Submitted:
12 January 2026
Posted:
13 January 2026
You are already at the latest version
Abstract
Background/Objectives: Neurodegenerative diseases (NDs) have a severe impact on patients’ quality of life, and effective treatments remain limited. As the focus is treating the symptoms, the root cause of the problem e commonly not addressed. Stem cells show an emerging potential due to the ability for self-renew combined with their ca-pability for differentiation into various cell lines, which makes them a strong candidate to regenerative therapies in general, and for application in neurological issues in par-ticular. This article provides an overview on the safety, efficacy and challenges associ-ated with the use of mesenchymal stem cells (MSCs), their derived secre-tome/exosomes and their combination with biomaterials in clinical and preclinical models of Alzheimer’s disease (AD), Parkinson’s disease (PD), Huntington’s disease (HD), amyotrophic lateral sclerosis (ALS) and multiple sclerosis (MS). Methods: A systematic search was conducted on PubMed, Web of Science and Scopus to identify published studies providing clinical and preclinical evidence on the use of MSCs in neurodegenerative disorders. Results: Overall, the literature consistently indicates that MSCs and their derivatives exert disease-modifying effects across multiple NDs. Across AD, PD, HD and ALS, preclinical studies uniformly report improvements in behavioural outcomes, attenuation of neuroinflammation, and neuroprotective effects, largely mediated by MSC paracrine signalling rather than direct cell replacement. Clinical studies to date consistently support the safety and feasibility of MSC-based therapies, while efficacy signals remain modest, heterogeneous and predominantly short-term, highlighting the need for larger, well-controlled trials. Conclusions: Inte-gration of genetic engineering, preconditioning, and EV technology may represent a paradigm shift in neuroregeneration, offering a scalable and minimally invasive fron-tier to improve long-term clinical outcomes in patients with AD, PD, HD, and ALS.
Keywords:
biomaterials
; exosomes
; mesenchymal stem cells
; neurodegenerative diseases
; regenerative medicine
; secretome
1. Introduction
Neurodegenerative diseases such as Alzheimer’s disease (AD), Parkinson’s disease (PD), Huntington’s disease (HD) and Amyotrophic Lateral Sclerosis (ALS) represent a significant and growing burden on global healthcare systems, affecting millions of individuals by imposing substantial challenges to their quality of life, functional independence, and overall mortality rates [1,2,3]. This range of diseases span an acute-to-chronic spectrum and affect particularly the central nervous system (CNS) — brain (cerebrum, cerebellum and brainstem), retina and spinal cord, the main organs responsible for processing all the primary body’s functions [4,5]. This system is composed of two major cellular compartments: neurons and glial cells. Neurons are electrically active cells, responsible for the generation and propagation of action potentials [6], creating a highly synchronized synaptic network that ensures cognitive, motor and sensory functions. Their function is supported by glial cells — astrocytes, microglia, oligodendrocytes and NG2 glia — which provide metabolic balance, immune surveillance and myelination to ensure rapid conduction of nervous impulses [7]. All these cells are fully interconnected in functional and physiological terms, and therefore any change in one of these cells mat affect others [8].
Neurodegenerative diseases share common pathophysiological mechanisms that result in progressive and irreversible neuronal dysfunction in different CNS regions. While the abnormal aggregation and accumulation of misfolded proteins represents a central hallmark for NDs, additional processes can be involved in their pathogenesis. The specific clinical phenotype derives from the type of protein involved and the particular brain regions where the protein aggregation predominates [9]. The accumulation of misfolded protein results in neuronal homeostasis disruption, associated with mitochondrial dysfunction, increased production of reactive oxidative species (ROS) and oxidative stress, ultimately damaging key cellular components such as lipids, proteins and DNA [10]. Consequently, the gradual deterioration of neurons and glial cells in these tissues leads to a loss of specific neurological functions, such as memory, movement and cognition [4]. Beyond the cerebral consequences, neurodegeneration can also affect other regions of CNS, producing characteristic functional deficits: in the cerebellum, neurodegeneration is primarily associated to motor dysfunction as well as cognitive and affective disturbances. Even though cerebellar involvement is not considered the main pathological feature in AD and PD, cerebellar atrophy [11,12] has been linked to motor and cognitive impairment, including deficits in learning, working memory and emotional dysregulation [13,14]. In the retina, this can cause vison loss and blindness [15], while in the spinal cord, it reflects in motor, sensory and autonomic dysfunction. After injury or conditions like ALS, there is progressive atrophy, demyelination and neuronal loss, leading to muscle weakness, paralysis and neuropathic pain [16,17].
For AD, conventional treatments include cholinesterase inhibitors and memantine, which are responsible for symptom attenuation but not for halting disease progression [18].
In PD cases, the gold standard therapy goes to Levodopa (L-DOPA), a metabolic precursor of dopamine in the brain, that is commonly combined with carbidopa for an increased bioavailability and therapeutic efficacy. Dopamine agonists or MAO-I inhibitors are also an option; however, they do not reverse or slow down the disease progress. [19]
Tetrabenazine is one of the first drugs to be used to control involuntary and jerky movements present in HD patients. This treatment is associated with significant side effects and does not halt disease progression. Other drugs, such as deutetrabenazine, a tetrabenazine analogue, have been introduced to achieve similar therapeutic goals, limiting their side effects [18], however it is still not ideal.
While some of these conditions are congenital, aging is considered a significant risk factor to their emergence and progress rate. Moreover, these diseases can progress to a state of dementia, which is expected to affect 150 million people globally by 2050 [2,20].
Although existing, available treatments are mainly supportive and focus on managing the symptoms and improving the patients’ quality of life. Effective therapies remain limited when it comes to underlying cause of the problem. This is due, in part, to the fact that the precise etiology of many neurological conditions remains unknown, limiting the potential to develop effective targeted therapies [21].
Given these challenges, stem cells have emerged as a promising area of research due to their remarkable therapeutic potential [22].
Mesenchymal stem cells (MSCs) are a promising strategy to restore homeostasis, promote neuroregeneration, and slow disease progression across a broad spectrum of neurodegenerative disorders, since they’re capable of healing and reducing inflammation in various tissues [23]. MSCs are multipotent stromal cells widely distributed in the body with good availability and ease of collection, isolation and in vitro culture, capable of being harvested from readily available sources such as autologous and allogenic bone marrow (BM-MSCs) and adipose tissue (A-MSCs), making them even more clinically desirable. They can also be isolated from human umbilical cord blood (hUCB-MSCs), dental pulp (DPSCs), placenta and peripheral blood (Figure 1) [24], among other tissues. Despite early evidence of MSC differentiation and cell replacement, recent studies suggest MSCs differ from other types of stem cells by their paracrine effects — extracellular vesicles (EVs), cytokines and growth factors — migration ability and immune response modification (immunomodulation) (Figure 1) [25]. Using autologous MSCs minimizes the risk of immunological rejection, even though allogenic MSCs are still used, since there is not a significant risk of immunogenicity associated with these cells [24]. MSCs and their derivates, such as the secretome and its components have therefore gained considerable attention, as their use has demonstrated promising results in several areas, including neurodegenerative diseases [26]. The secretome includes a variety of molecules such as cytokines, growth factors and microRNAs (miRNAs) which, in most cases, can be packaged into the EVs, allowing the preservation of the therapeutic characteristics of the MSCs, including angiogenesis promotion and effective tissue repair [4]. EVs are considered promising tools in this type of treatment, as they show an increased potential to cross blood-brain barrier (BBB), thereby enhancing the delivery efficiency and consequently their therapeutic effect within the CNS [27]. However, this crossing is influenced by multiple factors, such as cellular origin, size, surface charge, molecular composition and route of administration, remaining partially understood [28,29,30]. These mechanisms of action can be transferred and supported by ND models, validating their treatment potential as MSCs’ neuroregenerative, neuroprotective, and immunomodulatory properties are essential in the context of NDs. [4]. The main MSCs’ mechanisms within NDs encompass neuroinflammation reduction, fostering neuron survival in AD, the release of neurotrophic and immunomodulatory factors that support dopaminergic neuron survival and function in PD and stimulation of neurotropic, immunoregulatory, antioxidant, and antiapoptotic pathways in HD, for example [31]. The combination of multimodal biological efficacy, favourable safety profile, and logistical accessibility positions MSCs and their derived secretome or EVs as a highly desirable source in the quest for effective treatments for NDs.
In this systematic review, research advances, safety, efficacy and related adverse events will be discussed within the use of MSC therapies for NDs based on the data published in the literature.
2. MSC’s Therapies for Specific Neurological Disorders
Recent studies have been conducted to find effective therapeutic solutions for the treatment of ND using stem cells, due to their self-renewal, self-replicating, regenerative and differentiation capabilities [32].
2.1. Alzheimer’s Disease (AD)
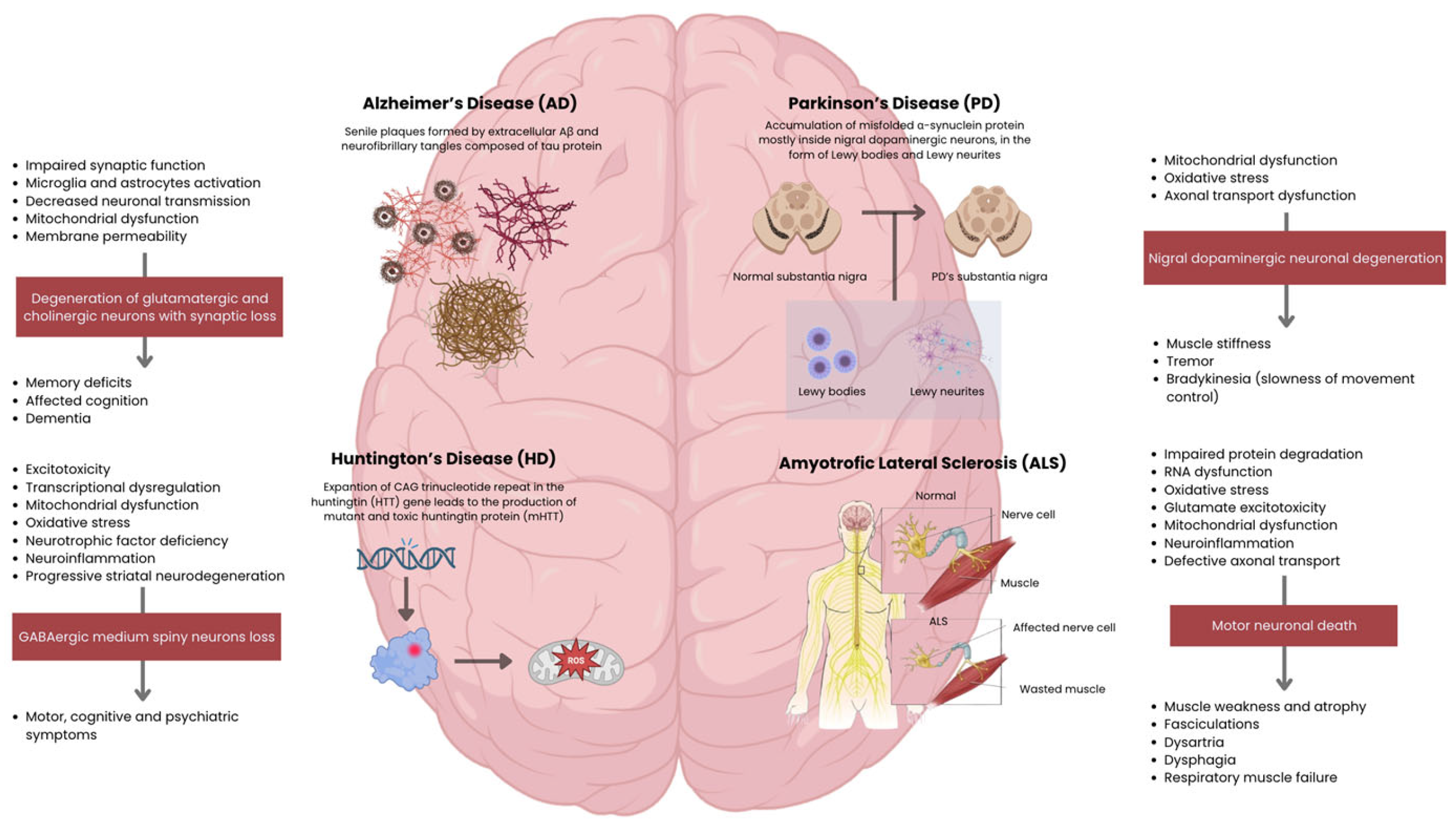
AD is one of the most prevalent types of NDs, mostly affecting the aging population. Clinically, AD is associated with dementia, characterized by a progressive loss of memory and impairment of one or more cognitive domains. Degeneration primarily affects hippocampal and cortical neurons, including glutamatergic and cholinergic populations, leading to memory loss and cognitive decline (Figure 2) [33,34].
Current evidence from pre-clinical and clinical studies suggests amyloid-β peptide (Aβ and tau protein) as the central contributor to AD pathophysiology [35]. Their deposition into insoluble states in determined histopathological brain structures — senile plaques formed by extracellular Aβ (between neuronal connections) and neurofibrillary tangles (NFTs) composed of intracellular tau — is a mark of more advanced disease. As Aβ aggregates into insoluble plaques between neurons, synaptic communication is compromised by neurotransmission impairment [36]. Beyond this mechanical disruption, Aβ plaques act as potent activators of the innate immune system. Microglia and astrocytes recognize them as a danger signal and attempt to clear the plaques, but their sustained activation leads to chronic neuroinflammation. This inflammatory state exacerbates neuronal damage through the release of inflammatory cytokines, ROS, and other neurotoxic mediators (Figure 2). Thus, Aβ accumulation contributes both to synaptic failure and to a self-perpetuating inflammatory cycle that accelerates neurodegeneration in AD [37]. Moreover, soluble and scattered forms of Aβ and tau — especially, their oligomer forms — can be also responsible for significant neurotoxic effects [38]. These small and mobile species can diffuse trough the extracellular space and cross neuronal membranes and synapses [39]. Because they are soluble and not stagnant, these molecules can interact directly with neurons and synapses, causing synaptic dysfunction through changes in neurotransmitter release [40], disruption of neuronal membranes by increasing their permeability, mitochondrial dysfunction within neurons [41], and neuroinflammation due to the circulation of foreign molecules detected by microglia and astrocytes, enhancing the inflammatory response (Figure 2) [42].
Current therapies are based on symptomatic relief rather than underlying the main root of this neurological disorder. Attempted therapeutics aiming the reduction of Aβ levels have proved unsuccessful. Similarly, tau-based clinical trials have not yet yielded positive results [43].
Studies utilizing various sources of MSCs — BM-MSCs, hUCB-MSCs and A-MSCs — demonstrated significant therapeutic effects across multiple pathological hallmarks of AD [44,45,46].
Preclinical studies have shown that MSCs and their derivatives can improve cognitive function and reduce AD pathology in animal models. For instance, MSC-derived EVs administered intranasally to mice led to better memory performance and reduced amyloid-beta plaque burden [47]. Other animal studies in mice models confirm that MSCs can decrease neuroinflammation, modulate autophagy and apoptosis, and improve synaptic health [48].
Clinical research has progressed from early safety trials to more advanced studies. A phase I trial using repeated intracerebroventricular injections of human umbilical cord blood MSCs in Alzheimer’s patients found the procedure to be well-tolerated, with only mild, transient side effects [49]. A recent phase I/II trial evaluating intranasal administration of adipose MSC-derived exosomes reported no treatment-related adverse events. Although the study was primarily designed to assess safety and feasibility, involving a small cohort, exploratory secondary outcomes suggested a cognitive improvement and less hippocampal shrinkage in the medium-dose group [46]. Additionally, a phase 2a randomized controlled trial of a BM-MSC therapy demonstrated safety and indications of efficacy, including slowed brain and hippocampal atrophy and improved clinical scores [50]. While preclinical results are consistently positive, clinical trials so far confirm safety but show only preliminary signs of efficacy. Larger and longer-term studies are needed to determine the true therapeutic benefit of MSCs for Alzheimer’s disease.
2.2. Parkinson’s Disease (PD)
PD is the second most common ND, primarily affecting aging population. The pathophysiology associated with this disease is related to the accumulation of misfolded α-synuclein protein inside neurons, in the form of Lewy bodies (LBs) and Lewy neurites [51]. PD is pathologically characterized by the loss of nigrostriatal dopaminergic innervation, although neurodegeneration is not limited to nigral dopaminergic neurons, which are responsible for producing dopamine in the substantia nigra and sending it to the striatum, enabling normal movement control (Figure 2). Such a widespread pathology makes PD a very heterogeneous disorder, and a reliable diagnostic test is not yet available. Clinical criteria, however, can only lead to a diagnosis of probable PD, while a definitive diagnosis requires histopathological assessment, with the identification of α-synuclein-containing LBs or Lewy neurites, suggesting that α-synuclein plays a central role in PD pathogenesis [52].
Preclinical studies highlight that both direct MSCs transplantation and administration of their secretome have demonstrated very promising results in behavioural and histological outcomes, highlighting the fact that their benefit is mainly determined by their secretome, which includes soluble factors and EVs, rather than the cells themselves [53]. Molecules found in the secretome multitarget disease-modifying effects on PD hallmarks, including α-synuclein aggregation in LBs and Lewy neurites (Figure 2), by neurotrophic factors secretion and EVs that cross the BBB, support dopaminergic neuron survival, and improve motor behaviour in toxin- and α-synuclein–based PD models [54,55]. In α-synuclein overexpression models, BM-MSC secretome decreases nigral α-synuclein levels, protects dopaminergic neurons in the substantia nigra and striatum, and modulates microglial reactivity, directly linking MSC paracrine signalling to attenuation of LBs–related pathology [56]. Systematic reviews of preclinical work show that MSC-EV therapy consistently improves motor scores and lowers pro-inflammatory cytokines, with effects that appear a few weeks after administration and last at least two months [53].
Early clinical studies have explored the safety and efficacy of MSC transplantation into PD patients: these findings have shown to date that MSC transplantation using autologous or allogeneic cells delivered via intravenous, intranasal, or intracerebral routes is generally safe and well-tolerated, with only mild or transient adverse events reported [57,58].
Clinical trials with BM-MSCs, such as the Venkataramana et al. pilot study [59], showed that autologous grafts into the subventricular zone of patients with severe PD were safe for up to 36 months and associated with subjective improvements in motor symptoms as well as reduced L-DOPA requirements in some cases, without abnormal MRI findings [60,61]. Subsequent trials expanded on these observations: intra-arterial delivery of dopaminergic-differentiated BM-MSCs to 53 patients demonstrated absence of immune or tumorigenic complications, and rapid post-procedural recovery [62]; administration of BMSCs into cerebral arteries in patients with progressive supranuclear palsy resulted in stable motor function for at least six months [63]; intravenous BMSC infusion reduced Unified Parkinson’s Disease Rating Scale (UPDRS) scores over one year in mild–moderate PD [64]. Parallel investigations using A-MSCs consistently reported reductions in UPDRS, regardless of administration route, including both allogeneic and autologous protocols [65].
Altogether, these trials across diverse MSC sources reinforce the strong safety profile of MSCs therapy and suggest a reproducible trend toward short-term clinical improvement in both motor and non-motor PD symptoms.
2.3. Huntington’s Disease (HD)
HD is an autosomal dominant ND caused by an expanded CAG trinucleotide repeat in the huntingtin (HTT) gene, leading to the production of mutant and toxic huntingtin protein (mHTT) [66]. mHTT primarily affects medium spiny GABAergic neurons in the striatum (caudate nucleus and putamen), leading to their progressive degeneration. Cortical neurons may also be affected as the disease progresses, contributing to cognitive decline and psychiatric symptoms [67].
The pathophysiology of HD involves multiple mechanisms: excitotoxicity, transcriptional dysregulation, mitochondrial dysfunction, oxidative stress, impaired proteostasis and reduced availability of neurotrophic factors. Additionally, astrocyte dysfunction and neuroinflammation contribute to disease progression, resulting in the characteristic motor, cognitive, and psychiatric symptoms (Figure 2) [68].
Although mutant huntingtin (mHTT) is the primary genetic driver of Huntington’s disease, current MSC-based strategies do not aim to directly suppress or eliminate mHTT expression. Instead, they are designed to mitigate downstream pathogenic processes triggered by mHTT, including neurotrophic factor deficiency, neuroinflammation, mitochondrial dysfunction, and progressive striatal neurodegeneration [69,70].
Across at least 15 rodent studies, BM-MSCs and DPSCs have demonstrated consistent functional and structural benefits in both toxin-based and genetic models of HD [70,71,72]. MSC treatment was associated with increased striatal volume, reduced ventricular enlargement, and improvements across multiple motor outcomes, including motor coordination, muscle strength, and neuromuscular activity. However, effects on cognitive performance were generally limited or absent [70].
Mechanistically, transplanted MSCs were shown to reduce apoptosis and neuroinflammation while upregulating neurotrophic factors, particularly brain-derived neurotrophic factor (BDNF) [73]. These effects appear to be mediated predominantly through paracrine mechanisms rather than direct neuronal differentiation [71,74]. Genetically engineered MSCs overexpressing BDNF (MSC/BDNF) further enhanced therapeutic outcomes, including attenuation of striatal atrophy, increased neurogenesis-like activity, and prolonged survival in transgenic HD mouse models [75].
Additionally, intranasal delivery has successfully targeted MSCs to the striatum, improving survival as well as dopaminergic and inflammatory markers, and represents a promising non-invasive administration route [76].
Clinically, human data are still limited to early-phase investigations. The PRE-CELL lead-in study followed early-stage HD patients to characterize disease progression and establish clinical and imaging endpoints for a subsequent Phase I intracerebral MSC/BDNF trial [77]. In parallel, Brazilian early-phase clinical trials are evaluating the long-term safety and potential motor and neuroprotective effects of repeated systemic MSC infusions; however, efficacy outcomes remain preliminary and inconclusive [78,79].
Overall, MSCs in HD are best viewed as promising but investigational, with a strong preclinical motor and structural benefits and early clinical programs underway, especially using engineered MSC for neurological factors’ delivery.
2.4. Amyotrophic Lateral Sclerosis (ALS)
ALS is a progressive neurodegenerative disorder characterized by the selective loss of motor neurons that normally control voluntary muscle contraction, typically leading to death within 2 to 4 years after symptom onset. Approximately 10% of ALS patients have a family history consistent with an autosomal dominant inheritance pattern. The remaining 90% of cases are sporadic, with no affected family members, and are classified as sporadic ALS (SALS) [80].
Although the precise mechanisms underlying motor neuron degeneration remain unclear, studies using SOD1 mutant models and other ALS-associated genes have implicated multiple molecular pathways. These include impaired protein degradation, RNA dysregulation, oxidative stress, glutamate excitotoxicity, mitochondrial dysfunction, aberrant neuroinflammation, and defective axonal transport, all contributing to motor neuron death [81,82]. Clinically, this neuronal loss manifests as progressive muscle weakness, atrophy and fasciculations, reflecting the combined involvement of lower and upper motor neurons (Figure 2) [83]. As the disease advances, patients develop dysarthria, dysphagia, and respiratory muscle failure, which ultimately represent the main cause of death in ALS [84]. Sensory functions are typically preserved, although a subset of patients may also exhibit cognitive and behavioural impairment, associated with frontotemporal dysfunction [85].
A systematic review and meta-analysis of preclinical ALS studies in transgenic mice and other rodent models found that MSC transplantation significantly delayed onset, slowed clinical progression and extended survival. Reviews emphasize that benefits are largely mediated by paracrine neurotrophic and anti-inflammatory actions, rather than neuron replacement [58,86].
MSCs secrete multiple neurotrophic and growth factors — Brain-Derived Neurotrophic Factor (BDNF), Glial cell line-Derived Neurotrophic Factor (GDNF), Vascular Endothelial Growth Factor (VEGF) [87] — and anti-inflammatory cytokines, that collectively modulate microglial and T-cell activation, and protect motor neurons from excitotoxicity and oxidative stress [88]. These effects contribute to the preservation of motor function and neuronal survival in ALS animal models.
Early-phase clinical trials focused on safety, feasibility and preliminary function outcomes confirmed that intraspinal autologous BM-MSC delivery had no serious transplant-related toxicity or tumour formation over months to years of follow-up. Also, intrathecal (IT) BM-MSC in 26 patients was safe and associated with transient slowing of ALS Functional Rating Scale (ALSFRS) decline and stabilization of forced vital capacity (FVC) in many patients for several months [89]. Repeated IT and intravenous (IV) autologous BM-MSC injections, delivered in three doses, at one-month intervals, were also safe, showing ALSFRS stabilization and improved FVC over three-month period. Similar repeated IT protocols showed acceptable safety over 12 months [90].
In clinical studies, MSC-based therapies for ALS have generated the most consistent human data to date, although definitive disease-modifying efficacy remains unproven. A phase III randomized, placebo-controlled trial of MSCs engineered to deliver neurotrophic factors (MSC NTF) did not meet its primary efficacy endpoint in the overall ALS population — ALSFRS-R total score. Secondary endpoints, such as biomarker analyses, however, revealed significant improvements in cerebrospinal fluid markers of neuroinflammation, neurodegeneration, and neurotrophic support in MSC-NTF-treated patients compared to placebo. In predefined subgroups of patients with less-advanced disease (ALSFRS-R ≥ 31–35), higher responder rates were observed. However, these groups presented a modest ALSFRS-R benefit (~ 2.4 points at 28 weeks), concluding that these effects were nominally significant but underpowered, indicating that clinical improvement remains limited [91].
3. Discussion
Across multiple NDs, MSCs have consistently demonstrated a favourable safety profile and a broad spectrum of biological activities that target key pathogenic mechanisms shared by AD, PD, HD and ALS. Rather than acting through direct neuronal replacement, MSCs exert their effects predominantly via paracrine mechanisms, including the secretion of neurotrophic factors, anti-inflammatory cytokines, and EVs [92]. This multimodal mechanism of action represents a major advantage in diseases characterized by complex, multifactorial and not fully understood pathophysiology.
Nevertheless, translating these biological properties into robust and sustained clinical benefit has proven challenging. One of the principal limitations associated with MSC administration is their limited survival [93], engraftment, and long-term persistence within the CNS. Following transplantation, MSCs are exposed to a hostile microenvironment marked by oxidative stress, inflammation, and ongoing neurodegeneration, which likely restricts their therapeutic durability. Moreover, systemically administered MSCs show inefficient homing to the brain and spinal cord, with significant cell trapping in peripheral organs and restricted passage across the BBB [94,95].
Another important challenge lies in the intrinsic heterogeneity of MSCs treatments [96]. Differences in tissue source, donor characteristics, isolation methods, and culture conditions contribute to variability in secretory profiles and therapeutic potency, complicating direct comparison across studies and potentially contributing to inconsistent clinical outcomes [97]. In addition, optimal dosing, timing of intervention, and frequency of administration remain insufficiently defined, with many clinical trials relying on empirical regimens that may not fully capture the therapeutic potential of MSCs [98].
Despite these challenges, the overall clinical experience to date remains encouraging: MSC-based therapies have repeatedly shown excellent safety profiles across intrathecal, intravenous, and intracerebral administration, with minimal serious adverse events reported in early-phase clinical trials [99,100]. Even in trials where primary clinical endpoints were not met, secondary outcomes and biomarker analyses frequently revealed biologically meaningful effects, such as modulation of neuroinflammation, preservation of neurotrophic support, and slowing of functional decline in selected patient subgroups [91]. These findings suggest that the modest clinical efficacy observed thus far may reflect suboptimal patient stratification, dosing strategies, or disease stage selection rather than a fundamental lack of therapeutic relevance.
4. Conclusions and Future Directions
This review emphasizes the progress in MSC therapy for NDs, including AD, PD, HD and ALS. Despite the remarkable advancements, particularly in early-phase clinical trials, the scarcity of late-stage trials highlights the necessity for further investigation.
Emerging strategies are actively addressing these challenges: advances in MSC preconditioning, genetic engineering, and manufacturing standardization aim to enhance cell survival, homing capacity, and secretory potency. In parallel, growing interest in MSC-derived EVs offers a promising cell-free alternative that retains many of the beneficial paracrine effects of MSCs while potentially overcoming safety, scalability, and delivery limitations. Moreover, increasing emphasis on biomarker-guided patient selection and early-stage intervention may allow future trials to better identify populations most likely to benefit from MSC-based therapies.
Future research should focus on broadening clinical trials to encompass more NDs, also addressing the issues of scalability and standardization in EVs production. The rising interest in EV-based therapeutics, alongside technological progress and an enhanced comprehension of their therapeutic potential, is anticipated to propel revolutionary treatment techniques for NDs. These advancements may facilitate more accurate, efficient, and less invasive procedures, thereby enhancing patient outcomes in these NDs.
Author Contributions
Conceptualization, A.T.; P.S.; R.A. and A.C.M.; methodology, A.T.; P.S.; R.A. and A.C.M.; validation, A.T.; P.S.; R.A. and A.C.M.; formal analysis, A.T.; P.S.; R.A. and A.C.M.; investigation, A.T.; P.S.; R.A. and A.C.M.; resources, A.C.M.; data curation, A.T.; P.S.; R.A. and A.C.M.; writing—original draft preparation, A.T.; P.S.; R.A. and A.C.M.; writing—review and editing, A.T.; P.S.; R.A. and A.C.M.; visualization, A.T.; P.S.; R.A. and A.C.M.; supervision, P.S.; R.A. and A.C.M.; project administration, A.T.; P.S.; R.A. and A.C.M.; funding acquisition, A.C.M. All authors have read and agreed to the published version of the manuscript.
Funding
The work was supported through the project UIDB/00211/2020 funded by FCT/MCTES through national funds and through the project NEUROBIOTECH - 16024 - COMPETE2030-FEDER-00716600 (Neurobiotech—Combining Novel Cell Therapies and Biodegradable Polymers to Promote Peripheral Nerve Regeneration) and 2022.10564.PTDC (InnovaBIOMAS). Patrícia Sousa (2023.00246.BD) acknowledges Fundação para a Ciência e Tecnologia (FCT) for financial support.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Further data on the reported results are available from the corresponding author on request.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
AD — Alzheimer’s Disease
ALS — Amyotrophic Lateral Sclerosis
A-MSCs — Adipose Tissue-derived Mesenchymal Stem Cells
BBB — Blood-brain barrier
BM-MSCs — Bone Marrow-derived Mesenchymal Stem Cells
CNS — Central Nervous System
DPSCs — Dental Pulp-derived Mesenchymal Stem Cells
EVs — Extracellular Vesicles
HD — Huntington’s Disease
HTT — Huntingtin Gene
hUCB-MSCs — Human Umbilical Cord Blood-derived Mesenchymal Stem Cells
IT — Intrathecal
IV — Intravenous
mHTT — Huntingtin mutated protein
miRNA — MicroRNA
MSC — Mesenchymal Stem Cell
NDs — Neurodegenerative Diseases
NFTs — Neurofibrillary Tangles
PD — Parkinson’s Disease
References
- Wang, S., et al., The Expanding Burden of Neurodegenerative Diseases: An Unmet Medical and Social Need. Aging Dis, 2024. 16(5): p. 2937-2952. [CrossRef]
- Deokate, N., et al., A Comprehensive Review of the Role of Stem Cells in Neuroregeneration: Potential Therapies for Neurological Disorders. Cureus, 2024. 16(8): p. e67506. [CrossRef]
- Singh, K., et al., A Review of the Common Neurodegenerative Disorders: Current Therapeutic Approaches and the Potential Role of Bioactive Peptides. Curr Protein Pept Sci, 2024. 25(7): p. 507-526. [CrossRef]
- Giovannelli, L., et al., Mesenchymal stem cell secretome and extracellular vesicles for neurodegenerative diseases: Risk-benefit profile and next steps for the market access. Bioactive Materials, 2023. 29: p. 16-35. [CrossRef]
- Chitnis, T. and H.L. Weiner, CNS inflammation and neurodegeneration. J Clin Invest, 2017. 127(10): p. 3577-3587. [CrossRef] [PubMed]
- Liu, Y., et al., Interactions of glial cells with neuronal synapses, from astrocytes to microglia and oligodendrocyte lineage cells. Glia, 2023. 71: p. 1383-1401. [CrossRef]
- Demmings, M., et al., (Re)building the nervous system: A review of neuron–glia interactions from development to disease. Journal of Neurochemistry, 2024. 169. [CrossRef]
- Rahman, M., et al., Emerging Role of Neuron-Glia in Neurological Disorders: At a Glance. Oxidative Medicine and Cellular Longevity, 2022. 2022.
- Tesco, G. and S. Lomoio, Pathophysiology of neurodegenerative diseases: An interplay among axonal transport failure, oxidative stress, and inflammation? Semin Immunol, 2022. 59: p. 101628. [CrossRef] [PubMed]
- Sweeney, P., et al., Protein misfolding in neurodegenerative diseases: implications and strategies. Transl Neurodegener, 2017. 6: p. 6. [CrossRef]
- Jacobs, H., et al., The cerebellum in Alzheimer's disease: evaluating its role in cognitive decline. Brain : a journal of neurology, 2018. 141 1: p. 37-47. [CrossRef] [PubMed]
- O'Callaghan, C., et al., Cerebellar atrophy in Parkinson's disease and its implication for network connectivity. Brain, 2016. 139(Pt 3): p. 845-55. [CrossRef]
- Iskusnykh, I., et al., Aging, Neurodegenerative Disorders, and Cerebellum. International Journal of Molecular Sciences, 2024. 25. [CrossRef] [PubMed]
- Liang, K. and E. Carlson, Resistance, vulnerability and resilience: A review of the cognitive cerebellum in aging and neurodegenerative diseases. Neurobiology of Learning and Memory, 2020. 170.
- Kaur, G. and N. Singh, The Role of Inflammation in Retinal Neurodegeneration and Degenerative Diseases. International Journal of Molecular Sciences, 2021. 23. [CrossRef] [PubMed]
- Ziegler, G., et al., Progressive neurodegeneration following spinal cord injury. Neurology, 2018. 90. [CrossRef] [PubMed]
- Anjum, A., et al., Spinal Cord Injury: Pathophysiology, Multimolecular Interactions, and Underlying Recovery Mechanisms. International Journal of Molecular Sciences, 2020. 21. [CrossRef]
- Akbar, A., et al., CRISPR in Neurodegenerative Diseases Treatment: An Alternative Approach to Current Therapies. Genes (Basel), 2025. 16(8). [CrossRef]
- Jankovic, J. and L.G. Aguilar, Current approaches to the treatment of Parkinson's disease. Neuropsychiatr Dis Treat, 2008. 4(4): p. 743-57. [CrossRef]
- Temple, S., Advancing cell therapy for neurodegenerative diseases. Cell Stem Cell, 2023. 30(5): p. 512-529. [CrossRef]
- Rahimi Darehbagh, R., et al., Stem cell therapies for neurological disorders: current progress, challenges, and future perspectives. Eur J Med Res, 2024. 29(1): p. 386. [CrossRef]
- Sakthiswary, R. and A.A. Raymond, Stem cell therapy in neurodegenerative diseases: From principles to practice. Neural Regen Res, 2012. 7(23): p. 1822-31.
- Li, Y., et al., Therapeutic potential of mesenchymal stem cells in neurodegenerative diseases. World Journal of Stem Cells, 2025.
- Patel, G.D., et al., Mesenchymal stem cell-based therapies for treating well-studied neurological disorders: a systematic review. Front Med (Lausanne), 2024. 11: p. 1361723. [CrossRef] [PubMed]
- Bagno, L.L., et al., Mechanism of Action of Mesenchymal Stem Cells (MSCs): impact of delivery method. Expert Opin Biol Ther, 2022. 22(4): p. 449-463. [CrossRef]
- Issa, E.H.B., et al., Therapeutic potential and challenges of mesenchymal stem cells in neurological disorders: A concise analysis. J Neuropathol Exp Neurol, 2025. 84(8): p. 668-679. [CrossRef]
- Quan, J., et al., Mesenchymal stem cell exosome therapy: current research status in the treatment of neurodegenerative diseases and the possibility of reversing normal brain aging. Stem Cell Research and Therapy, 2025. 16(1). [CrossRef] [PubMed]
- Krämer-Albers, E.-M., Extracellular Vesicles at CNS barriers: Mode of action. Current Opinion in Neurobiology, 2022. 75. [CrossRef]
- Banks, W., et al., Transport of Extracellular Vesicles across the Blood-Brain Barrier: Brain Pharmacokinetics and Effects of Inflammation. International Journal of Molecular Sciences, 2020. 21. [CrossRef]
- Nieland, L., et al., Engineered EVs designed to target diseases of the CNS. Journal of controlled release : official journal of the Controlled Release Society, 2023. 356: p. 493-506. [CrossRef]
- Liang, X.S., et al., Mesenchymal Stem Cell Therapy for Huntington Disease: A Meta-Analysis. Stem Cells Int, 2023. 2023: p. 1109967. [CrossRef]
- Aditya, B., B. Harshita, and S. Priyanka, Mesenchymal stem cell therapy for Alzheimer’s disease: A novel therapeutic approach for neurodegenerative diseases. Neuroscience, 2024. 555: p. 52-68. [CrossRef]
- Chen, Z.R., et al., Role of Cholinergic Signaling in Alzheimer's Disease. Molecules, 2022. 27(6). [CrossRef] [PubMed]
- Pushpa Tryphena, K., et al., Pathogenesis, diagnostics, and therapeutics for Alzheimer's disease: Breaking the memory barrier. Ageing Research Reviews, 2024. 101: p. 102481. [CrossRef] [PubMed]
- Murphy, M.P. and H. LeVine, 3rd, Alzheimer's disease and the amyloid-beta peptide. J Alzheimers Dis, 2010. 19(1): p. 311-23. [CrossRef]
- Zhang, H., et al., Role of Aβ in Alzheimer's-related synaptic dysfunction. Front Cell Dev Biol, 2022. 10: p. 964075. [CrossRef]
- McGroarty, J., et al., Inflammasome-Mediated Neuroinflammation: A Key Driver in Alzheimer's Disease Pathogenesis. Biomolecules, 2025. 15(5). [CrossRef]
- Tolar, M., et al., Neurotoxic Soluble Amyloid Oligomers Drive Alzheimer’s Pathogenesis and Represent a Clinically Validated Target for Slowing Disease Progression. International Journal of Molecular Sciences, 2021. 22. [CrossRef] [PubMed]
- Li, S. and D. Selkoe, A mechanistic hypothesis for the impairment of synaptic plasticity by soluble Aβ oligomers from Alzheimer’s brain. Journal of Neurochemistry, 2020. 154: p. 583-597. [CrossRef]
- Zhang, H., et al., Role of Aβ in Alzheimer’s-related synaptic dysfunction. Frontiers in Cell and Developmental Biology, 2022. 10. [CrossRef]
- Fišar, Z., Linking the Amyloid, Tau, and Mitochondrial Hypotheses of Alzheimer’s Disease and Identifying Promising Drug Targets. Biomolecules, 2022. 12. [CrossRef]
- Fanlo-Ucar, H., et al., The Dual Role of Amyloid Beta-Peptide in Oxidative Stress and Inflammation: Unveiling Their Connections in Alzheimer’s Disease Etiopathology. Antioxidants, 2024. 13. [CrossRef]
- Gulisano, W., et al., Role of Amyloid-β and Tau Proteins in Alzheimer's Disease: Confuting the Amyloid Cascade. J Alzheimers Dis, 2018. 64(s1): p. S611-s631. [CrossRef]
- Lu, Z., D. Zhi-fang, and Z. Jie-yuan, Immunomodulatory role of mesenchymal stem cells in Alzheimer's disease. Life Sciences, 2020. 246: p. 117405. [CrossRef]
- Wang, H., et al., Exploration of Cytokines That Impact the Therapeutic Efficacy of Mesenchymal Stem Cells in Alzheimer’s Disease. Bioengineering, 2025. 12. [CrossRef] [PubMed]
- Xie, X., et al., Clinical safety and efficacy of allogenic human adipose mesenchymal stromal cells-derived exosomes in patients with mild to moderate Alzheimer’s disease: a phase I/II clinical trial. General Psychiatry, 2023. 36. [CrossRef]
- Cone, A., et al., Mesenchymal stem cell-derived extracellular vesicles ameliorate Alzheimer's disease-like phenotypes in a preclinical mouse model. Theranostics, 2021. 11: p. 8129-8142. [CrossRef]
- Qin, C., et al., Transplantation of bone marrow mesenchymal stem cells improves cognitive deficits and alleviates neuropathology in animal models of Alzheimer’s disease: a meta-analytic review on potential mechanisms. Translational Neurodegeneration, 2020. 9. [CrossRef]
- Kim, H.J., et al., Intracerebroventricular injection of human umbilical cord blood mesenchymal stem cells in patients with Alzheimer’s disease dementia: a phase I clinical trial. Alzheimer's Research & Therapy, 2021. 13.
- Rash, B., et al., Allogeneic mesenchymal stem cell therapy with laromestrocel in mild Alzheimer’s disease: a randomized controlled phase 2a trial. Nature Medicine, 2025. 31: p. 1257-1266. [CrossRef] [PubMed]
- Kouli, A., K.M. Torsney, and W.L. Kuan, Parkinson’s Disease: Etiology, Neuropathology, and Pathogenesis, in Parkinson’s Disease: Pathogenesis and Clinical Aspects, T.B. Stoker and J.C. Greenland, Editors. 2018, Codon Publications Copyright: The Authors.: Brisbane (AU).
- Xu, L. and J. Pu, Alpha-Synuclein in Parkinson's Disease: From Pathogenetic Dysfunction to Potential Clinical Application. Parkinson's Disease, 2016. 2016.
- Wang, X., et al., Effectiveness of mesenchymal stem cell-derived extracellular vesicles therapy for Parkinson’s disease: A systematic review of preclinical studies. World Journal of Stem Cells, 2025. 17. [CrossRef] [PubMed]
- Volarević, A., et al., Therapeutic Potential of Mesenchymal Stem Cell-Derived Extracellular Vesicles in the Treatment of Parkinson’s Disease. Cells, 2025. 14. [CrossRef]
- Mendes-Pinheiro, B., et al., Bone Marrow Mesenchymal Stem Cells' Secretome Exerts Neuroprotective Effects in a Parkinson's Disease Rat Model. Frontiers in Bioengineering and Biotechnology, 2019. 7. [CrossRef] [PubMed]
- Marques, C.R., et al., Secretome of bone marrow mesenchymal stromal cells cultured in a dynamic system induces neuroprotection and modulates microglial responsiveness in an α-synuclein overexpression rat model. Cytotherapy, 2024. [CrossRef] [PubMed]
- Schiess, M., et al., Preliminary Report on the Safety and Tolerability of Bone marrow-derived Allogeneic Mesenchymal Stem Cells infused intravenously in Parkinson’s disease Patients (S16.008). Neurology, 2019. [CrossRef]
- Rahbaran, M., et al., Therapeutic utility of mesenchymal stromal cell (MSC)-based approaches in chronic neurodegeneration: a glimpse into underlying mechanisms, current status, and prospects. Cellular & Molecular Biology Letters, 2022. 27.
- Venkataramana, N., et al., Open-labeled study of unilateral autologous bone-marrow-derived mesenchymal stem cell transplantation in Parkinson's disease. Translational research : the journal of laboratory and clinical medicine, 2010. 155 2: p. 62-70. [CrossRef]
- Boika, A., et al., Mesenchymal stem cells in Parkinson’s disease: Motor and nonmotor symptoms in the early posttransplant period. Surgical Neurology International, 2020. 11.
- Neelam, K.V., et al., Open-labeled study of unilateral autologous bone-marrow-derived mesenchymal stem cell transplantation in Parkinson's disease. Translational Research, 2010. 155(2): p. 62-70.
- Venkataramana, N., et al., Bilateral Transplantation of Allogenic Adult Human Bone Marrow-Derived Mesenchymal Stem Cells into the Subventricular Zone of Parkinson's Disease: A Pilot Clinical Study. Stem Cells International, 2012. 2012.
- Patel, G.D., et al., Mesenchymal stem cell-based therapies for treating well-studied neurological disorders: a systematic review. Frontiers in Medicine, 2024. 11. [CrossRef] [PubMed]
- Schiess, M., et al., Allogeneic Bone Marrow–Derived Mesenchymal Stem Cell Safety in Idiopathic Parkinson's Disease. Movement Disorders, 2021. 36: p. 1825-1834. [CrossRef] [PubMed]
- Vij, R., et al., Safety and efficacy of adipose-derived mesenchymal stem cell therapy in elderly Parkinson's disease patients: an intermediate-size expanded access program. Cytotherapy, 2024. [CrossRef]
- McColgan, P. and S.J. Tabrizi, Huntington's disease: a clinical review. Eur J Neurol, 2018. 25(1): p. 24-34. [CrossRef]
- Jiang, A., et al., From Pathogenesis to Therapeutics: A Review of 150 Years of Huntington’s Disease Research. International Journal of Molecular Sciences, 2023. 24. [CrossRef] [PubMed]
- Jurcău, A., Molecular Pathophysiological Mechanisms in Huntington’s Disease. Biomedicines, 2022. 10. [CrossRef]
- Ferguson, M.W., et al., Current and Possible Future Therapeutic Options for Huntington's Disease. J Cent Nerv Syst Dis, 2022. 14: p. 11795735221092517. [CrossRef]
- Liang, X.-S., et al., Mesenchymal Stem Cell Therapy for Huntington Disease: A Meta-Analysis. Stem Cells International, 2023. 2023.
- Kerkis, I., et al., Neural and mesenchymal stem cells in animal models of Huntington’s disease: past experiences and future challenges. Stem Cell Research & Therapy, 2015. 6.
- Rossignol, J., et al., Reductions in behavioral deficits and neuropathology in the R6/2 mouse model of Huntington’s disease following transplantation of bone-marrow-derived mesenchymal stem cells is dependent on passage number. Stem Cell Research & Therapy, 2015. 6. [CrossRef]
- Rossignol, J., et al., Mesenchymal stem cell transplantation and DMEM administration in a 3NP rat model of Huntington's disease: Morphological and behavioral outcomes. Behavioural Brain Research, 2011. 217: p. 369-378. [CrossRef] [PubMed]
- Lo Furno, D., G. Mannino, and R. Giuffrida, Functional role of mesenchymal stem cells in the treatment of chronic neurodegenerative diseases. Journal of Cellular Physiology, 2018. 233: p. 3982-3999. [CrossRef]
- Kari, P., et al., Human Mesenchymal Stem Cells Genetically Engineered to Overexpress Brain-derived Neurotrophic Factor Improve Outcomes in Huntington's Disease Mouse Models. Molecular Therapy, 2016. 24(5): p. 965-977. [CrossRef] [PubMed]
- Yu-Taeger, L., et al., Intranasal Administration of Mesenchymal Stem Cells Ameliorates the Abnormal Dopamine Transmission System and Inflammatory Reaction in the R6/2 Mouse Model of Huntington Disease. Cells, 2019. 8. [CrossRef]
- Wheelock, V., et al., PRE-CELL: Clinical and Novel Biomarker Measures of Disease Progression in a Lead-In-Observational Study for a Planned Phase 1 Trial of Genetically-Modified Mesenchymal Stem Cells Over-Expressing BDNF in Patients with Huntington’s Disease (S25.004). Neurology, 2016. [CrossRef]
- Fink, K., et al., Developing stem cell therapies for juvenile and adult-onset Huntington’s disease. Regenerative medicine, 2015. 10: p. 623-646. [CrossRef]
- Giovannelli, L., et al., Mesenchymal stem cell secretome and extracellular vesicles for neurodegenerative diseases: Risk-benefit profile and next steps for the market access. Bioactive Materials, 2023. 29: p. 16-35. [CrossRef]
- Masrori, P. and P. Van Damme, Amyotrophic lateral sclerosis: a clinical review. Eur J Neurol, 2020. 27(10): p. 1918-1929. [CrossRef]
- Peggion, C., et al., SOD1 in ALS: Taking Stock in Pathogenic Mechanisms and the Role of Glial and Muscle Cells. Antioxidants, 2022. 11. [CrossRef] [PubMed]
- Gall, L., et al., Molecular and Cellular Mechanisms Affected in ALS. Journal of Personalized Medicine, 2020. 10. [CrossRef] [PubMed]
- Verma, A., Clinical Manifestation and Management of Amyotrophic Lateral Sclerosis, in Amyotrophic Lateral Sclerosis, T. Araki, Editor. 2021, Exon Publications Copyright: The Authors.: Brisbane (AU).
- Pasqualucci, E., et al., Management of Dysarthria in Amyotrophic Lateral Sclerosis. Cells, 2025. 14(14). [CrossRef]
- Achi, E.Y. and S.A. Rudnicki, ALS and Frontotemporal Dysfunction: A Review. Neurol Res Int, 2012. 2012: p. 806306. [CrossRef]
- Vercelli, A., et al., Human mesenchymal stem cell transplantation extends survival, improves motor performance and decreases neuroinflammation in mouse model of amyotrophic lateral sclerosis. Neurobiology of Disease, 2008. 31: p. 395-405. [CrossRef]
- Rahbaran, M., et al., Therapeutic utility of mesenchymal stromal cell (MSC)-based approaches in chronic neurodegeneration: a glimpse into underlying mechanisms, current status, and prospects. Cell Mol Biol Lett, 2022. 27(1): p. 56. [CrossRef]
- Tolstova, T., et al., Preconditioning of Mesenchymal Stem Cells Enhances the Neuroprotective Effects of Their Conditioned Medium in an Alzheimer’s Disease In Vitro Model. Biomedicines, 2024. 12. [CrossRef] [PubMed]
- Petrou, P., et al., Safety and Clinical Effects of Mesenchymal Stem Cells Secreting Neurotrophic Factor Transplantation in Patients With Amyotrophic Lateral Sclerosis: Results of Phase 1/2 and 2a Clinical Trials. JAMA neurology, 2016. 73 3: p. 337-344. [CrossRef]
- Oh, K.-W., et al., Phase I Trial of Repeated Intrathecal Autologous Bone Marrow-Derived Mesenchymal Stromal Cells in Amyotrophic Lateral Sclerosis. STEM CELLS Translational Medicine, 2015. 4. [CrossRef] [PubMed]
- Cudkowicz, M., et al., A randomized placebo-controlled phase 3 study of mesenchymal stem cells induced to secrete high levels of neurotrophic factors in amyotrophic lateral sclerosis. Muscle & Nerve, 2021. 65: p. 291-302.
- Di Santo, S. and H.R. Widmer, Paracrine factors for neurodegenerative disorders: special emphasis on Parkinson's disease. Neural Regen Res, 2016. 11(4): p. 570-1.
- Ghasemi, M., et al., Mesenchymal stromal cell-derived secretome-based therapy for neurodegenerative diseases: overview of clinical trials. Stem Cell Research & Therapy, 2023. 14.
- Sheikhi, K., et al., Recent advances in mesenchymal stem cell therapy for multiple sclerosis: clinical applications and challenges. Frontiers in Cell and Developmental Biology, 2025. 13. [CrossRef]
- Ullah, M., D.D. Liu, and A.S. Thakor, Mesenchymal Stromal Cell Homing: Mechanisms and Strategies for Improvement. iScience, 2019. 15: p. 421-438. [CrossRef]
- Isaković, J., et al., Mesenchymal stem cell therapy for neurological disorders: The light or the dark side of the force? Frontiers in Bioengineering and Biotechnology, 2023. 11. [CrossRef] [PubMed]
- Turlo, A.J., et al., Mesenchymal Stromal Cell Secretome Is Affected by Tissue Source and Donor Age. Stem Cells, 2023. 41(11): p. 1047-1059. [CrossRef]
- Van Den Bos, J., et al., Are Cell-Based Therapies Safe and Effective in the Treatment of Neurodegenerative Diseases? A Systematic Review with Meta-Analysis. Biomolecules, 2022. 12. [CrossRef]
- Staff, N.P., D.T. Jones, and W. Singer, Mesenchymal Stromal Cell Therapies for Neurodegenerative Diseases. Mayo Clin Proc, 2019. 94(5): p. 892-905. [CrossRef]
- Quynh Dieu, T., M. Huynh Nhu, and P. Duc Toan, Application of mesenchymal stem cells for neurodegenerative diseases therapy discovery. Regenerative Therapy, 2024. 26: p. 981-989. [CrossRef]
Figure 1.
Schematic representation of MSC sources and their therapeutic mechanisms in NDs. Following administration, MSCs exert their effects predominantly through the release of a bioactive secretome, composed of EVs, growth factors and immunomodulatory cytokines.
Figure 1.
Schematic representation of MSC sources and their therapeutic mechanisms in NDs. Following administration, MSCs exert their effects predominantly through the release of a bioactive secretome, composed of EVs, growth factors and immunomodulatory cytokines.
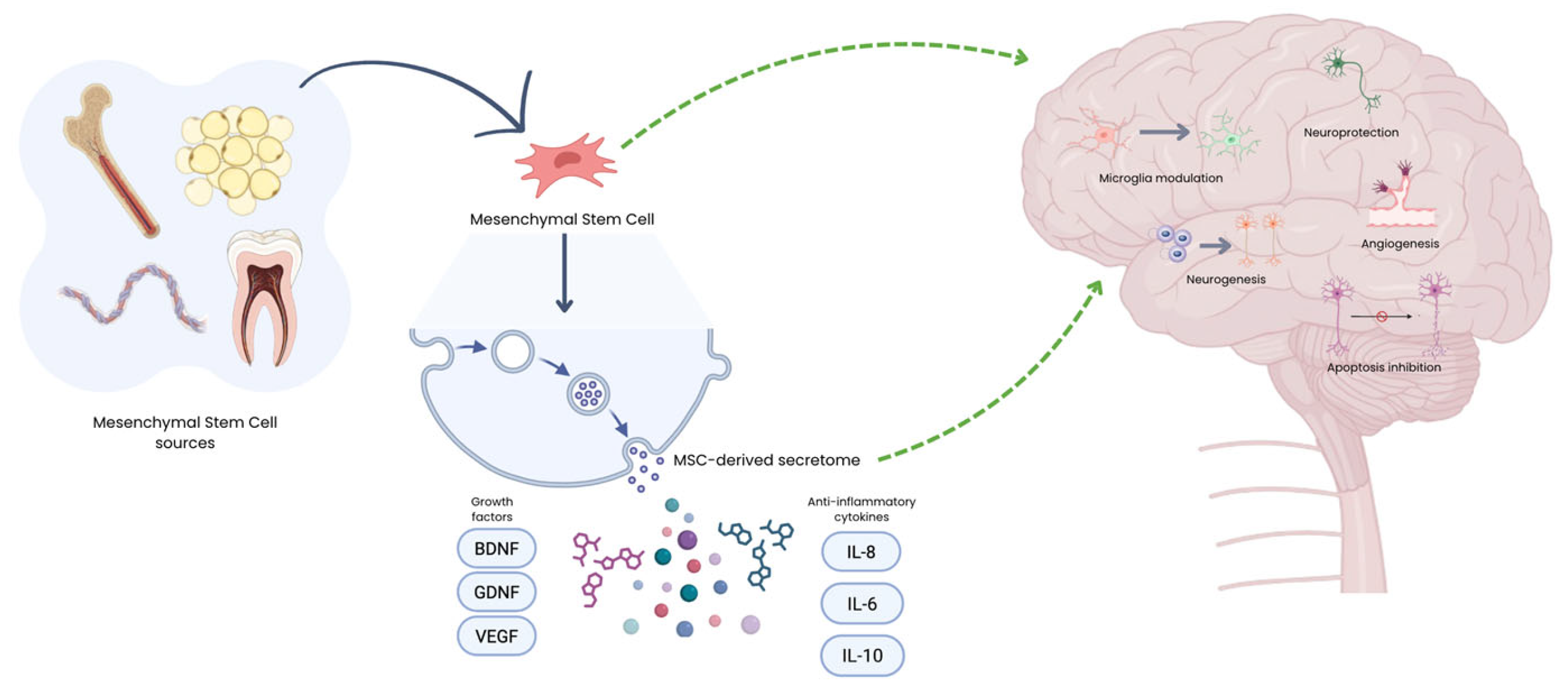
Figure 2.
Pathophysiological mechanisms and clinical hallmarks of major neurodegenerative diseases. Side panels delineate the progression from cellular dysfunction to specific neuronal loss and subsequent clinical manifestations.
Figure 2.
Pathophysiological mechanisms and clinical hallmarks of major neurodegenerative diseases. Side panels delineate the progression from cellular dysfunction to specific neuronal loss and subsequent clinical manifestations.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



