
Submitted:
10 June 2024
Posted:
11 June 2024
You are already at the latest version
Abstract
Blood stream infections (BSI) due to carbapenem-resistant gram-negative bacilli (CR-GNB), especially Klebsiella pneumoniae carbapenemase (KPC) and New-Delhi metallo-β-lactamase (NDM) producers, are a major concern of public health, as they are associated with high morbidity and mortality. We conducted a single-center, retrospective, observational study at a tertiary-care, teaching Greek hospital, to determine the incidence, 30-day and overall, in-hospital, crude mortality, risk factors and efficacy of best available treatment options in patients with BSIs from KPC- or NDM-producing GR-GNB. During the one-year study period, from 1st January to 31st December 2023, we recorded 133 episodes of BSIs in 118 unique patients; 79 episodes were due to KPC-producing and 54 to NDM-producing CR-GNB. Our study showed relatively high incidence of BSIs by both KPC- and NDM-producing CR-GNB (0.49 and 0.31 episodes per 1000 patient-days respectively). We found high 30-day crude mortality rates for patients with BSIs due to KPC- producing CR-GNB (26.4 %), and NDM-producing CR-GNB (37%), while BSIs due to NDM-producing P. aeruginosa had the highest 30-day (47.1%) and overall (70.6%) in-hospital, crude mortality. Beta-lactam/beta-lactamase inhibitors as monotherapy or in combination with other active agents used to treat KPC-producing CR-GNB were associated with improved survival rates (p=0.009).
Keywords:
Blood stream infections
; carbapenem-resistant gram-negative bacilli
; Klebsiella pneumoniae carbapenemase
; New-Delhi metallo-β-lactamase
1. Introduction
Carbapenem-resistant gram-negative bacilli (CR-GNB), especially those producing Klebsiella pneumoniae carbapenemases (KPCs) and New-Delhi metallo-β-lactamases (NDMs) represent a major public health problem [1]. KPCs are β-lactamases produced by gram-negative microorganisms that can hydrolyze nearly all β-lactams, including carbapenems, rendering them resistant to most available antibiotic options. First identified in the USA in 1996 [2], these enzymes have since spread in many countries around the world. NDMs are enzymes that belong to the greater family of metallo-β-lactamases (MBLs). These enzymes require zinc to function and can break down almost all β-lactamic antibiotics including carbapenems [3].
Greece is an endemic area for nosocomial infections due to KPC-producing gram-negative bacteria, while the emergence of NDM-producing K. pneumoniae in Greek hospitals has been described in 2013 [4,5,6,8]. An increase in the incidence of infections due to KPC-and NDM-producers has been observed in the post-COVID-19 years in Greek hospitals [9,10].
Infections caused by CR-GNB have been proved to be a high priority problem of global health, since they are associated with high morbidity and mortality rates and remain a challenge for clinicians in daily practice [11]. Mortality rates of patients with blood stream infections (BSI) caused by CR-GNB, especially KPC-1 producers, have been reported to be as high as 53.2% [12]. Carbapenem-resistant P. aeruginosa mortality rates vary ranging from 6% to 32.8% [13,14]. The European Antimicrobial Resistance Surveillance Network (EARS-Net) in 2022 has reported a 49.7% increase in the incidence of carbapenem-resistant K. pneumoniae blood stream infections, compared to 2019 (3.26 cases per 100.000 population in 2022 vs. 2.18 cases per 100.000 population in 2019) [7].
Little is known about mortality rates caused by specific CR-GNB. Understanding the epidemiology, risk factors, outcomes, and the efficacy of existing treatment options is crucial for designing strategies to tackle the problem of CR-GNB in the clinical setting. The aim of this single-center retrospective, observational, real-life study was to analyze the epidemiology and outcomes, especially in-hospital mortality rates, of BSIs caused by NDM- and KPC-producing CR-GNB, as well as identify possible risk factors and efficacy of treatment options, in a high-prevalence setting.
2. Results
We identified 133 episodes of bacteremia due to KPC-and NDM-producing CR-GNB in 118 unique patients, with a mean age of 67.8±14.7 years. Among them 71 (60.2%) were male. Ten patients had more than one episode of bacteremia during their hospital stay. Seven patients had 2 episodes and two patients had 3 episodes of bacteremia. One patient had 5 distinct episodes of bacteremia from KPC-producing K. pneumoniae.
Of the 118 unique patients, 72 (61%) had BSI due to KPC-producing CR-GNB (all isolates belonged to the Enterobacteriaceae order) and 46 (39%) had NDM-producing CR-GNB isolated; among them 17/46 (37%) Pseudomonas isolates and 29/46 (63%) Enterobacteriaceae isolates. During the one-year study period, the occurrence rate of BSIs caused by NDM-producers was 0.31 per 1000 patient-days, whereas BSIs due to KPC-producing CR-GNB had a higher incidence rate of 0.49 per 1000 patient-days. The incidence of CR-GNB BSIs, including both KPC- and NDM-producers, reached a rate of 0.69 per 1000 patient-days.
Patient demographics and basic characteristics along with comparisons between the three types of isolates are shown on Table 1. Sixty-one out of the 118 study patients met the primary endpoint, yielding an overall crude in-hospital mortality of 51.7%. Overall, in-hospital mortality amongst patients with NDM-producing Pseudomonas was 70.6% compared to NDM-producing CR-GNB at 51.7% and KPC-producing CR-GNB at 47.2%, a difference not meeting statistical significance overall (p=0.222). Similarly, comparing in pairs NDM vs. KPC patients, overall, in-hospital mortality did not differ (51.7% vs 47.2% respectively, p=0.826), nor was there a difference between NDM-producing Pseudomonas and Enterobacterales patients (70.6% vs 51.7% respectively, p=0.235). Τhe 30-day, after the index culture, crude in-hospital mortality was 40.7%, with BSIs from NDM-producing P. aeruginosa having the highest mortality (47.1%). We also calculated the mortality rates of all NDM-producing CR-GNB and KPC-producing CR-GN and found similarly high rates (37% vs 26.4%, p=0.305)
We further attempted to identify risk factors predicting in-hospital mortality within the NDM and the KPC populations. Table 2 presents differences amongst survivors and non-survivors in the NDM group. In Cox-regression survival analysis, neither surgical ward admission (HR 0.72, 95%CI 0.21-2.52, p=0.608) nor ICU (HR 1.75, 95%CI 0.69-4.41, p=0.236) conferred greater risk of death compared to medical wards. Similarly in Cox-regression, central venous catheter (HR 2.8, 95%CI 0.63-12.37, p=0.174), foley catheter (HR 3.76, 95%CI 0.49-28.86, p=0.204), mechanical ventilation (HR 2.19, 95%CI 0.91-5.28, p=0.081) and previous ICU admission (HR 1.28, 95%CI 0.55-2.97, p=0.573) did not increase in-hospital mortality risk.
Differences amongst survivors and non-survivors in the KPC group are presented in Table 3. In cox-regression analysis, having a hospital-acquired infection did not increase in-hospital mortality risk (HR 1.89, 95%CI 0.57-6.31, p=0.3). Use of beta-lactam/beta-lactamase inhibitors (BLBLIs) in the KPC population, however, significantly reduced the risk of death (HR 0.21, 95%CI 0.1-0.43, p<0.001). Kaplan Meier survival function by BLBLI use (p=0.009) is displayed in Figure 1.
With regards to the 133 microbial isolates, 27 (17.3%) were P. aeruginosa and 110 (82.7%) Enterobacterales, mainly K. pneumoniae (106/110). Table 4 presents a comparison between the NDM-producing and KPC-producing isolates. Fourty-two of the 54 NDM-producing isolates (77.8%) were resistant to aztreonam; only one out of 17 (5.9%) Pseudomonas isolates was resistant to colistin.
3. Discussion
This retrospective study was designed and conducted to evaluate the incidence, in-hospital mortality, efficacy of therapeutic options and risk factors of BSIs caused by NDM- and KPC producing CR-GNB. We identified 79 episodes of BSIs due to KPC-producing and 54 episodes of BSIs due to NDM-producing CR-GNB during one year. We found that the incidence of BSIs linked to KPC-producers was higher compared to the incidence of BSIs caused by NDM-producing (P. aeruginosa and Enterobacteriaceae included) CR-GNB. Overall and 30-day, crude in-hospital mortality was observed to be higher amongst patients with BSIs due to NDM-producing P. aeruginosa compared to those with BSIs due to KPC- or NDM-producing Enterobacteriaceae, although the difference did not reach statistical significance. The use of BLBLI as monotherapy or in combination with other active agents was associated with better survival rates for patients with KPC-producing CR-GNB.
Our study showed relatively high incidence of BSIs caused by both KPC and NDM producers. The incidence of KPC-producers was comparatively higher (0.49 per 1000 patient-days), indicating an endemic status in our country, aligning with our existing knowledge [7,17]. Other studies conducted in Greek hospitals or hospitals in countries endemic for CREs have reported the incidence of BSIs caused by carbapenem-resistant K. pneumoniae to range from 0.092 to 0.59 per 1000 patient-days [18,19,20,21]. Here we report a similar, albeit lower, incidence of BSIs caused by NDM-producing CR-GNB, a finding suggesting that those difficult to treat pathogens became endemic as well. Our study is, to our knowledge, the first to document similar incidence of BSIs caused by NDM- and KPC- producing CR-GNB.
An important finding of our study is the high in-hospital mortality observed among study patients. BSIs due to both NDM- and KPC-producing CR-GNB exhibited high 30-day and overall, in-hospital crude mortality rates. Although not statistically significant, BSIs due to NDM-producing P. aeruginosa were associated with the highest mortality (overall crude in-hospital mortality 70.6% and 30-day in-hospital mortality 47.1%). Similarly, unacceptably high mortality rates have been reported by other researchers from endemic areas. In the ALARICO study, a prospective multicenter study conducted in Italy, a region endemic for CR-GNB, the 30-day mortality attributable to metallo-β-lactamase producing (MBL) Enterobacterales, (most of which were NDM-producers), and KPC-producing Enterobacterales, was 36.4% and 26.6% respectively [13]. In another prospective, observational 3-year study from Italy, 30-day mortality for MBL Enterobacterales was reported to be 29.7%, including NDM- and VIM-producers [22], emphasizing the need for early antimicrobial treatment with active agents to improve the outcomes. Our study reported similar, albeit higher, 30-day in-hospital mortality rates, possibly attributed to the limited availability of active antibiotics, the hospital’s high proportion of immunocompromised patients and inadequate implementation of infection control measures. Remarkably, 19 patients did not receive any active antibiotics, yet some survived possibly due to timely and efficient source control and better overall patient health status. Limited data are available for the mortality rates of BSIs caused by NDM-producing P. aeruginosa. Nevertheless, it is well established that carbapenem-resistant P. aeruginosa is a global threat with concerning levels of morbidity and mortality [13,14]. Our study is the first to report an overall crude mortality rate of BSIs due to NDM-producing P. aeruginosa as high as 70.6%.
In our risk factor analysis, we found that patients with BSIs caused by NDM-producers tended to be significantly older, whereas patients with BSIs due to KPC-producing CR-GNB were more likely to have an underlying malignancy. The length of stay before index culture was significantly lower in the NDM group (1 [0–6], p=0.011). This result, combined with older age, indicates that this group of patients tend to have more frequent previous hospitalizations or to be more often residents in long-term care facilities. In the NDM group, the Cox-regression survival analysis showed that risk factors for adverse outcomes were the presence of central venous catheter and/or urinary catheter, mechanical ventilation, and prior admission in the intensive care unit, albeit these factors, did not achieve statistical significance. Within the same group of patients, the use of one or two concomitant active agents did not result in better survival rates. Researchers have shown that ceftazidime-avibactam (CZA-AVI) in combination with aztreonam is an effective treatment for patients with MBL infections, leading to a reduction in mortality rates; hence this combination has been included in current guidelines as first line option [23,24,25,26,27]. Falcone and colleagues in Italy studied MBL infections in a prospective study spanning 3 years [22]. In this study, 345 patients with MBL infections were included, most of whom had BSI (199/345). The authors concluded that the combination of ceftazidime-avibactam plus aztreonam lowers mortality rates. In our study, we did not observe better outcomes for patients with BSIs due to NDM-producing CR-GNB, treated with one or two active antimicrobials, possibly due to the small number of cases included, the lack of aztreonam in our country, which restricted its administration in most cases, and the high in vitro resistance rates [42/54 (77.8%)] of NDM-producing strains to aztreonam.
Within the KPC group, most patients were treated with a BLBLI. Noteworthy is the fact that all KPC strains were found to be resistant to aztreonam. Compared to non-survivors, in the KPC group the use of BLBLIs has resulted in better survival rates (33/38 (86.8%) vs 20/34 (58.8%), p=0.009), which is consistent with current knowledge. Several prospective and retrospective studies have shown the efficacy of ceftazidime-avibactam as first-line therapy against KPC Enterobacterales [27,28,29,30]. The use of ceftazidime-avibactam has been documented to improve survival rates for most infections due to KPC-producing CR-GNB, apart from lower respiratory tract infections. Newer agents, such as meropenem/varbobactam and imipenem/relebactam have been used for CZA-AVI resistant strains [31,32], yielding favourable outcomes.
4. Materials and Methods
4.1. Study Design
This is a single-center, retrospective study conducted at the General Hospital of Athens Laiko, a 580-bed, university-affiliated, teaching hospital, serving the greater area of Athens. All consecutive adult patients, with confirmed BSI due to KPC- or NDM-producing CR-GNB, during a one-year period, from 1st January 2023 to 31st December 2023, were included in the study. Patients with polymicrobial BSIs caused by multiple GNB, or by a CR-GNB plus gram-positive bacteria or fungi were excluded. We retrospectively reviewed the electronic and/or chart files of the patients, and by using a preformed clinical report form we collected data including demographics, medical history and underlying diseases, laboratory parameters at the time when index cultures were drawn, length of stay in the hospital, microbiological data and outcomes. All retrieved data were entered in an electronic database for statistical analysis. The primary outcome was the 30-day and overall, in-hospital crude mortality rate for patients with BSIs caused by different categories of CR-GNB and the comparison of BSIs due to KPC-producing CR-GNB to BSIs due to NDM-producing CR-GNB. Secondary outcomes included length of stay in the hospital and BSI recurrence
4.2. Definitions
BSI was defined according to the Centers for Disease Control and Prevention/National Healthcare Safety Network criteria [16]. BSIs were considered as hospital-acquired when positive index cultures were drawn at least 48 hours after patient’s admission to the hospital or if patients had been hospitalized for any reason within the previous 7 days, in accordance with the ECDC definitions [7]. Antibiotic susceptibilities were measured by MicroScan autoSCAN-4 Microbiology System (Beckman Coulter; Brea, California, USA). KPC and/or NDM detection was performed using NG-Test Carba 5 (NG Biotech; Guipry, France), a rapid in vitro multiplex immunoassay. Medications used were considered active, if the isolated microorganism was susceptible to them. Patients were considered neutropenic when their neutrophil counts were < 1000 /mL and were described as hypogammaglobulinemic when their measured gamma globulin levels were below 7g/L. For patients with multiple episodes of bacteremia during the study period, we used the first recorded episode as the index case.
4.3. Statistical Analysis
Categorical variables are expressed by absolute values and relative frequencies. Continuous variables are measured by mean and standard deviation (SD), for normally distributed variables, or median and interquartile range (IQR), for non-normally distributed variables. Normality was tested with the Shapiro-Wilks test and equality of variances by Levene’s test. Group comparisons were performed using the Mann-Whitney U test for continuous non-normally distributed variables and Student’s t-test for normally distributed variables. Group comparisons for categorical variables were performed using the Chi-square and ANOVA tests. Survival analysis was carried out using Kaplan-Meier curves and univariable Cox regression. The level of statistical significance was set to <0.05. All statistical analysis was performed using the IBM SPSS Statistics for Windows, version 25.0 (2017, IBM Corp., Armonk, NY, USA).
Our study has limitations, with the most important being its retrospective nature. Additionally, the results should be read with caution given the small number of cases included in the study. Nevertheless, this is, to our knowledge, the first study to describe comparatively the occurrence and mortality rates of BSIs caused by NDM- and KPC-producers in our country.
5. Conclusions
In conclusion, in the present retrospective observational study spanning one year, we found high incidence of BSIs due to NDM- and KPC-producing CR-GNB. We observed a high mortality for both KPC- and NDM-producing CR-GBN with the highest in-hospital mortality observed amongst patients with NDM-producing P. aeruginosa. Given the limited availability of effective antibiotic agents and the rising resistance to existing treatment options in our country for NDM strains, the finding that using one or two active antibiotics for NDM producers does not yield significant differences is noteworthy. Finally, in this study we confirmed current knowledge about BLBLIs as the best available treatment option for BSIs due to KPC-producing CR-GNB.
Author Contributions
Conceptualization, M.N.G., N.V.S. and E.A.A.; methodology, N.V.S. and M.N.G.; validation, M.N.G.; formal analysis, D.B.; investigation, E.A.A., S.Z., I.D., A.P., A.M., A.K.; resources, N.V.S.; writing—original draft preparation, E.A.A., D.B., N.V.S. and M.N.G.; writing—review and editing, E.A.A., M.N.G. and N.V.S.; supervision, M.N.G. and N.V.S. All authors have read and agreed to the submitted version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and National and institutional standards. The study has been approved by the internal review board of the Laiko Hospital, Athens, Greece (protocol code 5436 and 17 December 2022).
Informed Consent Statement
Patient consent was waived due to the non-interventional nature of the study.
Data Availability Statement
Raw data supporting the conclusions of this article will be made available by the authors, without undue reservation, to any qualified researcher, upon request.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
CR-GNB: carbapenem-resistant gram-negative bacilli, BSI: blood stream infections, KPC: Klebsiella pneumoniae carbapenemase, NDM: New-Delhi metallo-β-lactamase, MBL: metallo-β-lactamases, BLBLI: beta-lactam/beta-lactamase inhibitors, CZA/AVI: ceftazidime/avibactam
References
- Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022 Feb 12;399(10325):629-655. [CrossRef]
- Yigit, Hesna, et al. "Novel carbapenem-hydrolyzing β-lactamase, KPC-1, from a carbapenem-resistant strain of Klebsiella pneumoniae." Antimicrobial Agents and Chemotherapy 45.4 (2001): 1151-1161.
- Lee, Chang-Ro et al. “Global Dissemination of Carbapenemase-Producing Klebsiella pneumoniae: Epidemiology, Genetic Context, Treatment Options, and Detection Methods.” Frontiers in microbiology vol. 7 895. 13 Jun. 2016. [CrossRef]
- Voulgari, Evangelia, et al. "The Balkan region: NDM-1-producing Klebsiella pneumoniae ST11 clonal strain causing outbreaks in Greece." Journal of Antimicrobial Chemotherapy 69.8 (2014): 2091-2097.
- Spyropoulou, Aikaterini, et al. "The first NDM metallo-β-lactamase producing Klebsiella pneumoniae isolate in a University Hospital of Southwestern Greece." Journal of Chemotherapy 28.4 (2016): 350-351.
- Robert A Bonomo, Eileen M Burd, John Conly, Brandi M Limbago, Laurent Poirel, Julie A Segre, Lars F Westblade, Carbapenemase-Producing Organisms: A Global Scourge, Clinical Infectious Diseases, Volume 66, Issue 8, 15 April 2018, Pages 1290–1297.
- European Centre for Disease Prevention and Control. Antimicrobial resistance in the EU/EEA (EARS-Net) - Annual Epidemiological Report 2022. Stockholm: ECDC; 2023.
- Giakkoupi P, Tryfinopoulou K, Kontopidou F, Tsonou P, Golegou T, Souki H, Tzouvelekis L, Miriagou V, Vatopoulos A. Emergence of NDM-producing Klebsiella pneumoniae in Greece. Diagn Microbiol Infect Dis. 2013 Dec;77(4):382-4. [CrossRef]
- Polemis M, Mandilara G, Pappa O, et al. COVID-19 and Antimicrobial Resistance: Data from the Greek Electronic System for the Surveillance of Antimicrobial Resistance-WHONET-Greece (January 2018-March 2021). Life (Basel). 2021 Sep 22;11(10):996. [CrossRef]
- Tryfinopoulou K, Linkevicius M, Pappa O, Alm E, Karadimas K, Svartström O, Polemis M, Mellou K, Maragkos A, Brolund A, Fröding I, David S, Vatopoulos A, Palm D, Monnet DL, Zaoutis T, Kohlenberg A; Greek CCRE study group; Members of the Greek CCRE study group. Emergence and persistent spread of carbapenemase-producing Klebsiella pneumoniae high-risk clones in Greek hospitals, 2013 to 2022. Euro Surveill. 2023 Nov;28(47):2300571. [CrossRef]
- The Lancet. Antimicrobial resistance: an agenda for all. Lancet. 2024 Jun 1;403(10442):2349. [CrossRef]
- Wang, Minggui et al. “Clinical outcomes and bacterial characteristics of carbapenem-resistant Klebsiella pneumoniae complex among patients from different global regions (CRACKLE-2): a prospective, multicentre, cohort study.” The Lancet. Infectious diseases vol. 22,3 (2022): 401-412. [CrossRef]
- Falcone M, Tiseo G, Carbonara S, et al. Mortality Attributable to Bloodstream Infections Caused by Different Carbapenem-Resistant Gram-Negative Bacilli: Results From a Nationwide Study in Italy (ALARICO Network). Clin Infect Dis. 2023;76(12):2059-2069. [CrossRef]
- Reyes J, Komarow L, Chen L, et al. Global epidemiology and clinical outcomes of carbapenem-resistant Pseudomonas aeruginosa and associated carbapenemases (POP): a prospective cohort study. Lancet Microbe. 2023;4(3):e159-e170. [CrossRef]
- Baek, M.S., Kim, J.H., Park, J.H. et al. Comparison of mortality rates in patients with carbapenem-resistant Enterobacterales bacteremia according to carbapenemase production: a multicenter propensity-score matched study. Sci Rep 14, 597 (2024). [CrossRef]
- CDC/NHSN surveillance definitions for specific types of infections. Available at: https://www.cdc.gov/nhsn/PDFs/pscManual/17pscNosInfDef_current.pdf. Accessed 1 December 2023.
- Protonotariou, Efthymia et al. “Polyclonal Endemicity of Carbapenemase-Producing Klebsiella pneumoniae in ICUs of a Greek Tertiary Care Hospital.” Antibiotics (Basel, Switzerland) vol. 11,2 149. 25 Jan. 2022. [CrossRef]
- Iacchini, Simone et al. “Bloodstream infections due to carbapenemase-producing Enterobacteriaceae in Italy: results from nationwide surveillance, 2014 to 2017.” Euro surveillance : bulletin Europeen sur les maladies transmissibles = European communicable disease bulletin vol. 24,5 (2019): 1800159. [CrossRef]
- Cristina ML, Alicino C, Sartini M, et al. Epidemiology, management, and outcome of carbapenem-resistant Klebsiella pneumoniae bloodstream infections in hospitals within the same endemic metropolitan area. J Infect Public Health. 2018;11(2):171-177. [CrossRef]
- Alicino C, Giacobbe DR, Orsi A, et al. Trends in the annual incidence of carbapenem-resistant Klebsiella pneumoniae bloodstream infections: a 8-year retrospective study in a large teaching hospital in northern Italy. BMC Infect Dis. 2015;15:415. Published 2015 Oct 13. [CrossRef]
- Papadimitriou-Olivgeris M, Bartzavali C, Karachalias E, et al. A Seven-Year Microbiological and Molecular Study of Bacteremias Due to Carbapenemase-Producing Klebsiella Pneumoniae: An Interrupted Time-Series Analysis of Changes in the Carbapenemase Gene's Distribution after Introduction of Ceftazidime/Avibactam. Antibiotics (Basel). 2022;11(10):1414. Published 2022 Oct 14. [CrossRef]
- Falcone M, Giordano C, Leonildi A, et al. Clinical features and outcomes of infections caused by metallo-β-lactamases producing Enterobacterales: a 3-year prospective study from an endemic area. Clin Infect Dis. Published online November 30, 2023. [CrossRef]
- Falcone M, Daikos GL, Tiseo G, et al. Efficacy of Ceftazidime-avibactam Plus Aztreonam in Patients With Bloodstream Infections Caused by Metallo-β-lactamase-Producing Enterobacterales. Clin Infect Dis. 2021;72(11):1871-1878. [CrossRef]
- Paul M, Carrara E, Retamar P, et al. European Society of Clinical Microbiology and Infectious Diseases (ESCMID) guidelines for the treatment of infections caused by multidrug-resistant gram-negative bacilli (endorsed by European Society of Intensive Care Medicine). Clin Microbiol Infect 2022; 28:521–47.
- Tamma PD, Aitken SL, Bonomo RA, Mathers AJ, van Duin D, Clancy CJ. Infectious Diseases Society of America 2023 guidance on the treatment of antimicrobial resistant gram-negative infections. Clin Infect Dis 2023. [CrossRef]
- Tiseo G, Brigante G, Giacobbe DR, et al. Diagnosis and management of infections caused by multidrug-resistant bacteria: guideline endorsed by the Italian Society of Infection and Tropical diseases (SIMIT), the Italian Society of Anti-infective Therapy (SITA), the Italian Group for Antimicrobial stewardship (GISA), the Italian Association of Clinical Microbiologists (AMCLI) and the Italian Society of Microbiology (SIM). Int J Antimicrob Agents 2022; 60:106611.
- Shields RK, Nguyen MH, Chen L, et al. Ceftazidime-avibactam is superior to other treatment regimens against carbapenem-resistant Klebsiella pneumoniae bacteremia. Antimicrob Agents Chemother 2017; 61:8.
- van Duin D, Lok JJ, Earley M, et al. ; Antibacterial Resistance Leadership Group. Colistin versus ceftazidime-avibactam in the treatment of infections due to carbapenem-resistant Enterobacteriaceae. Clin Infect Dis 2018; 66:163–71.
- Jorgensen SCJ, Trinh TD, Zasowski EJ, et al. Real-world experience with ceftazidime-avibactam for multidrug-resistant gram-negative bacterial infections. Open Forum Infect Dis 2019; 6:ofz522.
- Tumbarello M, Raffaelli F, Giannella M, et al. Ceftazidime-Avibactam Use for Klebsiella pneumoniae Carbapenemase-Producing K. pneumoniae Infections: A Retrospective Observational Multicenter Study. Clin Infect Dis. 2021;73(9):1664-1676. [CrossRef]
- Papp-Wallace KM, Barnes MD, Taracila MA, et al. The Effectiveness of Imipenem-Relebactam against Ceftazidime-Avibactam Resistant Variants of the KPC-2 β-Lactamase. Antibiotics (Basel). 2023;12(5):892. Published 2023 May 11. [CrossRef]
- Shields RK, McCreary EK, Marini RVet al.. Early experience with meropenem-vaborbactam for treatment of carbapenem-resistant Enterobacteriaceae infections. Clin Infect Dis 2020; 71: 667–71.
Figure 1.
Kaplan Meier survival analysis in the Klebsiella pneumoniae carbapenemase population by use of beta-lactam/beta-lactamase inhibitor, p=0.009.
Figure 1.
Kaplan Meier survival analysis in the Klebsiella pneumoniae carbapenemase population by use of beta-lactam/beta-lactamase inhibitor, p=0.009.
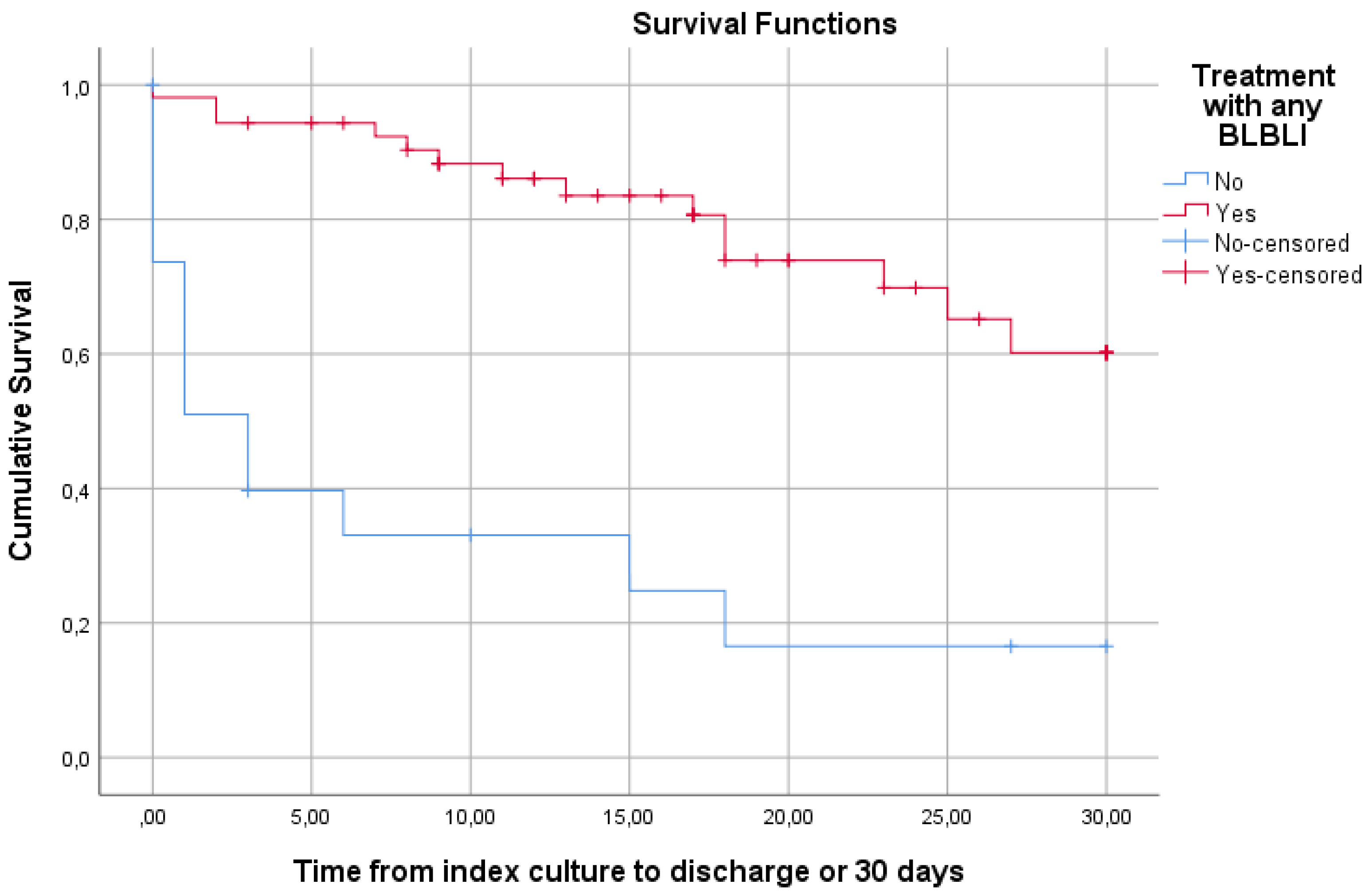

Table 1.
Basic characteristics of study participants and comparison between the three types of bacterial isolates.
Table 1.
Basic characteristics of study participants and comparison between the three types of bacterial isolates.
| Total N=118 |
Pseudomonas NDM N=17 |
CREs NDM N=29 |
CREs KPC N=72 |
P | ||
|---|---|---|---|---|---|---|
| Male gender | 71 (60.2) | 9 (52.9) | 20 (69) | 42 (58.3) | 0.495 | |
| Age (years) | 67.8±14.7 | 73.1±13.8 | 73±15.7 | 64.5±13.7 | 0.009 | |
| Cancer history | 53 (44.9) | 3 (17.6) | 9 (31) | 41 (56.9) | 0.003 | |
| LOS before index culture (days) | 7 [1–19] | 11 [1–20] | 1 [0–6] | 12 [2–25] | 0.011 | |
| Ward | 0.031 | |||||
| Medical | 88 (74.6) | 11 (64.7) | 23 (79.3) | 54 (75) | ||
| Surgical | 19 (16.1) | 1 (5.9) | 4 (13.8) | 14 (19.4) | ||
| ICU | 11 (9.3) | 5 (29.4) | 2 (6.9) | 4 (5.5) | ||
| Hospital acquired infection | 93 (78.8) | 2 (11.8) | 20 (69) | 58 (80.6) | 0.257 | |
| Central venous catheter | 65 (55.1) | 10 (71.4) | 14 (70) | 41 (71.9) | 0.987 | |
| Foley catheter | 67 (56.8) | 13 (92.9) | 15 (75) | 39 (68.4) | 0.175 | |
| Mechanical ventilation | 14 (11.9) | 5 (33.3) | 4 (20) | 5 (8.5) | 0.042 | |
| Previously in ICU | 20 (16.9) | 6 (35.3) | 4 (13.8) | 10 (13.9) | 0.093 | |
| Antibiotic resistance | ||||||
| Colistin | 37 (31.4) | 1 (5.9) | 15 (51.7) | 21 (29.2) | 0.004 | |
| Meropenem | 116 (98.3) | 17 (100) | 28 (96.6) | 71 (98.6) | 0.648 | |
| Aztreonam | 107 (90.7) | 10 (58.8) | 25 (86.2) | 72 (100) | <0.001 | |
| Treatment | ||||||
| Colimycin | 57 (48.3) | 15 (88.2) | 19 (65.5) | 23 (31.9) | <0.001 | |
| Ceftolozane/ tazobactam | 3 (2.5) | 1 (5.9) | 1 (3.4) | 1 (1.4) | 0.536 | |
| Meropenem | 20 (16.9) | 7 (41.2) | 7 (24.1) | 6 (8.3) | 0.003 | |
| Ceftazidime/ avibactam | 49 (41.5) | 3 (17.6) | 1 (3.4) | 45 (62.5) | <0.001 | |
| Meropenem/ vaborbactam | 10 (8.5) | 0 (0) | 2 (6.9) | 8 (11.1) | 0.315 | |
| Imipenem/ relebactam | 5 (4.2) | 1 (5.9) | 3 (10.3) | 1 (1.4) | 0.121 | |
| Tigecycline | 15 (12.7) | 1 (5.9) | 7 (24.1) | 7 (9.7) | 0.095 | |
| Active Drugs | 0.001 | |||||
| None | 28 (23.7) | 2 (11.8) | 14 (48.3) | 12 (16.7) | ||
| One | 71 (60.2) | 15 (88.2) | 10 (34.5) | 46 (63.9) | ||
| Two | 19 (16.1) | 0 (0) | 5 (17.2) | 14 (19.4) | ||
| Laboratory values | ||||||
| White blood cells (103/μl) | 8.1 [3-16.2] | 8.2 [4-16.4] | 11.9 [5.2-22.1] | 7.3 [1.4-13.4] | 0.071 | |
| Neutrophils (103/μl) | 6.7 [2.2-14.2] | 6.6 [2.4-14.6] | 11.2 [4.5-18] | 5.6 [1-12.3] | 0.067 | |
| Neutropenia | 23 (19.5) | 2 (11.8) | 3 (10.3) | 18 (25) | 0.167 | |
| Gamma globulins (g/l) | 9.8 [6.8-13] | 10 [7.7-12] | 10 [6.7-16] | 9.7 [6.1-13] | 0.713 | |
| Hypogamma-globulinemia | 24 (20.3) | 1 (11.1) | 6 (31.6) | 17 (31.5) | 0.447 | |
| Albumin (g/l) | 27.1 [22.9-32.3] | 27.3 [23.8-33] | 26.8 [23-33.9] | 27.1 [22.2-32] | 0.845 | |
| Recurrence of Bacteremia | 10 (8.5) | 2 (11.8) | 2 (6.9) | 6 (8.3) | 0.847 | |
| LOS after culture (days) | 13 [3–24] | 14 [4–31] | 12 [3–26] | 14 [5-24] | 0.976 | |
| Total LOS (days) | 24 [12-43] | 23 [15-49] | 18 [9-37] | 25 [13-46] | 0.523 | |
| In-hospital mortality | 61 (51.7) | 12 (70.6) | 15 (51.7) | 34 (47.2) | 0.222 | |
| 30-day mortality | 48 (40.7) | 8 (47.1) | 12 (41.4) | 28 (38.9) | 0.824 | |
Data is presented as N (%) or mean±SD or median [IQR 25-75]. P-values in bold denote statistical significance. LOS: length of stay, ICU: Intensive Care Unit,.
Table 2.
Comparison between survivors and non-survivors in the NDM population.
| Survivors N=19 |
Non-Survivors N=27 | p | |
|---|---|---|---|
| Male gender | 12 (63.2) | 17 (63) | 1 |
| Age (years) | 74.5±15.2 | 72±14.9 | 0.579 |
| Cancer history | 7 (36.8) | 5 (18.5) | 0.19 |
| LOS before index culture (days) | 1 [0-8] | 4 [1-15] | 0.261 |
| Ward | 0.05 | ||
| Medical | 17 (89.5) | 17 (63) | |
| Surgical | 2 (10.5) | 3 (11.1) | |
| ICU | 0 (0) | 7 (25.9) | |
| Hospital acquired infection | 13 (68.4) | 22 (81.5) | 0.484 |
| Central venous catheter | 5 (38.5) | 19 (90.5) | 0.002 |
| Foley catheter | 7 (58.3) | 21 (95.5) | 0.014 |
| Mechanical ventilation | 0 (0) | 9 (40.9) | 0.013 |
| Previously in ICU | 1 (5.3) | 9 (33.3) | 0.031 |
| Bacterial isolate | 0.235 | ||
| Pseudomonas | 5 (26.3) | 12 (44.4) | |
| Enterobacterales | 14 (73.7) | 15 (55.6) | |
| Antibiotic resistance | |||
| Colistin | 8 (42.1) | 8 (29.6) | 0.531 |
| Meropenem | 19 (100) | 26 (96.3) | 1 |
| Aztreonam | 11 (57.9) | 24 (88.9) | 0.032 |
| Treatment | |||
| Colimycin | 14 (73.7) | 20 (74.1) | 1 |
| Ceftolozane/ tazobactam | 1 (5.3) | 1 (3.7) | 1 |
| Meropenem | 5 (26.3) | 9 (33.3) | 0.749 |
| Ceftazidime/ avibactam | 2 (10.5) | 2 (7.4) | 1 |
| Meropenem/ vaborbactam | 0 (0) | 2 (7.4) | 0.504 |
| Imipenem/ relebactam | 1 (5.3) | 3 (11.1) | 0.632 |
| Tigecycline | 3 (15.8) | 5 (18.5) | 1 |
| Active Drugs | 0.970 | ||
| None | 7 (36.8) | 9 (33.3) | |
| One | 10 (52.6) | 15 (55.6) | |
| Two | 2 (10.5) | 3 (11.1) | |
| Laboratory values | |||
| White blood cells (103/μl) | 9.9 [5.1-18.1] | 10.3 [4.2-20.5] | 0.885 |
| Neutrophils (103/μl) | 8.6 [4.5-15.9] | 8.6 [2.5-17.9] | 0.964 |
| Neutropenia | 1 (5.3) | 4 (14.8) | 0.387 |
| Gamma globulins (g/l) | 11 [6.6-13.3] | 9.6 [7.2-20] | 0.872 |
| Hypogammaglobulinemia | 4 (28.6) | 3 (21.4) | 1 |
| Albumin (g/l) | 31.3 [24.3-36.6] | 25.3 [22.4-29.5] | 0.029 |
| Recurrence of Bacteremia | 1 (5.3) | 3 (11.1) | 0.632 |
| LOS after culture (days) | 16 [10-21] | 9 [2-33] | 0.32 |
| Total LOS (days) | 20 [10-33] | 23 [12-63] | 0.482 |
Data is presented as N (%) or mean±SD or median [IQR 25-75]. P-values in bold denote statistical significance. LOS: length of stay, ICU: Intensive Care Unit.
Table 3.
Comparison between survivors and non-survivors in the KPC population.
| Survivors N=38 |
Non-Survivors N=34 | p | |
|---|---|---|---|
| Male gender | 21 (55.3) | 21 (61.8) | 0.637 |
| Age (years) | 62.7±11.3 | 66.5±15.9 | 0.244 |
| Cancer history | 21 (55.3) | 20 (58.8) | 0.815 |
| LOS before index culture (days) | 9 [1-18] | 13 [4-31] | 0.057 |
| Ward | 0.186 | ||
| Medical | 27 (71.1) | 27 (79.4) | |
| Surgical | 10 (26.3) | 4 (11.8) | |
| ICU | 1 (2.6) | 3 (8.8) | |
| Hospital acquired infection | 27 (71.1) | 31 (91.2) | 0.039 |
| Central venous catheter | 16 (59.3) | 25 (83.3) | 0.075 |
| Foley catheter | 15 (55.6) | 24 (80) | 0.086 |
| Mechanical ventilation | 1 (3.7) | 4 (12.5) | 0.362 |
| Previously in ICU | 5 (13.2) | 5 (14.7) | 1 |
| Antibiotic resistance | |||
| Colistin | 8 (21.1) | 13 (38.2) | 0.127 |
| Meropenem | 38 (100) | 33 (97.1) | 0.472 |
| Treatment | |||
| Colimycin | 9 (23.7) | 14 (41.2) | 0.134 |
| Ceftolozane/tazobactam | 1 (2.6) | 0 (0) | 1 |
| Meropenem | 3 (7.9) | 3 (8.8) | 1 |
| Ceftazidime/avibactam | 30 (78.9) | 15 (44.1) | 0.003 |
| Meropenem/vaborbactam | 4 (10.5) | 4 (11.8) | 1 |
| Imipenem/ relebactam | 0 (0) | 1 (2.9) | 0.472 |
| Tigecycline | 2 (5.3) | 5 (14.7) | 0.243 |
| Any BLBLI | 33 (86.8) | 20 (58.8) | 0.009 |
| Active Drugs | 0.083 | ||
| None | 3 (7.9) | 9 (26.5) | |
| One | 28 (73.7) | 18 (52.9) | |
| Two | 7 (18.4) | 7 (20.6) | |
| BLBLI monotherapy | 27 (81.8) | 13 (65) | 0.2 |
| Laboratory values | |||
| White blood cells (103/μl) | 8.2 [4.6-12.2] | 4.8 [0.8-15.4] | 0.391 |
| Neutrophils (103/μl) | 6.7 [3.4-10.9] | 3.9 [0.5-14.2] | 0.369 |
| Neutropenia | 7 (18.4) | 11 (32.4) | 0.188 |
| Gamma globulins (g/l) | 10.5 [8.1-17] | 8.3 [5.9-11] | 0.098 |
| Hypogammaglobulinemia | 5 (19.2) | 12 (42.9) | 0.082 |
| Albumin (g/l) | 30 [24.1-33.7] | 24.1 [20.4-30.8] | 0.011 |
| Recurrence of Bacteremia | 3 (7.9) | 3 (8.8) | 1 |
| LOS after culture (days) | 17 [10-25] | 9 [1-24] | 0.045 |
| Length of stay (days) | 23 [17-33] | 28 [9-55] | 0.743 |
Data is presented as N (%) or mean±SD or median [IQR 25-75]. P-values in bold denote statistical significance. LOS: length of stay, ICU: Intensive Care Unit, BLBLI: beta-lactam/beta-lactamase inhibitor.
| NDM N=54(%) | KPC N=79(%) | p | ||
|---|---|---|---|---|
| Microbes | <0.001 | |||
| P. aeruginosa | 23 (42.6) | 0 (0) | ||
| K. pneumoniae | 30 (55.6) | 76 (95.2) | ||
| E. coli | 1 (1.9) | 2 (2.5) | ||
| K. aerogenes | 0 (0) | 1 (1.3) | ||
| Antibiotic resistance | ||||
| Colistin | 17 (31.5) | 22 (27.8) | 0.7 | |
| Meropenem | 53 (98.1) | 78 (98.7) | 1 | |
| Aztreonam | 42 (77.8) | 79 (100) | <0.001 | |
P-values in bold denote statistical significance.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



