
Submitted:
14 January 2026
Posted:
15 January 2026
You are already at the latest version
Abstract
Background/Objectives: The rising prevalence of extended-spectrum beta-lactamase (ESBL)–producing pathogens has emerged as a significant challenge in the treatment of pyelonephritis. This study aimed to determine the frequency of ESBL-producing agents in hospitalized patients with pyelonephritis, identify associated risk factors, and assess the appropriateness of empirical antimicrobial therapy. Methods: This prospective study included patients hospitalized with pyelonephritis in the Infectious Diseases Clinic of Ankara Training and Research Hospital between October 1, 2022, and February 29, 2024. Demographic features, comorbidities, urinary system pathologies, history of urinary tract interventions, recent hospitalization, antibiotic use within the previous three months, and prior urinary tract infections were compared between patients infected with ESBL-producing and non-ESBL-producing organisms. Antimicrobial susceptibility pro-files and the appropriateness of empirical treatments were evaluated. Statistical analyses were performed using SPSS version 25.0, with p< 0.05 considered statistically significant. Results: Escherichia coli (n=142) and Klebsiella spp. (n=43) were isolated in 180 of 204 patients. ESBL positivity was detected in 95 patients (52.7%). Male sex (p=0.007), history of urinary intervention (p=0.019), hospitalization within the previous month (p< 0.001), and antibiotic use in the last three months (p=0.002) were identified as significant risk factors for ESBL positivity. ESBL production was not associated with prolonged hospitalization; however, bacteremia significantly increased length of stay (p< 0.001). Antimicrobial susceptibility rates were markedly lower in the ESBL-positive group. The appropriateness of empirical therapy was also significantly reduced, with piperacillin–tazobactam being the most frequently inappropriate agent due to high resistance rates and unnecessary broad-spectrum use. Conclusions: ESBL-producing pathogens were highly prevalent among hospitalized patients with pyelonephritis. The low appropriateness of empirical therapy in ESBL-positive cases underscores the need for careful evaluation of ESBL risk factors prior to treatment initiation, as ESBL rates may approach 50%.
Keywords:
pyelonephritis
; extended spectrum beta-lactamases
; antibiotic resistance
; risk factors
; empirical therapy
1. Introduction
Pyelonephritis is a complicated upper urinary tract infection and represents a major cause of community-acquired infections for which timely and appropriate antimicrobial therapy is essential [1,2]. The causative pathogens are predominantly members of the Enterobacterales family, with Escherichia coli as the most frequently isolated organism, followed by Enterococcus species [3,4,5].
Resistance to third-generation cephalosporins and other antimicrobial agents among E. coli and Klebsiella spp. has increased substantially, with a marked global rise over the past two decades [5,6]. In Türkiye, E. coli remains the most frequently isolated pathogen in community-acquired urinary tract infections, followed by Klebsiella spp., with resistance rates showing a marked increase over recent years, consistent with global trends [7]. Rising antimicrobial resistance has been linked to increased rates of complications, therapeutic failure and prolonged hospitalization [8]. Delays in initiating appropriate antibiotic therapy are associated with an increased risk of complications, including bacteremia, sepsis and acute kidney injury and with higher morbidity and mortality [9].
In clinical practice antimicrobial therapy is frequently initiated empirically, as susceptibility results from urine cultures typically become available only after at least 48 hours. Therefore, local antimicrobial resistance data play a crucial role in guiding empirical antimicrobial therapy. Although antibiotics have substantially reduced infection-related mortality, inappropriate use contributes to antimicrobial resistance, clinical failure, increased healthcare costs and Clostridioides difficile infection [6,10].
Although numerous studies have examined antimicrobial resistance in urinary tract infections, few have simultaneously evaluated risk factors for extended-spectrum beta-lactamase (ESBL)–producing pathogens and the appropriateness of empirical antibiotic therapy based on culture results in hospitalized patients with community-acquired acute pyelonephritis. Most existing studies focus on uncomplicated urinary tract infections or heterogeneous patient populations, and prospective data from regions with high antimicrobial resistance rates remain limited [11,12].
This study aimed to evaluate the distribution of causative pathogens, determine the prevalence of extended-spectrum beta-lactamase (ESBL)–producing microorganisms, identify risk factors associated with ESBL production, and assess the appropriateness of empirical antibiotic therapy in patients hospitalized with community-acquired pyelonephritis.
2. Results
2.1. Study Population and Demographic Characteristics
A total of 360 patients hospitalized with pyelonephritis were screened during the 17-month study period. Following exclusion of 108 patients with known pre-treatment urine culture results and 48 patients with negative admission cultures, 204 patients were included in the final analysis.
Of these patients, 56.9% (n = 116) were female, with a mean age of 68.8 ± 18.0 years. At least one comorbidity was present in 88.7% of patients, and 26.5% (n = 54) had a history of urinary tract infection within the preceding year. Risk factors associated with pyelonephritis in the study cohort are summarized in Table 1.
Dysuria was the most common presenting symptom (67.6%), followed by chills (58.3%), fever (52.2%), nausea (52.5%), vomiting (38.7%), abdominal pain (20.1%), flank pain (17.6%), pollakiuria (14.7%), incontinence (10.8%), hematuria (8.8%), and urgency (2.9%).
2.2. Microbiological Results
A total of 218 pathogens were isolated from 204 patients. Dual pathogen growth was observed in 7% of cases. Escherichia coli was the most frequently isolated organism, accounting for 69.6% of all isolates. The distribution of pathogens is shown in Figure 1.
2.3. Distribution of ESBL and Associated Factors
Extended-spectrum beta-lactamase (ESBL)–producing organisms were identified in 95 patients, of whom 48 were male. ESBL positivity was significantly more frequent in male patients than in female patients (p = 0.007) (Table 2).
Among evaluated risk factors, a history of urological intervention was significantly more frequent in patients with ESBL-positive infections (p = 0.019) (Table 3). The mean duration of hospitalization did not differ significantly between the ESBL-positive and ESBL-negative groups (7.9 ± 2.5 vs. 7.3 ± 2.2 days; p = 0.078).
ESBL production rates were 52.1% in E. coli isolates and 55.3% in Klebsiella spp. isolates, with no significant difference between the two organisms (p = 0.73). Overall, bacteremia was observed in 24.4% of patients and in 23.2% of patients with ESBL-positive infections.
Recent hospitalization within the preceding month and antibiotic use within the previous three months were significantly more frequent among patients with ESBL-positive infections (p < 0.001 and p = 0.002, respectively) (Table 3).

Table 4.
| Variable | ESBL positive n (%) |
ESBL negative n (%) | p value |
|---|---|---|---|
| Hospitalization in the preceding month Yes No |
|||
| 28 (80.0) 67 (46.2) |
7 (20.0) 78 (53.8) |
<0,0011 | |
| Antibiotic exposure in the previous three months Yes No |
47 (67.1) 48 (43.6) |
23 (32.9) 62 (56.4) |
0,0021 |
| History of urinary tract infection within the previous year Yes No |
29 (60.4) 66 (50.0) |
19 (39.6) 66 (50.0) |
0,2161 |
1. Chi-square test.
2.4. Antimicrobial Susceptibility Results
Among ESBL-producing isolates, susceptibility rates were 86.8% for meropenem and amikacin, 83.5% for gentamicin and 71.4% for piperacillin–tazobactam. In contrast, susceptibility to amoxicillin–clavulanate and ciprofloxacin was substantially lower, at 35.2% and 20.2%, respectively.
Piperacillin–tazobactam resistance was identified in 26 of 91 ESBL-producing strains. Among these, 11 strains also exhibited concurrent carbapenem resistance and were excluded from further analysis. When the analysis was restricted to carbapenem-susceptible ESBL strains, the piperacillin–tazobactam resistance rate was 16.4%.
Detailed antibiotic susceptibility results are presented in Table 5.
Table 4.
Comparison of antibiotic susceptibility between ESBL-positive and ESBL-negative isolates.
| ESBL positive n:91 |
ESBL negative n:78 |
p value | |
|---|---|---|---|
|
Amikacin Resistant Sensitive to high doses Sensitive |
|||
| 5 (5.5) | 0(0) | ||
| 7 (7.7) | 0(0) | 0,0011 | |
| 79 (86.8) | 78 (100.0) | ||
|
Amoxicillin-clavulanic acid Resistant Sensitive |
59 (64.8) 32 (35.2) |
9 (11.5) 69 (88.5) |
<0,0011 |
|
Ciprofloxacin Resistant Sensitive to high doses Sensitive |
58 (65.2) 13 (14.6) 18 (20.2) |
7 (9.0) 0(0) 71 (91.0) |
<0,0011 |
|
Gentamicin Resistant Sensitive |
15 (16.5) 76 (83.5) |
1 (1.3) 77 (98.7) |
0,0011 |
|
Meropenem Resistant Sensitive to high doses Sensitive |
10 (11.0) 2 (2.2) 79 (86.8) |
0 (0) 0(0) 0(0) |
0,0011 |
|
Piperacillin-Tazobactam Resistant Sensitive |
26(28.6) 65 (71.4) |
1 (1.3) 77 (98.7) |
0,0011 |
Susceptibility rates were consistently higher among ESBL-negative isolates than among ESBL-positive isolates, with statistically significant differences observed across most antibiotics tested (p < 0.05). Trimethoprim–sulfamethoxazole (TMP–SMX) resistance was observed in 44.7% of ESBL-positive isolates, compared with 16.4% of ESBL-negative isolates.
Among ESBL-negative isolates, susceptibility to third-generation cephalosporins was high, with rates of 98.7% for ceftazidime, 98.7% for cefixime, and 91% for ceftriaxone. In contrast, resistance to the second-generation cephalosporin cefuroxime was observed in 50.0% of isolates.
2.5. Empirical Therapy and Treatment Modifications
The most frequently initiated empirical therapy was ceftriaxone (63.7%), followed by piperacillin–tazobactam (23%) and ertapenem (5.4%) (Table 5). Empirical therapy was modified in 53.9% of patients (n = 110), with 11% of modifications representing de-escalation and 89% escalation.
Table 5.
Rate of antibiotic revisions.
| Antibiotic change | n (%) |
|---|---|
|
All treatments Present absent |
|
| 110 (53.9) | |
| 94 (46.1) | |
|
Ceftriaxone Present Absent |
70 (53.8) 60 (46.2) |
|
Piperacillin-Tazobactam Present Absent |
29 (72.5) 11 (27.5) |
|
Ertapenem/Meropenem Present Absent |
7 (35.0) 13 (65.0) |
Among patients who received piperacillin–tazobactam as empirical therapy, the rate of treatment modification was significantly higher compared with those receiving other initial antibiotics (p = 0.036). Among the 29 patients who initially received piperacillin–tazobactam, therapy was de-escalated to ceftriaxone in 9 (31%) patients, whereas escalation was required in 20 (69%) patients. Reasons for escalation included piperacillin–tazobactam resistance (n = 11), bacteremia caused by ESBL-producing organisms (n = 4), clinical deterioration (n = 4), and concomitant soft tissue infection (n = 1).
The rate of empirical treatment modification was significantly higher in the ESBL positive group than in the ESBL negative group (74.7% vs. 29.4%, p < 0.001).
2.6. Clinical Outcomes and Mortality Rates
Of the 204 patients included in the study, 94.6% (n = 193) were discharged with clinical recovery, while 5.3% (n = 11) required admission to the intensive care unit (ICU). Eight of these patients were managed in our hospital’s ICU, and three were transferred to external centers. Among patients treated in our ICU, six died within 30 days, corresponding to an ICU mortality rate of 75%. There were no statistically significant differences in 30-day clinical outcomes between patients requiring empirical treatment modification and those who did not (Figure 2). The overall 30 day mortality rate for the entire cohort was 2.98%. Mortality data were unavailable for the three patients transferred to outside facilities.
2.7. Changes in Laboratory Parameters and Imaging Findings
During treatment, significant reductions were observed in white blood cell (WBC) count, C-reactive protein (CRP), procalcitonin (PCT), and creatinine levels, accompanied by a significant increase in glomerular filtration rate (GFR) (Table 6; all p < 0.05).
Imaging was performed with ultrasonography (USG) in 126 patients, abdominal computed tomography (CT) in 40 patients, and both modalities in 21 patients. Among the 61 patients who underwent abdominal CT, 47 (77%) had imaging performed in the emergency department prior to consultation with the infectious diseases team. Among patients who underwent imaging, urolithiasis, hydronephrosis, and radiological findings consistent with pyelonephritis were identified in 13.7%, 13.7%, and 30% of cases, respectively.
3. Discussion
According to the Infectious Diseases Society of America (IDSA) 2010 guidelines in effect at the time the study was conducted, acute pyelonephritis was classified as either complicated or uncomplicated and all patients included in this study met the criteria for complicated pyelonephritis. In the updated IDSA 2025 guidelines, all cases of pyelonephritis are categorized as complicated urinary tract infections, reflecting an evolution in disease classification and management [1,13]. In this context, the study population may be considered broadly aligned with current definitions; however, differences in guideline frameworks over time should be taken into account when interpreting the findings.
Urinary tract infections are well established as the most common source of Gram-negative bacteremia, and timely initiation of appropriate empirical antibiotic therapy is a key determinant of clinical outcomes, including reductions in morbidity and mortality [14,15]. However, increasing antimicrobial resistance among uropathogens complicates empirical treatment selection and often necessitates broader-spectrum antibiotic use [16]. While early effective therapy remains essential, the widespread use of broad-spectrum agents accelerates the selection and dissemination of resistant strains, underscoring the need to balance prompt treatment with antimicrobial stewardship principles [17].
In our study, E.coli accounted for approximately 70% of isolates, and the inclusion of Klebsiella spp. increased this proportion to over 90%, consistent with the established literature on the etiology of urinary tract infections. The predominance of these pathogens is clinically relevant, as increasing antimicrobial resistance among community-acquired strains—both globally and in Türkiye—progressively limits empirical treatment options and complicates timely initiation of appropriate therapy [6,11,18]. Several studies from Türkiye have reported a marked increase in ESBL positivity rates over recent years and the ESBL prevalence of 52.7% observed in our cohort is consistent with recent reports involving similar hospitalized patient populations [19]. This relatively high prevalence may, at least in part, reflect the inclusion of exclusively hospitalized patients and the increasing resistance patterns observed in our setting.
Although no significant difference was observed in bacteremia rates between patients infected with ESBL-positive and ESBL-negative pathogens, bacteremia was associated with a significantly longer length of hospital stay (p < 0.001) [20]. Although the length of hospital stay was somewhat longer among patients with bacteremia in the ESBL-positive group compared with the ESBL-negative group, this difference did not reach statistical significance. While several studies have reported prolonged hospitalization among patients infected with ESBL-producing pathogens, our findings demonstrated comparable mean lengths of stay between the two groups [21,22]. This observation may be related to the patient profile of our center. Given the high proportion of elderly patients, individuals with low socioeconomic status, and those requiring ongoing care, completion of treatment during hospitalization may have been preferred in order to mitigate potential challenges related to adherence to outpatient therapy after discharge.
According to 2023 data from the WHO European Region Antimicrobial Medicines Consumption Network, Türkiye is among the countries with the highest antibiotic consumption in the European Region [23]. This observation provides important contextual information that may be relevant when interpreting the high resistance rates observed in our study.
In the present study, empirical treatment modification was significantly more frequent among patients with ESBL-producing pathogens, reflecting the challenges of selecting adequate initial therapy in settings with high antimicrobial resistance. Previous studies have consistently identified recent antibiotic exposure, recent hospitalization, invasive procedures, and the presence of urinary catheters as key risk factors for infections caused by ESBL-producing Enterobacterales [19,24]. Consistent with previous reports, our findings demonstrate that hospitalization within the preceding month and antibiotic use within the previous three months were significantly associated with ESBL positivity. These associations are biologically plausible, as prior antibiotic exposure exerts selective pressure that facilitates the emergence and persistence of resistant strains, while recent hospitalization increases exposure to healthcare-associated pathogens with higher resistance profiles. Importantly, the presence of these risk factors was associated with an increased likelihood of inadequate empirical therapy, leading to subsequent treatment modification. Our findings reinforce the need to incorporate readily identifiable patient-specific risk factors into empirical antibiotic decision-making to improve initial treatment adequacy and potentially reduce the need for later therapeutic adjustments.
From an antimicrobial stewardship perspective broad-spectrum antibiotic use is a well-recognized risk factor for the development of antibiotic resistance, as excessive or unnecessary exposure exerts selective pressure on microbial populations [25]. In the context of urinary tract infections, Alshareef and colleagues demonstrated that implementation of antibiotic de-escalation strategies not only reduced the length of hospital stay but also lowered the likelihood of multidrug-resistant pathogen emergence [26]. Consequently, initiating broad-spectrum antibiotics unnecessarily or failing to de-escalate therapy when appropriate can contribute to the selection and proliferation of resistant strains, highlighting the importance of antibiotic stewardship in clinical practice.
Routine imaging is generally not required in acute pyelonephritis; however, ultrasonography or computed tomography should be reserved for patients with delayed clinical response, suspected complications or specific risk factors [27]. In our cohort, a substantial proportion of computed tomography examinations were performed in the emergency department prior to Infectious Diseases consultation. In settings with high patient volumes and limited access to early subspecialty consultation, diagnostic imaging may be more frequently utilized, sometimes independent of strict clinical indications. While such practices may facilitate rapid decision-making, early or routine computed tomography in clinically uncomplicated cases is likely to provide limited additional diagnostic value, while exposing patients to avoidable radiation and increasing healthcare costs [28]. These findings highlight the need for more judicious, guideline-based use of imaging modalities.
This prospective and single-center design of this study limits the generalizability of the findings. The inclusion of only hospitalized patients may not adequately reflect the full spectrum of community-acquired pyelonephritis, particularly cases managed in the outpatient setting. In addition, limitations in the availability of ertapenem during the study period may have influenced empirical treatment choices. Furthermore, mortality outcomes could not be ascertained for patients transferred to external intensive care units, which may have led to an underestimation of overall mortality rates.
The findings of this study highlight the importance of tailoring empirical antibiotic therapy in hospitalized patients with pyelonephritis according to local pathogen distribution and resistance patterns. In centers with a high prevalence of ESBL-producing organisms, the empirical use of piperacillin–tazobactam should be carefully considered, as it may necessitate frequent treatment modifications. Early revision of therapy based on culture results and the implementation of de-escalation strategies in appropriate patients should therefore be prioritized. Such an approach may support clinical success while reducing unnecessary use of broad-spectrum antibiotics and enhancing the effectiveness of antimicrobial stewardship programs.
4. Materials and Methods
This prospective study was conducted between 1 October 2022 and 29 February 2024 in the Infectious Diseases Department of a 670-bed tertiary care teaching and research hospital in Ankara, the capital of Türkiye. Ethical approval was obtained from the Clinical Research Ethics Committee of the University of Health Sciences Ankara Training and Research Hospital on 14 December 2022 (approval number: E-22-1100).
4.1. Patient Selection and Study Population
Patients aged ≥18 years who were hospitalized with a presumptive diagnosis of pyelonephritis and who received empirical antibiotic therapy were included in the study. Pyelonephritis was diagnosed based on clinical findings, including fever (≥38 °C), chills or rigors, flank pain, nausea, vomiting, and costovertebral angle tenderness. Patients presenting with urinary symptoms such as dysuria or pollakiuria in the absence of systemic signs were classified as having cystitis and were excluded from the study.
According to the IDSA guideline dated 17 July 2025, pyelonephritis is classified as a complicated urinary tract infection. However, at the time the study was conducted, factors such as male sex, pregnancy, urinary catheterization, anatomical or functional abnormalities (e.g., urolithiasis), and comorbid conditions including diabetes mellitus were considered complicating factors and were therefore classified as complicated pyelonephritis.
Patients whose urine culture results were already available at the time of admission and those with no growth in urine cultures obtained prior to empirical therapy were excluded from the study.
4.2. Data Collection
Demographic characteristics (including age and sex), urinary and systemic symptoms, comorbidities, coinfections, physical examination findings (including fever, mental status and costovertebral angle tenderness), and laboratory parameters—namely complete blood count, C-reactive protein (CRP), procalcitonin (PCT), blood urea nitrogen (BUN), creatinine, and glomerular filtration rate (GFR)—were prospectively recorded using standardized follow-up forms. Empirical antibiotic therapies and subsequent targeted treatments administered after the availability of urine culture results were also documented.
4.3. Sample Processing and Microbiological Evaluation
Pyuria was defined as the presence of ≥ 10 leukocytes per mm3 on microscopic examination of an uncentrifuged urine specimen using a Thoma counting chamber. For urine culture, samples were inoculated onto blood agar and Eosin Methylene Blue (EMB) agar using a calibrated 0.01 mL loop and incubated at 37 °C for 16–24 hours. Following incubation, the growth of a single organism or two organisms at a concentration of ≥105 colony-forming units (CFU)/mL was considered significant bacteriuria.
Identification of isolates with significant growth was performed using the VITEK® MS system (bioMérieux, France). Antimicrobial susceptibility testing of Gram-negative pathogens considered causative agents was performed using VITEK-2® AST-N423 cards. Antibiotic susceptibility profiles and ESBL phenotypes were determined using the VITEK-2 Compact system (bioMérieux, France). Susceptibility results were categorized as susceptible, resistant or susceptible at increased exposure based on the automated system. In parallel, antimicrobial susceptibility testing was also performed using the Kirby–Bauer disk diffusion method.
Escherichia coli or Klebsiella spp. isolates reported as ESBL-positive by the laboratory were classified as ESBL-producing strains.
4.4. Antimicrobial Susceptibility Testing
Antimicrobial susceptibility profiles and ESBL production of the study isolates were additionally assessed using the disk diffusion method according to the European Committee on Antimicrobial Susceptibility Testing (EUCAST) breakpoint tables (Version 9.0, 2019) [29].
Disk diffusion testing was performed using antibiotic disks supplied by Bioanalyse (Türkiye), including amoxicillin–clavulanic acid (20/10 µg), aztreonam (30 µg), cefuroxime (30 µg), ceftriaxone (30 µg), ceftazidime (30 µg), cefoxitin (30 µg), piperacillin–tazobactam (100/10 µg), imipenem (10 µg), meropenem (10 µg), ciprofloxacin (5 µg), gentamicin (10 µg), fosfomycin (50 µg) and trimethoprim–sulfamethoxazole (1.25/23.75 µg).
Bacterial suspensions were adjusted to a 0.5 McFarland standard and inoculated onto Mueller–Hinton agar plates (BD, France). An amoxicillin–clavulanic acid disk was placed at the center of the agar plate, while ceftazidime, ceftriaxone, cefoxitin, aztreonam, and imipenem disks were positioned at a distance of 25 mm from the central disk for ESBL screening.
Plates were incubated at 35 °C for 18–24 hours in an incubator (EN 500, NÜVE). Antimicrobial susceptibility results were interpreted according to EUCAST criteria.
4.5. Statistical Analysis
Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) for Windows, version 25.0 (IBM Corp., Armonk, NY, USA). The distribution of continuous variables was assessed using visual inspection of histograms and analytical tests, including the Kolmogorov–Smirnov and Shapiro–Wilk tests. Categorical variables were summarized as numbers and percentages, while normally distributed continuous variables were expressed as means and standard deviations. The Student’s t-test was used to compare continuous variables between two groups, whereas analysis of variance (ANOVA) was applied for comparisons among three or more groups. Comparisons of categorical variables were performed using the chi-square test or Fisher’s exact test, as appropriate. A p value of <0.05 was considered statistically significant.
5. Conclusions
In summary, this prospective single-center study provides contemporary real-world data on the epidemiology of community-acquired pyelonephritis requiring hospitalization in a setting with high antimicrobial resistance. The high prevalence of ESBL-producing Enterobacterales and the frequent need for empirical treatment modification—particularly among patients initially treated with piperacillin–tazobactam highlight the limitations of standardized empirical regimens in regions with evolving resistance patterns. These findings reinforce the critical role of local surveillance data, early culture-guided therapy optimization and antimicrobial stewardship–oriented decision-making in improving clinical outcomes while minimizing unnecessary broad-spectrum antibiotic exposure. Collectively, these results underscore the imperative for context-specific empirical therapeutic strategies and reinforce the value of individualized, data-driven decision-making in the management of hospitalized patients with acute pyelonephritis.
Author Contributions
Conceptualization, G.G and Ş.A.D.; methodology, Ş.A.D., E.K.K; software, M.A.; validation, Ş.A.D, E.K.K, R.B and S.K.; format analysis, G.G, Ş.AD, E.K.K.; investigation, G.G and Ş.A.D..; resources, S.Y and R.B.; data curation, G.G.; writing—original draft preparation, G.G.; writing—review and editing, Ş.A.D.; visualization, G.G and Ş.A.D. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
This study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Clinical Research Ethics Committee of the University of Health Sciences Ankara Training and Research Hospital on 14 December 2022 (approval number: E-22-1100).
Informed Consent Statement
Informed consent was obtained from all subjects involved in this study. Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
The data presented in the study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ESBL | Extended spectrum beta-lactamases |
| UTI | Urinary tract infection |
| ICU | Intensive care unit |
| DM | Diabetes mellitus |
References
- Trautner, B.W.; Cortés-Penfield, N.W.; Gupta, K.; Hirsch, E.B.; Horstman, M.; Moran, G.J.; Colgan, R.; O’Horo, J.C.; Ashraf, M.S.; Connolly, S.; et al. Complicated urinary tract infections: Treatment and management. Clin. Infect. Dis. 2025, 78, 123–134. [CrossRef]
- Foxman B. The epidemiology of urinary tract infection. Nat. Rev. Urol. 2010, 7, 653–660. [CrossRef]
- Johnson, J.R.; Russo, T.A. Acute pyelonephritis in adults. N. Engl. J. Med. 2018, 378, 48–59. [CrossRef]
- Stapleton, A.E.; Endo, Z.; Blaser, B.S.; Sobel J.D. Urinary tract infections. In: Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases, 10th ed.; Blaser, M.J., Cohen, J.I., Holland, S.M., Eds.; Elsevier: Philadelphia, PA, USA, 2025; pp. 909–929.e5. ISBN 978-0-323-93499-2.
- Larramendy, S.; Deglaire, V.; Dusollier, P.; Fournier, J.P.; Caillon, J.; Beaudeau, F.; Moret, L. Risk factors of extended-spectrum beta-lactamases-producing Escherichia coli community-acquired urinary tract infections: A systematic review. Infect. Drug Resist. 2020, 13, 3945–3955. [CrossRef]
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary tract infections: Epidemiology, mechanisms of infection and treatment options. Nat. Rev. Microbiol. 2015, 13, 269–284. [CrossRef]
- Şencan, İ.; Karabay, O.; Altay,F.A.; Yıldız, S.S.; Şimşek, H.; Gözükara, M.G.; Kuzi, S.; Karlıdağ, G.E.; Kaya, Ş.; Kul, G.; el al. Multidrug resistance in pathogens of community-acquired urinary tract infections in Turkey: A multicentre prospective observational study. Turk. J. Med. Sci. 2023, 53, 780–790. [CrossRef]
- Tenney, J.; Hudson, N.; Alnifaidy, H.; Li, J.T.C.; Fung, K.H. Risk factors for acquiring multidrug-resistant organisms in urinary tract infections: A systematic literature review. Saudi Pharm. J. 2018, 26, 678–684. [CrossRef]
- Belyayeva M, Leslie SW, Rout P, et al. Acute Pyelonephritis. [Updated 2024 Feb 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/sites/books/NBK519537.
- Angebault C.; Andremont A. Antimicrobial agent exposure and the emergence and spread of resistant microorganisms: Issues associated with study design. Eur. J. Clin. Microbiol. Infect. Dis. 2013, 32, 581–595. [CrossRef]
- Yıldırım, Ç.; Sarı, S.; Parmaksızoğlu Aydın, A.M.; Kilinç Toker, A.; Turunç Özdemir, A.; Erdem Kıvrak, E.; Mermer, S.; Kahraman, H.; Soysal, O.; Yıldırım, H.Ç.; et al. Extended-Spectrum Beta-Lactamase Production and Carbapenem Resistance in Elderly Urinary Tract Infection Patients: A Multicenter Retrospective Study from Turkey. Antibiotics 2025, 14, 719. [CrossRef]
- Zhou, Y.L.; Long, B.L.; Liu, H.L.; Wu, J.; Xia, H. Risk factors and drug resistance of adult community-onset urinary tract infections caused by Escherichia coli–producing extended-spectrum β-lactamase in the Chongqing region, China: A retrospective case-control study. BMJ Open 2024, 14, e090665. [CrossRef]
- Gupta, K.; Hooton, T.M.; Naber, K.G.; Wullt, B.; Colgan, R.; Miller, L.G.; Moran, G.J.; Nicolle, L.E.; Raz, R.; Schaeffer, A.J.; Soper, D.E. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin. Infect. Dis. 2011, 52, e103–e120. [CrossRef]
- Ince, D.; Fiawoo, S.; Choudhury, R.; Cosgrove, S.E.; Dobrzynski, D.; Gold, H.; Lee, J.H.; Percival, K.M.; Shulder, S.; Sony, D.; Spivak, E.S.; Tamma, P.D.; Nori, P. Epidemiology of Gram-negative bloodstream infections in the United States: Results from a cohort of 24 hospitals. Open Forum Infect. Dis. 2023, 10, ofad265. [CrossRef]
- Zhu, H.; Chen, Y.; Hang, Y.; Luo, H.; Fang, X.; Xiao, Y.; Cao, X.; Zou, S.; Hu, X.; Hu, L.; Zhong, Q. Impact of inappropriate empirical antibiotic treatment on clinical outcomes of urinary tract infections caused by Escherichia coli: A retrospective cohort study. J. Glob. Antimicrob. Resist. 2021, 26, 148–153. [CrossRef]
- Salam, M.A.; Al-Amin, M.Y.; Salam, M.T.; Pawar, J.S.; Akhter, N.; Rabaan, A.A.; Alqumber, M.A.A. Antimicrobial resistance: A growing serious threat for global public health. Healthcare 2023, 11, 1946. [CrossRef]
- Barlam, T.F.; Cosgrove, S.E.; Abbo, L.M.; MacDougall, C.; Schuetz, A.N.; Septimus, E.J.; Srinivasan, A.; Dellit, T.H.; Falck-Ytter, Y.T.; Fishman, N.O.; et al. Implementing an antibiotic stewardship program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin. Infect. Dis. 2016, 62, e51–e77. [CrossRef]
- Azap, O.K.; Arslan, H.; Serefhanoğlu, K.; Colakoğlu, S.; Erdoğan, H.; Timurkaynak, F.; Senger, S.S. Risk factors for extended-spectrum beta-lactamase positivity in uropathogenic Escherichia coli isolated from community-acquired urinary tract infections. Clin. Microbiol. Infect. 2010, 16, 147–151. [CrossRef]
- Kayaaslan, B.; Oktay, Z.; Hasanoglu, I.; Kalem, A.K.; Eser, F.; Ayhan, M.; Guner, R. Increasing rates of extended-spectrum β-lactamase-producing Escherichia coli and Klebsiella pneumoniae in uncomplicated and complicated acute pyelonephritis and evaluation of empirical treatments based on culture results. Eur. J. Clin. Microbiol. Infect. Dis. 2022, 41, 421–430. [CrossRef]
- Hsu, C.Y.; Fang, H.C.; Chou, K.J.; Chen, C.L.; Lee, P.T.; Chung, H.M. The clinical impact of bacteremia in complicated acute pyelonephritis. Am. J. Med. Sci. 2006, 332, 175–180. [CrossRef]
- Gofron, Z.F.; Aptekorz, M.; Gibas, K.W.; Kabała, M.; Martirosian, G. Retrospective study of the etiology, laboratory findings, and management of patients with urinary tract infections and urosepsis from a urology center in Silesia, southern Poland between 2017 and 2020. Med. Sci. Monit. 2022, 28, e935478. [CrossRef]
- Osthoff, M.; McGuinness, S.L.; Wagen, A.Z.; Eisen, D.P. Urinary tract infections due to extended-spectrum beta-lactamase-producing Gram-negative bacteria: Identification of risk factors and outcome predictors in an Australian tertiary referral hospital. Int. J. Infect. Dis. 2015, 34, 79–83. [CrossRef]
- World Health Organization. WHO Regional Office for Europe Antimicrobial Medicines Consumption (AMC) Network: AMC Data 2023. World Health Organization Regional Office for Europe, Copenhagen, Denmark, 2025. Available online: https://iris.who.int/handle/10665/380848 (accessed on 8 January 2026).
- Zhou, Y.L.; Long, B.L.; Liu, H.L.; Wu, J.; Xia, H. Risk factors and drug resistance of adult community-onset urinary tract infections caused by Escherichia coli-producing extended-spectrum β-lactamase in the Chongqing region, China: A retrospective case-control study. BMJ Open 2024, 14(10), e090665. [CrossRef]
- Muteeb, G.; Rehman, M.T.; Shahwan, M.; Aatif, M. Origin of antibiotics and antibiotic resistance, and their impacts on drug development: A narrative review. Pharmaceuticals 2023, 16(11), 1615. [CrossRef]
- Alshareef, H.; Alfahad, W.; Albaadani, A.; Alyazid, H.; Talib, R.B. Impact of antibiotic de-escalation on hospitalized patients with urinary tract infections: A retrospective cohort single center study. J. Infect. Public Health 2020, 13(7), 985–990. [CrossRef]
- Nelson, Z.; Aslan, A.T.; Beahm, N.P.; Blyth, M.; Cappiello, M.; Casaus, D.; Dominguez, F.; Egbert, S.; Hanretty, A.; Khadem, T.; et al. Guidelines for the prevention, diagnosis, and management of urinary tract infections in pediatrics and adults: A WikiGuidelines Group consensus statement. JAMA Netw. Open 2024, 7(11), e2444495. [CrossRef]
- Francisco, M.Z.; Altmayer, S.; Verma, N.; Watte, G.; Brandao, M.C.; Barros, M.C.; Mohammed, T.L.; Hochhegger, B. Appropriateness of computed tomography and ultrasound for abdominal complaints in the emergency department. Curr. Probl. Diagn. Radiol. 2021, 50(6), 799–802. [CrossRef]
- European Committee on Antimicrobial Susceptibility Testing (EUCAST). Breakpoint tables for interpretation of MICs and zone diameters. Version 19, EUCAST; Växjö, Sweden. Available online: https://www.eucast.org.
Figure 1.
Distribution of pathogens.
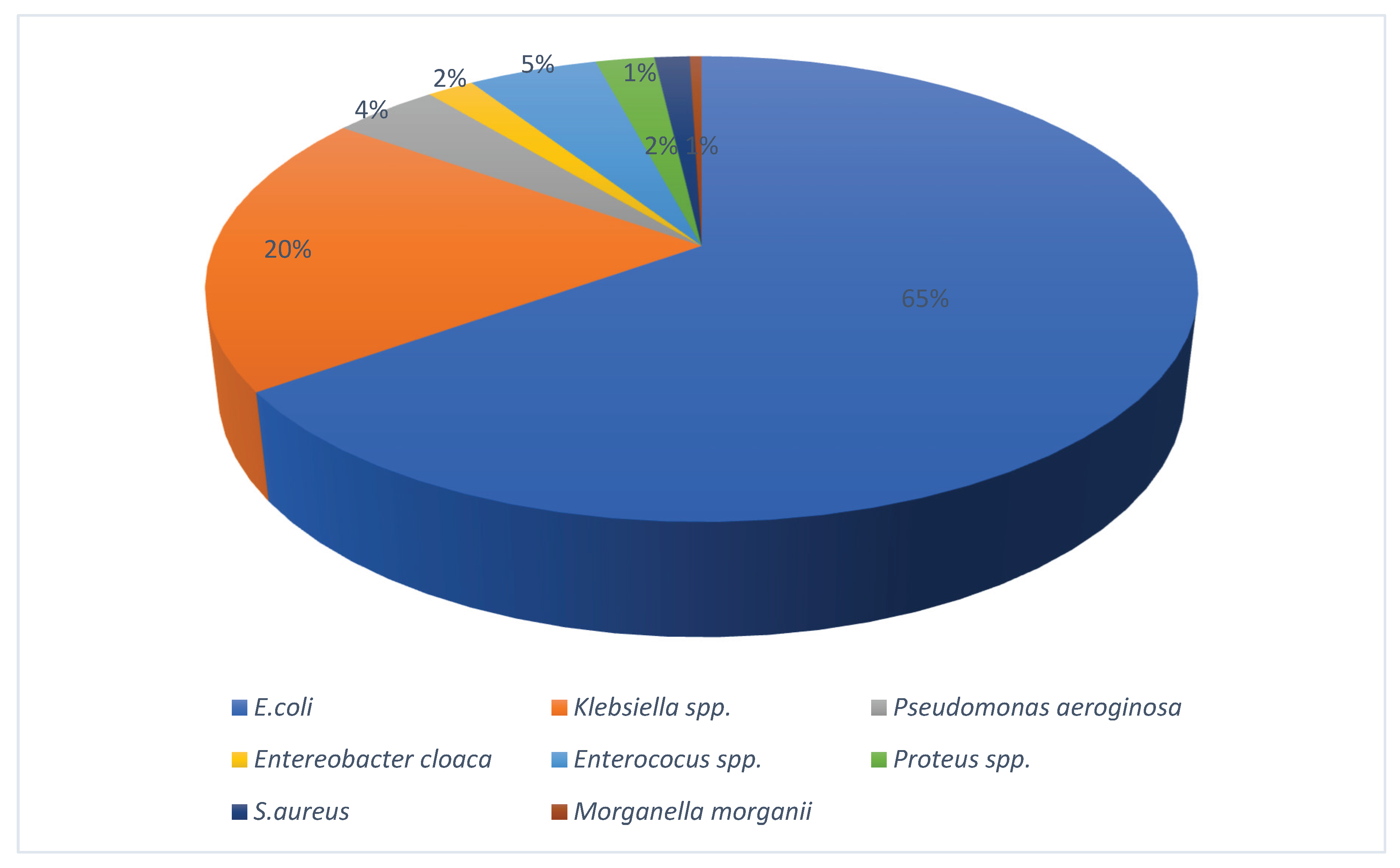
Figure 2.
Kaplan-Meier survival curve for 30 days survival.
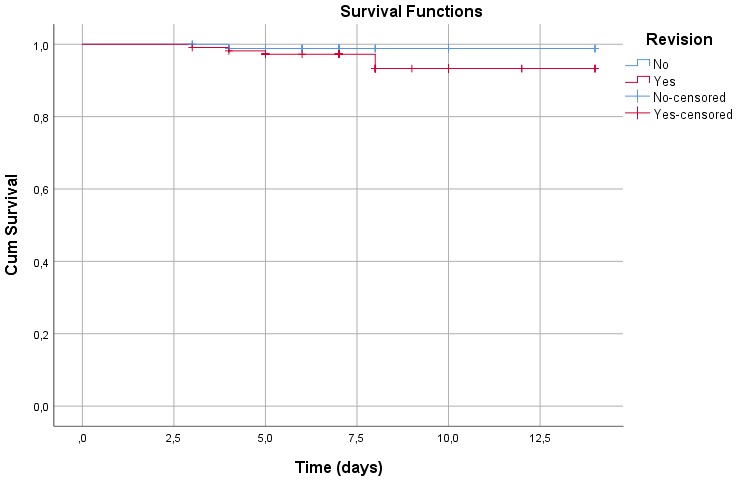
Table 1.
Urinary Tract-Related Risk Factor (n=204).
| Variable | Yes n(%) | No n(%) |
|---|---|---|
| History of UTI | 54 (26.5) | 150 (73.5) |
| CKD/Dialysis | 27 (13.2) | 177 (86.8) |
| Transurethral catheterization | 24 (11.8) | 180 (88.2) |
| Nephrostomy | 2 (1) | 202 (99) |
| Urethral Stent | 2 (1) | 202 (99) |
| Anatomical defect | 10 (4.9) | 194 (95.1) |
| Neurogenic bladder | 11 (5.4) | 193 (94.6) |
| Vesicoureteral reflux | 2 (1) | 202 (99) |
| BPH | 46 (22.5) | 158 (77.5) |
| Prostatitis | 1 (0.5) | 203 (99.5) |
| Urolithiasis | 28 (13.7) | 176 (86.3) |
| Urinary Intervention | 31 (15.2) | 174 (84.8) |
UTI: urinary tract infection. CKD: Chronic kidney disease.
Table 2.
Demographic characteristics and comorbidities of patients according to ESBL status.
| Variable | ESBL positive n (%) |
ESBL negative n (%) |
p value |
|---|---|---|---|
| Male | 48 (64.9) | 26 (35.1) | 0,0071 |
| Age (mean ± SD) | 68.2±16.7 | 68.7±18.4 | 0,8312 |
| Uncontrolled DM | 42 (53,8) | 36 (46,2) | 0,8021 |
| Hypertension | 54 (57,4) | 40 (42,6) | 0,1901 |
| Heart Failure | 18 (60,0) | 12 (40,0) | 0,3851 |
| COPD/Asthma | 15 (57,7) | 11 (42,3) | 0,5871 |
| Neurological disease | 29 (52,7) | 26 (47,3) | 0,9931 |
| Malignancy | 11 (55,0) | 9 (45,0) | 0,8331 |
| Immunosuppression | 9 (69,2) | 4 (30,8) | 0,2171 |
| CKD / Dialysis | 15 (60,0) | 10 (40,0) | 0,4361 |
* DM: Diabetes Mellitus. COPD: Chronic obstructive pulmonary disease. CKD: Chronic kidney disease.
Table 3.
ESBL distribution according to patient-related risk factors (n = 204).
| Variable | ESBL positive n (%) |
ESBL negative n (%) | p value |
|---|---|---|---|
|
Transurethral Catheterization Yes No |
11 (61,1) 84 (51,9) |
7 (38,9) 78 (48,1) |
0,4551 |
|
Nephrostomy / Urethral Stent Yes No |
2 (100,0) 93 (52,2) |
085 (47,8) | 0,4992 |
|
Anatomical Defect Yes No |
5 (71,4) 90 (52,0) |
2 (28,6) 83 (48,0) |
0,4492 |
|
Neurogenic Bladder Yes No |
5 (55,6) 90 (52,6) |
4 (44,4) 81 (47,4) |
1,0002 |
|
Vesicoureteral reflux Yes No |
2 (100,0) 93 (52,2) |
085 (47,8) | 0,4992 |
|
BPH Yes No |
24 (63,2) 71 (50,0) |
14 (36,8) 71 (50,0) |
0,1491 |
|
Prostatitis Yes No |
1 (100,0) 94 (52,5) |
085 (47,5) | 1,0002 |
|
Urolithiasis Yes No |
14 (66,7) 81 (50,9) |
7 (33,3) 78 (49,1) |
0,1751 |
|
Uriner Intervention Yes No |
18 (75,0) 77 (49,4) |
6 (25,0) 79 (50,6) |
0,0191 |
|
Urine Culture E. coli Klebsiella spp. |
74 (52,1) 21 (55,3) |
68 (47,9) 17 (44,7) |
0,7301 |
|
Bacteremia Yes No |
22 (23,2) 73 (76,8) |
22 (25,9) 63 (74,1) |
0,6711 |
|
Hospitalization in the preceding month Yes No |
28 (80.0) 67 (46.2) |
7 (20.0) 78 (53.8) |
<0,0011 |
|
Antibiotic exposure in the previous three months Yes No |
47 (67.1) 48 (43.6) |
23 (32.9) 62 (56.4) |
0,0021 |
| History of urinary tract infection within the previous year Yes No |
29 (60.4) 66 (50.0) |
19 (39.6) 66 (50.0) |
0,2161 |
|
Hospitalization Duration (days) Mean±SD |
7,9 ± 2,5 |
7,3 ± 2,2 |
0,0783 |
1. Chi-square test. 2. Fisher’s exact test. 3. T-test.
Table 6.
Changes in laboratory parameters during hospitalization.
| Title 1 | Day of admission | Day 3 of treatment | Day of discharge | p value |
|---|---|---|---|---|
| WBC (mean±SD) | 13,9 ± 6,2 | 9,1 ± 4,4 | 8,6 ± 3,7 | <0,0011 |
| CRP (mean±SD) | 140,7 ± 93,8 | 99,7 ± 76,3 | 29,2 ± 27,1 | <0,0011 |
| PCT (mean±SD) | 5,1 ± 9,0 | 4,0 ± 7,9 | 0,4 ± 0,4 | <0,0011 |
| Creatinin (mean±SD) | 1,5 ± 1,5 | 1,1 ± 0,7 | 1,0 ± 0,8 | <0,0011 |
| GFR (mean±SD) | 59,7 ± 30,9 | 71,0 ± 32,8 | 75,8 ± 31,5 | <0,0011 |
| Complete urine t | 146,3 ± 73,7 | 17,4 ± 42,6 | - | <0,0012 |
WBC: White blood cell. CRP: C reactive protein. PCT: Procalsitonin. GRF: Glomerular Filtration Rate.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



