
Submitted:
11 February 2025
Posted:
12 February 2025
You are already at the latest version
Abstract
Background: Return to work (RTW) after cancer can be a significant challenge with individuals when it comes to return to work (RTW), including physical, psychological, and workplace-related barriers. iCanWork, a multidisciplinary intervention integrating vocational rehabilitation (VR) and occupational therapy (OT), aims to address these challenges and promote sustainable RTW. Methods: This pilot randomized controlled trial evaluated the feasibility, acceptability, and preliminary efficacy of iCanWork among 23 individuals touched by cancer (ITBC) randomized to the intervention or control group. Feasibility was assessed by recruitment, retention, and adherence benchmarks. Acceptability was evaluated using participant satisfaction surveys. Preliminary efficacy was measured through RTW status, Work Ability Index (WAI) scores, and health-related quality of life (QoL) outcomes. Results: Feasibility benchmarks were achieved (92% recruitment, 83% retention). Participants found the intervention highly satisfactory for its tailored support. The iCanWork group demonstrated modest improvements in WAI scores (mean change: +2.54) and QoL domains, including Social Roles, while the control group exhibited declines. However, no significant differences in RTW rates or WAI scores were observed between groups, highlighting the need for enhanced and prolonged interventions. Conclusions: he iCanWork intervention is feasible and acceptable, showing potential to address critical barriers to RTW for cancer survivors. Larger trials are warranted to confirm efficacy and optimize intervention strategies for sustainable employment outcomes.
Keywords:
Return to Work (RTW)
; Individuals Touched by Cancer (ITBC)
; Cancer Survivorship
; Vocational Rehabilitation (VR)
; Occupational Therapy (OT)
; Work Ability Index (WAI)
; Feasibility Trial
1. Introduction
The growing incidence of cancer and improved survival rates present new challenges for the vocational reintegration of Individuals Touched by Cancer (ITBC). Throughout this study, we use ITBC to refer to individuals who have experienced a cancer diagnosis at some point in their lives. This term is used intentionally to acknowledge that while cancer may have been part of their journey, it does not define their identity. Unlike terms such as "cancer survivor" or "patient," ITBC is more inclusive, encompassing individuals at various stages of their experience—whether they are in treatment, post-treatment, or navigating life beyond cancer.
Returning to work is a crucial step in the healing process for cancer survivors, helping them regain a sense of normalcy and social reintegration [1]. Return to work (RTW) or vocational reintegration refers to the process by which an individual, after a prolonged absence due to health issues, an accident, or other personal reasons, returns to their previous job or transitions into a new job adapted to their current condition [2]. Successful vocational reintegration often involves workplace modifications, reassessment of skills and abilities, and ongoing support to facilitate both return to work and long-term job retention [3].
Despite the employment rate one year after a cancer diagnosis appearing relatively promising—ranging from 52% to 73%—oncology occupational studies reveal a more nuanced reality [4,5]. ITBC often face negative work outcomes that persist well beyond the first year post-diagnosis, lasting up to a decade [5]. Compared to their healthy counterparts, survivors experience an increased risk of extended sick leaves, resignations, reduced working hours, role changes, and early, unplanned retirement [6,7]. Additional challenges include diminished income, workplace discrimination, and adjustments to work methods. The uncertainty surrounding the chronic illness trajectory further complicates these work adjustments, making sustained employment particularly challenging for many survivors.
Addressing the complex and multifaceted challenges to vocational reintegration requires system-level solutions that consider the interplay between individual, organizational, and societal factors. Such as, returning to work does not necessarily mean a return to a normal workload or work life. Similar to the end of cancer treatment, a return to work does not mark full recovery or a return to previous functional levels. Many ITBC continue to experience physical and psychological effects following the end of treatment, which can persist for more than a year, such as fatigue and depression, significantly impacting their ability to work and overall job performance after returning to work [5,8,9]. Moreover, stigmatization in the workplace [10] and inadequate employer and colleague support [11], both practical and emotional, serve as major barriers to a successful return to work following a cancer diagnosis. These challenges heighten the risk of job market withdrawal, contributing to higher absenteeism, involuntary resignations, and long-term unemployment among survivors [12]. As a result, ITBC experience significant economic losses, with wage reductions estimated between 24% and 43%, depending on employment type [13]. Additionally, household income losses can be compounded by caregiving responsibilities, with associated costs ranging from $15,786 to $20,414 per patient annually, and household productivity losses reaching as high as $238,904 per household per year [13]. The cumulative impact of these barriers leads to substantial financial strain and diminished quality of life for survivors and their families [7].
A comprehensive understanding of systemic factors is essential to improving the healing process and RTW outcomes for ITBC. A multidisciplinary approach plays a critical role in this process, integrating vocational rehabilitation (VR) and occupational therapy (OT) to address the diverse challenges faced by cancer survivors. VR supports individuals in overcoming employment barriers such as work gaps and the need for accommodation through career counseling, job placement, and skills training. Meanwhile, occupational therapists help cancer survivors regain the ability to participate in their valued activities, from daily living to work. OT interventions may include adapting workspaces to accommodate physical limitations, teaching coping strategies for fatigue, or enhancing time management skills. Through personalized strategies, both VR and OT work collaboratively to improve survivors' functional abilities, quality of life, and overall readiness for workforce reintegration. However, despite these supports, many ITBC face significant barriers beyond individual rehabilitation, particularly due to systemic disparities in access to services and workplace accommodation.
In Canada, ITBC encounter workplace stigma, inconsistent employer accommodations, and limited vocational rehabilitation services [4]. Unlike leading European models, where RTW is integrated into oncology care, Canada’s approach remains largely employer-driven, fragmented, and unevenly available across provinces. The absence of nationally structured RTW policies further exacerbates disparities in employment support, often leaving survivors to self-navigate the reintegration process with little formal guidance [14].
The scale of this challenge to reintegrating the workforce following cancer is substantial. In 2024 alone, an estimated 247,100 Canadians were diagnosed with cancer, with over one-third (approximately 91,000) being of working age [15]. Beyond new diagnoses, a much larger population of 555,000 working-age Canadians currently live with or beyond cancer, many of whom experience persistent work-related challenges. Alarmingly, studies estimate that up to 40% of ITBC face unemployment risks, translating to 222,000 individuals at risk of leaving the workforce that could be prevented if adequate RTW support was available to them [16].
Existing interventions for oncology vocational reintegration interventions within oncology care centers are rare, with only one in Canada specifically offering such service [4], yet even this unique one remains untested, and lacks opportunity to work in tandem with occupational therapy (OT). Guided by recent Cochrane reviews [17,18], we propose the iCanWork to address critical gaps in existing care models. iCanWork is an online, one-on-one, professionally led, multidisciplinary intervention that integrates VR counselling and OT support.
The iCanWork intervention is built upon a comprehensive theoretical framework, specifically a four-factor vocational rehabilitation model (See Figure 1) [19,20,21]. This model addresses the multifaceted relationship among the impact of cancer on person-related functions and characteristics to systems factor, and work context and conditions that influence the RTW process. The first factor, Cancer's Impact on Functions, focuses on the effects of cancer and its treatments on pre-existing conditions, on physical, psychological, and cognitive functions, highlighting areas that may present challenges to RTW efforts. The second factor, Person-Related Characteristics, explores individual attitudes towards work and recovery, while considering socio-demographic elements such as age, gender, and income that shape the reintegration process. The third factor, Support Systems and Resources, evaluates the availability and effectiveness of healthcare/rehabilitation services, insurance, and social support systems that are essential for maintaining employment. Finally, the fourth factor, Work Context and Conditions examines job demands, workplace accommodations, and organizational culture to assess how these factors align with the individual’s work ability after cancer treatment.
Figure 2 provides an overview of the intervention's core components, detailing session goals, opportunities for improvement, expected outcomes, and the collaborative roles of the VR counselor and OT. The intervention begins by introducing participants to the iCanWork program, followed by an assessment based on the four-factor model, leading to the development of a personalized cancer and work profile. Participants receive tailored support to address individual barriers and actionable strategies for workplace reintegration through ongoing counseling sessions. These sessions also help participants navigate access to rehabilitative services, including consultations with specialists such as OTs. Additionally, the intervention includes a worksite assessment conducted by the OT, with input from the VR counselor. This step evaluates the participant's work abilities in relation to job demands [22], identifying compensatory strategies and accommodations to facilitate workplace reintegration.
The iCanWork program incorporates a person-centered, tailored approach to ensure that support aligns with each participant’s evolving needs. Regular sessions are conducted to monitor progress, revisiting and adjusting objectives as necessary to enhance work ability and facilitate both RTW and long-term employment sustainability. Each session includes discussions to identify situational needs, allowing for the determination of whether further support, including additional sessions, may be required to address specific challenges. After each session, participants receive summary reports that capture key discussions and collaboratively developed plans, ensuring alignment with their individualized employment goals. These reports also include educational materials, resource recommendations, and referrals to appropriate professionals, such as family physicians or neuropsychologists, when cognitive challenges are identified. Cognitive challenges are assessed using the Cancer and Work Cognitive Symptoms at Work Checklist [23], which was modified from the validated tool by Ottati and Feuerstein [24] to include individuals who have not yet returned to work. The modified version of this tool is accessible on the Cancer and Work website [23]. These tailored recommendations and resources aim to provide participants with comprehensive support for successful reintegration into the workforce.
The development of iCanWork followed an iterative and evidence-informed process, beginning in 2011 with the publication of Cancer and Returning to Work: A Practical Guide for Cancer Patients [25]. This workbook, authored by co-author M. Parkinson, a master’s-level oncology VR counselor with 30 years of experience in cancer-related RTW interventions, was evaluated by 60 experts with professional and lived experience, including ILWC and employer representatives. Recognized as a critical resource for clinical practice, the workbook laid the foundation for the creation of the Cancer and Work website, launched in 2016 [20]. This comprehensive 600-page platform provides evidence-based information, tools, and resources to support RTW. One of its key offerings, the iCanWork: 10 Step RTW Intervention, delivers step-by-step guidance for ILWC, healthcare providers, and employers to navigate the RTW process effectively.
Before launching the Cancer and Work website, our team conducted an acceptability evaluation of its content and resources. Feedback from 250 ILWC highlighted the comprehensiveness, completeness, and usefulness of both the website and the iCanWork: 10 Step RTW Intervention, though they also noted its complexity [26]. A second usability review in 2019 corroborated these findings and included a key recommendation to enhance the iCanWork: 10 Steps RTW Intervention with online support to increase accessibility and user engagement.
To maximize the potential efficacy of the enhanced iCanWork: 10 Steps RTW Intervention for ILWC, we have incorporated the latest recommendations from systematic reviews to integrate VR and OT expertise into the resource and theoretically grounded in the four-factor model [19,27,28]. This integration aims to provide a multidisciplinary approach that addresses the unique challenges faced by ILWC during their process of RTW. Notably, a VR/OT approach has not yet been adequately explored in this context, underscoring the innovative and necessary nature of this intervention [29,30,31]. This present study aimed to pilot-test iCanWork through a feasibility randomized controlled pilot trial. Specifically, the objectives of this pilot RCT were to assess iCanWork’s (a) feasibility; (b) its acceptability; and (c) its preliminary efficacy on four study outcomes: RTW, work ability, health-related quality of life, and satisfaction with therapist and service.
2. Materials and Methods
2.1. Study Design
This pilot randomized controlled trial (RCT) employed a 1:1 parallel group design, comparing an intervention group to a control group. The study followed the guidelines set forth by the Consolidated Standards of Reporting Trials (CONSORT) 2010 for randomized pilot and feasibility trials (Supplementary Table S1) [32], ensuring a structured and transparent reporting process. Additional guidance was drawn from the Template for Intervention Description and Replication (TIDieR) (Supplementary Table S2) [33], which provides a framework for describing interventions in detail. This study received ethical approval from the Research Ethics Boards of the first author primary clinical sites located in Montreal, Quebec.
2.2. Setting, Recruitment, Participants, and Sample Size
Participants for the study were recruited from ambulatory follow-up cancer care clinics at two participating cancer centers in Montreal, Quebec, through referrals from oncologists and nurses. Additionally, approximately half of the participants self-referred in response to advertisements placed on the Cancer and Work website and through Quebec-based cancer organizations, such as the Quebec Cancer Foundation, from May 2022 to August 2022.
Eligibility criteria included individuals who: (1) had been diagnosed with any type of cancer treated with curative intent and of working age (between 18 and 65 years at the time of diagnosis); (2) employed in a paid position at the time of diagnosis (full-time or part-time); (3) were on a cancer-related sick leave, including long-term disability leave, but for less than two years; (4) had not initiated a RTW, including partial RTW, since their leave due to cancer; (5) were able to read and understand English or French; and (6) resided in the province of Quebec. The inclusion criterion requiring participants to reside in Quebec was necessary because the work-focused health professionals delivering the intervention were licensed in the province of Quebec.
2.3. Randomization and Blinding
The study coordinator scheduled the initial appointment with eligible participants via videoconferencing. During this session, participants received a detailed explanation of the study’s purpose, followed by a question-and-answer period to address any concerns. Upon obtaining informed electronic consent, participants proceeded to complete baseline assessments (T0), which included demographic and medical information as well as the designated self-reported study questionnaires. Once baseline data collection was completed, the study coordinator accessed a secure, single-use locked folder to determine the participant’s allocation to either the iCanWork intervention or the control arm, using a 1:1 randomization ratio. The randomization sequence was pre-generated by a statistician at the Research Institute of the McGill University Health Centre (RI-MUHC) and securely maintained. To ensure allocation concealment and minimize potential bias, the sequence remained blinded to both the study coordinator and participants, thereby guaranteeing an impartial assignment process.
For participants allocated to the iCanWork intervention, the study coordinator scheduled their first session with the study’s VR counselor, which included the possibility of one to three sessions. Additionally, participants could receive one to two sessions with the study’s OT, contingent upon an assessment of their needs by the VRC, OT, and the participant (ITBC). All counseling sessions were conducted via videoconferencing and recorded to ensure fidelity in the delivery of the intervention. Fidelity was reviewed by CM, and MP for all sessions, with a specific focus on the first session, which was reviewed within 24 hours of its delivery. Recommendations for session delivery improvements were made by CM and MP during a videoconference within the first week of the session date, and these recommendations were communicated to the VRC or OT’ responsible for delivering the session to enhance consistency and adherence to the intervention protocol.
Participants allocated to the control group were informed they would not receive any services (e.g., VR counseling or OT sessions) but would instead be directed to the Cancer and Work website for educational resources related to RTW after cancer.
2.4. Study Groups
Intervention Group. The iCanWork RTW intervention was delivered via individual videoconferencing, focusing on addressing ILWC' health challenges (e.g., fatigue, cognitive impairments, anxiety) and incrementally building strategies to enhance work ability and sustainable employment. The intervention was grounded in the iCanWork 10-step approach, as outlined in Figure 2.
Participants received between one to three VR counselling sessions and, if needed, one to two OT sessions. These sessions were tailored to individual needs, with the first session lasting approximately 1.5 hours and subsequent sessions lasting an hour each. The number of sessions provided was constrained by funding limitations, though in practice, more sessions might be required.
The intervention emphasized flexibility to accommodate participants' preferences, offering sessions via telephone for those uncomfortable with videoconferencing, scheduled at a time convenient for them. Each session concluded with a written summary of recommendations, which was sent to the participant within 24 hours. Supplementary document S1 include examples of intake sessions and summary notes: an initial vocational rehabilitation assessment session with recommendations shared with the participant, an occupational therapist intake session with corresponding summary notes, and an example of a follow-up session conducted by the study’s vocational rehabilitation counselor.
Control Group. Participants in the control group were directed to the Cancer and Work website (www.cancerandwork.ca) [20], which serves as a standalone resource for RTW education. The website provides bilingual educational materials and does not include access to services like VR counseling or OT sessions. Control group participants were instructed to download a bilingual pamphlet summarizing the website’s key content. Additionally, participants were advised to consult their healthcare team for any further RTW-related concerns or guidance.
2.5. Data Collection
Demographic and clinical information was collected through a baseline assessment questionnaire completed by all participants prior to randomization (T1).
Feasibility of the iCanWork intervention was evaluated based on benchmarks set for its rates of participant i) accrual with at least 50% at three months of start of study enrolment, and ii) retention with 70%. These feasibility outcomes align with the Consolidated Standards of Reporting Trials (CONSORT) requirements for clinical trials in eHealth (CONSORT-EHEALTH v1.6.1) [36,37]. A study log was maintained by the study coordinator to systematically collect data on feasibility criteria throughout the study. For example, the log documented recruitment and retention rates, including the number of patients approached, self-referred participants, eligible and ineligible patients, reasons for ineligibility, participants declining participation (with reasons), and those who consented and were randomized.
To ensure fidelity of the intervention, we aimed to have 90% of sessions conducted by the VR counsellor or OT to be reviewed by the two principal study leads within 48 hours of completion [38]. This review process was implemented as an additional benchmark for maintaining consistency and adherence to the intervention protocol, ensuring high-quality delivery of the iCanWork intervention across all participants.
The acceptability of the iCanWork intervention was assessed using the Satisfaction with Therapy and Therapist Scale-Revised (STTS-R) [39]. Originally developed to evaluate satisfaction with group psychotherapy, the STTS-R was adapted to assess participants’ experiences with the iCanWork intervention. This 13-item scale employs a 5-point Likert format, ranging from strongly disagree (1) to strongly agree (5), and evaluates three key domains: satisfaction with the intervention, satisfaction with the therapist delivering the intervention, and perceived changes in the participant's condition. Higher scores indicate greater satisfaction and a more positive endorsement of the intervention.
The STTS-R was administered to participants in the intervention group at three months post-study enrollment. At six months post-enrollment, the twelve participants in the iCanWork intervention were invited to provide additional feedback using an open-ended prompt: 'In what ways, if any, did the support received from the iCanWork intervention help you with your return to work?' Recognized for its robust psychometric properties [39], the STTS-R remains a validated and reliable tool for assessing therapeutic acceptability. Its utility has been demonstrated in recent studies, including those focusing on internet-based interventions [40,41].
The preliminary efficacy of the iCanWork intervention was assessed using three self-reported study outcomes through questionnaires collected from all participants at baseline, prior to randomization (T1), and at three (T2) post-study enrollment. Two work outcomes and two clinical outcomes were evaluated. Work outcomes assessed were (1) work status assessed with a binary (Yes/No) item asking, "Are you back to work following your sick leave for cancer, in any form, part-time, full-time, or progressive return to work?" [42,43,44]; and (2) Work Ability Index (WAI): The WAI was measured using its first three items to evaluate current work ability against job demands, providing insights into participants' likelihood of sustaining employment [45,46,47]. Clinical outcomes were (1) Quality of Life (QoL) measured using the PROMIS-29 adult profiles (33), which assess seven health domains: physical function, anxiety, depression, fatigue, sleep disturbance, ability to participate in social roles and activities, and pain interference. These domains are known to influence the capacity for sustained employment [48,49]. A T-score was generated for each subscale, with higher scores indicating greater endorsement of the construct being assessed; and (2) Participant satisfaction with the iCanWork intervention, assessed through the STTS-R (detailed under Acceptability Assessment), was included as one of the clinical outcomes to evaluate the perceived effectiveness of the intervention.
2.6. Data Analysis
Data analysis was conducted using IBM SPSS Statistics (v26). Descriptive statistics, including means, standard deviations, frequencies, and percentages, were used to summarize participant demographics, clinical characteristics, and intervention benchmarks. Feasibility outcomes, such as recruitment uptake, retention rates, and questionnaire completion percentages, were evaluated against pre-established benchmarks. High ratings for acceptability survey items (scores of 4 or 5 on a 5-point Likert scale) were calculated and reported as percentages. All continuous variables were tested for normality using the Shapiro-Wilk test, supported by Q-Q plots and variance equality tests (e.g., Levene’s Test) to confirm the appropriateness of the statistical methods.
Baseline equivalence between groups was assessed using independent t-tests for continuous variables and chi-square tests (or Fisher’s Exact Test where appropriate) for categorical variables. Feasibility and adherence data, including reasons for unmet intervention benchmarks, were summarized descriptively.
For work outcomes, Kaplan-Meier survival analysis was used to examine time to RTW and compare survival distributions between intervention and control groups [47]. Log-Rank tests assessed differences in RTW times, while logistic regression explored potential predictors of RTW status, such as diagnosis and chemotherapy [49,50]. Work Ability Index (WAI) scores were categorized into predefined action groups (Poor, Moderate, Good, Excellent) [45]. Two-way mixed ANOVA was employed to evaluate the effects of group and time on WAI scores [49]. Additionally, Wilcoxon Signed Rank tests assessed within-group changes, and Mann-Whitney U tests compared baseline and follow-up distributions between groups. General Linear Models (GLM) were used to compare post-intervention scores between the iCanWork and control groups, adjusting for baseline values and examining interaction effects over time [47].For clinical quality of life outcomes, Mann-Whitney U tests were used to compare post-intervention scores (T2) between groups due to non-normal data distributions. Wilcoxon Signed Rank tests assessed within-group changes over time (T1 vs. T2).
3. Results
3.1. Participant Characteristics
A total of 23 participants were randomized, with 12 assigned to the iCanWork intervention group and 11 to the control group. The mean age was 45.6 years (SD = 9.01), with the majority being female (95.7%) and having completed higher education (78.2%). Breast cancer was the most common diagnosis (82.6%), and 78.3% of participants underwent chemotherapy. The mean duration from work leave to enrollment was 11.1 months (iCanWork = 9.75 months, Control = 12.5 months). The majority of participants were employed in occupations within professional health services, education, law, and social services, and business management fields, as categorized by the National Occupational Classification (NOC). No significant baseline differences in demographics or study variables were observed, except for Physical Function and Pain Interference, which were controlled for in subsequent analyses. Table 1 provides a full detail description of the study sample.
3.2. Feasibility
The feasibility benchmarks demonstrated strong outcomes across multiple metrics. The target sample size was 12 participants per group; by the end of the recruitment period, 12 participants were enrolled in the intervention group and 11 in the control group. Of the 25 self-referred participants, 23 met the inclusion criteria, agreed to participate, completed the baseline measure (T1), and were randomized, achieving a 92% recruitment rate. This exceeded the 50% recruitment benchmark at three months [51], and surpassed the 70% retention benchmark.
The overall retention rate, based on study questionnaire completion, was 83%. At the three-month (T2) follow-up, 100% of intervention participants and 63.6% (7/11) of control participants completed the questionnaire.
Intervention content fidelity was assessed through an independent review of all sessions delivered, conducted by the first two co-authors. Both the VR counsellor and the OT hired for the study received training in the iCanWork 10-steps intervention from the first two co-authors and successfully completed the accredited module of this intervention [52]. Notably, the OT hired was an experienced occupational therapist with over 20 years of practice in oncology. The review demonstrated that 90% of the session content was delivered as intended, with the content aim of each session highlighted in Figure 2, reflecting strong adherence to intervention protocols [51].
Regarding missing data, the intervention group had no missing responses, whereas the control group had higher rates of missing data at 23%, exceeding the acceptable threshold of 10% [51]. Yet, collectively, these findings demonstrate high feasibility and robust protocol adherence in the intervention group but suggest a need for adjustments to improve retention and data completion in the control group.
Participant Engagement and Benchmark Adherence
Table 2 provides a detailed summary of participant engagement with the intervention, specifically examining the delivery of VR counselling and OT sessions both before and after RTW. The before-RTW benchmark was defined as at least one VR session and one OT session, if deemed necessary. Similarly, the after-RTW benchmark required at least one VR session, one OT session, or both, depending on participant needs. The table highlights the extent to which participants met these benchmarks and illustrates the key challenges encountered during the study. These challenges included funding limitations, time constraints, scheduling difficulties, and the study’s conclusion before some participants attempted RTW.
In summary, 75% of participants met the session delivery benchmark before their RTW, while 41.7% met this benchmark after RTW. Key barriers to meeting post-RTW benchmarks included scheduling conflicts, participants not attempting RTW during the study period, and the study concluding before additional VR sessions could be provided. Participants P7, P8, and P11 were unable to complete the full intervention due to scheduling constraints and delays in attempting RTW. Similarly, participants P3, P6–P8, and P10–P12 did not receive post-RTW sessions for the same reasons. Notably, P11 and P12 expressed interest in additional VR sessions but were unable to receive them before the study concluded. These findings highlight the need for improved scheduling flexibility and extended study timelines to enhance intervention delivery and benchmark adherence after RTW.
3.3. Acceptability of the iCanWork Intervention
Participants reported high satisfaction with the iCanWork intervention, particularly highlighting the interventionist's listening skills, warmth, and non-critical attitude. On the Satisfaction with Therapist Scale (STTS-R) [39], 100% of participants agreed or strongly agreed with several items (Items 2, 4, 8, 10) (see Table 3 for full results). Overall satisfaction with the intervention, as measured by the Satisfaction with Therapy Scale (Item 1), was 75.0%, and 83.3% agreed that it helped address their specific problems (Item 13).
Participants in the control group reported noticeably lower satisfaction ratings across all items; however, responses were received from only 5 of the 11 participants, limiting the generalizability of these findings (Table 3). Satisfaction with the intervention (Item 1) was 40.0%, and perceived helpfulness of the intervention (Item 13) reached 80.0%. Lower ratings reflect limited engagement or perceived support within the intervention.
At six months post-enrollment, feedback was collected from the twelve participants in the iCanWork intervention through an open-ended question: "In what ways, if any, did the support received from the iCanWork intervention help you with your return to work?" Participants highlighted key areas where the intervention had a positive impact. Many reported feeling more confident in their ability to re-enter the workforce, attributing this to the program’s tailored support and guidance. Improved communication skills were also noted, as participants felt better equipped to articulate their needs and limitations to employers and colleagues. The program was described as instrumental in facilitating discussions about workplace accommodations, which contributed to smoother transitions back to work. Emotional support from the interventionist was frequently mentioned, helping participants manage anxiety and fear associated with returning to work. Additionally, practical strategies for managing workload and fatigue were highlighted as essential tools that enabled participants to navigate their return successfully. These qualitative insights illustrate the comprehensive benefits of the iCanWork intervention in addressing the complex challenges faced by ITBC in the process of returning to work.
3.4. Preliminary Efficacy
3.4.1. Return to Work Status
Table 4 presents the status and time to RTW by group allocation. At T2, 50% of participants in the iCanWork group returned to full-time work compared to 36.4% in the control group. Part-time RTW rates were 33.3% and 54.5%, respectively, while 16.7% of the iCanWork group and 9.1% of the control group did not return to work. Median time to RTW was 8 months for the iCanWork group and 11 months for the control group. Fisher’s Exact Test (p = 1.000) indicated no statistically significant difference in RTW rates between groups. Kaplan-Meier survival analysis revealed no significant difference in time to RTW between groups (Log-Rank test, p = 0.313).
3.4.2. Predictors of RTW
Logistic regression analysis examined age, diagnosis, chemotherapy, and patient-reported outcomes (physical function, anxiety, and pain interference) as predictors of RTW status. None of these variables were significant predictors (p > 0.05), likely due to the small sample size and variability in responses.
3.5. Work Ability Index (WAI)
Table 5 and Figure 3 provide an overview of Work Ability Index (WAI) scores at baseline (T1) and three months post-intervention (T2) for the iCanWork and Control groups. At T1, no significant differences were observed between the groups (U = 69.50, p = 0.833). The iCanWork group showed a slight increase in WAI scores from T1 to T2 (27.63 → 30.17), while the Control group exhibited a slight decrease (30.12 → 28.21). However, the Mann-Whitney U test at T2 revealed no significant group difference (U = 36.50, p = 0.650) (Table 5).
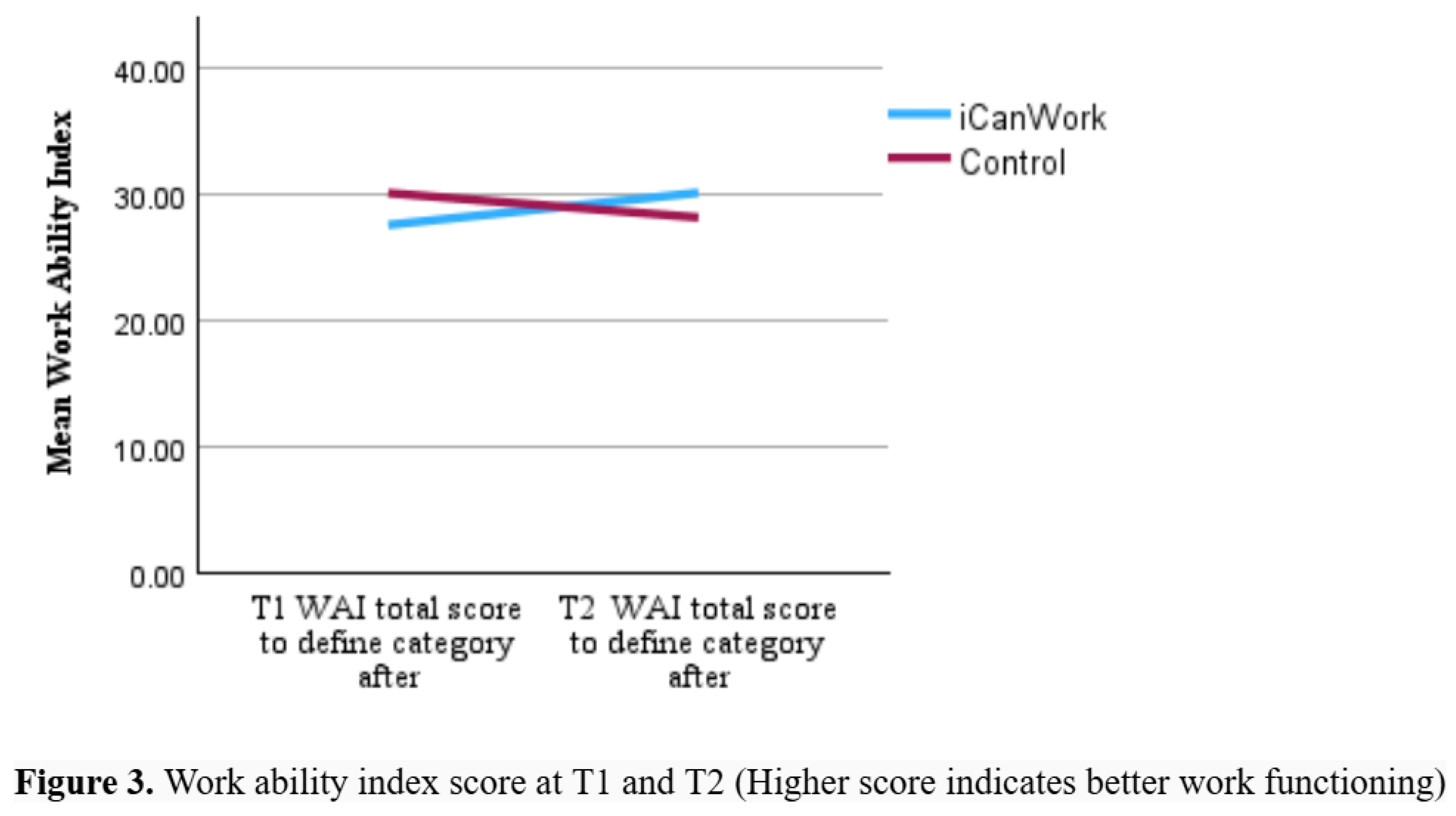
A two-way mixed ANOVA evaluated the effects of time (T1 vs. T2) and group (iCanWork vs. Control) on WAI scores. The analysis revealed no significant interaction between time and group (F(1,17) = 2.114, p = 0.164, ηp² = 0.111), indicating that changes in WAI scores over time did not differ significantly between groups. To provide further insights, WAI scores were categorized into four groups: Poor (7–27 points), Moderate (28–36 points), Good (37–43 points), and Excellent (44–49 points). Table 6 presents the distribution of participants in both groups falling within the Poor category (44.4% in iCanWork vs. 55.6% in Control). By T2, the proportion of participants in the Poor category increased to 71.4% in the iCanWork group but decreased to 28.6% in the Control group (Table 6).
Individual-level changes in WAI scores, as summarized in Table 7, reveal a mixed pattern of changes across both groups. In the iCanWork group, 50% of participants (6/12) demonstrated score improvements, while 5 participants experienced declines, and 1 participant remained unchanged.
A similar trend was observed in the Control group, where 3 participants improved, 3 showed declines, and 1 remained unchanged. Figure 2 visually illustrates these trends, showing a modest increase in mean WAI scores for the iCanWork group and a slight decrease for the Control group.
Despite these observations, the results highlight persistent work ability challenges in both groups over the three-month period. This underscores the need for extended follow-up and enhanced intervention strategies to achieve meaningful and sustained improvements in work ability among ITBC.
3.6. PROPr Domains
Table 8 presents a detailed overview of baseline and post-three months of the PROPr QoL seven domains for both study groups. Mann-Whitney U tests revealed significant differences between groups at T2 in Social Roles (p = 0.004), Pain Interference (p = 0.018), and Pain Intensity (p = 0.010). Participants in the iCanWork group reported higher Social Roles scores, while the control group had higher Pain Interference and Pain Intensity scores. No significant differences were observed for Physical Function, Anxiety, Depression, Fatigue, or Sleep Disturbance, though trends suggested potential group differences.
3.7. Specific Support Services Utilized Post-Consultation
Following their consultation, participants were recommended specific support services to address work functioning challenges and the impact of cancer and its treatment, including cancer-related fatigue and cognitive changes. These recommendations included physiotherapy and structured exercise programs for fatigue management, as well as referrals to physicians to investigate potential underlying biological causes. For cognitive changes, participants were advised to seek comprehensive assessments from a neuropsychologist or occupational therapist. At the three-month follow-up, 10 out of 12 participants in the intervention group reported utilizing services such as physiotherapy, occupational therapy, and osteopathy.
4. Discussion
This pilot randomized controlled trial of iCanWork provides important insights into the feasibility, acceptability, and preliminary efficacy of a multidisciplinary VR-led RTW intervention for ITBC, involving 23 participants—12 in the intervention group and 11 in the control group. The study demonstrated high feasibility, with a 92% recruitment rate and 83% retention rate, surpassing the established benchmarks for participant engagement. Participants rated iCanWork highly for its tailored support and helpfulness with VR guidance and OT services. While modest improvements were observed in work ability and quality of life measures, no statistically significant differences were found between the intervention and control groups. This highlights the need for a larger sample size and extended follow-up to better assess the intervention's effectiveness. Additionally, a more precise selection of measures that align with the intervention's impact, components, and intended outcomes is recommended to capture its true effects more accurately.
Comparison of iCanWork with Existing RTW Support Interventions
RTW interventions for ITBC vary widely in their structure, approach, and targeted outcomes. The iCanWork intervention uniquely integrates VR and OT within a flexible, person-centered framework, distinguishing it from existing models that focus solely on physical rehabilitation, employer training, or psychosocial counseling.
Compared to MiLES [53], which is employer-focused, iCanWork prioritizes worker-centered interventions, providing direct support to individuals rather than solely educating employers. Unlike Beyond Cancer [54], which focuses on long-term multimodal rehabilitation, iCanWork offers a structured yet adaptable VR and OT approach, ensuring personalized RTW planning. Similarly, Leensen et al. [55] combines occupational counseling with physical exercise, yet lacks the structured vocational assessment and workplace accommodations provided by iCanWork.
A major strength of iCanWork is its multidisciplinary stakeholder engagement, incorporating VR specialists, OTs, and work context and conditions data to comprehensively guide the RTW of ITBC. In contrast, Zaman et al. [46] emphasizes pre-treatment psychosocial counseling, while MiLES [53] focuses on employer education rather than direct survivor-centered work function support. Additionally, iCanWork supports individuals across all RTW stages, whereas Zovacevic et al. [56] emphasizes early prehabilitation and vocational reintegration, and Zaman et al. [46] primarily provides early work-related support before treatment.
Areas for Enhancement for iCanWork Based on Other RTW Interventions
While iCanWork presents several advantages, insights from other interventions suggest key areas for further development. One area of improvement is employer engagement, as seen in MiLES [53], which employs a web-based employer toolkit for workplace accommodations and phased RTW planning. iCanWork could benefit from developing an employer resource package to facilitate better workplace support, integration, and communication.
Another important enhancement is the integration of structured physical rehabilitation, as demonstrated in Leensen et al. [55,56]. Studies have shown that structured physical activity programs can improve RTW outcomes. Adding tailored exercise regimens or partnerships with physiotherapists could enhance fatigue management and physical function in iCanWork. Although the VR and OT professionals delivering iCanWork actively encourage participants to engage in physical activity and seek appropriate referrals, further strengthening these elements could optimize intervention outcomes. Specifically, participants are encouraged to consult a physiotherapist for a comprehensive assessment of physical limitations and rehabilitation needs, following obtaining medical clearance that engaging in physical activity is safe. Additionally, referrals to a kinesiologist are recommended to assist in developing a structured physical retraining program when necessary. These targeted efforts ensure that physical reconditioning is addressed as a core component of the RTW process, potentially mitigating cancer-related fatigue and improving functional capacity, thereby facilitating sustained workforce reintegration. By embedding structured physical rehabilitation within iCanWork, the intervention could provide a more holistic approach to addressing the multifaceted barriers cancer survivors face in returning to work.
Prehabilitation and early RTW screening are also valuable additions inspired by [56] and Zaman et al. [46]. Early intervention before treatment can improve RTW success. iCanWork could introduce prehabilitation assessments to identify work-related challenges early and develop pre-treatment vocational strategies to ensure a smoother reintegration process.
Finally, digital and remote RTW support, as utilized in iCanWork, MiLES [53], and Beyond Cancer [54], represents a significant strength of these approaches. The remote delivery of RTW interventions via Zoom, particularly through iCanWork’s telehealth model integrating VR and OT, improves accessibility for individuals in rural areas or those with mobility limitations. This flexible, individualized format effectively accommodates the diverse needs of ILWC.
Building upon this strength, integrating a digital component, such as a mobile application, could enhance intervention engagement by enabling participants to self-track their work ability, monitor progress, and receive tailored recommendations based on their evolving needs. The team at Cancer and Work is currently developing a digital AI-driven solution for delivering iCanWork, aiming to provide interactive, personalized support beyond live sessions. This innovation would not only improve scalability but also foster greater participant autonomy in managing their RTW journey while maintaining the high level of personalized support that is integral to iCanWork’s success.
Additionally, the Cancer and Work team has developed and validated the Cancer and Work Scale (CAWSE), a critical tool in oncology-specific vocational rehabilitation (in press). The CAWSE fills a significant gap in current RTW interventions by providing healthcare providers with a validated, oncology-focused assessment tool that enables targeted interventions to enhance RTW outcomes and long-term employment sustainability for individuals transitioning back to work (ITBC). Its integration into digital platforms could further streamline RTW assessments and personalize support strategies to optimize employment retention for cancer survivors.
Implications for Future Research & Policy
The persistence of poor work ability scores in both groups at follow-up highlights the need for prolonged support and extended RTW interventions. Future studies should incorporate extended follow-up periods to assess long-term employment sustainability. Additionally, the introduction of a partial disability program could provide ITBC with structured, gradual reintegration opportunities that balance work demands with ongoing health challenges.
Another key recommendation is a better selection of outcome measures that are more closely aligned with iCanWork’s potential areas of impact. While work ability remains a critical indicator, future studies should integrate measures that capture broader psychosocial and functional dimensions of RTW success, including sense of self-efficacy, autonomy, readiness for RTW, knowledge of workplace accommodations, meaning of work, and financial impact [57,58], and such as the tool CAWSE (in press). These domains are often integral to the RTW process for ITBC and could provide a more nuanced understanding of the intervention’s benefits.
Moreover, developing an AI-enhanced active control group could improve the comparability of future trials. Leveraging AI-based guidance using structured resources from the Cancer and Work website could offer scalable and interactive support for control participants. This approach would ensure a more rigorous evaluation of intervention effectiveness while maintaining ethical considerations by providing meaningful guidance to all study participants.
Conclusion
The iCanWork intervention demonstrates high feasibility and acceptability, with promising trends in work ability and QoL improvements. However, the lack of statistically significant differences suggests the need for larger, adequately powered trials, further intervention refinements, and better targeted measures to the intervention’ potential impact. Enhancing employer engagement, integrating structured physical rehabilitation, incorporating prehabilitation RTW screening, and expanding digital support tools could strengthen the intervention’s effectiveness and scalability. By addressing these gaps, iCanWork has the potential to become a comprehensive and sustainable RTW solution for individuals touched by cancer.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org; Table S1: CONSORT 2010 checklist of information to include when reporting a pilot or feasibility trial. Table S2: The template for intervention description and replication (TIDieR) checklist. Supplementary document S1: Examples of intake sessions and summary notes from the VR and OT hired for the study.
Author Contributions
Conceptualization, C.M. and M.P.; methodology, C.M. M.P., and N.D.; intervention fidelity and supervision, C.M. M.P., and K.J.; formal analysis, C.M., M.S., W.L.T., and N.D., and M.S.; investigation, C.M., M.P., K.J., W.L.T., N.D., and M.S.; resources, C.M., M.P., K.J., W.L.T., and N.D.; data curation, C.M., W.L.T., and N.D.; writing—original draft preparation, C.M., M.P., K.J., W.L.T., N.D., and M.S.; writing—review and editing, C.M., M.P., K.J., W.L.T., N.D., and M.S.; visualization, C.M., W.L.T., and N.D.; supervision, C.M. M.P, and K.J.; project administration, C.M., M.P., K.J., W.L.T., N.D., and M.S.; funding acquisition, C.M. All authors have read and agreed to the published version of the manuscript.
Funding
The study was funded by the Work Wellness Institute, awarded to authors C. Maheu and M. Parkinson.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Research Ethics Boards from the author C. Maheu primary scientist affiliation site McGill University Health Centre (protocol number: MP-2022-8238, approval dates: March 2022 and April 2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available upon reasonable request from the corresponding author. Due to the sensitive nature of health and vocational implications, as well as the potential risks of bias and stigmatization, access to the data is restricted.
Acknowledgments
The authors sincerely thank all the participants who generously gave their time and effort to contribute to the creation and assessment of the iCanWork program: a RTW intervention support for ILWC. Their invaluable insights and experiences have been essential in establishing iCanWork as a promising RTW intervention for ILWC.
Conflicts of Interest
All authors acknowledge having no conflicts of interest to declare. The funders had no role in the study design, data collection, and analysis, the decision to publish, or the preparation of the manuscript.
Abbreviations
The following abbreviations are used in this manuscript:
AI – Artificial Intelligence
ANOVA – Analysis of Variance
CAWSE – Cancer and Work Scale
CFIR – Consolidated Framework for Implementation Research
CONSORT – Consolidated Standards of Reporting Trials
ILWC – Individuals Living with Cancer
ITBC – Individuals Touched by Cancer
NOC – National Occupational Classification
NPT – Normalization Process Theory
OT – Occupational Therapy
PROM – Patient-Reported Outcome Measure
QoL – Quality of Life
RCT – Randomized Controlled Trial
RTW – Return to Work
STTS-R – Satisfaction with Therapy and Therapist Scale-Revised
TIDieR – Template for Intervention Description and Replication
VR – Vocational Rehabilitation
WAI – Work Ability Index
References
- Maheu, C., Parkinson, M., Wong, C., Yashmin, F., and Longpré, C. (2023). Self-Employed Canadians’ Experiences with Cancer and Work: A Qualitative Study. Curr. Oncol. 30, 4586–4602. [CrossRef]
- Sabariego, M., Rosas, M., Piludu, M.A., Acquas, E., Giorgi, O., and Corda, M.G. (2019). Active avoidance learning differentially activates ERK phosphorylation in the primary auditory and visual cortices of Roman high- and low-avoidance rats. Physiol. Behav. 201, 31–41. [CrossRef]
- Skivington, K., Lifshen, M., and Mustard, C. (2016). Implementing a collaborative return-to-work program: Lessons from a qualitative study in a large Canadian healthcare organization. Work 55, 613–624. [CrossRef]
- Fitch, M.I., and Nicoll, I. (2019). Returning to work after cancer: Survivors’, caregivers’, and employers’ perspectives. Psychooncology 28, 792–798.
- de Boer, A.G., Torp, S., Popa, A., Horsboel, T., Zadnik, V., Rottenberg, Y., Bardi, E., Bultmann, U., and Sharp, L. (2020). Long-term work retention after treatment for cancer: a systematic review and meta-analysis. J. Cancer Surviv. 14, 135–150. [CrossRef]
- de Boer, A.G.E.M., and Frings-Dresen, M.H.W. (2009). Employment and the common cancers: return to work of cancer survivors. Occup Med (Lond) 59, 378–380. [CrossRef]
- Short, P.F., Vasey, J.J., and Tunceli, K. (2005). Employment pathways in a large cohort of adult cancer survivors. Cancer 103, 1292–1301. [CrossRef]
- Sumari, M., Mohd Kassim, N., and A.Razak, N.A. (2022). A conceptualisation of resilience among cancer surviving employed women in malaysia. TQR. [CrossRef]
- Molinero, R.G., González, P.R., Zayas, A., and Guil, R. (2019). Resilience and workability among breast cancer survivors. Journal of Developmental and Educational Psychology. Revista INFAD de Psicología. 1.
- de Rijk, A., Amir, Z., Cohen, M., Furlan, T., Godderis, L., Knezevic, B., Miglioretti, M., Munir, F., Popa, A.E., Sedlakova, M., et al. (2020). The challenge of return to work in workers with cancer: employer priorities despite variation in social policies related to work and health. J. Cancer Surviv. 14, 188–199. [CrossRef]
- Greidanus, M.A., Tamminga, S.J., de Rijk, A.E., Frings-Dresen, M.H.W., and de Boer, A.G.E.M. (2019). What Employer Actions Are Considered Most Important for the Return to Work of Employees with Cancer? A Delphi Study Among Employees and Employers. J. Occup. Rehabil. 29, 406–422. [CrossRef]
- Awang, H., Tan, L.Y., Mansor, N., Tongkumchum, P., and Eso, M. (2017). Factors related to successful return to work following multidisciplinary rehabilitation. J. Rehabil. Med. 49, 520. [CrossRef]
- Iragorri, N., de Oliveira, C., Fitzgerald, N., and Essue, B. (2021). The indirect cost burden of cancer care in canada: A systematic literature review. Appl. Health Econ. Health Policy 19, 325–341. [CrossRef]
- Paltrinieri, S., Fugazzaro, S., Bertozzi, L., Bassi, M.C., Pellegrini, M., Vicentini, M., Mazzini, E., and Costi, S. (2018). Return to work in European Cancer survivors: a systematic review. Support. Care Cancer 26, 2983–2994. [CrossRef]
- Canadian Cancer Society (2024). Canadian Cancer Statistics Advisory Committee in collaboration with the Canadian Cancer Society, Statistics Canada and the Public Health Agency of Canada. Canadian Cancer Statistics: A 2024 special report on the economic impact of cancer in Canada (Toronto, ON, Canada: Canadian Cancer Society).
- de Boer, A.G.E.M., Taskila, T., Ojajärvi, A., van Dijk, F.J.H., and Verbeek, J.H.A.M. (2009). Cancer survivors and unemployment: a meta-analysis and meta-regression. JAMA 301, 753–762.
- de Boer, A.G., Tamminga, S.J., Boschman, J.S., and Hoving, J.L. (2024). Non-medical interventions to enhance return to work for people with cancer. Cochrane Database Syst. Rev. 3, CD007569. [CrossRef]
- Lamore, K., Dubois, T., Rothe, U., Leonardi, M., Girard, I., Manuwald, U., Nazarov, S., Silvaggi, F., Guastafierro, E., Scaratti, C., et al. (2019). Return to work interventions for cancer survivors: A systematic review and a methodological critique. Int. J. Environ. Res. Public Health 16, 1–21. [CrossRef]
- Parkinson, M., and Maheu, C. (2019). Cancer and Work . Canadian Oncology Nursing Journal / Revue canadienne de soins infirmiers en oncologie 29, 258–266.
- Maheu, C., Parkinson, M., Oldfield, M., Kita-Stergiou, M., Bernstein, L., Esplen, M.J., Hernandez, C., Zanchetta, M., Singh, M., and on behalf of the Cancer and Work core team members (2016). Cancer and Work. Cancer and Work. Available at: https://www.cancerandwork.ca/ [Accessed August 4, 2021].
- Parkinson, M., and Maheu, C. (2022). Supporting patients surviving cancer with return to work. www.fpon.ca, 4–5, 13. Available at: http://www.bccancer.bc.ca/health-professionals/networks/family-practice-oncology-network/journal-of-family-practice-oncology [Accessed July 23, 2022].
- Maheu, C., Kocum, L., Parkinson, M., Robinson, L., Bernstein, L.J., Zanchetta, M.S., Singh, M., Hernandez, C., Yashmin, F., and Esplen, M.J. (2021). Evaluation of usability and satisfaction of two online tools to guide return to work for cancer survivors on the cancer and work website. J. Occup. Rehabil. [CrossRef]
- Maheu, C., Parkinson, M., Oldfield, M., Kita-Stergiou, M., Bernstein, L., Esplen, M.J., Hernandez, C., Zanchetta, M., Singh, M., and on behalf of the Cancer and Work core team members. Checklist adapted for the Cancer and Work website (2016). Cancer and Work Cognitive Symptoms at Work Checklist. Cancer and Work. Available at: https://www.cancerandwork.ca/ [Accessed February 4, 2025].
- Ottati, A., and Feuerstein, M. (2013). Brief self-report measure of work-related cognitive limitations in breast cancer survivors. J. Cancer Surviv. 7, 262–273. [CrossRef]
- Nitkin, P., Parkinson, M., and Schultz, I.Z. (2011). Cancer and work – A Canadian perspective. Canadian Association of Psychological Oncology. Canadian Association of Psycho-Oncology.
- Maheu, C., Parkinson, M., Oldfield, M., Kita-Stergiou, M., Bernstein, L., Hernandez, C., Singh, M., Esplen, M.-J., Zanchetta, M., and on behalf of the Cancer and Work core team members (2020). Development and initial evaluation of the Cancer and Work website to provide a valuable resource to return to work after cancer. Submitted.
- Parkinson, M., and Maheu, C. (2024). Navigating return to work cancer survivor: Supportive strategies and insights. Plans & Trusts 42, 16–22.
- Parkinson, M., and Maheu, C. (2019). Cancer and work. Can. Oncol. Nurs. J. 29, 258–266.
- Tamminga, S.J., de Boer, A.G.E.M., Verbeek, J.H.A.M., and Frings-Dresen, M.H.W. (2010). Return-to-work interventions integrated into cancer care: a systematic review. Occup. Environ. Med. 67, 639–648.
- de Boer, A.G., Taskila, T., Tamminga, S.J., Frings-Dresen, M.H., Feuerstein, M., and Verbeek, J.H. (2011). Interventions to enhance return-to-work for cancer patients. Cochrane Database Syst. Rev., CD007569.
- de Boer, A.G.E.M., Greidanus, M.A., Dewa, C.S., Duijts, S.F.A., and Tamminga, S.J. (2020). Introduction to special section on: current topics in cancer survivorship and work. J. Cancer Surviv. 14, 101–105. [CrossRef]
- Eldridge, S.M., Chan, C.L., Campbell, M.J., Bond, C.M., Hopewell, S., Thabane, L., Lancaster, G.A., and PAFS consensus group (2016). CONSORT 2010 statement: extension to randomised pilot and feasibility trials. Pilot Feasibility Stud. 2, 64. [CrossRef]
- Hoffmann, T.C., Glasziou, P.P., Boutron, I., Milne, R., Perera, R., Moher, D., Altman, D.G., Barbour, V., Macdonald, H., Johnston, M., et al. (2014). Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ 348, g1687. [CrossRef]
- Sim, J., and Lewis, M. (2012). The size of a pilot study for a clinical trial should be calculated in relation to considerations of precision and efficiency. J. Clin. Epidemiol. 65, 301–308. [CrossRef]
- Julious, S.A. (2005). Sample size of 12 per group rule of thumb for a pilot study. Pharm. Stat. 4, 287–291. [CrossRef]
- Eysenbach, G. (2013). CONSORT-EHEALTH: implementation of a checklist for authors and editors to improve reporting of web-based and mobile randomized controlled trials. Stud. Health Technol. Inform. 192, 657–661.
- Eysenbach, G., and CONSORT-EHEALTH Group (2011). CONSORT-EHEALTH: improving and standardizing evaluation reports of Web-based and mobile health interventions. J. Med. Internet Res. 13, e126.
- Sheill, G., Guinan, E., Brady, L., Hevey, D., and Hussey, J. (2019). Exercise interventions for patients with advanced cancer: A systematic review of recruitment, attrition, and exercise adherence rates. Palliat. Support. Care 17, 686–696. [CrossRef]
- Oei, T.P., and Shuttlewood, G.J. (1999). Development of a satisfaction with therapy and therapist Scale. Aust. N. Z. J. Psychiatry 33, 748–753.
- Sidani, S., Epstein, D.R., and Fox, M. (2017). Psychometric evaluation of a multi-dimensional measure of satisfaction with behavioral interventions. Res. Nurs. Health 40, 459–469. [CrossRef]
- Eze, A., Anyebe, M.O., Nnamani, R.G., Nwaogaidu, J.C., Mmegwa, P.U., Akubo, E.A., Bako, V.N., Ishaya, S.N., Eze, M.I., Ekwueme, F.O., et al. (2023). Online cognitive-behavioral intervention for stress among English as a second language teachers: implications for school health policy. Front. Psychiatry 14, 1140300. [CrossRef]
- de Boer, A.G.E.M., Verbeek, J.H.A.M., Spelten, E.R., Uitterhoeve, A.L.J., Ansink, A.C., de Reijke, T.M., Kammeijer, M., Sprangers, M.A.G., and van Dijk, F.J.H. (2008). Work ability and return-to-work in cancer patients. Br. J. Cancer 98, 1342–1347. [CrossRef]
- Stapelfeldt, C.M., Momsen, A.-M.H., Jensen, A.B., Andersen, N.T., and Nielsen, C.V. (2021). Municipal return to work management in cancer survivors: a controlled intervention study. Acta Oncol. 60, 370–378. [CrossRef]
- Tamminga, S.J., Verbeek, J.H.A.M., Bos, M.M.E.M., Fons, G., Kitzen, J.J.E.M., Plaisier, P.W., Frings-Dresen, M.H.W., and de Boer, A.G.E.M. (2019). Two-Year Follow-Up of a Multi-centre Randomized Controlled Trial to Study Effectiveness of a Hospital-Based Work Support Intervention for Cancer Patients. J. Occup. Rehabil. 29, 701–710. [CrossRef]
- Ilmarinen, J. (2006). The Work Ability Index (WAI). Occup Med (Lond) 57, 160–160. [CrossRef]
- Zaman, A.C.G.N.M., Tytgat, K.M.A.J., Klinkenbijl, J.H.G., Boer, F.C. den, Brink, M.A., Brinkhuis, J.C., Bruinvels, D.J., Dol, L.C.M., van Duijvendijk, P., Hemmer, P.H.J., et al. (2021). Effectiveness of a Tailored Work-Related Support Intervention for Patients Diagnosed with Gastrointestinal Cancer: A Multicenter Randomized Controlled Trial. J. Occup. Rehabil. 31, 323–338. [CrossRef]
- Tamminga, S.J., Verbeek, J.H.A.M., Bos, M.M.E.M., Fons, G., Kitzen, J.J.E.M., Plaisier, P.W., Frings-Dresen, M.H.W., and de Boer, A.G.E.M. (2013). Effectiveness of a hospital-based work support intervention for female cancer patients - a multi-centre randomised controlled trial. PLoS ONE 8, e63271. [CrossRef]
- Nekhlyudov, L., Campbell, G.B., Schmitz, K.H., Brooks, G.A., Kumar, A.J., Ganz, P.A., and Von Ah, D. (2022). Cancer-related impairments and functional limitations among long-term cancer survivors: Gaps and opportunities for clinical practice. Cancer 128, 222–229. [CrossRef]
- Munir, F., Yarker, J., and McDermott, H. (2009). Employment and the common cancers: correlates of work ability during or following cancer treatment. Occup Med (Lond) 59, 381–389. [CrossRef]
- de Boer, A.G.E.M., de Wind, A., Coenen, P., van Ommen, F., Greidanus, M.A., Zegers, A.D., Duijts, S.F.A., and Tamminga, S.J. (2023). Cancer survivors and adverse work outcomes: associated factors and supportive interventions. Br. Med. Bull. 145, 60–71. [CrossRef]
- Leensen, M.C.J., Groeneveld, I.F., van der Heide, I., Rejda, T., van Veldhoven, P.L.J., Berkel, S. van, Snoek, A., Harten, W. van, Frings-Dresen, M.H.W., and de Boer, A.G.E.M. (2017). Return to work of cancer patients after a multidisciplinary intervention including occupational counselling and physical exercise in cancer patients: a prospective study in the Netherlands. BMJ Open 7, e014746. [CrossRef]
- Maheu, C., and Parkinson, M. (2021). Supporting cancer survivors with return to work e-course for primary care providers. www.fpon.ca, 2, 13. Available at: http://www.bccancer.bc.ca/family-oncology-network-site/Documents/2021SpringFPONjournal_Apr29web.pdf [Accessed July 21, 2022].
- Greidanus, M.A., de Boer, A.G.E.M., de Rijk, A.E., Frings-Dresen, M.H.W., and Tamminga, S.J. (2020). The MiLES intervention targeting employers to promote successful return to work of employees with cancer: design of a pilot randomised controlled trial. Trials 21, 363. [CrossRef]
- Sheppard, D.M., Frost, D., Jefford, M., O’Connor, M., and Halkett, G. (2020). Building a novel occupational rehabilitation program to support cancer survivors to return to health, wellness, and work in Australia. J. Cancer Surviv. 14, 31–35. [CrossRef]
- Leensen, M.C.J., Groeneveld, I.F., Rejda, T., Groenenboom, P., van Berkel, S., Brandon, T., de Boer, A.G.E.M., and Frings-Dresen, M.H.W. (2018). Feasibility of a multidisciplinary intervention to help cancer patients return to work. Eur J Cancer Care (Engl) 27, e12690. [CrossRef]
- Kovacevic, N., Žagar, T., Homar, V., Pelhan, B., Sremec, M., Rozman, T., and Besic, N. (2024). Benefits of early integrated and vocational rehabilitation in breast cancer on work ability, sick leave duration, and disability rates. Healthcare (Basel) 12. [CrossRef]
- Rath, H.M., Steimann, M., Ullrich, A., Rotsch, M., Zurborn, K.-H., Koch, U., Kriston, L., and Bergelt, C. (2015). Psychometric properties of the Occupational Stress and Coping Inventory (AVEM) in a cancer population. Acta Oncol. 54, 232–242. [CrossRef]
- Greidanus, M.A., de Boer, A.G.E.M., de Rijk, A.E., Brouwers, S., de Reijke, T.M., Kersten, M.J., Klinkenbijl, J.H.G., Lalisang, R.I., Lindeboom, R., Zondervan, P.J., et al. (2020). The Successful Return-To-Work Questionnaire for Cancer Survivors (I-RTW_CS): Development, Validity and Reproducibility. Patient 13, 567–582. [CrossRef]
Figure 1.
Cancer and Work: Four Factors Vocational Rehabilitation Model for Individuals Living with Cancer. Note: Revised from the original model, “Vocational Rehabilitation Model for Cancer Survivors” [19].
Figure 1.
Cancer and Work: Four Factors Vocational Rehabilitation Model for Individuals Living with Cancer. Note: Revised from the original model, “Vocational Rehabilitation Model for Cancer Survivors” [19].
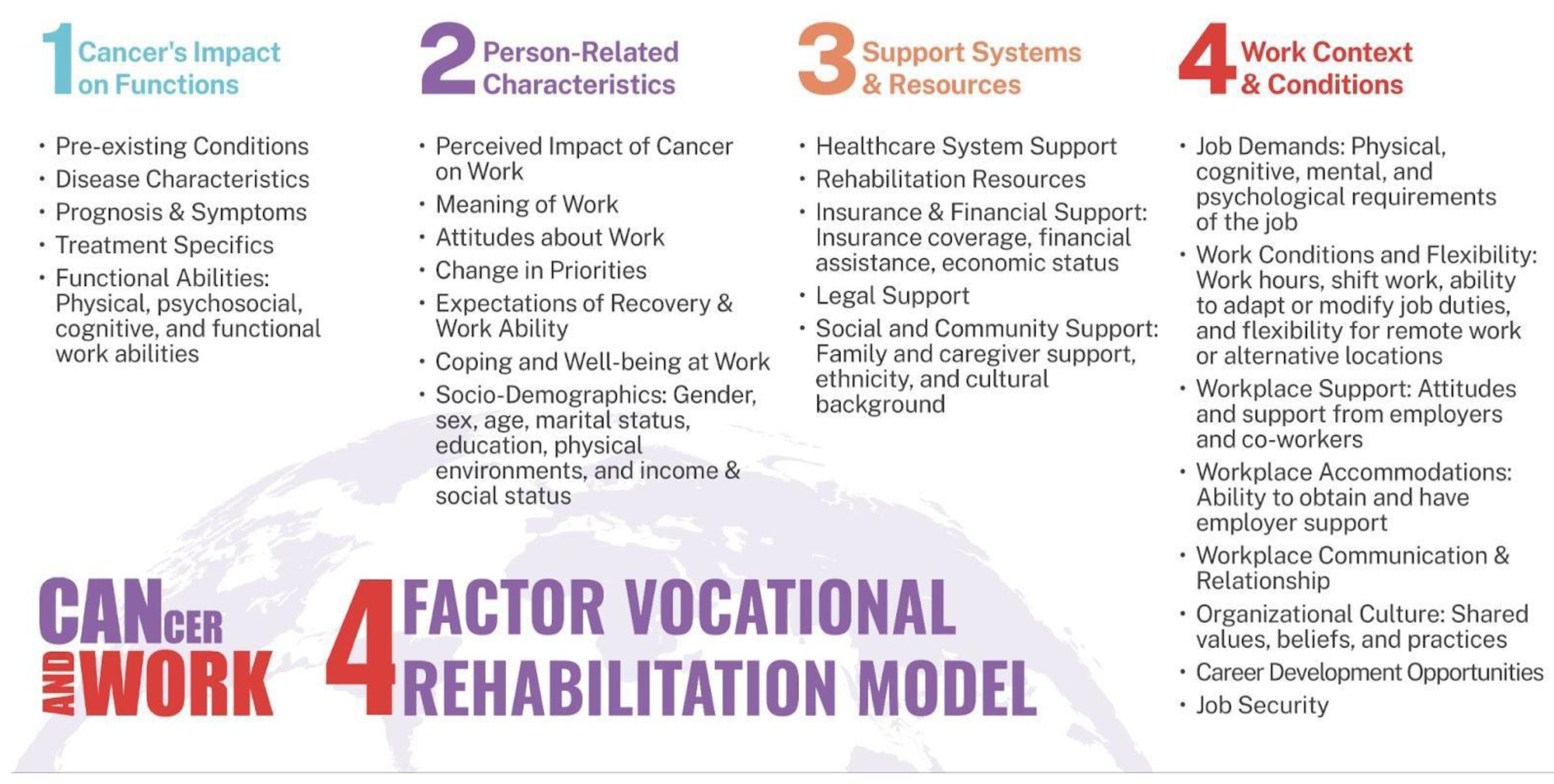
Figure 2.
iCanWork intervention components.
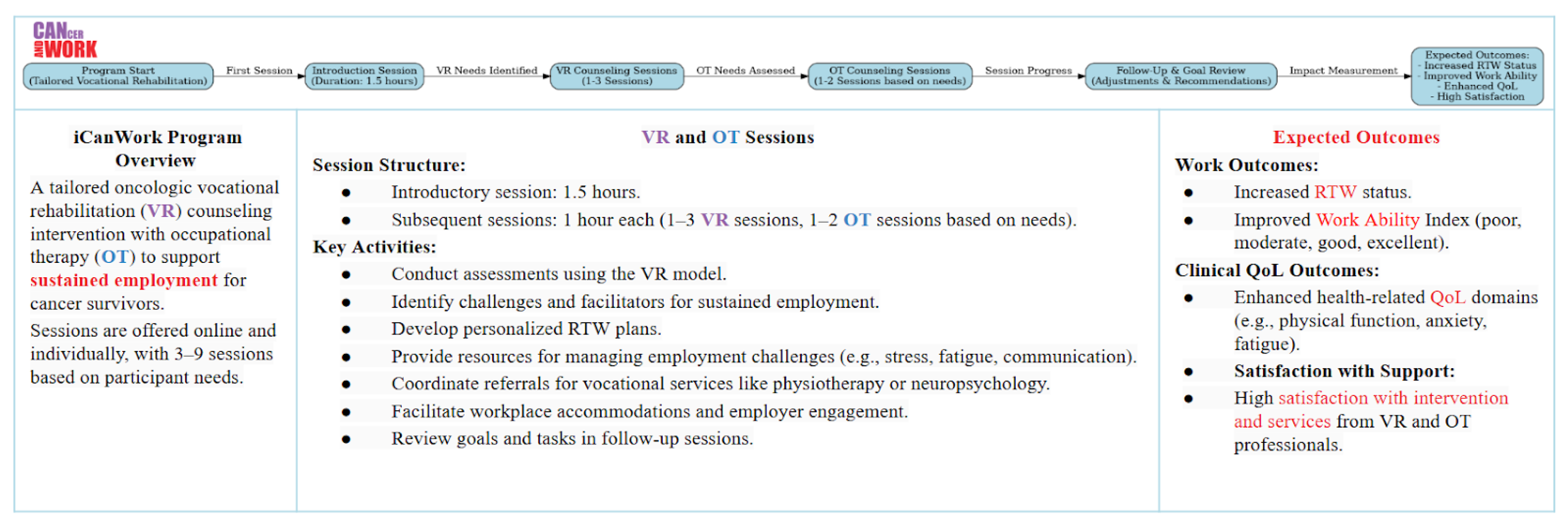

Table 1.
Participant Demographic and Clinical CharacteristicsNote. There were no significant differences between the two groups at baseline.
Table 1.
Participant Demographic and Clinical CharacteristicsNote. There were no significant differences between the two groups at baseline.
| Variable | iCanWork (n = 12) | Control (n = 11) | Total (N = 23) |
|---|---|---|---|
| Age (years) | Mean (SD): 43.08 ± 9.22 |
Mean (SD): 48.27 ± 8.34 |
Mean (SD): 45.57 ± 9.01 |
| Months to RTW | Mean (SD): 9.75 ± 5.34 |
Mean (SD): 12.55 ± 6.56 |
Mean (SD): 11.09 ± 5.99 |
| Gender | |||
| Women | 12 (100.0%) | 10 (90.9%) | 22 (95.7%) |
| Men | 0 (0.0%) | 1 (9.1%) | 1 (4.3%) |
| Marital Status | |||
| Married/Common law | 10 (62.5%) | 6 (37.5%) | 16 (69.6%) |
| Never Married | 2 (50.0%) | 2 (50.0%) | 4 (17.4%) |
| Separated | 0 (0.0%) | 2 (100.0%) | 2 (8.7%) |
| Other | 0 (0.0%) | 1 (100.0%) | 1 (4.3%) |
| Education | |||
| Less than High School | 0 (0.0%) | 1 (100.0%) | 1 (4.3%) |
| High School Graduate | 1 (100.0%) | 0 (0.0%) | 1 (4.3%) |
| Some College | 1 (33.3%) | 2 (66.7%) | 3 (13.0%) |
| University/College Graduate | 6 (46.2%) | 7 (53.8%) | 13 (56.5%) |
| Postgraduate | 4 (80.0%) | 1 (20.0%) | 5 (21.7%) |
| Diagnosis | |||
| Breast Cancer | 11 (91.7%) | 8 (72.7%) | 19 (82.6%) |
| Non-Hodgkin Lymphoma | 1 (8.3%) | 2 (18.2%) | 3 (13.0%) |
| Oral Cancer | 0 (0.0%) | 1 (9.1%) | 1 (4.3%) |
| Treatment | |||
| Chemotherapy (Yes) | 9 (75.0%) | 9 (81.8%) | 18 (78.3%) |
| Radiation (Yes) | 5 (41.7%) | 5 (45.5%) | 10 (43.5%) |
| Occupation (NOC) | |||
| 3114 – Professional health services | 2 (16.7%) | 0 (0.0%) | 2 (8.7%) |
| 1228 – Employment insurance | 1 (8.3%) | 0 (0.0%) | 1 (4.3%) |
| 0124 – Advertising, marketing | 1 (8.3%) | 0 (0.0%) | 1 (4.3%) |
| Occupations in education, law | 4 (33.3%) | 0 (0.0%) | 4 (17.4%) |
| 1253 – Records management | 2 (16.7%) | 4 (36.4%) | 6 (26.1%) |
| 0311 – Business managers | 2 (16.7%) | 3 (27.3%) | 5 (21.7%) |
| 1223 – Human resources | 0 (0.0%) | 1 (9.1%) | 1 (4.3%) |
| 1222 – Executive assistants | 0 (0.0%) | 1 (9.1%) | 1 (4.3%) |
| 6552 – Customer service | 0 (0.0%) | 1 (9.1%) | 1 (4.3%) |
| 4021 – College and instructors | 0 (0.0%) | 1 (9.1%) | 1 (4.3%) |
Table 2.
Participant Intervention Summary VR and OT Sessions .
| ID | Before RTW | After RTW | Reasons |
|---|---|---|---|
| P1 | 1 VR | 2 VR | Met the benchmark for before and after RTW. |
| P2 | 2 VR, 1 OT | 1 VR | Met the benchmark for before and after RTW. |
| P3 | 2 VR, 1 OT | 0 | Met before RTW; after RTW unmet due to scheduling issues. |
| P4 | 1 VR, 1 OT | 1 VR | Met the benchmark for before and after RTW. |
| P5 | 1 VR, 1 OT | 1 VR | Met the benchmark for before and after RTW. |
| P6 | 2 VR, 1 OT | 0 | Met before RTW; after RTW unmet due to scheduling issues. |
| P7 | 2 VR, 0 OT | 0 | Met before RTW; OT not delivered despite attempts. RTW not attempted. |
| P8 | 2 VR, 1 OT | 0 | Met before RTW; RTW not attempted during study time frame. |
| P9 | 1 VR, 1 OT | 1 VR | Met the benchmark for before and after RTW. |
| P10 | 2 VR, 1 OT | 0 | Met before RTW; RTW not attempted during study time frame. |
| P11 | 1 VR | 0 | Met before RTW; study ended before additional VR could occur. |
| P12 | 1 VR | 0 | Met before RTW; study ended before additional VR could occur. |
Table 3.
Participant Satisfaction with the iCanWork Intervention and Therapist (STTS-R) [33].
Table 3.
Participant Satisfaction with the iCanWork Intervention and Therapist (STTS-R) [33].
| Domain | Item | Intervention Count Agree (%) (n = 12) | Control Count Agree (%) (n = 5) |
|---|---|---|---|
| Satisfaction with Intervention | I am satisfied with the quality of the intervention I received (Item 1) | 9 (75.0%) | 2 (40.0%) |
| The interventionist listened to what I was trying to say (Item 2) | 12 (100.0%) | 2 (40.0%) | |
| My needs were met by the program (Item 3) | 8 (66.7%) | 2 (40.0%) | |
| The interventionist provided an adequate explanation (Item 4) | 12 (100.0%) | 2 (40.0%) | |
| I would recommend the program to a friend (Item 5) | 9 (75.0%) | 2 (40.0%) | |
| The interventionist was not negative or critical towards me (Item 6) | 9 (75.0%) | 2 (40.0%) | |
| I would return to the program if I needed help (Item 7) | 9 (75.0%) | 2 (40.0%) | |
| Satisfaction with Therapist | The interventionist was friendly and warm towards me (Item 8) | 12 (100.0%) | 2 (40.0%) |
| I am now able to deal more effectively with my problems (Item 9) | 5 (41.7%) | 2 (40.0%) | |
| I felt free to express myself (Item 10) | 12 (100.0%) | 2 (40.0%) | |
| I was able to focus on what was of real concern to me (Item 11) | 10 (83.3%) | 2 (40.0%) | |
| The interventionist seemed to understand what I was thinking and feeling (Item 12) | 9 (75.0%) | 2 (40.0%) | |
| Perceived Changes in Condition | How much did this intervention help with the specific problems that led you to the program? (Item 13) | 10 (83.3%) | 4 (80.0%) |
Table 4.
Status and Time to RTW by Group Allocation (T2).
| RTW Status | iCanWork (n = 12) | Control (n = 11) | Total (n = 23) |
|---|---|---|---|
| Returned Full-Time | 6 (50.0%) | 4 (36.4%) | 10 (43.5%) |
| Returned Part-Time | 4 (33.3%) | 6 (54.5%) | 10 (43.5%) |
| Did Not Return to Work | 2 (16.7%) | 1 (9.1%) | 3 (13.0%) |
| Median Time to RTW (months) | 8.0 | 11.00 | 11.0 |
| Mean Time to RTW (months) | 10.4 | 13.5 | 12.1 |
Note: Median Time to RTW: Reflects the time by which 50% of participants in each group returned to work. This value highlights the central tendency of RTW. Mean Time to RTW: Indicates the average time to RTW for each group. The mean provides additional context but may be influenced by outliers.
Table 5.
Work Ability Index at T1 and T2.
| Outcomes And Instruments | Group | Baseline (T1) Mean (SD) (n) |
3 Months Follow-up (T2) Mean (SD) (n) |
P-value |
|---|---|---|---|---|
| Overall Work Ability (7-49) |
Intervention | 27.63 (1.37) (n=12) | 30.17 (2.02) (n=12) | 0.111 |
| Control | 30.12 (1.7) (n=11) | 28.21 (2.65) (n=7) |
Table 6.
Work Ability Categories at T1 and T2.
| Time | WAI Category | iCanWork (n, %) |
Control (n, %) | Total (n) | Mann-Whitney U | Exact p-value |
|---|---|---|---|---|---|---|
| T1 | Poor (7–27 points) | 4 (44.4%) | 5 (55.6%) | 9 | ||
| Moderate (28–36 points) | 7 (58.3%) | 5 (41.7%) | 12 | |||
| Good (37–43 points) | 1 (50.0%) | 1 (50.0%) | 2 | 69.50 | 0.33 | |
| T2 | Poor (7–27 points) | 5 (71.4%) | 2 (28.6%) | 7 | ||
| Moderate (28–36 points) | 5 (55.6%) | 4 (44.4%) | 9 | |||
| Good (37–43 points) | 2 (66.7%) | 1 (33.3%) | 3 | 36.50 | 0.650 |
Table 7.
Work Ability Score Changed Observed at T2.
| Group | N Total | Increased Scores | Decreased Scores | Unchanged Scores |
|---|---|---|---|---|
| iCanWork | 12 | 6 | 5 | 1 |
| Control | 7 | 3 | 3 | 1 |
Table 8.
PROPr QoL domains .
| Domain | Group | Baseline Mean (SD) (T1) | Three months post- baseline (T2) Mean (SD) |
p-value (Within Group) | p-value (Between Groups) |
|---|---|---|---|---|---|
| Physical Function | iCanWork | 50.93 ± 7.845 | 50.89 ± 7.103 | 0.799 | |
| Control | 42.95 ± 6.783 | 44.31 ± 5.818 | 0.116 | 0.995 | |
| Anxiety | iCanWork | 58.75 ± 7.30 | 57.25 ± 6.70 | 0.423 | |
| Control | 59.21 ± 8.78 | 60.71 ± 9.78 | 0.753 | 0.574 | |
| Depression | iCanWork | 51.70 ± 8.05 | 53.44 ± 6.95 | 0.423 | |
| Control | 54.75 ± 9.58 | 59.11 ± 9.91 | 0.753 | 0.280 | |
| Fatigue | iCanWork | 52.23 ± 10.55 | 49.82 ± 5.57 | .350 | |
| Control | 58.57 ± 8.42 | 58.44 ± 8.10 | .753 | 0.040 | |
| Sleep disturbance | iCanWork | 51.05 ± 10.90 | 47.92 ± 10.61 | 0.173 | |
| Control | 58.66 ± 9.64 | 55.67 ± 8.38 | 0.225 | 0.131 | |
| Social roles and activities | iCanWork | 51.61 ± 1.39 | 51.61 ± 1.39 | .262 | |
| Control | 44.54 ± 6.67 | 43.63 ± 6.14 | .917 | 0.017 | |
| Pain interference | iCanWork | 48.78 ± 8.098 | 49.39 ± 8.249 | 0.735 | |
| Control | 58.14 ± 10.237 | 61.47 ± 6.265 | 0.893 | 0.006 | |
| Pain intensity | iCanWork | 2.70 (3.03) | 1.83 (2.41) | 0.262 | |
| Control | 3.80 (2.52) | 5.43 (2.15) | 0.202 | 0.036 |
Mean ± SD; a Higher scores represent a higher level of functioning, well-being, quality of life, work ability, and work functioning; b *p = < 0.05 (significance levels between the adjusted mean scores of the control and experimental groups after intervention). c Overall quality-of-life score is the PROMIS-Preference (PROPr) score, which provides a preference-based summary score for health states defined by 7 PROMIS domains. It ranges from −0.022 to 1.00. d PROPr sub-domain values are reported as T-scores with a mean of 50.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



