
Submitted:
15 January 2026
Posted:
16 January 2026
You are already at the latest version
Abstract
Background: Healthcare professionals experience continuous biological and psychosocial stressors that may disturb oral and systemic homeostasis. Alterations in salivary secre-tion, mucosal immunity, and microbiome composition reflect adaptive cellular responses to chronic occupational stress. Understanding these mechanisms may provide a biologi-cal framework for resilience and wellbeing in clinical everyday practice. Objective: To narratively review the evidence linking oral cellular and molecular mechanisms, -salivary biomarkers, epithelial and immune cell activity, and microbiome dynamics- with stress, fatigue, burnout, and wellbeing outcomes among healthcare professionals. Methods: A PRISMA-guided search of PubMed, Scopus, Web of Science, and Cochrane Oral Health identified studies investigating oral cellular or molecular parameters in relation to occu-pational stress or wellbeing indicators in healthcare settings. Eligible designs included observational, experimental, and interventional studies. Data were extracted using stand-ardized forms, quality was appraised via ROBINS-I and the Newcastle-Ottawa scale, and results were synthesized thematically. Results: Evidence from 99 studies suggests that chronic occupational stress elevates salivary cortisol, oxidative stress markers, and pro-inflammatory cytokines (IL-6, TNF-α), while reducing protective salivary immuno-globulin A and microbiome diversity. Balanced oral immune and microbial profiles were associated with better psychological adaptation and lower fatigue indices. Conclusions: Oral cellular homeostasis offers a promising window into the biological underpinnings of occupational stress and resilience in healthcare professionals. Systematic integration of salivary and mucosal biomarkers into workplace wellbeing programs could enhance ear-ly detection of dysregulated stress physiology. Future interdisciplinary research should bridge oral biology, occupational medicine, and mental health to strengthen sustainable wellbeing strategies across the health workforce.
Keywords:
epithelial-immune crosstalk
; mucosal homeostasis
; biopsychosocial models
; oxidative stress
; occupational stress response
; occupational wellbeing indices
; salivary diagnostics in workplace medicine
; oral homeostasis
; salivary biomarkers
; immune regulation
; microbiome
; healthcare professionals
; resilience
1. Introduction
The oral cavity constitutes a highly dynamic mucosal barrier where epithelial cells, saliva, immune mediators, and a diverse microbial community interact continuously to maintain tissue homeostasis [1,2]. The structural and functional complexity of the oral mucosa reflects its composite defense architecture meaning physical, biochemical, microbiological, and immunological layers that collectively regulate pathogen exclusion and immune tolerance [3,4]. Recent advances in mucosal immunology report that epithelial-immune crosstalk determines not only local oral health but also systemic inflammatory and neuroendocrine dynamics, highlighting the integrative nature of oral barrier biology [5,6]. The oral microbiome forms an essential component of this ecosystem, shaping immune maturation, barrier integrity, and inflammatory tone [7,8]. Dysbiosis within oral microbial communities has been linked to periodontal disease, mucosal inflammation, wound-healing dysregulation, and metabolic and neurocognitive outcomes, positioning oral microbial ecology as an important determinant of host systemic physiology [9,10]. Updated reviews have further shown that fluctuations in oral microbial composition interact with mucosal cytokine networks and epithelial signaling pathways, contributing to allostatic responses across the lifespan [11,12].
Complementing microbial mechanisms, saliva has emerged as a powerful, non-invasive diagnostic matrix that reflects both local oral status and systemic physiological states [13,14]. Salivary immunoglobulins, cytokines, proteomic signatures, and metabolites offer insight into mucosal immunity, inflammation, oxidative stress, and endocrine responses [15,16]. Contemporary analyses highlight saliva’s diagnostic potential in infection, oncology, metabolic disorders, and mucosal immunopathology, reinforcing its relevance for personalized health monitoring [17,18]. Indeed, recent immunobiology syntheses reveal that saliva integrates epithelial, microbial, and neuroendocrine signals, making it a sensitive biomarker matrix for stress-associated biological alterations [19,20].
Parallel to developments in oral biology, occupational wellbeing among healthcare professionals has become an urgent global concern, with high rates of burnout, chronic fatigue, circadian misalignment, depressive symptoms, and stress-related physiological dysregulation [21,22,23]. Systematic reviews consistently show that healthcare workers face elevated emotional and physical strain associated with workload pressure, moral distress, patient acuity, and disrupted work-rest cycles [24,25]. Importantly, biological studies increasingly demonstrate measurable physiological alterations, including immune suppression, cytokine activation, and neuroendocrine dysregulation, associated with occupational strain in healthcare environments [26,27]. Salivary biomarkers have been central in this research domain, with cortisol, SIgA, and pro-inflammatory cytokines widely used as indicators of occupational stress and allostatic load [28,29,30]. Methodological syntheses confirm that diurnal cortisol rhythms, cortisol awakening response, and stress-induced salivary cytokine fluctuations correlate strongly with occupational demands across nursing, emergency care, and shift-based medical work [31,32]. Evidence also suggests that mucosal immune components, including SIgA and epithelial-derived mediators, respond to acute and chronic stress exposure, further supporting the role of oral biomarkers in monitoring work-related physiological strain [14,33,34].
Despite these converging scientific trajectories, the interface between oral cellular homeostasis and occupational wellbeing in healthcare professionals remains substantially underexplored. Research in mucosal immunology has reported on the epithelial-immune-microbial signaling pathways but rarely considers psychosocial or occupational determinants as upstream modulators [1,5]. Conversely, occupational health studies employing salivary biomarkers often frame them as peripheral stress indicators rather than components of an interconnected mucosal system shaped by microbial and epithelial dynamics [28,30]. This disciplinary separation obscures potential bidirectional pathways through which occupational stress could influence oral homeostasis and through which oral mucosal biology might mediate resilience or vulnerability to chronic strain [33]. Healthcare professionals represent a uniquely relevant population in this context: continuous exposure to biological aerosols, pathogens, altered circadian patterns, and emotional labor may create distinct pressures on mucosal barrier immunity and microbiome stability [26,27]. Yet the extent to which occupational exposures reshape oral immune or microbial equilibrium, or how oral biomarkers might inform early detection of burnout and stress-related dysregulation, remains largely uncharacterized.
Accordingly, this narrative review aims to synthesize the current knowledge on oral cellular homeostasis, including salivary, immune, and microbiome pathways, and its potential links to occupational wellbeing in healthcare professionals. Specifically, we (i) summarize advances in oral mucosal immunity and microbiome science relevant to systemic regulation; (ii) review the diagnostic and physiological roles of salivary biomarkers in occupational contexts; and (iii) integrate emerging findings into a conceptual framework for understanding how oral biological mechanisms may interact with occupational stress, resilience, and wellbeing in healthcare settings.Within this interdisciplinary context, the present review is guided by a central question: how oral cellular homeostasis, capturing salivary endocrine and immune biomarkers, epithelial barrier function, and oral microbiome dynamics, relates to occupational wellbeing, stress physiology, and burnout vulnerability in healthcare professionals? Specifically, we examine whether chronic occupational demands, circadian disruption, and emotional strain can modulate salivary cortisol, SIgA, cytokines, or microbial community structure, and whether such biological shifts parallel validated psychological measures of stress, fatigue, and wellbeing. We further consider the methodological constraints that influence the interpretation of salivary and mucosal biomarkers and explore whether oral immune-microbial signatures may serve as early indicators of resilience or susceptibility under sustained professional pressure. Ultimately, this review seeks to outline how neuroendocrine-mucosal cross-talk might mediate the biological imprint of occupational stress and how an integrated oral-occupational health framework could enhance monitoring, prevention, and wellbeing strategies within healthcare settings. The PICO approach we used is in healthcare professionals (P), exposure to oral cellular mechanisms, including salivary, immune, and microbiome pathways (I), that is examined in relation to occupational wellbeing outcomes such as stress physiology, burnout, and resilience (O), and compared with populations experiencing lower occupational strain where applicable (C).
2. Materials and Methods
This work was designed as a narrative review aiming to synthesize current evidence on the biological mechanisms of oral cellular homeostasis -salivary, epithelial-immune, and microbiome pathways- and their potential relationship to occupational wellbeing in healthcare professionals. A narrative review methodology was selected because the research question spans multiple heterogeneous domains (oral immunology, microbiome science, salivary diagnostics, occupational medicine, psychoneuroimmunology), for which available studies vary widely in design, outcomes, biomarkers, and conceptual frameworks [35]. The goal was to provide an integrative, theory-building overview rather than a quantitative meta-analysis [36].
2.1. Search Strategy and Information Sources
The selection of databases was guided by the interdisciplinary nature of the research question, which spans oral biology, immunology, microbiome science, occupational health, and mental wellbeing. PubMed/MEDLINE was chosen as the primary biomedical database due to its comprehensive coverage of oral immunology, salivary diagnostics, stress physiology, and occupational health research, as well as its structured indexing through Medical Subject Headings (MeSH), which enabled precise mapping of core biological and psychosocial concepts. Scopus and Web of Science were included to ensure broader interdisciplinary coverage and citation tracking, capturing relevant studies published in dental science, public health, psychology, and systems biology journals that may not be indexed in PubMed alone. Cochrane Oral Health was additionally searched to identify high-quality evidence syntheses and intervention-focused studies relevant to oral health and preventive strategies.
Search queries were tailored to the indexing systems and search functionalities of each database. In PubMed/MEDLINE, both Medical Subject Headings (MeSH) and free-text keywords were employed to capture core concepts related to oral cellular homeostasis (including oral mucosa, oral immunity, saliva, and the oral microbiome), biological and stress-related biomarkers (such as cortisol, secretory IgA, cytokines, and metabolomics), and indicators of occupational wellbeing (including stress, burnout, fatigue, and healthcare professionals). Boolean operators (AND/OR) were applied to systematically combine conceptual domains while retaining thematic relevance. In Scopus and Web of Science, searches were conducted using keyword combinations applied to titles, abstracts, and author keywords in order to accommodate variations in terminology across disciplines. To ensure comprehensive coverage, the reference lists of all included articles and relevant narrative or systematic reviews were manually screened for additional eligible studies. Only peer-reviewed publications available in full English text were considered for inclusion.
2.2. Eligibility Criteria
Studies were eligible for inclusion if they met at least one of the following criteria: (1) examined oral epithelial, salivary, or microbiome mechanisms related to mucosal immunity or barrier homeostasis; (2) evaluated salivary biomarkers of stress, endocrine activity, immune activity, or inflammation; (3) assessed occupational stress, burnout, fatigue, psychological wellbeing, or physiological responses in healthcare professionals; (4) provided conceptual, mechanistic, or empirical insights bridging oral biology with systemic stress physiology. Overall, experimental, observational, interventional, and review studies were included. Exclusion criteria were: non-oral biomarkers without relevance to mucosal immunity, non-healthcare populations unless offering transferable biological mechanisms, animal studies without translational value, non-peer-reviewed documents, conference abstracts, and publications not available in English.
2.3. Study Selection Process
Two reviewers independently screened titles and abstracts for relevance. Full texts were retrieved for all studies meeting or potentially meeting the inclusion criteria. Disagreements were resolved through discussion and consensus. Although narrative in design, the review followed PRISMA principles for transparency in search and selection [37]. The heterogeneity of study designs, biomarkers, and occupational outcomes precluded quantitative meta-analysis.
PRISMA Flow Description
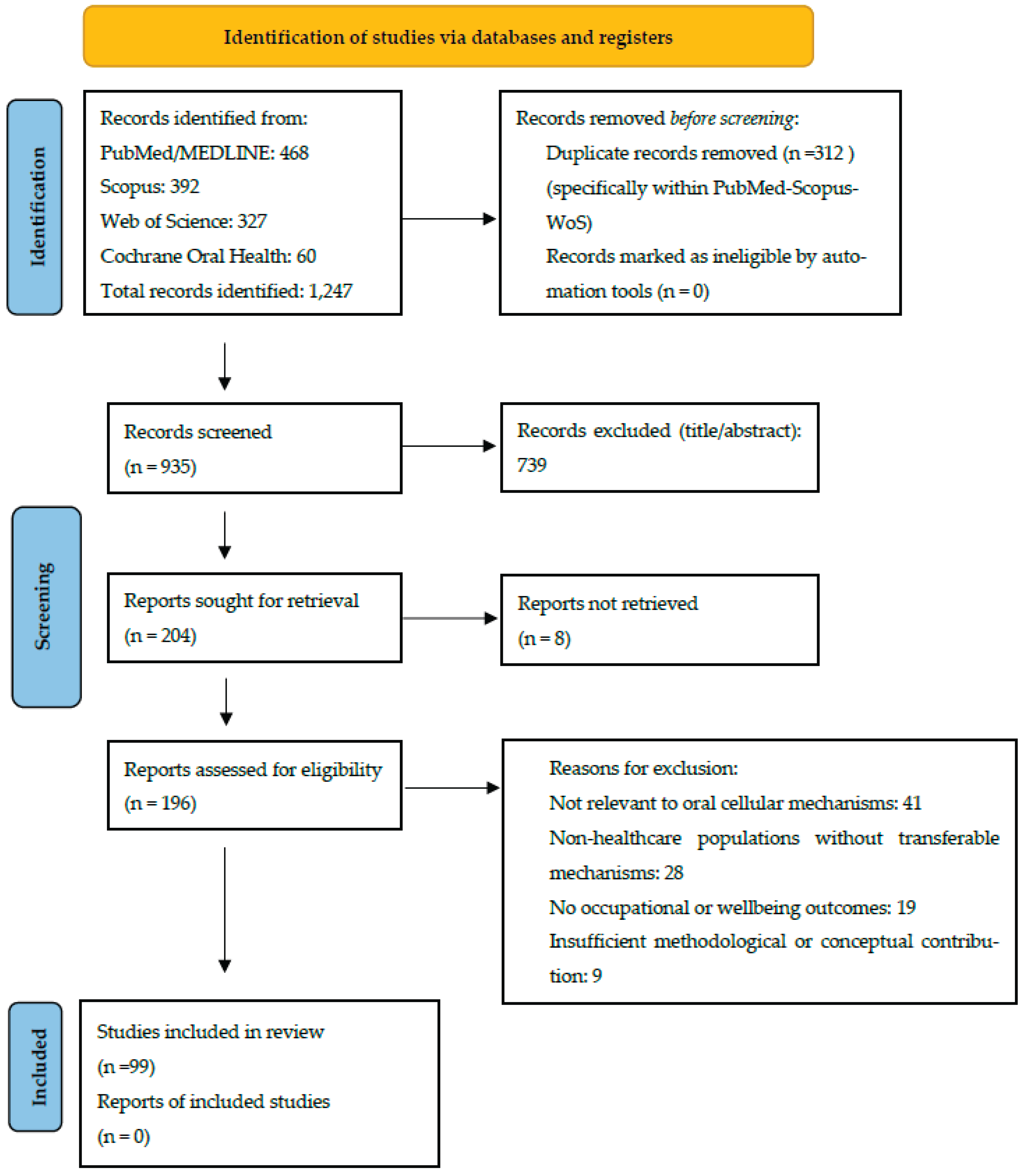
The literature search across PubMed/MEDLINE, Scopus, Web of Science, and Cochrane Oral Health initially yielded 1,247 records. After removal of 312 duplicate records, 935 unique articles remained for title and abstract screening. During the initial screening phase, 739 records were excluded because they did not address oral biology, salivary or mucosal mechanisms, occupational stress, or healthcare-related populations. The remaining 196 articles were assessed in full text for eligibility. Of these, 97 full-text articles were excluded for the following reasons: lack of relevance to oral cellular mechanisms (n = 41), focus on non-healthcare populations without transferable biological mechanisms (n = 28), absence of occupational or wellbeing-related outcomes (n = 19), or insufficient methodological or conceptual contribution (n = 9). A total of 99 studies met the inclusion criteria and were incorporated into the qualitative synthesis. These studies encompassed mechanistic immunology and microbiome research, salivary biomarker investigations, occupational health and wellbeing studies, and selected interventional trials relevant to stress biology and resilience in healthcare professionals. Given the heterogeneity of study designs, populations, biomarkers, and outcome measures, no quantitative meta-analysis was performed.
Figure 1.
Prisma flow chart of the study.
2.4. Data Extraction and Thematic Organization
Data extraction focused on: (i) study design; (ii) population characteristics; (iii) oral biomarkers assessed (salivary cortisol, SIgA, cytokines, microbiome profiles, epithelial immune markers); (iv) occupational or psychological outcomes (burnout, stress, fatigue, circadian disruption); and (v) mechanistic insights linking oral biology to systemic physiology. Thematic synthesis was applied, grouping emerging evidence into three major domains: (1) oral mucosal immunity and epithelial barrier regulation; (2) oral microbiome composition and its interaction with immunological and neuroendocrine pathways; (3) salivary biomarkers as indicators of stress physiology and occupational load in healthcare professionals.
Cross-domain integration was then performed to construct a conceptual model describing potential bidirectional pathways between oral cellular homeostasis and occupational wellbeing. Τhe model derived out of this search is to be seen in Figure 2.
2.5. Quality Considerations and Methodological Limitations
Given the narrative design of this review and the substantial heterogeneity of the included literature, the uniform application of formal risk-of-bias assessment tools (such as ROBINS-I, the Newcastle-Ottawa Scale, or RoB 2) was not considered appropriate across all study types. Instead, methodological quality was evaluated qualitatively, with attention to key features relevant to the research question, including sample size adequacy, validity and specificity of oral and salivary biomarkers, conditions and timing of saliva collection, analytical and laboratory techniques, control for diurnal and contextual variation, and the operationalization and measurement of occupational stressors. Particular consideration was given to methodological transparency and consistency in defining biological and psychosocial outcomes. Variability in biomarker assays, microbiome sequencing platforms, bioinformatic pipelines, and psychological assessment instruments was recognized as a major source of methodological heterogeneity, limiting direct comparability across studies [38]. These methodological differences were explicitly taken into account during the synthesis process and informed the relative weighting and interpretation of findings within and across thematic domains. Rather than serving as grounds for exclusion, such limitations were treated as critical contextual factors shaping the strength and transferability of the available evidence.
2.6. Review Scope and Conceptual Orientation
This review does not aim to present an exhaustive systematic catalogue of all relevant studies; rather, it integrates high-quality and mechanistically informative evidence to outline how oral immune-microbial-endocrine dynamics may intersect with occupational stress biology. The approach reflects the inherently interdisciplinary nature of the topic and seeks to advance conceptual understanding, generate hypotheses, and identify gaps requiring targeted empirical investigation.
3. Results
Across the final body of evidence included in this review, studies were organized into seven major thematic domains reflecting the core components of oral cellular homeostasis and their intersections with occupational wellbeing: (i) oral mucosal immunity and epithelial barrier regulation, (ii) oral microbiome composition and its systemic physiological links, (iii) integrated evidence on oral microbiome, mucosal immunity, saliva, and systemic-stress biology, (iv) occupational Stress, wellbeing & biomarkers, (v) dietary, nutritional, and food-related modulators of oral cellular homeostasis, and (vi) interventions targeting stress biology, oral homeostasis, and occupational wellbeing. This thematic categorization allowed for the synthesis of highly heterogeneous research designs, ranging from mechanistic immunology and microbiome analyses to cross-sectional wellbeing studies and randomized controlled interventions, while preserving the mechanistic coherence necessary for interpreting how oral biological pathways may mirror or modulate occupational stress physiology. Table 1 presents the key articles mapped to each domain, summarizing study characteristics, methodological approaches, and principal findings relevant to the conceptual model of oral homeostasis as a potential biomarker and resilience interface in healthcare professionals.
3.1. Oral Mucosal Immunity and Epithelial Barrier Responses
Across the selected literature, oral mucosal immunity emerges as a tightly regulated, multilayered system in which epithelial integrity, innate immune surveillance, and resident microbiota operate as a single functional unit [34]. Mechanistic analyses demonstrate that homeostasis depends on continuous bidirectional communication between epithelial cells, commensal microorganisms, and immune mediators, a process mediated by cytokines, antimicrobial peptides, and pattern-recognition receptors that calibrate tolerance and inflammation in real time [1]. The oral mucosa is described not merely as a physical barrier but as a metabolically active immune organ whose structural and immunological layers respond rapidly to environmental disturbances, microbial pressures, and endocrine changes [15,34,46,48]. Detailed immunological mapping confirms that the oral barrier consists of an epithelial-microbial-immune triad capable of immediate adaptation via tight-junction remodeling, mucin secretion, and activation of innate effectors such as defensins and secretory IgA [3,39]. Comparative mucosal analyses reveal that, unlike the gastrointestinal tract, the oral mucosa is exposed to higher microbial diversity, rapid antigenic turnover, and continuous mechanical and chemical stress, requiring a more vigilant innate immune posture and faster epithelial renewal [5]. Central to this defense are specialized lymphocyte subsets, most notably γδ T cells, which contribute to epithelial repair, microbial containment, and immune tolerance, and which have been shown to be sensitive to neuroendocrine modulators and stress-related dysregulation [6]. Parallel advances in neuroimmune biology show that sensory innervation of the oral mucosa is intimately connected with immune activation: neuropeptides, sympathetic mediators, and glucocorticoids influence epithelial cytokine expression, dendritic cell priming, and the balance between pro- and anti-inflammatory responses [7]. Under conditions of sustained stress, these neuroimmune pathways can induce transient barrier weakening, alter antimicrobial output, and shift inflammatory thresholds [1,7]. Further immunological work maps how epithelial cells act as both structural and immune sentinels, initiating rapid signaling through Toll-like receptors, inflammasome components, and chemokine networks that guide leukocyte recruitment and microbial containment [34]. When epithelial and immune homeostasis is perturbed, whether through microbial imbalance, endocrine fluctuation, or chronic systemic stress, the mucosa demonstrates measurable shifts in permeability, cytokine gradients, oxidative stress, and immune-cell composition [1,3]. These findings indicate overall that the oral mucosa is a dynamic neuroimmune barrier whose cellular homeostasis is exquisitely sensitive to systemic physiological stressors, including those commonly observed in healthcare work environments. This establishes a strong mechanistic basis for considering epithelial-immune-microbial interactions as potential early indicators of occupational strain and resilience [39]. As seen in Figure 3, the oral mucosa functions as a dynamic epithelial-immune-microbial interface regulated by continuous bidirectional signaling among epithelial cells, innate and adaptive immune mechanisms, resident microbiota, and neuroendocrine inputs. Systemic and occupational stressors modulate these interactions through endocrine and neural pathways, leading to measurable changes in barrier integrity, immune signaling, and inflammatory balance [7,11,12]. This model illustrates the mechanistic basis by which oral cellular homeostasis may act as a sensitive biological interface for stress-related dysregulation.
3.2. Oral Microbiome Composition and Oral-Systemic Biological Interactions
Across the contemporary literature, oral cellular homeostasis emerges as the product of tightly interconnected mucosal-microbial-immune interactions that operate dynamically across the lifespan and respond sensitively to systemic, hormonal, environmental, and psychosocial influences [28,33]. Conceptual immunology frameworks describe the mucosal surface as an adaptive immune ecosystem in which commensal microbiota actively shape immune maturation, tolerance, and inflammatory thresholds from early life to aging, rather than acting as passive colonizers [7,14]. This perspective is reinforced by multi-omics and longitudinal evidence linking oral health trajectories with cognitive aging and social determinants, suggesting that oral biological integrity reflects cumulative biological and environmental exposures over time [9,10]. Within this framework, periodontitis-related research provides a concrete disease model illustrating how microbial imbalance, immune dysregulation, and systemic signaling intersect [8]. Narrative and biomarker-focused reviews consistently demonstrate that alterations in the oral microbiome are mirrored by shifts in salivary inflammatory and metabolic markers, supporting saliva as a functional readout of ongoing host-microbe conflict [8,60]. Importantly, causal inference approaches strengthen this association: Mendelian randomization analyses suggest that gut microbiota composition may exert a direct causal influence on periodontitis risk, highlighting bidirectional oral-gut microbial crosstalk rather than isolated local pathology [40]. Parallel systematic analyses of endodontic and prosthodontic conditions further show that clinical interventions and anatomical changes, such as root canal infection or denture use, reshape microbial ecology toward more inflammation-prone configurations, emphasizing the sensitivity of oral ecosystems to both biological and mechanical stressors [9,42,43].
Hormonal and immune signaling represent critical modulatory layers within this system. Clinical and experimental syntheses demonstrate that endocrine environments, particularly stress- and sex-hormone fluctuations, reshape oral microbial composition and immune tone, providing a mechanistic bridge between psychosocial stress, HPA-axis activity, and oral dysbiosis [11,17]. At the cellular level, epithelial cells are increasingly recognized as active immune sentinels that integrate microbial signals, cytokine gradients, and neuroendocrine inputs to regulate barrier integrity and inflammatory responses [34]. Transcriptomic and proteomic studies of saliva extend this view, showing that salivary RNA and protein profiles capture both local immune activity and systemic physiological states, effectively positioning saliva as a multi-layered biosensor rather than a passive secretion [18,20]. The functional relevance of these interactions becomes particularly evident in contexts of immune challenge and environmental stress. Studies of viral infection, vaccination, and inflammatory disease demonstrate that oral mucosal immunity plays a decisive role in shaping systemic immune responses, viral susceptibility, and inflammatory resolution, with saliva-mediated mechanisms contributing to immune defense and pathogen control [46,47,48]. Microbiome-derived metabolites, including indole derivatives and short-chain fatty acids, further modulate immune signaling and inflammatory balance, reinforcing the concept that microbial metabolism constitutes a key regulatory layer of host immunity [50].
Finally, emerging interventional and environmental studies highlight the plasticity of oral biological systems. Nutritional interventions, micronutrient supplementation, and enriched environments have been shown to modulate salivary cortisol, immune markers, microbiome composition, and even emotional regulation, illustrating that oral cellular homeostasis responds measurably to modifiable behavioral and environmental inputs [45,51,54]. In sum, these findings converge on a unified model in which oral biology reflects and potentially mediates, the biological imprint of systemic stress, immune challenge, and lifestyle factors, supporting its relevance as both a mechanistic hub and a translational target in occupational and preventive health research.
3.3. Salivary Biomarkers of Endocrine, Immune, and Metabolic Activity
The evidence base on saliva converges on a central premise: saliva is a biologically active, information-dense matrix that integrates endocrine, immune, microbial, and metabolic signals at the oral mucosal interface and therefore functions as both a readout and a regulator of mucosal homeostasis [13,39]. Narrative syntheses emphasize that salivary composition captures local oral processes while remaining sensitive to systemic physiological states, which makes saliva particularly suitable for repeated, low-burden monitoring in clinical and occupational contexts where dynamic fluctuations are expected [13,16,17,18]. Mechanistically, saliva contains a layered repertoire of immune mediators (e.g., sIgA, cytokines, antimicrobial peptides), endocrine markers (e.g., cortisol), and molecular cargo (metabolites, proteins, nucleic acids, and extracellular vesicles), enabling multi-scale profiling of stress biology, immune tone, and disease susceptibility [14,17,18,40]. Importantly, methodological work suggests that salivary biomarker interpretability depends on sampling conditions, diurnal timing, assay characteristics, and contextual exposures, which are critical when translating saliva-based measures into occupational health monitoring [16,30].
From an immunological standpoint, saliva functions as a frontline effector of mucosal immunity: natural and inducible responses in the oral cavity rely on sIgA, cytokine signaling, and innate antimicrobial factors that collectively regulate microbial colonization and support epithelial integrity under continuous antigenic pressure [14,84]. Proteomic evidence further indicates that salivary proteins participate directly in host-microbe regulation by modulating adhesion, biofilm dynamics, and pathogen neutralization, linking molecular composition to ecological stability [18,49]. This ecological role is reinforced by microbiology-focused reviews showing that saliva is not merely a passive medium but actively stabilizes the oral microbiome through nutrient provisioning and selective antimicrobial pressure, thereby shaping community resilience and inflammatory thresholds [39,49,50]. In parallel, salivary metabolomics expands the diagnostic scope beyond single analytes toward systems-level signatures: metabolomic patterns reflect inflammatory and metabolic states bridging oral and systemic disease processes, while also offering potential for risk stratification and monitoring [15,52,53,54]. Transcriptomic approaches similarly position the salivary transcriptome as an accessible window into local and systemic gene expression programs relevant to immune activation and stress responses [55].
Emerging salivary “next-generation” biomarkers strengthen this integrative model. Reviews of salivary exosomes highlight their role as diagnostic and signaling mediators in oral disease, expanding saliva’s utility from biochemical readouts to intercellular communication platforms [70]. At the endocrine level, saliva-based hormone diagnostics consolidate the rationale for cortisol monitoring in stress-related contexts, supporting the linkage between HPA-axis dynamics and mucosal immune modulation [17,30]. Collectively, these lines of evidence support the interpretation that salivary immune-endocrine-omic profiles can capture early biological dysregulation and recovery dynamics, potentially complementing subjective measures and enabling translational monitoring frameworks in high-demand healthcare environments [13,16,39]. Further, endocrine signaling adds a second regulatory layer. Diagnostic reviews centered on hormone detection highlight saliva as a matrix for measuring free (biologically active) fractions of steroid hormones, particularly cortisol, with good correlation to serum levels and strong practical advantages for field and occupational studies [17]. Landmark work in occupational and environmental medicine established salivary cortisol as a core indicator of HPA-axis activation and stress-related physiological burden, supporting its use in shift-work, healthcare, and high-demand professions [28]. More recent methodological syntheses refined this picture, emphasizing that diurnal patterns, the cortisol awakening response, sampling timing, and assay characteristics critically influence interpretability, and must therefore be carefully standardized in research linking occupational conditions to salivary readouts [30,31]. Together, these findings position salivary cortisol and related hormones as central tools for quantifying the endocrine dimension of occupational stress biology.
Metabolomic and transcriptomic studies extend the scope of salivary biomarkers beyond individual molecules toward system-level signatures. Metabolomics work demonstrates that salivary metabolic profiles track systemic metabolic states, inflammation, and disease risk, offering a multiplex, hypothesis-generating view of physiological perturbations [15]. Parallel transcriptomic approaches show that salivary RNA expression patterns can mirror local and systemic gene regulation, including stress- and immune-related pathways, suggesting that saliva can function as a minimally invasive “liquid biopsy” of both mucosal and systemic responses [46,48,55,56,57,58,59]. These high-dimensional approaches are particularly relevant to occupational settings, where chronic low-grade stress may produce subtle, multi-parameter shifts rather than large changes in any single biomarker [18,58,62].
Importantly, several reviews and empirical studies converge on the idea that the diagnostic utility of saliva depends not only on what is measured, but on how, when, and in whom it is measured [59,60]. Narrative syntheses mention the impact of collection methods, circadian timing, flow rate, stimulation, storage, and analytical platform on biomarker reliability, stressing the need for strong protocol design in both research and applied monitoring [13,63,64,65,66]. Trials that manipulate environmental or behavioral conditions illustrate this point concretely: interventions such as tele-yoga, lifestyle modification for night-shift workers, or enriched environments have demonstrated measurable changes in salivary cortisol, inflammatory markers, and microbiota-related parameters, linking modifiable workplace or lifestyle factors to salivary biomarker trajectories [26,27,32]. These findings reinforce saliva’s responsiveness to psychosocial and occupational exposures [78,79,80,81,82,83].
Taken together, the available evidence portrays saliva as a multi-layered biosensor that captures endocrine activation, immune balance, microbial interaction, and metabolic status within a single, non-invasive biological matrix [39]. Hormonal dynamics, mucosal immune activity, microbiome-derived signals, and high-dimensional molecular profiles converge to produce measurable salivary biomarker patterns. The interpretability of these patterns depends on sampling conditions, circadian timing, and analytical methodology. This framework highlights saliva’s value for capturing the biological imprint of occupational stress and for monitoring physiological responses to workplace and lifestyle interventions (Figure 4). For the purposes of occupational wellbeing in healthcare professionals, this suggests that carefully selected and standardized salivary panels, combining cortisol dynamics, SIgA, cytokine profiles, and possibly metabolomic or transcriptomic signatures, could provide a sensitive window into the biological imprint of chronic work-related stress, as well as into the efficacy of resilience-building interventions [76,77,78].
3.4. Occupational Wellbeing in Healthcare and Its Intersection with Oral Biology
The literature on occupational wellbeing consistently portrays healthcare environments as high-strain systems in which chronic psychological load, organizational pressures, and moral distress accumulate into measurable biological dysregulation [22,41,85,86]. Scoping and systematic reviews document high rates of burnout, depression, anxiety, and suicidal ideation among healthcare professionals, with nurses, physicians, and other frontline staff showing persistent vulnerability across settings and countries [22,87,88,89,90,91,92,93,94,95]. Beyond psychological outcomes, these reviews emphasize that occupational distress is biologically embodied through alterations in circadian rhythms, hypothalamic-pituitary-adrenal (HPA) axis activity, immune function, and systemic inflammation, placing healthcare workers at long-term risk for cardiometabolic and neuropsychiatric morbidity [22].
Within this broader context, emerging work in dentistry and academic health settings provides more fine-grained insight into how stress is experienced and modulated. Cross-sectional data from Greek dentistry and nursing students indicate substantial burdens of stress, anxiety, and depression two years after the COVID-19 pandemic, but also highlight resilience, hope, and spiritual wellbeing as potential protective resources that may buffer the impact of academic responsibilities [85]. Similarly, comparative work on academic dental and nursing personnel shows that indices of quality of life and wellbeing are closely related to perceived quality of services and academic functioning, suggesting that staff wellbeing is not an isolated “soft” outcome but interwoven with educational performance and service delivery [86]. Together, such studies position oral health professionals and related academic staff as a meaningful subgroup within the broader healthcare workforce, facing both typical healthcare stressors and profession-specific demands (clinical precision, infection control, patient-facing communication, and teaching responsibilities). Interventional and integrative studies further delineate the modifiable components of occupational stress biology. An integrative review of non-pharmacological interventions for healthcare workers reports that structured stress-reduction strategies, such as mindfulness, relaxation practices, and behavioral programs, can yield improvements not only in self-reported wellbeing but also in physiological markers of stress and immune function [25]. Furthermore, a pilot randomized controlled trial on tele-yoga for healthcare workers on COVID-19 duty demonstrated reductions in burnout and improvements in mental health indices, accompanied by favorable shifts in immune markers, underlining the feasibility of remote, biologically meaningful interventions in high-demand clinical contexts [26]. Similarly, a randomized crossover lifestyle intervention in female night-shift healthcare workers reported benefits in metabolic and mental health parameters, with concomitant changes in salivary cortisol and related biomarkers, directly linking occupational scheduling, behavioral modification, and measurable stress physiology [27]. Such findings collectively indicate that occupational distress is not a fixed trait but a modifiable state, with interventions capable of recalibrating both psychological and biological endpoints.
Salivary and mucosal biomarkers sit at the intersection of these phenomena. Landmark work on salivary biomarkers in occupational and environmental medicine positioned saliva, particularly salivary cortisol, as a central non-invasive tool for assessing acute and chronic stress load in workplace settings [28]. More recent methodological syntheses refine this paradigm by articulating how sampling protocols, diurnal timing, and assay characteristics critically shape the interpretation of salivary cortisol and related markers in biobehavioral research [30]. The cortisol awakening response (CAR), in particular, has been identified as a sensitive, relatively stable index of HPA-axis activation under chronic stress, further reinforcing saliva’s utility for tracking occupational strain [31]. Randomized trials manipulating environmental richness in early life provide additional proof-of-principle that contextual factors can alter both salivary cortisol profiles and microbiota-related parameters, illustrating the plasticity of stress-related biomarkers in response to environmental modulation [32].
When viewed alongside the evidence on oral mucosal immunity (Section 3.1), microbiome dynamics (Section 3.2), and the complex biomarker landscape of saliva (Section 3.3), these occupational studies suggest a coherent, though still underdeveloped, picture. Healthcare workers, including dental professionals and academic staff-experience chronic psychosocial stress that is biologically inscribed through endocrine, immune, and metabolic pathways, many of which can be accessed via oral biomarkers [22,96,97]. At present, most occupational studies treat saliva primarily as a convenient stress readout [87,98,99]. However, the underlying science of oral epithelial barriers, immune responses, and microbial ecosystems indicates that the oral cavity itself may be an active participant in stress adaptation and vulnerability [100]. This creates a conceptual bridge between occupational wellbeing and oral cellular homeostasis, supporting the hypothesis that dentists and other healthcare professionals could be monitored and perhaps protected through integrated panels of salivary, immune, and microbiome indicators that capture both psychological load and mucosal resilience over time.
3.5. Dietary, Nutritional, and Food-Related Modulators of Oral Cellular Homeostasis
Dietary and nutritional factors constitute critical upstream modulators of oral cellular homeostasis, exerting their effects through interconnected immune, microbial, and metabolic pathways that closely parallel mechanisms described in intestinal and systemic biology [88,89]. Systematic and narrative syntheses demonstrate that diet shapes oral epithelial integrity, mucosal immune tone, and microbial ecology by regulating substrate availability, inflammatory signaling cascades, and redox balance within the oral environment [88,89,92]. Diets enriched in fermentable fibers, polyphenols, and bioactive micronutrients favor the production of microbial-derived metabolites, most notably short-chain fatty acids (SCFAs), which exert anti-inflammatory, barrier-stabilizing, and immunoregulatory effects, whereas highly processed, sugar-rich dietary patterns are consistently associated with dysbiosis, oxidative stress, and pro-inflammatory signaling in oral tissues [89,90,91,92,93]. Emerging evidence further indicates that dietary inflammatory potential is associated with distinct oral and gut microbiota profiles and systemic inflammatory markers, supporting the concept that diet-driven inflammation influences host-microbiome interactions across mucosal sites [90]. Mechanistic analyses highlight SCFAs as key mediators linking dietary substrates to epithelial energy metabolism, immune modulation, and microbial stability in both the oral cavity and the gastrointestinal tract [91,93]. Within this framework, prebiotics, probiotics, postbiotics, and synbiotics represent complementary nutritional strategies capable of reshaping microbial composition, strengthening epithelial defense mechanisms, and calibrating innate and adaptive immune responses [88,89]. Although much of the mechanistic evidence originates from gastrointestinal models, converging data support the transferability of these pathways to the oral cavity, where constant microbial exposure and rapid epithelial turnover render oral tissues particularly responsive to dietary inputs [91,92,93]. Collectively, these findings position diet not merely as a background lifestyle factor but as an active biological regulator of oral cellular homeostasis, with implications for inflammation control, immune balance, and stress-related vulnerability in healthcare populations [94]. Building on these diet-microbiome-immune interactions, postbiotics have emerged as a promising class of bioactive compounds through which nutritional modulation may exert targeted effects on oral cellular homeostasis.
- Postbiotics
Postbiotics appear as non-viable microbial cells or live microorganisms, structural components, or metabolites comprising diverse bioactive compounds such as short-chain fatty acids (SCFAs), exopolysaccharides (EPS), bacteriocins, antioxidant enzymes, surface layer proteins, and bacterial lysates. They use pattern recognition receptors and epigenetic modifications to enhance epithelial barrier function, regulate innate and adaptive immune responses, and modulate host gene expression [106]. Obesity, immune modulation, and mental health are the outcomes of their health-promoting potential, despite reduced viability and antibiotic resistance transfer issues [107,108].
A growing body of evidence indicates that postbiotics exert antioxidant, anti-inflammatory, immunomodulatory, and metabolic effects that are relevant to both systemic and oral health, supporting their role as biologically active mediators of diet-microbiome-host interactions [95,96,109,110]. Key postbiotic components, including short-chain fatty acids (SCFAs), polysaccharides, proteins, and bacterial cell wall fragments, contribute to microbial balance and protection against immune-mediated and inflammatory disorders by modulating epithelial function and immune signaling pathways [97,111,112]. In particular, Lactobacillus-derived postbiotics have demonstrated promising effects on glucose regulation, obesity-related metabolic dysregulation, and intestinal homeostasis, highlighting their relevance in the context of metabolic-immune crosstalk [98,113,114]. Complementary to postbiotics, prebiotics-defined as non-digestible substrates such as inulin and oligofructose-selectively stimulate beneficial microbial taxa, enhance SCFA production, and promote metabolically favorable shifts in bile acid and fatty acid metabolism, thereby reducing the risk of metabolic and inflammatory disorders [99,115,116]. Further, synbiotics, which combine probiotics and prebiotics, further optimize microbial survival and functionality, yielding synergistic effects on microbial stability and host immune responses [99]. Conclusively, the integrated use of prebiotics, probiotics, postbiotics, and synbiotics represents a complementary and biologically coherent strategy for modulating the microbiota and its downstream immune and metabolic effects, with emerging relevance for oral cellular homeostasis and disease prevention, although further mechanistic and long-term clinical studies are warranted [117,118].
Moreover, exopolysaccharides (EPSs) are high-molecular weight carbohydrate polymers produced by a range of commensal and probiotic microorganisms and are increasingly recognized as bioactive mediators of host-microbe interactions across mucosal surfaces [119]. Accumulating evidence demonstrates that EPSs exert a broad spectrum of health-promoting effects, including inhibition of pathogenic adhesion to epithelial surfaces, reinforcement of mucosal barrier integrity, and modulation of innate and adaptive immune responses [120,121,122]. Structurally, EPSs are classified into homopolysaccharides (HoPSs), composed of repeating units of a single monosaccharide, and heteropolysaccharides (HePSs), consisting of complex repeating units of different monosaccharides; this structural diversity is closely linked to functional specificity in epithelial interaction and immune modulation [123,124]. Recent mechanistic studies indicate that EPSs can interact directly with epithelial cells to enhance tight-junction protein expression and mucin production, thereby strengthening barrier function and contributing to mucosal homeostasis [122,125]. In parallel, EPSs have been shown to modulate immune signaling pathways by attenuating pro-inflammatory cytokine production and promoting regulatory immune responses, including effects on dendritic cell activation and T-cell polarization [126,127]. Beyond immunoregulation, anticancer properties of EPSs have been increasingly reported, including inhibition of tumor cell proliferation, induction of apoptosis, and modulation of oxidative stress pathways, with EPSs derived from Lactobacillus species receiving particular attention due to their consistent bioactivity and favorable safety profile [128,129,130]. Collectively, contemporary evidence supports EPSs as multifunctional microbial metabolites that contribute to mucosal barrier stability, immune balance, and epithelial resilience, with emerging relevance for oral cellular homeostasis within diet-microbiome-host interaction frameworks.
Further, SCFAs are absorbed and transported through the bloodstream to peripheral tissues, exerting systemic effects [131] playing critical roles in gut homeostasis, playing key roles as anti-inflammatory and immunomodulatory mediators and acting as a bridge between microbiota and host immunity [132]. In intestinal epithelial cells (IECs), acetyl-CoA is the metabolic product of SCFAs via the TCA cycle, offering energy production and immune cell function [133,134].
Additionally, bacteriocins are secreted by Gram-positive and Gram-negative bacteria, with either narrow or broad inhibitory spectra, and are ribosomally synthesized, proteinaceous antimicrobial peptides [135]. They protect themselves via immunity proteins and efflux pumps by producing strains [136]. Pore formation in bacterial membranes is their main action, leading to lysis, while reducing resistance development [137]. Primary bacteriocin producers are LABS-including Pediococcus, Leuconostoc, Lactococcus, Enterococcus, Streptococcus, Lactobacillus, and Bifidobacterium [138].
- Mechanisms of action of postbiotics and probiotics
Postbiotics and probiotics through multiple mechanisms engaging innate and adaptive immune responses exert notable immunomodulatory effects. Most specifically probiotics interact with TLRs (Toll-like receptors), which are pivotal components of the host’s initial defense against pathogenic microorganisms. Modulation of innate immune pathways is carried out by probiotics through TLR signaling. For instance, recognition of probiotic ligands and often formation of heterodimers such as TLR2/TLR6 is done by TLR2, inducing tolerogenic IL-10 secretion and mediation of anti-inflammatory effects [139,140].
Key intracellular signaling cascades, including nuclear factor-kappa B (NF-κB) and mitogen-activated protein kinases (MAPKs) are affected by probiotics thereby facilitating communication with the host immune system. Hence, this affects the production of anti-inflammatory cytokines and chemokines, ultimately contributing to maintaining immune homeostasis [141]. Similarly, postbiotics, particularly butyrate and propionate, exhibit substantial immunomodulatory effects. Butyrate enhances the diversity of regulatory T cells (Tregs), while propionate facilitates the expansion of peripheral Tregs within the intestinal mucosa. Colonic health is promoted by reducing luminal pH, stimulating epithelial cell proliferation, and enhancing colonic blood flow [119,142]. Their role is key in gluconeogenesis, serving as an essential energy source for colonocytes and intestinal epithelial cells. Finally, their contribution to cellular homeostasis by promotion of apoptosis in colon cancer cells, thereby supporting metabolic function and colorectal health is noteworthy [143].
In Figure 5 we show the interconnected pathways through which postbiotics and probiotics influence mucosal and systemic physiology. Postbiotics, including short-chain fatty acids (SCFAs), exopolysaccharides (EPSs), bacteriocins, and bacterial structural components, exert their effects predominantly via metabolic signaling and epigenetic regulation, whereas probiotics act through live microbial interactions with host epithelial and immune cells, primarily via pattern-recognition receptors such as Toll-like receptors (TLRs). These upstream signals converge on key intracellular pathways, including NF-κB and MAPK signaling, leading to modulation of innate and adaptive immune responses, promotion of regulatory T-cell (Treg) activity, and attenuation of pro-inflammatory cytokine production. Downstream outcomes include reinforcement of epithelial barrier integrity, stabilization of microbial ecosystems, regulation of metabolic function, and protection against chronic inflammation. Collectively, the figure conceptualizes how diet-microbiome-host interactions mediated by postbiotics and probiotics support oral cellular homeostasis and broader systemic resilience.
3.6. Interventions Targeting Stress Biology, Oral Homeostasis, and Occupational Wellbeing
Interventions relevant to occupational wellbeing increasingly operate across two complementary levels: (i) modulating stress physiology and mental health outcomes through scalable behavioral and digital strategies, and (ii) strengthening oral-systemic health through nutrition-focused approaches and structured coaching models that translate biological mechanisms into daily practice [99,100]. Digital lifestyle interventions show measurable benefits across stress, anxiety, depression, and broader wellbeing outcomes, supporting their role as scalable tools for prevention and early intervention in occupational contexts [100,101]. In parallel, non-pharmacological interventions used in healthcare environments, including mind-body and behavioral approaches, demonstrate clinically meaningful improvements in stress-related outcomes and support a multi-component approach to workforce resilience [25,105]. Evidence from an interventional trial in healthcare workers further suggests that structured mind-body programs such as tele-yoga can improve burnout-related outcomes while also influencing immune markers, reinforcing the biological plausibility of integrated stress-immune interventions in high-demand clinical settings [104]. Lifestyle programs targeting vulnerable occupational groups such as night-shift healthcare workers also indicate improvements in metabolic and mental health outcomes, aligning with the broader view that circadian and behavioral optimization can reduce allostatic load and improve wellbeing [144].
From the oral-systemic health perspective, nutrition-based interventions and diet-oriented health models provide a coherent framework for linking dietary modulation, microbiome balance, and inflammatory control with oral health outcomes, which may indirectly support occupational resilience by reducing chronic inflammatory burden [95,96,99,145]. Reviews focusing on functional foods, gut microbiome modulation, and metabolic health further emphasize that dietary strategies can shape host-microbe interactions relevant to inflammation and systemic regulation, particularly in conditions characterized by metabolic vulnerability such as diabetes [98]. Within dentistry, probiotic- and prebiotic-oriented approaches have been positioned not only as biological adjuncts but also as behaviorally mediated interventions that benefit from structured patient coaching, supporting sustained adherence and prevention-oriented oral health behaviors [97]. Coaching models for independent older adults further illustrate how effective intervention depends on implementation design, goal setting, tailored education, motivational support, and continuous feedback, rather than informational exposure alone, an approach that is transferable to occupational wellbeing programs in healthcare [95]. Finally, interventions targeting occupational wellbeing must also account for contextual and psychosocial determinants that shape stress trajectories, including caregiver burden and moral injury, which are increasingly recognized as high-impact drivers of distress in healthcare and allied settings [102,103]. Taken together, the evidence supports a layered intervention paradigm in which digital and behavioral stress-reduction tools, structured mind-body programs, circadian and lifestyle optimization, and nutrition- and coaching-based oral health strategies act synergistically to improve psychological outcomes while potentially influencing biological pathways linked to immune balance and systemic inflammation [25,99,100].
3.7. Conceptual Funnel of Occupational Stress, Oral Cellular Homeostasis, and Professional Wellbeing
Figure 6 illustrates the sequential pathway through which occupational exposures shape systemic stress physiology, disrupt oral cellular homeostasis (salivary, epithelial-immune, and microbiome mechanisms), and ultimately influence professional wellbeing outcomes. The current inverted-pyramid form highlights that intervention points appear last, positioned at the narrowest section of the model, reflecting the empirical reality that most healthcare systems respond to stress after dysregulation has already occurred-that is, only when burnout, fatigue, or biological strain becomes clinically visible [22,24]. However, the model is intentionally designed so that the pyramid can be conceptually reversed. When flipped, the intervention layer moves to the top, becoming the entry point rather than the final response. In this orientation, proactive measures, such as stress-modulating strategies, circadian alignment, microbiome-supportive behaviors, and saliva-based biomarker monitoring, act upstream to stabilize the systemic stress response, protect oral mucosal and microbial homeostasis, and prevent downstream impairment of wellbeing [25,27,28,31]. At the end, viewing the diagram in this reversible way emphasizes a key argument of this review: oral cellular mechanisms are not merely passive endpoints of occupational strain but early, sensitive interfaces where dysregulation can be detected and potentially corrected, before professional wellbeing deteriorates. Transforming the model from a reactive to a preventive scaffold aligns with broader calls for integrative occupational health strategies that combine biological, psychological, and organizational approaches to strengthen the resilience of healthcare professionals, including dentists [85,86].
It represents: 1. Occupational exposures (Clinical workload, psychosocial stressors, time pressure, circadian disruption, infection control demands, and interpersonal demands in healthcare settings.), 2. Systemic stress response (Activation of the HPA axis with altered cortisol rhythms (including changes in the cortisol awakening response), sympathetic overactivation, low-grade systemic inflammation, and disturbed circadian alignment.), 3. Disruption of oral cellular homeostasis (a. Salivary System: Changes in salivary cortisol, secretory IgA, cytokines (IL-6, TNF-α), antimicrobial peptides, and metabolic/proteomic signatures; reduced buffering and antimicrobial capacity. b. Epithelial–Immune Barrier: Altered tight junction integrity, impaired mucosal repair, increased inflammatory signaling, and compromised innate immune responses. c. Oral Microbiome: Reduced microbial diversity, dysbiosis, shifts toward pro-inflammatory or stress-responsive taxa, altered metabolite production (e.g., SCFAs, indole derivatives), and weakened ecological stability.), 4. Feedback to systemic physiology (Amplification of systemic inflammation, altered neuroimmune communication, impaired stress recovery, microbiome-gut-brain axis signaling, and endocrine-mucosal crosstalk contributing to chronic allostatic load.), 5. Professional wellbeing outcomes (Increased fatigue, burnout, emotional exhaustion, anxiety, depressive symptoms, cognitive overload, reduced resilience, reduced occupational engagement, and increased susceptibility to oral and systemic disease.)
3.8. Risk of Bias
Studies included in this review exhibit several methodological limitations that require cautious interpretation without diminishing the value of their findings. A substantial proportion of the microbiome, mucosal immunity, and occupational wellbeing literature remains cross-sectional, restricting the ability to determine directionality or causal pathways among stress physiology, oral cellular mechanisms, and wellbeing outcomes [7,11]. Microbiome studies vary in sequencing methods, sampling protocols, and analytical pipelines, which can introduce between-study heterogeneity and limit direct comparability. Also, research involving salivary biomarkers often shows inconsistencies in sampling timing and diurnal control, reflecting known challenges in biobehavioral research and contributing to potential measurement variability [28,30]. Further, occupational wellbeing studies, including those involving dental students, academic personnel, and healthcare workers, frequently rely on validated self-report instruments, which, while widely accepted, may introduce elements of recall bias and subjective variability [24,85,86]. Moreover, interventional studies report more structured designs, yet sample sizes and follow-up durations remain modest, limiting conclusions about long-term physiological effects [26,27]. Despite these limitations, the overall convergence of evidence across diverse methodologies supports the broader conceptual links explored in this review and highlights the need for stronger longitudinal and mechanistic research rather than diminishing the current findings.
4. Discussion
This review integrates evidence across oral biology, occupational health, and behavioral science to support the concept that oral cellular homeostasis operates as a sensitive biological interface of occupational stress and resilience in healthcare professionals, with dentistry representing a high-exposure occupational model [25,85,86,145,146]. Across these domains, convergent findings indicate that chronic occupational strain is biologically embodied through hypothalamic-pituitary-adrenal (HPA) axis activation, mucosal immune modulation, epithelial barrier alterations, and microbiome shifts, all of which are detectable in saliva and related oral biofluids [17,66,147,148]. Importantly, these biological signals exhibit dynamic temporal variability and may precede, or remain undetected by, self-report instruments, positioning saliva-based biomarkers as complementary, real-time indicators of physiological load in occupational settings [16,100,101].
As it was revealed, biological plausibility is supported by a coherent mechanistic cascade in which occupational stress activates the HPA axis, elevating cortisol and sympathetic tone, with downstream suppression of mucosal immunity and disruption of epithelial integrity [30,34]. Reduced secretory IgA levels, altered cytokine profiles, and impaired tight-junction regulation compromise epithelial turnover and barrier function, thereby reshaping microbial ecology within the oral cavity [14,17,49]. Resultant dysbiosis and low-grade inflammation can, in turn, feed back into systemic stress pathways via neuroimmune and metabolic signaling, reinforcing a bidirectional amplification loop between stress biology and mucosal dysfunction [53,66,75,81]. Within this framework, diet-derived modulators, particularly postbiotics such as short-chain fatty acids, exopolysaccharides, and bacteriocins, emerge as biologically credible intervention levers capable of stabilizing epithelial barriers, recalibrating immune signaling, and supporting microbial homeostasis [97,98,99]. Experimental and clinical nutrition studies further indicate that such microbial metabolites intersect immune, endocrine, and metabolic pathways, positioning nutritional strategies as modulators of both stress physiology and oral cellular resilience [45,61,74].
Additionally, integration with psychological and resilience-oriented models strengthens the interpretation of these biological findings. From a resilience perspective, stable salivary IgA patterns, preserved epithelial integrity, and balanced microbiome profiles are associated with adaptive stress recovery and reduced susceptibility to burnout and emotional dysregulation [26,100]. This supports a biopsychosocial model in which biological robustness at the mucosal interface contributes actively to emotional regulation, occupational sustainability, and mental well-being, rather than functioning solely as a passive marker of distress [101,103,144].
Key limitations of the current evidence base include the predominance of cross-sectional designs, modest sample sizes, heterogeneity in salivary sampling protocols and microbiome analytics, and a limited number of longitudinal or integrated multi-omics studies [15,16,55]. Critically, most intervention studies do not employ oral biomarkers as primary outcomes, constraining causal inference and delaying translational implementation in occupational health frameworks [25,27]. These limitations report on the need for standardized saliva collection protocols (including timing and diurnal control), harmonized analytical pipelines, and integrative study designs that combine biological, psychological, and occupational metrics to advance precision prevention strategies in high-stress healthcare professions [13,99,145].
Implications for future research and occupational health practice are both substantive and actionable. First, the deployment of salivary biomarker panels, including cortisol dynamics, secretory IgA, inflammatory cytokines, and targeted omics approaches, should be prioritized as early-warning indicators within occupational health surveillance frameworks, given their sensitivity to dynamic stress-related physiological changes [15,17,85,86,97,145,146,147,148]. Second, microbiome-informed monitoring should be incorporated for high-risk professional groups, as accumulating evidence links occupational strain with shifts in oral microbial ecology and mucosal immune balance [39,49,149,150,151,152,153].
Third, future interventions should adopt hybrid, systems-level designs that integrate stress-management strategies (e.g., mindfulness-based approaches, circadian alignment), targeted dietary and postbiotic interventions, and organizational or workload redesign, with outcomes evaluated against both biological (salivary, microbiome, immune) and psychological endpoints [26,99,145]. Finally, these findings support a shift towards a preventive, upstream occupational health model, moving beyond reactive burnout management to proactive stabilization of stress biology, mucosal immunity, and oral cellular homeostasis [22,27,96,97,98,99]. Collectively, this body of evidence repositions the oral cavity from a passive biomarker reservoir to an active biological interface within occupational stress physiology, offering feasible pathways for early detection, prevention, and resilience-building in healthcare workforces [13,14].
5. Conclusions
This narrative review highlights oral cellular homeostasis as a dynamic and sensitive interface linking occupational stress biology with immune, microbial, and epithelial regulation. Evidence suggests that salivary biomarkers and oral microbiome patterns capture real-time physiological responses to occupational strain, offering advantages over self-report measures alone. Dietary and behavioral modulators, particularly postbiotics and stress-management interventions, emerge as promising, biologically plausible strategies to support mucosal resilience and wellbeing. Integrating oral biomarker monitoring with preventive occupational health frameworks may enable earlier detection of risk, targeted interventions, and more sustainable resilience strategies for healthcare professionals.
Author Contributions
Conceptualization, M.A. and T.V.; methodology, M.A. and T.V.; software, M.A. and T.V.; validation, M.A. and T.V.; formal analysis, M.A. and T.V.; investigation, M.A. and T.V.; resources, M.A. and T.V.; data curation, M.A. and T.V.; writing-original draft preparation, M.A. and T.V.; writing—review and editing, M.A. and T.V.; visualization, M.A. and T.V.; supervision, M.A. and T.V.; project administration, M.A. and T.V.; funding acquisition, M.A. and T.V.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Lin, D.; Yang, L.; Wen, L.; Lu, H.; Chen, Q.; Wang, Z. Crosstalk between the oral microbiota, mucosal immunity, and the epithelial barrier regulates oral mucosal disease pathogenesis. Mucosal Immunol. Epub. 2021, 14, 1247–1258. [Google Scholar] [CrossRef]
- Ptasiewicz, M.; Grywalska, E.; Mertowska, P.; Korona-Głowniak, I.; Poniewierska-Baran, A.; Niedźwiedzka-Rystwej, P.; Chałas, R. Armed to the Teeth-The Oral Mucosa Immunity System and Microbiota. Int. J. Mol. Sci. 2022, 23, 882. [Google Scholar] [CrossRef]
- Şenel, S. An Overview of Physical, Microbiological and Immune Barriers of Oral Mucosa. Int. J. Mol. Sci. 2021, 22, 7821. [Google Scholar] [CrossRef]
- Suárez, L.J.; Arboleda, S.; Angelov, N.; Arce, R.M. Oral Versus Gastrointestinal Mucosal Immune Niches in Homeostasis and Allostasis. Front. Immunol. 2021, 12, 705206. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.Y.; Tan, Y.Q.; Zhou, G. γδ T cells in oral diseases. Inflamm. Res. 2024, 73, 867–876. [Google Scholar] [CrossRef]
- Wang, Z.; Song, K.; Kim, B.S.; Manion, J. Sensory neuroimmune interactions at the barrier. Mucosal Immunol. 2024, 17, 1151–1160. [Google Scholar] [CrossRef]
- Iliev, I.D.; Blander, J.M.; Collins, N.; Guo, C.J.; Longman, R.S.; Sonnenberg, G.F.; Zeng, M.Y.; Artis, D. Microbiota-mediated mechanisms of mucosal immunity across the lifespan. Nat. Immunol. Epub. 2025, 26, 1645–1659. [Google Scholar] [CrossRef]
- Radu, C.M.; Radu, C.C.; Zaha, D.C. Salivary and Microbiome Biomarkers in Periodontitis: Advances in Diagnosis and Therapy-A Narrative Review. Medicina 2025, 61, 1818. [Google Scholar] [CrossRef] [PubMed]
- Galindo-Moreno, P.; Lopez-Chaichio, L.; Padial-Molina, M.; Avila-Ortiz, G.; O’Valle, F.; Ravida, A.; et al. The impact of tooth loss on cognitive function. Clin. Oral Investig. 2022, 26, 3493–3500. [Google Scholar] [CrossRef]
- Liang, A.; Gomaa, N. Social capital associates with better cognitive health, oral health and epigenetic age deceleration: Findings from the Canadian longitudinal study on aging. Article ID 914150231208689; Int. J. Aging Hum. Dev. 2023. [Google Scholar]
- Rus, M.J.; Sauco Carballo, C.; Faria, F.D.; Simon-Soro, A. Hormonal Environment Shapes the Oral Microbiome. Adv. Exp. Med. Biol. 2025, 1472, 225–242. [Google Scholar] [CrossRef]
- Simon-Soro, A.; et al. Microbiome and inflammatory biomarkers associated with palatal wound healing. J. Periodontal Res. 2025, 60, 664–675. [Google Scholar] [CrossRef]
- Surdu, A.; Foia, L.G.; Luchian, I.; et al. Saliva as a Diagnostic Tool for Systemic Diseases-A Narrative Review. Medicina 2025, 61, 243. [Google Scholar] [CrossRef]
- Matsuoka, M; Soria, SA; Pires, JR; Sant'Ana, ACP; Freire, M. Natural and induced immune responses in oral cavity and saliva. BMC Immunol. 2025, 18;26(1), 34. [Google Scholar] [CrossRef]
- Zhao, X; Chen, X; Lu, Y; Zhou, Z; Lin, P; Lin, Y; Hu, S; Cui, L. Saliva metabolomics: a non-invasive frontier for diagnosing and managing oral diseases. J Transl Med. 2025, 24;23(1), 582. [Google Scholar] [CrossRef]
- Albagieh, H; Alshehri, AZ; Alduraywishi, AS; Aldaws, A; AlBalawi, SS; Abu Shaqqaf, HF; Almubayi, RA. Evaluation of Salivary Diagnostics: Applications, Benefits, Challenges, and Future Prospects in Dental and Systemic Disease Detection. Cureus 2025, 16;17(1), e77520. [Google Scholar] [CrossRef]
- Ferrari, C.R.; Moraes, S.M.; Buzalaf, M.A.R. Saliva-based Hormone Diagnostics: advances, applications, and future perspectives. Expert Rev. Mol. Diagn 2025, 25, 341–355. [Google Scholar] [CrossRef] [PubMed]
- Carneiro, M.C.; da Silva, N.D.G.; Ventura, T.M.O. Salivary Proteome Role in Infection and Immunity. Adv. Exp. Med. Biol. 2026, 1492, 747–773. [Google Scholar] [PubMed]
- Heller, D.; Nery, G.B.; Bachi, A.L.L.; Al-Hashimi, I. Positive Role of Saliva in the Oral Microbiome. Adv. Exp. Med. Biol. 2025, 1472, 103–118. [Google Scholar]
- Barnes, D.; Hoke, A.; Hammamieh, R.; Gautam, A. The Salivary Transcriptome: A Window into Local and Systemic Gene Expression Patterns. Methods Mol. Biol. 2025, 2880, 1–16. [Google Scholar] [PubMed]
- Antoniadou, M. Estimation of Factors Affecting Burnout in Greek Dentists before and during the COVID-19 Pandemic. Dent. J. 2022, 10, 108. [Google Scholar] [CrossRef]
- Ungurianu, A.; Marina, V. The Biological Clock Influenced by Burnout, Hormonal Dysregulation and Circadian Misalignment: A Systematic Review. Clocks Sleep 2025, 7, 63. [Google Scholar] [CrossRef]
- Zhang, Z; Hong, W; Zhang, Y; Li, X; Que, H; Wei, X. Mucosal immunity and vaccination strategies: current insights and future perspectives. Mol Biomed. 2025, 20;6(1), 57. [Google Scholar] [CrossRef]
- Nguyen, N.; Spooner, E.; O’Balle, P.; et al. The Relationship Between Depression, Burnout, and Suicide Among Healthcare Professionals: A Scoping Review. Worldviews Evid. Based Nurs. 2025, 22, e70037. [Google Scholar] [CrossRef]
- Meneses Damasceno, K.S.; Weyll Pimentel, M.M. Non-pharmacological therapies for stress reduction in healthcare workers: An integrative review. Article ID 10519815251367229; Work. 2025. [Google Scholar]
- Naveen, K.H.; Singh, D.; Srinivasan, S.; et al. Effect of tele-yoga on burnout, mental health and immune markers of healthcare workers: A pilot RCT. Complement. Ther. Med. 2024, 87, 103109. [Google Scholar] [CrossRef]
- Robinson, L.A.; Lennon, S.; Pegel, A.R.; Strickland, K.P.; Feeley, C.A.; Watts, S.O.; Van Der Pol, J.; Roberts, M.D.; Greene, M.W.; Frugé, A.D. A Randomized Controlled Crossover Lifestyle Intervention to Improve Metabolic and Mental Health in Female Healthcare Night-Shift Workers. Nutrients 2025, 17, 3342. [Google Scholar] [CrossRef]
- Koh, D.S.Q.; Koh, G.C.H. The use of salivary biomarkers in occupational and environmental medicine. Occup. Environ. Med. 2007, 64, 202–210. [Google Scholar] [CrossRef] [PubMed]
- Špiljak, B.; Vilibić, M.; Glavina, A.; Crnković, M.; Šešerko, A.; Lugović-Mihić, L. A Review of Psychological Stress among Students and Its Assessment Using Salivary Biomarkers. Behav. Sci. 2022, 12, 400. [Google Scholar] [CrossRef] [PubMed]
- Dong, F.; Sefcik, J.S.; Euiler, E.; Hodgson, N.A. Measuring salivary cortisol in biobehavioral research: A systematic review and methodological considerations. Brain Behav. Immun. Health 2024, 43, 100936. [Google Scholar] [CrossRef] [PubMed]
- Stalder, T.; Oster, H.; Abelson, J.L.; et al. The Cortisol Awakening Response: Regulation and Functional Significance. Endocr. Rev. 2025, 46, 43–59. [Google Scholar] [CrossRef]
- Shibata, C.; Muratsubaki, T.; Shibata, S.; et al. A randomized controlled trial of environmental richness on gastrointestinal symptoms, salivary cortisol, and gut microbiota in early childhood. Sci. Rep. 2025, 15, 8493. [Google Scholar] [CrossRef]
- Sato, Y; Saijo, Y; Yoshioka, E. Work stress and oral conditions: a systematic review of observational studies. BMJ Open 2021, 11(5), e046532. [Google Scholar] [CrossRef]
- Nittayananta, W. Oral Innate Immunity and the Role of Oral Epithelial Cells. Adv. Exp. Med. Biol. 2026, 1492, 23–39. [Google Scholar] [CrossRef] [PubMed]
- Mengelkoch, S; Miryam Schüssler-Fiorenza Rose, S; Lautman, Z; Alley, JC; Roos, LG; Ehlert, B; Moriarity, DP; Lancaster, S; Snyder, MP; Slavich, GM. Multi-omics approaches in psychoneuroimmunology and health research: Conceptual considerations and methodological recommendations. Brain Behav Immun. Epub. 2023, 114, 475–487. [Google Scholar] [CrossRef] [PubMed]
- Witte, EH; Ponocny, I. Meta-analysis: a tool for constructing theories or evaluating interventions or simply proving everyday assumptions? Front Psychol. 2024, 24;15, 1377336. [Google Scholar] [CrossRef]
- Page, MJ; et al. BMJ 2021, 372, n71. [CrossRef]
- Forry, SP; Servetas, SL; Kralj, JG; Soh, K; Hadjithomas, M; Cano, R; Carlin, M; Amorim, MG; Auch, B; Bakker, MG; Bartelli, TF; Bustamante, JP; Cassol, I; Chalita, M; Dias-Neto, E; Duca, AD; Gohl, DM; Kazantseva, J; Haruna, MT; Menzel, P; Moda, BS; Neuberger-Castillo, L; Nunes, DN; Patel, IR; Peralta, RD; Saliou, A; Schwarzer, R; Sevilla, S; Takenaka, IKTM; Wang, JR; Knight, R; Gevers, D; Jackson, SA. Variability and bias in microbiome metagenomic sequencing: an interlaboratory study comparing experimental protocols. Sci Rep. 2024, 29;14(1), 9785. [Google Scholar] [CrossRef]
- Xin, Y; Lei, H. The oral mucosal barrier: a dynamic gateway in oral and systemic health. Tissue Barriers Epub ahead of print. 2026, 5, 2610035. [Google Scholar] [CrossRef] [PubMed]
- Yu, J; Zuo, Y; Yang, L; Xu, Q. Causal effects of gut microbiota on periodontitis risk: a meta-analysis of Mendelian randomization studies. BMC Oral Health 2025, 12;25(1), 1775. [Google Scholar] [CrossRef]
- Zhang, W; Ge, Y; Yao, L; Yan, Q; Wei, J; Yin, Y; Liu, B. Changes of Microbiome in Human Papillomavirus Infection and Cervical Cancer: A Systematic Review and Meta-Analysis. Cancer Rep (Hoboken) 2025, 8(6), e70246. [Google Scholar] [CrossRef]
- Liu, RZ; Bai, LA; Luo, Y; Liu, P; Hua, F; Fan, W; Fan, B. The presence of Enterococcus in root canal infections based on next-generation sequencing: A systematic review and meta-analysis. Int Endod J. 2025, 58(9), 1331–1353. [Google Scholar] [CrossRef]
- Madhan Kumar, S; Natarajan, S; Ks, S; Sundarajan, SK; Natarajan, P; Arockiam, AS. Dentures and the oral microbiome: Unraveling the hidden impact on edentulous and partially edentulous patients - a systematic review and meta-analysis. Evid Based Dent. Epub. 2025, 26(3), 150. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, A; Alagundagi, DB; Bhide, M; Patil, P. Meta-analysis of RNA-seq Data Identifies Involvement of Interferon-Induced Genes to Facilitate Blood-Brain Barrier Traversal of Neuroinvasive Pathogens. J Mol Neurosci. 2025, 20;75(3), 109. [Google Scholar] [CrossRef]
- Lu, TL; Zheng, AC; Suzuki, K; Lu, CC; Wang, CY; Fang, SH. Supplementation of L-glutamine enhanced mucosal immunity and improved hormonal status of combat-sport athletes. J Int Soc Sports Nutr. 2024, 21(1), 2300259. [Google Scholar] [CrossRef]
- Flitter, BA; Gillard, J; Greco, SN; Apkarian, MD; D'Amato, NP; Nguyen, LQ; Neuhaus, ED; Hailey, DCM; Pasetti, MF; Shriver, M; Quigley, C; Frenck, RW, Jr.; Lindesmith, LC; Baric, RS; Wei, LJ; Tucker, SN; Cummings, JF. An oral norovirus vaccine generates mucosal immunity and reduces viral shedding in a phase 2 placebo-controlled challenge study. Sci Transl Med. 2025, 14;17(798), eadh9906. [Google Scholar] [CrossRef]
- Wang, Y; Li, J; Chen, R; Xu, Q; Wang, D; Mao, C; Xiang, Z; Wu, G; Yu, Y; Li, J; Zheng, Y; Chen, K. Emerging concepts in mucosal immunity and oral microecological control of respiratory virus infection-related inflammatory diseases. Microbiol Res. Epub. 2024, 289, 127930. [Google Scholar] [CrossRef]
- Hickman, HD; Moutsopoulos, NM. Viral infection and antiviral immunity in the oral cavity. Nat Rev Immunol 2025, 25(4), 235–249. [Google Scholar] [CrossRef]
- Heller, D; Nery, GB; Bachi, ALL; Al-Hashimi, I. positive role of saliva in the oral microbiome. Adv Exp Med Biol. Doi. 2015, 1472, 103–118. [Google Scholar] [CrossRef]
- Schütz, B; Krause, FF; Taudte, RV; Zaiss, MM; Luu, M; Visekruna, A. Modulation of Host Immunity by Microbiome-Derived Indole-3-Propionic Acid and Other Bacterial Metabolites. Eur J Immunol. 2025, 55(4), e202451594. [Google Scholar] [CrossRef]
- Katta, NM; Blampied, NM; Eggleston, M; Rucklidge, JJ. Micronutrients absorbed via the oral mucosa reduce emotion dysregulation in 5-10-year-old children: A three-phased randomized wait-list-controlled trial. PLoS One 2024, 19(12), e0311794. [Google Scholar] [CrossRef]
- Albahri, J; Allison, H; Whitehead, KA; Muhamadali, H. The role of salivary metabolomics in chronic periodontitis: bridging oral and systemic diseases. Metabolomics 2025, 7;21(1), 24. [Google Scholar] [CrossRef]
- Nejat Dehkordi, A; Maddahi, M; Vafa, P; Ebrahimi, N; Aref, AR. Salivary biomarkers: a promising approach for predicting immunotherapy response in head and neck cancers. Clin Transl Oncol. 2025, 27(5), 1887–1920. [Google Scholar] [CrossRef] [PubMed]
- Shibata, C; Muratsubaki, T; Shibata, S; Aizawa, E; Watanabe, S; Kanazawa, M; Fukudo, S. A randomized controlled trial of environmental richness on gastrointestinal symptoms, salivary cortisol, and gut microbiota in early childhood. Sci Rep. 2025, 12;15(1), 8493. [Google Scholar] [CrossRef]
- Barnes, D; Hoke, A; Hammamieh, R; Gautam, A. The Salivary Transcriptome: A Window into Local and Systemic Gene Expression Patterns. Methods Mol Biol. 2025, 2880, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Xu, B; Wen, Y; Lu, J; Liu, M; Luo, X; Huang, W; Xie, H; Cheng, Y; Qiu, H; Wu, X. Saliva as a TDM Matrix and Its Application in the Model-Informed Precision Dosing. J Clin Pharmacol. 2025, 65(12), 1650–1660. [Google Scholar] [CrossRef]
- Saravanan, C; S M N Mydin, RB; Mohamed Sheriff, NR; Kaur, G; Singh Dhaliwal, S; Musa, MY. Salivaomics in head and neck cancer. Clin Chim Acta 2025, 15, 565:119952. [Google Scholar] [CrossRef]
- Santamaria, MP; Mathias-Santamaria, IF; Ferreira Bonafé, AC; Gonzalez, OA; Kirakodu, S; Monteiro, MF; Casarin, RCV; Shaddox, LM; Miguel, MMV. Microbiome and Inflammatory Biomarkers Associated With Palatal Wound Healing. J Periodontal Res. 2025, 60(7), 664–675. [Google Scholar] [CrossRef]
- Main, S; Carrilho, MR; Alessandri-Bonetti, A; Sawicki, C; Rao, J; Hall, S; Sangalli, L. Salivary Markers as Potential Stress Descriptors for Pediatric Dental Patients: A Literature Review. Children (Basel) 2025, 14, 12(4):500. [Google Scholar] [CrossRef]
- Alavi, SE; Sharma, LA; Sharma, A; Ebrahimi Shahmabadi, H. Salivary Biomarkers in Periodontal Disease: Revolutionizing Early Detection and Precision Dentistry. Mol Diagn Ther. Epub. 2025, 29(6), 721–740. [Google Scholar] [CrossRef]
- Carter, MM; Demis, D; Perelman, D; St Onge, M; Petlura, C; Cunanan, K; Mathi, K; Maecker, HT; Chow, JM; Robinson, JL; Sabag-Daigle, A; Sonnenburg, ED; Buck, RH; Gardner, CD; Sonnenburg, JL. A human milk oligosaccharide alters the microbiome, circulating hormones, and metabolites in a randomized controlled trial of older adults. Cell Rep Med. Epub. 2025, 19;6(8), 102256. [Google Scholar] [CrossRef]
- Steffin, D; Ghatwai, N; Montalbano, A; Rathi, P; Courtney, AN; Arnett, AB; Fleurence, J; Sweidan, R; Wang, T; Zhang, H; Masand, P; Maris, JM; Martinez, D; Pogoriler, J; Varadarajan, N; Thakkar, SG; Lyon, D; Lapteva, N; Zhuyong, M; Patel, K; Lopez-Terrada, D; Ramos, CA; Lulla, P; Armaghany, T; Grilley, BJ; Gottschalk, S; Dotti, G; Metelitsa, LS; Heslop, HE; Brenner, MK; Sumazin, P; Heczey, A. Interleukin-15-armoured GPC3 CAR T cells for patients with solid cancers. Nature 2025, 637(8047), 940–946. [Google Scholar] [CrossRef]
- Pardiñas López, S; García-Caro, ME; Vallejo, JA; Aja-Macaya, P; Conde-Pérez, K; Nión-Cabeza, P; Khouly, I; Bou, G; Cendal, AIR; Díaz-Prado, S; Poza, M. Anti-inflammatory and antimicrobial efficacy of coconut oil for periodontal pathogens: a triple-blind randomized clinical trial. Clin Oral Investig. 2025, 14;29(4), 182. [Google Scholar] [CrossRef]
- McSorley, HJ; Hodge, SH. Epithelial cytokines in soil-transmitted helminth infections. Adv Parasitol. Epub. 2025, 129, 115–143. [Google Scholar] [CrossRef]
- Hoelting, TLB; Park, T; Brown, CC. Antigen-presenting cells as arbiters of mucosal tolerance and immunity. Nat Immunol. Epub. 2025, 26(11), 1890–1902. [Google Scholar] [CrossRef]
- Nehaoua, A; Gasmi, A; Noor, S; Benahmed, AG. The Oral Microbiome, Oral Hyperpermeability, and Periodontitis in Metabolic Syndrome. Adv Exp Med Biol. 2026, 1492, 101–120. [Google Scholar] [CrossRef] [PubMed]
- Shacklett, BL. Mucosal immunity in acute HIV: a review of recent work. Curr Opin HIV AIDS Epub. 2025, 1;20(3), 193–198. [Google Scholar] [CrossRef]
- Jung, W; Son, YM. Nanoparticle-Driven Modulation of Mucosal Immunity and Interplay with the Microbiome. J Microbiol Biotechnol. 2025, 12;35, e2404033. [Google Scholar] [CrossRef]
- Branchett, WJ; Saraiva, M; O'Garra, A. Regulation of inflammation by Interleukin-10 in the intestinal and respiratory mucosa. Curr Opin Immunol. 2024, 91, 102495. [Google Scholar] [CrossRef]
- Yu, MY; Liu, XC; Yu, ZL; Jia, J. The Application of Salivary Exosomes in the Diagnosis of Oral Disease. Chin J Dent Res. 2024, 27(4), 291–301. [Google Scholar] [CrossRef] [PubMed]
- LAA, J; Pa, P; Seng, CY; Rhee, JH; Lee, SE. Protein nanocages: A new frontier in mucosal vaccine delivery and immune activation. Hum Vaccin Immunother. Epub. 2025, 21(1), 2492906. [Google Scholar] [CrossRef]
- Bordoni, D; Fazio, A. Crosstalk between T cell gene regulation and intestinal epithelial cells: Insights into mucosal immunity. Adv Genet. Epub. 2025, 114, 23–65. [Google Scholar] [CrossRef]
- Letz, P; Huber, S; Velasquez, LN. Crosstalk between the microbiota and intestinal dendritic cells in IBD. Semin Immunopathol. 2025, 30;47(1), 37. [Google Scholar] [CrossRef]
- Jomova, K; Alomar, SY; Valko, R; Liska, J; Nepovimova, E; Kuca, K; Valko, M. Flavonoids and their role in oxidative stress, inflammation, and human diseases. Chem Biol Interact. 2025, 25;413, 111489. [Google Scholar] [CrossRef]
- Wang, L; Wei, C; Jing, J; Shao, M; Wang, Z; Wen, B; Lu, M; Jia, Z; Zhang, Y. The Effects of Polyphenols on Doxorubicin-Induced Nephrotoxicity by Modulating Inflammatory Cytokines, Apoptosis, Oxidative Stress, and Oxidative DNA Damage. Phytother Res. 2025, 39(5), 2147–2164. [Google Scholar] [CrossRef]
- Luo, J; Li, L; Shi, W; Xu, K; Shen, Y; Dai, B. Oxidative stress and inflammation: roles in osteoporosis. Front Immunol 2025, 16, 1611932. [Google Scholar] [CrossRef]
- Shao, R; Chen, R; Zheng, Q; Yao, M; Li, K; Cao, Y; Jiang, L. Oxidative stress disrupts vascular microenvironmental homeostasis affecting the development of atherosclerosis. Cell Biol Int. 2024, 48(12), 1781–1801. [Google Scholar] [CrossRef] [PubMed]
- Wang, M; Xiao, Y; Miao, J; Zhang, X; Liu, M; Zhu, L; Liu, H; Shen, X; Wang, J; Xie, B; Wang, D. Oxidative Stress and Inflammation: Drivers of Tumorigenesis and Therapeutic Opportunities. Antioxidants (Basel). 2025, 15;14(6), 735. [Google Scholar] [CrossRef]
- Tomaziu-Todosia Anton, E; Anton, GI; Scripcariu, IS; Dumitrașcu, I; Scripcariu, DV; Balmus, IM; Ionescu, C; Visternicu, M; Socolov, DG. Oxidative Stress, Inflammation, and Antioxidant Strategies in Cervical Cancer-A Narrative Review. Int J Mol Sci. 2025, 21;26(10), 4961. [Google Scholar] [CrossRef]
- Potiris, A; Moustakli, E; Trismpioti, E; Drakaki, E; Mavrogianni, D; Matsas, A; Zikopoulos, A; Sfakianakis, A; Tsakiridis, I; Dagklis, T; Zachariou, A; Christopoulos, P; Domali, E; Drakakis, P; Stavros, S. From Inflammation to Infertility: How Oxidative Stress and Infections Disrupt Male Reproductive Health. Metabolites. 2025, 11;15(4), 267. [Google Scholar] [CrossRef]
- Teixeira, AL; de Miranda, AS; Venna, VR; Himali, JJ; Bauer, ME. Understanding late-life depression: focus on inflammation. Curr Opin Psychiatry 2025, 1;38(5), 376–382. [Google Scholar] [CrossRef]
- Johnco, CJ; Matovic, D; Wuthrich, VM. Anxiety Disorders in Later Life. Psychiatr Clin North Am. Epub. 2024, 47(4), 741–752. [Google Scholar] [CrossRef]
- Aravapally, PSN; Chandrasekar, N; Verma, A; Shah, RP. Strategic approaches to assess and quantify the oxidative stress biomarkers in complex biological systems. Bioanalysis Epub. 2025, 17(8), 561–574. [Google Scholar] [CrossRef] [PubMed]
- Hsu, YT; Lee, HL; Wen, B; Daubert, D; Darveau, R. Gingival crevicular fluid during experimental gingivitis: A review of immune and tissue regulation. J Periodontol. 2025, 96(10), 1099–1112. [Google Scholar] [CrossRef]
- Μangoulia, P.; Kanellopoulou, A.; Manta, G.; Chrysochoou, G.; Dimitriou, E.; Kalogerakou, T.; Antoniadou, M. Exploring the Levels of Stress, Anxiety, Depression, Resilience, Hope, and Spiritual Well-Being Among Greek Dentistry and Nursing Students in Response to Academic Responsibilities Two Years After the COVID-19 Pandemic. Healthcare 2025, 13, 54. [Google Scholar] [CrossRef] [PubMed]
- Antoniadou, M; Mangoulia, P; Myrianthefs, P. Quality of Life and Wellbeing Parameters of Academic Dental and Nursing Personnel vs. Quality of Services. Healthcare (Basel) 2023, 21;11(20), 2792. [Google Scholar] [CrossRef]
- Mahdavi, N.; Shafiee Motlagh, M.; Ranjbar, A.; Ghaffari, F.; Faridan, M.; Tajik, L.; Mokhayeri, Y.; Heidarimoghadam, R. Salivary biomarkers as indicators of occupational fatigue. WORK: A Journal of Prevention, Assessment & Rehabilitation 2025, 80(4), 1743–1753. [Google Scholar] [CrossRef]
- García, HC; Orona, VU; Méndez, LF; Coronado, AA; Garza, MAG. Diet and nutrition key factors for oral microbiota composition: a systematic review. Food Nutr Res. 2025, 24, 69. [Google Scholar] [CrossRef] [PubMed]
- Curca, F.R.; Luchian, I.; Bida, F.C.; Virvescu, D.I.; Rotundu, G.; Butnaru, O.M.; Balan, G.; Surlari, Z.; Georgescu, A.; Pasarin, L.; et al. From Diet to Oral and Periodontal Health: Exploring the Crucial Role of Nutrition-A Narrative Review. Nutrients 2026, 18, 168. [Google Scholar] [CrossRef]
- Liu, J.; Zhang, Y.; Li, X. Stratified dietary inflammatory potential identifies oral and gut microbiota differences associated with cognitive function in older adults. Sci Rep 2025, 15, 18988. [Google Scholar] [CrossRef]
- Nireeksha; Maniangat Luke, A; Kumari, N S; Hegde, MN; Hegde, NN. Metabolic interplay of SCFA's in the gut and oral microbiome: a link to health and disease. Front Oral Health 2025, 25;6, 1646382. [Google Scholar] [CrossRef]
- Parveen, S.; Alqahtani, A.S.; Aljabri, M.Y.; Dawood, T.; Khan, S.S.; Gupta, B. Exploring the interplay: Oral–gut microbiome connection and the impact of diet and nutrition. Eur. J. Gen. Dent. 2024, 13, 165–176. [Google Scholar] [CrossRef]
- Mao, J.-S.; Cui, H.-Y.; Zhou, X.-Z.; Zhang, S.-W. Recent Progress in Exploring Dietary Nutrition and Dietary Patterns in Periodontitis with a Focus on SCFAs. Nutrients 2025, 17, 3150. [Google Scholar] [CrossRef]
- Santonocito, S; Polizzi, A; Isola, G. The Impact of Diet and Nutrition on the Oral Microbiome. Adv Exp Med Biol. 2025, 1472, 53–69. [Google Scholar] [CrossRef]
- Antoniadou, M.; Varzakas, T. Diet and Oral Health Coaching Methods and Models for the Independent Elderly. Appl. Sci. 2020, 10, 4021. [Google Scholar] [CrossRef]
- Antoniadou, M.; Varzakas, T. New Insights in Oral Health and Diets. Appl. Sci. 2021, 11, 11397. [Google Scholar] [CrossRef]
- Amargianitakis, M.; Antoniadou, M.; Rahiotis, C.; Varzakas, T. Probiotics, Prebiotics, Synbiotics and Dental Caries. New Perspectives, Suggestions, and Patient Coaching Approach for a Cavity-Free Mouth. Appl. Sci. 2021, 11, 5472. [Google Scholar] [CrossRef]
- Bezirtzoglou, E.; Stavropoulou, E.; Kantartzi, K.; Tsigalou, C.; Voidarou, C.; Mitropoulou, G.; Prapa, I.; Santarmaki, V.; Kompoura, V.; Yanni, E.A.; Antoniadou, M.; Varzakas, T.; Kourkoutas, Y. Maintaining Digestive Health in Diabetes: The Role of the Gut Microbiome and the Challenge of Functional Foods. Microorganisms 2021, 9, 516. [Google Scholar] [CrossRef]
- Antoniadou, M.; Varzakas, T. Dietary Interventions for Human General and Oral Health and Disease Reduction. Appl. Sci. 2024, 14, 5095. [Google Scholar] [CrossRef]
- Brinsley, J.; O’Connor, E.J.; Singh, B.; McKeon, G.; Curtis, R.; Ferguson, T.; Gosse, G.; Willems, I.; Marent, P.J.; Szeto, K.; Firth, J.; Maher, C. Effectiveness of Digital Lifestyle Interventions on Depression, Anxiety, Stress, and Well-Being: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2025, 27, e56975. [Google Scholar] [CrossRef] [PubMed]
- Linardon, J.; Anderson, C.; Messer, M.; McClure, Z.; Liu, C. Looking beyond depression: Meta-analysis of digital interventions for depression on eleven secondary mental health and wellbeing outcomes. Psychiatry Res. 2025, 351, 116657. [Google Scholar] [CrossRef]
- Gholami, S.; Chinonyerem, D.; Cooper, E.J.; Kuwornu, J.P. Understanding the Unmet Needs, Experiences, and Perspectives of COPD Caregivers: A Scoping Review. COPD 2025, 22, 2481260. [Google Scholar] [CrossRef]
- Williamson, V.; Kothari, R.; Bonson, A.; Campbell, G.; Greenberg, N.; Murphy, D.; Lamb, D. Moral injury prevention and intervention. Eur. J. Psychotraumatol. 2025, 16, 2567721. [Google Scholar] [CrossRef] [PubMed]
- Lobo, R; Kumar, SP; Tm, R. Professional Quality of Life Among Mental Health Nurses: A Systematic Review and Meta-Analysis. Int J Ment Health Nurs Epub. 2024, 33(6), 2005–2025. [Google Scholar] [CrossRef]
- Little, A.L. The A52 Breath Method: A Narrative Review of Breathwork for Mental Health and Stress Resilience. Stress Health 2025, 41, e70098. [Google Scholar] [CrossRef] [PubMed]
- Farahani, H. E.; Pourhajibagher, ·M.; Asgharzadeh, S.; Bahador, ·A. Postbiotics: Novel Modulators of Gut Health, Metabolism, and Their Mechanisms of Action. Probiotics and Antimicrobial Proteins. Nutrients 2026, 18(2). [Google Scholar] [CrossRef]
- Christensen, L; Roager, HM; Astrup, A; Hjorth, MF. Microbial enterotypes in personalized nutrition and obesity management. Am J Clin Nutr 2018, 108(4), 645–651. [Google Scholar] [CrossRef]
- Song, EJ; Han, K; Lim, TJ; Lim, S; Chung, MJ; Nam, MH; Kim, H; Nam, YD. Effect of probiotics on obesity-related markers per enterotype: a double-blind, placebo-controlled, randomized clinical trial. EPMA J. 2020, 11(1), 31–51. [Google Scholar] [CrossRef]
- Kumar, A; Green, KM; Rawat, M. A Comprehensive Overview of Postbiotics with a Special Focus on Discovery Techniques and Clinical Applications. Foods 2024, 13(18), 2937. [Google Scholar] [CrossRef]
- Zou, J; Chassaing, B; Singh, V; Pellizzon, M; Ricci, M; Fythe, MD; Kumar, MV; Gewirtz, AT. Fiber-Mediated Nourishment of Gut Microbiota Protects against Diet-Induced Obesity by Restoring IL-22-Mediated Colonic Health. Cell Host Microbe 2018, 23(1), 41–53.e4. [Google Scholar] [CrossRef]
- Aguilar-Toalá, J.E.; Garcia-Varela, R.; Garcia, H.S.; Mata-Haro, V.; González-Córdova, A.F.; Vallejo-Cordoba, B.; Hernández-Mendoza, A. Postbiotics: An Evolving Term within the Functional Foods Field. Trends Food Sci. Technol. 2018, 75, 105–114. [Google Scholar] [CrossRef]
- Compare, D; Rocco, A; Coccoli, P; Angrisani, D; Sgamato, C; Iovine, B; Salvatore, U; Nardone, G. Lactobacillus casei DG and its postbiotic reduce the inflammatory mucosal response: an ex-vivo organ culture model of post-infectious irritable bowel syndrome. BMC Gastroenterol 2017, 17(1), 53. [Google Scholar] [CrossRef]
- Kareem, KY; Hooi Ling, F; Teck Chwen, L; May Foong, O; Anjas Asmara, S. Inhibitory activity of postbiotic produced by strains of Lactobacillus plantarum using reconstituted media supplemented with inulin. Gut Pathog 2014, 6, 23. [Google Scholar] [CrossRef]
- Teame, T; Wang, A; Xie, M; Zhang, Z; Yang, Y; Ding, Q; Gao, C; Olsen, RE; Ran, C; Zhou, Z. Paraprobiotics and Postbiotics of Probiotic Lactobacilli, Their Positive Effects on the Host and Action Mechanisms: A Review. Front Nutr. 2020, 7, 570344. [Google Scholar] [CrossRef]
- Gibson, GR; Hutkins, R; Sanders, ME; Prescott, SL; Reimer, RA; Salminen, SJ; Scott, K; Stanton, C; Swanson, KS; Cani, PD; Verbeke, K; Reid, G. Expert consensus document: The International Scientific Association for Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of prebiotics. Nat Rev Gastroenterol Hepatol. 2017, 14(8), 491–502. [Google Scholar] [CrossRef]
- Kundi, ZM; Lee, JC; Pihlajamäki, J; Chan, CB; Leung, KS; So, SSY; Nordlund, E; Kolehmainen, M; El-Nezami, H. Dietary Fiber from Oat and Rye Brans Ameliorate Western Diet-Induced Body Weight Gain and Hepatic Inflammation by the Modulation of Short-Chain Fatty Acids, Bile Acids, and Tryptophan Metabolism. Mol Nutr Food Res Epub. 2021, 65(1), e1900580. [Google Scholar] [CrossRef]
- Barrea, L; Verde, L; Auriemma, RS; Vetrani, C; Cataldi, M; Frias-Toral, E; Pugliese, G; Camajani, E; Savastano, S; Colao, A; Muscogiuri, G. Probiotics and Prebiotics: Any Role in Menopause-Related Diseases? Curr Nutr Rep. Epub. 2023, 12(1), 83–97. [Google Scholar] [CrossRef]
- Krumbeck, JA; Walter, J; Hutkins, RW. Synbiotics for improved human health: recent developments, challenges, and opportunities. Annu Rev Food Sci Technol 2018, 9(1), 451–479. [Google Scholar] [CrossRef] [PubMed]
- Ma, L; Tu, H; Chen, T. Postbiotics in human health: a narrative review. Nutrients 2023, 15(2), 291. [Google Scholar] [CrossRef]
- Oerlemans, M.M.P.; Akkerman, R.; Ferrari, M.; Walvoort, M.T.C.; de Vos, P. Benefits of bacteria-derived exopolysaccharides on gastrointestinal microbiota, immunity and health. Adv. Exp. Med. Biol. 2021, 1287, 145–159. [Google Scholar] [CrossRef]
- Jurášková, D.; Ribeiro, S.C.; Silva, C.C.G.; Teixeira, J.A.; Rodrigues, L.R. Dextran-type exopolysaccharides produced by lactic acid bacteria: Structure, properties and applications. Foods 2022, 11, 2216. [Google Scholar] [CrossRef]
- Jurášková, D.; Teixeira, J.A.; Rodrigues, L.R. Health-promoting effects of dextran-type exopolysaccharides: From structure to function. Foods 2025, 14, 2635. [Google Scholar] [CrossRef]
- Song, Z.; Wang, X.; Zhang, L.; Wu, H.; Yang, Y. Structural diversity and biological functions of microbial exopolysaccharides: A comprehensive review. Int. J. Biol. Macromol. 2023, 237, 124132. [Google Scholar] [CrossRef]
- Tang, Y.; Li, X.; Chen, Z.; Liu, L.; Wu, J. Classification, biosynthesis and health-promoting effects of microbial exopolysaccharides. Carbohydr. Polym. 2023, 304, 120494. [Google Scholar]
- Yang, S.; Wang, J.; Zhang, X.; Liu, Y.; Li, H. Exopolysaccharides from lactic acid bacteria: Structure, epithelial adhesion and immunomodulatory activity. Food Sci. Hum. Wellness 2023, 12, 925–936. [Google Scholar]
- Luo, M.; Zhang, Y.; Chen, L.; Wang, J.; Li, Q. Immunomodulatory effects of Lactobacillus-derived exopolysaccharides on mucosal immune responses. Front. Nutr. 2024, 11, 1426358. [Google Scholar] [CrossRef]
- de Oliveira, R.S.; Gänzle, M.G.; Salminen, S.; Ouwehand, A.C. Bifidobacterium-derived exopolysaccharides modulate adaptive immunity through microbiota-dependent mechanisms. Cell Rep. 2025, 42, 112994. [Google Scholar]
- Wu, J.; Zhang, Y.; Ye, L.; Wang, C.; Li, X. Anticancer activities of microbial exopolysaccharides: Mechanisms and applications. Int. J. Biol. Macromol. 2021, 181, 80–92. [Google Scholar] [CrossRef]
- Ikram, M.; Ullah, M.; Khan, A.; Kim, M.O. Exopolysaccharides as emerging anticancer agents: Molecular mechanisms and therapeutic potential. Biomed. Pharmacother. 2024, 170, 115921. [Google Scholar] [CrossRef]
- Oleksy, M.; Klewicka, E. Exopolysaccharides produced by Lactobacillus strains: Biosynthesis and health-promoting properties. Carbohydr. Polym. 2018, 181, 575–587. [Google Scholar] [CrossRef]
- Hanus, M; Parada-Venegas, D; Landskron, G; Wielandt, AM; Hurtado, C; Alvarez, K; Hermoso, MA; López-Köstner, F; De la Fuente, M. Immune System, Microbiota, and Microbial Metabolites: The Unresolved Triad in Colorectal Cancer Microenvironment. Front Immunol. 2021, 26;12, 612826. [Google Scholar] [CrossRef]
- Gill, PA; van Zelm, MC; Muir, JG; Gibson, PR. Review article: short chain fatty acids as potential therapeutic agents in human gastrointestinal and inflammatory disorders. Aliment Pharmacol Ther. 2018, 48(1), 15–34. [Google Scholar] [CrossRef] [PubMed]
- Parada Venegas, D; De la Fuente, MK; Landskron, G; González, MJ; Quera, R; Dijkstra, G; Harmsen, HJM; Faber, KN; Hermoso, MA. Short Chain Fatty Acids (SCFAs)-Mediated Gut Epithelial and Immune Regulation and Its Relevance for Inflammatory Bowel Diseases. Front Immunol Erratum in: Front Immunol. 2019 Jun 28;10:1486. doi: 10.3389/fimmu.2019.01486.. 2019, 10, 277. [Google Scholar] [CrossRef]
- Asefa, Z.; Belay, A.; Welelaw, E.; Haile, M. Postbiotics and Their Biotherapeutic Potential for Chronic Disease and Their Future Perspective: A Review. Front. Microbiomes 2025, 4, 1489339. [Google Scholar] [CrossRef]
- Simons, A; Alhanout, K; Duval, RE. Bacteriocins, Antimicrobial Peptides from Bacterial Origin: Overview of Their Biology and Their Impact against Multidrug-Resistant Bacteria. Microorganisms. 2020, 8(5), 639. [Google Scholar] [CrossRef]
- Soltani, S; Hammami, R; Cotter, PD; Rebuffat, S; Said, LB; Gaudreau, H; Bédard, F; Biron, E; Drider, D; Fliss, I. Bacteriocins as a new generation of antimicrobials: toxicity aspects and regulations. FEMS Microbiol Rev. 2021, 8;45(1), fuaa039. [Google Scholar] [CrossRef]
- Huang, F; Teng, K; Liu, Y; Cao, Y; Wang, T; Ma, C; Zhang, J; Zhong, J. Bacteriocins: Potential for Human Health. Oxid Med Cell Longev. 2021, 10;2021, 5518825. [Google Scholar] [CrossRef]
- Darbandi, A; Asadi, A; Mahdizade Ari, M; Ohadi, E; Talebi, M; Halaj Zadeh, M; Darb Emamie, A; Ghanavati, R; Kakanj, M. Bacteriocins: Properties and potential use as antimicrobials. J Clin Lab Anal. 2022, 36(1), e24093. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H; Wu, L; Yan, G; Chen, Y; Zhou, M; Wu, Y; Li, Y. Inflammation and tumor progression: signaling pathways and targeted intervention. Signal Transduct Target Ther. 2021, 12;6(1), 263. [Google Scholar] [CrossRef]
- Chondrou, P.; Karapetsas, A.; Kiousi, D.E.; Vasileiadis, S.; Ypsilantis, P.; Botaitis, S.; Alexopoulos, A.; Plessas, S.; Bezirtzoglou, E.; Galanis, A. Assessment of the Immunomodulatory Properties of the Probiotic Strain Lactobacillus paracasei K5 In Vitro and In Vivo. Microorganisms 2020, 8, 709. [Google Scholar] [CrossRef]
- Balaguer, F; Enrique, M; Llopis, S; Barrena, M; Navarro, V; Álvarez, B; Chenoll, E; Ramón, D; Tortajada, M; Martorell, P. Lipoteichoic acid from Bifidobacterium animalis subsp. lactis BPL1: a novel postbiotic that reduces fat deposition via IGF-1 pathway. Microb Biotechnol. 2022, 15(3), 805–816. [Google Scholar] [CrossRef]
- Markowiak-Kopeć, P; Śliżewska, K. The Effect of Probiotics on the Production of Short-Chain Fatty Acids by Human Intestinal Microbiome. Nutrients 2020, 16;12(4), 1107. [Google Scholar] [CrossRef]
- Gurunathan, S; Thangaraj, P; Kim, JH. Postbiotics: Functional Food Materials and Therapeutic Agents for Cancer, Diabetes, and Inflammatory Diseases. Foods. 2023, 26;13(1), 89. [Google Scholar] [CrossRef]
- Robinson, L.A.; Lennon, S.; Pegel, A.R.; Strickland, K.P.; Feeley, C.A.; Watts, S.O.; Van Der Pol, J.; Roberts, M.D.; Greene, M.W.; Frugé, A.D. A Randomized Controlled Crossover Lifestyle Intervention to Improve Metabolic and Mental Health in Female Healthcare Night-Shift Workers. Nutrients 2025, 17, 3342. [Google Scholar] [CrossRef]
- Varzakas, T; Antoniadou, M. A Holistic Approach for Ethics and Sustainability in the Food Chain: The Gateway to Oral and Systemic Health. Foods 2024, 17;13(8), 1224. [Google Scholar] [CrossRef]
- Fekete, M; Lehoczki, A; Kryczyk-Poprawa, A; Zábó, V; Varga, JT; Bálint, M; Fazekas-Pongor, V; Csípő, T; Rząsa-Duran, E; Varga, P. Functional Foods in Modern Nutrition Science: Mechanisms, Evidence, and Public Health Implications. Nutrients. 2025, 28;17(13), 2153. [Google Scholar] [CrossRef]
- Ziaei, H; Rezaei, N. Introduction to Oral Immunity. Adv Exp Med Biol. 2026, 1492, 3–21. [Google Scholar] [CrossRef]
- Kowal, M; Sorokowski, P; David, O; Iuga, IA; Renwick, S; Sorokowska, A. Microbiome and well-being: a meta-analysis. NPJ Biofilms Microbiomes 2025, 29, 11(1):201. [Google Scholar] [CrossRef]
- Deng, Q; Wong, HM; Peng, S. Alterations in salivary profile in individuals with dental caries and/or obesity: A systematic review and meta-analysis. J Dent. 2024, 151, 105451. [Google Scholar] [CrossRef]
- Zhang, H; Xia, Z; Yu, S; Shi, H; Meng, Y; Dator, WL. Interventions for Compassion Fatigue, Burnout, and Secondary Traumatic Stress in Nurses: A Systematic Review and Network Meta-Analysis. Nurs Health Sci. 2025, 27(1), e70042. [Google Scholar] [CrossRef]
- Ross, PP; Okafor, LC; Rumps, MV; Mulcahey, MK. Promoting Wellness Among Orthopaedic Surgeons. JB JS Open Access. 2025, 7;10(1), e24.00090. [Google Scholar] [CrossRef]
- Chireh, B; Essien, SK; Swerhun, K; D'Arcy, C; Acharibasam, JW. Workplace stressors and mental health outcomes among personal support workers: A systematic review. Int J Nurs Stud. 2025, 168, 105093. [Google Scholar] [CrossRef]
- Rajasekaran, JJ; Krishnamurthy, HK; Bosco, J; Jayaraman, V; Krishna, K; Wang, T; Bei, K. Oral Microbiome: A Review of Its Impact on Oral and Systemic Health. Microorganisms. 2024, 29;12(9), 1797. [Google Scholar] [CrossRef]
Figure 2.
Occupational stress activates systemic stress biology, which interacts bidirectionally with oral salivary, epithelial-immune, and microbiome mechanisms. Disruption of oral cellular homeostasis may reflect and modulate occupational wellbeing, positioning the oral cavity as a potential interface for early detection and preventive intervention in healthcare professionals.
Figure 2.
Occupational stress activates systemic stress biology, which interacts bidirectionally with oral salivary, epithelial-immune, and microbiome mechanisms. Disruption of oral cellular homeostasis may reflect and modulate occupational wellbeing, positioning the oral cavity as a potential interface for early detection and preventive intervention in healthcare professionals.
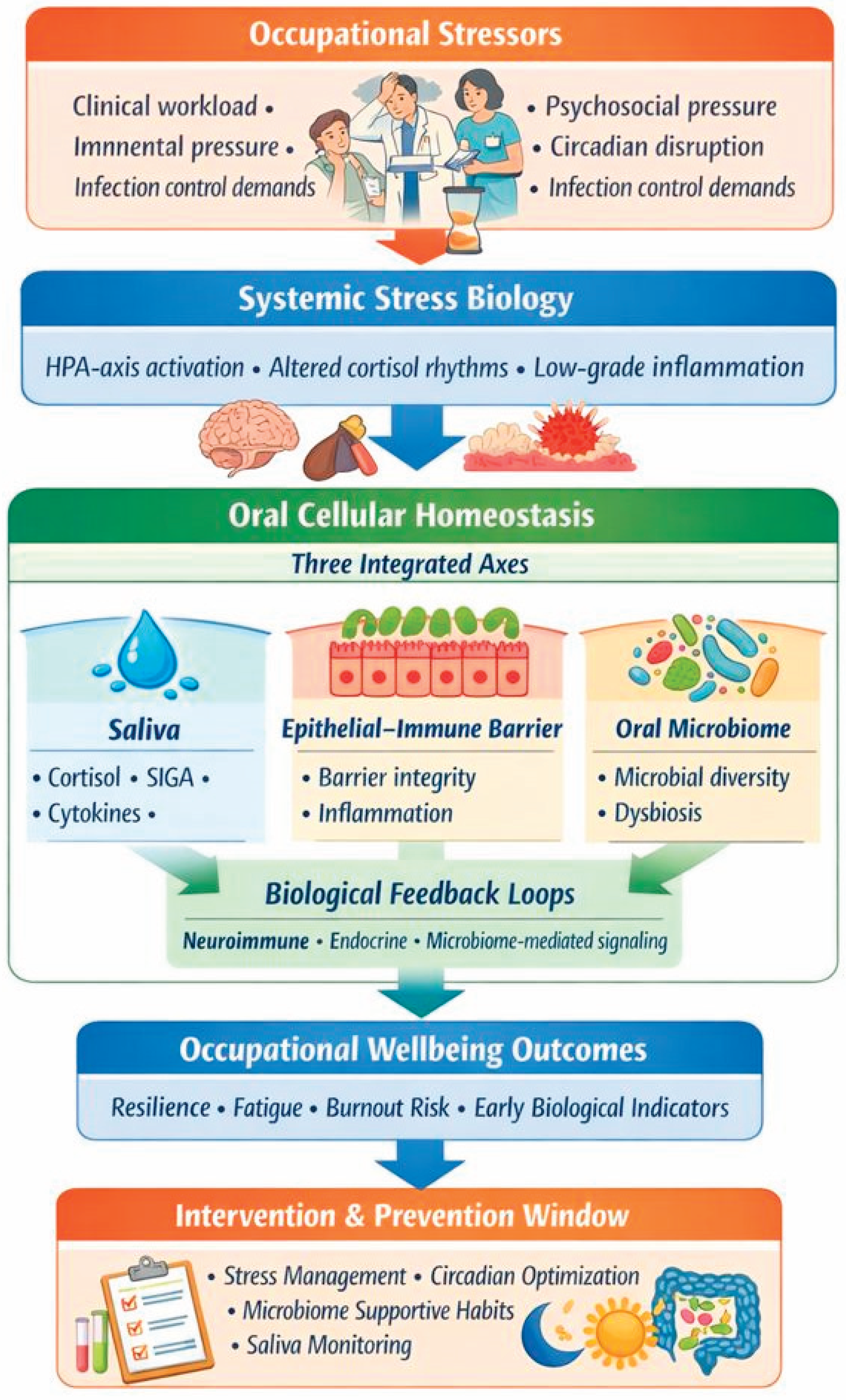
Figure 3.
Integrated model of oral mucosal immunity as a neuroimmune barrier system.
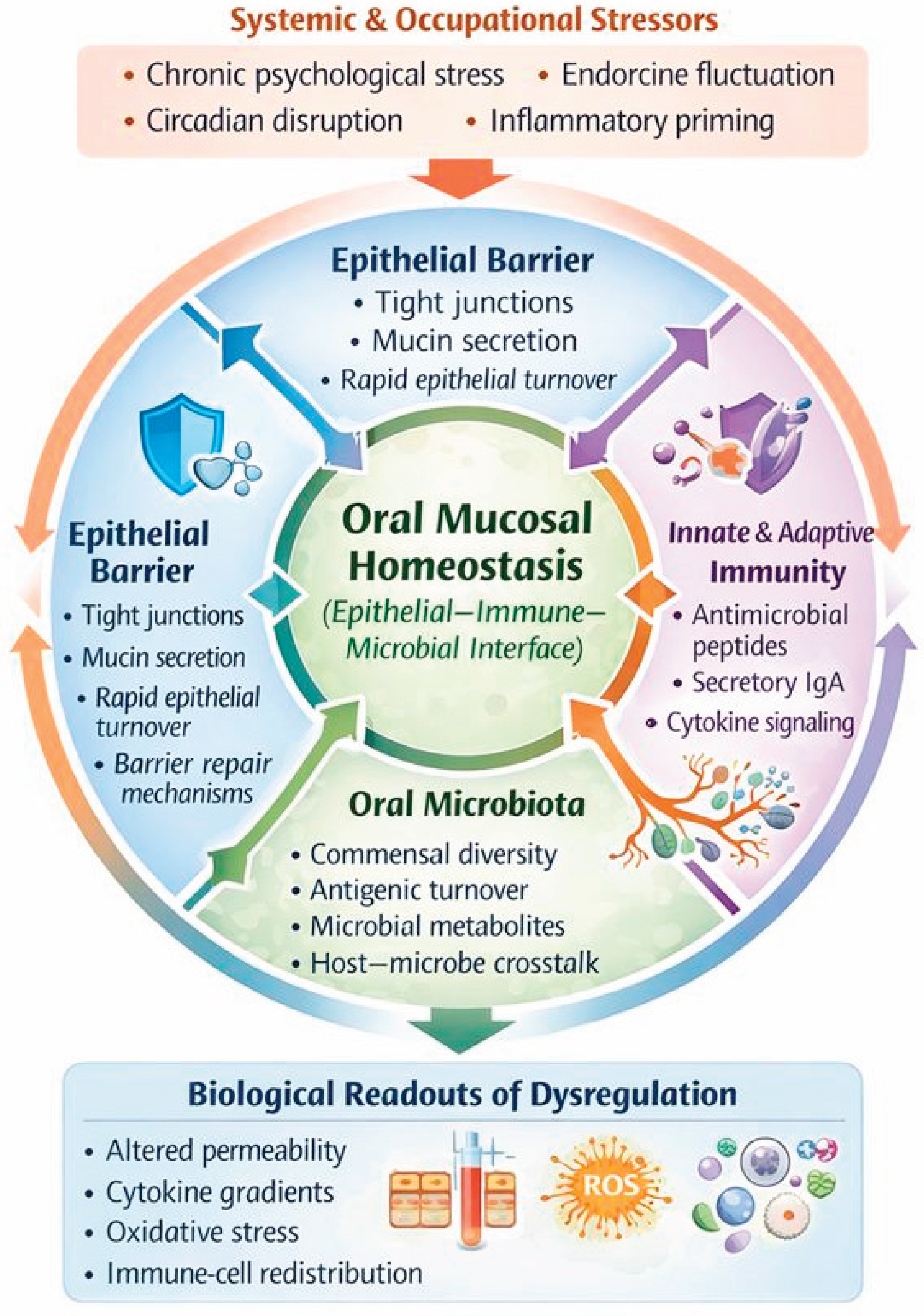
Figure 4.
Saliva as an integrative biosensor of systemic and local physiological activity.
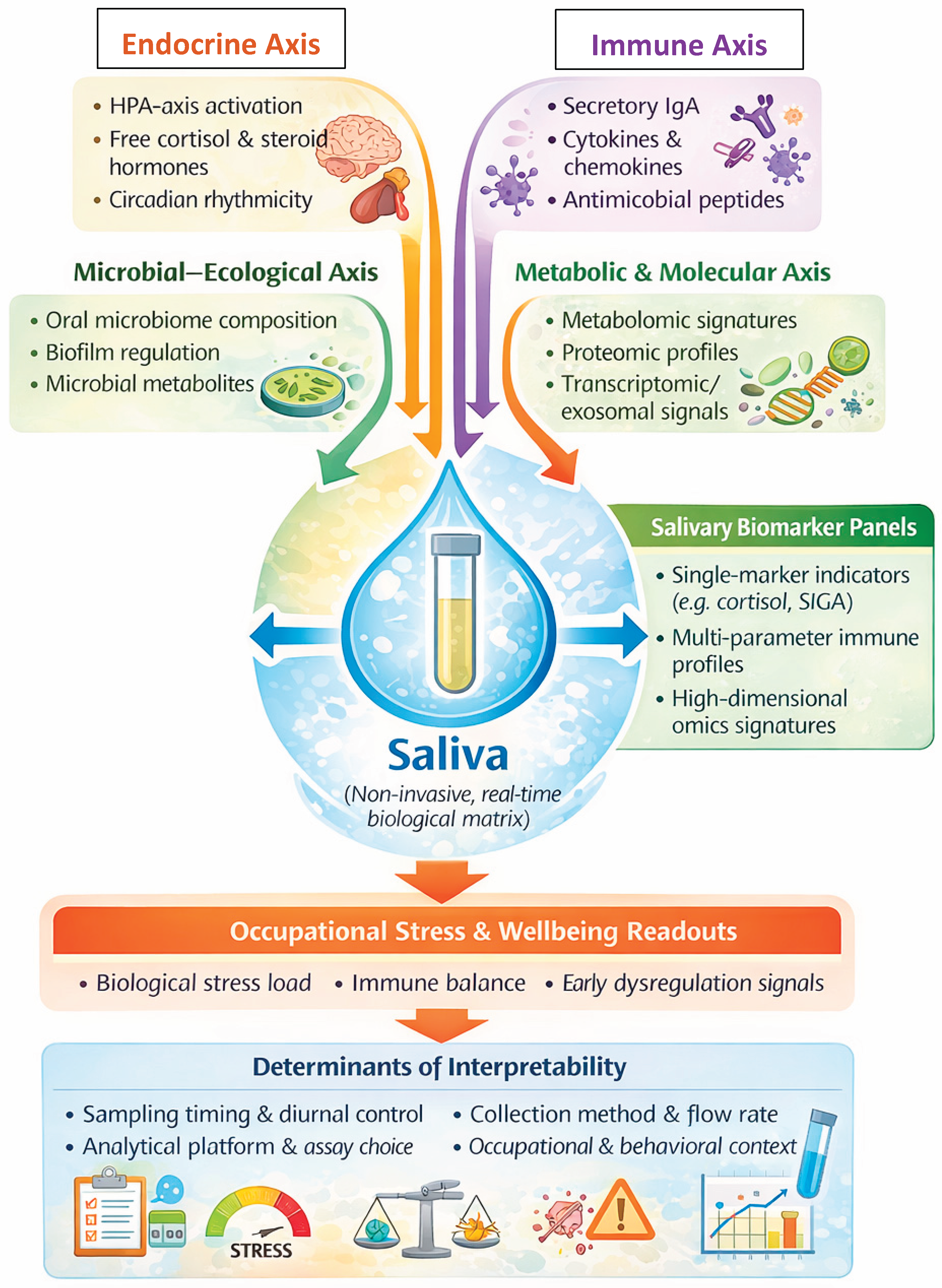
Figure 5.
Mechanisms of action of postbiotics and probiotics on mucosal and systemic homeostasis.
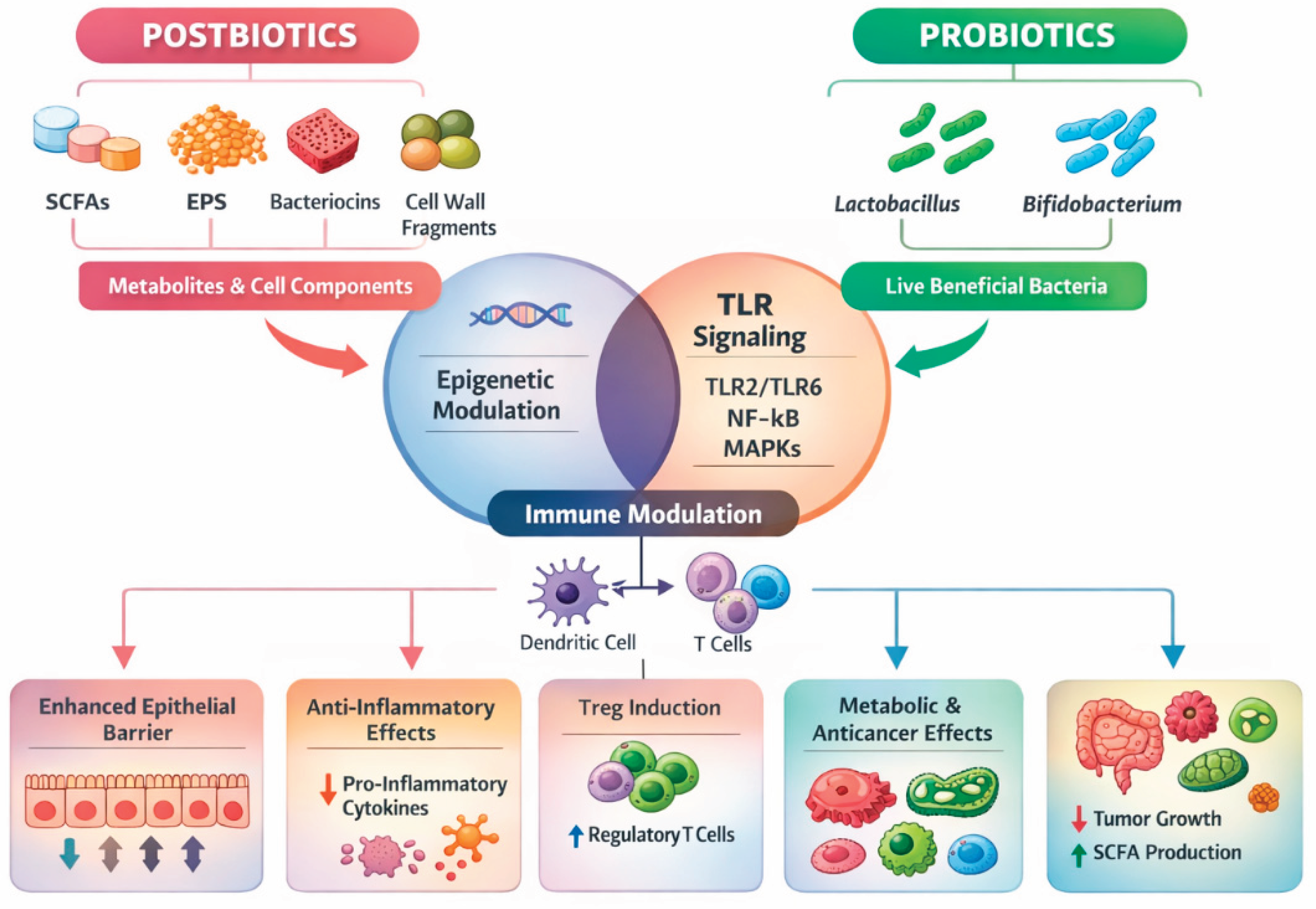
Figure 6.
Conceptual pathway linking occupational stress to oral cellular homeostasis and professional wellbeing.
Figure 6.
Conceptual pathway linking occupational stress to oral cellular homeostasis and professional wellbeing.
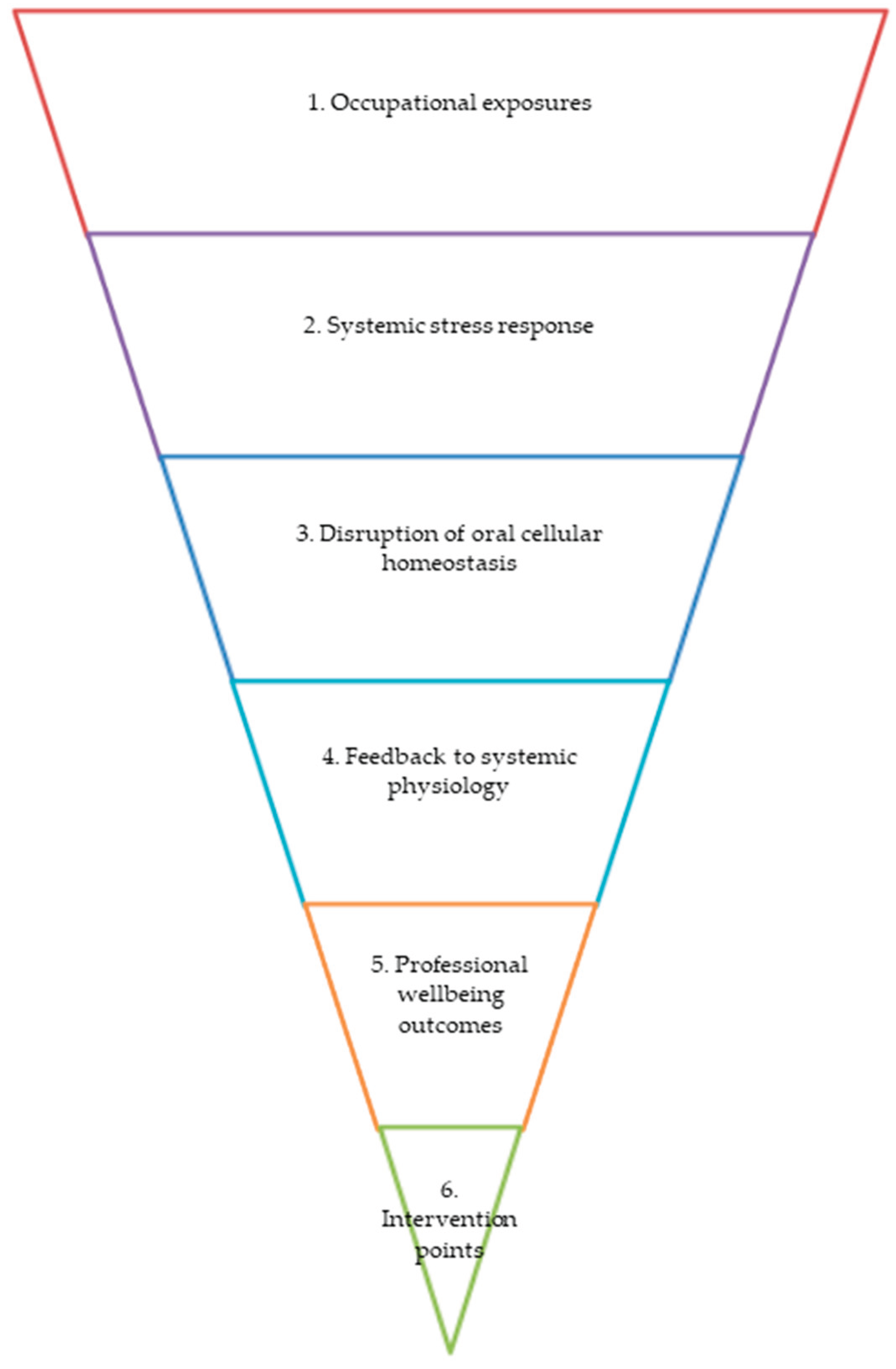

Table 1.
Key articles grouped by thematic domains relevant to oral cellular homeostasis and occupational wellbeing.
Table 1.
Key articles grouped by thematic domains relevant to oral cellular homeostasis and occupational wellbeing.
| A. Oral mucosal immunity & epithelial barrier biology | ||||||||
|---|---|---|---|---|---|---|---|---|
| Thematic domain | Authors & year | Study type / methods | Key findings / relevance | |||||
| Oral mucosal barrier mechanisms | [1] Lin et al., 2021 | Mechanistic immunology review | Microbe-epithelial-immune crosstalk; foundation of oral homeostasis. | |||||
| Physical & immune barriers of oral mucosa | [3] Şenel, 2021 | Comprehensive immunity review | Defines physical, microbial, immune layers of the oral barrier. | |||||
| Oral vs gastrointestinal immune niches | [5] Suárez et al., 2021 | Comparative immunology review | Highlights uniqueness of oral immune niche vs gut. | |||||
| γδ T cells in oral diseases | [6] Wei et al., 2024 | Immunology review | Shows γδ T cell roles in epithelial surveillance under stress. | |||||
| Sensory-neuroimmune interactions | [7] Wang et al., 2024 | Neuroimmune review | Demonstrates endocrine-neural modulation of mucosal immunity. | |||||
| Oral innate immunity & epithelial cells | [34] Nittayananta, 2026 | Immunology chapter | Maps epithelial innate mechanisms; core for homeostasis definition. | |||||
| Oral mucosal barrier & systemic health | [39] Xin & Lei, 2026 | Narrative review; mechanistic synthesis | Describes the oral mucosal barrier as a dynamic immune-epithelial interface regulating microbial balance, inflammation, and systemic signaling. | |||||
| B. Oral microbiome composition, stability & systemic links | ||||||||
| Lifespan mucosal-microbial interactions | [7] Iliev et al., 2025 | Conceptual immunology review | Microbiota shapes mucosal immunity across lifespan. | |||||
| Periodontitis microbiome biomarkers | [8] Radu et al., 2025 | Narrative review | Links microbiome & salivary biomarkers to inflammation. | |||||
| Hormonal effects on oral microbiome | [11] Rus et al., 2025 | Clinical/experimental review | Shows endocrine modulation of oral microbiome; relates to stress. | |||||
| Microbiome & wound healing | [12] Simon-Soro et al., 2025 | Human biomarker study | Microbial shifts correlate with inflammatory wound healing responses. | |||||
| Social capital-oral health-aging | [10] Liang & Gomaa, 2023 | Cohort multi-omics | Oral health, cognition & aging interconnected biologically. | |||||
| Tooth loss & cognitive decline | [9] Galindo-Moreno et al., 2022 | Systematic review | Oral health linked to neurocognitive outcomes. | |||||
| Gut-oral microbiome & periodontitis | [40] Yu et al., 2025 | Meta-analysis of Mendelian randomization studies | Supports a causal role of gut microbiota composition in periodontitis risk, strengthening oral-systemic microbiome links. | |||||
| Microbiome & viral-associated disease | [41] Zhang et al., 2025 | Systematic review & meta-analysis | Demonstrates microbiome alterations in viral infection-associated inflammatory diseases, highlighting immune-microbial interactions. | |||||
| Endodontic infections & microbiome | [42] Liu et al., 2025 | Systematic review & meta-analysis (NGS-based) | Identifies Enterococcus as a persistent endodontic pathogen, emphasizing microbial resilience under inflammatory stress. | |||||
| Prosthodontics & oral microbiome | [43] Madhan Kumar et al., 2025 | Systematic review & meta-analysis | Shows dentures significantly alter oral microbiome composition and inflammatory profiles. | |||||
| Immune signaling & barrier traversal | [44] Kulkarni et al., 2025 | Meta-analysis of RNA-seq data | Identifies interferon-induced genes facilitating barrier crossing, relevant to mucosal immune vulnerability. | |||||
| Nutritional modulation of immunity | [45] Lu et al., 2024 | Randomized intervention study | L-glutamine supplementation enhances mucosal immunity and hormonal balance under physical stress. | |||||
| Mucosal vaccination & immunity | [46] Flitter et al., 2025 | Phase 2 placebo-controlled trial | Oral vaccination induces mucosal immunity and reduces viral shedding, validating oral immune responsiveness. | |||||
| Oral mucosa & respiratory immunity | [47] Wang et al., 2024 | Narrative review | Highlights oral microecological control of virus-related inflammatory responses. | |||||
| Antiviral immunity in oral cavity | [48] Hickman & Moutsopoulos, 2025 | Narrative review | Positions the oral cavity as an active antiviral immune site with systemic relevance. | |||||
| Saliva-microbiome interactions | [49] Heller et al., 2025 | Narrative review | Describes saliva as an active regulator of microbial stability and host defense. | |||||
| Salivary metabolomics | [15] Zhao et al., 2025 | Narrative review | Establishes saliva metabolomics as a non-invasive tool linking oral and systemic disease. | |||||
| Microbial metabolites & immunity | [50] Schütz et al., 2025 | Mechanistic review | Shows microbiome-derived metabolites modulate host immune responses and inflammation. | |||||
| Oral epithelial innate immunity | [34] Nittayananta, 2026 | Narrative review | Details epithelial cells as immune sentinels maintaining oral barrier homeostasis. | |||||
| Saliva & systemic diagnostics | [13] Surdu et al., 2025 | Narrative review | Supports saliva as a diagnostic medium for systemic and inflammatory diseases. | |||||
| Oral immune responses | [14] Matsuoka et al., 2025 | Experimental & narrative synthesis | Describes natural and induced immune mechanisms in saliva and oral tissues. | |||||
| Micronutrients & emotional regulation | [51] Katta et al., 2024 | Randomized controlled trial | Shows orally absorbed micronutrients reduce emotion dysregulation, linking nutrition and neurobiology. | |||||
| Periodontitis & metabolomics | [52] Albahri et al., 2025 | Observational metabolomics study | Links salivary metabolic profiles with chronic periodontal inflammation. | |||||
| Saliva & cancer immunotherapy | [53] Nejat Dehkordi et al., 2025 | Narrative review | Highlights salivary biomarkers as predictors of immunotherapy response. | |||||
| Environment, stress & microbiome | [54] Shibata et al., 2025 | Randomized controlled trial | Demonstrates environmental enrichment alters cortisol levels and microbiome composition. | |||||
| Salivary transcriptomics | [55] Barnes et al., 2025 | Methodological review | Positions saliva transcriptomics as a window into systemic gene regulation. | |||||
| Saliva in precision dosing | [56] Xu et al., 2025 | Methodological review | Validates saliva as a matrix for therapeutic drug monitoring. | |||||
| Salivaomics in cancer | [57] Saravanan et al., 2025 | Narrative review | Integrates proteomic, metabolomic, and transcriptomic saliva data for disease monitoring. | |||||
| Salivary proteome & immunity | [18] Carneiro et al., 2026 | Narrative review | Describes salivary proteins as mediators of immune defense and infection control. | |||||
| Wound healing & microbiome | [58] Santamaria et al., 2025 | Observational study | Links microbiome profiles and inflammatory biomarkers with oral wound healing outcomes. | |||||
| Hormone diagnostics via saliva | [17] Ferrari et al., 2025 | Narrative review | Establishes saliva as a reliable matrix for endocrine and stress hormone assessment. | |||||
| Pediatric stress biomarkers | [59] Main et al., 2025 | Narrative review | Identifies salivary markers as indicators of stress in dental settings. | |||||
| Periodontal biomarkers | [60] Alavi et al., 2025 | Narrative review | Positions salivary biomarkers as tools for early detection and precision dentistry. | |||||
| Salivary diagnostics overview | [16] Albagieh et al., 2025 | Narrative review | Summarizes applications, benefits, and limitations of salivary diagnostics. | |||||
| C. Integrated evidence on oral microbiome, mucosal immunity, saliva, and systemic-stress biology | ||||||||
| Nutritional modulation of microbiome & hormones | [61] Carter et al., 2025 | Randomized controlled trial | Demonstrates that specific dietary oligosaccharides can simultaneously remodel the microbiome, circulating hormones, and metabolic profiles, supporting diet-driven regulation of immune–endocrine homeostasis. | |||||
| Immune amplification therapies | [62] Steffin et al., 2025 | Translational clinical study (CAR-T) | Illustrates how cytokine-enhanced immune signaling can reshape tumor-immune dynamics, highlighting systemic consequences of immune modulation relevant to mucosal immunity frameworks. | |||||
| Anti-inflammatory dietary interventions | [63] Pardiñas López et al., 2025 | Triple-blind randomized clinical trial | Provides clinical evidence that natural dietary agents exert antimicrobial and anti-inflammatory effects against periodontal pathogens, reinforcing nutrition as a modulator of oral inflammation. | |||||
| Epithelial cytokine signaling | [64] McSorley & Hodge, 2025 | Mechanistic parasitology review | Identifies epithelial-derived cytokines as central regulators of mucosal immune balance, relevant to stress- and infection-induced barrier modulation. | |||||
| Antigen presentation & mucosal tolerance | [65] Hoelting et al., 2025 | Mechanistic immunology review | Establishes antigen-presenting cells as key arbiters of tolerance versus inflammation at mucosal surfaces. | |||||
| Metabolic syndrome & oral permeability | [66] Nehaoua et al., 2026 | Narrative review | Links metabolic dysregulation with oral hyperpermeability and microbiome-driven inflammation, supporting oral–systemic disease integration. | |||||
| Viral infection & mucosal immunity | [67] Shacklett, 2025 | Narrative review | Highlights vulnerability and plasticity of mucosal immunity under acute viral stress. | |||||
| Nanotechnology & immune modulation | [68] Jung & Son, 2025 | Experimental/narrative review | Shows how nanoparticle-based strategies modulate mucosal immunity and microbiome interactions. | |||||
| Anti-inflammatory cytokine regulation | [69] Branchett et al., 2024 | Mechanistic immunology review | Positions IL-10 as a central regulator limiting mucosal inflammation across tissues. | |||||
| Salivary cortisol & stress biology | [30] Dong et al., 2024 | Systematic review | Defines methodological standards and limitations for using salivary cortisol as a stress biomarker. | |||||
| Salivary exosomes | [70] Yu et al., 2024 | Narrative review | Identifies salivary exosomes as emerging diagnostic and signaling mediators in oral disease. | |||||
| Vaccine delivery via mucosa | [71] Laa et al., 2025 | Narrative review | Describes protein nanocages as innovative platforms for mucosal immune activation. | |||||
| T cell-epithelial crosstalk | [72] Bordoni & Fazio, 2025 | Mechanistic genetics review | Explains how epithelial-T cell signaling regulates mucosal immune equilibrium. | |||||
| Microbiota-dendritic cell interactions | [73] Letz et al., 2025 | Mechanistic immunopathology review | Demonstrates microbiota-driven shaping of dendritic cell responses in chronic inflammation. | |||||
| Flavonoids & oxidative stress | [74] Jomova et al., 2025 | Mechanistic review | Links dietary flavonoids to redox balance and inflammatory control. | |||||
| Polyphenols & inflammatory injury | [75] Wang L. et al., 2025 | Experimental pharmacology study | Shows polyphenols mitigate inflammation and oxidative damage via cytokine modulation. | |||||
| Oxidative stress & immune dysfunction | [76] Luo et al., 2025 | Mechanistic immunology review | Establishes oxidative stress as a driver of immune-mediated tissue damage. | |||||
| Vascular inflammation | [77] Shao et al., 2024 | Mechanistic cell biology review | Demonstrates oxidative stress–induced microenvironmental disruption in chronic disease. | |||||
| Inflammation & tumorigenesis | [78] Wang M. et al., 2025 | Narrative review | Frames inflammation–oxidative stress axis as a universal oncogenic driver. | |||||
| Oxidative stress in cancer | [79] Tomaziu-Todosia Anton et al., 2025 | Narrative review | Reviews antioxidant strategies targeting inflammatory carcinogenesis. | |||||
| Infection, inflammation & fertility | [80] Potiris et al., 2025 | Narrative review | Highlights systemic consequences of chronic inflammation and oxidative stress. | |||||
| Inflammation & mental health | [81] Teixeira et al., 2025 | Narrative review | Positions inflammation as a biological substrate of late-life depression. | |||||
| Anxiety & aging | [82] Johnco et al., 2024 | Clinical psychiatry review | Connects stress-related disorders with biological aging processes. | |||||
| Oxidative stress biomarkers | [83] Aravapally et al., 2025 | Methodological review | Discusses advanced strategies for quantifying oxidative stress in complex systems. | |||||
| Gingival immune regulation | [84] Hsu et al., 2025 | Narrative review | Describes immune and tissue dynamics in experimental gingivitis. | |||||
| D. Occupational Stress, wellbeing & biomarkers | ||||||||
| Stress, anxiety, depression, resilience & spiritual wellbeing in students | [85] Mangoulia et al., 2025 | Cross-sectional observational study | Reports high psychological burden among dental & nursing students post-pandemic; highlights resilience & hope as protective factors; relevant to occupational wellbeing trajectories. | |||||
| Quality of life & wellbeing in academic dental personnel | [86] Antoniadou, Mangoulia & Myrianthefs, 2023 | Cross-sectional study comparing academic staff & service quality | Demonstrates associations between professional wellbeing, QoL parameters, and perceived quality of academic services; supports link between occupational strain and performance outcomes. | |||||
| Circadian dysregulation & burnout | [22] Ungurianu & Marina, 2025 | Systematic review | Burnout affects circadian biology; linked to cortisol. | |||||
| Immune & mucosal function under stress | [23] Zhang et al., 2025 | Immunology review | Chronic stress disrupts systemic and mucosal immunity. | |||||
| Burnout, depression & suicide in HCWs | [24] Nguyen et al., 2025 | Scoping review | High burden of psychological distress in healthcare. | |||||
| Stress-reduction therapies | [25] Meneses Damasceno et al., 2025 | Integrative review | Interventions improve physiological stress markers. | |||||
| Tele-yoga for HCWs | [26] Naveen et al., 2024 | Randomized controlled trial | Improves cortisol and immune markers. | |||||
| Night-shift worker intervention | [27] Robinson et al., 2025 | Randomized crossover trial | Improves salivary cortisol and metabolic responses. | |||||
| Salivary biomarkers in occupational medicine | [28] Koh & Koh, 2007 | Landmark review | Classic reference establishing saliva as biomarker matrix. | |||||
| Salivary cortisol methodology | [30] Dong et al., 2024 | Systematic methodological review | Timing, diurnal variation, sampling, assay accuracy. | |||||
| Cortisol Awakening Response | [31] Stalder et al., 2025 | Endocrine review | CAR as reliable HPA-axis stress indicator. | |||||
| Environmental richness & cortisol | [32] Shibata et al., 2025 | Randomized trial | Environment modulates cortisol & microbiota. | |||||
| Salivary biomarkers & occupational fatigue | [87] Mahdavi et al., 2025 | Observational study; salivary biomarker assessment | Demonstrates associations between salivary biomarkers and occupational fatigue, supporting saliva as a non-invasive indicator of work-related physiological strain. | |||||
| E. Dietary, nutritional, and food-related modulators of oral cellular homeostasis | ||||||||
| Diet-Oral Microbiota Interaction |
[88] García HC et al., 2025 | Systematic review | Diet is a key determinant of oral microbiota composition; fiber-rich diets support microbial diversity and immune balance, whereas high-sugar patterns promote dysbiosis and inflammation. | |||||
| Nutrition and Oral-Periodontal Health |
[89] Curca FR et al., 2026 | Narrative review | Links nutrition to oral and periodontal health via immune modulation, oxidative stress regulation, and microbiome-mediated effects on epithelial resilience and inflammation. | |||||
| Dietary Inflammatory Potential and Microbiome |
[90] Liu J et al., 2025 | Observational study with microbiome profiling | Higher dietary inflammatory potential is associated with altered oral and gut microbiota and increased systemic inflammation. | |||||
| SCFAs and Microbiome-Host Crosstalk |
[91] Nireeksha et al., 2025 | Narrative mechanistic review | Identifies SCFAs as metabolic mediators linking diet to immune regulation, epithelial energy metabolism, and microbial stability. | |||||
| Oral-Gut Microbiome Axis |
[92] Parveen S et al., 2024 | Narrative review | Examines oral-gut microbiome crosstalk and the role of diet in shaping microbial ecology and immune signaling. | |||||
| Dietary Patterns and Periodontitis | [93] Mao J.-S. et al., 2025 | Narrative review | High-fiber, anti-inflammatory diets protect against periodontal inflammation via SCFA production and immune modulation. | |||||
| Diet and Oral Microbiome |
[94] Santonocito S et al., 2025 | Book chapter / narrative synthesis | Dietary composition shapes oral microbiome structure, inflammatory signaling, and disease susceptibility. | |||||
| F. Interventions targeting stress biology, oral homeostasis, and occupational wellbeing | ||||||||
| Oral health coaching & dietary interventions | [95] Antoniadou & Varzakas, 2020 | Narrative review; coaching models | Structured oral health and diet coaching improves adherence, self-management, and preventive oral health behaviors in independent elderly populations. | |||||
| Diet, oral health, and systemic links | [96] Antoniadou & Varzakas, 2021 | Narrative review | Highlights diet as a modulator of oral and systemic inflammation, microbiome balance, and chronic disease risk. | |||||
| Probiotics, prebiotics, and caries prevention | [97] Amargianitakis et al., 2021 | Narrative review | Integrates probiotic-based strategies with patient coaching to support caries prevention and oral microbial balance. | |||||
| Functional foods, gut microbiome, and metabolic health | [98] Bezirtzoglou et al., 2021 | Systematic review | Demonstrates the role of microbiome-targeted functional foods in metabolic regulation and inflammatory control, with implications for oral-systemic health. | |||||
| Dietary interventions for disease prevention | [99] Antoniadou & Varzakas, 2024 | Narrative review | Presents dietary strategies as tools for reducing systemic and oral disease burden via immune and microbiome modulation. | |||||
| Digital lifestyle interventions & mental health | [100] Brinsley et al., 2025 | Systematic review & meta-analysis | Digital interventions significantly reduce stress, anxiety, and depression, supporting scalable occupational wellbeing strategies. | |||||
| Digital interventions beyond depression | [101] Linardon et al., 2025 | Meta-analysis | Shows broader wellbeing benefits of digital mental health interventions beyond depressive symptom reduction. | |||||
| Caregiver burden and psychosocial stress | [102] Gholami et al., 2025 | Scoping review | Identifies unmet psychosocial and emotional needs contributing to chronic stress and burnout in caregiving roles. | |||||
| Moral injury prevention | [103] Williamson et al., 2025 | Narrative review | Frames moral injury as a distinct stressor requiring targeted preventive and therapeutic interventions. | |||||
| Mind-body interventions & immune markers | [104] Naveen et al., 2024 | Pilot randomized controlled trial | Tele-yoga reduced burnout and improved immune markers in healthcare workers, linking stress reduction with biological outcomes. | |||||
| Non-pharmacological stress interventions | [25] Meneses Damasceno & Pimentel, 2025 | Integrative review | Summarizes effectiveness of non-pharmacological stress-reduction strategies in healthcare workers. | |||||
| Breathwork and stress resilience | [105] Little, 2025 | Narrative review | Breath-based interventions enhance stress resilience and emotional regulation through autonomic modulation. | |||||
| Lifestyle, circadian disruption, and metabolic health | [27] Robinson et al., 2025 | Randomized crossover trial | Lifestyle intervention improved metabolic and mental health outcomes in female night-shift healthcare workers. | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



