Submitted:
14 April 2024
Posted:
24 April 2024
You are already at the latest version
Abstract
Starvation of photoreceptors induced by reduced dysregulated ocular blood flow is proposed as a common pathway for the pathogenesis of retinitis pigmentosa (RP). The current study evaluated the safety and efficacy of ophthalmic nerve stimulation (ONS) as an ocular blood flow neuromodulator, combined with ascorbic acid (AA) as a potent anti-oxidant in the treatment of RP. Additionally, the initial characteristics of rod responders were identified. Forty participants with simple, non-syndromic RP presented with a characteristic triad of RP (the bone spicule pigmentation, attenuation of retinal blood vessels, and waxy optic disc pallor), were en-rolled in a prospective open-label single-armed interventional study. The severity of the disease was clinically graded into six stages. Patients with an established diagnosis of RP; aged ≥ 4 years, with best corrected visual acuity (BCVA) ≥ 20/400 were included. All participants were daily treated with bilateral ONS sessions combined with intravenous administration of AA for two weeks. The primary efficiency endpoint was 6 months’ changes in scotopic vision as measured by a 10-item, 100-point, Low Luminance Questionnaire-10 (LLQ-10). The secondary efficiency points included best corrected visual acuity (BCVA) and contrast sensitivity. Rod responders were defined by ≥ 25 points increment of LLQ-10 score at 6 months after treatment. The results showed that ONS combined with AA treatment significantly improved low luminance vision, BCVA, and contrast sensitivity in patients with RP (p≤ 0.05). At 6-month visit, twenty-four (60%) patients were identified as rod responders and 16 (40%) patients were rod-non-responders. The mean change in LLQ-10 score was (46.35 ±16.81) in rod responders versus (4.9 ± 7.6) in non-responders (p < 0.0001). A clinically significant improvement of BCVA (≥0.2 logMAR) and contrast sensitivity (≥0.3 log unit) were demonstrated in 50% of the right eyes of rod responders. No serious adverse effects were reported and headache in 5 patients (12.5%) was the only en-countered side effect in this study. In conclusion, ocular neuromodulation is a safe therapeutic strategy for RP. It significantly improved night vision, BCVA, and contrast sensitivity. Determinants of rod responders include a shorter duration of night blindness, an earlier stage of the disease, and a relatively thicker ganglion cell layer at baseline. Additionally, two therapeutic scenarios were recognized; an early disease-modifying intervention that restores night vision and reverses the disease process and a late cone rescue intervention that improves/maintains central vision.
Keywords:
Retinitis pimentosa
; Ocular neuromodulation
; Ophthalmic nerve stimulation
; Ascorbic acid
; Rod responders
; Substance P
; Night blindness
1. Introduction
Retinitis pigmentosa (RP) is a group of inherited eye conditions, affecting 1 in 3000 people, with most people becoming legally blind by the age of 40 [1]. It is characterized by progressive loss of rods followed by cone photoreceptor death, and abnormal hemodynamics of the eye [2]. Typically, RP presented with a characteristic tirade of bone-spicule pigmentation of the retina, attenuated retinal blood vessels, and optic nerve pallor. Currently, there is no treatment for RP, apart from Luxturna gene therapy [3], but with limited therapeutic target, since its indication is restricted to a group of patients with recessive RPE65 mutation.
RP is not merely caused by genetic factors; in fact, it is a complex multifactorial disorder. Other factors are assumed to contribute to its pathogenesis. Circulatory changes have been observed in the retina and choroid of RP patients, but it has remained unclear whether these play a role in the pathogenesis of the disease. The choroid is a densely vascularized structure contributing to the majority of oxygen and glucose supply to the photoreceptors, and the retinal pigment epithelium in the outer retina [4]. Evaluating choroidal hemodynamic changes has shown the reduction in choroidal blood flow is proportional to the progression of RP [5,6]. Recently, relative choroidal ischemia and reduced choroidal blood flow have been demonstrated in RP by measuring the choroidal vascularity index via OCT [7]. Photoreceptor changes seen in eyes with RP are directly correlated to a decrease in choroidal flow, leading to a strong association between relative choroidal ischemia and visual impairment [7]. Visual function and retinal structural changes were found to be associated with choriocapillaris defects but not with middle/large choroidal vascular defects [8]. The reduced choroidal vascularity index in patients with RP has been detected before the development of structural changes in the retina and choroid. [9]. Furthermore, a study reported a relationship between choroidal blood flow and reduced focal electroretinography responses [10]. The pulsatile blood flow is significantly reduced in RP patients and relative choroidal ischemia is closely associated with visual loss [5]. Retinal blood flow is also significantly decreased in RP, probably as a result of vascular remodeling in response to reduced metabolic demand [11]. The ocular blood flow is reduced not only in the retina and choroid but also in the retro-ocular vessels [12] including the ophthalmic artery and ciliary arteries [12]. Interestingly, signs of reduced ocular blood flow have been observed before the appearance of any of the fundoscopic features of RP [13]. Elevated levels of endothelin-1 were observed in plasma of RP patients, indicating increased endothelin-1 production [12,14,15]. Endothelin-1 is a potent vasoconstrictor peptide of 21 amino acids that is synthesized and released by endothelial cells. Thus, one may hypothesize that in patients with RP, increased endothelin levels lead to a predominance of vasoconstricting factors associated with a decrease in ocular blood flow and vascular dysregulation. It has been suggested that such a vascular dysregulation might play a primary role in the pathogenesis of RP [2]. The mechanisms responsible for reduced dysregulated ocular blood flow in RP patients are uncertain. It is also uncertain if ocular blood flow decline stems from disturbed neural control of ocular circulation or from vascular pathology, or both.
The blood supply to the choroid in mammals arises from the ophthalmic artery via the long and short ciliary arteries. Ophthalmic artery and its main branches including ciliary and choroidal arteries are all under both parasympathetic and sympathetic neural control with many also under local trigeminal control [16]. The parasympathetic input has a vasodilatory effect, while the sympathetic input has a vasoconstrictor effect [16,17].
Stimulation of sensory afferents from the ophthalmic nerve results in the activation of three pathways that lead to vasodilatation and increased ocular blood flow (Figure 1). The first is the activation of the trigeminovascular system via antidromic impulse [16,17,18]. The nasociliary nerve, which originates from the ophthalmic nerve, contains major vasodilatory innervation [19,20], and its stimulation results in the release of vasoactive neuropeptides from the free nerve endings, such as substance P (SP) and calcitonin gene-related peptide (CGRP) [21]. The second pathway results in parasympathetic vasodilation of the ocular vasculature via interactions with the facial nerve and sphenopalatine ganglion [22,23]. The third is an axon reflex between the trigeminal nerve and sphenopalatine ganglion [19]. Consistent with this, stimulation of the ophthalmic nerve in experimental animals was found to increase ocular blood flow [24], decrease carotid arterial resistance, [22] along with enhanced uveal release of SP, which is an 11 amino acid neuropeptide [25]. Overexpression of endogenous SP by ONS is capable of boosting both the ocular blood flow [16,17,24] and tissue regeneration by the recruitment of endogenous stem cells [26]. Moreover, SP can protect diverse types of cells including retinal pigment epithelium [27], and ganglion cells [28], and also contribute to the prevention of apoptosis [29,30], suppression of both inflammation [31,32] and oxidative stress [33,34]. SP was reported to modulate Akt/GSK-3β signaling, inhibit reactive oxygen species-induced cell death, preserve cell viability, and block cellular alterations [33,34,35]
Oxidative stress also plays a central role in the pathogenesis and progression of RP. Anti-oxidant interventions have been reported to substantially delay photoreceptor cell death [36]. The potential benefit of AA, the main antioxidant in the retina has been shown in several clinical settings with oxidative damage [37,38,39,40]. AA is highly concentrated in the retina, with many folds of plasma [41,42]. It is the most important antioxidant for the metabolic function of the retina [42]. The therapeutic, non-enzymatic scavenging of free radicals can be accomplished by AA, but only at supraphysiological concentrations [43]. To achieve this concentration in the retina, the intravenous route might be ideal to bypass tight control of oral administration [40]. Preclinical studies showed that a high dose of AA can restore vascular endothelial function and prevent microcirculatory flow impairment. AA can retrieve vascular responsiveness to vasoconstrictors and preserve the endothelial barrier [40]. Additionally, AA exerts sympatholytic effects via central action [44]. Therefore, it is reasonable to suggest that high-dose of intravenous AA could be beneficial in RP treatment
Pathogenesis of RP reflects a summation of primarily reduced dysregulated ocular blood flow, consecutive unstable oxygen supply, photoreceptor starvation, oxidative stress, and chronic inflammation of the retina. These vascular and cellular processes are ultimately combined to produce a rod followed by cone apoptosis. We suggest that relative choroidal hypoxia and starvation of photoreceptors caused by reduced dysregulated ocular blood flow represents an initial common pathway in the pathogenesis of RP, which can be a target for a novel therapeutic strategy that might halt rod and cone degeneration.
Based on the effects of ONS, AA, and the functioning of SP investigated in previous studies, we hypothesized that neuromodulation-based therapy for RP may be capable of recovering the functions of dormant rods and cones and preventing their death. This can be possibly achieved by increasing ocular blood flow, inhibiting apoptosis, inflammation, oxidative stress, and induction of regeneration by recruitment of endogenous stem cells. The study aims to evaluate the safety and efficacy of ONS paired with intravenous administration of ascorbate for treating participants with RP. Additionally, baseline predictive factors for night vision improvement were also defined.
2. Materials and Methods
Forty participants with RP were recruited into a prospective, open-label single-armed interventional study, conducted at Musallam Eye Centers, Palestinian Authority. This study was approved by the Institutional Review Board, and it adhered to the tenets of the Declaration of Helsinki. Written informed consent was obtained from all participants after an explanation of the purpose and possible outcome of therapy.
All ophthalmological examinations, staging of the disease, and patient selection were performed by a senior vitreoretinal specialist (the author). Supplementary Figure S1, showed details of participant’s enrollment. Following recruitment, all subjects with a medical history and established diagnosis of RP completed baseline vision testing, slit lamp examination, and fundoscopy. We interviewed the patients and created detailed family trees for each to determine the pattern of inheritance. The diagnosis of RP was based on clinical history, night vision impairment, constricted visual field, characteristic fundus appearance. Additionally, the diagnostic data from other centers like ERG were utilized whenever available. Spectral Domain Optical Coherence Tomography (SD-OCT) was performed within 2-4 weeks before treatment. The severity of the disease was clinically graded into six stages based on fundoscopy and (SD-OCT) findings (Table 1, Supplementary Figure S2 and S3).
For Sample size estimation the online One Arm Binomial program was used [45], with the power of 90% and = 0.05 with an expected proportion of responders 25%, the minimal sample was estimated to be at least 30 patients. Inclusion criteria were: patients with an established diagnosis of classic, simple, non-syndromic RP; aged ≥ 4 years, with BCVA ≥ 20/400. Classic RP is defined by the presence of a triad of bone-spicule pigmentation, attenuated retinal blood vessels, and waxy optic nerve pallor in both eyes and is associated with night vision blindness, and restricted peripheral visual field. Exclusion criteria were syndromic RP(e.g. Usher syndrome, Bardet Biedl syndrome), unilateral RP, sectorial RP, RP sin pigmentosa, retinitis punctate albescent, and RP masquerades [46], pregnancy, glaucoma, central retinal vein occlusion and retinal detachment.
Staging of RP
To evaluate the efficacy of new treatment options, it is important to measure the severity of the disease. Staging of RP is a method for measuring the severity of disease using objective clinical and bio-molecular criteria. Disease staging is vital for clinical trial inclusion, exclusion, and stratification of participants. Accurate staging aids in prognosis definition, treatment evaluation, and clinical decision-making.
Various RP staging systems exist, each utilizing different biomarkers. Some systems rely on a single marker, such as the width of the ellipsoid zone [47] or the baseline mean deviation in the visual field [48], while others incorporate multiple biomarkers. For instance, a system might use visual acuity, visual field width, and ellipsoid zone width, either singly [49] or in combination with multifocal electroretinography [50]. Alternative approaches assess severity through a combination of clinical appearance (lens condition, retinal pigmentation, and optic nerve appearance), BCVA, perimetry, and optical coherence tomography measurements [51]. Another multi-faceted system evaluates RP severity using color vision tests, visual field analysis, and clinical assessment of optic disc pallor, retinal pigmentary changes, and vascular attenuation [52]. Historically, the Ganzfeld flash electroretinogram (ERG) has been viewed as a benchmark for staging RP, despite its limitations.
However, current staging systems face challenges, particularly with the reliance on cone-related biomarkers and tests such as best-corrected visual acuity[49,50,51], ellipsoid zone width [47,49,50] and multifocal ERG [50], which may not accurately reflect the state of rod-cone dystrophy where cone function can be maintained even in advanced disease stages. Moreover, while visual field analysis offers a method for the detection of linear progression of deterioration and covers all clinical stages of the disease, it has limitations in the context of its application in advanced RP, concurrent eye conditions like cataracts or macular pathologies associated with RP, and its applicability in children. Notably, preclinical stages of RP are often overlooked in these staging systems.
To address these gaps, we propose a six-stage system that encompasses preclinical (Stage 0 and Stage I) and clinical stages of RP (Stage II to Stage V), (delineated in Table 1 and supplementary Figures S2 and S3). It tracks RP progression using characteristic fundoscopic triad changes, including bone spicule pigmentation, vascular alterations, and optic disc pallor. ERG detects preclinical stages (Stage 0 and Stage I). The asymptomatic stage 0 can last for months and years, while the patient may not have physical symptoms. Stage I marks the onset of symptomatic preclinical RP, characterized by initial night vision difficulties, absent fundoscopic changes, and diagnosable solely through ERG.
For clinically manifested RP stages (II-V), key indicators include alterations in retinal vasculature, pigmentation, and optic nerve pallor. Disease progression is marked by attenuation and the centripetal closure of retinal vessels, starting from the periphery and moving toward the optic disc (Supplementary Figure S3). Previous histopathological research revealed that thickening of the blood vessel walls and occlusion of their lumina correlate with sclerosis and atrophy of the retinal vasculature, which is shown as attenuated retinal arteries [53,54]. These vascular changes coincide with pigmentary alterations that begin in the retina's mid-periphery and spread concentrically towards the macula, eventually affecting the fovea in advanced disease stages (Stage V) (Supplementary Figure S2). Notably, changes in optic nerve pallor typically lag behind vascular and pigmentary developments, providing a chronological marker of disease progression.
Retinal vessel attenuation is widely acknowledged as a prevalent characteristic in individuals with RP, underscoring its significance as a biomarker for assessing disease severity. In a cross-sectional study [55], researchers demonstrated a correlation between the extent of retinal vessel attenuation and the severity of RP, as determined by visual field width. Additionally, it was found that both retinal arteries and veins were significantly narrower in individuals displaying a higher threshold for scotopic sensitivity, according to measurements by the Goldmann-Weekers adaptometer. A longitudinal study by Nakagawa et al. further revealed that the baseline calibers of the central retinal artery equivalent and central retinal vein equivalent were inversely related to visual acuity decline over three years, suggesting that smaller retinal vessels are indicative of greater reductions in visual acuity [56].
The presence and distribution of bone spicule pigmentation have also been utilized as an indirect marker of retinal atrophy, owing to its visibility during ophthalmoscopy and its strong association with photoreceptor loss regions. This pigmentation is a commonly used structural metric for staging RP, with its extensive distribution often observed in individuals at advanced stages of the disease. For instance, Smith et al. have noted that an increase in disease severity is implied when pigmentary changes extend beyond the vascular arcades toward the macula [51]. In a comprehensive study involving data from 928 RP patients, researchers explored the relationship between mean deviation (MD) scores, visual acuity, and retinal pigmentation [48]. They discovered that the average decline in MD over a decade was linked to an increase in retinal pigmentation, further establishing the connection between these parameters and the progression of RP. In support of our staging system, it has been found that greater vascular attenuation, concentric spread of intra-retinal pigmentation, and progressive pallor of the optic disc were inversely correlated with the central retinal artery peak-systolic velocity, an objective sign of advancing clinical stage of RP [57].
Development of the primary endpoint:
Low Luminance Questionnaire -10 (LLQ-10)
The primary endpoint, LLQ-10, was developed to address the predominant initial symptom of RP: difficulty in low-light conditions and at night. This symptom, associated with impaired rod-mediated sensitivity and dark adaptation delays, often manifests early in life. Therefore, the pediatric population will constitute the majority of RP patients for future studies that aim for early intervention and night vision restoration.
The clinical endpoint should be a ‘clinically meaningful measure of how a patient feels, functions or survives’ [58]. In other words, the outcome should be ‘relevant to the patient’ [59]. Given the importance of patient-centered outcomes in clinical trials, LLQ-10 serves as a valuable tool for assessing visibility issues in reduced light levels. LLQ-10, derived from the validated LLQ-32 questionnaire [60], was refined to prioritize items specific to low-luminance vision in RP patients. Careful selection of the questionnaire's content ensures relevance across both adult and pediatric cohorts, with parental assistance where necessary.
To evaluate the therapy outcome, LLQ-10 score changes from baseline to 6 months after treatment were calculated (The outcome measures). LLQ-10 has been used to quantify the participant’s visual dysfunction under low luminance, integrating aspects of visual acuity, mobility, visual field, depth of perception, reading, color vision, dependency on others' help, social functions, and mental health
In the assessment of the LLQ-10 score for pediatric subjects, a dual modality incorporating parental and self-reports was employed. Parents were provided with comprehensive explanations concerning each component of the questionnaire, including guidelines for accurate score measurement. This methodological approach aims to improve the precision of studies directed towards the combination of adult and pediatric populations, thereby augmenting the efficacy of assessing treatment effects in RP clinical trials. Participants or children assisted by parents rated how much difficulty they have performing each of the activities under low luminance on a 5-point Likert scale. Rod responders were identified as those in whom the LLQ-10 score increased by ≥ 25 points at 6 months after treatment.
The secondary efficiency points include BCVA and contrast sensitivity of the right eye. These visual functions were evaluated under standardized conditions by a single well-trained optometrist who was not aware of the previous results of the participant. BCVA was recorded in Snellen equivalents and then transformed into a logMAR unit. Contrast sensitivity was measured using a Pelli- Robson chart under standardized photopic illumination at one meter in each eye, using best correction spectacles. For safety purposes, the vital signs and electrocardiogram were monitored before, during, and after each session of ocular neuromodulation. Ocular and non-ocular adverse events were also reported.
The ocular neuromodulation protocol included the administration of AA followed by ONS over a period of two weeks. This therapeutic protocol was delivered by a senior nurse who had received a special training course regarding the new treatment under investigation. AA was given intravenously in a dose of 3 gm dissolved in 100 ml of saline infused at 5 ml min−1 for 20 min on the first day, followed by a drip infusion of 1 gm daily during the rest of the treatment period.
A modulated low magnitude, low-frequency vibration, with a frequency of approximately 60 Hz- 90 Hz and stimulation amplitude range of 1.5 μm- 3.5 μm was used for ONS. This setting was adopted to selectively activate the parasympathetic system and trigeminovascular system [17,61,62]. Modulated frequency and amplitude waveforms were used to avoid adaptation to mechanical stimulus. A hand-held and head-mounted prototypes of ophthalmic nerve stimulators (Figure 2B,C) were used to activate different stimulation sites (Figure 2A) by using modified commercially available micro-vibrators, along with different types of intranasal and extra-nasal application heads.
Bilateral ONS was applied to the subjects over a session of 30 minutes per day, 6 sessions per week, and one day off. Each session included intra-nasal vibrochemical, and extra-nasal vibrotactile stimulation over the nasal bridge and the supraorbital region in both sides (Figure 2A), using appropriate application heads. During intra-nasal vibrochemical stimulation, the nasal application head was covered by a rubber cape impregnated with 2% menthol cream (Dermacool plus R) as a transient receptor potential cation channel subfamily M (melastatin) member 8 (TRPM8) agonist (Figure 2B). Participants were assessed clinically, and by SD-OCT, and ILQ-10 at baseline and at 1, 6, 12, and 24 months after treatment
2. Statistical Analysis
The statistical analysis was performed using SPSSR, V. 21. The mean differences in the characteristics of the rod responders and rod-non-responders were compared using the independent sample t-test. The change in the mean value of visual function parameters between baseline and different post-treatment points was evaluated using a paired sample t-test. Since the data for most of the variables are not normally distributed, a non-parametric test (Mann-Whitney U test) was used to compare the median value of different parameters comparing the rod responders and rod-non-responders. The change in the median value of visual function parameters between baseline and different post-treatment points was evaluated using the Wilcoxon signed-rank test. The differences between the proportion of eyes that showed clinically significant improvement of visual function, among rod responders compared to rod-non–responders, and the relationship between the stage of the disease and rod responsiveness were evaluated using the Chi-square test.
To evaluate the change over time in visual functions (BCVA and contrast sensitivity) in the right eye for both rod responders and rod-non-responders starting from baseline, up to 24 months, the Friedman test for related samples was used. This test was also used to evaluate the change in visual function of the right eye of the whole cohort as well as for the left eye separately.
Correlation was performed between ILQ-10 score in the whole cohort at 6 months after treatment; and the characteristics of participants at baseline, which include the age, stage of the disease, duration of night blindness, BCVA, contrast sensitivity, and SD- OCT biomarkers.
Multivariate logistic regression was performed to study the factors that independently predict rod responders and to control for confounding factors including age, duration of night blindness, stage of the disease and BCVA, ganglion cell layer thickness, and central macular thickness at baseline. All tests were two-tailed and a p-value less than 0.05 was considered significant.
4. Results
Between April 14, 2018, and April 29, 2020, 40 participants (38 right eyes and 38 left eyes), aged between 4- 55 years (median; 24 years), among them 24 males (60%) were recruited. The pediatric population of the cohort aged ≤ 17 years (7 patients) constitutes 17.5 % of the cohort, among them, 4 patients aged <10 years. The hereditary forms were autosomal dominant (AD) in 2 participants (5%), autosomal recessive (AR) in 21 participants (52.5%), and sporadic in 17 participants (42.5%). None of the patients had an X-linked RP. The minimum follows up was 6 months, and maximum was 24 months after treatment. The demographics, baseline characteristics, and determinants of rod responders are presented in Table 3.
Twenty-four (60%) patients were identified as rod responders, and 16 (40%) patients were rod-non-responders. (Table 3). Table 4 shows the mean (mean ± SD) and the median value (median; 25th, 75th) of LLQ-10 for the whole cohort, rod responders, and rod-non responders at baseline and at different intervals after treatment. Figure 3A shows the median value of the low luminance vision score at different post-treatment intervals. In the whole cohort, the median score of LLQ-10 improved significantly from 21.3 points at baseline to 55.1 points (p=0.0001) at one month, 52.5 points (p= 0.0001) at 6 months, and to 52.5 points (p=0.0001) at 12 months and to a value of 55.5 points (p=0.001) at 24 months after treatment. Similarly, in rod responders; the median score of LLQ-10 improved significantly from 22.5 points at baseline to 77.5 points (p=0.0001) at one month, 66.3 points (p= 0.0001) at 6 months, 70.0 points (p=0.006) at 12 months and to a value of 70.0 points (p=0.003) at 24 months after treatment. In contrast, though the rod-non-responders showed a statistically significant improvement at 1 and 6-month visits only, this improvement was considered clinically insignificant
At the 6-month visit, the low luminance vision score was significantly improved in the whole cohort by (29.8 ± 24.7) points as compared to baseline (P < 0.0001). The mean change in LLQ-10 score was (46.35 ±16.81) in rod responders versus (4.9 ± 7.6) in non-responders (p=0.0001).
The baseline characteristics and determinants for rod responders are shown in Table 3. Compared to rod-non-responders, the rod responders were found to be statistically significantly younger (median age 21.5 yrs. vs 40.0 yrs.) (p=0.015), with better BCVA (median value; 0.34 vs 0.80 Log MAR unit) (P=0.03) and contrast sensitivity (0.70. vs 0.00 log unit) (p=0.056) at baseline. Additionally, the central retinal thickness (median value; 224.0 µm vs 185.5 µm) (p=0.04) and ganglion cell layer thickness (median value; 60.0 µm vs 49.0 µm) (p=0.02) were significantly thicker when compared to rod-non-responders.
Upon consideration of the disease stage (as illustrated in Table 3 and Figure 3D), it was observed that individuals exhibiting rod responsiveness were predominant in the earlier stages of the disease (P=0.0001). Notably, all patients in stage II (comprising 9 individuals) and 80% of patients in stage III (12 out of 15) demonstrated rod responsiveness.
Conversely, only 18% (2 out of 11) of patients in stage IV displayed rod responsiveness. It is noteworthy that within stage V, the sole patient who responded to treatment (rod-responder) presented with a central type of RP. Interestingly, she exhibited autosomal recessive RP, whereas two brothers who shared the same genetic condition presented with a peripheral phenotype.
Interestingly there was a negative correlation between the duration of night blindness and rod responsiveness (Table 3 and Figure 3E). The rod responders were found to have a significantly shorter median duration of night blindness compared to non-responders (median value; 10.0 yrs. vs 21.0 yrs.) (p=0.003). The majority of patients (81.3%) (13 out of 18) who experienced night blindness for 10 years or less were found to be rod responders. In contrast, only 28.57% (4 out of 14) and 10% (1 out of 10) of patients with 10-20 and > 20 years of night blindness were found to be rod responders. (Figure 3E)
On the other hand, correlation was performed between LLQ-10 score in the whole cohort at 6 months after treatment; and the characteristics of participants at baseline. The correlation coefficient [r] showed that LLQ-10 score at 6 months is significantly correlated with the stage of the disease (r = -0.717; p=0.0001), ganglion cell layer thickness (r=0.45; p=0.006), BCVA (r= 0.388; p=0.016), contrast sensitivity (r=0.534; p=0.001), age (r=0.525; p=0.001), and duration of night blindness (r=0.517; p=0.001). Multivariate logistic regression was performed to study the factors that independently predict rod responsiveness and control for confounding factors including age, duration of night blindness, stage of the disease, central macula thickness, and ganglion cell layer thickness. The rod responsiveness was statistically significantly predicted by the duration of the night blindness (p=0.047), stage of the disease (p=0.05), and ganglion cell layer thickness (p=0.03).
When the BCVA is considered, the data from the right eye is only analyzed. The mean as well as the median values of BCVA of the right eye of the whole cohort were significantly improved at all post-treatment visits when compared to baseline (Table 4). The median value of BCVA was improved from 0.50 log Mar unit at the baseline to 0.26 Log Mar unit (p=0.0001) at one month; 0.3 Log Mar unit (p=0.0001) at 6 months; 0.3 Log Mar unit (p=0.006) at 12 months and to a value of 0.32 log Mar unit (p=0.03) at 24 months after treatment (Table 4 and Figure 3B).
At 6 months’ visit, 42.5% of the right eyes of the whole cohort demonstrated a clinically significant improvement of BCVA (improvement of ≥0.2 logMAR unit). Such improvement was demonstrated in 50% of the right eyes of rod responders compared to 31.3 % of the right eyes of rod-non-responders. This difference, however, was not statistically significant. (Figure 3F).
Upon consideration of the change over time in BCVA of the right eye for both rod responders and rod-non-responders starting from baseline, up to 24 months, using the Friedman test for related samples, the results were significant for the rod responders (p= 0.003) and rod-non- responders (p=0.04).
As regards to the effect of neuromodulation on contrast sensitivity, the data from the right eye was only analyzed. The mean, as well as median values of contrast sensitivity of the right eye of the whole cohort, were significantly improved at all post-treatment visits when compared to baseline. (Table 4). The median value of contrast sensitivity was improved from 0.18 Log units at the baseline; to 0.75 log units (p=0.0001) at 1 month; 0.70 log units (p=0.0001) at 6 months; 0.9 log units (p=0.003) at 12 months and to a value of 0.9 log unit (P=0.02) at 24 months after treatment (Table 4 and Figure 3C).
At 6-month visit, 37.5% of the right eyes of the whole cohort demonstrated a clinically significant improvement of contrast sensitivity (improvement of ≥0.3 log unit). Additionally, there was a statistically significant difference in the proportion of right eyes that showed a clinically significant improvement of contrast sensitivity among the rod responders compared to that of rod-non-responders (p < 0.03). 50.0% of the eyes of rod responders and 18.8% of the eyes of rod-non-responders had a clinically significant improvement in contrast sensitivity (Figure 3F)
On considering the change over time in contrast sensitivity of the right eye for both, rod responders and rod-non-responders starting from baseline, up to 24 months, using the Friedman test for related samples, the results were significant for the rod responders (p= 0.002) and rod-non-responders (p=0.008).
We also analyzed the therapeutic effects of ocular neuromodulation on the right and left eye separately by considering the change of BCVA and contrast sensitivity over time starting from baseline, up to 24 months, using the Friedman test for related samples. The results were significant for the right eye (p=0.0001), as well as for the left eye (p=0.0001) when the BCVA was considered. Furthermore, a similar result was also found when contrast sensitivity in the right and left eye was analyzed (the right (p=0.0001), and left eye (p=0.0001). This indicates that ocular neuromodulation significantly improves BCVA and contrast sensitivity in both eyes in a simultaneous fashion.
Clinically significant regression was noticed in 6 (11.8%) patients 6-12 months after the treatment. At 24 months’ visit, 20 out of 22 participants (91%) showed signs of visual regression that justified re-treatment. No serious adverse effects were reported and headache in 5 patients was the only encountered side effect in this study.
5. Discussion
The current study reported a successful use of ocular neuromodulation as a novel treatment for RP that was previously considered incurable. It has led to clinically meaningful and statistically significant improvements in visual functions including navigation under low illumination conditions, BCVA, and contrast sensitivity. We have identified patient characteristics that may predict a positive response to treatment. These include younger age, early stage of the disease, and short duration of night blindness at baseline. Additionally, central retinal thickness and ganglion cell layer thickness at baseline, SD-OCT biomarkers, were associated with rod responsiveness.
In this study, we found that the most robust improvement in visual function for the subjects with early stages of the disease was night vision as measured by LLQ-10. The process of rod cell apoptosis occurs over years [63], suggesting that there was a much wider window of opportunity for applying ocular neuromodulation for the early rod-related stage of RP. Recovery of night vision was likely to be related to the reactivation of dormant/starving rods via enhanced oxygen and glucose delivery and shunting metabolites toward aerobic glucose metabolism [64]. A recent study has demonstrated a protective effect of restored glucose transport to mutant rods in RP [65].
In RP, reduced dysregulated ocular blood flow[2,5,6,10], decreased choroidal vascularity index [7,8,9]. progressive retinal vessel attenuation [55,56] and reduction of vessel density, along with alteration of the foveal avascular zone have been reported in several studies [55,66]. Early development of the annular scotoma was noticed at the mid-periphery opposite the choroidal watershed zone between the anterior and posterior ciliary arteries [67]. Clinically, it is well known that watershed zones play an important role in the development of ischemic lesions in the involved tissue. Therefore, from the foregoing description, it is evident that the rods that lie opposite the equatorial watershed zones of the choroid are more susceptible to ischemic insult and energy failure. This predilection for atrophy in mid peripheral area with high rod density supports the notion that rod photoreceptor damage is primarily of vascular origin. Nevertheless, the unmet oxygen and glucose requirements of mutant rods might be triggering factors for the disease process in RP.
BCVA and contrast sensitivity were not the primary outcome measures of this rod-mediated disease. Nevertheless, the visual acuity and contrast sensitivity were significantly improved in the whole cohort. (Figure 3B,C). This improvement was maintained for months and years after treatment before the occurrence of regression which was seen earlier and more frequent in rod-non-responders. We propose that the reversal of cone dormancy via modulation of ocular blood flow might increase the density of functioning cones in the fovea and decrease intercone spacing thereby improving visual acuity and contrast sensitivity. Restoration of glucose delivery to starving cones was found effective in the reversal of the state of dormancy in these photoreceptors [64,68]
Several lines of evidence indicate that altered blood flow regulation may contribute to the pathogenesis of RP [15]. Recent data support the hypothesis that the endothelin system is involved in the processes that lead to vascular dysregulation and neuroinflammation in RP [69]. The endothelin (ET) system encompasses three active peptides, endothelin 1 (ET-1), endothelin 2 (ET-2) and endothelin 3 (ET-3) and two G protein-coupled receptors (ETA and ETB [70]. ETA receptors are present in vascular smooth muscle cells and mediate endothelin-induced vasoconstriction [70]. Because of its potent vasoconstrictor effects, ET-1 and ET-2 has been hypothesized to play a role in the ocular vascular dysregulation in RP. Furthermore, there is increasing evidence that endothelin system is up regulated by cigarette smoking [71], and exposure to light [69,72,73]. In particular, several lines of evidence indicate that cigarette smoking [74] and exposure to light [69,72,73] contribute to the progression of the disease. Endothelin receptor antagonists have been investigated in RP experimental model to inhibit harmful effects of the peptide. These drugs have shown favorable effects in animal studies [69,72,75], but clinical trials with endothelin receptor antagonists have not been as successful as anticipated [76]. Established complexes between ET-1 and ETA have a half-life of ≤77 hours. [77]. Because of this tight binding of ET-1 on ETA, functional capacity of endothelin receptor antagonists was found to be greatly reduced [78,79]. Interestingly, the long-lasting vasoconstrictor effects of Endothelin 1 can be terminated by exogenous or endogenously expressed calcitonin gene related peptide. [80]. Then overexpression of calcitonin gene related peptide via ONS may represent a novel strategy to treat endothelin 1–associated vasoconstriction and ocular vascular dysregulation
In normal retinas, the action of various proangiogenic factors is in balance with the action of endogenous antiangiogenic factors. There is considerable evidence that vascular endothelial growth factor A (VEGF A) is a prime regulator of angiogenesis [81]. In patients with RP, the concentration of VEGF-A in aqueous humor is lower than in non-RP subjects [82] and its level decreases with disease progression [15]. By attempting to redress this imbalance, it might be possible to normalize retinal vessels. One validated mechanism of vascular normalization is enhancement of VEGF signaling. The angiogenic effect of indirect activation of the vagus nerve [83,84] via its neuronal connection with ophthalmic neve might play a role [85]. Furthermore, sensory neurons of the ophthalmic nerve might also promote angiogenesis of the retina via SP signaling in response to antidromic ONS [86]. SP can induce enhancement of migration, proliferation, and differentiation of endothelial cells, [87] and recruitment of circulating angiogenic cells and endogenous stem cells to the injury site [26,88]. We thus hypothesized that ONS promoted angiogenesis of the retina by increasing both VEGF and SP levels. Our primary impression indicated that the appearance of a normalized vascular phenotype of the retina (Figure 4) can only be achieved when ocular neuromodulation is applied at the earliest possible time before irreversible vascular remodeling of the retina occurs (vascular normalization window).
Neuroinflammation is a key component of neurodegenerative processes affecting the retina and thus constitutes a promising target for the treatment of RP [89]. The specific molecular anti-inflammatory events that occur in the retina as a result of ocular neuromodulation therapy remain to be established. One possible explanation for reduction in retinal inflammation is improved ocular hemodynamics which results in attenuation of retinal hypoxia and ischemia at the cellular level [90]. Significant reductions of TNF-α and IL-6 levels in response to ONS have also been reported [90]. Additionally, the anti-inflammatory effect of the indirect activation of the vagus nerve via its neuronal connection with ophthalmic neve could not be ruled out [85,91]. On the other hand, neuroinflammation of the retina and subsequent cone damage is mediated at least in part by oxidative stress [36,92]. AA is highly concentrated in the retina [41,42]. Supraphysiological doses of ascorbate have anti-inflammatory effects; hence it is an extremely effective antioxidant and plays a central role in the regulation of intracellular redox state. AA also has sympatholytic effects and is efficient in improving endothelium-dependent vasodilatation by restoring nitric oxide activity [93].
On the other hand, microglial activation is an important pathologic hallmark of RP [94]. During the rapid rods degenerative phase in the RP experimental model, microglial cells switch from an alternative or anti-inflammatory and neuroprotective profile (M2) to a classic or proinflammatory and neurotoxic profile (M1) [95]. Microglia proliferate and infiltrate the photoreceptor layer and subretinal space, where they function as reactive phagocytes, phagocytose dead and stressed photoreceptors, secrete proinflammatory cytokines (e.g., TNFα and IL-1β), and chemokine, and recruit infiltrating immune cells [96,97]. Due to the mutant genetic background, however, microglial activation persists, and the continuous production of inflammatory and cytotoxic factors exacerbates photoreceptor loss until the late stage, at which point photoreceptors mostly die and the retinal structure is severely damaged [98]. Therapeutic regulation of the M1/M2 balance may represent a new therapeutic option for the treatment of neuroinflammation in RP regardless of genetic mutation. SP has been demonstrated to suppress inflammation in different experimental settings by promoting M2 polarization [32,99,100]. Then up-regulation of SP in the outer retina via ONS could offer anti-inflammatory effects directly by M2 polarization on the degenerating retina, or indirectly via recruitment of mesenchymal stem cells which has been shown to promote M2 polarization and inhibit M1 polarization both in vivo and in vitro studies [101]
Previous clinical studies have evaluated the effect of electrical stimulation on RP [102,103,104]. These studies have made use of a range of electrical stimulation settings, as well as several stimulation sites including transcorneal, transdermal, and transorbital electrical stimulation but with limited improvement of vision [102,103,104]. This is probably related to poor spatial resolution of electrical stimuli, the site of stimulation, and the late timing of intervention. On the other hand, vibrotactile ONS is emerging as an exciting and potentially more advantageous alternative to traditional electrical stimulation. In the present study, vibrochemical ONS has proved to be safe, and effective and it might provide a long-lasting method for modification of the neural circuit of the ocular circulation via external stimulation. Vibrotactile/ Vibro-chemical ONS has the potential of up-regulation of ocular parasympathetic system and trigeminovascular system [17,61,62]. It can selectively activate SP/CGRP-containing afferents fibers of the ophthalmic nerve.
TRPM8 is found in a subset of unmyelinated (C-type) afferents fibers of the trigeminal ganglion [105]. TRPM8 nerve fibers were observed throughout the sub-epithelium of human nasal mucosa with profuse fibers surrounding blood vessels [106]. Co-localization of SP, and TRPM8 in the slowly adapting nociceptive C fibers and mechanoreceptor Aδ fibers of ophthalmic nerve provide an ideal opportunity for selective activation of SP containing neurons. This was achieved by using mechanical stimulation and chemical stimulation via TRPM8 agonist (menthol) [107]. Overexpression of SP in response to ONS may have both neuroprotective and neuro-regenerative effects upon the photoreceptors and other retinal cells via a wide range of effects. These include augmentation of ocular blood flow [16,17,24], retinal pigment epithelium proliferation [108], prevention of apoptosis [29], induction of regeneration by the recruitment of endogenous stem cells [26] and suppression of neuroinflammation [31,32,99,100,101].
Intranasal pathway as a site for vibrochemical ONS has many advantages which include the presence of plenty of mechanoreceptors and chemoreceptors distributed in a specific manner in the nasal mucosa as shown by electrophysiological studies [109]. The nasal vestibule is innervated by the anterior ethmoid nerve, a branch of the nasociliary nerve that contains major vasodilatory innervation [19,20], with higher amounts of vasoactive neuropeptides, such as SP and calcitonin gene-related peptide [21,110]. Moreover, 72% of anterior ethmoid nerve is composed of unmyelinated C fibers, and 72% of anterior ethmoid nerve myelinated fibers are of mechanoreceptor Aδ fibers [111]. Administration of vibrochemical stimulation intra- nasally is ideal as it is located closer to the all-important targets to be stimulated. This includes the anterior ethmoid nerve, sphenopalatine ganglion, and mid-brain area where much of the autonomic functions lie.
The stimulation parameters, site of stimulation, duration, and schedule of the neurostimulation used for the treatment of RP were variable. A 30-minute session of nerve stimulation is a common feature among a number of studies including the present study [102,103,104,112,113]. The frequency of sessions varied from one session daily [112], one session weekly [113], or one session every two weeks’ sessions [103] for periods that might extend up to 52 weeks. In the present study, daily sessions of ONS for two consecutive weeks have been employed.
Identification of stimulation parameters and paradigms that yield maximal visual recovery is an important step in the translation of ONS-based ocular blood flow modulation and SP/CGRP expression for the treatment of RP. The potential of selective activation of SP/CGRP-loaded trigeminovascular system via stimulation of branches nasociliary nerve, one of the main divisions of the ophthalmic nerve has been demonstrated in a number of pre-clinical studies [19,20,25]. Furthermore, Hiraba et al have utilized vibrotactile stimulation settings of 89 Hz frequency and 1.9 μm amplitude for selective activation of the parasympathetic system [62], which in turn leads to vasodilatation and increased ocular blood flow [22,23]. Considering the heterogeneity of RP patient characteristics as well as the stage of the disease, it is possible that some subgroups may be more responsive to one set of stimulation settings than others. Nevertheless, the current study utilized a standard, non-individualized set of stimulation parameters and observed significant improvement in visual functions in most patients. This supports the notion that a relatively wide effective therapeutic range exists and individual variability is unlikely to preclude benefits. Regardless of the underlying mechanism, the differential responses to stimulation parameters highlight the utility of optimizing stimulation parameters to yield the greatest response. Further studies in the future are needed to explore the influence of timing, the stimulus parameters, and the bioavailability of expressed SP on the treatment efficacy. The manipulation of stimulation parameters alone or combined with inhibition of SP degradation may be required to optimize efficacy for clinical implementation.
The ocular neuromodulation protocol has the potential to induce glutamate-mediated neural plasticity and permanent changes in the targeted neural circuit, such as intra-retinal neural circuits and the trigeminovascular circuits of the eye. Glutamate is the main excitatory neurotransmitter in the retina [114]. It has been also implicated in retrograde signaling [115].
During the early stages of retinal degeneration, decreased glutamate release from rod photoreceptors prompts the breakdown of synaptic structures, dendritic sprouting, ectopic contact formation, and gliosis in downstream neurons, ultimately compromising the retinal circuit [116,117]. However, rod reactivation through gene therapy in a mouse model of retinal degeneration not only reinstates rod function along with glutamate release but also reverses retinal remodeling, inducing synaptogenesis and restoring visual signaling in the adult retina [118].
Enhancing endogenous glutamate release therapeutically could effectively stimulate the retina along established visual pathways, potentially offering more naturalistic vision management for RP. This enhancement may contribute to the rapid improvement in visual functions observed following ocular neuromodulation therapy. In contrast, non-selective electrical stimulation via retinal prosthesis simultaneously excites both the OFF and ON pathways in the inner nuclear layer, necessitating prolonged rehabilitation [119]. While gene therapy has shown success in restoring some visual function by repairing defective rod photoreceptors, limited success has been noted in adults, with continued retinal degeneration observed in some patients [120].
On the other hand, the neuromodulatory effects of ocular neuromodulation therapy on rod and cone functions appear to be long-lasting in both children and adults, likely due to the recovery of photoreceptor function and glutamate-mediated synaptogenesis. It's worth noting that ocular neuromodulation therapy may exert a dual action in restoring retinal glutamate levels, through glutamate released by recovered photoreceptors and the spillover of choroidal glutamate produced by retrograde ONS. The restoration of extracellular glutamate levels in the retina can prompt the modulation of existing neuronal circuitry and the secondary formation of new permanent neuronal connections in both the retina and the visual pathway. Thus, the term “neuronal plasticity”, which traditionally refers to long-lasting changes in neuronal structure and function, would be applicable
Defining the neuromodulation therapy intervention points is essential to developing effective treatments that both restore and maintain vision. In this study, we addressed the question of how different stages of the disease, respond to therapeutic intervention. We showed that intervention at early stage of the disease (stage II and Stage III) or within 10 years of night blindness, the treatment can significantly restore night vision. Interestingly, the onset of therapeutic effects appeared within days after treatment, while the peak of its action took 2 weeks to reach, suggesting that some rewiring and/or circuit stabilization were developed after ocular neuromodulation. Following late intervention, almost no scotopic vision can be restored. Accordingly, two therapeutic scenarios of ocular neuromodulation have been recognized; an early disease-modifying intervention that might prevent or reverse the disease process and a late cone rescue intervention that aims to improve/maintain central vision (Figure 5).
The maximum net benefit of the early disease-modifying intervention is anticipated when ocular neuromodulation is applied at the earliest possible timeframe. The affected individuals benefit from the intervention before any significant loss to rods, which contain rod-derived cone viability factor, an essential factor for cone survival [121]. Importantly, intervention at the early stages of the disease not only results in better scotopic and central vision but also produces a relatively long-lasting improvement in visual functions. The duration of action of ocular neuromodulation therapy was maintained up to 24 months in rod responders (Figure 3A–C). Nevertheless, the long-term follow-up indicated that ocular neuromodulation would lose some of its efficacy at some point. Therefore, follow-up and re-treatment are mandatory to achieve efficacy, such that the visual improvements are maintained and effects do not diminish over time. Based on our clinical observation, the durability of treatment varies among patients with different stages of the disease. Retreatment is anticipated to be necessary after six months for patients in stages IV or V, after 12 months for those in stage III, and after 18 months for patients in stage II. However, no data is available regarding the need for retreatment in stage 0 and stage I. It is interesting to note that re-treatment courses of ocular neuromodulation appear to be effective in restoring vision achieved by the primary treatment.
The ocular neuromodulation is emerging as a universal non-invasive therapeutic strategy for RP regardless the genetic background. It significantly improved night vision in the whole cohort by 29.6% at 6 months after treatment. Moreover, a clinically significant improvement in the BCVA and contrast sensitivity was also noticed. Unlike ocular neuromodulation, the recently developed Luxturna gene therapy is an invasive procedure that needs vitrectomy and a delicate maneuver for subretinal injection. At 6 and 12 months after surgery, the treated patients showed no improvement in the BCVA or contrast sensitivity. The mean value of scotopic vision, however, was significantly improved by 22.5% as judged by the multi-luminance mobility test [3]. Nevertheless, vision improvement under low luminance is almost equal in both therapeutic strategies. This comparison, however, is not valid as the severity of the disease, genotype and the proportion of pediatric participants are different in the two studies. Additionally, the multi-luminance mobility test was designed to evaluate the mobility of individuals under an artificial environment, whereas the LLQ-10, subjectively evaluates different aspects of daily life, under low luminance from RP patient’s perspectives. Nevertheless, in future studies, both subjective and objective methods should be utilized to appropriately measure the therapeutic effects of novel treatments on low-luminance vision in patients with RP.
The LLQ-10-based metrics are short, quick, accessible, and affordable tools for assessing the therapeutic response to ocular neuromodulation. LLQ-10 score effectively categorizes patients into two groups: those who respond well to treatment (high score) and those who don't (low score). This differentiation remains consistent over time, indicating the ILQ-10's reliability for tracking changes in patients' responses. The clinical validity of LLQ-10 is further supported by correlations between LLQ-10 scores at 6 months’ post-treatment and baseline participant characteristics. These correlations demonstrate significant associations between LLQ-10 scores and the stage of the disease, duration of night blindness, age of participant, ganglion cell layer thickness, central macular thickness, best-corrected visual acuity, and contrast sensitivity.
Luxturna gene for RP is formulated as a potential single-dose therapeutic intervention, offering a distinctive advantage over ocular neuromodulation, which necessitates multiple treatment sessions. In the context of ocular neuromodulation, both eyes are treated simultaneously, allowing patients to promptly resume their regular activities after the daily session. Conversely, gene therapy entails one surgery for each eye, 1 week apart. The inherent invasiveness of the procedure contributes to an extended recovery period, including the necessary adjustments in head posture and post-operative care.
In terms of safety, no ocular complications have been reported after the use of ocular neuromodulation, and systemic complications are so far restricted to headaches. In stark contrast, gene therapy introduces the potential for serious post-surgical complications, including endophthalmitis, retinal detachment, elevated intraocular pressure, cataracts, and inflammation, necessitating perioperative systemic steroid therapy. Additionally, late-onset chorio-retinal peri foveal retinal atrophy may manifest in certain instances [122], underscoring the safety profile of ocular neuromodulation as a comparatively secure option.
Furthermore, the implementation of gene therapy demands specialized facilities, intricate laboratory processes, and proficient medical practitioners, thereby restricting its accessibility to specific medical centers. Significantly, the exorbitant cost associated with gene therapy, amounting to USD 850,000 for the treatment of both eyes, further constrains its widespread adoption. In contrast, ocular neuromodulation requires less infrastructure and resources, rendering it a more affordable and accessible choice for a larger population worldwide.
This study is subject to three primary limitations. Firstly, the absence of a control group poses challenges in making valid comparisons within the treatment group. While placebo-controlled designs offer a robust framework for such comparisons, they often necessitate large sample sizes to detect subtle effects, particularly in conditions like RP where the desired effect size may be small. Alternatively, single-arm trials may be considered, especially in scenarios where the patient pool is limited. Single-arm trials are best utilized when the natural history of the disease is well understood and the spontaneous improvement in participants or long-lasting placebo effects are minimal or nonexistent [123]. Furthermore, the exposure of controls to intravenous placebo treatment and intranasal/extranasal false ONS for 30 minutes for a couple of weeks may raise ethical concerns. It is plausible that placebo mechanisms may contribute to short-term, but not long-term improvement of BCVA and contrast sensitivity in a disease with progressive course. Additionally, sustained enhancements in night vision among early-stage RP patients suggest otherwise. Nevertheless, this is a long-term, open-labeled single-armed intervention, and was intended to be an exploratory one. In the future, a proper control group should be considered in a multicenter double-blind prospective study.
Secondly, the utilization of LLQ-10 in the pediatric population introduces limitations. While the components of LLQ-10 were carefully selected to assess outcomes across both adult and pediatric cohorts with parental assistance, the inclusion of only a small number of pediatric patients, particularly those under 10 years old (4 patients), raises concern about the generalizability of the findings. Nevertheless, LLQ-10 demonstrates validity in stratifying patients into rod responders and rod-non-responders based on the stage of the disease, and structural measures, such as central retinal thickness and ganglion cell layer thickness, and are instrumental in tracking the longitudinal changes in scotopic vision, albeit the necessity of combining subjective and objective methods for comprehensive assessment in future studies.
Thirdly, the absence of electroretinography (ERG) as a diagnostic tool before patient recruitment is a notable limitation. ERG plays a crucial role in RP diagnosis, particularly in detecting preclinical stages and differentiating advanced stages of RP from other retinal pathologies. In this study, the diagnosis of RP was based on clinical history (night blindness and constricted visual field), nutritional background, the family tree of inherited cases, the presence of classical signs of RP in fundus examination, and established diagnostic criteria and corroborative evidence including ERG results from other clinical centers. The exclusion of preclinical cases and atypical RP presentations or (RP masquerades) [46] was also undertaken. Thenappan et al. emphasized that the integrity of a precise clinical assessment remains indispensable for the diagnosis of both RP and RP masquerade conditions[46]. Currently the genetic testing lacks utility as a screening tool for inherited retinal diseases, including RP [46]. Nevertheless, genetic testing is essential for evaluating the efficacy of non-gene-based therapy for RP with different genetic mutations, and the lack of a defined genotype is considered as another limitation in this study.
In conclusion, this study introduces vibrochemical ONS combined with ascorbate as a novel noninvasive method for the treatment of RP, a disease that currently has no treatment. It demonstrates the efficacy and safety of ocular neuromodulation as a universal treatment for different types of RP irrespective of their genetic background. The neuroprotective effects of ocular neuromodulation therapy are probably mediated by overexpression of SP/CGRP and modification of the neural circuit of the ocular circulation.
Patents
Ismail Musallam has pending US and Israeli patents licensed to himself for which he has waived financial interest.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Funding
none.
Acknowledgments
The authors gratefully acknowledge Nurse Tahani Qahooq for her assistance.
Conflicts of Interest
Ismail Musallam has a pending US and Israeli patents licensed to himself for which he has waived financial interest.
References
- Sandberg MA, Rosner B, Weigel-DiFranco C, Dryja TP, Berson EL. Disease course of patients with X-linked retinitis pigmentosa due to RPGR gene mutations. Investigative ophthalmology & visual science. 2007;48(3):1298-304. [CrossRef]
- Konieczka K, Flammer AJ, Todorova M, Meyer P, Flammer J. Retinitis pigmentosa and ocular blood flow. EPMA J. 2012;3(1):17-. [CrossRef]
- Russell S, Bennett J, Wellman JA, Chung DC, Yu ZF, Tillman A, et al. Efficacy and safety of voretigene neparvovec (AAV2-hRPE65v2) in patients with RPE65-mediated inherited retinal dystrophy: a randomised, controlled, open-label, phase 3 trial. Lancet (London, England). 2017;390(10097):849-60. [CrossRef]
- Linsenmeier RA, Padnick-Silver L. Metabolic dependence of photoreceptors on the choroid in the normal and detached retina. Investigative ophthalmology & visual science. 2000;41(10):3117-23.
- Langham ME, Kramer T. Decreased choroidal blood flow associated with retinitis pigmentosa. Eye (London, England). 1990;4 ( Pt 2):374-81. [CrossRef]
- Zhang Y, Harrison JM, Nateras OS, Chalfin S, Duong TQ. Decreased retinal-choroidal blood flow in retinitis pigmentosa as measured by MRI. Documenta ophthalmologica Advances in ophthalmology. 2013;126(3):187-97. [CrossRef]
- Abdolrahimzadeh S, Di Pippo M, Ciancimino C, Di Staso F, Lotery AJ. Choroidal vascularity index and choroidal thickness: potential biomarkers in retinitis pigmentosa. Eye. 2023;37(9):1766-73. [CrossRef]
- Shen C, Li Y, Wang Q, Chen YN, Li W, Wei WB. Choroidal vascular changes in retinitis pigmentosa patients detected by optical coherence tomography angiography. BMC ophthalmology. 2020;20(1):384. [CrossRef]
- Cetin EN, Parca O, Akkaya HS, Pekel G. Association of retinal biomarkers and choroidal vascularity index on optical coherence tomography using binarization method in retinitis pigmentosa. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2020;258(1):23-30. [CrossRef]
- Falsini B, Anselmi GM, Marangoni D, D'Esposito F, Fadda A, Di Renzo A, et al. Subfoveal choroidal blood flow and central retinal function in retinitis pigmentosa. Investigative ophthalmology & visual science. 2011;52(2):1064-9. [CrossRef]
- Grunwald JE, Maguire AM, Dupont J. Retinal hemodynamics in retinitis pigmentosa. American journal of ophthalmology. 1996;122(4):502-8. [CrossRef]
- Cellini M, Strobbe E, Gizzi C, Campos EC. ET-1 plasma levels and ocular blood flow in retinitis pigmentosa. Canadian journal of physiology and pharmacology. 2010;88(6):630-5. [CrossRef]
- Wolf S, Pöstgens H, Bertram B, Schulte K, Teping C, Reim M. [Hemodynamic findings in patients with retinitis pigmentosa]. Klinische Monatsblatter fur Augenheilkunde. 1991;199(5):325-9.
- Vingolo EM, Lupo S, Grenga PL, Salvatore S, Zinnamosca L, Cotesta D, et al. Endothelin-1 plasma concentrations in patients with retinitis pigmentosa. Regulatory peptides. 2010;160(1-3):64-7. [CrossRef]
- Cellini M, Santiago L, Versura P, Caramazza R. Plasma levels of endothelin-1 in retinitis pigmentosa. Ophthalmologica Journal international d'ophtalmologie International journal of ophthalmology Zeitschrift fur Augenheilkunde. 2002;216(4):265-8. [CrossRef]
- Reiner A, Fitzgerald MEC, Del Mar N, Li C. Neural control of choroidal blood flow. Progress in retinal and eye research. 2018;64:96-130. [CrossRef]
- McDougal DH, Gamlin PD. Autonomic control of the eye. Comprehensive Physiology. 2015;5(1):439-73. [CrossRef]
- Goadsby PJ, Edvinsson L, Ekman R. Release of vasoactive peptides in the extracerebral circulation of humans and the cat during activation of the trigeminovascular system. Annals of neurology. 1988;23(2):193-6. [CrossRef]
- Suzuki N, Hardebo JE, Owman C. Trigeminal fibre collaterals storing substance P and calcitonin gene-related peptide associate with ganglion cells containing choline acetyltransferase and vasoactive intestinal polypeptide in the sphenopalatine ganglion of the rat. An axon reflex modulating parasympathetic ganglionic activity? Neuroscience. 1989;30(3):595-604. [CrossRef]
- Hosaka F, Yamamoto M, Cho KH, Jang HS, Murakami G, Abe S. Human nasociliary nerve with special reference to its unique parasympathetic cutaneous innervation. Anatomy & cell biology. 2016;49(2):132-7. [CrossRef]
- Suzuki N, Hardebo JE, Owman C. Origins and pathways of cerebrovascular nerves storing substance P and calcitonin gene-related peptide in rat. Neuroscience. 1989;31(2):427-38. [CrossRef]
- Lambert GA, Bogduk N, Goadsby PJ, Duckworth JW, Lance JW. Decreased carotid arterial resistance in cats in response to trigeminal stimulation. Journal of neurosurgery. 1984;61(2):307-15. [CrossRef]
- Goadsby PJ, Edvinsson L. The trigeminovascular system and migraine: studies characterizing cerebrovascular and neuropeptide changes seen in humans and cats. Annals of neurology. 1993;33(1):48-56. [CrossRef]
- Stjernschantz J, Geijer C, Bill A. Electrical stimulation of the fifth cranial nerve in rabbits: effects on ocular blood flow, extravascular albumin content and intraocular pressure. Experimental eye research. 1979;28(2):229-38. [CrossRef]
- Bill A, Nilsson SF. Control of ocular blood flow. Journal of cardiovascular pharmacology. 1985;7 Suppl 3:S96-102.
- Kim JH, Jung Y, Kim BS, Kim SH. Stem cell recruitment and angiogenesis of neuropeptide substance P coupled with self-assembling peptide nanofiber in a mouse hind limb ischemia model. Biomaterials. 2013;34(6):1657-68. [CrossRef]
- Lee D, Hong HS. Substance P Alleviates Retinal Pigment Epithelium Dysfunction Caused by High Glucose-Induced Stress. Life (Basel, Switzerland). 2023;13(5). [CrossRef]
- Ou K, Mertsch S, Theodoropoulou S, Wu J, Liu J, Copland DA, et al. Restoring retinal neurovascular health via substance P. Experimental cell research. 2019;380(2):115-23. [CrossRef]
- Backman LJ, Eriksson DE, Danielson P. Substance P reduces TNF-α-induced apoptosis in human tenocytes through NK-1 receptor stimulation. British journal of sports medicine. 2014;48(19):1414-20. [CrossRef]
- Yang J-H, Guo Z, Zhang T, Meng XX, Xie L-S. Restoration of endogenous substance P is associated with inhibition of apoptosis of retinal cells in diabetic rats. Regulatory peptides. 2013;187:12-6. [CrossRef]
- Yoo K, Son BK, Kim S, Son Y, Yu S-Y, Hong HS. Substance P prevents development of proliferative vitreoretinopathy in mice by modulating TNF-α. Mol Vis. 2017;23:933-43.
- Lim JE, Chung E, Son Y. A neuropeptide, Substance-P, directly induces tissue-repairing M2 like macrophages by activating the PI3K/Akt/mTOR pathway even in the presence of IFNγ. Scientific reports. 2017;7(1):9417. [CrossRef]
- Baek SM, Yu SY, Son Y, Hong HS. Substance P promotes the recovery of oxidative stress-damaged retinal pigmented epithelial cells by modulating Akt/GSK-3β signaling. Molecular vision. 2016;22:1015-23.
- Kim DY, Piao J, Hong HS. Substance-P Inhibits Cardiac Microvascular Endothelial Dysfunction Caused by High Glucose-Induced Oxidative Stress. Antioxidants (Basel, Switzerland). 2021;10(7). [CrossRef]
- Piao J, Hong HS, Son Y. Substance P ameliorates tumor necrosis factor-alpha-induced endothelial cell dysfunction by regulating eNOS expression in vitro. Microcirculation (New York, NY : 1994). 2018;25(3):e12443. [CrossRef]
- Campochiaro PA, Iftikhar M, Hafiz G, Akhlaq A, Tsai G, Wehling D, et al. Oral N-acetylcysteine improves cone function in retinitis pigmentosa patients in phase I trial. The Journal of clinical investigation. 2020;130(3):1527-41. [CrossRef]
- Henry PT, Chandy MJ. Effect of ascorbic acid on infarct size in experimental focal cerebral ischaemia and reperfusion in a primate model. Acta neurochirurgica. 1998;140(9):977-80. [CrossRef]
- Ranjan A, Theodore D, Haran RP, Chandy MJ. Ascorbic acid and focal cerebral ischaemia in a primate model. Acta neurochirurgica. 1993;123(1-2):87-91. [CrossRef]
- Huang J, Agus DB, Winfree CJ, Kiss S, Mack WJ, McTaggart RA, et al. Dehydroascorbic acid, a blood-brain barrier transportable form of vitamin C, mediates potent cerebroprotection in experimental stroke. Proceedings of the National Academy of Sciences of the United States of America. 2001;98(20):11720-4. [CrossRef]
- Oudemans-van Straaten HM, Spoelstra-de Man AM, de Waard MC. Vitamin C revisited. Critical care (London, England). 2014;18(4):460. [CrossRef]
- Rose RC, Bode AM. Ocular ascorbate transport and metabolism. Comparative biochemistry and physiology A, Comparative physiology. 1991;100(2):273-85. [CrossRef]
- Hosoya K, Minamizono A, Katayama K, Terasaki T, Tomi M. Vitamin C transport in oxidized form across the rat blood-retinal barrier. Investigative ophthalmology & visual science. 2004;45(4):1232-9. [CrossRef]
- Jackson TS, Xu A, Vita JA, Keaney JF, Jr. Ascorbate prevents the interaction of superoxide and nitric oxide only at very high physiological concentrations. Circulation research. 1998;83(9):916-22. [CrossRef]
- Bruno RM, Daghini E, Ghiadoni L, Sudano I, Rugani I, Varanini M, et al. Effect of acute administration of vitamin C on muscle sympathetic activity, cardiac sympathovagal balance, and baroreflex sensitivity in hypertensive patients. The American journal of clinical nutrition. 2012;96(2):302-8. [CrossRef]
- SWOG:. Cancer Research Network – Cancer Research and Biostatistics. https://stattoolscraborg/Calculators/oneArmSurvivalColoredhtml.
- Thenappan A, Nanda A, Lee CS, Lee SY. Retinitis Pigmentosa Masquerades: Case Series and Review of the Literature. Journal of clinical medicine. 2023;12(17). [CrossRef]
- Oh R, Bae K, Yoon CK, Park UC, Park KH, Lee EK. Quantitative microvascular analysis in different stages of retinitis pigmentosa using optical coherence tomography angiography. Scientific reports. 2024;14(1):4688. [CrossRef]
- Ito N, Miura G, Shiko Y, Kawasaki Y, Baba T, Yamamoto S. Progression Rate of Visual Function and Affecting Factors at Different Stages of Retinitis Pigmentosa. BioMed research international. 2022;2022:7204954. [CrossRef]
- Iftikhar M, Lemus M, Usmani B, Campochiaro PA, Sahel JA, Scholl HPN, et al. Classification of disease severity in retinitis pigmentosa. The British journal of ophthalmology. 2019;103(11):1595-9. [CrossRef]
- Oner A, Sinim Kahraman N. A New Classification for Retinitis Pigmentosa Including Multifocal Electroretinography to Evaluate the Disease Severity. Open Journal of Ophthalmology. 2023;13:37-47. [CrossRef]
- Smith HB, Chandra A, Zambarakji H. Grading severity in retinitis pigmentosa using clinical assessment, visual acuity, perimetry and optical coherence tomography. International ophthalmology. 2013;33(3):237-44. [CrossRef]
- O'Neill JJ, McKay GJ, Simpson DA, Silvestri G. Retinitis Pigmentosa Assessment Severity Scale (RPASS) for Use in Scientific Analysis and Classification of Disease Progression. Investigative ophthalmology & visual science. 2006;47(13):1419-.
- Milam AH, Li ZY, Fariss RN. Histopathology of the human retina in retinitis pigmentosa. Progress in retinal and eye research. 1998;17(2):175-205. [CrossRef]
- Li ZY, Possin DE, Milam AH. Histopathology of bone spicule pigmentation in retinitis pigmentosa. Ophthalmology. 1995;102(5):805-16. [CrossRef]
- Ma Y, Kawasaki R, Dobson LP, Ruddle JB, Kearns LS, Wong TY, et al. Quantitative Analysis of Retinal Vessel Attenuation in Eyes with Retinitis Pigmentosa. Investigative ophthalmology & visual science. 2012;53(7):4306-14. [CrossRef]
- Nakagawa S, Oishi A, Ogino K, Makiyama Y, Kurimoto M, Yoshimura N. Association of retinal vessel attenuation with visual function in eyes with retinitis pigmentosa. Clinical ophthalmology (Auckland, NZ). 2014;8:1487-93. [CrossRef]
- Albakri AS, Al-Shahwan E, Nowilaty SR. Correlation Of Retinitis Pigmentosa Disease Stage With Orbital Color Doppler Imaging. Investigative ophthalmology & visual science. 2012;53(14):6846-.
- Lesko LJ, Atkinson AJ, Jr. Use of biomarkers and surrogate endpoints in drug development and regulatory decision making: criteria, validation, strategies. Annual review of pharmacology and toxicology. 2001;41:347-66. [CrossRef]
- Medeiros FA. Biomarkers and Surrogate Endpoints: Lessons Learned From Glaucoma. Investigative ophthalmology & visual science. 2017;58(6):Bio20-bio6. [CrossRef]
- Owsley C, McGwin G, Jr., Scilley K, Kallies K. Development of a questionnaire to assess vision problems under low luminance in age-related maculopathy. Investigative ophthalmology & visual science. 2006;47(2):528-35. [CrossRef]
- Reiner A, Fitzgerald MC, C. L. Neural Control of Ocular Blood Flow. Editors. Ocular Blood Flow. Berlin Heidelberge:springer; 2012.
- Hiraba H, Inoue M, Gora K, Sato T, Nishimura S, Yamaoka M, et al. Facial vibrotactile stimulation activates the parasympathetic nervous system: study of salivary secretion, heart rate, pupillary reflex, and functional near-infrared spectroscopy activity. BioMed research international. 2014;2014:910812. [CrossRef]
- Li ZY, Kljavin IJ, Milam AH. Rod photoreceptor neurite sprouting in retinitis pigmentosa. The Journal of neuroscience : the official journal of the Society for Neuroscience. 1995;15(8):5429-38.
- Wang W, Lee SJ, Scott PA, Lu X, Emery D, Liu Y, et al. Two-Step Reactivation of Dormant Cones in Retinitis Pigmentosa. Cell reports. 2016;15(2):372-85. [CrossRef]
- Wang W, Kini A, Wang Y, Liu T, Chen Y, Vukmanic E, et al. Metabolic Deregulation of the Blood-Outer Retinal Barrier in Retinitis Pigmentosa. Cell reports. 2019;28(5):1323-34.e4. [CrossRef]
- Toto L, Borrelli E, Mastropasqua R, Senatore A, Di Antonio L, Di Nicola M, et al. Macular Features in Retinitis Pigmentosa: Correlations Among Ganglion Cell Complex Thickness, Capillary Density, and Macular Function. Investigative ophthalmology & visual science. 2016;57(14):6360-6. [CrossRef]
- Hayreh SS. In vivo choroidal circulation and its watershed zones. Eye (London, England). 1990;4 ( Pt 2):273-89. [CrossRef]
- Punzo C, Kornacker K, Cepko CL. Stimulation of the insulin/mTOR pathway delays cone death in a mouse model of retinitis pigmentosa. Nature neuroscience. 2009;12(1):44-52. [CrossRef]
- Shigesada N, Shikada N, Shirai M, Toriyama M, Higashijima F, Kimura K, et al. Combination of blockade of endothelin signalling and compensation of IGF1 expression protects the retina from degeneration. Cellular and molecular life sciences : CMLS. 2024;81(1):51. [CrossRef]
- Kedzierski RM, Yanagisawa M. Endothelin system: the double-edged sword in health and disease. Annual review of pharmacology and toxicology. 2001;41:851-76. [CrossRef]
- Derella CC, Tingen MS, Blanks A, Sojourner SJ, Tucker MA, Thomas J, et al. Smoking cessation reduces systemic inflammation and circulating endothelin-1. Scientific reports. 2021;11(1):24122. [CrossRef]
- Kobayashi Y, Watanabe S, Shirai M, Yamashiro C, Ogata T, Higashijima F, et al. Light-dependent induction of Edn2 expression and attenuation of retinal pathology by endothelin receptor antagonists in Prominin-1- deficient mice. 2020.
- Dellett M, Sasai N, Nishide K, Becker S, Papadaki V, Limb GA, et al. Genetic background and light-dependent progression of photoreceptor cell degeneration in Prominin-1 knockout mice. Investigative ophthalmology & visual science. 2014;56(1):164-76. [CrossRef]
- Oishi A, Noda K, Birtel J, Miyake M, Sato A, Hasegawa T, et al. Effect of smoking on macular function and retinal structure in retinitis pigmentosa. Brain communications. 2020;2(2):fcaa117. [CrossRef]
- Zhu X, Lin X, Xu Y, Li N, Zhou Q, Sun X, et al. Effect of Dual Endothelin Receptor Antagonist on a Retinal Degeneration Animal Model by Regulating Choroidal Microvascular Morphology. Journal of ophthalmology. 2021;2021:5688300. [CrossRef]
- Kirkby NS, Hadoke PW, Bagnall AJ, Webb DJ. The endothelin system as a therapeutic target in cardiovascular disease: great expectations or bleak house? British journal of pharmacology. 2008;153(6):1105-19. [CrossRef]
- De Mey J, Compeer MG, Meens MJJMCP. Endothelin-1, an endogenous irreversible agonist in search of an allosteric inhibitor. 2009;1:246-57. [CrossRef]
- Meens MJ, Compeer MG, Hackeng TM, van Zandvoort MA, Janssen BJ, De Mey JG. Stimuli of sensory-motor nerves terminate arterial contractile effects of endothelin-1 by CGRP and dissociation of ET-1/ET(A)-receptor complexes. PloS one. 2010;5(6):e10917. [CrossRef]
- Hilal-Dandan R, Villegas S, Gonzalez A, Brunton LL. The quasi-irreversible nature of endothelin binding and G protein-linked signaling in cardiac myocytes. The Journal of pharmacology and experimental therapeutics. 1997;281(1):267-73. [CrossRef]
- Meens MJPMT, Mattheij NJA, Nelissen J, Lemkens P, Compeer MG, Janssen BJA, et al. Calcitonin Gene-Related Peptide Terminates Long-Lasting Vasopressor Responses to Endothelin 1 In Vivo. Hypertension. 2011;58(1):99-106. [CrossRef]
- Ferrara N. Vascular endothelial growth factor: molecular and biological aspects. Current topics in microbiology and immunology. 1999;237:1-30. [CrossRef]
- Salom D, Diaz-Llopis M, García-Delpech S, Udaondo P, Sancho-Tello M, Romero FJ. Aqueous humor levels of vascular endothelial growth factor in retinitis pigmentosa. Investigative ophthalmology & visual science. 2008;49(8):3499-502. [CrossRef]
- Lv YX, Zhong S, Tang H, Luo B, Chen SJ, Chen L, et al. VEGF-A and VEGF-B Coordinate the Arteriogenesis to Repair the Infarcted Heart with Vagus Nerve Stimulation. Cellular physiology and biochemistry : international journal of experimental cellular physiology, biochemistry, and pharmacology. 2018;48(2):433-49. [CrossRef]
- Luo B, Wu Y, Liu SL, Li XY, Zhu HR, Zhang L, et al. Vagus nerve stimulation optimized cardiomyocyte phenotype, sarcomere organization and energy metabolism in infarcted heart through FoxO3A-VEGF signaling. Cell death & disease. 2020;11(11):971. [CrossRef]
- Rogers RC, Kita H, Butcher LL, Novin D. Afferent projections to the dorsal motor nucleus of the vagus. Brain research bulletin. 1980;5(4):365-73. [CrossRef]
- Liu L, Dana R, Yin J. Sensory neurons directly promote angiogenesis in response to inflammation via substance P signaling. FASEB journal : official publication of the Federation of American Societies for Experimental Biology. 2020;34(5):6229-43. [CrossRef]
- Ziche M, Morbidelli L, Pacini M, Geppetti P, Alessandri G, Maggi CA. Substance P stimulates neovascularization in vivo and proliferation of cultured endothelial cells. Microvascular research. 1990;40(2):264-78. [CrossRef]
- Kohara H, Tajima S, Yamamoto M, Tabata Y. Angiogenesis induced by controlled release of neuropeptide substance P. Biomaterials. 2010;31(33):8617-25. [CrossRef]
- Yoshida N, Ikeda Y, Notomi S, Ishikawa K, Murakami Y, Hisatomi T, et al. Laboratory evidence of sustained chronic inflammatory reaction in retinitis pigmentosa. Ophthalmology. 2013;120(1):e5-12. [CrossRef]
- Li C, Chiluwal A, Afridi A, Chaung W, Powell K, Yang WL, et al. Trigeminal Nerve Stimulation: A Novel Method of Resuscitation for Hemorrhagic Shock. Critical care medicine. 2019;47(6):e478-e84. [CrossRef]
- Borovikova LV, Ivanova S, Zhang M, Yang H, Botchkina GI, Watkins LR, et al. Vagus nerve stimulation attenuates the systemic inflammatory response to endotoxin. Nature. 2000;405(6785):458-62. [CrossRef]
- Komeima K, Rogers BS, Lu L, Campochiaro PA. Antioxidants reduce cone cell death in a model of retinitis pigmentosa. Proceedings of the National Academy of Sciences of the United States of America. 2006;103(30):11300-5. [CrossRef]
- Taddei S, Virdis A, Ghiadoni L, Magagna A, Salvetti A. Vitamin C improves endothelium-dependent vasodilation by restoring nitric oxide activity in essential hypertension. Circulation. 1998;97(22):2222-9. [CrossRef]
- Gupta N, Brown KE, Milam AH. Activated microglia in human retinitis pigmentosa, late-onset retinal degeneration, and age-related macular degeneration. Experimental eye research. 2003;76(4):463-71. [CrossRef]
- Zhou T, Huang Z, Sun X, Zhu X, Zhou L, Li M, et al. Microglia Polarization with M1/M2 Phenotype Changes in rd1 Mouse Model of Retinal Degeneration. Frontiers in neuroanatomy. 2017;11:77. [CrossRef]
- Zhao L, Zabel MK, Wang X, Ma W, Shah P, Fariss RN, et al. Microglial phagocytosis of living photoreceptors contributes to inherited retinal degeneration. EMBO molecular medicine. 2015;7(9):1179-97. [CrossRef]
- Blank T, Goldmann T, Koch M, Amann L, Schön C, Bonin M, et al. Early Microglia Activation Precedes Photoreceptor Degeneration in a Mouse Model of CNGB1-Linked Retinitis Pigmentosa. Frontiers in immunology. 2017;8:1930. [CrossRef]
- Zhang L, Cui X, Jauregui R, Park KS, Justus S, Tsai YT, et al. Genetic Rescue Reverses Microglial Activation in Preclinical Models of Retinitis Pigmentosa. Molecular therapy : the journal of the American Society of Gene Therapy. 2018;26(8):1953-64. [CrossRef]
- Jiang MH, Chung E, Chi GF, Ahn W, Lim JE, Hong HS, et al. Substance P induces M2-type macrophages after spinal cord injury. Neuroreport. 2012;23(13):786-92. [CrossRef]
- Ahn W, Chi G, Kim S, Son Y, Zhang M. Substance P Reduces Infarct Size and Mortality After Ischemic Stroke, Possibly Through the M2 Polarization of Microglia/Macrophages and Neuroprotection in the Ischemic Rat Brain. Cellular and molecular neurobiology. 2023;43(5):2035-52. [CrossRef]
- Liu Y, Zeng R, Wang Y, Huang W, Hu B, Zhu G, et al. Mesenchymal stem cells enhance microglia M2 polarization and attenuate neuroinflammation through TSG-6. Brain Res. 2019;1724:146422. [CrossRef]
- Jolly JK, Wagner SK, Martus P, MacLaren RE, Wilhelm B, Webster AR, et al. Transcorneal Electrical Stimulation for the Treatment of Retinitis Pigmentosa: A Multicenter Safety Study of the OkuStim® System (TESOLA-Study). Ophthalmic research. 2020;63(3):234-43. [CrossRef]
- Miura G, Sugawara T, Kawasaki Y, Tatsumi T, Nizawa T, Baba T, et al. Clinical Trial to Evaluate Safety and Efficacy of Transdermal Electrical Stimulation on Visual Functions of Patients with Retinitis Pigmentosa. Scientific reports. 2019;9(1):11668. [CrossRef]
- de Rossi F, Guidobaldi M, Turco S, Amore F. Transorbital electrical stimulation in retinitis pigmentosa. Better results joining visual pattern stimulation? Brain stimulation. 2020;13(5):1173-4. [CrossRef]
- Iftinca M, Altier C. The cool things to know about TRPM8! Channels (Austin, Tex). 2020;14(1):413-20. [CrossRef]
- Keh SM, Facer P, Yehia A, Sandhu G, Saleh HA, Anand P. The menthol and cold sensation receptor TRPM8 in normal human nasal mucosa and rhinitis. Rhinology. 2011;49(4):453-7.
- Bae JY, Kim JH, Cho YS, Mah W, Bae YC. Quantitative analysis of afferents expressing substance P, calcitonin gene-related peptide, isolectin B4, neurofilament 200, and Peripherin in the sensory root of the rat trigeminal ganglion. The Journal of comparative neurology. 2015;523(1):126-38. [CrossRef]
- Hong HS, Kim S, Nam S, Um J, Kim YH, Son Y. Effect of substance P on recovery from laser-induced retinal degeneration. Wound repair and regeneration : official publication of the Wound Healing Society [and] the European Tissue Repair Society. 2015;23(2):268-77. [CrossRef]
- Scheibe M, van Thriel C, Hummel T. Responses to trigeminal irritants at different locations of the human nasal mucosa. The Laryngoscope. 2008;118(1):152-5. [CrossRef]
- Atalay B, Bolay H, Dalkara T, Soylemezoglu F, Oge K, Ozcan OE. Transcorneal stimulation of trigeminal nerve afferents to increase cerebral blood flow in rats with cerebral vasospasm: a noninvasive method to activate the trigeminovascular reflex. Journal of neurosurgery. 2002;97(5):1179-83. [CrossRef]
- McCulloch PF, Faber KM, Panneton WM. Electrical stimulation of the anterior ethmoidal nerve produces the diving response. Brain Res. 1999;830(1):24-31. [CrossRef]
- Bittner AK, Seger K, Salveson R, Kayser S, Morrison N, Vargas P, et al. Randomized controlled trial of electro-stimulation therapies to modulate retinal blood flow and visual function in retinitis pigmentosa. Acta ophthalmologica. 2018;96(3):e366-e76. [CrossRef]
- Schatz A, Pach J, Gosheva M, Naycheva L, Willmann G, Wilhelm B, et al. Transcorneal Electrical Stimulation for Patients With Retinitis Pigmentosa: A Prospective, Randomized, Sham-Controlled Follow-up Study Over 1 Year. Investigative ophthalmology & visual science. 2017;58(1):257-69. [CrossRef]
- Kalloniatis M, Tomisich G. Amino acid neurochemistry of the vertebrate retina. Progress in retinal and eye research. 1999;18(6):811-66. [CrossRef]
- Zilberter Y, Harkany T, Holmgren CD. Dendritic release of retrograde messengers controls synaptic transmission in local neocortical networks. The Neuroscientist : a review journal bringing neurobiology, neurology and psychiatry. 2005;11(4):334-44. [CrossRef]
- Puthussery T, Taylor WR. Functional changes in inner retinal neurons in animal models of photoreceptor degeneration. Advances in experimental medicine and biology. 2010;664:525-32. [CrossRef]
- Marc RE, Jones BW, Watt CB, Strettoi E. Neural remodeling in retinal degeneration. Progress in retinal and eye research. 2003;22(5):607-55. [CrossRef]
- Wang T, Pahlberg J, Cafaro J, Frederiksen R, Cooper AJ, Sampath AP, et al. Activation of Rod Input in a Model of Retinal Degeneration Reverses Retinal Remodeling and Induces Formation of Functional Synapses and Recovery of Visual Signaling in the Adult Retina. The Journal of neuroscience : the official journal of the Society for Neuroscience. 2019;39(34):6798-810. [CrossRef]
- Wu J, Rountree CM, Kare S-S, Ramkumar PK, Finan JD, Troy JB. Progress on Designing a Chemical Retinal Prosthesis. 2022;16. [CrossRef]
- Cideciyan AV, Jacobson SG, Beltran WA, Sumaroka A, Swider M, Iwabe S, et al. Human retinal gene therapy for Leber congenital amaurosis shows advancing retinal degeneration despite enduring visual improvement. Proceedings of the National Academy of Sciences of the United States of America. 2013;110(6):E517-25. [CrossRef]
- Aït-Ali N, Fridlich R, Millet-Puel G, Clérin E, Delalande F, Jaillard C, et al. Rod-derived cone viability factor promotes cone survival by stimulating aerobic glycolysis. Cell. 2015;161(4):817-32. [CrossRef]
- Gange WS, Sisk RA, Besirli CG, Lee TC, Havunjian M, Schwartz H, et al. Perifoveal Chorioretinal Atrophy after Subretinal Voretigene Neparvovec-rzyl for RPE65-Mediated Leber Congenital Amaurosis. Ophthalmology Retina. 2022;6(1):58-64. [CrossRef]
- Evans SR. Clinical trial structures. Journal of experimental stroke & translational medicine. 2010;3(1):8-18. [CrossRef]
Figure 1.
Schematic of neural pathways that control ocular blood flow (OBF). SNS; sympathetic nervous system, PNS; parasympathetic nervous system, TVS: trigeminovascular system, TG: trigeminal ganglion, PPG: pterygopalatine ganglion, SSN: superior salivatory nucleus, SCG: superior cervical ganglion, RVLM: rostro-ventrolateral medulla, SP: substance P, CGRP; calcitonin gene-related peptide, Ach: acetylcholine, NO: nitric oxide, VAP: vasoactive intestinal polypeptide, NA: noradrenaline, NPY; neuropeptide Y.
Figure 1.
Schematic of neural pathways that control ocular blood flow (OBF). SNS; sympathetic nervous system, PNS; parasympathetic nervous system, TVS: trigeminovascular system, TG: trigeminal ganglion, PPG: pterygopalatine ganglion, SSN: superior salivatory nucleus, SCG: superior cervical ganglion, RVLM: rostro-ventrolateral medulla, SP: substance P, CGRP; calcitonin gene-related peptide, Ach: acetylcholine, NO: nitric oxide, VAP: vasoactive intestinal polypeptide, NA: noradrenaline, NPY; neuropeptide Y.
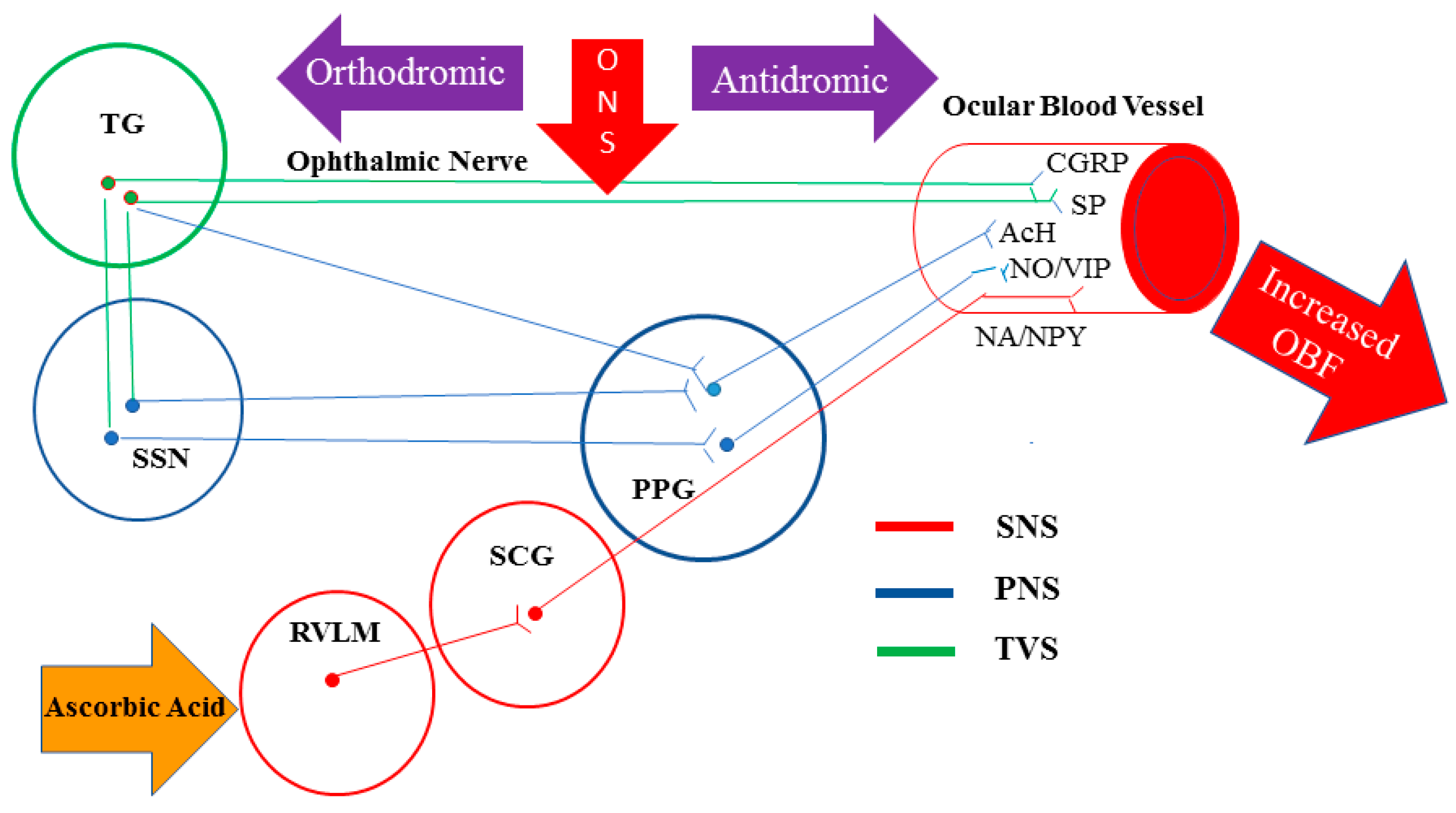
Figure 2.
(A) Sites of ophthalmic nerve stimulation(ONS); (1) Intranasal: for stimulation of anterior ethmoid nerve at the nasal septum, (2) Nasal bridge: for stimulation of infratrochlear nerve, a branch of nasociliary nerve and external nasal nerve, the terminal branch of external anterior ethmoid nerve, (3) Supraorbital region: for stimulation of supraorbital and supratrochlear nerve, branches of frontal nerve. (B) Handheld vibrotactile ophthalmic nerve stimulator. An intranasal application head is designed to be small enough to fit comfortably and safely within the restricted size of the nasal vestibule and optionally made by polyethyl methacrylate to prevent the warming produced by the vibration. (C) Head-mounted vibrotactile ophthalmic nerve stimulator with two application heads over the supraorbital region on both sides.
Figure 2.
(A) Sites of ophthalmic nerve stimulation(ONS); (1) Intranasal: for stimulation of anterior ethmoid nerve at the nasal septum, (2) Nasal bridge: for stimulation of infratrochlear nerve, a branch of nasociliary nerve and external nasal nerve, the terminal branch of external anterior ethmoid nerve, (3) Supraorbital region: for stimulation of supraorbital and supratrochlear nerve, branches of frontal nerve. (B) Handheld vibrotactile ophthalmic nerve stimulator. An intranasal application head is designed to be small enough to fit comfortably and safely within the restricted size of the nasal vestibule and optionally made by polyethyl methacrylate to prevent the warming produced by the vibration. (C) Head-mounted vibrotactile ophthalmic nerve stimulator with two application heads over the supraorbital region on both sides.
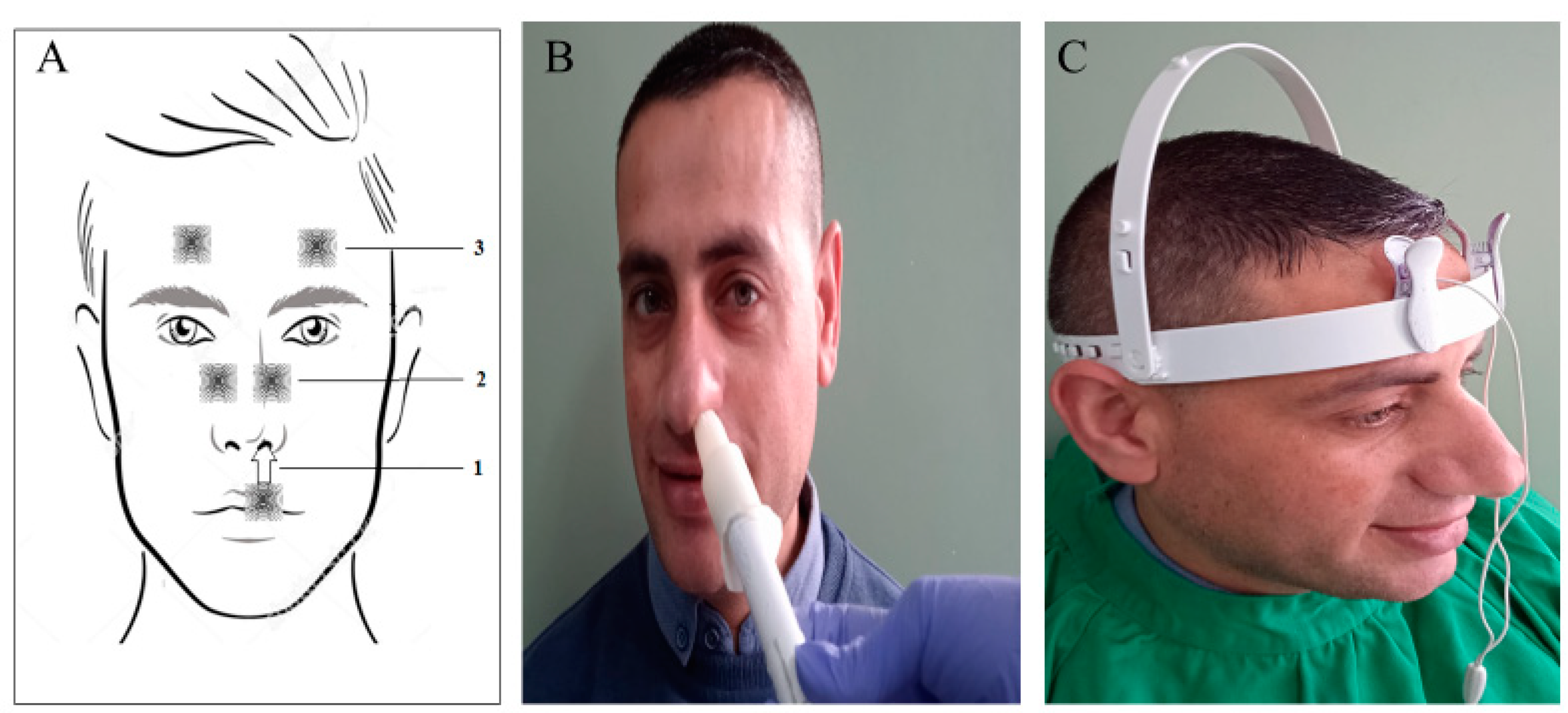
Figure 3.
Ocular Neuromodulation: Changes in visual functions and predictors for rod responders in study participants: (A) Median value of LLQ-10 score among the whole cohort (grey line), rod-responders (blue line), and rod-non-responders (red line) at baseline and post-treatment visits. (B) The median value of best corrected visual acuity (BCVA) (LogMAR unit) in the right eye among the whole cohort at baseline and post-treatment visits. (C) The median value of contrast sensitivity (Log unit) in the right eye among the whole cohort at baseline and post-treatment visits. In (A), (B), and (C) figures; * (* p≤ 0.05); statistically significant differences in the median value of ILQ-10 score, BCVA, and contrast sensitivity at different post-treatment visits compared to baseline respectively (D) Proportion (%) of rod responders (Blue bar) and rod-non-responders (red bar) among participants at different bassline stages of the disease. The percentage (%) of rod responders and rod- non-responders are included in the graph. Individuals exhibiting rod responsiveness were predominant in the earlier stages of the disease (P=0.0001). (E) Proportion (%) of rod responders (blue bar) and rod-non-responders (red bar) among participants with different durations of night blindness at baseline. The percentage of rod responders and rod-non-responders is included in the graph. The rod responders were found to have a significantly shorter median duration of night blindness compared to rod-non-responders (10.0 yrs. vs 21.0 yrs.) (p=0.003). (E) Proportion (%) of right eyes of rod responders (blue bare) versus rod-non-responders of the whole cohort that showed a clinically significant improvement of BCVA (improvement of ≥0.2 logMAR) and contrast sensitivity (improvement of ≥0.3 log unit) (* p≤ 0.05), N.S; Not significant).
Figure 3.
Ocular Neuromodulation: Changes in visual functions and predictors for rod responders in study participants: (A) Median value of LLQ-10 score among the whole cohort (grey line), rod-responders (blue line), and rod-non-responders (red line) at baseline and post-treatment visits. (B) The median value of best corrected visual acuity (BCVA) (LogMAR unit) in the right eye among the whole cohort at baseline and post-treatment visits. (C) The median value of contrast sensitivity (Log unit) in the right eye among the whole cohort at baseline and post-treatment visits. In (A), (B), and (C) figures; * (* p≤ 0.05); statistically significant differences in the median value of ILQ-10 score, BCVA, and contrast sensitivity at different post-treatment visits compared to baseline respectively (D) Proportion (%) of rod responders (Blue bar) and rod-non-responders (red bar) among participants at different bassline stages of the disease. The percentage (%) of rod responders and rod- non-responders are included in the graph. Individuals exhibiting rod responsiveness were predominant in the earlier stages of the disease (P=0.0001). (E) Proportion (%) of rod responders (blue bar) and rod-non-responders (red bar) among participants with different durations of night blindness at baseline. The percentage of rod responders and rod-non-responders is included in the graph. The rod responders were found to have a significantly shorter median duration of night blindness compared to rod-non-responders (10.0 yrs. vs 21.0 yrs.) (p=0.003). (E) Proportion (%) of right eyes of rod responders (blue bare) versus rod-non-responders of the whole cohort that showed a clinically significant improvement of BCVA (improvement of ≥0.2 logMAR) and contrast sensitivity (improvement of ≥0.3 log unit) (* p≤ 0.05), N.S; Not significant).
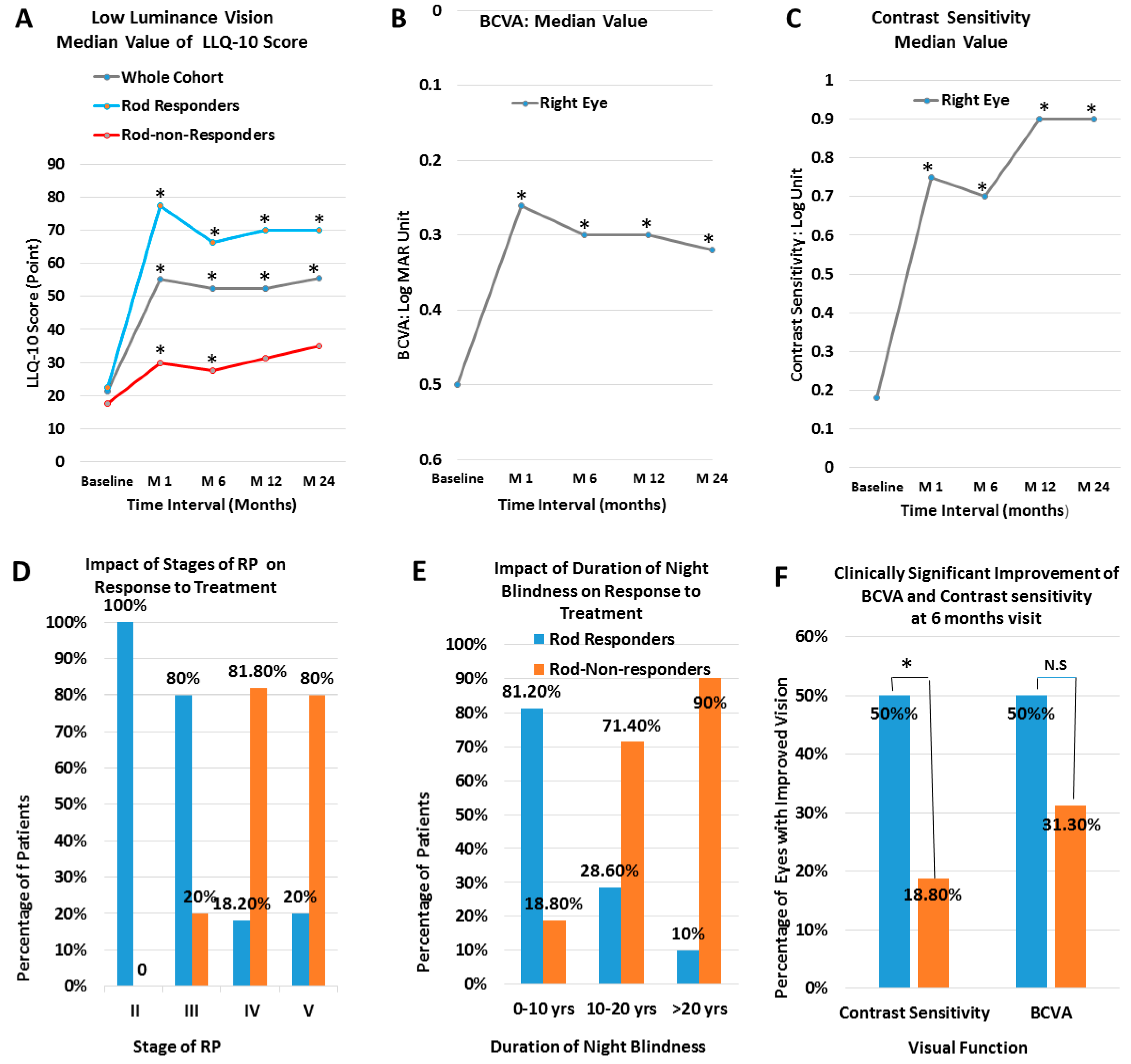
Figure 4.
OCT Angio of OD and OS of a six-year-old boy with stage II RP at baseline (pre-treatment) and 26 months (post-treatment) after ocular neuromodulation therapy. The vascular density increased significantly at the para-foveal region at the level of superficial and deep capillary plexus in both eyes. The foveal avascular zone gets smaller after treatment. Yellow arrows indicate the site of non-perfused/drop out of capillaries at the level of the superficial and deep retinal plexus before treatment.
Figure 4.
OCT Angio of OD and OS of a six-year-old boy with stage II RP at baseline (pre-treatment) and 26 months (post-treatment) after ocular neuromodulation therapy. The vascular density increased significantly at the para-foveal region at the level of superficial and deep capillary plexus in both eyes. The foveal avascular zone gets smaller after treatment. Yellow arrows indicate the site of non-perfused/drop out of capillaries at the level of the superficial and deep retinal plexus before treatment.
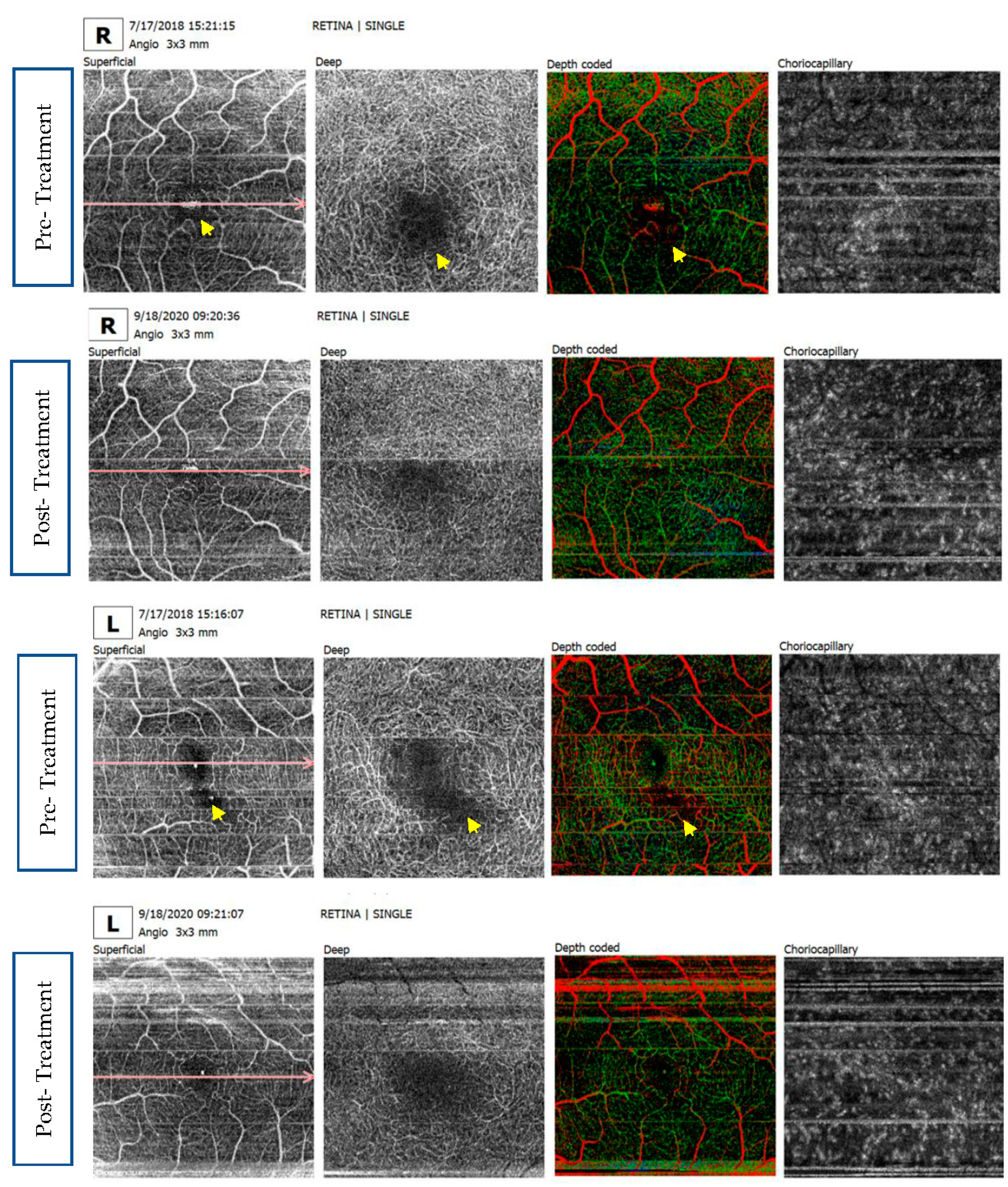
Figure 5.
Photoreceptors degeneration and the effect of ocular neuromodulation therapy on the course of the disease. (A) The natural course of rods (black line) and cones (white line) degeneration in RP. The blue arrow indicates the time of initiation of ocular neuromodulation. (B) and (C) ocular neuromodulation therapy initiated at the early rod degeneration phase (stage I and II) respectively. The green line represents an early disease-modifying effect of ocular neuromodulation therapy to reverse the disease process via restoration of the function of dormant rods. (D) ocular neuromodulation therapy initiated at the transitional phase (stage III). The green line represents the anticipated modified course of rod and cone photoreceptors. In (E), and (F), the interrupted green line represents a cone rescue strategy wherein ocular neuromodulation therapy is initiated at stages, IV and V respectively (Late cone degeneration phase of RP).
Figure 5.
Photoreceptors degeneration and the effect of ocular neuromodulation therapy on the course of the disease. (A) The natural course of rods (black line) and cones (white line) degeneration in RP. The blue arrow indicates the time of initiation of ocular neuromodulation. (B) and (C) ocular neuromodulation therapy initiated at the early rod degeneration phase (stage I and II) respectively. The green line represents an early disease-modifying effect of ocular neuromodulation therapy to reverse the disease process via restoration of the function of dormant rods. (D) ocular neuromodulation therapy initiated at the transitional phase (stage III). The green line represents the anticipated modified course of rod and cone photoreceptors. In (E), and (F), the interrupted green line represents a cone rescue strategy wherein ocular neuromodulation therapy is initiated at stages, IV and V respectively (Late cone degeneration phase of RP).
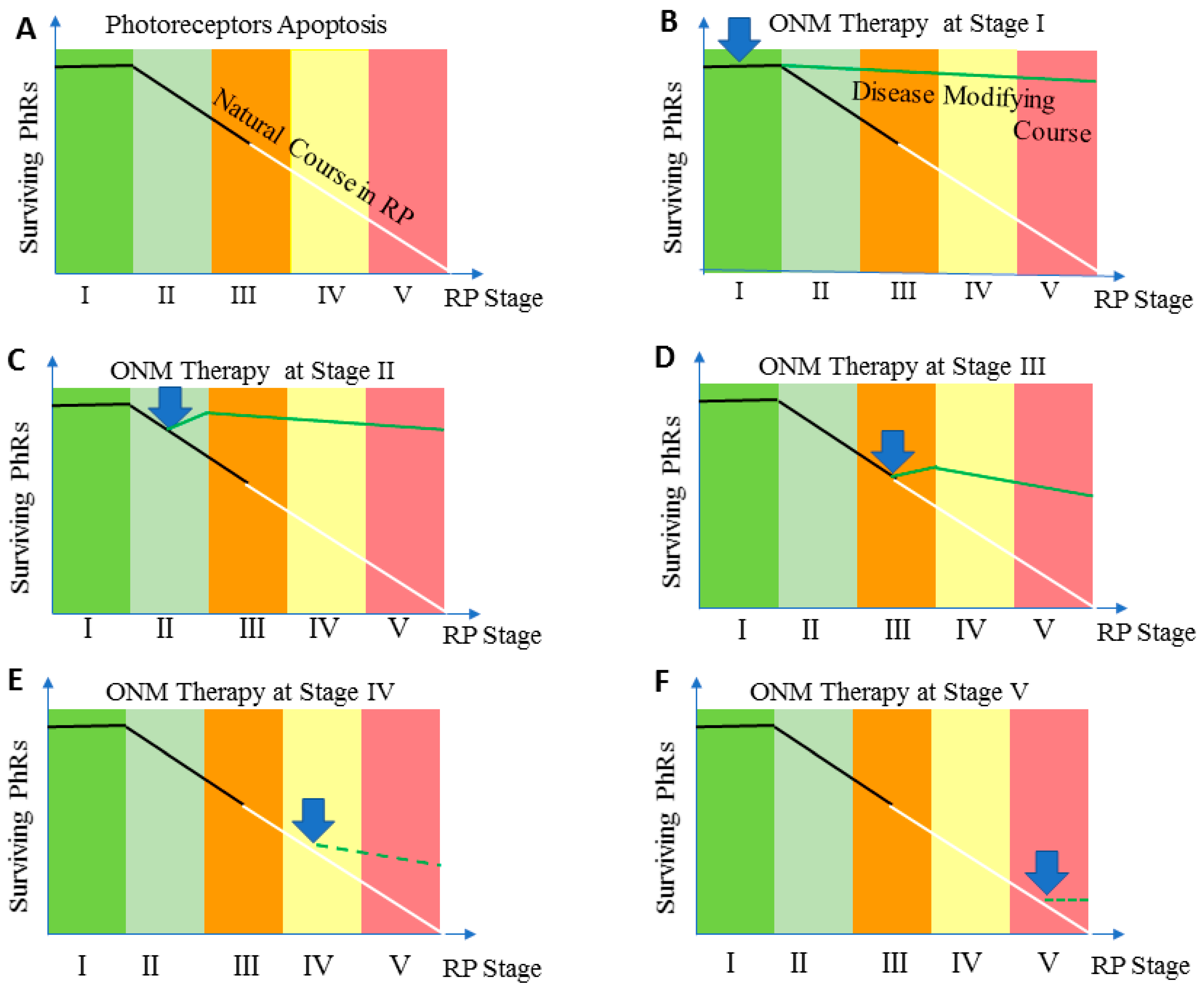

Table 1.
Staging of RP.
| Stage | Clinical Description |
|---|---|
| Stage 0 | Patients experience no symptoms related to retinitis pigmentosa. Fundus examination reveals a normal-looking retina with no pigmentary changes, no visible retinal blood vessel changes, or optic nerve pallor. Classic electroretinogram findings for retinitis pigmentosa are detected |
| Stage 1 | Patients may experience mild night vision disturbance. Fundus examination reveals a normal-looking retina with no pigmentary changes, no visible retinal blood vessel changes, or optic nerve pallor. Classic electroretinogram findings for retinitis pigmentosa are detected |
| Stage II | Mild attenuation of retinal blood vessels that extend anteriorely beyond the mid periphery of the retina but not reaching ora serrata, no or mild optic disc pallor, bone spicule pigmentary changes are limited to mid-periphery of the retina. |
| Stage III | Moderate attenuation of retinal blood vessels that extend anteriorely up to mid-periphery with mild optic nerve pallor. Pigmentary changes are located at mid-periphery and extend centrally reaching the vascular arcade. |
| Stage IV | Severe attenuation of retinal blood vessels ended with the formation of a complete vascular arcade, combined with moderate optic nerve pallor. Pigmentary changes are becoming more diffuse and extend centrally to the inside of the vascular arcade, but sparing the macula. Central retinal thickness is less than 150 µ as measured by Spectral Domain Optical Coherance Tomography |
| Stage V | Very severe attenuation or complete obliteration of retinal blood vessels that ended at a short distance forming incomplete vascular arcade (≤ 4 disc diameter) from optic nerve disc. Optic pallor is remarkable and the macula is involved in pigmentary changes. Stage V is also coined to any retina with a central retinal thickness of 100 µm or less as measured by Spectral Domain Optical Coherance Tomography |
Table 2.
Low Luminance Questionnaire-10 (LLQ-10).
| Q | Subject | Question Text |
|---|---|---|
| 1 | Night Vision | Rate how much difficulty you have seeing at night. |
| 2 | Peripheral vision | Rate how much difficulty you have in your peripheral vision at night. |
| 3 | Reading in dim light | Rate how much difficulty you have in reading menus in dimly lit restaurants or reading the newspaper/book without good lighting. |
| 4 | Depth of Perception | Rate how much difficulty you have in-depth perception at night. |
| 5 | Color Vision | Rate how much difficulty you have seeing colors at night. |
| 6 | Home life | Rate how much difficulty you have seeing furniture in dimly lit rooms. |
| 7 | Social life | Rate how much difficulty you have going out to nighttime social events such as sports events, the theater, friend’s homes, church, mosque, or restaurants? |
| 8 | Parties in dim light | Rate how much difficulty seeing in candlelight? |
| 9 | Dependency on others | Rate how often you depend on others to help you because of your vision at night or under poor lighting? |
| 10 | Psychological Stress | Rate how often you are worried or concerned that you might fall at night because of your vision? |
Scoring Instructions: Each of the 10 questionnaire items should be answered by one of the following: (1) No difficulty at all (10 points). (2) Little difficulty (7.5 points). (3) Some or moderate difficulty. (5 points). (4) A lot of difficulties (2.5 points). (5) Completely blind under these conditions (0 points). The total score on the LLQ-10 ranges from 0-100 points, with a higher score indicating better vision under low luminance. The scotopic vision difficulties are further classified into four levels of dysfunction according to the LLQ-10 score. Level 4; (0-25) which indicates absolute night blindness /Minimal scotopic vision, level 3 severe night blindness (>25-50), level 2; moderate night blindness (>50-75) and level 1 (>75-100) with almost normal scotopic vision. Rod responders were identified as those in whom the LLQ-10 score increased by ≥ 25 points at 6 months’ post-treatment.
Table 3.
Baseline characteristics and determinants of rod responders.
| Character | Total cohort |
Rod Responders |
Non-Rod-Responders | P Value |
|---|---|---|---|---|
| Participant Number | 40 (76 eyes) | 24 (60%) | 16 (40%) | |
|
Age,( Mean ±SD) Age (Median)(median; 25th,75th) Range |
28.4 ± 14.1 yrs. 24.0 yrs. (19,40) 4-55 yrs. |
23.9 ± 12.2 21.5 yrs. (16.5,32.0) 4-49 yrs. |
35.1 ± 14.3 yrs. 40.00 yrs. (21.3,47.0) 7-52 yrs. |
0.02 0.015 |
| Gender; Male/Female (males %) | 24/16 (60%) | 13/11 (54.2%) | 10/6 (62.5%) | NS |
|
Range/ Duration of night blindness (mean ±SD) (Median) |
2-46 yrs. 16.2 ± 12.3 yrs. |
2-30 yrs. 10.9 ± 6.7 yrs. 10.0 yrs |
3-46 yrs. 24.2 ± 14.6 yrs. 21.00 yrs |
0.0001 0.003 |
|
Duration of Night Blindness 0-10 10-20 >20 |
16 (100%) 14 (100%) 10 (100%) |
13(81.2%) 4 (28.6%) 1 (10%) |
3 (18.8%) 10 (71.4%) 9 (90%) |
|
|
Stage of the Disease * II, no. of patients (%) III, no. of patients/ (%) IV, no. of patients (%) V, no. of patients/ (%) |
9 (100%) 15 (100%) 11 (100%) 5 (100%) |
9 (100%) 12 (80%) 2 (18.2%) 1 (20%) |
0 (0%) 3 (20%) 9 (81.8%) 4 (80%) |
0.0001 |
|
LLQ-10 Score (mean ± SD) LLQ-10 Score (median) (median; 25th,75th) |
23.1 ± 13.0 21.3 (12.5, 34.4) |
23.6 ± 11.6 22.5 (15.0,34.4) |
22.2 ± 15.2 17.5 (12.5,34.4) |
NS NS |
|
BCVA: logMAR (mean ±SD) BCVA: logMAR (Median)(median; (median; 25th,75th) |
0.54 ± 0.35 0.50 (0.20,0.80) |
0.44 ± 0.33 0.34 (0.2,0.6) |
0.69 ± 0.33 0.8 (0.5,1.0) |
0.03 0.03 |
|
Contrast Sensitivity log unit (mean ±SD) Contrast Sensitivity (Median) log unit (median; 25th,75th) |
0.43 ± 0.48 0.18 (0,0.9) |
0.57 ± 0.50 0.7 (0,0.9) |
0.25 ± 0.38 00 (0, 0.6) |
0.074 0.056 |
| Central retinal thickness, mean ± SD (µm) (Median) (µm) ( 25th,75th) | 215.1 ± 64.4 203.0 (175.5,261.0 |
231.3 ± 59.9 224.0 (184.0,270.0) |
188.5 ± 64.6 185.5 (134.8,221.3) |
0.05 0.04 |
| Nerve Fiber Layer Thickness, (mean ± SD) (µm) (Median (µm) | 42.4 ± 11.3 41.0 (35.3,47.8) |
43.1 ± 12.7 41.0 (35.0, 48.3) |
41.2 ± 8.9 41.0 (35.3, 48.3) |
NS NS |
| Ganglion Cell Layer Thickness, mean ± SD (µm) (Median (µm) | 59.9 ± 16.8 57.0 (50,70.8) |
65.4 ± 16.2 60.0 (51.0, 77.0) |
50.2 ± 13.4 49.0 (40.5, 55.5) |
0.0001 0.002 |
Table 4.
Visual functions at various post-treatment intervals .
| Baseline | 1 month | 6 months | 12 months | 24 months | |
|---|---|---|---|---|---|
|
LLQ-10 score (Whole Cohort): (Mean ± SD) P value Median Value (median; 25th, 75th) P value |
23.1 ± 13.0 21.3 (12.5,34.4) |
55.1 ± 28.6 (p=0.0001) 55.1 (37.5,85.0) (p= 0.0001) |
52.8 ± 27.2 (p=0.0001) 52.5 (37.5,85.0) (p=0.0001) |
52.9 ± 27.4 (p=0.0001) 52.5 (30.6,82.5) (p=0.0001) |
56.5 ± 28.0 (p=0.0001) 55.5 (32.5,85.0) (p=0.001) |
|
LLQ-10 score (Rod Responders): (Mean ± SD) P value Median Value (median; 25th, 75th) P value |
(23.6 ± 11.6) 22.5 (15.0,34.4) |
(73.5 ± 16.6) (p=0.0001) 77.5 (57.5,89.4) (p=0.0001) |
(70.0 ± 16.2) (p=0.0001) 66.3 (53.8,86.9) (p= 0.0001) |
(69.7 ± 20.5) (p=0.0001) 70.0 (52.5,86.9) (p=0.001) |
(68.9 ± 23.7) (p= 0.0001) 70.0 (54.0,90.0.0) (p=0.002) |
| BCVA (Whole Cohort, RE) (Log Mar) (Mean ± SD) P value Median Value (median; 25th, 75th) P value |
0.54 ±0.35 0.50 (0.02, 0.80) |
0.33 ±0.29 (p= 0.0001) 0.26 (0.03, 0.52) (p=0.0001) |
0.36 ± 0.30 (p= 0.0001) 0.3 (0.04, 0.6) (p=0.0001) |
0.40 ±0.34 (p=0.013) 0.3 (0.16, 0.6) (p=0.006) |
0.37 ± 0.29 (p=0.03) 0.32 (0.12, 0.57) (P=0.03) |
| Contrast Sensitivity (whole cohort RE) (Mean ± SD) P value Median Value (median; 25th, 75th) P value |
(0.43 ± 0.48) 0.18 (0.0, 0.9) |
(0.71 ± 0.51) (p=0.0001) 0.75 (0.21, 1.25) (p=0.0001) |
(0.65 ± 0.53) (p= 0.0001) 0.7 (0.03, 1.25) (p=0.0001) |
(0.71 ± 0.55) (p=0.002) 0.9 (0.0, 1.25) (p=0.003) |
(0.70 ± 0.53) (p=0.02) 0.9 (0.0, 1.22) (p=0.02) |
The median value as well as the mean value ± SD (standard deviation) of different visual functions (low luminance vision, best corrected visual acuity, and contrast sensitivity) at baseline and at 1,6,12 and 24 months after treatment. LLQ-10 (low luminance questionnaire 10. RE; right eye.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



