1. Introduction
Gastric cancer (GC) occurs if uncontrolled growth of cancerous mucosal cells in the stomach lining, It which takes several years to be detectable in size.
Helicobacter pylori is a gastric bacterial pathogen associated with human GC. Sugano et al. reported that patients with
H. pylori-associated gastritis and gastric ulcers had a higher risk of GC than those with duodenal ulcers, indicating that gastric atrophy remains a risk factor after
H. pylori eradication therapy. Clinical research conducted by a Japanese medical team concluded that careful monitoring, such as endoscopic examination, is required after the successful eradication of
H. pylori in patients at higher risk [
1].
H. pylori infection is associated with GC development. The cytotoxin-associated gene A (CagA) protein of
H. pylori, which is delivered to gastric epithelial cells via bacterial type IV secretion, is an oncoprotein that induces malignant neoplasms in mammals. Genetic alterations of
H. pylori, most commonly CagA and vaculating cytotoxin (VacA), are the most common, and CagA-positive
H. pylori strains increase the risk of atrophic gastritis and GC [
2]. GC is caused by a specific genetic background and infection with CagA positive-
H. pylori. Currently, many clinical studies have been conducted to identify the genes associated with GC development.
Breast cancer susceptibility gene 1 (BRCA1) is a tumor suppressor gene located on human chromosome 17 and involved in DNA repair and cell cycle regulation. BRCA1 encodes a protein that helps repair damaged DNA. This maintains the stability of the genetic information in the cell. If an abnormality occurs during cell division, BRCA1 either suppresses cell proliferation or induces apoptosis. There have been reports of an association between BRCA1 mutations and risk of cancer development. If there is a germinal mutation in the BRCA1 gene, the risk of developing hereditary breast and ovarian cancer (HBOC) is significantly increased owing to reduced DNA repair function.
H. pylori is a spiral-shaped bacterium that inhabits the gastric lining. Even in a highly acidic stomach, H. pylori survives using an enzyme called urease, to break down urea into ammonia, which neutralizes stomach acid. There is a strong association between H. pylori and stomach cancer; H. pylori is among the main causes of gastric cancer. Approximately 50% of the global population is infected with H. pylori, and chronic infection of the gastric mucosa is closely associated with the development of atrophic gastritis and gastric ulcers. In developed countries, H. pylori infection increases the risk of GC by at least six-fold. H. pylori strains carrying a gene called CagA, cause more severe atrophic gastritis than CagA-negative H. pylori strains and are epidemiologically strongly associated with the development of gastric cancer. H. pylori infection has been suggested to be involved in the development of lymphoma derived from gastric mucosa-associated lymphoid tissue (MALT).
Momozawa et al. performed next-generation sequencing (NGS) on genes of patients with GC and healthy individuals to identify the genetic biomarkers of GC and reported significantly more pathogenic variants (PVs) in germline
BRCA1 (
gBRCA1) and/or
gBRCA2 in patients with GC than in healthy individuals. However, in the four cohorts without CagA derived from
H. pylori of
gBRCA1/2 (gBRCA1/2) wild-type (wt),
gBRCA1/2 PVs
, gBRCA1 PVs
/gBRCA2 wt
, and gBRCA1 wt
/gBRCA2 PVs
, the incidence of GC by 80 years of age was <10%. Although individuals without
gBRCA1/2 PVs are infected with CagA-positive
H. pylori, the incidence of GC is low. Therefore, clinical data do not indicate that
BRCA1/2 PVs increase the incidence of GC. A large-scale clinical study by Momozawa et al. showed that patients with
gBRCA1/2 PVs infected with Helicobacter pylori had a ≥40% incidence of GC by 80 years of age. However, healthy individuals with
gBRCA1/2 wt have a 10% incidence of GC by 80 years of age, despite
H. pylori infection [
3,
4].
2. Results
This clinical research reported that the incidence of GC in 183 HBOC families with HBOC and
gBRCA1 PVs or
gBRCA2 PVs was significantly higher than that in 189 healthy individuals with
gBRCA1/2 wt (189 families) (
Table 1). The prevalence of
H. pylori infection in patients with GC from HBOC families was similar to that in those with GC from healthy
gBRCA1/2 wt families, with an
H. pylori infection rate of approximately 90% (
Table 1). Furthermore, the incidence of GC from families with HBOC and other families was 74.57% and 53.67% in men, respectively.
A novel treatment method was examined using cancer genome panel testing in 47,211 Japanese patients with advanced-stage/metastatic GC. Overall, 2417 (97.11%) of 2489 patients with advanced stage/metastatic GC were infected with H.pylori based on cancer genome panel testing at the Cancer Genome Medicine in Japanese University. Of the 173 patients with GC from families with HBOC, 161 (93.06%) had an H. pylori infection. Of the 41 patients with GC from families without HBOC, 39 (95.12%) had H. pylori infection. The incidence of H.pylori infection was comparable between patients with GC from families with and without HBOC.
Thus, individuals who carry gBRCA1/2 PV but are not infected with
H. pylori do not have a higher incidence of GC. Compared to individuals with
gBRCA1/2 wt, those with
gBRCA1/2 PVs have a higher incidence of GC owing to
H. pylori infection [
4,
5,
6]. Therefore, taking antibiotics for
H. pylori reduce the incidence of GC, even in carriers of
gBRCA1/2 PVs.
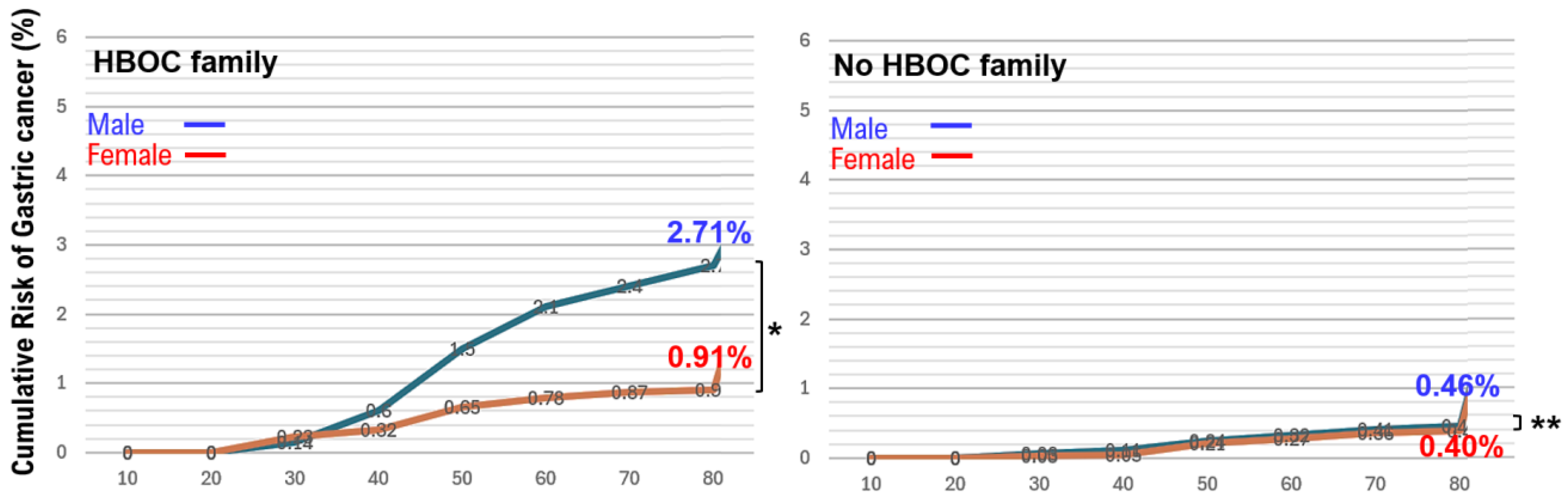
In families with HBOC, the risk of developing stomach cancer in men is higher than the risk of developing stomach cancer in women. However, in families without HBOC, the risk of developing stomach cancer in men is roughly equal to the risk of developing stomach cancer in women. Therefore, our medical staff examined the cumulative risk (%) of stomach cancer by the age of 80 in each cohort.I n families with HBOC, the cumulative risk of gastric cancer in men by their 80s is 2.71% an d in women is 0.91% (Figurre 1). In families without HBOC, the cumulative risk of gastric cancer in men by their 80s is 0.46% and in women is 0.40% (
Figure 1). The lifetime risk of developing stomach cancer is reported to be two to three times higher than the lifetime risk of developing stomach cancer in women. This is thought to be due to the fact that in HBOC families, the cumulative rate of stomach cancer in men is approximately three times higher than the cumulative rate in women.
3. Discussion
The incidence of GC increases after 50 years of age, particularly among men. However, the reason the incidence rate of GC is higher in men than in women remains unclear. The analyses conducted did not considered the individuals’ genetic backgrounds. Previously, our clinical team investigated the incidence of gastric cancer in families with HBOC. The incidence of gastric cancer is influenced by an individual's genetic background, including whether they have
gBRCA1/2 PVs, and significantly increased by
H. pylori infection. Recently,
H. pylori infection and GC are closely associated. In 1994, the World Health Organization (WHO) designated
H. pylori as a group I carcinogen (definite carcinogen), similar to tobacco[
7]. Momozawa et al. and Hayashi et al. have shown that pathogenic variants in BRCA1 or BRCA2 have a significant impact on GC development, similar to infection with CagA positive-
H. pylori. Individual genetic backgrounds, especially the homologous recombination deficiency (HRD) genes, BRCA1/2 PVs,
ATM,
BARD1,
BRCA1,
BRCA2,
BRIP1,
CHEK2,
PALB2,
RAD51C, and
RAD51D, have a significant impact on GC development caused by
H. pylori-infection [
3,
5,
8]. Kanno et al. provided a clinical explanation for the impact of BRCA1/2 PVs on the development of GC. The higher incidence of GC in men may be due to the underlying cause of hereditary GC.
Several viruses are known to cause cancers. Human papillomavirus (HPV) is considered the main cause of cervical cancer [9]. HPV is spread through sexual contact; therefore, anyone with sexual contact is at risk of HPV infection. Most individuals may be infected with HPV, but many infected individuals eliminate HPV through their own immune system. However, HPV rarely becomes chronic and can cause cervical or penile cancers. Hepatitis B (HBV) and C virus (HCV) infect the liver cells, causing chronic hepatitis and cirrhosis [10,11]. Furthermore, hepatocellular carcinoma (HCC) often develops from chronic cirrhosis caused by HBV or HCV infection. HBV is primarily transmitted through blood, whereas HCV is primarily transmitted through needles and blood products. However, no study has reported the relationship between these viral infections and HRD, including BRCA1/2 PVs, during carcinogenesis. CagA, secreted by H. pylori, binds to BRCA1/2 PVs and inhibits apoptosis of infected cells [12,13]. Virus-derived proteins bind to BRCA1/2 PVs and induce cancer. Future research will shed light on the roles of virus-derived factors and their complexes with BRCA1/2 PVs in carcinogenesis. An effective way to prevent viral infections is to administer a vaccine against the virus. However, the development of an effective vaccine is challenging.
There are some cancers in which sex differences are observed in incidence rates. The incidence of HCC is approximately twice as high in men as that in women; most common among individuals aged >80 years. The incidence of HCC begins to increase in men in their 40s and women in their 50s [14]. HCC is caused by chronic hepatitis and cirrhosis due to HBV and HCV infection; however, the incidence rate has been decreasing owing to thorough infection prevention measures and advances in antiviral therapy [15]. However, there has been an increase in the incidence of HCC associated with alcohol-related liver disease and metabolic dysfunction associated with steatotic liver disease (MASLD), which is not accompanied by viral infections [16]. This may be caused by lifestyle-related diseases, such as alcohol consumption, obesity, diabetes, hypertension, and dyslipidemia. However, the molecular biological mechanisms that explain the sex differences in liver cancer incidence remain unclear.
Through a large-scale evaluation of patients with different clinical and demographic characteristics, we identified genes associated with an increased risk of GC in families with HBOC and BRCA1/2 PVs. H. pylori infection modified the risk of GC associated with germline BRCA1/2 PVs in patients with HBOC. The study results suggest that the evaluation and eradication of H. pylori infection may be important in families with HBOC and gBRCA1/2 PVs.
4. Materials and Methods
4.1. Cancer Gene Panel Profiling
HBOC 183 families: 4847 participants, 173 patients with gastric cancer. Non-HBOC 189 families: 4755 participants, 41 patients with gastric cancer. Between December 2019 and August 2025, 47,211 novel treatments were investigated using cancer genome panel testing (FoundationOne® CDx test: n = 38,981; OncoGuideTM NCC Oncopanel test, Riken Genesis, Yokohama, Kanagawa, Japan, n = 8,230) in cancer genomic medicine conducted at Japanese national universities. We examined a novel treatment method using cancer genome panel testing in 2,489 Japanese patients with advanced-stage or metastatic GC.
4.2. Diagnostic Testing for H. pylori Infection
We used highly sensitive tests, such as urea breath and stool H. pylori antigen tests, which should be used combined with the ABC method. We stained tissue sections obtained from surgical treatments with hematoxylin and eosin (H&E) or Giemsa, and observed them under a microscope. Direct observation allows for the detection of H. pylori. Another advantage is that H. pylori infection can be diagnosed even if the bacterium is in the coccoid form (spherical bacteria), which cannot be cultured and has no urease activity.
Of the 173 patients with GC from families with HBOC, 161 (93.06%) had H. pylori infection. Of the 41 patients with GC from families without HBOC, 39 (95.12%) presented with H. pylori infection. The incidence of H. pylori infection was comparable between patients with GC from families with and without HBOC.
4.3. Ethical Considerations for Human Study
This esearch on human cancer genome information derived from the results of cancer gene panel testing was conducted at Kyoto University, its affiliated hospitals, and the National Hospital Organization Kyoto Medical Center in accordance with institutional guidelines (IRB approval nos.: 50-201504, NHOKMC-2023-2, and H31-cancer-2). This study included personal and/or medical information and the case report/case history of an identifiable individual. Therefore, the data were anonymized in accordance with the anonymization policy. All patients with advanced-stage/metastatic disease were briefed regarding the clinical study, and they agreed to participate in the current study by providing informed consent.
Ethics committee name: IRB of the National Hospital Organization Headquarters (approval code: H31-cancer-2; approval dates: November 09, 2019, and June 17, 2013).
Ethics committee name: IRB of Kyoto University (approval code: R34005; approval date: August 01, 2022).
The authors attended a research ethics education course through the Education for Research Ethics and Integrity (Association for the Promotion of Research Integrity (APRIN) e-learning program [eAPRIN]) agency. The authors’ completion numbers are AP0000151756, AP0000151757, AP0000151769, AP0000151781, and AP000351128.
4.4. Disclosure
The authors declare no potential conflicts of interest. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
4.5. Statistical Analyses
Statistical analyses included the Kolmogorov-Smirnov test, independent t-test or Wilcoxon test, Chi-square and McNemar tests, correlation analysis, logistic regression, and ROC analysis.
Author Contributions
T.H. is responsible for research design, writing manuscript. TH, and I.K. was involved in the literature search, study design, data collection, data interpretation, and I.K. reviewed the manuscript. T.H. and I.K. are responsible for final content. All authors have read and approved the final version of the manuscript.
Funding
The costs of conducting our clinical research are covered by the following research grants: Japan Society for Promoting Science for TH (no. 19K09840), START-program Japan Science and Technology Agency (JST) for TH (no. STSC20001), National Hospital Organization Multicenter Clinical Study for TH (grant no. 2019-Cancer in general-02), and Japan Agency for Medical Research and Development (AMED) (no. 22ym0126802j0001), Tokyo, Japan. These research funds were provided by Japanese government research institutes, and therefore the funders were not involved in the establishment of the clinical research program, the collection and analysis of data, the public dissemination of research findings, or the preparation of the manuscript.
Data Availability Statement
The data are available and publicly available on various websites. Details are provided in the first paragraph of the Results section. Information from this clinical study and the associated transparency statement in the medical journal article are available online.
https://kyoto.hosp.go.jp/html/guide/medicalinfo/ clinical research/expand/gan.html (accessed on 15 March 2025).
Acknowledgments
The authors thank all medical staff for clinical research at the National Hospital Organization Kyoto Medical Center. The authors declare no potential conflicts of interest. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- Sugano, K; Suzuki, C; Ota, M; Iwakiri, R. Gastric cancer risk after Helicobacter pylori eradication in gastritis and peptic ulcer: a retrospective cohort study in Japan. BMC Gastroenterol. 2025, 25, 463. [Google Scholar] [CrossRef] [PubMed]
- Hatakeyama, M. Helicobacter pylori CagA and gastric cancer: a paradigm for hit-and-run carcinogenesis. Cell Host Microbe 2014, 15, 306–316. [Google Scholar] [CrossRef] [PubMed]
- Momozawa, Y; Sasai, R; Usui, Y; Shiraishi, K; Iwasaki, Y; Taniyama, Y; Parsons, MT; Mizukami, K; Sekine, Y; Hirata, M; Kamatani, Y; Endo, M; Inai, C; Takata, S; Ito, H; Kohno, T; Matsuda, K; Nakamura, S; Sugano, K; Yoshida, T; Nakagawa, H; Matsuo, K; Murakami, Y; Spurdle, AB; Kubo, M. Expansion of Cancer Risk Profile for BRCA1 and BRCA2 Pathogenic Variants. JAMA Oncol. 2022, 8, 871–878. [Google Scholar] [CrossRef]
- Usui, Y; Taniyama, Y; Endo, M; Koyanagi, YN; Kasugai, Y; Oze, I; Ito, H; Imoto, I; Tanaka, T; Tajika, M; Niwa, Y; Iwasaki, Y; Aoi, T; Hakozaki, N; Takata, S; Suzuki, K; Terao, C; Hatakeyama, M; Hirata, M; Sugano, K; Yoshida, T; Kamatani, Y; Nakagawa, H; Matsuda, K; Murakami, Y; Spurdle, AB; Matsuo, K; Momozawa, Y. Helicobacter pylori, Homologous-Recombination Genes, and Gastric Cancer. N Engl J Med. 2023, 388, 1181–1190. [Google Scholar] [CrossRef]
- Hayashi, T; Sano, K; Okada, M; Ura, T; Konishi, I. Hereditary Gastric Cancer Is Linked With Hereditary Breast and Ovarian Cancer. World J Oncol. 2024, 15, 722–730. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, T; Sano, K; Okada, M; Ura, T; Konishi, I. Efficacy and Tolerability of Olaparib Plus Paclitaxel in Patients with Gastric Cancer Associated with Hereditary Breast and Ovarian Cancer. Curr Oncol. 2024, 31, 6723–6734. [Google Scholar] [CrossRef] [PubMed]
- De Luca, A; Iaquinto, G. Helicobacter pylori and gastric diseases: a dangerous association. Cancer Lett. 2004, 213, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Pilie, PG; Tang, C; Mills, GB; Yap, TA. State-of-the-art strategies for targeting the DNA damage response in cancer. Nat Rev Clin Oncol 2019, 16, 81–104. [Google Scholar] [CrossRef] [PubMed]
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).