1. Introduction
Cancer-related cognitive impairment (CRCI) represents a prevalent, troublesome, and debilitating side-effect among cancer survivors [
1,
2,
3]. These cognitive difficulties include mental cloudiness, reduced cognitive abilities, and slower reaction times [
4], affecting domains such as memory, attention, processing speed, and executive functions [
5,
6]. CRCI can manifest at any stage from pre-treatment through post-treatment [
7,
8,
9], with severity ranging from mild to severe [
10]. Although often transient [
11], some individuals experience lasting impairment persisting up to 20 years post-treatment [
12]. Prevalence estimates range from 44.2% to 75% [
7,
9,
13,
14], significantly affecting psychosocial well-being [
15,
16], daily functioning, interpersonal relationships, employment, and social participation [
1,
3,
16,
17,
18].
These findings raise the importance of developing interventions targeting long-term cognitive issues in cancer survivors [
19]. Consistent with this, the World Health Organization (WHO) Package for Rehabilitation from Cancer identifies cognitive functioning as a key rehabilitation area for cancer survivors [
20]. Among non-pharmacological approaches—including cognitive training and rehabilitation, exercise/physical activity, mind-body interventions, and multimodal programs [
8,
21,
22,
23,
24,
25]—cognitive rehabilitation has emerged as particularly effective [
21,
25,
26,
27,
28], and is endorsed as a first-line intervention by international [
29] and European guidelines [
14,
26,
30].
Cognitive rehabilitation integrates “skills training” (cognitive training) and/or “strategy training” (psychoeducation and/or cognitive behavioral therapy for CRCI) [
26,
31,
32]. Administered individually or in a group format across multiple sessions [
8,
33], either in-person or remotely (synchronously or asynchronously) [
26,
31,
33], evidence indicates that cognitive rehabilitation reduces cognitive complaints, improves objective cognitive abilities (mainly memory, executive functions, and processing speed), enhances quality of life, and addresses related symptoms such as mood and fatigue [
31,
33]. Effects are maintained for months post-intervention [
31,
33]. Despite high satisfaction and feasibility [
27,
31], implementation faces challenges, notably high attrition rates (3-42%) driven by intervention length and time commitment [
33,
34]. These challenges raise critical questions regarding the feasibility and sustainability of integrating cognitive rehabilitation into routine cancer survivorship care [
19].
Although empirical evidence shows cognitive rehabilitation’s efficacy [
27], it has not yet been adopted for Portuguese cancer survivors [
35]. To ensure successful implementation and encourage treatment adherence, it is essential to examine whether individuals are willing to accept and use this treatment [
36,
37,
38]. According to Sekhon et al.’s [
37] Theoretical Framework of Acceptability (TFA), acceptability reflects “the extent to which people delivering or receiving a healthcare intervention consider it to be appropriate, based on anticipated or experienced cognitive and emotional responses to the intervention” (p.8) across seven domains: affective attitude, burden, perceived effectiveness, ethicality, intervention coherence, opportunity costs, and self-efficacy. Critically, this framework can be used to assess acceptability either prospectively (before engaging with the intervention), concurrently (during the intervention), or retrospectively (after the intervention). This differentiation is crucial, as prospective acceptability influences initial engagement, whereas retrospective acceptability impacts sustained participation [
37,
39].
Assessing patient acceptability is especially important, since interventions that are considered acceptable tend to result in higher treatment adherence and improved clinical outcomes [
37,
40]. Nevertheless, this construct has rarely been systematically examined within cognitive rehabilitation for CRCI, with previous studies reporting satisfaction and feasibility metrics following participation in interventions [
31] but limited information on its prospective acceptability [
19]. Understanding the factors that may influence the acceptability of cognitive rehabilitation interventions in cancer, such as sociodemographic and clinical characteristics, knowledge, and psychological capabilities, is crucial. This helps identify cancer survivors who may be less receptive to these treatments and informs strategies to enhance their acceptance and adapt interventions to individual and social contexts [
41,
42,
43]. Therefore, in this study carried out with Portuguese cancer survivors, we aimed to: (1) develop and evaluate the psychometric properties (construct validity and reliability) of the Acceptability of Cognitive Rehabilitation Interventions Survey - Cancer Survivors (ACRIS-CS) based on the TFA; (2) examine prospective acceptability of cognitive rehabilitation in this population; and (3) identify key factors influencing prospective acceptability. This study will provide a theoretically based instrument to assess the acceptability of cognitive rehabilitation interventions among cancer survivors and will contribute to improving our knowledge of prospective acceptability, helping to outline strategies to increase cancer survivors’ adherence to these interventions.
2. Materials and Methods
2.1. Study Design, Participants, and Recruitment
This study employed a cross-sectional, observational design with a convenience sample as part of a broader project conducted in Portugal. The CanCOG® - Cognitive Rehabilitation in Cancer project aims to develop a cognitive rehabilitation program for non-central nervous system (non-CNS) cancer survivors and was approved by the Ethics and Deontology Committee of the University of Aveiro (approval numbers: 30-CED/2019/ January 22, 2020, and 30-CED/2021/ October 6, 2021).
Individuals were eligible if they were: (1) Portuguese adults aged 18-65 years; (2) self-identified as non-CNS cancer survivors (defined as any individual diagnosed with cancer, from diagnosis through the remainder of life, including those in active treatment [
44,
45]); (3) undergoing or having received cancer treatment; and (4) reporting cognitive complaints. A screening question (“Have you been experiencing any cognitive difficulties since being diagnosed with and treated for cancer [e.g., difficulties with memory, attention, concentration, reasoning, decision-making, or planning]?”) requiring a Yes/No response confirmed eligibility for self-reported cognitive complaints [
19,
46,
47]. Only individuals responding “Yes” could participate. Exclusion criteria included: (1) psychiatric or communication disorders or other severe medical conditions (assessed via self-report); (2) brain or CNS metastasis; (3) diagnosed brain injury or neurological disease (e.g., stroke, head injury, epilepsy, dementia, Parkinson’s disease, multiple sclerosis), or (4) substance or alcohol abuse, as these could impact cognitive functioning [
19].
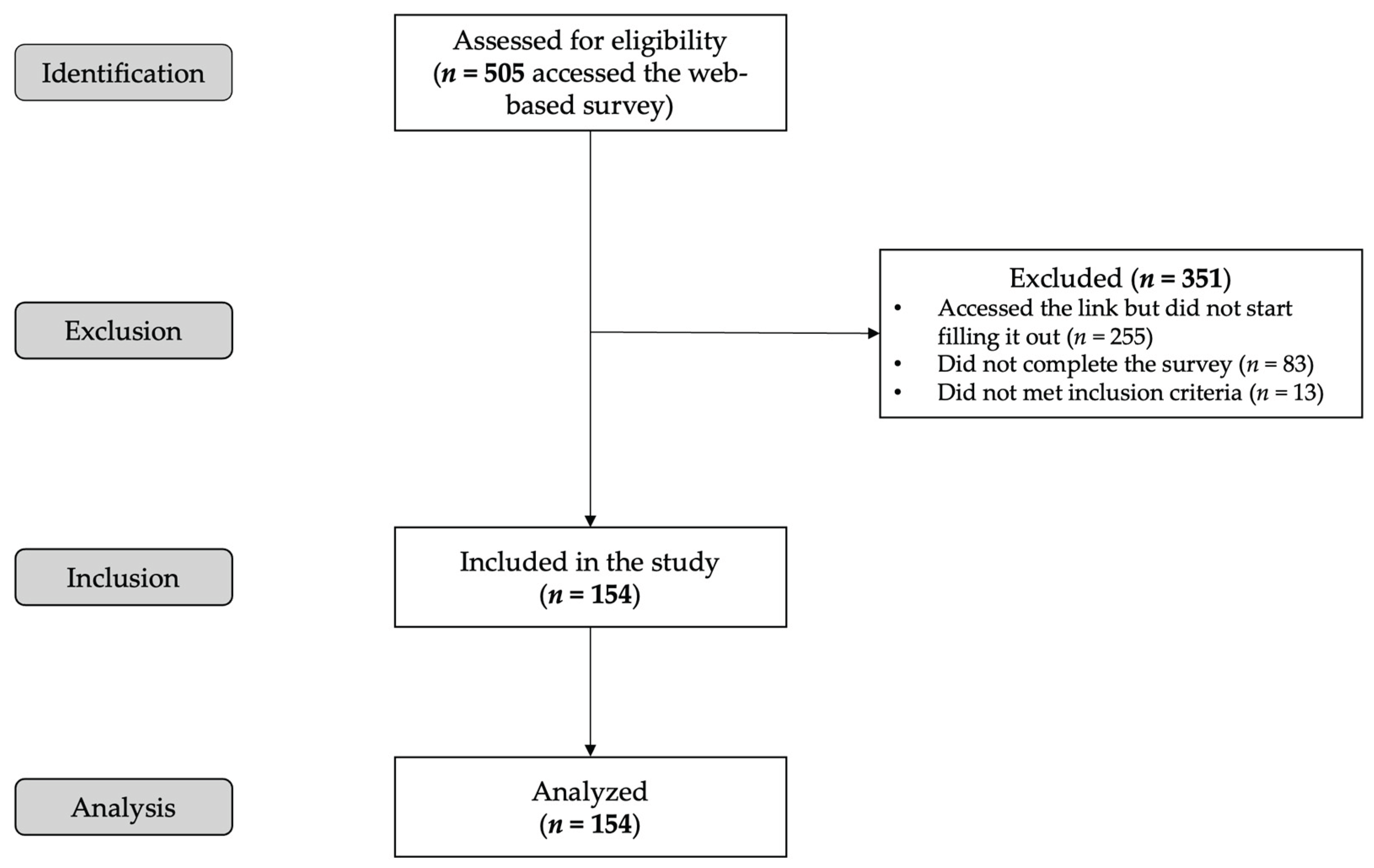
Participants were recruited between September 2022 and April 2023 through: (1) social media advertisements targeting Portuguese adult cancer survivors, shared in support groups and cancer association pages; (2) collaboration with national cancer associations disseminating study information via email; (3) article about the study published on a research center webpage; and (4) direct email to non-CNS cancer survivors from previous research studies who consented to future contact. Snowball sampling encouraged participants to share information.
Figure 1 presents the participant flowchart following STROBE guidelines.
The study was conducted in accordance with the Declaration of Helsinki [
48] and ethical guidelines of the American Psychological Association [
49] and Portuguese Psychologists Association [
50]. Participants were informed that participation was voluntary, that data would remain confidential, and that they could withdraw at any time without consequences. No incentives were offered. Survivors provided informed consent electronically by selecting “Yes” to “Do you accept to participate in this study?” after all information about the study had been provided.
2.2. Measures
Data were collected via a web-based self-completion survey, programmed in LimeSurvey
® [
51] for cross-browser compatibility and hosted on a secure server at the University of Aveiro, Portugal.
2.2.1. Sociodemographic and Clinical Characteristics
Participants’ sociodemographic (age, sex, marital status, education, employment status) and clinical characteristics (cancer type, cancer stage, time since diagnosis, current treatment status, treatment modalities received, psychological support history, and psychotropic medication use) were collected. See
Table 1 for detailed operational definitions.
2.2.2. Anxiety and Depressive Symptoms
The Hospital Anxiety and Depression Scale (HADS) was used to assess anxiety and depressive symptoms [
52,
53]. This self-report scale consists of 14 items divided into two subscales: anxiety (7 items) and depression (7 items). Items are rated on 4-point Likert scales (0–3), with subscale scores ranging from 0 to 21 (higher scores indicate more severe symptoms). The Portuguese validation study showed good psychometric properties [
52]. In the present study, Cronbach’s alpha was acceptable for both subscales, with a value of 0.83 for anxiety and 0.81 for depression.
2.2.3. Cognitive Symptoms
The Perceived Cognitive Impairment (CogPCI) subscale of the Portuguese version of the Functional Assessment of Cancer Therapy-Cognitive Function-Version 3 (FACT-Cog-v3) [
13,
54,
55] was used to assess perceived cognitive functioning. It consists of 20 items rated on a 5-point Likert scale (“0 = Never” to “4 = Several times a day”) with a score range of 0–80. Higher scores indicate better perceived cognitive functioning. The Portuguese validation studies demonstrated strong psychometric properties [
13,
55]. In the present study, Cronbach’s alpha was 0.95.
2.2.4. Knowledge of CRCI
Awareness of the existence of CRCI was assessed using a single item adapted from Schagen et al. [
56,
57]: “How familiar are you with the idea and/or aware that cognitive difficulties can be a secondary symptom of cancer and/or cancer treatments?”, rated on a 5-point Likert scale (“0 = No, not at all [familiar]” to “4 = Totally [familiar]”).
2.2.5. Acceptability of Cognitive Rehabilitation: ACRIS-CS
The ACRIS-CS was developed following established procedures for scale construction and validation in health and behavioral research [
58,
59]. Item development was grounded in Sekhon et al.’s [
37,
39] TFA literature review and adapted from previous instruments [
60,
61]. Eleven items were phrased in a prospective (i.e., forward-looking) manner, assessing participants’ perceptions before intervention delivery. Items operationalized all seven TFA component constructs: (1) Affective attitude (three items; how individuals feel about the intervention); (2) Burden (two items; the perceived amount of effort required to participate in the intervention); (3) Perceived effectiveness (one item; the extent to which the intervention is perceived as likely to achieve its purpose); (4) Ethicality (one item; the extent to which the intervention aligns with an individual’s value system); (5) Intervention coherence (one item; extent to which the participant understands the intervention and how it works); (6) Opportunity costs (two items; the extent to which participants perceive the need to give up benefits, profits, or values to engage in the intervention); and (7) Self-efficacy (one item; the participants’ confidence in their ability to perform the required behavior(s) to participate in the intervention). To ensure common understanding, cognitive rehabilitation programs were described at the beginning of the instructions.
Appendix A includes the full scale, both the original European Portuguese version and an English translation version (please note that the English version is a free translation to allow all readers to be familiar with the instrument, but it has not been validated). Participants responded using a 5-point Likert scale, with scores ranging from “1 = Strongly disagree” to “5 = Strongly agree.” Higher scores indicated greater acceptability (more positive perceptions) of cognitive rehabilitation interventions. Negatively worded items were reverse-scored for consistency. The content validity of the scale was evaluated by four clinicians and researchers with expertise in CRCI and cognitive rehabilitation.
2.3. Data Analysis
Statistical analyses were performed with the Statistical Package for the Social Sciences (IBM SPSS, version 30.0.0; IBM SPSS, Inc., Chicago, IL), considering a significance level of p < 0.05.
Descriptive statistics, i.e., absolute/relative frequencies or central tendency/dispersion measures as appropriate, were first calculated for the sample’s sociodemographic and clinical characteristics.
Construct validity was determined by factorial validity. Sample size for assessing ACRIS-CS structural validity followed COSMIN guidelines [
62], which recommend a ratio of seven participants per variable. With 11 items, the minimum sample size would be 77 (7 × 11 items = 77). An exploratory factor analysis (EFA) using principal component analysis (PCA) and an oblique (promax) rotation was conducted to assess ACRIS-CS latent factors and determine its structural (construct) validity. The Kaiser-Meyer-Olkin (KMO) test [
63] and the Bartlett test of sphericity [
64] were used to evaluate sampling adequacy (KMO > 0.5) and the appropriateness of the extracted factors (
p < 0.05), respectively. Factor loadings and communalities > 0.40 were considered adequate [
65]. To determine the number of factors to retain, the Kaiser’s criterion (eigenvalues > 1) [
66] and Cattell’s scree plot (examining a scree plot for breaks) [
67] were employed. To simplify interpretation and obtain a continuous indicator of acceptability for cognitive rehabilitation, Likert summated scales were calculated for each EFA-identified factor and for the ACRIS-CS total score. Since the factors contained different numbers of items, the sum-scales were standardized to a 0-100 range [
68], with higher scores indicating greater acceptability.
Reliability, through internal consistency, was assessed using Cronbach’s alpha (acceptable if > 0.70 and high if > 0.90) [
69].
Acceptability examination employed descriptive statistics, correlations, and regression analysis. Medians and interquartile ranges (IQR) were reported for Likert-scale data following best practices for ordinal data [
70], with means and standard deviations (
SD) provided for standardized scale scores. Pearson correlations assessed the association between acceptability and continuous variables (age, survival time, perceived cognitive impairment, anxiety, and depression). Point-biserial correlations examined dichotomous variables (sex, education level, treatment status, psychological counselling history, psychotropic medication use, knowledge of CRCI). According to Cohen [
71], correlation coefficients between 0.10 and 0.29 were considered weak, those between 0.30 and 0.49 moderate, and those between 0.50 and 1.0 strong. A multiple linear regression analysis examined predictors of acceptability based on the preliminary correlations. Only the variables that were significantly (
p < 0.05) associated with the ACRIS-CS total score were included in the regression model. The backward method was used for this purpose, due to the exploratory nature of the study. Categorical variables with more than two categories were transformed into dummy variables. Regression assumptions (independence of residuals, normality, linearity, multicollinearity, and homoscedasticity) were examined and met.
3. Results
3.1. Sample Characteristics
A sample of 154 participants was included (see
Figure 1 for enrollment flowchart).
Table 1 presents sociodemographic and clinical characteristics. The mean age was 47.28 years (
SD = 8.96, range = 18-65). The sample was predominantly female (94.8%,
n = 146), married or in a de facto relationship (70.1%,
n = 108), university educated (63.8%,
n = 97), and employed (61.6%,
n = 93). Breast cancer was the most common diagnosis (72.7%,
n = 112), 48.1% (
n = 74) had localized cancer, and the average length of survival was 5.70 years (
SD = 6.16, range = 1-48 years). More than half had completed treatment (50.6%,
n = 78). Approximately 59.1% (
n = 91) received psychological/psychiatric support, and 45.5% (
n = 70) used psychotropic medications. Psychological distress, as assessed by the HADS, revealed a mean score of 10.01 (
SD = 4.24) for anxiety symptoms and of 6.86 (
SD = 4.04) for depression. Finally, participants had a mean score of 37.76 (
SD = 16.83) on the CogPCI FACT-Cog-v3 subscale for perceived cognitive impairment, and a substantial proportion (40.2%,
n = 62) reported no or only slight knowledge of CRCI.
3.2. ACRIS-CS Item Descriptives
Table 2 presents ACRIS-CS item frequencies, medians, and IQR. Items with highest agreement (“Agree” and “Totally agree” combined) were “Participation in a cognitive rehabilitation program would be helpful to address my cognitive difficulties” (item 3; 88.3%), “I feel that participation in a cognitive rehabilitation program would be positive for me” (item 1; 86.3%), and “I recognize that participation in cognitive rehabilitation programs would improve my cognitive functions” (item 2; 82.5%). Items with highest disagreement (“Disagree” and “Totally disagree” responses combined) included “Participating in a cognitive rehabilitation program would require a lot of time and energy from me” (item 11; 35.1%), “I feel that participating in a cognitive rehabilitation program would compromise my daily routine” (item 5; 30.5%), and “I would easily integrate cognitive training exercises into my daily routine between sessions of a cognitive rehabilitation program” (item 4; 14.9%).
3.3. Psychometric Properties of ACRIS-CS
3.3.1. Item Properties
No missing data occurred as the online survey required respondents to answer all items.
Table 2 shows that most items’ medians approximated 3. As shown in
Table 3, skewness and kurtosis values ranged from -2 to 2, indicating a normal distribution [
72]. All items demonstrated relatively large and positive corrected item–total correlations (r ≈ 0.30; range: 0.255-0.704). Minimal reliability variation occurred when individual items were excluded. Inter-item correlations mostly exceeded 0.30 (ranging from 0.004 to 0.867). Item 9 (ethicality) showed the lowest correlations with other items.
3.3.2. Structural Validity: Exploratory Factor Analysis
The sample met the recommended 7:1 ratio for EFA (154 participants:11 items = 14:1 [
62]
. PCA with oblique (promax) rotation yielded KMO = 0.847 (excellent sampling adequacy) and a significant Bartlett’s test (ꭕ² (55) = 864.431,
p < 0.001), confirming correlation matrix structure.
The EFA identified three factors with eigenvalues > 1, as confirmed by the scree plot (
Table 4). All items demonstrated factor loadings > 0.40, indicating strong factor relevance. Although item 10 exhibited cross-loading on two factors, its inclusion was guided by conceptual justification. Collectively, the three factors accounted for 68.70% of the total variance, with Factor 1 accounting for 44.17%, Factor 2 for 15.06%, and Factor 3 for 9.47%
. Following the TFA conceptual framework, item content, and recommendations of Timm et al. [
58], these factors were labeled as (1) Affective attitude and effectiveness (6 items on how the participants felt about the intervention and the extent to which the intervention was perceived as likely to achieve its purpose); (2) Perceived benefits and self-efficacy (3 items describing the extent to which the participants understood the potential benefits of the intervention and the confidence level to perform the actions required to participate in the intervention); and (3) Perceived burden (2 items on the perceived amount of effort that was required to participate in the intervention).
3.3.3. Reliability: Internal Consistency
The ACRIS-CS demonstrated acceptable internal consistency for the total scale (Cronbach’s α = 0.84) and for subscales: Factor 1 (α = 0.85), Factor 2 (α = 0.73), and Factor 3 (α = 0.75) (
Table 4).
3.4. Acceptability of Cognitive Rehabilitation
Table 5 presents descriptive statistics for ACRIS-CS total and subscale scores. Cancer survivors demonstrated high prospective acceptability, with an overall
mean of 67.36 (
SD = 12.10, range = 34-100). Notably, 21.4% (
n = 33/154) exceeded a score of 75 (Q3), indicating very high acceptability. When examining the three identified factors (as detailed in
Table 5), the acceptability subscale related to affective attitude and perceived effectiveness of interventions (Factor 1) achieved the highest mean score of 75.43 (
SD = 13.41, range = 42-100). Factor 2, associated with perceived benefits and self-efficacy, had a mean score of 63.20 (
SD = 16.10, range = 17-100), and Factor 3, focused on perceived burden, yielded a mean score of 49.35 (
SD = 20.75, range = 0-100).
3.5. Factors that Influence the Acceptability of Cognitive Rehabilitation
Table 6 presents the correlation coefficients for the relationships between sociodemographic, clinical, psychological, and cognitive variables and the ACRIS-CS total score. Preliminary correlations identified significant, weak-to-moderate associations with treatment status (
r = -0.259,
p = 0.001) and knowledge of CRCI (
r = 0.251,
p = 0.002). No statistically significant associations were observed for age, sex, education level, survival time, psychological counseling history, psychotropic medication use, perceived cognitive impairment, and psychological distress.
Based on the correlation results, the regression model included treatment status and knowledge of CRCI.
Table 7 shows the multiple regression model predicting acceptability. Treatment status (
β = -0.248,
p = 0.001) and knowledge of CRCI (
β = 0.240,
p = 0.002) emerged as significant predictors, jointly explaining 11.3% of variance (R
2 adjusted = 0.113,
F(2, 151) = 10.736,
p < 0.001). Survivors in active treatment showed higher acceptability (B = -2.636, 95% CI [-4.234, -1.039]) than those who completed treatment, as well as survivors who were familiar with CRCI (B = 2.598, 95% CI [0.970, 4.227]) compared to those who were not.
4. Discussion
This study developed and validated the ACRIS-CS, examined the prospective acceptability of cognitive rehabilitation among cancer survivors, and identified factors influencing acceptability. The results demonstrate that the ACRIS-CS has strong psychometric properties—including construct validity and reliability—and reveal high prospective acceptability for cognitive rehabilitation in this population.
The EFA yielded a three-factor structure, explaining 68.70% of the total variance, with good factor loadings (most > 0.70), indicating strong structural validity [
73]. The consolidation of TFA’s seven conceptual domains into three empirical factors warrants theoretical consideration. In healthcare acceptability research, similar factor-structure simplifications have been observed [
58], suggesting that, while TFA’s seven domains provide comprehensive theoretical coverage, they may operate as higher-order constructs in practice. Specifically, affective attitude merged with perceived effectiveness (Factor 1), suggesting survivors experience an integrated positive valence toward cognitive rehabilitation—their emotional responses and effectiveness beliefs are psychologically unified rather than distinct. The grouping of intervention coherence, ethicality, and opportunity costs with perceived benefits and self-efficacy (Factor 2) suggests these domains function as a unified “understanding and confidence” dimension. When survivors understand what cognitive rehabilitation involves (coherence), view it as ethically appropriate, and perceive limited opportunity costs, they simultaneously experience greater confidence in participating and recognizing potential benefits. Perceived burden emerged as an independent factor (Factor 3), highlighting its conceptual and empirical distinctiveness. Survivors can simultaneously hold positive attitudes, believe in effectiveness, feel confident, and yet perceive participation as burdensome—these dimensions operate independently. This finding aligns with implementation science frameworks that emphasize that multiple barriers can coexist with positive intentions and underscores why high acceptability does not guarantee uptake or retention without addressing practical obstacles [
36]. The ACRIS-CS achieved acceptable internal consistency (α = 0.85), with subscale alphas ranging from 0.73 to 0.85, comparable to similar acceptability instruments [
58].
Cancer survivors demonstrated high prospective acceptability (mean = 67.36), with 21.4% exceeding a score of 75, indicating strong receptivity to cognitive rehabilitation. These findings align with previous research showing that survivors recognize cognitive difficulties and express openness to interventions [
19,
27,
31]. However, examination of individual factors revealed an important discrepancy: while affective attitude and perceived effectiveness scores were high (mean = 75.43), perceived burden ratings were also moderate (mean = 49.35). This pattern highlights a critical implementation challenge: survivors value cognitive rehabilitation and believe in its benefits, yet practical barriers may impede sustained participation. This finding is consistent with high attrition rates (3-42%) documented in cognitive rehabilitation trials [
34]. It emphasizes the importance of addressing perceived practical obstacles through intervention design modifications, such as flexible delivery formats (e.g., telehealth), shorter sessions, and asynchronous components [
26,
31]. Recent evidence supports the feasibility and effectiveness of remote cognitive rehabilitation [
74,
75,
76], suggesting that technology-enabled delivery may simultaneously maintain clinical benefits while reducing the burden.
The regression analysis identified two significant predictors jointly explaining 11.3% of acceptability variance: being in active cancer treatment and having knowledge of CRCI. Survivors currently undergoing treatment demonstrated higher acceptability compared to those who completed treatment. This finding challenges the conventional assumption that cognitive rehabilitation is best delivered after treatment. It may instead reflect two factors: heightened symptom salience—cognitive difficulties often become more noticeable during active treatment, increasing perceived need and intervention relevance—and greater healthcare engagement during this phase, as frequent clinical contact facilitates the introduction of interventions and normalizes additional supportive services [
8,
77]. The finding that being aware of CRCI predicts acceptability underscores the critical role of patient education. Healthcare providers should proactively educate patients about the cognitive effects of cancer and treatments, validating these symptoms and facilitating early identification and intervention. Integration of CRCI information into survivorship care plans, as recommended by international guidelines [
29,
30], could enhance awareness and uptake. Importantly, several variables did not predict acceptability, including age, education, perceived cognitive impairment, and psychological distress. The modest variance explained (11.3%) indicates that other unmeasured factors—such as social support, financial constraints, geographic accessibility, and prior rehabilitation experiences—are likely to contribute to acceptability.
4.1. Limitations
Several limitations warrant consideration. The reliance on a cross-sectional design prevents drawing causal inferences regarding the relationships between predictors and acceptability. The sample, while providing valuable insights, was non-probabilistic, self-selected, and primarily composed of highly educated, female, breast cancer survivors recruited online, which limits generalizability to the broader cancer survivor population. Future studies should validate the ACRIS-CS in independent samples, include more diverse participants, and employ longitudinal designs to better understand this phenomenon. Furthermore, the reliance on self-reported data may be subject to bias. This study assessed only prospective acceptability; the TFA distinguishes between prospective (anticipated) and retrospective (experienced) acceptability [
37,
39], and both forms should be examined to understand complete engagement trajectories. Finally, the modest variance explained suggests that qualitative research exploring survivors’ lived experiences could identify additional factors to enhance explanatory models of acceptability.
4.2. Implications and Future Research
This study has significant implications for clinical practice, policymakers, and future research directions. An essential contribution of this study is the development and validation of the ACRIS-CS, a new theoretically grounded instrument specifically designed to measure the acceptability of cognitive rehabilitation interventions among cancer survivors. The ACRIS-CS demonstrated strong psychometric properties, making it a reliable and valid tool for future research in this field. Its inclusion in this study provided a detailed understanding of the factors that influence acceptability, and the instrument can easily be used by other researchers and clinicians interested in assessing the potential adoption of cognitive rehabilitation programs.
Nevertheless, future research should prioritize validation across diverse, independent samples. Future studies should also provide evidence of prior experience with cognitive rehabilitation programs, explore barriers and facilitators to their adoption, and examine preferences regarding program characteristics. Together, these findings will contribute to a broader picture of cognitive rehabilitation implementation among cancer survivors.
5. Conclusions
The ACRIS-CS is a valid and reliable instrument for assessing the prospective acceptability of cognitive rehabilitation among cancer survivors. Consistent with clinical guidelines that recommend cognitive rehabilitation as a first-line intervention for CRCI, this measure supports its integration into survivorship care pathways by identifying survivors who may be less receptive to these interventions before treatment delivery. By systematically assessing perceived benefits, burden, and self-efficacy, the ACRIS-CS may inform stepped, personalized approaches, including targeted psychoeducation and preparatory support, to enhance adherence and improve clinical outcomes of cognitive rehabilitation in routine oncology care.
Author Contributions
Conceptualization, A.F.O., A.B., L.L., H.S., A.T. and I.M.S.; methodology, A.F.O., A.B., L.L., H.S., A.T. and I.M.S.; formal analysis, A.F.O. and A.B.; investigation, A.F.O., A.B. and L.L.; data curation, A.F.O. and A.B.; writing—original draft preparation, A.F.O. and A.B.; writing—review and editing, A.F.O., A.B., L.L., H.S., A.T. and I.M.S.; supervision, A.T. and I.M.S.; project administration, A.F.O., A.T. and I.M.S.; funding acquisition, A.F.O., A.T. and I.M.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by national funds through FCT - Fundação para a Ciência e a Tecnologia, I.P., within RISE-Health R&D Unit (UID/06397/2025) and the William James Center for Research R&D Unit (UID/04810/2025). The first author was awarded a PhD fellowship (SFRH/BD/138785/2018 and COVID/BD/152948/2023).
Institutional Review Board Statement
Statement: The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics and Deontology Committee of the University of Aveiro, Portugal (approval numbers: 30-CED/2019/ January 22, 2020, and 30-CED/2021/ October 6, 2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding authors upon reasonable request.
Acknowledgments
The authors extend their sincere gratitude to the cancer survivors who generously participated in this study, contributing their time and valuable insights. The authors also express their appreciation to the collaborating institutions that facilitated the recruitment process. Furthermore, special thanks are extended to Diâner Felipe Queiroz, Natasha Powidayko, João Queiroz, Joana Costa, and Mariana Ramalhete for their invaluable assistance in preparing the study protocol. Additionally, the authors acknowledge Dr. Wendy Jacobs for providing valuable information regarding pre-existing knowledge about CRCI.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| ACRIS-CS |
Acceptability of Cognitive Rehabilitation Interventions Survey for Cancer Survivors |
| CNS |
Central nervous system |
| CogPCI FACT-Cog-v3 |
Perceived Cognitive Impairment subscale of the Functional Assessment of Cancer Therapy-Cognitive Function-Version 3 |
| CRCI |
Cancer-related cognitive impairment |
| EFA |
Exploratory factor analysis |
| HADS |
Hospital Anxiety and Depression Scale |
| IQR |
Interquartile ranges |
| KMO |
Kaiser-Meyer-Olkin |
| PCA |
Principal component analysis |
| SD |
Standard deviation |
| TFA |
Theoretical Framework of Acceptability |
| WHO |
World Health Organization |
Appendix A
Appendix A.1. European Portuguese Version of the ACRIS-CS
Questionário de Aceitabilidade face às Intervenções de Reabilitação Cognitiva – Sobreviventes de Cancro (ACRIS-CS)
Este questionário avalia a aceitabilidade de intervenções de reabilitação cognitiva entre sobreviventes de cancro. Antes de preencher este questionário, por favor, leia a seguinte descrição dos programas de reabilitação cognitiva:
“A reabilitação cognitiva é uma abordagem em que um profissional de saúde qualificado ajuda os pacientes a desenvolver estratégias compensatórias para gerir dificuldades cognitivas específicas (tais como usar agendas, planificadores ou sistemas de lembretes e aprender técnicas para minimizar distrações). O profissional também fornece informação útil sobre o funcionamento do cérebro, os défices cognitivos e suas consequências na vida diária (psicoeducação). Adicionalmente, a reabilitação cognitiva pode oferecer treino cognitivo (“treino mental”), que envolve exercícios repetidos concebidos para melhorar capacidades cognitivas, tais como a atenção, a memória, a velocidade de processamento e as funções executivas. Estes exercícios são praticados tanto durante as sessões com o profissional como em casa entre sessões.
Os programas de reabilitação cognitiva podem ser realizados individualmente ou em grupo, presencialmente ou remotamente (por meio de videoconferência ou de plataformas online). Os programas abrangem, tipicamente, múltiplas sessões ao longo de várias semanas.”
Com base nesta descrição, por favor, indique o seu nível de concordância (se Discorda Totalmente, Discorda, está Neutro(a), Concorda ou Concorda Totalmente) com cada uma das seguintes afirmações sobre programas de reabilitação cognitiva que podem ou não refletir as suas expectativas ou opiniões.
“Perante dificuldades cognitivas relacionadas com o cancro/tratamentos…”
| |
|
Discordo fortemente |
Discordo |
Neutro(a) |
Concordo |
Concordo fortemente |
| 1 |
Sinto que a participação num programa de reabilitação cognitiva seria positiva para mim |
|
|
|
|
|
| 2 |
Reconheço que a participação em programas de reabilitação cognitiva iria melhorar as minhas funções cognitivas |
|
|
|
|
|
| 3 |
A participação num programa de reabilitação cognitiva seria útil para lidar com as minhas dificuldades cognitivas |
|
|
|
|
|
| 4 |
Teria facilidade em integrar na minha rotina diária a realização de exercícios de treino cognitivo entre as sessões de um programa de reabilitação cognitiva |
|
|
|
|
|
| 5 |
Sinto que a participação num programa de reabilitação cognitiva iria comprometer a minha rotina diária |
|
|
|
|
|
| 6 |
Teria facilidade em integrar na minha rotina diária a participação num programa de reabilitação cognitiva |
|
|
|
|
|
| 7 |
Os programas de reabilitação cognitiva seriam eficazes para resolver/melhorar as minhas dificuldades cognitivas |
|
|
|
|
|
| 8 |
Tenho confiança de que seria capaz de realizar todas as tarefas de um programa de reabilitação cognitiva |
|
|
|
|
|
| 9 |
A participação num programa de reabilitação cognitiva não iria colidir com as minhas crenças e valores |
|
|
|
|
|
| 10 |
Os programas de reabilitação cognitiva seriam uma opção de intervenção atrativa para mim |
|
|
|
|
|
| 11 |
Participar num programa de reabilitação cognitiva exigiria de mim muito tempo e energia |
|
|
|
|
|
Cotação:
Inverter a cotação dos itens 5 e 11 (1 → 5, 2 → 4, 3 → 3, 4 → 2, 5 → 1)
-
Calcular as pontuações das subescalas:
Fator 1 (Atitude Afetiva e Eficácia): Pontuação média dos itens 1, 2, 3, 7, 9 e 10
Fator 2 (Benefícios Percecionados e Autoeficácia): Pontuação média dos itens 4, 6 e 8
Fator 3 (Sobrecarga Percecionada): Pontuação média dos itens 5R e 11R
Calcular a pontuação total: Pontuação média de todos os 11 itens (após inversão da cotação)
Padronizar para escala 0-100: ((pontuação – 1) / 4) × 100
Interpretação: Pontuações mais elevadas indicam maior aceitabilidade.
Appendix A.2. English Translated Version of the ACRIS-CS [Free Translation, Not Validated]
The following presents the English translation of the ACRIS-CS. The validated European Portuguese version should be used with the European Portuguese-speaking population. Translation to other languages should follow established translation and cultural adaptation procedures (forward translation, back translation, expert review, cognitive debriefing) with subsequent psychometric validation.
Acceptability of Cognitive Rehabilitation Interventions Survey - Cancer Survivors (ACRIS-CS)
This questionnaire assesses the acceptability of cognitive rehabilitation interventions among cancer survivors. Before completing this questionnaire, please read the following description of cognitive rehabilitation programs:
“Cognitive rehabilitation is an approach where a qualified healthcare professional helps patients develop compensatory strategies to manage specific cognitive difficulties (such as using agendas, planners, or reminder systems, and learning techniques to minimize distractions). The professional also provides useful information about brain functioning, cognitive deficits, and their consequences in daily life (psychoeducation). Additionally, cognitive rehabilitation can offer cognitive training (“mental training”), which involves repeated exercises designed to improve cognitive abilities such as attention, memory, processing speed, and executive functions. These exercises are practiced both during sessions with the professional and at home between sessions.
Cognitive rehabilitation programs can be delivered individually or in groups, in person or remotely (via videoconferencing or online platforms). Programs typically span multiple sessions across several weeks.”
Based on this description, please indicate your level of agreement (whether you Totally Disagree, Disagree, are Neutral, Agree, or Totally Agree) with each of the following statements about cognitive rehabilitation programs that may or may not reflect your expectations or opinions.
“Faced with cognitive difficulties related to cancer/treatments…”
| |
|
Totally disagree |
Disagree |
Neutral |
Agree |
Totally agree |
| 1 |
I feel that participation in a cognitive rehabilitation program would be positive for me |
|
|
|
|
|
| 2 |
I recognize that participation in cognitive rehabilitation programs would improve my cognitive functions |
|
|
|
|
|
| 3 |
Participation in a cognitive rehabilitation program would help address my cognitive difficulties |
|
|
|
|
|
| 4 |
I would easily integrate cognitive training exercises into my daily routine between sessions of a cognitive rehabilitation program |
|
|
|
|
|
| 5 |
I feel that participating in a cognitive rehabilitation program would compromise my daily routine |
|
|
|
|
|
| 6 |
I would easily integrate participation in a cognitive rehabilitation program into my daily routine |
|
|
|
|
|
| 7 |
Cognitive rehabilitation programs would be effective in resolving/improving my cognitive difficulties |
|
|
|
|
|
| 8 |
I am confident that I would be able to perform all tasks in a cognitive rehabilitation program |
|
|
|
|
|
| 9 |
Participation in a cognitive rehabilitation program would not conflict with my beliefs and values |
|
|
|
|
|
| 10 |
Cognitive rehabilitation programs would be an attractive intervention option for me |
|
|
|
|
|
| 11 |
Participating in a cognitive rehabilitation program would require a lot of time and energy from me |
|
|
|
|
|
Scoring:
Reverse-score items 5 and 11 (1 → 5, 2 → 4, 3 → 3, 4 → 2, 5 → 1)
-
Calculate subscale scores:
Factor 1 (Affective Attitude and Effectiveness): Average score of items 1, 2, 3, 7, 9, and 10
Factor 2 (Perceived Benefits and Self-Efficacy): Average score of items 4, 6, and 8
Factor 3 (Perceived Burden): Average score of items 5R and 11R
Calculate total score: Average score of all 11 items (after reverse-scoring)
Standardize to 0-100: ((score – 1) / 4) x 100
Interpretation: Higher scores indicate greater acceptability.
References
- Boykoff, N.; Moieni, M.; Subramanian, S.K. Confronting Chemobrain: An in-Depth Look at Survivors’ Reports of Impact on Work, Social Networks, and Health Care Response. Journal of Cancer Survivorship 2009, 3, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Gaynor, A.M.; Root, J.C.; Ahles, T.A. Neuropsychological Impact of Cancer and Cancer Treatments. In Psycho-Oncology (Fourth Edition); Breitbart, W.S., Butow, P.N., Jacobsen, P.B., Lam, W.W.T., Lazenby, M., Loscalzo, M.J., Eds.; Oxford University Press: New York, NY, 2021; pp. 283–290. [Google Scholar]
- Haywood, D.; Dauer, E.; Baughman, F.D.; Lawrence, B.J.; Rossell, S.L.; Hart, N.H.; O’Connor, M. “Is My Brain Ever Going to Work Fully Again?”: Challenges and Needs of Cancer Survivors with Persistent Cancer-Related Cognitive Impairment. Cancers (Basel) 2023, 15, 5331. [Google Scholar] [CrossRef]
- Staat, K.; Segatore, M. The Phenomenon of Chemo Brain. Clin J Oncol Nurs 2005, 9, 713–721. [Google Scholar] [CrossRef]
- Bernstein, L.J.; McCreath, G.A.; Komeylian, Z.; Rich, J.B. Cognitive Impairment in Breast Cancer Survivors Treated with Chemotherapy Depends on Control Group Type and Cognitive Domains Assessed: A Multilevel Meta-Analysis. Neurosci Biobehav Rev 2017, 83, 417–428. [Google Scholar] [CrossRef]
- Horowitz, T.S.; Treviño, M.; Gooch, I.M.; Duffy, K.A. Understanding the Profile of Cancer-Related Cognitive Impairments: A Critique of Meta-Analyses. J Natl Cancer Inst 2019, 111, djz100. [Google Scholar] [CrossRef] [PubMed]
- Dijkshoorn, A.B.C.; van Stralen, H.E.; Sloots, M.; Schagen, S.B.; Visser-Meily, J.M.A.; Schepers, V.P.M. Prevalence of Cognitive Impairment and Change in Patients with Breast Cancer: A Systematic Review of Longitudinal Studies. Psychooncology 2021, 30, 635–648. [Google Scholar] [CrossRef]
- Mayo, S.J.; Lustberg, M.; Dhillon, H.M.; Nakamura, Z.M.; Allen, D.H.; Ah, D.; Janelsins, M.C.; Chan, A.; Olson, K.; Chia, J.T.; et al. Cancer-Related Cognitive Impairment in Patients with Non-Central Nervous System Malignancies: An Overview for Oncology Providers from the MASCC Neurological Complications Study Group. Supportive Care in Cancer 2021, 29, 2821–2840. [Google Scholar] [CrossRef]
- Whittaker, A.L.; George, R.P.; O’Malley, L. Prevalence of Cognitive Impairment Following Chemotherapy Treatment for Breast Cancer: A Systematic Review and Meta-Analysis. Sci Rep 2022, 12, 2135. [Google Scholar] [CrossRef]
- Di Iulio, F.; Cravello, L.; Shofany, J.; Paolucci, S.; Caltagirone, C.; Morone, G. Neuropsychological Disorders in Non-Central Nervous System Cancer: A Review of Objective Cognitive Impairment, Depression, and Related Rehabilitation Options. Neurological Sciences 2019, 40, 1759–1774. [Google Scholar] [CrossRef] [PubMed]
- Collins, B.; MacKenzie, J.; Tasca, G.A.; Scherling, C.; Smith, A. Persistent Cognitive Changes in Breast Cancer Patients 1 Year Following Completion of Chemotherapy. Journal of the International Neuropsychological Society 2014, 20, 370–379. [Google Scholar] [CrossRef]
- Koppelmans, V.; Breteler, M.M.B.; Boogerd, W.; Seynaeve, C.; Gundy, C.; Schagen, S.B. Neuropsychological Performance in Survivors of Breast Cancer More than 20 Years after Adjuvant Chemotherapy. Journal of Clinical Oncology 2012, 30, 1080–1086. [Google Scholar] [CrossRef]
- Oliveira, A.F.; Marques-Fernandes, S.A.; Bártolo, A.; Bem-Haja, P.; Torres, A.; Santos, I.M. Establishing Diagnostic Cut-off Scores for the Perceived Cognitive Impairment Subscale of the Functional Assessment of Cancer Therapy-Cognitive Function—Version 3 in Portuguese Cancer Survivors. Psychooncology 2025, 34, e70278. [Google Scholar] [CrossRef]
- Sleurs, C.; Amidi, A.; Wu, L.M.; Kiesl, D.; Zimmer, P.; Lange, M.; Rogiers, A.; Giffard, B.; Binarelli, G.; Borghgraef, C.; et al. Cancer-Related Cognitive Impairment in Non-CNS Cancer Patients: Targeted Review and Future Action Plans in Europe. Crit Rev Oncol Hematol 2022, 180, 103859. [Google Scholar] [CrossRef]
- Haywood, D.; Henry, M.; Dauer, E.; Lederman, O.; Farley, M.; Henneghan, A.M.; O’Connor, M.; Jefford, M.; Rossell, S.L.; Hart, N.H. Cancer-Related Cognitive Impairment as a Key Contributor to Psychopathology in Cancer Survivors: Implications for Prevention, Treatment and Supportive Care. Supportive Care in Cancer 2024, 32, 480. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.S. Chemotherapy-Related Cognitive Impairment - The Breast Cancer Experience. Oncol Nurs Forum 2012, 39, E31–E40. [Google Scholar] [CrossRef] [PubMed]
- Selamat, M.H.; Loh, S.Y.; Mackenzie, L.; Vardy, J. Chemobrain Experienced by Breast Cancer Survivors: A Meta-Ethnography Study Investigating Research and Care Implications. PLoS One 2014, 9, e108002. [Google Scholar] [CrossRef]
- Von Ah, D.; Storey, S.; Tallman, E.; Nielsen, A.; Johns, S.A.; Pressler, S.J. Cancer, Cognitive Impairment, and Work-Related Outcomes: An Integrative Review. Oncol Nurs Forum 2016, 43, 602–616. [Google Scholar] [CrossRef]
- Crouch, A.; Von Ah, D.; Storey, S. Addressing Cognitive Impairment after Breast Cancer: What Do Women Want? Clinical Nurse Specialist 2017, 31, 82–88. [Google Scholar] [CrossRef]
- Hart, N.H.; Stout, N.L.; Haywood, D.; Ashbury, F.D.; Chan, R.J.; Fitch, M.I.; Jefford, M.; Lustberg, M.B.; Etemadi, Y.; Rauch, A. World Health Organization Package of Interventions for Rehabilitation for Cancer: A MASCC-Endorsed Resource for Global Action to Address Unmet Rehabilitation Needs of People Affected by Cancer. Supportive Care in Cancer 2024, 32, 417. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.S.K.; Wang, X.; Niu, N.; Liang, M.; Zeng, Y. Neuropsychological Interventions for Cancer-Related Cognitive Impairment: A Network Meta-Analysis of Randomized Controlled Trials. Neuropsychol Rev 2022, 32, 893–905. [Google Scholar] [CrossRef]
- Haywood, D.; Henneghan, A.M.; Chan, A.; Chan, R.J.; Dhillon, H.M.; Lustberg, M.B.; Vardy, J.L.; O’Connor, M.; Elvidge, N.; Dauer, E.; et al. The Effect of Non-Pharmacological Interventions on Cognitive Function in Cancer: An Overview of Systematic Reviews. Supportive Care in Cancer 2025, 33, 151. [Google Scholar] [CrossRef] [PubMed]
- Pike, K.E.; Li, L.; Naismith, S.L.; Bahar-Fuchs, A.; Lee, A.; Mehrani, I.; Bentvelzen, A.; Lautenschlager, N.T.; O’Connell, M.E.; Blackberry, I.; et al. Implementation of Cognitive (Neuropsychological) Interventions for Older Adults in Clinical or Community Settings: A Scoping Review. Neuropsychol Rev 2025, 35, 588–616. [Google Scholar] [CrossRef] [PubMed]
- Treanor, C.J.; Mcmenamin, U.C.; O’Neill, R.F.; Cardwell, C.R.; Clarke, M.J.; Cantwell, M.; Donnelly, M. Non-Pharmacological Interventions for Cognitive Impairment Due to Systemic Cancer Treatment (Review). Cochrane Database of Systematic Reviews 2016, CD011325. [Google Scholar] [CrossRef]
- Zeng, Y.; Dong, J.; Huang, M.; Zhang, J. e.; Zhang, X.; Xie, M.; Wefel, J.S. Nonpharmacological Interventions for Cancer-Related Cognitive Impairment in Adult Cancer Patients: A Network Meta-Analysis. Int J Nurs Stud 2020, 104, 103514. [Google Scholar] [CrossRef]
- Duivon, M.; Lange, M.; Binarelli, G.; Lefel, J.; Hardy-Léger, I.; Kiasuwa-Mbengi, R.; Méric, J.B.; Charles, C.; Joly, F. Improve the Management of Cancer-Related Cognitive Impairment in Clinical Settings: A European Delphi Study. Journal of Cancer Survivorship 2024, 18, 1974–1997. [Google Scholar] [CrossRef]
- Nakamura, Z.M.; Ali, N.T.; Crouch, A.; Dhillon, H.; Federico, A.; Gates, P.; Grech, L.; Kesler, S.R.; Ledbetter, L.; Mantovani, E.; et al. Impact of Cognitive Rehabilitation on Cognitive and Functional Outcomes in Adult Cancer Survivors: A Systematic Review. Semin Oncol Nurs 2024, 40, 151696. [Google Scholar] [CrossRef]
- Yang, P.; Hu, Q.; Zhang, L.; Shen, A.; Zhang, Z.; Wang, Q.; Lu, Q. Effects of Non-Pharmacological Interventions on Cancer-Related Cognitive Impairment in Patients with Breast Cancer: A Systematic Review and Network Meta-Analysis. European Journal of Oncology Nursing 2025, 75, 102804. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. NCCN Guidelines Version 2.2025 Survivorship. Available online: https://www.nccn.org/guidelines/guidelines-detail?category=3&id=1466#:~:text=Guidelines-,NCCN%20Guidelines,-Version%202.2025 (accessed on 1 November 2025).
- Antares Consulting and Unicancer; Sciensano. Guide: Practices and Recommendations for the Management of Cognitive Impairment after Cancer. Available online: https://www.ipaac.eu/res/file/outputs/wp4/practices-recommendations-cancer-cognitive-impairements.pdf (accessed on 1 November 2025).
- Binarelli, G.; Duivon, M.; Joly, F.; Ahmed-Lecheheb, D.; Lange, M. Cancer-Related Cognitive Impairment: Current Perspectives on the Management of Cognitive Changes Following Cancer Treatment. Expert Rev Neurother 2023, 23, 249–268. [Google Scholar] [CrossRef]
- Clare, L.; Woods, R.T. Cognitive Training and Cognitive Rehabilitation for People with Early-Stage Alzheimer’s Disease: A Review. Neuropsychological Rehabilitation: An International Journal 2004, 14, 385–401. [Google Scholar] [CrossRef]
- Fernandes, H.A.; Richard, N.M.; Edelstein, K. Cognitive Rehabilitation for Cancer-Related Cognitive Dysfunction: A Systematic Review. Supportive Care in Cancer 2019, 27, 3253–3279. [Google Scholar] [CrossRef] [PubMed]
- Yan, X.; Wei, S.; Liu, Q. Effect of Cognitive Training on Patients with Breast Cancer Reporting Cognitive Changes: A Systematic Review and Meta-Analysis. BMJ Open 2023, 13, e058088. [Google Scholar] [CrossRef]
- Oliveira, A.F.; Sosa-Napolskij, M.; Torres, A.; Queiroz, D.F.; Bártolo, A.; Sousa, H.; Monteiro, S.; Van Dyk, K.; Ercoli, L.M.; Santos, I.M. CanCOG®: Cultural Adaptation of the Evidence-Based UCLA Cognitive Rehabilitation Intervention Program for Cancer Survivors in Portugal. Healthcare 2023, 11, 141. [Google Scholar] [CrossRef]
- Proctor, E.; Silmere, H.; Raghavan, R.; Hovmand, P.; Aarons, G.; Bunger, A.; Griffey, R.; Hensley, M. Outcomes for Implementation Research: Conceptual Distinctions, Measurement Challenges, and Research Agenda. Administration and Policy in Mental Health and Mental Health Services Research 2011, 38, 65–76. [Google Scholar] [CrossRef]
- Sekhon, M.; Cartwright, M.; Francis, J.J. Acceptability of Healthcare Interventions: An Overview of Reviews and Development of a Theoretical Framework. BMC Health Serv Res 2017, 17, 88. [Google Scholar] [CrossRef]
- Skivington, K.; Matthews, L.; Simpson, S.A.; Craig, P.; Baird, J.; Blazeby, J.M.; Boyd, K.A.; Craig, N.; French, D.P.; McIntosh, E.; et al. A New Framework for Developing and Evaluating Complex Interventions: Update of Medical Research Council Guidance. The BMJ 2021, 374, n2061. [Google Scholar] [CrossRef]
- Sekhon, M.; Cartwright, M.; Francis, J.J. Acceptability of Health Care Interventions: A Theoretical Framework and Proposed Research Agenda. Br J Health Psychol 2018, 23, 519–531. [Google Scholar] [CrossRef]
- Sekhon, M.; Cartwright, M.; Lawes-Wickwar, S.; McBain, H.; Ezra, D.; Newman, S.; Francis, J.J. Does Prospective Acceptability of an Intervention Influence Refusal to Participate in a Randomised Controlled Trial? An Interview Study. Contemp Clin Trials Commun 2021, 21, 100698. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, J.M.; Alegría, M.; Prihoda, T.J.; Copeland, L.A.; Zeber, J.E. How the Relationship of Attitudes toward Mental Health Treatment and Service Use Differs by Age, Gender, Ethnicity/Race and Education. Soc Psychiatry Psychiatr Epidemiol 2011, 46, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Pedro, L.M.R.; de Oliveira, M.F.; Pereira, M.D.; da Fonseca, A.D.; Canavarro, M.C. Factors Associated with Prospective Acceptability and Preferences for Unified Transdiagnostic Cognitive-Behavioral Treatments and Group Therapy in the Portuguese General Population. Administration and Policy in Mental Health and Mental Health Services Research 2024, 51, 857–876. [Google Scholar] [CrossRef] [PubMed]
- Young, B.; Robb, K.A. Understanding Patient Factors to Increase Uptake of Cancer Screening: A Review. Future Oncology 2021, 17, 3757–3775. [Google Scholar] [CrossRef]
- Hewitt, M.; Greenfield, S.; Stovall, E. From Cancer Patient to Cancer Survivor: Lost in Transition; The National Academies Press: Washington, D.C., 2006; ISBN 978-0-309-09595-2. [Google Scholar]
- Mollica, M.A.; Doose, M.; Reed, C.; Tonorezos, E. Defining Concepts in Cancer Survivorship. Cancer 2025, e70039. [Google Scholar] [CrossRef]
- Buchanan, N.D.; Dasari, S.; Rodriguez, J.L.; Lee Smith, J.; Hodgson, M.E.; Weinberg, C.R.; Sandler, D.P. Post-Treatment Neurocognition and Psychosocial Care among Breast Cancer Survivors. Am J Prev Med 2015, 49, S498–S508. [Google Scholar] [CrossRef] [PubMed]
- Lange, M.; Licaj, I.; Clarisse, B.; Humbert, X.; Grellard, J.-M.; Tron, L.; Joly, F. Cognitive Complaints in Cancer Survivors and Expectations for Support: Results from a Web–Based Survey. Cancer Med 2019, 8, 2654–2663. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Participants. JAMA 2025, 333, 71–74. [Google Scholar] [CrossRef]
- American Psychological Association. Publication Manual of the American Psychological Association, Seventh Edition; American Psychological Association, Ed.; 2020.
- Ordem dos Psicólogos Portugueses. Regulamento n.o 898/2024, Código Deontológico Da Ordem Dos Psicólogos Portugueses (OPP); 2024.
- LimeSurvey GmbH LimeSurvey: An Open Source Survey Tool. Available online: https://www.limesurvey.org/ (accessed on 29 December 2025).
- Pais-Ribeiro, J.; Silva, I.; Ferreira, T.; Martins, A.; Meneses, R.; Baltar, M. Validation Study of a Portuguese Version of the Hospital Anxiety and Depression Scale. Psychol Health Med 2007, 12, 225–237. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Wagner, L.I.; Sweet, J.; Butt, Z.; Lai, J.; Cella, D. Measuring Patient Self-Reported Cognitive Function: Development of the Functional Assessment of Cancer Therapy-Cognitive Function Instrument. J Support Oncol 2009, 7, 32–39. [Google Scholar]
- Oliveira, A.F.; Santos, I.M.; Fernandes, S.; Bem-Haja, P.; Torres, A. Validation Study of the Functional Assessment of Cancer Therapy-Cognitive Function-Version 3 for the Portuguese Population. BMC Psychol 2022, 10, 305. [Google Scholar] [CrossRef] [PubMed]
- Schagen, S.B.; Das, E.; Vermeulen, I. Information about Chemotherapy-Associated Cognitive Problems Contributes to Cognitive Problems in Cancer Patients. Psychooncology 2012, 21, 1132–1135. [Google Scholar] [CrossRef] [PubMed]
- Schagen, S.B.; Das, E.; van Dam, F.S.A.M. The Influence of Priming and Pre-Existing Knowledge of Chemotherapy-Associated Cognitive Complaints on the Reporting of Such Complaints in Breast Cancer Patients. Psychooncology 2009, 18, 674–678. [Google Scholar] [CrossRef] [PubMed]
- Timm, L.; Annerstedt, K.S.; Ahlgren, J.Á.; Absetz, P.; Alvesson, H.M.; Forsberg, B.C.; Daivadanam, M. Application of the Theoretical Framework of Acceptability to Assess a Telephone-Facilitated Health Coaching Intervention for the Prevention and Management of Type 2 Diabetes. PLoS One 2022, 17, e0275576. [Google Scholar] [CrossRef]
- Boateng, G.O.; Neilands, T.B.; Frongillo, E.A.; Melgar-Quiñonez, H.R.; Young, S.L. Best Practices for Developing and Validating Scales for Health, Social, and Behavioral Research: A Primer. Front Public Health 2018, 6, 149. [Google Scholar] [CrossRef]
- Fonseca, A.; Gorayeb, R.; Canavarro, M.C. Women’s Use of Online Resources and Acceptance of e-Mental Health Tools during the Perinatal Period. Int J Med Inform 2016, 94, 228–236. [Google Scholar] [CrossRef]
- Sousa, M.; Moreira, H.; Canavarro, M.C.; Barreto Carvalho, C. Estudo de Aceitabilidade Das Intervenções Psicológicas via Telefone Para Sobreviventes de Cancro Dos Açores [Azorean Cancer Survivors’ Acceptability of Psychological Telephone-Based Interventions]. Revista Psicologia, Diversidade e Saúde 2021, 10, 37–56. [Google Scholar] [CrossRef]
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Bouter, L.M.; De Vet, H.C.W. The COSMIN Checklist for Assessing the Methodological Quality of Studies on Measurement Properties of Health Status Measurement Instruments: An International Delphi Study. Quality of Life Research 2010, 19, 539–549. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, H.F. An Index of Factorial Simplicity. Psychometrika 1974, 39, 31–36. [Google Scholar] [CrossRef]
- Bartlett, M.S. Tests of Significance in Factor Analysis. British Journal of Statistical Psychology 1950, 3, 77–85. [Google Scholar] [CrossRef]
- Costello, A.B.; Osborne, J.W. Best Practices in Exploratory Factor Analysis: Four Recommendations for Getting the Most from Your Analysis. Practical Assessment, Research & Evaluation 2005, 10, 1–9. [Google Scholar] [CrossRef]
- Kaiser, H.F. The Application of Electronic Computers to Factor Analysis. Educ Psychol Meas 1960, 20, 141–151. [Google Scholar] [CrossRef]
- Cattell, R.B. The Scree Test for the Number of Factors. Multivariate Behav Res 1966, 1, 245–276. [Google Scholar] [CrossRef]
- Fayers, P.M.; Machin, D. Quality of Life: The Assessment, Analysis and Reporting of Patient-Reported Outcomes; Third Edition; John Wiley & Sons, Ltd.: Oxford, 2016. [Google Scholar]
- Nunnally, J.C.; Bernstein, I.H. Psychometric Theory (Third Edition); McGraw-Hill, Inc.: New York, 1994. [Google Scholar]
- Kaur, P.; Stoltzfus, J.; Yellapu, V. Descriptive Statistics. Int J Acad Med 2018, 4, 60–63. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences (Second Edition); Lawrence Erlbaum Associates: New York, 1988. [Google Scholar]
- George, D.; Mallery, P. IBM SPSS Statistics 29 Step by Step: A Simple Guide and Reference (Eighteenth Edition); Routledge: New York, NY, 2024. [Google Scholar]
- De Vet, H.C.W.; Terwee, C.B.; Mokkink, L.B.; Knol, D.L. Measurement in Medicine: A Practical Guide; Cambridge University Press: New York, 2011. [Google Scholar]
- Chen, Y.-X.; Zhou, Y.; Zhang, X.-L.; He, W.; Ye, Q.; Xu, M. Digital Health Interventions for Cancer-Related Cognitive Impairment in Breast Cancer Patients: A Scoping Review. Digit Health 2025, 11, 1–23. [Google Scholar] [CrossRef]
- Kim, Y.; Kang, S.J. Computerized Programs for Cancer Survivors with Cognitive Problems: A Systematic Review. Journal of Cancer Survivorship 2019, 13, 911–920. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, Y.; Li, R.; Sun, Z.; Li, Q. Web-Based Cognitive Interventions on Subjective Cognitive Impairment in Cancer Survivors: A Systemic Review. Int J Nurs Sci 2024, 11, 429–438. [Google Scholar] [CrossRef] [PubMed]
- Merceur, M.; Reilly, K.T.; Bonan, I.; Holé, J.; Hummel, E.; Cogné, M.; Jacquin-Courtois, S. A Systematic Review of Rehabilitation Programs for Cognitive Impairment Related to Breast Cancer: Different Programs at Different Times? Ann Phys Rehabil Med 2024, 67, 101832. [Google Scholar] [CrossRef] [PubMed]
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).