
Submitted:
27 June 2025
Posted:
02 July 2025
You are already at the latest version
Abstract
Background: Occupational resilience (OR) is an emerging construct defined as the degree of persistence in any specified activity. Given that persistence in activities is the key determinant of both the manner and extent to which activities influence health, OR is a promising novel construct. However, there are currently no validated OR measures, making it difficult for researchers and clinicians to apply the construct. Methods: Drawing from previously published qualitative research and established theories on activity performance, the Occupational Resilience Measure (ORM 1.0) was developed and tested with graduate occupational therapy students. Subsequently, six expert clinicians evaluated the ORM using an anonymous online survey. Results: Participants determined that ORM 1.0 demonstrates validity for the construct it assesses. They also suggest that ORM 1.0 is clinically relevant and a unique evaluation instrument. Discussion: The ORM 1.0 instrument comprises 20 items, which produce an aggregate score ranging from 20 to 100, along with four subtest scores corresponding to the variables History, Experience, Benefits, and Adaptation. Subtest scores facilitate the identification of variables that exert a more pronounced impact on the overall ORM 1.0 score, allowing ORM measurements to inform intervention strategies in clinical practice. ORM scores have potential for application in predicting health outcomes in epidemiological studies. Although ORM 1.0 may need further refinement, it has considerable potential to contribute significantly to advances in clinical practice and scientific research in a unique way.
Keywords:
occupational resilience
; occupational identify
; lifestyle change
; habituation
; activity persistence
; perseverance
; addiction
; adaptation
1. Introduction
An individual’s capacity to persist in the performance of an activity is termed occupational resilience (OR) [1]. OR is the principal factor determining the extent to which an activity influences health; yet there are no validated and reliable measures of the construct that are usable across activity types and contexts. To appreciate the significance of OR, the key factors that determine how activities influence health must be understood.
The most prominent factor is the activity type. For example, within the range of associated health risks, engagement in smoking and alcohol consumption have been linked to significantly higher prevalence of lung cancer (Centers for Disease Control and Prevention, 2024) and liver disease [2] respectively. While some activities are associated with negative health, others are known to improve health. These may include physical activity [3,4], personal hygiene [5], social interaction [6], and religious activities [7,8,9] among others.
Activities possess a variety of mechanisms of action through which they influence health. Consequently, based on the nature of an activity, certain activities may serve as substitutes for others due to similarities in operational mechanisms. Hiking can operate similarly to dancing, biking, or exercising on fitness machines. These activities offer resistance, facilitate the mobilization of joints and muscles, and promote caloric expenditure. Certain types of activities possess a limited or unique set of mechanisms of action. For instance, sleep is unique in that it restores neural functioning and takes away sleep debt that accumulates during wakefulness [10,11]. Leisure and recreational activities encompass numerous mechanisms of action [12]. Routine activities like personal hygiene may be mundane and become easily taken for granted. Nonetheless, research has demonstrated that these activities exert a substantial impact on health [5,13], and the variability in their mechanisms of action is likely considerable.
In addition to activity type, the level of intensity at which individuals engage in an activity considerably influences health outcomes. Research shows low smoking levels have a weaker link to lung cancer than moderate to very high levels [14,15]. Similarly, scholars differentiate between heavy and light drinking regarding alcohol's health effects (Boersma et al., 2020), highlighting the importance of considering intensity.
The third essential activity factor that shapes health outcomes is the degree of persistence. An individual with high persistence will continue an activity over time, resisting significant barriers such as limited finances, time constraints, illness or disability, aging, and environmental changes. The barriers to such activities inevitably occur as people advance through life stages and embrace changing roles. High persistence might lead to ongoing involvement in activities despite risks; for example, sharing needles to use drugs despite the risk of contracting HIV [16].
As high OR in certain activities may lead to addiction, there probably exists a bidirectional relationship between high OR and addiction. It is now understood that activities that may initially be performed due to social influences can lead to physiological dependence or addictions that perpetuate engagement as a result of addiction. Literature reveals some of these activities: gambling [17], alcohol use [15], work [18], social media use [19], and internet use [20] among others. Such activities result in individuals engaging in activities despite their strong desire to stop. A high OR score may, therefore, be a result of addiction.
The level of intensity and duration do not have a linear relationship with OR, but they shape OR in evolving and dynamic ways. The activity type answers the question: OR in what? Duration considers the length of time of involvement, which can potentially lead to eventual addiction in applicable scenarios (e.g., substances, gambling, and sexual activities, etc.). Intensity is determined by the amount or quantity in some quantifiable form, such as number of cigarettes, volume of alcohol, and hours of exercise. The significant variations in OR between people and across activities, lead to notable differences in health status between people during COVID-19 lockdowns [4,13]. Accurate measurement of OR may predict health status, but studies are needed to validate this hypothesis across activities and populations.
- Occupational Resilience Construct and its Significance
OR represents a novel construct that emerged from the field of occupational therapy. Everyday activities are termed occupations; they occupy people with meaningful tasks that require time investment and are either voluntarily chosen or mandated [21,22]. While the term 'activity' is sometimes differentiated from 'occupation'[21,23,24], in this paper, the two terms are used interchangeably.
In interdisciplinary literature OR is associated with employment and careers. It refers to the capacity of individuals to persist in certain professions; for example, police [25], physicians [26], and nurses [27]. This understanding of occupational resilience originates from understanding occupation as a profession or vocation. One assessment used to measure occupational resilience understood in this way is Connor-Davidson Resilience Scale [28].
In this paper, the term occupation, as defined in the occupational therapy literature, applies. It encompasses the full spectrum of meaningful, everyday activities that individuals engage in as part of their daily living [21,29,30]. Subsequently, OR refers to “the capacity for persistence in the performance of an occupation [i.e., any activity], where capacity is examined from both duration and intensity of engagement in a specified occupation” [1].
The key benefit of ORM 1.0 is its ability to quantify OR, in contrast to the traditional use of descriptors such as very low, low, moderate, high, and very high [2,14]. This allows it to potentially help evaluate the effectiveness of interventions designed to improve OR. Such quantified scores can also be applied to determine the range of scores within which health challenges, or health benefits, associated with an activity emerge. Epidemiological studies using this measure can guide public health policies by identifying OR score ranges that indicate concern for negative health outcomes or aspirations for positive ones.
In evaluating OR, it is highly recommended to consider the intricate tapestry of occupations that collectively weave the individual’s life narrative. An activity can either vie for scarce time and resources or offer support. For example, unemployment might severely limit recreational pursuits, while the reverse situation proves equally valid.
- Developing the Occupational Resilience Measure (ORM 1.0)
The development of the Occupational Resilience Measure (Version 1 is called ORM 1.0) was predicated on the assumption that universal principles underpin persistence across all human activities. This assumption is based upon two considerations: a naturalistic study identified five factors that engender persistence (Muriithi & Muriithi, 2023, 2025) and known theories that have associated constructs linked to activity persistence that align with these factors.
The use of qualitative studies to guide instrument development has been endorsed by experts [31]. The referenced qualitative study described lived experiences of refugee musicians who had been displaced from their home countries, but they persisted in music performance across several countries, including the United States. According to [32,33] the factors contributing to their persistence in music performance include: 1) History (long-term participation in the activity leading to identity as musicians); 2) Benefits (desirable effects of the activity); 3) Experience (competence, talent, leading to social recognition); 4) Adaptation (changing to deal with environmental barriers); and 5) Environment (opportunities provided by local environment). As shown in Figure 1, only the first 4 individual-related factors were considered in the development of the ORM, excluding Environment, as the tool assesses a trait that can overcome environmental challenges to enable persistence.
It is also recommended to consider theory in instrument development [31]. We evaluated relevant theories to determine the degree to which the factors in [32,33] corresponded with measurable and modifiable variables already associated with activity performance or persistence. We found strong links between these 4 factors and a variety of constructs of which examples are provided in Table 1. The links between these four factors and constructs in occupation-focused theories increased confidence that the 4 factors can be considered as variables that are measurable, modifiable, and relevant for clinical practice and research. Additionally, this strengthened our belief that these 4 factors could constitute distinct and meaningful domains for the proposed measure. Furthermore, the theories and associated measures provided considerable insight into the formulation of a suitable scale. ORM 1.0 uses a Likert-type scale, which is oft used in measuring related constructs (e.g., Occupational Self-Assessment [34], and Canadian Occupational Performance Measure [35]. ORM 1.0 was designed to follow similar procedures for administration, scoring, and interpretation. The scale is straightforward and suitable for self-administration; however, it is essential that relevant activities are carefully identified, if necessary, with a clinician guiding the process.
The 4 factors discussed in [32,33] were developed as subscales of ORM 1.0, with 20 total items included. The number of items in each subscale were based on domain coverage rather than equalizing them across subscales. The numbers of items were 5, 5, 6, 4 for History, Experience, Benefits, and Adaptation subscales respectively. All items used the same Likert-type scale [Strongly Disagree = 1; Disagree = 2; Neutral = 3; Agree = 4 & Strongly Agree = 5]. Consequently, although the total ORM 1.0 scores spanned from 20 to 100, the maximum scores for individual subscales differed, with the History and Experience subscales each having a maximum score of 25, the Benefits subscale a maximum score of 30, and the Adaptation subscale a maximum score of 20.
Thus, ORM 1.0 is multidimensional, integrating 4 domains related to the sustained performance of activities into a unified assessment instrument. This approach is informed by facet theory, which posits that constructs analogous to OR are most effectively assessed through a formative amalgamation of scores derived from multiple dimensions [36,37].
After the development of ORM 1.0, it underwent testing with two cohorts of doctoral students in occupational therapy, yielding promising outcomes. Only three items needed to be edited for improved comprehensibility between the two tests. In these tests, students were asked, considering long-term personal experience, to self-administer ORM for activities they regularly did, those they occasionally did, and those they never or rarely did. Scores varied extensively in these tests, suggesting ORM 1.0 scores potentially conveyed one’s degree of persistence in an activity as was intended.
This paper is part of a series of papers that will establish the essential properties of the ORM 1.0. The article describes the construct OR and provides justification for its measurement. It also describes the process of ORM 1.0 development. Furthermore, the article reports opinions of experts who responded to a survey designed to answer the question: to what extent will occupational therapy professionals regard ORM 1.0 as clinically relevant, unique, and valid for measuring OR?
2. Materials and Methods
The study received approval from the Institutional Review Board (IRB) at A. T. Still University of Health Sciences (Exempt Protocol #2021-191), categorizing it as minimal risk. Data were collected from six occupational therapy experts. Occupational therapists are known for their use of everyday activities (occupations), as the means and ends of intervention [21,22,38]. Hence, they were regarded as the most suitable healthcare professionals to consult for the content validation of ORM 1.0. Experts in the field consulted during the validation of assessment tools should be the most knowledgeable professionals in the specific area of study [31,39,40].
- Data collection
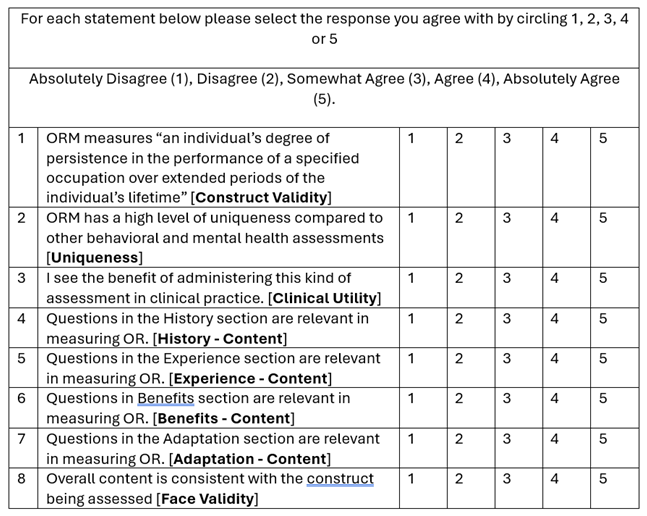
Participants were occupational therapy clinicians with at least 10 years of assessment experience in clinical practice, who also teach in masters or doctoral programs at academic institutes in USA; and have a Ph.D. or OTD. The participants were purposively selected to ensure that only individuals with the adequate capacity to evaluate the scale were involved. A package was disseminated to participants via email. It comprised a copy of the assessment, justification for the new assessment, guidelines for administration, scoring, and interpretation of results. Instructions to administer the assessment prior to completing an online survey were also included. The Qualtrics platform was used to administer the anonymous survey, asking participants to answer the questions listed in Table 2.
- Data Analysis
The analysis was primarily descriptive; no inferential analysis was planned for this study. Descriptive statistics were summarized as frequency (percentage) for each of the eight questions in the survey and presented using a stacked bar diagram.
3. Results
The survey response rate was 60%, with 6 out of 10 invited participants successfully submitting a completed anonymous survey facilitated through the Qualtrics platform. One participant did not complete the entire survey and was excluded from the analysis. The distribution of agreement categories across each of the survey questions is presented in Figure 2.
The assessment of content and face validity, as reflected in items 1 and 8 in Table 2, yielded identical ratings for both surveyed items, with distributions as follows: Absolutely Agree (67%), Agree (17%), and Somewhat Agree (17%). With respect to uniqueness (item 2 in Table 2), ORM 1.0 is perceived as a unique measure, as evidenced by ratings of Absolutely Agree (50%) and Agree (50%). Participants perceived the administration of ORM 1.0 within clinical practice as beneficial, as evidenced by the Clinical Utility ratings: Absolutely Agree (50%), Agree (33%), and Somewhat Agree (17%). Participants were tasked with evaluating items 4 through 7 (referenced in Table 2) to determine the extent to which individual test items corresponded with the underlying construct being assessed. Figure 2 demonstrates that participants deemed items within each subscale relevant to the construct under examination. Nevertheless, the Experience subscale received marginally more favorable ratings (Absolutely Agree (67%), Agree (33)%) in comparison to the other three subscales, which were rated Absolutely Agree (67%), Agree (17%), and Somewhat Agree (17%).
4. Discussion
This paper justifies the need for a new assessment and describes the process of developing ORM 1.0 for measuring OR. The paper describes the whole process, ending with a presentation of outcomes of a brief survey that conveys the opinions of six scholar-clinicians who evaluated ORM 1.0. Having emerged as a construct in a qualitative study describing the lived experiences of refugee musicians [41], OR was later expounded as a general construct that applies to all people, all activities, and all contexts [1]. A re-examination of the same data revealed that five factors shaped OR in the case of refugee musicians [32,33]. After excluding the Environment factor, which is not a personal attribute, the remaining 4 factors were developed as subscales of ORM 1.0, creating a multidimensional instrument.
The consideration of theory in ORM 1.0 development was highly beneficial. It helped to discover that History, Experience, Benefits, and Adaptation align with known constructs associated with persistent activity performance in occupation-based theories. As indicated in Table 1, habituation and occupational identity closely reflect the History factor. Similarly, the Experience factor closely aligns with occupational competence [42], relative mastery [43,44], and occupational performance [23]. Strong congruence between all 4 factors and constructs known to be measurable and modifiable was a meaningful observation. We had high confidence that a measure grounded in these factors would be a strong predictor of persistence in any specified activity and potentially also a predictor of health.
OR results may be used in clinical practice and research in several ways. Firstly, they may be used, assuming OR is a modifiable variable [1], as an outcome measure in clinical practice and experiments. One conceivable method of optimizing OR is addressing each of the 4 integrated variables that shape OR—History, Experience, Benefits, and Adaptation—either concurrently or sequentially. Secondly, ORM 1.0 scores could possibly be used in predicting health when the activity is specified and its health effects are known. OR scores may reveal, for example, the range of scores for alcohol consumption that is considerably detrimental to health, making it usable in epidemiological research.
That OR is modifiable is a hypothesis that requires empirical testing. Literature on lifestyle change programs shows that addressing persistence in activity is usually part of such interventions, and specific activities have been targeted because of their known effects of health (e.g., physical activity [45,46], healthy eating [47], mindfulness [48]). Utilizing ORM 1.0 to evaluate activity performance outcomes presupposes that the resultant changes will manifest at a magnitude discernible by this measure, a proposition that needs empirical validation as well. Because ORM 1.0 is a multidimensional scale with scores ranging from 20 to 100, it appears likely that it would detect even relatively small changes in OR that may occur as a result of an intervention or a lifestyle change.
ORM 1.0's multidimensional nature is crucial for clinical practice. The provision of subscale scores enables clinicians to discern the specific domain(s) in which a client demonstrates either weakness or strength, thereby facilitating more targeted interventions. A client who obtains low scores in the History subscale, for instance, indicates limited or inconsistent patterns in participation in an activity. According to Kielhofner’s definitions (2008), habituation [measurable and modifiable] and occupational identity [develops with performance] strongly align with this factor. For such clients, interventions that build habits and routines can foster sustained participation to improve History scores. One example of an intervention that is known to address deficits in the History domain is Lifestyle Redesign [49]. Such interventions cultivate healthy habits and routines that are, in theory, expected to develop occupational identity [42].
An individual receives low scores in the Experience subscale if they have limited experience or restricted performance skills. In the referenced theories, associated constructs are measurable and/or modifiable: occupational performance [23], relative mastery [43] and occupational competence [42]. When skills are severely limited due to illness, developmental challenges, or inexperience, building performance skills can become the key area of focus in intervention planning. Rehabilitation specialists apply various known strategies in developing activity performance skills.
Low scores in the Benefits subscale signify low motivation, a lack of meaning, or low interest in a specified activity. Volitional Questionnaire [50] is one of the tools that have been used to evaluate this factor. Some evidence-based interventions that address this factor include Motivational Interviewing [51] and Cognitive Behavioral Therapy [52] among others.
A person who lacks creativity and problem-solving skills will likely get low scores in the Adaptation subscale. Numerous assessments are available evaluating cognitive functions associated with adaptation, and rehabilitation specialists have applied both cognitive rehabilitation [to improve cognition] and cognitive adaptation [adapt environment or task]. Evidence shows that deficits in attention, memory, and executive function can be improved through specific interventions e.g., [53], and such improvements would likely improve scores in the Adaptation subscale.
Although ORM 1.0 scores can be meaningful in clinical practice and research, they must be interpreted with caution. The link between OR and health cannot be simply labeled as positive or negative. Occupations typically linked to positive health can result in negative consequences if done at the wrong time or context. For example, when engaged in at an appropriate time and context, sexual activity serves as a generally beneficial human occupation. However, it has led to teen pregnancy becoming a public health issue across various nations [54]. Similarly, work, an activity generally associated with positive health outcomes, has been implicated in the emergence of health issues associated with burnout [55,56]. On the other hand, an activity commonly linked to negative health effects, such as alcohol consumption, may not pose significant health risks when undertaken infrequently or when alcohol is consumed in modest quantities [14]. This underscores the importance of considering both the intensity and duration, as these factors—far more than the mere classification of the activity itself as health or unhealthy—play a profound role in determining the ultimate impact on one's health outcomes.
ORM 1.0 is designed to measure OR in all forms of activity – healthy and unhealthy. Evaluating all activities using the same scale is consistent with an emerging, more inclusive understanding of occupation. The concept 'dark side of occupation', which is gaining traction in occupational science, encourages us to embrace a broader perspective of occupation [57]. Applying one measure for all activities is in some way to acknowledge that all activities belong to the same family of phenomena – things that people do and consider meaningful. However, ‘meaningful’ is not necessarily ‘healthy’. Activities that are illegal, addictive, taboo, and unhealthy need to be studied, measured, and addressed in scientific research [57,58,59]. Perhaps greater understanding of such activities will in the future help to improve the approaches being applied to optimize health and well-being. Through its ability to quantify OR across activity types, ORM 1.0 holds potential to illuminate the intricate and dynamically changing ties between activity participation and health.
- Limitations
While the manuscript introduces the first iteration of ORM 1.0, OR is an emergent construct undergoing theoretical refinements. It is anticipated that future iterations of ORM will also undergo refinements to achieve stronger validity, reliability, and other psychometric properties. Further research is needed to evaluate aspects like test-retest reliability, internal consistency, whether items should be added or removed from the first version etc. In addition, clinical trials will test the degree to which OR is changeable, and how well ORM 1.0 detects change resulting from interventions. Additionally, more studies will reveal if ORM 1.0 will have significant value in various types of studies.
5. Conclusions
This article describes the steps taken to develop a new measure of OR, an innovative construct that has been defined herein. The structure of the proposed measure and potential applications were substantiated. Quantifiable survey results from experts indicated high agreement, contributing to the establishment of ORM 1.0 as a valid, clinically relevant, and unique measure. Further research is needed to strengthen the measure and to test the proposed applications in clinical practice, clinical trials, and in epidemiological studies.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, B.M.; methodology, B.M.; formal analysis, B.M. and M.B.; investigation, B.M.; data curation, M.B and B.M.; writing—original draft preparation, B.M.; writing—review and editing, B.M. and M.B.; visualization, B.M. and M.B.; project administration, B.M.; funding acquisition, B.M. All authors have read and agreed to the published version of the manuscript.
Funding
Research reported in this publication was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under award number K12TR004924. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board A. T. Still University of Health Sciences (Protocol #2021-191, September 22, 2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Acknowledgments
We want to thank Mario Schootman (Translational Research Institute, University of Arkansas for Medical Sciences) for his presubmission review and recommendations that were helpful in improving the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Muriithi, B. A. K.; Muriithi, J.; Jyothi, G.; Radziak, J.; Story, A. Occupational resilience: Construct and practice implications in occupational therapy [preprint]. Research Square 2022. [CrossRef]
- Boersma, P.; Villarroel, M. A.; Vahratian, A. Heavy drinking among U.S. adults, 2018; NCHS Data Brief, no 374. Hyattsville, MD: National Center for Health Statistics. 2020. https://www.cdc.gov/nchs/products/databriefs/db374.htm.
- Chi, X.; Liang, K.; Chen, S.-T.; Huang, Q.; Huang, L.; Yu, Q.; Jiao, C.; Guo, T.; Stubbs, B.; Hossain, M. M.; et al. Mental health problems among Chinese adolescents during the COVID-19: The importance of nutrition and physical activity. Int. J. Clin. Health Psychol. 2021, 21 (3), 100218-100210. [CrossRef]
- Killgore, W. D. S.; Taylor, E. C.; Cloonan, S. A.; Dailey, N. S. Psychological resilience during the COVID-19 lockdown. Psychiatry Res. 2020, 291, 2, Letter. [CrossRef]
- de Oliveira Almeida, K.; Nogueira Alves, I. G.; de Queiroz, R. S.; de Castro, M. R.; Gomes, V. A.; Santos Fontoura, F. C.; Brites, C.; Neto, M. G. A systematic review on physical function, activities of daily living and health-related quality of life in COVID-19 survivors. Chronic Illness 2023, 19 (2), 279-303. [CrossRef]
- Baumeister, R. F.; Leary, M. R. The need to belong: Desire for interpersonal attachments as a fundamental human motivation. Psychol. Bull. 1995, 117 (3), 497, Article. [CrossRef]
- Balboni, T. A.; VanderWeele, T. J.; Doan-Soares, S. D.; Long, K. N. G.; Ferrell, B. R.; Fitchett, G.; Koenig, H. G.; Bain, P. A.; Puchalski, C.; Steinhauser, K. E.; et al. Spirituality in serious illness and health. JAMA 2022, 328 (2), 184-197. [CrossRef]
- Idler, E.; Jalloh, M. F.; Cochrane, J.; Blevins, J. Religion as a social force in health: Complexities and contradictions. BMJ (Online) 2023, 382, e076817-e076817. [CrossRef]
- King, D. G. Religion and health relationship: A review. J. Religion Health 1990, 29 (2), 101. [CrossRef]
- Khazaie, H.; Najafi, F.; Chehri, A.; Rahimi-Movaghar, A.; Amin-Esmaeili, M.; Moradi-Nazar, M.; Zakiei, A.; Pasdar, Y.; Ahmadi, A.; Mohammadi, R. Circadian rhythm sleep disorders in the young population and their relationship with psychological distress and disability. J. Turk. Sleep Med. 2023, 10 (3), 199-205, Article. [CrossRef]
- Matricciani, L.; Paquet, C.; Galland, B.; Short, M.; Olds, T. Children's sleep and health: A meta-review. Sleep Med. Rev. 2019, 46, 136-150. [CrossRef]
- Fancourt, D.; Aughterson, H.; Finn, S.; Walker, E.; & Steptoe, A. How leisure activities affect health: A narrative review and multi-level theoretical framework of mechanisms of action. The Lancet. Psychiatry 2021. [CrossRef]
- Muriithi, B. A. K.; Bay, R. C. The effects of occupational disruption during COVID-19 lockdowns on health: A cross-sectional study. PeerJ 2024, 12, e17594. [CrossRef]
- Roy, P.; Laha, A. K. Understanding Lung Cancer: Tobacco Smoking Linkage; SAGE Publications: Thousand Oaks, CA, USA, 2017.
- Karlsson, H. From social drinking to alcohol addiction: Decision making and its neural substrates along a spectrum from social drinking to alcohol addiction. Doctoral Thesis, Linköping University Electronic Press, 2024. [CrossRef]
- Ball, L. J.; Puka, K.; Speechley, M.; Wong, R.; Hallam, B.; Wiener, J. C.; Koivu, S.; Silverman, M. S. Sharing of injection drug preparation equipment is associated with HIV infection: A cross-sectional study. J. Acquir. Immune Defic. Syndr. 2019, 81 (4), e99-e103. [CrossRef]
- Potenza, M. N.; Balodis, I. M.; Derevensky, J.; Grant, J. E.; Petry, N. M.; Verdejo-Garcia, A.; Yip, S. W. Gambling disorder. Nat. Rev. Dis. Primers 2019, 5 (1), 51-51. [CrossRef]
- Bereznowski, P.; Atroszko, P. A.; Konarski, R. Work addiction, work engagement, job burnout, and perceived stress: A network analysis. Front. Psychol. 2023, 14, 1130069. [CrossRef]
- Xiao, W.; Peng, J.; Liao, S. Exploring the associations between social media addiction and depression: Attentional bias as a mediator and socio-emotional competence as a moderator. Int. J. Environ. Res. Public Health 2022, 19 (20), 13496. [CrossRef]
- Adams, M. E. Internet Addiction: Prevalence, Risk Factors and Health Effects; Nova Publications: Hauppauge, New York, USA, 2017.
- American Occupational Therapy Association. Occupational therapy practice framework: Domain and process (4th ed.). Am. J. Occup. Ther. 2020, 74 (Suppl. 2), 7412410010. [CrossRef]
- World Federation of Occupational Therapists. About occupational therapy. Available online: https://wfot.org/about/about-occupational-therapy (accessed on 8 March 2025).
- Townsend, E. A.; Polatajko, H. J. Enabling Occupation II: Advancing an Occupational Therapy Vision for Health, Well-being, & Justice Through Occupation; CAOT Publications ACE: Ottawa, Canada, 2007.
- Pierce, D. Untangling occupation and activity. Am. J. Occup. Ther. 2001, 55 (2), 138-146. [CrossRef]
- Chitra, T.; Karunanidhi, S. The impact of resilience training on occupational stress, resilience, job satisfaction, and psychological well-being of female police officers. J. Police and Criminal Psychol. 2021, 36 (1), 8-23, Article. [CrossRef]
- West, C. P.; Dyrbye, L. N.; Sinsky, C.; Trockel, M.; Tutty, M.; Nedelec, L.; Carlasare, L. E.; Shanafelt, T. D. Resilience and burnout among physicians and the general US working population. JAMA Network Open 2020, 3 (7), e209385. [CrossRef]
- Babanataj, R.; Mazdarani, S.; Hesamzadeh, A.; Gorji, M. H.; Cherati, J. Y. Resilience training: Effects on occupational stress and resilience of critical care nurses. Int. J. Nurs. Prac. 2019, 25 (1), e12697-n/a. [CrossRef]
- Connor, K. M.; Davidson, J. R. T. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depress. Anxiety 2003, 18 (2), 76-82. [CrossRef]
- Hinojosa, J.; Kramer, P. Statement - Fundamental concepts of occupational therapy: Occupation, purposeful activity, and function. Am. J. Occup. Ther. 1997, 51 (10), 864-866. [CrossRef]
- Clark, F. A.; Carlson, M. E.; Jackson, J.; Wolfe, R. J.; Parham, D.; Frank, G.; Pierce, D.; Zemke, R. Occupational science - Academic innovation in the service of occupational therapy’s future. Am. J. Occup. Ther. 1991, 45 (4), 300-310. [CrossRef]
- Streiner, D. L.; Norman, G. R.; Cairney, J. Health Measurement Scales: A Practical Guide to their Development and Use; Oxford University Press: Oxford, UK, 2015.
- Muriithi, B. A. K.; Muriithi, J. A qualitative exploration of relations between salutogenesis and persistent music performance among refugees resettled in the United States. Int. J. Environ. Res. Public Health 2025, 22 (1), 9. [CrossRef]
- Muriithi, B. A. K.; Muriithi, J. Lived experience of refugee musicians: Factors that enable performance of music among resettled immigrants facing what can be unsurmountable barriers. Am. J. Occup. Ther. 2023, 77 (Supplement_2), 7711505004-7711505004p7711505001. [CrossRef]
- Popova, E. S.; Ostrowski, R. K.; Wescott, J. J.; Taylor, R. R. Development and validation of the Occupational Self-Assessment-Short Form (OSA-SF). Am. J. Occup. Ther. 2019, 73 (3), 7303205020p7303205021-7303205020p7303205010. [CrossRef]
- Canadian Association of Occupational Therapists. About COPM. Canadian Association of Occupational Therapists. Available online: https://www.thecopm.ca/about/ (accessed 23 January 2025).
- Guttman, L. Measurement as structural theory. Psychometrika 1971, 3 (4), 329-347.
- Guttman, R.; Greenbaum, C. W. Facet theory: Its development and current status. European Psychologist 1998, 3 (1), 13-36. [CrossRef]
- McLaughlin Gray, J. Putting occupation into practice: Occupation as ends, occupation as means. Am. J. Occup. Ther. 1998, 52 (5), 354-364. [CrossRef]
- Boateng, G. O.; Neilands, T. B.; Frongillo, E. A.; Melgar-Quinonez, H. R.; Young, S. L. Best practices for developing and validating scales for health, social, and behavioral research: A primer. Front. Public Health 2018, 6, 149-149. [CrossRef]
- De Vet, H. C. W.; Terwee, C. B.; Mokkink, L. B.; Knol, D. L. Measurement in Medicine; Cambridge University Press: Cambridge, UK, 2018.
- Muriithi, B.; Muriithi, J. Occupational Resilience: A new concept in occupational science. Am. J. Occup. Ther. 2020, 74 (S1), 7411505137-7411505137p7411505131. [CrossRef]
- Kielhofner, G. Model of Human Occupation: Theory and Application; Wolters Kluwer: Baltimore, MD, USA, 2008.
- Schkade, J. K.; Schultz, S. Occupational adaptation: Toward a holistic approach for contemporary practice, Part 1. Am. J. Occup. Ther. 1992, 46 (Sep 92), 829-837. [CrossRef]
- Schultz, S.; Schkade, J. K. Occupational adaptation: Toward a holistic approach for contemporary practice, Part 2. Am. J. Occup. Ther. 1992, 46 (10), 917-925. [CrossRef]
- Rippe, J. M. Lifestyle Medicine; CRC Press, Boca Raton, FL, USA, 2024.
- Radenkovic, D.; Aswani, R.; Ahmad, I.; Kreindler, J.; Robinson, R. Lifestyle medicine and physical activity knowledge of final year UK medical students. BMJ Open Sport & Exercise Med. 2019, 5 (1), e000518-e000518. [CrossRef]
- Rippe, J. M. Nutrition in Lifestyle Medicine; Springer International Publishing, 2017. [CrossRef]
- Sarris, J.; O'Neil, A.; Coulson, C. E.; Schweitzer, I.; Berk, M. Lifestyle medicine for depression. BMC Psychiatry 2014, 14 (1), 107-107. [CrossRef]
- Pyatak, E. A.; Carandang, K.; Collins, C. R.; Carlson, M. Optimizing occupations, habits, and routines for health and well-being with Lifestyle Redesign®: A synthesis and scoping review. Am. J. Occup. Ther. 2022, 76 (5). [CrossRef]
- Chern, J. S.; Kielhofner, G.; de las Heras, C. G.; Magalhaes, L. C. The Volitional Questionnaire: Psychometric development and practical use. Am. J. Occup. Ther. 1996, 50 (7), 516-525. [CrossRef]
- Miller, W. R.; Rollnick, S. Motivational Interviewing: Helping People Change and Grow, 4th ed.; The Guilford Press: New York, USA, 2023.
- Beck, J. S. Cognitive Behavior Therapy: Basics and Beyond; The Guilford Press: New York, USA, 2021.
- Manzine, P. R.; Pavarini, S. C. I. Cognitive rehabilitation: Literature review based on levels of evidence. Dementia & neuropsychologia 2009, 3 (3), 248-255. [CrossRef]
- Dutton, S.; Mamun, M. S. A.; Davison, C. M. Exploring teen pregnancy as a public health problem: A critical scoping review of public health research on teen pregnancy in Canada. Societies 2024, 15 (1), 1. [CrossRef]
- Atroszko, P. A.; Demetrovics, Z.; Griffiths, M. D. Work addiction, obsessive-compulsive personality disorder, burn-out, and global burden of disease: Implications from the ICD-11. Int. J. Environ. Res. Public Health 2020, 17 (2), 660. [CrossRef]
- World Health Organization. Burn-out an "occupational phenonenon": International Classification of Diseases. Available online: https://www.who.int/news/item/28-05-2019-burn-out-an-occupational-phenomenon-international-classification-of-diseases (accessed on 21 January 2025).
- Twinley, R. Illuminating the Dark Side of Occupation : International Perspectives from Occupational Therapy and Occupational Science; Routledge, 2021.
- Twinley, R.; Addidle, G. Considering violence: The dark side of occupation. Br. J. Occup. Ther. 2012, 75 (4), 202-204. [CrossRef]
- Twinley, R. The dark side of occupation: A concept for consideration. Aust. Occup. Ther. J. 2013, 60 (4), 301-303. [CrossRef]
Figure 1.
Structure and Domains of ORM 1.0.
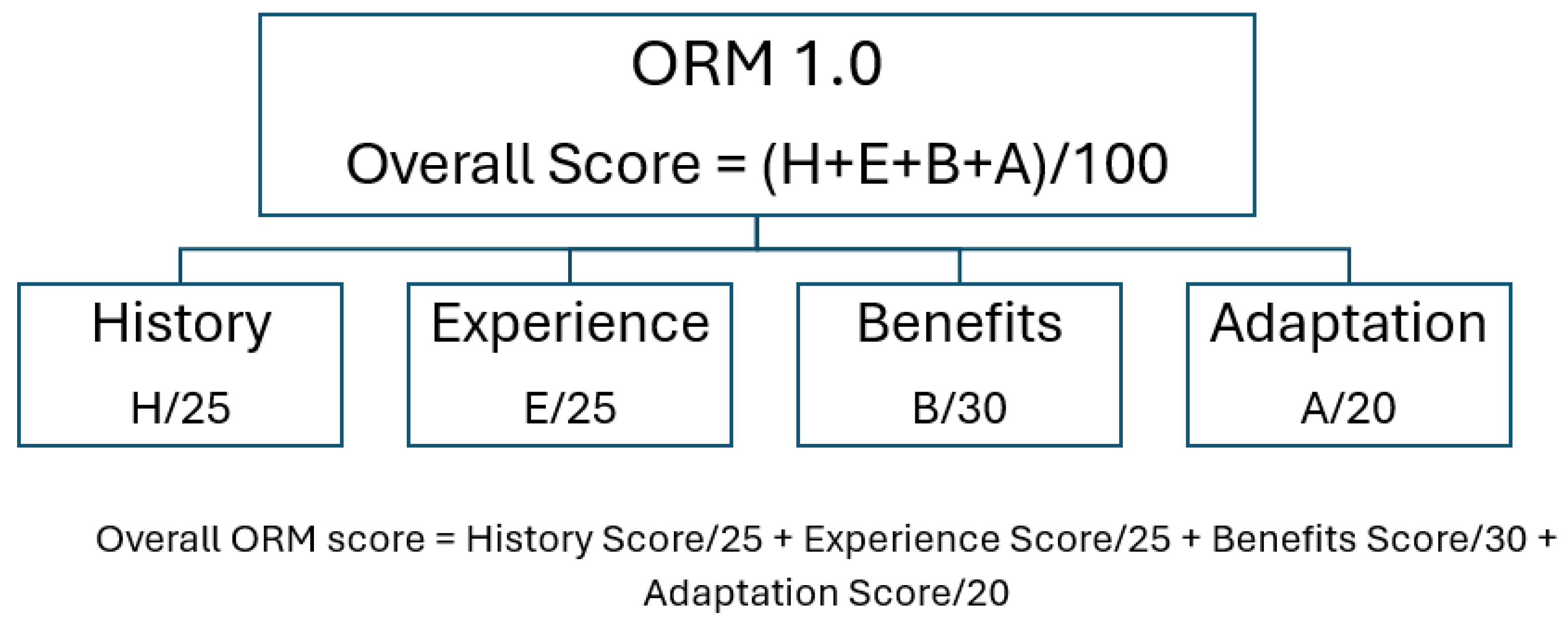
Figure 2.
Survey Results.
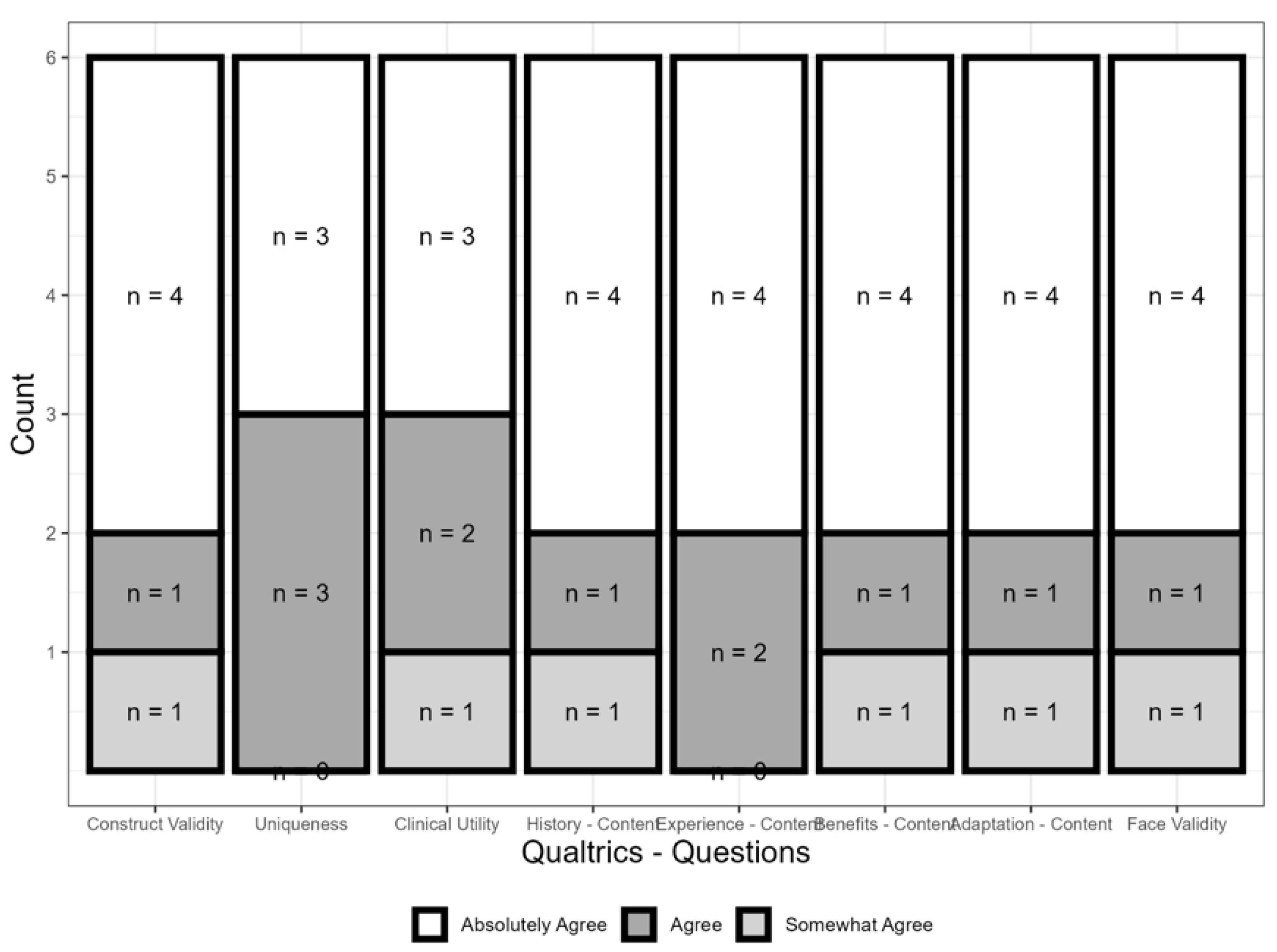

Table 1.
ORM 1.0 Domains and related constructs.
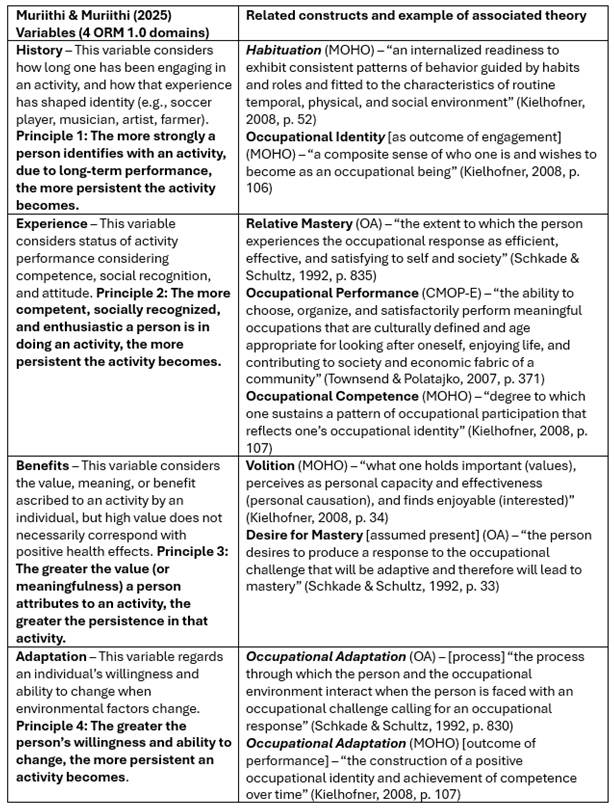 |
Table 2.
Survey Questions.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



