results: 43 patients included with female preponderance (58.6%) , mean age 61.5 years. The mean BMI was 38.1kg/m2 (IQR: 25.4-62) and 28 patients (65.1%) had a history of prior wound/mesh infection. Repair within 48 hours was performed in 14 patients. Overall polypropylene prosthetic was implanted in 26 patients, and bioprosthetic/absorbable mesh was used in the remaining; , the mean surface area of implanted mesh was 561 cm2. The most common wound complications identified were skin separation (30.2%) and seroma formation (48.8%). Hernia recurrence occurred in 4 (9.3%) patients with mean followup 24.1 months (9-37). Three patients had central lightweight mesh rupture and 1 had recurrence (bioprosthetic mesh); all were subsequently repaired.
Conclusion: Despite a small volume of patients, our palliative ventral hernia repair pathway offers durable repair with an acceptable risk of recurrence and mesh infection in patients who would otherwise be considered non-operative. Local surgical site complications were frequent but did not appear to affect the risk of recurrence or long-term complications.
Keywords:
ventral hernia antibiotics beads mesh
1. Introduction:
The incidence of ventral hernia in the United States is increasing [1]. Wound complications, mesh infection and hernia recurrence remain concerns with any ventral hernia repair [2]. The commonly used Carolinas Equation for Determining Associated Risks of ventral hernia repair (CeDAR) application can provide an estimate of wound infection with a risk less than or equal to 10% generally considered acceptable [3]. While there are a multitude of approaches to ventral hernia repair there remains a gap for patients who are not “ideal candidates” and are at high risk for wound complications and recurrence. These patients are typically NOT offered ventral herniorrhaphy, but many go on to present urgently or emergently. The surgical options in this setting are limited and are profoundly high risk especially in the setting of strangulation. Surgeons are placed in the difficult position of watching a high-risk hernia or offering a suboptimal repair.
As a quaternary care medical center our surgical group decided to approach these complicated ventral hernias using palliative ventral hernia pathway. This pathway helped us selecting patients who were deemed inoperable due to failed previous surgeries, loss of domain, multiple comorbidities including obesity but not candidates for bariatric surgery, infected muscle flap, failed component separation, recent recurring episodes of incarceration with small bowel obstruction where only other option would be a bridge biologic mesh, and not candidates for formal abdominal reconstruction. None of the patients were candidates for bariatric surgery due to multiple prior surgeries and loss of domain. We devised this technique utilizing orthopedic infectious disease literature where antibiotics beads were used to prevent infection [4,5,6].
The core of this practice is herniorrhaphy using a mesh onlay repair and antibiotic beads to prevent wound infection associated with mesh onlay technique.
This study was designed to evaluate the outcomes of our novel approach for ventral hernia repair in this complex patient population. Herein we discuss our surgical pathway, surgical steps, postoperative management strategy, follow-up plan, the lessons learned, and future directions.
2. Methods
This retrospective review examined patients undergoing palliative ventral herniorrhaphy at Mayo Clinic Rochester Minnesota from January of 2017 to June 2019. A total of 43 consecutive patients were identified. This study has been reviewed by the Institutional Review Board (IRB) and have therefore been performed by the ethical standards laid down in an appropriate version of the Declaration of Helsinki (as revised in Brazil 2013). Informed consent was taken from all patients. BlueSky statistics software version 7.0 Chicago IL, USA was used for data analysis. We calculated means and proportions for perioperative variables. Post-operative characteristics were compared between groups using Fisher’s exact test for different variables.
2.1. Procedural Details
Hernia Repair
Patients presented for initial consultation with one of 4 surgeons providing this palliative approach. Initial evaluation included history, physical exam, and abdominal/pelvic computed tomography (CT) imaging with intravenous contrast (Figure 1). Herniorrhaphy was only offered to patients that had no readily identifiable need for repeat future laparotomy. Hence to this point, patients who had not previously undergone cholecystectomy underwent ultrasound examination to evaluate for cholelithiasis. If cholelithiasis was identified, then the patient was offered cholecystectomy as a staged procedure during the same hospital admission. Patients identified to have infected mesh were offered total mesh explantation as a staged procedure as well. Stage 1 included a cholecystectomy with bile spillage and/or mesh explantation, temporary abdominal closure with ABTHERA™ device and initiation of systemic antibiotic therapy. . Stage 2 was performed 48 hours after initial operation and entailed ventral hernia repair with mesh onlay and antibiotic bead implantation. Patients completed a seven-day course of empiric or culture directed antibiotics. If the mesh is not infected and cholecystectomy was performed without evidence of bile spillage then herniorhaphy was performed in same setting. s. The goal at the time of herniorrhaphy was to raise skin flaps to expose the external oblique aponeurosis for overlap on mesh of 3 to 5 cm in all directions. If the umbilicus was to be mobilized as part of a skin flap, umbilectomy was performed to reduce risk of postoperative wound complications. The rectus muscles were medialized if possible and fascial closure performed with interrupted 0 PDS ™ figure of 8 sutures taking 1 cm bites of tissue; tails of every other suture were left long to thread through the prosthetic mesh. For patients in which rectus muscles could not approximated to midline, a portion of hernia sac was preserved as a barrier between the mesh and intraperitoneal contents. The hernia sac was closed with interrupted PDS ™ figure of 8 sutures. If hernia sac was retained, the border of fascial edge was marked for later placement of fixation sutures to prevent recurrent herniation between the mesh onlay and the external oblique aponeurosis. If good quality fascial closure could be achieved, bioprosthetic (SurgiMend®) or bioabsorbable mesh (Phasix ™) was placed in onlay fashion. If the rectus muscles could not be brought to midline or fascial closure was felt to be of poor quality (as determined by the operating surgeon) permanent polypropylene mesh was placed in an onlay fashion. Early in the protocol we used lightweight polypropylene mesh, but three patients suffered central mesh rupture; so, within the first year we switched to using medium weight polypropylene mesh (Ventralight ™) with the adhesion barrier scraped off. An outer perimeter of 0 PDS™ sutures was placed to tack the mesh to the external oblique. Adequate tension was placed on these sutures to avoid wrinkling of the mesh and to take tension off the midline suture line. Numerus simple sutures of 0 PDS ™ were placed at 0.5-1 cm intervals to fill in the space between the outer perimeter of sutures and the medial extent of the fascia. The goal of these sutures was to obliterate dead space between the prosthesis and the external oblique but also to share the load of forces on the mesh between numerous points of fixation. Round JP drains (19 French) were placed under each flap and remained in situ until output was less than 30 ml/day from each drain for two consecutive days.
Antibiotic Beads
Antibiotics beads were created by mixing a half dose of bone cement with 1 g of Vancomycin, 1.2 g of Gentamicin and 50 mg of Amphotericin. Beads were rolled to 1 - 1.5 cm in diameter, and strung on a 0 Prolene™ suture. This string of beads was placed in the wound, we then placed above mentioned two 19 French drains, after which the skin was closed with vertical mattress sutures of 0 Prolene™ followed by skin stapling device (Figure 2). An Incisional wound vac was applied for 3-5 days. Sutures, skin staples and one JP drain were left in place for 30 days to avoid seroma.
3. Results
Details for the 43 identified patients are prestented in Table 1. Urgent repair (during hospital stay after acute presentation) was performed in 14 (32.5%) cases. Overall polypropylene mesh was implanted in 26 patients; bioprosthetic/absorbable mesh was implanted for hernia repair in the remaining 17 cases. The mean surface area of implanted mesh was 561 cm2. Antibiotic bead exchange was performed in 38 (88.3%) cases; beads are still indwelling in 28 (65.1%) cases (Table 2).
Several wound complications were identified; skin separation (30.2%) and seroma (48.8%) were the most common (Table 3). Hernia recurrence was seen in 4 (9.3%) cases with mean followup 24.1 months (9-37). As noted above, 3 cases had central lightweight permanent mesh rupture, and one developed recurrence after placement bioprosthetic mesh which were subsequently repaired. There was one incidence of patient death (2.3%) related to wound infection and one incidence of mesh infection that required explantation and repair revision (Table 3).
4. Discussion
In this study using a novel technique for ventral hernia repair, recurrence was seen in 4 (9.3%) cases with mean followup 24.1 months (9-37). Holihan et al documented 16.5% (0–36%) ventral hernia recurrence rate using mesh onlay technique in their meta-analysis [4]. As we have gained experience, we have noted that hernia recurrence is associated with use of lightweight permanent mesh. Low density mesh (lightweight) is associated with increased risk of hernia recurrence when compared with high density mesh (heavy weight) [5]. We had three patients who had hernia recurrence due to central mesh rupture with lightweight mesh which prompted us to use medium weight mesh for these repairs. One patient who was on chronic high dose steroid therapy developed hernia recurrence with the use of bioprosthetic mesh onlay.
Various authors have suggested that morbid obesity (BMI, ≥40 kg/m2) and other risk factors should be considered as contraindication for large ventral hernia repair [6,7]. While limiting ventral herniorrhaphy to ideal patients may improve recurrence and complication rates, there remains a large population of patients with ventral hernias who are not ideal candidates and remain at high risk for acute incarceration and strangulation. As our group performs complex abdominal wall reconstructions, but also cares for patients coming to the emergency department with ventral hernia incarceration and strangulation, we recognized a gap in care for those patients considered high risk for herniorrhaphy. This led us to develop a palliative ventral hernia technique which could be offered to these patients to protect them from hernia strangulation. This required a change in our philosophy from trying a single procedure to managing ventral hernia as a chronic disease, possibly necessitating multiple repeat interventions. Despite the known complications of the mesh onlay technique, including skin complications and seroma, we chose this technique because mesh could be more easily explanted if infection did ensue, the herniorrhaphy could be repeated in case of recurrence and this technique does not preclude component separation in the future if the patient were to undergo significant weight loss. Chevrel and others have described variations of onlay mesh repair, including intraperitoneal onlay mesh techniques,While the Chevrel technique of myofascial advancement for reinforcement reduced recurrence, all of the onlay techniques remain at increased risk for surgical site infection. [8] We adopted the use of antibiotic beads to try to reduce the risk of mesh infection, which we have always considered to be the devastating complication in this high-risk cohort of patients. The average BMI of the patients in this study was 38 kg/m2 (35% of patients had BMI ≥40 kg/m2) and 65% had history of prior wound or mesh infection. Most of these patients had previously been denied ventral herniorrhaphy due to their complexity and expected poor outcome.
The Ventral Hernia Working Group describes hernia specific complications as surgical site occurrence (SSO) to standardize the nomenclature when studying outcomes after hernia repair. SSO is a category of complications that includes surgical site infection (SSI), seroma, hematoma, wound dehiscence, and enterocutaneous fistula [9]. Petro et al found an association between SSO and the complexity of hernia repair using a hernia staging system that focuses on the defect size and presence of contamination [10]. Most of our patients would be categorized as stage 2 and 3 categories per the Petro et al classification with skin separation in 13(30.2%), hematoma in 1(2.3%), and seroma formation in 22 (48.8%). Patients with skin separation including hematoma were debrided in the same hospitalization to prevent further wound complications. Patients with seroma first managed with percutaneous radiology guided drain placement, but patients with chronic seroma formation underwent antibiotic bead exchange, irrigation, and debridement.
Studies have shown that the rate of surgical site infection exceeds 50% after single stage infected ventral hernia repair [11,12]. Kugler et al mentioned dual stage approach in the presence of infected field to decrease the risk of SSI [13]. We have used the same approach in 17 (39.5%) patients who underwent staged ventral hernia repair due to infected field.
Buchholz et al first described the use of antibiotic beads in Europe in 1970s [14]. It originated within the orthopedics literature to provide a depot source of antibiotic into an infected surgical field. Use of antibiotic beads has been subsequently described in prosthetic infections in vascular, cardiac, orthopedic surgery, trauma, and in contaminated fields [15,16,17]. Antibiotic beads can be retained for a long period of time and therefore allow for an extended period of local antimicrobial coverage [18]. They can also maintain the minimum inhibitory concentrations for months, and risk of systemic antibiotic toxicity and exposure remains low [19]. With the available literature on the clinical use of antibiotic beads and our own group experience of using antibiotic beads to salvage infected ribs stabilization hardware [20], we adopted this to try to reduce the risk and the morbidity of ventral hernia mesh infection in these patients. Despite high risk of SSO in our patient population, only 2 patients (4.65%) developed SSI. We presume that this is related to our use of antibiotic beads to suppress local bacterial growth with the goal of preventing mesh infection. Additionally, we know that with mobilization of skin flaps we create a relatively ischemic setting which is at risk of infection. The beads work to counteract this risk. As we gained experience with this approach, we did refine our practice. We initially exchanged or explanted beads in almost every patient (88.3%) at 3–6-month intervals but as we gained experience, we realized that in patients in which beads were well incorporated in scar without an associated seroma that explantation of beads appeared unnecessary and was associated with additional morbidity. In patients without seroma, we left the beads in situ for an indefinite time.. We have left beads in place in 28 (65%) patients without apparent side effects.
We have refined our technique as we gained experience in our cohort to minimize SSO to include using numerous skin staples with spaced Prolene™ interrupted vertical mattress sutures, placing an incisional wound vac, avoiding abdominal binder to prevent skin flap ischemia, keeping at least one drain for one month and ensuring that abdominal wall closure is tight enough to take tension off the skin closure. We have one death in our series. This patient has had extensive skin flap necrosis, which we attributed due to use of an abdominal binder on more than expected ischemic flaps. Despite multiple returns to the OR we were unable to get skin to heal due to skin flap loss. In addition to an infected abdominal wound with exposed mesh this patient also had a chronic unrepairable vesicovaginal fistula with chronic nephrostomy tubes. Rather than undergo mesh explantation and ongoing management of a chronic abdominal wound the patient chose comfort cares. This case does highlight the importance of adequate skin closure over the mesh as well as the importance of avoiding skin flap necrosis.
As we have gained experience with this technique, we incorporated lessons learned into the care of these patients. As our goal is to obviate the need for future surgery disrupting hernia repair, we have embraced incidental cholecystectomy based on prior study at our institution cumulative probability of 21.5 % of requiring cholecystectomy within 5 years of laparotomy for colorectal surgery [21]. Because of the high risk of seroma formation leading to skin separation, the vertical mattress sutures and skin staples used for skin closure are left in place for 1 month. Likewise, we now leave one subcutaneous drain in place for 1 month. Incisional VAC dressings are now utilized for 5 days postoperatively. We no longer use lightweight polypropylene mesh because of the risk of central mesh rupture. We use more numerous and densely placed tacking sutures to obliterate dead space under the mesh as well as to share load, particularly in morbidly obese patients. Even in morbidly obese patients, we limit mesh overlap to healthy fascia to 5 cm to protect skin perforator vessels. When reoperating on these patients for recurrence or infection after mesh onlay, we can excise infected and bridging mesh, but can leave healthy mesh that is densely attached to external oblique and the use of antibiotic beads seems to prevent infection of the otherwise healthy retained mesh.
Limitations and Future Directions
This was the retrospective small case series hence may not be true representative of causative outcomes, but we are working in prospective fashion to get data from ongoing patients and will report the outcomes accordingly in our future study.
5. Conclusions
Implantation of antibiotic beads with onlay ventral herniorrhaphy for high-risk patients does not appear to decrease risk of surgical site occurrences but does appear in this early review to have a reasonably low risk of hernia recurrence and low risk of mesh infection requiring explantation.. This technique appears to provide an option for high-risk patients with ventral hernia who are at risk for strangulation who are not “optimal” candidates for traditional surgical options.
References
- Poulose BK, Shelton J, Phillips S, Moore D, Nealon W, Penson D, et al. Epidemiology and cost of ventral hernia repair: making the case for hernia research. Hernia. 2012;16(2):179-83. [CrossRef]
- Mariette C, Wind P, Micelli Lupinacci R, Tresallet C, Adham M, Arvieux C, et al. Practice patterns in complex ventral hernia repair and place of biological grafts: a national survey among French digestive academic surgeons. J Visc Surg. 2014;151(1):9-16. [CrossRef]
- Arnold MR, Kao AM, Otero J, Marx JE, Augenstein VA, Sing RF, et al. Mesh fistula after ventral hernia repair: What is the optimal management? Surgery. 2020;167(3):590-7. [CrossRef]
- Holihan JL, Nguyen DH, Nguyen MT, Mo J, Kao LS, Liang MK. Mesh Location in Open Ventral Hernia Repair: A Systematic Review and Network Meta-analysis. World J Surg. 2016;40(1):89-99. [CrossRef]
- Holihan JL, Hannon C, Goodenough C, Flores-Gonzalez JR, Itani KM, Olavarria O, et al. Ventral Hernia Repair: A Meta-Analysis of Randomized Controlled Trials. Surg Infect (Larchmt). 2017;18(6):647-58. [CrossRef]
- Desai KA, Razavi SA, Hart AM, Thompson PW, Losken A. The Effect of BMI on Outcomes Following Complex Abdominal Wall Reconstructions. Ann Plast Surg. 2016;76 Suppl 4:S295-7. [CrossRef]
- Evans KK, Chim H, Patel KM, Salgado CJ, Mardini S. Survey on ventral hernias: surgeon indications, contraindications, and management of large ventral hernias. Am Surg. 2012;78(4):388-97. [CrossRef]
- Kockerling F. What Do We Know About the Chevrel Technique in Ventral Incisional Hernia Repair? Front Surg. 2019;6:15. [CrossRef]
- Ventral Hernia Working G, Breuing K, Butler CE, Ferzoco S, Franz M, Hultman CS, et al. Incisional ventral hernias: review of the literature and recommendations regarding the grading and technique of repair. Surgery. 2010;148(3):544-58. [CrossRef]
- Petro CC, O'Rourke CP, Posielski NM, Criss CN, Raigani S, Prabhu AS, et al. Designing a ventral hernia staging system. Hernia. 2016;20(1):111-7. [CrossRef]
- Krpata DM, Stein SL, Eston M, Ermlich B, Blatnik JA, Novitsky YW, et al. Outcomes of simultaneous large complex abdominal wall reconstruction and enterocutaneous fistula takedown. Am J Surg. 2013;205(3):354-8; discussion 8-9. [CrossRef]
- Trevino JM, Franklin ME, Jr., Berghoff KR, Glass JL, Jaramillo EJ. Preliminary results of a two-layered prosthetic repair for recurrent inguinal and ventral hernias combining open and laparoscopic techniques. Hernia. 2006;10(3):253-7. [CrossRef]
- Kugler NW, Bobbs M, Webb T, Carver TW, Milia D, Paul JS. A dual-stage approach to contaminated, high-risk ventral hernia repairs. J Surg Res. 2016;204(1):200-4. [CrossRef]
- Buchholz HW, Engelbrecht H. [Depot effects of various antibiotics mixed with Palacos resins]. Chirurg. 1970;41(11):511-5.
- Huiras P, Logan JK, Papadopoulos S, Whitney D. Local antimicrobial administration for prophylaxis of surgical site infections. Pharmacotherapy. 2012;32(11):1006-19. [CrossRef]
- Morgenstern M, Vallejo A, McNally MA, Moriarty TF, Ferguson JY, Nijs S, et al. The effect of local antibiotic prophylaxis when treating open limb fractures: A systematic review and meta-analysis. Bone Joint Res. 2018;7(7):447-56.
- White TL, Culliford AT, Zomaya M, Freed G, Demas CP. Use of Antibiotic-Impregnated Absorbable Beads and Tissue Coverage of Complex Wounds. Am Surg. 2016;82(11):1068-72. [CrossRef]
- McConoughey SJ, Howlin RP, Wiseman J, Stoodley P, Calhoun JH. Comparing PMMA and calcium sulfate as carriers for the local delivery of antibiotics to infected surgical sites. J Biomed Mater Res B Appl Biomater. 2015;103(4):870-7. [CrossRef]
- Aiken SS, Cooper JJ, Florance H, Robinson MT, Michell S. Local release of antibiotics for surgical site infection management using high-purity calcium sulfate: an in vitro elution study. Surg Infect (Larchmt). 2015;16(1):54-61. [CrossRef]
- Junker MS, Kurjatko A, Hernandez MC, Heller SF, Kim BD, Schiller HJ. Salvage of rib stabilization hardware with antibiotic beads. Am J Surg. 2019;218(5):869-75. [CrossRef]
- Juhasz ES, Wolff BG, Meagher AP, Kluiber RM, Weaver AL, van Heerden JA. Incidental cholecystectomy during colorectal surgery. Ann Surg. 1994;219(5):467-72; discussion 72-4. [CrossRef]
Figure 1.
(A&B) Axial section of CT scan shows a 61-year-old male patient with large ventral hernia with loss of domain. (C&D) Axial section of CT scan shows post hernia repair with antibiotic beads in situ.
Figure 1.
(A&B) Axial section of CT scan shows a 61-year-old male patient with large ventral hernia with loss of domain. (C&D) Axial section of CT scan shows post hernia repair with antibiotic beads in situ.
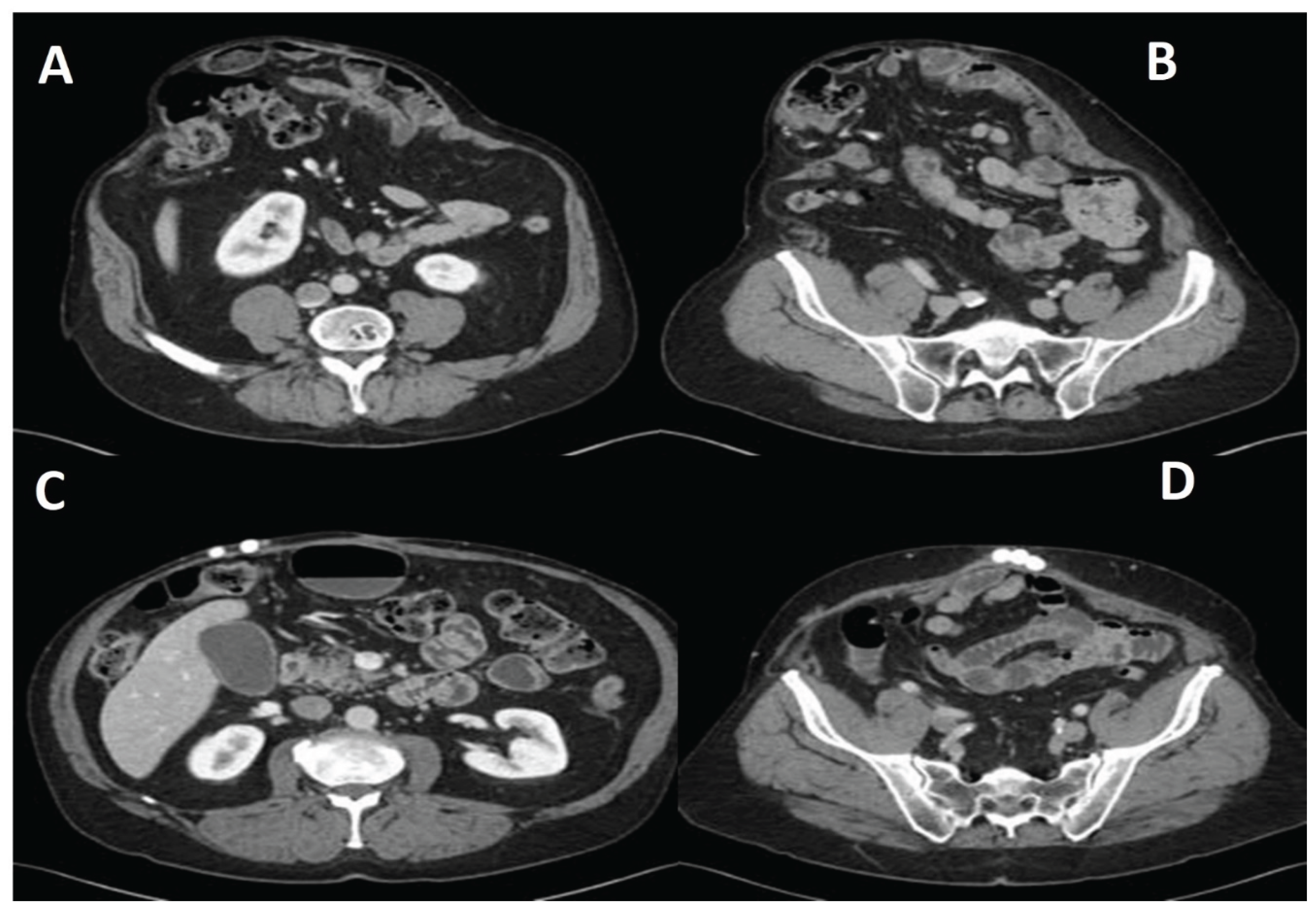
Figure 2.
Intraoperative photographs of the same 61-year-old male seen in Figure 1. (A) Arrow shows antibiotic beads string sutured over Onlay mesh; JP drain is also visible. (B) Skin closed using a combination of closely spaced staples and occasional sutures with occasional Prolene™ vertical mattress Sutures.
Figure 2.
Intraoperative photographs of the same 61-year-old male seen in Figure 1. (A) Arrow shows antibiotic beads string sutured over Onlay mesh; JP drain is also visible. (B) Skin closed using a combination of closely spaced staples and occasional sutures with occasional Prolene™ vertical mattress Sutures.
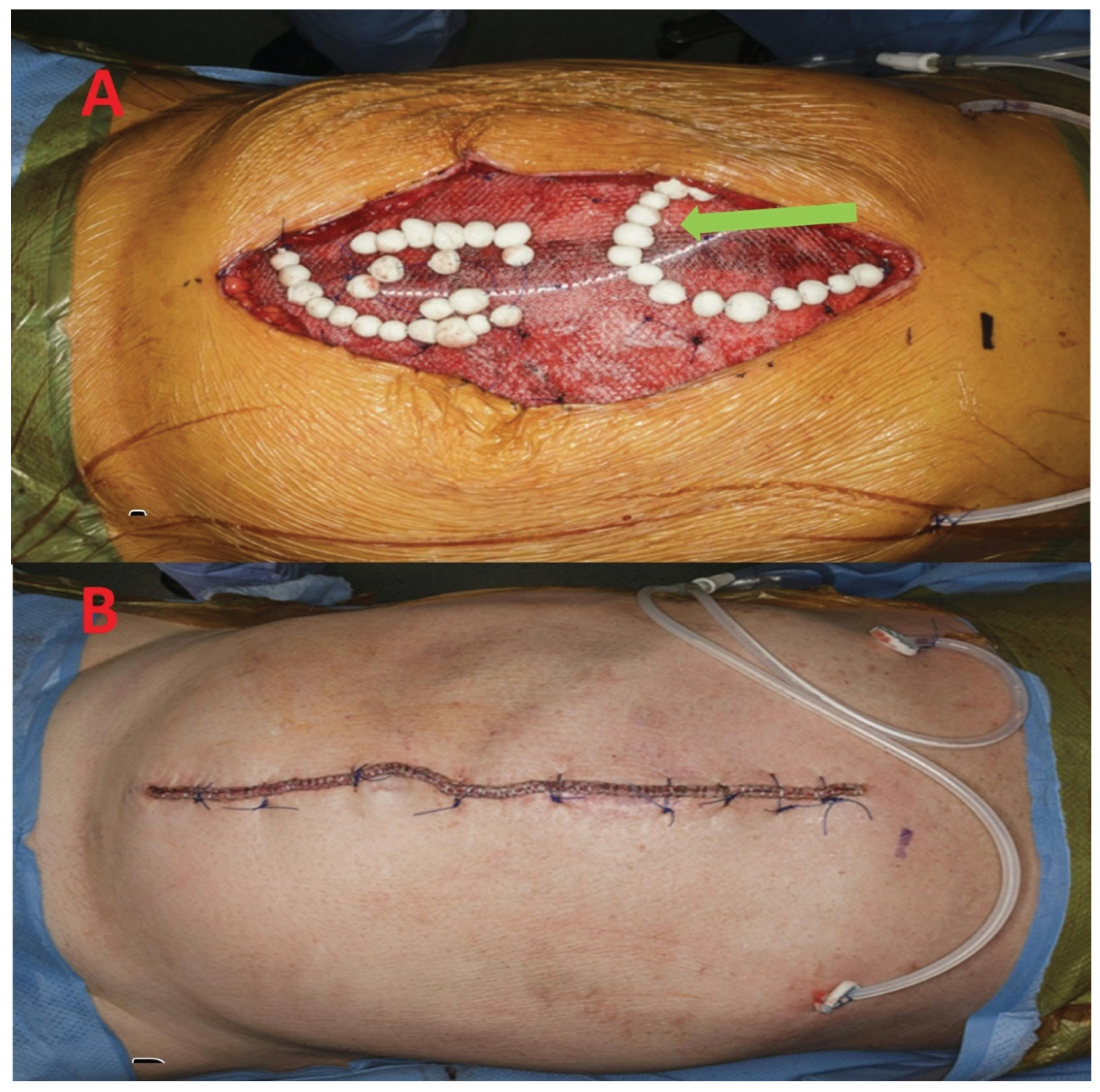

Table 1.
Patient cohort characteristics.
| Preoperative characteristics | Values |
|---|---|
| Age, y, mean (IQR) | 61.5 (23.0 – 83.0) |
| Female sex, n (%) | 24 (58.6) |
| BMI, kg/m2, mean (IQR) | 38.1 (25.4 – 62.0) |
| Current smoker, n (%) | 4 (9.3) |
| Anticoagulation use, n (%) | 7 (16.2) |
| Hypertension, n (%) | 30 (69.7) |
| COPD, n (%) | 13 (30.2) |
| Diabetes mellitus, n (%) | 11 (25.5) |
| Steroid use, n (%) | 3 (6.9) |
| Prior wound/mesh infection, n (%) | 28 (65.1) |
| Methicillin resistant Staphylococcus (MRSA), n (%) | 3 (6.9) |
Table 2.
Operative characteristics.
| Operative characteristics | Values |
|---|---|
| Nature of surgery Elective, n (%) Urgent, n (%) |
29 (67.4) 14 (32.5) |
| Types of mesh Polypropylene, n (%) Absorbable, n (%) |
26 (60.4) 17 (39.5) |
| Mean surface area of mesh, cm2 | 561 |
| Antibiotic beads Exchanged, n (%) Left in-situ, n (%) |
38 (88.3) 28 (65.1) |
Table 3.
Postoperative characteristics.
| Postoperative characteristics | Values |
|---|---|
| Hernia recurrence, n (%) Central lightweight mesh rupture, n (%) |
4 (9.3) 3 (6.9) |
| Skin separation, n (%) Repeated skin separation, n (%) |
13 (30.2) 3 (6.9) |
| Hematoma, n (%) | 1 (2.3) |
| Seroma, n (%) | 22 (48.8) |
| Mesh infection, n (%) | 2 (4.65) |
| Mortality, n (%) | 1 (2.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



