
Submitted:
09 January 2026
Posted:
12 January 2026
You are already at the latest version
Abstract
Ocular diseases – including glaucoma, diabetic retinopathy, and age-related macular degeneration – remain major global causes of irreversible vision loss. Despite therapeutic advances, current interventions that address the convergent metabolic, inflammatory, vascular and neurodegenerative components of these diseases are limited. Glucagon‑like peptide‑1 receptor agonists (GLP‑1RAs), widely used for type 2 diabetes and obesity, have emerged as multi-target candidates for ocular therapeutics due to their pleiotropic anti‑inflammatory, antioxidant, vasculoprotective, and neuroprotective properties. Increasing preclinical and clinical evidence indicates that GLP‑1RAs preserve blood–retina barrier integrity, inhibit pathological angiogenesis, reduce inflammation, promote antioxidant responses and protect retinal neurons from degeneration. However, rare ocular adverse events – including nonarteritic anterior ischemic optic neuropathy and “early worsening” of diabetic retinopathy – highlight the need for a balanced and comprehensive consideration of evidence. This review synthesizes mechanistic in-sights, experimental findings, clinical data, and safety considerations to critically assess the potential of GLP‑1RAs as disease‑modifying therapeutics for ocular disorders and outlines translational challenges and research priorities to guide future ophthalmology‑focused investigations.
Keywords:
ocular disease
; glucagon-like peptide-1 receptor agonists
; glaucoma
; diabetic retinopathy
; age-related macular degeneration
1. Introduction
Glucagon-like peptide-1 receptor agonists (GLP-1RAs) have rapidly transformed the management of type 2 diabetes mellitus (T2DM) and obesity, owing to their robust metabolic, cardiovascular and renal benefits [1]. Beyond systemic effects, a growing body of evidence indicates that GLP-1RAs exert potent anti-inflammatory, antioxidant, and neuroprotective actions within ocular tissues, including retinal neurons, Müller glia, retinal pigment epithelium (RPE), and microvascular endothelial cells [2,3]. These pleiotropic properties, combined with the expending global use of GLP-1RAs, have generated substantial interest in their potential role in ocular diseases such as glaucoma, diabetic retinopathy (DR), and age-related macular degeneration (AMD), where chronic inflammation, oxidative stress, and neurodegeneration are central drivers of pathology [4].
Clinical observations have increasingly supported this emerging paradigm. Several large observational and retrospective cohort studies have reported reduced incidence or slower progression of ocular disease among GLP-1RA users in both diabetic and non-diabetic populations [5,6,7]. GLP-1 receptor (GLP-1R), a class B1 G protein-coupled receptor, is expressed in multiple human ocular compartments [8,9] and its activation triggers intracellular signaling pathways – including cAMP/PKA, exchange protein directly activated by cAMP (EPAC-2), ERK1/2, and PI3K/Akt signaling – that attenuate oxidative stress, modulate glial/immune activation, stabilize mitochondrial function, and suppress pro-inflammatory cytokine cascades [10,11]. Additional effects on vascular integrity and extracellular matrix (ECM) remodeling may further contribute to anti-angiogenic activity.
Preclinical studies demonstrate that GLP-1RAs promote retinal ganglion cell (RGC) survival, improve mitochondrial homeostasis, and mitigate microglial activation [12]. Clinical data suggest reduced glaucoma risk [13,14], and potential benefits in DR and AMD [15]. However, emerging concerns regarding adverse ocular events – including reports of nonarteritic anterior ischemic optic neuropathy (NAION) [16,17], early DR worsening in high-risk individuals with rapid glycemic decline [18,19], and mixed outcomes in AMD [20] – underscore the need for risk-stratified application.
This review integrates current molecular insights, preclinical findings, and human clinical data to evaluate the potential of GLP-1RAs as novel disease-modifying agents for ocular disorders. We further discuss translational opportunities and key safety considerations that must be addressed before GLP-1RAs can be advanced as multi-targeted ophthalmic therapeutics.
2. Mechanisms of Action of GLP-1RAs in Ocular Tissues
GLP-1RAs, including native GLP-1 analogs (albiglutide, beinaglutide, dulaglutide, liraglutide, semaglutide and tirzepatide) and exendin-4-based agents (exenatide and lixisenatide), exert ocular effects primarily through direct activation of GLP-1R expressed on retinal neurons, Müller glia, RPE, vascular endothelial cells, as well as through systemic modulation of inflammation and metabolism [21]. Their detailed molecular mechanisms in ocular tissues are summarized in Table 1, and their actions converge on four interrelated domains relevant to ocular health illustrated in Figure 1.
2.1. Neuroprotection
The retina’s exceptional metabolic demand and unique architecture render it highly vulnerable to metabolic (hyperglycemia, obesity), mechanical (elevated IOP), ischemia and age-related stressors [22]. Excitotoxicity, mitochondrial dysfunction, oxidative stress, and glial activation represent shared neurodegenerative pathways across diverse ocular disorders [23]. GLP-1RAs counteract these processes through multiple complementary mechanisms by reducing glutamate-induced excitotoxicity, modulating voltage-gated calcium channel activity, promoting microglia-mediated production of neurotrophic factors and enhancing GABAergic signaling [24]. Exendin-4 increases GABAAR-mediated tonic currents in retinal neurons, stabilizing neuronal excitability [25,26], while downstream ERK1/2–HDAC6 signaling supports axonal transport and mitochondrial trafficking, thereby protecting optic nerve and RGC function [27]. Activation of PINK1/Parkin-mediated mitophagy pathway facilitates clearance of damaged mitochondria and supports energy homeostasis [28]. Together, these mechanisms preserve RGC survival, maintain optic nerve integrity and protect visual function in glaucomatous, ischemic and diabetic stress environment.
2.2. Vascular Integrity and ECM Homeostasis
GLP-1RAs reinforce blood-retina barrier (BRB) stability and counteract pathological angiogenesis by upregulating tight junction protein expression (occludin, claudin-5) and reducing vascular permeability [29]. These agents indirectly suppress VEGF-driven angiogenesis, thereby limiting neovascularization in proliferative DR and neovascular AMD [30]. Through cAMP/PKA-mediated inhibition of NF-κB signaling, GLP-1RAs downregulate inflammatory and angiogenic gene expression in retinal cells. In Müller glia and RPE, GLP-1R activation reduces reactive gliosis, dampens cytokine release, and restores ECM balance, ultimately mitigating fibrosis [31]. These effects collectively help preserve retinal structure and microvascular homeostasis across DR, ischemic retinopathies and AMD.
2.3. Anti-Inflammatory Effects
Chronic activation of microglia and astrocytes drives cytokine/chemokine release, leukostasis and reactive oxygen species (ROS) generation - all major contributors to retinal injury and neurodegeneration [32,33,34,35]. GLP-1RAs exert anti-inflammatory activity through both systemic and local ocular pathways [36]. In individuals with T2DM, GLP-1RA liraglutide treatment reduces circulating inflammatory macrophages and modulates innate immune activity [37]. In the retina, systemic and topical administration of native GLP-1/GLP-1RAs suppresses glial activation in db/db mice [38]. Semaglutide downregulates monocyte chemoattractant protein-1 (MCP-1) and related chemokines, thereby inhibiting monocyte migration and infiltration into ocular tissues [39,40]. GLP-1RAs shift microglia/macrophage from pro-inflammatory (M1)-like toward anti-inflammatory (M2)-like phenotypes, suppressing NF-κB and NLRP3 inflammasome signaling, reducing TNF-α and IL-1β, and enhancing IL-10 production [41,42]. These effects are particularly relevant in glaucoma, where microglial-derived cytokines drive neurotoxic A1 astrocyte formation and BRB disruption [43,44], underscoring the therapeutic relevance of GLP-1RA-mediated immunomodulation. Importantly, many anti-inflammatory actions appear independent of glycemic control and weight loss [45].
2.4. Antioxidant and Mitochondrial Support
Oxidative stress accelerates neuronal apoptosis, vascular dysfunction and RPE damage across DR and AMD. GLP-1RAs provide mitochondrial and antioxidant support through activation of nuclear factor erythroid 2–related factor 2 (Nrf2), a master regulator of antioxidant response, leading to increased expression of antioxidant enzymes such as superoxide dismutase (SOD), catalase, and glutathione peroxidase, while restraining ROS production [46,47]. Concurrently, GLP-1RAs stimulate peroxisome proliferator-activated receptor gamma coactivator 1-alpha (PGC-1α)-driven mitochondrial biogenesis, improve mitochondrial dynamics, and enhance mitophagy [48]. These actions preserve cellular energy homeostasis and reduce oxidative injury, positioning GLP-1RAs as promising candidates for ocular disorders involving mitochondrial dysfunction and mitochondrial compromise (Figure 2).
3. Preclinical and Clinical Evidence Across Ocular Diseases
3.1. Glaucoma
Glaucoma comprises a heterogeneous group of optic neuropathies characterized by progressive RGC loss, retinal nerve fiber layer thinning, and irreversible optic nerve damage. Although elevated intraocular pressure (IOP) is a major risk factor, glaucoma pathogenesis also involves neuroinflammation, excitotoxicity, mitochondrial dysfunction, vascular dysregulation, and ECM remodeling - mechanisms that closely align with the biological actions of GLP-1RAs.
Preclinical studies consistently demonstrate robust neuroprotective and anti-inflammatory effects of GLP-1RAs. Both systemic and topical administration of GLP-1RA agents such as lixisenatide, liraglutide, semaglutide and the CNS-penetrant NLY01 reduce microglial/macrophage activation, protect RGCs and optic nerve axons from degeneration, preserve mitochondrial integrity, and prevent IOP elevation and vascular remodeling in diabetic and ocular hypertension models [49,50,51]. These multifaceted effects are thought to involve cAMP/PKA-mediated suppression of NF-κB signaling, reduced cytokine-driven secondary neurodegeneration, and improved mitochondrial homeostasis.
Clinical evidence mirrors these findings. A population-based case-control study of 1,961 patients reported significantly lower glaucoma incidence among GLP-1RA users with T2DM [52]. Several retrospective cohort studies similarly observed reduced rates of open-angle glaucoma in GLP-1RA-treated individuals compared with matched controls [53]. A large nationwide nested case-control study found a strong correlation between GLP-1RAs treatment with a 19% reduction in glaucoma onset, particularly among patients with more than three years of exposure [54]. Additional real-world data indicate reduced risk of glaucoma and ocular hypertension at 1-, 2-, and 3-year follow-up, suggesting early benefits that may accumulate over time, although differences in background antidiabetic therapy may contribute to heterogeneity [55]. Notably, a recent large retrospective cohort of 61,057 overweight or obese nondiabetic patients showed significantly lower risk of primary open-angle glaucoma (POAG) and ocular hypertension at 3- and 5-year follow-up among GLP-1RA users compared with alternative weight-loss medications [56]. Although these findings are observational, the consistency across datasets and alignment with mechanistic pathways strengthen the biological plausibility that GLP-1RAs may function as disease-modifying neuroprotectants in glaucoma.
3.2. Diabetic Retinopathy (DR)
DR arises from chronic hyperglycemia-induced metabolic stress, leading to microvascular degeneration, inflammatory activation, BRB breakdown, neuronal dysfunction, and retinal ischemia. Neurodegeneration frequently precedes microvascular lesions, highlighting the need for therapies targeting early neuronal injury. Clinically, DR is divided into two broad forms; an early non-proliferative form (NPDR) characterized by pericyte loss, vascular permeability, capillary occlusion, and basement membrane thickening and an advanced proliferative form (PDR) featuring vitreous hemorrhage, pathological neovascularization, and retinal detachment. A key pathological feature common to both forms of DR is diabetic macula edema (DME), which is a consequence of BRB breakdown leading to intraretinal plasma leakage, retinal swelling, and vision loss [57]. GLP-1RAs target upstream drivers and stabilize BRB integrity, positioning them as potential neurovascular disease-modifying agents beyond glucose lowering [58].
Preclinical studies demonstrate neuroprotective effects of GLP-1RAs on the retina across multiple diabetic models. GLP-1RAs prevent retinal neurodegeneration by reducing apoptosis, facilitating presynaptic GABA release and improving synaptic function in RGCs [59]. Exendin-4 inhibits voltage-gated calcium channels, promoting RGC survival under diabetic stress [60]. GLP-1RAs reduce inflammatory macrophage frequency and downregulate MCP-1 and chemokines (CXCL-1/10, CCL-2) that promote retinal leukostasis. GLP-1RAs shift microglia from M1- to M2-like phenotypes, suppressing NF-κB and NLRP3 inflammasome activity [61,62]. Liraglutide and related agents also upregulate tight-junction proteins, reduce vascular leakage, and preserve BRB integrity [63,64]. These findings indicate that GLP-1RAs act on both neuronal and microvascular components, supporting the hypothesis that GLP-1RAs may act as “upstream” DR therapeutics, intervening before irreversible vascular damage occurs.
Clinical data on DR are more heterogeneous due to differences in baseline DR severity, glycemic control trajectories, and patient selection. A meta-analysis of randomized controlled trials (RCTs) reported increased early-stage DR events versus placebo, but reduced progression to advanced DR compared with insulin therapy, suggesting context-dependent risk [65]. Mendelian randomization analyses found an inverse association between GLP-1R expression and severe DR, indicating the potential of GLP-1RAs in reducing the risk of DR in T2DM patients [66]. However, the SUSTAIN-6 trial identified a higher rate of DR complications with semaglutide (HR 1.76), particularly in patients with pre-existing moderate-severe DR and large, rapid reductions in HbA1c, supporting the “early worsening” phenomenon seen with other potent glucose-lowering therapies [18,67,68]. In contrast, EXSCEL (exenatide) showed no significant differences in DR outcomes compared with placebo [69]. Overall, these findings do not negate the potential benefits of GLP-1RAs, but instead emphasize the importance of risk stratification, avoiding overly rapid glycemic correction, and close retinal monitoring during treatment initiation in individuals with established DR.
3.3. Age-Related Macular Degeneration (AMD)
AMD is a leading cause of irreversible central vision loss in older adults and remains a major unmet need despite anti-VEGF therapies and emerging complement inhibitors [70,71]. Chronic inflammation, metabolic dysfunction, mitochondrial impairment, oxidative damage, and ECM remodeling contribute to both early non-exudative AMD and progression to geographic atrophy (GA) or neovascular AMD (nAMD) [72]. Given that GLP-1RAs modulate many of these pathways, interest in their potential role in AMD pathobiology has grown.
Preclinical research, though limited, is promising. A recent study demonstrates that liraglutide suppresses NLRP3 inflammasome activation and reduces IL-1β release in laser-induced choroidal neovascularization (CNV), significantly reducing CNV lesion area [73]. This suggests that GLP-1RAs may modulate innate immune responses relevant to neovascular AMD pathogenesis.
Observational studies and large real-world datasets provide intriguing early evidence. A large retrospective cohort of nearly 10,000 GLP-1RA users show significantly lower rates of both non-exudative and exudative AMD compared with users of metformin, insulin, and statins [74]. Another diabetes cohorts similarly show significantly reduced onset and progression of AMD among GLP-1RA users, indicating possible disease-modifying effects in early-stage disease [75]. In a TriNetX analysis of >45,000 nondiabetic overweight/obese individuals, GLP-1RAs were associated with lower incidence of non-exudative AMD over 5- to 10-year follow-up, though no significant effect was seen on progression to nAMD [76]. Collectively, these findings suggest that GLP-1RAs may be most effective in early or intermediate AMD stages, where inflammatory and metabolic dysregulation dominate, but may have more limited roles in advanced angiogenic disease.
3.4. Cataract
Although cataract formation primarily involves lens-intrinsic protein aggregation and oxidative stress, systemic metabolic and inflammatory states influence risk. GLP-1RAs may reduce cataract development by improving systemic oxidative balance and metabolic stress; reducing chronic inflammation that accelerates lens opacification; modulating pathways that influence osmotic and glycation-related lens damage. A recent large retrospective cohort study leveraging the TriNetX Global Collaborative Network reported significantly reduced risk of age-related cataract among nondiabetic overweight/obese individuals treated with GLP-1RAs compared with other weight-loss medications or no pharmacotherapy [77]. Similar protective trends appear in T2DM populations, although prospective validation is needed. Given the long-time course of cataract development and the favorable safety profile of GLP-1RAs, prevention studies may be feasible.
3.5. Uveitis
Uveitis encompasses a diverse group of intraocular inflammatory conditions that can cause irreversible vision loss through persistent cytokine-mediated tissue injury, macular edema, and secondary glaucoma [78]. Non-infectious uveitis is strongly associated with dysregulated T-cell responses and aberrant innate immune activation. Emerging real-world evidence suggests that GLP-1RA use can reduce the risk of developing non-infectious uveitis. A large TriNetX-based cohort study reported a 51.7% relative reduction in risk of developing a new diagnosis of uveitis among GLP-1RA users compared with matched non-users, in both diabetic and non-diabetic populations [79]. Compared with other anti-diabetic agents, GLP-1RAs conferred greater protection than metformin and insulin, though slightly less than SGLT2 inhibitors. These data support further exploration of GLP-1RAs as systemic adjuncts in inflammatory ophthalmic diseases.
4. Safety Considerations
As the use of GLP-1RAs continues to expand for diabetes, obesity, and cardiometabolic indications, several ophthalmic safety signals have emerged from observational studies and pharmacovigilance datasets. Although such adverse events (AEs) remain rare, patterns across independent data sources warrant careful clinical attention. Importantly, the overall benefits of GLP-1RAs must be weighed against these potential risks, particularly in patients with pre-existing ocular vulnerability [80,81,82].
4.1. Nonarteritic Anterior Ischemic Optic Neuropathy (NAION)
Among reported ocular AEs, NAION has received the greatest scrutiny, particularly in relation to semaglutide. Multiple real-world datasets have reported higher NAION incidence among semaglutide users compared with matched non-users. A neuro-ophthalmology referral-registry cohort reported significantly higher NAION incidence among semaglutide users compared with matched non-GLP-1RA controls, with hazard ratios (HRs) of 4.28 in individuals with T2DM and 7.64 in those with obesity [83]. A large TriNetX diabetic cohort found an increased NAION risk emerging after at least two years of semaglutide exposure [84]. Danish/Norwegian register-based studies similarly showed approximately two-fold increase in NAION risk among semaglutide users, prompting regulatory review by both the European Medicines Agency (EMA) and the World Health Organization (WHO) [85,86]. Pharmacovigilance analyses using the FDA Adverse Event Reporting System (FAERS) and VigiBase demonstrated disproportionate reporting of NAION with semaglutide compared with other glucose-lowering medications [87,88,89]. Collectively, although these convergent signals highlight a potential association between GLP-1RA exposure, especially semaglutide, and NAION, causality has not been established. NAION is multifactorial and influenced by vascular risk, optic disc anatomy, sleep apnea, and systemic hemodynamic changes. The contribution of rapid metabolic shifts—including blood pressure changes and glycemic improvements—remains an area of active investigation.
4.2. Other Retinal and Optic Nerve Events
Beyond NAION, pharmacovigilance data have also identified signal enrichment for other rare ocular AEs – including retinopathy exacerbation, retinal detachment, vitreous hemorrhage and optic nerve disorders [90]. Although these events are uncommon, their emergence across multiple independent datasets suggests the need for continued monitoring, particularly as GLP-1RA use expands into larger and healthier populations where baseline ocular risk is lower.
4.3. Conflicting Evidence and Null Findings
Despite these concerning signals, several large and well-designed epidemiologic studies have not consistently replicated the elevated NAION risk. A large multinational population-based study found no significant increase in the risk of NAION among semaglutide users compared to those receiving other glucose-lowering or weight-loss medications [91]. A comprehensive systematic review and meta-analysis similarly concluded that the overall incidence of ocular AEs with semaglutide remains low, and that current evidence is insufficient to confirm a direct causal relationship [92]. These discrepancies highlight the limitations of current data, including heterogeneity in baseline vascular risk, DR severity, follow-up duration, and confounding by indication. Overall, current evidence supports a cautious but not prohibitive approach to GLP-1RA use from an ophthalmic safety perspective.
4.4. Clinical Implications
Given emerging but inconclusive data, clinicians should adopt a risk-informed monitoring strategy when prescribing GLP-1RAs, especially semaglutide. Patients, particularly those with risk factors such as pre-existing optic nerve vulnerability, severe sleep apnea, or vascular risk factors, may benefit from baseline ophthalmic evaluation prior to initiation of semaglutide or similar agents. Symptoms such as sudden visual field loss, dyschromatopsia, or decreased visual acuity, should prompt urgent ophthalmic referral. Close retinal monitoring should be performed during periods of rapid metabolic improvement in patients with moderate to severe diabetic retinopathy, as accelerated glycemic correction is associated with the well-characterized phenomenon of early DR worsening. As global use of GLP-1RAs continues to grow and expands to younger, healthier populations, prospective ophthalmology-specific studies and robust post-marketing surveillance will be essential for identifying true risk, clarifying mechanisms, and guiding evidence-based safety recommendations.
5. Challenges and Prospectives
Although GLP-1RAs show substantial promise as multi-target therapeutics for ocular disorders, several scientific, clinical, and translational barriers must be addressed before they can be reliably incorporated into routine ophthalmic care. The following subsections highlight key knowledge gaps and future directions necessary to fully realize the therapeutic potential of GLP-1RAs in vision science.
5.1. Need for Targeted Ocular Delivery Strategies
To date, most preclinical and clinical studies evaluating GLP-1RAs in ocular disease have relied on systemic administration, making it difficult to isolate direct ocular effects from improvements in glycemia, inflammation, or cardiovascular function. Because GLP-1RAs are large peptides with limited penetration across ocular barriers, the development of ocular-targeted delivery systems is essential. Future research should prioritize targeted ocular delivery approaches, including topical formulations designed for enhanced corneal or conjunctival penetration; intravitreal injections for achieving therapeutically relevant concentrations in retinal tissues; sustained-release platforms, including injectable depots or biodegradable implants; and viral vector-based gene therapy capable of achieving sustained intraocular or tissue-specific GLP-1R activation. Such approaches would minimize systemic confounding, reduce off-target exposure, and more precisely define the true retina-specific therapeutic index of GLP-1RAs.
5.2. Need for Rigorous Prospective Clinical Trials
Current human evidence for ocular benefits largely derives from retrospective cohort analyses or post-hoc evaluations of systemic trials not originally designed around ophthalmic outcomes. To validate GLP-1RAs as potential disease-modifying agents, prospective, ophthalmology-focused clinical trials are urgently needed, particularly those incorporating standardized measures of retinal structure with high-resolution structural imaging (OCT), vascular leakage and BRB integrity (OCT-A, fluorescein angiography), neurodegeneration biomarkers, inflammatory cytokine and chemokine profiling, and functional visual outcomes (ERG). Such trials should also evaluate GLP-1RA subclasses and dosing strategies to determine whether ocular effects are agent-specific or reflect a broader class mechanism.
5.3. Safety Evaluation and Risk Stratification
Given the context-dependent risk of early DR worsening and emerging safety concerns related to optic nerve adverse events, a more refined understanding of patient-level susceptibility is needed. Future studies must identify risk factors for adverse outcomes (e.g., pre-existing DR severity, rate of HbA1c decline, vascular comorbidities, or severe sleep apnea), define safe thresholds and timeframes for glycemic correction in high-risk eyes; establish standardized monitoring protocols to detect early signs of NAION, optic neuropathy, or accelerated DR progression; and compare ocular safety profiles across individual GLP-1RAs, dual agonists (e.g., tirzepatide) and emerging multi-agonist therapy. A precision-medicine approach will be essential to maximize therapeutic benefit while minimizing risk.
5.4. Implications for the Ophthalmic Community
As GLP-1RA use expands globally across metabolic, cardiovascular, and weight-management indications, ophthalmologists are uniquely positioned to define their role as potential disease-modifying agents in eye care. Moving forward, the field should integrate molecular insights from retinal biology and neuroinflammation; advanced ocular imaging and functional testing, real-world data from large health-system datasets, and patient-specific risk stratification based on systemic and ocular characteristics. By bringing together molecular mechanisms, clinical imaging, and population-based data, the ophthalmic community can help identify which patients and disease stages stand to benefit most from GLP-1RA therapy. If these knowledge gaps are addressed, GLP-1RAs may represent a new class of multimodal therapeutics targeting shared neurovascular and inflammatory pathways underlying many of the leading causes of vision loss.
6. Conclusions
GLP-1RAs are emerging as compelling multi-target therapeutic candidates for ocular diseases, owing to their convergent actions on neuroinflammation, mitochondrial dysfunction, oxidative stress, and vascular instability. Across glaucoma, DR, AMD, and other retinal and optic nerve disorders, both preclinical and clinical evidence consistently points to protective effects on neuronal survival, vascular integrity, and inflammatory responses. These benefits appear to extend beyond glycemic control, suggesting a broader potential for GLP-1RAs as disease-modifying agents in ophthalmology.
Despite this encouraging trajectory, important challenges remain. Current clinical data are derived largely from retrospective analyses or systemic trials not designed with ophthalmic endpoints in mind, making it difficult to disentangle direct ocular effects from systemic metabolic improvements. Additionally, emerging safety considerations—such as early DR worsening in patients with rapid glycemic correction and rare optic nerve events including NAION—underscore the need for careful patient selection, structured monitoring, and mechanistically informed risk stratification.
Looking ahead, the development of ocular-targeted delivery methods, combined with rigorously designed prospective clinical trials incorporating structural, vascular, inflammatory, and functional endpoints, will be essential for determining the true therapeutic potential of GLP-1RAs in ocular disease.
With continued multidisciplinary investigation and thoughtful clinical integration, GLP-1RAs have the potential to inaugurate a new class of therapeutics aimed at the shared neurovascular and inflammatory mechanisms that contribute to the most common causes of irreversible vision loss worldwide.
Author Contributions
Conceptualization, X.G.; investigation, X.G., F.Ӧ.; writing - original draft preparation, X.G.; writing - review and editing, F.Ö.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The authors thank colleagues at the Vision Center and Rebecca D. Considine Research Institute for insightful discussions and support.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Drucker, D.J. GLP-1-based therapies for diabetes, obesity and beyond. Nat Rev Drug Discov 2025, 24, 631–650. [Google Scholar] [CrossRef]
- Wong, C.K.; Drucker, D.J. Antiinflammatory actions of glucagon-like peptide-1-based therapies beyond metabolic benefits. J Clin Invest 2025, 135. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.L.; Finn, A.P. Glucagon-like peptide-1 receptor agonists and the eye. Curr Opin Ophthalmol 2025, 36, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Jayaram, H.; Kolko, M.; Friedman, D.S.; Gazzard, G. Glaucoma: now and beyond. Lancet 2023, 402, 1788–1801. [Google Scholar] [CrossRef] [PubMed]
- Talebi, R.; Fortes, B.H.; Yu, F.; Coleman, A.L.; Tsui, I. Real-world Associations Between GLP-1 Receptor Agonist Use and Diabetic Retinopathy Accounting for Longitudinal Glycemic Control. Retina 2025. [Google Scholar] [CrossRef]
- Nadeem, N.; Al Issa, R.M.; Shah, A.; Wardeh, R.; Rashid, F.; Abdelgadir, E.I.; Bashier, A. In The Eye Of Controversy: A Deeper Look Into The Impact Of Glucagon-Like Peptide 1 Receptor Agonists (GLP1RA) on Diabetic Retinopathy and Non-arteritic anterior ischemic optic neuropathy (NAION). Can J Diabetes 2025. [Google Scholar] [CrossRef]
- Tauqeer, Z.; Bracha, P.; Hua, P.; Yu, Y.; Cui, Q.N.; VanderBeek, B.L. Glucagon-Like Peptide-1 Receptor Agonists are Not Associated with an Increased Risk of Progressing to Vision-Threatening Diabetic Retinopathy. Ophthalmic Epidemiol 2025, 32, 390–393. [Google Scholar] [CrossRef]
- Hebsgaard, J.B.; Pyke, C.; Yildirim, E.; Knudsen, L.B.; Heegaard, S.; Kvist, P.H. Glucagon-like peptide-1 receptor expression in the human eye. Diabetes Obes Metab 2018, 20, 2304–2308. [Google Scholar] [CrossRef]
- Puddu, A.; Sanguineti, R.; Montecucco, F.; Viviani, G.L. Retinal pigment epithelial cells express a functional receptor for glucagon-like peptide-1 (GLP-1). Mediators Inflamm 2013, 2013, 975032. [Google Scholar] [CrossRef]
- Drucker, D.J. Mechanisms of Action and Therapeutic Application of Glucagon-like Peptide-1. Cell Metab 2018, 27, 740–756. [Google Scholar] [CrossRef]
- Zheng, Z.; Zong, Y.; Ma, Y.; Tian, Y.; Pang, Y.; Zhang, C.; Gao, J. Glucagon-like peptide-1 receptor: mechanisms and advances in therapy. Signal Transduct Target Ther 2024, 9, 234. [Google Scholar] [CrossRef]
- Cui, Q.N.; Stein, L.M.; Fortin, S.M.; Hayes, M.R. The role of glia in the physiology and pharmacology of glucagon-like peptide-1: implications for obesity, diabetes, neurodegeneration and glaucoma. Br J Pharmacol 2022, 179, 715–726. [Google Scholar] [CrossRef] [PubMed]
- Amaral, D.C.; Guedes, J.; Cruz, M.R.B.; Cheidde, L.; Nepomuceno, M.; Magalhaes, P.L.M.; Brazuna, R.; Mora-Paez, D.J.; Huang, P.; Razeghinejad, R.; et al. GLP-1 Receptor Agonists Use and Incidence of Glaucoma: A Systematic Review and Meta-Analysis. Am J Ophthalmol 2025, 271, 488–497. [Google Scholar] [CrossRef] [PubMed]
- Asif, M.; Asif, A.; Rahman, U.A.; Farooqi, H.A.; Fatima, O.; Ali, W.; Jafar, U.; Jaber, M.H. Incidence of Glaucoma in Type 2 Diabetes Patients Treated With GLP-1 Receptor Agonists: A Systematic Review and Meta-Analysis. Endocrinol Diabetes Metab 2025, 8, e70059. [Google Scholar] [CrossRef] [PubMed]
- Talcott, K.E.; Rachitskaya, A.V.; Singh, R.P. Glucagon-Like Peptide-1 Receptor Agonist Use and Age-Related Macular Degeneration-Where Do We Stand? JAMA Ophthalmol 2025. [Google Scholar] [CrossRef]
- Hsu, A.Y.; Kuo, H.T.; Wang, Y.H.; Lin, C.J.; Shao, Y.C.; Chiang, C.C.; Hsia, N.Y.; Lai, C.T.; Tseng, H.; Wu, B.Q.; et al. Semaglutide and Nonarteritic Anterior Ischemic Optic Neuropathy Risk Among Patients With Diabetes. JAMA Ophthalmol 2025, 143, 400–407. [Google Scholar] [CrossRef]
- Amini, A.; Hamann, S.; Larsen, M. Semaglutide and non-arteritic anterior ischaemic optic neuropathy: Review and interpretation of reported association. Acta Ophthalmol 2025, 103, 615–621. [Google Scholar] [CrossRef]
- Marso, S.P.; Bain, S.C.; Consoli, A.; Eliaschewitz, F.G.; Jodar, E.; Leiter, L.A.; Lingvay, I.; Rosenstock, J.; Seufert, J.; Warren, M.L.; et al. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N Engl J Med 2016, 375, 1834–1844. [Google Scholar] [CrossRef]
- Yoshida, Y.; Joshi, P.; Barri, S.; Wang, J.; Corder, A.L.; O’Connell, S.S.; Fonseca, V.A. Progression of retinopathy with glucagon-like peptide-1 receptor agonists with cardiovascular benefits in type 2 diabetes - A systematic review and meta-analysis. J Diabetes Complications 2022, 36, 108255. [Google Scholar] [CrossRef]
- Shor, R.; Mihalache, A.; Noori, A.; Shor, R.; Kohly, R.P.; Popovic, M.M.; Muni, R.H. Glucagon-Like Peptide-1 Receptor Agonists and Risk of Neovascular Age-Related Macular Degeneration. JAMA Ophthalmol 2025, 143, 587–594. [Google Scholar] [CrossRef]
- Xie, Z.; Yang, Z.; Tian, D.; Chen, Y. Unlocking the potential of GLP-1 receptor agonists in ocular therapeutics: from molecular pathways to clinical impact. Front Pharmacol 2025, 16, 1618079. [Google Scholar] [CrossRef] [PubMed]
- Usategui-Martin, R.; Fernandez-Bueno, I. Neuroprotective therapy for retinal neurodegenerative diseases by stem cell secretome. Neural Regen Res 2021, 16, 117–118. [Google Scholar] [CrossRef] [PubMed]
- Cuenca, N.; Fernandez-Sanchez, L.; Campello, L.; Maneu, V.; De la Villa, P.; Lax, P.; Pinilla, I. Cellular responses following retinal injuries and therapeutic approaches for neurodegenerative diseases. Prog Retin Eye Res 2014, 43, 17–75. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, C.R.; Andersen, A.; Knop, F.K.; Vilsboll, T. How glucagon-like peptide 1 receptor agonists work. Endocr Connect 2021, 10, R200–R212. [Google Scholar] [CrossRef]
- Zhang, T.; Ruan, H.Z.; Wang, Y.C.; Shao, Y.Q.; Zhou, W.; Weng, S.J.; Zhong, Y.M. Signaling Mechanism for Modulation by GLP-1 and Exendin-4 of GABA Receptors on Rat Retinal Ganglion Cells. Neurosci Bull 2022, 38, 622–636. [Google Scholar] [CrossRef]
- Shao, Y.Q.; Wang, Y.C.; Wang, L.; Ruan, H.Z.; Liu, Y.F.; Zhang, T.H.; Weng, S.J.; Yang, X.L.; Zhong, Y.M. Topical administration of GLP-1 eyedrops improves retinal ganglion cell function by facilitating presynaptic GABA release in early experimental diabetes. Neural Regen Res 2026, 21, 800–810. [Google Scholar] [CrossRef]
- Cai, X.; Li, J.; Wang, M.; She, M.; Tang, Y.; Li, J.; Li, H.; Hui, H. GLP-1 Treatment Improves Diabetic Retinopathy by Alleviating Autophagy through GLP-1R-ERK1/2-HDAC6 Signaling Pathway. Int J Med Sci 2017, 14, 1203–1212. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.R.; Ma, X.F.; Lin, W.J.; Hao, M.; Yu, X.Y.; Li, H.X.; Xu, C.Y.; Kuang, H.Y. Neuroprotective Role of GLP-1 Analog for Retinal Ganglion Cells via PINK1/Parkin-Mediated Mitophagy in Diabetic Retinopathy. Front Pharmacol 2020, 11, 589114. [Google Scholar] [CrossRef]
- Goncalves, A.; Lin, C.M.; Muthusamy, A.; Fontes-Ribeiro, C.; Ambrosio, A.F.; Abcouwer, S.F.; Fernandes, R.; Antonetti, D.A. Protective Effect of a GLP-1 Analog on Ischemia-Reperfusion Induced Blood-Retinal Barrier Breakdown and Inflammation. Invest Ophthalmol Vis Sci 2016, 57, 2584–2592. [Google Scholar] [CrossRef]
- Zhou, L.; Xu, Z.; Oh, Y.; Gamuyao, R.; Lee, G.; Xie, Y.; Cho, H.; Lee, S.; Duh, E.J. Myeloid cell modulation by a GLP-1 receptor agonist regulates retinal angiogenesis in ischemic retinopathy. JCI Insight 2021, 6. [Google Scholar] [CrossRef]
- Shan, Y.; Gao, X.; Zhao, K.; Xu, C.; Li, H.; Hu, Y.; Lin, W.; Ma, X.; Xu, Q.; Kuang, H.; et al. Liraglutide intervention improves high-glucose-induced reactive gliosis of Muller cells and ECM dysregulation. Mol Cell Endocrinol 2023, 576, 112013. [Google Scholar] [CrossRef] [PubMed]
- Whitcup, S.M.; Nussenblatt, R.B.; Lightman, S.L.; Hollander, D.A. Inflammation in retinal disease. Int J Inflam 2013, 2013, 724648. [Google Scholar] [CrossRef] [PubMed]
- Soto, I.; Krebs, M.P.; Reagan, A.M.; Howell, G.R. Vascular Inflammation Risk Factors in Retinal Disease. Annu Rev Vis Sci 2019, 5, 99–122. [Google Scholar] [CrossRef] [PubMed]
- Egwuagu, C.E. Chronic intraocular inflammation and development of retinal degenerative disease. Adv Exp Med Biol 2014, 801, 417–425. [Google Scholar] [CrossRef]
- Petrillo, F.; Gesualdo, C.; Platania, C.B.M.; D’Amico, M.; Trotta, M.C. Editorial: Chronic Inflammation and Neurodegeneration in Retinal Disease. Front Pharmacol 2021, 12, 784770. [Google Scholar] [CrossRef]
- Puddu, A.; Maggi, D. Anti-Inflammatory Effects of GLP-1R Activation in the Retina. Int J Mol Sci 2022, 23. [Google Scholar] [CrossRef]
- Hogan, A.E.; Gaoatswe, G.; Lynch, L.; Corrigan, M.A.; Woods, C.; O’Connell, J.; O’Shea, D. Glucagon-like peptide 1 analogue therapy directly modulates innate immune-mediated inflammation in individuals with type 2 diabetes mellitus. Diabetologia 2014, 57, 781–784. [Google Scholar] [CrossRef]
- Hernandez, C.; Bogdanov, P.; Corraliza, L.; Garcia-Ramirez, M.; Sola-Adell, C.; Arranz, J.A.; Arroba, A.I.; Valverde, A.M.; Simo, R. Topical Administration of GLP-1 Receptor Agonists Prevents Retinal Neurodegeneration in Experimental Diabetes. Diabetes 2016, 65, 172–187. [Google Scholar] [CrossRef]
- Pontes-da-Silva, R.M.; de Souza Marinho, T.; de Macedo Cardoso, L.E.; Mandarim-de-Lacerda, C.A.; Aguila, M.B. Obese mice weight loss role on nonalcoholic fatty liver disease and endoplasmic reticulum stress treated by a GLP-1 receptor agonist. Int J Obes (Lond) 2022, 46, 21–29. [Google Scholar] [CrossRef]
- Christou, G.A.; Katsiki, N.; Blundell, J.; Fruhbeck, G.; Kiortsis, D.N. Semaglutide as a promising antiobesity drug. Obes Rev 2019, 20, 805–815. [Google Scholar] [CrossRef]
- Robinson, E.; Cassidy, R.S.; Tate, M.; Zhao, Y.; Lockhart, S.; Calderwood, D.; Church, R.; McGahon, M.K.; Brazil, D.P.; McDermott, B.J.; et al. Exendin-4 protects against post-myocardial infarction remodelling via specific actions on inflammation and the extracellular matrix. Basic Res Cardiol 2015, 110, 20. [Google Scholar] [CrossRef]
- Sampedro, J.; Bogdanov, P.; Ramos, H.; Sola-Adell, C.; Turch, M.; Valeri, M.; Simo-Servat, O.; Lagunas, C.; Simo, R.; Hernandez, C. New Insights into the Mechanisms of Action of Topical Administration of GLP-1 in an Experimental Model of Diabetic Retinopathy. J Clin Med 2019, 8. [Google Scholar] [CrossRef]
- Liddelow, S.A.; Guttenplan, K.A.; Clarke, L.E.; Bennett, F.C.; Bohlen, C.J.; Schirmer, L.; Bennett, M.L.; Munch, A.E.; Chung, W.S.; Peterson, T.C.; et al. Neurotoxic reactive astrocytes are induced by activated microglia. Nature 2017, 541, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Guttenplan, K.A.; Stafford, B.K.; El-Danaf, R.N.; Adler, D.I.; Munch, A.E.; Weigel, M.K.; Huberman, A.D.; Liddelow, S.A. Neurotoxic Reactive Astrocytes Drive Neuronal Death after Retinal Injury. Cell Rep 2020, 31, 107776. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.K.; Yusta, B.; Koehler, J.A.; Baggio, L.L.; McLean, B.A.; Matthews, D.; Seeley, R.J.; Drucker, D.J. Divergent roles for the gut intraepithelial lymphocyte GLP-1R in control of metabolism, microbiota, and T cell-induced inflammation. Cell Metab 2022, 34, 1514–1531 e1517. [Google Scholar] [CrossRef] [PubMed]
- Oh, Y.S.; Jun, H.S. Effects of Glucagon-Like Peptide-1 on Oxidative Stress and Nrf2 Signaling. Int J Mol Sci 2017, 19. [Google Scholar] [CrossRef]
- Tu, Y.; Li, L.; Zhu, L.; Guo, Y.; Du, S.; Zhang, Y.; Wang, Z.; Zhang, Y.; Zhu, M. Geniposide Attenuates Hyperglycemia-Induced Oxidative Stress and Inflammation by Activating the Nrf2 Signaling Pathway in Experimental Diabetic Retinopathy. Oxid Med Cell Longev 2021, 2021, 9247947. [Google Scholar] [CrossRef]
- Ren, X.; Sun, L.; Wei, L.; Liu, J.; Zhu, J.; Yu, Q.; Kong, H.; Kong, L. Liraglutide Up-regulation Thioredoxin Attenuated Muller Cells Apoptosis in High Glucose by Regulating Oxidative Stress and Endoplasmic Reticulum Stress. Curr Eye Res 2020, 45, 1283–1291. [Google Scholar] [CrossRef]
- Sterling, J.K.; Adetunji, M.O.; Guttha, S.; Bargoud, A.R.; Uyhazi, K.E.; Ross, A.G.; Dunaief, J.L.; Cui, Q.N. GLP-1 Receptor Agonist NLY01 Reduces Retinal Inflammation and Neuron Death Secondary to Ocular Hypertension. Cell Rep 2020, 33, 108271. [Google Scholar] [CrossRef]
- Lawrence, E.C.N.; Guo, M.; Schwartz, T.D.; Wu, J.; Lu, J.; Nikonov, S.; Sterling, J.K.; Cui, Q.N. Topical and systemic GLP-1R agonist administration both rescue retinal ganglion cells in hypertensive glaucoma. Front Cell Neurosci 2023, 17, 1156829. [Google Scholar] [CrossRef]
- Mouhammad, Z.A.; Rombaut, A.; Bermudez, M.Y.G.; Vohra, R.; Tribble, J.R.; Williams, P.A.; Kolko, M. Systemic semaglutide provides a mild vasoprotective and antineuroinflammatory effect in a rat model of ocular hypertensive glaucoma. Mol Brain 2025, 18, 54. [Google Scholar] [CrossRef]
- Sterling, J.; Hua, P.; Dunaief, J.L.; Cui, Q.N.; VanderBeek, B.L. Glucagon-like peptide 1 receptor agonist use is associated with reduced risk for glaucoma. Br J Ophthalmol 2023, 107, 215–220. [Google Scholar] [CrossRef]
- Chuang, C.C.; Wang, K.; Chang, C.K.; Lee, C.Y.; Huang, J.Y.; Wu, H.H.; Yang, P.J.; Yang, S.F. Prescription of glucagon-like peptide 1 agonists and risk of subsequent open-angle glaucoma in individuals with type 2 diabetes mellitus. Int J Med Sci 2024, 21, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Niazi, S.; Gnesin, F.; Thein, A.S.; Andreasen, J.R.; Horwitz, A.; Mouhammad, Z.A.; Jawad, B.N.; Niazi, Z.; Pourhadi, N.; Zareini, B.; et al. Association between Glucagon-like Peptide-1 Receptor Agonists and the Risk of Glaucoma in Individuals with Type 2 Diabetes. Ophthalmology 2024, 131, 1056–1063. [Google Scholar] [CrossRef] [PubMed]
- Muayad, J.; Loya, A.; Hussain, Z.S.; Chauhan, M.Z.; Alsoudi, A.F.; De Francesco, T.; Ahmed, I.I.K. Comparative Effects of Glucagon-like Peptide 1 Receptor Agonists and Metformin on Glaucoma Risk in Patients with Type 2 Diabetes. Ophthalmology 2025, 132, 271–279. [Google Scholar] [CrossRef] [PubMed]
- Vasu, P.; Dorairaj, E.A.; Weinreb, R.N.; Huang, A.S.; Dorairaj, S.K. Risk of Glaucoma in Patients without Diabetes Using a Glucagon-Like Peptide 1 Receptor Agonist. Ophthalmology 2025, 132, 859–868. [Google Scholar] [CrossRef]
- Duh, E.J.; Sun, J.K.; Stitt, A.W. Diabetic retinopathy: current understanding, mechanisms, and treatment strategies. JCI Insight 2017, 2. [Google Scholar] [CrossRef]
- Varughese, G.I.; Jacob, S. Existing and emerging GLP-1 receptor agonist therapy: Ramifications for diabetic retinopathy screening. J R Coll Physicians Edinb 2024, 54, 170–173. [Google Scholar] [CrossRef]
- Liu, J.; Wang, H.; Huang, C. Exendin-4, a GLP-1 receptor agonist, suppresses diabetic retinopathy in vivo and in vitro. Arch Physiol Biochem 2025, 131, 1–10. [Google Scholar] [CrossRef]
- Wang, Y.C.; Wang, L.; Shao, Y.Q.; Weng, S.J.; Yang, X.L.; Zhong, Y.M. Exendin-4 promotes retinal ganglion cell survival and function by inhibiting calcium channels in experimental diabetes. iScience 2023, 26, 107680. [Google Scholar] [CrossRef]
- Wang, Z.J.; Han, W.N.; Chai, S.F.; Li, Y.; Fu, C.J.; Wang, C.F.; Cai, H.Y.; Li, X.Y.; Wang, X.; Holscher, C.; et al. Semaglutide promotes the transition of microglia from M1 to M2 type to reduce brain inflammation in APP/PS1/tau mice. Neuroscience 2024, 563, 222–234. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.K.; McLean, B.A.; Baggio, L.L.; Koehler, J.A.; Hammoud, R.; Rittig, N.; Yabut, J.M.; Seeley, R.J.; Brown, T.J.; Drucker, D.J. Central glucagon-like peptide 1 receptor activation inhibits Toll-like receptor agonist-induced inflammation. Cell Metab 2024, 36, 130–143 e135. [Google Scholar] [CrossRef] [PubMed]
- Wei, L.; Mo, W.; Lan, S.; Yang, H.; Huang, Z.; Liang, X.; Li, L.; Xian, J.; Xie, X.; Qin, Y.; et al. GLP-1 RA Improves Diabetic Retinopathy by Protecting the Blood-Retinal Barrier through GLP-1R-ROCK-p-MLC Signaling Pathway. J Diabetes Res 2022, 2022, 1861940. [Google Scholar] [CrossRef] [PubMed]
- Oezer, K.; Kolibabka, M.; Gassenhuber, J.; Dietrich, N.; Fleming, T.; Schlotterer, A.; Morcos, M.; Wohlfart, P.; Hammes, H.P. The effect of GLP-1 receptor agonist lixisenatide on experimental diabetic retinopathy. Acta Diabetol 2023, 60, 1551–1565. [Google Scholar] [CrossRef]
- Kapoor, I.; Sarvepalli, S.M.; D’Alessio, D.; Grewal, D.S.; Hadziahmetovic, M. GLP-1 receptor agonists and diabetic retinopathy: A meta-analysis of randomized clinical trials. Surv Ophthalmol 2023, 68, 1071–1083. [Google Scholar] [CrossRef]
- Zheng, D.; Li, N.; Hou, R.; Zhang, X.; Wu, L.; Sundquist, J.; Sundquist, K.; Ji, J. Glucagon-like peptide-1 receptor agonists and diabetic retinopathy: nationwide cohort and Mendelian randomization studies. BMC Med 2023, 21, 40. [Google Scholar] [CrossRef]
- Vilsboll, T.; Bain, S.C.; Leiter, L.A.; Lingvay, I.; Matthews, D.; Simo, R.; Helmark, I.C.; Wijayasinghe, N.; Larsen, M. Semaglutide, reduction in glycated haemoglobin and the risk of diabetic retinopathy. Diabetes Obes Metab 2018, 20, 889–897. [Google Scholar] [CrossRef]
- Akil, H.; Burgess, J.; Nevitt, S.; Harding, S.P.; Alam, U.; Burgess, P. Early Worsening of Retinopathy in Type 1 and Type 2 Diabetes After Rapid Improvement in Glycaemic Control: A Systematic Review. Diabetes Ther 2022, 13, 1–23. [Google Scholar] [CrossRef]
- Bethel, M.A.; Stevens, S.R.; Buse, J.B.; Choi, J.; Gustavson, S.M.; Iqbal, N.; Lokhnygina, Y.; Mentz, R.J.; Patel, R.A.; Ohman, P.; et al. Exploring the Possible Impact of Unbalanced Open-Label Drop-In of Glucose-Lowering Medications on EXSCEL Outcomes. Circulation 2020, 141, 1360–1370. [Google Scholar] [CrossRef]
- Fleckenstein, M.; Keenan, T.D.L.; Guymer, R.H.; Chakravarthy, U.; Schmitz-Valckenberg, S.; Klaver, C.C.; Wong, W.T.; Chew, E.Y. Age-related macular degeneration. Nat Rev Dis Primers 2021, 7, 31. [Google Scholar] [CrossRef]
- Rush, R.B.; Klein, W.; Reinauer, R.M. Real-World Outcomes with Complement Inhibitors for Geographic Atrophy: A Comparative Study of Pegacetacoplan versus Avacincaptad Pegol. Clin Ophthalmol 2025, 19, 1167–1174. [Google Scholar] [CrossRef] [PubMed]
- Fleckenstein, M.; Mitchell, P.; Freund, K.B.; Sadda, S.; Holz, F.G.; Brittain, C.; Henry, E.C.; Ferrara, D. The Progression of Geographic Atrophy Secondary to Age-Related Macular Degeneration. Ophthalmology 2018, 125, 369–390. [Google Scholar] [CrossRef] [PubMed]
- Machida, A.; Suzuki, K.; Nakayama, T.; Miyagi, S.; Maekawa, Y.; Murakami, R.; Uematsu, M.; Kitaoka, T.; Oishi, A. Glucagon-Like Peptide 1 Receptor Agonist Stimulation Inhibits Laser-Induced Choroidal Neovascularization by Suppressing Intraocular Inflammation. Invest Ophthalmol Vis Sci 2025, 66, 15. [Google Scholar] [CrossRef] [PubMed]
- Allan, K.C.; Joo, J.H.; Kim, S.; Shaia, J.; Kaelber, D.C.; Singh, R.; Talcott, K.E.; Rachitskaya, A.V. Glucagon-like Peptide-1 Receptor Agonist Impact on Chronic Ocular Disease Including Age-Related Macular Degeneration. Ophthalmology 2025, 132, 748–757. [Google Scholar] [CrossRef]
- McLaughlin, S.A.; Davila, N.; Shields, C.; Bineshfar, N.; Banaee, T.; Williams, B.K., Jr. Impact of GLP-1 receptor agonists for type 2 diabetes mellitus on the development and progression of age-related macular degeneration. Retina 2025. [Google Scholar] [CrossRef]
- Ahuja, A.S.; Paredes, A.A., 3rd; Young, B.K. Glucagon-Like Peptide-1 Receptor Agonists and Age-Related Macular Degeneration. JAMA Ophthalmol 2025. [Google Scholar] [CrossRef]
- Ahuja, A.S.; Paredes, A.A., 3rd; Ahuja, S.A.; Young, B.K. Glucagon-like Peptide-1 Receptor Agonist Use and Risk of Cataract Development. Am J Ophthalmol 2026, 281, 666–673. [Google Scholar] [CrossRef]
- Seve, P.; Cacoub, P.; Bodaghi, B.; Trad, S.; Sellam, J.; Bellocq, D.; Bielefeld, P.; Sene, D.; Kaplanski, G.; Monnet, D.; et al. Uveitis: Diagnostic work-up. A literature review and recommendations from an expert committee. Autoimmun Rev 2017, 16, 1254–1264. [Google Scholar] [CrossRef]
- Mohan, N.; Srivastava, S.K.; Schulgit, M.J.; Nowacki, A.S.; Kaelber, D.C.; Sharma, S. Glucagon-Like Peptide-1 Receptor Agonists and Risk of Uveitis. JAMA Ophthalmol 2025, 143, 823–832. [Google Scholar] [CrossRef]
- Ntentakis, D.P.; Correa, V.; Ntentaki, A.M.; Delavogia, E.; Narimatsu, T.; Efstathiou, N.E.; Vavvas, D.G. Effects of newer-generation anti-diabetics on diabetic retinopathy: a critical review. Graefes Arch Clin Exp Ophthalmol 2024, 262, 717–752. [Google Scholar] [CrossRef]
- Singh, H.; Natt, N.K.; Nim, D.K. Association between glucagon-like peptide-1 agonists and risk of diabetic retinopathy: a disproportionality analysis using FDA adverse event reporting system data. Expert Rev Endocrinol Metab 2025, 20, 147–152. [Google Scholar] [CrossRef]
- Carter, P.; Simo, R.; Lovestam-Adrian, M.; Pearce, I.; Bain, S.C.; Dinah, C.; Davies, S.J.; Strain, W.D.; Burgess, P.; Gamble, A.; et al. Addressing the risk of ocular complications of GLP-1RAs; a multi-disciplinary expert consensus. Diabetes Obes Metab 2025, 27, 7535–7543. [Google Scholar] [CrossRef] [PubMed]
- Hathaway, J.T.; Shah, M.P.; Hathaway, D.B.; Zekavat, S.M.; Krasniqi, D.; Gittinger, J.W., Jr.; Cestari, D.; Mallery, R.; Abbasi, B.; Bouffard, M.; et al. Risk of Nonarteritic Anterior Ischemic Optic Neuropathy in Patients Prescribed Semaglutide. JAMA Ophthalmol 2024, 142, 732–739. [Google Scholar] [CrossRef] [PubMed]
- Cai, C.X.; Hribar, M.; Baxter, S.; Goetz, K.; Swaminathan, S.S.; Flowers, A.; Brown, E.N.; Toy, B.; Xu, B.; Chen, J.; et al. Semaglutide and Nonarteritic Anterior Ischemic Optic Neuropathy. JAMA Ophthalmol 2025, 143, 304–314. [Google Scholar] [CrossRef] [PubMed]
- Simonsen, E.; Lund, L.C.; Ernst, M.T.; Hjellvik, V.; Hegedus, L.; Hamann, S.; Jorstad, O.K.; Gulseth, H.L.; Karlstad, O.; Pottegard, A. Use of semaglutide and risk of non-arteritic anterior ischemic optic neuropathy: A Danish-Norwegian cohort study. Diabetes Obes Metab 2025, 27, 3094–3103. [Google Scholar] [CrossRef]
- Grauslund, J.; Taha, A.A.; Molander, L.D.; Kawasaki, R.; Moller, S.; Hojlund, K.; Stokholm, L. Once-weekly semaglutide doubles the five-year risk of nonarteritic anterior ischemic optic neuropathy in a Danish cohort of 424,152 persons with type 2 diabetes. Int J Retina Vitreous 2024, 10, 97. [Google Scholar] [CrossRef]
- Azab, M.; Pasina, L. Semaglutide: Nonarteritic Anterior Ischemic Optic Neuropathy in the FDA adverse event reporting system - A disproportionality analysis. Obes Res Clin Pract 2025, 19, 77–79. [Google Scholar] [CrossRef]
- Zhou, J.; Huang, W.; Xie, Y.; Shen, H.; Liu, M.; Wu, X. Risk of ophthalmic adverse drug reactions in patients prescribed glucagon-like peptide 1 receptor agonists: a pharmacovigilance study based on the FDA adverse event reporting system database. Endocrine 2025, 88, 80–90. [Google Scholar] [CrossRef]
- Lakhani, M.; Kwan, A.T.H.; Mihalache, A.; Popovic, M.M.; Nanji, K.; Xie, J.S.; Feo, A.; Rabinovitch, D.; Shor, R.; Sadda, S.; et al. Association of Glucagon-Like Peptide-1 Receptor Agonists With Optic Nerve and Retinal Adverse Events: A Population-Based Observational Study Across 180 Countries. Am J Ophthalmol 2025, 277, 148–168. [Google Scholar] [CrossRef]
- Wang, L.; Volkow, N.D.; Kaelber, D.C.; Xu, R. Semaglutide or Tirzepatide and Optic Nerve and Visual Pathway Disorders in Type 2 Diabetes. JAMA Netw Open 2025, 8, e2526327. [Google Scholar] [CrossRef]
- Chou, C.C.; Pan, S.Y.; Sheen, Y.J.; Lin, J.F.; Lin, C.H.; Lin, H.J.; Wang, I.J.; Weng, C.H. Association between Semaglutide and Nonarteritic Anterior Ischemic Optic Neuropathy: A Multinational Population-Based Study. Ophthalmology 2025, 132, 381–388. [Google Scholar] [CrossRef]
- Natividade, G.R.; Spiazzi, B.F.; Baumgarten, M.W.; Bassotto, C.; Pereira, A.A.; Fraga, B.L.; Scalco, B.G.; Mattes, N.R.; Lavinsky, D.; Kramer, C.K.; et al. Ocular Adverse Events With Semaglutide: A Systematic Review and Meta-Analysis. JAMA Ophthalmol 2025, 143, 759–768. [Google Scholar] [CrossRef]
Figure 1.
Ocular and systemic mechanisms of GLP-1 receptor agonists (GLP-1RAs). GLP-1RAs exert multifaceted therapeutic effects across four interconnected domains relevant to ocular disease. Neuroprotection (↓ glutamate excitotoxicity, ↑ GABAergic tone, ↑ mitophagy), Anti-inflammatory (↓ TNF-α/IL-1β/IL-6; reduced microglial activation and monocyte infiltration), Antioxidant & Mitochondrial support (↑ SOD/GSH; ↓ ROS; improved mitochondrial integrity), and Vascular integrity & ECM (BRB stabilization; ↓ permeability; restraint of pro-angiogenic signaling; reduced fibrosis). Together, these mechanisms position GLP-1RAs as promising multi-target agents for neurovascular and inflammatory ocular disorders.
Figure 1.
Ocular and systemic mechanisms of GLP-1 receptor agonists (GLP-1RAs). GLP-1RAs exert multifaceted therapeutic effects across four interconnected domains relevant to ocular disease. Neuroprotection (↓ glutamate excitotoxicity, ↑ GABAergic tone, ↑ mitophagy), Anti-inflammatory (↓ TNF-α/IL-1β/IL-6; reduced microglial activation and monocyte infiltration), Antioxidant & Mitochondrial support (↑ SOD/GSH; ↓ ROS; improved mitochondrial integrity), and Vascular integrity & ECM (BRB stabilization; ↓ permeability; restraint of pro-angiogenic signaling; reduced fibrosis). Together, these mechanisms position GLP-1RAs as promising multi-target agents for neurovascular and inflammatory ocular disorders.
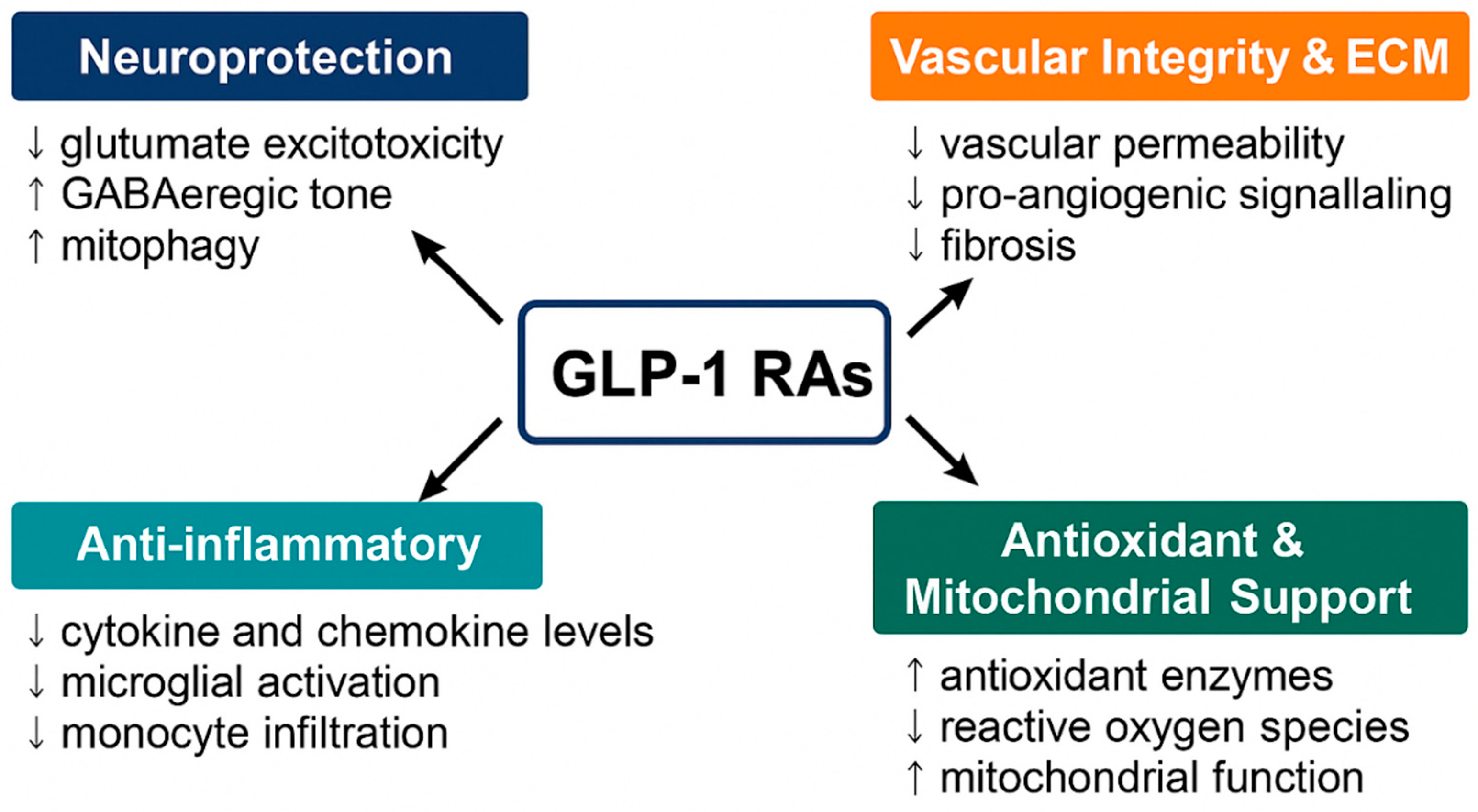
Figure 2.
Mechanisms of GLP-1RAs in Antioxidant Defense and Mitochondrial Support. GLP-1RAs exert dual protective effects by reducing oxidative stress and enhancing mitochondrial function. Through activation of Nrf2, GLP-1RAs upregulate antioxidant enzymes, decrease ROS production, and attenuate inflammation. Concurrently, GLP-1RAs stimulate PGC-1α, promoting mitochondrial biogenesis, improving mitochondrial dynamics, enhancing ATP synthesis, and facilitating mitophagy.
Figure 2.
Mechanisms of GLP-1RAs in Antioxidant Defense and Mitochondrial Support. GLP-1RAs exert dual protective effects by reducing oxidative stress and enhancing mitochondrial function. Through activation of Nrf2, GLP-1RAs upregulate antioxidant enzymes, decrease ROS production, and attenuate inflammation. Concurrently, GLP-1RAs stimulate PGC-1α, promoting mitochondrial biogenesis, improving mitochondrial dynamics, enhancing ATP synthesis, and facilitating mitophagy.
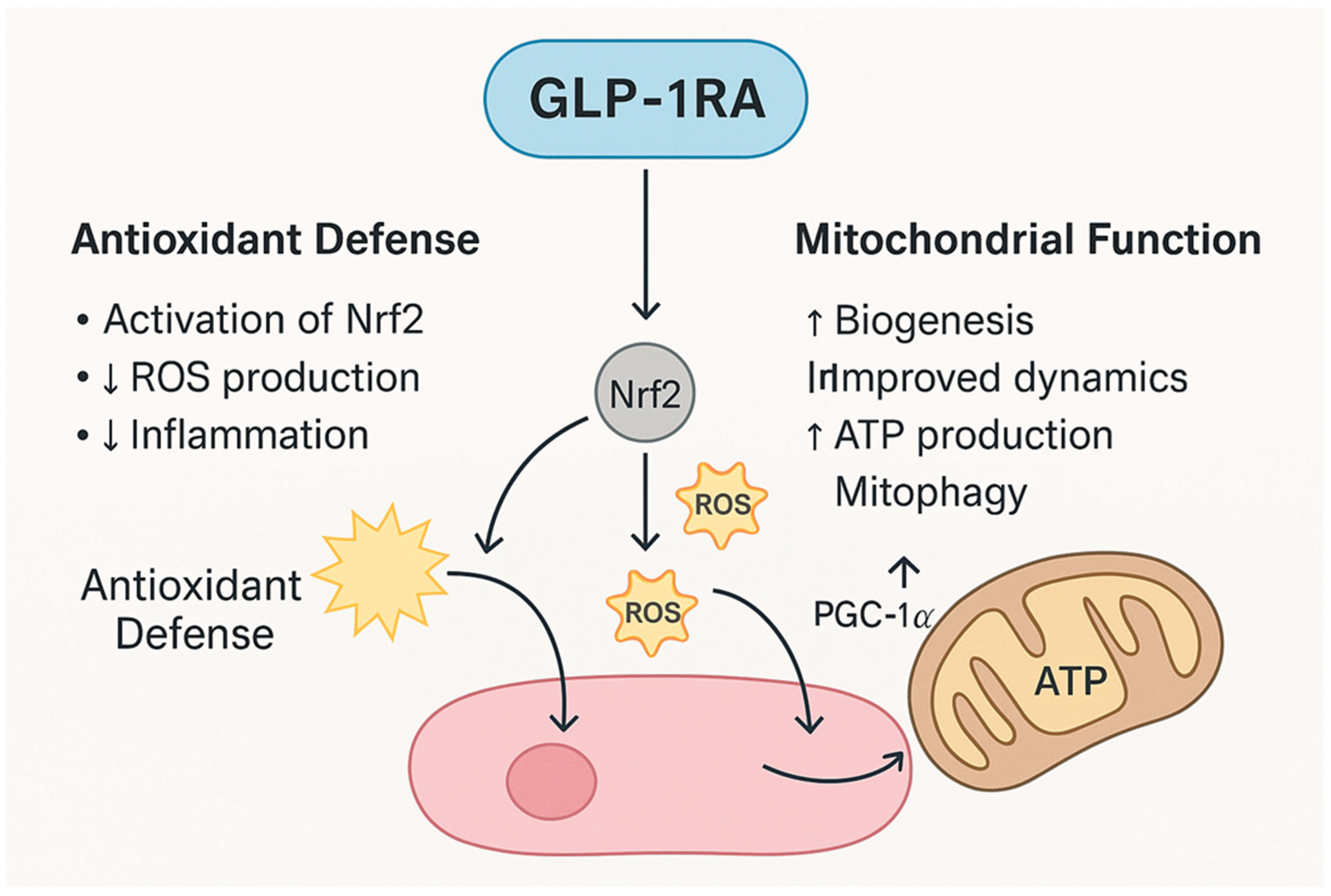

Table 1.
Summary of Molecular Mechanisms of GLP-1RAs in ocular tissues.
| Mechanisms of Actions |
Ocular Targets |
Molecular Pathways |
Molecular Effectors |
Functional Outcomes | Ocular Disease |
GLP-1 RAs | Ref. |
|---|---|---|---|---|---|---|---|
| Neuroprotection (RGC survival) | RGCs, Amacrine cells |
GLP-1R→cAMP/ PKA, PI3K/Akt, ERK1/2; modulation of Ca2+ channels; GABAergic tone |
↑BDNF signaling; ERK1/2–HDAC6 axis (axonal transport); PINK1/Parkin mitophagy; | Resilience to excitotoxic/ ischemic stress; preserved axoplasmic flow |
Glaucoma (RGC loss), optic neuropathy, DR |
Exenatide, liraglutide, semaglutide |
[24,25] |
|
Mitochondrial quality control |
RGCs, photo- receptors |
AMPK→PINK1/ Parkin; Mitophagy; ERK1/2–HDAC6 |
↑Mitophagy; ↓damaged mitochondria; stabilized mitochondrial trafficking; |
Sustained ATP; ↓ROS-induced apoptosis | Glaucoma, DR, AMD | Exenatide, liraglutide, semaglutide | [26,27] |
| Endothelial barrier stabilization | Retinal vascular endothelium; pericytes |
PI3K/Akt; Rac1/cytoskeletal junctions | ↑Tight-junction proteins (occludin/ claudin-5); ↓leukostasis |
Preserved BRB; ↓vascular leakage & edema |
DME; ischemic retinopathies |
Liraglutide, dulaglutide | [28,29] |
|
Anti-angiogenic responses |
Endothelium; RPE |
Indirect VEGF modulation; HIF-1α restraint | ↓VEGF/VEGFR signaling; ↓endothelial proliferation |
↓Pathologic neovascularization |
PDR, nAMD | Class | [30,31] |
| Microglial & macroglial modulation | Microglia, Müller glia | cAMP/PKA; NF-κB and NLRP3 inhibition | ↓TNF-α, IL-1β, IL-6; microglial deactivation | ↓Neuroinflammation; ↓secondary neuronal damage |
DR, AMD, glaucoma | Class | [35,36,37,38,39,40,41,42,43] |
|
Antioxidant defense |
Neurons; Endothelium; RPE |
AMPK/Nrf2 activation |
↑SOD, ↑GSH; ↓NADPH oxidase activity |
↓ROS load; Protection from hyperglycemia- induced oxidative stress |
DR, AMD | Class | [45,46,47] |
|
Neurovascular coupling & IOP control |
TM/uveoscleral outflow; optic nerve head | cAMP signaling; nitric-oxide (NO) pathways |
Potential outflow enhancement; vascular autoregulation | ↓IOP (in some reports); optic nerve perfusion support | Glaucoma | Class | [49,50,51] |
|
Immune modulation beyond retina |
Uveal tract, choroid | Systemic + local anti-inflammation | ↓Leukocyte recruitment |
↓Risk of ocular inflammation | Uveitis (noninfectious) | Class | [31,32,33,34] |
|
Systemic metabolic context |
Retina, choroid |
Rapid HbA1c reduction; BP/volume shifts |
Transient perfusion stress |
“Early worsening” of DR in vulnerable eyes |
DR safety concerns |
Class | [63,64] |
Abbreviations: AMPK, AMP-activated protein kinase; BDNF, brain-derived neurotrophic factor; BP, blood pressure; BRB, blood retina barrier; DME, diabetic macular edema; DR, diabetic retinopathy; GSH, glutathione; IOP, intraocular pressure; nAMD, neovascular AMD; NF-κB, nuclear factor kappa-light-chain-enhancer of activated B cells; NLRP3, NOD-, LRR- and pyrin domain-containing protein 3; PDR, proliferative DR; RGC, retinal ganglion cell; SOD, superoxide dismutase; TM, trabecular meshwork; VEGF, vascular endothelial growth factor.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



