Figure 1.
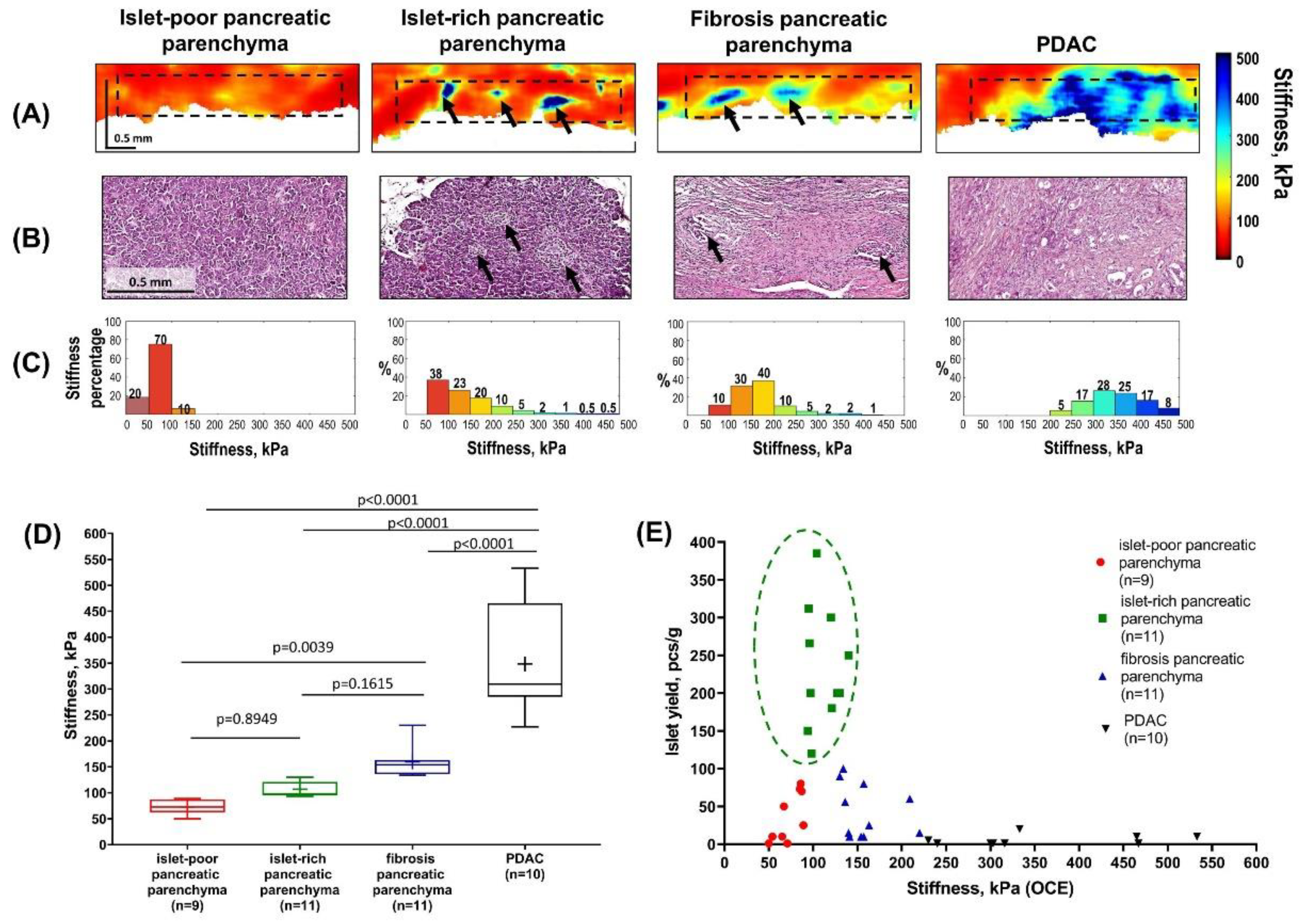
Quantification of the stiffness of intact pancreatic parenchyma (islet-poor and islet-rich) and pancreatic lesion groups (parenchymal fibrosis and/or PDAC invasion) using compression optical coherence elastography (OCE) and comparison with islet yield from collagenase-treated pancreatic tissue.
Figure 1.
Quantification of the stiffness of intact pancreatic parenchyma (islet-poor and islet-rich) and pancreatic lesion groups (parenchymal fibrosis and/or PDAC invasion) using compression optical coherence elastography (OCE) and comparison with islet yield from collagenase-treated pancreatic tissue.
Total pancreatectomy in patients with pancreatic pathology is associated with low postoperative mortality (approximately 5%) [
1], but it results in severe endocrine insufficiency and significant metabolic complications, including brittle diabetes mellitus that is difficult to manage [
2]. To prevent postoperative diabetes and its sequelae, intraportal islet autotransplantation (TPIAT) is performed after total pancreatectomy. This procedure reduces dependence on long-term insulin therapy and improves glycemic control [
3]. Accurate quantification of pancreatic tissue quality is essential for evaluating the feasibility and efficiency of islet isolation from post-pancreatectomy specimens [
4] and may be influenced by the extent and pattern of pancreatic morphological damage. The presence of fibrosis of varying severity, including post-chemotherapy fibrosis, fibrocystic changes, inflammatory processes, or tumor invasion in patients with pancreatic cancer, all of which are associated with increased tissue stiffness, may adversely affect the isolation of viable, functional islets of Langerhans [
4,
5,
6,
7]. From this perspective, pancreatic tissue obtained from patients with pancreatic ductal adenocarcinoma can be regarded as a clinically relevant, fibrosis-dominant model, enabling systematic investigation of stiffness-related alterations and their impact on islet isolation under controlled conditions. Until now, pancreatic tissue characterization has relied primarily on biopsy with histological analysis or medical imaging modalities such as ultrasound, computed tomography, or magnetic resonance imaging [
8]. However, these methods can be labor-intensive or lack sufficient spatial resolution to effectively visualize the microstructural features of pancreatic tissue and the presence of islets. Consequently, there is a need for novel intraoperative imaging techniques, and optical coherence elastography (OCE) represents a promising candidate.
The study was carried out on 41 freshly excised human pancreatic specimens obtained from 41 patients (ages 38–83) with stage I or II (T1–2 N0–1 M0) pancreatic ductal adenocarcinomas (PDACs) after pancreatectomy. Nine patients developed type 2 diabetes mellitus before their cancer diagnosis. Eleven patients had received neoadjuvant chemotherapy with FOLFIRINOX prior to resection. For each patient, pancreatic parenchyma samples were obtained at a distance of at least 10 mm from the tumor. The specimens ranged in size from 0.5x1.0x0.5 cm3 to 1.0x2.0x0.5 cm3.
(A) OCE images of the four morphological types of pancreatic tissue were acquired using a 20 kHz spectral-domain OCT system with a central wavelength of 1.3 µm [
9,
10,
11] combined with the phase-sensitive compression OCE mode for assessing the biomechanical properties of the tissues [
12]. For OCE image reconstruction and evaluation of the absolute stiffness (Young’s modulus, kPa) of the pancreatic tissues, the specimen was compressed by the OCT probe through an intermediate layer of reference silicone with 100 kPa [
12,
13,
14]. OCE estimates were obtained for a standardized stress (2±1 kPa in this study) to account for the fact that human pancreas is a nonlinear viscoelastic soft tissue [
15,
16]. It was established that homogeneous low stiffness values (75 kPa) characterized islet-poor pancreatic parenchyma. In contrast, heterogeneous distribution of low stiffness values with isolated areas of increased stiffness (> 250 kPa) was observed in islet-rich (black arrows) pancreatic parenchyma. In cases where fibrosis pancreatic parenchyma was present due to chronic pancreatitis, stiffness values increased (100 kPa) compared to intact pancreatic parenchyma. When regions of a PDAC were present, stiffness values significantly exceeded those of intact and fibrosis pancreatic parenchyma, reaching over 400 kPa in extensive high-stiffness areas.
As a result, OCE with a spatial resolution of 30–50 µm enables identification of pancreatic islets at the histological scale based on localized high-stiffness inclusions within the surrounding softer acinar tissue and allows estimation of islet abundance, which may serve as a potential indicator for successful islet isolation. Additionally, OCE enables the detection of acinar tissue areas without islets, as well as significantly harder regions of PDAC and fibrotic pancreatic parenchyma, which could lead to a reduction in tissue quality and a low yield of islets.
(B) After OCE imaging, histological sections were prepared; their planes coincided with the OCE images and stained with hematoxylin and eosin (H&E). Histological analysis verified the OCE data and demonstrated the pancreatic samples of preserved pancreatic parenchyma, both islet-poor and islet-rich (black arrows), as well as parenchyma with PDAC and fibrous parenchyma with reduced acinar tissue. Islet-poor pancreatic parenchyma is a normal variant and is likely related to the anatomical site of sampling. The presence of fibrous parenchyma is a common observation in PDAC and is a consequence of block of the main pancreatic duct, chronic pancreatitis or effects of chemotherapy [
4,
17,
18].
(C) The next step was to obtain and analyze the "stiffness spectra" for the pancreatic specimens, i.e. histograms showing percentages of pixels with different Young’s modulus values within a chosen region of interest (~350 × 3200 μm, outlined by a black dashed rectangle in (A)). The analysis of normalized histograms for the four morphological groups of the pancreas show demonstrates a significant shift in the stiffness distribution: in islet-poor pancreatic parenchyma, 90% of pixels had extremely low stiffness values below 100 kPa. Conversely, the "stiffness spectra" for islet-rich pancreatic parenchyma, fibrous pancreatic parenchyma and PDAC shifts toward higher stiffness values. Notably, pancreatic parenchyma with islets exhibits the most heterogeneous distribution of stiffness, with a clear decrease in the proportion of the softest tissue components (to 38%) and the presence of a small fraction of pixels (~9%) measuring over 250 kPa and corresponding morphologically to the presence of pancreatic islets. In cases of fibrotic parenchyma, the proportion of the softest tissue components decreases to 10%, whereas intermediate average stiffness values (~80%) predominate. For PDAC, the proportion of stiffer areas (˃250 kPa) is highest, exceeding 95%. In comparison with a mean stiffness shown in the next panel (D), such stiffness distributions give more detailed representation about the difference between various pancreatic samples.
(D) The distribution diagram of mean stiffness values for pancreatic samples —both non-pathological and with signs of damage—showed a statistically significant increase in stiffness in postoperative pancreatic samples exhibiting fibrosis due to chronic pancreatitis or tumor invasion, compared to intact pancreatic parenchyma. In this study, to provide more accurate identification of certain pancreatic tissue structures in the OCE images, we scanned a large specimen field and then analyzed the area consisting of 3–4 stitched OCE images. For each patient, three OCE images were quantitatively analyzed to better capture the consistency of stiffness measurements, taking into account morphological heterogeneity and the focal nature of certain pathological changes. Center line in the boxes – median; “+” – mean values; box limits – 25th and 75th percentiles; whiskers - minimum and maximum values within the 1.5× interquartile range of the first and third quartile. Segment indicates a statistically significant difference between the study groups (the Mann-Whitney U-test for multiple comparison were used to detect significant differences in numerical data between independent groups), where p – the magnitude of the statistical significance of the differences between states of pancreatic tissue, n – is the number of examined pancreatic specimens for each group.
(E) Distribution of the number of isolated Langerhans islets relative to the stiffness values in pancreatic samples. Islet isolation was performed according to a previously developed method [
5]. Briefly, pancreatic tissue samples were subjected to enzymatic digestion using collagenase NB1 (3 mg/mL) and neutral protease (0.8 mg/mL). Digestion was performed in two stages and lasted 20–35 min in total (20–30 min followed by an additional 5–10 min). After digestion, enzymatic activity was monitored by dithizone staining to assess the release of islets from acinar tissue. If more than 50% of islets remained attached, a short additional incubation with collagenase was performed. Enzymatic digestion was stopped by dilution with cold wash solution, followed by repeated centrifugation and washing steps at 4 °C. The digested tissue was then filtered, and islets were purified using a discontinuous Ficoll density gradient.
As a result, it was demonstrated that the success of islet isolation depends on the quality of the pancreatic parenchyma sample. A high yield of islets (≥120 pcs/g) was observed in samples with medium stiffness (75–150 kPa), corresponding morphologically to acinar tissue rich in islets. The number of isolated islets decreased (≤110 pcs/g) in samples with high stiffness (>150 kPa), indicative of fibrosis or tumor invasion, and also in samples with low stiffness (<70 kPa), which morphologically corresponded to acinar tissue devoid of islets. Furthermore, both previous studies and our preliminary observations indicate that hyperglycemia and diabetes may arise secondary to pancreatic cancer progression or neoadjuvant therapy [
19] and are associated with reduced islet yield and altered islet quality [
20,
21].
Importantly, pancreatic tissue adjacent to PDAC exhibits structural and biomechanical alterations, including increased extracellular matrix deposition and reduced enzymatic digestibility, that overlap with changes reported in chronic pancreatitis and other fibrotic pancreatic conditions [
8,
22,
23,
24]. These pathological changes can potentially impair the isolation process and affect the quality of islets for subsequent transplantation. This aligns with previous studies showing that histologically confirmed chronic pancreatitis results in poor islet isolation [
25], and that fibrotic tissue is more resistant to collagenase digestion [
26].
Along with the promising results, several limitations of the OCE method should be acknowledged, including limited penetration depth (approximately 2 mm in air) and relatively small tissue scanning fields (up to 4 mm). In addition, in the present study OCE enabled detection of the presence and spatial distribution of pancreatic islets but did not allow for cellular-level characterization. The resolution of OCE images (typically 30–50 μm) does not reach that of histological analysis, therefore minor discrepancies in the size of individual structural components of the tissue may occur. Owing to the lack of cellular resolution, the exact size of individual islets and their total number within pancreatic tissue could not be determined. Nevertheless, the OCE data presented above can already be used to select “soft” intact pancreatic parenchyma as a potential indicator of islet yield. The obtained results suggest that OCE–based assessment of pancreatic tissue quality using stiffness as a prognostic indicator of islet yield may also be relevant for selected non-oncologic pancreatic conditions characterized by fibrosis.
Therefore, for the first time, the potential of the OCE method was demonstrated for an objective, quantitative assessment of post-operative pancreatic tissue samples based on the level and distribution pattern of stiffness (Young's modulus) values in kPa, with the aim of selecting samples for subsequent isolation of Langerhans islets. Furthermore, we believe that the results reported here represent a baseline in the use of this technique and are a first step towards establishing its use in a clinical setting. In the future, the use of C-OCE to measure the elastic properties (stiffness) of the pancreas during surgery may be the next step forward for quantitative assessment of pancreatic quality. Using such a technique, pancreas could be examined in vivo intraoperatively—before resection, during resection in the resection bed, and after resection on the resected specimen.
Author Contributions
Conceptualization, D.K., A.K. and V.Z.; investigation, E.G., E.V., J.T., A.A. and P.E.; analyzed the data, E.G., E.V. and A.P.; writing the original paper, E.G., E.V., A.P. and A.K.; writing the review and editing, L.L., M.S., and N.G.; supervised the work, V.Z. All authors have read and agreed to the published version of the manuscript.
Funding
The study was supported by the Ministry of Healthcare of the Russian Federation for PRMU, grant No. ZKFN-2024-0001.
Institutional Review Board Statement
This study has been approved by the Local Ethics Committee of the Privolzhsky Research Medical University (Protocol #3 from March 29, 2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patients to publish data in scientific literature.
Data Availability Statement
Data available on request from the corresponding author.
Acknowledgments
We thank Prof. V.Y. Zaitsev, Dr. A.L. Matveyev, Dr. L.A. Matveev and Dr. A.A. Sovetsky who developed the OCE technique used in this study. We thank Prof. M.V. Shirmanova for her scientific advice.
Conflicts of Interest
The authors declare no conflicts of interest.
The following abbreviations are used in this manuscript:
| OCE |
Optical coherence elastography |
| PDAC |
Pancreatic ductal adenocarcinoma |
| OCT |
Optical coherence tomography |
| H&E |
Hematoxylin and eosin |
References
- Passeri, M.J.; Baker, E.H.; Siddiqui, I.A.; Templin, M.A.; Martinie, J.B.; Vrochides, D.; Iannitti, D.A. Total Compared with Partial Pancreatectomy for Pancreatic Adenocarcinoma: Assessment of Resection Margin, Readmission Rate, and Survival from the U.S. National Cancer Database. Curr Oncol 2019, 26, e346–e356. [CrossRef]
- Bellin, M.D.; Beilman, G.J.; Sutherland, D.E.; Ali, H.; Petersen, A.; Mongin, S.; Kirchner, V.; Schwarzenberg, S.J.; Trikudanathan, G.; Freeman, M.L.; et al. How Durable Is Total Pancreatectomy and Intraportal Islet Cell Transplantation for Treatment of Chronic Pancreatitis? J Am Coll Surg 2019, 228, 329–339. [CrossRef]
- McEachron, K.R.; Bellin, M.D. Total Pancreatectomy and Islet Autotransplantion for Chronic and Recurrent Acute Pancreatitis. Curr Opin Gastroenterol 2018, 34, 367–373. [CrossRef]
- Kobayashi, T.; Manivel, J.C.; Carlson, A.M.; Bellin, M.D.; Moran, A.; Freeman, M.L.; Bielman, G.J.; Hering, B.J.; Dunn, T.; Sutherland, D.E.R. Correlation of Histopathology, Islet Yield, and Islet Graft Function after Islet Autotransplantation in Chronic Pancreatitis. Pancreas 2011, 40, 193–199. [CrossRef]
- Zagainov, V.E.; Kuchin, D.M.; Kashina, A.V.; Lugovaya, L.A.; Zarechnova, N.V.; Galanina, T.A.; Naraliev, N.U.; Kolesnik, Y.I.; Vasilchikova, E.A.; Ermakova, P.S.; et al. Total Pancreatectomy with Islet Autotransplantation (TPIAT) as a Technique to Treat Chronic Idiopathic Pancreatitis: Early Experience Analysis. Sovrem Tekhnologii Med 2024, 16, 44–56. [CrossRef]
- Chinnakotla, S.; Radosevich, D.M.; Dunn, T.B.; Bellin, M.D.; Freeman, M.L.; Schwarzenberg, S.J.; Balamurugan, A.N.; Wilhelm, J.; Bland, B.; Vickers, S.M.; et al. Long-Term Outcomes of Total Pancreatectomy and Islet Auto Transplantation for Hereditary/Genetic Pancreatitis. J Am Coll Surg 2014, 218, 530–543. [CrossRef]
- Matsuda, Y.; Inoue, Y.; Hiratsuka, M.; Kawakatsu, S.; Arai, T.; Matsueda, K.; Saiura, A.; Takazawa, Y. Encapsulating Fibrosis Following Neoadjuvant Chemotherapy Is Correlated with Outcomes in Patients with Pancreatic Cancer. PLoS One 2019, 14, e0222155. [CrossRef]
- Miller, F.H.; Lopes Vendrami, C.; Hammond, N.A.; Mittal, P.K.; Nikolaidis, P.; Jawahar, A. Pancreatic Cancer and Its Mimics. Radiographics 2023, 43, e230054. [CrossRef]
- Gelikonov, V.M.; Romashov, V.N.; Shabanov, D.V.; Ksenofontov, S.Yu.; Terpelov, D.A.; Shilyagin, P.A.; Gelikonov, G.V.; Vitkin, I.A. Cross-Polarization Optical Coherence Tomography with Active Maintenance of the Circular Polarization of a Sounding Wave in a Common Path System. Radiophys Quantum El 2018, 60, 897–911. [CrossRef]
- Moiseev, A.A.; Gelikonov, G.V.; Terpelov, D.A.; Shilyagin, P.A.; Gelikonov, V.M. Noniterative Method of Reconstruction Optical Coherence Tomography Images with Improved Lateral Resolution in Semitransparent Media. Laser Phys. Lett. 2013, 10, 125601. [CrossRef]
- Rodimova, S.; Gubarkova, E.; Bobrov, N.; Shchechkin, I.; Kozlova, V.; Zolotova, N.; Potapov, A.; Kiseleva, E.; Gelikonov, G.; Gladkova, N.; et al. Optical Coherence Tomography Angiography, Elastography, and Attenuation Imaging for Evaluation of Liver Regeneration. Diagnostics (Basel) 2025, 15, 977. [CrossRef]
- Zaitsev, V.Y.; Matveyev, A.L.; Matveev, L.A.; Sovetsky, A.A.; Hepburn, M.S.; Mowla, A.; Kennedy, B.F. Strain and Elasticity Imaging in Compression Optical Coherence Elastography: The Two-Decade Perspective and Recent Advances. J Biophotonics 2021, 14, e202000257. [CrossRef]
- Matveyev, A.L.; Matveev, L.A.; Sovetsky, A.A.; Gelikonov, G.V.; Moiseev, A.A.; Zaitsev, V.Y. Vector Method for Strain Estimation in Phase-Sensitive Optical Coherence Elastography. Laser Phys. Lett. 2018, 15, 065603. [CrossRef]
- Sovetsky, A.A.; Matveyev, A.L.; Matveev, L.A.; Gubarkova, E.V.; Plekhanov, A.A.; Sirotkina, M.A.; Gladkova, N.D.; Zaitsev, V.Y. Full-Optical Method of Local Stress Standardization to Exclude Nonlinearity-Related Ambiguity of Elasticity Estimation in Compressional Optical Coherence Elastography. Laser Phys. Lett. 2020, 17, 065601. [CrossRef]
- Wex, C.; Fröhlich, M.; Brandstädter, K.; Bruns, C.; Stoll, A. Experimental Analysis of the Mechanical Behavior of the Viscoelastic Porcine Pancreas and Preliminary Case Study on the Human Pancreas. J Mech Behav Biomed Mater 2015, 41, 199–207. [CrossRef]
- Gubarkova, E.V.; Sovetsky, A.A.; Matveev, L.A.; Matveyev, A.L.; Vorontsov, D.A.; Plekhanov, A.A.; Kuznetsov, S.S.; Gamayunov, S.V.; Vorontsov, A.Y.; Sirotkina, M.A.; et al. Nonlinear Elasticity Assessment with Optical Coherence Elastography for High-Selectivity Differentiation of Breast Cancer Tissues. Materials (Basel) 2022, 15, 3308. [CrossRef]
- Caban, M.; Małecka-Wojciesko, E. Pancreatic Incidentaloma. J Clin Med 2022, 11, 4648. [CrossRef]
- Tao, X.; Xiang, H.; Pan, Y.; Shang, D.; Guo, J.; Gao, G.; Xiao, G.G. Pancreatitis Initiated Pancreatic Ductal Adenocarcinoma: Pathophysiology Explaining Clinical Evidence. Pharmacol Res 2021, 168, 105595. [CrossRef]
- Hwangbo, Y.; Lee, E.K. Acute Hyperglycemia Associated with Anti-Cancer Medication. Endocrinol Metab (Seoul) 2017, 32, 23–29. [CrossRef]
- Qi, M.; McFadden, B.; Valiente, L.; Omori, K.; Bilbao, S.; Juan, J.; Rawson, J.; Oancea, A.R.; Scott, S.; Nair, I.; et al. Human Pancreatic Islets Isolated From Donors With Elevated HbA1c Levels: Islet Yield and Graft Efficacy. Cell Transplant 2015, 24, 1879–1886. [CrossRef]
- Liang, R.; Sun, P.; Cai, X.; Liu, T.; Wang, L.; Liu, N.; Ding, X.; Zhang, B.; Liu, Z.; Zou, J.; et al. Characteristics of Research-Focused Human Islet Preparations from Organ Donors with Type 2 Diabetes. Islets 15, 2219104. [CrossRef]
- Huang, C.-T.; Lin, C.-K.; Lee, T.-H.; Liang, Y.-J.; Huang, C.-T.; Lin, C.-K.; Lee, T.-H.; Liang, Y.-J. Pancreatic Fibrosis and Chronic Pancreatitis: Mini-Review of Non-Histologic Diagnosis for Clinical Applications. Diagnostics 2020, 10. [CrossRef]
- Le Cosquer, G.; Maulat, C.; Bournet, B.; Cordelier, P.; Buscail, E.; Buscail, L. Pancreatic Cancer in Chronic Pancreatitis: Pathogenesis and Diagnostic Approach. Cancers (Basel) 2023, 15, 761. [CrossRef]
- Calomino, N.; Carbone, L.; Kelmendi, E.; Piccioni, S.A.; Poto, G.E.; Bagnacci, G.; Resca, L.; Guarracino, A.; Tripodi, S.; Barbato, B.; et al. Western Experience of Hepatolithiasis: Clinical Insights from a Case Series in a Tertiary Center. Medicina 2025, 61. [CrossRef]
- Liu, X.; Matsumoto, S.; Okitsu, T.; Iwanaga, Y.; Noguchi, H.; Yonekawa, Y.; Nagata, H.; Kamiya, H.; Ueda, M.; Hatanaka, N.; et al. Analysis of Donor- and Isolation-Related Variables from Non-Heart-Beating Donors (NHBDs) Using the Kyoto Islet Isolation Method. Cell Transplant 2008, 17, 649–656. [CrossRef]
- Matsumoto, S.; Noguchi, H.; Naziruddin, B.; Onaca, N.; Jackson, A.; Nobuyo, H.; Teru, O.; Naoya, K.; Klintmalm, G.; Levy, M. Improvement of Pancreatic Islet Cell Isolation for Transplantation. Proc (Bayl Univ Med Cent) 2007, 20, 357–362. [CrossRef]
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |